Submitted:
30 May 2023
Posted:
01 June 2023
You are already at the latest version
Abstract
Background: Cancer patients require cross-professional care during the diagnosis and treatment periods. Therefore, methods for effectively carrying out case management are essential to tumor care.
Purpose: To investigate the effects of using the community software LINE Official Ac-count on oral cancer case management.
Methods: An experimental design was used; 100 patients were randomly divided into two groups by using a computer-generated random number table. The experimental group used LINE Official Account, which gave them self-care information, timely messages, and one-on-one health-care consultations. The control group followed standard healthcare practices.
Results: The experimental group was satisfied with the self-care information provided by LINE Official Account (86.9%), patients regularly checked the self-care information (89.4%) and would check the information when receiving a push notification (54.3%). Ten patients used the one-on-one consultation(20.0%). LINE Official Account had a significant effect on the rate of participation in support groups. Generalized estimating equations indicated a significant difference between the two groups regarding the overall quality of life over 7 days (P = 0.023).
Conclusion: Community software applications used in oncological case management can improve self-management and empower, also enable tracking of long-term follow-up effectiveness and reinforce the case manager’s role as a family therapist. Therefore, this study recommends that case manager systems be incorporated into mobile applications to increase the sustainable management, accessibility, effectiveness, and satisfaction of oncological management systems. This study also provides the value of Sustainable Development Goals (SDGs) with Good Health and Well-being, and decreased social withdrawal among patients with oral cancer.
Keywords:
patients with oral cancer
; LINE official account
; oncological case management
; interdisciplinary team
; SDG “Good Health and Well-being”
1. Introduction
Oral cancer is not only one of the most common head and neck tumors in Taiwan but also the key preventive and control project of the Taiwanese National Health Department. Oral cancer is currently treated using multidisciplinary integrated treatment in which tumor-reductive surgery, radiotherapy, systematical chemotherapy, and other health-care disciplines are employed to achieve the strongest curative effect and increase the quality of life of patients (1). Ian et al. (2) noted that the face is the region of the body in which any physical anomalies are most apparent. Unlike patients with other types of tumor, patients with oral cancer experience changes to their physical appearance that are caused by tumor wounds during the terminal stage. Such physical changes can lead to body image disturbance, social withdrawal, lower self-confidence, and pain.
Patients can seek care and consultation from hospitals but may struggle locating care after they are discharged, particularly for patients with oral cancer who have developed a lisp. When communicating, the patient may express a sense of frustration that may subsequently affect care workers (3, 4). Lian et al. (5) noted that patients with oral cancer cannot always obtain follow-up care; however, a medical team comprising facial and oral surgeons, prosthodontic physicians, language experts, psychological therapists, and social workers could provide appropriate medical resources for these patients and develop a plan for rehabilitation and care.
Multidisciplinary collaboration can resolve the issue of previously fragmented medical care and effectively integrate medical resources in patient care (6-8). During this process, the case manager acts similar to a home care nurse and serves as the main point of contact between the patient and the medical system. Furthermore, the case manager can help patients and their family members gather proper medical resources and acquire disease-related knowledge and accessible consultations. Case managers also promote communication and cooperation among medical teams, assist patients and their family members in understanding treatments, monitor the treatment plan of patients, closely follow plans to avoid delays in treatment, increase patients’ ability to make treatment-related decisions, and promote self-care (8, 9). Therefore, effective case management is essential in tumor care; however, related research on oral cancer has focused on care provided after operations and during hospitalization. Thus, this study evaluated the community resources and long-term care demands of patients with oral cancer from multiple perspectives. Additionally, the study evaluated the demand and long-term care resources of the community and established appropriate case management care and its integration into the long-term care system. We anticipate that patients will independently look for information, ask for help, and stay in contact with their respective case manager. Patients may be empowered with a sense of independence, security, and trust that assists them with tumor-related treatment, accommodation, rehabilitation, and symptom control.
The case management work that must be done after a patient has been discharged is generally conducted through phone tracking or when the patient visits a physician. Although the literature indicates that case managers often provide a 24-hour service and do not turn their phone off, such practices are illegal and inhumane for case managers according to the Labor Standards Act (10). Patients facing an emergency must be immediately transported to a hospital for treatment. However, some nonemergency factors, such as nutritional supplements, swallowing, and language training, still affect the quality of life and mental health of patients and can affect health issues. If a consultation with a case manager is available for patients, these patients may have greater access to care and be more trusting, and the case manager can learn more about the problems the patients encounter after they are discharged. Particularly for patients with oral cancer who may find it difficult to bring a matter up verbally, providing a convenient and in-person consultation is necessary.
Diagnosing the stage of a case of cancer has been recognized as a pivotal prognostic event for patients with cancer. For patients with oral cancer, pretreatment intervals during the time to treatment can strongly affect survival. However, two-thirds of patients with oral cancer receive their diagnosis when the disease is in stage III or IV, for which the 5-year survival rate is 50% or lower; therefore, improving the quality of life and mortality rate for patients with cancer is essential (11). Teng et al. (12) noted that community software maintains quality of life after care is provided to patients with oral cancer.
