Submitted:
21 May 2023
Posted:
22 May 2023
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Long COVID (LC) encompasses a constellation of long-term symptoms experienced by at least 10% of people after the initial SARS-CoV-2 infection, and so far has affected about 65 million people. The etiology of LC remains unclear; however, many pathophysiological pathways may be involved, including viral persistence; chronic, low grade inflammatory response; immune dysregulation and defective immune response; reactivation of latent viruses; autoimmunity; persistent endothelial dysfunction and coagulopathy; gut dysbiosis; hormonal dysregulation, mitochondrial dysfunction; and autonomic nervous system dysfunction. There are no specific tests for the diagnosis of LC, and clinical features including laboratory findings and biomarkers may not specifically relate to LC. Therefore, it is of paramount importance to develop and validate biomarkers that can be employed for the prediction, diagnosis and prognosis of LC and its therapeutic response. Promising candidate biomarkers that are found in some patients are markers of systemic inflammation including acute phase proteins, cytokines and chemokines; biomarkers reflecting SARS-CoV-2 persistence, reactivation of herpesviruses and immune dysregulation; biomarkers of endotheliopathy, coagulation and fibrinolysis; microbiota alterations; diverse proteins and metabolites; hormonal and metabolic biomarkers; as well as cerebrospinal fluid biomarkers. At present, there are only two reviews summarizing relevant biomarkers; however, they do not cover the entire umbrella of current biomarkers or their link to etiopathogenetic mechanisms, and the diagnostic work-up in a comprehensive manner. Herein, we aim to appraise and synopsize the available evidence on the typical laboratory manifestations and candidate biomarkers of LC, their classification based on main LC symptomatology in the frame of the epidemiological and pathogenetic aspects of the syndrome, and furthermore assess limitations and challenges as well as potential implications in candidate therapeutic interventions.
Keywords:
biomarkers
; COVID-19
; epidemiology
; laboratory
; long COVID
; pathogenesis
; post-acute sequelae of SARS-CoV-19 infection (PASC)
; post COVID
; post-COVID syndrome (PCS)
1. Introduction
The World Health Organization (WHO) declared COVID-19 a pandemic about 3 years ago, on March 11, 2020. As of May 17, 2023, an estimated 766,440,796 confirmed cases of COVID-19 have occurred, which have resulted in 6,932,591 deaths [1]. Despite the great direct and indirect loss of life [2], accompanied by considerable societal and financial detrimental consequences of COVID-19 [3], cases of SARS-CoV-2 infection appear to gradually decline in severity at an individual patient level. Accumulated knowledge regarding COVID-19 pathogenesis and clinical experience that has resulted in improved patient care, increasing levels of collective immunity due to convalescence from natural infection or vaccine coverage, and evolving SARS-CoV-2 variant characteristics may have contributed to this phenomenon [4,5]. The predominance of the Omicron variant may be considered a milestone in the course of the pandemic, due to the generally milder features of associated infection in comparison to earlier strains [6]. The currently dominant Omicron XBB.1.5 subvariant appears to also follow this trend [7,8].
With a steadily low mortality rate of SARS-CoV-2 infection, attention is shifted towards survivors who exhibit durable symptoms following apparent clinical recovery [9]. The persistence of clinical manifestations well after successful infection clearance has been described under the umbrella term “long-COVID (LC)”, which covers a wide range of very heterogenous morbid conditions following documented SARS-CoV-2 infection. Even though these disorders are rarely life threatening, they are associated with a considerable detrimental impact on patient’s quality of life [10], which combined with the high prevalence of LC, account for a large percentage of overall health care and societal impact associated with the pandemic. According to modest estimates, LC affects at least 10% of infected individuals, which currently translates into roughly 76 million cases globally [11].
Τhe term “long COVID” is used to describe the presence of clinical manifestations and/or complications persisting or manifesting four weeks after initial SARS-CoV-2 infection. Two fairly distinct conditions may be distinguished: “ongoing symptomatic COVID-19” denotes the presence of symptoms and/or signs persisting over 4 to 12 weeks, while “post-COVID-19 condition” refers to manifestations appearing during or after SARS-CoV-2 infection persisting for over 12 weeks and cannot be attributed to a plausible alternative diagnosis [12,13].
Not surprisingly, this broad definition includes conditions with a great variety of clinical manifestations ranging from constitutional, non-specific physical symptoms to signs of isolated organ dysfunction, including neuropsychiatric disorders [11,14,15]. Likewise, many putative mechanisms have been implicated in the pathogenesis of LC, including viral persistence, endothelial dysfunction, coagulation disorders and microthrombotic manifestations, disruption of gut microbiota, neuroinflammation, autoimmunity and mast cell activation, reactivation of dormant viral pathogens and perturbations of brainstem and autonomic nervous signaling, among others [11,16,17,18]. Accordingly, a wide range of non-specific laboratory findings have also been associated with LC, albeit with few indexes showing promise as candidate biomarkers for identification of possible cases [11,19].
There is an urgent need to pinpoint patient-level risk factors and characteristics in order to successfully identify patients at a high risk of developing LC and to properly diagnose this syndrome. At present, there are only two reviews (one scoping and one systematic) summarizing relevant biomarkers; however, these reviews do not cover the entire current umbrella of biomarkers nor their link to etiopathogenetic mechanisms, as well as the diagnostic work-up in a comprehensive manner [20,21]. Herein, we aim to review the available evidence on the typical laboratory manifestations and candidate biomarkers of LC, their classification based on main LC symptomatology in the frame of the epidemiological and pathogenetic aspects of the syndrome, and furthermore assess potential implications in candidate therapeutic interventions.
2. Epidemiology of Long COVID and risk factors
The exact frequency of LC is challenging to determine, due to the non-specific nature of its clinical manifestations, the absence of consequent screening and the lack of diagnostic markers which likely result in under reporting. Furthermore, several reports are confounded by the absence of a comparator control group free of recent SARS-CoV-2 infection, for a precise estimate of COVID-attributable symptoms to be feasible. According to modest estimates, around 10% of non-hospitalized survivors experience persistent symptoms [11], while percentages are considerably higher among those hospitalized, with more than 70% reporting at least one compatible clinical manifestation [22]. These numbers may not reflect the true healthcare and societal impact of LC by themselves, if the high incidence of SARS-CoV-2 infection on one hand, and the relative long duration (often, several months) of postinfectious manifestations on the other [23], are not taken into account. This likely results in a considerably higher overall true prevalence of LC-associated debilitating symptoms in the general population [24]. Furthermore, although LC is often considered as a spectrum of chiefly benign disorders with a principal impact on quality of life, rather than loss of life, conditions falling into its spectrum contribute to a significant fraction of excess COVID-19-attributable death, mostly indirectly [25].
It is noteworthy that the emergence of new variants and the subsequent evolution of the features of individual infections as well as the pandemic itself as a whole, are accompanied by a shift in the epidemiological features of LC [26]. With respect to the Omicron variant, the subvariants of which are currently dominant on a worldwide scale, persistent symptoms following infection are likely of lower severity and shorter duration compared with the earlier wildtype, alpha, beta and delta variants [24,27], being also of lower overall relative prevalence compared with non-infected controls [28]. A recent pooled analysis of two population-based cohorts has shown that the risk of LC is lower after infection with the Omicron variant and following vaccination [29]. Interestingly, the incidence and severity of the Multisystem Inflammatory Syndrome in Children (MIS-C) decreased during the Omicron wave of the pandemic in comparison to earlier waves [30]. It is currently unclear if this observation is primary a consequence of the altered natural course of infection caused by the omicron variant or simply confounded by the effects of increasing vaccine coverage (see below) or the increasing prevalence of reinfections and breakthrough infections in the Omicron era [31,32,33,34].
Although most epidemiological data have been collected from adult populations, children of all ages and adolescents are considerably more likely to report chronic symptoms in the spectrum of LC after documented SARS-CoV-2 infection compared with non-infected controls of similar age [35,36]. Of note, post-COVID neurodevelopmental sequelae may also be encountered in infants of mothers infected during pregnancy in the first year of life [37]. Furthermore, certain pathogenetic features (e.g., inflammatory, immunological, pertinent to endothelial dysfunction), as well as diverse clinical manifestations of LC may overlap with those of the Multisystem Inflammatory Syndrome in Children (MIS-C), which was originally described in pediatric populations in the early post-infection period [38]. According to the case definition of MIS-C [39], it is certain that a proportion of affected patients also fall into the category of LC, at least in the “ongoing symptomatic COVID-19” category. Semantics aside, this may harbor implications for the better understanding not only of LC, but also of the pathophysiology of MIS-C which remains largely elusive, while also guiding of potential therapeutic interventions for both conditions [38].
Apart from the aforementioned impact of different viral variants, there are a number of patient-level risk factors which have been demonstrated to confer a higher risk for LC. According to a recent meta-analysis of 41 studies, among the population of COVID-19 survivors, older age (Odds Ratio-OR 1.21), female sex (OR 1.56), higher Body Mass Index (BMI, OR 1.15), smoking (OR 1.10), presence of (physical as well as mental) co-morbidities (OR 2.48), hospitalization or admission in the intensive care unit (ICU, OR 2.38) are associated with a higher risk of LC [40]. A longer hospital stay [41], black or Hispanic ethnic background and a low socioeconomic status have also been associated with a higher risk [11,42]. In pediatric populations, age younger than 5 years, female sex, black or Hispanic race and the presence of chronic co-morbidities have been implicated as risk factors [43]. Particularly, children with LC were more likely to suffer from attention deficit hyperactivity disorder, chronic urticaria and allergic rhinitis before SARS-CoV-2 infection [44].
Regarding the impact of prior immunization, and although relevant data from available studies are not unequivocal, the risk for LC after infection following vaccination is likely lower than that of unvaccinated individuals [31]. Analysis in a random sample of adults in the United Kingdom revealed a 41% lower risk of LC following infection among those that had received two vaccine doses (either mRNA-based, adenovirus vector, or combined), compared with those who received no vaccination [45]. Data from the US Department of Veterans Affairs national healthcare database demonstrated a more modest risk reduction of 15% [46]. When focusing on the prevention of specific symptoms, such as brain fog or muscle pain, the observed effects may be of greater magnitude [47]. Interestingly, the effect of vaccination in individuals already diagnosed with LC is variable, with 61.9% reporting no change, 16.7% amelioration and 21.4% worsening in symptoms, suggesting that active immunization following native infection may not be generalizable as a secondary prevention strategy among affected individuals [48]. Regarding reinfections and severity of COVID-19, a recent meta-analysis has found no significant difference in the clinical pattern and severity of infection between primary infection and reinfection [49]. However, available data with respect to LC risk following reinfection in both vaccinated and unvaccinated individuals are scarce, although existing evidence points towards an increased risk for LC after repeated infection [50].
3. Clinical manifestations of long COVID
A wide range of non-specific clinical symptoms and manifestations from virtually every organ and system have been reported as long-term sequelae of SARS-CoV-2 infection. General systemic symptoms (chronic fatigue, arthralgia/myalgia, sleep disorders) are frequently reported. As COVID-19 is primarily a respiratory infection, symptoms related to the respiratory system are common, such as chronic cough, breathlessness, exertional dyspnea, and chest tightness, which occasionally -but not always- reflect a chronic postinfectious respiratory pathology, with abnormal lung function tests and/or radiological changes [51,52,53]. Upper airway-related symptoms (voice changes, hoarseness, rhinorrhea, impaired hearing, loss of smell/taste) are also reported. Disorders related to the cardiovascular system (exercise intolerance, chest pain, palpitations, thrombotic manifestations) are also frequent and potentially pathogenetically related to the dysfunction of the cardiovascular autonomic system (see below). Gastrointestinal manifestations (appetite loss, constipation, nausea, abdominal pain, acid reflux) may parallel perturbations of the gut flora or be related to the prolonged intestinal viral shedding. Most prominently, neuropsychiatric disorders are considered typical features of the LC spectrum, ranging from mental fatigue, inability to concentrate and poor memory (collectively referred to as “brain fog”) to major depression, anxiety and post-traumatic stress disorder. Skin rashes and hair loss are frequently reported [11,54].
The variety and heterogeneity of LC clinical manifestations, as well as their non-specific nature contribute to the challenge of the systematic study of LC as a uniform syndrome. Nonetheless, it is likely that groups or clusters of symptoms exist (namely, central neurological, cardiorespiratory, systemic/inflammatory and abdominal clusters), which are more likely to affect individuals as a group rather than as a constellation of chaotic manifestations independently of each other [55]. Interestingly, specific symptom clusters appear to be associated with LC following infection by different SARS-CoV-2 variants [55]. This observation may have important implications not only for the identification of patient groups likely to benefit from specific therapeutic interventions, but also for deciphering the underlying pathogenetic mechanisms that drive LC development.
The range of subjective symptoms reported in conjunction with LC may or may not be associated with objectively proven underlying organ damage. This is an important consideration, since the latter may constitute a significantly more objective prognosis-determining factor than the self-report of the clinical symptom. Objective and lasting organ involvement is not uncommon in the context of LC, with 69% and 59% of affected patients exhibiting dysfunction of at least one organ 6- and 12-months following SARS-CoV-2 infection, respectively, while the corresponding frequencies for multiorgan involvement are 23% and 27%, respectively [56].
One of the earliest recognized features of LC is the dysfunction of the autonomic nervous system, a condition with unknown pathogenesis, duration and prognosis, manifesting itself with signs of dysregulated system functions, primarily of the cardiovascular autonomic nervous system, most prominently postural orthostatic tachycardia, inappropriate resting sinus tachycardia and exercise intolerance [57,58]. Before the COVID-19 era, the bulk of evidence linking cardiac autonomic neuropathy with worse cardiovascular prognosis and propensity towards life-threatening cardiac arrhythmias was derived from observations in patients with diabetes mellitus (DM) [59]. Likewise, it would be plausible that autonomic dysfunction is a major driver of ongoing cardiovascular symptoms in LC [60], contributing to the increased cardiovascular risk and worse prognosis of affected patients [61].
COVID-19 shares a bidirectional relationship with type 1 and type 2 DM [62]; on one hand, pre-existing DM predisposes to a more severe and complicated infection course [34,63,64,65,66]. On the other hand, a higher risk of newly diagnosed type 1 or type 2 DM has been demonstrated among survivors of SARS-CoV-2 infection [62,67]. It can be assumed that at least in the case of type 2 DM, a proportion of new diagnoses may represent incidental discoveries of undiagnosed pre-existing DM cases emerging through the contact of infected patients with healthcare services. However, the underlying mechanisms driving the association between SARS-CoV-2 infection and the emergence of DM are unclear. In the case of type 1 DM, triggering of an autoimmune process directed against pancreatic beta cells may be assumed [68]; otherwise, there is evidence of a direct adipocyte viral infection and subsequent adipose tissue dysfunction, resulting in insulin resistance (IR) and promotion of overt hyperglycemia and type 2 DM [69].
4. Are clinical manifestations and pathogenesis unique to SARS-CoV-2 infection?
As the spectrum of LC manifestations is becoming increasingly understood among clinicians and researchers, the question arises whether this is a unique feature of SARS-CoV-2 infection itself, or whether it shares resemblance with similar syndromes observed following respiratory -or other- viral illnesses. Undoubtedly, the magnitude and sheer number of cases during the last three years allowed for the better study and characterization of this syndrome in conjunction with COVID-19. Nevertheless, chronic post-viral syndromes have been described in conjunction with earlier coronavirus outbreaks. Chronic fatigue was reported by 60% of SARS survivors 12 months post recovery [70], and as many as 40% of survivors ~41 months following the acute infection [71]. Similar symptoms were reported among 48% and 33% of Middle East Respiratory Syndrome (MERS) survivors 12 and 18 months after the initial illness, respectively, in conjunction with depressive and post-traumatic stress disorder features [72].
Many of those with post-SARS syndrome fulfilled the definition of International Chronic Fatigue Syndrome Study Group for Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS) [71,73,74]. Apart from chronic fatigue, poor cognitive function, shortness of breath, functional gastrointestinal disorders and palpitations are other typical features [75]. Furthermore, features of ME/CFS have been described in conjunction with other epidemic/pandemic (H1N1 influenza virus [76], Ebola virus [77], West-Nile virus [78]) and non-epidemic (most commonly, by Herpesviridae: EBV, CMV, VZV, HHV-6, HHV-7) [79] viral illnesses. Interestingly, the prevalence of ME/CSF globally is approximately 1% (17 to 24 million affected individuals) [80]. It seems plausible that a considerable proportion of individuals affected by LC would fulfill formal criteria for ME/CFS, and furthermore that a certain fraction of LC cases corresponds to a post-viral syndrome not specific to SARS-CoV-2 infection, although further research into the underlying mechanisms of this condition is needed to support this hypothesis.
5. Pathogenesis of Long COVID
The underlying pathogenetic mechanisms in LC are not fully elucidated; however, there are several interacting pathways that may contribute to the symptomatology of LC, as summarized in Figure 1. Overall, the following mechanisms are implicated in the pathobiology of LC:
1) A chronic, low grade inflammatory response is associated in several cases with the severity of ongoing symptoms particularly in patients who were hospitalized [81]. This hyperinflammatory response may be facilitated partly by mast cell activation, attributed to the loss of genetic regulation of mast cells by SARS-CoV-2 [82,83].
2) Immune dysregulation is linked to decreased B cell and T cell numbers, increased innate immunity and persistent SARS-CoV-2 shedding, which further contribute to the chronic inflammatory response and immune activation in LC [84,85].
3) SARS-CoV-2 (spike protein and viral mRNA) may persist in certain patients with LC in cryptic tissue reservoirs following acute COVID-19, triggering repeated and sustained immune responses leading to chronic symptoms [86,87]. The spike protein, which represents one of the main virulence factors of SARS-CoV-2, is a significant viral protein for the attachment of the virus to target cells bearing the angiotensin-converting 2 enzyme (ACE-2) surface receptors. Moreover, the spike protein may be released by the host cell via extracellular vesicles (EVs) and reach distant tissues and organs through the circulation [88].
Viral persistence is observed in certain viruses, such as herpesviruses (Herpes Simplex Virus/HSV, Varicella-Zoster Virus/VZV, Epstein-Barr Virus/EBV, Cytomegalovirus/CMV), Human Immunodeficiency Virus (HIV), hepatitis viruses (HBV and HCV), human papillomavirus (HPV), which may not be cleared from the host after the initial phase remaining in a chronically lytic and/or latent conformation in the host [88].
4) Insufficient immune responses and antibody production against SARS-CoV-2 in the acute phase of COVID-19 infection may be associated with viral persistence [89]. Interestingly, immunologic imprinting, where pre-existing immune responses against related coronaviruses, such as 229E, HKU1, NL63, and OC43, as well as defective immune responses against SARS-CoV2 in the cerebrospinal fluid (CSF) may lead to incomplete virus clearance from the brain, persistent neuroinflammation and neurological post-acute sequelae of COVID-19 [90].
5) The reactivation of latent viruses such as EBV, VZV, HSV, and HHV-6 during and after acute COVID-19 infection in various organs may lead to a plethora of chronic symptoms after COVID-19 (e.g., fatigue, myalgia, cognitive disorders) [91]. These viruses have been implicated in several disorders, including rheumatoid arthritis, multiple sclerosis, lymphomas and cancers [92,93,94,95,96,97].
6) SARS-CoV-2 may trigger autoimmunity via molecular mimicry, epitope spreading and activation of antigen-presenting cells (APCs) following the example of other viruses and bacteria, such as HCV, enteroviruses (coxsackievirus B), EBV, Helicobacter pylori, Yersinia enterocolitica, etc [98,99,100,101]. Immunodominant epitopes of SARS-CoV-2 (e.g., nucleocapsid protein, spike protein) may share homology with host proteins providing insight into viral pathogenesis following COVID-19 [102,103].
7) SARS-CoV-2 infection could cause gut dysbiosis altering the balance of gut microbiota, acting also as a bacteriophage, causing epithelial permeability and translocation of pathogens into the circulation [104,105]. Gut dysbiosis could additionally be implicated in viral persistence, chronic inflammation, immune dysregulation and endothelial dysfunction [83,106,107,108,109,110].
8) LC is characterized by a persistent endothelial dysfunction and a hypercoagulable state [111]. SARS-CoV-2 may also affect the endothelial cells throughout a plethora of tissues, altering cell morphology and leading to apoptosis of endothelial cells. For example, in the brain, the infection of the microvascular endothelium in the subcortical white matter is documented by the presence of microscopic hemorrhagic and ischemic lesions while, in the heart, there is edema of endothelial cells in small arterioles, venules and capillaries as well as necrosis of individual myocytes [112,113]. The attachment of activated neutrophils in capillaries and their subsequent obstruction in several organs including the heart, brain and lungs in conjunction with the presence of fibrin amyloid microclots which provoke tissue hypoxia and oxidative stress may be implicated in the symptomatology of LC [83,114]. In turn, oxidative stress stimulates the generation of proinflammatory cytokines, establishing a vicious cycle [115,116,117,118]. The presence of fibrin aggregates or microclots and activated thrombocytes have also been documented in the blood of patients suffering from type 2 DM, acute COVID-19 infection and ME/CFS contributing to the chronic inflammatory and thrombotic phenomena of these entities [119,120,121].
9) LC is also associated with hormonal dysregulation, characterized by a dysfunction of the hypothalamus–pituitary–adrenal axis [122]. This dysregulation may be caused by hypophysitis, hypothalamic damage, neuroinflammation and molecular mimicry of some viral aminoacids that mimic ACTH residues [122,123]. Moreover, IR in conjunction with activated immune-inflammatory, oxidative, and nitrosative stress pathways may be implicated in neurotoxicity and depressive symptoms observed in LC [124]. IR may be associated with lower metabolic activity in the medial prefrontal cortex and hippocampal volume, neurocognitive impairments, defective synaptic plasticity and neurodegeneration [125]. Interestingly, metabolic dysfunction (i.e., obesity, IR,metabolic syndrome and type 2 DM) constitute predisposing risk factors for severe acute COVID-19 while recent data have underscored that the combination of metabolic dysfunction, chronic immune activation and viral persistence in adipose tissue could exacerbate or predispose to LC [126]. Finally, deficiency in melatonin, a sleep hormone with enhancing adaptive immune response properties, has been associated with a higher risk for COVID-19 [127]. It could also be a predisposing factor in LC as observed in other viral infections and chronic inflammatory disorders [128].
10) Cognitive impairment and neurological symptoms in LC may be attributed to delayed clearance of SARS-CoV-2, endothelial dysfunction and microclot formation, neuronal injury, neuroinflammation, blood brain barrier disruption with infiltrating polyreactive autoantibodies, microglial reactivity and impaired neurogenesis [11,47,129,130,131]. Autonomic nervous system dysfunction and symptoms consistent with dysautonomia, such as orthostatic hypotension, tachycardia, fatigue, temperature dysregulation, etc could be due to the dysfunctional signalling in the brainstem and/or vagus nerve; the presence of autoantibodies against G protein-coupled adrenergic receptor and muscarinic acetylcholine receptor; small fiber neuropathy; neuroinflammation; the failure of peripheral vasoconstriction associated with relative hypovolemia; and cerebral hypoperfusion [83,132].
6. Laboratory findings and biomarkers in long COVID
The main laboratory findings and biomarkers in acute severe COVID-19 encompass biomarkers of systemic inflammation including proinflammatory cytokines, chemokines and complement proteins as well as biomarkers of endothelial injury and coagulation cascades including markers of platelet activation and neutrophil extraction trap formation [111,135]. In particular, the cardinal laboratory features with prognostic potential are: lymphopenia, either isolated or in parallel with an increased absolute neutrophil count, elevated concentrations of C-reactive protein (CRP), interleukin (IL)-6 and IL-2R, increased levels of lactate dehydrogenase (LDH), D-dimer, ferritin, hepatic function markers and troponins [136,137,138]. Besides the elevation of D-dimer, other biomarkers of coagulation abnormalities such as the prolongation of PT and aPTT, the presence of severe thrombocytopenia and the elevation of fibrin degradation products, may reflect life-threatening disseminated intravascular coagulation (DIC), which requires increased vigilance and prompt intervention [139,140,141,142]. All these biomarkers are associated with an increased risk of disease worsening, including acute myocardial infarction, venous thromboembolism and acute ischemic stroke [111,135]. On the contrary, venous thromboembolic disorders, deep vein thrombosis and pulmonary embolism are not primary characteristics of LC. Table 1 synopsizes the main differences in risk factors, clinical and laboratory characteristics between acute severe COVID-19 and LC.
Regarding LC, it is important to mention that there are no specific tests that can be used for its diagnosis. Likewise, clinical features as well as laboratory findings and biomarkers may not safely be attributed to LC. Therefore, the diagnostic evaluation should be personalized, while reassuring at the same time the patient that LC is a clinical entity with a broad spectrum of clinical manifestations and not a psychological or psychiatric disorder. For example, some clinicians may misdiagnose POTS or ME/CFS with mental health disorders, such as anxiety or depression disorders [11,143].
The initial diagnostic work-up should take into account that persisting clinical manifestations belong to the spectrum of LC and not to an underlying disorder. Table 2 presents a general laboratory and imaging diagnostic approach to help clarify symptom etiology, rule out other underlying disorders and evaluate clinical manifestations and resolution of some features of LC.
Besides the usual hematologic, biochemical, coagulation and inflammatory markers, including CRP, serum ferritin, the diagnostic approach may comprise cardiac markers, hormonal and vitamin markers, glycemic indices such as glucose or hemoglobin A1c and determination of autoantibodies. These basic tests often return results within the normal reference range in patients with LC; however, some inflammatory biomarkers may persist for longer [11,81]. The imaging diagnostic approach is important for the evaluation of pulmonary fibrosis resolution with a repeated chest CT scan); cardiac function with a cardiac ultrasound; neurologic and cognitive disorders with brain magnetic resonance imaging, etc. [144]. It is important to mention that some diagnostic tools may be used for the evaluation of features of LC, such as the validated “symptom burden questionnaire for LC” (SBQ-LC), tests examining orthostatic intolerance for the postural orthostatic tachycardia syndrome (POTS), cardiac magnetic resonance for cardiovascular abnormalities and residual pathology, electrocardiogram depicting novel QRS fragmentation due to cardiac injury, pulmonary function tests, etc [144,145,146,147]. Nevertheless, the majority of diagnostic tools for LC is under development such as the use of hyperpolarized magnetic resonance to identify abnormalities of pulmonary gas exchange, imaging to detect microclots or small fiber neuropathy [11,148], while some other tests were also used in patients with ME/CFS and dysautonomia, such as the determination of serum or salivary cortisol, antibodies against herpesviruses, total immunoglobulin concentrations (IgG, IgA, IgM, IgG3), test for Natural Killer Cell Function, tests for orthostatic intolerance, etc. [149]. It is of paramount importance to develop and validate biomarkers for the prediction, diagnosis and prognosis of LC and its therapeutic response. In the following subsections and Table 3, we discuss some promising biomarkers for the prediction, diagnosis and prognosis of LC as well as biomarkers associated with clinical manifestations of LC.
