
Submitted:
28 April 2023
Posted:
29 April 2023
You are already at the latest version
Abstract
Mechanical bowel obstruction is a common symptom for admission to emergency services, diagnosed annually in more than 300,000 patients in the States, from whom 51% will undergo emergency laparotomy. This condition is associated with serious morbidity and mortality, but it also causes a high financial burden due to long hospital stay. The EUPEMEN project aims to incorporate the expertise and clinical experience of national clinical specialists into development of perioperative rehabilitation protocols. Providing special recommendations for all aspects of patient perioperative care and the participation of diverse specialists, the EUPEMEN protocol for bowel obstruction, as presented in the current paper, aims to provide faster postoperative recovery and reduce length of hospital stay, postoperative morbidity and mortality rate.
Keywords:
bowel obstruction
; perioperative care
; care program
; surgical rehabilitation
; EUPEMEN project
1. Introduction
Surgery is indicated to cure or palliate numerous physical ailments. However, surgery leads to adverse effects that affect daily living by impairing quality of life and increase the cost of health system because of longer hospitalization time of the patient. The goal of the multimodal surgical rehabilitation or enhanced recovery after surgery is the application of a series of perioperative procedure measures and strategies aimed at patients who are going to undergo a surgical procedure with the objective of reducing secondary stress caused by the surgical intervention and thus achieve enhanced recovery of the patient and decrease complications and mortality [1, 2]. These care programs are based on scientific evidence, encompass all aspects of patient care, and require multidisciplinary management, with the participation of diverse specialists. Starting at the diagnosis, their aim is to recognize patients’ individual needs, to optimize their treatment before, during and after surgery [1, 2].
In order to implement these programs at hospitals in Europe, 5 partners with health and university profile of 4 different EU countries have created the EUPEMEN project. The objective is to prepare a guideline with the protocols to be implemented by the multidisciplinary specialists involved. The Eupemen project has been carried out by Fundación Instituto de Investigación Sanitaria Aragón-IISA as coordinator and Azienda Unità Sanitaria Locale Ferrara – AUSLFE, Univerzita Karlova – CUNI, Universidad Miguel Hernández de Elche – UMH and “G. Papanikolaou – GPAP” General Hospital of Thessaloniki as partners. The main objective of the EUPEMEN project is to create and disseminate protocols for multimodal surgical rehabilitation based on the experience and previous knowledge of the five partners belonging to the health field and higher education. The technical activities of the project included the preparation of the EUPEMEN Multimodal Rehabilitation manual with the protocols of 6 different modules: Bariatric Surgery, Oesophageal Surgery, Gastric Cancer Surgery, Colon Surgery, Hepatobiliary Surgery, and Urgent abdominal surgery, including appendectomy and small bowel obstruction (SBO).
2. Bowel Obstruction
Bowel obstruction is one of the most common surgical emergencies worldwide and accounts for about 15% of cases requiring admission for abdominal pain and constitute about 20% of acute surgical cases [3,4]. SBO accounts for the majority of cases with a percentage of about 75-80% while the rest 20-25% are caused by large bowel obstruction [5].
SBO has been recognized as a medical emergency from the ancient years as descriptions of the disease date back even in the era of ancient Egypt and ancient Greece [6,7]. It is a quiet common emergency medical issue as about 2-4% of abdominal pain cases seen in the emergency department and a percentage as high as 12-16% of surgical admissions are due to SBO [6,8]. In developed countries the most common cause of SBO are adhesions from previous abdominal surgery accounting for 65-78% of the cases, while less common but still not so rare causes are hernias and neoplasms accounting for 10% and 5% respectively [6,9,10]. While the classical dogma of surgery “never let the sun set on a small bowel obstruction” has been challenged the last years and there has been increased focus on successful nonoperative management including the gastrografin challenge [8,9] surgery remains a great part of SBO management and SBO accounts for 20% of all emergency surgical procedures and more than 300,000 operations are performed annually for SBO in the U.S.A. [6,11].
For the less common large bowel obstruction, the main cause is neoplasm which account for about 50 - 60%, with volvulus found in 10 - 20% and diverticula in another 10 - 20% [3-5]. Contrary to SBO, most cases of large bowel obstruction will require surgical treatment as the majority of cases won’t resolve by observation in combination with medical treatment [3-5].
3. Enhanced Recovery after Surgery (ERAS)
Enhanced Recovery After Surgery (ERAS) is a modern approach to perioperative care of surgical patients that aims to reduce surgical stress and thus improve recovery of patients [1, 2]. Enhanced recovery protocols aim to ensure that patients are in the best possible conditions before surgery, receive the most optimal surgery and anaesthesia and postoperative care [1, 2]. Implementation of enhanced recovery protocols relies on the close collaboration of all specialists participating in the perioperative process, as well as of the actual patients and their relatives [1, 2]. The concept of improving recovery after surgery was introduced in the 1990s by Professor Henrik Kehlet [1]. The original protocols were written for colorectal surgery [12,13]. The protocols have since been shown in several randomized clinical trials and meta-analyses to reduce postoperative complications, length of hospitalization, improve clinical recovery parameters and to reduce hospital costs [14-19]. Enhanced recovery protocols have now been developed for a wide range of surgical fields, including foregut surgery, pancreatobiliary surgery, gynecological surgery, and urology [14-19]. In 2015, in a further attempt to improve postoperative outcomes, the Intensified Recovery in Abdominal Surgery (Via RICA) protocol was developed and published [20]. Via RICA is a detailed enhanced recovery protocol for abdominal surgery based on interdisciplinary consensus. An update for the Via RICA has since been developed, which includes several other surgical disciplines other than abdominal [21]. Promoting this concept further a protocol on SBO has been developed by the EUPEMEN project which can be found also online (https://eupemen.eu/wp-content/uploads/2022/10/Eupemen-Protocol-Bowel-Obstruction.pdf).
4. The EUPEMEN Bowel Obstruction Protocol (Figure 1)
4.1. Preoperative Phase
In the preoperative phase of the management of a patient with SBO, which is performed by the surgeon and the anaesthesiologist, it is important to complete the following routine preoperative assessment that includes physical examination, abdominal X-ray and full blood laboratory analysis including C-reactive protein (CRP).
Also, clinical scoring systems should be implemented for the assessment of elderly patients. Fragility scores should be used such as the Modified Frailty Index and VIG Express and the Beers criteria should be reviewed for preventing delirium in adults over 65 years old. Despite the fact that there is no perfect score, any score is better than none [22-26].
Normothermia should be ensured preoperatively in all patients but especially in frail patients by using heat blankets [27-30]
One of the most crucial issues is perioperative glycaemic control. Specifically, for diabetic patients the local hospital protocols for diabetics undergoing surgery should be used while in patients at risk of developing insulin resistance (obese and elderly patients) and in surgeries lasting more than one hour, blood glucose levels higher than 180 mg/dL should be avoided [31-34].
Contrary to the protocols in non-emergency surgery nasogastric tube placement is recommended in all cases, while urinary catheterization should be avoided and be used only if necessary.
Perioperative care bundles to prevent surgical site infections are highly recommended and antibiotic prophylaxis should be given in all cases and the type of antibiotics should be chosen according to the local hospital policy [36-39].
Despite the emergent character of the procedure informed consent is required and the patient should be fully informed of the planned procedure and its potential complications, as it decreases hospital stay and allows early discharge. Competent patients should give signed informed consent [40-42].
