
Submitted:
13 June 2023
Posted:
13 June 2023
You are already at the latest version
Abstract
Oral health involves physiological functions related to mouth, teeth and orofacial structures, but also includes psychological and social dimensions. In this sense, oral health is an integrated part of human general health and well-being. Our aim was to access and evaluate the general oral health status of a high- and elite-level sample of Portuguese athletes from different sports. One hundred and sixteen participants were examined regarding their dental relationships, teeth and periodontal health, the presence of parafunctional activities (bruxism), and current or past orthodontic treatment. Our sample were predominantly adolescents and young adults, including 54 high-level and 62 elite subjects (71 males and 45 males) from 11 different sports, but mainly from swimming and athletics. Most sport performers presented with normocclusion (77%), despite the presence of other sagittal, transverse and vertical malocclusions. Twenty-three participants were affected by dental caries and six had missing teeth. Gingivitis (~40%) and dental calculus (~30%) were presented in our sample. Bruxism signs (47%) and current or past orthodontic treatment (~22%) were also found. Oral health conditions are not under control among high- and elite-level athletes, supporting the importance of healthcare needs and oral health promotion strategies in sports.
Keywords:
health
; dentistry
; oral disease
; sport
; sport dentistry
1. Introduction
Defined by the World Health Organization and the Fédération Dentaire Internationale (World Dental Federation), oral health encompasses a group of necessary functions related to mouth, teeth and orofacial structures (such as eating and breathing), and psychological and social dimensions (including the capacity of smiling and speaking) [1,2]. Thus, oral health is a fully free-disease, pain and discomfort state, supporting an individual´s ability to live, work and socialize, and integrating their overall health status, well-being and quality of life [1,3]. However, oral health is challenged by a range of diseases and conditions and has been long neglected in the global health programs. Persisting inequalities in access to oral healthcare remain a worldwide challenge.
As an integral part of general health, oral health conditions may affect exercise performance in view of the well-recognized effects (e.g. pain, systemic inflammatory states, eating, breathing and sleeping disturbances, and related psychological and social impacts) [4,5,6]. Nevertheless, challenges to oral healthcare are also linked with the demanding training schedules and nutritional requirements in sport. Having a disease-free mouth is often overlooked as an important determinant of an athlete´s health and performance [7]. Although these findings are not new, research on dental care in sport has been traditionally focused on preventing dental/orofacial trauma, for instance by wearing a mouthguard. Fortunately, sports dentistry has been emerged as a discipline and upcoming field within dentistry to prevent, deal and manage stomatognathic system diseases and associated injuries related to sports practice [8].
Sports dentistry is a multidisciplinary field concerned with the prevention, diagnosis and treatment of exercise/sports-related orofacial injuries to ensure excellent oral health for athletes. Currently, sports dentistry not only deals with the prevention and treatment of sport dental injuries, but also specific oral diseases associated with exercise and sport practice [9]. Sports dentistry is in constantly developing and should be brought to the attention of all athletes so they are aware of its applications and possibilities. By strengthening the balance between the human body and the oral cavity, sports dentistry should reduce the chance of orofacial traumas, increase the recovery time from muscular injuries, enhance posture and stability and promote better breathing and sleeping, enhancing overall health state and sport performance. Given growing health concerns and incidence of oral diseases in athletes, sports dentistry has been the subject of recent attention, having the potential to be an integrative discipline in sports medicine teams [8]. However, it is not yet well recognized in many countries, and only considered as a specialty in Brazil and United States of America [10].
Oral problems such as tooth decay, periodontal issues and missing teeth are the most prevalent diseases worldwide, affecting more than 3.5 billion people and forming a public health challenge [2,3]. As a part of general population, athletes are also included, with reports of a high prevalence of oral problems [4,11,12], no matter how specialized they are in their sports. Since athletes should be focused on their health and recovery, and regularly engaged in rehabilitation, medical and nutritional support, the reasons why dental problems are prevalent among this population seems are unclear. Nevertheless, athletes are likely a vulnerable population to oral cavity problems, worsened by risk factors related to training and competition such as decreased salivary flow, immunological disturbances, orofacial trauma and commonly high intake of carbohydrates [13,14,15]. Despite that, the main reasons for oral health needs in sport are the same as the general population, i.e., oral health is largely overlooked and underfunded, there is a lack of prioritization of oral healthcare and people are not well informed on the risks that these diseases pose to their global health and daily life or, at least, on their exercise activities or sport performance.
Reports from the literature indicate high levels of oral health problems among sport practitioners independent of their sport, competitive level and age [4,12,16]. Considering that all sports are different, and the training regimes and performance requirements diverge according to the competitive level, it is still unclear whether the prevalence and incidence of oral health conditions in this population relates to their behaviors when engaged in training and competition. While some of the risk factors for developing oral health problems among athletes are (more or less) described as sports-related, their oral health problems can be a part of the global burden of oral diseases worldwide, and possibly related to their socioeconomic status, environmental issues or political conditions.
