
Submitted:
20 June 2023
Posted:
21 June 2023
You are already at the latest version
Abstract
Background: Sarcoma may show similarities to malignant melanoma in terms of morphologic and immunohistochemical aspects, hence making it difficult to differentiate between these two neoplasms during the diagnostic process. This systematic review aims to summarize available evidence on cases of sarcoma that were initially diagnosed as melanoma. Methods: A comprehensive search was conducted including MEDLINE/Pubmed, EMBASE and SCOPUS through March 2023. We included case series and case reports of sarcoma patients that were initially diagnosed as malignant melanoma. PRISMA guidelines were followed. Results: Twenty-three case reports and four case series with a total of 34 patients were included. The clinical presentation was heterogeneous, and the most involved anatomical regions were lower limbs (24%), head/neck (24%) and upper limbs (21%). IHC positivity was reported for S100 (69%), HMB45 (63%), MelanA (31%) and MiTF (3%). The main reasons for second assessment were unusual presentation (48%) and uncertain diagnosis (28%). EWSR1 translocation was investigated in 17/34 patients (50%) and found positive in 16/17 (94%). The final diagnosis was clear cell sarcoma (50%) or other soft tissue sarcomas (50%). Conclusions: Melanoma and some histotypes of sarcoma share many similarities. In case of atypical lesions, a second diagnosis should be considered, and ESWR1 translocation should be investigated.
Keywords:
Melanoma
; Sarcoma
; Mimicking.
1. Introduction
The 2020 World Health Organization (WHO) Classification of Soft Tissue Tumors indicates sarcomas as rare tumors that are further subclassified in approximately 70 subtypes, each characterized by a distinct morphology, that often translates into a specific clinical behavior as well as into specific therapeutic approaches [1,2]. They can occur anywhere in the body, affecting the extremities in 50% of cases, the trunk and retroperitoneum in 40%, and the head and neck in 10% [3].
Of note, some of these neoplasms can be confused with cutaneous melanoma since they share similar clinical, histological, and immunohistochemical features [4]. In addition, they are rare tumors that are often overlooked by the clinician who does not pose the diagnostic suspicion to the pathologist [2,5,6]. Therefore, health care specialists may encounter some difficulties in differentiating between sarcoma and melanoma during the diagnostic process. For example, clear cell sarcoma (CCS) clinically presents as a deep and small (<5 cm) soft tissue lesion, often juxtaposed with tendons, fascia, or aponeurosis, which may mistakenly suggest some forms of melanoma such as acral melanoma, nodular melanoma, or amelanotic melanoma [7,8]. Moreover, CCS shows a phenotype identical to that of conventional melanoma, characterized by strong expression of S100 protein in 100% of cases and variable expression of HMB-45, Melan-A, and MiTF. As a matter of fact, CCS can be genetically differentiated from melanoma due to some peculiarities, including i) the typical reciprocal translocation t(12;22) (q13;q12) that gives rise to the EWSR1-ATF1 oncogene and ii) the absence of BRAF/NRAS mutations that can often characterize melanoma [4]. Other examples include malignant peripheral nerve sheath tumor (MPNST) and Kaposi's sarcoma. MPNST usually arises from peripheral nerves and may be associated with patients with neurofibromatosis type 1 (NF1). The clinical presentation involves the development of a painful and/or rapidly expanding mass with associated neurological deficits. The biological behavior of MPNSTs has been described as unpredictable, and the differential diagnosis includes several tumors, particularly spindle cell/desmoplastic melanoma, which serves as the main differential because of the higher incidence, remarkably similar morphology, and overlapping immunochemical markers [9,10]. Kaposi's sarcoma is typical of immunocompromised patients and may also present as a single papular skin lesion clinically mimicking melanoma, from which can be distinguished by histologic and immunohistochemical appearance [11].
The clinical presentation of such neoplasm may mislead the physician, with potential implications on therapeutic strategy and prognosis. For example, surgical widening of the margins varies according to the neoplasm under treatment (melanoma or sarcoma), chemo-radiotherapy could be offered to sarcoma, but melanoma patients could benefit from a different first-line approach such as immunotherapy or target therapy or both,and sentinel lymph node biopsy is routinely performed in the diagnostic workup of melanoma but is still under debate for soft tissue sarcoma [12,13,14].
Awareness of the similarities between sarcoma and melanoma, and the ability to recognize the two entities play a crucial role in patient care. However, a clinician may have little-to-no direct experience on this matter and may retrieve only limited information from a case report or a small case series.
This systematic review aimed at summarizing available evidence on cases of sarcoma that were initially diagnosed as malignant melanoma, to help clinicians in the diagnostic process, to improve patient care.
2. Materials and Methods
2.1. Study design
This is a systematic review of case series and case reports describing cases of sarcoma that were initially diagnosed as malignant melanoma. The review was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [15]. The review protocol was registered in PROSPERO (CRD42023403882).
2.2. Search strategy
We systematically searched MEDLINE/PubMed, EMBASE, and SCOPUS to detect eligible studies. The search strategy was conducted without language restrictions through March 2023. In PubMed, the following search strategy was used: sarcoma mimicking melanoma OR sarcoma resembling melanoma OR melanoma-like. The search strategy was tailored to conform to the other electronic sources. The lists from each source were joined and the duplicates were removed. Two investigators (FC, AD) separately evaluated titles and abstracts of the records and removed those unfit outside the scope of the review. The full-text of all potentially eligible records were examined to dismiss those not fulfilling the inclusion criteria. Finally, the reference lists of included records were hand-searched to detect further studies of interest. Any disagreement was solved by consensus with a third investigator (PDF). Studies not including human subjects were excluded. No language restrictions were applied.
2.3. Data collection
Two investigators (FC, AD) independently extracted relevant data from the included articles. For each article, study features, patient characteristics, tumor information and outcome measures were collected. A third investigator (ABF) checked the extracted data. Any inconsistency was solved by consensus.
