
Submitted:
05 April 2023
Posted:
06 April 2023
You are already at the latest version
Abstract
Background: This practice guideline was developed by the Chronic Kidney Disease (CKD) Task Force, which was composed of clinical and methodological experts. The Saudi Arabian Ministry of Health and its Health Holding Company commissioned this guideline project to support the realization of the Vision 2030's healthcare transformation pillar. Methods: The guideline synthesis was guided by the GRADE-ADOLOPMENT methodology. Results: The final adoloped guideline addressed 12 clinical questions on blood pressure management in patients with CKD through a set of recommendations and performance measures. The recommendations included antihypertensive agents in children, non-renin angiotensin system inhibition (Non-RASi) vs RASi in adults, intensive vs standard blood pressure targets, early vs late assessment for kidney replacement therapy (KRT), late vs early preparation strategy for KRT, CKD symptoms during assessment for KRT or conservative management, initiation of KRT in patients with deteriorating CKD, choice of KRT modality or conservative management in certain CKD patient groups, changing or discontinuing KRT modalities, review frequency for KRT or conservative management, and Information, education and support. Conclusions: These conditional recommendations were based on low to very low certainty of evidence that highlights the need for high-quality randomized trials comparing different antihypertensive agents in patients with CKD.
Keywords:
chronic kidney disease
; antihypertensive
; practice guidelines
; recommendations
; performance measures
; GRADE
; adolopment
; AGREE II
; RIGHT-Ad@pt
; evidence-based healthcare
; Saudi Arabia
1. Summary of recommendations
1.1. Background
This guideline was developed by a chronic kidney disease (CKD) Task Force of local experts under the auspices of The Saudi Arabian Ministry of Health and its Health Holding Company that established a National Guidelines Center to support the Vision 2030 healthcare transformation pillar and new Model of Care [1].
CKD is a major public health issue globally and in Saudi Arabia, with its incidence and prevalence increasing significantly over the last several decades. Kidney disease is the third leading cause of death in Saudi Arabia, with the country's age-adjusted death rate from kidney disease ranking fifth in the world [2].
An international conference in 2019 by Kidney Disease Improving Global Outcomes (KDIGO) acknowledged that, unlike some chronic diseases with established screening strategies, there was no agreement on whether health systems and governments should prioritize early detection and interventions for CKD. The conference consensus was that CKD screening, risk stratification, and treatment should be implemented immediately for high-risk individuals, ideally in primary or community care settings with local context tailoring.
Despite the fact that guidelines have the potential to slow the progression of CKD, adherence has been shown to be low in typical practice settings around the world [3]. One of the primary goals of these guidelines is to encourage adherence to evidence-based CKD management recommendations.
1.2. Methods
These CKD national guidelines are based on updated and original systematic reviews of evidence conducted in partnership with Elsevier Clinical Solutions, Epistemonikos Foundation, and Rezonanz with international clinical and methodological expert collaborators. The panel followed standards and best practices for guideline development recommended by the Guidelines International Network (GIN) [4,5]. The panel used the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) approach to assess the certainty in the evidence of effects and formulate recommendations, the GIN-McMaster Guideline Development Checklist, and the GRADE-ADOLOPMENT methodology that was developed by the McMaster GRADE Center as a result of establishing a national guideline program by the Saudi Arabian Ministry of Health between 2012 and 2015 [6,7].
1.3. Interpretation of strong and conditional (weak) recommendations
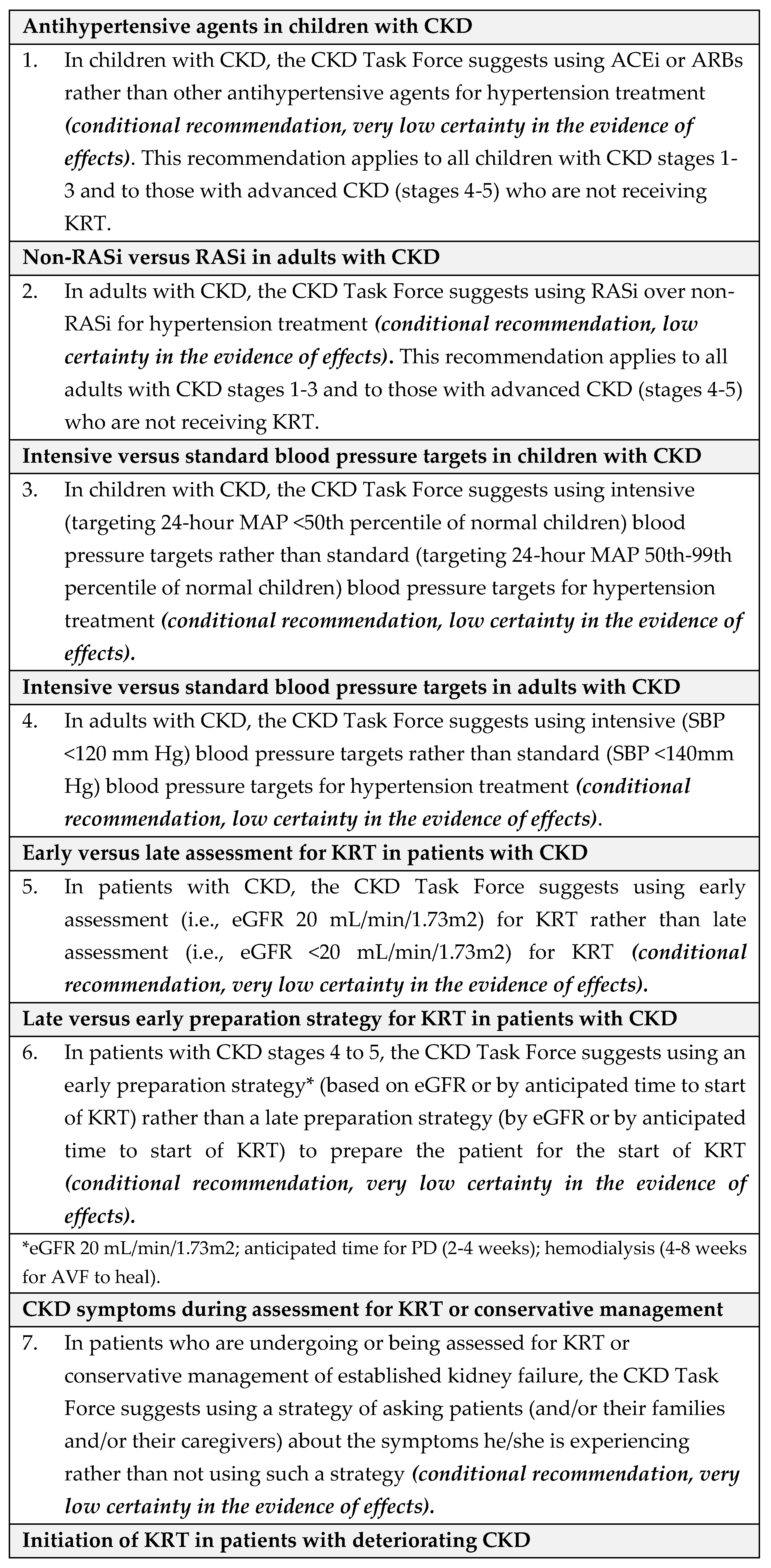
The strength of a recommendation is expressed as either strong ("the CKD Task Force recommends..."), or conditional ("the CKD Task Force suggests…") and has the following interpretation (Table 1.1) and (Table 1.2).

Table 1.1.
Summary of Recommendations for Blood Pressure Management and Kidney Replacement Therapy in Adults and Children with CKD in Saudi Arabia.
Table 1.1.
Summary of Recommendations for Blood Pressure Management and Kidney Replacement Therapy in Adults and Children with CKD in Saudi Arabia.
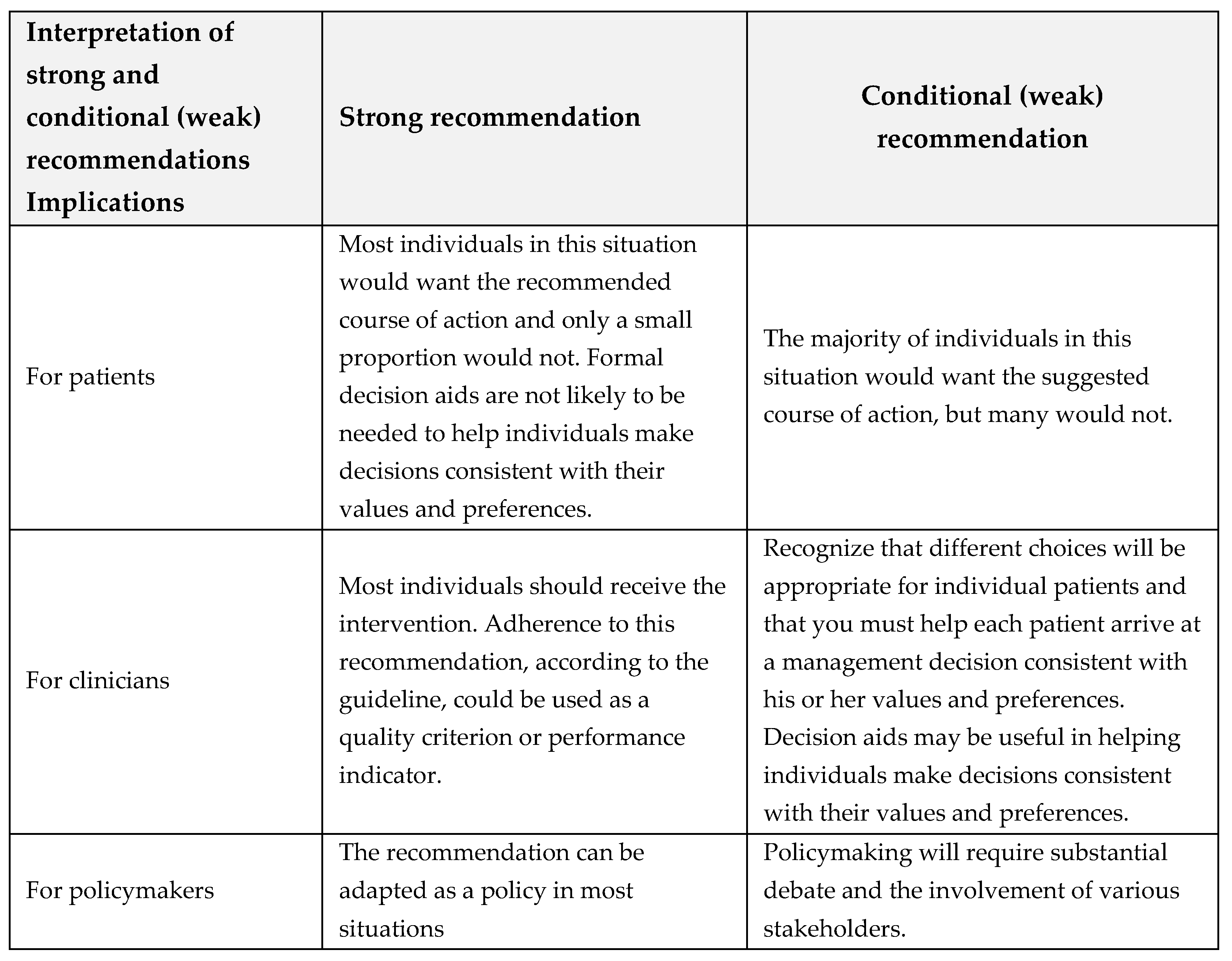
Table 1.2.
