Submitted:
07 June 2023
Posted:
07 June 2023
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
The SARS coronavirus 2 (SARS-CoV-2) is the causative agent of the 2019 coronavirus disease (COVID-19) pandemic that has executed 6.9 million people and infected over 765 million. It’s become a major worldwide health alarm and is also known to cause abnormalities in various systems, including the hematologic system. COVID-19 infection primarily affects the lower res-piratory tract and can lead to a cascade of events, including a cytokine storm, intravascular thrombosis, and subsequent complications such as arterial and venous thromboses. COVID-19 can cause thrombocytopenia, lymphopenia, and neutrophilia, which are associated with worse out-comes. Prophylactic anticoagulation is essential to prevent complication and death rate associated with the virus's effect on the coagulation system. It is crucial to recognize these complications early and promptly start therapeutic anticoagulation to improve patient outcomes. While rare, COVID-19-induced disseminated intravascular coagulation exhibits some similarities to DIC induced by sepsis. LDH, D-dimer, ferritin, and CRP biomarker are often increase in serious COVID-19 cases and poor prognosis. Understanding the pathophysiology of the disease and identifying risk factors for adverse outcomes is critical for effective management of COVID-19.
Keywords:
SARS-CoV-2
; Hematology
; COVID-19
; Biomarkers
1. Introduction
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) is the causative agent of COVID-19 pandemic, responsible for the incidence of COVID-19 infections globally, which has affected over 765 million people, led to 6.9 million deaths worldwide, and has become a major global health concern [1]. SARS-CoV-2 is related from Coronaviridae family, which consists of a variety of enveloped RNA viruses of positive sense [2]. SARS-CoV-2 has become the seventh coronavirus that has affected the global population by causing human infection and triggering the worldwide coronavirus 2019 (COVID-19). SARS-CoV-2’s genome sequencing indicated a close relationship to bat coronaviruses, with 96.2% homology. It has a stronger attachment ability for the angiotensin-converting enzyme 2 receptor (ACE-2) to enter host cells and can spread more rapidly than SARS-CoV. [3,4]. It is transmitted mainly through close contact or droplets and causes fatal disease in 5% of cases, with a mortality rate of 2.3%. COVID-19 can cause a wide range of clinical symptoms, that can manifest from minor respiratory illness to life-threatening pneumonia, even ARDS or organ dysfunction in critical cases, hence adding to the high fatality rate among SARS-CoV-2-infected population [4,5,6]. Cofactors include age, the built environment (such as smoking or drug adductors), and co-existing diseases (such as hypertension, diabetes, or liver, lung, and heart disorders) all these factors have a significant role in the mortality rate [7]. Similar to the other two highly virulent coronaviruses that emerged in 2003 with severe acute respiratory syndrome (SARS) and 2012 with Middle East respiratory syndrome (MERS), the most frequently symptoms of COVID-19 observed are fever and respiratory symptoms like cough with sputum and dyspnea [8]. COVID-19 primarily impact the respiratory tract affected by the SARS-CoV-2 virus, but increasing evidence suggests that it can also affect multiple organs, including the gastrointestinal, neurological, renal, immune, hepatic, and haematological systems. Hematologic manifestations in COVID-19 patients, which have since been widely recognized as having significant prognostic implications, commonly result in venous thromboembolism and related complications, which contribute to increased mortality rates [11]. Autopsy studies have revealed microthrombi in multiple organs, emphasizing the need for effective thromboprophylaxis and treatment. Anomalies in thrombocytopenia and lymphopenia, as well as coagulation panel dysfunctions, are more pronounced among severely affected COVID-19 patients who do not survive. Therefore, early monitoring of hematologic abnormalities is crucial in the diagnosis, prognosis, and management of COVID-19 patients. The aim of this review article is to present a comprehensive overview of the haematological complications associated with COVID-19 with a focus on pathogenesis, biomarkers, and management options.
2. COVID-19 and the hematological abnormalities
The presence of SARS-CoV-2 virus has been identified to cause COVID-19 with pneumonia like etiology, certain studies give much attention that has been observed like hematological abnormalities by SARS-CoV-2 virus [9]. Hematological involvement is widely recognized in coronavirus infections of humans and animals that may vary depending on the strain, species and intensity of the infection’s virulence [10,11]. Previous studies have discovered that patients with SARS and MERS had differ hematological complication varies in various studies and population. However, certain studies have found that thrombocytopenia and lymphopenia are prevalent in significant number of MERS and SARS patients, with reported rates ranging from 25%-90%. [12,13] Moreover, smaller amount of coagulation abnormalities had also been observed in SARS patients [12].
Although early studies suggested that COVID-19 blood disorder symptoms were uncommon, more recent studies has shown the fact that blood disorder symptoms including breathlessness, discomfort or chest pain, weakness and fatigue, headache, easy bruising or bleeding, lightheadedness, fast heart beating or heart palpitation, shortness of breath and swelling of the ankle or legs are present in 30–70% of patients [14,15,16]. In one study in the initial two months of the pandemic outbreak in China, 7,736 patients were observed retrospectively to compare the clinical features of severe and non-severe cases. The researcher observed infected individuals with a severe version of the illness had more likely to have low blood counts across all lineages. Among the patients observed that 83.2% had lymphopenia, 33.7% lymphopenia had, and 36.2% had leukopenia. Blood counts showed thrombocytopenia to be the most common abnormality, occurring in 96% of critical cases and 80% of non-critical cases respectively. In critical cases, the average hemoglobin level has been observed to be lower than in non-critical cases (12.8 g/dL against 13.5 g/dL). Moreover, thrombocytopenia was present in 57.7% of the extremely critical cases and in 31.6% of the less serious cases [5]. Similar findings were found in other observational studies from China patients with COVID-19, although with fewer participants (41, 99, 138, and 201). Lymphopenia was present throughout all categories and was more prevalent in more severe cases. [17,18]
Patients with ARDS and those without ARDS were compared in additional prevalence study, take up 201 individuals with established COVID-19 from Hubei province and found that Lymphocyte and CD-8 T-cell counts exhibited a significant decreased in ARDS patients while the study provided indication that infected people with neutrophilia were more likely to risk of mortality [19].Hematological parameters of COVID-19 patients were the focus of a descriptive research conducted on 69 individuals at Singapore’s National Centre for Infectious Diseases (NCID). It was found that 29 percent of patients had severe leukopenia, 36.9 percent of patients had lymphopenia, and 5 of 25 had severe lymphopenia (absolute lymphocyte count [ALC] 0.5 109/L). Seven out of nine patients in the ICU were lymphopenia, and four of them had severe lymphopenia. Twenty percent of their patients also experienced moderate thrombocytopenia (platelet count 100-150 109/L) [20]. This should alert hematologists to be more suspicious of at-risk patients who initially present with signs of a blood problem, rather than anticipating for respiratory symptoms to develop. It can help in early isolation, detection and treatment of the COVID-19 virus [21].
Recently a study by Zhang et al. attempted to describe modifications between COVID-19 patients with hematologic disorders (26/84) and those without. They identify blood disease in COVID-19 patients despite finding minor differences in most lab results that had higher fibrinogen and D-Dimer level as well as lower levels of lymphocytes and platelets more frequently than those patients without hematological disorders while the study also found that patients with hematological disorders have high mortality rate and long stay at hospital as compared to without disorders [22] Another study also found that COVID-19 patient with hematological disorders had lower level of lymphocytes and platelets as well higher levels of ferritin, fibrinogen and D-dimer and also have higher incidence of ARDS with higher mortality as compared to patients without the disorders [23]. Patients without hematological disorders symptoms are more likely to be discharged home and cured than those with hematological disorder symptoms. This could be due to outcome and severity of COVID-19 virus that can vary depend on various factors including immune response, underlying health conditions, patients age and other severe complication that infected individuals who initially do not present with typical symptoms of respiratory tract have entered advanced stages of the illness [24].
3. Hematological system and their complications
The pathophysiology of illness caused by COVID-19 contains several organ systems essential for homeostasis [25]. Excessive inflammatory reaction to SARS-CoV-2 directly leads to release of endogenous compounds favoring altered vascular hemostasis [26]. The liberation of procoagulant and proinflammatory cytokines has a direct effect on blood coagulation [27], thereby triggering the development of systemic coagulation and thromboembolic states, causing widespread damage to the body tissues and organs, especially those most sensitive to ischemic processes tissues and organs such as cardiovascular system, brain vessels, and lung tissues [28]
3.1. Complication in the hematological system and their mechanism
There are several hypotheses as to why SARS-Cov-2 seems to produce hematological problems, but further investigation is needed to establish the exact molecular mechanism. However, various mechanism has been proposed in Figure 1 [29]. Firstly, interaction of SARS-CoV-2 and ACE2-receptor might result to hematological disorders. A recent analysis of bioinformatics data indicates that ACE2-receptor mediates the SARS-Cov-2 cell entrance mechanism, SARS-CoV-2 penetrate the cells by using the S protein to recognize and bind to ACE2. This leads to changes in the S1 domain and exposure of cleavage sites for proteases like TMPRSS2 or furin, which cleave the S protein between S1 and S2, allowing the virus to merge with the cell membrane and enter the cell. After gaining inside the cell, the virus undergoes a similar replication cycle to other RNA viruses while its expression is not limited in the alveolar cells of the lungs, but also extends in a variety of various tissues (including intestinal smooth muscle, heart, liver, kidneys, and the endothelium of blood vessels)[25]and lets the virus to hematogenously spread throughout the body via the circulatory system to directly infect blood vessels causing complications of blood including thromboembolic events and coagulation disorders [29,30]. Due to a vicious cycle, M1 macrophages create chemical mediators, that decreases the density of enzyme ACE2 receptors in blood vessels due to viral endocytosis, and levels of angiotensin II rise, causing vascular, proinflammatory and profibrotic consequences [31]. Additionally, this mechanism serves as a positive feedback loop to increase ACE2 production. Repetitive stimulation of these cycles enhances the spread of an infection and consequently raises level of angiotensin II and can also take part in the pathophysiology of COVID-19 by causing heightened inflammation, vasospasm and fibrosis. [30,32,33]. A prothrombotic phenotype is generated due to the enhanced activation of inflammatory cytokines IL-1 and IL-6 by activated M1 phenotype macrophages (Interferon-7) and excessive Ang II activity leading to increased permeability, endothelial cells activation and co-expression of adhesion molecules [34,35]. In addition, this is observed via increased in the synthesis of various chemicals (such as tissue factor, plasminogen activator inhibitor factors I, and von Willebrand factor (VWF) take part in hemostasis, which cause hemostatic alteration that leads to endothelial inflammation, prothrombotic and preadhesive [27,36] Since SARS-CoV-2 infects endothelial cells directly, this indicates persistent inflammation on in blood vessels throughout the body that ultimately leads to endotheliitis with symptoms include blood clots, brain fog, shortness of breath and fatigue.
