
Submitted:
25 April 2023
Posted:
25 April 2023
You are already at the latest version
Abstract
The search for biological markers, which allow a relatively accurate assessment of the individual course of pulmonary sarcoidosis at the time of diagnosis remains one of the research priorities in this field of pulmonary medicine. The aim of our study was to investigate possible prognostic factors for pulmonary sarcoidosis with a special focus on cellular immune inflammation markers. 2 years follow-up of the study population after initial prospective and simultaneous analysis of lymphocyte activation markers expression in the blood, as well as bronchoalveolar lavage fluid (BALF), and lung biopsy tissue of patients with newly diagnosed pulmonary sarcoidosis, was done. We found that some blood and BAL fluid immunological markers and lung computed tomography (CT) patterns have been associated with a different course of sarcoidosis. We revealed five markers that had a significant negative association with the course of sarcoidosis (worsening pulmonary function tests and/or the chest CT changes) – blood CD4+CD31+ and CD4+CD44+ T lymphocytes, BALF CD8+CD31+ and CD8+CD103+ T lymphocytes and a number of lung nodules on chest CT at the time of the diagnosis. Cut-off values, sensitivity, specificity, and odds ratio for predictors of sarcoidosis progression were calculated. These markers may be reasonable predictors of sarcoidosis progression.
Keywords:
sarcoidosis
; bronchoalveolar lavage
; chest computed tomography
; biological markers
1. Introduction
Sarcoidosis is a systemic inflammatory disease of unknown etiology, which affected the lungs in most patients [1]. The manifestation and course of sarcoidosis are highly variable [2]. Usually, the course of pulmonary sarcoidosis is more favorable in radiological stage I as well as Löfgren’s syndrome, and often unfavorable (progressive) in stages II-III. However, the individual course of pulmonary sarcoidosis is unpredictable. It can range from a complete resolution of radiological symptoms and normalization of pulmonary function test (PFT) indices to the onset and progression of pulmonary fibrosis, which in some cases can be relatively rapid – within a few years of disease manifestation [3,4].
Many clinical, biological, radiological, and PFT markers as possible predictors of the course of the disease have been studied. These include serum angiotensin-converting enzyme, C-reactive protein, immunoglobulins, soluble interleukin-2 receptor, Krebs von den Lungen-6, blood and bronchoalveolar lavage fluid (BALF) T and B lymphocytes subtypes/activation markers expression, high-resolution computed tomography (CT), fluorine-18 fluorodeoxyglucose-positron emission tomography/CT [5,6,7,8,9,10,11]. However, no reliable biological marker allows a relatively accurate assessment of the individual course of pulmonary sarcoidosis at the time of diagnosis. The search for such markers remains one of the research priorities in this field of pulmonary medicine [12,13,14,15,16].
The aim of our study was to investigate possible prognostic factors for pulmonary sarcoidosis. In the search for a potentially suitable marker for daily clinical practice, we hypothesized that these factors could include radiological lung signs and PFT indices, besides, a special focus was paid to cellular immune inflammation markers. As sarcoidosis is a disease of the immune response, we searched for potential cellular immune markers that could reflect persistent inflammation and the onset of pulmonary fibrosis. In this paper, we extended our previous study [17,18] through 2 years follow-up of the study population after initial prospective and simultaneous analysis of clinical symptoms, radiological findings, PFT tests, lymphocyte activation markers expression in the blood as well as BALF, and lung biopsy tissue of patients with newly diagnosed pulmonary sarcoidosis.
2. Materials and Methods
Study Design and Patient Enrollment
A total of 71 consecutive patients (33 females and 38 males) with newly diagnosed pulmonary sarcoidosis were prospectively enrolled in the study at the Center of Pulmonology and Allergology of Vilnius University Hospital Santaros Klinikos (Table 1). The diagnosis was confirmed according to the American Thoracic Society/European Respiratory Society/World Association for Sarcoidosis and other Granulomatous Disorders statement [19]. Clinical symptoms, radiological findings, PFT indices, T lymphocyte activation markers expression in blood and BALF (of all the patients), as well as bronchoscopic lung biopsy tissue (of 35 patients without Löfgren’s syndrome) analyses, were performed (Table 2, Table 3). All study tests were done over two weeks, on average [18].
All study patients were Caucasian. None of the patients had any relevant medical history or comorbidity. The study was conducted in accordance with the Declaration of Helsinki (as revised in 2013).
Follow-up testing and modeling of predicting the course of sarcoidosis
After the initial comprehensive examination of the patients, all subjects were followed up. In this study, the final assessment for patients was accomplished 2 years after the initial investigation, 52 patients came for re-examination. The dynamics of PFT indices (FVC, FEV1, TLC, RV, DLCO) and chest CT changes (nodules, consolidation, ground glass areas, lymphadenopathy) were evaluated as described earlier [17,18]. None of the patients was treated with steroids or immunosuppressants/immunomodulators during the study period because it was no absolute clinical indication for treatment.
The dynamics of PFT indices were assessed as follows: 1) negative (progressive disease) when the value of the indices worsened by ≥10%, 2) positive when the value of the PFT indices has improved by ≥10%, 3) in other cases, the status was assessed as stable.
For chest CT findings, a profusion score for consolidation and ground glass was assigned to each lung zone based on the percentage of the lung zone involved: 0 points (no involvement), 1 point (1–25%), 2 points (26–50%), 3 points (51–75%) and 4 points (>75% of lung zone). A nodule profusion score was based on the number of nodules per zone (Figure 1): 0= no nodules, 1=1–5 nodules, 2=6–10 nodules, 3=11–15 nodules, and 4=>15 [17,20].
The dynamics of chest CT changes were assessed as follows: 1) negative, when the score worsened by ≥1 point, 2) positive (fewer radiological changes on chest CT) when the score improved by ≥1 point, 3) in other cases, the condition was assessed as stable.
Modeling the dependence of disease progression on other variables, a univariate and multivariate logistic regression model was constructed.
Statistical Analysis
Statistical analysis was performed using SPSS software, Version 20.0 (Statistical Package for Social Sciences, IBM, USA) to present mean and standard deviation. Shapiro-Wilks test was used to check the normality of quantitative variables. The Student's t-test was used to analyze two independent samples satisfying normality, while the Mann-Witney test was used for those that did not satisfy normality. The cut-off values of quantitative indicators were determined based on ROC (Receiver operating characteristic) curves. Corresponding cut-off values, sensitivity and specificity, and AUC (area under the ROC curve) and its 95% confidence interval (CI) were presented. Indicators were divided into groups using a cut-off value, and odds ratios (ORs) and their 95% CIs were calculated. Differences were considered statistically significant when the p<0.05.
3. Results
For the majority of the subjects, the PFT indices did not change or improved over 2 years. 10% or more FVC (%) increased in 25.0%, decreased in 9.6%, and remained unchanged in 65.4% of the patients; FEV1 (%) increased in 25.0%, decreased in 5.8%, and unchanged in 69.2% of the patients; TLC (%) increased in 32.7%, decreased in 15.4%, and unchanged in 51.9% of patients; RV (%) increased in 51.9%, decreased in 23.1%, and remained unchanged in 25.0% of the patients; DLCO (%) increased in 40.4%, decreased in 17.3%, and unchanged in 42.3% of the patients. However, when comparing entire study group values of the PFT indices determined at the time of inclusion and after two years of observation, no statistically reliable differences were found.
