
Submitted:
02 June 2023
Posted:
05 June 2023
You are already at the latest version
Abstract
Previous studies have shown that immunization within the first hours/days after birth promotes the shift from the intrauterine Th2 immune response toward the Th1 immunity resulting in lower risk of developing allergic diseases. We are currently conducting a prospective cohort study among 307 participants divided into groups based on their TB and hepatitis B vaccination status (vaccinated at birth, within the first 12 months of life or unvaccinated) and also based on whether the participants had factors contributing to the development of allergic diseases. In each group we assessed the fact of primary diagnosis of atopic dermatitis at 12 and 18 months of age. It was demonstrated that atopic dermatitis (AD) was diagnosed from birth to 12 months of age much less frequently in those infants who had received the tuberculosis (TB) vaccine from day 3 to day 7 and hepatitis B vaccine within the first 24 hours of birth, including newborns with a high risk of developing allergic diseases. The probability of onset of AD at 12 and 18 months was also lower in timely vaccinated children, even though a burdened allergic anamnesis starts playing a more central role in development of AD at this age. Our findings testify to the fact that timely BCG-M and hepatitis B vaccination can produce a protective effect against the onset of AD, yet this effect diminishes with aging.
Keywords:
BCG
; hepatitis B
; vaccination
; allergy
; atopic eczema
Introduction
Over the past few decades in developed countries we see an inexplicably growing incidence of allergic diseases characterized as the “allergy epidemic”. In particular, global incidence of AD, especially in industrially advanced countries, has grown 2-3-fold – AD is diagnosed in 15-20% of children and in 1 to 3% of adults worldwide [1]. The onset of the disease most often occurs before the age of 5, and early diagnosis and treatment are critically important for prevention of AD complications and improvement of the quality of life [2].
At the same time the comprehensive immunization coverage increased in order to reduce the communicable diseases morbidity and mortality, which resulted in an assumption that some vaccines might increase the risk of developing allergic diseases in children. Immunization is generally recognized as one of the most important achievements of public health saving millions of lives every year [3,4]. Only during the first decade of the 20th century the measles, polio and diphtheria, tetanus and pertussis vaccines annually prevented approximately 2.5 million additional deaths in children of first 5 years of life. The growth of measles vaccination global coverage which continued in early 21st century resulted in reducing measles deaths by 83% between 2000 and 2021 thus preventing in total up to 55.8 million deaths [4,5]. It should be noted that the greatest expansion of routine immunization programmes, also due to successes in development of new types of vaccines, started from 1990s when hepatitis B, rubella, Haemophilus influenzae type b and other vaccines were introduced. All this favors an active discussion of whether a ubiquitous growth of incidence of allergic diseases is possibly the price we pay for preventing higher incidence of communicable diseases.
The science data we currently have both confirm and negate the association between vaccination and allergic diseases [6,7,8,9,10].
To substantiate such direct association, some researchers suggest the hygiene hypothesis based on which each case of acute infection a child has had supposedly promotes the reduction of risk of allergic diseases in that child [11]. Which may lead us to the conclusion that a major increase in prevalence of various clinical forms of allergic diseases that we see over the past two decades is caused by changes in the environment due to improved hygiene and lower incidence of childhood infections that are being prevented mostly by paediatric vaccination [12].
On the other hand, the best evidence of lack of any association between routine immunization and allergies was obtained as a result of a Swedish double-blind study of pertussis vaccination of 9,289 children – the study did not find any association between vaccination against pertussis and development of bronchial obstruction, eczema and pollinosis [9,10].
The goal of the Tasmanian Longitudinal Health Study (TLHS), a population-based cohort study in children and adults aged 7 to 44, was to look for any association between child immunization and bronchial asthma (BA) and other allergic diseases [13]. Based on study results, no connection was found between any childhood vaccine (diphtheria, tetanus, pertussis, polio, smallpox vaccines) and diagnosing BA, food allergy or pollinosis in the study participants at age 44.
Among the first immunoprophylactic vaccines administered to neonates in some countries in the first days of life are hepatitis B and TB vaccines. As part of the national immunization schedule in the Russian Federation the BCG-M vaccine against tuberculosis is to be given on day 3 to 7 of life, and the hepatitis B vaccine is to be given within 24 hours of birth [14]. Not only the BCG vaccine is meant to protect against the severe forms of tuberculosis, but it also produces a non-specific effect on the immune system [15]. These vaccination effects are explained by the so called BCG-trained immunity when various types of epigenetic modifications occur at binding of the vaccine with NOD-2 macrophage receptors, including the DNA modifications non-coding the RNA, histone modifications and chromatine remodeling [16]. All this leads to changes in cell metabolism, regulation of development of monocytes, macrophages and other cells of the trained innate immunity. These processes are most prominent during the first weeks of the child’s life when after vaccination the immune response shifts from Th2-type to predominantly Th1-type cell response.
An unpredictable additional protective effect of mass administration of BCG vaccine was described in early 2020 in the period of spread of the first wave of the novel coronavirus infection SARS-CoV-2 (the initial, ancestor Wuhan strain SARS-CoV-2). When studying the epidemiology of COVID-19 it was noticed that in the countries with the highest incidence of COVID-19 the population was not given the BCG vaccine [17,18]. In particular, after analyzing the relationship between the incidence of COVID-19 and the results of implementation of national BCG immunization schedules in 178 countries around the world, American researchers hypothesized there was a protective effect of the BCG vaccine and discovered that in countries with the existent routine immunization against TB the SARS-CoV-2 incidence and death rate were lower [19]. In spring 2020 a list of epidemiological studies was published demonstrating the protective effect of the fact of population being immunized by the BCG vaccine that helped reduce COVID-19 morbidity and mortality in various countries around the globe [20,21,22].
The key goal of our study was to investigate whether the vaccination of infants against TB (with BCG-M) and hepatitis B may play a role in development of atopic dermatitis being one of the most common clinical forms of allergic diseases.
To obtain the most valid results we believe it necessary to take into consideration the factors predisposing to early onset of atopic dermatitis, such as a burdened family history of allergic diseases, mother taking antibiotics during pregnancy or antibiotics given to the neonate after birth and delay in breastfeeding initiation [23,24].
Materials and Methods
Participants and Data
We are conducting a prospective observational cohort study in 307 children born in the same period (in April-June 2021) residing in the same part of Moscow and being monitored at children’s municipal outpatient clinic No. 133 of the Department of Health of the city of Moscow. We are planning an 18-year follow-up (the first checkpoint is at 18 months and then at the age of 3). The study design is described in Figure 1.
All study participants have the same level of access to care and same quality of care. After discharge from the maternity hospital a paediatrician examines the neonates twice at their home, this is why in children’s medical records there is information on family history as well as social and living conditions.
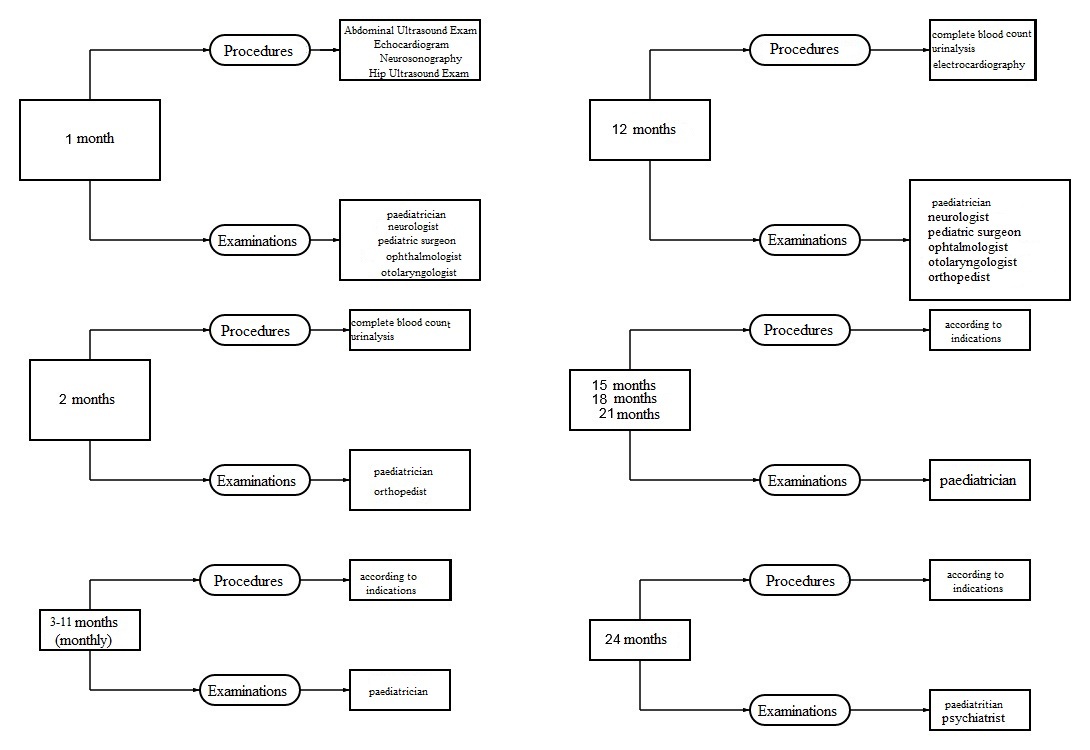
Based on current Russian law during their first year all infants are entitled to state-funded preventive monthly well-child visits and checkups by a paediatrician and specialty physicians (based on decreed schedule as shown in Figure 2) for assessment of their growth and psychomotor development, nutritional and general health status and also for immunization. The participants of our study went to the children’s municipal outpatient clinic for routine well-child checkups by a paediatrician at least once every three months.
The study participants between 12 and 23 months of age had well-child visits with a paediatrician at least twice during the year, their health status was evaluated and routine immunization was performed. 12 participants dropped out of the study during the first year of follow-up due to relocation, and 8 participants dropped out by the age of 18 months.