4.2. Intraoperative Phase
In the preoperative phase of the management of a patient with SBO, which is performed by the surgeon, the anaesthesiologist and the nurse the WHO surgical checklist should be used as it increases patient safety [43-46].
Regarding the anaesthesiologist approach the intraoperative elements of the EUPEMEN protocol are routine intraoperative monitoring, which should include non-invasive blood pressure measurement, electrocardiogram with 5 leads (V5 and DII recommended), fraction of inspired oxygen (FiO2), pulse oximetry (with % O2 Saturation), capnography (EtCO2) [47,48], central temperature [49-51], intraoperative blood glucose and fluid therapy balance, rapid sequence induction for anaesthesia and no face mask ventilation in order to reduce aspiration of gastric contents, perioperative oxygenation with a fraction of inspired oxygen between 0.6 and 0.8. Moreover, goal-directed fluid therapy using non-invasive hemodynamic monitoring systems should be used. If such systems are not available, balanced solutions should be given continuously according to the surgical approach: 3-5 ml/kg/h for laparoscopy and 5-7 ml/kg/h for laparotomy [52-55]. Also, epidural analgesia should be used in open surgery [56,57] and prophylaxis of postoperative nausea and vomiting should be done by the administration of antiemetic therapy according to the Apfel score [58-60].
Regarding the surgical elements of the intraoperative component of the EUPEMEN protocol for SBO minimally invasive approaches should only be used in highly selected cases according to the experience of the surgeon. In most cases open surgery should be preferred and abdominal drains should be avoided as much as possible [61-64]. Furthermore, urinary catheterization should be avoided and be used only if necessary [67-69].
In the concept of the multidisciplinary management of those patients it is the responsibility of the whole team to achieve perioperative glycaemic control. For diabetic patients’ local hospital protocols for diabetics undergoing surgery should be used while in patients at risk of developing insulin resistance (obese and elderly patients) and in surgeries lasting more than one hour, blood glucose levels higher than 180 mg/dL must be avoided [70-72]. Normothermia should be maintained throughout the procedure by the use of thermal blankets and heated fluids [30, 73-77] and thromboembolic prophylaxis consisting of compression stockings or intermittent compression and low-molecular weight heparin should be given according to the local hospital policy [78-82]. Last, but not least perioperative care bundles to prevent surgical site infections are recommended.
4.3. Immediate Postoperative Phase
In the immediate postoperative phase of the management of a patient with SBO, which is performed by the surgeon, the anaesthesiologist and the nurse active temperature maintenance is mandatory and body temperature should be routinely measured with the goal to prevent hypothermia [73-77]. Oxygen saturation should be routinely measured to prevent hyposaturation and if needed oxygen therapy should be used. In the concept of the multidisciplinary management of those patients it is the responsibility of the whole team to achieve perioperative glycaemic control. For diabetic patients, local hospital protocols for diabetics undergoing surgery should be used while in patients at risk of developing insulin resistance (obese and elderly patients) and in surgeries lasting more than one hour, blood glucose levels higher than 180 mg/dL must be avoided. Thromboembolic prophylaxis consisting of compression stockings or intermittent compression and low-molecular weight heparin should be given according to the local hospital policy.
Regarding analgesia it is mandatory to implement opioid-sparing multimodal analgesia [83-86] and a restrictive fluid therapy protocol. Early mobilisation is one of the goals of the protocol in the immediate postoperative phase and the patients should sit up by two hours after surgery and should begin ambulation 8 hours after surgery with respect to night time hours for sleeping [87-92].
In terms of feeding the patient should be kept nil per os while the withdrawal of the nasogastric tube should be assessed at 12 hours after surgery and the removal of the urinary catheter, if it has been used, should be assessed 12 hours after surgery.
4.4. First Postoperative Day
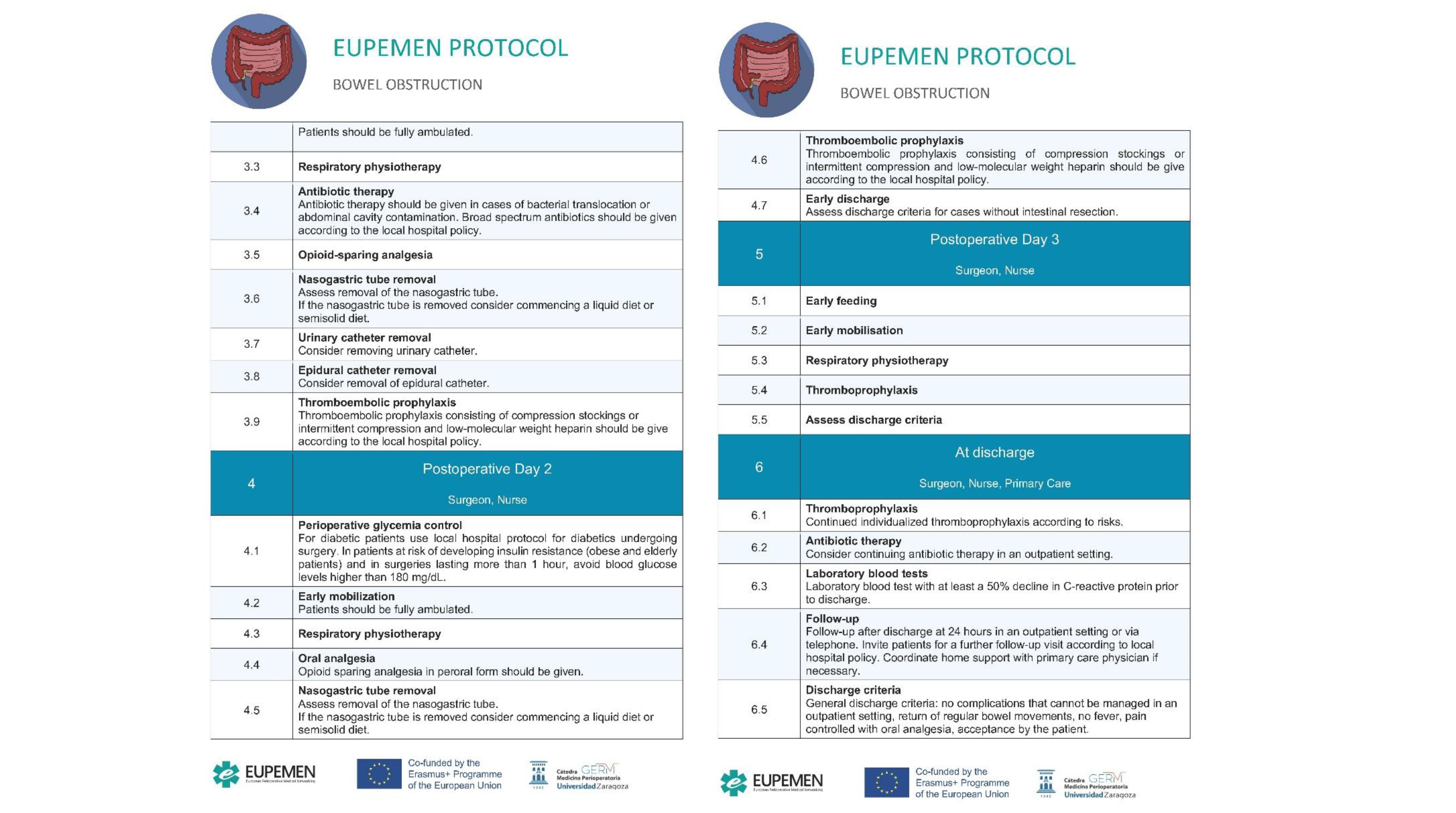
During the 1st postoperative day of the management of a patient with SBO, which is performed by the surgeon and the nurse perioperative glycaemic control is one of the key steps. For diabetic patients, local hospital protocols for diabetics undergoing surgery should be used while in patients at risk of developing insulin resistance (obese and elderly patients) and in surgeries lasting more than one hour, blood glucose levels higher than 180 mg/dL must be avoided [70-72]. Early mobilization is mandatory in the concept of the protocol and the patients should be fully ambulated in the 1st postoperative day while respiratory physiotherapy is a key element of the protocol [93-97].