2.4. Assessment of the quality of included studies
The quality of the included studies was assessed according to eight criteria: i) clear criteria for inclusion of the patient(s), ii) valid methods for identification of the initial condition, iii) valid methods for identification of the final condition, iv) in a case series, consecutive inclusion of patients, v) clear reporting of demographics, vi) clear reporting of clinical information, vii) reporting of the time of the second assessment, and viii) reporting of the reason for the second assessment. The criteria were adapted from the Joanna Briggs Institute (JBI) critical appraisal tool [16] to fit the context under evaluation (case series and case reports describing cases of sarcoma that were initially diagnosed as malignant melanoma). Two investigators (FC, MA) independently appraised the risk of bias of the included studies and any inconsistency was solved by consensus with all authors.
2.5. Data synthesis
The selection procedure was presented in a flow-chart. Pertinent data were extracted from included studies and summarized in tables. The inclusion of case reports and very small case series precluded the feasibility of a meaningful metanalysis, hence a narrative synthesis of included studies was conducted.
3. Results
3.1. Search results
The search identified 365 non-duplicated records. After excluding 321 records based on title/abstract, 43 potentially eligible records were retrieved for full text review. Of these, 17 were excluded due to different design (n=4), different topic (n=12) or different participants (n=1). Another two records were excluded because the full-text could not be found. Three additional records were identified via hand search. Finally, 27 records [9,11,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41] were included in the narrative synthesis (Figure 1).
3.2. Narrative synthesis of the findings
The synthesis included 23 case reports (85%) and four case series (15%). Three studies (11%) were published in 1989-2000, seven (26%) in 2001-2011 and 17 (63%) in 2012-2022. Study and patient characteristics are summarized in Table 1 and Table 2.
Overall, the studies reported on a total of 34 patients (aged 12-86 years), including 25 males (74%) and nine females (26%). The initial diagnosis was melanoma (24 patients, 71%) or suspect of melanoma (10 patients, 29%). The clinical presentation was heterogeneous (Table 1) and the involved anatomical regions included lower limbs (8/33 patients, 24%), head/neck (8/33 patients, 24%), upper limbs (7/33 patients, 21%), visceral area (4/33 patients, 12%), trunk (3/33 patients, 9%) and genital area (3/33 patients, 9%) (the information was not available in one patient).
IHC positivity was reported for S100 (22/32 patients, 69%), HMB45 (20/32 patients, 63%), MelanA (10/32 patients, 31%) and MiTF (1/32 patients, 3%).
The reason for second assessment and/or diagnostic re-evaluation included unusual presentation (12/25, 48%), uncertain diagnosis (7/25, 28%), expert opinion (2/25, 8%), no response to treatment (1/25, 4%), search for EWSR1 translocation (1/25, 4%), review after surgery (1/25, 4%) or review after death (1/25, 4%), while the information was not reported in nine patients.
EWSR1 translocation was investigated in 17/34 patients (50%), and found positive in 16 CCS and one MPNST.
The final diagnosis was clear cell sarcoma in 17 patients (50%) and soft tissue sarcoma in 17 patients (50%). The latter included sarcoma of perivascular epithelioid cells (n=4), malignant peripheral nerve sheath tumor (n=4), Kaposi's Sarcoma (n=1), chondroid syringoma (n=1), cutaneous angiosarcoma (n=1), cutaneous epithelioid angiosarcoma (n=1), epithelioid malignant Schwannoma (n=1), malignant giant cell tumor of soft tissue (n=1), malignant schwannoma (n=1), myeloid sarcoma (n=1) and pleomorphic sarcoma (n=1).
An overview of the main findings is displayed in Figure 2.
3.3. Critical appraisal of the quality of included studies
Table 3 summarizes the quality assessment of the included studies. All studies (27/27, 100%) reported clear criteria for inclusion of the patient(s). Valid methods for identification of the initial (melanoma) and final (sarcoma) conditions were described by 16/27 (59%) and 18/27 (67%) studies, respectively. All case series (4/4, 100%) included consecutive patients. Clear reporting of demographics and clinical information were found in 27/27 (100%) and 24/27 (89%) studies, respectively. Only one study (4%) specified the timing of the second assessment, and 17/27 studies (63%) clearly reported the reason for the second assessment.
4. Discussion
This systematic review evaluated the available evidence on cases of sarcoma that were initially diagnosed as malignant melanoma. Our search yielded only case reports and small case series [9,11,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41] which individually can provide sparce information to the health care provider, but summarizing data from such sources may allow a better understanding of the topic. Of note, most studies were published in the last decade, which may suggest a rising interest in differentiating sarcoma from melanoma during the diagnostic process.
Overall, the clinical presentation of such cases was heterogeneous, and some sarcomas were initially misdiagnosed because several aspects such as clinical factors, localization of the lesion, and histologic appearance suggested a malignant melanoma [9,17,18,19,20,21,22,23,24,25,26,27,28,32,33,34,35,39,40,41]. In some cases, the clinician considered other diagnoses but finally opted for a melanoma [29,30,31,36,37,38]. Furthermore, immunohistochemistry could not be helpful for differentiating sarcoma from melanoma, which was suggested by the positivity of some markers such as S100, HBMG-45 and MelanA [9,17,18,19,20,21,22,23,26,27,29,30,31,32,33,34,35,36,37,38,39]. Hence, the rarity of cases of sarcoma mimicking melanoma likely played an important role in opting for melanoma as the reasonable initial diagnosis of choice. The reader should be aware that we assume such rarity given the few cases in literature, but we do not have robust information about the real magnitude of cases of sarcoma mimicking melanoma.
In fact, the main reasons for the second assessment leading to a diagnosis of sarcoma were the unusual presentation and the uncertainty about the diagnosis, which suggested further investigations to the clinicians [9,18,19,20,21,22,23,29,30,32,33,35,38]. In few cases, the second assessment was done because the patient did not respond to the treatment [17] or during a retrospective review of cases [21,24].
This implies that the correct identification of a sarcoma mimicking melanoma relies on the health care provider being aware of the possibility of such case and being able to identify when unusual features merit further investigations.
In addition, this also means that the prevalence of such cases is unknown, because the literature does not include episodes when the health care provider did not feel the need for further investigations and no systematic investigations have been conducted in large series of melanoma patients.