Analysis of medical records and documents (vaccination certificate, maternity hospital discharge document, records of child examination by physicians) was performed based on data copied from the Unified Medical Information and Analysis System (EMIAS) functioning in Moscow where all medical data on all children residing in Moscow is entered. Due to this system any loss of results or their misinterpretation is absolutely impossible. Data from obstetric histories and family health histories, social and living conditions, vaccination status, results of actual examination of a child as well as final medical reports by paediatrician and specialty physicians were analized.
In order to consider a possible effect of the first TB and hepatitis B vaccination all study participants were divided into 3 groups:
- Vaccinated at birth (with BCG-M, hepatitis B vaccine or both). Vaccination was considered timely if it was performed within time limits specified in the National Immunization Schedule;
- Vaccinated in a catch-up mode in the first year of life (with BCG-M, hepatitis B vaccine or both);
- Unvaccinated in the first year of life.
In each group children were subdivided into 2 subgroups depending on whether they had any factors predisposing for development of allergic diseases: children without the risk of allergic disorders and children with the risk of allergic disorders.
The following were considered to be the risk factors for development of allergic diseases:
- Cesarean birth;
- antibiotic treatment of the mother during pregnancy or antibiotic treatment of the neonate during first week of life;
- late breastfeeding initiation (more than 30 minutes after birth);
- allergic diseases in nearest relatives (a burdened family history).
The clinical endpoint of the study was the fact of primary diagnosis of AD made by the moment of assessment of the patients’ medical data performed at 12 and at 18 months. Atopic dermatitis was diagnosed based on clinical findings and medical history in conformity with international and national clinical guidelines, such diagnosis being based on relevant IСD-10-CM codes.
Ethical Considerations
Considering that by design this study is characterized as a completely non-interventional observational prospective study in which the subject of research is medical documentation and the study objectives include analysis of depersonalized data, expert examination of the study protocol by the ethics committee was not performed.
Eligibility Criteria
Inclusion criteria:
- consent obtained from parents or legal representatives;
- infants born from April through June 2021, residing in the area near Moscow children’s municipal outpatient clinic No.133 to which they are assigned and being permanently monitored at the said clinic;
- infants having no absolute medical contraindications for vaccination;
- infants having no reasonable temporary medical contraindications for vaccination at birth;
- infants born after 35 weeks’ gestation.
Exclusion criteria:
- change of health facility to which a child is assigned to;
- withdrawal of consent by the child’s representatives at any phase of the study.
Data Analysis and Statistics
Statistical analysis was performed using the Analysis ToolPak of Microsoft Office Excel 2010.
Categorical data were described in absolute values and percentages. Comparison of percentages in analysis of multi-way contingency tables (cross tabulation) was performed using the Pearson Chi-Square test, and in analysis of confusion matrices the Fisher’s exact test was used. P-values less than 0.05 were considered statistically significant at CI=95%.
Results
From April through June 2021 a total of 307 children were included in the study. Characteristics of the study participants based on gender, vaccination status, presence of burdened history of allergic diseases and onset of AD are shown in Table 1.
155 boys and 140 girls participated in the study. One third of the study participants (n=93; 31.5%) had established risk factors for development of allergic diseases.
We discovered an insufficient TB and hepatitis B vaccination coverage in infants in their first year of life. In particular, 231 infant (78.3%) received the TB vaccine and 204 neonates (69.2%) received a hepatitis B vaccine at the maternity hospital. Only 203 study participants (68.8%) received both vaccines timely. In the first year of life in the framework of catch-up vaccination 50 infants (16.9%) received the BCG-M vaccine and 69 infants (23.3%) started their hepatitis B vaccination. By 12 months 14 infants (4.7%) had not received a TB vaccine, 22 infants (7.5%) had not received a single dose of hepatitis B vaccine and 14 infants (4.7 %) had not been vaccinated against both infections.
By 18 months AD was diagnosed in 93 children (32.4%). Among them 73 study participants (78.5%) had the onset of atopic dermatitis in their first year of life – 34 of them (46.6%) had risk factors for allergies. In 20 study participants (21.5%) the onset of AD was between 12 and 18 months of age and all of them (100%) were from the high risk group.
In Table 2 you see the data on infants with the onset of AD by 12 months depending on whether and when they had been vaccinated against TB and hepatitis B and based on whether they had any risk factors for allergic diseases.
AD was diagnosed in the first year of life in 35 study participants (15.2%) who had received the BCG-M vaccine on day 3 to 7 after birth, in 33 infants (66%) vaccinated later and in 5 infants (35.7%) unvaccinated against TB. In the subgroup of infants with risk factors for development of allergic diseases AD was diagnosed in 11 infants (18%) BCG-M-vaccinated at the maternity hospital, in 18 infants (75%) vaccinated in their first year of life and in 5 infants (62.5%) unvaccinated with BCG-M in their first year of life. In the subgroup of infants having no risk factors for allergic diseases AD was diagnosed in 24 infants (14.1%) who had received the TB vaccine at the maternity hospital and in 15 infants (57.7%) vaccinated during their first year of life. Among infants with established AD diagnosis and without a burdened history of allergic diseases there were no infants who had not received the BCG-M vaccine. Data on prevalence of AD depending on BCG-M vaccination status is given in Table 2A and in Figure 3.
AD was diagnosed in the first year of life in 36 study participants (17.6%) vaccinated against hepatitis B within 24 hours of birth, in 31 infant (44.9%) vaccinated later and in 7 unvaccinated infants (31.8%). In the subgroup of infants having risk factors for developing allergic diseases AD was diagnosed in 12 infants (24%) vaccinated at the maternity hospital, in 17 infants (50%) vaccinated in their first year of life and in 4 infants (44.4%) who had not received the hepatitis B vaccine. In the subgroup of infants having no risk factors for allergic diseases AD was diagnosed in 24 infants (15.6%) vaccinated at the maternity hospital, in 14 infants (40.0%) vaccinated in their first year of life and in 3 infants (23.1%) who had not been vaccinated against hepatitis B. Data on prevalence of AD depending on hepatitis B vaccination status is shown in Table 2B and in Figure 4.
AD was diagnosed in the first year of life in 33 infants (16.3%) timely vaccinated with both vaccines, in 6 infants who had received at least one of the vaccines at the maternity hospital, and in 35 (56.5%) infants who had not been vaccinated at the maternity hospital with either vaccine. In the subgroup of infants having risk factors of allergic diseases AD was diagnosed in 10 infants (20.8%) vaccinated against both infections at the maternity hospital, in 3 infants (20.0%) who had received at least one vaccine on time, and in 21 infant (70.0%) not vaccinated at the maternity hospital. In the subgroup of infants having no risk of allergic diseases AD was diagnosed in 23 infants (14.8%) vaccinated at the maternity hospital with both vaccines, in 2 infants (11.1%) vaccinated with at least one vaccine and 14 infants (48.3%) who had not received any vaccines. Data on prevalence of AD depending on TB and hepatitis B vaccination status is shown in Table 2C and in Figure 5.
Table 3 contains data of 18 months old patients with confirmed diagnosis of AD depending on whether and when they had been vaccinated against TB and hepatitis B and on presence of any predisposing factors of allergies.
During the whole follow-up period of 18 months AD was diagnosed in 52 study participants (23.1%) timely vaccinated with BCG-M, in 35 children (71.4%) vaccinated later and in 6 children (46.2%) who had not received any vaccine in their first year of life. In the subgroup of infants having risk factors for allergic diseases AD was diagnosed in 26 children (44.1%) vaccinated against TB at the maternity hospital, in 20 children (83.3%) vaccinated in their first year of life and in 5 infants (71.4%) who had not received the BCG-M. In the subgroup of children having no risk factors for development of allergic diseases AD was diagnosed in 26 children (15.7%) vaccinated with BCG-M at the maternity hospital, in 15 children (100%) with untimely vaccination and in 1 unvaccinated child (16.7%). Data on prevalence of AD depending on BCG-M vaccination status of children is shown in Table 3A and in Figure 6.
During the first 18 months of life AD was diagnosed in 43 study participants (21.7%) vaccinated against hepatitis B within 24 hours of birth, in 34 children (50.0%) vaccinated later and in 10 unvaccinated children (47.6%). In the subgroup of children having risk factors for allergic diseases AD was diagnosed in 25 children (52.1%) vaccinated against hepatitis B at the maternity hospital, in 21 child (61.8%) vaccinated in the first year of life and in 7 children (87.5%) who had not received the hepatitis B vaccine. In the subgroup of children having no risk factors for development of allergic diseases AD was diagnosed in 18 children (12.0%) vaccinated at the maternity hospital, in 13 children (38.2%) vaccinated in their first year of life and in 9 children (69.2%) who had not received the hepatitis B vaccine. Data on prevalence of AD depending on hepatitis B vaccination status of children is shown in Table 3B and in Figure 7.
By 18 months AD was diagnosed in 44 study participants (22.3%) with timely vaccination with both vaccines, in 8 children (25.8 %) who had received at least one of the vaccines at the maternity hospital, and in 35 (59.3%) children who had not been vaccinated at the maternity hospital with either vaccine. In the subgroup of children having risk factors for development of allergic diseases AD was diagnosed in 25 children (51.0%) vaccinated at the maternity hospital with BCG-M and hepatitis B vaccine, in 6 children (42.9%) who had received at least one vaccine on time, and in 22 children (42.9%) not vaccinated at the maternity hospital. In the subgroup of children with no risk factors for allergic diseases AD was diagnosed in 23 children (15.4%) who had received both vaccines at the maternity hospital, in 2 children (11.8 %) vaccinated with at least one vaccine, and in 13 children (41.9 %) who had not received any vaccines. Data on prevalence of AD depending on TB and hepatitis B vaccination status is given in Table 3C and in Figure 8.
Discussion
AD remains a widespread disease in the paediatric population all around the world. Incidence of AD varies in different countries – from 0.65% in Tunisia to 35% in Sweden [25,26]. In the framework of the ongoing discussion of the possible role of mass immunization programmes in the growing incidence of allergic diseases we believe it important to investigate the possible contribution of immunization performed in the first days after birth in development of the earliest forms of allergic diseases in children. For this very purpose we evaluated the prevalence of newly diagnosed AD over the first 18 months of life in children permanently monitored by a paediatrician at Moscow children’s outpatient clinic No.133 depending on whether these children were immunized against TB and hepatitis B and on how timely their immunization was. The results of the study should be highly significant for implementation of routine immunization programmes, especially in children having a burdened history of allergic diseases.