Summary of Recommendations for Blood Pressure Management and Kidney Replacement Therapy in Adults and Children with CKD in Saudi Arabia.
Table 1.2.
Summary of Recommendations for Blood Pressure Management and Kidney Replacement Therapy in Adults and Children with CKD in Saudi Arabia.
2. Introduction
2.1. The aim of this guideline
The aim of this CPG is to assist healthcare workers caring for adults and children with CKD choose the best antihypertensive medication and decide how intensively to treat high blood pressure in CKD patients with hypertension. Implementing these recommendations is expected to slow CKD progression and, eventually, reduce patients' need for KRT services, improving quality of life and lowering healthcare costs.
2.2. Description of the health problem(s)
Chronic Kidney Disease (CKD) is defined as "abnormalities of kidney structure or function, present for >3 months, with implications for the health of an individual, which can occur abruptly and either resolve or become chronic. End-stage kidney disease (ESKD) is the most serious complication of CKD [8].
The classification of CKD is based on the cause, the glomerular filtration rate category (G1-G5), and the albuminuria category (A1-A3). The term CKD refers to a group of diseases that affect kidney structure and/or function. The clinical manifestation is determined by the underlying cause, severity, and rate of progression.
Patients with early-stage kidney disease are frequently asymptomatic, which delays diagnosis and treatment of the underlying cause. Despite all efforts to improve CKD management, many patients will progress to ESKD and require KRT.
Markers, rather than direct examination of kidney tissue, are used to infer kidney damage. These markers can provide information about the origin or location of the damage, whether it is in the parenchyma, large blood vessels, or collecting systems. Proteinuria, the presence of increased amounts of protein in the urine, and albuminuria, the abnormal loss of albumin in the urine, are two of these markers.
The urinary loss rate is used to express the adult normative values for albuminuria and proteinuria. Albumin excretion rate (AER) and protein excretion rate (PER) are terms used to describe the rate of albumin and protein loss in the urine. Based on AER, CKD is identified by a threshold of 30 mg/24 hours maintained for more than 3 months (roughly equivalent to an albumin: creatinine ratio [ACR] of 30 mg/g or 3mg/mmol in a random untimed urine sample) [9].
Normal protein excretion in children is defined as 4 mg/m2/hour, abnormal proteinuria as 4-40 mg/m2/hour, and nephrotic proteinuria as >40 mg/m2/hour, >1 gm/m2/day in a 24-hour urine collection, or a spot urine protein:creatinine ratio of >2 mg/mg [10,11].
Because of its greater sensitivity for low levels of proteinuria, urine ACR should be used to detect proteinuria in adults, children, and young people rather than protein:creatinine ratio. To confirm the result, an ACR between 3 mg/mmol and 70 mg/mmol should be measured in a subsequent early morning sample. If the initial ACR is 70 mg/mmol or higher, no repeat sample is required. Proteinuria with a confirmed ACR of 3 mg/mmol is considered clinically significant [12].
The presence or absence of systemic disease, as well as the location of pathologic-anatomic findings within the kidney, are used to classify CKD [13]. For additional details, refer to the relevant CKD classification table in the full CPG document (Supplementary material, Document S1).
2.3. Epidemiology
Over the last several decades, the incidence and prevalence of CKD have reportedly increased in Saudi Arabia. This could be due to changes in lifestyle (and thus an increase in diabetes), population growth, an increase in life expectancy (due to a shift in age demographics), and urbanization [14]. However, there are no nationwide population-based registries that reflect the true burden of CKD and ESKD, and it is possible that true estimates exceed what is reflected in this current guideline. As a result, current estimates are primarily based on single-center observational studies or studies conducted almost or more than a decade ago [15,16,17,18].
The increasing number of people requiring KRT reflects the high burden of kidney disease. According to Saudi Center for Organ Transplantation (SCOT) estimates, there were 21,496 dialysis patients in Saudi Arabia in 2020, with 19,715 on hemodialysis (92%) and 1,781 on peritoneal dialysis (PD) (8%). The figure below shows that the number of patients undergoing dialysis, both modalities combined, increases by a net 5% each year (reproduced with permission from reference [19]).
2.4. Description of the target users
This CPG is intended for primary (family medicine), secondary (general internists and pediatricians), and tertiary (kidney specialists) healthcare providers who care for children and adults with CKD in Saudi Arabia, as well as their families and caregivers. It also intends to inform the work of dialysis nurses, clinical pharmacists, KRT and conservative management providers, as well as healthcare leaders involved in the planning of local and regional KRT services and policymakers developing national CKD health population programs.
3. Materials and Methods
3.1. Organization, Panel Composition, Planning and Coordination
Chronic Kidney Disease (CKD) Task Force
A multidisciplinary local group of ten experts led by a Clinical Lead developed this guideline. Adult and pediatric nephrologists, KT specialists, a clinical pharmacist, and a patient representative from Saudi Arabia comprised this Task Force. Members came from a variety of Ministry of Health, University, Military, and National Guard institutions, geographical regions, and medical societies, with several participants having received epidemiology and guideline methodology training (KAA, SA, YSA, MRJ, KIA, MA, SKA, JAK, AHM, and MA).
Guideline Methodology Support Team
An international team of 15 experts based at (or contracted by) Elsevier assisted the CKD Task Force's work. The CKD Task Force and Guideline Support Team communicated primarily through WhatsApp groups created specifically to share content and files, updates, arrange meetings, share meeting links, and solicit feedback. Email was primarily used to communicate meeting invitations and attachments (KB, JJYN, HG, XA, HJ, MS, RC, JSV, KB, JG, MS, SB, SF, NG, and SPV).
The CKD Task Force and Elsevier Guideline Team held six remotely held 2:30-3:00 hour-long working sessions to select the PICO questions to be included (guideline scope), conduct outcomes prioritization, and formulate recommendations. Prior to workshops and during the draft finalization phase, pre-session surveys were used to elicit Task Force members' opinions. Before each meeting, the agenda and relevant pre-reading materials were shared with the CKD Task Force, and minutes were distributed after each session.
For details on the names, roles, and geographical locations of the members of both collaborative teams refer to in the full CPG document (Supplementary material, Document S1).
3.2. Guideline Funding and Management of Conflicts of Interest
The members of the CKD Task Force, including the Clinical Lead and invited external peer reviewers, did not receive financial compensation for their contributions to the development of this guideline. The Guideline Support Team's activities were supported by a contract between the Ministry of Health's Health Holding Company and Elsevier Ltd.
All members of the CKD Task Force, Guideline Support team, and external peer reviewers were asked to declare any relevant Conflicts of Interest from the previous four years using a Declaration of Interest form customized from the World Health Organization form. They were also asked to keep the National Guidelines Center's Program Board informed of any changes to their conflicts of interest.
Declarations covered both direct (financial) and indirect (non-financial) conflicts relevant to the guideline topic up to agreed-upon thresholds. They were managed using the GRADEpro guideline development tool and securely stored in accordance with international best practices as well as local data retention, confidentiality, and security guidelines. Declared conflicts of interest were to be assessed by a Responsible Officer nominated by the Guidelines Center Program Board in accordance with WHO assessment steps to ensure that only participants free of conflicts voted on related recommendations.
Any conflicts of interest were read out at the start of each Task Force meeting and checked for updates. In all resulting reports and work products, a summary of all declarations and actions taken to manage any declared interests is published.
All Task Force members confirmed that they had no conflicts of interest to declare. All members of the Guideline Support Team declared that they were Elsevier salaried or freelance employees contracted to support the establishment of the National Guidelines Center and the development of its first 12 guidelines.
3.3. Selection of questions and outcomes of interest
Identifying the source guideline(s) aligned with local needs
As a starting point for guideline adaptation, the Guideline Support Team conducted a systematic search for high-quality local (Saudi or Gulf region) or international guidelines. The Appraisal of Guidelines for Research and Evaluation Instrument Version II (or AGREE II) was used to evaluate the quality of the identified candidate guidelines ("AGREE II. https://www.agreetrust.org/wp-content/uploads/2017/12/AGREE-II-Users-Manual-and-23-item-Instrument-2009-Update-2017.pdf," n.d.). As a source of clinical questions, the following two source guidelines were chosen:
The CKD Task Force prioritized the 20 clinical questions addressed by these two source guidelines for the Saudi Arabia setting. First, CKD Task Force members rated the clinical questions on a 9-point scale via an online survey. The clinical questions were ranked based on the CKD Task Force members' median scores. During the scoping workshop, 11 questions were identified as the most pertinent, with the patient representative suggesting an additional question (Question 12). The 12 prioritized health questions were reported in the full CPG document (Supplementary material).
The voting quorum was established at 70% of all Task Force members with voting rights attending a session or providing input via email/survey response. The Task Force used consensus-based decision making during scoping, recommendations, and finalization, with a 70% consensus threshold.
The CKD Task Force predetermined the outcomes of interest for each question by rating their importance in an online survey. Outcomes included were those reported in the original resources as well as others deemed critical for decision-making by the CKD Task Force. For details on the list of prioritized outcomes per each question refer to in the full CPG document (Supplementary material, Document S1).
3.4. Evidence Review and Development of Recommendations
For each of the questions addressed, the original guidelines included SoF tables or evidence profiles. The electronic searches of the systematic reviews included in the original source guidelines were updated by the Guideline Support Team. They also conducted a thorough search of regional evidence on epidemiology, patient values and preferences, resource utilization, accessibility, feasibility, and impact on health equity (reported in the full CPG document, Supplementary material).
The Center of Health Technology Assessment - Ministry of Health provided local information on required resources and cost-effectiveness. The Guideline Support Team developed EtD frameworks that summarized each of the data points used in the original guideline as well as all relevant regional information identified using the GRADEpro guideline development tool (McMaster University, Hamilton, ON, Canada, and Evidence Prime, Inc., Kraków, Poland). The team calculated the risk difference by multiplying the pooled risk ratio by the baseline risk of each outcome to estimate the absolute effect of the interventions. The median of the risks observed in the included trials' control groups was used as the baseline risk. The baseline risk observed in large observational studies was taken into account whenever possible.
The GRADE approach was used to categorize the evidence's quality, which was based on judgments about the risk of bias, precision, consistency, directness, and likelihood of publication bias [7].
3.5. Development of recommendations
The CKD Task Force reviewed the original guideline recommendations, updated them in light of new evidence, and adapted them to local circumstances based on literature searches conducted in October 2021 during four online meetings held between 3rd and 17th December, 2021. Baseline risks for prioritized outcomes, patient values and preferences, equity, acceptability, cost-effectiveness and resource impact, feasibility, and implementation were among the local contextual factors considered. The Saudi Health Technology Agency provided additional cost information.
Four approaches were used to consider patient values and preferences including: (1) Obtaining relevant content from the source guidelines that will be adapted; (2) Systematic PubMed searches to summarize the best available evidence published in the last ten years; (3) Clinical experience of members of the CKD Task Force with direct patient contact; and (4) Patient representative input.
Prior to the Recommendations Workshops, the CKD Task Force received evidence summaries for each question as part of the EtD framework.