Autopsy studies have also been conducted to further comprehend the haematological system involvement in COVID-19; however, in an autopsy study from 26 deceased COVID-19 patients by lax and colleagues. Blood clots in the tiny arteries cause a disorder called thrombotic microangiopathy, which was found in 11 of the 26 patients, leading to damage to vital organs like the kidneys and lungs. The study also found that many patients exhibited haematological problems such as anemia and leukocytosis, as well as high levels of D-dimer, a protein fragment that indicates the existence of blood clots [37]. Another study also investigated autopsy specimens from 12 COVID-19 patients. The investigation revealed that all 12 patients had multiple organs affected, including the heart, lungs, and kidney, by microvascular thrombosis, or blood clot development in small blood vessels. Haematological problems such as thrombocytopenia and lymphopenia were also common among the patients, and the study showed that many of them had increased levels of D-dimer as well [38].
All these findings and hypotheses may have clear implications for transmission prevention measures, especially for hospitalized COVID-19 patients. There are currently few studies on how hematological disorders affect transmission precautions for COVID-19 patients who are hospitalized. However, it has been observed in a study that patients with hematological complications might have an increased chance of developing COVID-19 because of their increased exposure to healthcare professionals during their prolonged hospitalizations. Data from 193 COVID-19 patients hospitalized in Italy revealed that those with hematological diseases had to stay in the hospital longer and were more likely to get healthcare-associated infections than those without hematological disorders. According to the study’s authors, individuals with hematological illnesses may require additional transmission precautions like isolation and personal protective equipment (PPE) for healthcare staff [39]. Current recommendations state that minimum 2 negative RT-PCR tests on respiratory specimens for SARS-CoV-2 taken 24 hours apart should be used at the moment of discharge of hospitalized COVID-19 cases with haematological disorders.
4. COVID-19 and pre-existing hematological complication
In general, patients with COVID-19 who also suffer from co-morbidities have a lower chance of a successful recovery. This could potentially impact the management of patients with pre-existing hematological disorders. Cancer patients have an increased vulnerability to developing infections, although it is still unknown whether hematological malignancies overall are more susceptible to contract SARS-CoV-2 than general population. The prevalence of blood disease symptoms was particularly high in cancer patients and in COVID-19 in general. For example, in one study, 53 hospitalized patients with COVID-19 had active hematologic malignancies including lymphoma, leukemia or multiple myeloma and investigate that 34 (64%) of patients required hospitalization and rate of mortality was 25%. The study also found that mortality rate was higher in infected population with lymphoma in contrast to other hematological malignancies in infected cases [24]. A retrospective study with 1392 patients with cancer and covid-19 have also been focused on a comparison of inpatients and outpatients with cancer and cancer history. The study observed that 18.3% of the patients had leukopenia and 19.5% had thrombocytopenia. The study also found that covid-19 cases with hematological malignancies had increased risk of leukopenia and thrombocytopenia compared to tumor cancer patients, while also observed that mortality rate is higher in thrombocytopenia patients as contrast to patients without these blood abnormalities [40].
4.1. Coagulation manifestations
There is growing evidence that COVID-19 infection causes hemostatic manifestation. Venous thromboembolism (VTE) is more familiar in critically ill individuals due to immobility, systemic inflammation from critical illness (like severe acute pancreatitis), desiccation, endothelial stasis, and dysfunction [41]. Some patient-associated risk factors for VTE development are metabolic syndrome e.g., (diabetes, hypertension, obesity), coronary heart disease, history of VTE inherited thrombophilia and peripheral artery disease [42,43].It is known that infections in critically sick patients can cause disseminated intravascular coagulation (DIC) a condition where the blood clots abnormally throughout the body lead to damage endothelium, activation of intravascular coagulation ,activation of neutrophils and life threating complications[44].
Patients with DIC have a condition called sepsis-induced coagulopathy (SIC), which occurs earlier in the patient and is less severe. These changes occur sequentially, and if the cause is left untreated, SIC becomes DIC. [45]. In 2009, the International Society on Thrombosis and Hemostasis (ISTH) published a scoring system showing that coagulopathy caused by COVID-19 meets the criteria for SIC or DIC. [46]. Moreover, there is also an agreement that coagulopathy in COVID-19-related DIC resembles thrombotic microangiopathy, that complement activation damages endothelial cells, and that COVID-19-associated DIC is thought to be caused by a virus that causes inflammation, which causes bleeding all over the body [47,48]. Figure 2 outlines the COVID-19 associated hematologic manifestations.
An increasingly clear clinical picture of COVID-19 infection shows a increase chance of venous thromboembolism (VTE), especially in severe illness with arterial thrombotic, deep venous thrombosis (DVT) instances as mini stroke [49,50,51]. The exact thrombotic issues had to be recorded with either a contrast-enhanced computed tomography (CT) scan or a doppler ultrasound, scans were requested at the treating physician’s decision. Cui and colleagues from China analyzed 81 covid 19 patients and 25% were found to have VTE while thromboprophylaxis details was not given [52]. Among 388 Italian patients in a retrospective cohort analysis, 61 (16%) were brought to the ICU, 327 (82%) of patients were treated in normal medical wards, and 78% were given thromboprophylaxis. The overall incidence of thromboembolic instances occurred in 21 percent, only 8 infected cases received diagnosis of overt DIC, but 7 did not survive. D-dimer levels increased rapidly in the non-survivors, which is consistent with recent studies [53]. Recently a Dutch analysis of 184 critically ICU cases with COVID-19 infection receiving thromboprophylaxis showed at least 31% of thromboembolic events. The predominant thrombotic consequence was pulmonary embolism (81%). Independent predictors of thrombotic events were prothrombin times less than 3 s and aPTT less than 5 s (hazard ratio (HR) 4.1, 95% CI 1.9-9.1).[50]. Another study found that out of 75 patients hospitalized to the ICU infected with COVID-19, 46.6% had thromboembolic events [54]. Similarly, postoperative thromboprophylaxis for this group of patients has very sparse indications. The initial COVID-19 flow in New York City had 11,249 patients, and 1.7% of them developed venous or arterial thromboembolism (VTE or thromboembolism). [55]. As shown in this trial, preventive anticoagulation with enoxaparin or rivaroxaban reduced coagulation complications by 46%. [55] On the other hand, patients with COVID-19 pneumonitis, may bleed and clot simultaneously when treated with anti-coagulants, making this condition patho-physiologically distinct [56]. Major bleeding occurred in 1.73 % of patients within 90 days of discharge, while only 13.2 % of the population received thromboprophylaxis [55]. Wichmann and coworkers found that deep venous thrombosis (DVT) was present in 58% of autopsied cases involving 12 patients. Despite the presence of pulmonary embolism (PE) in 4/3 patients (33%), microthrombi were frequently observed in the small lung arteries [57]. Diffuse microvascular thrombi have been found in a variety of organs in autopsy study performed in China [58]. Prominent PE was detected in 4 of 21 COVID-19 patients in another autopsy group, and alveolar capillary micro-thrombosis was detected in 5 of 11 patients (45%). Thrombotic microangiopathy of the glomerular capillaries was present in 3 of them [59].
4.2. Thrombocytopenia
In moderate COVID-19 infection, PT and aPTT may be ordinary or mildly prolonged, but they will be significantly prolonged in severe illness [60]. Platelet counts range from normal to mildly elevated in mild disease and markedly low in severe disease. [61]. D-dimer and fibrinogen increases, on the other hand, are associated with the severity of the illness [62]. Some of these findings are prognostically important. Despite this, most data come from looking back at previous cohorts or conducting subgroup analyses. D-dimer 0.5 g/mL was more common in very ill patients and affected 46.4% (260) of 560 patients among 1099 Chinese patients with COVID-19. Platelet count or thrombocytopenia (150 *109/L) was observed in 315/869 (36.2%) patients, and individuals with severe infection show a remarkable decrease [63]. Other descriptive studies from China with 99 hospitalized patients showed that 36% about one third of the infected cases had high level of D-dimer and 12% of the patient had acquired thrombocytopenia [18]. Patients in the COVID-19 ICU often see a decrease in their thrombocytes. Thrombocytopenia has been considerably lower in infected cases with serious infection, according to a meta-analysis of 1,779 cases infect with COVID-19 from 9 separate trials (Mean difference in thrombocytes: 31×109/L; 95% CI = 35-29 × 109/L) More than five times the probability of critical SARS-CoV-2 infection has a correlation to having a low platelet count (OR = 5.1; 95% CI = 1.8-14.6). The etiology of thrombocytopenia is complex, but potential contributing factors include endothelial cell injury from ventilatory dysfunction and stimulation of platelet, abnormal platelet dispersion of megakaryocytes in the bronchial blood vessels and affect myelotoxicity from thrombocytopenia and SARS-CoV-2 Infect. [10]. Another retrospective study including 41 patients confirmed that those requiring hospitalization in the ICU had increased PT and D-dimer levels than those who did not. Only 5% of the patients had severe (100 109/L) thrombocytopenia [17]. In a retrospective study Cui et al. analyzed that a D-dimer threshold levels predict VTE with a susceptibility of 85.0%, specificity of 88.5%, and an NPV (negative predictive value) of 94.7% among 81 patients [52]. Similarly, a retrospective analysis of 1449 COVID-19 infected cases in China found that those who ultimately passed away had higher mean and median values for D-dimer, PT, and aPTT. Increased mortality was associated with rising levels of D-dimer, fibrinogen and platelets counts [64]. A case series study of 30 diagnosed COVID-19 cases showed that patients whose platelet counts peaked had worse clinical outcomes [65]. Furthermore, the peak platelet-to-lymphocyte ratio (PLR) value during treatment also played a significant role in determining how long a patient stayed in the hospital. It was suggested that increases in platelet count and long stay in the hospital have been linked to the cytokine storm.