In our study it was established that AD was diagnosed in one-third of children by 18 months of age (32.4%) which on the whole is higher than the Russian national statistics for 2018 being 20% for paediatric population [27]. And the majority of those children had the onset of AD in their first year of life (78.5%) as compared to those who were 18 months old (21.5%). This is in line with the epidemiological observations of the inverse relationship between the prevalence and incidence of AD and the patient age [28].
In this study we investigated a possible impact of BCG-M and hepatitis B vaccines on the onset of AD. All study participants were divided into groups depending on the time of vaccination (at birth, in the first year of life or unvaccinated) and also by presence or absence of risk factors for development of allergic diseases (a Cesarean birth, late breastfeeding initiation, antibiotic treatment of the infant’s mother during pregnancy, close relatives with allergic diseases). To distinguish between the effect of vaccination and that of predisposing factors, we evaluated AD diagnosed by 12 and by 18 months of age separately for the subgroup of children with risk factors for allergic diseases and the subgroup of children having no such risk factors.
Independently of the type of vaccine a child had received (BCG-M, hepatitis B vaccine or both) and of the time the vaccine had been given (timely vaccination, catch-up vaccination or no immunization) the AD incidence was higher in the subgroup of children with risk factors for allergic diseases. And predisposition to allergies plays the key role in the onset of AD in the second year of life because all children who first developed AD between 12 and 18 months were from the high-risk subgroup. The unquestionable significance of the impact of the above mentioned predisposing factors on development of AD is demonstrated in the group of unvaccinated children: the majority of participants with the diagnosed AD are in the subgroup of patients with risk factors for allergies. This underscores the representativeness of the sample and validity of the data obtained.
In the course of the study we also discovered untimely vaccination with BCG-M and hepatitis B vaccines in the paediatric population we monitored in our study, as evidenced by insufficient TB and hepatitis B immunization coverage in the first week and in the first 24 hours of life - 78.3% and 69.2% respectively.
The lowest detectability of AD by 12 months was in the group of timely vaccinated infants independently of whether they had allergy risk factors or not. We registered a protective effect against development of AD produced by the BCG-M and by hepatitis B vaccines as well as when both vaccines had been given in the first 7 days after birth. The prevalence of AD is significantly higher among children who had not received any vaccines at the maternity hospital, as compared to those who had been fully vaccinated and those who had received at least one vaccine at the maternity hospital (70% vs 20% and 20.8%, respectively, p<0.01). This statistically significant difference was established both for the group of children without risk factors and for the group of children with a burdened allergic history. For the overall population of children statistically significant differences in the number of cases of onset of AD were found when comparing groups of infants with timely vaccination and of those who had not been immunized against both TB and hepatitis B in their first year of life. For separate subgroups the findings are not statistically significant due to the small number of participants.
This data is in line with the results of many other randomized trials in one of which it was demonstrated that if the BCG-Denmark (Danish strain 1331) vaccine is given immediately after birth to newborns predisposed to allergies, it reduces the incidence of AD in their first year of life [29,30]. In the study performed by Farooqi I.S. and Hopkin J.M. with 1934 participants in Oxfordshire county (U.K.) [31] a weak positive association was discovered between vaccination against pertussis and development of allergic diseases, yet no connection was found between the measles vaccine and onset of allergic disorders.
Our findings are no surprise: it is well known that the hepatitis B vaccine can have a protective effect on immune response like it is with BCG and reduce the level of total IgE [32]. In this case the discovery of protective effect of infant immunization can be used to prevent the development of atopic diseases in older age, as also shown in other more recent studies [33,34].
On the contrary, one should not neglect published data showing negative effect of immunization on development of allergic diseases. In particular, in the study performed by T.Kempetal [35] during the 10-year follow-up of 1265 children born in 1977 it was discovered that only 23 unvaccinated children had no allergies. Yet the authors of the study declared too many restrictions and biased conditions in their study methodology that might have skewed the findings.
Unlike the Australian study in which delayed vaccination with diphtheria, tetanus and acellular pertussis vaccine (DTaP) was associated with lower incidence of AD and fewer drugs prescribed for its therapy [36], our study has not demonstrated any protective effect of the catch-up TB and hepatitis B immunization as compared to timely vaccination of infants.
One of systematic reviews did not discover any possible association between TB vaccination and onset of allergic diseases [37]. During analysis of the existing literature one study was discovered which demonstrated a shift toward increased Th1 cell response in patients with various allergies after getting the hepatitis B vaccine which can also be considered an indirect evidence of protective role of immunization [32].
Based on our study results, the protective effect of timely vaccination against the onset of AD is especially strong in the first year of life and diminishes in the second year. In the children we observed in our study this trend was still present by the age of 18 months, but was fading away. Moreover, one should remember that all our patients who developed AD in the second year of life had allergy risk factors, and the majority of them had timely vaccination. Much more frequently the onset of AD during the first 18 months of life occurred in children without allergy risk factors who had not received a single vaccine in the maternity hospital, while in high-risk group children such correlation was insignificant. This might be explained by a stronger effect of a predisposing factor on the pathogenesis of allergic disease and diminishing protective effect of vaccination in the second year of life.
Similar results were obtained in an extended meta-analysis which demonstrated the temporariness of protective effect of neonatal BCG-M vaccination against the development of BA in children from ages 6 through 11, while in adolescents ages 13 through 17 this effect was not present any more [38].
This observation correlates with the data from other studies that established no significant association between BCG-M vaccine and the development of food allergy in infants by the age of 13 months [30,39]. Based on results obtained we might hypothesize that vaccination has a protective effect mainly in the first year of life, both in general population and in infants with high risk of development of allergic diseases, and in the second year of life this effect weakens. Yet it is highly problematic to evaluate the association between the onset of AD and vaccination because the sample we studied was small.
We should also mention the advantages of our study increasing the representativeness of the sample data as compared to earlier studies. Here are some of these advantages:
- follow-up of children living in the same part of a big city and having similar social and living conditions;
- continuous health supervision of all children participating in the study starting from their birth which promotes active detection of early-onset disorders;
- uniform approach to organization and implementation of preventive vaccination and also to diagnosing AD;
- data on vaccination status is retrieved from electronic medical records which significantly minimizes the risk of data loss and the risk of getting wrong data.
Yet we have to admit that we did not take into consideration immunization against other communicable diseases and did not investigate whether the children participating in our study had received a second and third shot of hepatitis B vaccine. Such effect of the association between the prevalence of BA and AD among infants at 12 months of age and the number of inactivated vaccines given in the first 6 months of life was hypothesized in an earlier study which was based on the cumulative exposure to adjuvants contained in each dose of the vaccineы used [40].
In addition, in our study we did not look into the effect of other factors predisposing for development of allergic diseases such as duration of breastfeeding, exposure to secondhand smoke, the age of introduction of complementary foods, presence of pets in the household, intake of medicinal products, etc.
To obtain more valid data the follow-up of the study participants should be continued, also in order to evaluate the severity and progress of AD and the need for pharmacotherapy depending on the vaccination status of children. And we also need analysis of more numerous groups of participants having all possible risk factors for development of allergic diseases.
And please keep in mind that when making final decision on possible impact of paediatric vaccination on development of allergic diseases in infancy one should realize with responsibility the consequences it may lead to as this can possibly undermine the effectiveness of immunization programmes.
Conclusions
The growing incidence of allergic diseases is a genuine concern all around the world. Our study results demonstrate that TB and hepatitis B vaccines given in the first hours/days after child’s birth not only do not promote early onset of allergic diseases but they can prevent the development of AD in children, including those having genetic predisposition for allergic diseases. This is due to the Th2/Th1 shift of immune response in neonates who received timely vaccination, and such vaccination has the strongest protective effect in the first year of the child’s life. The data obtained can be used for awareness-building in communication with patients’ parents and healthcare professionals with the purpose of enhancing immunization adherence.
Conflicts of Interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
- C. Avena-Woods. Overview of Atopic Dermatitis. Am J Manag Care. 2017;23:-S0.
- Eichenfield LF, Tom WL, Chamlin SL, et al. Guidelines of care for the management of atopic dermatitis: section 1. diagnosis and assessment of atopic dermatitis. J Am Acad Dermatol. 2014;70(2):338-351. [CrossRef]
- Centers for Disease Control and Prevention (CDC). Ten great public health achievements--United States, 1900-1999. MMWR Morb Mortal Wkly Rep. 1999 Apr 2;48(12):241-3. Centers for Disease Control and Prevention (CDC). [PubMed]
- Ten great public health achievements--worldwide, 2001-2010. MMWR Morb Mortal Wkly Rep. 2011 Jun 24;60(24):814-8. [PubMed]
- Anna, A. Minta et all. Progress Toward Regional Measles Elimination — Worldwide, 2000–2021. Morbidity and Mortality Weekly Report. 2022;71(47):1489-1495.
- Wickens, K. , Crane J., Kemp T. et al. A case-control study of risk factors for asthma in New Zealand children. Aust N Z J Public Health. 2001; 25:44–49. 20. [CrossRef]
- Mullooly, JP. , Pearson J., Drew L. et al. Wheezing lower respiratory disease and vaccination of full-term infants. Pharmacoepidemiol Drug Saf. 2002; 11:21–30. [CrossRef]
- Henderson J, North K, Griffiths M, Harvey I, Golding J. Pertussis vaccination and wheezing illnesses in young children: prospective cohort study. The Longitudinal Study of Pregnancy and Childhood Team. BMJ. 1999; 318:1173–1176. [CrossRef]
- Nilsson L, Kjellman NI, Storsaeter J, Gustafsson L, Olin P. Lack of association between pertussis vaccination and symptoms of asthma and allergy. JAMA. 1996; 275:760. 23. [CrossRef]
- Nilsson L, Kjellman NI, Bjorksten B. A randomized controlled trial of the effect of pertussis vaccines on atopic disease. Arch PediatrAdolesc Med. 1998;152: 734–738. 7: 1998;152.