Thromboembolic prophylaxis consisting of compression stockings or intermittent compression and low-molecular weight heparin should be given according to the local hospital policy.
Regarding the patients’ medications, antibiotic therapy should be given only in cases of bacterial translocation or abdominal cavity contamination. Broad spectrum antibiotics should be given according to the local hospital policy. Otherwise, the administration of antibiotic prophylaxis only is sufficient. Moreover, regarding pain management opioid-sparing analgesia must be used [60, 98-105].
In order to easily mobilize the patient nasogastric tube, urinary catheter and epidural catheter removal should be considered. If the nasogastric tube is removed consider commencing a liquid diet or semisolid diet [106, 107].
4.5. Second Postoperative Day
During the 2st postoperative day of the management of a patient with SBO, which is performed by the surgeon and the nurse perioperative glycaemic control is one of the key steps. For diabetic patients, local hospital protocols for diabetics undergoing surgery should be used while in patients at risk of developing insulin resistance (obese and elderly patients) and in surgeries lasting more than one hour, blood glucose levels higher than 180 mg/dL must be avoided [70-72]. Early mobilization is mandatory in the concept of the protocol and the patients should be fully ambulated in the 1st postoperative day while respiratory physiotherapy is a key element of the protocol [93-97]. Thromboembolic prophylaxis consisting of compression stockings or intermittent compression and low-molecular weight heparin should be given according to the local hospital policy. Moreover, regarding pain management opioid-sparing analgesia must be used per os.
In order to easily mobilize the patient nasogastric tube removal should be considered. If the nasogastric tube is removed, consider commencing a liquid diet or semisolid diet. Lastly, early discharge should be assessed according to discharge criteria for cases without intestinal resection.
4.6. Third Postoperative Day
During the 3rd postoperative day of the management of a patient with SBO, which is performed by the surgeon and the nurse, early feeding and early mobilization are key elements as well as respiratory physiotherapy and thromboprophylaxis. Early discharge should be assessed according to discharge criteria.
4.7. Discharge
Patient discharge from the hospital involves the surgeon, nurse and primary care. Regarding thromboprophylaxis, continued individualized thromboprophylaxis should be administrated according to risks while regarding antibiotic therapy it should be consider continuing antibiotic therapy in an outpatient setting in patient with indications. For the patient to be discharged the laboratory blood test should show at least a 50% decline in CRP prior to discharge. Follow-up is mandatory for all patients and follow-up after discharge at 24 hours in an outpatient setting or via telephone should be done. Also, patients should be invited for a further follow-up visit according to local hospital policy and if necessary, home support with primary care physician should be coordinated.
Finally, the general discharge criteria are no complications that cannot be managed in an outpatient setting, return of regular bowel movements, no fever, pain controlled with oral analgesia and, importantly, acceptance by the patient.
Figure 1.
The EUPEMEN Protocol for Bowel Obstruction for the Preoperative, Intraoperative and Postoperative Period.
Figure 1.
The EUPEMEN Protocol for Bowel Obstruction for the Preoperative, Intraoperative and Postoperative Period.

5. ERAS in Bowel Obstruction
The ERAS protocols have been proved to be effective in reducing postoperative complications, morbidity, length of hospital stay and overall cost in elective surgical procedures. While it seems more difficult to implement these protocols in emergency surgery, there are a few studies that have showed not only the feasibility of the protocols in bowel obstruction, both and mainly of the large intestine but also of the small intestine too, but also its advantages [108]. Specifically, the implementation of the ERAS protocol in patients undergoing emergency surgery for bowel obstruction has led to shorter hospital stay [108-111], decreased morbidity including pulmonary complications, paralytic ileus, surgical site infections [108, 110], an increased recovery of gastrointestinal function including decreased time to passing flatus [108], less postoperative pain and better quality of life [108, 110], a decreased inflammatory response including reduced CRP and procalcitonin values and also an increased efficacy of treatment in the ERAS group [110].
6. The EUPEMEN project
The goal of the EUPEMEN project is to bring together the expertise and experience of national clinical champions who have previously helped to deliver major change programmes in their countries and to use them to spread these protocols in Europe. This main goal has been achieved with the next specifics objectives:
- Preparation of an educational project (that included a teaching the teachers’ model);
- Implementation in a significant number of European hospitals of the evidence-based protocols in a homogeneous and standardised way;
- Collection of data about hospital stay, morbidity and mortality of European Surgical patients that once analysed through machine learning algorithm, will be of relevant interest to better know the surgical risk of an individual patient, hence to prevent perioperative complications.
The direct target groups the project aims are health professionals who are directly in charge of the care of surgical patients: surgeons, anaesthesiologists and nurses, as well as health professionals related to the interdisciplinary treatment of these patients: nutritionists, stoma-therapists, physiotherapists, rehabilitators, gastroenterologists, radiotherapists, oncologists, and pathologists. Moreover, as the effectiveness, as depicted by reduction of hospital stays and optimization of the use of other resources, is one of the advantages of these programs, health centres administrator, clinical managers and quality coordinators will also benefit from the project. Finally, due to the characteristics of enhanced recovery, primary care physicians play a very active role too. The indirect target groups of the project are the patients and their relatives and the patients’ associations, while the project’s stakeholders are local, regional, and national authorities and diseases associations.
The technical activities of the project were:
-
The preparation of the EUPEMEN Multimodal Rehabilitation manual with the protocols of 6 different modules:
- Bariatric Surgery;
- Oesophageal Surgery;
- Gastric Cancer Surgery;
- Colon Surgery;
- Hepatobiliary Surgery;
- Urgent abdominal surgery, including appendectomy and small bowel obstruction (SBO).
- The development of the EUPEMEN online platform (https://eupemen.eu/): to host the e-learning training course and a collaborative area to improve and to participate in the protocols;
- The training of the trainers to teach the future teachers the different protocol to be able to teach them in the different hospitals;
- The dissemination of the results in 5 Multiplier events, one per partner, to promote the protocols;
- The organization of 4 transnational meetings, one per country;
- The translation into English of the Recovery Intensification for optimal Care in Adult’s surgery - RICA from the Spanish de Recuperación Intensificada en Cirugía del Adulto (RICA).
The results of the project were the development of the EUPEMEN Protocols Training Programme for health professionals, the training of 200 multidisciplinary professionals in all the direct target groups involved in perioperative procedure from each partner in one local forum with 40 participants. Furthermore, the implementation of the protocols in, at least, 5 hospitals in Europe and the creation of a professional network with capacity to train stakeholders in hospitals, and to audit the trainers to guarantee the correct implementation of the programme. Long-term effect and impact of the project will be to decrease the secondary effects after surgery for patients, consequently, with a faster patient recovery, to reduce morbidity and mortality caused after surgical operations and to reduce the length of stay in the hospital and, consequently, save money for the public health system and to have more free beds for other new requested patients.