Radiologic changes on CT images improved or remained unchanged at 2 years in most of the patients. The enlargement of the mediastinal lymph nodes shown by CT at the time of diagnosis disappeared in 50.0%, decreased in 25.0%, and remained unchanged in 25.0% of the patients. Nodules that were seen in the lungs at the time of disease manifestation disappeared in 41.4%, decreased score in 9.8%, increased score in 4.9%, and remained unchanged in 43.9% of the patients. Ground-glass opacity that was seen on CT disappeared in 75.0% and remained in 25.0% of the patient. Consolidation disappeared in 55.6%, remained unchanged in 22.2%, decreased in 11.1%, and increased in 11.1% of the patient. Similarly to PFT indices, there were no statistically significant changes in any of the CT scores overall of the whole group over 2 years.
In searching for predictors of sarcoidosis progression, by the logistic regression model, only five markers had a significant negative association with the course of sarcoidosis – blood CD4+CD31+ and CD4+CD44+ T lymphocytes, BALF CD8+CD31+ and CD8+CD103+ T lymphocytes, and a number of lung nodules on chest CT at the time of the diagnosis (Table 4 and Figure 2).
4. Discussion
Although the course of sarcoidosis is highly variable [21], in most cases sarcoidosis does not progress [22,23]. In our study group, PFT indices and CT lung parenchyma changes remained stable or even improved for most patients (approximately 80% and 90% of all the patients respectively) at 2 years follow-up. However, in a part of cases diseases progress. Moreover, as it was indicated by Schimmelpennink et al, sarcoid patients with pulmonary fibrosis had a higher mortality rate [24].
The biological mechanisms underlying sarcoidosis activity – persistent inflammation and the onset and development of fibrosis – still are not well characterized [25]. We hypothesized that one or more of our selected immune markers are involved in inflammation and lung fibrogenesis in sarcoidosis. The following immune markers were chosen for this prospective patient observational study: CD4+CD31+, CD4+CD38+, CD4+CD44+, CD4+CD103+, CD8+CD31+, CD8+CD38+, CD8+CD44+, CD8+CD103+ (in both blood and BALF), CD38+, CD44+, CD103+, collagen (in lung tissue) [18].
We also sought to evaluate whether objective chest CT findings and PFT indices present at the time of disease manifestation can be prognostic factors for the course of sarcoidosis. For that purpose the following CT and PFT markers were chosen for the evaluation and long-term monitoring: lung nodules, linear opacities, consolidation, and ground glass scores, FVC, FEV1, TLC, VC, RV, and DLCO [17].
We found that of all indices tested, two immune blood T lymphocytes markers (CD4+CD31+ and CD4+CD44+), two BALF T lymphocytes markers (CD8+CD31+ and CD8+CD103+), and one chest CT sign (a number of lung nodules) are potential prognostic factors for the sarcoidosis course. Surprisingly, none of the PFT indices, lung tissue immune markers, or other (eg, demographic) indicators proved suitable for prediction in our study population. To our knowledge, none of our selected immune indices were analyzed as sarcoidosis prognostic markers. Due to the novelty of our data, it was not possible to directly compare our results with the results of other studies. Therefore, the interpretation of the results of our study is challenging.
Using a logistic regression model, we found that if blood CD4+CD31+ T lymphocytes were ≤14.5%, the odds ratio for disease progression was 13.78 (p=0.02). Moreover, the odds ratio for the probability of sarcoidosis progression was 10.00 (p=0.01) when BALF CD8+CD31+ T lymphocytes were ≥13.5%. CD31 is an integral membrane protein expressed by endothelial cells, dendritic cells, platelets, and other blood cells, including T lymphocytes. CD31 is a co-modulator of T-cell immunity, involved in leukocyte–leukocyte interactions, as well as in interactions between lymphocytes and the vascular endothelium, leukocyte extravasation, and migration to the inflamed tissues through intercellular junctions. CD31 plays a role in the regulation of vascular stability [26,27,28]. In CD4+ T cells CD31+ is expressed in naïve recent thymic emigrants but is downregulated after acute T cell activation and absent from memory cells. Unlike memory CD4+ T cells, memory CD8+ T cells retain CD31+ expression and have the potential to be modulated by this inhibitory receptor [29,30].
In experimental models, it was shown that some, but not all CD31 deficient mice strains spontaneously develop a fatal chronic pulmonary disease with some similarities to that seen in patients with idiopathic pulmonary fibrosis (IPF) [26,28]. Ziora et al. found that serum concentrations of the soluble CD31 were significantly higher in IPF patients in comparison with the control group and the sarcoid patients (the whole group of all stages) [31], but due to the wide CD31 receptor distribution in different cell types, it is difficult to guess if this increment depends on lung vasculature, platelets, leucocytes or other cell types. We studied CD31 expression on well-defined cells, T lymphocytes. It is known, that CD31 expression is reduced by shedding in activated T-cells and CD31 is possibly associated with T-cell subsets with immunosuppressive function [27]. Our results regarding the possible prognostic role of the low CD31+ marker expression on blood CD4+ T cells together with the high expression on BALF CD8+ T cells appear to be in indirect agreement with the results of other studies regarding CD31.
Our study showed that if blood CD4+CD44+ T lymphocytes were ≤37.5%, the probability of disease progression was 15.31 (p<0.001). CD44 is a family of cell surface glycoproteins, also termed hyaladherin (HA), belonging to the group of cell adhesion molecules. The cluster of differentiation 44 (CD44) is a multi-structural and multi-functional transmembrane glycoprotein, involved in cell-to-cell and cell-to-matrix interactions and participates in the regulation of hyaluronic metabolism, activation, and migration of lymphocytes, as well as the release of cytokines in areas of inflammation. CD44 participates in a wide variety of cellular functions, including lymphocyte activation, recirculation, and homing [32,33,34], alongside CD31 being an alternative pathway for leukocyte extravasation to the lung compartment [26]. CD44 pathway may be important in the development of fibrosis [35]. Culty et al. had shown that CD44 expression is greater in the area of granuloma formation and fibrosis [36]. Because our study showed a potential prognostic value for blood CD44+ only but not for BALF CD44+, it is difficult to unambiguously interpret our findings at the present time.
Our last revealed potential immune prognostic factor is BALF CD8+CD103+ T cells. We found that when BALF CD8+CD103+ T lymphocytes were ≥15.5%, the odds ratio for disease progression was 8.75 (p=0.01). CD103 is integrin αEβ7, an adhesion molecule expressed on most of the intraepithelial CD4+ lymphocytes in the mucosa [37]. It is known that this molecule can promote T-cell migration into the epithelium and is involved in the retention of lymphocytes in the mucosa. Constant CD103 expression can reflect antigen(-s) persistence in the lung tissue [38,39,40,41]. The interaction of effector CD8+ T cells with cognate antigen in the lung results in increased and prolonged expression of the tissue retention markers, such as CD103, and increases expression of the adhesion molecule, a very late activation antigen (VLA-1) [42]. Moreover, CD8+CD103+ may be involved in the autoimmune process [43]. However, it should be noted that there is an imbalance in circulating, alveolar, and lymph node CD8+CD103+ T cells in the development of sarcoidosis [44]. Similar to the CD31+ marker, it seems that our results regarding the possible prognostic role of the CD8+CD103+ marker are in indirect agreement with the results of other authors.