We believe that misdiagnosing a sarcoma as a melanoma may have potential implications for patient care because of the different therapeutic approaches, including sentinel node biopsy, first-line therapy and surgical therapy [12,13,14]. Unfortunately, available information is insufficient to assess the prognostic effect of such misdiagnosing.
Interestingly, half of the sarcomas found at the second assessment were CCS [17,18,19,20,21,22,23,26,29,30,31,32,33]. We believe that the common features shared by CCS and melanoma [7,8] and the lower incidence of CCS were likely to be reponsible for the initial misdiagnosis. When investigated, EWSR1 translocation was found positive in almost of all cases [17,18,19,20,21,22,26,29,30,31,32,33], hence the clinician may benefit from the inclusion of the investigation of EWSR1 translocation in the initial diagnostic process.
This systematic review has some limitations that should be considered by the reader. First, the research topic was prone to be described in case reports and very small case series, hence limiting the available information and the potential for further analyses. Second, the lack of epidemiological studies prevented from any considerations about the prevalence of cases of sarcoma that were initially diagnosed as melanoma. Third, information about the timing of the second assessment would provide interesting information but it was largely missing in the literature. Fourth, the role of EWSR1 translocation in the identification of CCS could not be investigated because of selected reporting (the included studies reported some CCS with positive EWSR1 and one MPNST with negative EWSR1).
Within its limitations, our systematic review underlines an underreported problem in the diagnosis of melanoma and sarcoma, inform the physician about features that can make the differential diagnosis difficult, and highlights the importance of searching for the EWSR1 translocation in the diagnostic process.
5. Conclusions
Atypical skin lesions could be misdiagnosed as melanomas if they share many similarities. Physicians should be aware of such possibility in the diagnostic process, as it may have potential implications on the treatment strategy. In case of atypical skin lesions, it could be useful to investigate the presence of EWSR1 translocation, since CSS are the most common histology to be found in case of re-evaluation. Referral to tertiary expert centers may be recommended. Further investigations are required to better understand the epidemiology of the mislead diagnosis and to raise awareness of the issue.
Author Contributions
Conceptualization, F.C. and P.DF.; methodology, F.C.; formal analysis, F.C., F.C.; investigation, F.C. and A.D.; writing—original draft preparation, F.C., F.C., A.D. and P.DF.; writing—review and editing, C.DP., M.R., M.A., S.M. and A.BF.; supervision, M.R., M.A., S.M. and A.BF. All authors have read and agreed to the published version of the manuscript.
Funding
This research has received "Current Research" funds from the Italian Ministry of Health to cover publication costs.
Data Availability Statement
The data presented in this study are available within the article.
Acknowledgments
The authors wish to thank “Piccoli Punti ONLUS” and “Fondazione Lucia Valentini Terrani” for their long-lasting support.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Gatta G, van der Zwan JM, Casali PG, et al.; RARECARE working group. Rare cancers are not so rare: the rare cancer burden in Europe. Eur J Cancer 2011;47:2493-511. [CrossRef]
- Sbaraglia M, Bellan E, Dei Tos AP. The 2020 WHO Classification of Soft Tissue Tumours: news and perspectives. Pathologica. 2021 Apr;113(2):70-84. [CrossRef]
- American Cancer Society Key statistics for soft tissue sarcomas (https://www.cancer.org/cancer/soft-tissue-sarcoma/about/key-statistics.html. (Accessed April 10, 2023).
- Hisaoka M, Ishida T, Kuo TT, Matsuyama A, Imamura T, Nishida K, Kuroda H, Inayama Y, Oshiro H, Kobayashi H, Nakajima T, Fukuda T, Ae K, Hashimoto H. Clear cell sarcoma of soft tissue: a clinicopathologic, immunohistochemical, and molecular analysis of 33 cases. Am J Surg Pathol. 2008;32(3):452-60. [CrossRef]
- Panagopoulos I, Mertens F, Isaksson M, Mandahl N. Absence of mutations of the BRAF gene in malignant melanoma of soft parts (clear cell sarcoma of tendons and aponeuroses) Cancer Genet Cytogenet. 2005;156:74–76. [CrossRef]
- Patel RM, Downs-Kelly E, Weiss SW, et al. Dual-color, break-apart fluorescence in situ hybridization for EWS gene rearrangement distinguishes clear cell sarcoma of soft tissue from malignant melanoma. Mod Pathol. 2005;18:1585–1590. [CrossRef]
- Dim DC, Cooley LD, Miranda RN. Clear cell sarcoma of tendons and aponeuroses: a review. Arch Pathol Lab Med. 2007; 131:152–156. [CrossRef]
- Pavlidis NA, Fisher C, Wiltshaw E. Clear-cell sarcoma of tendons and aponeuroses: a clinicopathologic study. Presentation of six additional cases with review of the literature. Cancer. 1984; 54:1412–1417.
