
Submitted:
10 May 2023
Posted:
11 May 2023
You are already at the latest version
Abstract
Physical rehabilitation aims to help people recover their mobility and strength after an
injury or illness. One way to evaluate progress in rehabilitation is through isokinetic prototype
tests that describe the dynamic characteristics of an isokinetic leg extension device for
rehabilitation and control action. These tests use an isokinetic system to assess muscle strength
and performance in a patient during isometric or isokinetic contraction. An experimental
prototype allows the performance of the device to be evaluated in a controlled environment prior
to use by the patient. In order to achieve physical recovery from musculoskeletal injuries in the
lower limbs and achieve the reintegration of the affected subject into society as an independent
and autonomous individual in their daily activities, a control model is presented that introduces a
medical isokinetic rehabilitation protocol, where the element that allows carrying out such
protocol consists of a magnetic particle brake whose control action is strongly influenced by the
dynamics of the system when in contact with the end user, specifically the patient's legs in the
stretch from the knee to the ankle. The results of these tests are valuable for health professionals
seeking to measure their patient’s progress during the rehabilitation process and determine when
it is safe and appropriate to advance in their treatment.
Keywords:
Dynamic modeling
; electric brake control
; isokinetic
; isokinetic control
; dynamometry
; rehabilitation.
1. Introduction
An isokinetic testing protocol based on an experimental prototype is an approach to evaluate the effectiveness of a device or treatment by using a prototype and an isokinetic testing system. The isokinetic concept refers to the ability of the system to maintain a constant speed during muscle contraction, allowing for accurate measurement of strength and performance. Also, an experimental prototype allows the performance of the device to be evaluated in a controlled environment prior to patient use.
Isokinetic rehabilitation is a technique used to recover muscle injuries and other conditions that affect the ability to move and perform physical activities. This technique is based on the use of isokinetic devices, which are machines that allow exercising muscles at a constant speed and measuring their torque. It has been shown to be effective in the recovery of leg muscles injuries, allowing patients to exercise safely with controlled intensity, which facilitates the recovery of muscle strength and endurance. This technique can also help prevent muscle wasting and atrophy in patients with physical disabilities or prolonged periods of inactivity.
This research aims to design a control system for an isokinetic rehabilitation protocol for the recovery of leg muscle injuries. For this purpose, a study of the dynamic components involved in lower limb extension will be performed using the rehabilitation device from Universidad del Valle, seen in Figure 1, which implements a magnetic particle brake to restrict the extension movement; It has speed control and serves as a model to facilitate the demonstration of the effectiveness of isokinetic rehabilitation, recovery of muscle strength and endurance in patients with leg muscle injuries; the device is similar to an isokinetic dynamometer with the difference that it has a robustness that facilitates a customized configuration [1].
2. Literature Review
An isokinetic dynamometer is used in sports, exercise, and clinical settings to measure muscle strength, torque, and power. The device allows specific testing on different joints and muscle groups, adapting to different speeds and ranges of motion. Isolation of the joint of interest allows a complete evaluation to compare right and left limbs, detecting potential injury risks or areas for improvement. Isokinetic dynamometry is used to evaluate and strengthen limbs by measuring maximum force at a specific speed during movement; dynamometry systems allow comparison of concentric and eccentric muscle contractions while maintaining a constant speed; they are commonly used in physical therapy clinics for patients who have suffered injuries or are in post-surgical state, making comparisons between the affected and non-affected limb. The percentage of the strength of the non-affected limb is used to determine when a patient can return to physical activity. In countries such as the United States, these systems are still used to assess limb strength, although they were used more frequently in the past [2].
Regarding the ability to assess muscles across a full range of movements, isokinetic testing has several advantages over isometric testing. Isokinetic testing allows the health specialist to analyze agonist-antagonist relationships, determine maximum strength, evaluate endurance and other indicators of muscle capacity. Through specialized computer tools, it is possible to compare two limbs and provide feedback during the test, delivering valuable information on the degree of recovery of average strength. For patients with extreme cases of weakness, evaluations can be performed with isokinetic devices using torque values obtained through comparison between passive isokinetic motion and concentric maximum effort movement, two of the most significant variables in this type of test [3].
Dynamometry is a technique used to measure muscle strength, which includes different functional and manual muscle tests. Functional tests are easy to perform and do not require equipment, but they have limitations in their exact relationship to muscle strength. Manual muscle testing is a technique used in neurological examinations but requires an experienced examiner and has high variability due to evaluators. Isometric dynamometry measures static muscle strength, while isokinetic dynamometry measures dynamic muscle strength. These techniques provide accurate information about muscle strength of all major muscle groups of the upper and lower extremities. However, comparisons between different studies are rarely made due to the lack of standardization of test procedures and different equipment in laboratories and neuromuscular centers [4].
Some studies have evaluated the reliability of different dynamometers in measuring maximum torque in knee flexion and extension in athletes; the results showed that knee maximum flexion and extension tests performed in specific contractions with different times of use had similar values; this indicates that the measurement of muscle strength of the dynamometer does not change over time. Therefore, the hypothesis is not supported; the study suggests that the IsoMed-2000 isokinetic dynamometer is suitable for evaluating muscle strength and changes in athletes, despite some measurement errors; it can be used in physiotherapy and rehabilitation clinics and for athletes in injury risk analysis and muscle strength development. However, it is not reliable for measuring knee flexion torque. Furthermore, this study also highlights that the control system of the IsoMed-2000 dynamometer may not be robust enough. As a result, the dynamometer may not be reliable in certain conditions or for specific populations. It is essential to be mindful of this limitation when using the device to evaluate muscle strength and to be careful when interpreting the results. It would be beneficial to consider alternative methods or equipment with a more robust control system for measuring knee flexion torque [5]. Several rehabilitation solutions are currently available on the market, but few focus on developing standard isokinetic exercises. Most solutions focus on traditional physical therapy, such as physiotherapy, occupational therapy, and pain therapy. These solutions are based on strengthening and stretching exercises and may include equipment such as elastic bands, weights, and cardio machines. Although these solutions can effectively improve mobility and strength, they do not specifically focus on developing isokinetic exercises, and their control is limited to the device’s dimensions.
Isokinetic exercises are a specific rehabilitation approach based on using isokinetic machines to exercise muscles at a constant speed. This approach is considered more accurate and safer than traditional exercises, as it allows for a more precise measurement of strength and performance [6]. However, although isokinetic exercises are a valuable technique for rehabilitation, they are not as common in the market because they require specialized equipment and trained personnel. Commercial isokinetic dynamometry systems are specialized devices that measure muscle strength and performance in patients with muscle injuries. However, devices such as the Biodex 4 [7] or the Cybex 6000/HUMAC [8] are insufficient to apply a complete isokinetic rehabilitation protocol, as they do not include all the necessary components for a complete treatment. These types of systems require direct supervision from medical staff, which increases the cost of treatment and limits the number of patients that can be treated in one day; this makes treatment more expensive and less accessible for patients [9]. These devices are also insufficient to apply a complete isokinetic rehabilitation protocol. They focus mainly on strength evaluation and do not include a complete exercise and therapy program for injury recovery [10].
The study [11] compared two machines, the SMM iMoment and the Biodex System Pro 4, regarding their reliability in measuring knee flexion and extension at different speeds. The study concluded that the differences between the machines were insignificant and that most of the variations in results could be attributed to biological differences between subjects and the difficulty of repeating the same performance on different occasions [12]. However, some technical differences were identified that could impact the results, such as the damping system and seat fixation. The authors found that the machines modulate between high and moderate absolute reliability compared to other studies [13]. The study suggests that the manufacturer of the SMM iMoment machine improves the software to validate control objectively by adjusting the parameter to patient’s dimensions, changing the mechanism, and simplifying the movement and fixation system [14].
Additionally, these devices are expensive and not very durable, requiring a significant investment in equipment and qualified personnel. Also, they do not consider the dynamics of the mechanisms and the patient for isokinetic control, which limits their effectiveness in muscle injury rehabilitation. It is important to continue researching and developing solutions to improve the accessibility and effectiveness of isokinetic exercises in rehabilitation. In summary, although isokinetic exercises are a valuable technique for rehabilitation, current solutions on the market do not aim to develop this technique due to the lack of availability, cost, and access to the necessary equipment and trained personnel. However, it is important to continue researching and developing solutions to improve the accessibility and effectiveness of isokinetic exercises in rehabilitation.
3. Architecture
Characterizing a device for isokinetic rehabilitation of the leg with an architecture, see Figure 1, requires careful consideration, such as the dynamic equations of motion, the angle between the patellar tendon and the tibia, the calculation of the force components of the patellar tendon, the torque generated by the tendon along the leg, the characterization of a magnetic brake, and the design of a controller. These factors are critical to ensure effective and safe rehabilitation of patients. For example, the accuracy in the calculation of the patellar tendon force will enable a good estimation of the generated torque. At the same time, proper characterization of the magnetic brake will guarantee suitable control of the resistance during the exercise. Furthermore, the design of an efficient controller will be crucial to ensure an adequate and safe response to changes in leg position and speed during rehabilitation.
3.1. Definition of Physical Variables Involved in the Rehabilitation System
In a testing scenario, the kinematic and dynamic characteristics of the bodies interacting within the system must be considered to achieve rehabilitation through techniques that allow controlling the speed of a patient’s leg extension.
During lower limb rehabilitation processes, particularly for the case of the knee and leg, activities of limb extension are performed, in which the body posture remains seated with a slight inclination of the back. The goal is to extend the leg from a reference position of 0° when the leg is perpendicular to the ground and extend it to achieve an inclination of 90° while keeping the axis of the leg parallel to the ground [15]. Figure 2 shows the behavior of an uncontrolled leg extension. The angular position change is seen in Figure 2a, and the angular speed change is seen in Figure 2b, of a leg during the extension initiated at 0 radians and extended to approximately 1.5 radians.
To improve this pre-process and the rehabilitation process, it has been suggested to implement a feature where the patient performs the extension process with an equal speed throughout the entire arc of motion, as ensuring the speed requires the body to control the force with which the leg is lifted and in turn facilitates the collection of information on the patient’s activity. Figure 3 shows an ideal leg extension with constant speed through the rehabilitation exercise.
The considered variables involved in each subsystem are the following: is the torque due to components of the force on the patellar tendon; is the torque due to the weight of the leg; is the torque due to the pedal of the mechanical brake system; is the torque opposing the movement generated by the magnetic brake; is the torque observed at the knee reference point concerning the system; is the mass of the leg; is the current angular speed at the time of measurement in ; is the previous speed at the time of measurement in ; is the sampling time; is the length of the leg; is the angle measured in radians of the position of the leg upright relative to the ground, and the thigh that is in a horizontal position to the ground with a reference point such as the knee, ; is gravity acceleration equivalent to 9.81 ; is the mass of the machine pedal; is the distance of the pedal from the axis to the point of contact with the leg; is the angular acceleration; is the moment of inertia calculated as ; is the angle measured in radians generated between the patellar tendon and the tibia; is the voltage applied to the brake system; is the resistance of the brake system for an applied voltage and dependent on the system current for a given moment; is the motor constant measured in .
Within the dynamic of the patient-machine system, the sum of torques is equal to the angular movement acceleration, , by the leg inertia, , that is, . Equation (1) shows the sum of torques expressed in the individual torques for each component considered in the rehabilitation device system. The generated counterclockwise torques are the ones produced by the patellar tendon force, , and the torque due to the movement of the leg when lifting, , are represented positively. In contrast, in a clockwise direction, the torque due to the weight of the leg, , the weight of the pedal, , and the opposing torque induced by the brake, , when actuated, are present.
where, is the torque due to Coriolis and centrifugal forces, is the torque due to gravity, and is the net torque at the knee joint. Figure 4 shows the extended leg experiments with the torques produced by the gravitational forces due to the device on the pedal weight and the human leg weight and how they interact negatively on the opposite direction of the knee torque.