Unlike BALF immune markers, no lung tissue immune markers were identified as prognostic indicators in our study. Perhaps, we could explain this finding by the fact that during bronchoscopic forceps biopsy, only a few (usually 4-6) pieces of the lung, about 2 mm in size each, are usually obtained. BAL, on the other hand, washes out immune cells from approximately one million alveoli [45].
A number of lung nodules on chest CT is a single non-immunological prognostic factor for the sarcoidosis course revealed in our study. We found that the odds ratio for sarcoidosis progression was 18.46 at ≥15.0 nodules in the lungs on chest CT (p<0.001). CT appearances of sarcoidosis mirror the perilymphatic spreading of the granulomatous process observed pathologically. Nodules represent aggregates of granulomas [46]. Pulmonary sarcoidosis manifests with different CT patterns (so-called typical and atypical) [47]. Several authors evaluated associations between CT patterns and activity scores with the decline of respiratory function [48]. Distefano et al. in their retrospective study of 55 patients found that patients with atypical manifestations had greater worsening in PFT [49]. However, another study did not find a correlation between clinical deterioration and radiological changes [50]. Although the chest CT sarcoidosis activity score is promising, prospective dynamic studies are necessary [21,51].
None of the PFT indices at the time of manifestation of sarcoidosis was found to be a possible prognostic marker of disease course in our study. Unlike our study results, McDonnell et al in their retrospective observational study found that low DLCO at sarcoidosis presentation may identify patients without Löfgren’s syndrome who are more likely to develop physiological progression [52]. However, other authors [23,53] did not confirm their findings.
Other specific potential prognostic factors found in other studies, but not confirmed or not investigated in our study are older patients’ age [23,53,54], C reactive protein [52], and extrapulmonary involvement of disease [7,53].
Our study has strengths and limitations. The first strength is that it was a comprehensive study, including clinical, radiological, lung function, immune markers in the blood, BALF, and lung biopsy tissue. The second strength is that it was a prospective study with the main primary objective to search for prognostic markers [17,18]. The third strength is that the study was conducted in a highly experienced IPL center at a large university hospital [17,18,55,56,57,58,59,60]. The fourth strength is that we evaluated the natural course of sarcoidosis in our study population.
The limitation of the study is that this was a single-center study. However, our center is the primary center for interstitial lung disease in our country, therefore, these results may reflect the sarcoidosis patient in our population. The second limitation is that there was no genetic testing of the subjects [61]. Another limitation is that patients did not undergo positron emission tomography/CT [62]. When this study was started, these tests were not yet routine in our clinical practice.
5. Conclusions
Our results show that some blood and BAL fluid immunological markers and lung CT patterns have been associated with a different course of sarcoidosis. The blood CD4+CD31+ T lymphocyte and CD4+CD44+ T lymphocyte counts, the BAL fluid CD8+CD31+ T lymphocyte and CD8+ CD103+ T lymphocyte counts, and the number of lung nodules on chest CT may be reasonable predictors of sarcoidosis progression. Further studies are needed to consolidate these findings.
Author Contributions
E.D.: the study design, data analysis, writing and supervision; R.A.: original draft preparation, data analysis; R.M. and L.J.: conceptualization, data analysis; J.B.: data analysis; R.A., J.B., L.J., V.G., A.L., I.Z. and E.Ž.: investigation; I.Z.: data analysis; A.L.: supervision; A.M.: statistical analysis; All authors: reviewing and editing. All authors have read and agreed to the published version of the manuscript.
Funding
The study was funded by the EU structural support project No VP1-3.1-ŠMM-01-V-03-002, (2011– 2014): Improvement of Training of High Qualification Specialists Conformed to the State and Society Needs in Biomedical field (BIOMEDOKT).