- Strachan, DP. Family size, infection and atopy: the first decade of the “hygiene hypothesis”. Thorax. 2000 Aug;55 Suppl 1(Suppl 1):S2-10. PMID: 10943631; PMCID: PMC1765943. [CrossRef]
- Umetsu DT, McIntire JJ, Akbari O, Macaubas C, DeKruyff RH. Asthma: an epidemic of dysregulated immunity. Nat Immunol. 2002 Aug;3(8):715-20. [CrossRef] [PubMed]
- Matheson MC, Haydn Walters E, Burgess JA. et al. Childhood immunization and atopic disease into middle-age--a prospective cohort study. Pediatr Allergy Immunol. 2010 Mar; 21(2 Pt 1):301-6. Epub 2009 Dec 7. [CrossRef] [PubMed]
- Prikaz MZ RF ot 06.12.2021 №1122n «Ob utverzhdenii natsionalnogo kalendarya profilakticheskikh provivok i kalendarya profilakticheskikh provivok po epidemicheskim pokazaniyam».
- Chen, J., Gao, L., Wu, X. et al. BCG-induced trained immunity: history, mechanisms and potential applications. J TranslMed 21, 106 (2023). [CrossRef]
- Moorlag SJCFM, Rodriguez-Rosales YA, Gillard J. et al. BCG Vaccination Induces Long-Term Functional Reprogramming of Human Neutrophils. Cell Rep. 2020 Nov 17;33(7):108387. PMID: 33207187; PMCID: PMC7672522. [CrossRef]
- Escobar LE, Molina-Cruz A, Barillas-Mury C. BCG vaccine protection from severe coronavirus disease 2019 (COVID-19). PNAS. 2020; 117(30):17720–17726. [CrossRef]
- Miller A, Reandelar M-J, Fasciglione K, et al. Correlation between universal BCG vaccination policy and reduced morbidity and mortality for COVID-19: an epidemiological study. medRxiv. Preprint March 2020. [CrossRef]
- Hegarty P-K, Kamat A, Zafirakis H, DiNardo A. BCG vaccination may be protective against COVID-19. PreprintMarch 2020. 20 March. [CrossRef]
- Sala G., Miyakawa T. Association of BCG vaccination policy with prevalence and mortality of COVID-19. medRxiv. Preprint May 2020. 20 May. [CrossRef]
- Shet A, Ray D, Malavige N, et al. Differential COVID-19-attributable mortality and BCG vaccine use in countries. medRxiv. Preprint April 2020. 20 April. [CrossRef]
- Berg MK, Yu Q, Salvador CE, et al. Mandated BCG vaccination predicts flattened curves for the spread of COVID-19. medRxiv.Preprint April 2020. 20 April. [CrossRef]
- Untersmayr E., Bax HJ., Bergmann C. et al. AllergoOncology: Microbiota in allergy and cancer - A European Academy for Allergy and Clinical Immunology position paper. Allergy. 2019 Jun;74(6):1037-1051. Epub 2019 Mar 6. PMCID: PMC6563061. [CrossRef]
- Kiwako Yamamoto-Hanada et al. Influence of antibiotic use in early childhood on asthma and allergic diseases at age 5. Ann Allergy Asthma Immunol. 119 (2017) 54-58.
- Hadi HA, Tarmizi AI, Khalid KA, Gajdács M, Aslam A, Jamshed S. The Epidemiology and Global Burden of Atopic Dermatitis: A Narrative Review. Life (Basel). 2021 Sep 9;11(9):936. PMID: 34575085; PMCID: PMC8470589. [CrossRef]
- Wollenberg A., Barbarot S., Bieber T. et al. Consensus-based European guidelines for treatment of atopic eczema (atopic dermatitis) in adults and children: part I. J Eur Acad Dermatol Venereol. 2018;32(5): 657–682. [CrossRef]
- Klinicheskiye recommendatsii «Atopichesky dermatit», odobrenniye Nauchno-prakticheskim sovetom Minzdrava Rossii. 2021.
- Kubanov A.A., Bogdanova E.V. Organizatsiya i rezultaty okazaniya meditsinskoi pomoschi po profilyu “dermatovenerologhiya” v Rossiiskoi Federatsii. Itoghi 2018 goda. Vestnik dermatologhii I venerologhii. 2019; 95(4):8–23. [CrossRef]
- Pittet LF, Messina NL, et al. Prevention of infant eczema by neonatal Bacillus Calmette-Guérin vaccination: The MIS BAIR randomized controlled trial. Allergy. 2022 Mar;77(3):956-965. Epub 2021 Aug 9. [CrossRef] [PubMed]
- Thøstesen LM, Kjaergaard J, et al. Neonatal BCG vaccination and atopic dermatitis before 13 months of age: A randomized clinical trial. Allergy. 2018 Feb;73(2):498-504. Epub 2017 Oct 9. [CrossRef]
- Farooqi IS, Hopkin JM. Early childhood infection and atopic disorder. Thorax. 1998;53:927–932.
- Shurmipa IA., Meshkova RYa., Sazonenkova LV. Rol’ sistemy tsitokinov u patsientov s allergopatologiei, privitykh rekombinantnymi vaktsinami protiv gepatita B. Mir virusnykh gepatitov. 2005; (11):5–6. (In Russ).33. Zhao K, Miles P, Hubbard R, et al. Bacille Calmette Guerin Vaccination in Early Childhood and Risk of Allergic Disease: A Systematic Review and Meta-analysis of data from 13 large scale studies. Authorea. 2020. [CrossRef]
- Navaratna S, EstcourtM J, Burgess J, et al. Childhood vaccination and allergy: A systematic review and meta-analysis. Allergy. 2021;76(7):2135–2152. [CrossRef]
- Kemp T, Pearce N, Fitzharris P, et al. Is infant immunization a risk factor for childhood asthma or allergy? Epidemiology. 1997;8:678–680.
- Kiraly N, Koplin JJ, Crawford NW, Bannister S, Flanagan KL, Holt PG, et al. Timing of routine infant vaccinations and risk of food allergy and eczema at one year of age. Allergy. 2016;71:541–9. [CrossRef]
- Arnoldussen DL, Linehan M, Sheikh A. BCG vaccination and allergy: a systematic review and meta-analysis. J Allergy Clin Immunol. 2011 Jan;127(1):246-53, 253.e1-21. Epub 2010 Oct 8. PMID: 20933258. [CrossRef]
- Mary F. Linehan et al. Does BCG vaccination protect against childhood asthma? Final results from the Manchester Community Asthma Study retrospective cohort study and updated systematic review and meta-analysis. J Allergy Clin Immunol. 2014;133:688-95. [CrossRef]
- Thøstesen LM, Kjaer HF, Pihl GT, Nissen TN, Birk NM, Kjaergaard J, Jensen AKG, Aaby P, Olesen AW, Stensballe LG, Jeppesen DL, Benn CS, Kofoed PE. Neonatal BCG has no effect on allergic sensitization and suspected food allergy until 13 months. PediatrAllergyImmunol. 2017 Sep;28(6):588-596. [CrossRef]
- Yamamoto-Hanada et al. Cumulative inactivated vaccine exposure and allergy development among children: a birth cohort from Japan. Environmental Health and Preventive Medicine. 2020; 25:27. [CrossRef]
Figure 1.
Study design.
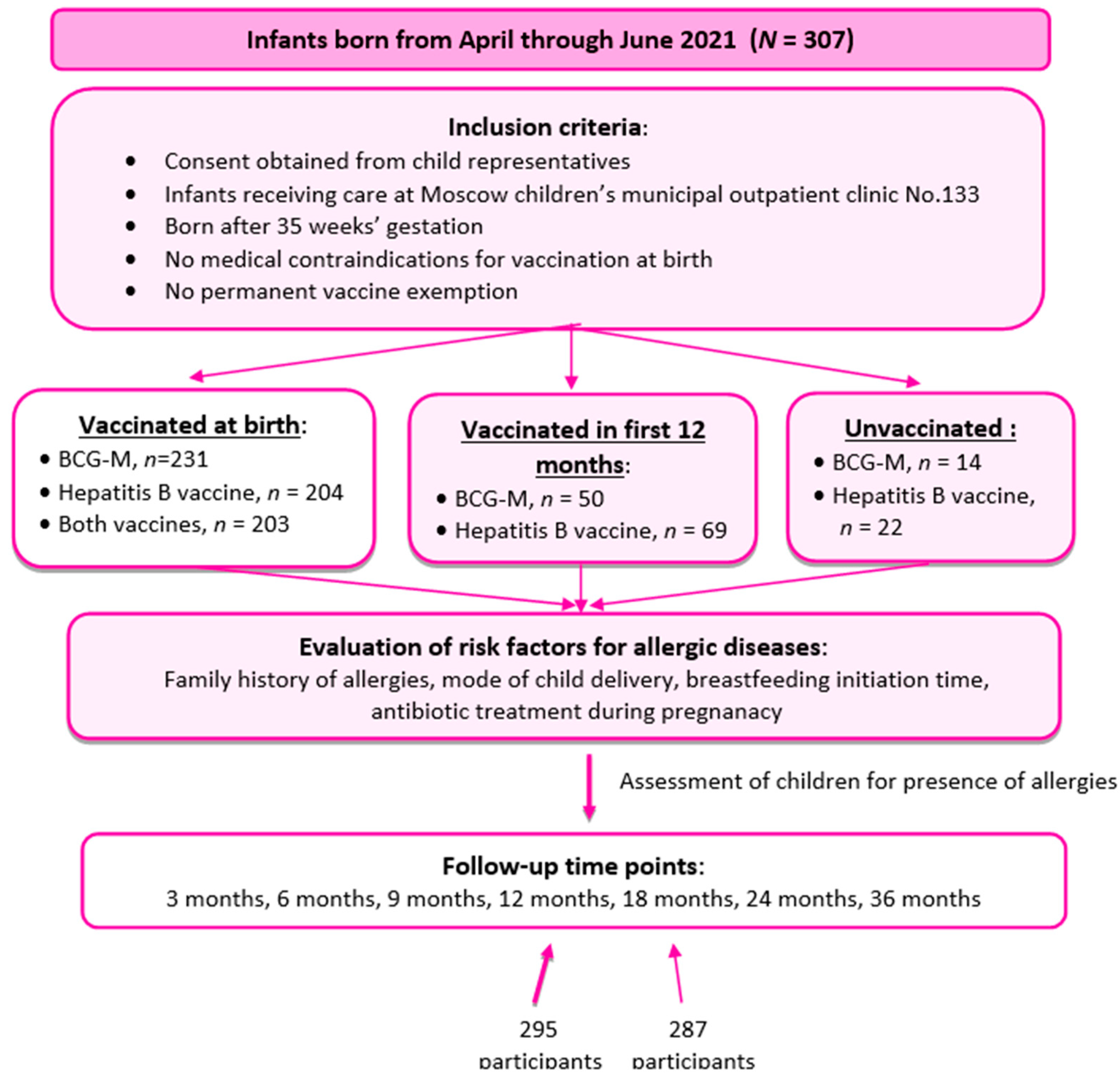
Figure 2.