At the knee joint, a human knee with the leg at the maximum extension experiences torque reduction due to the gravity and the sum of the inertia moments of the angular acceleration and the inertia moments of the human leg and the device pedal which are ignored due to the minimum impact to the exercise. Figure 4 reactions at the knee joint are shown in Equation (2).
Every other instant where the leg is in the movement of being extended, what the knee joint is experiencing dynamic variables due to the anthropomorphically values can be seen in Figure 5.
In the maximum leg extension seen in Figure 4, the radial acceleration becomes zero because the leg stops moving upon extension. In the case presented by Figure 5 a, the sum of torques due to gravity for the human, and machine, are counterbalanced by the torque generated by the patellar tendon force going in the opposite direction, for this case .
A simplified model is proposed to derive the system torques based on the following patient measurements, as seen in Figure 5b. In this case, the depth of the tendon within the leg is considered, forming a right-angled triangle that can be vectorially decomposed, as Figure 6 indicates.
To facilitate the following calculation, it is estimated that the value of the center of gravity of the leg is exactly half the length of the leg. Using the Equation (2), and knowing that , and , the torque due to the moment of inertial in the knee joint is Equation (3).
Next, the force in the patellar tendon is solved as Equation (4).
3.2. Considerations for Calculation of Angle
Based on [16] and [17], for tendon length, , the variations are approximately from 1/12 of the length of the leg, which is measured from the center of the knee to the foot’s sole, when the leg is fully extended (, to 1/11 of when the leg is flexed (, and from the surface of the knee locating the patellar bone to a horizontal reference to the fixation of the patellar tendon with the tibia bone with an approximate value of 1/55 of the length of the leg, . Figure 7a proposes a simple decomposition of the dimensions of the length of the patellar tendon when the leg is fully extended and when is fully flexed for the extension exercise, which generates a lineal behavior that permits to find the relation between the patient’s leg length and the length of the patellar tendon. For a description of the length relation can be used to propose a point where the length of the extended and flexed leg meets over the tibial bone to establish the compressive angle as seen in Figure 7b.
For a leg of length , the patellar tendon distance (), as a function of the angle is seen in Equation (5):
The angle generated by the patellar tendon and the adjacent side is calculated in Equation (6):
Likewise, using the trigonometric identity ; the Equation (6) can be viewed as as function of angle shown in Equation (7):
3.3. Consideration for Calculation of the Patellar Tendon Force Components
The patellar tendon is responsible for exerting the force that generates the torque capable of lifting the lower leg during extension; the length of the patellar tendon is calculated based on the angle and is expressed as Considering a right triangle with the upper vertex at the lower contact with the patella and the furthest end at the rigid anchor point with the tibia, as seen in Figure 8, the distances to a point perpendicular under the patella and horizontal to the anchor point of the patellar tendon can be calculated, which facilitates the subsequent calculation of angle .
Knowing that the side perpendicular to the angle is ; then, the horizontal side (), to the angle is calculated using the Pythagorean theorem as . The components on the patellar tendon forces, seen in the Figure 9, are and .
Therefore, the torque component, , due to the patellar tendon force is calculated in the Equation (8).
The component of the distance used to calculate the torque in the Equation (8) can be extracted and denoted as . Then, the distant component of seen on Equation (5) is replaced by generating the Equation (9) as:
For a particular case, the supply voltage to the brake is zero, there will be no counter-torque, therefore . Thus, replacing into Equation (9) the resultant force is seen in Equation (10):
Taking the difference of the current speed with respect to the previous one over the sample time can be replaced by angular acceleration, as follows in Equation (11):
Then the torque applied by the patellar tendon is .
3.4. Considerations for Calculation of Torque Generated by the Tendon along the Leg
The torque generated by the tendon during leg extension can be obtained by simplifying the model of the leg as seen in Figure 10 and considering the tendon force as a beam suspended over a pulley symbolizing the knee and the origin point for measurement.
Considering the vertical directions of the force exerted by the patellar tendon in the upward direction and the force caused by the weight of the leg in a downward direction, the human torque, seen in Equation (12), can be expressed as the difference of these two components as follows, taking as reference the distances from the knee to the tendon anchor point and half the distance of the leg to calculate the weight due to gravity thus as follows:
3.5. Considerations for Magnetic Brake Characterization
For the case of the brake, when the system is working in the off condition, it does not generate an opposing torque to the leg movement; therefore, at the initial phase of the protocol, it is assumed that no torque is applied to the system. On the other hand, when the brake is in the on condition, the voltage applied to the electrical system that makes the brake to generate an electric current is conditioned by the electrical structure of the selected brake [18] and for this case can be reduced to a constant that involves the brake material, circuits and dimensions which is denominated . This constant with the interaction of the electrical conditions of voltage and resistance of the circuit produces a torque, , and is opposite to the torque generated by the extension of the leg, .
Regarding the leg moment of inertia seen in Equation (4), a patient’s leg placed in the rehabilitation device pushing on a weight sensor, which captures the mass (, is measuring the force executed by the extension when the brake is in condition. The torque of the excited leg will be equivalent to the difference of the moment of inertia with the torque generated by the brake as seen in Equation (13).
Regarding the particle brake seen in Figure 1b, the Figure 11 shows the relationship between generated torque and supplied current [18], this can be used to infer a linear relationship between them:
From the behavior of the curve from Figure 11, the correspondent points are taken to be used as a basis for a linear regression algorithm to obtain an equation that describes the change in the total percentage of braking torque as function of the applied current, therefore Using the brake manufacturer’s data, is possible to determine the torque generated by the magnetic brake as a function of the current consumed by the system at a given time, so the following expression is obtained, . Therefore, the magnetic brake constant implemented in the system is . Due to the linear behavior of the current, in the case of the electrical voltage at 12 V, the brake torque is . The internal resistance of the element due to the physical and electrical components is .
3.6. Controller Design Considerations
Elements are required that can measure the state of the system in a required instant, for the rehabilitation device this requirement is solved by using a position sensor. This sensor is calibrated with an initial position for an extension movement when the leg is attached to the system and at rest, generating a right angle between the thigh and the leg in an upright position as seen in Figure 12. Position measures can be used in conjunction with the sampling time to evaluate the speed of the extension movement.
The element to be controlled is the particle brake, specifically its power supply system, by performing an electrical resistance function, the amount of voltage that reaches the brake is manipulated and in the same way the action of the brake in the form of counter torque is modulated according to the speed parameters to be controlled. The controller objective is to modify the impedance for the voltage source and modulate the counter torque of the brake, , to force the patient’s leg extension speed to keep its value under the threshold of the speed set by the device operator.
A proportional action for a rehabilitation device extension speed controller can be understood as the relation between the evaluated speed with the threshold speed, and the voltage supply needed to feed the brake, so that the difference of the speeds remains positive, which means that the evaluated speed keeps its value under the threshold, in which case the brake is in the off condition. The controller action increases or decreases the gain or the value of the brake resistivity according to the speed difference, also known as the error signal respect to time, . In case the speed difference evaluates a negative value, which means that the evaluated speed is over the threshold, the controller increases the gain of the voltage source to the brake circuit by increasing . Consequently, a control action , proportional to the angular speed error, , is deployed, where is the proportional gain [19].
With this application, a quick response is achieved when the control action must generate rapid brake resistance; however, if the speed is close to the set point and the response is exceeded, it generates a delay in the response of the system. To improve the performance of the control action, there is an additional integrative control [20]. This type of control seeks to reduce and eliminate the steady-state error, which was present in the previous case when requiring a slow response from the controller with low gain, in this case, the error signal is integrated during the period of the control action, so the response of the controller is delayed by the integrator constant, , this directly affects the proportional delay and is represented in Equation (14).
4. Results and Discussions
Figure 13 shows a dynamic system which involves the subsystems in the proposed rehabilitation exercise of a leg extension patient. The input block pos_ref[rad] is an array of the values taken during an uncontrolled human leg extension, this measure is used by the system as the signal that defines the angular position of the leg during the extension, Theta[rad]. The block Fn_Phi_rad is an operator that converts the Theta[Rad] signal into the Phi[rad] signifying the calculation of phi. The input block vel_ref[deg/s] is an array of the threshold value for the speed limit selected by the device operator, in the planted scenario its value is set as reference speed of , this signal is transformed to used by the error calculation for the control subsystem. Function blocks are implemented to calculate the torque signals T_WL[Nm] for the torque generated by the leg weight; T_WPB[Nm] for the torque generated by the device pedal weight; T_a[Nm] for the torque generated due to motions dynamics; Tao_B[Nm] for the torque generated by the brake action; Tao_H[Nm] for the human torque seen on Equation (13); and ang_accel[rad/] for the system acceleration.
For the controller dynamic observed in Equation (17), its implementation within the rehabilitation device is seen in Figure 13 as the Fn_activate_controller and PI_Controller blocks, red box with dotted lines, which receives the error signal and modifies an activation function to regulate the voltage supply to generate a controlled , is seen in Figure 14.