2. Purpose
The present study explored the effects of the community software LINE Official Account on the quality of life, symptoms, and active participation in treatment of patients after their discharge from hospital. LINE Official Account provides oral-cancer-related care information, timely notifications, consultation activities, health lectures, and one-on-one consultations without time and space constraints.
3. Materials and Methods
3.1. Experimental Design
3.1.1. We evaluated the health-care, long-term care, and community resources required by patients with oral cancer. We held a focus group with medical center, medical care, social welfare, and long-term care experts (including nurses, case managers, nutritionists, medical social workers, consulting psychologists, therapists, and volunteers) who are engaged in oral cancer care in Taichung City.
The following questions were asked during the focus group:
- (1)
- What care problems do patients with oral cancer encounter after they are discharged?
- (2)
- What questions do patients with oral cancer and their family members have?
- (3)
- In your opinion, what health-care information or community resources should we provide for patients with oral cancer?
- (4)
- In your opinion, how can tumor care be integrated into a long-term care system and be made more convenient and consistent?
3.1.2. We then explored the effects of using LINE Official Account on the quality and quantity of care information, health consultation, and patients’ participation rate.
- (1)
- Patients: The inclusion criteria were as follows: (a) having a diagnosis of oral cancer for longer than 6 months regardless of hospitalization or being an outpatient who met the criteria of the International Classification of Diseases, Clinical Modification, Ninth Edition (ICD-9-CM) disease classification codes 140.0–149.9, (b) older than 20 years, and (c) having a primary caregiver with access to a smartphone.
- (2)
- Research Design: An experimental design was adopted. The patients provided basic data (demographics, disease attributes, and therapeutic history) and data on symptom distress, quality of life, and health-care needs by completing a questionnaire; this was done after case collection and before grouping. The patients were randomly divided into two groups by using a computer-generated simple random number table. A total of 55 patients were in the experimental group, and 45 patients were in the control group. In the experimental group, LINE Official Account was used by the patients to receive self-care information, timely notifications, and one-on-one health-care consultations. By contrast, the control group followed standard health-care practices. In the second and third measurements (Months 3 and 5 after case collection, respectively), the patients answered the same questionnaire as they completed in the first measurement.
- (3)
-
Pretest and Posttest Instruments: The scales used to gather data from the patients were as follows:
- ➢
- Symptom Distress Scale (SDS): The SDS covers 22 symptom distresses that are common in patients with cancer; a Likert scale ranging from 1 to 5 is used for scoring. The lowest score is 22, and the highest is 110; the higher the score, the more severe the symptom distress. The internal reliability (Cronbach's α value) of the SDS is 0.87, and its content validity index (CVI) is 0.92, thus indicating favorable reliability and validity.
- ➢
- Health-care demand scale: To evaluate the health-care needs of patients with cancer, a questionnaire was developed that contains 20 items (13), including items on health-related needs at the physiological, psychological, and social levels. The questionnaire was based on clinical experience and the patient need assessment tool. A Likert scale from 1 to 5 was used for scoring. The reliability of this scale (Cronbach's α) was 0.82, whereas the CVI was 0.85–0.95 after expert evaluation.
- ➢
- European Organization for Research and Treatment of Cancer Quality of Life Questionnaire C30: The Chinese version of this scale has been issued to and is suitable for all patients with cancer. The scale contains 30 items in 15 dimensions: five functional dimensions (body, role, cognitive, emotional, and societal functions), three symptom dimensions (fatigue, pain, and vomiting), one question regarding general health and quality of life, and six single items (each symptom is used as a dimension). Regarding scoring, items 29 and 30 were scored 1–7 (seven levels), whereas the other items were scored in four levels; the higher the score for the five functional dimensions, the higher the quality of life. However, the higher the score for the symptom dimensions, the poorer the quality of life. The score for each dimension and total score were calculated using the formula proposed by Hinz et al. (2012). After the calculations, the score was 0–100, and the total quality of life score of the Quality of Life Questionnaire C30 was calculated as follows: first, the scores for the nine symptoms (fatigue, nausea, vomiting, pain, dyspnea, insomnia, anorexia, constipation, diarrhea, and economic hardship) were calculated until the score was valid; then, the average value of the total scores was determined from the 15 dimensions; the higher the total quality of life score, the higher the quality of life.
- (4)
- LINE Official Account Content
A mobile application is a third-party smartphone application program that is similar to computer software. In addition to being a messaging app, LINE features an app called LINE Official Account (i.e., the LINE app for official business accounts); this app is geared toward enterprise users and primarily used for sales and marketing. Conversely, LINE is used between friends as a messaging and social media app. However, LINE Official Account Life Circle is an open community suitable for small-business marketing; its interface is similar to that of LINE group chats and is easy to learn. LINE Official Account has two key functions: (1) sending messages to multiple people at once, and (2) one-on-one chatting. LINE Official Account has a high degree of privacy, and the option of 1-on-1 messaging provides a personal line of communication that does not interfere with other people on the app (14, 15).