Schedule of well-child visits and chekups .
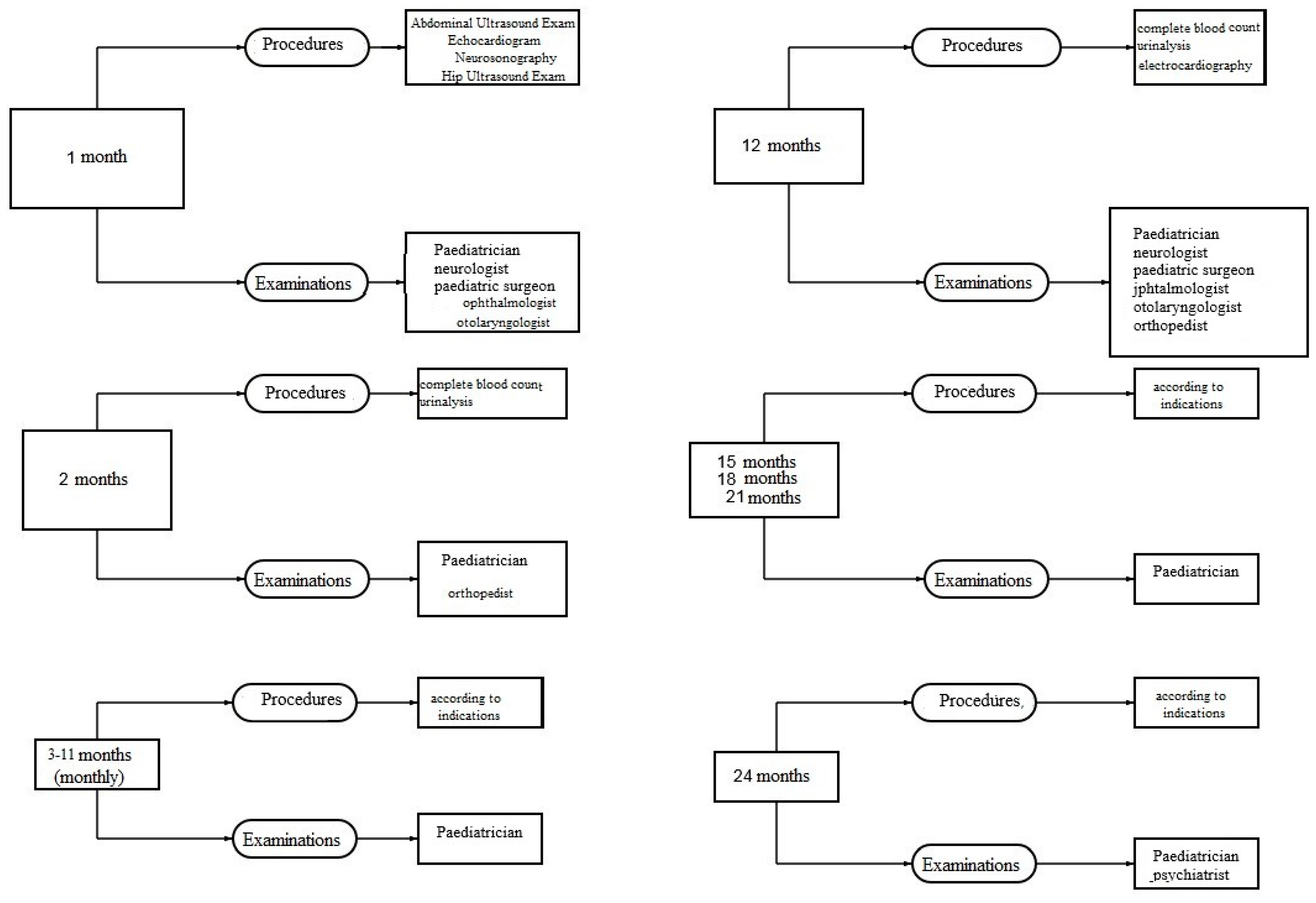
Figure 3.
Atopic dermatitis prevalence in the first year of life depending on BCG-M vaccination status and presence of risk factors for allergic diseases, % (n=295).
Figure 3.
Atopic dermatitis prevalence in the first year of life depending on BCG-M vaccination status and presence of risk factors for allergic diseases, % (n=295).
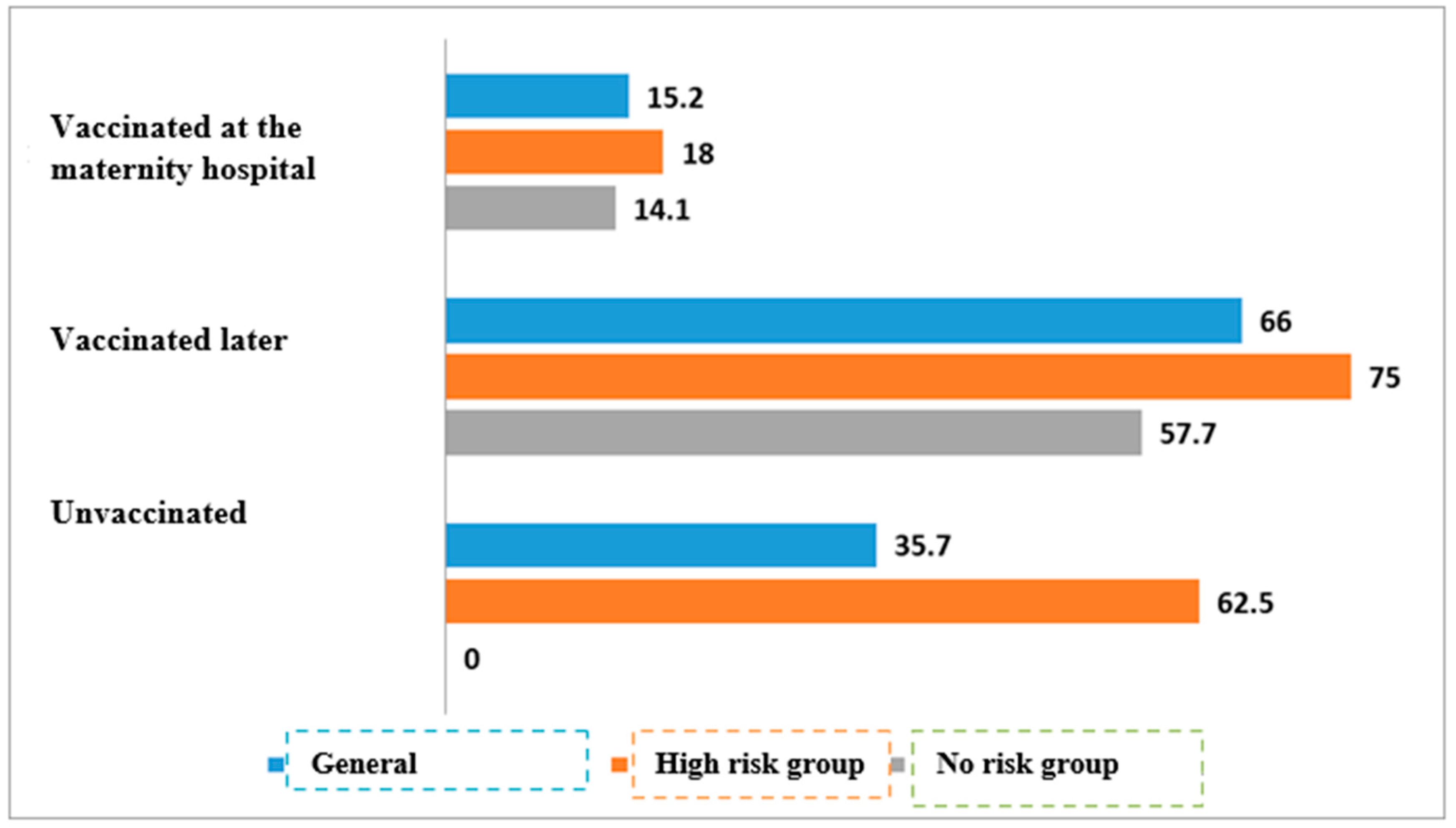
Figure 4.
Prevalence of atopic dermatitis in the first year of life depending on hepatitis B vaccination status and presence of risk factors for allergic diseases, % (n=295).
Figure 4.
Prevalence of atopic dermatitis in the first year of life depending on hepatitis B vaccination status and presence of risk factors for allergic diseases, % (n=295).