Following the GRADE approach, the CKD Task Force agreed on the direction and strength of recommendations through group discussion and deliberation [21]. Each EtD criteria judgment and the final recommendation were voted on, with a 70% threshold for each vote.
The recommendations' strength is expressed as either strong ('guideline CKD Task Force recommends...') or conditional ('guideline CKD Task Force suggests...') and has explicit implications (Table 1.1.) [21]. Understanding how to interpret these two grades is critical for making sound clinical decisions.
The overall guideline development process, including funding, CKD Task Force formation, conflict of interest management, internal and external review, and organizational approval, was guided by policies and procedures derived from the Guidelines International Network (GIN)-McMaster Guideline Development Checklist (http://cebgrade.mcmaster.ca/guidecheck.html ) in order to meet Institute of Medicine and GIN recommendations for trustworthy guidelines (For more information on the process refer to the full CPG document in the Supplementary material, Document S1).
3.6. Document review
The CKD Task Force and the Guideline Support Team reviewed and adjusted the draft guideline in an iterative process until a final version was signed off on by the Task Force during a Guideline Finalization Workshop. The CKD Task Force Lead guided the process (For more details on the stepwise approach used by the CKD Task Force to make decisions about EtD criteria and their agreement on the final recommendations refer to the full CPG document, Supplementary material, Document S1).
3.7. Peer review and Approval
The CKD National Guideline draft was peer reviewed by 4 national and international experts who were not directly involved in its development (FS, RR, AA, and MS). All peer reviewers were required to complete a Conflict of Interest form.
The peer review process included a survey with ten questions divided into three sections: evidence synthesis, recommendations, and adoption and implementation. A free-text field was provided after each question for additional inputs.
Some peer reviewers provided additional feedback directly into the draft manuscript in the form of tracked changes or comments. The Guideline Support Team reviewed all comments received and discussed the resulting changes with the Clinical Lead and members of the CKD Task Force, followed by a finalization workshop to address outstanding questions.
Following that, the guideline was submitted for review to nominated members of the Saudi Health Council's (SHC) Scientific Committee, and the draft guideline was posted on the SHC website for public comment. The SHC Scientific Committee officially approved the guideline as a national guideline after evaluating all feedback and making any necessary changes.
3.8. How to use this guideline
This guideline is intended to aid in decision-making rather than to establish a standard of care. As a result, the recommendations in this document should not be interpreted as prescribing a single course of treatment. Variations in practice are to be expected once the clinician considers the patient's needs and preferences, available resources, and institutional or type of practice-specific limitations. Healthcare professionals who use these recommendations should consider how they will be implemented in their own clinical practice.
3.9. Guideline Registration
This guideline is registered with the Guidelines International Network (GIN) Library and Registry: https://guidelines.ebmportal.com/node/70091
3.10. Guideline Reporting Checklists
This CPG has been reported in compliance with two CPG reporting checklists: The Appraisal of Guidelines for Research and Evaluation (AGREE) Reporting Checklist (AGREE Reporting Checklist - AGREE Enterprise website (agreetrust.org)) (Supplementary material: Table S1) and The Reporting Items for Practice Guidelines in Healthcare (RIGHT) extension for Adapted CPGs (RIGHT-Ad@pt Checklist) (RIGHT-Ad@pt Checklist - Right (right-statement.org)) (Supplementary material: Table S2) [22,23]
4. Results
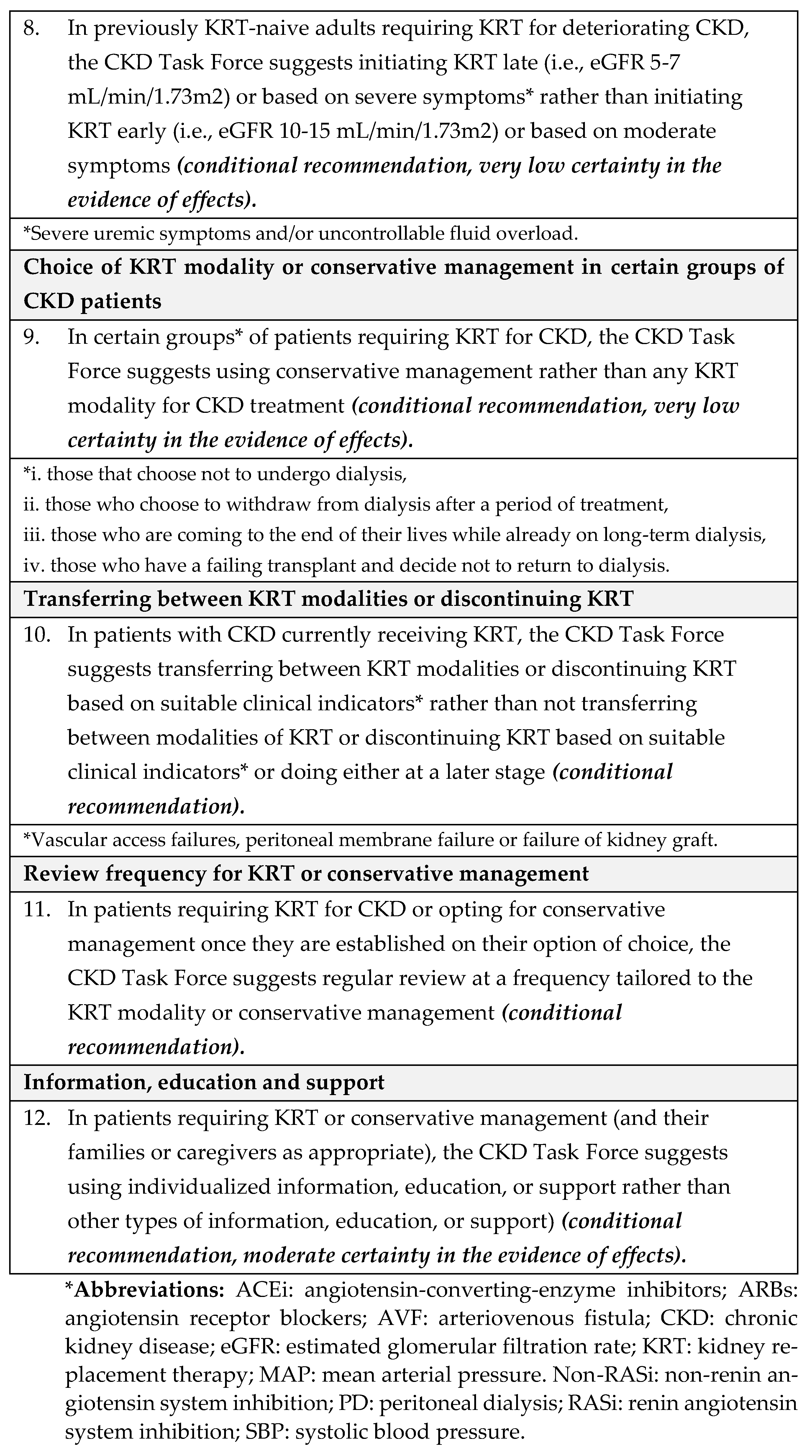
Table 1.2 shows the summary of the recommendations, their strength, and the certainty in the evidence of effects according to the GRADE system. The following are the detailed recommendations, rationale, and related attributes:
4.1. Recommendations
Decision criteria and additional considerations
The CKD Task Force noted that hyperkalemia and progression of CKD (decrease in GFR) were known complications of antihypertensive medications and that the recommendation did not apply to children with advanced CKD who are not receiving dialysis in view of the increased risk of hyperkalemia in this population. They recommended that serum potassium levels be monitored 7-10 days after initiation of therapy and—in addition to GFR and albuminuria—during annual check-ups (more frequently in CKD stages G3b-G5).
Evidence summary
The literature search for the KDIGO 2021 Clinical Practice Guideline for the Management of Blood Pressure (BP) in CKD [8] identified one open-label RCT evaluating the effectiveness of enalapril compared to no enalapril [24]. Our update search conducted in October 2021 found no additional studies for inclusion.
Benefits and harms
The included RCT of 41 children aged 2 to 18 years, with GFR between 15-60 mL/min/1.73 m2 compared enalapril at 0.4 mg/kg /day versus no enalapril [24]. The evidence is very uncertain about the effect of enalapril on kidney failure (relative risk [RR], 0.45; 95% confidence interval [CI], 0.13-1.50; very low certainty in the evidence of effects]. At 12 months, the study found no difference in the rate and speed of GFR decline (mL/min/1.73 m2) (mean difference [MD], -1.2; 95% CI, -4.05 - 1.65; very low certainty in the evidence of effects) but a significantly greater mean proteinuria (urine protein/creatinine [mg/mg]) reduction with enalapril (MD, -1.13; 95% CI -1.82 - -0.44; very low certainty in the evidence of effects). Systolic (mmHg) (MD, -0.6; 95% CI -1.12 - 0.08; very low certainty in the evidence of effects) and diastolic blood pressure (mmHg) (MD, -0.64; 95% CI -1.10 - 0.18; very low certainty in the evidence of effects) over the study period were significantly lower with enalapril. The RCT did not evaluate all-cause or cardiovascular mortality, cardiovascular morbidity, doubling serum creatinine, acute kidney injury, left ventricular hypertrophy, or encephalopathy. The CKD Task Force concluded that the balance between desirable and undesirable effects probably favors the use of antihypertensive agents.
Certainty in the evidence
We rated the overall certainty in the evidence of effects as very low based on the lowest certainty in the evidence for the critical outcomes, owing to very serious risk of bias, and serious imprecision of the estimates.
Values
A nominal group technique SONG-Kids study [25] cited in the 2021 KDIGO guideline [8] aimed to identify important outcomes for young people with CKD and their caregivers. It reported that both children with kidney disease and their caregivers rated kidney function as an important outcome, and blood pressure control was also rated as an important outcome by caregivers. The guideline’s Work Group noted that most patients would value these clinical benefits despite the inconvenience and potential risk of side effects from blood pressure management. The CKD Task Force concluded that due to the insufficient evidence there was possibly important uncertainty about how much people value the main outcomes, so input about their preferences would need to be sought from individual patients or caregivers before initiation of therapy.
Resource use and cost-effectiveness
We did not identify direct evidence on resource requirements for blood pressure treatment but received information from the Saudi Health Technology Agency – Ministry of Health about cost per package of antihypertensive agents (see Cost table in the Appendices of Document S1). A microsimulation model applied to SPRINT showed that intensive blood pressure control prevented cardiovascular disease events and prolonged life regardless of whether benefits were reduced after 5 years or persisted for the patient’s remaining lifetime, at levels below the willingness-to-pay thresholds (51 to 79% below the threshold of $50000 per quality-adjusted life-years and 76 to 93% below the threshold of $100000 per quality-adjusted life-years) [26].
The 2021 KDIGO Work Group [8] noted that in particular when treating patients with CKD (G1–G4, A2) where the indication for antihypertensive therapy was not strong, consideration should be given to the clinical impact on the patient and the costs of starting RASi, including the need for additional clinic visits and lab testing. The CKD Task concluded that blood pressure treatment probably leads to moderate savings as the costs of antihypertensive agents were low compared with those of future complications of CKD, they might prevent such as prevention of future KT or dialysis, as well as possible improvement in future quality of life. They also judged that cost-effectiveness probably favored the intervention given the indirect evidence from the cost-effectiveness study [26].