3.2. The expert opinions of the focus group and the common distresses and needs of patients after they are discharged are shown in Table 1.
3.3. The long-term care resources required by patients with oral cancer after they are discharged include the following: language and swallowing training; subsidy and disability certificate applications; nutrition supplements, cooking, and healthy food; control of fatigue, pain, and insomnia; oral cleaning and tumor wound care; patient support groups; and psychological consultations. Home care nurses cannot monitor patients every day, and clinics and support centers cannot always accept patients or may be incapable of providing nursing. Care for patients with oral cancer is currently in dire need of long-term investment in resources, particularly for tumor wound care at the end of oral cancer.
3.4. We constructed an oral cancer health-care information app (Table 2). The app notified the patients in the experimental group and provided one-on-one chatting.

Table 2.
Numbers and content of the oral cancer health-care information app.
| No. | Sub. No | Contents |
|---|---|---|
| 0 | Welcome to the general catalogue of [Taichung Veterans General Hospital Dental Patients Association] | |
| 1 | Watch [Our Good Friends]—integrate cancer resources | |
| 2 | Watch [Oral Cancer and Face Injury]—Sunshine Social Welfare Foundation | |
| 2.1 | Sunshine Social Welfare Foundation service origin | |
| 2.2 | Understanding oral cancer | |
| 2.3 | Treatment of oral cancer | |
| 2.4 | Care and rehabilitation of oral cancer | |
| 2.5 | Prognosis and tracking of oral cancer | |
| 2.6 | Psychological adjustment and support for oral cancer | |
| 2.7 | Social resources network for oral cancer | |
| 2.8 | Common Q&As | |
| 3 | Watch [Difficulty speaking and swallowing?] | |
| 3.1 | Japazi–Swallowing Healthy Exercise—national language | |
| 3.2 | Japazi–Swallowing Healthy Exercise—Taiwanese | |
| 4 | Watch [Dining is Most Important]−nutrition, please click on the following figure | |
| 4.1 | Nutritional recipe model (including liquid diet) | |
| 4.2 | Sunshine Social Welfare Foundation Gourmet recipes (participation) | |
| 4.3 | Sunshine Social Welfare Foundation Gourmet recipes (appraisal) | |
| 4.4 | Your recipe nutritional recipes | |
| 4.5 | Nutrient formula instruction | |
| 4.6 | Diet myths Q&A | |
| 5 | Watch [What to do if you can’t work after falling ill?] | |
| 6 | Watch [Video show], please click on the following figure and select | |
| 6.1 | Sunshine Social Welfare Foundation Knight Dream—true journey | |
| 6.2 | 300 km Prayer Road—full edition | |
| 6.3 | Areca catechu under the sun | |
| 6.4 | Disease information | |
| 6.5 | Taichung Veterans General Hospital Hospice Care Advocacy Film | |
| 6.6 | Sunshine Social Welfare Foundation Film: Red Alert | |
| 6.7 | Lost smile | |
| 7 | If you need to contact us, click on the following figure and select | |
| 7.1 | Taichung Veterans General Hospital Dental Patients Advisory Network | |
| 7.2 | Contact a case management nurse | |
| 7.3 | Night and holidays emergency consultation line | |
| 8 | Watch [Oral patients association course & sharing], … | |
| 8.1 | Comfortable nursing—oral care | |
| 8.2 | Psychological adjustment for oral cancer | |
| 8.3 | Feed you—nutrition | |
| 8.4 | Patient sharing—Mr. Fu | |
| 8.5 | Patient sharing—Mr. Pan |
3.5. Ethical Considerations: Ethical approval was obtained from the ethics committee of Taichung Veterans Hospital in Taichung, Taiwan (CF16030A). The patients provided informed consent before data were collected. The same LINE Official Account program was administered to the patients in the control group 5 months after the completion of data collection
3.6. Data analysis: Microsoft Excel was used to enter and manipulate data. SPSS 18.0 was employed to conduct differential analysis on the data, and the GEE was used to conduct repeated-measurement analysis.
4. Results
4.1. Basic Data of Patients
In total, 100 patients with oral cancer were recruited. Overall, the most common disease history duration was greater than 6 months but less than 1 year (41%). The vast majority of the patients were men (91%). Most were older than 50 years (72%), married (85%), and middle class (61%); had a junior or senior high school education (69%); were Buddhist (85%); had quit smoking, chewing betel nuts, and drinking alcohol (60%–76%); had received surgery, chemotherapy, or radiation therapy once (69%–87%); were not at that time undergoing surgery, chemotherapy, or radiation therapy (87%–95%); and used a smartphone to receive information and notifications (78%). The percentages of patients with each stage of cancer were all approximately 20%–30%.