- Biglow LR, Cuda J, Dotson J. A Rare Case of Epithelioid Malignant Peripheral Nerve Sheath Tumor Mimicking Malignant Melanoma. Cureus. 2021;13(2):e13424. [CrossRef]
- Gaspard M, Lamant L, Tournier E, et al. Evaluation of eight melanocytic and neural crest-associated markers in well-characterized series of 124 malignant peripheral nerve sheath tumours (MPNST): useful to distinguish MPNST from melanoma? Histopathology. 2018;73:969–982. [CrossRef]
- Zoufaly, A., Schmiedel, S., Lohse, A., & van Lunzen, J. (2007). Intestinal Kaposi's sarcoma may mimic gastrointestinal stromal tumor in HIV infection. World journal of gastroenterology, 13(33), 4514–4516. [CrossRef]
- Shafiq MB Sr, Rafi I, Shoaib A, Ali S, Iqbal F, Latif T, Mushtaq U. The Outcome of Extremity Soft Tissue Sarcomas in Terms of Resection Margins: A Study From a Cancer Dedicated Center. Cureus. 2022;14(6):e26086. [CrossRef]
- Kollender R, Merimsky O, Sternheim A, Gortzak Y, Dadia S, Doron A, Novikov I, Kollender Y, Soyfer V. Radiation Therapy Before Repeat Wide Resection for Unplanned Surgery of Soft Tissue Sarcoma ("Oops" Operation) Results in Improved Disease-Free Survival. Adv Radiat Oncol. 2022;7(6):101007. [CrossRef]
- Keung EZ, Krause KJ, Maxwell J, Morris CD, Crago AM, Houdek MT, Kane J, Lewis V, Callegaro D, Miller B, Lazar AJ, Gladdy R, Raut CP, Fabbri N, Al-Refaie W, Fairweather M, Wong SL, Roland CL. Sentinel Lymph Node Biopsy for Extremity and Truncal Soft Tissue Sarcomas: A Systematic Review of the Literature. Ann Surg Oncol. 2023;30(2):958-967. [CrossRef]
- Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, Shamseer L, Tetzlaff JM, Akl EA, Brennan SE, Chou R, Glanville J, Grimshaw JM, Hróbjartsson A, Lalu MM, Li T, Loder EW, Mayo-Wilson E, McDonald S, McGuinness LA, Stewart LA, Thomas J, Tricco AC, Welch VA, Whiting P, Moher D. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021 Mar 29;372:n71. [CrossRef]
- Munn Z, Barker TH, Moola S, Tufanaru C, Stern C, McArthur A, Stephenson M, Aromataris E. Methodological quality of case series studies: an introduction to the JBI critical appraisal tool. JBI Evid Synth. 2020;18(10):2127-2133. [CrossRef]
- Potter AJ, Dimitriou F, Karim RZ, Mahar A, Chan C, Long GV, Scolyer RA. Cutaneous clear cell sarcoma with an epidermal component mimicking melanoma. Pathology. 2022;54(3):369-371. [CrossRef]
- Tahiri Elousrouti L, Hammas N, Elmernissi FZ, Elfatemi H, Chbani L. Clear-Cell Sarcoma With an Unusual Presentation Mimicking Metastatic Melanoma. Cureus. 2022;14(11):e32010. [CrossRef]
- Zhang X, Zhang PJ, Sussman R, Litzky LA, Kucharczuk JC, Deshpande C. Atypical clear cell sarcoma of the pleura presenting as large pleural effusion with 22q12 abnormality: A challenging case with twists and turns. Human Pathology: Case Reports. 2021;24:200489. [CrossRef]
- Nawrocki S, Fitzhugh VA, Groisberg R, Aviv HA, Maghari A. A rare case of primary dermal clear cell sarcoma with focal epidermotropism: An entity difficult to distinguish from melanoma. J Cutan Pathol. 2020;47(7):621-624. [CrossRef]
- Obiorah IE, Ozdemirli M. Clear cell sarcoma in unusual sites mimicking metastatic melanoma. World J Clin Oncol. 2019;10(5):213-221. [CrossRef]
- Donzel M, Zidane-Marinnes M, Paindavoine S, Breheret R, de la Fouchardière A. Clear cell sarcoma of the soft palate mimicking unclassified melanoma. Pathology. 2019;51(3):331-334. [CrossRef]
- Obiorah IE, Brenholz P, Özdemirli M. Primary Clear Cell Sarcoma of the Dermis Mimicking Malignant Melanoma. Balkan Med J. 2018;35(2):203-207. [CrossRef]
- Curry JL, Tetzlaff MT, Wang SA, Landon G, Alouch N, Patel SP, Nagarajan P, Gupta S, Aung PP, Devine CE, Khoury JD, Loghavi S, Prieto VG, DiNardo CD, Gershenwald JE. Case Report of Myeloid Sarcoma Masquerading as In-Transit Metastasis at a Previous Melanoma Site: Avoiding a Diagnostic Pitfall. Am J Dermatopathol. 2018;40(11):831-835. [CrossRef]
- Leon-Castillo A, Chrisinger JSA, Panse G, Samdani RT, Ingram DR, Ravi V, Prieto VG, Wang WL, Lazar AJ. Index report of cutaneous angiosarcomas with strong positivity for tyrosinase mimicking melanoma with further evaluation of melanocytic markers in a large angiosarcoma series. J Cutan Pathol. 2017;44(8):692-697. [CrossRef]
- Zivanovic M, Luzar B, Bacchi CE, Calonje JE. Cutaneous clear cell sarcoma with intraepidermal component mimicking spitzoid melanoma. Virchows Arch. 2017:471(Suppl 1):S1–S352.
- Jackson CR, Minca EC, Kapil JP, Smith SC, Billings SD. Superficial malignant peripheral nerve sheath tumor with overlying intradermal melanocytic nevus mimicking spindle cell melanoma. J Cutan Pathol. 2016;43(12):1220-1225. [CrossRef]
- Castriconi M, Antropoli M, Grillo M, Andreano M, Santoro M, Villamania E. Unusual bleeding of a giant cell fibroblastoma: a soft tissue sarcoma of the skin mimicking metastatic melanoma. Ann Ital Chir. 2015;86(ePub):S2239253X15023701.
- Sayah M, Hammer S. Colonic Clear Cell Sarcoma Associated With Neurofibromatosis Type 2. American Journal of Clinical Pathology. 2015;144 (Issue suppl_2):A409. [CrossRef]
- Liu C, Ren Y, Li X, Cao Y, Chen Y, Cui X, Li L, Li F. Absence of 19 known hotspot oncogenic mutations in soft tissue clear cell sarcoma: two cases report with review of the literature. Int J Clin Exp Pathol. 2014;7(8):5242-9.