6.1. Biomarkers of systemic inflammation
In response to a viral infection at the acute phase, the immune system activates several cells (T cells, macrophages, etc.) releasing different inflammatory molecules including cytokines and chemokines. SARS-CoV-2 infection may trigger a “cytokine storm” characterized by a moderate proinflammatory cytokine release associated with severe monocyte dysregulation [192]. Acute respiratory distress syndrome (ARDS), one of the leading causes of death in patients with COVID-19, is mainly triggered by the cytokine storm [193]. Interestingly, varied and relapsing symptoms of LC may be due to increased cytokines, released by an abnormal immune response [194].
In the past 2 years, there have been several case-control, prospective and retrospective studies that have investigated inflammatory biomarkers in LC, yielding mixed results. An early meta-analysis of 15 studies on the prevalence of long-term effects in LC including laboratory abnormalities reported limited evidence for systemic inflammation after 4 months approximately post-infection [15]. In particular, 8% of patients had elevated CRP and ferritin while 3% and 4% of patients had increased levels of IL-6 and procalcitonin respectively [15]. However, this was an early meta-analysis that included a very small number of studies examining laboratory abnormalities with a moderate number of participants. In contrast, a very recent meta-analysis of 23 studies (14 prospective and 9 retrospective case-control) with 18 meta-analyzed biomarkers has found that survivors of LC presented higher levels of CRP, D-dimer, lactate dehydrogenase (LDH) and leukocytes than controls without LC; however, the effect sizes were small [150]. After sensitivity analyses, lymphocytes and IL-6 were also significantly elevated in cases with LC. In particular, differences in the levels of D-dimer, LDH, and lymphocytes were prominent in the group of patients with organ abnormalities assessed by imaging and functional studies while differences in levels of IL-6 were observed in the group of patients with persistence of symptoms [150]. Furthermore, differences in the levels of LDH, leukocytes, and N-terminal pro b-type natriuretic peptide (NT-Pro-BNP) were found in the group of patients with symptoms less than 6 months, while differences in D-dimer levels were found in patients with symptoms more than 6 months. IL-8, a chemokine activating neutrophils at the inflammation site, was found elevated in LC patients compared to healthy controls based on only two studies [150]. Finally, another meta-analysis of 22 case-control observational studies has found that IL-6 were higher in patients with LC compared with healthy individuals and those without post-acute sequelae of COVID-19 but lower than in patients during the acute phase of COVID-19 [151]. IL-6, which is a practical biomarker of systemic inflammation and adverse outcomes of acute COVID-19, may serve as a useful predictor of LC after a time window of 4 weeks post infection informing on the “early stage” of LC [151]. In several studies, higher levels of IL-6 were sustained for up to 7 months in patients with LC [81,156,195,196]. Likewise, in some studies, CRP, the acute-phase protein of hepatic origin that is elevated following the release of IL-6 by macrophages and T cells, is persistently increased in LC patients from the early phase [197] and up to 7 months after [20,182].
Additional studies on cytokines and chemokines have shown an augmentation of IL-2 (which stimulates the growth of helper, cytotoxic and regulatory T cells), IL-17 (which is associated with inflammation and auto-immunity), interferon (IFN)-γ (which is critical for innate and adaptive immunity against viral infections), CCL3 and CCL5 in the early phase of LC [20,156,195,198,199]. Patients experiencing LC with cognitive symptoms have shown elevated CCL11, which is associated with inhibition of neurogenesis, aging and cognitive function, compared to those with LC but without cognitive symptoms [200,201]. Contradictory results were reported on anti-inflammatory cytokines IL-4 and IL-10 which were found reduced or elevated in LC patients [156,199]. Compared to recovered patients, IFN-γ remained elevated at 2 months, tumor necrosis factor-α (TNF-α) at 4 months and IFN-β and IFN-λ1 at 11 months in LC patients [85,195]. Interestingly, the genotype AA of the IFNG gene was more frequently found in LC patients [202]. Other acute phase proteins that respond to proinflammatory cytokines and rise following inflammation and tissue injury such as serum amyloid 1 (SAA1) and SAA4 were increased in the microclots of patients with LC at 3 months [182].
Overall, certain phenotypes of LC are associated with increased biomarkers of systemic inflammation; however, data are limited. These biomarkers may present a predictive value to detect patients at risk of LC as well as a diagnostic value for certain LC phenotypes. Further longitudinal studies are required to observe if the pattern of elevation of certain cytokines follows a similar pattern seen in ME/CSF, where some cytokines decrease after being elevated in the first years of the disease despite the persistence of symptoms [203].
6.2. Immune profiling in long COVID
Studies investigating immune dysregulation in patients with LC have found a plethora of alterations in immune cells. Increased inflammatory monocytes (CD14+, CD16+, CCR5+) were found in cases before the development of LC and in the convalescent chronic period [156] along with elevated non-classical monocytes, which are also associated with various chronic inflammatory and autoimmune conditions [152]. Studies have also documented increased Natural Killer (NK) cells expressing markers of memory and activation, higher plasmacytoid dendritic cells exhibiting CD86 and CD38 markers, which play an important role in antiviral immunity and have been implicated in the initiation and development of many autoimmune and inflammatory diseases, and decreases in the numbers of conventional dendritic cells [85,152,154].
Interestingly, individuals with LC present B and T cell abnormalities persisting for at least one year, including decreased naive B and T cells; increased B cells and double negative B cells, which expand in older individuals, but also accumulate prematurely in autoimmune and infectious diseases; decreased CD4+ and CD8+ effector memory cells; increased or decreased SARS-CoV-2 CD8+ T cells expressing cytotoxic markers in patients with respiratory symptoms or gastrointestinal symptoms respectively; reduced exhausted lymphocytes (CD4+/CD8+ expressing PD1) before clinical manifestations of LC; and increased exhausted lymphocytes in the convalescent period of LC [20,85,152,154,168,204].
No firm conclusions can be drawn about T regulatory (Tregs) cells alterations in LC due to inconclusive data [153]. After their initial infection with SARS-CoV-2, patients with LC manifest dysregulation of Treg cell function. These cells play a crucial role in self-tolerance by inhibiting T cell proliferation and cytokine production and preventing autoimmunity. However, there are contradictory findings with higher and lower frequencies of Treg amid CD4+ cells in cases with LC compared to recovered subjects [154,155] while a lower Treg proportion was found in 121 patients with LC compared to controls [156].
Overall, although there is no specific immune signature due to the heterogeneity of LC; the abnormalities in the immunophenotype of cases with LC underscore a prolonged antiviral immune response which is common during chronic exposure to viral antigens and viral persistence.
6.3. Biomarkers reflecting SARS-CoV-2 persistence
Several studies with a small number of participants as well as case series and reports have found components of viral persistence which may trigger symptoms of LC, particularly gastrointestinal symptoms, such as viral proteins (spike and nucleocapsid) and/or SARS-CoV-2 RNA in feces, plasma, urine, brain, muscles, eyes, lymph nodes, cardiovascular organs, liver and lung tissue [87,157,158,159,161,205]. A histopathological study in infected tissues by performing autopsies on 44 COVID-19 cases has found SARS-CoV-2 RNA broadly distributed in 84 distinct anatomical sites up to 230 days after infection. Interestingly, notwithstanding that viral RNA was indetectable in plasma amid all deceased cases, viral persistence was identified throughout a plethora of tissues using high-sensitivity droplet digital PCR, suggesting the sustained presence of low viral load in biospecimens of COVID-19 patients [87]. Moreover, intestinal endoscopic studies particularly in patients with inflammatory bowel disease (IBD) have shown SARS-CoV-2 presence in the gut epithelium or stools even after 6 months post-infection, suggestive of a potential viral reservoir triggering sustained inflammatory responses in some cases of LC [158,160,206]. Interestingly, detectable SARS-CoV-2 RNA in stool samples and increased circulating spike, S1, and nucleocapsid (N) antigens were found in children with MIS-C compared to children with acute COVID-19 or controls, suggesting that viral persistence may trigger the hyperinflammatory responses defining MIS-C [161]. Nonetheless, Sigal et al. did not show any persistence of plasma spike antigen in a multicentric cohort study of children with MIS-C employing an ultra-sensitive electro-chemiluminescent immunoassay [207].
Overall, current available evidence has highlighted that the duration of SARS-CoV-2 infection in cases may persist longer than determined by PCR-negative tests on nasopharyngeal swabs or bronchoalveolar lavage fluids. Sustained low grade multisystem inflammation in both adults and children may be attributed to lingering SARS-CoV-2 infection or reinfection [208]. The use of anti-viral agents against SARS-CoV2 such as nirmatrelvir with ritonavir could eradicate viral reservoirs and attenuate symptoms of LC.
6.4. Humoral and cellular response against SARS-CoV-2 in long COVID
Adaptive immune responses are a key component for the control of viral infection, the severity of the infection and the protection from reinfection. During acute infection, immune responses are crucial for establishing the coordinated immune response required for the development of antibody and memory B cells. Clinical trials have documented that neutralizing antibodies to SARS-CoV-2 may decrease severity of disease, mortality and length of hospitalization [209].
Conflicting results have been reported regarding anti-SARS-CoV-2 antibody response and the occurrence of LC with both positive, neutral and negative associations of SARS-CoV-2-specific antibody titers against spike, S, the receptor-binding domain (RBD) domain of the spike protein or N protein in both hospitalized and non-hospitalized patients [89,152,162,163,164,165].
T cells play a critical role in COVID-19 immunity, severity and mortality, yet relatively little is known about their contribution to LC. A limited set of studies that have investigated SARS-CoV-2-specific T cell responses have implicated T cells in LC, albeit with contradictory findings. While certain studies have reported increased SARS-CoV-2-specific T cell responses in LC in comparison to non-LC cases [162,196], a rapid decay of subsets of SARS-CoV-2-specific CD8+ T cells was observed in the context of LC in another study [165]. Also, the kinetics of antigen-specific T cell responses varied in LC, with individuals presenting similar antigen-specific T cell responses at the early and intermediate phases of convalescence and even elevated responses at a later time point [162]. In one study, a decreased proportion of CD8+ T cells expressing CD107a, a marker of degranulation, in response to the N peptide pool stimulation, and a faster decline in the frequency of N-specific interferon-γ-producing CD8+ T cells were observed in patients with LC after 4 months of COVID-19 onset [165].
6.5. Biomarkers reflecting reactivation of latent viruses
Herpesviruses are ubiquitous and may establish lifelong latency following primary infection. The inability of maintaining latency with short-term or long-term implications may be caused by other infections. In a recent meta-analysis, the prevalence of active herpesviruses infections in COVID-19 patients was 41% for EBV, 3% for HHV-6, 28% for HSV, 25% for CMV, 22% for HSV1, and 18% for VZV, while severe COVID-19 is associated with a 6-fold higher chance for active EBV infection [210]. Interestingly, EBV reactivation in the acute phase of COVID-19 infection may be associated with severe COVID-19 [211].
Reactivated herpesviruses, particularly EBV and HHV-6, were documented in patients with LC [152,166,167,168,169]. Regarding EBV reactivation, EBV viremia or increased titers of anti-EBV antibodies (IgM/IgG against Viral Capsid antigen/VCA and IgG against EBV-encoded nuclear antigen/EBNA) may be early predictive biomarkers of LC. Reactivation may occur soon after or concurrently with COVID-19 infection [152,166,167,168,169,210]. One study demonstrated that early EBV viremia may be associated with fatigue and respiratory symptoms [168], while in two studies increased antibody titers against EBV were associated with fatigue, cognitive dysfunction [166], headache, psycho-neurological disorders, respiratory symptoms and myalgia, and increased liver enzymes, CRP and D-dimer [167]. Reactivation of EBV infection has also been found amid patients with ME/CFS suggesting that EBV is an important factor for the development of the disease [79,212]. Interestingly, an altered and chronically aroused anti-viral profile against latent viruses (EBV, HHV6 and human endogenous retrovirus K), particularly IgG against EBV-encoded nuclear antigen-1 (EBNA1), was noted in patients with ME/CFS after mild/asymptomatic COVID-19 [213].
6.6. Biomarkers reflecting autoimmunity
Infections may trigger antibody polyreactivity and autoimmunity, which are generally considered detrimental [214]. COVID-19 encompasses a broad spectrum of clinical phenotypes that exhibit exaggerated and misdirected host immune responses [215]. Patients with COVID-19 show marked elevations in autoantibody reactivities as compared to uninfected people, with an increased prevalence of autoantibodies against immunomodulatory proteins (e.g., cytokines, chemokines, complement components and cell-surface proteins) that may alter immune function and impede the control of the virus [216]. Autoantibodies, particularly those that neutralize type I IFNs, have been documented to be related with immune dysregulation and COVID-19 severity and death [217], and have been proposed to be associated with LC.
To date, contradictory results have been reported for autoantibodies as a major component in the pathogenesis of LC. In particular, there are studies that did not report a specific profile of autoantibodies, including anti-IFN and anti-IFN-α2 autoantibodies or antinuclear (ANA) antibodies [174,218], that could differentiate patients with LC from recovered patients or controls, [152,171,174,218]. On the contrary, other studies have reported a plethora of autoantibodies in LC, including elevated ANA antibodies (e.g., anti-U1-snRNP and anti-SS-B/La), anti-neuronal antibodies, anti-IFN antibodies, autoantibodies against ACE2, angiotensin II AT1 receptor, angiotensin 1-7 MAS receptor, β2-adrenoreceptor and muscarinic M2 receptor [168,172,173,175,219,220]. Interestingly, in one cohort study, the presence of antibodies against specific chemokines (CCL21, CXCL13 and CXCL16) was negatively associated with the development of LC at 1-year post-infection [170]. It is possible that autoantibodies to certain chemokines may positively impact the long-term outcome of COVID-19 by antagonizing or regulating the activation, recruitment and retention of activated T and B cells in diverse anatomic sites [170]. Finally, in some studies, specific autoantibodies were associated with clinical phenotypes of LC. ANAs were associated with persistent symptoms of fatigue and dyspnea [172], antineuronal antibodies in CSF and serum with cognitive impairment [173], and anti-IFN-α2 or anti-IFN-λ autoantibodies with respiratory symptoms of LC [168,175].
6.7. Endothelial or vascular biomarkers
Recent data have shown that endothelial inflammation and damage in COVID-19 could lead to long-term implications for vascular function [177,221]. Endotheliopathy is also observed in LC being associated with the disease [83]. Furthermore, increased inflammatory mediators in LC may lead to the upregulation of cell adhesion molecules and angiogenesis factors, and the shedding of the protective glycocalyx matrix of the capillary endothelium with subsequent significant alterations in microvascular resistance and hemodynamics [83,222]. The adhesion of hyperactivated neutrophils to capillaries in the brain, lungs, heart and other tissues or organs may further be implicated in the pathogenesis of LC [83,114]. In a recent observational study, elevated endothelin-1, a biomarker that mediates vasoconstriction, and decreased angiopoietin-2, a biomarker of vascular angiogenesis, were reported in patients with LC and fatigue [177]. Interestingly, decreased angiopoietin-2 was found exclusively in LC and could be a differentiation biomarker between LC and ME/CFS [177]. In another study, angiopoietin-1 and P-selectin, a protein synthesized by activated thrombocytes and endothelial cells that acts as a cell adhesion molecule, presented excellent sensitivity and specificity for predicting LC status among 16 blood biomarkers of vascular transformation [176]. However, a larger cross-sectional study did not find significant differences in vascular biomarkers between patients recovered from COVID-19 one year after hospital discharge and controls [178].
6.8. Biomarkers of coagulation and fibrinolysis
Endothelial dysfunction and hypercoagulability may present in some patients approximately 1 year after recovery from COVID-19 [223]. Interestingly, some patients with LC have a genetic predisposition for thrombophilia based on the evaluation of related genetic polymorphisms [223]. Individuals with LC may present with anomalous fibrin amyloid microclots that block capillaries and cause tissue hypoxia, dysfunction in oxygen exchange and tissue damage upon restoration of oxygen supply (ischemia-reperfusion injury) [83,224]. These microclots which are resistant to fibrinolysis may trigger oxidative stress and the secretion of proinflammatory cytokines, establishing a vicious cycle that may be implicated in the plethora of clinical manifestations observed in LC [83,182,224]. Several studies have shown that microclots were identified in the plasma of patients with LC, carrying altered levels of coagulation and fibrinolysis proteins, that are involved in endothelial injury, platelet activation, coagulation and fibrinolysis, such as increased von Willebrand factor (vWF), platelet factor 4, fibrinogen chains α and β, factor XIII, plasminogen and antiplasmin (α2AP), and decreased plasma kallikrein [181,182]. Numerous proinflammatory molecules, such as SAA, antibodies and complement components trapped inside microclots were also detected by proteomics in LC [111,181,182,225]. Interestingly, ME/CFS is also characterized by substantial and measurable alterations in platelet hyperactivation, coagulability, and fibrinoid microclot formation; nevertheless, the load of microclots is greater in LC [119].
A meta-analysis of 23 prospective and retrospective studies with 18 meta-analyzed biomarkers has shown that elevated D-dimer presents a diagnostic utility in LC albeit of small effect, being present in some patients with organ abnormalities and in patients with duration of symptoms more than 6 months [150]. Concentrations of D-dimer have also been associated with severe COVID-19 infection [226]. Interestingly, abnormal D-dimer levels were found in children with LC and more symptoms at 12 weeks post-infection compared to children that had fully recovered at the 8-12 weeks [180]. Collectively, these findings underscore the contribution of endotheliopathy, coagulopathy and failed fibrinolysis in the pathogenesis of LC.
6.9. Hormonal and metabolic biomarkers
Endocrine dysfunction may also be implicated in LC pathogenesis. Two longitudinal multi-omics studies have reported persistent low levels of cortisol as a robust distinctive characteristic between patients with LC, convalescent individuals and healthy controls [152,168]. In the yet unpublished, exploratory, cross-sectional and longitudinal study of 220 individuals, plasma cortisol in patients with LC was half of that in age-, sex- and BMI-matched controls at 400 days post-infection, while hypocortisolemia was the most significant predictor for LC occurrence based on machine learning tools [152]. Moreover, a recent multi-omics, longitudinal study has shown that low plasma cortisol in conjunction with the presence of anti-IFN autoantibodies were found in patients with LC and respiratory symptoms 3 months later [168]. Intriguingly, low cortisol secretion by the adrenal glands was not compensated by an increase in adrenocorticotropic hormone (ACTH), suggesting a dysfunction in the hypothalamus-pituitary-adrenal (HPA) axis. This dysfunction is compatible with clinical manifestations present in primary adrenal insufficiency (Addison’s disease), such as fatigue, brain fog, muscle weakness, nausea, abdominal pain, body hair loss, anxiety or depression, etc. [227]. Interestingly, hypocortisolemia with hypo-responsiveness of the HPA axis and chronic fatigue are observed in patients with ME/CFS, chronic stress disorders and fibromyalgia, and some post-viral infection syndromes such as post-SARS and post-MERS [72,122,228,229,230]. Low cortisol has also been documented in acute COVID-19 [231]. Notably, the triad of hypocortisolemia, reactivation of EBV and T-cell exhaustion has also been reported in ME/CSF which accounts for a significant percentage of LC patients [232,233].
Regarding other hormonal and metabolic alterations, in a retrospective analysis of 186 patients with LC but without convalescent or control patients, low cortisol was associated with dysosmia/dysgeusia. Low serum growth hormone and increased serum FT4 were linked to general fatigue while higher thyrotropin (TSH) and a lower of FT4/TSH was found in the initially severe LC cases [183]. In another retrospective cohort study, patients with LC presented increased new onset IR, while increased IR was significantly linked to depressive symptoms [124]. Interestingly, lower adiponectin, which is associated with obesity, metabolic syndrome and IR and cancer [234,235,236,237,238,239,240,241,242,243,244] was detected in digested microclots of LC patients compared to the control group [181]. Finally, in a randomized trial of 1,125 adults aged 30 to 85 with overweight or obesity in the US, there was a 42% relative reduction in the incidence of LC in the metformin group compared to its blinded control [245].
6.10. Various proteins as biomarkers
In a prospective longitudinal cohort study of 2,320 participants discharged from hospital, plasma proteome data have shown that 13 inflammatory proteins were associated with the severe group of LC [81]. The highest protein concentration was trefoil factor 2 (TFF2), a protein released with mucin from mucosal epithelium comprising lung and gastric mucosa, suggesting persistent mucosal epithelial abnormalities and inflammatory cell activation. Increased IL-6 and CD70 were associated with cognitive impairment, highlighting the role of CD70 in neuroinflammation in the CNS. Furthermore, higher serum agrin, which has been detected in older adults with sarcopenia, was associated with physical impairment [81]. In another longitudinal proteomic case-control study of 156 healthcare workers, a plasma proteomic signature associated with lipid, atherosclerosis and cholesterol metabolism pathways, complement and coagulation cascades, autophagy, and lysosomal function at the time of seroconversion had the potential to predict patients who are more likely to suffer from LC [184]. Finally, another proteomic study found evidence of a failed fibrinolytic system in LC associated with the entrapment of many proinflammatory proteins, which may be important for patients with pre-existing comorbidities, including cardiovascular disease and type 2 DM [181].
6.11. Metabolites as biomarkers
Metabolomics could be a powerful tool for diagnostic, prognostic and drug intervention analysis in COVID-19 as well as in LC [246]. Although there is no a characteristic metabolite signature associated with LC, some studies have shown that LC may present: 1) an altered fatty acid metabolism and dysfunctional mitochondria-dependent lipid catabolism consistent with previously reported mitochondrial dysfunction during exercise [134]; 2) an activation of the kynurenine pathway, and specifically the elevation of the metabolites quinolinic acid, 3-hydroxyanthranilic acid and kynurenine is linked to cognitive impairment in LC [187]; 3) a dysregulation in the sphingolipid metabolism that could be associated with fatigue and muscular pain in LC [185]. Overall, based on metabolomics studies, mitochondrial dysfunction, impaired energy metabolism, altered lipid metabolism and redox state imbalance are main hallmarks of LC.
6.12. Microbiota alterations in long COVID
Gut dysbiosis may contribute to the development of several metabolic, autoimmune and inflammatory disorders, including ME/CFS [240,247,248,249]. Several lines of evidence have shown the replication of SARS-CoV-2 in human enterocytes, its detection in stool samples as well as an altered intestinal microbiota composition in patients with COVID-19, which correlate with disease severity and inflammatory biomarkers [250]. Gut dysbiosis could persist after disease resolution and be implicated in LC [251]. Indeed, based on some prospective follow-up studies in recovered COVID-19 patients and controls, gut microbiota dysbiosis may be present at one-year after discharge in recovered COVID-19 patients, being predictive of LC occurrence [188,189].
Patients with LC may present: 1) reduced bacterial diversities; 2) lower relative abundance of Short-chain fatty acids (SCFA)-producing beneficial symbionts, such as Eubacterium_hallii_group, Subdoligranulum, Ruminococcus, Dorea, Coprococcus, and Eubacterium_ventriosum [188,189]; 3) lower levels of butyrate-producing bacteria that are associated with LC at 6 months [189]; 4) increased abundance of Ruminococcus gnavus, Bacteroides vulgatus and decreased abundance of Faecalibacterium prausnitzii [189]. Interestingly, microbiota transfer from individuals with LC provoked a decline in brain cognitive properties and dysfunctional lung defense in mice, which was partially prevented by the administration of the commensal probiotic Bifidobacterium longum [252]. Probiotics, prebiotics and synbiotics, that have shown beneficial metabolic and immunologic properties [248,253,254,255], could be used as adjunct therapeutic tools in LC in the future. Finally, although there are no data on mycobiota alterations in LC, a study has found increased levels of fungal translocation from the gut and/or the lung epithelia, determined by β-glucan, a fungal cell wall polysaccharide, in the plasma of individuals of LC, suggesting the important role of fungal translocation in chronic immune activation due to gut barrier permeability [256].
Overall, all these findings suggest that an individual’s intestinal microbiome configuration at the time of SARS-CoV-2 infection may alter the susceptibility to long-term complications of COVID-19. Nonetheless, these alterations may represent reactive changes to LC; therefore, future research including prospective longitudinal studies with a multi-omics approach of non-hospitalized patients followed from the time of infection until the development of persistent symptoms is required to delineate the exact contribution of intestinal dysbiosis to LC.
6.13. Cerebrospinal fluid biomarkers
Cerebrospinal fluid (CSF) analysis is a diagnostic mainstay in neuroinflammatory disorders. Nevertheless, limited information on CSF data in patients with LC is currently available [129]. In a systematic review, non-specific inflammatory CSF abnormalities were frequently found in patients with COVID-19 and neurological symptoms; however, the elevation of neurodegeneration biomarkers could suggest that neuronal damage may present unknown long-term implications [257]. In a retrospective multicenter analysis of 150 lumbar punctures in 127 patients with PCR-proven COVID-19 and neurological involvement, the CSF profile has shown markers of blood-brain barrier disruption in the absence of intrathecal inflammation, which is compatible with cerebrospinal endotheliopathy [258]. This blood-brain barrier dysfunction as well as the increased levels of cytokines and chemokines may be implicated in both acute neurologic symptoms as well as in LC. Another study with a small sample size in patients with neuro-COVID, has shown an increase in CSF biomarkers of neuroinflammation and neurofilament light chain, indicative of neuronal damage [259]. In a cross-sectional and long-term longitudinal study with a multi-omics approach, the prevailing signs of severe neuro-COVID were dysfunction of the blood-brain barrier, increased microglia activation biomarkers and a polyclonal B cell response targeting self-antigens and non-self-antigens [129]. Patients with neuro-COVID-19 presented with decreased regional brain volumes related with specific CSF markers; nonetheless, COVID-19 patients with cytokine storm did not show an inflammatory CSF profile [129].