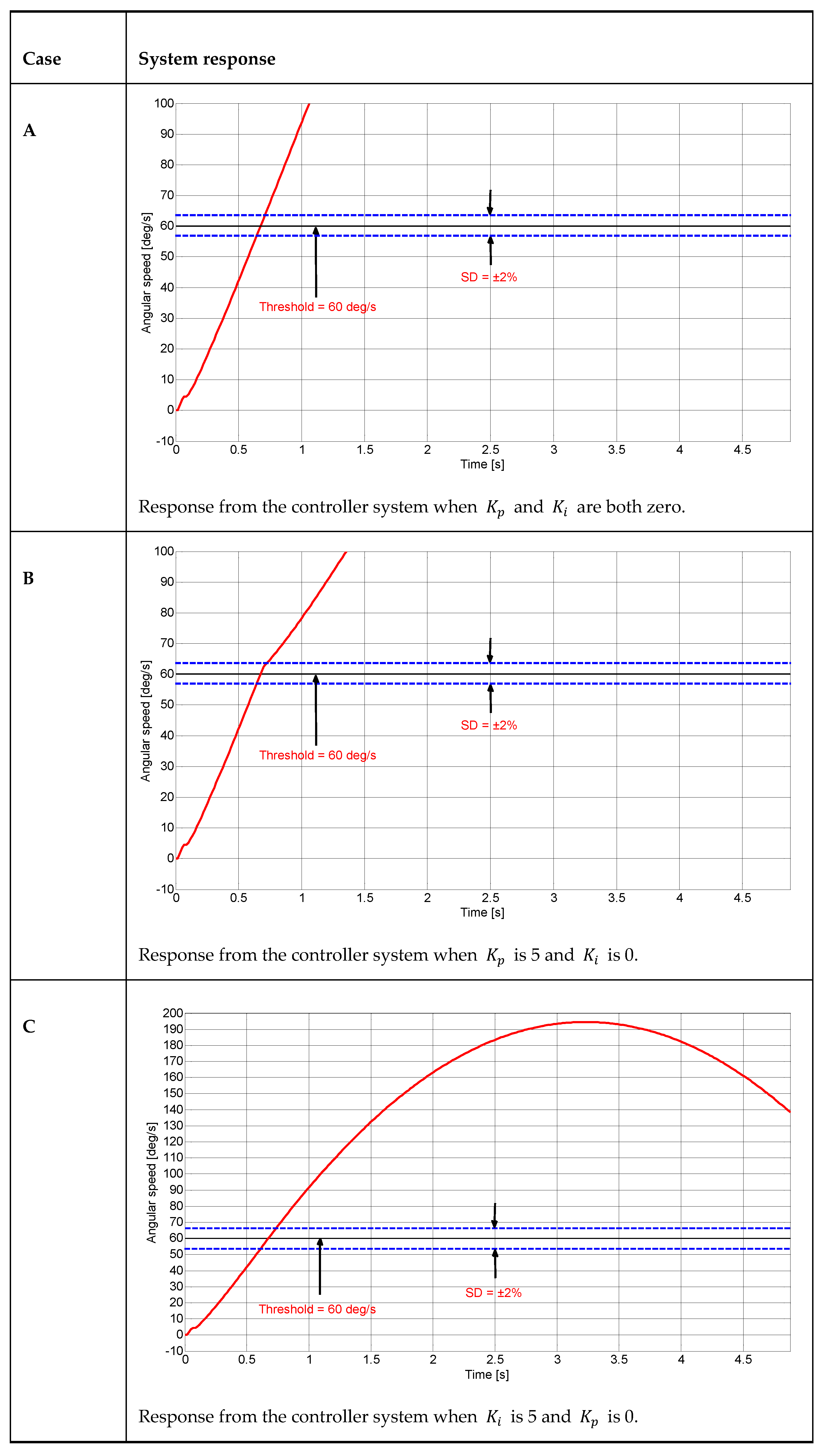
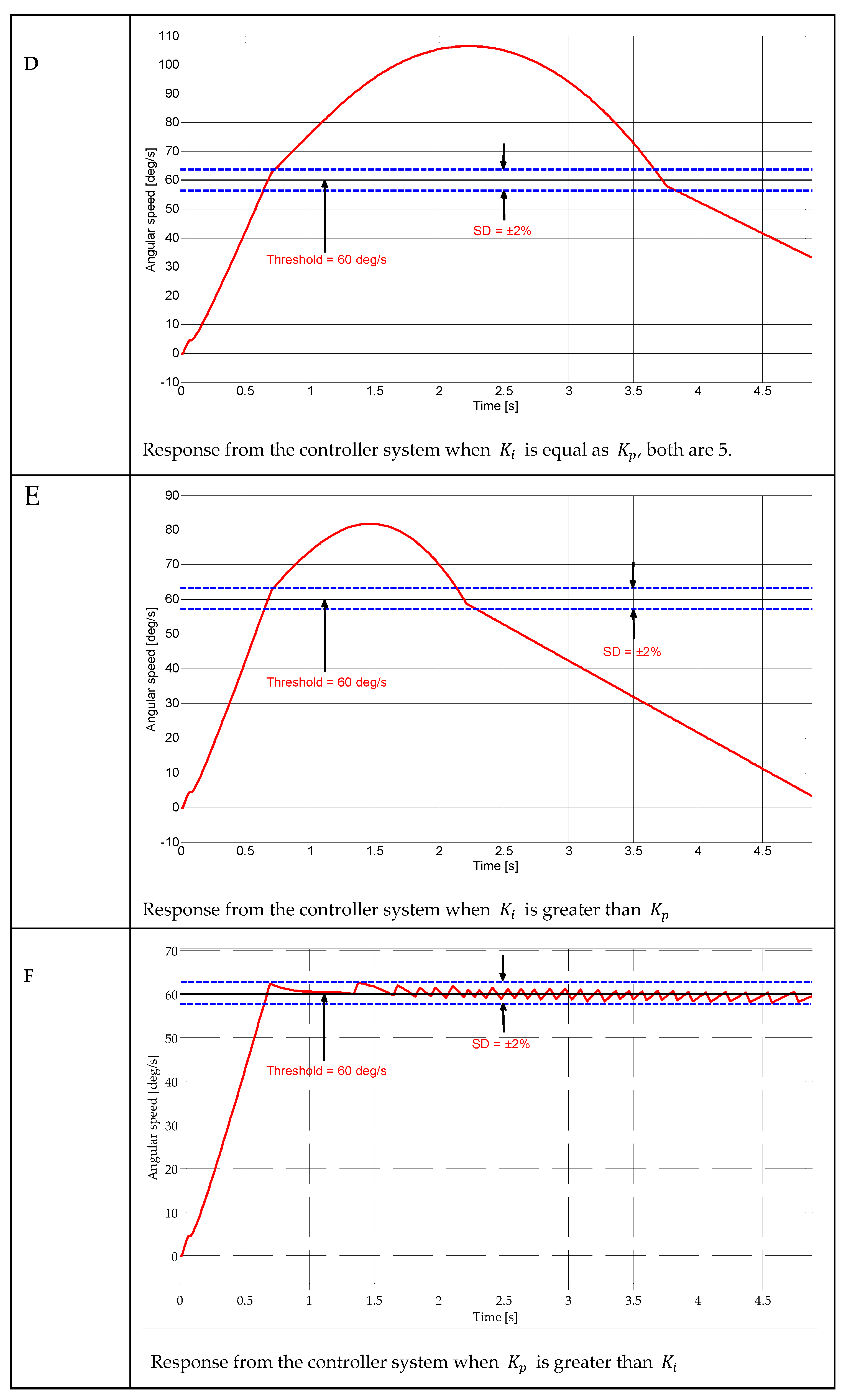
Table 1 shows a 6-case scenario for different values for the controller parameters and applied to the control subsystem seen in Figure 14.
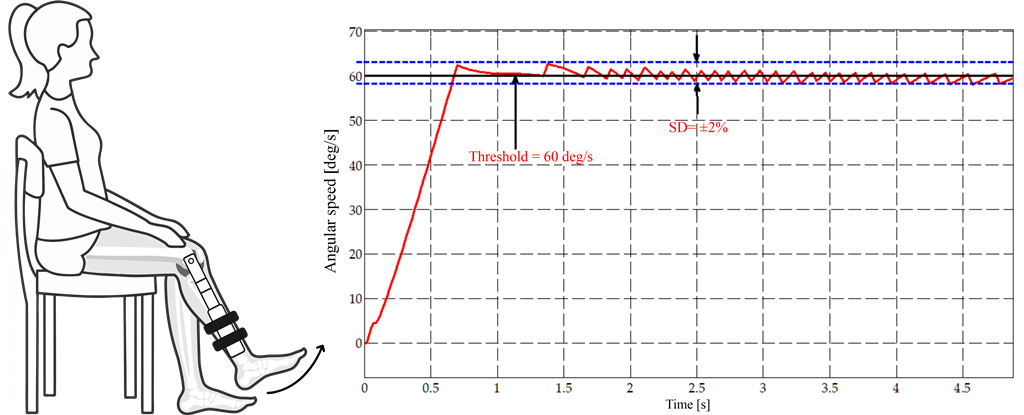
The cases shown on Appendix A (Figure A1) demonstrated that only in and scenario where is greater than the response of the system satisfies the purpose of the speed controller. The following Figure 15 shows the dynamic system response when the scenario F is executed, x-axis represents time in seconds and y-axis represents the angular position in degrees, when the patient’s leg extension speed (red, sloped) exceeds the reference speed limit (black, horizontal) and how the control action forced the leg speed dynamics to reduce each time the threshold is exceeded.
The use of controllers to regulate the speed of human joint movements can generate certain ripples in the speed signal that affect the smoothness of the movements. However, these ripples can be smoothed out by using first and second-order filters, which can be adjusted within the system bandwidth. In this way, sudden accelerations in the human joint can be avoided from interfering with the natural and fluid movement of the body, thus improving the user experience and the precision of controlled movement.
5. Conclusions
After carrying out the development of a technique for a control system that guarantee isokinetic control in rehabilitation devices for the recovery of muscle injuries in human legs, we reach the following conclusions:
Viewing the knee joint and the adjunct sections of the leg as a simplified geometric figure, as triangles, facilitates the understanding of the ligament and muscle junction interactions used in the flexion and extension moments of the leg.
The speed control system used in isokinetic rehabilitation is the key to ensuring the safety and effectiveness of the treatment. This system uses a particle magnetic brake that accurately adjusts the rotation speed of the pulley. For purpose-built speed control systems, computational simulation tools that reflect the dynamic characteristics of the subsystems present in the medical device are necessary, which is reflected in a reduction of physical resources when dealing with testing methods to develop a digital dynamic system comparable to physical device prototypes. The constant rotational speed enabled by the speed control system is essential to accurately measure the torque generated in a determinate time by the human muscles.
The use of the proportional-integrator controller for the speed control system enhance the response of the system to variations taken in early moments and during the time period of the exercise, compared to the application of only a proportional-type control element, resulting in a quick response to both fast and slow changes in control action to alter the patient’s extension speed, without compromising the tendon response, and provides organized and efficient information for further biomedical analysis.
Isokinetic rehabilitation is a technique that promises to be effective in the recovery of leg muscle injuries. The physical variables of elements involved in the mechanical system must be considered, such as the patient’s anthropometric variables, physical variables of the mechanical and electrical components of the device, and the dynamics in which the bodies interact.
Biomedical devices, such as the isokinetic rehabilitation system, are excellent measures devices that help to collect data for patient evolution studies, in addition to the guidelines recommended by medical professionals, it allows for improvement to be observed when a maximum permissible speed is guaranteed during the extension process, which in turn can be observed by analyzing human torque and the force exerted by the anatomical elements responsible for extension. These results could be useful to guide the treatment of patients with muscular leg injuries and to improve the effectiveness of isokinetic rehabilitation in general.
Author Contributions
J.A.P.G. designed the dynamic modeling. S.G-M. assembled the dynamic modeling into Simulink-MATLAB and designed the control system. J.A.P.G. and J.I.G-M. analyzed and interpreted the data. J.A.P.G. wrote the original document draft. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
This project was approved by the “Grupo Interdisciplinario de Innovación Biotecnológica y Transformación Ecosocial – BioNovo” from Universidad del Valle.
Data Availability Statement
Not applicable.
Acknowledgments
We grant acknowledgments to Universidad del Valle for loan the required devices and spaces for measurement and data acquisition of the mechanical and anthropomorphic data used in this study.
Conflicts of Interest
The authors have no conflict of interest to declare.
Appendix A
Figure A1.
Control system scenarios for PI controller parameter selection. The speed limit threshold s established at 60 .
Figure A1.
Control system scenarios for PI controller parameter selection. The speed limit threshold s established at 60 .
References
- J. A. Camacho, C. D. Chamorro, J. A. Sanabria, N. G. Caicedo, and J. I. García, “Implementation of a Service-Oriented Architecture for Applications in Physical Rehabilitation,” Revista Facultad de Ingeniería, vol. 26, no. 46, pp. 113–121, Sep. 2017. [CrossRef]
- L. Parrington and K. Ball, “Biomechanical Considerations of Laterality in Sport,” in Laterality in Sports, Elsevier, 2016, pp. 279–308. [CrossRef]
- M. Mendoza and R. G. Miller, “Muscle Strength, Assessment of,” in Encyclopedia of the Neurological Sciences, Second., Elsevier, 2014, pp. 190–193. [CrossRef]
- H. Andersen, “Motor neuropathy,” in Handbook of Clinical Neurology, vol. 126, 2014, pp. 81–95. [CrossRef]
- T. Kocahan, B. Akınoğlu, A. E. Yilmaz, T. Rosemann, and B. Knechtle, “Intra- and Inter-Rater Reliability of a Well-Used and a Less-Used IsoMed 2000 Dynamometer for Knee Flexion and Extension Peak Torque Measurements in a Concentric Test in Athletes,” Applied Sciences, vol. 11, no. 11, p. 4951, May 2021. [CrossRef]
- J. Riesterer, M. Mauch, J. Paul, D. Gehring, R. Ritzmann, and M. Wenning, “Relationship between pre- and post-operative isokinetic strength after ACL reconstruction using hamstring autograft,” BMC Sports Sci Med Rehabil, vol. 12, no. 1, p. 68, Dec. 2020. [CrossRef]
- Mirion Technologies, “System 4 Dynamometer,” https://m.biodex.com/sites/default/files/documents/brochure_system4_ops-4127.pdf, Sep. 2022.