Other contextual factors
- Equity: We did not identify direct evidence to address equity for this question. The CKD Task Force concluded that given Saudi Arabia’s comprehensive health coverage, there would probably be no disadvantages associated with the use of antihypertensive treatment in children with CKD on equity from implementing the recommendation.
- Acceptability: We did not identify direct evidence to address acceptability for this question. The CKD Task Force used their collective experience with antihypertensive therapy to judge that this pharmacological therapy was acceptable to stakeholders in Saudi Arabia, such as providers and decision-makers.
- Feasibility: We did not identify direct evidence to address feasibility for this question. The CKD Task Force judged that there was no reason to suspect differences in feasibility regarding the availability of antihypertensive treatments in Saudi Arabia.
- Implementation: The 2021 KDIGO guideline [8] reported that implementing ABPM for monitoring the treatment of hypertension is challenging [27]. For instance, blood pressure monitors are not always available when needed; they require time from a parent or other adult to return the monitor to the clinic; they are expensive; and in certain situations, there is a low probability of finding elevated blood pressure using ABPM, such as children with clinic blood pressure at <25th percentile.
For additional details, refer to the relevant EtD framework and SoF table in the full CPG document (Supplementary material, Document S1).
Research needs for recommendation 1
The 2021 KDIGO guideline listed as research recommendation to ascertain when antihypertensive medications should be initiated, and identify the best blood pressure measurement technique and setting to define hypertension and blood pressure targets for pediatric CKD patients [8]. The CKD Task Force did not add any further research needs and pointed out the difficulties of performing large RCTs in the pediatric population.
Decision criteria and additional considerations
The RASi used commonly in Saudi Arabia include ACEi and ARBs, whereas non-RASi drug classes include beta blockers, calcium channel blockers (CCBs) and aldosterone antagonists.
Evidence summary
The literature search for the KDIGO 2021 Clinical Practice Guideline for the Management of Blood Pressure (BP) in CKD [8] identified 3 RCTs with a total of 330 participants comparing beta blockers vs RASi [28,29,30] and 5 RCTs with a total of 2,992 participants comparing CCBs vs RASi [31,32,33,34]. Our update search conducted in October 2021 found 1 additional RCT with 269 participants comparing non-RASi vs ramipril (35).
Benefits and harms
Betablockers compared with RASi results in no difference in cardiovascular mortality (RR, 0.67; 95% CI, 0.11-3.90; low certainty in the evidence of effects), corresponding to 57 fewer events (102 fewer to 17 more); cardiovascular morbidity (RR, 0.59; 95% CI, 0.28-1.22; low certainty in the evidence of effects), corresponding to 70 fewer events (122 fewer to 37 more), kidney failure (RR, 1.84; 95% CI, 0.94-3.62; low certainty in the evidence of effects), corresponding to 162 fewer events (12 fewer to 504 more), systolic blood pressure (MD, 2.12; 95% CI, -6.70 – 10.94; low certainty in the evidence of effects); and proteinuria (n/M) (RR, 1.27; 95% CI, 0.31-5.19; low certainty in the evidence of effects), corresponding to 64 more events (165 fewer to 1000 more). The evidence also suggests that betablockers compared to RASi results in a slight increase in diastolic blood pressure (MD, 1.93; 95% CI, 1.32 – 2.53; low certainty in the evidence of effects; and may result in a reduction in hyperkalemia and hyperkalemia (OR, 0.26; 95% CI, 0.08-0.89.; low certainty in the evidence of effects), corresponding to 57 fewer more events (72 fewer to 8 fewer).
Calcium Channel Blockers compared with RASi may result in no difference in cardiovascular mortality, (RR, 1.05; 95% CI, 0.81-1.38; low certainty in the evidence of effects), corresponding to 4 more events (14 fewer to 27 more); cardiovascular morbidity, (RR, 0.93; 95% CI, 0.61-1.42; low certainty in the evidence of effects), corresponding to 2 more events (12 fewer to 13 more); systolic blood pressure, (MD, 0.32; 95% CI, -5.34 - 5.97; low certainty in the evidence of effects); diastolic blood pressure, (MD, -1.33; 95% CI, -4.51 - 1.85; low certainty in the evidence of effects); eGFR change from baseline (MD, 0.02; 95% CI, -0.33 – 0.37; low certainty in the evidence of effects); proteinuria assessed as g/g creatinine (MD, 0.08; 95% CI, -1.42 - 1.58; low certainty in the evidence of effects); and proteinuria assess as g/24 (OR, 4.33; 95% CI, 0.71-26.53; low certainty in the evidence of effects), corresponding to 266 more events (35 fewer to 670 more).
Non RASi compared with RASi (ramipril) may result in no difference in cardiovascular mortality (RR, 1.97; 95% CI, 0.98-3.96; low certainty in the evidence of effects), corresponding to 76 more events (2 fewer to 233 more); cardiovascular morbidity, (RR, 0.54; 95% CI, 0.10-2.91; low certainty in the evidence of effects), corresponding to 13 fewer events (26 fewer to 55 more); and hyperkalemia (OR, 1.10; 95% CI, 0.54-2.2; low certainty in the evidence of effects), corresponding to 11 more events (55 fewer to 118 more) [28,29,31,32,33,34,35]. No other critical outcomes were reported in the body of evidence [8]. The CKD Task Force concluded that based on the available evidence, the balance between desirable and undesirable effects probably favors RASi.
Certainty in the evidence
We rated the overall certainty in the evidence of effects as low based on the lowest certainty in the evidence for the critical outcomes, owing to serious risk of bias, and very serious imprecision of the estimates.
Values
We did not identify primary studies addressing the relative importance of the outcomes for this question. In the opinion of the 2021 KDIGO Work Group [8], most well-informed patients with CKD and severely increased albuminuria would place emphasis on preventing cardiovascular outcomes in addition to preventing CKD progression despite the inconvenience and potential risk of side effects from blood pressure management. The CKD Task Force judged that this also applied to adults in Saudi Arabia and that there was probably no important variability in patients’ values and preferences.
Resource use and cost-effectiveness
We did not identify direct evidence on resource requirements for blood pressure treatment but received information from the Center of Health Technology Assessment – Ministry of Health about cost per package of antihypertensive agents (see Cost table in Supplementary material, Document S1). The 2021 KDIGO Work Group [8] noted that in particular when treating patients with CKD (G1–G4, A2) where the indication for antihypertensive therapy was not strong, consideration should be given to the clinical impact on the patient and the costs of starting RASi, including the need for additional clinic visits and lab testing. The CKD Task Force discussed the issue of immediate costs (cost of antihypertensive agents), considering possible long-term savings such as prevention of future KT or dialysis, as well as possible improvement in future quality of life. They noted that blood pressure treatment led to moderate savings as the costs of antihypertensive agents were low compared with those of future complications of CKD they might prevent and concluded that cost-effectiveness probably favored the comparison. This, added to the fact that average cost of RASi is lower than non-RASi, would favor the recommendation.
Other contextual factors
- Equity: We did not identify direct evidence to address equity for this question. The CKD Task Force concluded that in view of Saudi Arabia’s comprehensive health coverage, there would probably be no disadvantages associated with the use of antihypertensive treatment in adults with CKD on equity from implementing the recommendation.
- Acceptability We did not identify direct evidence to address acceptability for this question. The CKD Task Force used their collective experience with antihypertensive therapy in Saudi Arabia to judge that this pharmacological therapy was acceptable to stakeholders in Saudi Arabia, such as providers and decision-makers.
- Feasibility: We did not identify direct evidence to address feasibility for this question.
- Implementation: We did not identify direct evidence to address implementation for this question.
For additional details, please refer to the relevant EtD framework and SoF table in the full CPG document (Supplementary material, Document S1).
Research needs for recommendation 2
The 2021 KDIGO Guideline identified as research needs the undertaking of adequately powered RCT to evaluate cardiovascular and kidney effects of ARB versus dihydropyridine CCB among patients with KT [8]. Also, since RASi in patients with CKD G3–G4, A1 and A2 with or without diabetes have not been adequately studied, future studies should examine if RASi, in the presence or absence of other reno-protective agents such as SGLT2 inhibitors and glucagon-like peptide-1 (GLP-1) receptor agonists, provide kidney, cardiovascular, and survival benefits to this important subgroup [8]. Finally, there is insufficient evidence on the role of diuretics as first line therapy for the treatment of high blood pressure in patients with CKD. Therefore, it would be helpful to clarify the role of diuretics as initial therapy in this population [8].
The NICE Guideline, identified as research need understanding the clinical effectiveness of RASi in patients with CKD older than 75 years [12].
Decision criteria and additional considerations
Based on the available evidence and in line with the KDIGO 2021 Clinical Practice Guideline for the Management of Blood Pressure (BP) in CKD [8], the CKD Task Force suggests targeting 24-hour MAP <50th percentile for intensive blood pressure control. Please see section 7.2 for additional details on measuring blood pressure in children.
Evidence summary
The literature search for the 2021 KDIGO guideline [8] identified one RCT compared intensive blood pressure control (targeting 24-hour MAP <50th percentile of normal children) versus standard blood pressure control (targeting 24-hour MAP 50th-99th percentile of normal children) [36]. Our update search conducted in October 2021 found no additional studies for inclusion.
Benefits and harms
The included RCT (the “Effect of Strict Blood Pressure Control and ACE Inhibition on the Progression of CKD in Pediatric Patients” (ESCAPE) trial of 385 children aged 3 to 18 years) showed that intensive blood pressure control significantly slowed CKD progression (time to a decline of 59% in GFR, progression to ESKD), with no statistically significant difference in the type or incidence of adverse events or rates of withdrawal [36]. Children with glomerular disorders, GFR <45 ml/min per 1.73 m2, and PCR >1.5 g/g (150 mg/mmol) seemed to benefit the most.
The evidence suggests that intensive blood pressure does not reduce mortality (RR, 0.34; 95% CI, 0.01-8.39; low certainty in the evidence of effects); this corresponds to 3 fewer (5 fewer to 38 more) death per 1000 patients based on a baseline risk of 0.5%, and 220 fewer (331 fewer to 1000 more) per 1000 patients based on a baseline risk of 33.4% from observational data (ref). There is no difference in decreasing kidney failure (RR, 0.67; 95% CI, 0.41-1.10; low certainty in the evidence of effects), corresponding to 57 fewer events (102 fewer to 17 more); systolic blood pressure (MD, -2.00; 95% CI, -4.97- 0.97; low certainty in the evidence of effects); and diastolic blood pressure (MD, -1.0; SD, -3.7 - 1.7; low certainty in the evidence of effects). Intensive blood pressure may reduce glomerular filtration rate slightly (MD, -1.4; 95% CI, -2.79 - 0.00; low certainty in the evidence of effects). Mean Targeting the intensified blood pressure control required a larger number of antihypertensive agents than the conventional target, and systolic blood pressure (SBP) was found to be higher in the group of participants with higher blood pressure targets. The study was not powered for and did not demonstrate statistically significant effects for all-cause mortality or kidney failure. Neither did it report data on other critical outcomes such as cardiovascular mortality, cardiovascular morbidity, doubling serum creatinine, acute kidney injury, proteinuria, or left ventricular hypertrophy. The CKD Task Force concluded that the balance between desirable and undesirable effects probably favored intensive blood pressure control.
Certainty in the evidence
We rated the overall certainty in the evidence of effects as low based on the lowest certainty in the evidence for the critical outcomes, owing to serious risk of bias, and serious imprecision of the estimates.