No significant intergroup differences were found between these data. Before they could complete the questionnaire for the second time, two patients each in the experimental group and the control group died. Before they could complete the questionnaire for a third time, two patients in the control group died (Figure 1).
4.2. Questions, Treatment Suggestions, and Tracking Results of the One-on-One LINE Official Account Consultation System
Ten patients in the experimental group asked questions on the app; there were 13 questions in total from April 22 to September 10, 2016, mainly about swallowing problems, nutrition, chemotherapy announcements, psychological support, and registration.
4.3. Effects of Timely Notifications from LINE Official Account on Support Group Participation
According to the statistics of the patients’ association for July 17, 2016, patients with oral cancer under case collection within the support group included 11 people, 10 of which were in the experimental group and one in the control group. The 10 patients in the experimental group all reported that they received notifications over LINE Official Account, and the patient in the control group received information from their case manager when returning to the hospital for a consultation. According to the statistics, the timely notifications from LINE Official Account effectively informed the patients that they could and should participate in support groups (P = 0.021; Table 3).
4.4. Changes in Symptom Distress, Quality of Life, and Health-Care Needs
According to the posttest results, both symptom distress and health-care needs decreased but quality of life improved in the control group; however, in the experimental group, health-care needs decreased but symptom distress and quality of life increased. The differences were not found to be significant (P > 0.05). Regarding the second test, the GEE analysis indicated a significant difference between the two groups regarding overall quality of life over 7 days (P = 0.023). By conducting in-depth analysis of the posttest, we discovered that both the general health score and quality of life score over 7 days in the control group were poorer than those in the pretest. However, no significant difference was found between the pretest and posttest in the experimental group.
4.5. Satisfaction with Disease Care Information Provided Over LINE Official Account
In the experimental group, 40 patients (86.9) were satisfied with the current provision of disease care information. Forty-two patients (89.4%) received messages from our Oral Cancer Patients Support Group LINE Official Account. Another 25 patients (54.3%) consumed most of the provided information with a viewing rate of 100%. Ten patients (23.3%) read a LINE Official Account message every day, and only seven patients (14.9%) considered the information provided by our Oral Cancer Patients Support Group LINE Official Account to meet their needs. Those very satisfied with messages provided by the Taichung Veterans General Hospital Dental Patients Association LINE Official Account totaled 45 (95.8%); 32 patients (68.1%) were satisfied with the consultation mode when encountering problems at home; 15 patients (31.9%) had once encountered a problem but did not know whom to ask; 9 patients (19.1%) had once asked a question through our Oral Cancer Patients Support Group LINE Official Account; and 45 patients (95.8%) thought our Oral Cancer Patients Support Group LINE Official Account was helpful (Table 5). Thus, providing patients with an information system for receiving timely notifications is helpful and can significantly improve the response rate of patients, and decrease their social withdrawal of patients.
4. Discussion
According to our results, the care information and health consultation for patients with oral cancer provided over LINE Official Account did not significantly affect the quality of life, symptom distress, or health-related needs of our participants (P > 0.05). However, the two groups’ overall quality of life over 7 days did significantly differ (P = 0.023). In the control group, the results in the posttest were poorer than those in the pretest (P = 0.005), but the results in the experimental group indicated no significant difference between the posttest and pretest. Thus, LINE Official Account may help patients maintain their quality of life.
In the experimental group, 40 patients were satisfied with the self-care information provided over LINE Official Account (86.9%), 42 patients regularly checked the self-care information (89.4%), and 25 patients checked push notifications (54.3%). Ten patients (20%) in the experimental group asked 13 questions in total through the one-on-one consultation system; these questions mainly concerned oral infection, language and swallowing problems, nutrition, chemotherapy, psychological support, and registration problems. Timely notifications from LINE Official Account significantly affected participation in support group activities (P = 0.021).
The Deloitte Centre for Health Solutions (2014) reported that health and social care have transitioned to digital technology and that 75% of the British public voluntarily seeks health-care information online. For community health-care providers, the introduction of a mobile app similar to LINE Official Account was found to reduce paperwork by 60%, increase communication and contact time with patients by 29%, decrease hospital admissions by 35%, reduce drug use by 53%, and reduce the length of hospital stays by 59%. In the present study, LINE Official Account provided oral cancer-related care information; informed patients of support activities, nutrition lectures, and other messages; and offered one-on-one consultations without time constraints. Patients, their family members, and case managers often consider LINE Official Account to be convenient and worth applying to case management. Overall, the benefits achieved by this research plan are in line with the SDGs with Good Health and Well-being, and decreased social withdrawal among patients with oral cancer.
5. Conclusions
Cancer is a chronic disease, and patients require cross-team professional care during the early diagnosis and treatment period and often also during the rehabilitation and tracking periods. We make the following suggestions regarding patient care after discharge:
- An “Oncology Management Five-Part Care Mode Concept Map” (Figure 2) should be constructed that consists of the patient, family, team, community, and course, with patients at the center and case managers as their counterparts.