7. Discussion
The main objective of the project is the uniform, consistent, consensual and multi-centre implementation of the program of perioperative medicine based on the evidence resulting from the clinical pathway of Recovery Intensification for optimal Care in Adult’s surgery (RICA), published by the Ministry of Health, Social Services and Equality and the Aragon Health Sciences Institute, in the hospital centres at a European level, as the implementation of the program in hospitals will mean an important decrease in perioperative complications (morbidity and mortality) in patients included in the program, as well as a shortening of global hospital stays, an improvement in the efficiency of professionals, the inclusion of patients and caregivers in the making of decisions concerning processes, a better and earlier reincorporation of them in their family and social/work environment and an overall improvement of the care given; all of which is related to an overall decrease in the cost per process and resulting in safer processes. The two Intellectual Outputs that were developed were a training manual for the implementation and correct execution of the protocols and a teaching and learning platform completed through the collaboration and cooperation of the participants. The advantages of the project were that these intellectual outputs are innovative and have a transnational added value, as they will be elaborated taking into account the particularities of the different health systems of the participating countries, which will help to elaborate valid protocols in the different countries of the EU, the researchers involved in the project are professionals with experience in research and innovation, and also the innovation of the proposal to modify clinical practice by making it safer and promoting teamwork through the creation of multidisciplinary clinical units that will create synergies that will demonstrate clinical talent and excellence. The evaluation of the implementation results is proposed as a secondary objective by means of the analysis of established indicators and comparing the previously known clinical results with those from the new program, both in the short and long term.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Figures S1–5: The EUPEMEN Protocol for Bowel Obstruction for the Preoperative, Intraoperative and Postoperative Period.
Author Contributions
“Conceptualization, OI, JR, JMU, CF, AA, PK, LSG, APB, AW, ABE, MT.; methodology, OI, JR, JMU, CF, AA, PK, LSG, APB, AW, ABE, MT.; software ABE.; validation OI, JR, JMU, CF, AA, PK, LSG, APB, AW, ABE, MT; formal analysis OI, JR, JMU, CF, AA, PK, LSG, APB, AW, ABE, MT.; investigation, OI, JR, JMU, CF, AA, PK, LSG, APB, AW, ABE, MT .; resources, OI, JR, JMU, CF, AA, PK, LSG, APB, AW, ABE, MT.; data curation, OI, JR, JMU, CF, AA, PK, LSG, APB, AW, ABE, MT ; writing—original draft preparation OI, JR, JMU, CF, AA, PK, LSG, APB, AW, ABE, MT, EA.; writing—review and editing OI, JR, JMU, CF, AA, PK, LSG, APB, AW, ABE, MT, EA; visualization, OI, JR, JMU, CF, AA, PK, LSG, APB, AW, ABE, MT.; supervision, OI, JR, JMU, CF, AA, PK, LSG, APB, AW, ABE, MT.; project administration, OI, JR, JMU, CF, AA, PK, LSG, APB, AW, ABE, MT.; funding acquisition, OI, JR, JMU, CF, AA, PK, LSG, APB, AW, ABE, MT. All authors have read and agreed to the published version of the manuscript.”
Funding
The EUPENEM project has been funded with support of the Erasmus+ Programme of the European Union (Agreement number 2020-1-ES01-KA203-082681). This publication reflects the views only of the author, and the Commission cannot be held responsible for any use which may be made of the information contained therein.
Institutional Review Board Statement
Not applicable.
Data Availability Statement
Data is contained within the webpage The data presented in this study are available in [https://eupemen.eu/]
Acknowledgments
The EUPENEM project has been funded with support of the Erasmus+ Programme of the European Union (Agreement number 2020-1-ES01-KA203-082681). This publication reflects the views only of the author, and the Commission cannot be held responsible for any use which may be made of the information contained therein.
Conflicts of Interest
The authors declare no conflict of interest
References
- Ljungqvist O, Scott M, Fearon KC. Enhanced Recovery After Surgery: A Review. JAMA Surg 2017, 152, 292–298. [Google Scholar] [CrossRef] [PubMed]
- Scott MJ, Baldini G, Fearon KCH, Feldheiser A, Feldman LS, Gan TJ, Ljungqvist O, Lobo DN, Rockall TA, Schricker T, Carli F. Enhanced Recovery After Surgery (ERAS) for gastrointestinal surgery, part 1: pathophysiological considerations. Acta Anaesthesiol Scand 2015, 59, 1212–1231. [Google Scholar] [CrossRef] [PubMed]
- Catena F, De Simone B, Coccolini F, Di Saverio S, Sartelli M, Ansaloni L. Bowel obstruction: a narrative review for all physicians. World J Emerg Surg. 2019, 14, 20. [Google Scholar] [CrossRef]
- Gore RM, Silvers RI, Thakrar KH, Wenzke DR, Mehta UK, Newmark GM, Berlin JW. Bowel Obstruction. Radiol Clin North Am. 2015, 53, 1225–1240. [Google Scholar] [CrossRef]
- Johnson WR, Hawkins AT. Large Bowel Obstruction. Clin Colon Rectal Surg. 2021, 34, 233–241. [Google Scholar] [CrossRef]
- Long B, Robertson J, Koyfman A. Emergency Medicine Evaluation and Management of Small Bowel Obstruction: Evidence-Based Recommendations. J Emerg Med 2019, 56, 166–176. [Google Scholar] [CrossRef] [PubMed]
- Detz DJ, Podrat JL, Muniz Castro JC, Lee YK, Zheng F, Purnell S, Pei KY. Small bowel obstruction. Curr Probl Surg 2021, 58, 100893. [Google Scholar] [CrossRef] [PubMed]
- D'Agostino R, Ali NS, Leshchinskiy S, Cherukuri AR, Tam JK. Small bowel obstruction and the gastrografin challenge. Abdom Radiol (NY) 2018, 43, 2945–2954. [Google Scholar] [CrossRef]
- Aka AA, Wright JP, DeBeche-Adams T. Small Bowel Obstruction. Clin Colon Rectal Surg. 2021, 34, 219–226. [Google Scholar] [CrossRef]
- Bower KL, Lollar DI, Williams SL, Adkins FC, Luyimbazi DT, Bower CE. Small Bowel Obstruction. Surg Clin North Am. 2018, 98, 945–971. [Google Scholar] [CrossRef]
- Diamond M, Lee J, LeBedis CA. Small Bowel Obstruction and Ischemia. Radiol Clin North Am. 2019, 57, 689–703. [Google Scholar] [CrossRef] [PubMed]
- Gustafsson UO, Scott MJ, Schwenk W, Demartines N, Roulin D, Francis N, McNaught CE, MacFie J, Liberman AS, Soop M, Hill A, Kennedy RH, Lobo DN, Fearon K, Ljungqvist O; Enhanced Recovery After Surgery Society. Guidelines for perioperative care in elective colonic surgery: Enhanced Recovery After Surgery (ERAS®) Society recommendations. Clin Nutr. 2012, 31, 783–800. [Google Scholar] [CrossRef] [PubMed]
- Nygren J, Thacker J, Carli F, Fearon KC, Norderval S, Lobo DN, Ljungqvist O, Soop M, Ramirez J; Enhanced Recovery After Surgery Society. Guidelines for perioperative care in elective rectal/pelvic surgery: Enhanced Recovery After Surgery (ERAS®) Society recommendations. Clin Nutr. 2012, 31, 801–816. [Google Scholar] [CrossRef] [PubMed]