Values
We did not identify primary studies evaluating the values and preferences of patients (or their families / caregivers) for this question. The SONG-Kids study cited in the 2021 KDIGO guideline [8] reported that both children with kidney disease and their caregivers rated kidney function as an important outcome, and blood pressure control was also rated as an important outcome by caregivers [25]. In the judgment of the Work Group, most patients would value the clinical benefits associated with intensive blood pressure control despite the inconvenience and potential risk of harms associated with it (such as multiple medications, more frequent dosing, possible adverse events if dehydrated, and the burden of monitoring with 24-hour ABPM. Patients for whom medication burden or the burden of ABPM monitoring are particularly important concerns may be more inclined not to follow this recommendation. The CKD Task Force concluded that in the absence of direct evidence there was possibly important uncertainty about how much people value the main outcomes, so input about their preferences would need to be sought from individual patients or caregivers before initiation of intensive blood pressure control.
Resource use and cost-effectiveness
We did not identify direct evidence on resource requirements for blood pressure treatment but received information from the Saudi Health Technology Agency about cost per package of antihypertensive agents (see Cost table in Appendix 14.9). Indirect evidence from a cost-effectiveness study determining the lifetime health benefits and health care cost of intensive versus standard blood pressure management in adults suggests that intensive blood pressure is cost-effective [26].The 2021 KDIGO Work Group [8] judged that the potential benefits associated with ABPM outweighed the costs and inconvenience associated with its implementation. Patients and families in areas where ABPM is less affordable will be less inclined to follow this recommendation and may choose to use clinic-based auscultatory blood pressure monitoring instead.
Other contextual factors
- Equity: We did not identify direct evidence to address equity for this question. The CKD Task Force concluded that given Saudi Arabia’s comprehensive health coverage, there would probably be no disadvantages associated with the use of antihypertensive treatment in children with CKD on equity from implementing the recommendation.
- Acceptability: We did not identify direct evidence to address acceptability for this question. The ESCAPE trial suggests that lower blood pressure targets are usually acceptable to patients and health care providers [36]. The CKD Task Force used their collective experience with antihypertensive therapy in Saudi Arabia to judge that this pharmacological therapy was acceptable to stakeholders in Saudi Arabia, such as providers and decision-makers.
- Feasibility: We did not identify direct evidence to address feasibility for this question.
- Implementation: The 2021 KDIGO guideline [8] reported that implementing ABPM for monitoring the treatment of hypertension is challenging [27]. For instance, blood pressure monitors are not always available when needed; they require time from a parent or other adult to return the monitor to the clinic; they are expensive; and there are certain situations where there is a low probability of finding elevated blood pressure by ABPM such as children with clinic blood pressure at <25th percentile.
For additional details, please see the EtD framework and SoF table in (Supplementary material, Document S1).
Research needs for recommendation 3
The research need identified in the source guideline, and accepted by the CKD Task Force, was the undertaking of RCTs that define targets for treatment when ABPM cannot be obtained repeatedly, for example, with home-based or office-based auscultatory or oscillometric blood pressure, with kidney disease progression and cardiovascular disease as outcomes [8]. The CKD Task Force also noted that there was insufficient evidence about the effects of intensive lowering blood target compared to higher blood pressure target in children with CKD.
The CKD Task Force considers there is a need for developing and conducting new RCTs to justify blood pressure targets, and that also includes assessment of outcomes that do not yet provide evidence and to make the data available to other countries. They also describe the need to set up a National Research Center that collects all the research done in Saudi Arabia and to encourage independent research centers of each university to exchange information and prevent wastage of research and duplication of efforts.
Additional considerations
Evidence summary
The 2021 KDIGO guideline [8] identified nine RCTs (37; 39; 39; Ku et al., 2017; Pahor et al., 1998; 35; Sarnak et al., 2005) and conducted a meta-analysis comparing the effects of introducing intensive (SBP <120 mm Hg) versus standard (SBP <140 mm Hg) blood pressure target on blood pressure control in adults with CKD. Our update search conducted in October 2021 found no additional studies for inclusion.
Benefits and harms
Intensive blood pressure targets likely reduces mortality (RR, 0.85; 95% CI, 0.76-0.96; moderate certainty in the evidence of effects), corresponding to 17 fewer events per 1000 patients (27 fewer to 4 fewer), kidney failure (RR, 0.90; 95% CI, 0.82-0.99; moderate certainty in the evidence of effects), corresponding to 18 fewer events (32 fewer to 2 fewer), SBP (MD, -8.12; SD, -13.13 - -3.1; moderate certainty in the evidence of effects), DBP (MD, -4.30; SD, -6.46 - -2.15; moderate certainty in the evidence of effects), and hyperkalemia (RR, 1.34; 95% CI, 1.01-1.78; low certainty in the evidence of effects), corresponding to 20 more events (1 more to 4 more (37; 39; Ku et al., 2017; Pahor et al., 1998; 35; Sarnak et al., 2005; The SPRINT Research Group, 2015). There is no difference between intensive blood pressure targets compared to standard blood pressure targets on cardiovascular mortality (RR, 0.96; 95% CI, 0.44-2.08; low certainty in the evidence of effects), corresponding to 1 fewer event (15 fewer to 29 more) cardiovascular morbidity (RR, 0.89; 95% CI, 0.73-1.09; low certainty in the evidence of effects), corresponding to 26 fewer events (63 fewer to 21 more), and eGFR change from baseline (MD, 1.60; 95% CI, -0.72 - 3.92; low certainty in the evidence of effects) [36,37,38,39,40]. None of the included studies had reported information on doubling serum creatinine, acute kidney injury left ventricular hypertrophy and encephalopathy.
Certainty in the evidence
We rated the overall certainty in the evidence of effects as low based on the lowest certainty in the evidence for the critical outcomes, owing to very serious risk of bias, and serious imprecision of the estimates.
Values
We did not find primary evidence addressing the relative importance of the outcomes for this question. In the opinion of the 2021 KDIGO Work Group, most well-informed patients with CKD and severely increased albuminuria would place emphasis on preventing cardiovascular outcomes in addition to preventing CKD progression despite the inconvenience and potential risk of side effects from blood pressure management. The CKD Task Force concurred that this also applied to adults in Saudi Arabia and that there was probably no important variability in patients’ values and preferences.
Resource use and cost-effectiveness
We did not identify direct evidence on resource requirements for blood pressure treatment but received information from the Saudi Health Technology Agency about cost per package of antihypertensive agents (see Cost table in Appendix 14.9). The 2021 KDIGO Work Group [8] noted that in particular when treating patients with CKD (G1–G4, A2) where the indication for antihypertensive therapy was not strong, consideration should be given to the clinical impact on the patient and the costs of starting RASi, including the need for additional clinic visits and lab testing. The CKD Task Force discussed the issue of immediate costs (cost of antihypertensive agents), considering possible long-term savings such as prevention of future KT or dialysis, as well as possible improvement in future quality of life. They noted that overall, blood pressure treatment led to moderate savings as the costs of antihypertensive agents were low compared with those of future complications of CKD they might prevent and concluded that cost-effectiveness probably favored the intervention.
Other contextual factors
- Equity: We did not identify direct evidence to address equity for this question. The CKD Task Force concluded that given Saudi Arabia’s comprehensive health coverage, there would probably be no disadvantages associated with the use of antihypertensive treatment in children with CKD on equity from implementing the recommendation.
- Acceptability We did not identify direct evidence to address acceptability for this question. The CKD Task Force used their collective experience with antihypertensive therapy in Saudi Arabia to judge that this pharmacological therapy was acceptable to stakeholders in Saudi Arabia, such as providers and decision-makers.
- Feasibility: We did not identify direct evidence to address feasibility for this question.
- Implementation: We did not identify direct evidence to address implementation for this question.
For additional details, please see the EtD framework and SoF table in (Supplementary material, Document S1).
Research needs for recommendation 4
The 2021 KDIGO guideline listed as research recommendation adequately powered RCTs to evaluate cardiovascular and kidney effects of targeting SBP <120 mm Hg versus <130 mm Hg SBP among patients with KTs [8]. Also, the undertaking of RCTs comparing treatment based on ABPM or HBPM versus standardized office blood pressure measurements. Treatment based on ABPM or HBPM includes not treating patients with “white-coat” hypertension, not intensifying treatment for the “white-coat” effect, treatment of masked hypertension, and intensifying treatment for masked uncontrolled hypertension.
Finally, information is needed on how patient values and preferences influence decisions related to blood pressure-lowering therapy. This would be an ideal topic for the Standardized Outcomes in Nephrology (SONG) initiative [8].
Additional considerations
The NICE guideline [20] recommended to start assessment for KRT or conservative management at least one year before therapy was likely to be required, including for patients with a failing KT.
Evidence summary
The NICE guideline [20] included one retrospective cohort study involving 3,014 participants comparing early and late nephrologist referral [41]. Our update search conducted in October 2021 found no additional studies for inclusion addressing this clinical question.
Benefits and harms
Early referral compared to late referral may reduce mortality at 90 days (RR, 0.67; 95% CI, 0.60-0.76; very low certainty in the evidence of effects], corresponding to 115 fewer events per 1000 patients (140 fewer to 84 fewer), but there is no difference on mortality from 91 days to 1 year (RR, 0.07; 95% CI, 0.84-1.13; very low certainty in the evidence of effects), corresponding to 8 fewer events (45 fewer to 37 more). However, the evidence is very uncertain [41]. The study did not report any other critical outcomes such as patient/family/caregiver health related quality of life, impact late referral rates, pre-emptive transplantation rates, proportion of patients receiving KRT after assessment, symptom scores, cognitive impairment, growth, malignancy, or adverse events. The NICE committee noted that when considering the timing of referral for assessment, allowing sufficient time to prepare for KRT needs to be balanced with minimizing referral of those that will never receive it.
Certainty in the evidence
We rated the overall certainty in the evidence of effects as very low based on the lowest certainty in the evidence for the critical outcomes, owing to very serious risk of bias, and serious imprecision of the estimates. The NICE committee [20] and CKD Task Force also noted that referral to a nephrologist is only a proxy for the full multidisciplinary assessment required. Whereas a nephrology referral may happen for a variety of reasons other than assessment for KRT (such as investigating the etiology of the condition and actions to treat and monitor the condition, and preserve renal function), the assessment for KRT often requires transfer of patient care from an individual nephrology consultant-led review to a multidisciplinary review. This usually follows recognition that the person with kidney disease has reached a stage that requires planning of how to manage the progressive nature of their condition, and the multidisciplinary team is needed to cover all aspects of the person’s care and future care plans.
Values
We did not find primary evidence addressing the relative importance of the outcomes for this question. Patient representatives and advocates presenting at the KDIGO Controversies Conference on Early Identification & Intervention in CKD in October 2019 expressed a strong belief that patients prefer earlier CKD screening and diagnosis [42]. They also emphasized that the decisions concerning age to initiate testing, the frequency of repeat testing and time to forgo or end testing should be personalized based on risk factors, preferences, and life expectancy. A systematic review found that hemodialysis had the lowest utility value (ranging from 0.44 to 0.72), with higher utility value for PD (ranging from 0.53 to 0.81), and the highest utility value calculated for KT (ranging from 0.57 to 0.90) [20,43].