Whether or not oral health problems reported among athletes are related to their sport practices, overall health and well-being are important to achieve high-performance results. Therefore, and particularly at younger ages, regular oral screening and strategies to promote good oral hygiene routines are imperative to minimize the negative health and performance impacts resulting from poor oral conditions. Based on the reciprocal relationship between dentistry and sport, i.e., how sports may impact an athlete´s oral health and the effects of oral health-related problems on their sports performance would be useful information for preventative programs. The aim of this study was to access and evaluate, through a clinical perspective, the general oral health status of a high- and elite-level sample of athletes from different sports.
2. Materials and Methods
One hundred and sixteen Portuguese athletes of a high- and elite-level, healthy and competing national and internationally in different sports volunteered for this cross-sectional study. Their main physical and training background characteristics were 18.2 ± 4.1 years of age, 171.2 ± 10.0 cm of height, 65.3 ± 13.0 kg of body mass, 9.2 ± 3.7 years of practice and 17.2 ± 6.6 h of weekly training in their specific sport. Subjects ‘oral health was assessed during three days during a training evaluation and control session to provide personal advice for their training and competitions and, for most of them, as a part of preparation to the Paris 2024 Olympic Games. All the experiments were approved by the local Ethics Committee and participants (or parent/guardian for the participants under 18 years old) read and signed a consent form to participate in accordance with the Declaration of Helsinki.
Intraoral health screening appointments were performed under good lightning conditions while participants were seated, and by an experienced clinical dentist using simple dental tools such as a disposable plastic mirrors, tongue depressors and gloves [17,18]. All procedures were minimally invasive and painless, aimed to make a gross assessment and for recognizing abnormal conditions of dental relationships, teeth and periodontal health, and the presence of parafunctional activities (bruxism), current or past orthodontic treatment. All subjects were encouraged to visit a dentist under clinical environment to confirm our diagnosis and for provision of an individualized oral management and treatment plan. During the appointment, subjects were instructed to control and maintain a healthy oral status and educated on the possible negative effects on sport performance resulting from poor oral health.
Oral screening was recorded across the three anatomical planes (sagittal, transverse and vertical). In the sagittal plane, dental occlusion was visually assessed by the first molar relationship according to Angle´s classification [19,20]: (i) class I, i.e., normocclusion, when the mesiobuccal cusp of upper first permanent molar occluded with mesiobuccal groove of the lower first permanent molar; (ii) class II, i.e., distocclusion, when the mesiobuccal groove of the lower first molar is posteriorly positioned when in occlusion with the mesiobuccal cusp of the upper first molar and (iii) class III, i.e., mesioclusion, when the mesiobuccal groove of the lower first molar is anteriorly positioned when in occlusion with the mesiobuccal cusp of the upper first molar.
In the transverse and vertical planes, malocclusions were also evaluated for the presence of: (i) crossbite - a misalignment of teeth affecting a single or a group of teeth, where upper teeth fit inside the lower ones; (ii) dental crowding - a dental misalignment caused by inadequate space for the teeth; (iii) open bite - when there is no vertical overlap or contact between upper and lower teeth; (iv) edge-to-edge bite - when the incisal edges of the upper teeth bite directly onto the incisal edges of the lower teeth; (v) overjet - an excessive horizontal distance between anterior upper and lower teeth and (vi) overbite - when the upper anterior teeth excessively overlap the lower anterior teeth with the posterior teeth closed. Crossbite and open bite were considered if dental arches were affected unilaterally, bilaterally, anteriorly, or posteriorly.
Subjects with decayed teeth, missing (excluding the third molars) and/or filled were counted as also the number of teeth affected from these conditions. Periodontal status was evaluated and considered when gum-related inflammatory states were visible (as redness and bleeding) and accompanied by supragingival calcified bacterial plaque (i.e., dental calculus) [17]. Bruxism diagnosis was validated when at least one of the following signs was presented: tongue indentation(s), tooth wear and masticatory muscles hypertrophy (masseter and temporalis) [21]. For each participant, a code number was assigned to maintain the confidentiality of their information. Data were then organized in Excel® (version 2303, Microsoft Corporation, Washington, USA) spreadsheets, checked and exported to SPSS software (version 27.0.1.0, IBM Corp., Armonk, NY, USA) to obtain all data frequencies.
3. Results
Our sample included 54 high level and 62 elite subjects (71 males and 45 females) from 11 different sports (see Figure 1). The participants were primarily from swimming and athletics, representing 34 and 26% of the total sample, particularly front crawlers (n= 15), breastrokers (n= 13), backstrokers (n= 4), butterflyers (n= 7), middle/long-distance runners (n= 19), sprinters (n= 1), race walkers (n= 2), decathlon specialists (n= 2), high jumpers (n= 1), shot putters (n= 1), and hammer, javelin and discus throwers (n= 1, 1 and 2, respectively). Elite athletes were evident all sports (excepted for tennis) and high-level subjects were observed for swimming, athletics, tennis, pentathlon, and triathlon. Male subjects were evaluated across all sports, however females were only distributed among swimming, athletics, canoeing, gymnastics, surfing and shooting.