- Gustafsson UO, Scott MJ, Hubner M, Nygren J, Demartines N, Francis N, Rockall TA, Young-Fadok TM, Hill AG, Soop M, de Boer HD, Urman RD, Chang GJ, Fichera A, Kessler H, Grass F, Whang EE, Fawcett WJ, Carli F, Lobo DN, Rollins KE, Balfour A, Baldini G, Riedel B, Ljungqvist O. Guidelines for Perioperative Care in Elective Colorectal Surgery: Enhanced Recovery After Surgery (ERAS®) Society Recommendations: 2018. World J Surg. 2019, 43, 659–695. [Google Scholar] [CrossRef] [PubMed]
- Bisch SP, Jago CA, Kalogera E, Ganshorn H, Meyer LA, Ramirez PT, Dowdy SC, Nelson G. Outcomes of enhanced recovery after surgery (ERAS) in gynecologic oncology - A systematic review and meta-analysis. Gynecol Oncol. 2021, 161, 46–55. [Google Scholar] [CrossRef] [PubMed]
- Noba L, Rodgers S, Chandler C, Balfour A, Hariharan D, Yip VS. Enhanced Recovery After Surgery (ERAS) Reduces Hospital Costs and Improve Clinical Outcomes in Liver Surgery: a Systematic Review and Meta-Analysis. J Gastrointest Surg. 2020, 24, 918–932. [Google Scholar] [CrossRef] [PubMed]
- Lee Y, Yu J, Doumouras AG, Li J, Hong D. Enhanced recovery after surgery (ERAS) versus standard recovery for elective gastric cancer surgery: A meta-analysis of randomized controlled trials. Surg Oncol. 2020, 32, 75–87. [Google Scholar] [CrossRef] [PubMed]
- Ye Z, Chen J, Shen T, Yang H, Qin J, Zheng F, Rao Y. Enhanced recovery after surgery (ERAS) might be a standard care in radical prostatectomy: a systematic review and meta-analysis. Ann Palliat Med. 2020, 9, 746–758. [Google Scholar] [CrossRef]
- Noba L, Rodgers S, Doi L, Chandler C, Hariharan D, Yip V. Costs and clinical benefits of enhanced recovery after surgery (ERAS) in pancreaticoduodenectomy: an updated systematic review and meta-analysis. J Cancer Res Clin Oncol. 2023. [CrossRef]
- Grupo de trabajo. Vía Clínica de Recuperación Intensificada en Cirugía Abdominal (RICA). Vía clínica de recupe- ración intensificada en cirugía abdominal (RICA) Ministerio de Sanidad, Servicios Sociales e Igualdad. Instituto Aragonés de Ciencias de la Salud. 2014. Available online: http://portal.guiasalud.es/contenidos/iframes/documentos/opbe/2015-07/ViaClinica-RICA.pdf.
- Ramirez, Jose & Ruiz-López, Pedro & Gurumeta, Alfredo & Arroyo-Sebastian, Antonio & Bruna-Esteban, M. & Sanchez, Alberto & Calvo-Vecino, José & García-Erce, José & García-Fernández, Alfredo & Toro, Manuel & Grima, Francisco & Ramírez, Ana & Loinaz, Carmelo & Raldúa, Natividad & Calabuig, Juan & Muñoz, Manuel & Quintas, Carmen & Bretón, Julia & Ojeda Thies, Cristina & Ríos, Jorge. (2021). CLINICAL PATHWAY Recovery Intensification for optimal Care in Adult's surgery.
- Dalton A, Zafirova Z. Preoperative Management of the Geriatric Patient: Frailty and Cognitive Impairment Assessment. Anesthesiol Clin. 2018, 36, 599–614. [Google Scholar] [CrossRef]
- Subramaniam S, Aalberg J, Soriano RP, Divino CM. New 5-Factor Modified Frailty Index Using American College of Surgeons NSQIP Data. J Am Coll Surg. 2018, 226, 173–181. [Google Scholar] [CrossRef] [PubMed]
- Wang J, Zou Y, Zhao J, Schneider DB, Yang Y, Ma Y et al. The Impact of Frailty on Outcomes of Elderly Patients After Major Vascular Surgery: A Systematic Review and Meta-analysis. Eur J Vasc Endovasc Surg. 2018, 56, 591–602. [Google Scholar] [CrossRef] [PubMed]
- Castellví Valls J, Borrell Brau N, Bernat MJ, Iglesias P, Reig L, Pascual L et al. Colorectal carcinoma in the frail surgical patient. Implementation of a Work Area focused on the Com- plex Surgical Patient improves postoperative outcome. Cir Esp. 2018, 96, 155–161. [Google Scholar]
- Shen Y, Hao Q, Zhou J, Dong B. The impact of frailty and sarcopenia on postoperative outcomes in older patients undergoing gastrectomy surgery: a systematic review and me- ta-analysis. BMC Geriatr. 2017, 17, 188. [Google Scholar]
- Torossian A, Bräuer A, Höcker J, Bein B, Wulf H, HornEP. Preventing inadvertent perioperative hypothermia. Clinical Practice Guideline. Dtsch Arztebl Int. 2015, 112, 166–172. [Google Scholar]
- Warttig S, Alderson P, Campbell G,Smith AF. Interventionsfor treating inadvertent postoperative hypothermia. Interventionsfor treating inadvertent postoperative hypothermia. Cochrane Database Syst Rev. 2014, CD009892. [Google Scholar]
- Hooper VD, Chard R, Clifford T, Fetzer S, Fossum S, Godden B, et al. ASPAN’s evidence- based clinical practice guideline for the promotion of perioperative normothermia: second edition. J Perianesth Nurs. 2010, 25, 346–365. [Google Scholar] [CrossRef] [PubMed]
- Akhtar Z, Hesler BD, Fiffick AN, Mascha EJ, Sessler DI, Kurz A, et al. A randomized trial of prewarming on patient satisfaction and thermal comfort in outpatient surgery. J Clin Anesth. 2016, 33, 376–385. [Google Scholar] [CrossRef]
- Protocolo de Trabajo del IQZ 2017. Disponible en (última consulta 01-06-2020): https://infeccionquirurgicazero.es/es/documentos-y-materiales/protocolos-de-trabajo.
- Pontes JPJ, Mendes FF, Vasconcelos MM, Batista NR. [Evaluation and perioperative management of patients with diabetes mellitus. A challenge for the anesthesiologist]. Rev Bras Anestesiol 2018, 68, 75–86. [Google Scholar]
- Akiboye F, Rayman G. Management of Hyperglycemia and Diabetes in Orthopedic Surgery. Curr Diab Rep 2017, 17, 13. [Google Scholar] [CrossRef] [PubMed]
- Dhatariya K, Levy N, Hall GM. The impact of glycaemic variability on the surgical patient. Curr Opin Anaesthesiol 2016, 29, 430–437. [Google Scholar] [CrossRef]
- Barker P, Creasey PE, Dhatariya K, Levy N, Lipp A, Nathanson MH et al. Peri-operative management of the surgical patient with diabetes 2015: Association of Anaesthetists of Great Britain and Ireland. Anaesthesia 2015, 70, 1427–1440. [Google Scholar] [CrossRef]
- Allegranzi B, Zayed B, Bischoff P, Kubilay NZ, de Jonge S, de Vries F, et al. New WHO re- commendations on intraoperative and postoperative measures for surgical site infection prevention: an evidence-based global perspective. Lancet Infect Dis. diciembre de 2016, 16, e288–303. [Google Scholar]
- Allegranzi B, Bischoff P, de Jonge S, Kubilay NZ, Zayed B, Gomes SM, et al. New WHO re- commendations on preoperative measures for surgical site infection prevention: an evidence-based global perspective. Lancet Infect Dis. diciembre de 2016, 16, e276–e287. [Google Scholar]
- Badia JM, Casey AL, Petrosillo N, Hudson PM, Mitchell SA, Crosby C. Impact of surgical site infection on healthcare costs and patient outcomes: a systematic review in six European countries. J Hosp Infect. mayo de 2017, 96, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Proyecto Infección Quirúrgica Zero del Sistema Nacional de Salud. Sociedad Española de Medicina Preventiva, Salud Pública e Higiene. 2016.