- Oral-cancer-related care information should be provided to promote patient participation in self-care, provide cross-team care, and give patients crucial information after they are discharged.
- A one-on-one consultation system without pressure or time constraints should be offered.
- A self-evaluation system should be constructed in which patients can evaluate their condition and upload data; a nurse will then review the patient data and provide guidance.
- Family members should be allowed to log on, leave messages, learn about patient care, ease the burden on family members, and provide family members with an outlet to express emotions and seek care resources.
- Small-scale, multifunctional, long-term stations should be established and nursing functions at health centers should be expanded to care for oral cancer wounds and patients with terminal illness.
Sample Power version 2.0 should be used by researchers to make calculations regarding sample sizes. Scores 1–7 for quality of life over 7 days can be used to calculate an average value. The average posttest values for the experimental and control groups were 4.1 and 4.9 in this study, respectively, with a standard deviation of 1.4 and a power of 73.5%. If these values are used with a power of 80%, 100 patients are required.
Author Contributions
CHC: Project management. YYC: Study design, statistical analysis, and conclusion. MHH: Literature review, coordinator for submission. HLCW: English draft revision. YSC: Case recruitment, management, and contact.
Funding
The Ministry of Health and Welfare for the study grant (project number: MOHW105-TDU-B-211-134002).
Institutional Review Board Statement
Ethical approval was obtained from the ethics committee of Taichung Veterans Hospital in Taichung, Taiwan (CF16030A)..
Informed Consent Statement
Written informed consent has been obtained from the patient(s) to publish this paper.
Acknowledgments
We would like to thank all the patients who participated in this study and the Ministry of Health and Welfare for the study grant.
Conflicts of Interest
The authors declare no conflict of interests, and the funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- Jameel M, Shahla B, Kedar K, Christine HC. Recent advances and future directions in clinical management of head and neck squamous cell carcinoma. Cancers (2021) 13:338. [CrossRef]
- Ian K, Roeline WP, Bart PMS, Annemieke K, Bregje D, Onwuteaka P. Spiritual care at the end of life in the primary care setting: experiences from spiritual caregivers- a mixed methods study. BMC Palliat Care (2019) 18. [CrossRef]
- Anne-Marie K, Gilmour J, Wissen K. Nurses’ experiences caring for patients surgically treated for oral cavity cancer. nursing Praxis in New Zealand (2018) 34:7-19. [CrossRef]
- Dawson C, Al-Qamachi L, Martin T. Speech and swallowing outcomes following oral cavity reconstruction. Curr Opin Otolaryngol Head Neck Surg (2017) 25:200-204. [CrossRef]
- Lian SY, Chang TT, Wu WW, Wang TJ. Caring for patients with oral cancer in Taiwan: the challenges faced by family caregivers. Eur J Cancer Care (2019) 28:e12891. [CrossRef]
- Chang PH, Chang CH, Chuo YH, Lin CC, Lai HC, Chiang PJ, Cheng CS, Huang PC. Effectiveness of an integrated cancer care program on symptom distress and health care needs of initial operative patients with oral cancer. J VGH Nurs (2017) 34:227-38. [CrossRef]
- Koh J, Walsh P, D'Costa I, Bhatti O. Head and neck squamous cell carcinoma survivorship care. Royal Aust College Gen Pract (2019) 48:846-48. [CrossRef]
- Caitlin G, Breukink SO, Claessens D, Slok AHM, Kimman ML. Patient- reported outcome measures in oncology: a qualitative study of the healthcare professional’s perspective. Support Care Cancer (2021) 29:5253-5361. [CrossRef]
- Joo JY, Liu MF. Effectiveness of Nurse- led Management in cancer care: systematic review. Clin Nurs Res (2019) 28:968-991. [CrossRef]
- Yin YN, Wang Y, Jiang NJ, Long DR. Can case management improve cancer patients quality of life? A systematic review following PRISMA. Medicine (2020) 99:e22448. [CrossRef]
- Constanza SH, Enric JS, Antoni MR, Albert ED, José LL. Time-to-treatment in oral cancer: Causes and implications for survival. Cancers (2021) 13:1321. [CrossRef]
- Teng EF, Chang YY, Chang PH, Chuo YH, Tsai YJ, Hsu CY, Shen CC, Chang CH. Using social software to improve quality of life of patients of oral cancer. J VGH Nurs (2018) 35:223-233. [CrossRef]
- Coyle N, Goldstein ML, Passik S, Fishman B, Portenoy R. Development and validation of a patient needs assessment tool (PNAT) for oncology clinicians. Cancer Nurs (1996) 19:81-92. [CrossRef]
- LINE Official Account Official website. (2016). http://at.line.me/tw/ (Accessed August 15, 2022).
- Xu JY, Qiu LL, Hsu CY, Wu YW, Lin HH, Chen CC, Chen MS. Adoption, Acceptability, and Effectiveness of new communication app (LINE Official Account) for post-discharge patients with cardiovascular diseases: a pilot study in a medical center. J Healthc Manag (2017) 18:292-314. [CrossRef]
Figure 1.