4.3. Lymphopenia
SARS-CoV-2 illness is linked with decreased CD4+, CD8+ T-cell, NK-cell, and B-cell lymphocyte counts in critically ill patients and is thought to occur through a separate mechanism. [66]. It is known that SARS-CoV-2 enters host cells by attaching its spike protein to the ACE2 receptor, thereby enabling the virus to invade the cell and replicate that cause SARS-CoV-2 infection. Lymphocytes also express these receptors on their surface. Therefore, virus may trigger lysis by binding directly to these cells. Multiple inflammatory cytokines are produced and released in response to infection. Lymphocyte shrinkage and apoptosis caused by this powerful cytokine activity can reduce lymphocyte regeneration [29,30]. Moreover, CD4+ T cells also have an important function as immunological modulators, including the suppression of inflammation [67]. Therefore, lymphopenia may play a role in the chain reaction that leads to excessive inflammation. Disease progression is influenced by natural killer cells and reduced CTLs (cytotoxic T lymphocytes) because they are essential for resisting viral infection [68]. Lymphopenia has been observed in a considerable quantity of COVID-19 patients particularly T cell in critically ill population but is generally reversible even after recovery from COVID-19 and is thought as a risk for increased mortality, seriousness and worse prognosis [69]. Lymphopenia also affect CTLs, NK and B cells as well that has been linked to the disease severity [70]. Viral respiratory infections
Transient lymphopenia has frequently been studied in various viral flu infections including RSV (respiratory syncytial virus), H3N2v virus, and SARS [71]. However, the number and duration of lymphocytes in COVID-infected patients appear to be more severe and selective for T-cell lineage, and they are also found to be prolonged compared to other viral respiratory illnesses.[72]. Lymphopenia was observed in 70.4% (19/27) of the most severely ill patients at a hospital in Wuhan during the early stages of the COVID-19 outbreak, with T cells declining more than B lymphocytes. Surprisingly when symptomatic disease was treated, CD4+ and CD8+ T cells were considerably enhanced, whereas B lymphocytes and NK cells were not. This suggests a possible correlation between clinical and immunological recovery, which can be assessed by an increasing peripheral CD4 and CD8 count [73]. In another study, the CD4/CD8 ratio remained within the normal range, but CD8+ T cells improved more after treatment. [74]. According to a study of the hematologic features of infected cases hospitalized to China’s Wuhan Union Hospital observed that patients with critical illness had low count of lymphocyte and a higher NLR (neutrophil-to-lymphocyte ratio) than those with severe or moderate illness, The average number of lymphocytes in this study was reduced in patients with severe disease (0.54 ×109/L) compared to those with intermediate disease (1.2×109/L). In addition, higher NLR has also linked to the intense inflammatory response observed in sepsis, and subsequent lymphocyte loss due to SARS-CoV-2. [21]. In another study conducted at five hospitals in Wuhan, China, patients who died of COVID-19 had lower median lymphocyte counts than survivors. [64]. In Wuhan, other studies have found that people who did not survived from COVID-19 had longer severe lymphopenia compared to those who survived, and the rate of lymphocyte decline remained until decease. Surviving infected cases had the lowest lymphocyte counts on day 7, but then saw an improvement during their hospitalization. Patients with persistently low lymphocyte counts were found to have a higher risk of mortality [75]. As a result, monitoring lymphocyte counts can be useful in assessing disease severity and predicting consequences in COVID-19 infected cases. Tan et al. developed a model to classify disease severity and predict prognosis based on the lymphocyte percentage (LYM%) in COVID-19 patients. The model suggests that patients with a LYM% less than 20% on 2nd week after symptom onset have a favorable outcome and make full recovery rapidly, while those with a LYM% greater than 20% are classified as severe cases. After 3rd week of experiencing symptom, infected cases with a LYM% less than 20% are likely to recover, those with a LYM between 5% and 20% are susceptible for decompensation, and those with a LYM% less than 5% are considered to be in critical condition and necessitate intensive care. Certainly, covid-19 infected individuals often exhibited lymphopenia and is considered a crucial indicator for prognosis and the severity of the illness.
The impact of COVID-19-induced lymphopenia on the immune system has been studied further. Zheng et al. investigated the immune-mediated features of leukocytes in peripheral blood from 16 COVID-19 patients in China ,Kunming and concluded that COVID-19 impaired the CD4 T cells functions and caused excessive activation, consequently, lymphopenia caused by CD8+ T cell depletion may compromise the immune reaction to SARS-CoV-2 in severely ill patients [76].Qin et al. conducted a group analysis of 452 individuals with COVID-19 infection in Wuhan and found that their immune responses were dysregulated. Researchers discovered that severe cases had decreased monocyte, eosinophil, and basophil percentages while increasing neutrophil and leukocyte counts. Analysis of lymphocyte subpopulations in 44 infected COVID-19 cases also showed a reduction in B, T, and NK cells, with a marked difference between severe and non-serious cases. In severe instances, SARS-CoV-2 was found to reduce T-cell counts to close to 50% of the lower limit of normal (461.6/L compared to 663.8/L; p = 0.027), demonstrating that T cells were more affected than other cell types. Subset analysis of T cells revealed that those with COVID-19 had decreased numbers of both helper T (CD3+ and CD4+) cells and suppressor T (CD3+ and CD8+) cells. These results suggested that COVID-19 may cause immune system malfunction by directly harming lymphocytes during the acute infection stage [77]. A high incidence of lymphopenia, ranging from 67-75% has been consistently reported among covid-19 patients who have severe illness, it may be correlate with increased quantity of cytokines such as IL-6, IL-10 or TNF (tumor necrosis factor) [78,79]. These cytokines and TNF may have a direct impact on T cell population [80], and also might have indirect impact through other type of cells including neutrophils and dendritic cells [81,82]
Therefore, the reduction in the amount of T lymphocytes, especially in the periphery, is a major hallmark of many people with severe disease, but the mechanisms of lymphopenia in COVID-19 remain incompletely known. Why the lymphopenia is more prevalent in T cells, and possibly only CD8+ T cells, is still unknown. Lymphopenia has been shown to increase activation of T cell and proliferation in animal studies [83]. Future research should emphasis on elucidating the role of lymphopenia in COVID-19 patients, as treatments like IL-7 may be useful in reducing T cell hyperactivation and, potentially, immunopathology.
4.4. Neutrophilia
COVID-19-related disruption of immune regulation contribute to various alterations in immune system including neutrophil. Additionally, neutrophilia might be related to an overlying bacterial infection, which is more common in severely ill patients. [65] Certainly, COVID-19 can cause hyperinflammatory responses and overproduction of cytokines, which activate and attract immune cells like macrophages, monocytes and neutrophils infiltration into lungs tissue. These cells can worsen tissue damage and increase the severity of the illness [67]. A study examined the immunological responses of 13 COVID-19 patients and observed that the illness has elevated cytokines proportion with IL-6, IL-10, and TNF-alpha, along with enhanced monocytes and neutrophil counts. As a result, the hyperactive reaction and subsequent cytokine storm in COVID19 may contribute to the excessive recruitment and neutrophils stimulation and monocytes, which can lead to lung damage and other problems.[84] Another study examined cytokine levels and COVID-19 severity. Patients with serious COVID-19 illness were high IL-6, IL-8, and TNF-α levels, along with higher neutrophil and monocyte counts. The study reveals that the cytokine storm, neutrophil and monocyte activation may contribute to COVID-19 progression and severity [85]. Autopsy of lung tissue samples from Chinese COVID-19 patients examined neutrophil infiltration of lung capillaries and fibrin deposition in inflamed capillaries generate acute inflammation causes widespread alveolar destruction and ARDS and also suggest that neutrophil infiltration may contribute to the acute injury of lungs in COVID-19 severe cases [86]. Another Italian study observed extensive alveolar damage, hyaline membrane development, and microthrombi in the pulmonary vasculature in COVID-19 lung tissue samples, suggesting severe endothelial injury [87]. Neutrophils have been identified as an indicator of respiratory symptom severity and poor outcomes in COVID-19. Neutrophil extracellular traps (NETs) are the main mechanism by which neutrophils induce inflammation in various organs and play a crucial role in damaged organs. [88].
NET is a network of chromatin and antimicrobial proteins in the extracellular space, such as cathelicidin, calprotectin, myeloperoxidase (MPO), neutrophil elastase (NE), and others. The composition of NETs can vary and is influenced by the stimulus that initiates their release from neutrophils to trap and kill pathogens. NETs are antimicrobial, but they also cause a lot of damage to the host’s tissue and make inflammation worse in many acute and chronic illnesses, including lung diseases [89]. Neutrophil elastase activation also participates in the excessive formation of NETs in the inflammation cascade, which can lead to microthrombosis, tissue damage, and organ failure involving the Lungs, heart, and kidney, and contributes to a diversity of infections pathogenesis, including SARS-COV-2. It’s mainly occurred due to dysregulated signaling during severe immune response in which NETs activate macrophages to generate proinflammatory cytokines IL-1β and TNF- α, this further promotes NET formation. Moreover IL-1 β generates IL-6, that stick to soluble IL-6 receptor released by neutrophils and causes signaling associated with a proinflammatory state [90]. Individuals with severe COVID-19 had raised level of NETs in their blood, thrombi, and lungs. This suggests that neutrophils and NETs might be essential in the pathophysiology of COVID-19 and their association have worse outcomes in various inflammatory and infectious illnesses.[91]. Neutrophilia infiltration activation has been linked with COVID-19 disease development and a higher risk of emerging ARDS, and mortality. Several studies have established that critical covid-19 patients’ blood and tissues have elevated level of neutrophils compared to those who have mild illness. The NLR (neutrophil to lymphocyte ratio), is a simple marker of systematic inflammation, has also been described to predict critical illness and mortality in infected people with SARS-cov-19. [92]. Ding et al. showed a case-control analysis on COVID-19 infected 72 in-patients to determine whether there was a connection between length of hospital stay and changes in haematological blood parameters. Of the 72 patients, 39 (54.2%) developed lymphopenia and 20 (27.2%) developed leukopenia; 15 (20.8%) were classified as severe instances and 57 (70.2%) were classified as mild cases. Lymphocyte counts often decreased in severe patients while leukocyte and neutrophil counts and the neutrophil-lymphocyte ratio (NLR) were markedly increase in mild-infected patients. Platelet counts in non-severe patients were found to rise gradually throughout the course of the study. They also found that NLR was positively correlated with hospital stay duration beginning on day five, suggesting that NLR was involved in predicting the prognosis for COVID-19 patients.[93]. Recent research has suggested that NLR can be utilized to indicate the severity of SARS-CoV-2 illness in its early stages. Prognosis for illness progression was best predicted by NLR, followed by patients age, in a study observed in Beijing, China. Infected people with NLR 3.13 and age ≥50 years had a 50% chance of developing critical illness, while individuals with NLR 3.13 and age < 50 years had a 9.1% low incidence.[94]. A similar finding, from a retrospective cohort study conducted at Wuhan University, indicated that COVID-19 hospitalized patients with a greater NLR had a significantly increased risk of mortality from any cause.[95]. A review of 38 studies was conducted to assess the significance of the NLR in expecting severity of the infection and mortality in COVID-19 infected cases. The meta-analysis revealed that elevated NLR values on admission were related with increased chances disease severity and fatality. This suggests that NLR is a useful biomarker for predicting the diagnosis of COVID-19 patients. Also, the difference in NLR values was greater between surviving and non-surviving patients compared with critically ill and non-critically ill patients. Patients with high NLR levels on admission had approximately double the risk of death compared with patients with normal NLR levels. Age, sex, diabetes, arterial hypertension, and cardiovascular diseases did not influence these relationships. [96] Certainly, the measurement of NLR from routine serum testing is a simple and effective way for clinicians to recognize COVID-19 infected populations that have a higher chance of developing serious sickness and death, which may help in prioritizing treatment, allocating medical sources, and classifying patients into higher levels of attention. [95].