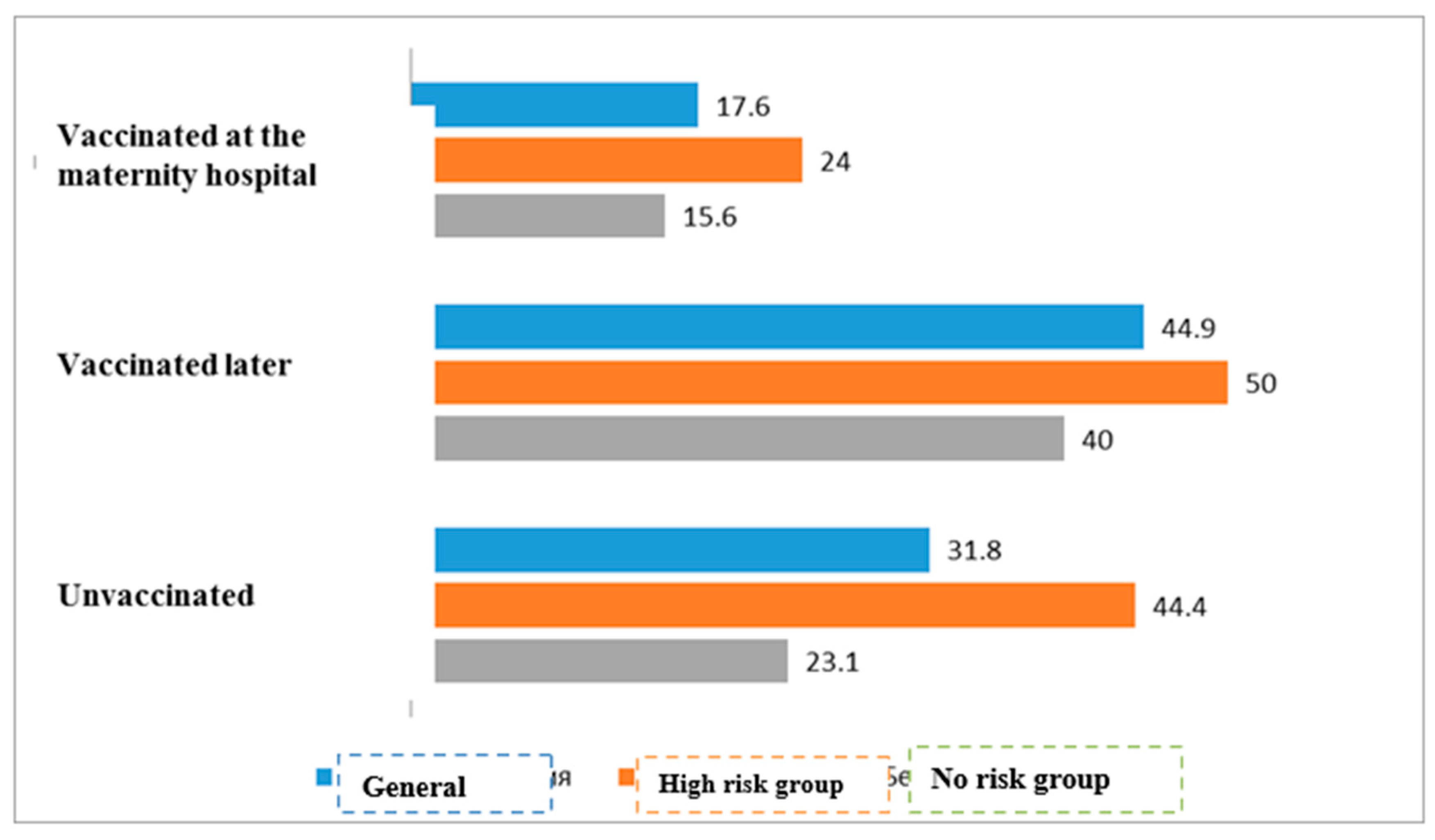
Figure 5.
Prevalence of atopic dermatitis in the first year of life depending on timeliness of TB and hepatitis B vaccination and presence of risk factors for allergic diseases, % (n=295) .
Figure 5.
Prevalence of atopic dermatitis in the first year of life depending on timeliness of TB and hepatitis B vaccination and presence of risk factors for allergic diseases, % (n=295) .
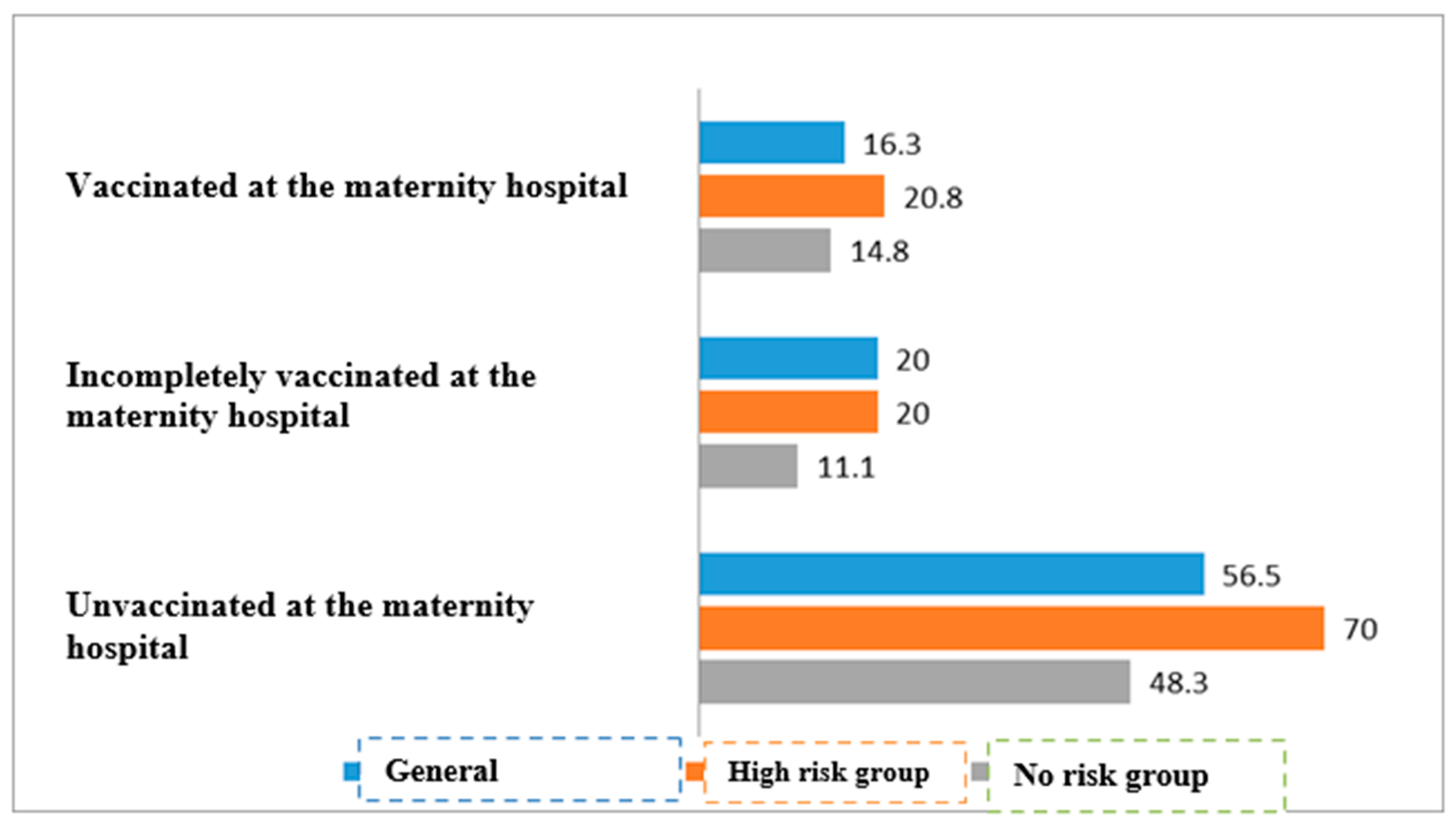
Figure 6.
Prevalence of atopic dermatitis by 18 months of age depending on BCG-M vaccination status and presence of risk factors for allergic diseases, % (n=287).
Figure 6.
Prevalence of atopic dermatitis by 18 months of age depending on BCG-M vaccination status and presence of risk factors for allergic diseases, % (n=287).
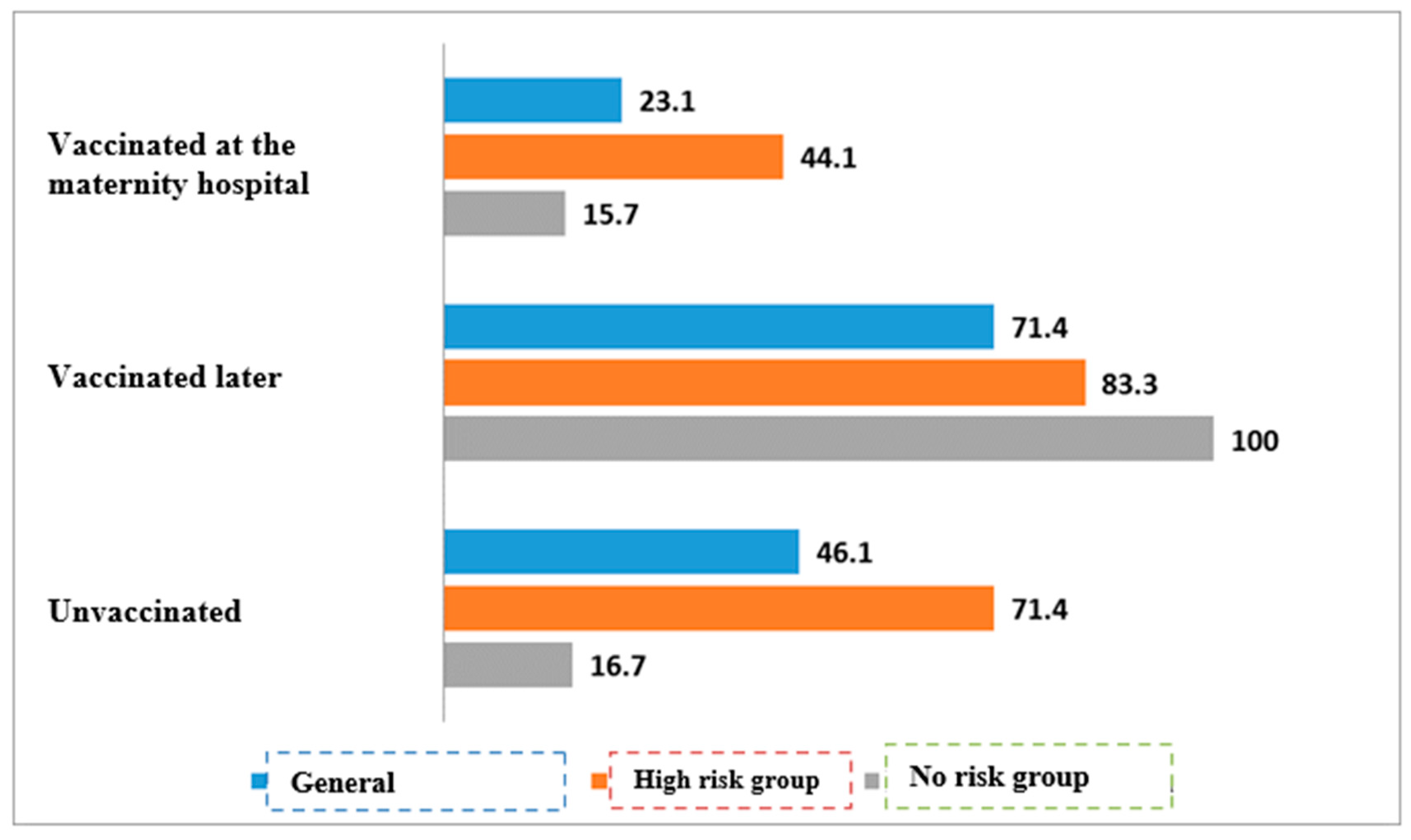
Figure 7.