Institutional Review Board Statement
This study was approved by the Vilnius Regional Biomedical Research Ethics Committee (No. 158200-12-5591160).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on reasonable request from the corresponding author.
Acknowledgments
None.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Crouser, E.D.; Maier, L.A.; Wilson, K.C.; Bonham, C.A.; Morgenthau, A.S.; Patterson, K.C.; Abston, E.; Bernstein, R.C.; Blankstein, R.; Chen, E.S.; Culver, D.A.; Drake, W.; Drent, M.; Gerke, A.K.; Ghobrial, M.; Govender, P.; Hamzeh, N.; James, W.E.; Judson, M.A.; Kellermeyer, L.; Knight, S.; Koth, L.L.; Poletti, V.; Raman, S.V.; Tukey, M.H.; Westney, G.E.; Baughman, R.P. Diagnosis and Detection of Sarcoidosis. An Official American Thoracic Society Clinical Practice Guideline. Am J Respir Crit Care Med. 2020, 201, e26–e51. [Google Scholar] [CrossRef] [PubMed]
- Franzen, D.P.; Brutsche, M.; Nilsson, J.; Böni, C.; Daccord, C.; Distler, O.; Elsener, D.; Funke-Chambour, M.; Gruner, C.; Hayward-Könnecke, H.; Hostettler, K.E.; Kündig, T.; Ribi, C.; Seebach, J.D.; Seeger, H.; Vrugt, B.; Kolios, A.G.A. Sarcoidosis - a multisystem disease. Swiss Med Wkly. 2022, 152, w30049. [Google Scholar] [CrossRef] [PubMed]
- Culver, D.A.; Judson, M.A. New advances in the management of pulmonary sarcoidosis. BMJ. 2019, 367, l5553. [Google Scholar] [CrossRef]
- Drent, M.; Crouser, E.D.; Grunewald, J. Challenges of Sarcoidosis and Its Management. N Engl J Med. 2021, 385, 1018–1032. [Google Scholar] [CrossRef] [PubMed]
- McDonnell, M.J.; Saleem, M.I.; Wall, D.; Gilmartin, J.J.; Rutherford, R.M.; O'Regan, A. Predictive value of C-reactive protein and clinically relevant baseline variables in sarcoidosis. Sarcoidosis Vasc Diffuse Lung Dis. 2016, 33, 331–340. [Google Scholar] [PubMed]
- Zhou, Y.; Zhang, Y.; Zhao, M.; Li, Q.; Li, H. sIL-2R levels predict the spontaneous remission in sarcoidosis. Respir Med. 2020, 171, 106115. [Google Scholar] [CrossRef]
- Belhomme, N.; Jouneau, S.; Bouzillé, G.; Decaux, O.; Lederlin, M.; Guillot, S.; Perlat, A.; Jégo, P. Role of serum immunoglobulins for predicting sarcoidosis outcome: A cohort study. PLoS One. 2018, 13, e0193122. [Google Scholar] [CrossRef]
- Bergantini, L.; Bianchi, F.; Cameli, P.; Mazzei, M.A.; Fui, A.; Sestini, P.; Rottoli, P.; Bargagli, E. Prognostic Biomarkers of Sarcoidosis: A Comparative Study of Serum Chitotriosidase, ACE, Lysozyme, and KL-6. Dis Markers. 2019, 2019, 8565423. [Google Scholar] [CrossRef]
- Ishiyama, M.; Soine, L.A.; Vesselle, H.J. Semi-quantitative metabolic values on FDG PET/CT including extracardiac sites of disease as a predictor of treatment course in patients with cardiac sarcoidosis. EJNMMI Res. 2017, 7, 67. [Google Scholar] [CrossRef]
- Benamore, R.; Kendrick, Y.R.; Repapi, E.; Helm, E.; Cole, S.L.; Taylor, S.; Ho, L.P. CTAS: a CT score to quantify disease activity in pulmonary sarcoidosis. Thorax. 2016, 71, 1161–1163. [Google Scholar] [CrossRef]
- Kraaijvanger, R.; Janssen Bonás, M.; Vorselaars, A.D.M.; Veltkamp, M. Biomarkers in the Diagnosis and Prognosis of Sarcoidosis: Current Use and Future Prospects. Front Immunol. 2020, 11, 1443. [Google Scholar] [CrossRef] [PubMed]
- Grunewald, J.; Grutters, J.C.; Arkema, E.V.; Saketkoo, L.A.; Moller, D.R.; Müller-Quernheim, J. Publisher Correction: Sarcoidosis. Nat Rev Dis Primers. 2019, 5, 49. [Google Scholar] [CrossRef] [PubMed]
- Kobak, S. Catch the rainbow: Prognostic factor of sarcoidosis. Lung India. 2020, 37, 425–432. [Google Scholar] [CrossRef] [PubMed]
- Judson, M.A. The ability to predict the clinical course of pulmonary sarcoidosis from data that is right in front of us. J Bras Pneumol. 2022, 48, e20220012. [Google Scholar] [CrossRef] [PubMed]
- Hu, X.; Zou, L.; Wang, S.; Zeng, T.; Li, P.; Shen, Y.; Chen, L. Performance of Serum Angiotensin-Converting Enzyme in Diagnosing Sarcoidosis and Predicting the Active Status of Sarcoidosis: A Meta-Analysis. Biomolecules. 2022, 12, 1400. [Google Scholar] [CrossRef] [PubMed]
- Malkova, A.; Zinchenko, Y.; Starshinova, A.; Kudlay, D.; Kudryavtsev, I.; Glushkova, A.; Yablonskiy, P.; Shoenfeld, Y. Sarcoidosis: Progression to the chronic stage and pathogenic based treatment (narrative review). Front Med (Lausanne). 2022, 9, 963435. [Google Scholar] [CrossRef]