Study process.
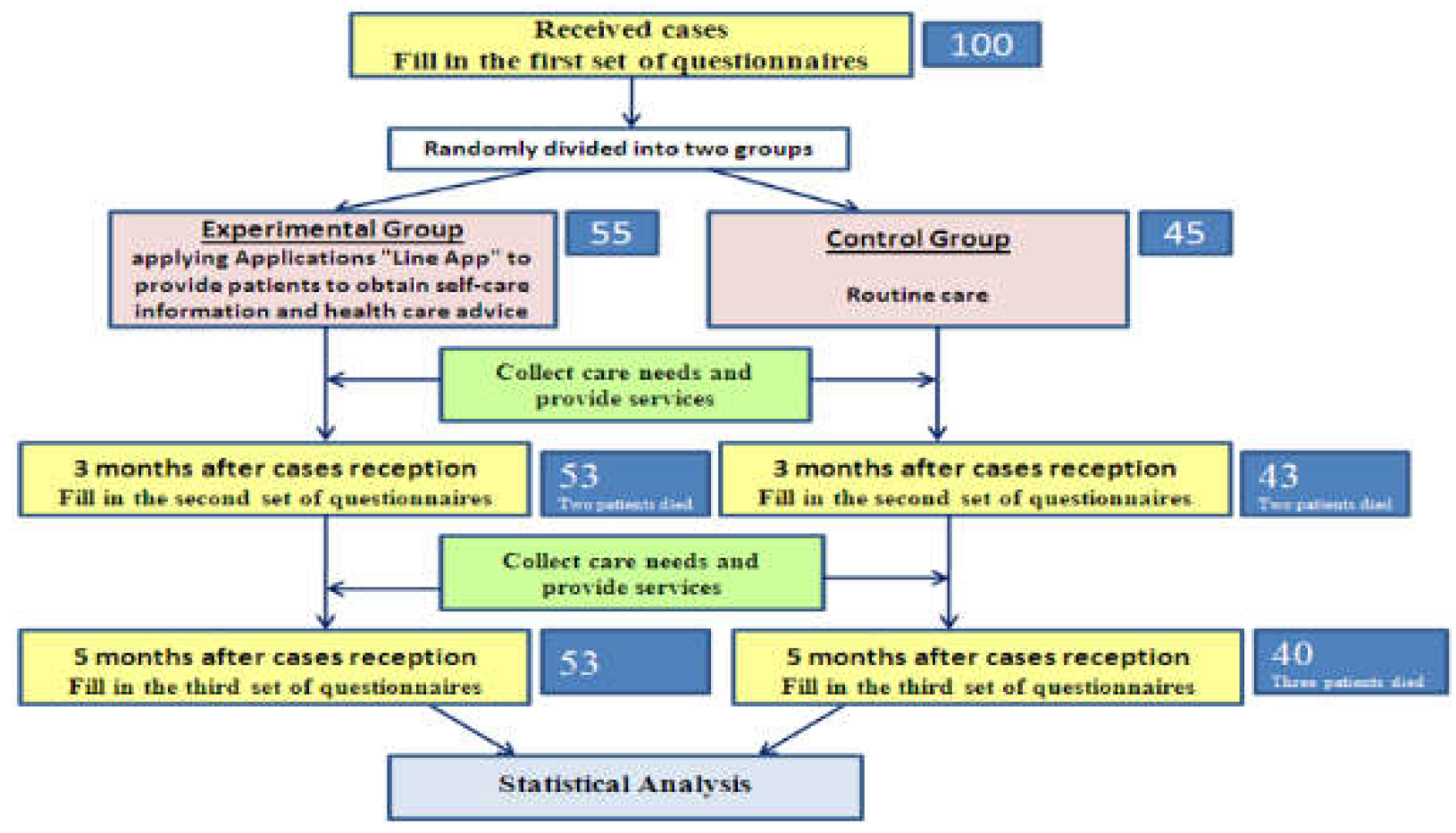
Figure 2.
Oncology case management five-part care mode concept map.