LC is more prevalent in patients with severe neuro-COVID and is linked to specific plasma and CSF biomarkers. In a long-term follow-up study, within CSF, low levels of the anti-inflammatory protein TRANCE (RANKL) in conjunction with increased levels of the proinflammatory protein TNFRSF9 and IFN-γ levels were the best single protein predictors for LC [129]. Furthermore, the upregulation of plasma CLM-6, monocyte chemotactic proteins (MCP)-3 and ST1A1, which are involved in macrophage and monocyte activation and infiltration in the central nervous system (CNS) and in autoimmune encephalitis, may predict LC [129,260]. After mild COVID-19, sustained inflammatory response may not be a major component in the pathogenesis of LC with neurological symptoms based on CSF findings in subjects with cognitive impairment developing one to six months after recovery [190]. In this small case-control study within a prospective study evaluating recovery from COVID-19, although the majority of participants presented normal values in CSF for many parameters (white blood cells, glucose, CSF/serum albumin ratio, IgG index, etc), a higher proportion of abnormal CSF findings and an abnormal oligoclonal banding pattern were detected in 77% and 69% of patients with LC and cognitive impairment versus 0% of controls, underscoring a potential abnormal autoimmune response [190]. Finally, in a prospective case-control study of 60 hospitalized neuro-COVID patients, only levels of protein 14-3-3 and neurofilament light chain (NfL) in the CSF, which are biomarkers of neuroaxonal damage, were significantly associated with the degree of neurologic disability in daily activities at 18 months follow-up [191].
Overall, all these biomarkers are associated with neuropathologic mechanisms including peripherally induced cytokine alterations followed by blood-brain barrier dysfunction with intrusive polyreactive autoantibodies, endothelial dysfunction and coagulopathy, increased reactivity of microglia, neuroinflammation and neuronal damage.
7. Biomarkers classifying clinical manifestations in long COVID
LC represents a heterogeneous complex multi-system disorder with different clinical manifestations; hence, it would be ideal to categorize it for diagnostic, prognostic and therapeutic purposes. Notwithstanding that the majority of biomarkers analyzed in this review concerns the totality of LC, candidate specific biomarkers for major distinctive clinical features of LC are classified into the following groups: general symptoms including fatigue and muscle pain; respiratory symptoms; neurologic symptoms; and gastrointestinal symptoms. Figure 2 depicts main candidate biomarkers for symptom-distinctive features of LC.
7.1. Candidate biomarkers for general symptoms and fatigue
Overall, altered levels of D-dimer, LDH, and lymphocytes were characteristic of patients with organ abnormalities evaluated by imaging and functional studies whilst increased levels of IL-6, D-dimer and CRP were observed in some patients with persistence of symptoms (more than 6 months) [20,81,150,156,182,195,196]. Interestingly, D-dimer was increased in children with LC and persistent symptoms [180]. In some patients, increased concentrations of IL-6 and CRP are informative of the early stage of LC [151,197]. Symptoms of fatigue and physical impairment are associated with early EBV viremia; increased antibody titers against EBV, anti-Spike SARS-CoV-2 IgG at 2 months after infection, and ANAs; higher serum endothelin-1, agrin and FT4; lower angiopoietin-2, cortisol and growth hormone; as well as altered metabolites in the sphingolipid metabolism [81,152,164,166,168,172,177,183,185]. More importantly, decreased angiopoietin-2 was reported exclusively in LC differentiating LC from ME/CFS [177].
7.2. Candidate biomarkers for neurological symptoms
Neurological symptoms are common in LC [15] being associated with increased levels of proinflammatory cytokines IL-6, MCP-1 and TNF-α in certain patients [261]. Cognitive dysfunction was associated with reactivation of EBV; increased CCL11, IL-6, CD70 and antineuronal antibodies; elevated concentrations of S-sulfocysteine; higher levels of metabolites of the kynurenine pathway (quinolinic acid, 3-hydroxyanthranilic acid, and kynurenine) [124,166,173,187,201,256,262]. In CSF, cognitive impairment was associated with a greater frequency of CSF abnormalities and abnormal oligoclonal banding; a higher frequency of anti-neuronal antibodies; and increased levels of proteins 14-3-3 and NfL [173,190,191]. Elevated levels of cytoskeletal proteins NfL and glial fibrillary acidic protein (GFAP), which maintain the stability of neuronal axons and astrocytes, and β-glucan were linked to worse headaches and persistent neuropathic pain in patients with LC [261,263]. Depressive symptoms were linked to new onset IR, as expressed by an increased Homeostatic Model Assessment for Insulin Resistance (HOMA-IR) score [124] while dysosmia/dysgeusia was associated with low serum cortisol [183]. Finally, elevated levels of exosomes containing SARS-CoV-2 proteins and lower levels of mitochondrial proteins may be promising biomarkers for neuropsychiatric symptoms [264]; however, more studies are required to delineate their significance in neurological LC.
7.3. Candidate biomarkers for respiratory symptoms
Pulmonary lesions represent frequent sequelae of SARS-CoV-2 infection with a considerable proportion of COVID-19 survivors from previous variants presenting residual lung lesions such as ground-glass opacity and fiber streak shadow [265]. Cough and dyspnea are the most frequent and persistent symptoms lasting more than 7 months in 20% and 40% of patients respectively [266]. In a study with convalescent patients followed one year after discharge, patients with pulmonary sequelae presented a prominent immunologic profiling characterized by the activation of cytotoxic T cells expressing markers of exhaustion and senescence, NK cells, and γδ T cells, as well as a deficit of suppressive cells [265]. In other patients, respiratory symptoms were associated with early EBV viremia and increased antibody titers against EBV [166,168], elevated ANAs and anti-IFN-α2 or anti-IFN-λ autoantibodies [168,172,175]; low plasma cortisol [168] and higher S-sulfocysteine [256]. Finally, another study has shown that patients with respiratory symptoms of LC exhibited higher levels of CRP, IL-6 and SARS-CoV-2-CD4+/CD8+ T cells secreting IFN-γ or TNF-α at 7 months post-infection [196].
7.4. Candidate biomarkers for gastrointestinal and other specific symptoms
Promising biomarkers for gastrointestinal manifestations in LC and MIS-C include SARS-CoV-2 RNA in stool and increased circulating viral proteins (S, S1, N); increased levels of zonulin, LPB, β-glucan, autoAb La/SS-B and CMV-specific CD8+ T cells as well as elevated SARS-CoV-2-specific CD8+ T cells expressing cytotoxic markers [20,158,161,168,256]. Finally, in a prospective observational study one year after hospital discharge of 263 COVI-19 survivors of whom 26.2% had hair loss, lower levels of Growth Arrest-Specific 6 (Gas6) and its soluble receptor Axl (sAxl) were associated with a history of alopecia [267].
8. Limitations of studies and challenges
In this review, we have appraised and summarized biomarkers related to LC. Nevertheless, no specific biomarker and laboratory test or panel of biomarkers may differentiate LC from other disease entities with adequate certainty. Previous data have shown that many phenotypes and distinct sub-diagnoses could exist under the umbrella of LC; therefore, sequelae of COVID-19 may certainly not be due to a unique pathogenetic pathway. Moreover, due to the heterogeneous and multifaceted pathogenesis of LC, the diagnostic and predictive performance of the majority of biomarkers is modest.
There are many methodological limitations in the studies evaluating laboratory findings and biomarkers for the prediction, diagnosis and prognosis of LC. In the beginning, there was an absence of a consensus disease definition for LC which led to misclassification of subjects. Misclassification could arise when it is difficult to differentiate long-term symptoms potentially attributed to LC from symptoms due to other conditions both related or unrelated to LC. Another significant shortcoming was the reliance on self-reported information regarding LC status, which could lead to selection bias. The timing of symptom onset is also subject to recall bias particularly when information is collected many months after acute COVID. More importantly, some studies focused on hospitalized cohorts which are not representative of the general population. Other issues include the false negative rate of PCR tests which could classify participants as controls as well as the limited utility of antibody titers to determine previous SARS-CoV-2 infection [11]. On the contrary, some studies did not stipulate laboratory-confirmed diagnosis of COVID-19 and focused on most common symptoms and different time periods with great variability [268].
Most studies were underpowered due to small sample sizes, particularly for control groups, and included convenient cohorts with participants who were not lost in follow-up. Many studies had a retrospective design where most of the biomarkers were determined after the onset of LC symptoms; hence, altered biomarkers could be an epiphenomenon of LC. Finally, the majority of studies were conducted in the early phase of the pandemic examining a limited set of biomarkers; therefore, it is not clear how these biomarkers are useful for LC due to omicron subvariants.
9. Therapeutic perspectives and challenges
Although most therapeutic approaches put to test against LC have targeted symptom alleviation [269], a comprehensive evaluation of symptoms and clinical signs of affected patients is imperative, in order to timely recognize “red flag” features pointing towards underlying objective systemic disorders that are likely to have a decisive impact on patient prognosis. Likewise, meticulous laboratory, radiological and other functional investigations should be reserved for patients exhibiting such features, and not necessarily be broadly offered as a screening process in all cases of ongoing symptoms following acute infection. Overall, in order to optimize patient access to adequate care and reduce the burden on secondary and tertiary hospitals, evaluation and initial management ought to be commissioned to primary care units, after adequate information and education of primary care physicians. Ideally, primary patient care should be based on uniform evaluation algorithms and standardized procedures. Regarding patients exhibiting “red flag” symptoms or manifestations of debilitating magnitude, further referral to specialist care should be carried out through interdisciplinary ambulatory COVID clinics, offering facilitated access to specialized personnel and investigations, essentially acting as a link between primary and hospital care [270].
Not surprisingly for a constellation of symptoms and disorders as broad as those described under the umbrella term “LC”, no single therapeutic intervention with proven benefit for all affected patients exists. However, there exist certain candidate treatments which may be potentially effective for specific patient groups or symptom clusters. Among those with chronic fatigue, interventions with demonstrated benefit in ME/CFS may prove useful, most prominently lifestyle management (pacing, optimization of energy management, regular rests, etc.) or even pharmacologic interventions such as naltrexone [11,270]. Similar to the management of other causes of dysautonomia with postural hypotension, these findings in the context of LC may benefit from high salt and fluid intake, beta-blockers, low-dose fludrocortisone, and desmopressin, among others, depending on clinical presentation [271].
Among agents approved for the treatment of SARS-CoV-2 infection, the combination of nirmatrelvir with ritonavir (marketed under the name Paxlovid) has shown potential effectiveness in the mitigation of LC symptoms. Geng et al. reported a case of a patient with ongoing symptoms 6 months following breakthrough SARS-CoV-2 infection, which were alleviated after a 5-day Paxlovid course [272]. Furthermore, in a recent study among 281,793 patients who had at least 1 risk factor for progression to severe COVID-19, those who received Paxlovid for 5 days (n=35,717) had a 26% lower risk of LC compared with those receiving no antiviral or monoclonal antibody treatment [273]. Nevertheless, other cohort studies have failed to demonstrate corresponding benefits on long term COIVD sequalae by Paxlovid treatment [274,275].
By the lack of specific therapeutic agents to tackle LC, repurposing of drugs marketed for other indications may show promise towards that end. Metformin, a first-line drug for the treatment of DM type 2 with documented in vitro [276,277] and in vivo [277] activity against SARS-CoV-2 showed effectiveness for LC prevention in a recent randomized, placebo-controlled clinical trial [245]. Using a parallel-group design, 1,125 ambulatory individuals with overweight or obesity and documented SARS-CoV-2 infection within three days prior to enrollment were randomized between rapidly titrated metformin treatment and placebo, and additionally between ivermectin and/or fluvoxamine treatment vs. placebo. The duration of all study intervention was 14 days. Diagnosis of LC 300 days following randomization was a prespecified study outcome and occurred at a 42% lower rate among those that received metformin vs. placebo. No additional effects were noted for ivermectin or fluvoxamine [245]. An important implication of these findings is the need for interventions as early as at first diagnosis of acute infection for LC prevention. Although the reported results are definitely promising, more studies are needed in order to generalize these findings in population with additional risk factors for LC other than overweight/obesity.
AXA1125 is a novel orally administered endogenous metabolic modulator structurally consisting of five amino acids, which improves mitochondrial efficiency and promotes beta oxidation [278]. In a recent randomized controlled trial, oral administration of AXA1125 twice daily for four weeks to patients with fatigue-predominant LC resulted in greater symptomatic improvement vs. placebo (assessed by the 28 Chalder Fatigue Questionnaire [CFQ-11] fatigue score). There were no improvements in skeletal muscle mitochondrial function assessed by magnetic spectroscopy. Although these findings are definitely promising, the relatively short follow-up duration of this study should be taken into account [279].
To date, more than 36 randomized trials have been registered in ClinicalTrials.gov [280] which include a mixture of dietary and herbal supplements, vitamins, cell-based treatments, anti-inflammatory agents, steroids, anti-coagulants, anti-depressants, lifestyle intervention, etc. All these heterogeneous trials are not generally focused on a cluster of LC while they are small in size not corresponding to the millions of prevalent LC cases. Larger multi-center high-quality and methodologically robust randomized placebo-controlled trials conducted with standardization of outcomes are needed to confirm any benefit from treatments found in smaller trials [281].
10. Concluding remarks- Quo vadis?
The constellation of symptoms and disorders in the spectrum of LC, though seldom life-threatening, have a significant negative impact on individual functional status and quality of life. Given its high incidence and prevalence following acute infection, LC is a condition with a considerable societal and health care impact. With rates of direct morbidity and mortality by acute infection subsiding due to broad vaccination- and infection-related immunity as well as less virulent SARS-CoV-2 strains, the relative impact of long-term sequelae associated with SARS-CoV-2 infection is gaining on importance.
There is an imperative need to determine the features of those at high risk for LC but also specific characteristics within patient groups most likely to benefit from therapeutic interventions. Since clinical risk factors themselves do not suffice for this task, focus has been set in the recognition of sensitive and reliable diagnostic biomarkers. Unfortunately, this effort has yielded little robust results to date, plagued among others by methodological issues pertinent to the available, mostly retrospective, epidemiological studies. Future attempts should be focused on evaluating ideally readily available serum, radiological or other biomarkers, which will additionally aid to shed more light on the underlying mechanisms that drive LC development. In turn, these should be put to test in the frame of randomized clinical trials of candidate therapeutic interventions, in order to promote precision medicine in the management of affected patients.
Author Contributions
MD conceived the idea of the review, organized its plan and supervised the study. MD, DT and NV wrote parts of the manuscript. IK, GP, GSC and DP performed literature search and prepared the Tables. GSC made the Figures. DT, FM and MD reviewed the manuscript. The corresponding author states that all authors meet authorship criteria.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int/ (accessed on 17 May 2023).
- Lee, W.E.; Woo Park, S.; Weinberger, D.M.; Olson, D.; Simonsen, L.; Grenfell, B.T.; Viboud, C. Direct and indirect mortality impacts of the COVID-19 pandemic in the United States, March 1, 2020 to January 1, 2022. Elife 2023, 12. [Google Scholar] [CrossRef] [PubMed]
- Nicola, M.; Alsafi, Z.; Sohrabi, C.; Kerwan, A.; Al-Jabir, A.; Iosifidis, C.; Agha, M.; Agha, R. The socio-economic implications of the coronavirus pandemic (COVID-19): A review. Int J Surg 2020, 78, 185–193. [Google Scholar] [CrossRef] [PubMed]
- Tsilingiris, D.; Vallianou, N.G.; Karampela, I.; Liu, J.; Dalamaga, M. Potential implications of lipid nanoparticles in the pathogenesis of myocarditis associated with the use of mRNA vaccines against SARS-CoV-2. Metabol Open 2022, 13, 100159. [Google Scholar] [CrossRef] [PubMed]
- Marzianο, V.; Guzzetta, G.; Menegale, F.; Sacco, C.; Petrone, D.; Urdiales, A.; del Manso, M.; Bella, A.; Fabiani, M.; Vescio, M.; et al. The decline of COVID-19 severity and lethality over two years of pandemic. 2022. [Google Scholar] [CrossRef]
- Sigal, A. Milder disease with Omicron: is it the virus or the pre-existing immunity? Nat Rev Immunol 2022, 22, 69–71. [Google Scholar] [CrossRef] [PubMed]
- Mahase, E. Covid-19: What do we know about XBB.1.5 and should we be worried? Bmj 2023, 380, 153. [Google Scholar] [CrossRef] [PubMed]
- WHO. XBB.1.5 Updated Risk Assessment, 24 February 2023. Available online: https://www.who.int/docs/default-source/coronaviruse/22022024xbb.1.5ra.pdf (accessed on 15 May 2023).
- Siddiqui, S.; Alhamdi, H.W.S.; Alghamdi, H.A. Recent Chronology of COVID-19 Pandemic. Front Public Health 2022, 10, 778037. [Google Scholar] [CrossRef] [PubMed]
- Líška, D.; Liptaková, E.; Babičová, A.; Batalik, L.; Baňárová, P.S.; Dobrodenková, S. What is the quality of life in patients with long COVID compared to a healthy control group? Front Public Health 2022, 10, 975992. [Google Scholar] [CrossRef]
- Davis, H.E.; McCorkell, L.; Vogel, J.M.; Topol, E.J. Long COVID: major findings, mechanisms and recommendations. Nat Rev Microbiol 2023, 21, 133–146. [Google Scholar] [CrossRef]
- Jennings, G.; Monaghan, A.; Xue, F.; Mockler, D.; Romero-Ortuño, R. A Systematic Review of Persistent Symptoms and Residual Abnormal Functioning following Acute COVID-19: Ongoing Symptomatic Phase vs. Post-COVID-19 Syndrome. J Clin Med 2021, 10. [Google Scholar] [CrossRef]
- WHO. A clinical case definition of post COVID-19 condition by a Delphi consensus, 6 October 2021. Available online: https://www.who.int/publications/i/item/WHO-2019-nCoV-Post_COVID-19_condition-Clinical_case_definition-2021.1 (accessed on 15 May 2023).
- Roe, K. The Symptoms and Clinical Manifestations Observed in COVID-19 Patients/Long COVID-19 Symptoms that Parallel Toxoplasma gondii Infections. J Neuroimmune Pharmacol 2021, 16, 513–516. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Leon, S.; Wegman-Ostrosky, T.; Perelman, C.; Sepulveda, R.; Rebolledo, P.A.; Cuapio, A.; Villapol, S. More than 50 long-term effects of COVID-19: a systematic review and meta-analysis. Sci Rep 2021, 11, 16144. [Google Scholar] [CrossRef]
- Castanares-Zapatero, D.; Chalon, P.; Kohn, L.; Dauvrin, M.; Detollenaere, J.; Maertens de Noordhout, C.; Primus-de Jong, C.; Cleemput, I.; Van den Heede, K. Pathophysiology and mechanism of long COVID: a comprehensive review. Ann Med 2022, 54, 1473–1487. [Google Scholar] [CrossRef] [PubMed]
- Dalamaga, M.; Karmaniolas, K.; Matekovits, A.; Migdalis, I.; Papadavid, E. Cutaneous manifestations in relation to immunologic parameters in a cohort of primary myelodysplastic syndrome patients. J Eur Acad Dermatol Venereol 2008, 22, 543–548. [Google Scholar] [CrossRef] [PubMed]
- Mentis, A.A.; Dalamaga, M.; Lu, C.; Polissiou, M.G. Saffron for “toning down” COVID-19-related cytokine storm: Hype or hope? A mini-review of current evidence. Metabol Open 2021, 11, 100111. [Google Scholar] [CrossRef] [PubMed]
- Varghese, J.; Sandmann, S.; Ochs, K.; Schrempf, I.M.; Frömmel, C.; Dugas, M.; Schmidt, H.H.; Vollenberg, R.; Tepasse, P.R. Persistent symptoms and lab abnormalities in patients who recovered from COVID-19. Sci Rep 2021, 11, 12775. [Google Scholar] [CrossRef] [PubMed]
- Espín, E.; Yang, C.; Shannon, C.P.; Assadian, S.; He, D.; Tebbutt, S.J. Cellular and molecular biomarkers of long COVID: a scoping review. EBioMedicine 2023, 91, 104552. [Google Scholar] [CrossRef] [PubMed]
- Lai, Y.J.; Liu, S.H.; Manachevakul, S.; Lee, T.A.; Kuo, C.T.; Bello, D. Biomarkers in long COVID-19: A systematic review. Front Med (Lausanne) 2023, 10, 1085988. [Google Scholar] [CrossRef]
- Nasserie, T.; Hittle, M.; Goodman, S.N. Assessment of the Frequency and Variety of Persistent Symptoms Among Patients With COVID-19: A Systematic Review. JAMA Netw Open 2021, 4, e2111417. [Google Scholar] [CrossRef]
- Mizrahi, B.; Sudry, T.; Flaks-Manov, N.; Yehezkelli, Y.; Kalkstein, N.; Akiva, P.; Ekka-Zohar, A.; Ben David, S.S.; Lerner, U.; Bivas-Benita, M.; et al. Long covid outcomes at one year after mild SARS-CoV-2 infection: nationwide cohort study. Bmj 2023, 380, e072529. [Google Scholar] [CrossRef]
- UK Office for National Statistics. Prevalence of ongoing symptoms following coronavirus (COVID-19) infection in the UK. Available online: https://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/conditionsanddiseases/datasets/alldatarelatingtoprevalenceofongoingsymptomsfollowingcoronaviruscovid19infectionintheuk (accessed on 17 May 2023).