5. Biomarkers
SARS-CoV-2 may involve in a wide range of COVID-19 severity, from asymptomatic to life-threatening infections, and its epidemic has directed to an urgent need to identify serum biomarkers that can indicate illness severity. During the incubation period, leukocytes and lymphocytes remain unaffected, but in the second phase of the disease, the virus can cause viremia, leading to pneumonia and potentially causing respiratory failure. [17]. In severe cases of COVID-19, as described earlier, lymphocyte counts are reduced while levels of inflammatory markers such as CRP (C-reactive protein), ferritin, and ESR (Erythrocyte Sedimentation Rate) are increased. High levels of ALT/AST, D-dimer, and LDH (lactate dehydrogenase) can also be detected in the blood. [97] as shown in Figure 3.
CRP, a biomarker produced by the liver and induced by IL-6, is commonly elevated in severe cases of COVID-19, making it a sensitive marker of inflammation and tissue damage. Several studies suggest that serum CRP level serve as dependable marker of both the presence and intensity of the SARS-CoV-2 sickness. Several studies have examined that serum CRP levels are a dependable marker of the existence and SARS-CoV-2 disease severity [98]. In Wuhan, China, a survey discovered that there was a rise in the advancement of the disease among patients with CRP levels exceeding 41.8 μg/mL [99]. In an alternative study, CRP intensity and pulmonary abnormalities observed via CT scan were studied, and the results showed that in the initial phase of COVID-19, elevated CRP levels correlate with both size of the lung lesion and extent of disease severity [100]. A different investigation assessed the relationship between CRP levels and CT intensity scores, which assign a numerical value based on visual examination of many lung lobes. The study revealed a direct association between CRP levels and CT outcomes. The authors suggest that CRP may be a more reliable predictor than CT scans in earlier stages of infection, when CT outcomes may not express substantial differences. [101]
LDH (Lactate dehydrogenase) is main enzyme found in almost every tissue in the body, including the blood cells, heart, lungs, liver, muscles and, kidneys and plays a crucial role in cellular metabolism to convert pyruvate to lactate and vice versa [97]. LDH is known as a biomarker because when its level becomes elevated in the blood, it signals the occurrence of tissue injury or infection. When tissue or cells become damaged that express LDH leading to higher LDH levels in the serum. Therefore, an increase in LDH is often observed in various diseases such as liver disease, heart disease, cancer and infection like COVID-19 and also proposed that in COVID-19 individuals elevated LDH levels is considered to be an indication of severity and worse prognosis [102]. As mentioned earlier, elevated LDH levels are often associated with the intensity of SARS-CoV-2 sickness. These levels are supposed to connected to tissue damage and inflammation, with elevated levels of LDH being associated with this condition [97]. A report evaluated a series of cases and established that high LDH levels upon admission, advanced age, CRP and lymphopenia were linked to the requirement of intensive care unit (ICU) [102]. Martinez and colleagues compared the levels of certain compounds in severe COVID-19 individuals and those with ARDS (infected group) to non-ARDS (moderate group) pneumonia. The results pointed out that infected COVID-19 individuals had elevated range of CRP, LDH, and ferritin, which exhibited a mark increase in critical cases than in mild to moderate ones. Furthermore, severe cases showed increased systemic inflammation, as indicated by elevated leukocyte, LDH, ferritin, IL-6, and TNF-α levels a week after admission. The study implies that elevated levels of inflammatory markers and a decrease in certain protective factors may contribute to lead to elevated rate of fatality in COVID-19 hospitalized cases. The best markers for predicting disease severity were found to be TT, ferritin, and LDH, whereas D-dimer, MMP-9 significances has notably elevated in critically ill patients during hospitalization. [103]. Although further research is needed, LDH has been related with an unfavorable outcome in COVID-19. D-dimer is a protein fragment that is generated when blood clots are detected in the body, and this protein is called fibrin. As a result of its lysis, D-dimer is released into the blood, signifying initiation of fibrinolysis and coagulation. [97]. D-dimer is an additional significant biomarker often used to examine blood clotting complications and as a potential prognostic factor and diagnostic tool for COVID-19 infection severity. A preliminary study that examined coagulation indicators in patients with COVID-19 associated pneumonia found that those who died from COVID-19 had considerably increase levels of D-dimer upon hospital entry, and these levels remained elevated later in the disease in all fatal cases [104]. Kaftan et al. conducted predictive levels of biomarkers in individuals with Covid-19. In addition, D-Dimer is a fibrin degradation test used for diagnosing thrombotic diseases. Previous studies have shown that higher levels of D-Dimer are associated with severe community-acquired pneumonia and chronic obstructive pulmonary disease. In COVID-19 cases, D-Dimer levels increased than 1 μg/mL are a risk factor for mortality, and levels greater than 2.0 μg/mL on hospitalization are linked with disease severity and mortality. D-Dimer might be useful indicator for managing COVID-19 patients.[105]. Even after adjusting for age or gender, an increased level of D-dimer remained an important factor regardless of the presence of underlying diseases.
Ferritin not only exhibits the function of storing iron, but it is also recognized as an indicator or biomarker of an acute phase reactant that responds to inflammatory stimuli, as its level can increase in response to cytokines like IL-6 that are produced during infection or an inflammatory response. The H subunit of ferritin, which is produced in response to inflammatory stimuli and may operate as an immunological regulator with both inflammatory promoting and immunoregulatory properties, is one of two subunits that make up ferritin.[106]. Elevated ferritin levels in COVID-19 cases are supposed to be linked to cytokine storms, which are an increased immune response that can occur in serious COVID-19 patients [107]. The cytokine storm is considered of high amount of cytokines associated with inflammation released into the body, which can cause tissue or organ damage and can lead to the development of serious complications such as ARDS so ferritin levels are high in response to infection or inflammation. Studies have shown that ferritin also serves as a useful biomarker, and its elevated level is linked with disease intensity and poor consequences in individuals with COVID-19 sickness [108]. A report showed in Wuhan, China, retrospectively evaluated a cohort of infected cases and initiate that high ferritin levels, along with several further biomarkers such as CRP, neutrophilia, lymphocytopenia and D-dimer, LDH, were markedly linked with a greater risk of developing ARDS. However, the study did not find an association between ferritin and illness mortality [19]. Another study showed that high elevated levels of serum ferritin (>3000 ng/mL) in 8% of our population upon admission, 13% shifts to ICU and 12% patients had expired along with high levels of CRP, D-dimers and low lymphocyte counts, were determined an autonomous serious chance for disease acuteness in COVID-19 cases. Additionally, highly elevated ferritin showed an independent correlation with hemoglobin counts with a poor outcome. [108]. Besides ferritin and IL-6, other commonly used inflammatory biomarkers are important in monitoring in COVID-19 patients. Troponin is a protein present in heart muscles cell and its elevation in the serum shows heart muscles damage. Studies showed that elevated troponin levels in covid patients are associated with disease severity and increase mortality [109].
Extra-thyroidal procalcitonin levels increase during severe bacterial infections due to endotoxins and cytokines, while viral infections lead to downregulation of procalcitonin. In uncomplicated COVID-19 cases, procalcitonin levels are usually within the reference range. However, elevated levels may indicate both a bacterial infection and progression of serious illness [110]. Procalcitonin levels slightly higher in the serum may help to distinguish among COVID-19 infected and COVID-19 non-infected individuals, and the increase in procalcitonin is more significant in critically ill patients [111]. Xu et al. showed that elevated levels of procalcitonin are closely associated with CRP and NLR among COVID 19 individuals admitted to the hospital with high mortality.[112]. Kidney and Liver function markers have been found to be important indicators of serious illness and fatality in COVID-19 cases. Studies have shown that elevated levels of enzymes like ALT, AST and creatinine, or the progression of acute renal infection, are significantly connected with a greater risk of death in COVID-19 infected cases. In addition, a systematic review has demonstrated that acute renal infection is an indicator of poor clinical outcomes in COVID-19 cases [113].
6. Conclusion
In conclusion, COVID-19 affects multiple systems in the body and has significant hematologic manifestations. It leads to a state of hypercoagulability, possibly due to immune-mediated factors, and can cause substantial harm. Various laboratory parameters, including D-dimer and LDH, may carry prospective values, although close monitoring and interpreting of these biomarkers can aid in predicting patient outcomes and making informed clinical decisions in developing a personalized treatment therapy for serious patients. Thromboprophylaxis is essential to prevent VTE, and early identification of potentially fatal problems such as DIC, PE, and stroke is critical for improving the patient’s health. Diagnostic testing for these abnormalities can help identify high-risk patients and provide timely interventions to improve their clinical prognosis. Overall, a heightened approach is necessary to manage risky and severely ill individuals with COVID-19.
Author Contributions
Shama prepared the manuscript with contributions from Asif Mahmood, Shahid Mehmood and Wen Zhang. and Asif Mahmood conceived its structure and content. All authors have read and agreed to the published version of the manuscript.
Funding
This research was supported by National Key Research and Development Programs of China No.2022YFC2603801 and Funding for Kunlun Talented People of Qinghai Province, High-end Innovation and Entrepreneurship talents—Leading Talents No. 202208170046.
Acknowledgments
We would like to thank National Key Research and Development Programs of China and Funding for Kunlun Talented People of Qinghai Province, High-end Innovation and Entrepreneurship talents programs for supporting and funding our study.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Coronavirus Disease (COVID-19) Pandemic. World Health Organization (WHO). Available at: https://www.who.int/emergencies/diseases/novel-coronavirus-2019.