Data related to oral health screening for the different sports are presented in Table 1. In the sagittal plane, most subjects presented a normal molar occlusion (Angle class I, 77%), being also observed disto and mesiocclusal molar relationships in our sample (Angle class II and III, 13 and 10%, respectively). Transverse and vertical malocclusions were also reported for 39 individuals (crossbite, n= 6; dental crowding, n= 13; open bite, n= 3; edge-to-edge bite, n= 6; overjet, n= 7 and overbite, n= 4). Subsequent evaluation of caries, missing teeth and fillings showed that 23, six and 37 subjects were affected, being the total number of decayed, missed and filled teeth 43, 11 and 94 (respectively). The worst findings regarding periodontal health were visible clinical signals of gum inflammation (n= 46, ~40%) and dental calculus (n= 35, ~30%). We observed that almost half of our sample (47%) presented bruxism signs as tongue indentation(s), tooth wear and/or masticatory muscle hypertrophy. Twenty-five subjects were under or already had completed orthodontic treatment.
4. Discussion
The idea that sport performers are healthy is a common-sense perception, but training and competing at high level may significantly impair physical, mental and social health outcomes. This scenario turns the generalized understanding connection between high performance and health into a paradox. Beyond surpassing their limits of training volume and intensity, competing even sick or injured, high- and elite- level athletes have intrinsic aims and motivations and are consistently under pressure from their support team to surpass their best performance [22,23]. This often results in a focus, and occasionally a zealous focus, in optimizing performance, but does not necessarily mean a full healthy state where physical, mental and social dimensions are well-combined and harmonized. Our findings showed that oral health conditions, as an important and integrated part of general health, are not entirely under control among high- and elite-level Portuguese athletes from different sports.
Poor oral health conditions reported in professional and elite performers from different sports [6,12,16]. The explanations for dental care needs in sports include nutritional and diet considerations (such as the needs for high and frequent carbohydrate intake, energy drinks, gels and bars intake), dehydration and decreased salivary flow, immune system suppression and host response impairment (due to demanding training schedules) [13,14,15]. Together, these factors create an acidogenic oral environment and impair the buffering function of saliva, which in turn could predispose to development of dental caries [12,24,25]. Moreover, inadequate oral hygiene practices, unsupported healthcare and/or overlooking oral dental care as an important aspect of general health are other key-factors contributing to lower oral status maintenance [5,26].
Although little attention has been paid to good oral health conditions and their influence in sports, they may play an essential role, especially for excellent standards of general health required at high and elite levels. First, an unproper dental occlusion, i.e., the misalignment matching between maxillary and mandibular teeth can impair temporomandibular joint, breathing pattern and masticatory efficiency [27,28,29], but also posture control and body balance [30,31]. For example, posture and balance are important factors affecting gymnastics or shooting sports performance [32,33]. Secondly, teeth decay and periodontal disease can form infectious and inflammatory loci with acute and local repercussions, and induce whole body harmful consequences for sport performers, such as pain, systemic inflammation, muscle fatigue, muscular injuries recidivism and poor recovery [5,34,35].
Apart from physical effects affecting performance directly or indirectly, poor oral health conditions may also have negative psychological and social impacts, consequently affecting self-confidence and socialization (like embarrassments to smile, laugh and show their teeth) [4,24]. The combined influence of poor oral health on physiological, psychological and social conditions may affect an athlete´s capacity to eat, drink, sleep and, at their extreme limit, could eliminate athletes from competition, or compromise all effort of many years of training to a preventable dental problem.
The theory that oral bacteria may contribute to illness from the mouth to distant sites of human body has been studied for decades [36], but dental problems (despite generally thought of as something harmful) still are widely considered as referring strictly to the mouth. However, oral cavity diseases also have been related with several other problems with systemic impacts such as, but not limited to, cardiovascular (heart problems), degenerative (e.g., Alzheimer´s disease) and metabolic illnesses (e.g., diabetes) [37,38]. Although a local dental emergency (e.g., tooth abscess) could unnecessarily compromise the moment of truth during a competition, systemic effects of poor oral healthcare in athletes later life should not be neglected.
Oral health assessment outcomes from high performance and elite athletes in our study confirms with other studies detailing needs for oral healthcare in this population [6,12,16]. Over the years, it is found that more participants need for dental treatments during the Olympic Games events [39,40,41], turning the dental care the second busiest service provided by the polyclinic of the Olympic Village [42]. In the 2008 Olympic Games there were reported 516 cases of athletes requiring dental care [42]. A dental screening conducted during the London 2012 Olympic Games also reported oral problems as teeth decay (55%), gingivitis (76%) and dental erosion (45%) among 278 elite athletes [16]. In comparison, our results showed a lower percentage of subjects affected by dental caries (~20%) and gingivitis (~40%). Nevertheless, unhealthy teeth and gums are still the most prevalent oral diseases described among athletes [5,6,16].