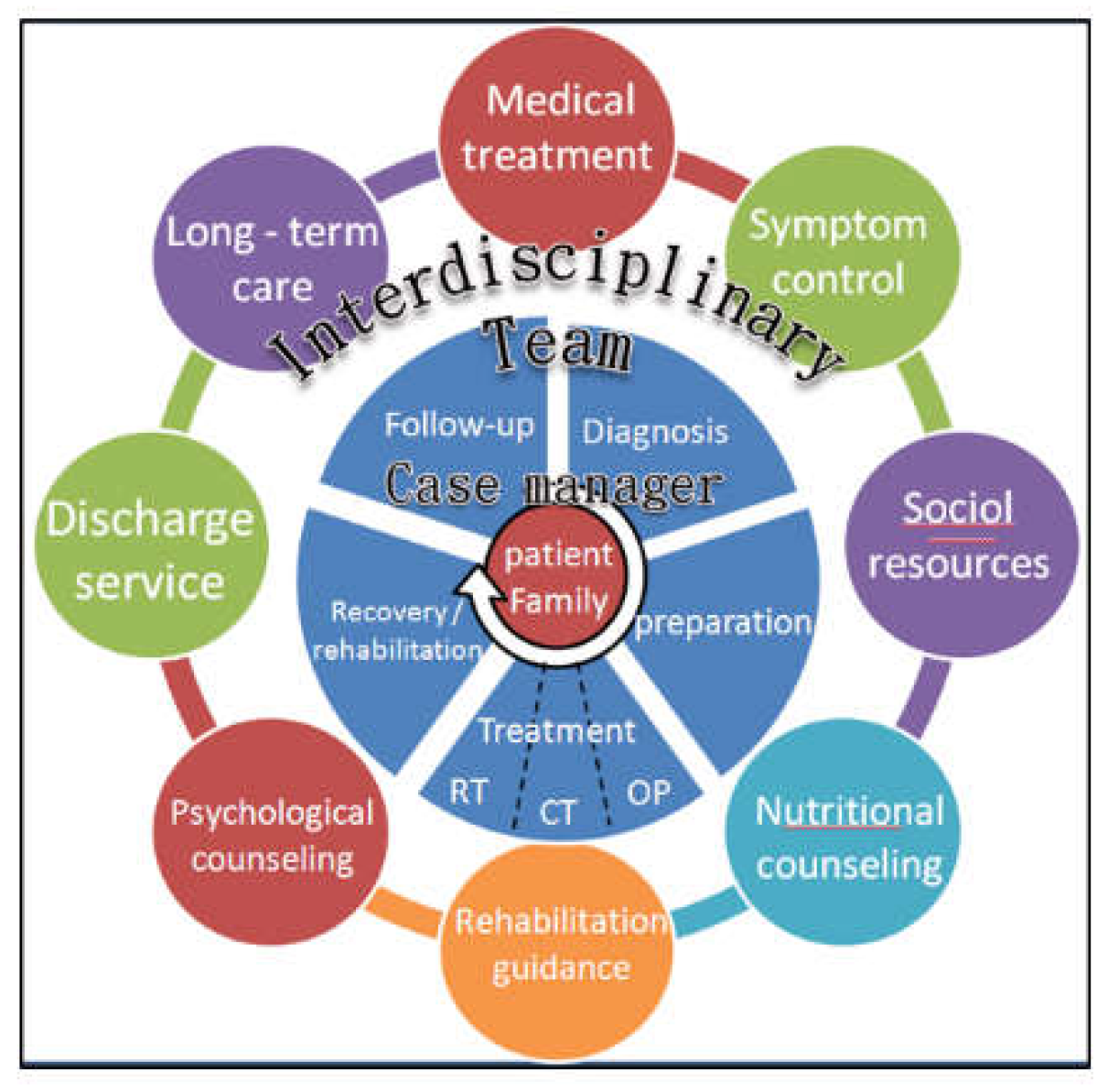
Table 1.
Expert opinions of the focus group and the common distresses and needs of patients with oral cancer after they are discharged from hospital.
Table 1.
Expert opinions of the focus group and the common distresses and needs of patients with oral cancer after they are discharged from hospital.
| Focus group participants | Patient need and distress | Suggestions |
|---|---|---|
| Medical center Oral cancer care team | Patients have difficulty swallowing and speaking | 1. Provide a health education list regarding oral movement and swallowing skills. 2. Provide referral services. 3. Document the experiences of patients with oral cancer. 4. Encourage patients to find and take part in support group activities. |
| The oral mucosa is broken, and food intake is reduced after electrotherapy | 1. Remind patients about the application of glutamine. 2. Referral care nurses should provide health education for oral care. 3. Provide nutrition information. 4. Provide mouthwash information. |
|
| Patients are unaware of whether they meet the criteria to apply for a disability certificate | During a follow-up visit, patients should ask their physician whether they meet the criteria for somatopsychic disturbance. |
|
| Long-term care professionals | Patients require oral care and wound care | 1. Cleaning for patients. 2. Suggest using alcohol-free mouthwash properly. 3. Use propolis mouthwash, which has a bactericidal effect and may thus promote wound healing. |
| Patients require pain control | Understand the situation of patients using acesodyne. | |
| Patients have a nutrition demand | Refer to a dietitian. | |
| Patients have a rehabilitation demand | Refer to the Sunshine Social Welfare Foundation to teach patients about mouth-opening exercises, improving shoulder and neck stiffness, and swallowing training. |
|
| Social welfare professionals | Patients have nutrition intake and financial problems | Provide a nutrition program support plan for patients. |
| Patients require oral cleaning and education on nutrition and health | Provide home care service plan tracking and home rehabilitation. | |
| Patients require mood adjustment | 1. Hold group activities for patients. 2. Invite the volunteer team comprising those who previously had oral cancer to share and visit. 3. Encourage other patients through group interactions. |
Table 3.