- inc Computer Sports Medicine, “The HUMAC NORM,” https://humacnorm.com/humac-norm/, 2022.
- V. van Tittelboom et al., “Reliability of Isokinetic Strength Assessments of Knee and Hip Using the Biodex System 4 Dynamometer and Associations With Functional Strength in Healthy Children,” Front Sports Act Living, vol. 4, Feb. 2022. [CrossRef]
- R. W. Bohannon, “Isokinetic testing of muscle strength of older individuals post-stroke: An integrative review,” Isokinet Exerc Sci, vol. 28, pp. 303–316, 2020. [CrossRef]
- L. T. , G. N. , & K. M. Vogrin M., “Peak Torque Comparison between SMM iMoment and Biodex System Pro 4 Isokinetic Dynamometers,” Acta Medico-Biotechnica, vol. 13, no. 2, pp. 46–54, Nov. 2021.
- M. T. Gross, G. M. Huffman, C. N. Phillips, and J. A. Wray, “Intramachine and Intermachine Reliability of the Biodex and Cybex ® II for Knee Flexion and Extension Peak Torque and Angular Work,” Journal of Orthopaedic & Sports Physical Therapy, vol. 13, no. 6, pp. 329–335, Jun. 1991. [CrossRef]
- J. B. de Araujo Ribeiro Alvares et al., “Inter-machine reliability of the Biodex and Cybex isokinetic dynamometers for knee flexor/extensor isometric, concentric and eccentric tests,” Physical Therapy in Sport, vol. 16, no. 1, pp. 59–65, Feb. 2015. [CrossRef]
- T. C. Valovich-mcLeod, S. J. Shultz, B. M. Gansneder, D. H. Perrin, and J. M. Drouin, “Reliability and validity of the Biodex system 3 pro isokinetic dynamometer velocity, torque and position measurements,” Eur J Appl Physiol, vol. 91, no. 1, pp. 22–29, Jan. 2004. [CrossRef]
- C. M. Powers, S. R. Ward, M. Fredericson, M. Guillet, and F. G. Shellock, “Patellofemoral Kinematics During Weight-Bearing and Non-Weight-Bearing Knee Extension in Persons With Lateral Subluxation of the Patella: A Preliminary Study,” Journal of Orthopaedic & Sports Physical Therapy, vol. 33, no. 11, pp. 677–685, Nov. 2003. [CrossRef]
- C. , Zooker, R. , Pandarinath, MJ. , Kraeutler, M. Ciccotti, SB. ; Cohen, and P. Deluca, “Clinical measurement of patellar tendon: accuracy and relationship to surgical tendon dimensions.,” Rothman Institute Faculty Papers, vol. 32, Jul. 2013.
- R. M. Nunley, D. Wright, J. B. Renner, B. Yu, and W. E. Garrett, “Gender Comparison of Patellar Tendon Tibial Shaft Angle with Weight Bearing,” Research in Sports Medicine, vol. 11, no. 3, pp. 173–185, Jul. 2003. [CrossRef]
- Rui‘an Guoxin Electronic Equipment Factory, “GXFZ - A series solenoid powder brake,” http://www.gx-dz.cn/en/872.htm, 2022.
- Ali HI. and Saeed AH., “Robust Tuning of PI-PD Controller for Antilock Braking System,” Al-Nahrain Journal for Engineering Sciences (NJES) , vol. 20, no. 4, pp. 983–995, 2017.
- D. Izci and S. Ekinci, “Comparative Performance Analysis of Slime Mould Algorithm For Efficient Design of Proportional–Integral–Derivative Controller,” Electrica, vol. 21, no. 1, pp. 151–159, Jan. 2021. [CrossRef]
Figure 1.
Rehabilitation device configured for a lower limb rehabilitation system from Universidad del Valle [1]. (1) Control screen, (2) Emergency stop, (3) Foot pedal, (4) Support structure, (5) Chassis, and (6) Magnetic brake.
Figure 1.
Rehabilitation device configured for a lower limb rehabilitation system from Universidad del Valle [1]. (1) Control screen, (2) Emergency stop, (3) Foot pedal, (4) Support structure, (5) Chassis, and (6) Magnetic brake.
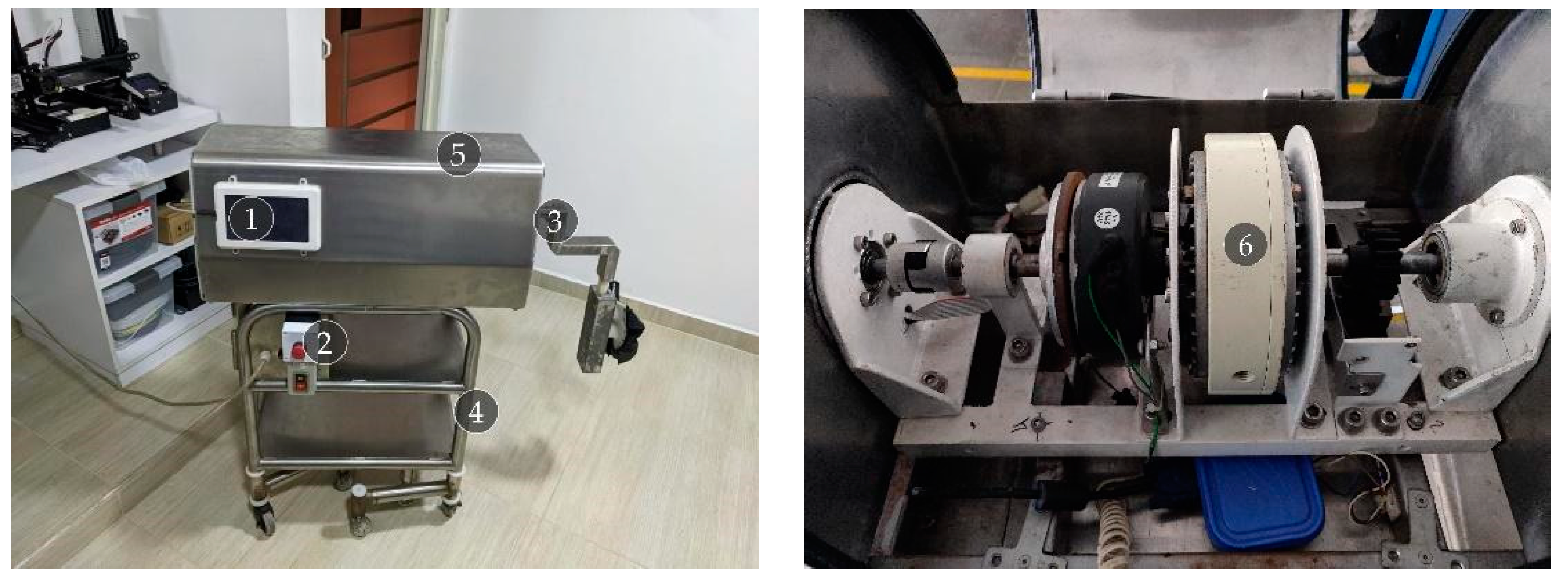
Figure 2.
The behavior of the lower limb during extension a. Angular position at the knee joint for uncontrolled extension. A tendency for linear growth of extension can be observed over time from 0 radians to approximately 1.5 radians. b. Angular speed at the knee joint during an uncontrolled leg extension. Multiple peaks can be observed during the extension of the leg reaching approximately 1.5 radians per second at the maximum speed segment.
Figure 2.
The behavior of the lower limb during extension a. Angular position at the knee joint for uncontrolled extension. A tendency for linear growth of extension can be observed over time from 0 radians to approximately 1.5 radians. b. Angular speed at the knee joint during an uncontrolled leg extension. Multiple peaks can be observed during the extension of the leg reaching approximately 1.5 radians per second at the maximum speed segment.
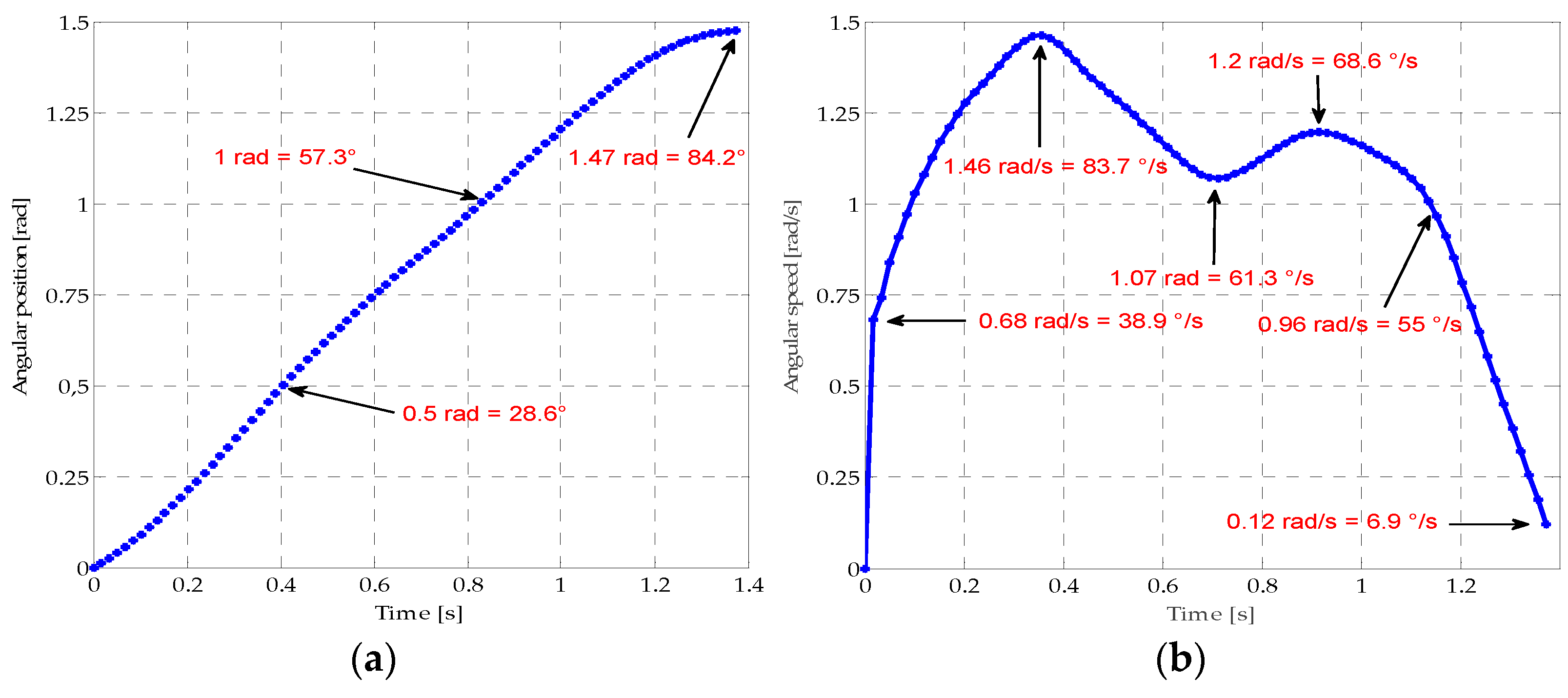
Figure 3.