- Nelson G, Bakkum-Gamez J, Kalogera E, Glaser G, Altman A, Meyer LA et al. Guidelines for perioperative care in gynecologic/oncology: Enhanced Recovery After Surgery (ERAS) Society recommendations-2019 update. Int J Gynecol Cancer. 2019, 29, 651–668. [Google Scholar] [CrossRef]
- Gustafsson UO, Scott MJ, Hubner M, Nygen J, Demartines N Francis N, et al. Guidelines for Perioperative Care in Elective Colorectal Surgery: Enhanced Recovery After Surgery (ERAS®) Society Recommendations: 2018. World J Surg. 2019, 43, 659–695. [Google Scholar] [CrossRef]
- Wongkietkachorn A, Wongkietkachorn N, Rhunsiri P. Preoperative needs-based education to reduce anxiety, increase satisfaction, and decrease time spent in day surgery: a randomized controlled trial. World J Surg. 2018, 42, 666–674. [Google Scholar] [CrossRef] [PubMed]
- Programa de Cirugía Segura del Sistema Nacional de Salud. Ministerio de Sanidad, Servi- cios Sociales e Igualdad. 2016.
- De Jager E, McKenna C, Bartlett L3, Gunnarsson R, Ho YH. postoperative Adverse Events Inconsistently Improved by The World Health Organization Surgical Safety Checklist: A Systematic Literature Review of 25 Studies. World J Surg. 2016, 40, 1842–1858. [Google Scholar] [CrossRef]
- Abbott TEF, Ahmad T, Phull MK, Fowler AJ, Hewson R, Biccard BM, Chew MS, Gillies M, Pearse RM; International Surgical Outcomes Study (ISOS)group. The surgical safety chec- klist and patient outcomes after surgery: prospective observational cohort study, systematic review and meta-analysis. Br J Anaesth. 2018, 120, 146–155. [Google Scholar] [CrossRef]
- Biccard BM, Rodseth R, Cronje L, Agaba P, Chikumba E, Du Toit L, Farina Z, Fischer S, Go- palan PD, Govender K, Kanjee J, Kingwill A, Madzimbamuto F, Mashava D, Mrara B, Mudely M, Ninise E, Swanevelder J, Wabule A.A meta-analysis of the efficacy of preoperative surgical safety checklists to improve perioperative.
- Lam T, Nagappa M, Wong J, Singh M, Wong D, Chung F. Continuous Pulse Oximetry and Capnography Monitoring for Postoperative Respiratory Depression and Adverse Events: A Systematic Review and Meta-analysis. Anesth Analg. 2017, 125, 2019–2029. [Google Scholar] [CrossRef] [PubMed]
- Frerk C, Mitchell VS, McNarry AF, Mendonca C, Bhagrath R, Patel A et al. Difficult Airway Society 2015 guidelines for management of unanticipated difficult intubation in adults. Br J Anaesth 2015, 115, 827–8481. [Google Scholar] [CrossRef] [PubMed]
- Urits I, Jones MR, Orhurhu V, Sikorsky A, Seifert D, Flores C, et al. A Comprehensive Update of Current Anesthesia Perspectives on Therapeutic Hypothermia. Adv Ther 2019, 36, 2223–2232. [Google Scholar] [CrossRef] [PubMed]
- Calvo Vecino JM, Casans Francés R, Ripollés Melchor J, Marín Zaldívar C, Gómez Ríos MA, Pérez Ferrer A, et al. No Intencionada de la SEDAR. Clinical practice guideline. Unintentional perioperative hypothermia. Rev Esp Anestesiol Reanim. 2018, 65, 564–588. [Google Scholar]
- Madden LK, Hill M, May TL, Human T, Guanci MM, Jacobi J, Moreda MV, et al. The Implementation of Targeted Temperature Management: An Evidence-Based Guideline from the Neurocritical Care Society. Neurocrit Care. 2017, 27, 468–487. [Google Scholar] [CrossRef]
- Makaryus R, Miller TE, Gan TJ. Current concepts of fluid management in enhanced recovery pathways. Br J Anaesth 2018, 120, 376–383. [CrossRef]
- Joosten A, Delaporte A, Ickx B, Touihri K, Stany I, Barvais L, et al. Crystalloid versus colloid for intraoperative goal-directed fluid therapy using a closed-loop system: A randomized, double-blinded, controlled trial in major abdominal surgery. Anesthesiology 2018, 128, 55–66. [Google Scholar] [CrossRef] [PubMed]
- Kapoor PM, Magoon R, Rawal RS, Mehta Y, Taneja S, Ravi R, et al. Goal-directed therapy improves the outcome of high-risk cardiac patients undergoing off-pump coronary artery bypass. Ann Card Anaesth 2017, 20, 83–89. [Google Scholar] [CrossRef]
- Bacchin MR, Ceria CM, Giannone S, Ghisi D, Stagni G, Greggi T, et al. Goal-direted fluid therapy based on stroke volume variation in patients undergoing major spine surgery in the prone position: A cohort study. Spine 2016, 41, E1131–E1137. [Google Scholar] [CrossRef]
- Salicath JH, Yeoh ECY, Bennett MH. Epidural analgesia versus patient-controlled intravenous analgesia for pain following intra-abdominal surgery in adults. Cochrane Database of Systematic Reviews 2018, 8, CD010434. [Google Scholar]
- Guay J, Nishimori M, Kopp S. Epidural local anaesthetics versus opioid-based analgesic regimens for postoperative gastrointestinal paralysis, vomiting and pain after abdominal surgery. Cochrane Database of Systematic Reviews 2016, 7, CD001893. [Google Scholar]
- Apfel CC, Läärä E, Koivuranta M, Greim CA, Roewer N. A simplified risk scorefor predicting postoperative nausea and vomiting: conclusions from cross-validations between two centers. Anesthesiology 1999, 91, 693–700. [Google Scholar] [CrossRef]
- Apfel CC, Philip BK, Cakmakkaya OS, Shilling A,ShiY-Y, LeslieJB, et al. Whoi s at risk for postdischarge nausea and vomiting after ambulatory surgery? Anesthesiology 2012, 117, 475–486. [Google Scholar] [CrossRef] [PubMed]
- Apfel CC, Heidrich FM, Jukar-Rao S, Jalota L, Hornuss C, Whelan RP, et al. Evidence-ba- sed analysis of risk factors for postoperative nausea and vomiting. Br J Anaesth 2012, 109, 742–753.