- Ahmad, F, B.; Anderson, R.N.; Cisewski, J.A.; Sutton, P.D. Identification of deaths with post-acute sequelae of COVID-19 from death certificate literal text: United States, January 1, 2020–June 30, 2022. NCHS Vital Statistics Rapid Release; no 25. December 2022. [CrossRef]
- Du, M.; Ma, Y.; Deng, J.; Liu, M.; Liu, J. Comparison of Long COVID-19 Caused by Different SARS-CoV-2 Strains: A Systematic Review and Meta-Analysis. Int J Environ Res Public Health 2022, 19. [Google Scholar] [CrossRef] [PubMed]
- Antonelli, M.; Pujol, J.C.; Spector, T.D.; Ourselin, S.; Steves, C.J. Risk of long COVID associated with delta versus omicron variants of SARS-CoV-2. Lancet 2022, 399, 2263–2264. [Google Scholar] [CrossRef] [PubMed]
- Nehme, M.; Vetter, P.; Chappuis, F.; Kaiser, L.; Guessous, I. Prevalence of Post-Coronavirus Disease Condition 12 Weeks After Omicron Infection Compared With Negative Controls and Association With Vaccination Status. Clin Infect Dis 2023, 76, 1567–1575. [Google Scholar] [CrossRef] [PubMed]
- Ballouz, T.; Menges, D.; Kaufmann, M.; Amati, R.; Frei, A.; von Wyl, V.; Fehr, J.S.; Albanese, E.; Puhan, M.A. Post COVID-19 condition after Wildtype, Delta, and Omicron SARS-CoV-2 infection and prior vaccination: Pooled analysis of two population-based cohorts. PLoS One 2023, 18, e0281429. [Google Scholar] [CrossRef] [PubMed]
- Levy, N.; Koppel, J.H.; Kaplan, O.; Yechiam, H.; Shahar-Nissan, K.; Cohen, N.K.; Shavit, I. Severity and Incidence of Multisystem Inflammatory Syndrome in Children During 3 SARS-CoV-2 Pandemic Waves in Israel. Jama 2022, 327, 2452–2454. [Google Scholar] [CrossRef] [PubMed]
- Amanatidou, E.; Gkiouliava, A.; Pella, E.; Serafidi, M.; Tsilingiris, D.; Vallianou, N.G.; Karampela, I.; Dalamaga, M. Breakthrough infections after COVID-19 vaccination: Insights, perspectives and challenges. Metabol Open 2022, 14, 100180. [Google Scholar] [CrossRef] [PubMed]
- Dalamaga, M.; Nasiri-Ansari, N.; Spyrou, N. Perspectives and Challenges of COVID-19 with Obesity-Related Cancers. Cancers (Basel) 2023, 15. [Google Scholar] [CrossRef]
- Tsilingiris, D.; Nasiri-Ansari, N.; Spyrou, N.; Magkos, F.; Dalamaga, M. Management of Hematologic Malignancies in the Era of COVID-19 Pandemic: Pathogenetic Mechanisms, Impact of Obesity, Perspectives, and Challenges. Cancers (Basel) 2022, 14. [Google Scholar] [CrossRef]
- Syriga, M.; Karampela, I.; Dalamaga, M.; Karampelas, M. The effect of COVID-19 pandemic on the attendance and clinical outcomes of patients with ophthalmic disease: A mini-review. Metabol Open 2021, 12, 100131. [Google Scholar] [CrossRef]
- Kikkenborg Berg, S.; Palm, P.; Nygaard, U.; Bundgaard, H.; Petersen, M.N.S.; Rosenkilde, S.; Thorsted, A.B.; Ersbøll, A.K.; Thygesen, L.C.; Nielsen, S.D.; et al. Long COVID symptoms in SARS-CoV-2-positive children aged 0-14 years and matched controls in Denmark (LongCOVIDKidsDK): a national, cross-sectional study. Lancet Child Adolesc Health 2022, 6, 614–623. [Google Scholar] [CrossRef]
- Sørensen, A.I.V.; Spiliopoulos, L.; Bager, P.; Nielsen, N.M.; Hansen, J.V.; Koch, A.; Meder, I.K.; Ethelberg, S.; Hviid, A. A nationwide questionnaire study of post-acute symptoms and health problems after SARS-CoV-2 infection in Denmark. Nat Commun 2022, 13, 4213. [Google Scholar] [CrossRef] [PubMed]
- Edlow, A.G.; Castro, V.M.; Shook, L.L.; Kaimal, A.J.; Perlis, R.H. Neurodevelopmental Outcomes at 1 Year in Infants of Mothers Who Tested Positive for SARS-CoV-2 During Pregnancy. JAMA Netw Open 2022, 5, e2215787. [Google Scholar] [CrossRef] [PubMed]
- Vella, L.A.; Rowley, A.H. Current Insights Into the Pathophysiology of Multisystem Inflammatory Syndrome in Children. Curr Pediatr Rep 2021, 9, 83–92. [Google Scholar] [CrossRef] [PubMed]
- Melgar, M.; Lee, E.H.; Miller, A.D.; Lim, S.; Brown, C.M.; Yousaf, A.R.; Zambrano, L.D.; Belay, E.D.; Godfred-Cato, S.; Abrams, J.Y.; et al. Council of State and Territorial Epidemiologists/CDC Surveillance Case Definition for Multisystem Inflammatory Syndrome in Children Associated with SARS-CoV-2 Infection - United States. MMWR Recomm Rep 2022, 71, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Tsampasian, V.; Elghazaly, H.; Chattopadhyay, R.; Debski, M.; Naing, T.K.P.; Garg, P.; Clark, A.; Ntatsaki, E.; Vassiliou, V.S. Risk Factors Associated With Post-COVID-19 Condition: A Systematic Review and Meta-analysis. JAMA Intern Med 2023. [Google Scholar] [CrossRef] [PubMed]
- Asadi-Pooya, A.A.; Akbari, A.; Emami, A.; Lotfi, M.; Rostamihosseinkhani, M.; Nemati, H.; Barzegar, Z.; Kabiri, M.; Zeraatpisheh, Z.; Farjoud-Kouhanjani, M.; et al. Risk Factors Associated with Long COVID Syndrome: A Retrospective Study. Iran J Med Sci 2021, 46, 428–436. [Google Scholar] [CrossRef] [PubMed]
- Subramanian, A.; Nirantharakumar, K.; Hughes, S.; Myles, P.; Williams, T.; Gokhale, K.M.; Taverner, T.; Chandan, J.S.; Brown, K.; Simms-Williams, N.; et al. Symptoms and risk factors for long COVID in non-hospitalized adults. Nat Med 2022, 28, 1706–1714. [Google Scholar] [CrossRef] [PubMed]
- Rao, S.; Lee, G.M.; Razzaghi, H.; Lorman, V.; Mejias, A.; Pajor, N.M.; Thacker, D.; Webb, R.; Dickinson, K.; Bailey, L.C.; et al. Clinical Features and Burden of Postacute Sequelae of SARS-CoV-2 Infection in Children and Adolescents. JAMA Pediatr 2022, 176, 1000–1009. [Google Scholar] [CrossRef]
- Merzon, E.; Weiss, M.; Krone, B.; Cohen, S.; Ilani, G.; Vinker, S.; Cohen-Golan, A.; Green, I.; Israel, A.; Schneider, T.; et al. Clinical and Socio-Demographic Variables Associated with the Diagnosis of Long COVID Syndrome in Youth: A Population-Based Study. Int J Environ Res Public Health 2022, 19. [Google Scholar] [CrossRef]
- Ayoubkhani, D.; Bosworth, M.L.; King, S.; Pouwels, K.B.; Glickman, M.; Nafilyan, V.; Zaccardi, F.; Khunti, K.; Alwan, N.A.; Walker, A.S. Risk of Long COVID in People Infected With Severe Acute Respiratory Syndrome Coronavirus 2 After 2 Doses of a Coronavirus Disease 2019 Vaccine: Community-Based, Matched Cohort Study. Open Forum Infect Dis 2022, 9, ofac464. [Google Scholar] [CrossRef]
- Al-Aly, Z.; Bowe, B.; Xie, Y. Long COVID after breakthrough SARS-CoV-2 infection. Nat Med 2022, 28, 1461–1467. [Google Scholar] [CrossRef] [PubMed]
- Antar, A.A.R.; Yu, T.; Demko, Z.O.; Hu, C.; Tornheim, J.A.; Blair, P.W.; Thomas, D.L.; Manabe, Y.C. Long COVID brain fog and muscle pain are associated with longer time to clearance of SARS-CoV-2 RNA from the upper respiratory tract during acute infection. medRxiv 2023. [Google Scholar] [CrossRef] [PubMed]
- Tsuchida, T.; Hirose, M.; Inoue, Y.; Kunishima, H.; Otsubo, T.; Matsuda, T. Relationship between changes in symptoms and antibody titers after a single vaccination in patients with Long COVID. J Med Virol 2022, 94, 3416–3420. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, N.N.; Nguyen, Y.N.; Hoang, V.T.; Million, M.; Gautret, P. SARS-CoV-2 Reinfection and Severity of the Disease: A Systematic Review and Meta-Analysis. Viruses 2023, 15. [Google Scholar] [CrossRef] [PubMed]
- Bowe, B.; Xie, Y.; Al-Aly, Z. Acute and postacute sequelae associated with SARS-CoV-2 reinfection. Nat Med 2022, 28, 2398–2405. [Google Scholar] [CrossRef]
- Fonseca, A.; Lima, R.; Ladeira, I.; Guimarães, M. Evaluation of pulmonary function in post-COVID-19 patients - when and how should we do it? J Bras Pneumol 2021, 47, e20210065. [Google Scholar] [CrossRef]
- Fortini, A.; Rosso, A.; Cecchini, P.; Torrigiani, A.; Lo Forte, A.; Carrai, P.; Alessi, C.; Fabbrizzi, F.; Lovicu, E.; Sbaragli, S.; et al. One-year evolution of DLCO changes and respiratory symptoms in patients with post COVID-19 respiratory syndrome. Infection 2022, 50, 513–517. [Google Scholar] [CrossRef]
- Kanne, J.P.; Little, B.P.; Schulte, J.J.; Haramati, A.; Haramati, L.B. Long-term Lung Abnormalities Associated with COVID-19 Pneumonia. Radiology 2023, 306, e221806. [Google Scholar] [CrossRef]
- Michelen, M.; Manoharan, L.; Elkheir, N.; Cheng, V.; Dagens, A.; Hastie, C.; O’Hara, M.; Suett, J.; Dahmash, D.; Bugaeva, P.; et al. Characterising long COVID: a living systematic review. BMJ Glob Health 2021, 6. [Google Scholar] [CrossRef]
- Canas, L.S.; Molteni, E.; Deng, J.; Sudre, C.H.; Murray, B.; Kerfoot, E.; Antonelli, M.; Chen, L.; Rjoob, K.; Pujol, J.C.; et al. Profiling post-COVID syndrome across different variants of SARS-CoV-2. 2022. [Google Scholar] [CrossRef]
- Dennis, A.; Cuthbertson, D.J.; Wootton, D.; Crooks, M.; Gabbay, M.; Eichert, N.; Mouchti, S.; Pansini, M.; Roca-Fernandez, A.; Thomaides-Brears, H.; et al. Multi-organ impairment and long COVID: a 1-year prospective, longitudinal cohort study. J R Soc Med 2023, 116, 97–112. [Google Scholar] [CrossRef] [PubMed]
- Fedorowski, A.; Sutton, R. Autonomic dysfunction and postural orthostatic tachycardia syndrome in post-acute COVID-19 syndrome. Nat Rev Cardiol 2023, 20, 281–282. [Google Scholar] [CrossRef] [PubMed]
- Espinosa-Gonzalez, A.B.; Master, H.; Gall, N.; Halpin, S.; Rogers, N.; Greenhalgh, T. Orthostatic tachycardia after covid-19. Bmj 2023, 380, e073488. [Google Scholar] [CrossRef] [PubMed]
- Agashe, S.; Petak, S. Cardiac Autonomic Neuropathy in Diabetes Mellitus. Methodist Debakey Cardiovasc J 2018, 14, 251–256. [Google Scholar] [CrossRef] [PubMed]
- Guo, B.; Zhao, C.; He, M.Z.; Senter, C.; Zhou, Z.; Peng, J.; Li, S.; Fitzpatrick, A.L.; Lindström, S.; Stebbins, R.C.; et al. Long-term cardiac symptoms following COVID-19: a systematic review and meta-analysis. medRxiv 2023. [Google Scholar] [CrossRef]
- Xie, Y.; Xu, E.; Bowe, B.; Al-Aly, Z. Long-term cardiovascular outcomes of COVID-19. Nat Med 2022, 28, 583–590. [Google Scholar] [CrossRef] [PubMed]
- Harding, J.L.; Oviedo, S.A.; Ali, M.K.; Ofotokun, I.; Gander, J.C.; Patel, S.A.; Magliano, D.J.; Patzer, R.E. The bidirectional association between diabetes and long-COVID-19 - A systematic review. Diabetes Res Clin Pract 2023, 195, 110202. [Google Scholar] [CrossRef]
- Nassar, M.; Daoud, A.; Nso, N.; Medina, L.; Ghernautan, V.; Bhangoo, H.; Nyein, A.; Mohamed, M.; Alqassieh, A.; Soliman, K.; et al. Diabetes Mellitus and COVID-19: Review Article. Diabetes Metab Syndr 2021, 15, 102268. [Google Scholar] [CrossRef]
- Karampela, I.; Vallianou, N.; Magkos, F.; Apovian, C.M.; Dalamaga, M. Obesity, Hypovitaminosis D, and COVID-19: the Bermuda Triangle in Public Health. Curr Obes Rep 2022, 11, 116–125. [Google Scholar] [CrossRef]
- Dalamaga, M.; Christodoulatos, G.S.; Karampela, I.; Vallianou, N.; Apovian, C.M. Understanding the Co-Epidemic of Obesity and COVID-19: Current Evidence, Comparison with Previous Epidemics, Mechanisms, and Preventive and Therapeutic Perspectives. Curr Obes Rep 2021, 10, 214–243. [Google Scholar] [CrossRef]
- Vallianou, N.G.; Evangelopoulos, A.; Kounatidis, D.; Stratigou, T.; Christodoulatos, G.S.; Karampela, I.; Dalamaga, M. Diabetes Mellitus and SARS-CoV-2 Infection: Pathophysiologic Mechanisms and Implications in Management. Curr Diabetes Rev 2021, 17, e123120189797. [Google Scholar] [CrossRef] [PubMed]
- Al-Aly, Z. Diabetes after SARS-CoV-2 infection. Lancet Diabetes Endocrinol 2023, 11, 11–13. [Google Scholar] [CrossRef] [PubMed]
- Kendall, E.K.; Olaker, V.R.; Kaelber, D.C.; Xu, R.; Davis, P.B. Association of SARS-CoV-2 Infection With New-Onset Type 1 Diabetes Among Pediatric Patients From 2020 to 2021. JAMA Netw Open 2022, 5, e2233014. [Google Scholar] [CrossRef] [PubMed]
- Tsilingiris, D.; Dalamaga, M.; Liu, J. SARS-CoV-2 adipose tissue infection and hyperglycemia: A further step towards the understanding of severe COVID-19. Metabol Open 2022, 13, 100163. [Google Scholar] [CrossRef] [PubMed]
- Tansey, C.M.; Louie, M.; Loeb, M.; Gold, W.L.; Muller, M.P.; de Jager, J.; Cameron, J.I.; Tomlinson, G.; Mazzulli, T.; Walmsley, S.L.; et al. One-year outcomes and health care utilization in survivors of severe acute respiratory syndrome. Arch Intern Med 2007, 167, 1312–1320. [Google Scholar] [CrossRef] [PubMed]
- Lam, M.H.; Wing, Y.K.; Yu, M.W.; Leung, C.M.; Ma, R.C.; Kong, A.P.; So, W.Y.; Fong, S.Y.; Lam, S.P. Mental morbidities and chronic fatigue in severe acute respiratory syndrome survivors: long-term follow-up. Arch Intern Med 2009, 169, 2142–2147. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.H.; Shin, H.S.; Park, H.Y.; Kim, J.L.; Lee, J.J.; Lee, H.; Won, S.D.; Han, W. Depression as a Mediator of Chronic Fatigue and Post-Traumatic Stress Symptoms in Middle East Respiratory Syndrome Survivors. Psychiatry Investig 2019, 16, 59–64. [Google Scholar] [CrossRef]
- Moldofsky, H.; Patcai, J. Chronic widespread musculoskeletal pain, fatigue, depression and disordered sleep in chronic post-SARS syndrome; a case-controlled study. BMC Neurol 2011, 11, 37. [Google Scholar] [CrossRef]
- Fukuda, K.; Straus, S.E.; Hickie, I.; Sharpe, M.C.; Dobbins, J.G.; Komaroff, A. The chronic fatigue syndrome: a comprehensive approach to its definition and study. International Chronic Fatigue Syndrome Study Group. Ann Intern Med 1994, 121, 953–959. [Google Scholar] [CrossRef]
- CDC. Myalgic encephalomyelitis/chronic fatigue syndrome: Symptoms. Available online: https://www.cdc.gov/me-cfs/symptoms-diagnosis/symptoms.html (accessed on 17 May 2023).
- Magnus, P.; Gunnes, N.; Tveito, K.; Bakken, I.J.; Ghaderi, S.; Stoltenberg, C.; Hornig, M.; Lipkin, W.I.; Trogstad, L.; Håberg, S.E. Chronic fatigue syndrome/myalgic encephalomyelitis (CFS/ME) is associated with pandemic influenza infection, but not with an adjuvanted pandemic influenza vaccine. Vaccine 2015, 33, 6173–6177. [Google Scholar] [CrossRef]
- Wilson, H.W.; Amo-Addae, M.; Kenu, E.; Ilesanmi, O.S.; Ameme, D.K.; Sackey, S.O. Post-Ebola Syndrome among Ebola Virus Disease Survivors in Montserrado County, Liberia 2016. Biomed Res Int 2018, 2018, 1909410. [Google Scholar] [CrossRef]
- Garcia, M.N.; Hause, A.M.; Walker, C.M.; Orange, J.S.; Hasbun, R.; Murray, K.O. Evaluation of prolonged fatigue post-West Nile virus infection and association of fatigue with elevated antiviral and proinflammatory cytokines. Viral Immunol 2014, 27, 327–333. [Google Scholar] [CrossRef]
- Shikova, E.; Reshkova, V.; Kumanova, А.; Raleva, S.; Alexandrova, D.; Capo, N.; Murovska, M. Cytomegalovirus, Epstein-Barr virus, and human herpesvirus-6 infections in patients with myalgic еncephalomyelitis/chronic fatigue syndrome. J Med Virol 2020, 92, 3682–3688. [Google Scholar] [CrossRef]
- Lim, E.J.; Ahn, Y.C.; Jang, E.S.; Lee, S.W.; Lee, S.H.; Son, C.G. Systematic review and meta-analysis of the prevalence of chronic fatigue syndrome/myalgic encephalomyelitis (CFS/ME). J Transl Med 2020, 18, 100. [Google Scholar] [CrossRef]
- Clinical characteristics with inflammation profiling of long COVID and association with 1-year recovery following hospitalisation in the UK: a prospective observational study. Lancet Respir Med 2022, 10, 761–775. [CrossRef]
- Kritas, S.K.; Ronconi, G.; Caraffa, A.; Gallenga, C.E.; Ross, R.; Conti, P. Mast cells contribute to coronavirus-induced inflammation: new anti-inflammatory strategy. J Biol Regul Homeost Agents 2020, 34, 9–14. [Google Scholar] [CrossRef]
- Turner, S.; Khan, M.A.; Putrino, D.; Woodcock, A.; Kell, D.B.; Pretorius, E. Long COVID: pathophysiological factors and abnormalities of coagulation. Trends Endocrinol Metab 2023, 34, 321–344. [Google Scholar] [CrossRef]
- Hu, F.; Chen, F.; Ou, Z.; Fan, Q.; Tan, X.; Wang, Y.; Pan, Y.; Ke, B.; Li, L.; Guan, Y.; et al. A compromised specific humoral immune response against the SARS-CoV-2 receptor-binding domain is related to viral persistence and periodic shedding in the gastrointestinal tract. Cell Mol Immunol 2020, 17, 1119–1125. [Google Scholar] [CrossRef]
- Phetsouphanh, C.; Darley, D.R.; Wilson, D.B.; Howe, A.; Munier, C.M.L.; Patel, S.K.; Juno, J.A.; Burrell, L.M.; Kent, S.J.; Dore, G.J.; et al. Immunological dysfunction persists for 8 months following initial mild-to-moderate SARS-CoV-2 infection. Nat Immunol 2022, 23, 210–216. [Google Scholar] [CrossRef]
- Pinho, J.R.R.; Oliveira, K.G.; Sitnik, R.; Maluf, M.M.; Rodrigues, P.H.S.; Santana, R.A.F.; Welter, E.R.; Irony, O. Long term persistence of coronavirus SARS-CoV-2 infection. Einstein (Sao Paulo) 2021, 19, eRC6369. [Google Scholar] [CrossRef] [PubMed]
- Stein, S.R.; Ramelli, S.C.; Grazioli, A.; Chung, J.Y.; Singh, M.; Yinda, C.K.; Winkler, C.W.; Sun, J.; Dickey, J.M.; Ylaya, K.; et al. SARS-CoV-2 infection and persistence in the human body and brain at autopsy. Nature 2022, 612, 758–763. [Google Scholar] [CrossRef]
- Karn, V.; Ahmed, S.; Tsai, L.W.; Dubey, R.; Ojha, S.; Singh, H.N.; Kumar, M.; Gupta, P.K.; Sadhu, S.; Jha, N.K.; et al. Extracellular Vesicle-Based Therapy for COVID-19: Promises, Challenges and Future Prospects. Biomedicines 2021, 9. [Google Scholar] [CrossRef]
- García-Abellán, J.; Padilla, S.; Fernández-González, M.; García, J.A.; Agulló, V.; Andreo, M.; Ruiz, S.; Galiana, A.; Gutiérrez, F.; Masiá, M. Antibody Response to SARS-CoV-2 is Associated with Long-term Clinical Outcome in Patients with COVID-19: a Longitudinal Study. J Clin Immunol 2021, 41, 1490–1501. [Google Scholar] [CrossRef]
- Spatola, M.; Nziza, N.; Jung, W.; Deng, Y.; Yuan, D.; Dinoto, A.; Bozzetti, S.; Chiodega, V.; Ferrari, S.; Lauffenburger, D.A.; et al. Neurologic sequelae of COVID-19 are determined by immunologic imprinting from previous coronaviruses. Brain 2023. [Google Scholar] [CrossRef]
- Proal, A.D.; VanElzakker, M.B. Long COVID or Post-acute Sequelae of COVID-19 (PASC): An Overview of Biological Factors That May Contribute to Persistent Symptoms. Front Microbiol 2021, 12, 698169. [Google Scholar] [CrossRef]
- Sausen, D.G.; Basith, A.; Muqeemuddin, S. EBV and Lymphomagenesis. Cancers (Basel) 2023, 15. [Google Scholar] [CrossRef]
- Lupo, J.; Truffot, A.; Andreani, J.; Habib, M.; Epaulard, O.; Morand, P.; Germi, R. Virological Markers in Epstein-Barr Virus-Associated Diseases. Viruses 2023, 15. [Google Scholar] [CrossRef]
- Lanz, T.V.; Brewer, R.C.; Ho, P.P.; Moon, J.S.; Jude, K.M.; Fernandez, D.; Fernandes, R.A.; Gomez, A.M.; Nadj, G.S.; Bartley, C.M.; et al. Clonally expanded B cells in multiple sclerosis bind EBV EBNA1 and GlialCAM. Nature 2022, 603, 321–327. [Google Scholar] [CrossRef]
- Du Toit, A. EBV linked to multiple sclerosis. Nat Rev Microbiol 2022, 20, 189. [Google Scholar] [CrossRef]
- Vallianou, N.G.; Tsilingiris, D.; Karampela, I.; Liu, J.; Dalamaga, M. Herpes zoster following COVID-19 vaccination in an immunocompetent and vaccinated for herpes zoster adult: A two-vaccine related event? Metabol Open 2022, 13, 100171. [Google Scholar] [CrossRef] [PubMed]
- Argyrakopoulou, G.; Dalamaga, M.; Spyrou, N.; Kokkinos, A. Gender Differences in Obesity-Related Cancers. Curr Obes Rep 2021, 10, 100–115. [Google Scholar] [CrossRef] [PubMed]
- O’Leary, K. Mounting evidence for EBV links to multiple sclerosis. Nat Med 2022, 28, 2450. [Google Scholar] [CrossRef] [PubMed]
- Nekoua, M.P.; Alidjinou, E.K.; Hober, D. Persistent coxsackievirus B infection and pathogenesis of type 1 diabetes mellitus. Nat Rev Endocrinol 2022, 18, 503–516. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Cao, Z.M.; Zhang, L.L.; Dai, X.C.; Liu, Z.J.; Zeng, Y.X.; Li, X.Y.; Wu, Q.J.; Lv, W.L. Helicobacter Pylori and Autoimmune Diseases: Involving Multiple Systems. Front Immunol 2022, 13, 833424. [Google Scholar] [CrossRef] [PubMed]
- Zangiabadian, M.; Mirsaeidi, M.; Pooyafar, M.H.; Goudarzi, M.; Nasiri, M.J. Associations of Yersinia Enterocolitica Infection with Autoimmune Thyroid Diseases: A Systematic Review and Meta-Analysis. Endocr Metab Immune Disord Drug Targets 2021, 21, 682–687. [Google Scholar] [CrossRef] [PubMed]