Behavior of the lower limb during extension a. Angular position at the knee joint for ideal controlled extension. A better tendency for linear growth in the extension over time can from 0 rad to approximately 1.5 rad is observed. b. Angular speed at the knee joint during an ideal controlled leg extension. A linear growth trend in extension speed is observed at the onset of motion, reaching stability at approximately 1.1
Figure 3.
Behavior of the lower limb during extension a. Angular position at the knee joint for ideal controlled extension. A better tendency for linear growth in the extension over time can from 0 rad to approximately 1.5 rad is observed. b. Angular speed at the knee joint during an ideal controlled leg extension. A linear growth trend in extension speed is observed at the onset of motion, reaching stability at approximately 1.1
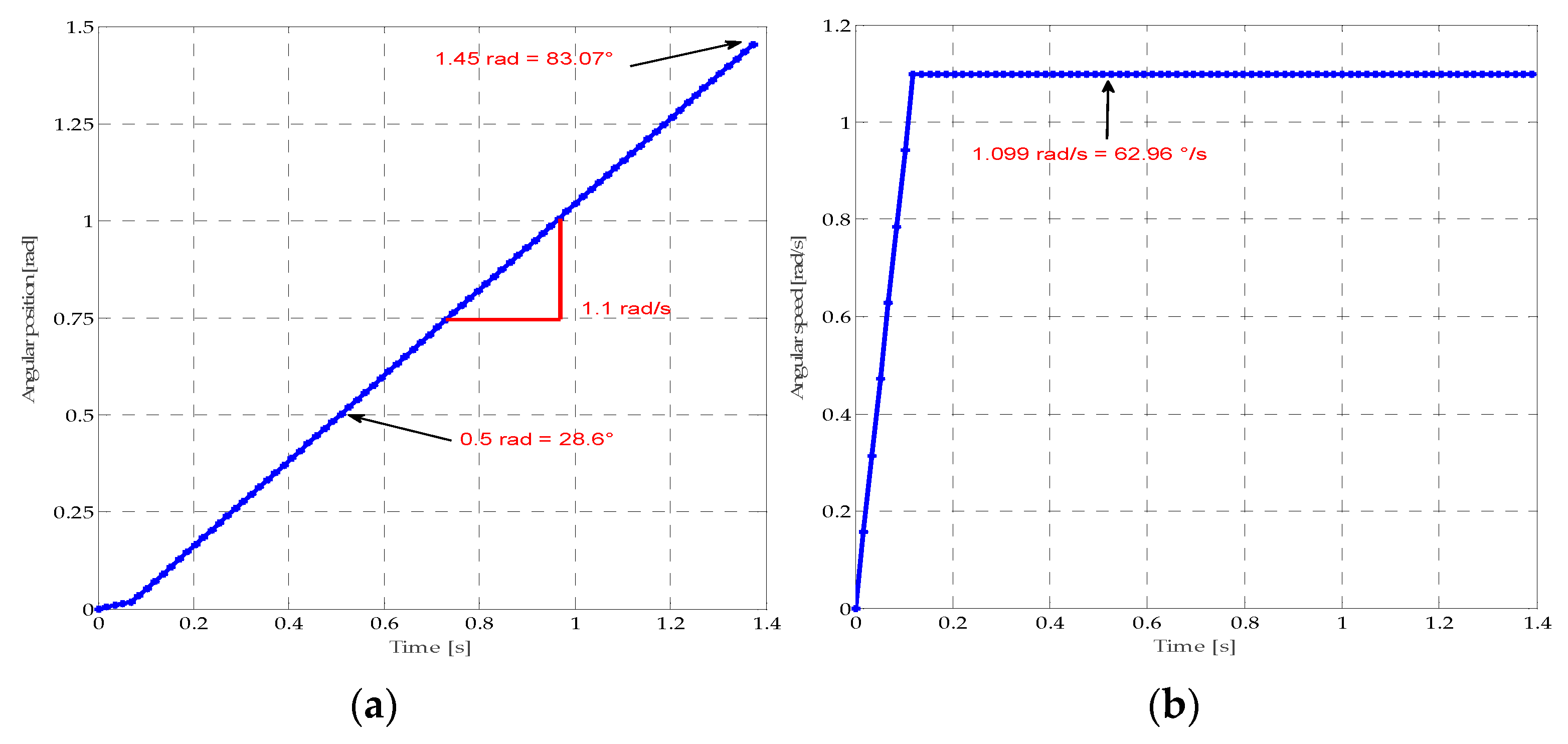
Figure 4.
Torques are associated with knee joint extension.
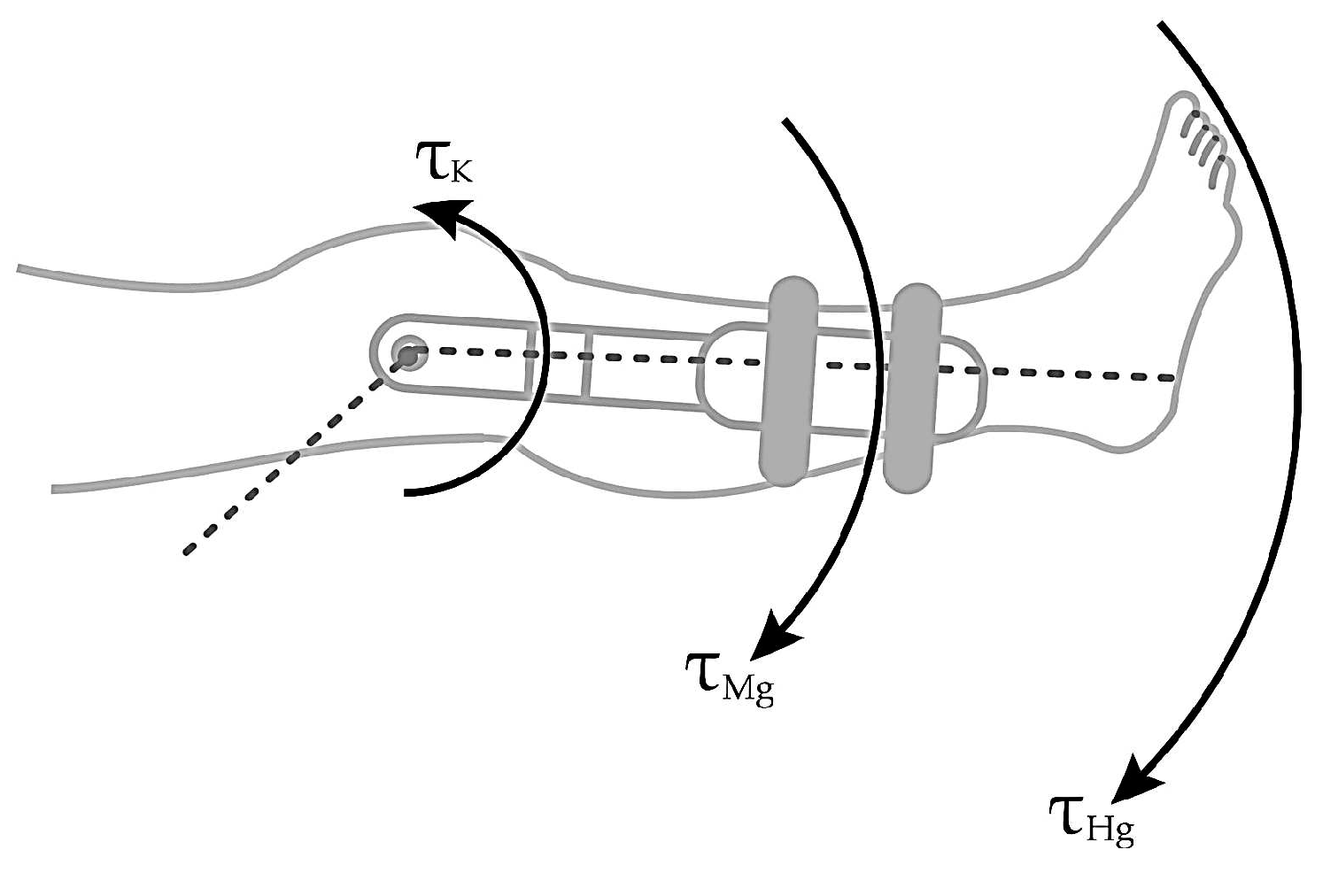
Figure 5.
The dynamics of a lower limb during the extension. a. Torques in the knee joint for maximum extension. b. Diagram of forces and distances in the human leg.
Figure 5.
The dynamics of a lower limb during the extension. a. Torques in the knee joint for maximum extension. b. Diagram of forces and distances in the human leg.
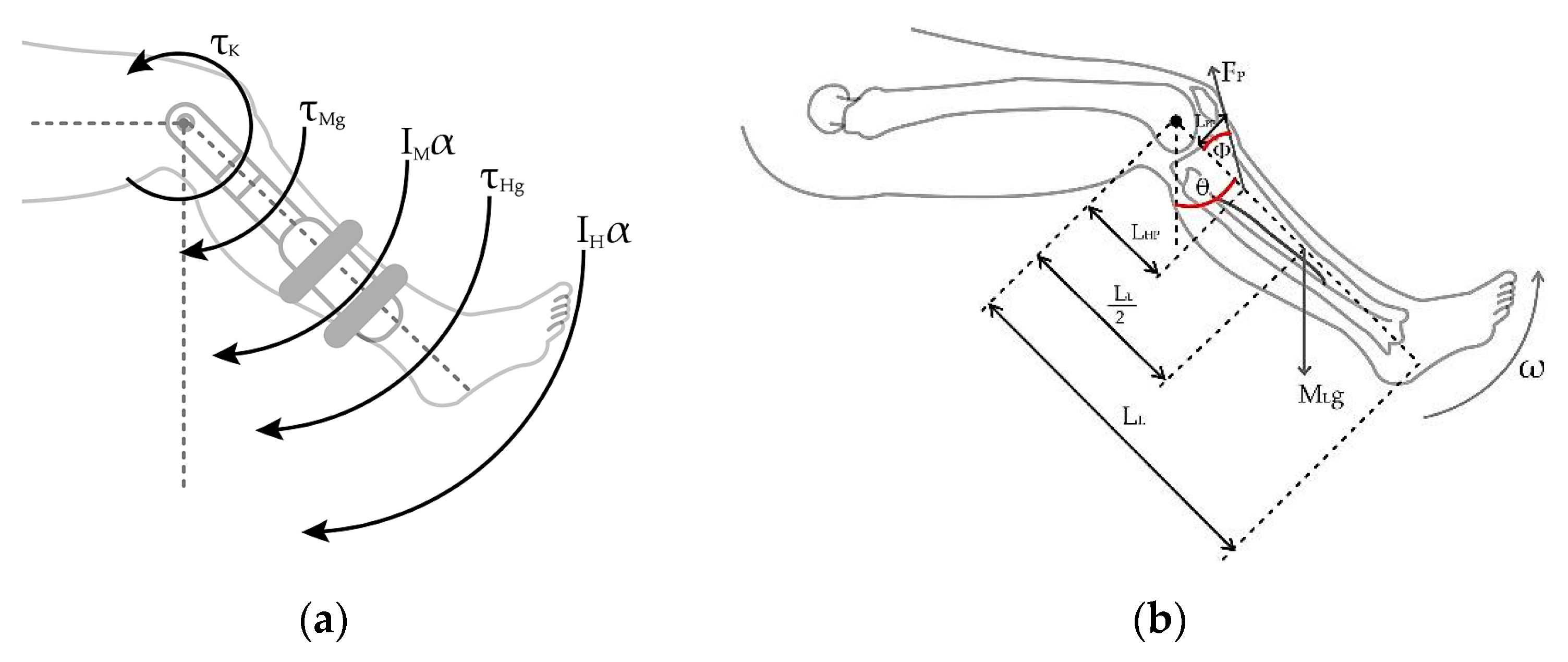
Figure 6.