- Aleksonienė, R.; Zeleckienė, I.; Matačiūnas, M.; Puronaitė, R.; Jurgauskienė, L.; Malickaitė, R.; Strumilienė, E.; Gruslys, V.; Zablockis, R.; Danila, E. Relationship between radiologic patterns, pulmonary function values and bronchoalveolar lavage fluid cells in newly diagnosed sarcoidosis. J Thorac Dis. 2017, 9, 88–95. [Google Scholar] [CrossRef]
- Aleksonienė, R.; Besusparis, J.; Gruslys, V.; Jurgauskienė, L.; Laurinavičienė, A.; Laurinavičius, A.; Malickaitė, R.; Norkūnienė, J.; Zablockis, R.; Žurauskas, E.; Danila, E. CD31+, CD38+, CD44+, and CD103+ lymphocytes in peripheral blood, bronchoalveolar lavage fluid and lung biopsy tissue in sarcoid patients and controls. J Thorac Dis. 2021, 13, 2300–2318. [Google Scholar] [CrossRef]
- Costabel, U.; Hunninghake, G.W. ATS/ERS/WASOG statement on sarcoidosis. Sarcoidosis Statement Committee. American Thoracic Society. European Respiratory Society. World Association for Sarcoidosis and Other Granulomatous Disorders. Eur Respir J. 1999, 14, 735–737. [Google Scholar] [CrossRef]
- Erdal, B.S.; Crouser, E.D.; Yildiz, V.; King, M.A.; Patterson, A.T.; Knopp, M.V.; Clymer, B.D. Quantitative computerized two-point correlation analysis of lung CT scans correlates with pulmonary function in pulmonary sarcoidosis. Chest. 2012, 142, 1589–1597. [Google Scholar] [CrossRef]
- Simmering, J.; Stapleton, E.M.; Polgreen, P.M.; Kuntz, J.; Gerke, A.K. Patterns of medication use and imaging following initial diagnosis of sarcoidosis. Respir Med. 2021, 189, 106622. [Google Scholar] [CrossRef] [PubMed]
- Akram, M.J.; Khalid, U.; Abu Bakar, M.; Butt, F.M.; Ashraf, MB. Sarcoidosis: epidemiology, characteristics, and outcomes over 10 years - a single-center study in Pakistan. Expert Rev Respir Med. 2022, 16, 133–143. [Google Scholar] [CrossRef] [PubMed]
- Casal, A.; Suárez-Antelo, J.; Soto-Feijóo, R.; Ferreiro, L.; Rodríguez-Núñez, N.; Lama, A.; Riveiro, V.; Toubes, M.E.; Lourido, T.; Ricoy, J.; Rábade, C.; Zamarrón, C.; Rodríguez, C.; Abelleira, R.; Álvarez-Dobaño, J.M.; Golpe, A.; de Alegría, A.M.; Antúnez, J.R.; Gude, F.; Valdés, L. Sarcoidosis. Disease progression based on radiological and functional course: Predictive factors. Heart Lung. 2022, 56, 62–69. [Google Scholar] [CrossRef]
- Schimmelpennink, M.C.; Meek, D.B.; Vorselaars, A.D.M.; Langezaal, L.C.M.; van Moorsel, C.H.M.; van der Vis, J.J.; Veltkamp, M.; Grutters, J.C. Characterization of the PF-ILD phenotype in patients with advanced pulmonary sarcoidosis. Respir Res. 2022, 23, 169. [Google Scholar] [CrossRef] [PubMed]
- Bonham, C.A.; Strek, M.E.; Patterson, K.C. From granuloma to fibrosis: sarcoidosis associated pulmonary fibrosis. Curr Opin Pulm Med. 2016, 22, 484–91. [Google Scholar] [CrossRef] [PubMed]
- Schenkel, A.R.; Chew, T.W.; Chlipala, E.; Harbord, M.W.N.; Muller, W.A. Different susceptibilities of PECAM-deficient mouse strains to spontaneous idiopathic pneumonitis. Exp Mol Pathol. 2006, 81, 23–30. [Google Scholar] [CrossRef] [PubMed]
- Marelli-Berg, F.M.; Clement, M.; Mauro, C.; Caligiuri, G. An immunologist’s guide to CD31 function in T-cells. J Cell Sci 2013, 126, 2343–2352. [Google Scholar] [CrossRef]
- Lishnevsky, M.; Young, L.C.; Woods, S.J.; Groshong, S.D.; Basaraba, R.J.; Gilchrist, J.M.; Higgins, D.M.; Gonzalez-Juarrero, M.; Bass, T.A.; Muller, W.A.; Schenkel, A.R. Microhemorrhage is an early event in the pulmonary fibrotic disease of PECAM-1 deficient FVB/n mice. Exp Mol Pathol. 2014, 97, 128–136. [Google Scholar] [CrossRef]
- Guedes, A.G.; Jude, J.A.; Paulin, J.; Rivero-Nava, L.; Kita, H.; Lund, F.E.; Kannan, M.S. Airway responsiveness in CD38-deficient mice in allergic airway disease: studies with bone marrow chimeras. Am J Physiol Lung Cell Mol Physiol. 2015, 308, L485–L493. [Google Scholar] [CrossRef]
- Newman, D.K.; Fu, G.; McOlash, L.; Schauder, D.; Newman, P.J.; Cui, W.; Rao, S.; Johnson, B.D.; Gershan, J.A.; Riese, M.J. PECAM-1 (CD31) expression in naïve and memory, but not acutely activated, CD8+ T cells. J Leukoc Biol. 2018, 104, 883–893. [Google Scholar] [CrossRef]
- Ziora, D.; Jastrzębski, D.; Adamek, M.; Czuba, Z.; Kozielski, J.J.; Grzanka, A.; Kasperska-Zajac, A. Circulating concentration of markers of angiogenic activity in patients with sarcoidosis and idiopathic pulmonary fibrosis. BMC Pulm Med. 2015, 15, 113. [Google Scholar] [CrossRef] [PubMed]