A study conducted among Dutch elite athletes before 2016 Rio Olympic Games showed that elite athletes were remarkably affected by poor oral health conditions, with near half of athletes requiring dental healthcare [43]. Our findings of healthcare needs in our sample are also in accordance with results from oral health screenings of high-level and elite Portuguese swimmers, handball and football players [17,18,44]. These findings also confirm that oral health disease prevalence and incidence do not appear to be related to athletes´ socioeconomic status or geographic location since poor oral health are affecting athletes from different developed countries. Our cohort of high and elite level athletes seems to have fewer oral health problems than the reported for other subjects of the same performance level. However, it is possible that our participants have a greater dental healthcare assessment and follow-up since almost ~22% were undergoing or already have done orthodontic treatment.
The presence of malocclusions in sport performers were also identified in different studies for the three anatomical planes and, as similar to our findings, the normocclusion in the sagittal plane (Angle class I) was reported as the most frequent first molar relationship [12,17,45]. Despite the current study sample only encompassing individual sports, our findings are also consistent with oral health screenings of professional and elite team sports [18,44,46]. From our results, we observed a large percentage of bruxism signs in our sample, possibly induced by higher stress levels from training and competing at excellent level. This is an important finding since bruxism may affect dental and articular structures, and induce masticatory muscle pain and headaches [21]. Nevertheless, bruxism signs may also be caused by unconscious or voluntary biting tasks performed during exercise, resulting from high-intensity efforts or to improve muscle strength and posture stability [47,48].
In Portugal, oral healthcare is largely provided by private clinics, but several public oral health programs have been developed by the government to primary prevent the oral diseases and support the dental treatment needs. One of these programs is particularly focused on children and adolescents, including free dental checks covering ages from two to 18 years old [49]. Nevertheless, although an improvement in Portuguese oral healthcare and an easier access to dental appointments in the last years have been observed [50,51], more than 60% of subjects (n= 1075) at 18 years old are affected by dental caries) [50]. Based on the low to moderate prevalence of oral health problems among Portuguese adolescents [50,52], and despite studies indicating that athletes are a higher risk population for developing dental problems, we cannot conclude that oral health problems found in our sample are directly related with their sports practice. However, the main question is: if athletes and their support medical teams were more aware and informed about the need for good oral health practices and their possible deleterious effects on their sporting results, would the results of the current study be different?
The study of oral health status including a substantial number of Portuguese high and elite level athletes from different sports should translate to other settings of adolescents and young adults. However, given that conducting our research among high-level and elite athletes during training sessions is challenging given a substantial time commitment and potential interference to training, testing and competition schedules, we acknowledge some limitations. First, since oral health assessment were conducted using simple dental tools, without specialized sources including x-ray, our oral health-related data should be interpreted carefully given the potential for some oral diagnoses to be underestimated or not fully detected. Secondly, since our observations were not conducted under a dedicated clinical environment, we also acknowledge a limitation during the tooth decay assessment, particularly for the diagnosis of initial non-cavitated “white” dental lesions where specific conditions are important for their detection (such as tooth dryness).
Another limitation of our study is the fact that no comparison was made between high-level and elite athletes, nor between sports, given the small number of athletes in some comparison groups, i.e., we did not have high-level athletes in some sports and other sports had a small sample size (e.g., shooting, sailing and triathlon vs swimming and athletics). To better understand the reciprocal relationship between oral problems and sport performance, epidemiological studies on representative samples are necessary. We also recommend that investigators in future studies give priority to collecting data (e.g. using questionnaires or interviews) on nutritional habits, history of muscular injuries and performance outcomes, to better understand the inter-relationship between oral problems and sport performance. Complementarily, the impact of oral health-related illness on performance should be evaluated by self-reports, also collecting data about missed training or competition events resulting from oral disease conditions.
5. Conclusions
One of the biggest challenges for dentistry in sports is the awareness of the athletes, their coaches, and overall support team on interaction between day-to-day sports training and oral health-related problems. In fact, since individuals engaged in sport may not perceive the training/competition as a risk for oral status and the importance of a healthy oral mouth for an entire balanced body system, their sport performance might be limited or even compromised. From our results, we have identified that oral health conditions are not under control among high level and elite sport athletes. This is a striking finding in cohort of otherwise healthy active adolescents and young adults as most of the oral problems found are preventable. Therefore, integrating oral health screening as a part of general health assessment and use of effective promotion strategies are needed. This approach should be highly valuable in enhancing health and well-being of athletes and to minimize the possible performance impacts from poor oral conditions. Given common oral diseases found in athletes and their potential links to exercise, sport and performance, sports dentistry should be integrated as a part of a comprehensive sports medicine program.