Presence of the patellar tendon and the separation angle between the tibia and the tendon.
Figure 6.
Presence of the patellar tendon and the separation angle between the tibia and the tendon.
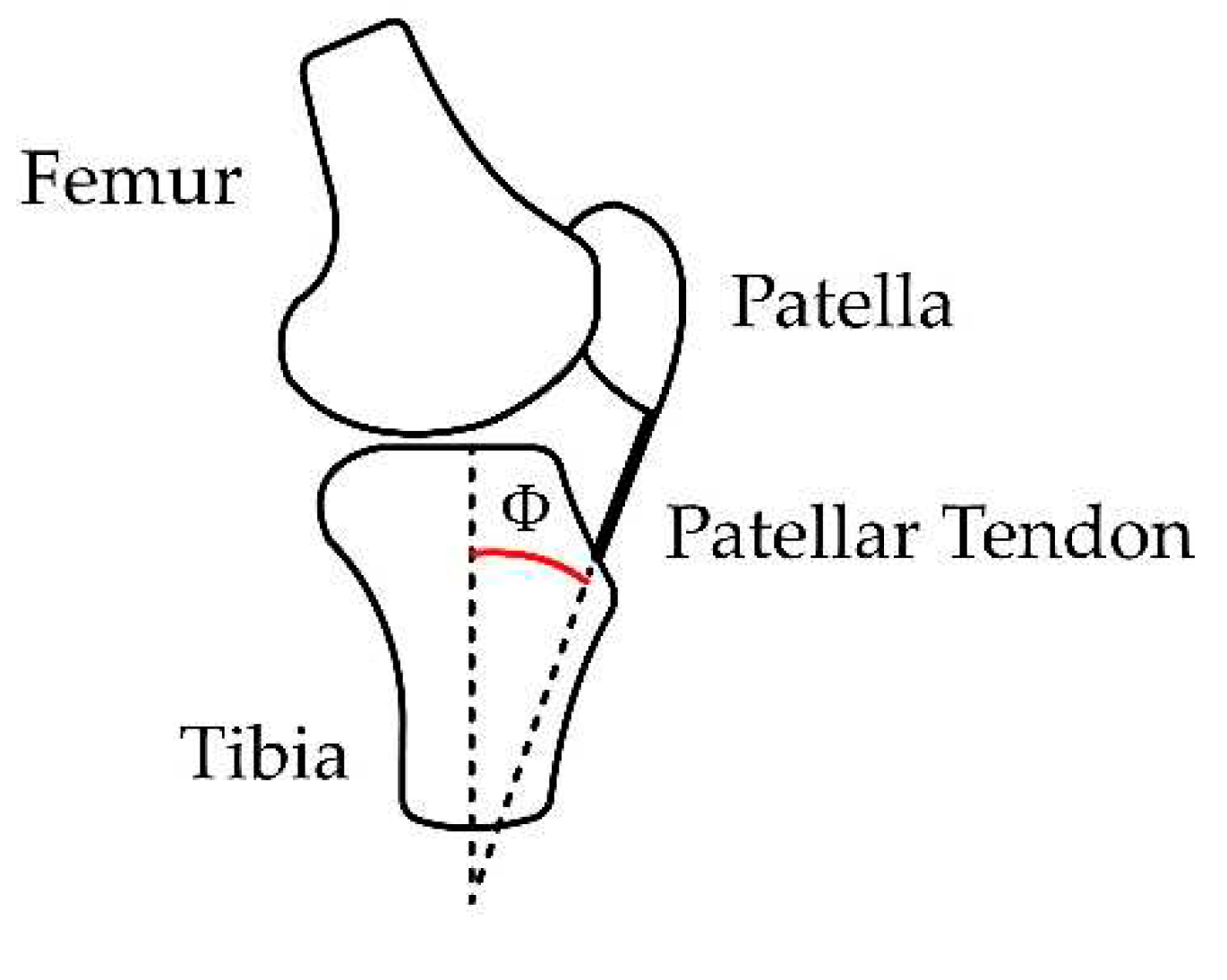
Figure 7.
Measurements and distances for calculation of measured in radians due to the leg extension. a. Relation between with respect to the leg extension angle. b. location regarding the tendon length during the leg extension. Variation of according to the leg extension from 0 to 90°.
Figure 7.
Measurements and distances for calculation of measured in radians due to the leg extension. a. Relation between with respect to the leg extension angle. b. location regarding the tendon length during the leg extension. Variation of according to the leg extension from 0 to 90°.
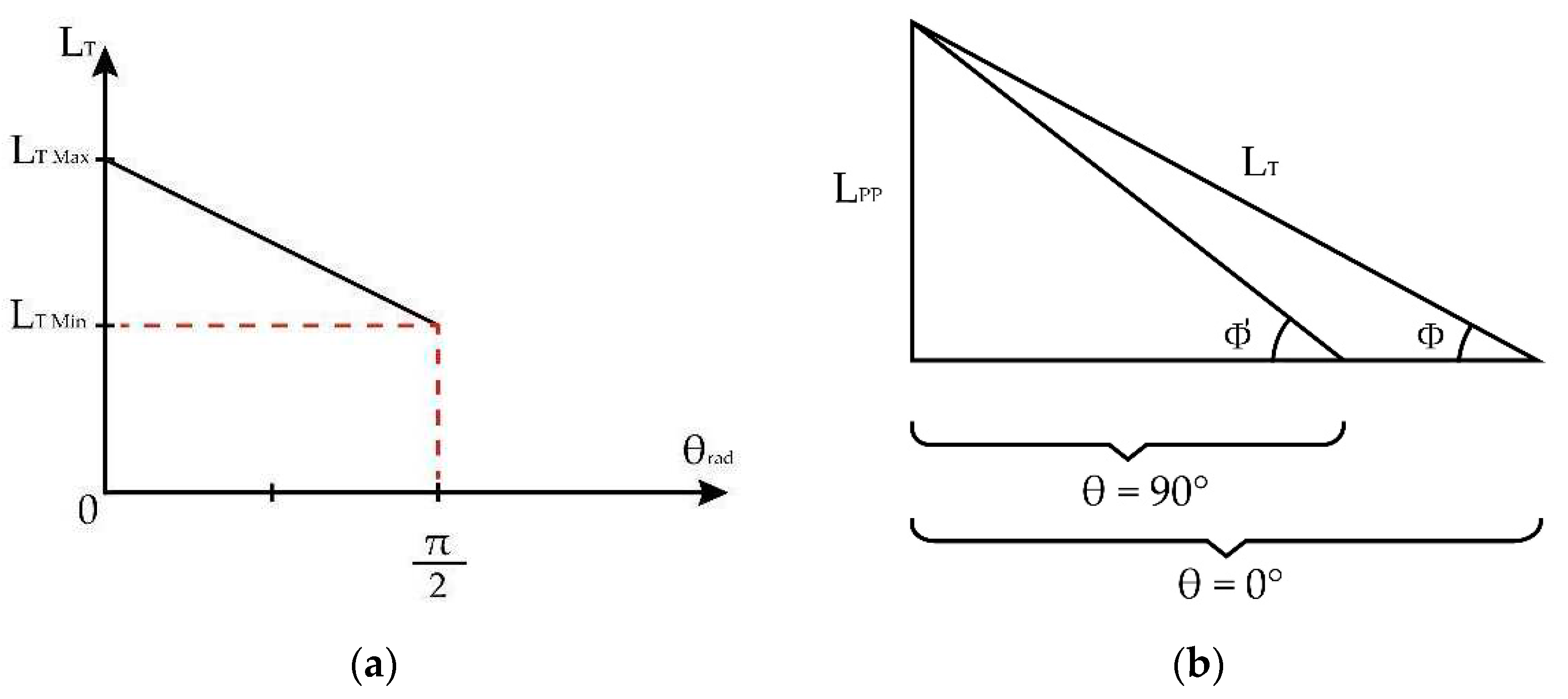
Figure 8.
View of the triangle formed by the patellar tendon at the positions of maximum extension, (1.57 radians), and reference flexion, (0 radians).
Figure 8.
View of the triangle formed by the patellar tendon at the positions of maximum extension, (1.57 radians), and reference flexion, (0 radians).
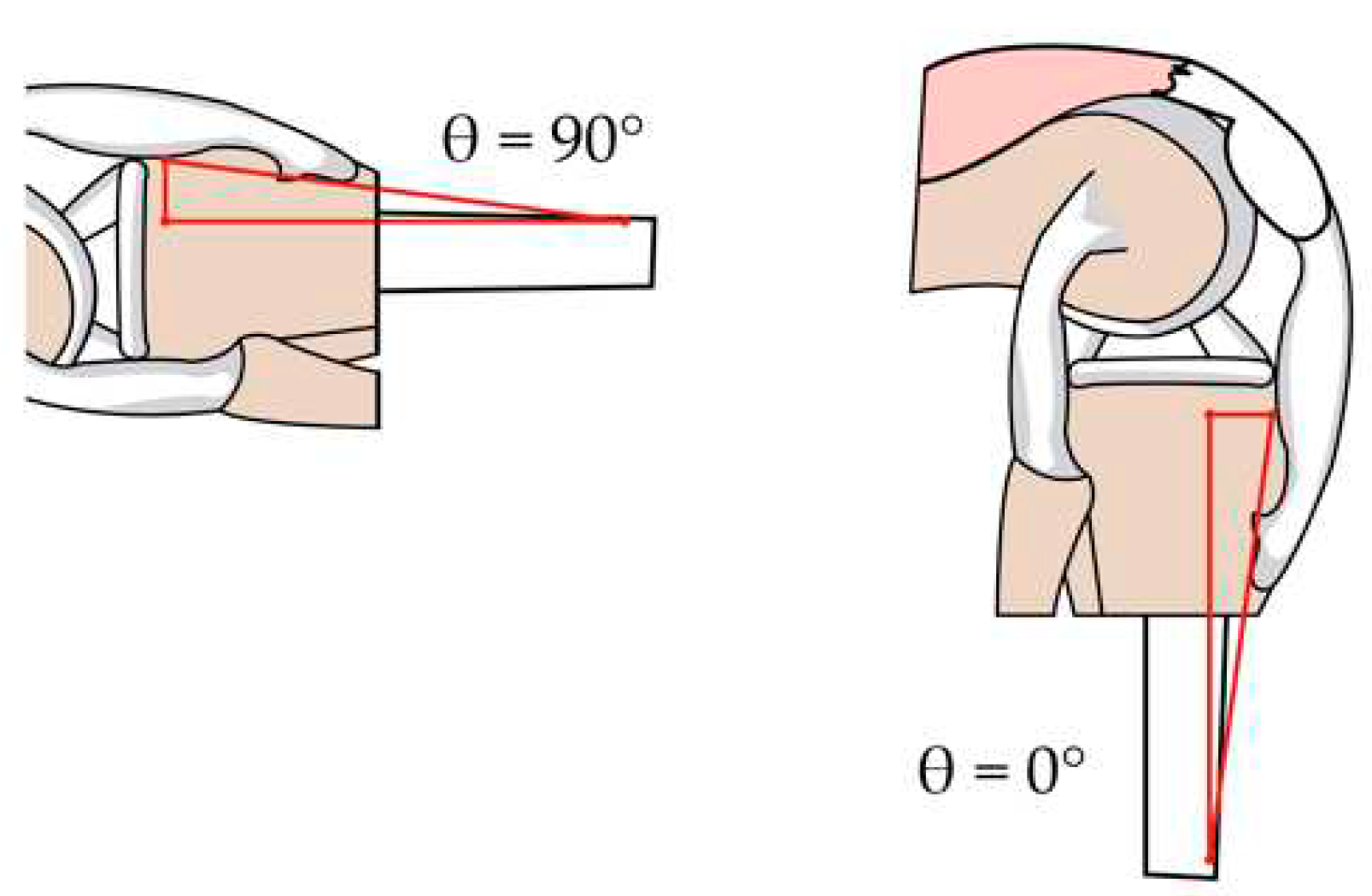
Figure 9.