Prevalence of atopic dermatitis by 18 months of age depending on hepatitis B vaccination status and presence of risk factors for allergic diseases, % (n=287) .
Figure 7.
Prevalence of atopic dermatitis by 18 months of age depending on hepatitis B vaccination status and presence of risk factors for allergic diseases, % (n=287) .
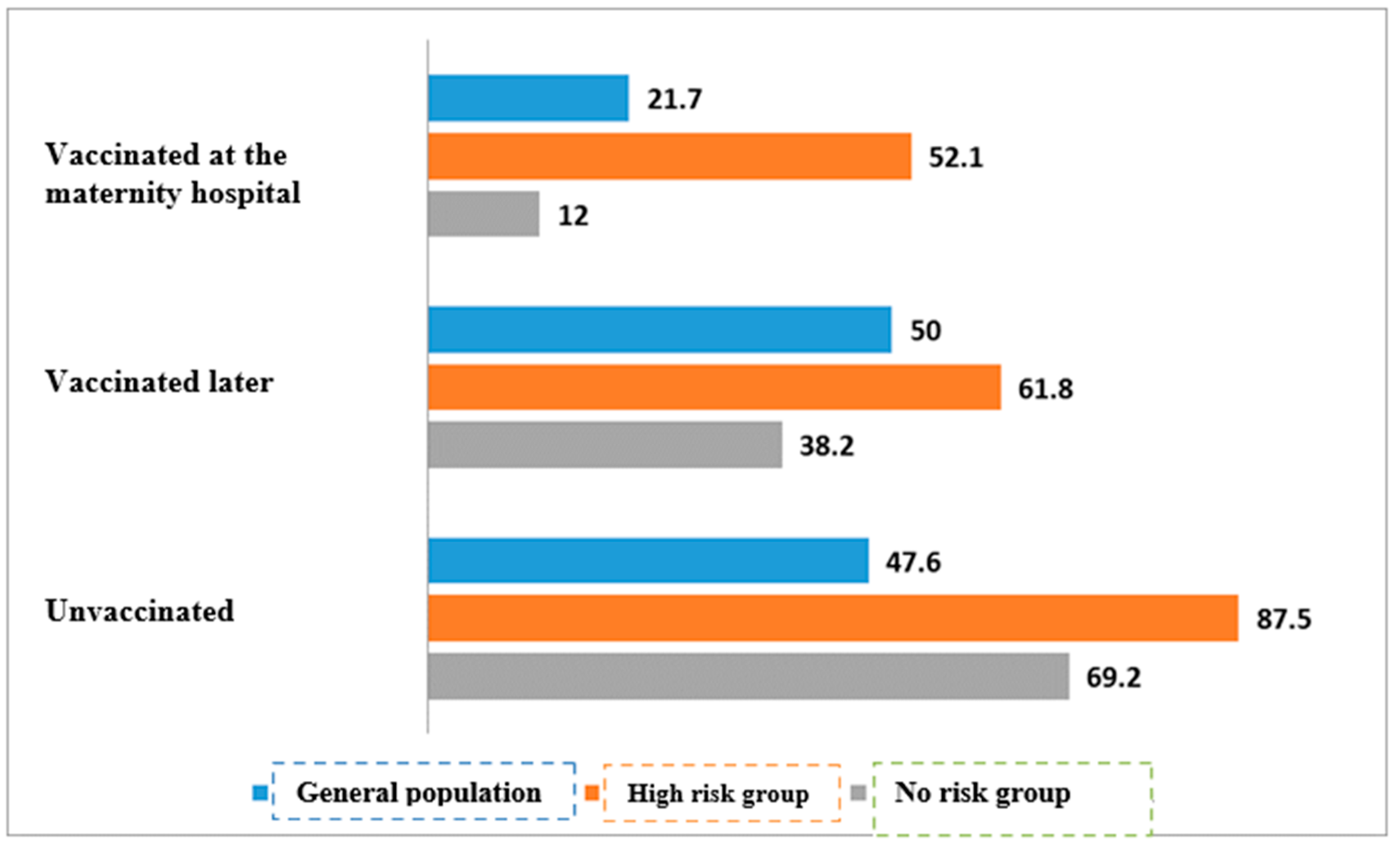
Figure 8.
Prevalence of atopic dermatitis by 18 months depending on timeliness of TB and hepatitis B vaccination and presence of risk factors for allergic diseases, % (n=287).
Figure 8.
Prevalence of atopic dermatitis by 18 months depending on timeliness of TB and hepatitis B vaccination and presence of risk factors for allergic diseases, % (n=287).
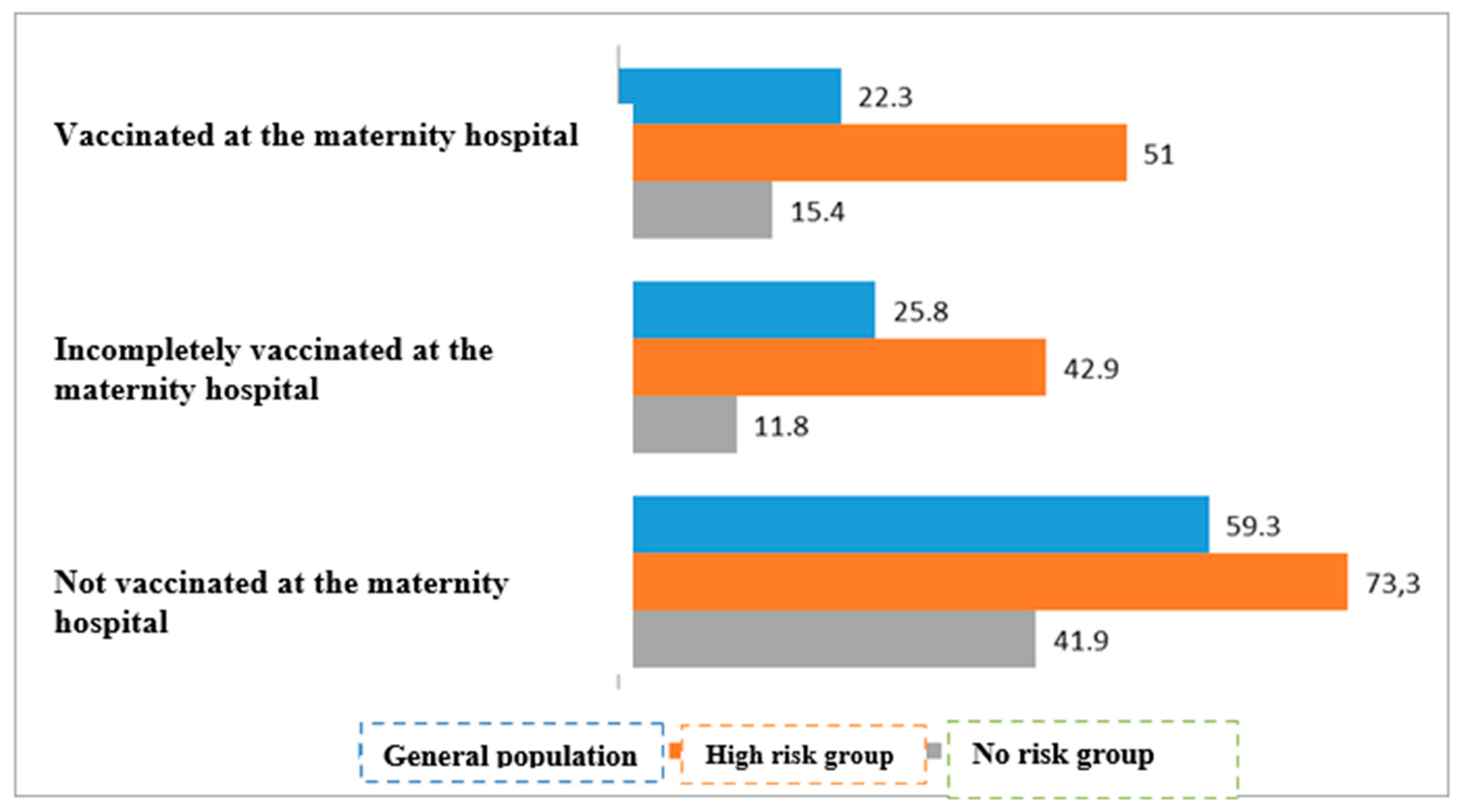

Table 1.