- Shimizu, Y.; Van Seventer, G.A.; Siraganian, R.; Wahl, L.; Shaw, S. Dual role of the CD44 molecule in T cell adhesion and activation. J Immunol. 1989, 143, 2457–63. [Google Scholar] [CrossRef]
- Goodison, S.; Urquidi, V.; Tarin, D. CD44 cell adhesion molecules. Mol Pathol. 1999, 52, 189–96. [Google Scholar] [CrossRef] [PubMed]
- Rivera, N.V.; Hagemann-Jensen, M.; Ferreira, M.A.R.; Kullberg, S.; Eklund, A.; Martin, N.G.; Padyukov, L.; Grunewald, J. Common variants of T-cells contribute differently to phenotypic variation in sarcoidosis. Sci Rep. 2017, 7, 5623. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Zhang, X.; Long, M.; Yuan, M.; Yin, J.; Luo, W.; Wang, S.; Cai, Y.; Jiang, W.; Chao, J. Macrophage-derived GPNMB trapped by fibrotic extracellular matrix promotes pulmonary fibrosis. Commun Biol. 2023, 6, 136. [Google Scholar] [CrossRef] [PubMed]
- Culty, M.; O’Mara, T.E.; Underhill, C.B.; Yeager, H. Jr.; Swartz, R.P. Hyaluronan receptor (CD44) expression and function in human peripheral blood monocytes and alveolar macrophages. J Leukoc Biol. 1994, 56, 605–11. [Google Scholar] [CrossRef] [PubMed]
- d'Alessandro, M.; Carleo, A.; Cameli, P.; Bergantini, L.; Perrone, A.; Vietri, L.; Lanzarone, N.; Vagaggini, C.; Sestini, P.; Bargagli, E. BAL biomarkers' panel for differential diagnosis of interstitial lung diseases. Clin Exp Med. 2020, 20, 207–16. [Google Scholar] [CrossRef]
- Sung, S.S.; Fu, S.M.; Rose, C.E. Jr.; Gaskin, F.; Ju, S.T.; Beaty, S.R. A major lung CD103 (alphaE)-beta7 integrin-positive epithelial dendritic cell population expressing Langerin and tight junction proteins. J Immunol. 2006, 176, 2161–72. [Google Scholar] [CrossRef]
- Beauchamp, N.M.; Yammani, R.D.; Alexander-Miller, M.A. CD8 marks a subpopulation of lung-derived dendritic cells with differential responsiveness to viral infection and toll-like receptor stimulation. J Virol. 2012, 86, 10640–50. [Google Scholar] [CrossRef]
- Laidlaw, B.J.; Zhang, N.; Marshall, H.D.; Staron, M.M.; Guan, T.; Hu, Y.; Cauley, L.S.; Craft, J.; Kaech, S.M. CD4+ T cell help guides formation of CD103+ lung-resident memory CD8+ T cells during influenza viral infection. Immunity. 2014, 41, 633–45. [Google Scholar] [CrossRef]
- Bernatchez, E.; Gold, M.J.; Langlois, A.; Lemay, A.M.; Brassard, J.; Flamand, N.; Marsolais, D.; McNagny, K.M.; Blanchet, MR. Pulmonary CD103 expression regulates airway inflammation in asthma. Am J Physiol Lung Cell Mol Physiol. 2015, 308, L816–L826. [Google Scholar] [CrossRef] [PubMed]
- McMaster, S.R.; Wein, A.N.; Dunbar, P.R.; Hayward, S.L.; Cartwright, E.K.; Denning, T.L.; Kohlmeier, J.E. Pulmonary antigen encounter regulates the establishment of tissue-resident CD8 memory T cells in the lung airways and parenchyma. Mucosal Immunol. 2018, 11, 1071–8. [Google Scholar] [CrossRef]
- Wu, H.; Liao, W.; Li, Q.; Long, H.; Yin, H.; Zhao, M.; Chan, V.; Lau, C.S.; Lu, Q. Pathogenic role of tissue-resident memory T cells in autoimmune diseases. Autoimmun Rev. 2018, 17, 906–911. [Google Scholar] [CrossRef] [PubMed]
- d'Alessandro, M.; Gangi, S.; Cavallaro, D.; Bergantini, L.; Mezzasalma, F.; Cattelan, S.; Baglioni, S.; Abbritti, M.; Cameli, P.; Bargagli, E. CD103 Expression on Regulatory and Follicular T Cells in Lymph Nodes, Bronchoalveolar Lavage Fluid and Peripheral Blood of Sarcoidosis Patients. Life (Basel). 2022, 12, 762. [Google Scholar] [CrossRef] [PubMed]
- Helmers, R.A.; Dayton, C.S.; Floerchinger, C.; Hunninghake, G.W. Bronchoalveolar lavage in interstitial lung disease: effect of volume of fluid infused. J Appl Physiol (1985). 1989, 67, 1443–6. [Google Scholar] [CrossRef] [PubMed]
- Nishimura, K.; Itoh, H.; Kitaichi, M.; Nagai, S.; Izumi, T. Pulmonary sarcoidosis: correlation of CT and histopathologic findings. Radiology. 1993, 189, 105–9. [Google Scholar] [CrossRef] [PubMed]
- Criado, E.; Sánchez, M.; Ramírez, J.; Arguis, P.; de Caralt, T.M.; Perea, R.J.; Xaubet, A. Pulmonary sarcoidosis: typical and atypical manifestations at high-resolution CT with pathologic correlation. Radiographics. 2010, 30, 1567–86. [Google Scholar] [CrossRef] [PubMed]
- Keijsers, R.G.; van den Heuvel, D.A.; Grutters, J.C. Imaging the inflammatory activity of sarcoidosis. Eur Respir J. 2013, 41, 743–51. [Google Scholar] [CrossRef]