- Nelson G, Bakkum-Gamez J, Kalogera E, Glaser G, Altman A, Meyer LA, et al. Guidelines for perioperative care in gynecologic/oncology: Enhanced Recovery After Surgery (ERAS) Society recommendations-2019 update. Int J Gynecol Cancer. 2019, 29, 651–668. [Google Scholar] [CrossRef]
- Gustafsson UO, Scott MJ, Hubner M, Nygren J, Demartines N, Francis N, et al. Guidelines for Perioperative Care in Elective Colorectal Surgery: Enhanced Recovery After Surgery (ERAS®) Society Recommendations: 2018. World J Surg. 2019, 43, 659–695. [Google Scholar] [CrossRef] [PubMed]
- Denost Q, Rouanet P, Faucheron JL, Panis Y, Meunier B, Cotte E, et al. French Research Group of Rectal Cancer Surgery (GRECCAR). To Drain or Not to Drain Infraperitoneal Anas- tomosis After Rectal Excision for Cancer: The GRECCAR 5 Randomized Trial. Ann Surg. 2017, 265, 474–480. [Google Scholar] [CrossRef]
- Carmichael JC, Keller DS, Baldini G, Bordeianou L, Weiss E, Lee L et al. Clinical Practice Guidelines for Enhanced Recovery After Colon and Rectal Surgery From the American Society of Colon and Rectal Surgeons and Society of American Gastrointestinal and Endoscopic Surgeons. Dis Colon Rectum. 2017, 60, 761–784. [Google Scholar] [CrossRef] [PubMed]
- Zhang HY, Zhao CL, Xie J, Ye YW, Sun JF, Ding ZH, et al. To drain or not to drain in colorectal anastomosis: a meta-analysis. Int J Colorectal Dis. 2016, 31, 951–960. [Google Scholar] [CrossRef]
- Musser JE, Assel M, Guglielmetti GB, Pathak P, Silberstein JL, Sjoberg DD, et al. Impact of routine use of surgical drains on incidence of complications with robot-assisted radical prostatectomy. J Endourol. 2014, 28, 1333–1337. [Google Scholar] [CrossRef]
- Patel DN, Felder SI, Luu M, Daskivich TJ, K NZ, Fleshner P. Early Urinary Catheter Removal Following Pelvic Colorectal Surgery: A Prospective, Randomized, Noninferiority Trial. Dis Colon Rectum 2018, 61, 1180–1186. [Google Scholar] [CrossRef]
- Alyami M, Lundberg P, Passot G, Glehen O, Cotte E. Laparoscopic Colonic Resection Without Urinary Drainage: Is It “Feasible”? J Gastrointest Surg 2016, 20, 1388–1392.
- Zhang P, Hu WL, Cheng B, Cheng L, Xiong XK, Zeng YJ. A systematic review and meta- analysis comparing immediate and delayed catheter removal following uncomplicated hysterectomy. Int Urogynecol J 2015, 26, 665–674. [Google Scholar] [CrossRef] [PubMed]
- Kotagal M, Symons RG, Hirsch IB, Umpierrez GE, Farrokhi ET, Flum DR, SCOAP-Ceertain Collaborative. Perioperative hyperglycemia and risk of adverse events among patients with and without diabetes. Ann Surg 2015, 261, 97–103. [Google Scholar] [CrossRef]
- Weimann A, Braga M, Carli F, Higashiguchi T, Hübner M, Klek S, et al. ESPEN guideline: Clinical nutrition in surgery. Clin Nutr 2017, 36, 623–650. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association. 15. Diabetes Care in the Hospital: Standards of Medical Care in Diabetes-2019. Diabetes Care. 2019, 42 (Suppl 1), S173–S181. [Google Scholar] [CrossRef]
- Torossian, A. Thermal management during anaesthesia and thermoregulation standards for the prevention of inadvertent perioperative hypothermia. Best Pract Res Clin Anaesthesiol. 2008, 22, 659–668. [Google Scholar] [CrossRef]
- Warttig S, Alderson P, Campbell G, Smith AF. Interventions for treating inadvertent postoperative hypothermia. Cochrane Database Syst Rev. 2014, CD009892. [Google Scholar]
- Madrid E, Urrútia G, Roqué i Figuls M, Pardo-Hernandez H, Campos JM et al. Active body surface warming systems for preventing complications caused by inadvertent perioperative hypothermia in adults. Cochrane Database Syst Rev. 2016, 4, CD009016. [Google Scholar]
- Campbell G, Alderson P, Smith AF, Warttig S. Warming of intravenous andirrigationfluids for preventing inadvertent perioperative hypothermia. Cochrane Database Syst Rev. 2015, CD009891. [Google Scholar]
- Calvo Vecino JM, Casans Francés R, Ripollés Melchor J, Marín Zaldívar C, Gómez Ríos MA, Pérez Ferrer A, et al. Clinical practice guideline. Unintentional perioperative hypothermia. Rev Esp Anestesiol Reanim. 2018, 65, 564–588. [Google Scholar]
- Felder S, Rasmussen MS, King R, Sklow B, Kwaan M, Madoff R, et al. Prolonged thrombo-prophylaxis with low molecular weight heparin for abdominal or pelvic surgery. Cochrane Database Syst Rev. 2019, 3, CD004318. [Google Scholar] [CrossRef]
- Vivas D, Roldán I, Ferrandis R, Marín F, Roldán V, Tello-Montoliu A, et al. Perioperative and Periprocedural Management of Antithrombotic Therapy: Consensus Document of SEC, SEDAR, SEACV, SECTCV, AEC, SECPRE, SEPD, SEGO, SEHH, SETH, SEMERGEN, SEMFYC, SEMG, SEMICYUC, SEMI, SEMES, SEPAR, SENEC, SEO, SEPA, SERVEI, SECOT and AEU. Rev Esp Cardiol. 2018, 71, 553–564. [Google Scholar] [CrossRef]
- Falck-Ytter Y, Francis CW, Johanson NA, Curley C, Dahl OE, Schulman S, et al: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012, 141 (Suppl. 2), e278S–e325S.