- Lake, C.M.; Breen, J.J. Sequence similarity between SARS-CoV-2 nucleocapsid and multiple sclerosis-associated proteins provides insight into viral neuropathogenesis following infection. Sci Rep 2023, 13, 389. [Google Scholar] [CrossRef] [PubMed]
- Tsilingiris, D.; Vallianou, N.G.; Karampela, I.; Dalamaga, M. Vaccine induced thrombotic thrombocytopenia: The shady chapter of a success story. Metabol Open 2021, 11, 100101. [Google Scholar] [CrossRef]
- Brogna, C.; Brogna, B.; Bisaccia, D.R.; Lauritano, F.; Marino, G.; Montano, L.; Cristoni, S.; Prisco, M.; Piscopo, M. Could SARS-CoV-2 Have Bacteriophage Behavior or Induce the Activity of Other Bacteriophages? Vaccines (Basel) 2022, 10. [Google Scholar] [CrossRef]
- Zuo, T.; Zhang, F.; Lui, G.C.Y.; Yeoh, Y.K.; Li, A.Y.L.; Zhan, H.; Wan, Y.; Chung, A.C.K.; Cheung, C.P.; Chen, N.; et al. Alterations in Gut Microbiota of Patients With COVID-19 During Time of Hospitalization. Gastroenterology 2020, 159, 944–955. [Google Scholar] [CrossRef]
- Vallianou, N.; Kounatidis, D.; Christodoulatos, G.S.; Panagopoulos, F.; Karampela, I.; Dalamaga, M. Mycobiome and Cancer: What Is the Evidence? Cancers (Basel) 2021, 13. [Google Scholar] [CrossRef]
- Spyrou, N.; Vallianou, N.; Kadillari, J.; Dalamaga, M. The interplay of obesity, gut microbiome and diet in the immune check point inhibitors therapy era. Semin Cancer Biol 2021, 73, 356–376. [Google Scholar] [CrossRef] [PubMed]
- Vallianou, N.; Dalamaga, M.; Stratigou, T.; Karampela, I.; Tsigalou, C. Do Antibiotics Cause Obesity Through Long-term Alterations in the Gut Microbiome? A Review of Current Evidence. Curr Obes Rep 2021, 10, 244–262. [Google Scholar] [CrossRef] [PubMed]
- Tsigalou, C.; Vallianou, N.; Dalamaga, M. Autoantibody Production in Obesity: Is There Evidence for a Link Between Obesity and Autoimmunity? Curr Obes Rep 2020, 9, 245–254. [Google Scholar] [CrossRef] [PubMed]
- Koliaki, C.; Liatis, S.; Dalamaga, M.; Kokkinos, A. The Implication of Gut Hormones in the Regulation of Energy Homeostasis and Their Role in the Pathophysiology of Obesity. Curr Obes Rep 2020, 9, 255–271. [Google Scholar] [CrossRef] [PubMed]
- Ahamed, J.; Laurence, J. Long COVID endotheliopathy: hypothesized mechanisms and potential therapeutic approaches. J Clin Invest 2022, 132. [Google Scholar] [CrossRef]
- Paniz-Mondolfi, A.; Bryce, C.; Grimes, Z.; Gordon, R.E.; Reidy, J.; Lednicky, J.; Sordillo, E.M.; Fowkes, M. Central nervous system involvement by severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2). J Med Virol 2020, 92, 699–702. [Google Scholar] [CrossRef] [PubMed]
- Fox, S.E.; Li, G.; Akmatbekov, A.; Harbert, J.L.; Lameira, F.S.; Brown, J.Q.; Vander Heide, R.S. Unexpected Features of Cardiac Pathology in COVID-19 Infection. Circulation 2020, 142, 1123–1125. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.; Hu, B.; Hu, C.; Zhu, F.; Liu, X.; Zhang, J.; Wang, B.; Xiang, H.; Cheng, Z.; Xiong, Y.; et al. Clinical Characteristics of 138 Hospitalized Patients With 2019 Novel Coronavirus-Infected Pneumonia in Wuhan, China. Jama 2020, 323, 1061–1069. [Google Scholar] [CrossRef]
- Kassi, E.; Dalamaga, M.; Hroussalas, G.; Kazanis, K.; Merantzi, G.; Zachari, A.; Giamarellos-Bourboulis, E.J.; Dionyssiou-Asteriou, A. Adipocyte factors, high-sensitive C-reactive protein levels and lipoxidative stress products in overweight postmenopausal women with normal and impaired OGTT. Maturitas 2010, 67, 72–77. [Google Scholar] [CrossRef]
- Hroussalas, G.; Kassi, E.; Dalamaga, M.; Delimaris, I.; Zachari, A.; Dionyssiou-Asteriou, A. Leptin, soluble leptin receptor, adiponectin and resistin in relation to OGTT in overweight/obese postmenopausal women. Maturitas 2008, 59, 339–349. [Google Scholar] [CrossRef]
- Tsilingiris, D.; Tzeravini, E.; Koliaki, C.; Dalamaga, M.; Kokkinos, A. The Role of Mitochondrial Adaptation and Metabolic Flexibility in the Pathophysiology of Obesity and Insulin Resistance: an Updated Overview. Curr Obes Rep 2021, 10, 191–213. [Google Scholar] [CrossRef] [PubMed]
- Kassi, E.; Dalamaga, M.; Faviou, E.; Hroussalas, G.; Kazanis, K.; Nounopoulos, C.; Dionyssiou-Asteriou, A. Circulating oxidized LDL levels, current smoking and obesity in postmenopausal women. Atherosclerosis 2009, 205, 279–283. [Google Scholar] [CrossRef] [PubMed]
- Nunes, J.M.; Kruger, A.; Proal, A.; Kell, D.B.; Pretorius, E. The Occurrence of Hyperactivated Platelets and Fibrinaloid Microclots in Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS). Pharmaceuticals (Basel) 2022, 15. [Google Scholar] [CrossRef] [PubMed]
- Xiang, M.; Wu, X.; Jing, H.; Novakovic, V.A.; Shi, J. The intersection of obesity and (long) COVID-19: Hypoxia, thrombotic inflammation, and vascular endothelial injury. Front Cardiovasc Med 2023, 10, 1062491. [Google Scholar] [CrossRef] [PubMed]
- Kell, D.B.; Laubscher, G.J.; Pretorius, E. A central role for amyloid fibrin microclots in long COVID/PASC: origins and therapeutic implications. Biochem J 2022, 479, 537–559. [Google Scholar] [CrossRef] [PubMed]
- Bansal, R.; Gubbi, S.; Koch, C.A. COVID-19 and chronic fatigue syndrome: An endocrine perspective. J Clin Transl Endocrinol 2022, 27, 100284. [Google Scholar] [CrossRef] [PubMed]
- Wheatland, R. Molecular mimicry of ACTH in SARS - implications for corticosteroid treatment and prophylaxis. Med Hypotheses 2004, 63, 855–862. [Google Scholar] [CrossRef] [PubMed]
- Al-Hakeim, H.K.; Al-Rubaye, H.T.; Jubran, A.S.; Almulla, A.F.; Moustafa, S.R.; Maes, M. Increased insulin resistance due to Long COVID is associated with depressive symptoms and partly predicted by the inflammatory response during acute infection. Braz J Psychiatry 2023. [Google Scholar] [CrossRef]
- Dodd, S.; Sominsky, L.; Siskind, D.; Bortolasci, C.C.; Carvalho, A.F.; Maes, M.; Walker, A.J.; Walder, K.; Yung, A.R.; Williams, L.J.; et al. The role of metformin as a treatment for neuropsychiatric illness. Eur Neuropsychopharmacol 2022, 64, 32–43. [Google Scholar] [CrossRef]
- Scherer, P.E.; Kirwan, J.P.; Rosen, C.J. Post-acute sequelae of COVID-19: A metabolic perspective. Elife 2022, 11. [Google Scholar] [CrossRef]
- Tan, D.X.; Reiter, R.J. Mechanisms and clinical evidence to support melatonin’s use in severe COVID-19 patients to lower mortality. Life Sci 2022, 294, 120368. [Google Scholar] [CrossRef] [PubMed]
- Cardinali, D.P.; Brown, G.M.; Pandi-Perumal, S.R. Possible Application of Melatonin in Long COVID. Biomolecules 2022, 12. [Google Scholar] [CrossRef] [PubMed]
- Etter, M.M.; Martins, T.A.; Kulsvehagen, L.; Pössnecker, E.; Duchemin, W.; Hogan, S.; Sanabria-Diaz, G.; Müller, J.; Chiappini, A.; Rychen, J.; et al. Severe Neuro-COVID is associated with peripheral immune signatures, autoimmunity and neurodegeneration: a prospective cross-sectional study. Nat Commun 2022, 13, 6777. [Google Scholar] [CrossRef] [PubMed]
- Spudich, S.; Nath, A. Nervous system consequences of COVID-19. Science 2022, 375, 267–269. [Google Scholar] [CrossRef] [PubMed]
- Leng, A.; Shah, M.; Ahmad, S.A.; Premraj, L.; Wildi, K.; Li Bassi, G.; Pardo, C.A.; Choi, A.; Cho, S.M. Pathogenesis Underlying Neurological Manifestations of Long COVID Syndrome and Potential Therapeutics. Cells 2023, 12. [Google Scholar] [CrossRef] [PubMed]
- Raj, S.R.; Bourne, K.M.; Stiles, L.E.; Miglis, M.G.; Cortez, M.M.; Miller, A.J.; Freeman, R.; Biaggioni, I.; Rowe, P.C.; Sheldon, R.S.; et al. Postural orthostatic tachycardia syndrome (POTS): Priorities for POTS care and research from a 2019 National Institutes of Health Expert Consensus Meeting - Part 2. Auton Neurosci 2021, 235, 102836. [Google Scholar] [CrossRef] [PubMed]
- Díaz-Resendiz, K.J.G.; Benitez-Trinidad, A.B.; Covantes-Rosales, C.E.; Toledo-Ibarra, G.A.; Ortiz-Lazareno, P.C.; Girón-Pérez, D.A.; Bueno-Durán, A.Y.; Pérez-Díaz, D.A.; Barcelos-García, R.G.; Girón-Pérez, M.I. Loss of mitochondrial membrane potential (ΔΨ(m) ) in leucocytes as post-COVID-19 sequelae. J Leukoc Biol 2022, 112, 23–29. [Google Scholar] [CrossRef]
- Guntur, V.P.; Nemkov, T.; de Boer, E.; Mohning, M.P.; Baraghoshi, D.; Cendali, F.I.; San-Millán, I.; Petrache, I.; D’Alessandro, A. Signatures of Mitochondrial Dysfunction and Impaired Fatty Acid Metabolism in Plasma of Patients with Post-Acute Sequelae of COVID-19 (PASC). Metabolites 2022, 12. [Google Scholar] [CrossRef]
- Terpos, E.; Ntanasis-Stathopoulos, I.; Elalamy, I.; Kastritis, E.; Sergentanis, T.N.; Politou, M.; Psaltopoulou, T.; Gerotziafas, G.; Dimopoulos, M.A. Hematological findings and complications of COVID-19. Am J Hematol 2020, 95, 834–847. [Google Scholar] [CrossRef]
- Chen, G.; Wu, D.; Guo, W.; Cao, Y.; Huang, D.; Wang, H.; Wang, T.; Zhang, X.; Chen, H.; Yu, H.; et al. Clinical and immunological features of severe and moderate coronavirus disease 2019. J Clin Invest 2020, 130, 2620–2629. [Google Scholar] [CrossRef]
- Kotecha, T.; Knight, D.S.; Razvi, Y.; Kumar, K.; Vimalesvaran, K.; Thornton, G.; Patel, R.; Chacko, L.; Brown, J.T.; Coyle, C.; et al. Patterns of myocardial injury in recovered troponin-positive COVID-19 patients assessed by cardiovascular magnetic resonance. Eur Heart J 2021, 42, 1866–1878. [Google Scholar] [CrossRef]
- Helms, J.; Tacquard, C.; Severac, F.; Leonard-Lorant, I.; Ohana, M.; Delabranche, X.; Merdji, H.; Clere-Jehl, R.; Schenck, M.; Fagot Gandet, F.; et al. High risk of thrombosis in patients with severe SARS-CoV-2 infection: a multicenter prospective cohort study. Intensive Care Med 2020, 46, 1089–1098. [Google Scholar] [CrossRef] [PubMed]
- Karampela, I.; Christodoulatos, G.S.; Vallianou, N.; Tsilingiris, D.; Chrysanthopoulou, E.; Skyllas, G.; Antonakos, G.; Marinou, I.; Vogiatzakis, E.; Armaganidis, A.; et al. Circulating Chemerin and Its Kinetics May Be a Useful Diagnostic and Prognostic Biomarker in Critically Ill Patients with Sepsis: A Prospective Study. Biomolecules 2022, 12. [Google Scholar] [CrossRef] [PubMed]
- Karampela, I.; Christodoulatos, G.S.; Dalamaga, M. The Role of Adipose Tissue and Adipokines in Sepsis: Inflammatory and Metabolic Considerations, and the Obesity Paradox. Curr Obes Rep 2019, 8, 434–457. [Google Scholar] [CrossRef] [PubMed]
- Dalamaga, M.; Karmaniolas, K.; Nikolaidou, A.; Papadavid, E. Hypocalcemia, hypomagnesemia, and hypokalemia following hydrofluoric acid chemical injury. J Burn Care Res 2008, 29, 541–543. [Google Scholar] [CrossRef] [PubMed]
- Karampela, I.; Kandri, E.; Antonakos, G.; Vogiatzakis, E.; Christodoulatos, G.S.; Nikolaidou, A.; Dimopoulos, G.; Armaganidis, A.; Dalamaga, M. Kinetics of circulating fetuin-A may predict mortality independently from adiponectin, high molecular weight adiponectin and prognostic factors in critically ill patients with sepsis: A prospective study. J Crit Care 2017, 41, 78–85. [Google Scholar] [CrossRef] [PubMed]
- Shaw, B.H.; Stiles, L.E.; Bourne, K.; Green, E.A.; Shibao, C.A.; Okamoto, L.E.; Garland, E.M.; Gamboa, A.; Diedrich, A.; Raj, V.; et al. The face of postural tachycardia syndrome - insights from a large cross-sectional online community-based survey. J Intern Med 2019, 286, 438–448. [Google Scholar] [CrossRef]
- Roca-Fernandez, A.; Wamil, M.; Telford, A.; Carapella, V.; Borlotti, A.; Monteiro, D.; Thomaides-Brears, H.; Kelly, M.; Dennis, A.; Banerjee, R.; et al. Cardiac abnormalities in Long COVID 1-year post-SARS-CoV-2 infection. Open Heart 2023, 10. [Google Scholar] [CrossRef]
- Hughes, S.E.; Haroon, S.; Subramanian, A.; McMullan, C.; Aiyegbusi, O.L.; Turner, G.M.; Jackson, L.; Davies, E.H.; Frost, C.; McNamara, G.; et al. Development and validation of the symptom burden questionnaire for long covid (SBQ-LC): Rasch analysis. Bmj 2022, 377, e070230. [Google Scholar] [CrossRef]
- Jamal, S.M.; Landers, D.B.; Hollenberg, S.M.; Turi, Z.G.; Glotzer, T.V.; Tancredi, J.; Parrillo, J.E. Prospective Evaluation of Autonomic Dysfunction in Post-Acute Sequela of COVID-19. J Am Coll Cardiol 2022, 79, 2325–2330. [Google Scholar] [CrossRef]
- Stavileci, B.; Özdemir, E.; Özdemir, B.; Ereren, E.; Cengiz, M. De-novo development of fragmented QRS during a six-month follow-up period in patients with COVID-19 disease and its cardiac effects. J Electrocardiol 2022, 72, 44–48. [Google Scholar] [CrossRef] [PubMed]
- Grist, J.T.; Collier, G.J.; Walters, H.; Kim, M.; Chen, M.; Abu Eid, G.; Laws, A.; Matthews, V.; Jacob, K.; Cross, S.; et al. Lung Abnormalities Detected with Hyperpolarized (129)Xe MRI in Patients with Long COVID. Radiology 2022, 305, 709–717. [Google Scholar] [CrossRef] [PubMed]
- Bateman, L.; Bested, A.C.; Bonilla, H.F.; Chheda, B.V.; Chu, L.; Curtin, J.M.; Dempsey, T.T.; Dimmock, M.E.; Dowell, T.G.; Felsenstein, D.; et al. Myalgic Encephalomyelitis/Chronic Fatigue Syndrome: Essentials of Diagnosis and Management. Mayo Clin Proc 2021, 96, 2861–2878. [Google Scholar] [CrossRef] [PubMed]
- Yong, S.J.; Halim, A.; Halim, M.; Liu, S.; Aljeldah, M.; Al Shammari, B.R.; Alwarthan, S.; Alhajri, M.; Alawfi, A.; Alshengeti, A.; et al. Inflammatory and vascular biomarkers in post-COVID-19 syndrome: A systematic review and meta-analysis of over 20 biomarkers. Rev Med Virol 2023, 33, e2424. [Google Scholar] [CrossRef] [PubMed]
- Yin, J.X.; Agbana, Y.L.; Sun, Z.S.; Fei, S.W.; Zhao, H.Q.; Zhou, X.N.; Chen, J.H.; Kassegne, K. Increased interleukin-6 is associated with long COVID-19: a systematic review and meta-analysis. Infect Dis Poverty 2023, 12, 43. [Google Scholar] [CrossRef] [PubMed]
- Klein, J.; Wood, J.; Jaycox, J.; Lu, P.; Dhodapkar, R.M.; Gehlhausen, J.R.; Tabachnikova, A.; Tabacof, L.; Malik, A.A.; Kamath, K.; et al. Distinguishing features of Long COVID identified through immune profiling. medRxiv 2022. [Google Scholar] [CrossRef]
- Haunhorst, S.; Bloch, W.; Javelle, F.; Krüger, K.; Baumgart, S.; Drube, S.; Lemhöfer, C.; Reuken, P.; Stallmach, A.; Müller, M.; et al. A scoping review of regulatory T cell dynamics in convalescent COVID-19 patients - indications for their potential involvement in the development of Long COVID? Front Immunol 2022, 13, 1070994. [Google Scholar] [CrossRef]
- Galán, M.; Vigón, L.; Fuertes, D.; Murciano-Antón, M.A.; Casado-Fernández, G.; Domínguez-Mateos, S.; Mateos, E.; Ramos-Martín, F.; Planelles, V.; Torres, M.; et al. Persistent Overactive Cytotoxic Immune Response in a Spanish Cohort of Individuals With Long-COVID: Identification of Diagnostic Biomarkers. Front Immunol 2022, 13, 848886. [Google Scholar] [CrossRef]
- Utrero-Rico, A.; Ruiz-Ruigómez, M.; Laguna-Goya, R.; Arrieta-Ortubay, E.; Chivite-Lacaba, M.; González-Cuadrado, C.; Lalueza, A.; Almendro-Vazquez, P.; Serrano, A.; Aguado, J.M.; et al. A Short Corticosteroid Course Reduces Symptoms and Immunological Alterations Underlying Long-COVID. Biomedicines 2021, 9. [Google Scholar] [CrossRef]
- Patterson, B.K.; Guevara-Coto, J.; Yogendra, R.; Francisco, E.B.; Long, E.; Pise, A.; Rodrigues, H.; Parikh, P.; Mora, J.; Mora-Rodríguez, R.A. Immune-Based Prediction of COVID-19 Severity and Chronicity Decoded Using Machine Learning. Front Immunol 2021, 12, 700782. [Google Scholar] [CrossRef]
- Swank, Z.; Senussi, Y.; Manickas-Hill, Z.; Yu, X.G.; Li, J.Z.; Alter, G.; Walt, D.R. Persistent Circulating Severe Acute Respiratory Syndrome Coronavirus 2 Spike Is Associated With Post-acute Coronavirus Disease 2019 Sequelae. Clin Infect Dis 2023, 76, e487–e490. [Google Scholar] [CrossRef] [PubMed]
- Natarajan, A.; Zlitni, S.; Brooks, E.F.; Vance, S.E.; Dahlen, A.; Hedlin, H.; Park, R.M.; Han, A.; Schmidtke, D.T.; Verma, R.; et al. Gastrointestinal symptoms and fecal shedding of SARS-CoV-2 RNA suggest prolonged gastrointestinal infection. Med 2022, 3, 371–387. [Google Scholar] [CrossRef] [PubMed]
- Tejerina, F.; Catalan, P.; Rodriguez-Grande, C.; Adan, J.; Rodriguez-Gonzalez, C.; Muñoz, P.; Aldamiz, T.; Diez, C.; Perez, L.; Fanciulli, C.; et al. Post-COVID-19 syndrome. SARS-CoV-2 RNA detection in plasma, stool, and urine in patients with persistent symptoms after COVID-19. BMC Infect Dis 2022, 22, 211. [Google Scholar] [CrossRef] [PubMed]
- Zollner, A.; Koch, R.; Jukic, A.; Pfister, A.; Meyer, M.; Rössler, A.; Kimpel, J.; Adolph, T.E.; Tilg, H. Postacute COVID-19 is Characterized by Gut Viral Antigen Persistence in Inflammatory Bowel Diseases. Gastroenterology 2022, 163, 495–506. [Google Scholar] [CrossRef] [PubMed]
- Yonker, L.M.; Gilboa, T.; Ogata, A.F.; Senussi, Y.; Lazarovits, R.; Boribong, B.P.; Bartsch, Y.C.; Loiselle, M.; Rivas, M.N.; Porritt, R.A.; et al. Multisystem inflammatory syndrome in children is driven by zonulin-dependent loss of gut mucosal barrier. J Clin Invest 2021, 131. [Google Scholar] [CrossRef]
- Files, J.K.; Sarkar, S.; Fram, T.R.; Boppana, S.; Sterrett, S.; Qin, K.; Bansal, A.; Long, D.M.; Sabbaj, S.; Kobie, J.J.; et al. Duration of post-COVID-19 symptoms is associated with sustained SARS-CoV-2-specific immune responses. JCI Insight 2021, 6. [Google Scholar] [CrossRef]
- Augustin, M.; Schommers, P.; Stecher, M.; Dewald, F.; Gieselmann, L.; Gruell, H.; Horn, C.; Vanshylla, K.; Cristanziano, V.D.; Osebold, L.; et al. Post-COVID syndrome in non-hospitalised patients with COVID-19: a longitudinal prospective cohort study. Lancet Reg Health Eur 2021, 6, 100122. [Google Scholar] [CrossRef]
- Blomberg, B.; Mohn, K.G.; Brokstad, K.A.; Zhou, F.; Linchausen, D.W.; Hansen, B.A.; Lartey, S.; Onyango, T.B.; Kuwelker, K.; Sævik, M.; et al. Long COVID in a prospective cohort of home-isolated patients. Nat Med 2021, 27, 1607–1613. [Google Scholar] [CrossRef]
- Peluso, M.J.; Deitchman, A.N.; Torres, L.; Iyer, N.S.; Munter, S.E.; Nixon, C.C.; Donatelli, J.; Thanh, C.; Takahashi, S.; Hakim, J.; et al. Long-term SARS-CoV-2-specific immune and inflammatory responses in individuals recovering from COVID-19 with and without post-acute symptoms. Cell Rep 2021, 36, 109518. [Google Scholar] [CrossRef]
- Peluso, M.J.; Deveau, T.M.; Munter, S.E.; Ryder, D.; Buck, A.; Beck-Engeser, G.; Chan, F.; Lu, S.; Goldberg, S.A.; Hoh, R.; et al. Chronic viral coinfections differentially affect the likelihood of developing long COVID. J Clin Invest 2023, 133. [Google Scholar] [CrossRef]
- Zubchenko, S.; Kril, I.; Nadizhko, O.; Matsyura, O.; Chopyak, V. Herpesvirus infections and post-COVID-19 manifestations: a pilot observational study. Rheumatol Int 2022, 42, 1523–1530. [Google Scholar] [CrossRef] [PubMed]
- Su, Y.; Yuan, D.; Chen, D.G.; Ng, R.H.; Wang, K.; Choi, J.; Li, S.; Hong, S.; Zhang, R.; Xie, J.; et al. Multiple early factors anticipate post-acute COVID-19 sequelae. Cell 2022, 185, 881–895. [Google Scholar] [CrossRef] [PubMed]
- Gold, J.E.; Okyay, R.A.; Licht, W.E.; Hurley, D.J. Investigation of Long COVID Prevalence and Its Relationship to Epstein-Barr Virus Reactivation. Pathogens 2021, 10. [Google Scholar] [CrossRef] [PubMed]
- Muri, J.; Cecchinato, V.; Cavalli, A.; Shanbhag, A.A.; Matkovic, M.; Biggiogero, M.; Maida, P.A.; Moritz, J.; Toscano, C.; Ghovehoud, E.; et al. Autoantibodies against chemokines post-SARS-CoV-2 infection correlate with disease course. Nat Immunol 2023, 24, 604–611. [Google Scholar] [CrossRef] [PubMed]
- Bodansky, A.; Wang, C.Y.; Saxena, A.; Mitchell, A.; Takahashi, S.; Anglin, K.; Huang, B.; Hoh, R.; Lu, S.; Goldberg, S.A.; et al. Autoantigen profiling reveals a shared post-COVID signature in fully recovered and Long COVID patients. medRxiv 2023. [Google Scholar] [CrossRef] [PubMed]
- Son, K.; Jamil, R.; Chowdhury, A.; Mukherjee, M.; Venegas, C.; Miyasaki, K.; Zhang, K.; Patel, Z.; Salter, B.; Yuen, A.C.Y.; et al. Circulating anti-nuclear autoantibodies in COVID-19 survivors predict long COVID symptoms. Eur Respir J 2023, 61. [Google Scholar] [CrossRef] [PubMed]