- Distefano, G.; Vancheri, A.; Palermo, M.; Tiralongo, F.; Foti, P.V.; Mauro, L.A.; Vancheri, C.; Basile, A.; Palmucci, S. Morphological Patterns of Sarcoidosis and Clinical Outcome: Retrospective Analysis through a Multidisciplinary Approach. Diagnostics (Basel). 2020, 10, 212. [Google Scholar] [CrossRef]
- Polverosi, R.; Russo, R.; Coran, A.; Battista, A.; Agostini, C.; Pomerri, F.; Giraudo, C. Typical and atypical pattern of pulmonary sarcoidosis at high-resolution CT: relation to clinical evolution and therapeutic procedures. Radiol Med. 2014, 119, 384–92. [Google Scholar] [CrossRef]
- Duan, J.; Xu, Y.; Zhu, H.; Zhang, H.; Sun, S.; Sun, H.; Wang, W.; Xie, S. Relationship between CT activity score with lung function and the serum angiotensin converting enzyme in pulmonary sarcoidosis on chest HRCT. Medicine (Baltimore). 2018, 97, e12205. [Google Scholar] [CrossRef] [PubMed]
- McDonnell, M.J.; Saleem, M.I.; Wall, D.; Gilmartin, J.J.; Rutherford, R.M.; O'Regan, A. Predictive value of C-reactive protein and clinically relevant baseline variables in sarcoidosis. Sarcoidosis Vasc Diffuse Lung Dis. 2016, 33, 331–340. [Google Scholar] [PubMed]
- Silva, A.L.; Melo, N.; Caetano Mota, P.; Lima, B.; Pereira, J.M.; Cunha, R.; Guimarães, S.; Souto-Moura, C.; Morais, A. Pulmonary Sarcoidosis: Prognostic Factors at Diagnosis in Patients from North of Portugal. Reumatol Clin (Engl Ed). 2020, 16, 468–472. [Google Scholar] [CrossRef] [PubMed]
- Kirkil, G.; Lower, E.E.; Baughman, R.P. Predictors of Mortality in Pulmonary Sarcoidosis. Chest. 2018, 153, 105–113. [Google Scholar] [CrossRef] [PubMed]
- Danila, E.; Jurgauskiene, L.; Malickaite. R. BAL fluid cells and pulmonary function in different radiographic stages of newly diagnosed sarcoidosis. Adv Med Sci. 2008, 53, 228–33. [Google Scholar] [CrossRef]
- Danila, E.; Zurauskas, E.; Loskutoviene, G.; Zablockis, R.; Nargela, R.; Birzietyte, V.; Valentinaviciene, G. Significance of bronchoscopic lung biopsy in clinical practice. Adv Med Sci. 2008, 53, 11–6. [Google Scholar] [CrossRef]
- Danila, E.; Zurauskas, E. Diagnostic value of epithelioid cell granulomas in bronchoscopic biopsies. Intern Med. 2008, 47, 2121–6. [Google Scholar] [CrossRef]
- Danila, E.; Jurgauskiene, L.; Norkuniene, J.; Malickaite, R. BAL fluid cells in newly diagnosed pulmonary sarcoidosis with different clinical activity. Ups J Med Sci. 2009, 114, 26–31. [Google Scholar] [CrossRef]
- Danila, E.; Norkūniene, J.; Jurgauskiene, L.; Malickaite, R. Diagnostic role of BAL fluid CD4/CD8 ratio in different radiographic and clinical forms of pulmonary sarcoidosis. Clin Respir J. 2009, 3, 214–21. [Google Scholar] [CrossRef]
- Pocienė, I.; Gauronskaitė, R.; Galkauskas, D.; Mainelis, A.; Gruslys, V.; Danila, E. Age as a Risk Factor in the Occurrence of Complications during or after Bronchoscopic Lung Biopsy. Geriatrics (Basel). 2022, 7, 34. [Google Scholar] [CrossRef]
- Ozyilmaz, E.; Ozturk, O.G.; Durmaz, A.; Othman Hasan, O.; Guzelbaba, B.; Seydaoglu, G.; Kuleci, S.; Hanta, I.; Erken, E.; Kocabas, A. Early prediction of sarcoidosis prognosis with HLA typing: a 5 year follow-up study. Sarcoidosis Vasc Diffuse Lung Dis. 2018, 35, 184–191. [Google Scholar] [CrossRef] [PubMed]
- Ishiyama, M.; Soine, L.A.; Vesselle, H.J. Semi-quantitative metabolic values on FDG PET/CT including extracardiac sites of disease as a predictor of treatment course in patients with cardiac sarcoidosis. EJNMMI Res. 2017, 7, 67. [Google Scholar] [CrossRef]
Figure 1.
Examples of scores for nodules in the lung. a. Score 1 = 1–5 nodules. b. Score 2 = 6–10 nodules (samples show 8 nodules in the left lung lower lobe). c. Score 4 = >15 nodules.
Figure 1.
Examples of scores for nodules in the lung. a. Score 1 = 1–5 nodules. b. Score 2 = 6–10 nodules (samples show 8 nodules in the left lung lower lobe). c. Score 4 = >15 nodules.
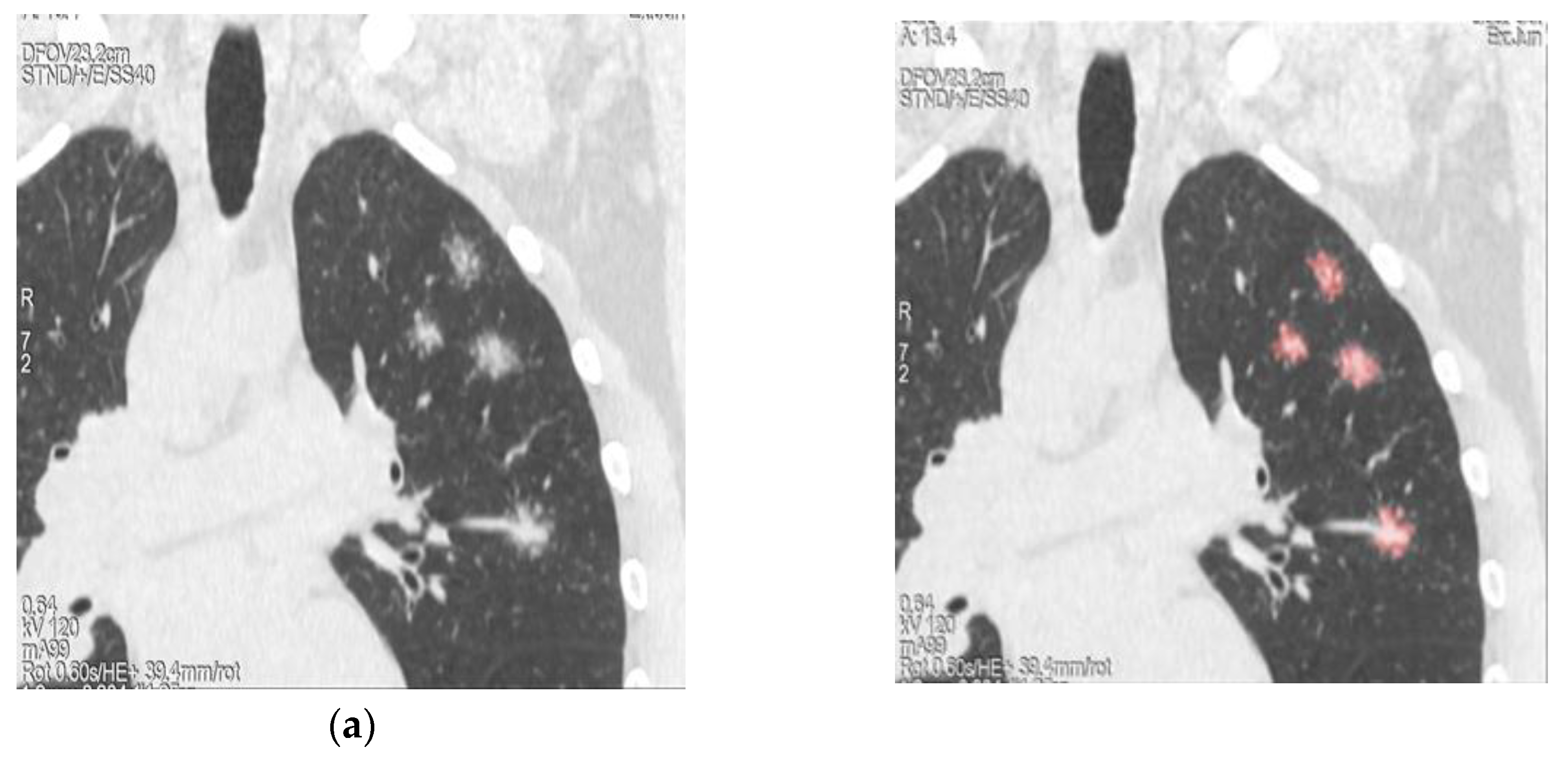
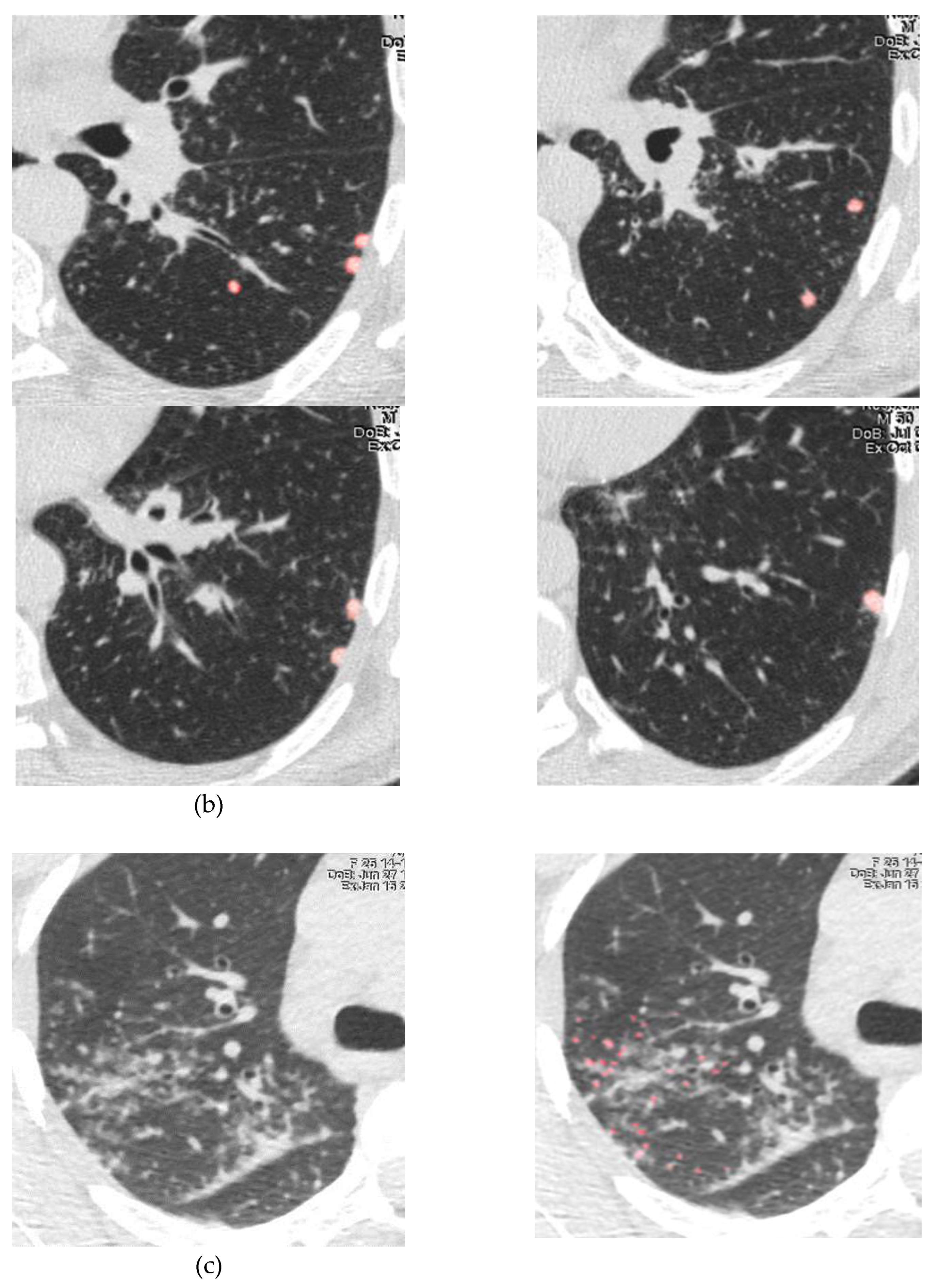
Figure 2.
ROC curves for predictors of sarcoidosis progression. a. Blood CD4+CD31+. b. Blood CD4+CD44+. c. BALF CD8+CD31+. d. BALF CD8+CD103+. e. Number of lung nodules on CT.
Figure 2.
ROC curves for predictors of sarcoidosis progression. a. Blood CD4+CD31+. b. Blood CD4+CD44+. c. BALF CD8+CD31+. d. BALF CD8+CD103+. e. Number of lung nodules on CT.