Resource use and cost-effectiveness
We did not identify primary studies addressing the resources required to manage CKD patients with KRT.
- Cost of condition: CKD affects about 10 percent of the population worldwide, with over 2 million people worldwide reported to have ESKD [44]. In higher-income countries, treatment costs are enormous: a 2010 report from the United Kingdom (UK) National Health Service estimates its annual CKD spending at £1.45 billion, more than half of which was for KRT [45]. Australia has estimated it will spend over $12 billion on ESKD patients through 2020 [46]. At the same time, KRT remains entirely unaffordable to the majority of ESKD patients in low- and middle-income countries throughout the world, with over 1 million people dying annually from lack of treatment [47].
- Cost of interventions: According to a report estimating unit and annual cost for KTs in the UK, the initial assessment clinic costs include annual cost per patient £2,537 (Saudi Riyals [SAR] 13,137), and annual expenditure of £6,421,018 (SAR 33,238,174). A study conducted at a Saudi dialysis center assessed the health services cost of hemodialysis based on data gathered over 3.5 years [48]. The mean total cost per hemodialysis session came to US $297 (1,114 SAR), and the mean total cost of dialysis per patient per year was US $46,332 (173,784 SAR). Another study conducted in Saudi Arabia compared medical cost of transplantation following desensitization versus maintenance hemodialysis over a 4-year period [49]. The average annual cost of medical care per transplant patient was US $133,291, US $14,233, US $5,536, and US $4,402 in the first, second, third, and fourth year respectively. The average 4-year actual total cost per patient was significantly lower in the KT group compared to the hemodialysis group (US $210,779 vs US $317,186.3; p=0.017). A systematic review evaluating dialysis cost in low and middle-income countries found the annual cost per patient for hemodialysis to be lower compared to PD (ranging from international dollars (Int$) 3,424 to Int$ 42,785 with hemodialysis vs Int$ 7,974 to Int$ 47,971 with PD) [50]. The main cost drivers for hemodialysis were direct medical cost (especially drugs and consumables) and dialysis solutions and tubing for PD. A systematic review of cost-effectiveness of KRT modalities also reported that KT was the most cost-effective KRT modality, but that PD was more cost-effective than hemodialysis [43]. Most studies suggested that KT held a dominant position over hemodialysis and PD in terms of both lower costs and higher effectiveness. Five studies suggested that increased uptake of KT and PD by new ESKD patients would reduce costs and improve health outcomes or would be more cost-effective than current practice patterns.
Other contextual factors
- Equity: We did not identify direct evidence to address equity or feasibility for this question.
- Acceptability: We did not identify direct evidence to address acceptability for this question but found indirect evidence from a study evaluating the implementation of a multidisciplinary care (MDC) clinic for patients with advanced CKD [51]. The study suggested possible improvement in adherence to CKD intervention targets and good participants’ acceptability of the MDC program consisting of clinical outcomes assessment, self-care advice, and KRT options.
- Feasibility: We did not identify direct evidence to address feasibility for this question.
- Implementation: The CKD Task Force suggested using doubling serum creatinine as an indicator for early assessment of CKD, especially in the remote areas of Saudi Arabia, where hospital infrastructure and proper laboratory facilities may be limited, and the use of GFR may not be possible.
For additional details, please see the EtD framework and SoF table in (Supplementary material, Document S1).
Research needs for recommendation 5
No research recommendations were reported in the NICE guideline [20] for this question, and the CKD Task Force did not add any research needs.
Additional considerations
The NICE guideline recommended [20] to aim to create access via a catheter placed by an open surgical technique around two weeks prior to anticipated start of PD. When planning hemodiafiltration or hemodialysis via an AVF, it recommended to use ultrasound scanning to determine vascular access sites for creating the AVF, and to create the arteriovenous graft (AVG) around 6 months before the anticipated start of dialysis to allow for maturation and to allow for the possibility of the first fistula failing or needed further interventions before use.
Evidence summary
The literature search conducted for the NICE guideline [20] on early versus late preparation strategy included one RCT [52] and two non-randomized studies assessing maturation requirements of AVF for hemodialysis [53,54]. The RCT compared initiation of PD 1 week vs 2 weeks vs 4 weeks after PD insertion in 122 adults over 18 years of age. One of the observational studies included 14,459 adults >70 years of age and focused on AVF placement one or one-two months before initiation of KRT [53]. The other study evaluated the time from AVF creation to use <30 days versus >30 days among 414 adults over the age of 18 years [54]. Our update search conducted in October 2021 found no further studies for inclusion addressing the clinical question.
Benefits and harms
Any late preparation strategy (based on eGFR or by anticipated time to start of KRT) may result in a slight increase in mortality (HR, 1.26; 95% CI, 1.03-1.54; very low certainty in the evidence of effects); AVF failure in hemodialysis access (HR, 1.94; 95% CI, 1.344-2.82; very low certainty in the evidence of effects); leak in PD access between 1 to 4 weeks (RR, 11.56; 95% CI, 1.57-85.42; low certainty in the evidence of effects), corresponding to 258 more events (14 more to 1000 more); and leak in PD access between 1 to 2 weeks (RR, 2.96; 95% CI, 1.03-8.53; low certainty in the evidence of effects), corresponding to 187 more events (3 more to 717 more).
The evidence suggests that any late preparation strategy (based on eGFR or by anticipated time to start of KRT) results in no difference in modality failure in PD access between 1 to 4 weeks (RR, 0.15; 95% CI, 0.02-1.17; low certainty in the evidence of effects), corresponding to 145 fewer events (167 fewer to 29 more); infections in PD access between 1 to 4 weeks (RR, 5.26; 95% CI, 0.64-43.00; low certainty in the evidence of effects), corresponding to 104 more events (9 fewer to 1000 more); modality failure in PD access between 1 to 2 weeks (RR, 1.08; 95% CI, 0.07-16.63; low certainty in the evidence of effects), corresponding to 2 more events (22 fewer to 372 more); infections in PD access between 1 to 2 weeks (RR, 5.38; 95% CI, 0.66-44.07; low certainty in the evidence of effects), corresponding to 104 more events (8 fewer to 1000 more); modality failure in PD access between 2 to 4 weeks (RR, 0.14; 95% CI, 0.02-1.08; low certainty in the evidence of effects), corresponding to 147 fewer events (167 fewer to 14 more); infections in PD access between 2 to 4 weeks (RR, 0.98; 95% CI, 0.66-15.09; low certainty in the evidence of effects), corresponding to 0 fewer events (23 fewer to 344 more), and leak in PD access between 2 to 4 weeks (RR, 3.90; 95% CI, 0.46-33.48; low certainty in the evidence of effects), corresponding to 71 more events (13 fewer to 792 more).
Certainty in the evidence
We rated the overall certainty in the evidence of effects as very low based on the lowest certainty in the evidence for the critical outcomes, owing to very serious risk of bias, and serious imprecision of the estimates.
Values
We did not identify primary studies addressing the relative importance of the outcomes for this question. Indirect evidence from a systematic review found that patients highly value the benefits of hemodialysis, PD, and KT [43]. Hemodialysis had the lowest utility value (ranging from 0.44 to 0.72), with higher utility value for PD (ranging from 0.53 to 0.81), and the highest utility value calculated for KT (ranging from 0.57 to 0.90). In seven of the nine studies included in the review, KT utility was higher than PD utility, and PD utility was higher than hemodialysis utility. In two of the nine studies, KT utility was higher than PD and hemodialysis utility, with PD and hemodialysis utility being equal. One study suggested that conflicting results of utility valuations existed among different valuation methods. For example, continuous ambulatory PD patients’ European Quality of Life five-dimension scale (EQ-5D) scores were higher than those of center hemodialysis patients, while continuous ambulatory PD patients’ Standard Gamble and Time Trade-Off scores were lower than those of center hemodialysis patients.
Resource use and cost-effectiveness
We did not identify primary studies addressing the resources required to manage CKD patients with KRT.
- Cost of interventions: According to a report estimating unit and annual cost for KT in the UK, the initial assessment clinic costs include annual cost per patient £2,537 (SAR 13,137), and annual expenditure of £6,421,018 (SAR 33,238,174). A study conducted at a Saudi dialysis center assessed the health services cost of hemodialysis based on data gathered over 3.5 years [48]. It found that the mean total cost per hemodialysis session came to US $297 (1,114 SAR), and the mean total cost of dialysis per patient per year was US $46,332 (173,784 SAR). Another study conducted in Saudi Arabia compared medical cost of transplantation following desensitization versus maintenance hemodialysis over a 4-year period [48]. The average annual cost of medical care per transplant patient was US $133,291, US $14,233, US $5,536, and US $4,402 in the first, second, third, and fourth year respectively. The average 4-year actual total cost per patient was significantly lower in the KT group compared to the hemodialysis group (US $210,779 vs US $317,186.3; p=0.017). A systematic review evaluating dialysis cost in low and middle-income countries found the annual cost per patient for hemodialysis to be lower compared to PD (ranging from international dollars (Int$) 3,424 to Int$ 42,785 with hemodialysis vs Int$ 7,974 to Int$ 47,971 with PD) [50]. It reported that the main cost drivers for hemodialysis were direct medical cost (especially drugs and consumables) and dialysis solutions and tubing for PD. A systematic review of cost-effectiveness of KRT modalities also reported that KT was the most cost-effective KRT modality but that PD was more cost-effective than hemodialysis [43]. Most studies suggested that KT held a dominant position over hemodialysis and PD in terms of both lower costs and higher effectiveness. Five studies suggested that increased uptake of KT and PD by new ESKD patients would reduce costs and improve health outcomes or would be more cost-effective than current practice patterns.
Other contextual factors
- Acceptability: We did not identify direct evidence to address acceptability for this question [51].
- Feasibility: We did not identify direct evidence to address feasibility for this question.
- Implementation: We did not identify direct evidence to address implementation for this question.
For additional details, please see the EtD framework and SoF table in (Supplementary material, Document S1).
Research needs for recommendation 6
With regard to research needs, the CKD Task Force identified:
- The timing of creating percutaneous and laparoscopic PD access for different KRT options.
- The clinical and cost-effectiveness of initial hemodialysis versus initial peritoneal dialysis for people who start dialysis in an unplanned approach.
- The best timing for transplant listing for those on KRT considering transplantation.
The CKD Task Force also accepted the following research needs listed in the NICE guideline [20]: What is the most clinical and cost-effective strategy for timing of preemptive transplantation, and what is the optimum timing of listing for transplantation?
Additional considerations
This recommendation is in line with NICE guidance to ask patients throughout the course of KRT and conservative management about any symptoms they have, explore whether their symptoms are due to CKD, their treatment or another cause, and to explain the likely cause of the symptoms to the patient (and/or family/caregivers) including how well treatment may be expected to control them. Patients may feel uncomfortable talking about some symptoms (for example sexual dysfunction) and may not associate them with CKD or its treatment.
Evidence summary
The literature search conducted for the NICE guideline on symptom recognition did not find any studies on the effectiveness of symptom identification but reported thirty-four qualitative studies on symptoms reported by patients and caregivers [20]. Twenty-eight of these explored the views of adult patients on KRT. One study provided the views of adolescent patients; four studies focused on the views of patients and caregivers on KT, and one study dealt with views of parents whose children were on KRT or considering KRT. Twenty-nine studies conducted in-depth semi-structured interviews with transcripts analyzed using a phenomenological reduction or thematic analysis. Four studies used focus group sessions, while one study conducted an open-ended survey distributed online. Our update search conducted in October 2021 found two additional observational studies using a survey and questionnaires to capture the views of patients undergoing hemodialysis to explore symptom experiences and symptom clusters respectively [58,59].