- Franke, C.; Boesl, F.; Goereci, Y.; Gerhard, A.; Schweitzer, F.; Schroeder, M.; Foverskov-Rasmussen, H.; Heine, J.; Quitschau, A.; Kandil, F.I.; et al. Association of cerebrospinal fluid brain-binding autoantibodies with cognitive impairment in post-COVID-19 syndrome. Brain Behav Immun 2023, 109, 139–143. [Google Scholar] [CrossRef]
- Peluso, M.J.; Mitchell, A.; Wang, C.Y.; Takahashi, S.; Hoh, R.; Tai, V.; Durstenfeld, M.S.; Hsue, P.Y.; Kelly, J.D.; Martin, J.N.; et al. Low Prevalence of Interferon α Autoantibodies in People Experiencing Symptoms of Post-Coronavirus Disease 2019 (COVID-19) Conditions, or Long COVID. J Infect Dis 2023, 227, 246–250. [Google Scholar] [CrossRef]
- Rojas, M.; Rodríguez, Y.; Acosta-Ampudia, Y.; Monsalve, D.M.; Zhu, C.; Li, Q.Z.; Ramírez-Santana, C.; Anaya, J.M. Autoimmunity is a hallmark of post-COVID syndrome. J Transl Med 2022, 20, 129. [Google Scholar] [CrossRef]
- Patel, M.A.; Knauer, M.J.; Nicholson, M.; Daley, M.; Van Nynatten, L.R.; Martin, C.; Patterson, E.K.; Cepinskas, G.; Seney, S.L.; Dobretzberger, V.; et al. Elevated vascular transformation blood biomarkers in Long-COVID indicate angiogenesis as a key pathophysiological mechanism. Mol Med 2022, 28, 122. [Google Scholar] [CrossRef]
- Haffke, M.; Freitag, H.; Rudolf, G.; Seifert, M.; Doehner, W.; Scherbakov, N.; Hanitsch, L.; Wittke, K.; Bauer, S.; Konietschke, F.; et al. Endothelial dysfunction and altered endothelial biomarkers in patients with post-COVID-19 syndrome and chronic fatigue syndrome (ME/CFS). J Transl Med 2022, 20, 138. [Google Scholar] [CrossRef]
- Tong, M.; Yan, X.; Jiang, Y.; Jin, Z.; Zhu, S.; Zou, L.; Liu, Y.; Zheng, Q.; Chen, G.; Gu, R.; et al. Endothelial Biomarkers in Patients Recovered from COVID-19 One Year after Hospital Discharge: A Cross-Sectional Study. Mediterr J Hematol Infect Dis 2022, 14, e2022033. [Google Scholar] [CrossRef] [PubMed]
- Constantinescu-Bercu, A.; Kessler, A.; de Groot, R.; Dragunaite, B.; Heightman, M.; Hillman, T.; Price, L.C.; Brennan, E.; Sivera, R.; Vanhoorelbeke, K.; et al. Analysis of thrombogenicity under flow reveals new insights into the prothrombotic state of patients with post-COVID syndrome. J Thromb Haemost 2023, 21, 94–100. [Google Scholar] [CrossRef] [PubMed]
- Di Gennaro, L.; Valentini, P.; Sorrentino, S.; Ferretti, M.A.; De Candia, E.; Basso, M.; Lancellotti, S.; De Cristofaro, R.; De Rose, C.; Mariani, F.; et al. Extended coagulation profile of children with Long Covid: a prospective study. Sci Rep 2022, 12, 18392. [Google Scholar] [CrossRef] [PubMed]
- Kruger, A.; Vlok, M.; Turner, S.; Venter, C.; Laubscher, G.J.; Kell, D.B.; Pretorius, E. Proteomics of fibrin amyloid microclots in long COVID/post-acute sequelae of COVID-19 (PASC) shows many entrapped pro-inflammatory molecules that may also contribute to a failed fibrinolytic system. Cardiovasc Diabetol 2022, 21, 190. [Google Scholar] [CrossRef] [PubMed]
- Pretorius, E.; Vlok, M.; Venter, C.; Bezuidenhout, J.A.; Laubscher, G.J.; Steenkamp, J.; Kell, D.B. Persistent clotting protein pathology in Long COVID/Post-Acute Sequelae of COVID-19 (PASC) is accompanied by increased levels of antiplasmin. Cardiovasc Diabetol 2021, 20, 172. [Google Scholar] [CrossRef] [PubMed]
- Sunada, N.; Honda, H.; Nakano, Y.; Yamamoto, K.; Tokumasu, K.; Sakurada, Y.; Matsuda, Y.; Hasegawa, T.; Otsuka, Y.; Obika, M.; et al. Hormonal trends in patients suffering from long COVID symptoms. Endocr J 2022, 69, 1173–1181. [Google Scholar] [CrossRef] [PubMed]
- Captur, G.; Moon, J.C.; Topriceanu, C.C.; Joy, G.; Swadling, L.; Hallqvist, J.; Doykov, I.; Patel, N.; Spiewak, J.; Baldwin, T.; et al. Plasma proteomic signature predicts who will get persistent symptoms following SARS-CoV-2 infection. EBioMedicine 2022, 85, 104293. [Google Scholar] [CrossRef]
- López-Hernández, Y.; Oropeza-Valdez, J.J.; García Lopez, D.A.; Borrego, J.C.; Murgu, M.; Valdez, J.; López, J.A.; Monárrez-Espino, J. Untargeted analysis in post-COVID-19 patients reveals dysregulated lipid pathways two years after recovery. Front Mol Biosci 2023, 10, 1100486. [Google Scholar] [CrossRef]
- López-Hernández, Y.; Aquino, J.M.; López, D.A.G.; Zheng, J.; Borrego, J.C.; Torres-Calzada, C.; Elizalde-Díaz, J.P.; Mandal, R.; Berjanskii, M.; Martínez-Martínez, E.; et al. The plasma metabolome of long COVID-19 patients two years after infection. 2023. [Google Scholar] [CrossRef]
- Cysique, L.A.; Jakabek, D.; Bracken, S.G.; Allen-Davidian, Y.; Heng, B.; Chow, S.; Dehhaghi, M.; Pires, A.S.; Darley, D.R.; Byrne, A.; et al. Post-acute COVID-19 cognitive impairment and decline uniquely associate with kynurenine pathway activation: a longitudinal observational study. 2022. [Google Scholar] [CrossRef]
- Zhang, D.; Zhou, Y.; Ma, Y.; Chen, P.; Tang, J.; Yang, B.; Li, H.; Liang, M.; Xue, Y.; Liu, Y.; et al. Gut Microbiota Dysbiosis Correlates With Long COVID-19 at One-Year After Discharge. J Korean Med Sci 2023, 38, e120. [Google Scholar] [CrossRef] [PubMed]
- Liu, Q.; Mak, J.W.Y.; Su, Q.; Yeoh, Y.K.; Lui, G.C.; Ng, S.S.S.; Zhang, F.; Li, A.Y.L.; Lu, W.; Hui, D.S.; et al. Gut microbiota dynamics in a prospective cohort of patients with post-acute COVID-19 syndrome. Gut 2022, 71, 544–552. [Google Scholar] [CrossRef] [PubMed]
- Apple, A.C.; Oddi, A.; Peluso, M.J.; Asken, B.M.; Henrich, T.J.; Kelly, J.D.; Pleasure, S.J.; Deeks, S.G.; Allen, I.E.; Martin, J.N.; et al. Risk factors and abnormal cerebrospinal fluid associate with cognitive symptoms after mild COVID-19. Ann Clin Transl Neurol 2022, 9, 221–226. [Google Scholar] [CrossRef] [PubMed]
- Guasp, M.; Muñoz-Sánchez, G.; Martínez-Hernández, E.; Santana, D.; Carbayo, Á.; Naranjo, L.; Bolós, U.; Framil, M.; Saiz, A.; Balasa, M.; et al. CSF Biomarkers in COVID-19 Associated Encephalopathy and Encephalitis Predict Long-Term Outcome. Front Immunol 2022, 13, 866153. [Google Scholar] [CrossRef] [PubMed]
- Bonnet, B.; Cosme, J.; Dupuis, C.; Coupez, E.; Adda, M.; Calvet, L.; Fabre, L.; Saint-Sardos, P.; Bereiziat, M.; Vidal, M.; et al. Severe COVID-19 is characterized by the co-occurrence of moderate cytokine inflammation and severe monocyte dysregulation. EBioMedicine 2021, 73, 103622. [Google Scholar] [CrossRef] [PubMed]
- Montazersaheb, S.; Hosseiniyan Khatibi, S.M.; Hejazi, M.S.; Tarhriz, V.; Farjami, A.; Ghasemian Sorbeni, F.; Farahzadi, R.; Ghasemnejad, T. COVID-19 infection: an overview on cytokine storm and related interventions. Virol J 2022, 19, 92. [Google Scholar] [CrossRef] [PubMed]
- Low, R.N.; Low, R.J.; Akrami, A. A review of cytokine-based pathophysiology of Long COVID symptoms. Front Med (Lausanne) 2023, 10, 1011936. [Google Scholar] [CrossRef]
- Peluso, M.J.; Lu, S.; Tang, A.F.; Durstenfeld, M.S.; Ho, H.E.; Goldberg, S.A.; Forman, C.A.; Munter, S.E.; Hoh, R.; Tai, V.; et al. Markers of Immune Activation and Inflammation in Individuals With Postacute Sequelae of Severe Acute Respiratory Syndrome Coronavirus 2 Infection. J Infect Dis 2021, 224, 1839–1848. [Google Scholar] [CrossRef]
- Littlefield, K.M.; Watson, R.O.; Schneider, J.M.; Neff, C.P.; Yamada, E.; Zhang, M.; Campbell, T.B.; Falta, M.T.; Jolley, S.E.; Fontenot, A.P.; et al. SARS-CoV-2-specific T cells associate with inflammation and reduced lung function in pulmonary post-acute sequalae of SARS-CoV-2. PLoS Pathog 2022, 18, e1010359. [Google Scholar] [CrossRef]
- Cortellini, A.; Gennari, A.; Pommeret, F.; Patel, G.; Newsom-Davis, T.; Bertuzzi, A.; Viladot, M.; Aguilar-Company, J.; Mirallas, O.; Felip, E.; et al. COVID-19 Sequelae and the Host Proinflammatory Response: An Analysis From the OnCovid Registry. J Natl Cancer Inst 2022, 114, 979–987. [Google Scholar] [CrossRef] [PubMed]
- Hu, S.J.; Weng, Z.C. [Influence of stimulation of the skin receptive field on evoked discharges of the polymodal nociceptors in rats]. Sheng Li Xue Bao 1988, 40, 437–443. [Google Scholar] [PubMed]
- Queiroz, M.A.F.; Neves, P.; Lima, S.S.; Lopes, J.D.C.; Torres, M.; Vallinoto, I.; Bichara, C.D.A.; Dos Santos, E.F.; de Brito, M.; da Silva, A.L.S.; et al. Cytokine Profiles Associated With Acute COVID-19 and Long COVID-19 Syndrome. Front Cell Infect Microbiol 2022, 12, 922422. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Castañeda, A.; Lu, P.; Geraghty, A.C.; Song, E.; Lee, M.H.; Wood, J.; Yalçın, B.; Taylor, K.R.; Dutton, S.; Acosta-Alvarez, L.; et al. Mild respiratory SARS-CoV-2 infection can cause multi-lineage cellular dysregulation and myelin loss in the brain. bioRxiv 2022. [Google Scholar] [CrossRef]
- Venkataramani, V.; Winkler, F. Cognitive Deficits in Long Covid-19. N Engl J Med 2022, 387, 1813–1815. [Google Scholar] [CrossRef] [PubMed]
- da Silva, R.; de Sarges, K.M.L.; Cantanhede, M.H.D.; da Costa, F.P.; Dos Santos, E.F.; Rodrigues, F.B.B.; de Nazaré do Socorro de Almeida Viana, M.; de Meira Leite, M.; da Silva, A.L.S.; de Brito, M.T.M.; et al. Thrombophilia and Immune-Related Genetic Markers in Long COVID. Viruses 2023, 15. [Google Scholar] [CrossRef] [PubMed]
- Hornig, M.; Montoya, J.G.; Klimas, N.G.; Levine, S.; Felsenstein, D.; Bateman, L.; Peterson, D.L.; Gottschalk, C.G.; Schultz, A.F.; Che, X.; et al. Distinct plasma immune signatures in ME/CFS are present early in the course of illness. Sci Adv 2015, 1. [Google Scholar] [CrossRef] [PubMed]
- Glynne, P.; Tahmasebi, N.; Gant, V.; Gupta, R. Long COVID following mild SARS-CoV-2 infection: characteristic T cell alterations and response to antihistamines. J Investig Med 2022, 70, 61–67. [Google Scholar] [CrossRef]
- Cheung, C.C.L.; Goh, D.; Lim, X.; Tien, T.Z.; Lim, J.C.T.; Lee, J.N.; Tan, B.; Tay, Z.E.A.; Wan, W.Y.; Chen, E.X.; et al. Residual SARS-CoV-2 viral antigens detected in GI and hepatic tissues from five recovered patients with COVID-19. Gut 2022, 71, 226–229. [Google Scholar] [CrossRef]
- Gaebler, C.; Wang, Z.; Lorenzi, J.C.C.; Muecksch, F.; Finkin, S.; Tokuyama, M.; Cho, A.; Jankovic, M.; Schaefer-Babajew, D.; Oliveira, T.Y.; et al. Evolution of antibody immunity to SARS-CoV-2. Nature 2021, 591, 639–644. [Google Scholar] [CrossRef]
- Sigal, G.B.; Novak, T.; Mathew, A.; Chou, J.; Zhang, Y.; Manjula, N.; Bathala, P.; Joe, J.; Padmanabhan, N.; Romero, D.; et al. Measurement of Severe Acute Respiratory Syndrome Coronavirus 2 Antigens in Plasma of Pediatric Patients With Acute Coronavirus Disease 2019 or Multisystem Inflammatory Syndrome in Children Using an Ultrasensitive and Quantitative Immunoassay. Clin Infect Dis 2022, 75, 1351–1358. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.; Zhao, H.; Espín, E.; Tebbutt, S.J. Association of SARS-CoV-2 infection and persistence with long COVID. Lancet Respir Med 2023. [Google Scholar] [CrossRef] [PubMed]
- Barouch, D.H. Covid-19 Vaccines - Immunity, Variants, Boosters. N Engl J Med 2022, 387, 1011–1020. [Google Scholar] [CrossRef] [PubMed]
- Banko, A.; Miljanovic, D.; Cirkovic, A. Systematic review with meta-analysis of active herpesvirus infections in patients with COVID-19: Old players on the new field. Int J Infect Dis 2023, 130, 108–125. [Google Scholar] [CrossRef] [PubMed]
- Manoharan, S.; Ying, L.Y. Epstein Barr Virus Reactivation during COVID-19 Hospitalization Significantly Increased Mortality/Death in SARS-CoV-2(+)/EBV(+) than SARS-CoV-2(+)/EBV(-) Patients: A Comparative Meta-Analysis. Int J Clin Pract 2023, 2023, 1068000. [Google Scholar] [CrossRef] [PubMed]
- Ruiz-Pablos, M.; Paiva, B.; Montero-Mateo, R.; Garcia, N.; Zabaleta, A. Epstein-Barr Virus and the Origin of Myalgic Encephalomyelitis or Chronic Fatigue Syndrome. Front Immunol 2021, 12, 656797. [Google Scholar] [CrossRef] [PubMed]
- Apostolou, E.; Rizwan, M.; Moustardas, P.; Sjögren, P.; Bertilson, B.C.; Bragée, B.; Polo, O.; Rosén, A. Saliva antibody-fingerprint of reactivated latent viruses after mild/asymptomatic COVID-19 is unique in patients with myalgic-encephalomyelitis/chronic fatigue syndrome. Front Immunol 2022, 13, 949787. [Google Scholar] [CrossRef]
- Suurmond, J.; Diamond, B. Autoantibodies in systemic autoimmune diseases: specificity and pathogenicity. J Clin Invest 2015, 125, 2194–2202. [Google Scholar] [CrossRef]
- Knight, J.S.; Caricchio, R.; Casanova, J.L.; Combes, A.J.; Diamond, B.; Fox, S.E.; Hanauer, D.A.; James, J.A.; Kanthi, Y.; Ladd, V.; et al. The intersection of COVID-19 and autoimmunity. J Clin Invest 2021, 131. [Google Scholar] [CrossRef]
- Wang, E.Y.; Mao, T.; Klein, J.; Dai, Y.; Huck, J.D.; Jaycox, J.R.; Liu, F.; Zhou, T.; Israelow, B.; Wong, P.; et al. Diverse functional autoantibodies in patients with COVID-19. Nature 2021, 595, 283–288. [Google Scholar] [CrossRef]
- Bastard, P.; Gervais, A.; Le Voyer, T.; Rosain, J.; Philippot, Q.; Manry, J.; Michailidis, E.; Hoffmann, H.H.; Eto, S.; Garcia-Prat, M.; et al. Autoantibodies neutralizing type I IFNs are present in ~4% of uninfected individuals over 70 years old and account for ~20% of COVID-19 deaths. Sci Immunol 2021, 6. [Google Scholar] [CrossRef] [PubMed]
- Peluso, M.J.; Thomas, I.J.; Munter, S.E.; Deeks, S.G.; Henrich, T.J. Lack of Antinuclear Antibodies in Convalescent Coronavirus Disease 2019 Patients With Persistent Symptoms. Clin Infect Dis 2022, 74, 2083–2084. [Google Scholar] [CrossRef] [PubMed]
- Arthur, J.M.; Forrest, J.C.; Boehme, K.W.; Kennedy, J.L.; Owens, S.; Herzog, C.; Liu, J.; Harville, T.O. Development of ACE2 autoantibodies after SARS-CoV-2 infection. PLoS One 2021, 16, e0257016. [Google Scholar] [CrossRef] [PubMed]
- Wallukat, G.; Hohberger, B.; Wenzel, K.; Fürst, J.; Schulze-Rothe, S.; Wallukat, A.; Hönicke, A.S.; Müller, J. Functional autoantibodies against G-protein coupled receptors in patients with persistent Long-COVID-19 symptoms. J Transl Autoimmun 2021, 4, 100100. [Google Scholar] [CrossRef] [PubMed]
- Fogarty, H.; Townsend, L.; Morrin, H.; Ahmad, A.; Comerford, C.; Karampini, E.; Englert, H.; Byrne, M.; Bergin, C.; O’Sullivan, J.M.; et al. Persistent endotheliopathy in the pathogenesis of long COVID syndrome. J Thromb Haemost 2021, 19, 2546–2553. [Google Scholar] [CrossRef] [PubMed]
- Jarrott, B.; Head, R.; Pringle, K.G.; Lumbers, E.R.; Martin, J.H. “LONG COVID”-A hypothesis for understanding the biological basis and pharmacological treatment strategy. Pharmacol Res Perspect 2022, 10, e00911. [Google Scholar] [CrossRef] [PubMed]
- Fan, B.E.; Wong, S.W.; Sum, C.L.L.; Lim, G.H.; Leung, B.P.; Tan, C.W.; Ramanathan, K.; Dalan, R.; Cheung, C.; Lim, X.R.; et al. Hypercoagulability, endotheliopathy, and inflammation approximating 1 year after recovery: Assessing the long-term outcomes in COVID-19 patients. Am J Hematol 2022, 97, 915–923. [Google Scholar] [CrossRef] [PubMed]
- Kell, D.B.; Pretorius, E. The potential role of ischaemia-reperfusion injury in chronic, relapsing diseases such as rheumatoid arthritis, Long COVID, and ME/CFS: evidence, mechanisms, and therapeutic implications. Biochem J 2022, 479, 1653–1708. [Google Scholar] [CrossRef]
- Pretorius, E.; Venter, C.; Laubscher, G.J.; Kotze, M.J.; Oladejo, S.O.; Watson, L.R.; Rajaratnam, K.; Watson, B.W.; Kell, D.B. Prevalence of symptoms, comorbidities, fibrin amyloid microclots and platelet pathology in individuals with Long COVID/Post-Acute Sequelae of COVID-19 (PASC). Cardiovasc Diabetol 2022, 21, 148. [Google Scholar] [CrossRef]
- Du, W.N.; Zhang, Y.; Yu, Y.; Zhang, R.M. D-dimer levels is associated with severe COVID-19 infections: A meta-analysis. Int J Clin Pract 2021, 75, e14031. [Google Scholar] [CrossRef]
- Rushworth, R.L.; Torpy, D.J.; Falhammar, H. Adrenal Crisis. N Engl J Med 2019, 381, 852–861. [Google Scholar] [CrossRef] [PubMed]
- Demitrack, M.A.; Dale, J.K.; Straus, S.E.; Laue, L.; Listwak, S.J.; Kruesi, M.J.; Chrousos, G.P.; Gold, P.W. Evidence for impaired activation of the hypothalamic-pituitary-adrenal axis in patients with chronic fatigue syndrome. J Clin Endocrinol Metab 1991, 73, 1224–1234. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.J.; Ko, Y.C.; Chow, L.H.; Hsiao, F.J.; Liu, H.Y.; Wang, P.N.; Chen, W.T. Salivary cortisol is associated with cognitive changes in patients with fibromyalgia. Sci Rep 2021, 11, 1311. [Google Scholar] [CrossRef] [PubMed]
- Leow, M.K.; Kwek, D.S.; Ng, A.W.; Ong, K.C.; Kaw, G.J.; Lee, L.S. Hypocortisolism in survivors of severe acute respiratory syndrome (SARS). Clin Endocrinol (Oxf) 2005, 63, 197–202. [Google Scholar] [CrossRef] [PubMed]
- Choy, K.W. Cortisol concentrations and mortality from COVID-19. Lancet Diabetes Endocrinol 2020, 8, 808. [Google Scholar] [CrossRef] [PubMed]
- Kedor, C.; Freitag, H.; Meyer-Arndt, L.; Wittke, K.; Hanitsch, L.G.; Zoller, T.; Steinbeis, F.; Haffke, M.; Rudolf, G.; Heidecker, B.; et al. A prospective observational study of post-COVID-19 chronic fatigue syndrome following the first pandemic wave in Germany and biomarkers associated with symptom severity. Nat Commun 2022, 13, 5104. [Google Scholar] [CrossRef] [PubMed]
- Bonilla, H.; Quach, T.C.; Tiwari, A.; Bonilla, A.E.; Miglis, M.; Yang, P.C.; Eggert, L.E.; Sharifi, H.; Horomanski, A.; Subramanian, A.; et al. Myalgic Encephalomyelitis/Chronic Fatigue Syndrome is common in post-acute sequelae of SARS-CoV-2 infection (PASC): Results from a post-COVID-19 multidisciplinary clinic. Front Neurol 2023, 14, 1090747. [Google Scholar] [CrossRef] [PubMed]
- Dalamaga, M.; Christodoulatos, G.S. Adiponectin as a biomarker linking obesity and adiposopathy to hematologic malignancies. Horm Mol Biol Clin Investig 2015, 23, 5–20. [Google Scholar] [CrossRef]
- Dalamaga, M.; Karmaniolas, K.; Chamberland, J.; Nikolaidou, A.; Lekka, A.; Dionyssiou-Asteriou, A.; Mantzoros, C.S. Higher fetuin-A, lower adiponectin and free leptin levels mediate effects of excess body weight on insulin resistance and risk for myelodysplastic syndrome. Metabolism 2013, 62, 1830–1839. [Google Scholar] [CrossRef]
- Dalamaga, M.; Crotty, B.H.; Fargnoli, J.; Papadavid, E.; Lekka, A.; Triantafilli, M.; Karmaniolas, K.; Migdalis, I.; Dionyssiou-Asteriou, A.; Mantzoros, C.S. B-cell chronic lymphocytic leukemia risk in association with serum leptin and adiponectin: a case-control study in Greece. Cancer Causes Control 2010, 21, 1451–1459. [Google Scholar] [CrossRef]
- Dalamaga, M.; Karmaniolas, K.; Nikolaidou, A.; Chamberland, J.; Hsi, A.; Dionyssiou-Asteriou, A.; Mantzoros, C.S. Adiponectin and resistin are associated with risk for myelodysplastic syndrome, independently from the insulin-like growth factor-I (IGF-I) system. Eur J Cancer 2008, 44, 1744–1753. [Google Scholar] [CrossRef] [PubMed]
- Dalamaga, M.; Nikolaidou, A.; Karmaniolas, K.; Hsi, A.; Chamberland, J.; Dionyssiou-Asteriou, A.; Mantzoros, C.S. Circulating adiponectin and leptin in relation to myelodysplastic syndrome: a case-control study. Oncology 2007, 73, 26–32. [Google Scholar] [CrossRef] [PubMed]
- Marouga, A.; Dalamaga, M.; Kastania, A.N.; Antonakos, G.; Thrasyvoulides, A.; Kontelia, G.; Dimas, C.; Vlahakos, D.V. Correlates of serum resistin in elderly, non-diabetic patients with chronic kidney disease. Clin Lab 2013, 59, 1121–1128. [Google Scholar] [CrossRef] [PubMed]
- Papadavid, E.; Gazi, S.; Dalamaga, M.; Stavrianeas, N.; Ntelis, V. Palmoplantar and scalp psoriasis occurring during anti-tumour necrosis factor-alpha therapy: a case series of four patients and guidelines for management. J Eur Acad Dermatol Venereol 2008, 22, 380–382. [Google Scholar] [CrossRef]
- Papadavid, E.; Vlami, K.; Dalamaga, M.; Giatrakou, S.; Theodoropoulos, K.; Gyftopoulos, S.; Stavrianeas, N.; Papiris, S.; Rigopoulos, D. Sleep apnea as a comorbidity in obese psoriasis patients: a cross-sectional study. Do psoriasis characteristics and metabolic parameters play a role? J Eur Acad Dermatol Venereol 2013, 27, 820–826. [Google Scholar] [CrossRef]