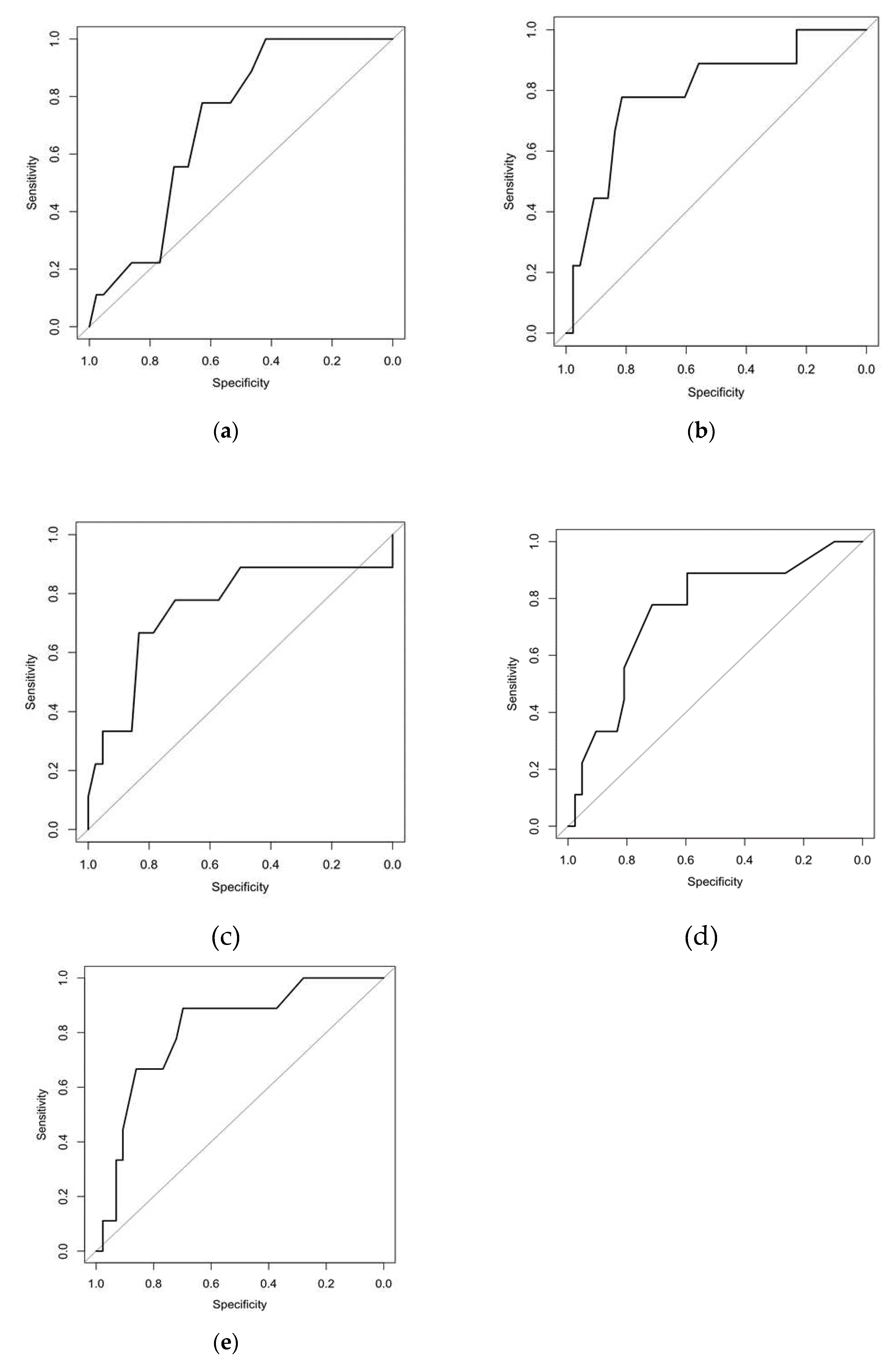

Table 1.
Characteristics of the study population.
| Demographics | Sarcoidosis patients (n=71) |
|---|---|
| Sex (male/female) | 38/33 |
| Age (years) | 37 (21–68) |
| Löfgren syndrome (yes/no) | 27/44 |
| Smoker (yes/never) | 25/46 |
| FVC, % pred | 104±15 |
| FEV1, % pred | 97±13 |
| FEV1/FVC, % | 79±6 |
| TLC, % pred | 99±12 |
| VC, % pred | 106±14 |
| RV, % pred | 90±21 |
| DLCO, % pred | 76±11 |
| BALF total cells count, x 106/mL | 375±192 |
| BALF macrophages, % | 60.8±19.2 |
| BALF lymphocytes, % | 38.4±19.2 |
| BALF neutrophils, % | 0.5±0.8 |
| BALF eosinophils, % | 0.2±0.3 |
| BALF CD4, % | 69.9±17.7 |
| BALF CD8, % | 18.8±13.3 |
| BALF CD4+/CD8+ | 6.1±4.8 |
Age is presented as the median and range. Parameters of pulmonary function are presented as the mean ± standard deviation. FVC, forced vital capacity; pred, predicted; FEV1, forced expiratory volume in one second; TLC, total lung capacity; VC, vital capacity; RV, residual capacity; DLCO, diffusing capacity of carbon monoxide. BALF – bronchoalveolar lavage fluid. Data are presented as mean ± standard deviation.
Table 2.
Lymphocyte subtypes/activation markers expression in blood and BALF.
| Cells | Blood (n=71) |
BALF (n=71) |
|---|---|---|
| CD4+, % | 41.1±8.5 | 69.9±17.7 |
| CD8+, % | 27.1±9.0 | 18.8±13.3 |
| CD4+/CD8+ | 1.7±0.7 | 6.1±4.8 |
| CD31+CD4+, % | 12.5±6.5 | 5.9±4.5 |
| CD38+CD4+, % | 23.4±9.1 | 24.0±14.1 |
| CD44+CD4+, % | 45.6±9.9 | 75.7±13.4 |
| CD103+CD4+, % | 2.3±6.9 | 8.7±8.2 |
| CD31+CD8+, % | 19.1±7.7 | 10.1±8.5 |
| CD38+CD8+, % | 20.3±7.4 | 5.9±6.5 |
| CD44+CD8+, % | 38.8±11.1 | 20.9±12.5 |
| CD103+CD8+, % | 3.7±4.7 | 13.3±11.3 |
Data are presented as the mean ± standard deviation.
Table 3.
Lung tissue lymphocyte subsets and collagen in sarcoidosis patients.
| Cells | Sarcoidosis (n=35) |
|---|---|
| CD4+, total | 7375±8391 |
| CD8+, total | 3873±7067 |
| CD38+, total | 2803.4±5167 |
| CD44+, total | 10322±8094 |
| CD103+, total | 1532±1589 |
| CD4+, % | 19.1±11.7 |
| CD8+, % | 8.1±6.3 |
| CD38+, % | 6.0±6.2 |
| CD44+, % | 27.2±10.3 |
| CD103+, % | 4.3±3.0 |
| CD4+ density, mm2 | 705±519 |
| CD8+ density, mm2 | 315±269 |
| CD38+ density, mm2 | 235±266 |
| CD44+ density, mm2 | 1002±502 |
| CD103+ density, mm2 | 158±118 |
| Collagen, % | 20.2±7.4 |
Data are presented as the mean ± standard deviation.
Table 4.
Cut-off values, sensitivity, specificity, and odds ratio for predictors of sarcoidosis progression.
Table 4.
Cut-off values, sensitivity, specificity, and odds ratio for predictors of sarcoidosis progression.
| Criteria | Cut-off | Sp | Sn | AUC | AUC (CI 95%) | OR | CI 95% | P value |
|---|---|---|---|---|---|---|---|---|
| CD4+CD31+ blood, % | ≤14.5 | 0.419 | 1.000 | 0.708 | 0.555; 0.861 | 13.78 | 0.75; 252.06 | 0.020 |
| CD4+CD44+ blood, % | ≤37.5 | 0.814 | 0.778 | 0.795 | 0.622; 0.968 | 15.31 | 2.66; 88.04 | <0.001 |
| CD8+CD31+ BALF, % | ≥13.5 | 0.833 | 0.667 | 0.751 | 0.536; 0.967 | 10.00 | 2.01; 49.83 | 0.010 |
| CD8+CD103+ BALF, % | ≥15.5 | 0.714 | 0.778 | 0.754 | 0.574; 0.933 | 8.75 | 1.59; 48.29 | 0.010 |
| Number of lung nodules | ≥15.0 | 0.698 | 0.889 | 0.810 | 0.658; 0.962 | 18.46 | 2.09; 163.05 | <0.001 |
Sp – specificity, Sn – sensitivity, OR – odds ratio. 95 % CI – 95 % confidence interval, AUC – area under the curve.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