Author Contributions
Conceptualization, F.C., A.R.S., J.P.V.-B., J.C.P., D.B.P and R.J.F.; methodology, F.C., J.C.P. and R.J.F.; formal analysis, F.C., D.B.P and R.J.F.; investigation, F.C., A.R.S., J.P.V.-B., J.C.P., D.B.P and R.J.F.; resources, J.P.V.-B., J.C.P. and R.J.F.; writing—original draft preparation, F.C., D.B.P. and R.J.F.; writing—review and editing, F.C., A.R.S., J.P.V.-B., J.C.P., D.B.P and R.J.F.; visualization, F.C. and A.R.S.; supervision, J.P.V.-B., J.C.P., D.B.P and R.J.F.; project administration, J.P.V.-B. and R.J.F.; funding acquisition, J.P.V.-B. and R.J.F. All authors have read and agreed to the published version of the manuscript.
Funding
This work was supported by the Fundação para a Ciência e a Tecnologia (FCT) and European Union (EU), grant number 2020.05012.BD.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Ethics Committee of the Faculty of Sport of the University of Porto (CEFADE282020).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The dataset generated during the current study is available from the corresponding author on reasonable request.
Acknowledgments
The authors would like to acknowledge all study participants and collaborators.
Conflicts of Interest
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- Glick, M.; Williams, D.M.; Kleinman, D.V.; Vujicic, M.; Watt, R.G.; Weyant, R.J. A new definition for oral health developed by the FDI World Dental Federation opens the door to a universal definition of oral health. J. Public Health Dent. 2017, 77, 3–5. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization: Draft Global Oral Health Action Plan (2023-2030). Available online: https://www.who.int/publications/m/item/draft-global-oral-health-action-plan-(2023-2030) (accessed on 11 April 2023).
- World Health Organization: Global oral health status report: towards universal health coverage for oral health by 2030. Available online: https://www.paho.org/en/documents/global-oral-health-status-report-towards-universal-health-coverage-oral-health-2030 (accessed on 11 April 2023).
- Gallagher, J.; Ashley, P.; Petrie, A.; Needleman, I. Oral health and performance impacts in elite and professional athletes. Community Dent Oral Epidemiol. 2018, 46, 563–568. [Google Scholar] [CrossRef] [PubMed]
- Ashley, P.; Di Iorio, A.; Cole, E.; Tanday, A.; Needleman, I. Oral health of elite athletes and association with performance: a systematic review. Br J Sports Med. 2015, 49, 14–19. [Google Scholar] [CrossRef]
- Opazo-García, C.; Moya-Salazar, J.; Chicoma-Flores, K.; Contreras-Pulache, H. Oral health problems in high-performance athletes at 2019 Pan American Games in Lima: a descriptive study. BDJ open. 2021, 7, 21. [Google Scholar] [CrossRef]
- Bryant, S.; McLaughlin, K.; Morgaine, K.; Drummond, B. Elite athletes and oral health. Int J Sports Med. 2011, 32, 720–724. [Google Scholar] [CrossRef]
- Stamos, A.; Mills, S.; Malliaropoulos, N.; Cantamessa, S.; Dartevelle, J.-L.; Gündüz, E. The European Association for Sports Dentistry, Academy for Sports Dentistry, European College of Sports and Exercise Physicians consensus statement on sports dentistry integration in sports medicine. Dent Traumatol. 2020, 36, 680–684. [Google Scholar] [CrossRef]
- Roettger, M.; Mills, S. Modern Sports Dentistry. 1st ed.; Springer Cham, Switzerland, 2018; pp. 3–6.
- Sousa, M.; Mendes, J.J.; Godinho, C. Medicina Dentária Desportiva: Ideologia ou Necessidade? Proelium 2016, 7, 135–164. [Google Scholar]
- Needleman, I.; Ashley, P.; Fine, P.; Haddad, F.; Loosemore, M.; de Medici, A.; et al. Oral health and elite sport performance. Br J Sports Med 2015, 49, 3–6. [Google Scholar] [CrossRef] [PubMed]
- de la Parte, A.; Monticelli, F.; Toro-Román, V.; Pradas, F. Differences in Oral Health Status in Elite Athletes According to Sport Modalities. Sustainability. 2021, 13, 7282. [Google Scholar] [CrossRef]
- Hinds, L. Sports drinks and their impact on dental health. BDJ Team. 2019, 6, 11–17. [Google Scholar] [CrossRef]
- Tripodi, D.; Cosi, A.; Fulco, D.; D’Ercole, S. The Impact of Sport Training on Oral Health in Athletes. Dent J. 2021, 9, 51. [Google Scholar] [CrossRef] [PubMed]