- Papadavid, E.; Dalamaga, M.; Vlami, K.; Koumaki, D.; Gyftopoulos, S.; Christodoulatos, G.S.; Papiris, S.; Rigopoulos, D. Psoriasis is associated with risk of obstructive sleep apnea independently from metabolic parameters and other comorbidities: a large hospital-based case-control study. Sleep Breath 2017, 21, 949–958. [Google Scholar] [CrossRef]
- Pavlidou, A.; Dalamaga, M.; Kroupis, C.; Konstantoudakis, G.; Belimezi, M.; Athanasas, G.; Dimas, K. Survivin isoforms and clinicopathological characteristics in colorectal adenocarcinomas using real-time qPCR. World J Gastroenterol 2011, 17, 1614–1621. [Google Scholar] [CrossRef]
- Dalamaga, M.; Karmaniolas, K.; Lekka, A.; Antonakos, G.; Thrasyvoulides, A.; Papadavid, E.; Spanos, N.; Dionyssiou-Asteriou, A. Platelet markers correlate with glycemic indices in diabetic, but not diabetic-myelodysplastic patients with normal platelet count. Dis Markers 2010, 29, 55–61. [Google Scholar] [CrossRef]
- Bramante, C.T.; Buse, J.B.; Liebovitz, D.; Nicklas, J.; Puskarich, M.A.; Cohen, K.; Belani, H.; Anderson, B.; Huling, J.D.; Tignanelli, C.; et al. Outpatient treatment of Covid-19 with metformin, ivermectin, and fluvoxamine and the development of Long Covid over 10-month follow-up. medRxiv 2022. [Google Scholar] [CrossRef]
- Bruzzone, C.; Conde, R.; Embade, N.; Mato, J.M.; Millet, O. Metabolomics as a powerful tool for diagnostic, pronostic and drug intervention analysis in COVID-19. Front Mol Biosci 2023, 10, 1111482. [Google Scholar] [CrossRef]
- König, R.S.; Albrich, W.C.; Kahlert, C.R.; Bahr, L.S.; Löber, U.; Vernazza, P.; Scheibenbogen, C.; Forslund, S.K. The Gut Microbiome in Myalgic Encephalomyelitis (ME)/Chronic Fatigue Syndrome (CFS). Front Immunol 2021, 12, 628741. [Google Scholar] [CrossRef] [PubMed]
- Vallianou, N.G.; Kounatidis, D.; Tsilingiris, D.; Panagopoulos, F.; Christodoulatos, G.S.; Evangelopoulos, A.; Karampela, I.; Dalamaga, M. The Role of Next-Generation Probiotics in Obesity and Obesity-Associated Disorders: Current Knowledge and Future Perspectives. Int J Mol Sci 2023, 24. [Google Scholar] [CrossRef] [PubMed]
- Papavasileiou, G.; Tsilingiris, D.; Spyrou, N.; Vallianou, N.G.; Karampela, I.; Magkos, F.; Dalamaga, M. Obesity and main urologic cancers: Current systematic evidence, novel biological mechanisms, perspectives and challenges. Semin Cancer Biol 2023, 91, 70–98. [Google Scholar] [CrossRef] [PubMed]
- Yeoh, Y.K.; Zuo, T.; Lui, G.C.; Zhang, F.; Liu, Q.; Li, A.Y.; Chung, A.C.; Cheung, C.P.; Tso, E.Y.; Fung, K.S.; et al. Gut microbiota composition reflects disease severity and dysfunctional immune responses in patients with COVID-19. Gut 2021, 70, 698–706. [Google Scholar] [CrossRef]
- Zhang, F.; Lau, R.I.; Liu, Q.; Su, Q.; Chan, F.K.L.; Ng, S.C. Gut microbiota in COVID-19: key microbial changes, potential mechanisms and clinical applications. Nat Rev Gastroenterol Hepatol 2023, 20, 323–337. [Google Scholar] [CrossRef] [PubMed]
- de Almeida, V.M.; Engel, D.; Ricci, M.F.; Cruz, C.S.; Lopes, I.S.; Alves, D.A. et al. Mirna d’ Auriol5Gut microbiota from patients with mild COVID-19 cause alterations in mice that resemble post-COVID syndrome. 2022. [Google Scholar] [CrossRef]
- Dalamaga, M.; Karmaniolas, K.; Arsenis, G.; Pantelaki, M.; Daskalopoulou, K.; Papadavid, E.; Migdalis, I. Cedecea lapagei bacteremia following cement-related chemical burn injury. Burns 2008, 34, 1205–1207. [Google Scholar] [CrossRef]
- Papadavid, E.; Dalamaga, M.; Kapniari, I.; Pantelidaki, E.; Papageorgiou, S.; Pappa, V.; Tsirigotis, P.; Dervenoulas, I.; Stavrianeas, N.; Rigopoulos, D. Lobomycosis: A case from Southeastern Europe and review of the literature. J Dermatol Case Rep 2012, 6, 65–69. [Google Scholar] [CrossRef]
- Bader-Larsen, K.S.; Larson, E.A.; Dalamaga, M.; Magkos, F. A Narrative Review of the Safety of Anti-COVID-19 Nutraceuticals for Patients with Cancer. Cancers (Basel) 2021, 13. [Google Scholar] [CrossRef]
- Giron, L.B.; Peluso, M.J.; Ding, J.; Kenny, G.; Zilberstein, N.F.; Koshy, J.; Hong, K.Y.; Rasmussen, H.; Miller, G.E.; Bishehsari, F.; et al. Markers of fungal translocation are elevated during post-acute sequelae of SARS-CoV-2 and induce NF-κB signaling. JCI Insight 2022, 7. [Google Scholar] [CrossRef]
- Domingues, R.B.; Leite, F.; Senne, C. Cerebrospinal fluid analysis in patients with COVID-19-associated central nervous system manifestations: a systematic review. Arq Neuropsiquiatr 2022, 80, 296–305. [Google Scholar] [CrossRef] [PubMed]
- Jarius, S.; Pache, F.; Körtvelyessy, P.; Jelčić, I.; Stettner, M.; Franciotta, D.; Keller, E.; Neumann, B.; Ringelstein, M.; Senel, M.; et al. Cerebrospinal fluid findings in COVID-19: a multicenter study of 150 lumbar punctures in 127 patients. J Neuroinflammation 2022, 19, 19. [Google Scholar] [CrossRef] [PubMed]
- Chaumont, H.; Kaczorowski, F.; San-Galli, A.; Michel, P.P.; Tressières, B.; Roze, E.; Quadrio, I.; Lannuzel, A. Cerebrospinal fluid biomarkers in SARS-CoV-2 patients with acute neurological syndromes. Rev Neurol (Paris) 2023, 179, 208–217. [Google Scholar] [CrossRef] [PubMed]
- Guillot, F.; Garcia, A.; Salou, M.; Brouard, S.; Laplaud, D.A.; Nicot, A.B. Transcript analysis of laser capture microdissected white matter astrocytes and higher phenol sulfotransferase 1A1 expression during autoimmune neuroinflammation. J Neuroinflammation 2015, 12, 130. [Google Scholar] [CrossRef] [PubMed]
- Peluso, M.J.; Sans, H.M.; Forman, C.A.; Nylander, A.N.; Ho, H.E.; Lu, S.; Goldberg, S.A.; Hoh, R.; Tai, V.; Munter, S.E.; et al. Plasma Markers of Neurologic Injury and Inflammation in People With Self-Reported Neurologic Postacute Sequelae of SARS-CoV-2 Infection. Neurol Neuroimmunol Neuroinflamm 2022, 9. [Google Scholar] [CrossRef]
- Fernández-Castañeda, A.; Lu, P.; Geraghty, A.C.; Song, E.; Lee, M.-H.; Wood, J.; Yalçın, B.; Taylor, K.R.; Dutton, S.; Acosta-Alvarez, L.; et al. Mild respiratory SARS-CoV-2 infection can cause multi-lineage cellular dysregulation and myelin loss in the brain. 2022. [Google Scholar] [CrossRef]
- Magdy, R.; Eid, R.A.; Fathy, W.; Abdel-Aziz, M.M.; Ibrahim, R.E.; Yehia, A.; Sheemy, M.S.; Hussein, M. Characteristics and Risk Factors of Persistent Neuropathic Pain in Recovered COVID-19 Patients. Pain Med 2022, 23, 774–781. [Google Scholar] [CrossRef] [PubMed]
- Peluso, M.J.; Deeks, S.G.; Mustapic, M.; Kapogiannis, D.; Henrich, T.J.; Lu, S.; Goldberg, S.A.; Hoh, R.; Chen, J.Y.; Martinez, E.O.; et al. SARS-CoV-2 and Mitochondrial Proteins in Neural-Derived Exosomes of COVID-19. Ann Neurol 2022, 91, 772–781. [Google Scholar] [CrossRef]
- Wu, J.; Tang, L.; Ma, Y.; Li, Y.; Zhang, D.; Li, Q.; Mei, H.; Hu, Y. Immunological Profiling of COVID-19 Patients with Pulmonary Sequelae. mBio 2021, 12, e0159921. [Google Scholar] [CrossRef]
- Davis, H.E.; Assaf, G.S.; McCorkell, L.; Wei, H.; Low, R.J.; Re’em, Y.; Redfield, S.; Austin, J.P.; Akrami, A. Characterizing long COVID in an international cohort: 7 months of symptoms and their impact. EClinicalMedicine 2021, 38, 101019. [Google Scholar] [CrossRef]
- Apostolo, D.; D’Onghia, D.; Tonello, S.; Minisini, R.; Baricich, A.; Gramaglia, C.; Patrucco, F.; Zeppegno, P.; Acquaviva, A.; Balbo, P.E.; et al. Decreased Gas6 and sAxl Plasma Levels Are Associated with Hair Loss in COVID-19 Survivors. Int J Mol Sci 2023, 24. [Google Scholar] [CrossRef] [PubMed]
- Haslam, A.; Olivier, T.; Prasad, V. The definition of long COVID used in interventional studies. Eur J Clin Invest 2023, e13989. [Google Scholar] [CrossRef] [PubMed]
- Fawzy, N.A.; Abou Shaar, B.; Taha, R.M.; Arabi, T.Z.; Sabbah, B.N.; Alkodaymi, M.S.; Omrani, O.A.; Makhzoum, T.; Almahfoudh, N.E.; Al-Hammad, Q.A.; et al. A systematic review of trials currently investigating therapeutic modalities for post-acute COVID-19 syndrome and registered on WHO International Clinical Trials Platform. Clin Microbiol Infect 2023, 29, 570–577. [Google Scholar] [CrossRef] [PubMed]
- Greenhalgh, T.; Sivan, M.; Delaney, B.; Evans, R.; Milne, R. Long covid-an update for primary care. Bmj 2022, 378, e072117. [Google Scholar] [CrossRef] [PubMed]
- Chadda, K.R.; Blakey, E.E.; Huang, C.L.; Jeevaratnam, K. Long COVID-19 and Postural Orthostatic Tachycardia Syndrome- Is Dysautonomia to Be Blamed? Front Cardiovasc Med 2022, 9, 860198. [Google Scholar] [CrossRef] [PubMed]
- Peluso, M.J.; Anglin, K.; Durstenfeld, M.S.; Martin, J.N.; Kelly, J.D.; Hsue, P.Y.; Henrich, T.J.; Deeks, S.G. Effect of Oral Nirmatrelvir on Long COVID Symptoms: 4 Cases and Rationale for Systematic Studies. Pathog Immun 2022, 7, 95–103. [Google Scholar] [CrossRef] [PubMed]
- Xie, Y.; Choi, T.; Al-Aly, Z. Association of Treatment With Nirmatrelvir and the Risk of Post-COVID-19 Condition. JAMA Intern Med 2023. [Google Scholar] [CrossRef]
- Bajema, K.L.; Berry, K.; Streja, E.; Rajeevan, N.; Li, Y.; Yan, L.; Cunningham, F.; Hynes, D.M.; Rowneki, M.; Bohnert, A.; et al. Effectiveness of COVID-19 treatment with nirmatrelvir-ritonavir or molnupiravir among U.S. Veterans: target trial emulation studies with one-month and six-month outcomes. medRxiv 2022. [Google Scholar] [CrossRef]
- Durstenfeld, M.S.; Peluso, M.J.; Lin, F.; Peyser, N.D.; Isasi, C.; Carton, T.W.; Henrich, T.J.; Deeks, S.G.; Olgin, J.E.; Pletcher, M.J.; et al. Association of Nirmatrelvir/Ritonavir Treatment with Long COVID Symptoms in an Online Cohort of Non-Hospitalized Individuals Experiencing Breakthrough SARS-CoV-2 Infection in the Omicron Era. 2023. [Google Scholar] [CrossRef]
- Parthasarathy, H.; Tandel, D.; Siddiqui, A.H.; Harshan, K.H. Metformin suppresses SARS-CoV-2 in cell culture. Virus Res 2022, 323, 199010. [Google Scholar] [CrossRef]
- Ventura-López, C.; Cervantes-Luevano, K.; Aguirre-Sánchez, J.S.; Flores-Caballero, J.C.; Alvarez-Delgado, C.; Bernaldez-Sarabia, J.; Sánchez-Campos, N.; Lugo-Sánchez, L.A.; Rodríguez-Vázquez, I.C.; Sander-Padilla, J.G.; et al. Treatment with metformin glycinate reduces SARS-CoV-2 viral load: An in vitro model and randomized, double-blind, Phase IIb clinical trial. Biomed Pharmacother 2022, 152, 113223. [Google Scholar] [CrossRef] [PubMed]
- Daou, N.; Viader, A.; Cokol, M.; Nitzel, A.; Chakravarthy, M.V.; Afeyan, R.; Tramontin, T.; Marukian, S.; Hamill, M.J. A novel, multitargeted endogenous metabolic modulator composition impacts metabolism, inflammation, and fibrosis in nonalcoholic steatohepatitis-relevant primary human cell models. Sci Rep 2021, 11, 11861. [Google Scholar] [CrossRef] [PubMed]
- Finnigan, L.E.M.; Cassar, M.P.; Koziel, M.J.; Pradines, J.; Lamlum, H.; Azer, K.; Kirby, D.; Montgomery, H.; Neubauer, S.; Valkovič, L.; Raman, B. Efficacy and tolerability of an endogenous metabolic modulator (AXA1125) in fatigue-predominant long COVID: a single-centre, double-blind, randomised controlled phase 2a pilot study. eClinicalMedicine. (In press). 2023, 101946. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://clinicaltrials.gov/ (accessed on 15 May 2023).
- Kritis, P.; Karampela, I.; Kokoris, S.; Dalamaga, M. The combination of bromelain and curcumin as an immune-boosting nutraceutical in the prevention of severe COVID-19. Metabol Open 2020, 8, 100066. [Google Scholar] [CrossRef]
Figure 1.
Potential pathophysiological mechanisms involved in the development of long COVID following acute SARS-CoV-2 infection. (All images are constructed with the free medical site http://smart.servier.com/ (accessed on May 15, 2023) by Servier licensed under a Creative Commons Attribution 3.0 Unported License).
Figure 1.
Potential pathophysiological mechanisms involved in the development of long COVID following acute SARS-CoV-2 infection. (All images are constructed with the free medical site http://smart.servier.com/ (accessed on May 15, 2023) by Servier licensed under a Creative Commons Attribution 3.0 Unported License).
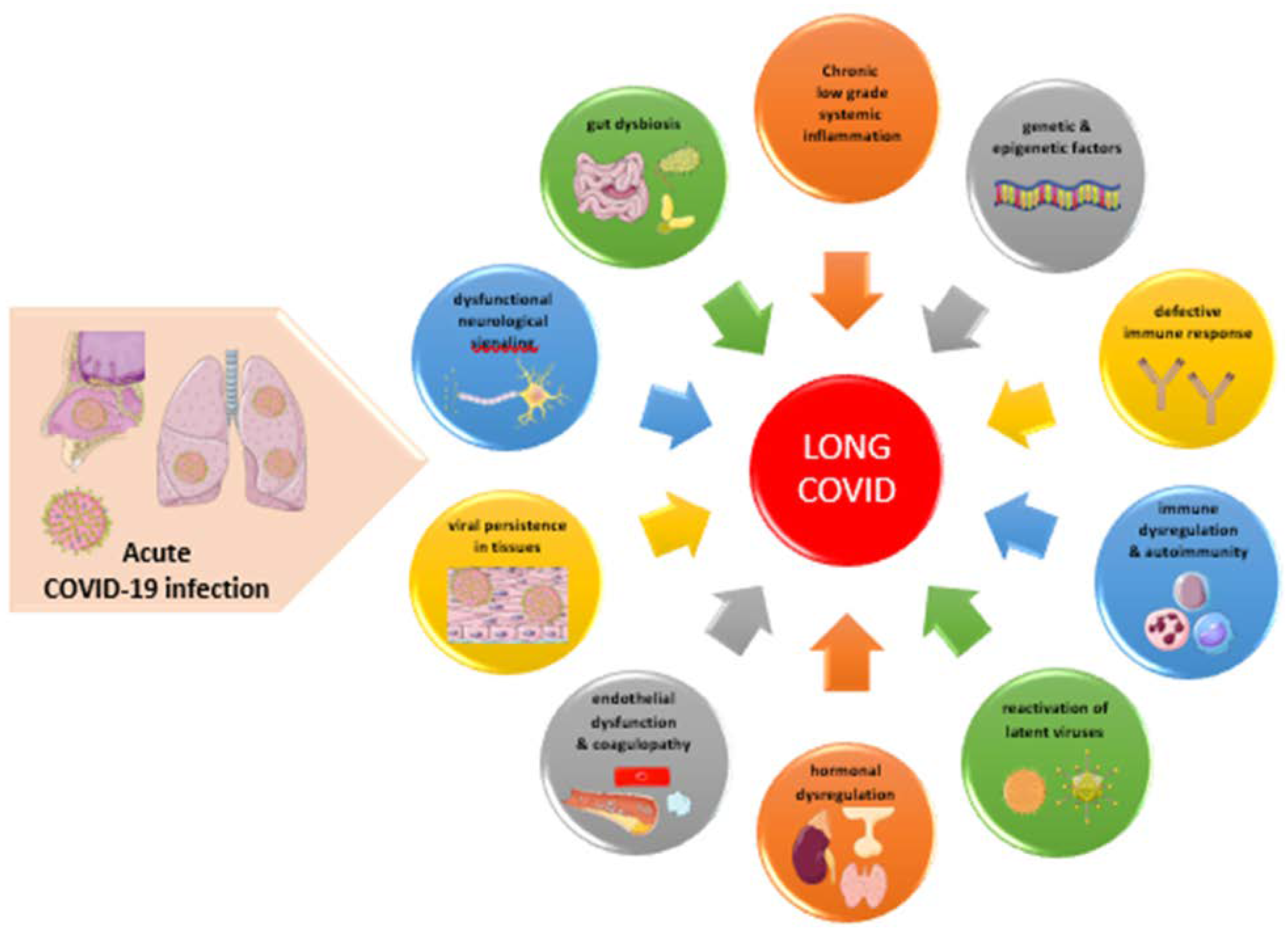
Figure 2.
Candidate biomarkers classifying clinical manifestations in long COVID (LC). Abbreviations: ANAs: antinuclear antibodies; CMV: Cytomegalovirus; CRP: C-Reactive Protein; CSF: Cerebrospinal fluid; EBV: Epstein-Barr Virus; GFAP: glial fibrillary acidic protein; GH: Growth Hormone; HOMA-IR: Homeostatic Model Assessment for Insulin Resistance; IFN: Interferon; IL: interleukin; LBP: Lipopolysaccharide Binding Protein; MCP: Monocyte Chemotactic Protein; NfL: neurofilament light chain protein; NK: Natural Killer; SARS-CoV-2: Severe Acute Respiratory Syndrome Coronavirus 2; TNF: tumor necrosis factor; , (All images are originated from the free medical site http://smart.servier.com/ (accessed on May 15, 2023) by Servier licensed under a Creative Commons Attribution 3.0 Unported License).
Figure 2.
Candidate biomarkers classifying clinical manifestations in long COVID (LC). Abbreviations: ANAs: antinuclear antibodies; CMV: Cytomegalovirus; CRP: C-Reactive Protein; CSF: Cerebrospinal fluid; EBV: Epstein-Barr Virus; GFAP: glial fibrillary acidic protein; GH: Growth Hormone; HOMA-IR: Homeostatic Model Assessment for Insulin Resistance; IFN: Interferon; IL: interleukin; LBP: Lipopolysaccharide Binding Protein; MCP: Monocyte Chemotactic Protein; NfL: neurofilament light chain protein; NK: Natural Killer; SARS-CoV-2: Severe Acute Respiratory Syndrome Coronavirus 2; TNF: tumor necrosis factor; , (All images are originated from the free medical site http://smart.servier.com/ (accessed on May 15, 2023) by Servier licensed under a Creative Commons Attribution 3.0 Unported License).
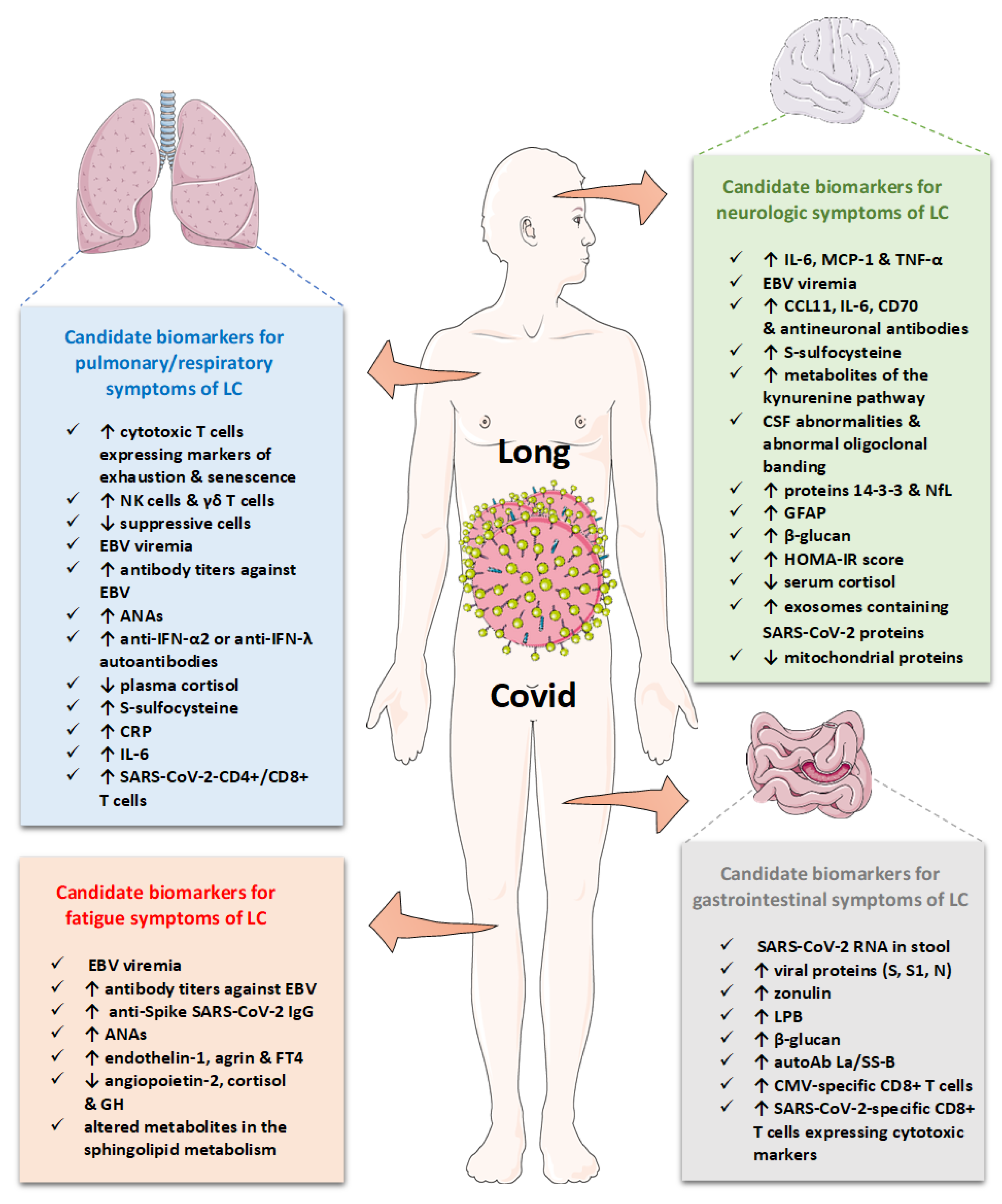

Table 1.
Main risk factors, clinical and laboratory findings in acute severe COVID-19 and long COVID.
Table 1.
Main risk factors, clinical and laboratory findings in acute severe COVID-19 and long COVID.
| Main Characteristics | Acute severe COVID-19 | long COVID |
|---|---|---|
| Age | Older age | ↑ % of diagnoses between the ages 36-50 years |
| Gender | More frequent in males | More frequent in females |
| Predisposing factors & Comorbidities | -Older age, Obesity, T2DM, CVD, asthma or chronic lung disease, sickle cell disease, immunocompromised patients, hematologic malignancies, chronic kidney disease, patients under immunosuppressive treatments -Racial and ethnic minority groups -People with low income -Unvaccinated individuals |
-Obesity, T2DM, connective tissue disorders, allergic rhinitis, ADHD, -More frequent in Black and Hispanic Americans -People with low income -Poor rest in the early period after COVID-19 -↑ risk after severe COVID-19 -Most cases involve non-hospitalized patients with a mild acute COVID-19 |
| Laboratory findings & biomarkers | Lymphopenia, ↑CRP, ↑ Neutrophils, ↑ IL-6, ↑ IL-10, ↑ D-dimer, ↑ LDH, ↑ ferritin |
In certain patients: ↑ IL-6, ↑ CRP, ↑ D-dimer, detectable SARS-CoV-2 RNA in stool or gut mucosa, biomarkers of EBV reactivation, anti-IFN-α2 or anti-IFN-λAbs, ↑ ET-1 and ↓Ang-2, ↓ cortisol, metabolites of mitochondrial dysfunction, ↑% of CSF abnormalities and ↑ biomarkers of neuronal damage (For more details see Table 3) |
| CVD features | Pulmonary embolism, deep vein thrombosis, AMI, heart failure | Chest pain, palpitations, myocarditis, cardiac impairment, POTS |
| Neurologic features | Headache, Ischemic stroke, ataxia, seizures, anosmia, ageusia | Brain fog, fatigue, musculoskeletal pain, cognitive impairment, paresthesia, sleep disorder, dizziness, memory loss, dysautonomia, tinnitus |
| Pulmonary features | Cough, dyspnea, hypoxia, bilateral lung infiltrates | Cough, dyspnea, abnormal gas exchange, ground glass lung |
| Gastrointestinal features | Abdominal pain, nausea, vomiting, diarrhea, T1DM, ↑ transaminases | Abdominal pain, nausea |
| Endocrine abnormalities | ↑ T1DM, ↑ T2DM thyroiditis |
Diabetes, hypocortisolism |
| Dermatologic findings | Skin rashes (maculopapular, chilblain-like, urticarial, vesicular, livedoid, and petechial lesions), hair loss | Most common alopecia, various skin rashes |
| Renal manifestations | Acute Kidney Injury Acute Tubular Necrosis |
↓eGFR, |
| Manifestations from the reproductive system | Menstrual irregularities ↑ urinary frequency and nocturia |
Menstrual irregularities ↑ premenstrual symptoms Erectile dysfunction ↓ sperm count |
Abbreviations: ADHD: Attention Deficit Hyperactivity Disorder; AMI: Acute Myocardial Infraction; Ang: angiopoietin; CRP: C-Reactive Protein; CVD: cardiovascular disease; eGFR: estimated Glomerular Filtration Rate; ET: endothelin; IFN: Interferon; IL: interleukin; POTS: Postural Orthostatic Tachycardia Syndrome; T1DM: diabetes mellitus type 1; T2DM: diabetes mellitus type 2.
Table 2.
General clinical, laboratory and imaging diagnostic approach.
| General laboratory work-up |
| Complete blood count |
| Erythrocyte sedimentation rate |
| General biochemical tests: Glucose, HbA1c, urea, creatinine, electrolytes (sodium, potassium, calcium, phosphate) |
| Indices of hepatic function: AST, ALT, γ-GT, ALP |
| CPK, ferritin, LDH |
| Indices of cardiac function: troponin, BNP or NT-proBNP |
| Indices of thyroid function: TSH, fT4 |
| Indices of coagulation and fibrinolysis: D-dimer, fibrinogen, PT, aPTT |
| Indices of inflammation: CRP, IL-6 |
| Vitamins: 25-OHD, B12 |
| Autoantibodies and Complement: RF, anti-CCP, ANA, ACA, C3, C4 |
| Imaging and other function tests |
| High resolution Chest Computed Tomography |
| Computed Tomography Pulmonary Angiogram (CTPA) |
| Pulmonary function tests (spirometry, diffusion capacity, lung volumes) |
| Pulse Oxymetry |
| Six minute walk test (6MWT) |
| Electrocardiogram |
| Cardiac ultrasound |
| Cardiac magnetic resonance |
| Cardiopulmonary exercise testing (CPET) |
| Brain magnetic resonance |
| Questionnaires and clinical tests |
| Tilt table test for POTS or 10-Minute NASA Lean Test for orthostatic intolerance |
| Dyspnea scales (mMRC, NYHA) |
| Questionnaire SBQ-LC |
| Questionnaires for anxiety: BAI, HAM-A, GAD-7 |
| Questionnaires for depression: BDI, HAM-D, PHQ-2,-9 |
| Some Promising tests |
| Cortisol/ four-point salivary cortisol test |
| IgG, IgA, IgM |
| Natural Killer cell function tests |
| Panels for reactivated herpesviruses (EBV, CMV, VZV, HHV-6) |
| SARS-CoV-2 RNA in stool or gut mucosa |
| Endothelin-1 and Angiopoietin-2 |
| Hyperpolarized gas magnetic resonance of the lungs |
Abbreviations: ACA: Anti-cardiolipin antibodies ; ALP: Alkaline phosphatase; ALT: alanine transaminase; ANA: antinuclear antibodies; anti-CCP: anti-cyclic citrullinated peptide antibodies; AST: aspartate aminotransferase; aPTT: activated Partial Thromboplastin Time; BAI: Beck’s Anxiety Inventory; BDI: Beck Depression Inventory; BNP: B-type natriuretic peptide; CMV: Cytomegalovirus; CTPA: CT pulmonary angiogram; CRP: C-Reactive Protein; CPK: Creatine Phosphokinase; DLCO: Diffusing Capacity of Carbon monoxide; EBV: Epstein-Barr Virus; ECG: electrocardiogram; fT4: free thyroxine; GAD-7: Generalized Anxiety Disorder scale; HAM-A: Hamilton Anxiety Scale; HAM-D: Hamilton Depression Scale; HHV-6: Human HerpesVirus-6; Ig: Immunoglobulin; LDH: Lactate Dehydrogenase; NASA: National Aeronautics and Space Administration; NT-proBNP: N-terminal pro b-type natriuretic peptide; PHQ-2,9: Patient Health Questionnaire; POTS: Postural orthostatic tachycardia syndrome; PT: Prothrombin Time; RF: Rheumatoid Factor; SBQ-LC: Symptom Burden Questionnaire for LC; TSH: Thyroid Stimulating Hormone; VZV: Varicella-Zoster Virus; γ-GT: gamma-Glutamyl Transferase; 25-OHD: 25-hydroxyvitamin D.
Table 3.
Major studies depicting potential predictive, diagnostic and prognostic biomarkers in long COVID.
Table 3.