Benefits and harms
The qualitative review reported in the NICE guideline identified no critical themes but symptoms or the impact of symptoms. The major symptoms identified were fatigue, breathlessness, pain, depression, immobility, itching, nausea, anxiety, cognitive fluctuations, dizziness, insomnia, weakness, weight gain and infection. The two studies identified on update of evidence also delineated gastrointestinal, musculoskeletal, neurological, irritation of skin, depression, sleep disturbances and anemia as important symptoms.
Certainty in the evidence
We rated the overall certainty in the evidence of effects as very low based on the lowest certainty in the evidence for the critical outcomes, owing to methodological limitations and concerns regarding adequacy for the assessment of outcomes.
Values
We did not identify direct evidence to address the relative importance of the outcomes for this question.
Resource use and cost-effectiveness
We did not identify direct evidence to address resources use and cost-effectiveness for this question.
Other contextual factors
- Equity: We did not identify direct evidence to address equity for this question.
- Acceptability: We did not identify direct evidence to address acceptability for this question. However, we found indirect evidence on acceptability from a study evaluating the implementation of a MDC clinic for patients with advanced CKD [49]. The study suggested possible improvement in adherence to CKD intervention targets and good participants’ acceptability of the MDC program consisting of clinical outcomes assessment, self-care advice, and KRT options.
- Feasibility: We did not identify direct evidence to address feasibility for this question.
- Implementation: We did not identify direct evidence to address implementation for this question.
For additional details, please see the EtD framework and SoF table in (Supplementary material, Document S1).
Research needs for recommendation 7
No research recommendations were reported in the NICE guideline [20] for this question, and the CKD Task Force did not add any research needs.
Additional considerations
The NICE guideline [20] noted that the decision when to start KRT should consider the patient’s presence and severity of uremic symptoms (refractory pruritus, and nausea and vomiting, in particular in the morning) and fluid overload (edema, weight gain, and breathlessness), preference, biochemistry, and eGFR, and made on an individual basis. Some patients may prefer an agreed starting point based on eGFR but may need dialysis before this because symptoms are affecting normal daily activities. On the other hand, some patients with slowly progressing CKD may not recognize and report symptoms that indicate that dialysis is needed. It is important to establish whether more general symptoms such as fatigue and depression are due to uremia or not, and to discuss their impact on daily life.
Evidence summary
The literature search conducted for the NICE guideline [20] identified three studies—one RCT and two non-randomized study—addressing this question [60,61,62]. The RCT known as the IDEAL trial was conducted across 32 centers in New Zealand and Australia among 828 adults with CKD (including patients with a failing transplant) and compared planned initiation of dialysis with eGFR 10-14 mL/min/1.73m2 (early start) versus with eGFR 5-7 mL/min/1.73m2 (late start) [61]. The first non-randomized study was a cohort study with 671 adults aged 18 and older who had their first pre-emptive transplant between 1984 and 2006 [60]. The second study evaluated the records of 4,046 adults who had undergone a living donor KT as initial form of KRT [62]. Our update search conducted in October 2021 found two additional retrospective cohort studies among children (<18 years of age), with one study [64] including 2,963 children from 21 European countries and the other [63] evaluating 15,170 children who started KRT between 1995 and 2015.
Benefits and harms
For hemodialysis or PD, early preparation compared with late preparation may result in no difference in mortality based on eGFR (RR, 1.04; 95% CI, 0.87-1.24; low certainty in the evidence of effects), corresponding to 15 more events (48 fewer to 88 more); mortality in age <18 years (HR, 1.25; 95% CI, 0.96-1.64; very low certainty in the evidence of effects); growth <18 years (MD, -0.03; 95% CI, -0.15 - 0.09; very low certainty in the evidence of effects); patient, family/caregiver health related quality of life (MD, 0.00; 95% CI, -0.03 - 0.03; very low certainty in the evidence of effects); pre-emptive transplantation rates at age <18 years, (HR, 0.97; 95% CI, 0.89-1.06; very low certainty in the evidence of effects); and adverse events (RR, 0.89; 95% CI, 0.75-1.06; low certainty in the evidence of effects), corresponding to 45 more events (103 fewer to 25 more).
For patients undergoing kidney transplant with an eGFR ≥15ml/min vs <10ml/min, early preparation compared with late preparation may result in no difference in mortality (HR, 1.35; 95% CI, 0.89-2.05; very low certainty in the evidence of effects).
For transplant at eGFR 10 -14.9 ml/min vs <10ml/min, early preparation compared with late preparation may result in no difference in mortality (HR, 0.99; 95% CI, 0.69-1.42; very low certainty in the evidence of effects) [60,61,63,64]
Certainty in the evidence
We rated the overall certainty in the evidence of effects as very low based on the lowest certainty in the evidence for the critical outcomes, owing to very serious risk of bias, and serious imprecision of the estimates.
Values
We did not identify primary studies addressing the relative importance of the outcomes for this question. Indirect evidence from a systematic review found that patients highly value the benefits of hemodialysis, PD, and KT [43]. Hemodialysis had the lowest utility value (ranging from 0.44 to 0.72), with higher utility value for PD (ranging from 0.53 to 0.81), and the highest utility value calculated for KT (ranging from 0.57 to 0.90). In seven of the nine studies included in the review, KT utility was higher than PD utility, and PD utility was higher than hemodialysis utility. In two of the nine studies, KT utility was higher than PD and hemodialysis utility, with PD and hemodialysis utility being equal. One study suggested that conflicting results of utility valuations existed among different valuation methods. For example, continuous ambulatory PD patients’ EQ-5D scores were higher than those of center hemodialysis patients, while continuous ambulatory PD patients’ standard gamble (SG) and time tradeoff (TTO) scores were lower than those of center hemodialysis patients.
Resource use and cost-effectiveness
A systematic review of cost-effectiveness of KRT modalities reported that KT was the most cost-effective KRT modality but that PD was more cost-effective than hemodialysis [43]. Most studies suggested that KT held a dominant position over hemodialysis and PD in terms of both lower costs and higher effectiveness. Five studies suggested that increased uptake of KT and PD by new ESKD patients would reduce costs and improve health outcomes or would be more cost-effective than current practice patterns.
Other contextual factors
- Equity: We did not identify direct evidence to address equity for this question.
- Acceptability: We did not identify direct evidence to address acceptability for this question.
- Feasibility: We did not identify direct evidence to address feasibility for this question.
- Implementation: We did not identify direct evidence to address implementation for this question.
For additional details, please see the EtD framework and SoF table in (Supplementary material, Document S1).
Research needs for recommendation 8
The NICE guideline [20] identified a research need for the following question: What is the most clinical and cost-effective strategy for timing of pre-emptive transplantation? A question raised by the CKD Task Force was whether initiation of dialysis can be delayed safely with aggressive medical management [68].
Additional considerations
The NICE guideline [20] recommended to offer a choice of KRT or conservative management (supportive management including symptom and complications control, and advance care planning) to patients who are likely to need KRT, with the decision to be based on individual factors (such as frailty, cognitive impairment and multimorbidity) and patient preference. Especially in the later stages of CKD, patients may decide against KRT. Conservative management is generally (although not always) less appropriate for younger, healthier people, and rarely an option for children.
Evidence summary
The literature search conducted for the NICE guideline [20] identified one non-randomized study addressing this question. This UK study reviewed the records of 844 patients attending a Nephrology clinic based on data from a hospital database from 1990 – 2008, including 106 patients with KRT and 77 patients with conservative management [65]. Our update search conducted in October 2021 found no further studies for inclusion addressing the clinical question.
Benefits and harms
The evidence is very uncertain about the effect of any KRT (hemodialysis and/or peritoneal dialysis and/or transplant) on mortality in over 75 years in a follow up period from 1 to 18 years (HR, 0.85; 95% CI, 0.57-1.27; very low certainty in the evidence of effects). Dialysis may result in a slight increase in mortality in over 75 years in a median follow up period of 2 years (HR, 2.94; 95% CI, 1.56-5.53; very low certainty in the evidence of effects) [65]. There was insufficient evidence on other outcomes such as cognitive impairment, growth, impact late referral rates, patient and caregiver health related quality of life, pre-emptive transplantation rates, proportion receiving KRT after assessment, symptom scores, or adverse events.
Certainty in the evidence
We rated the overall certainty in the evidence of effects as very low based on the lowest certainty in the evidence for the critical outcomes, owing to very serious risk of bias, and serious imprecision of the estimates.
Values
We did not identify primary studies addressing the relative importance of the outcomes for this question.
Indirect evidence suggests patient representatives and advocates described that there is a strong belief that patients overwhelmingly prefer earlier CKD screening and diagnosis and that patient education has the potential to improve self-management and disease prognosis 70 [8].
One systematic review described the following regarding the relative importance of outcomes and patients’ preferences for hemodialysis, PD, and KT. Patients highly value the benefits of hemodialysis, PD, and KT [43]. The utility values for hemodialysis ranged from 0.44 to 0.72; for PD from 0.53 to 0.81; for KT from 0.57 to 0.90. In seven of the nine studies, KT utility was higher than PD utility, and PD utility was higher than hemodialysis utility. In two of the nine studies, KT utility was higher than PD and hemodialysis utility, with PD and hemodialysis utility being equal. One study suggests that conflicting results of utility valuations existed among different valuation methods. For example, continuous ambulatory PD patients’ EQ-5D scores were higher than those of center hemodialysis patients, while continuous ambulatory PD patients’ SG and TTO scores were lower than those of center hemodialysis patients [43].
Resource use and cost-effectiveness
We did not identify primary studies addressing the resources required to manage CKD patients with conservative management or renal replacement therapy.
- Cost of interventions: initial assessment clinic has an annual cost per patient of £2,537 (SAR 13,137), and an annual expenditure of £6,421,018 (SAR 33,238,174). The mean total cost per hemodialysis session was calculated as 297 US dollars (USD) (1,114 SAR), and the mean total cost of dialysis per patient per year was 46,332 USD (173,784 SAR) [48]. One study conducted in Saudi Arabia described that an average annual cost of medical care per patient after transplantation in the first, second, third, and fourth year was USD $133,291, USD $14,233, USD $5,536, and USD $4,402, respectively. The average 4-year actual total cost per patient was USD $210,779 and USD $317,186.3 in the kidney transplant group and the hemodialysis group; respectively (p=0.017) [49].
- In terms of cost-effectiveness, one study assessed the value for money and budget impact of offering hemodialysis as a first-line treatment, or the hemodialysis-first policy, and the PD first policy compared to a supportive care option in patients with ESKD in Indonesia [66]. The PD-first policy was found to be more cost-effective compared to the hemodialysis-first policy. Budget impact analysis provided evidence on the enormous financial burden for the country if the current practice, where hemodialysis dominates PD, continues for the next five years.