- Gleeson, M.; McDonald, W.A.; Pyne, D.B.; Cripps, A.W.; Francis, J.L.; Fricker, P.A. Salivary IgA levels and infection risk in elite swimmers. Med Sci Sports Exerc. 1999, 31, 67–73. [Google Scholar] [CrossRef] [PubMed]
- Needleman, I.; Ashley, P.; Petrie, A.; Fortune, F.; Turner, W.; Jones, J. Oral health and impact on performance of athletes participating in the London 2012 Olympic Games: a cross-sectional study. Br J Sports Med. 2013, 47, 1054–1058. [Google Scholar] [CrossRef]
- Cardoso, F.; Monteiro, A.S.; Fernandes, A.; Vilas-Boas, J.P.; Pinho, J.C.; Pyne, D.B.; Fernandes, R.J. Oral health in young elite swimmers. Trends Sport Sci. 2020, 27, 49–55. [Google Scholar]
- Rios, M.; Fernandes, R.J.; Cardoso, R.; Monteiro, A.S.; Cardoso, F.; Fernandes, A.; Silva, G.; Fonseca, P.; Vilas-Boas, J.P.; Silva, J.A. Physical Fitness Profile of High-Level Female Portuguese Handball Players. Int J Environ Res Public Health, 2023, 20, 5751. [Google Scholar] [CrossRef] [PubMed]
- Angle, E.H. Classification of malocclusion. Dent Cosm. 1899, 41, 248–264. [Google Scholar]
- Yadav, D.; Rani, M.S.; Shailaja, A.M.; Anand, D.; Sood, N.; Gothi, R. Angle´s Molar Classification Revisited. J Indian Orthod Soc. 2014, 48, 382–387. [Google Scholar] [CrossRef]
- Lobbezoo, F.; Ahlberg, J.; Raphael, K.G.; Wetselaar, P.; Glaros, A.G.; Kato, T. International consensus on the assessment of bruxism: report of a work in progress. J Oral Rehabil. 2018, 45, 837–844. [Google Scholar] [CrossRef]
- Maffetone, P.B.; Laursen, P.B. Athletes: Fit but Unhealthy? Sport Med - Open. 2016, 2, 24. [Google Scholar] [CrossRef]
- Dijkstra, H.P.; Pollock, N.; Chakraverty, R.; Alonso, J.M. Managing the health of the elite athlete: a new integrated performance health management and coaching model. Br J Sports Med. 2014, 48, 523–531. [Google Scholar] [CrossRef]
- Khan, K.; Qadir, A.; Trakman, G.; Aziz, T.; Khattak, M.I.; Nabi, G. Sports and Energy Drink Consumption, Oral Health Problems and Performance Impact among Elite Athletes. Nutrients. 2022, 14, 5089. [Google Scholar] [CrossRef]
- González-Aragón Pineda, A.E.; García Pérez, A.; García-Godoy, F. Salivary parameters and oral health status amongst adolescents in Mexico. BMC Oral Health. 2020, 20, 190. [Google Scholar] [CrossRef]
- Needleman, I.; Ashley, P.; Fine, P.; Haddad, F.; Loosemore, M.; Medici, A. Consensus statement: oral health and elite sport performance. Br Dent J. 2014, 21, 587–590. [Google Scholar] [CrossRef]
- Magalhães, I.B.; Pereira, L.J.; Marques, L.S.; Gameiro, G.H. The influence of malocclusion on masticatory performance. A systematic review. Angle Orthod. 2010, 80, 981–987. [Google Scholar] [CrossRef] [PubMed]
- Pullinger, A.G.; Seligman, D.A.; Solberg, W.K. Temporomandibular disorders. Part II: Occlusal factors associated with temporomandibular joint tenderness and dysfunction. J Prosthet Dent. 1988, 59, 363–367. [Google Scholar] [CrossRef] [PubMed]
- Souki, B.Q.; Pimenta, G.B.; Souki, M.Q.; Franco, L.P.; Becker, H.M.G.; Pinto, J.A. Prevalence of malocclusion among mouth breathing children: do expectations meet reality? Int J Pediatr Otorhinolaryngol. 2009, 73, 767–773. [Google Scholar] [CrossRef]
- El Ouali, E.M.; Zouhal, H.; Bahije, L.; Ibrahimi, A.; Benamar, B.; Kartibou, J. Effects of Malocclusion on Maximal Aerobic Capacity and Athletic Performance in Young Sub-Elite Athletes. Sports. 2023, 11. [Google Scholar] [CrossRef] [PubMed]
- Maurer, C.; Stief, F.; Jonas, A.; Kovac, A.; Groneberg, D.A.; Meurer, A. Influence of the lower jaw position on the running pattern. PLoS One. 2015, 10, e013571. [Google Scholar] [CrossRef]
- Dias, A.A.; Redinha, L.A.; Silva, L.M.; Pezarat-Correia, P.C. Effects of Dental Occlusion on Body Sway, Upper Body Muscle Activity and Shooting Performance in Pistol Shooters. Appl bionics Biomech 2018, 2018, 9360103. [Google Scholar] [CrossRef]
- Mon, D.; Zakynthinaki, M.; Cordente, C.; Barriopedro, M.; Sampedro, J. Body sway and performance at competition in male pistol and rifle Olympic shooters. Biomed Hum Kinet. 2014, 6. [Google Scholar] [CrossRef]