Major studies depicting potential predictive, diagnostic and prognostic biomarkers in long COVID.
| Study, year | Study design/population | Main Findings | Utility |
|---|---|---|---|
| Biomarkers of systemic inflammation | |||
| Yong SJ et al., 2023 [150] | Meta-analysis of 23 studies (14 prospective and 9 retrospective case control) with 18 meta-analyzed biomarkers | -↑ CRP, D-dimer, LDH and leukocytes in LC patients than those without LC -↑ lymphocytes and IL-6 in LC patients than those without LC -↑ IL-8 in LC than healthy controls |
-Diagnostic utility in LC; however small effects -↑ D-dimer, LDH, and lymphocytes in patients with organ abnormalities -↑ IL-6 in patients with symptom persistence - ↑ LDH, leucocytes, NT-pro-BNP in patients with duration of symptoms <6 months -↑ D-dimer in patients with duration of symptoms ≥6 months |
| Yin JX et al., 2022 [151] | Meta-analysis of 22 case-control observational studies | -↑ IL-6 levels in LC patients than controls -↑ IL-6 levels in LC patients than those with non-postacute sequelae of severe COVID-19 -↑ IL-6 levels in patients with acute COVID-19 than patients with LC |
-IL-6 may predict LC -IL-6 may characterize early stage of LC. |
| Lopez-Leon S et al., 2021 [15] | 21 meta-analyses on the prevalence of long-term effects in LC, 15 studies, 47,910 patients (age: 17–87 years). | -↑ CRP in 8% of patients (95% CI: 5–12) -↑ ferritin in 8% of patients (95% CI: 4–14) -↑ procalcitonin in 4% of patients (95% CI: 2–9) -↑ IL-6 in 3% of patients (95% CI: 1–7) |
Limited evidence for systemic inflammation after 4 months approximately post-viral infection. |
| Immune profiling in long COVID | |||
| Klein J et al., 2022 [152] | 220 participants (101 LC, 41 CC, 41 HC, and 37 HCW) at >400 days post infection Cross-sectional study |
LC is characterized by: ↑ non-classical monocytes, ↑ activated B cells, ↑ double-negative B cells, ↑ exhausted T cells, ↑ IL-4/IL-6 secreting CD4 T cells, ↓ conventional DC1 ↓ central memory CD4 T cells |
Integration of immune phenotyping data into machine learning models may identify distinguishing features in the classification of LC |
| Haunhorst S et al., 2022 [153] | Scoping review of 3 studies examining Tregs in LC | -Galán M et al. [154] 2.5X ↑Tregs in LC compared to subjects that recovered completely -Utrero-Rico et al. [155] ↓ Tregs in LC compared to subjects that recovered completely - ↓ Tregs in LC compared to seronegative controls [156] |
No firm conclusions can be drawn about Treg alterations in LC |
| Phetsouphanh C et al., 2022 [85] | LC group (n= 31) asymptomatic matched controls/MC (n = 31) compared to individuals infected with common cold coronavirus (HCoV) (n= 25) and unexposed healthy donors (n= 13) |
↑ activated innate immune cells, ↓ naive T and B cells ↑ expression of type I IFN (IFN-β) and type III IFN (IFN-λ1) that remained persistently high at 8 months after infection. |
|
| Patterson BK et al., 2021 [156] | Case-control & longitudinal study 121 cases with LC 29 healthy controls 26 cases with mild-moderate COVID-19 48 cases with severe COVID-19 |
-↑ B-cells in LC compared to HC -↑ inflammatory monocytes CD14+, CD16+, CCR5+ compared to HC -↓CD4+ and CD8+ T-cells expressing PD-1 (exhausted lymphocytes), and T-reg in LC compared to HC |
-↑ Inflammatory monocytes and ↓ exhausted lymphocytes detected in patients who later developed LC (predictive biomarkers). - ↑ Inflammatory monocytes and ↑ exhausted lymphocytes in the convalescence period of LC |
| Biomarkers reflecting SARS-CoV-2 persistence | |||
| Swank Z et al., 2022 [157] | 63 individuals previously infected with SARS-CoV-2, 37 of whom were diagnosed with LC |
↑ circulating Spike protein in LC cases, but not in convalescent controls up to 12 months | SARS-CoV-2 viral reservoirs may persist in the body |
| Natarajan A et al., 2022 [158] | 113 individuals with mild to moderate COVID-19 Longitudinal study |
- SARS-CoV-2 RNA in the feces at 4 months after diagnosis (12.7%) - SARS-CoV-2 RNA in the feces at 7 months after diagnosis (3.8%) |
GI symptoms (abdominal pain, nausea, vomiting) are related with fecal shedding of SARS-CoV-2 RNA |
| Stein SR et al., 2022 [87] | Autopsies on 44 patients who died with COVID-19 | - Persistent SARS-CoV-2 RNA in multiple anatomic sites, including throughout the brain, as late as 230 day - ≥50% of late cases had persistent RNA in the myocardium, lymph nodes from the head and neck and from the thorax, sciatic nerve, ocular tissue, and in all sampled regions of the CNS, except the dura mater. |
SARS-CoV-2 can cause systemic infection and persist in the body for months in certain patients |
| Tejerina F et al., 2022 [159] | Cohort of 29 patients who reported persistent symptoms at least 4w after COVID-19 | - 45% had positive plasma RT-PCR results -51% were positive in at least one RT-PCR sample (plasma, urine, or stool). |
Potential systemic viral persistence associated with persistent symptoms |
| Zollner A et al., 2022 [160] | Cohort of 46 patients with IBD 219 days (range, 94-257) after confirmed COVID-19 | - SARS-CoV-2 RNA in the gut mucosa ∼7 months after mild acute COVID-19 in 69.5% - Nucleocapsid protein persisted in 52.2% patients in gut epithelium and CD8+ T cells. -Not detectable viral antigens in stool |
-Viral persistence markers associated with symptoms of LC |
| Yonker LM et al., 2021 [161] | 19 children with MIS-C, 26 with acute COVID-19, and 55 controls. | -89% of cases with MIS-C had GI symptoms versus 27% of children with acute COVID-19 - Detectable viral loads in the stool (1.5 × 102 to 2.5 × 107 RNA copies/mL) in the majority of cases -↑ plasma zonulin and LBP compared to controls - ↑ SARS-CoV-2 spike, S1, and nucleocapsid antigens compared to controls |
- Prolonged exposure to SARS-CoV-2 in the GI tract of children with MIS -Loss of mucosal barrier integrity -SARS-CoV-2 antigenemia may trigger the hyperinflammatory responses defining MIS-C |
| Humoral and cellular response against SARS-CoV-2 in long COVID | |||
| Klein J et al., 2022 [152] | 220 participants (101 LC, 41 CC, 41 HC, and 37 HCW) at >400 days post infection Cross-sectional study |
↑ IgG against Spike and S1 in LC compared to vaccination-matched controls | -Potential predictive biomarker of LC |
| Files JK et al., 2021 [162] | A longitudinal study of 50 cases with COVID-19: -20 with persistent symptoms (30-208 days) -30 with symptom resolution within 20 days. |
In patients with persistent symptoms: -↑ IgG avidity to SARS-CoV-2 spike protein - sustained T cell response magnitudes - ↑ antigen-specific CD4+ T cell responses against Spike (late phase) - ↑ antigen-specific CD8+ T cell populations |
↑ T cell response magnitude in individuals with prolonged symptoms |
| García-Abellán J et al., 2021 [89] | Prospective, longitudinal study of 146 hospitalized COVID-19 patients | ↓ peak IgG against Spike associated with LC symptoms at 6 months | -Potential predictive biomarker of LC |
| Augustin M et al., 2021 [163] | A longitudinal prospective cohort study of 958 non- hospitalized patients with confirmed COVID-19 | ↓ baseline levels of IgG against S1 domain of the spike associated with long-term symptoms | -Potential predictive biomarker of LC |
| Blomberg B et al., 2021 [164] | A prospective cohort study of 312 patients (247 home-isolated and 65 hospitalized) | -↑ IgG against spike protein and -↑ microneutralizing antibody titers detected after 2 months independently associated with both persistent fatigue and total number of symptoms at 6 months | -Increased antibody titers predictive biomarker of LC symptoms |
| Peluso MJ et al., 2021 [165] | A prospective cohort study of 70 individuals with PCR-confirmed COVID-19 | - No significant differences in early and late (1 and 4 months) antibody levels (IgG against SARS-CoV-2 Spike, RBD, and two preparations of the N protein) between cases with and without persistent symptoms. - No differences in T cell responses at initial time point between cases with and without persistent symptoms -↓ CD8+ T cells expressing CD107a against N peptide in cases with LC -↓ N-specific interferon-γ-producing CD8+ T cells in cases with LC |
|
| Biomarkers reflecting reactivation of latent viruses | |||
| Peluso MJ et al., 2023 [166] | A cohort of 280 adults with prior COVID-19 | -↑ early antigen-diffuse EBV IgG positivity associated with fatigue at 4m -↑ IgG against EBNA associated with fatigue and neurocognitive dysfunction, at 4 m after infection |
Reactivation of EBV is associated with fatigue and cognitive dysfunction in LC |
| Klein J et al., 2022 [152] | 220 participants (101 LC, 41 CC, 41 HC, and 37 HCW) at >400 days post infection Cross-sectional study |
↑ titers of anti-EBV antibodies, even though overall seroprevalence is not different from HC or CC | Altered humoral responses to distinct herpesviruses in LC as predictive biomarker |
| Zubchenko S et al., 2022 [167] | 88 patients with LC | - EBV reactivation in 42.6% -HHV6 reactivation in 25.0% -EBV plus HHV6 reactivation in 32.4% |
Reactivation was associated with ↑ slight fever temperature, headache, psycho-neurological disorders, pulmonary abnormalities and myalgia, liver enzymes, CRP and D-dimer, and ↓ cellular immune response |
| Su Y et al., 2022 [168] | A cohort of 309 COVID-19 patients from initial diagnosis to convalescence (2-3 months later) 457 HC |
-EBV viremia at T1 was associated with LC (fatigue and respiratory symptoms) at 3m post-infection | -EBV viremia may be a predictive biomarker of LC |
| Gold JE et al., 2021 [169] | A cohort of randomly 185 surveyed COVID-19 patients -56 developed LC |
-↑ EBV early antigen-diffuse IgG or ↑EBV viral capsid antigen (VCA) IgM in 66.7% of LC versus 10% of controls | -EBV reactivation may be a predictive biomarker of LC |
| Biomarkers reflecting autoimmunity | |||
| Muri J et al., 2023 [170] | A cohort of 71 COVID-19 convalescent patients at month 6 (on average) post disease onset, 23 HC | -IgG antibodies against chemokines CCL21, CXCL13 and CXCL16 at month 6 distinguished LC from no LC groups - Levels of CCL21, CXCL13 and CXCL16 predicted the absence of persistent symptoms with 77.8% accuracy |
-Ab against specific chemokines were associated with favorable disease outcome and negatively correlated with the development of LC at 1 year post-infection. |
| Bodansky A et al., 2023 [171] | A cohort of 121 individuals with LC, 64 with prior COVID-19 and full recovery, and 57 pre-COVID controls. | - Significant differences in autoreactivity between COVID-19 patients and pre-COVID controls. -No patterns of autoreactivity that separate individuals with LC to individuals fully recovered from COVID-19. |
Absence of LC specific autoreactivities |
| Son K et al., 2023 [172] | A cohort of 106 convalescent COVID-19 patients with varying acute phase severities at 3, 6 and 12 months post-recovery, 22 HCs and 34 with other respiratory infections | -Abs to U1-snRNP and anti-SS-B/La were both positively associated with persistent symptoms of fatigue and dyspnea - Pro-inflammatory cytokines such as TNF-α and CRP predicted ↑ ANAs at 12 months. |
Persistently positive ANAs at 12 months post-COVID are associated with persisting symptoms and inflammation in a subset of COVID-19 survivors |
| Franke C et al., 2023 [173] | A prospective study of 50 patients with reported cognitive problems | -92% had normal routine CSF parameters -52% had anti-neuronal Abs (n = 9 in serum only, n = 3 in CSF only and n = 14 in both, including those against myelin, Yo, Ma2/Ta, GAD65 and NMDA receptor, but also a variety of undetermined epitopes on brain sections). |
Abnormal cognitive status is associated with anti-neuronal Abs in CSF |
| Peluso MJ et al., 2022 [174] |
A prospective study of 215 participants with convalescent COVID-19 tested over 394 time points, including 121 people with LC | -2 out of 215 had IFN-α2-specific autoantibodies across all sample timepoints | No detectable anti-IFN-α2 antibodies in LC |
| Klein J et al., 2022 [152] | 220 participants (101 LC, 41 CC, 41 HC, and 37 HCW) Cross-sectional study |
No significant differences in the total number of autoantibody reactivities per participant across groups using REAP, a high throughput method for the measurement of Ab reactivity against >6,000 extracellular and secreted human proteins |
No specific autoAbs that could differentiate participants with LC from controls |
| Su Y et al., 2022 [168] | A cohort of 309 COVID-19 patients from initial diagnosis to convalescence (2-3 months later). 457 HC Determination of an auto-Ab panel: anti-IFN-α2, and 5 anti-nuclear auto-Abs (Ro/SS-A, La/SS-B, U1-snRNP, Jo-1, and P1) at clinical diagnosis and convalescence |
- Patients with autoAbs at convalescence (44%) already exhibited mature (class-switched) auto-Abs as early as at diagnosis (56%). -Inverse correlations between SARS-CoV-2 IgGs (class-switched) and autoAbs. - |
- IFN-α2 autoAbs uniquely associated with respiratory symptoms of LC - ↑ multiple autoAbs at convalescence are associated with GI symptoms and sputum production of LC |
| Rojas M et al., 2022 [175] | Case-control study 100 patients with LC with a median post-COVID time: 219 (IQR: 143 to 258) days. 30 pre-pandemic HC |
-Latent autoimmunity in 83% of patients -Polyautoimmunity in 62% of patients -anti-IFN autoAbs in 5-10% of patients -Anti-SARS-CoV-2 IgG correlated with autoAbs |
-IgG anti-IFN-λ Abs were associated with the persistence of respiratory symptoms. -Latent autoimmunity correlates with Ab response against SARS-CoV-2 |
| Endothelial or vascular biomarkers | |||
| Patel MA et al., 2022 [176] | A case-control study of 23 LC patients, one to six months post-infection, and 23 ward COVID patients, 23 ICU COVID patients and 23 HCs | -Angiogenesis markers (ANG-1 and P-SEL) had excellent sensitivity and specificity for LC status (AUC = 1.00) among 16 blood biomarkers of vascular transformation. -ANG-1 levels were associated with female sex and a lack of disease interventions at follow-up |
-Diagnostic utility and classification of LC status (accuracy 96%) |
| Haffke M et al., 2022 [177] | A case-control study of 30 LC patients with persistent fatigue and exertion intolerance (14 with 14 post-COVID ME/CFS) and 15 age- and sex matched seronegative HCs |
-↑ ET-1 concentration in both ME/CFS and LC patients compared to HCs and post-convalescent controls -↓ Ang-2 in both LC patients and post-convalescent controls compared to HCs |
-LC patients with fatigue present ↑ ET-1 and ↓ Ang-2 - Ang-2 levels exclusively in LC could be a differentiation biomarker between PCS and ME/CFS |
| Tong M et al., 2022 [178] | A cross-sectional study of 345 COVID-19 (39% had LC symptoms) and 119 age and gender-matched HCWs | -No significant differences in vascular biomarkers (serum levels of VCAM-1, ICAM-1, P-selectin) between COVID-19 survivors and controls | |
| Biomarkers of coagulation and fibrinolysis | |||
| Yong SJ et al., 2023 [150] | Meta-analysis of 23 studies (14 prospective and 9 retrospective case control) with 18 meta-analyzed biomarkers | -↑ D-dimer, CRP, LDH and leukocytes in LC patients than those without LC -↑ lymphocytes and IL-6 in LC patients than those without LC -↑ IL-8 in LC than healthy controls |
-Diagnostic utility in LC; however small effects -↑ D-dimer, LDH, and lymphocytes in patients with organ abnormalities -↑ D-dimer in patients with duration of symptoms ≥6 months |
| Constantinescu-Bercu A et al., 2023 [179] | A cohort of 21 patients with LC with a median time of 23 months of follow up and controls | -↑ platelet binding on both collagen and anti-VWF A3 in patients with LC compared with controls, which positively correlated with VWF, VWF(Ag):ADAMTS13 ratio, and inversely correlated with ADAMTS13 activity | -LC is a prothrombotic state |
| Di Gennaro L et al., 2022 [180] | A case-control study of 75 children with previously confirmed COVID-19 in a pediatric post-covid unit ≥ 8 weeks after the initial infection | -↑ D-Dimer levels in LC children compared to children that had fully recovered at the 8-12 weeks (p = 0.04), and 12 week follow up or more (p = 0.05), and in children with three or more symptoms at 12 weeks (p = 0.002). -No significant differences in other coagulation factors between LC children and controls |
Abnormal D-dimer levels in children with LC and more symptoms |
| Kruger et al., 2022 [181] | A case-control study of 99 LC patients and 29 HCs. | -↑ platelet factor 4 (PF4), VWF, and α-2 antiplasmin (α-2-AP) in LC - ↓ plasma kallikrein in LC - Significant platelet hyperactivation was noted in LC |
Failed fibrinolytic system in LC |
| Pretorius E et al., 2021 [182] | A cross sectional study of 11 patients with LC, 13 HCs, 15 with COVID-19 (before treatment), 10 with T2DM | - Microclots in both acute COVID-19 and LC plasma samples are resistant to fibrinolysis (compared to plasma from controls and T2DM) -↑ SAA in LC than controls - Platelets from LC patients are hyperactivated -in the digested clots ↑ α2 antiplasmin, plasminogen, coagulation factor XIII A chain, vWF, fibrinogen alpha chain, C7, CRP in LC than controls |
Abnormal fibrinolysis and coagulopathy in LC |
| Hormonal and metabolic biomarkers | |||
| Al-Hakeim HK et al., 2023 [124] | Retrospective cohort study with controls 86 patients with LC 39 HC |
-↑ HOMA2-IR, fasting blood glucose, and insulin levels in LC -33.7% of patients vs 0% of controls had HOMA-IR >1.8 |
- LC is associated with new-onset IR -↑ IR was significantly associated with depressive symptoms |
| Su Y et al., 2022 [168] | A cohort of 309 COVID-19 patients from initial diagnosis to convalescence (2-3 months later) 457 HC |
-↓ cortisol and cortisone in patients with LC at convalescence - ↑ proteins associated with the negative regulation of the circadian sleep/wake cycle in patients with neurological symptoms |
- Patients with respiratory symptoms at convalescence exhibited ↓ cortisol and cortisone |
| Klein J et al., 2022 [152] | 220 participants (101 LC, 41 CC, 41 HC, and 37 HCW) Cross-sectional study |
↓ serum cortisol in LC ↑ in healthy (uninfected) controls, ↓ in convalescent controls, and ↓↓ in cases with LC |
-Serum cortisol was the most significant individual predictor of LC |
| Sunada N et al., 2022 [183] | 186 patients with LC Retrospective analysis |
-↓ serum GH and ↑ serum FT4 in patients with general fatigue -↓cortisol in patients with dysosmia/dysgeusia -↑ serum TSH and ↓ ratio of FT4/TSH in initial severe LC cases |
|
| Other proteins as biomarkers | |||
| The PHOSP-COVID Collaborative Group, 2022 [81] | A prospective, longitudinal cohort study 2,320 participants discharged from hospital; 807 (32·7%) participants completed 5-month and 1-year visits. |
Plasma proteome data for 296 protein features: -↑ of 13 proteins in the severe group of LC |
-↑ IL-6 and CD70 in cognitive impairment cluster compared with the mild cluster |
| Captur G et al., 2022 [184] | A nested longitudinal proteomic case-control study of 156 healthcare workers | Differentially abundant proteins in HCW with persistent symptoms (>6w): proteins with lipid, atherosclerosis and cholesterol metabolism pathways, complement and coagulation cascades, autophagy, and lysosomal function | Potential predictive value for LC at the time of seroconversion |
| Metabolites as biomarkers | |||
| López-Hernández Y et al., 2023 [185] | A longitudinal retrospective analysis of COVID-19 patients (n=22), LC patients (n=25) and controls (n=15) | - Fatigue (59%) and musculoskeletal (50%) were most relevant and persistent symptoms. - Sterols, bile acids, isoprenoids, and fatty esters were affected in both COVID-19 and postCOVID-19 patients -↑ species of phosphatidylcholines and sphingomyelins in LC compared to controls |
- Dysregulation in sphingolipid metabolism could be associated with fatigue and muscular pain |
| López-Hernández Y et al., 2023 [186] | A retrospective longitudinal analysis of 108 participants (HC, COVID-19 and LC patients) | -↑ Lactic acid, lactate/pyruvate ratio, ornithine/citrulline ratio, sarcosine, and arginine in LC -↑ IL-17 in LC |
- Mitochondrial dysfunction, redox state imbalance, impaired energy metabolism, and chronic immune dysregulation in LC |
| Guntur VP et al., 2022 [134] | Case-control study of 29 patients with LC, 16 CC and 30 HC | -↑ free- and carnitine-conjugated mono-, poly-, and highly unsaturated fatty acids, ↓ levels of mono-,di- and tricarboxylates, polyamines (spermine) and taurine in LC -milder disturbances in fatty acid metabolism and ↑ spermine and taurine in recovered patients -tryptophan depletion not normalized in LC |
-Altered fatty acid metabolism and dysfunctional mitochondria-dependent lipid catabolism associated with mitochondrial dysfunction during exercise |
| Cysique LA et al., 2022 [187] | A prospective study of 128 SARS-CoV-2 positive patients | - ↑ quinolinic acid, 3-hydroxyanthranilic acid, and kynurenine were significantly associated with cognitive decline. | The kynurenine pathway metabolites are potential therapeutic targets for COVID-19-related cognitive impairment. |
| Microbiota alterations in long COVID | |||
| Zhang D et al., 2023 [188] | A prospective follow-up study of 187 recovered subjects; 84 reported LC symptoms at one-year after discharge; 32 HCs 16S rRNA sequencing of stool samples |
- Gut microbiota dysbiosis in symptomatic recovered patients -↓ bacterial diversities in LC -↓ relative abundance of SCFAs-producing salutary symbionts, such as Eubacterium_hallii group, Subdoligranulum, Ruminococcus, Dorea, Coprococcus, and Eubacterium_ventriosum group in LC |
-Gut microbiota dysbiosis in recovered patients at one-year after discharge -Gut microbiota dysbiosis in LC |
| Liu Q et al., 2022 [189] | A prospective study of 106 patients with a spectrum of COVID-19 severity from admission to 6 months and 68 non-COVID-19 controls | -↑ Ruminococcus gnavus, Bacteroides vulgatus in LC -↓ Faecalibacterium prausnitzii in LC -↓ Butyrate-producing bacteria in LC |
- Gut microbiota composition at admission was predictive of LC occurrence. |
| Cerebrospinal fluid biomarkers | |||
| Etter MM et al., 2022 [129] | A cohort study of 40 neuro-COVID patients; 25 HCs and 25 non-MS inflammatory neurological disease controls | - CSF levels: ↑ pro-inflammatory proteins (TNFRSF9, IFN-γ) and ↓ anti-inflammatory mediators (TRANCE(RANKL), TRAIL) are predictive for LC - plasma CLM-6, MCP-3 and ST1A1 may predict LC |
-Prediction of LC |
| Apple AC et al., 2022 [190] | A case-control study of 22 participants with cognitive LC and 10 cognitive controls within the prospective study LIINC | - CSF abnormality in 77% of LC patients versus 0% of cognitive controls - Normal values for CSF white blood cells, glucose, calculated CSF/serum albumin ratio, IgG index, CSF IgG level, and serum IgG level in all participants - Abnormal oligoclonal banding in 69% of LC patients versus 0% of cognitive controls |
- ↑% of CSF abnormalities in patients with LC and cognitive impairment after mild COVID-19 |
| Guasp M et al., 2022 [191] | A prospective study of 60 hospitalized neuro-COVID patients, 25 of them with encephalopathy and 14 with encephalitis. 46 serum samples from HCs and 24 CSF samples from subjects with mild subjective cognitive complaints Follow-up: 18 months | - ↑ IL-18, IL-6, and IL-8 in both serum and CSF in neuro-COVID patients compared to HCs -↑ 14-3-3, NfL and IL-18, IL-1RA and IL-8 are associated with acute COVID-19 severity -↑ CSF 14-3-3 and NfL correlate with the degree of neurologic disability in the daily activities at 18 months |
- ↑ CSF levels of neuronal damage biomarkers during the acute phase of COVID-19 are prognostic biomarkers of worse long-term clinical outcome of patients |
Abbreviations: Ab: antibody; ANA: antinuclear antibodies; Ang-2: Angiopoietin-2; CC: Convalescent Control; CD: Dendritic Cell; CI: Confidence Intervals; CNS: Central Nervous System; CSF: Cerebrospinal Fluid; EBV: Epstein-Barr Virus; EBNA: EBV-encoded Nuclear Antigen; ET-1: Endothelin-1; HC: Healthy Control; FT4: Free thyroxine; GH: Growth Hormone; GI: Gastrointestinal; HHV: Human Herpesvirus; HOMA-IR: Homeostasis Model Assessment-Insulin Resistance; HW: Healthcare Worker; IBD: inflammatory bowel disease; ICAM-1: Intercellular Adhesion Molecule-1; IFN: Interferon; IL: interleukin; IQR: Interquartile Range; LC: long COVID; LDH: Lactate dehydrogenase; MIS-C: Multisystem Inflammatory Syndrome in children; NfL: neurofilament light chain protein; NK: Natural Killer Cell; NT-Pro-BNP: N-terminal pro b-type natriuretic peptide; PASC: post-acute sequelae SARS-CoV-2 infection; REAP: Rapid Extracellular Antigen Profiling; SCFAs: Short-chain fatty acids; T2DM: diabetes mellitus type 2 VCA: Viral Capsid Antigen; VCAM: Vascular Cell Adhesion Molecule 1;VEGF: Vascular Endothelial Growth Factor; VWF: Von Willebrand factor.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