- Gorbalenya AE, Baker SC, Baric RS, de Groot RJ, Drosten C, Gulyaeva AA, et al. (Coronaviridae Study Group of the International Committee on Taxonomy of Viruses). The Species Severe Acute Respiratory Syndrome-Related Coronavirus: Classifying 2019-Ncov and Naming it SARS-CoV-2. Nat Microbiol (2020) 5(4):536–44. [CrossRef]
- Kim, K. S. , Ejima, K., Iwanami, S., Fujita, Y., Ohashi, H., Koizumi, Y.,... & Iwami, S. (2021). A quantitative model used to compare within-host SARS-CoV-2, MERS-CoV, and SARS-CoV dynamics provides insights into the pathogenesis and treatment of SARS-CoV-2. PLoS biology, 19(3), e3001128. [CrossRef]
- Standl, F.; Jöckel, K.-H.; Brune, B.; Schmidt, B.; Stang, A. Comparing SARS-CoV-2 with SARS-CoV and influenza pandemics. Lancet Infect. Dis. 2020, 21, e77–E77. [Google Scholar] [CrossRef]
- Guan, W.J.; Ni, Z.Y.; Hu, Y.; Liang, W.H.; Ou, C.Q.; He, J.X.; Liu, L.; Shan, H.; Lei, C.L.; Hui, D.S.C.; et al. China Medical Treatment Expert Group for Covid-19. Clinical Characteristics of Coronavirus Disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef]
- Li, Q. et al. Early transmission dynamics in Wuhan, China, of novel coronavirus-infected pneumonia. N. Engl. J. Med. 1199. [Google Scholar]
- Shah, H.; Khan, S.H.; Dhurandhar, N.V.; Hegde, V. The triumvirate: why hypertension, obesity, and diabetes are risk factors for adverse effects in patients with COVID-19. Acta Diabetol. 2021, 58, 831–843. [Google Scholar] [CrossRef]
- Su, S.; Wong, G.; Shi, W.; Liu, J.; Lai, A.C.K.; Zhou, J.; Liu, W.; Bi, Y.; Gao, G.F. Epidemiology, Genetic Recombination, and Pathogenesis of Coronaviruses. Trends Microbiol. 2016, 24, 490–502. [Google Scholar] [CrossRef]
- Shahri, M.K.; Niazkar, H.R.; Rad, F. COVID-19 and hematology findings based on the current evidences: A puzzle with many missing pieces. Int. J. Lab. Hematol. 2020, 43, 160–168. [Google Scholar] [CrossRef]
- Lippi, G.; Plebani, M.; Henry, B.M. Thrombocytopenia is associated with severe coronavirus disease 2019 (COVID-19) infections: A meta-analysis. Clin. Chim. Acta 2020, 506, 145–148. [Google Scholar] [CrossRef]
- Wang, X.; Li, C.; Guo, D.; Wei, S.; Geng, Y.; Wang, E.; Wang, Z.; Zhao, X.; Su, M.; Liu, Q.; et al. Co-Circulation of Canine Coronavirus I and IIa/b with High Prevalence and Genetic Diversity in Heilongjiang Province, Northeast China. PLOS ONE 2016, 11, e0146975–e0146975. [Google Scholar] [CrossRef]
- Lee, N.; Hui, D.; Wu, A.; Chan, P.; Cameron, P.; Joynt, G.M.; Ahuja, A.; Yung, M.Y.; Leung, C.; To, K.; et al. A Major Outbreak of Severe Acute Respiratory Syndrome in Hong Kong. New Engl. J. Med. 2003, 348, 1986–1994. [Google Scholar] [CrossRef]
- Lu, L.; Zhong, W.; Bian, Z.; Li, Z.; Zhang, K.; Liang, B.; Zhong, Y.; Hu, M.; Lin, L.; Liu, J.; et al. A comparison of mortality-related risk factors of COVID-19, SARS, and MERS: A systematic review and meta-analysis. J. Infect. 2020, 81, e18–e25. [Google Scholar] [CrossRef] [PubMed]
- Yang, M.; Ng, M.H.; Li, C.K. Thrombocytopenia in patients with severe acute respiratory syndrome (review). Hematology 2005, 10, 101–105. [Google Scholar] [CrossRef] [PubMed]
- Wong, R.S.M.; Wu, A.; To, K.F.; Lee, N.; Lam, C.W.K.; Wong, C.K.; Chan, P.K.S.; Ng, M.H.L.; Yu, L.M.; Hui, D.S.; et al. Haematological manifestations in patients with severe acute respiratory syndrome: retrospective analysis. BMJ 2003, 326, 1358–1362. [Google Scholar] [CrossRef]
- Terpos, E.; Ntanasis-Stathopoulos, I.; Elalamy, I.; Kastritis, E.; Sergentanis, T.N.; Politou, M.; Psaltopoulou, T.; Gerotziafas, G.; Dimopoulos, M.A. Hematological findings and complications of COVID-19. Am. J. Hematol. 2020, 95, 834–847. [Google Scholar] [CrossRef]
- Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y, Zhang L, Fan G, Xu J, Gu X, Cheng Z, Yu T, Xia J, Wei Y, Wu W, Xie X, Yin W, Li H, Liu M, Xiao Y, Gao H, Guo L, Xie J, Wang G, Jiang R, Gao Z, Jin Q, Wang J, Cao B (2020) Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. 4: Lancet 395(10223), 1022.
- Chen N, Zhou M, Dong X, Qu J, Gong F, Han Y, Qiu Y, Wang J, Liu Y, Wei Y, Xia J, Yu T, Zhang X, Zhang L (2020) Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: a descriptive study. 5: Lancet 395(10223), 1022.
- Wu, C.; Chen, X.; Cai, Y.; Xia, J.; Zhou, X.; Xu, S.; Huang, H.; Zhang, L.; Zhou, X.; Du, C.; et al. Risk Factors Associated With Acute Respiratory Distress Syndrome and Death in Patients With Coronavirus Disease 2019 Pneumonia in Wuhan, China. JAMA Intern. Med. 2020, 180, 934–943. [Google Scholar] [CrossRef] [PubMed]
- Fan, B.E. Hematologic parameters in patients with COVID-19 infection: a reply. Am. J. Hematol. 2020, 95, E215–E215. [Google Scholar] [CrossRef]
- Liao, D.; Zhou, F.; Luo, L.; Xu, M.; Wang, H.; Xia, J.; Gao, Y.; Cai, L.; Wang, Z.; Yin, P.; et al. Haematological characteristics and risk factors in the classification and prognosis evaluation of COVID-19: a retrospective cohort study. Lancet Haematol. 2020, 7, e671–e678. [Google Scholar] [CrossRef]
- Zhang L, Yan X, Fan Q, Liu H, Liu X, Liu Z, et al. D-dimer levels on admission to predict in-hospital mortality in patients with Covid-19. J Thromb Thrombolysis. 1: 2020;50(3), 2020.
- Gholizadeh P, Safari H, Rostami M, Daneshmandi S, Yousefi M, Gholizadeh A. Hematological findings in COVID-19 patients with and without pneumonia: a case-control study. J Clin Pathol. 7: 2020;73(11), 2020.
- Passamonti, F.; Cattaneo, C.; Arcaini, L.; Bruna, R.; Cavo, M.; Merli, F.; Angelucci, E.; Krampera, M.; Cairoli, R.; Della Porta, M.G.; et al. Clinical characteristics and risk factors associated with COVID-19 severity in patients with haematological malignancies in Italy: a retrospective, multicentre, cohort study. Lancet Haematol. 2020, 7, e737–e745. [Google Scholar] [CrossRef]
- Jin, Y.; Ji, W.; Yang, H.; Chen, S.; Zhang, W.; Duan, G. Endothelial activation and dysfunction in COVID-19: from basic mechanisms to potential therapeutic approaches. Signal Transduct. Target. Ther. 2020, 5, 293. [Google Scholar] [CrossRef]
- Liu, P.P.; Blet, A.; Smyth, D.; Li, H. The science underlying Covid-19: Implications for the cardiovascular system. Circulation 2020, 142, 68–78. [Google Scholar] [CrossRef] [PubMed]
- Zachariah, U.; Nair, S.; Goel, A.; Balasubramanian, K.; Mackie, I.; Elias, E.; Eapen, C. Targeting raised von Willebrand factor levels and macrophage activation in severe COVID-19: Consider low volume plasma exchange and low dose steroid. Thromb. Res. 2020, 192, 2–2. [Google Scholar] [CrossRef] [PubMed]
- Giustino, G.; Pinney, S.P.; Lala, A.; Reddy, V.Y.; Johnston-Cox, H.A.; Mechanick, J.I.; Halperin, J.L.; Fuster, V. Coronavirus and Cardiovascular Disease, Myocardial Injury, and Arrhythmia. J. Am. Coll. Cardiol. 2020, 76, 2011–2023. [Google Scholar] [CrossRef]
- Gajendra, S. Spectrum of hematological changes in COVID-19. . 2022, 12, 43–53. [Google Scholar] [PubMed]
- Hamming, I.; Cooper, M.; Haagmans, B.; Hooper, N.; Korstanje, R.; Osterhaus, A.; Timens, W.; Turner, A.; Navis, G.; van Goor, H. The emerging role of ACE2 in physiology and disease. J. Pathol. 2007, 212, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Andrade, B.S.; Siqueira, S.; Soares, W.R.d.A.; Rangel, F.d.S.; Santos, N.O.; Freitas, A.d.S.; da Silveira, P.R.; Tiwari, S.; Alzahrani, K.J.; Góes-Neto, A.; et al. Long-COVID and Post-COVID Health Complications: An Up-to-Date Review on Clinical Conditions and Their Possible Molecular Mechanisms. Viruses 2021, 13, 700. [Google Scholar] [CrossRef] [PubMed]
- Gheblawi, M.; Wang, K.; Viveiros, A.; Nguyen, Q.; Zhong, J.C.; Turner, A.J.; Raizada, M.K.; Grant, M.B.; Oudit, G.Y. Angiotensinconverting enzyme 2: Sars-cov-2 receptor and regulator of the renin-angiotensin system: Celebrating the 20th anniversary of the discovery of ace2. Circ. Res. 2020, 126, 1456–1474. [Google Scholar] [CrossRef]
- Oudit, G.Y.; Kassiri, Z.; Jiang, C.; Liu, P.P.; Poutanen, S.M.; Penninger, J.M.; Butany, J. SARS-coronavirus modulation of myocardial ACE2 expression and inflammation in patients with SARS. Eur. J. Clin. Investig. 2009, 39, 618–625. [Google Scholar] [CrossRef]
- Escher, R.; Breakey, N.; Lämmle, B. Severe COVID-19 infection associated with endothelial activation. Thromb. Res. 2020, 190, 62–62. [Google Scholar] [CrossRef]
- Aird, W.C. Phenotypic heterogeneity of the endothelium: Ii. Representative vascular beds. Circ. Res. 2007, 100, 174–190. [Google Scholar]
- Boisrame-Helms, J.; Kremer, H.; Schini-Kerth, V.; Meziani, F. Endothelial dysfunction in sepsis. Curr. Vasc. Pharmacol. 2013, 11, 150–160. [Google Scholar]
- Lax, S. F. , Skok, K., Zechner, P., Kessler, H. H., Kaufmann, N., Koelblinger, C.,... & Trauner, M. (2020). Pulmonary arterial thrombosis in COVID-19 with fatal outcome: results from a prospective, single-center, clinicopathologic case series.
- Fox, S.E.; Akmatbekov, A.; Harbert, J.L.; Li, G.; Brown, J.Q.; Heide, R.S.V. Pulmonary and cardiac pathology in African American patients with COVID-19: an autopsy series from New Orleans. Lancet Respir. Med. 2020, 8, 681–686. [Google Scholar] [CrossRef]
- Girmenia C, Bertaina A, Piciocchi A, et al. COVID-19 in patients with hematological malignancies: a retrospective case series from eight Italian referral hospitals.J Hematol Oncol. 2020;13(1):119. [CrossRef]
- Martin-Romano EA, Sanchez-Lopez M, Saez MC, et al. Thrombocytopenia and lymphopenia in patients with cancer and COVID-19. Br J Cancer. 2021;124(2):320-325. [CrossRef]
- Hasan SS, Radford S, Kow CS, Zaidi STR (2020) Venous thromboembolism in critically ill COVID-19 patients receiving prophylactic or therapeutic anticoagulation: a systematic review and meta-analysis. 8: J Thromb Thrombolysis 50(4).