- Sidiropoulos M, Busam K, Guitart J, Laskin WB, Wagner AM, Gerami P. Superficial paramucosal clear cell sarcoma of the soft parts resembling melanoma in a 13-year-old boy. J Cutan Pathol. 2013;40(2):265-8. [CrossRef]
- Falconieri G, Bacchi CE, Luzar B. Cutaneous clear cell sarcoma: report of three cases of a potentially underestimated mimicker of spindle cell melanoma. Am J Dermatopathol. 2012;34(6):619-25. [CrossRef]
- Rodríguez-Martín M, Sáez-Rodríguez M, Esquivel B, Gonzáalez RS, Cabrera AN, Herrera AM. Clear cell sarcoma: a case mimicking primary cutaneous malignant melanoma. Indian J Dermatol. 2009;54(2):168-72. [CrossRef]
- Tanas MR, Rubin BP. Malignant neuroectodermal tumor with melanocytic and rhabdomyoblastic differentiation. Rare Tumors. 2009;1(2):e26. [CrossRef]
- Brightman LA, Demierre MF, Byers HR. Macrophage-rich epithelioid angiosarcoma mimicking malignant melanoma. J Cutan Pathol. 2006;33(1):38-42. [CrossRef]
- Matsuda Y, Saoo K, Hosokawa K, Yamakawa K, Yokohira M, Zeng Y, Takeuchi H, Iwai J, Shirai T, Obika K, Imaida K. Epithelioid malignant peripheral nerve sheath tumor. Report of a case with inflammatory infiltration. Pathol Res Pract. 2005;201(4):355-60. [CrossRef]
- Demir Y, Tokyol C. Superficial malignant schwannoma of the scalp. Dermatol Surg. 2003;29(8):879-81. [CrossRef]
- Bonetti F, Martignoni G, Colato C, Manfrin E, Gambacorta M, Faleri M, Bacchi C, Sin VC, Wong NL, Coady M, Chan JK. Abdominopelvic sarcoma of perivascular epithelioid cells. Report of four cases in young women, one with tuberous sclerosis. Mod Pathol. 2001;14(6):563-8. [CrossRef]
- Ferreiro JA, Nascimento AG. Hyaline-cell rich chondroid syringoma. A tumor mimicking malignancy. Am J Surg Pathol. 1995;19(8):912-7. [CrossRef]
- Honma K, Watanabe H, Ohnishi Y, Tachikawa S, Tachikawa K. Epithelioid malignant schwannoma. A case report. Acta Pathol Jpn. 1989 Mar;39(3):195-202. [CrossRef]
- Gould E, Albores-Saavedra J, Rothe M, Mnaymneh W, Menendez-Aponte S. Malignant giant cell tumor of soft parts presenting as a skin tumor. Am J Dermatopathol. 1989;11(3):197-201. [CrossRef]
Figure 1.
Flow-chart of selection process.
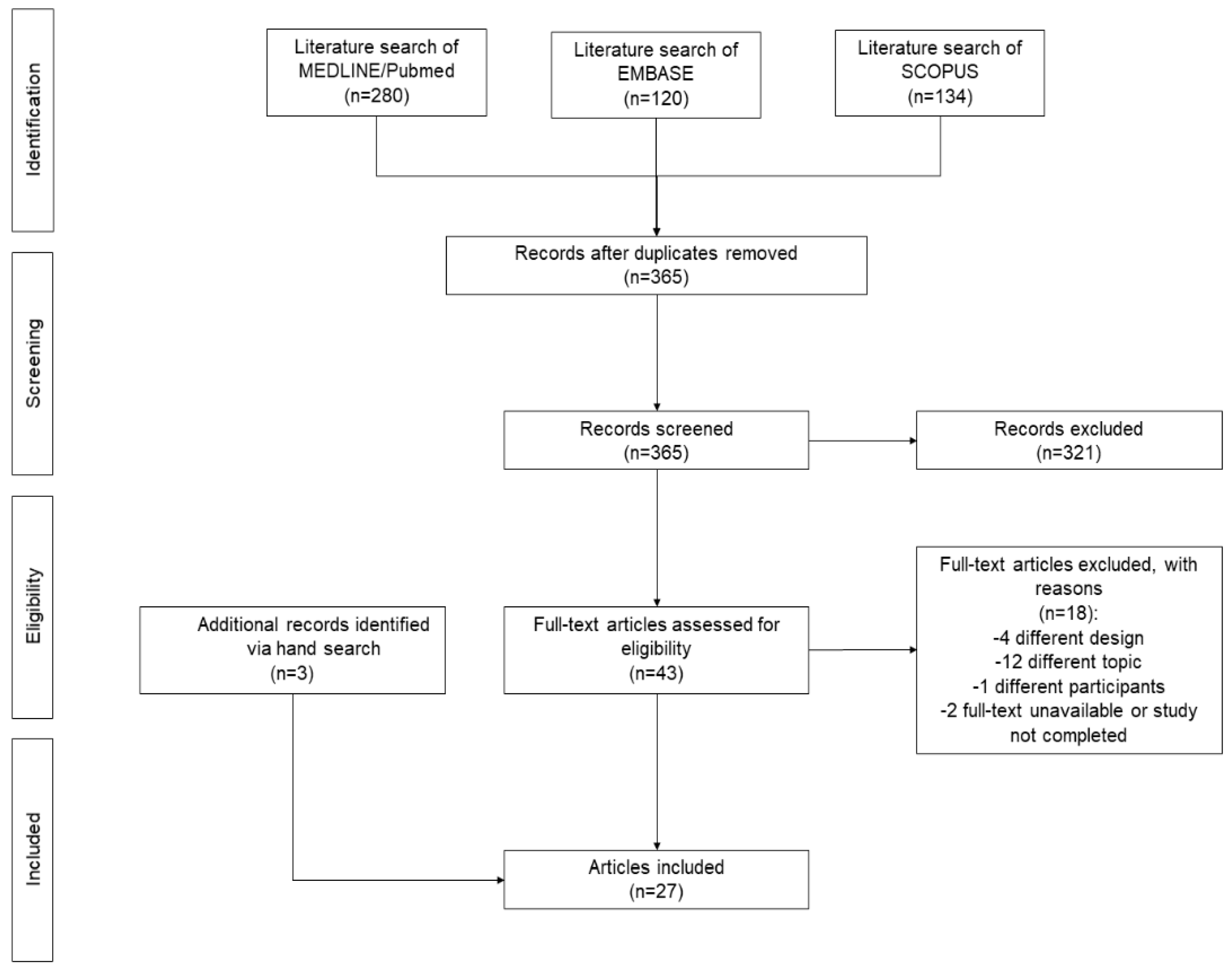
Figure 2.