The study participant characteristics.
| Number of subjects (absolute / %) | ||
|---|---|---|
| Boys / Girls | 155/140 | 52.5%/47.5% |
| Having risk factors for development of AD | 93 | 31.5% |
| BCG-М given at the maternity hospital | 231 | 78.3% |
| Hepatitis B vaccine (V1, or 1st dose) given at the maternity hospital | 204 | 69.2% |
| Both vaccines given at the maternity hospital | 203 | 68.8% |
| BCG-М given in the first year of life | 50 | 16.9% |
| Hepatitis B vaccine (V1, or 1st dose) given in the first year of life | 69 | 23.3% |
| BCG-М unvaccinated | 14 | 4.7% |
| Hepatitis B (V1, or 1st dose) unvaccinated | 22 | 7.5% |
| Onset of AD before 12 months of age (and percentage of infants with risk factors) |
73 (34) | 24.7% (46.6%) |
| Onset of AD between 12 and 18 months of age (and percentage of infants with risk factors) | 20 (20) | 6.8% (100%) |
Table 2.
Distribution of study participants depending on vaccination time and type, on presence of risk factors for allergic diseases and onset of AD by 12 months, n=295.
Table 2.
Distribution of study participants depending on vaccination time and type, on presence of risk factors for allergic diseases and onset of AD by 12 months, n=295.
| 2А. TB vaccination | ||||||
| TB vaccination status, all infants | Аtopic dermatitis | P-value | ||||
| With AD (n/%) | Without AD (n/%) | |||||
| Vaccinated at the maternity hospital | 35/231 | 15.2% | 196/231 | 84.8% | <0.01 | |
| Vaccinated later | 33/50 | 66% | 17/50 | 34% | ||
| Unvaccinated | 5/14 | 35.7% | 9/14 | 64.3% | ||
| TB vaccination status, infants with risk for allergic diseases | Atopic dermatitis | P-value | ||||
| With AD (n/%) | Without AD (n/%) | |||||
| Vaccinated at the maternity hospital | 11/61 | 18% | 50/61 | 82% | <0.01 | |
| Vaccinated later | 18/24 | 75% | 6/24 | 25% | ||
| Unvaccinated | 5/8 | 62.5% | 3/8 | 37.5% | ||
| TB vaccination status, infants with no risk for allergic diseases | Atopic dermatitis | P-value | ||||
| With AD (n/%) | Without AD (n/%) | |||||
| Vaccinated at the maternity hospital | 24/170 | 14.1% | 146/170 | 85.9% | * | |
| Vaccinated later | 15/26 | 57.7% | 11/26 | 42.3% | ||
| Unvaccinated | 0/6 | 0% | 6/6 | 100% | ||
| 2В. Hepatitis B vaccination | ||||||
| Hepatitis B vaccination status, all infants | Atopic dermatitis | P-value | ||||
| With AD (n/%) | Without AD (n/%) | |||||
| Vaccinated at the maternity hospital | 36/204 | 17.6% | 168/204 | 82.4% | 0.043 | |
| Vaccinated later | 31/69 | 44.9% | 38/69 | 55.1% | ||
| Unvaccinated | 7/22 | 31.8% | 15/22 | 68.2% | ||
| Hepatitis B vaccination status, infants with risk of allergic diseases | Atopic dermatitis | P-value | ||||
| With AD (n/%) | Without AD (n/%) | |||||
| Vaccinated at the maternity hospital | 12/50 | 24.0% | 38/50 | 76.0% | <0.01 | |
| Vaccinated later | 17/34 | 50.0% | 17/34 | 50.0% | ||
| Unvaccinated | 4/9 | 44.4% | 5/9 | 55.6% | ||
| Hepatitis B vaccination status, infants with no risk for allergic diseases | Atopic dermatitis | P-value | ||||
| With AD (n/%) | Without AD (n/%) | |||||
| Vaccinated at the maternity hospital | 24/154 | 15.6% | 130/154 | 84.4% | * | |
| Vaccinated later | 14/35 | 400% | 21/35 | 60.0% | ||
| Unvaccinated | 3/13 | 23.1% | 10/13 | 76.9% | ||
| 2С. TB and hepatitis B vaccination | ||||||
| TB and hepatitis B vaccination status, all infants | Atopic dermatitis | P-value | ||||
| With AD (n/%) | Without AD (n/%) | |||||
| Both vaccines given in maternity hospital | 33/203 | 16.3% | 170/203 | 83.7% | <0.01 | |
| At least one vaccine given in maternity hospital | 6/30 | 20.0 % | 24/30 | 80.0% | ||
| No vaccination available in maternity hospital | 35/62 | 56.5% | 27/62 | 43.5% | ||
| Tb and hepatitis B vaccination status, infants with risk for allergic diseases | Atopic dermatitis | P-value | ||||
| With AD (n/%) | Without AD (n/%) | |||||
| Both vaccines given in maternity hospital | 10/48 | 20.8% | 38/48 | 79.2% | <0.01 | |
| At least one vaccine given in maternity hospital | 3/15 | 20.0% | 11/15 | 80.0% | ||
| No vaccination available in maternity hospital | 21/30 | 70.0%% | 9/30 | 30.0% | ||
| TB and hepatitis B vaccination status, infants with no risk for allergic diseases | Atopic dermatitis | P-value | ||||
| With AD (n/%) | Without AD (n/%) | |||||
| Both vaccines given in maternity hospital | 23/155 | 14.8% | 132/155 | 85.2% | <0.01 | |
| At least one vaccine given in maternity hospital | 2/18 | 11.1% | 16/18 | 88.9% | ||
| No vaccination available in maternity hospital | 14/29 | 48.3% | 15/29 | 51.7% | ||
Table 3.
Distribution of study participants depending on time and type of vaccination and on presence or absence of risk factors for development of allergic diseases and onset of AD by 18 months, n=287.
Table 3.
Distribution of study participants depending on time and type of vaccination and on presence or absence of risk factors for development of allergic diseases and onset of AD by 18 months, n=287.
| 3А. Tuberculosis vaccination | ||||||
|
TB vaccination status, all infants |
Atopic dermatitis | P-value | ||||
| With AD (n/%) | Without AD (n/%) | |||||
| Vaccinated at the maternity hospital | 52/225 | 23.1% | 173/225 | 76.9% | <0.01 | |
| Vaccinated later | 35/49 | 71.4% | 14/49 | 28.6% | ||
| Unvaccinated | 6/13 | 46.2% | 7/13 | 53.8% | ||
| TB vaccination status, infants with risk of allergic diseases | Atopic dermatitis | P-value | ||||
| With AD (n/%) | Without AD (n/%) | |||||
| Vaccinated at the maternity hospital | 26/59 | 44.1% | 33/59 | 55.9% | <0.01 | |
| Vaccinated later | 20/24 | 83.3% | 4/24 | 16.7% | ||
| Unvaccinated | 5/7 | 71.4% | 2/7 | 28.6% | ||
| TB vaccination status, infants with no risk of allergic diseases | Atopic dermatitis | P-value | ||||
| With AD (n/%) | Without AD (n/%) | |||||
| Vaccinated at the maternity hospital | 26/166 | 15.7% | 140/166 | 84.3% | * | |
| Vaccinated later | 15/15 | 100,0% | 0/15 | 0% | ||
| Unvaccinated | 1/6 | 16.7% | 5/6 | 83.3% | ||
| 3В. Hepatitis B vaccination | ||||||
| Hepatitis B vaccination status, all infants | Atopic dermatitis | P-value | ||||
| With AD (n/%) | Without AD (n/%) | |||||
| Vaccinated at the maternity hospital | 43/198 | 21.7% | 155/198 | 78.3% | <0.01 | |
| Vaccinated later | 34/68 | 50.0% | 34/68 | 50.0% | ||
| Unvaccinated | 10/21 | 47.6% | 11/21 | 52.4% | ||
| Hepatitis B vaccination status, infants with risk of allergic diseases | Atopic dermatitis | P-value | ||||
| With AD (n/%) | Without AD (n/%) | |||||
| Vaccinated at the maternity hospital | 25/48 | 52.1% | 23/48 | 47.9% | * | |
| Vaccinated later | 21/34 | 61.8% | 13/34 | 38.2% | ||
| Unvaccinated | 7/8 | 87.5% | 1/8 | 12.5% | ||
| Hepatitis B vaccination status, infants with no risk of allergic diseases | Atopic dermatitis | P-value | ||||
| With AD (n/%) | Without AD (n/%) | |||||
| Vaccinated at the maternity hospital | 18/150 | 12.0% | 132/150 | 88.0% | <0.01 | |
| Vaccinated later | 13/34 | 38.2% | 21/34 | 61.8% | ||
| Unvaccinated | 9/13 | 69.2% | 4/13 | 30.8% | ||
| 3С. TB and hepatitis B vaccination | ||||||
| TB and hepatitis B vaccination status, all infants | Atopic dermatitis | P-value | ||||
| With AD (n/%) | Without AD (n/%) | |||||
| Both vaccines given in maternity hospital | 44/197 | 22.3% | 153/197 | 77.7% | <0.01 | |
| At least one vaccine given in maternity hospital | 8/31 | 25.8% | 23/31 | 74.2% | ||
| No vaccination available in maternity hospital | 35/59 | 59.3% | 24/59 | 40.7% | ||
| TB and hepatitis B vaccination status, infants with risk of allergic diseases | Atopic dermatitis | P-value | ||||
| With AD (n/%) | Without AD (n/%) | |||||
| Both vaccines given in maternity hospital | 25/49 | 51.0% | 24/49 | 49.0% | <0.01 | |
| At least one vaccine given in maternity hospital | 6/14 | 42.9% | 8/14 | 57.1% | ||
| No vaccination available in maternity hospital | 22/30 | 73.3% | 8/30 | 26.7% | ||
| TB and hepatitis B vaccination status, infants with no risk of allergic diseases | Atopic dermatitis | P-value | ||||
| With AD (n/%) | Without AD (n/%) | |||||
| Both vaccines given in maternity hospital | 23/149 | 15.4% | 126/149 | 84.6% | <0.01 | |
| At least one vaccine given in maternity hospital | 2/17 | 11.8% | 15/17 | 88.2% | ||
| No vaccination available in maternity hospital | 13/31 | 41.9% | 18/31 | 58/1% | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