Effect of timely LINE Official Account notifications on participation in support group activities (N = 100).
Table 3.
Effect of timely LINE Official Account notifications on participation in support group activities (N = 100).
| Total (N=100) | CP (n=45) |
EG (n=55) |
p value | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| N | % | n | % | n | % | |||||
| Paticipants | 0.021* | |||||||||
| NO | 89 | (89.0%) | 44 | (97.8%) | 45 | (82%) | ||||
| YES | 11 | (11.0%) | 1 | (2.2%) | 10 | (18%) | ||||
Fisher's exact test. *P < 0.05. **P < 0.01. EG: experimental group; CP: control group.
Table 4.
GEE results for quality of life.
| Total | Function | Symptom | Quality of life over 7 days |
|||||||||||||
| Variable | Coefficient (B) | SE | p value | Coefficient (B) | SE | p value | Coefficient (B) | SE | p value | Coefficient (B) | SE | p value | ||||
| Interception | 81.46 | 2.25 | 87.52 | 2.07 | 88.44 | 1.97 | 68.41 | 3.31 | ||||||||
| Group | ||||||||||||||||
| CG | ref. | ref. | ref. | ref. | ||||||||||||
| EG | 0.42 | 2.95 | .887 | 0.97 | 2.73 | .721 | -0.40 | 2.68 | .882 | 0.68 | 4.24 | .873 | ||||
| Test | ||||||||||||||||
| First | ref. | ref. | ref. | ref. | ||||||||||||
| Second | -8.54 | 2.07 | <.001** | -0.73 | 1.49 | .624 | 0.18 | 1.59 | .908 | -25.06 | 4.75 | <.001** | ||||
| Third | 0.87 | 1.73 | .615 | 1.94 | 1.61 | .227 | 1.88 | 1.79 | .296 | -1.20 | 2.78 | .667 | ||||
| GP*Second | 3.77 | 2.92 | .196 | -1.33 | 2.43 | .583 | -1.53 | 2.35 | .513 | 14.19 | 6.24 | .023* | ||||
| GP*Third | -1.06 | 2.46 | .666 | -4.13 | 2.35 | .079 | -1.11 | 2.34 | .637 | 2.05 | 4.08 | .615 | ||||
Generalized estimating equation. *P < 0.05, **P < 0.01. EG: experimental group; CP: control group.
Table 5.
Experimental group’s satisfaction with care information and health consultation over LINE Official Account.
Table 5.
Experimental group’s satisfaction with care information and health consultation over LINE Official Account.
| Questions | N | n | % | |
|---|---|---|---|---|
| 1 | Are you satisfied with the provision of disease care information? Very dissatisfied Dissatisfied Tolerable Satisfied Very satisfied |
46 |
1 0 5 25 15 |
2.2 0.0 10.9 54.3 32.6 |
| 2 | Do you consume the information provided by the LINE Official Account of Taichung Veterans General Hospital Dental Patients Association? Yes No |
47 |
42 5 |
89.4 10.6 |
| 3 | At what frequency do you consume information from the LINE Official Account of Taichung Veterans General Hospital Dental Patients Association? Every day Every week Every month When I receive information When I inquire about problems |
43 |
10 6 2 25 0 |
23.3 14.0 4.7 58.1 0.0 |
| 4 | Does the information provided by the LINE Official Account of Taichung Veterans General Hospital Dental Patients Association meet your needs? Not at all Sometimes Yes |
47 |
1 39 7 |
2.1 83.0 14.9 |
| 5 | Are you satisfied with the information provided by the LINE Official Account of Taichung Veterans General Hospital Dental Patients Association? Very dissatisfied Dissatisfied Satisfied Very satisfied |
47 |
1 1 32 13 |
2.1 2.1 68.1 27.7 |
| 6 | Are you satisfied with the consultation mode when you encounter problems at home? Very dissatisfied Dissatisfied Tolerable Satisfied Very satisfied |
47 |
0 15 29 3 |
0.0 31.9 61.7 6.4 |
| 7 | Are you ever unsure who to ask when you encounter a problem? Yes No |
47 |
15 32 |
31.9 68.1 |
| 8 | Have you ever asked questions using the LINE Official Account of Taichung Veterans General Hospital Dental Patients Advisory Network? Yes No |
47 |
9 38 |
19.1 80.9 |
| 9 | Are you satisfied with answers given through consultations on the LINE Official Account of Taichung Veterans General Hospital Dental Patients Advisory Network? Very dissatisfied Dissatisfied Satisfied Very satisfied |
9 |
0 1 6 2 |
0.0 11.1 66.7 22.2 |
| 10 | What is your opinion of the help given by the LINE Official Account of Taichung Veterans General Hospital Dental Patients Advisory Network? Very unhelpful Unhelpful Helpful Very helpful |
47 |
0 2 37 8 |
0.0 4.3 78.7 17.0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