Overview of main findings. CCS: clear cell sarcoma. MPNST: malignant peripheral nerve sheath tumor. SPEC: sarcoma of perivascular epithelioid cells. STS: soft tissue sarcoma.
Figure 2.
Overview of main findings. CCS: clear cell sarcoma. MPNST: malignant peripheral nerve sheath tumor. SPEC: sarcoma of perivascular epithelioid cells. STS: soft tissue sarcoma.
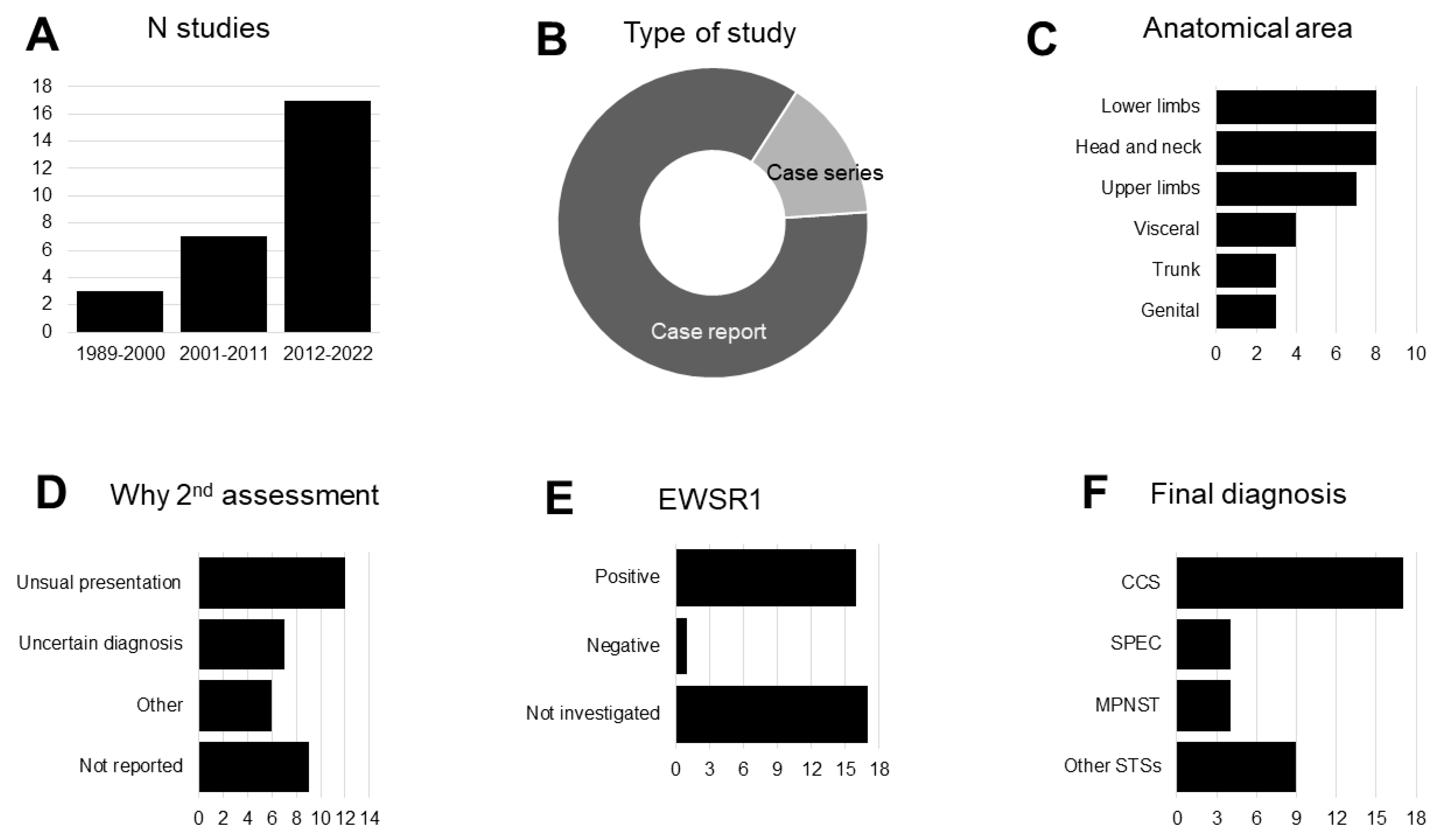

Table 1.
Characteristics of included studies: patient characteristics and clinical presentation.