Cartesian components with respect to patellar tendon force.

Figure 10.
Reduction of components for human torque calculation.
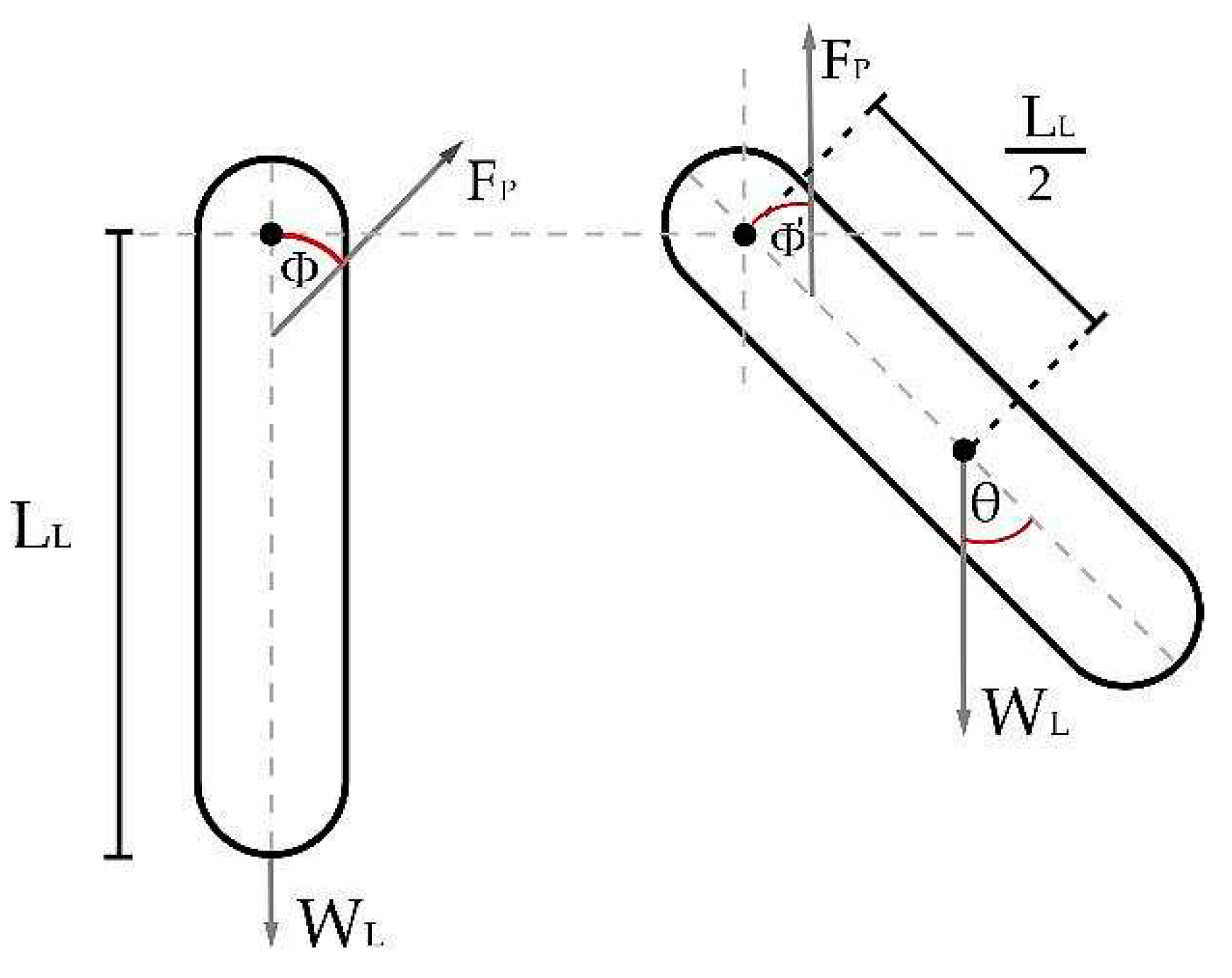
Figure 11.
Average current percentage vs. average torque percentage for a GXFZ-B-6 model [18].
Figure 11.
Average current percentage vs. average torque percentage for a GXFZ-B-6 model [18].
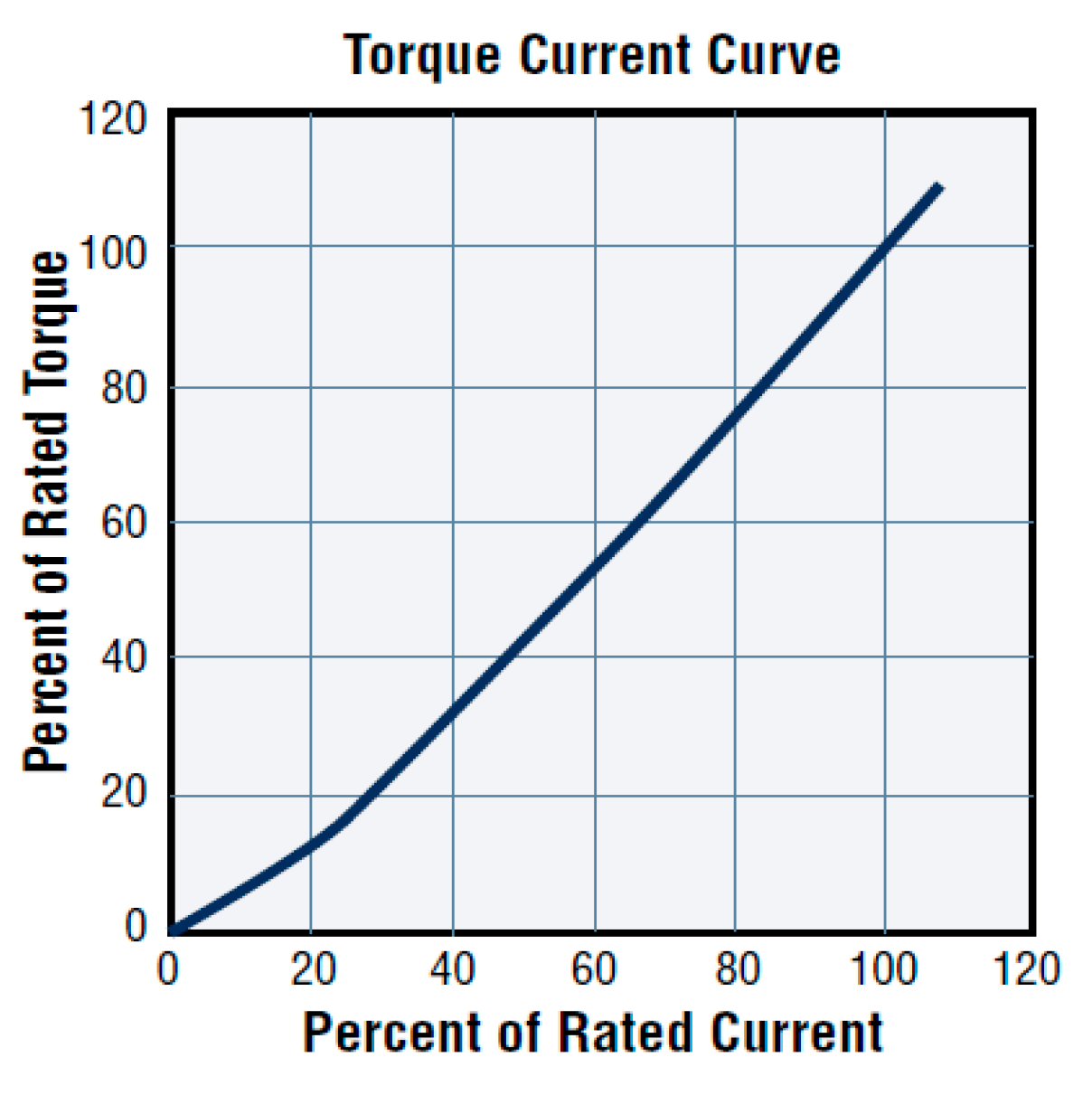
Figure 12.
Patient’s leg attached to the rehabilitation device.
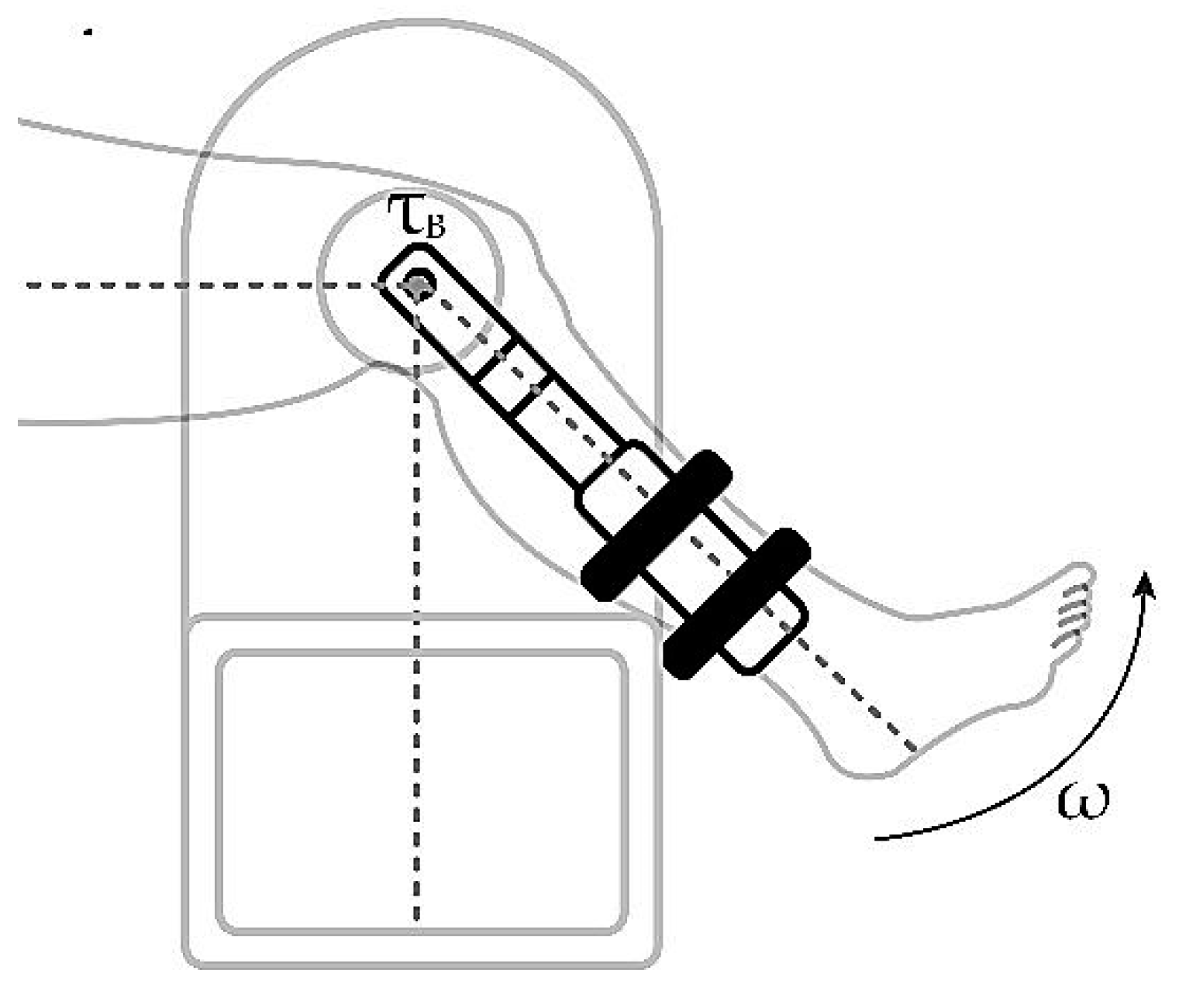
Figure 13.