- Previtali E, Bucciarelli P, Passamonti SM, Martinelli I (2011) Risk factors for venous and arterial thrombosis. Blood Transfus 9(2):120–138.
- Gu SX, Tyagi T, Jain K, Gu VW, Lee SH, Hwa JM, Kwan JM, Krause DS, Lee AI, Halene S, Martin KA, Chun HJ, Hwa J (2020) Thrombocytopathy and endotheliopathy: crucial contributors to COVID-19 thromboinflammation.
- Papageorgiou C, Jourdi G, Adjambri E, Walborn A, Patel P, Fareed J, Elalamy I, Hoppensteadt D, Gerotziafas GT (2018) Disseminated intravascular coagulation: an update on pathogenesis, diagnosis, and therapeutic strategies. 8: Clin Appl Thromb Hemost 24(9_suppl).
- Iba T, Levy JH, Raj A, Warkentin TE (2019) Advance in the management of sepsis-induced coagulopathy and disseminated intravascular coagulation. J Clin Med 8(5).
- Levi M, Toh CH, Thachil J, Watson HG (2009) Guidelines for the diagnosis and management of disseminated intravascular coagulation. British Committee for Standards in Haematology. Br J Haematol 145(1):24–33.
- Iba T, Levy JH, Connors JM, Warkentin TE, Thachil J, Levi M (2020) The unique characteristics of COVID-19 coagulopathy. Crit Care 24(1):360.
- Campbell CM, Kahwash R (2020) Will complement inhibition be the new target in treating COVID-19–related systemic thrombosis? 1: Circulation 141(22), 1739.
- Hess DC, Eldahshan W, Rutkowski E (2020) COVID-19-related stroke. Transl Stroke Res 11(3):322–325.
- Klok FA, Kruip M, van der Meer NJM, Arbous MS, Gommers D, Kant KM, Kaptein FHJ, van Paassen J, Stals MAM, Huisman MV, Endeman H (2020) Incidence of thrombotic complications in critically ill ICU patients with COVID-19. Thromb Res 191:145–147.
- Gunasekaran K, Amoah K, Rajasurya V, Buscher MG (2020) Stroke in a young COVID-19 patient. Qjm 113(8):573–574.
- Cui S, Chen S, Li X, Liu S, Wang F (2020) Prevalence of venous thromboembolism in patients with severe novel coronavirus pneumonia. 1: J Thromb Haemost 18(6), 1421.
- Lodigiani C, Iapichino G, Carenzo L, Cecconi M, Ferrazzi P, Sebastian T, Kucher N, Studt JD, Sacco C, Alexia B, Sandri MT, Barco S (2020) Venous and arterial thromboembolic complications in COVID-19 patients admitted to an academic hospital in Milan, Italy. 9: Thromb Res 191.
- Beun R, Kusadasi N, Sikma M, Westerink J, Huisman A (2020) Thromboembolic events and apparent heparin resistance in patients infected with SARS-CoV-2. 1: Int J Lab Hematol 42(Suppl 1).
- Giannis, D.; Allen, S.L.; Tsang, J.; Flint, S.; Pinhasov, T.; Williams, S.; Tan, G.; Thakur, R.; Leung, C.; Snyder, M.; et al. Postdischarge thromboembolic outcomes and mortality of hospitalized patients with COVID-19: the CORE-19 registry. Blood 2021, 137, 2838–2847. [Google Scholar] [CrossRef]
- Bunch, C.M.; Thomas, A.V.; Stillson, J.E.; Gillespie, L.; Khan, R.Z.; Zackariya, N.; Shariff, F.; Al-Fadhl, M.; Mjaess, N.; Miller, P.D.; et al. Preventing Thrombohemorrhagic Complications of Heparinized COVID-19 Patients Using Adjunctive Thromboelastography: A Retrospective Study. J. Clin. Med. 2021, 10, 3097. [Google Scholar] [CrossRef]
- Wichmann D, Sperhake JP, Lütgehetmann M, Steurer S, Edler C, Heinemann A, Heinrich F, Mushumba H, Kniep I, Schröder AS, Burdelski C, de Heer G, Nierhaus A, Frings D, Pfefferle S, Becker H, Bredereke-Wiedling H, de Weerth A, Paschen HR, Sheikhzadeh-Eggers S, Stang A, Schmiedel S, Bokemeyer C, Addo MM, Aepfelbacher M, Püschel K, Kluge S (2020) Autopsy findings and venous thromboembolism in patients with COVID-19. 2: Ann Intern Med 173.
- Tian S, Hu W, Niu L, Liu H, Xu H, Xiao SY (2020) Pulmonary pathology of early-phase 2019 novel coronavirus (COVID-19) pneumonia in two patients with lung cancer. 7: J Thorac Oncol 15(5).
- Menter T, Haslbauer JD, Nienhold R, Savic S, Hopfer H, Deigendesch N, Frank S, Turek D, Willi N, Pargger H, Bassetti S, Leuppi JD, Cathomas G, Tolnay M, Mertz KD, Tzankov A (2020) Postmortem examination of COVID-19 patients reveals diffuse alveolar damage with severe capillary congestion and variegated findings in lungs and other organs suggesting vascular dysfunction. Histopathology. 1: 77.
- Aggarwal M, Dass J, Mahapatra M (2020) Hemostatic abnormalities in COVID-19: an update. 1: Indian J Hematol Blood Transfus 36(4).
- Wool GD, Miller JL (2020) The impact of COVID-19 disease on platelets and coagulation. Pathobiology.
- Long H, Nie L, Xiang X, Li H, Zhang X, Fu X, Ren H, Liu W, Wang Q, Wu Q (2020) D-dimer and prothrombin time are the significant indicators of severe COVID-19 and poor prognosis. Biomed Res Int 2020:6159720–6159710.
- Guan W-j, Ni Z-y, Hu Y, Liang W-h, Ou C-q, He J-x, Liu L, Shan H, Lei C-l, Hui DSC, Du B, Li L-j, Zeng G, Yuen K-Y, Chen R-c, Tang C-l, Wang T, Chen P-y, Xiang J, Li S-y, Wang J-l, Liang Z-j, Peng Y-x, Wei L, Liu Y, Hu Y-h, Peng P, Wang J-m, Liu J-y, Chen Z, Li G, Zheng Z-j, Qiu S-q, Luo J, Ye C-j, Zhu S-y, Zhong N-s (2020) Clinical characteristics of coronavirus disease 2019 in China. 1: N Engl J Med 382(18), 1708.
- Li Q, Cao Y, Chen L, Wu D, Yu J, Wang H, He W, Chen L, Dong F, Chen W (2020) Hematological features of persons with COVID-19.
- Seyit, M.; Avci, E.; Nar, R.; Senol, H.; Yilmaz, A.; Ozen, M.; Oskay, A.; Aybek, H. Neutrophil to lymphocyte ratio, lymphocyte to monocyte ratio and platelet to lymphocyte ratio to predict the severity of COVID-19. Am. J. Emerg. Med. 2020, 40, 110–114. [Google Scholar] [CrossRef]
- Schwartz, M.D.; Emerson, S.G.; Punt, J.; Goff, W.D. Decreased naïve T-cell production leading to cytokine storm as cause of increased COVID-19 severity with comorbidities. Aging Dis. 2020, 11, 742–745. [Google Scholar] [CrossRef]
- Henry BM, Vikse J, Benoit S, Favaloro EJ, Lippi G (2020) Hyperinflammation and derangement of renin-angiotensin-aldosterone system in COVID-19: a novel hypothesis for clinically suspected hypercoagulopathy and microvascular immunothrombosis. 1: Clin Chim Acta 507.
- Zhang C, Wang XM, Li SR, Twelkmeyer T, Wang WH, Zhang SY, Wang SF, Chen JZ, Jin X, Wu YZ, Chen XW, Wang SD, Niu JQ, Chen HR, Tang H (2019) NKG2A is a NK cell exhaustion checkpoint for HCV persistence. 1: Nat Commun 10(1), 1507.