| First author | Year | Type of study | N pts | Sex | Age (years) | Initial diagnosis a | Anatomical region | Site | Clinical presentation | IHC positivity |
|---|---|---|---|---|---|---|---|---|---|---|
| Potter AJ | 2022 | Case report | 1 | M | 30 | Melanoma | Lower limbs | Toe | Ulcerated nodular cutaneous lesion on the distal third toe, which had been present for several years | S100, HMB45, SOX10 |
| Tahiri EL | 2022 | Case report | 1 | M | 31 | Melanoma | Lower limbs | Heel | Heel mass nodule | S100, HMB45, MelanA |
| Biglow LR | 2021 | Case report | 1 | F | 47 | Melanoma | Upper limbs | Finger | Subcutaneous nodule at the finger without any obvious nevus or skin color changes | S100, SOX10, vimentina, BCL2 |
| Zhang X | 2021 | Case report | 1 | M | 68 | Melanoma | Visceral | Pleura | Dyspnea, cough following a dental abscess that was treated with root canal procedure; imaging studies revealed a large right pleural effusion, raising the concern of an empyema | SOX10, S100, HMB45, Melan-A |
| Nawrocki S | 2020 | Case report | 1 | M | 25 | Melanoma | Lower limbs | Left inguinal region | Raised blood blister that changed colors | S100, HMB45, Melan A |
| Obiorah IE |
2019 |
Case series |
2 |
F | 37 | Melanoma | Head and neck | Left neck | Complaint of left jaw pain and swelling. | HMB45, S100, CD31, CD34, CD68 |
| M | 33 | Melanoma | Trunk | Back | Mid back pain radiating to the flanks, and leg weakness and numbness, with gait abnormalities | HMB45, S100, Vimentine | ||||
| Donzel M | 2019 | Case report | 1 | M | 27 | Melanoma | Head and neck | Palate | Palatal ulcerations. Ill-defined and erythematous, with a friable centre, superficial erosions, and irregular, raised edges | HMB45, SOX10, Melan A |
| Obiorah IE | 2018 | Case report | 1 | F | 43 | Melanoma | Head and neck | Right neck | Mall nodule on the right side of her neck | S100, HMB45, vimentina |
| Curry JL | 2018 | Case report | 1 | M | 68 | Melanoma | Upper limbs | Left upper harm | Primary tumor not told; recurrence: new, slightly tender, 1.0 cm purpuric cutaneous nodule within the lymphatic drainage field of his previous primary melanoma of his left upper arm | CD11, CD43, CD68 |
| Leon-Castillo A | 2017 | Case report | 1 | M | 65 | Melanoma | Head and neck | Occipital scalp | Large multi-nodular cutaneous occipital scalp lesion with erythematous background | CD31, ERG, D2-40, factor VIII–related antigen, Tyrosinase, HMB45, melan A |
| Zivanovic M | 2017 | Case report | 1 | M | 20 | Melanoma | Lower limbs | Foot | N/A | S100, melanA, HMB45 |
| Jackson CR | 2016 | Case report | 1 | M | 56 | Melanoma | Trunk | Chest | Flesh-colored chest lesion for 7 years | S100, SOX10, CD34 |
| Castriconi M | 2015 | Case report | 1 | M | 56 | Melanoma | Upper limbs | Right axilla | Giant mass located on the right axilla. | N/A |
| Sayah M | 2015 | Case report | 1 | F | 54 | Suspect of melanoma | Visceral | Cecum | Severe iron deficiency anemia and hematochezia | S100, cytokeratins, HMB45 |
| Liu C | 2014 |
Case series |
2 | M | 29 | Suspect of melanoma | Upper limbs | Left thumb | Solid gray-white tumor | HMB45, Melan A, CD56, S100, vimentine, NSE |
| M | 76 | Suspect of melanoma | Visceral | Jejunum | Complaining of bowel obstruction, macroscopic examination: tumor (2.5 cm×2.2 cm×1.5 cm) with a whitish-grey surface. | S100, vimentine, NSE | ||||
| Sidiropoulos M | 2012 | Case report | 1 | M | 13 | Suspect of melanoma | Head and neck | Lower lip | Symptomatic papule on the lower lip that was suggestive of a mucocele. | S100, CD99, sinaptofisina, HMB45, MiTF |
| Falconieri G | 2012 |
Case series |
3 | M | 12 | Melanoma | Lower limbs | Left foot | Lesion in the dorsal aspect of foot | S100, Melan A |
| M | 60 | Melanoma | Lower limbs | Upper thigh | Slowly growing pigmented nodular lesion | S100 | ||||
| F | 29 | Melanoma | Lower limbs | Right foot | Lesion in the sole of the foot | S100, Melan A, HMB45 | ||||
| Rodríguez MM | 2009 | Case report | 1 | M | 53 | Melanoma | Upper limbs | Right harm | Painful lesion erythematous, dome-shaped, nodular lesion, 1.3 cm in diameter, firm to palpation and movable with a serohemorragic crust on its surface | S100, HMB45 |
| Tanas MR | 2009 | Case report | 1 | M | 67 | Melanoma | Trunk | Abdomen | Abdominal mass | S100, HMB45, MiFT, Melan A |
| Zoufaly A | 2007 | Case report | 1 | M | 69 | Melanoma | N/A | N/A | N/A | N/A |
| Brightman LA | 2006 | Case report | 1 | M | 86 | Melanoma | Head and neck | Scalp | Large irregular dark grey-blue plaque with an adjacent speckled tan nodule | S100, CD31, CD34 |
| Matsuda Y | 2005 | Case report | 1 | M | 75 | Suspect of melanoma | Lower limbs | Left thight | Oval-shaped mass, elastic soft, and adherent to the left thigh on palpation | S-100, NSE, GFAP, MBP, cromogranina A e sinaptofisina, |
| Demir Y | 2003 | Case report | 1 | M | 80 | Suspect of melanoma | Head and neck | Scalp | Painless ulceration on his scalp | S100 |
| Bonetti F | 2001 |
Case series |
4 | F | 28 | Suspect of melanoma | Visceral | Ileum | Abdominal pain | HMB45, MART 1 |
| F | 19 | Suspect of melanoma | Genital | Uterus | Abdominal pain | HMB45 | ||||
| F | 40 | Suspect of melanoma | Genital | Uterus | Surgery because of uterine leiomyomas; during the operation, a2.5x12x1.5 cm pelvic nodule was accidentally found and thought to represent endometriosis | HMB45 | ||||
| F | 41 | Suspect of melanoma | Genital | Myometrium | Presumed fibroids in uterus | HMB45, MART 1 | ||||
| Ferreiro JA | 1995 | Case report* | 1 | M | 75 | Melanoma | Head and neck | Face | Not painful mass of the face | keratin, S100, vimentine |
| Honma K | 1989 | Case report | 1 | M | 65 | Melanoma | Upper limbs | Left axillary fossa | N/A | Leu7, NSE |
| Gould E | 1989 | Case report b | 1 | M | 78 | Melanoma | Upper limbs | Left arm | Black nodule above the elbow | a1 anti-chymotrypsin (AACT), a1 antitrypsin (AAC) |
Table 2.