Dynamic modeling for the human-machine system in closed-loop.
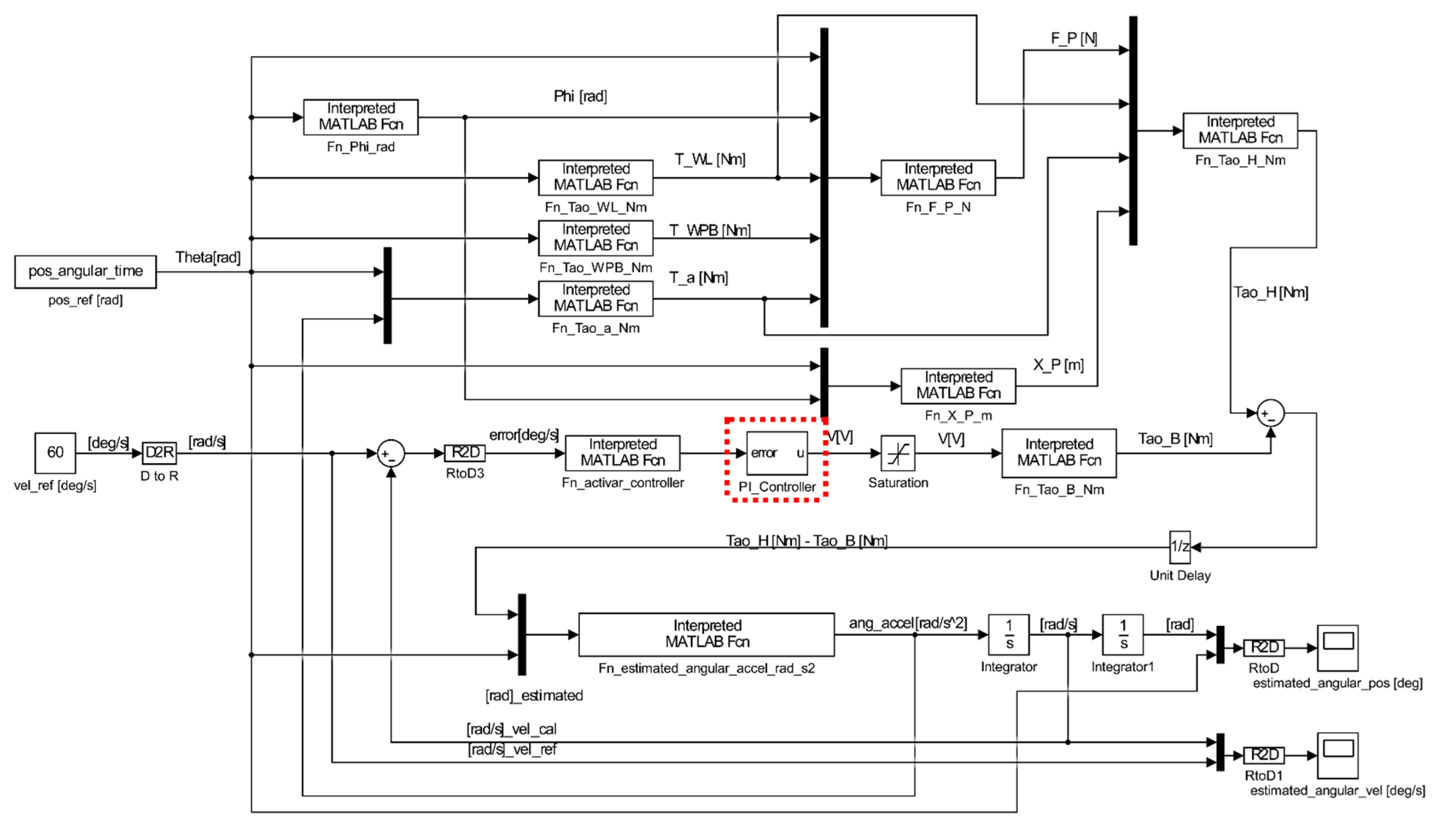
Figure 14.
Control system implemented with proportional and integrative control.
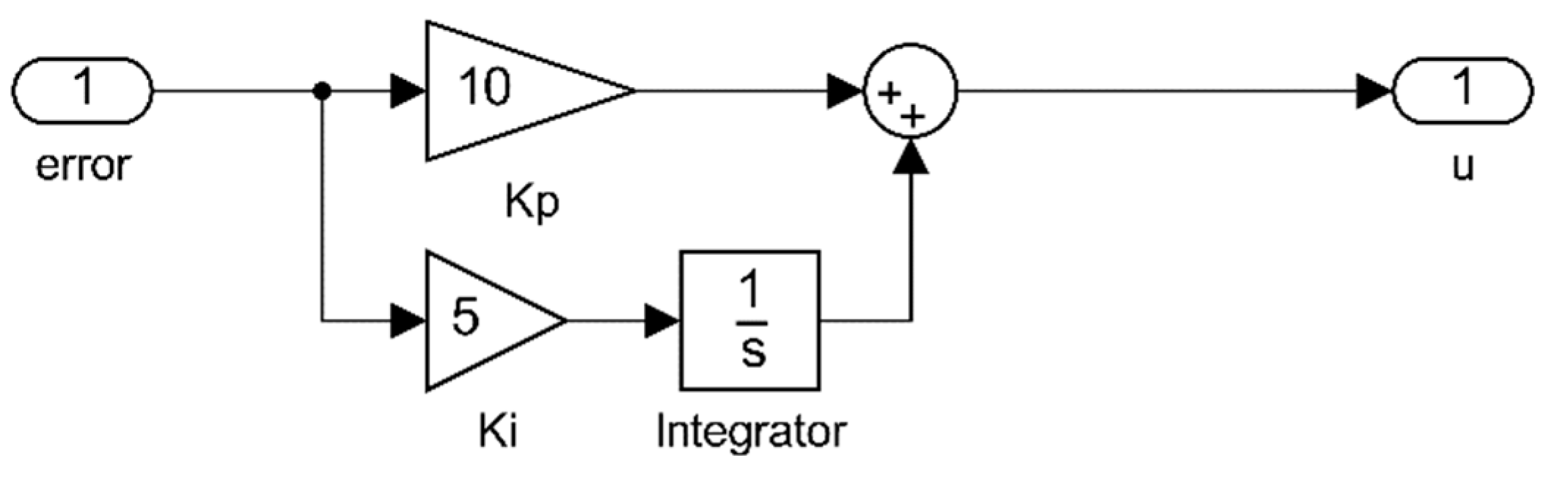
Figure 15.
Time response of the dynamic system when the controller A is applied.
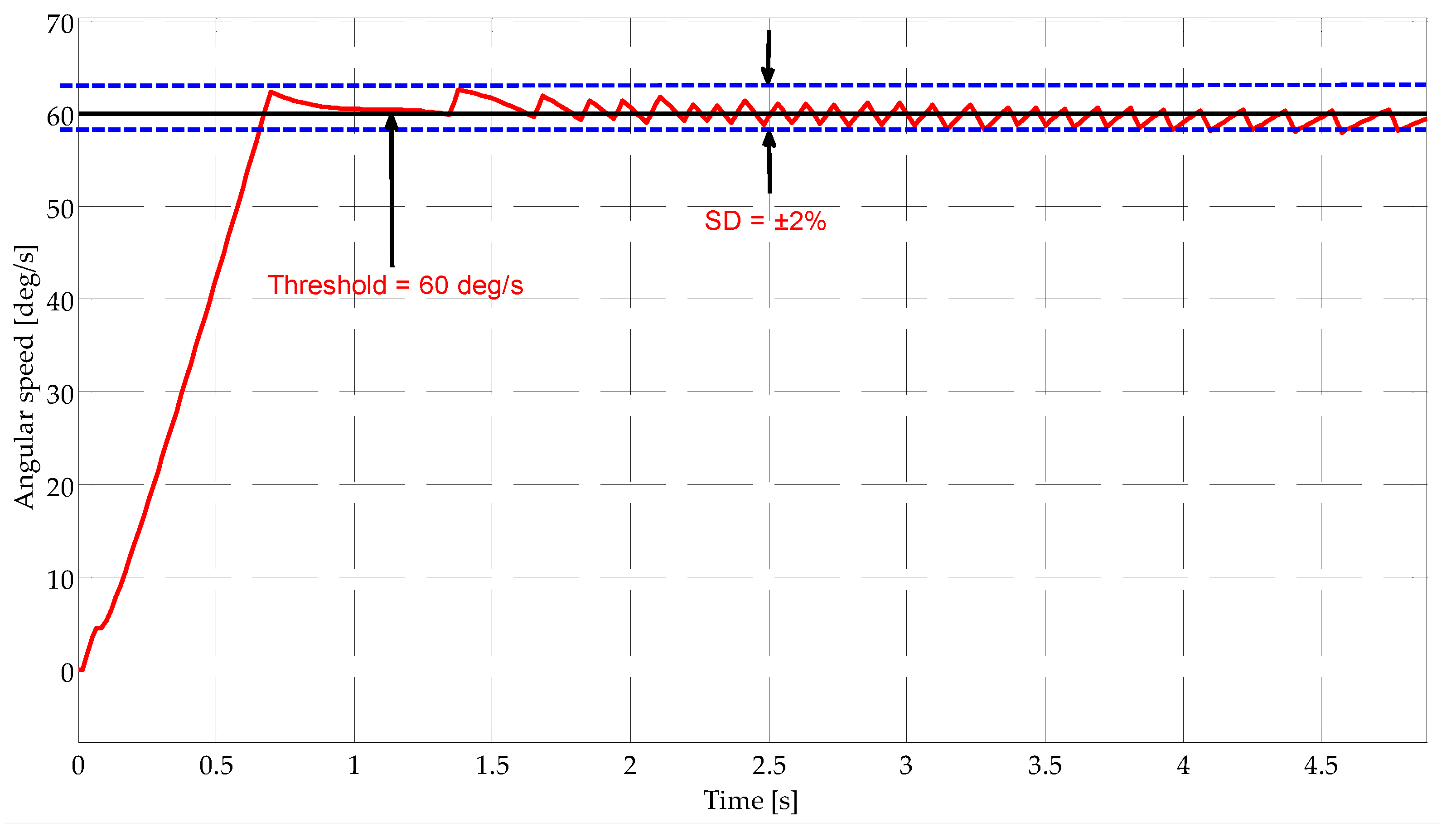

Table 1.
Different parameters implemented for the control system seen in Figure 14.
Table 1.
Different parameters implemented for the control system seen in Figure 14.
| Case | ||
|---|---|---|
| A | 0 | 0 |
| B | 5 | 0 |
| C | 0 | 5 |
| D | 5 | 5 |
| E | 5 | 10 |
| F | 10 | 5 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