- Merle, C.L.; Wuestenfeld, J.C.; Fenkse, F.; Wolfarth, B.; Haak, R.; Schmalz, G. The Significance of Oral Inflammation in Elite Sports: A Narrative Review. Sport Med Int Open. 2022, 6, E69–E79. [Google Scholar] [CrossRef] [PubMed]
- Solleveld, H.; Goedhart, A.; Vanden Bossche, L. Associations between poor oral health and reinjuries in male elite soccer players: a cross-sectional self-report study. BMC Sport Sci Med Rehabil. 2015, 7, 11. [Google Scholar] [CrossRef]
- Barnett, M.L. The oral-systemic disease connection. An update for the practicing dentist. J Am Dent Assoc. 2006, 137. [Google Scholar]
- Mealey, B.L. Periodontal disease and diabetes. A two-way street. J Am Dent Assoc. 2006, 137, S26–S31. [Google Scholar] [CrossRef]
- Demmer, R.T.; Desvarieux, M. Periodontal infections and cardiovascular disease: the heart of the matter. J Am Dent Assoc. 2006, 137, S14–S20. [Google Scholar] [CrossRef]
- Soler, B.D.; Batchelor, P.A.; Sheiham, A. The prevalence of oral health problems in participants of the 1992 Olympic Games in Barcelona. Int Dent J. 1994, 44, 44–48. [Google Scholar]
- Forrest, J.O. The dental condition of Olympic Games contestants-a pilot study. Dent Pract Dent Rec. 1969, 20, 95–101. [Google Scholar]
- Piccininni, P.M.; Fasel, R. Sports dentistry and the olympic games. J Calif Dent Assoc. 2005, 33, 471–483. [Google Scholar] [CrossRef]
- Yang, X.-J.; Schamach, P.; Dai, J.-P.; Zhen, X.-Z.; Yi, B.; Liu, H.; et al. Dental service in 2008 Summer Olympic Games. Br J Sports Med. 2011, 45, 270–274. [Google Scholar] [CrossRef]
- Kragt, L.; Moen, M.H.; Van Den Hoogenband, C.-R.; Wolvius, E.B. Oral health among Dutch elite athletes prior to Rio 2016. Phys Sportsmed. 2019, 47, 182–188. [Google Scholar] [CrossRef]
- Botelho, J.; Vicente, F.; Dias, L.; Júdice, A.; Pereira, P.; Proença, L. Periodontal Health, Nutrition and Anthropometry in Professional Footballers: A Preliminary Study. Nutrients. 2021, 13. [Google Scholar] [CrossRef] [PubMed]
- Gay-Escoda, C.; Vieira Pereira, D.; Ardèvol, J.; Pruna, R.; Fernandez, J.; Valmaseda-Castellón, E. Study of the effect of oral health on the physical condition of professional soccer players of Football Club Barcelona. Med Oral Patol Oral Cir Bucal. 2011, 16, e436–e439. [Google Scholar] [CrossRef]
- Souza, J.; Grande, R.; Bahls, R.; Santos, F. Evaluation of the oral health conditions of volleyball athletes. Rev Bras Med do Esporte. 2020, 26, 239–242. [Google Scholar] [CrossRef]
- Ringhof, S.; Hellmann, D.; Meier, F.; Etz, E.; Schindler, H.; Stein, T. The effect of oral motor activity on the athletic performance of professional golfers. Front Psychol. 2015, 6. [Google Scholar] [CrossRef] [PubMed]
- Ebben, W.P.; Flanagan, E.P.; Jensen, R.L. Jaw clenching results in concurrent activation potentiation during the countermovement jump. J Strength Cond Res. 2008, 22, 1850–1854. [Google Scholar] [CrossRef]
- SNS 24. Available online: https://www.sns24.gov.pt/servico/cheques-dentista/ (accessed on 5 May 2023).
- Calado, R.; Ferreira, C.S.; Nogueira, P.; Melo, P. Caries prevalence and treatment needs in young people in Portugal: the third national study. Community Dent Health. 2017, 34, 107–111. [Google Scholar]
- Veiga, N.J.; Pereira, C.M.; Ferreira, P.C.; Correia, I.J. Prevalence of dental caries and fissure sealants in a Portuguese sample of adolescents. PLoS One. 2015, 10, e0121299. [Google Scholar] [CrossRef]
- Veiga, N.J.; Cecchi, M.H.R.D.; Martins, J.; da Cunha, I.P.; Meneghim, M.D.C.; Correia, M.J.; Couto, P. Dental caries and oral health behavior assessments among Portuguese adolescents. J Oral Res. 2020, 9, 300–308. [Google Scholar] [CrossRef]
Figure 1.
Distribution of the participants by sport, high- and elite-level of performance (green and blue) and male and female (violet and pink) displayed at the upper, middle and lower panels (respectively).
Figure 1.
Distribution of the participants by sport, high- and elite-level of performance (green and blue) and male and female (violet and pink) displayed at the upper, middle and lower panels (respectively).