- Anderson DR, Morgano GP, Bennett C, Dentali F, Francis CW, Garcia DA, et al American Society of Hematology 2019 guidelines for management of venous thromboembolism: prevention of venous thromboembolism in surgical hospitalized patients. Blood Adv. 2019, 3, 3898–3944. [CrossRef] [PubMed]
- Afshari A, Fenger-Eriksen C, Monreal M, Verhamme P; ESA VTE Guidelines Task Force. European guidelines on perioperative venous thromboembolism prophylaxis: Mechanical prophylaxis. Eur J Anaesthesiol. 2018, 35, 112–11. [Google Scholar] [CrossRef] [PubMed]
- Mulier JP, Dillemans B. Anaesthetic Factors Affecting Outcome After Bariatric Surgery, a Retrospective Levelled Regression Analysis. OBES SURG. 2019, 29, 1841–1850. [Google Scholar] [CrossRef] [PubMed]
- Frauenknecht J, Kirkham KR, Jacot-Guillarmod A, Albrecht E. Analgesic impact of intra- operative opioids vs. opioid-free anaesthesia: a systematic review and meta-analysis. Anaesthesia. 2019, 74, 651–662. [Google Scholar] [CrossRef] [PubMed]
- Mulier JP,Wouters R,Dillemans B,DeckockMl. ARandomizedControlled,Double-Blind Trial Evaluating the Effect of Opioid-Free Versus Opioid General Anaesthesia on Postoperative Pain and Discomfort Measured by the QoR-40. J Clin Anesth Pain Med. 2018, 2, 2–6. [Google Scholar]
- Mulier JP, Dillemans B. Deep Neuromuscular Blockade versusRemifentanil or Sevoflurane to Augment Measurable Laparoscopic Workspaceduring Bariatric Surgery Analysed bya Rando- misedControlledTrial. Journal of Clinical Anesthesiaand Pain Medicine 2018, 7, 2–4. [Google Scholar]
- Castelino T, Fiore JF Jr, Niculiseanu P et al The effect of early mobilization protocols on postoperative outcomes following abdominal and thoracic surgery: a systematic review. Surgery. 2016, 159, 991–1003. [CrossRef]
- de Almeida EPM, de Almeida JP, Landoni G, et al. Early mobilization programme improves functional capacity after major abdominal cancer surgery: a randomized controlled trial [with consumer summary]. British Journal of Anaesthesia 2017, 119, 900–907. [Google Scholar] [CrossRef] [PubMed]
- Schaller SJ, Anstey M, Blobner M etal. Early, goal-directed mobilization in the surgical intensive care unit: a randomized controlled trial. Lancet. 2016, 388, 1377–1388. [Google Scholar] [CrossRef] [PubMed]
- Fiore JF Jr, Castelino T, Pecorelli Net al. Ensuring early mobilization within an enhanced recovery program for colorectal surgery: a randomized controlled trial. Ann Surg 2017, 266, 223–231. [Google Scholar] [CrossRef] [PubMed]
- Gustafsson UO, Scott MJ, Hubner M, et al. Guidelines for Perioperative Care in Elective Colorectal Surgery: Enhanced Recovery After Surgery (ERAS_) Society Recommendations: 2018. World J Surg 2019, 43, 659–695. [Google Scholar] [CrossRef] [PubMed]
- Wolk S, Linke S, Bogner A. Use of Activity Tracking in Major Visceral Surgery-the Enhanced Perioperative Mobilization Trial: a Randomized Controlled Trial. J Gastrointest Surg 2019, 23, 1218. [Google Scholar] [CrossRef] [PubMed]
- Katsura M, Kuriyama A, Takeshima T, Fukuhara S, Furukawa TA. Preoperative inspiratory muscle training for postoperative pulmonary complications in adults undergoing cardiac and major abdominal surgery. Cochrane Database Syst Rev. 2015, 5, CD010356. [Google Scholar] [CrossRef]
- Kalil-Filho FA, Campos ACL, Tambara EM, Tomé BKA, Treml CJ, Kuretzki CH, et al. Phy- siotherapeutic approaches and the effects on inspiratory muscle force in patients with chronic obstructive pulmonary disease in the pre-operative preparation for abdominal sur- gical procedures. Arq Bras Cir Dig. 2019, 32, e1439. [Google Scholar] [CrossRef]
- Kendall F, Oliveira J, Peleteiro B, Pinho P, Bastos PT. Inspiratory muscle training is effective to reduce postoperative pulmonary complications and length of hospital stay: a systematic review and meta-analysis. Disabil Rehabil. 2018, 40, 864–882. [Google Scholar] [CrossRef]
- Alaparthi GK, Augustine AJ, Anand R, Mahale A. Comparison of Diaphragmatic Breathing Exercise, Volume and Flow Incentive Spirometry, on Diaphragm Excursion and Pulmonary Function in Patients Undergoing Laparoscopic Surgery: A Randomized Controlled Trial. Minim Invasive Surg 2016, 2016, 1967532. [Google Scholar]
- Karlsson E, Farahnak P, Franzén E, Nygren-Bonnier M, Dronkers J, van Meeteren N, et al. Feasibility of preoperative supervised home-based exercise in older adults undergoing colorectal cancer surgery-A randomized controlled design. PLoS One. 2019, 14, e0219158. [Google Scholar]
- Martinez V, Beloeil H, Marret E, Fletcher D, Ravaud P, Trinquart L. Non-opioid analgesics in adults after major surgery: systematic review with network meta-analysis of randomized trials. British Journal of Anaesthesia. 2017, 118, 22–31. [Google Scholar] [CrossRef]
- Salicath JH, Yeoh ECY, Bennett MH. Epidural analgesia versus patient-controlled intrave-nous analgesia for pain following intra-abdominal surgery in adults. Cochrane Database of Systematic Reviews. 2018, 8, CD010434. [Google Scholar]
- Jørgensen H, Wetterslev J, Møiniche S, Dahl JB. Epidural local anaesthetics versus opioid-based analgesic regimens on postoperative gastrointestinal paralysis, PONV and pain after abdominal surgery. Cochrane Database Syst Rev. 2000, CD001893.
- McDaid C, Maund E, Rice S, Wright K, Jenkins B, Woolacott N. Paracetamol and selective and non-selective non-steroidal anti-inflammatory drugs (NSAIDs) for the reduction of morphine-related side effects after major surgery: a systematic review. Health Technol Assess. 2010,1–153, iii–iv.
- MacFater WS, Rahiri J-L, Lauti M, Su’a B, Hill AG. Intravenous lignocaine in colorectal sur- gery: a systematic review. ANZ J Surg. 2017, 87, 879–885. [Google Scholar] [CrossRef] [PubMed]
- Weibel S, Jokinen J, Pace NL, Schnabel A, Hollmann MW, Hahnenkamp K, et al. Efficacy and safety of intravenous lidocaine for postoperative analgesia and recovery after surgery: a systematic review with trial sequential analysis. Br J Anaesth. 2016, 116, 770–783. [Google Scholar] [CrossRef] [PubMed]
- Weibel S, Jelting Y, Pace NL, Helf A, Eberhart LH, Hahnenkamp K, et al. Continuous intra- venous perioperative lidocaine infusion for postoperative pain and recovery in adults. Co- chrane Database Syst Rev. 2018, 6, CD009642. [Google Scholar]
- Baeriswyl M, Zeiter F, Piubellini D, Kirkham KR, Albrecht E. The analgesic efficacy of trans- verse abdominis plane block versus epidural analgesia: a systematic review with meta- analysis. Medicine. 2018, 97. [Google Scholar]
- Willcutts KF, Chung MC, Erenberg CL, Finn KL, Schirmer BD, Byham-Gray LD. Early oral feeding as compared with traditional timing of oral feeding after upper gastrointestinal surgery. Ann Surg 2016, 264, 54e63. [Google Scholar]
- Weimann A, Braga M, Carli F, Higashiguchi T, Hübner M, Klek S, et al. ESPEN guideline: Clinical nutrition in surgery. Clin Nutr 2017, 36, 623–650. [Google Scholar] [CrossRef] [PubMed]
- Sharma J, Kumar N, Huda F, Payal YS. Enhanced Recovery After Surgery Protocol in Emergency Laparotomy: A Randomized Control Study. Surg J (NY) 2021, 7, e92–e99. [Google Scholar] [CrossRef]
- Shida D, Tagawa K, Inada K, Nasu K, Seyama Y, Maeshiro T, Miyamoto S, Inoue S, Umekita N. Modified enhanced recovery after surgery (ERAS) protocols for patients with obstructive colorectal cancer. BMC Surg 2017, 17, 18. [Google Scholar]
- Miao X, Tao L, Huang L, Li J, Pan S. Application of Laparoscopy Combined with Enhanced Recovery after Surgery (ERAS) in Acute Intestinal Obstruction and Analysis of Prognostic Factors: A Retrospective Cohort Study. Biomed Res Int. 2022, 2022, 5771526. [Google Scholar]
- Saurabh K, Sureshkumar S, Mohsina S, Mahalakshmy T, Kundra P, Kate V. Adapted ERAS Pathway Versus Standard Care in Patients Undergoing Emergency Small Bowel Surgery: a Randomized Controlled Trial. J Gastrointest Surg. 2020, 24, 2077–2087. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