- Tan, L.; Wang, Q.; Zhang, D.; Ding, J.; Huang, Q.; Tang, Y.-Q.; Wang, Q.; Miao, H. Correction: Lymphopenia predicts disease severity of COVID-19: a descriptive and predictive study. Signal Transduct. Target. Ther. 2020, 5, 1–1. [Google Scholar] [CrossRef]
- Giamarellos-Bourboulis, E.J.; Netea, M.G.; Rovina, N.; Akinosoglou, K.; Antoniadou, A.; Antonakos, N.; Damoraki, G.; Gkavogianni, T.; Adami, M.-E.; Katsaounou, P.; et al. Complex Immune Dysregulation in COVID-19 Patients with Severe Respiratory Failure. Cell Host Microbe 2020, 27, 992–1000. [Google Scholar] [CrossRef]
- McClain, M.T.; Park, L.P.; Nicholson, B.; Veldman, T.; Zaas, A.K.; Turner, R.; Lambkin-Williams, R.; Gilbert, A.S.; Ginsburg, G.S.; Woods, C.W. Longitudinal analysis of leukocyte differentials in peripheral blood of patients with acute respiratory viral infections. J. Clin. Virol. 2013, 58, 689–695. [Google Scholar] [CrossRef]
- Liu, K.; Fang, Y.-Y.; Deng, Y.; Liu, W.; Wang, M.-F.; Ma, J.-P.; Xiao, W.; Wang, Y.-N.; Zhong, M.-H.; Li, C.-H.; et al. Clinical characteristics of novel coronavirus cases in tertiary hospitals in Hubei Province. Chin. Med J. 2020, 133, 1025–1031. [Google Scholar] [CrossRef]
- Ashrafi, F.; Nematollahi, P.; Salmasi, M.; Hedayat, A.; Amra, B. Association of lymphocyte subsets with mortality in severe COVID-19 pneumonia patients. J. Clin. Lab. Anal. 2021, 35, e24046. [Google Scholar] [CrossRef]
- Ganji, A.; Farahani, I.; Khansarinejad, B.; Ghazavi, A.; Mosayebi, G. Increased expression of CD8 marker on T-cells in COVID-19 patients. Blood Cells, Mol. Dis. 2020, 83, 102437–102437. [Google Scholar] [CrossRef] [PubMed]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef] [PubMed]
- Zheng, H.-Y.; Zhang, M.; Yang, C.-X.; Zhang, N.; Wang, X.-C.; Yang, X.-P.; Dong, X.-Q.; Zheng, Y.-T. Elevated exhaustion levels and reduced functional diversity of T cells in peripheral blood may predict severe progression in COVID-19 patients. Cell. Mol. Immunol. 2020, 17, 541–543. [Google Scholar] [CrossRef]
- Qin, C.; Zhou, L.; Hu, Z.; Zhang, S.; Yang, S.; Tao, Y.; Xie, C.; Ma, K.; Shang, K.; Wang, W.; et al. Dysregulation of Immune Response in Patients With Coronavirus 2019 (COVID-19) in Wuhan, China. Clin. Infect. Dis. 2020, 71, 762–768. [Google Scholar] [CrossRef]
- Diao, B.; Wang, C.; Tan, Y.; Chen, X.; Liu, Y.; Ning, L.; Chen, L.; Li, M.; Liu, Y.; Wang, G.; et al. Reduction and Functional Exhaustion of T Cells in Patients With Coronavirus Disease 2019 (COVID-19). Front. Immunol. 2020, 11, 827. [Google Scholar] [CrossRef]
- Mazzoni, A.; Salvati, L.; Maggi, L.; Capone, M.; Vanni, A.; Spinicci, M.; Mencarini, J.; Caporale, R.; Peruzzi, B.; Antonelli, A.; et al. Impaired immune cell cytotoxicity in severe COVID-19 is IL-6 dependent. J. Clin. Investig. 2020, 130, 4694–4703. [Google Scholar] [CrossRef]
- Böttcher, J.P.; Schanz, O.; Garbers, C.; Zaremba, A.; Hegenbarth, S.; Kurts, C.; Beyer, M.; Schultze, J.L.; Kastenmüller, W.; Rose-John, S.; et al. IL-6 trans-Signaling-Dependent Rapid Development of Cytotoxic CD8+ T Cell Function. Cell Rep. 2014, 8, 1318–1327. [Google Scholar] [CrossRef]
- Liu, Y.; Du, X.; Chen, J.; Jin, Y.; Peng, L.; Wang, H.H.; Luo, M.; Chen, L.; Zhao, Y. Neutrophil-to-lymphocyte ratio as an independent risk factor for mortality in hospitalized patients with COVID-19. J. Infect. 2020, 81, e6–e12. [Google Scholar] [CrossRef]
- Ma, Y. et al. Predictive value of the neutrophil-to-lymphocyte ratio (NLR) for diagnosis and worse clinical course of the COVID-19: findings from ten provinces in China. [CrossRef]
- Surh, C.D.; Sprent, J. Homeostasis of Naive and Memory T Cells. Immunity 2008, 29, 848–862. [Google Scholar] [CrossRef]
- Liu, Y.; Zhang, C.; Huang, F.; Yang, Y.; Wang, F.; Yuan, J.; Zhang, Z.; Qin, Y.; Li, X.; Zhao, D.; et al. Elevated plasma levels of selective cytokines in COVID-19 patients reflect viral load and lung injury. Natl. Sci. Rev. 2020, 7, 1003–1011. [Google Scholar] [CrossRef]
- Thierry, A.R.; Pastor, B.; Abraham, J.-D.; Pisareva, E.; Mazard, T. Abstract P11: The elevated level of the main markers of neutrophil extracellular traps in metastatic colorectal cancer plasma highlights the enhanced risk of severe forms of COVID-19 in cancer patients. Clin. Cancer Res. 2021, 27, P11–P11. [Google Scholar] [CrossRef]
- Yao, X.H.; Li, T.Y.; He, Z.C.; Ping, Y.F.; Liu, H.W.; Yu, S.C.; Mou, H.M.; Wang, L.H.; Zhang, H.R.; Fu, W.J.; et al. A pathological report of three COVID-19 cases by minimally invasive autopsies. Zhonghua Bing Li Xue Za Zhi 2020, 49, E009. [Google Scholar]
- Carsana, L.; Sonzogni, A.; Nasr, A.; Rossi, R.S.; Pellegrinelli, A.; Zerbi, P.; Rech, R.; Colombo, R.; Antinori, S.; Corbellino, M.; et al. Pulmonary post-mortem findings in a series of COVID-19 cases from northern Italy: a two-centre descriptive study. Lancet Infect. Dis. 2020, 20, 1135–1140. [Google Scholar] [CrossRef] [PubMed]
- Yaqinuddin, A.; Kvietys, P.; Kashir, J. COVID-19: Role of neutrophil extracellular traps in acute lung injury. Respir. Investig. 2020, 58, 419–420. [Google Scholar] [CrossRef] [PubMed]
- Pastorek, M.; Dúbrava, M.; Celec, P. On the Origin of Neutrophil Extracellular Traps in COVID-19. Front. Immunol. 2022, 13, 821007. [Google Scholar] [CrossRef]
- Oury, C.; Marichal, T. Neutrophil extracellular traps: key drivers of severe Covid-19. 27. [CrossRef]
- Middleton EA, He X-Y, Denorme F, Campbell RA, Ng D, Salvatore SP, et al. Neutrophil extracellular traps (NETs) contribute to immunothrombosis in COVID-19 acute respiratory distress syndrome. Blood [Internet]. 2020.
- Al-Sharwey, H.M.A.; Helmy, M.W.; Mostafa, K.S.; Aiad, K. NEUTROPHIL - LYMPHOCYTE RATIO AS AN ANTICIPATORY FACTOR IN THE PROGNOSIS OF MORTALITY AND SEVERITY IN COVID-19 PATIENTS. ALEXMED ePosters 2023, 5, 18–19. [Google Scholar] [CrossRef]
- Ding, X.; Yu, Y.; Lu, B.; Huo, J.; Chen, M.; Kang, Y.; Lou, J.; Liu, Z. Dynamic profile and clinical implications of hematological parameters in hospitalized patients with coronavirus disease 2019. cclm 2020, 58, 1365–1371. [Google Scholar] [CrossRef]
- Liu J, Liu Y, Xiang P, Pu L, Xiong H, Li C, Zhang M, Tan J, Xu Y, Song R, Song M, Wang L, Zhang W, Han B, Yang L, Wang X, Zhou G, Zhang T, Li B, Wang Y, Chen Z, Wang X (2020) Neutrophil-to-lymphocyte ratio predicts critical illness patients with 2019 coronavirus disease in the early stage. J Transl Med 18(1):206.
- Liu Y, Du X, Chen J, Jin Y, Peng L, Wang HHX, Luo M, Chen L, Zhao Y (2020) Neutrophil-to-lymphocyte ratio as an independent risk factor for mortality in hospitalized patients with COVID-19. e: J Infect 81(1).
- Simadibrata, D.M.; Calvin, J.; Wijaya, A.D.; Ibrahim, N.A.A. Neutrophil-to-lymphocyte ratio on admission to predict the severity and mortality of COVID-19 patients: A meta-analysis. Am. J. Emerg. Med. 2021, 42, 60–69. [Google Scholar] [CrossRef]
- Kermali M, Khalsa RK, Pillai K, Ismail Z, Harky A (2020) The role of biomarkers in diagnosis of COVID-19 – a systematic review. 1: Life Sci 254, 1177.
- Wang L (2020) C-reactive protein levels in the early stage of COVID-19. Med Mal Infect 50(4):332–334.
- Liu F, Li L, Xu M, Wu J, Luo D, Zhu Y, Li B, Song X, Zhou X (2020) Prognostic value of interleukin-6, C-reactive protein, and procalcitonin in patients with COVID-19. 1: J Clin Virol 127, 1043.
- Wang L (2020) C-reactive protein levels in the early stage of COVID-19. Med Mal Infect 50(4):332–334.
- Tan C, Huang Y, Shi F, Tan K, Ma Q, Chen Y, Jiang X, Li X (2020) C-reactive protein correlates with computed tomographic findings and predicts severe COVID-19 early. 8: J Med Virol 92(7).
- Thakur, B.; Bora, K.; Chakraborty, M. Association of Serum Lactate Dehydrogenase and Qualitative C-Reactive Protein with the Severity of COVID-19 Disease. J. Clin. Diagn. Res. 2022, 16, BC1–BC4. [Google Scholar] [CrossRef]
- Mesa, A.M.; César, E.C.; Martín-Montañez, E.; Alvarez, E.S.; Lopez, P.M.; Romero-Zerbo, Y.; Garcia-Fernandez, M.; Garrido, J.L.V. Acute Lung Injury Biomarkers in the Prediction of COVID-19 Severity: Total Thiol, Ferritin and Lactate Dehydrogenase. Antioxidants 2021, 10, 1221. [Google Scholar] [CrossRef]
- Tang N, Li D, Wang X, Sun Z (2020) Abnormal coagulation parameters are associated with poor prognosis in patients with novel coronavirus pneumonia. J Thromb Haemost 18(4):844–847.
- Kaftan, A.; Hussain, M.; Algenabi, A.; Naser, F.; Enaya, M. Predictive Value of C-reactive Protein, Lactate Dehydrogenase, Ferritin and D-dimer Levels in Diagnosing COVID-19 Patients: a Retrospective Study. Acta Inform. Medica 2021, 29, 45–50. [Google Scholar] [CrossRef]
- Dahan, S.; Segal, G.; Katz, I.; Hellou, T.; Tietel, M.; Bryk, G.; Amital, H.; Shoenfeld, Y.; Dagan, A. Ferritin as a Marker of Severity in COVID-19 Patients: A Fatal Correlation. . 2020, 22, 494–500. [Google Scholar]
- Chen, J.; He, Z.-X.; Wang, F.-K. RETRACTED ARTICLE: Evaluation of ferritin level in COVID-19 patients and its inflammatory response. Appl. Nanosci. 2022, 13, 3121–3121. [Google Scholar] [CrossRef] [PubMed]
- Para, O.; Caruso, L.; Pestelli, G.; Tangianu, F.; Carrara, D.; Maddaluni, L.; Tamburello, A.; Castelnovo, L.; Fedi, G.; Guidi, S.; et al. Ferritin as prognostic marker in COVID-19: the FerVid study. Postgrad. Med. 2021, 134, 58–63. [Google Scholar] [CrossRef] [PubMed]
- Henry, B.M.; de Oliveira, M.H.S.; Benoit, S.; Plebani, M.; Lippi, G. Hematologic, biochemical and immune biomarker abnormalities associated with severe illness and mortality in coronavirus disease 2019 (COVID-19): A meta-analysis. Clin. Chem. Lab. Med. 2020, 58, 1021–1028. [Google Scholar] [CrossRef] [PubMed]
- Heidari-Beni, F. , Vahedian-Azimi, A., Shojaei, S., Rahimi-Bashar, F., Shahriary, A., Johnston, T. P., & Sahebkar, A. (2021). The level of procalcitonin in severe COVID-19 patients: a systematic review and meta-analysis. Clinical, Biological and Molecular Aspects of COVID-19, 277-286.