Characteristics of included studies: second assessment and final diagnosis.
| First author | Year | Why second assessment and/or diagnostic re-evaluation | EWSR1 translocation | Final diagnosis |
|---|---|---|---|---|
| Potter AJ | 2022 | Unresponsive to treatment | Positive | Clear cell sarcoma |
| Tahiri EL | 2022 | Unusual presentation | Positive | Clear cell sarcoma |
| Biglow LR | 2021 | Unusual presentation | Negative | Malignant peripheral nerve sheath tumor |
| Zhang X | 2021 | Uncertain diagnosis | Positive | Clear cell sarcoma |
| Nawrocki S | 2020 | Uncertain diagnosis | Positive | Clear cell sarcoma |
| Obiorah IE | 2019 |
Review after death | Positive | Clear cell sarcoma |
| Uncertain diagnosis | Positive | Clear cell sarcoma | ||
| Donzel M | 2019 | Uncertain diagnosis | Positive | Clear cell sarcoma |
| Obiorah IE | 2018 | Uncertain diagnosis | N/A | Clear cell sarcoma |
| Curry JL | 2018 | Review after surgery | N/A | Myeloid sarcoma |
| Leon-Castillo A | 2017 | N/A | N/A | Cutaneous angiosarcoma |
| Zivanovic M | 2017 | N/A | Positive | Clear cell sarcoma |
| Jackson CR | 2016 | Expert opinion | N/A | MPNST - malignant peripheral nerve sheath tumors |
| Castriconi M | 2015 | N/A | N/A | Pleomorphic sarcoma |
| Sayah M | 2015 | Unusual presentation | Positive | Clear cell sarcoma |
| Liu C | 2014 |
Unusual presentation | Positive | Clear cell sarcoma |
| Unusual presentation | Positive | Clear cell sarcoma | ||
| Sidiropoulos M | 2012 | Research for EWSR1 translocation | Positive | Clear cell sarcoma |
| Falconieri G | 2012 |
Unusual presentation | Positive | Clear cell sarcoma |
| Unusual presentation | Positive | Clear cell sarcoma | ||
| Unusual presentation | Positive | Clear cell sarcoma | ||
| Rodríguez MM | 2009 | Uncertain diagnosis | Positive | Clear cell sarcoma |
| Tanas MR | 2009 | N/A | N/A | Malignant peripheral nerve sheath tumor |
| Zoufaly A | 2007 | N/A | N/A | Kaposi's sarcoma |
| Brightman LA | 2006 | Uncertain diagnosis | N/A | Cutaneous epithelioid angiosarcoma |
| Matsuda Y | 2005 | N/A | N/A | Malignant peripheral nerve sheath tumor |
| Demir Y | 2003 | Expert opinion | N/A | Malignant schwannoma |
| Bonetti F | 2001 |
Unusual presentation | N/A | Sarcoma of perivascular epithelioid cells |
| Unusual presentation | N/A | Sarcoma of perivascular epithelioid cells | ||
| Unusual presentation | N/A | Sarcoma of perivascular epithelioid cells | ||
| Unusual presentation | N/A | Sarcoma of perivascular epithelioid cells | ||
| Ferreiro JA | 1995 | N/A | N/A | Chondroid syringoma |
| Honma K | 1989 | N/A | N/A | Epithlioid malignant Schwannoma |
| Gould E | 1989 | N/A | N/A | Malignant Giant Cell Tumor of soft tissue |
Table 3.
Summary of the quality assessment of the included studies.
| First author | Year | Clear criteria for inclusion | Valid methods for the identification of the initial condition | Valid methods for identification of the final condition | In a case series, consecutive inclusion of participant | Clear reporting of demographics | Clear reporting of clinical information | Reporting of time of second assessment | Reporting of reason for second assessment |
|---|---|---|---|---|---|---|---|---|---|
| Potter AJ | 2022 | Yes | Yes | Yes | N/A | Yes | Yes | No | Yes |
| Tahiri EL | 2022 | Yes | Yes | yes | N/A | Yes | Yes | No | Yes |
| Biglow LR | 2021 | Yes | Yes | Unclear | N/A | Yes | Yes | No | Yes |
| Zhang X | 2021 | Yes | Yes | Yes | N/A | Yes | Yes | Unclear | Yes |
| Nawrocki S | 2020 | Yes | Yes | Yes | N/A | Yes | Yes | No | Yes |
| Obiorah IE | 2019 | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Donzel M | 2019 | Yes | Yes | Yes | N/A | Yes | Yes | No | Yes |
| Obiorah IE | 2018 | Yes | Yes | Yes | N/A | Yes | Yes | No | Yes |
| Curry JL | 2018 | Yes | Yes | Yes | N/A | Yes | Yes | No | Yes |
| Leon-Castillo A | 2017 | Yes | Yes | Yes | N/A | Yes | Yes | No | No |
| Zivanovic M | 2017 | Yes | Yes | Yes | N/A | Yes | No | No | No |
| Jackson CR | 2016 | Yes | Yes | Unclear | N/A | Yes | Yes | No | Yes |
| Castriconi M | 2015 | Yes | Yes | Unclear | N/A | Yes | Yes | No | No |
| Sayah M | 2015 | Yes | Unclear | Yes | N/A | Yes | Yes | No | Yes |
| Liu C | 2014 | Yes | Unclear | Yes | Yes | Yes | Yes | No | Yes |
| Sidiropoulos M | 2012 | Yes | Unclear | Yes | N/A | Yes | Yes | No | Yes |
| Falconieri G | 2012 | Yes | Yes | Yes | Yes | Yes | Yes | No | Yes |
| Rodríguez MM | 2009 | Yes | Unclear | Yes | N/A | Yes | Yes | No | Unclear |
| Zoufaly A | 2007 | Yes | Yes | No | N/A | Yes | No | No | No |
| Tanas MR | 2009 | Yes | Unclear | Unclear | N/A | Yes | Yes | No | No |
| Brightman LA | 2006 | Yes | Yes | Yes | N/A | Yes | Yes | No | Yes |
| Matsuda Y | 2005 | Yes | Unclear | Unclear | N/A | Yes | Yes | No | No |
| Demir Y | 2003 | Yes | Unclear | Yes | N/A | Yes | Yes | No | Yes |
| Bonetti F | 2001 | Yes | Unclear | Yes | Yes | Yes | Yes | No | Yes |
| Ferreiro JA | 1995 | Yes | Unclear | Unclear | N/A | Yes | Yes | No | No |
| Honma K | 1989 | Yes | Unclear | Unclear | N/A | Yes | No | No | No |
| Gould E | 1989 | Yes | Unclear | unclear | N/A | Yes | Yes | No | No |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