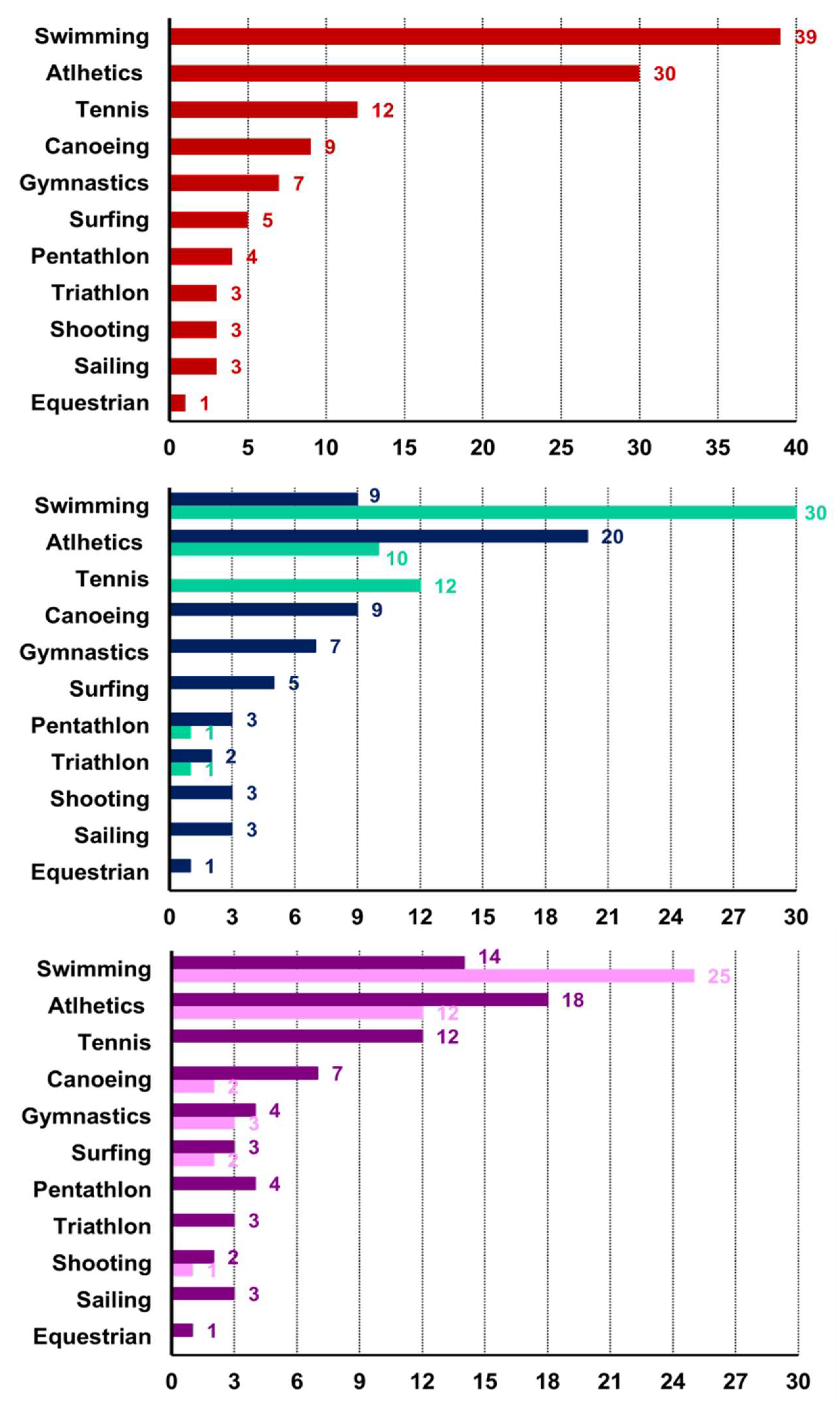

Table 1.
Oral health-related data across the studied sports.
| Sport | Angle classes | Malocclusions | Caries | Missing teeth |
Fillings | Gingivitis | Visible calculus |
Bruxism signs |
Orthodontics | |||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| I | II | III | ||||||||||
| Swimming | 31 | 5 | 3 | 11 | 8 | 1 | 9 | 18 | 16 | 14 | 12 | |
| Athletics | 24 | 5 | 1 | 10 | 6 | 3 | 12 | 14 | 9 | 16 | 7 | |
| Tennis | 7 | 1 | 4 | 5 | 3 | - | 6 | 6 | 5 | 4 | 3 | |
| Canoeing | 6 | 1 | 2 | 5 | 1 | - | 5 | 1 | 1 | 6 | - | |
| Gymnastics | 6 | 1 | - | 3 | 1 | - | 1 | 1 | 1 | 5 | 2 | |
| Surfing | 5 | - | - | 2 | 2 | - | - | - | - | 2 | - | |
| Pentathlon | 4 | - | - | 1 | 1 | - | 1 | 2 | 1 | 2 | - | |
| Triathlon | 3 | - | - | - | - | - | 1 | 2 | 2 | 2 | 1 | |
| Shooting | 2 | - | 1 | 1 | - | 1 | 1 | 1 | 1 | 2 | - | |
| Sailing | 1 | 1 | 1 | - | 1 | 1 | 1 | 1 | 1 | - | - | |
| Equestrian | - | 1 | - | 1 | - | - | - | - | - | 1 | - | |
| *Values represent the number of subjects in each diagnosis. | ||||||||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