- Waris, A.; Din, M.; Iqbal, N.; Yar, L.; Khalid, A.; Nawaz, M.; Baset, A.; Ali, M. Evaluation of serum procalcitonin level as a biomarker for disease severity in COVID-19 patients. New Microbes New Infect. 2021, 43, 100922. [Google Scholar] [CrossRef]
- Xu, J.-B.; Xu, C.; Zhang, R.-B.; Wu, M.; Pan, C.-K.; Li, X.-J.; Wang, Q.; Zeng, F.-F.; Zhu, S. Associations of procalcitonin, C-reaction protein and neutrophil-to-lymphocyte ratio with mortality in hospitalized COVID-19 patients in China. Sci. Rep. 2020, 10, 1–10. [Google Scholar] [CrossRef]
- Malik, P.; Patel, U.; Mehta, D.; Patel, N.; Kelkar, R.; Akrmah, M.; Gabrilove, J.L.; Sacks, H. Biomarkers and outcomes of COVID-19 hospitalisations: systematic review and meta-analysis. BMJ Evidence-Based Med. 2021, 26, 107–108. [Google Scholar] [CrossRef]
Figure 1.
Mechanism of SARS-CoV-2. The mechanism of infection of SARS-CoV-2 is comparable to other coronaviruses, involving the S protein’s interaction with ACE2 (step 1). The S protein comprises of S1 subunit and S2 subunits, with former containing a RBD (receptor binding domain), that binds to ACE2-recetor, and the latter possessing the membrane fusion machinery facilitating cellular entry. Binding of ACE2 to S1 results in conformational changes in the protein, which exposes cleavage sites for proteases like TMPRSS2 or furin located in the cell membrane. This protease activity leads to the separation of S1 and S2 (step 2), activating the membrane fusion machinery of S1 (step 3), and enabling virus entry via endocytosis. Following cellular entry, the virus follows a similar RNA virus replication cycle.
Figure 1.
Mechanism of SARS-CoV-2. The mechanism of infection of SARS-CoV-2 is comparable to other coronaviruses, involving the S protein’s interaction with ACE2 (step 1). The S protein comprises of S1 subunit and S2 subunits, with former containing a RBD (receptor binding domain), that binds to ACE2-recetor, and the latter possessing the membrane fusion machinery facilitating cellular entry. Binding of ACE2 to S1 results in conformational changes in the protein, which exposes cleavage sites for proteases like TMPRSS2 or furin located in the cell membrane. This protease activity leads to the separation of S1 and S2 (step 2), activating the membrane fusion machinery of S1 (step 3), and enabling virus entry via endocytosis. Following cellular entry, the virus follows a similar RNA virus replication cycle.

Figure 2.
COVID-19 associated hematologic manifestations like changes in blood cell counts (lymphopenia, neutrophilia, thrombocytopenia), coagulation disorders (DIC, increased risk of VTE), and abnormal levels of D-dimer, CRP, LDH and clotting factors. These issues show the complex connection between the virus, immune response, and blood clotting.
Figure 2.
COVID-19 associated hematologic manifestations like changes in blood cell counts (lymphopenia, neutrophilia, thrombocytopenia), coagulation disorders (DIC, increased risk of VTE), and abnormal levels of D-dimer, CRP, LDH and clotting factors. These issues show the complex connection between the virus, immune response, and blood clotting.
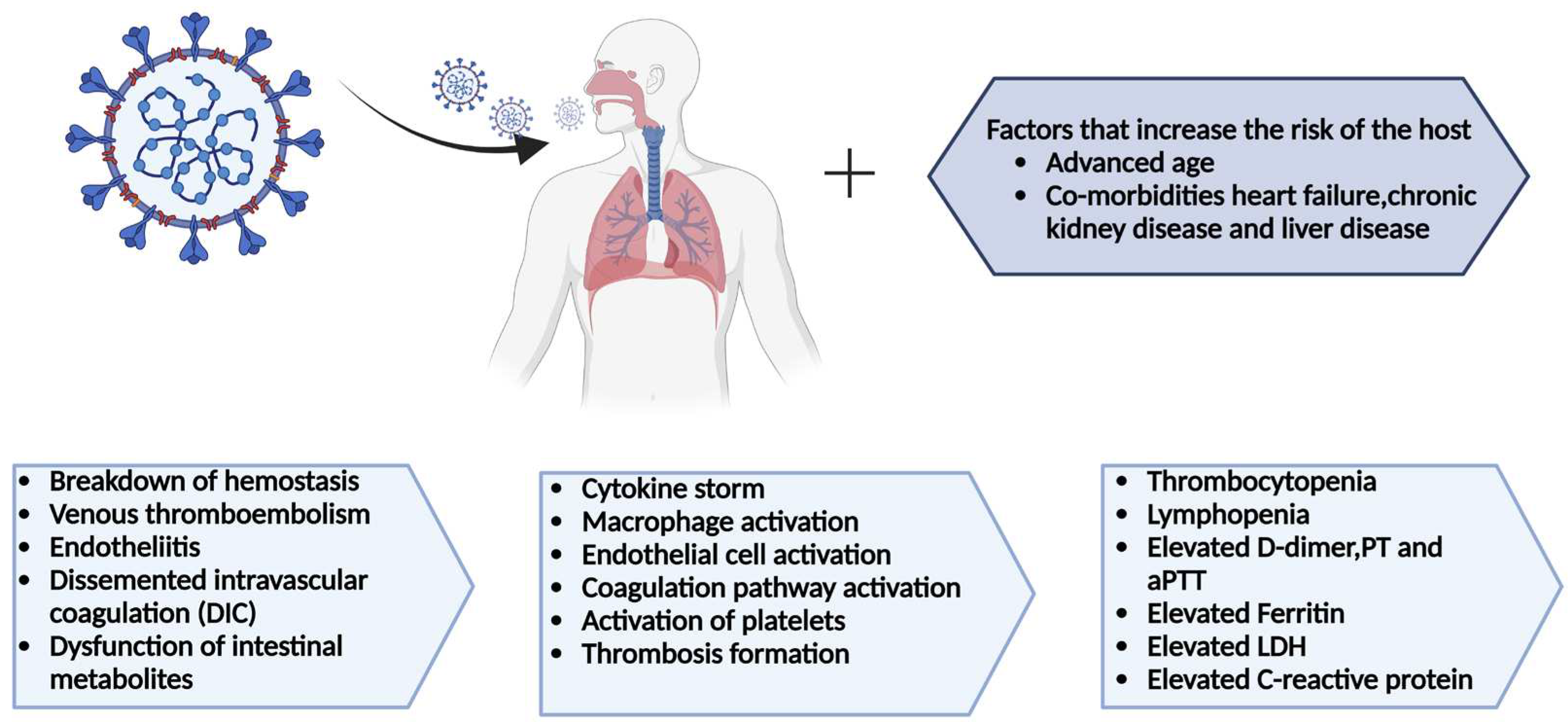
Figure 3.
In severe COVID-19 cases, biomarkers anomalies play a critical role in assessing disease severity and prognosis. These biomarkers include elevated levels of inflammatory markers, hematological biomarkers and altered coagulation parameters, as well as other biomarkers indicating tissue damage and organ dysfunction.
Figure 3.
In severe COVID-19 cases, biomarkers anomalies play a critical role in assessing disease severity and prognosis. These biomarkers include elevated levels of inflammatory markers, hematological biomarkers and altered coagulation parameters, as well as other biomarkers indicating tissue damage and organ dysfunction.
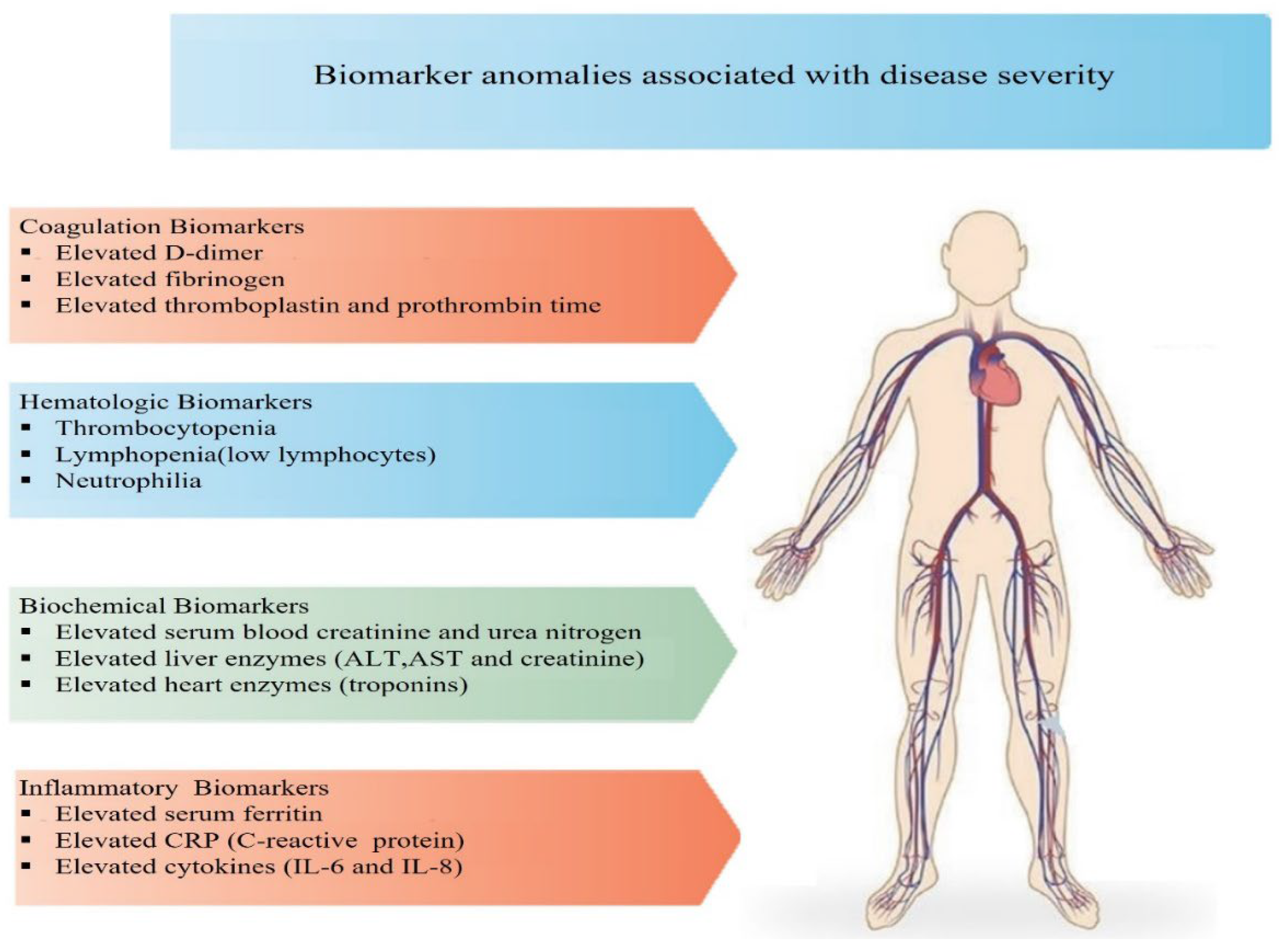
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