-
Costs:
- ○
-
Life years saved
- ▪
- Supportive care option: 0.21
- ▪
- PD first option: 5.93
- ▪
- Hemodialysis first option: 5.93
- ○
-
Quality-adjusted life years (QALY)
- ▪
- Supportive care option: 0.076
- ▪
- PD first option: 4.40
- ▪
- Hemodialysis first option: 4.34
- ○
-
Incremental cost-effectiveness ratio
- ▪
- Supportive care: Not reported
- ▪
- PD first option: 193.2 million IDR
- ▪
- Hemodialysis first option: 2017.4 million IDR
- ○
-
Cost-effectiveness acceptability
- ▪
- At the threshold of willingness to pay 43 million IDR (1 GDP), supportive care was the best option. (probability = 1.00)
- ▪
- At willingness to pay >190million IDR, PD first was the most cost-effective option (probability >0.5)
- ▪
- Hemodialysis first was not the best cost-effective option at any level of willingness to pay.
A CADTH Review [67] demonstrated the results from the cost-effectiveness acceptability curve. Supportive care remained the most cost-effective option up to a threshold of <200 million IDR, after which PD first option was the most cost effective. Hemodialysis first option was not the best cost-effective option at any level of willingness to pay (43 million IDR equates roughly to $4,000 CAD).
Other contextual factors
- Equity: We did not identify direct evidence to address equity for this question.
- Acceptability: We did not identify direct evidence to address acceptability for this question. However, the included study provided information on the survival of patients who have chosen to forego dialysis and demonstrated that in patients aged >75 years with high extra-renal comorbidity, the survival advantage conferred by KRT over conservative management is likely to be small [65]. Our update search conducted in October 2021 identified a protocol for a pilot RCT aiming to explore the feasibility and acceptability of Conservative Kidney Management Options and Advance Care Planning Education—COPE, change in communication of preferences and differences in the intervention’s effects on knowledge and communication of preferences by race (Stallings et al., 2021).
- Feasibility: We did not identify direct evidence to address feasibility for this question.
- Implementation: We did not identify direct evidence to address implementation for this question.
For additional details, please see the EtD framework and SoF table in (Supplementary material, Document S1).
Research needs for recommendation 9
The research needs identified by the NICE guideline [20], and confirmed by the CKD Task Force, were as follows:
- What is the clinical and cost-effectiveness of conservative management versus dialysis in frail, older people? [20].
- Can a CKD Frailty Index be used to inform patient decision-making? [68].
- What would constitute the index—could it be based on the Integrated Palliative Care Outcome Scale (IPOS)-Renal index? [68] And finally,
- Could a CKD Frailty Index be combined with traditional and novel biomarkers and clinical scoring systems (serial assessments of fluid status, nutritional status and/or body composition) to guide initiation of dialysis? [68]
Additional considerations
The NICE guideline [20] recommended to offer information on all medically appropriate treatment options when discussing switching KRT modality. Switching treatment modality or stopping KRT should be considered if medically indicated or if the patient (or, where appropriate, the family/caregiver) asks for this, and planned wherever possible. The guideline advised against routinely switching patients on PD to a different modality in anticipation of potential future complications (e.g., encapsulating peritoneal sclerosis) but rather to monitor risk factors (such as loss of ultrafiltration). It recommended to seek specialist advice on the need for switching modality when women become pregnant or wish to become pregnant. The need for a switch in these situations would depend on the adequacy of dialysis, the health of the fetus and the control of urea.
Evidence summary
Neither the literature search conducted for the NICE guideline [20] nor our update search identified any evidence addressing this question.
Benefits and harms
Insufficient evidence to inform what are the benefits and harms of any particular strategy for transferring between KRT modalities or for discontinuing KRT.
Certainty in the evidence
We did not rate the overall certainty in the evidence of effects for all reported outcomes due to insufficient evidence.
Values
We did not identify primary studies addressing the relative importance of the outcomes for this question. A review summarizing the literature on the transition between different KRT modalities noted that transitioning from one KRT modality to another can have a huge impact on the well-being and lifestyle of patients and their caregivers (INTEGRATED group consists of (in alphabetical order) et al., 2019). One study defined six categories of transitions of care during advanced CKD: (1) transition from non-dialysis-dependent CKD to de novo dialysis therapy; (2) transition from non-dialysis dependent CKD to pre-emptive transplantation; (3) transition among or across dialysis modalities, formats and frequency (hemodialysis to PD or vice versa, in-center to home; (4) transition from dialysis therapy to KT; (5) transition from a gradually failing KT back to dialysis therapy; and (6) transition from any of the above stages to partial or full transitions can be present in patients with CKD (Kalantar-Zadeh et al., 2017). There is uncertainty regarding what factors make patients’ transition and their caregivers’ experiences successful, stressful, or even unsuccessful. Moreover, data are lacking on how patients and their caregivers perceive such a transition, what their ideas and emotions are, and how they cope with them [68].
Resource use and cost-effectiveness
We did not identify primary studies addressing the resources required and cost-effectiveness to manage CKD patients with KRT. We report indirect evidence regarding the cost of the disease and different CKD interventions.
- Cost of disease
CKD affects about 10 percent of the population worldwide, including an estimated 1 in 7 adult Americans. In the US, Medicare spending totals more than $64 billion each year to care for Americans with CKD and an additional $34 billion to care for patients with ESKD (Initiative, 2018).
The impact of kidney disease extends well beyond the United States; over 2 million people worldwide have ESKD. In higher-income countries, treatment costs are enormous: a 2010 report from the UK National Health Service estimates its annual CKD spending at £1.45 billion—more than half of which was for KRT [45]—while Australia has estimated it will spend over $12 billion on ESKD patients through 2020 [46]. At the same time, KRT remains entirely unaffordable to the majority of ESKD patients in low- and middle-income countries throughout the world, with over 1 million people dying annually from lack of treatment [47].
- Cost of interventions
Initial assessment clinic: annual cost per patient £2,537 (SAR 13,137), annual expenditure £6,421,018 (SAR 33,238,174). The mean total cost per hemodialysis session was calculated as 297 US USD (1,114 SAR), and the mean total cost of dialysis per patient per year was 46,332 USD (173,784 SAR) [48]. One study conducted in Saudi Arabia described that an average annual cost of medical care per patient after transplantation in the first, second, third, and fourth year was US $133,291, US $14,233, US $5,536, and US $4,402; respectively. The average 4-year actual total cost per patient was US $210,779 and US $317,186.3 in the kidney transplant group and the hemodialysis group; respectively (p=0.017) [49]. One systematic review reported annual costs of hemodialysis and PD in low and middle-income countries. The annual cost per patient for hemodialysis ranged from Int$ 3,424 to Int$ 42,785, and PD ranged from Int$ 7,974 to Int$ 47,971. Direct medical cost especially drugs and consumables for hemodialysis and dialysis solutions and tubing for PD were the main cost drivers [50].
In terms of cost-effectiveness, one systematic review directly addresses the cost-effectiveness of different KRT. KT was the most cost-effective KRT modality and PD was more cost-effective than hemodialysis. Most studies suggested that KT held a dominant position over hemodialysis and PD with both lower costs and higher effectiveness. Five studies suggested that increased uptake of KT and PD by new ESKD patients would reduce costs and improve health outcomes or would be more cost-effective than current practice patterns [43].
Other contextual factors
- Equity: We did not identify direct evidence to address equity for this question.
- Acceptability: We did not identify direct evidence to address acceptability for this question. Indirect evidence from one study provided information on the survival of patients who have chosen to forego dialysis. The study demonstrated that in patients aged >75 years with high extra-renal comorbidity, the survival advantage conferred by KRT over conservative management is likely to be small [65].
- Feasibility: We did not identify direct evidence to address feasibility for this question.
- Implementation: We did not identify direct evidence to address implementation for this question.
Our update search conducted in October 2021 identified a protocol for a pilot RCT aiming to explore the feasibility and acceptability of Conservative Kidney Management Options and Advance Care Planning Education—COPE, change in communication of preferences and differences in the intervention’s effects on knowledge and communication of preferences by race (Stallings et al., 2021).
For additional details, please see the EtD framework and SoF table in (Supplementary material, Document S1).
Research needs for recommendation 10
The NICE guideline [20] identified the following research need, confirmed by the CKD Task Force: What is the clinical and cost-effectiveness of strategies for switching KRT modality?
The review summarizing the literature on the transition between different KRT modalities (INTEGRATED group consists of (in alphabetical order) et al., 2019) reported a number of unanswered questions related to transition of care in CKD, including whether the transition to KRT and the type and modality of the transition should be selected based on pre-dialysis patient data; regarding the outcome predictability of pre-ESKD conditions with selection of dialysis modality (hemodialysis versus PD), format (in-center versus home), frequency (daily versus infrequent) and vascular access (pre-emptive AVF or PD catheter placement versus no access placement until dialysis starts); regarding what factors make patients’ transition and their caregivers’ experiences successful, stressful, or even unsuccessful; and how patients and their caregivers perceive such a transition, what their ideas and emotions are, and how they cope with them.
Additional considerations
The NICE guideline committee [20] noted that what is reviewed will vary according to clinical circumstances but may include serum biochemistry, blood pressure and weight. Some reviews will need to be carried out face to face, whereas others can be done remotely. Increasing the frequency of review may allow for faster recognition of deterioration in the health state of patients on KRT and conservative management, and may improve communication, adherence with treatment and the prevention of complications. These benefits must be weighed against the potential harms of treatment burden for the patient and healthcare services, in particular those related to KRT where patients may have many different healthcare contacts and multiple weekly hospital visits due to the severity of their condition and comorbidities.
- Transplant: Practice for assessing transplant function can vary between centers but commonly involves eGFR measurement every 3 months and eGFRs being reviewed by the renal team on a 3-6 monthly basis. Children are usually assessed at least every 3 months. The general health of people with a stable KT is typically assessed at least once a year and includes the assessment of cardiovascular risk factors.
- Dialysis: In the absence of any evidence, it is difficult to make any specific recommendations about the ideal frequency of review in people on dialysis. Patients receiving in-center dialysis may be reviewed too frequently as it is logistically easy to do.
- Conservative management: Frequency of review in this patient group is highly dependent on the prognosis of the patient and stage of treatment. The frequency of review will increase as the person’s condition deteriorates, based on individual circumstances and preferences. Face-to-face review is likely to be particularly important for patients receiving conservative management to assess current functional status.
Evidence summary
Neither the literature search conducted for the NICE guideline [20] nor our update search identified any evidence addressing this question.
Benefits and harms
Insufficient evidence to inform what are the benefits and harms on how frequently patients on different forms of KRT should be reviewed.
Certainty in the evidence
We did not rate the overall certainty in the evidence of effects for all reported outcomes due to insufficient evidence.
Values
We did not find primary studies addressing the relative importance of the outcomes for this question. Patient representatives and advocates presenting at the KDIGO Controversies Conference on Early Identification & Intervention in CKD in October 2019 expressed a strong belief that patients prefer earlier CKD screening and diagnosis [42]. They also emphasized that the decisions concerning age to initiate testing, the frequency of repeat testing and time to forgo or end testing should be personalized based on risk factors, preferences, and life expectancy.
One systematic review described the following regarding the relative importance of outcomes and patients’ preferences for hemodialysis, PD, and KT. Patients highly value the benefits of hemodialysis, PD, and KT [43]. The utility values for hemodialysis ranged from 0.44 to 0.72; for PD from 0.53 to 0.81; for KT from 0.57 to 0.90. In seven of the nine studies, KT utility was higher than PD utility, and PD utility was higher than hemodialysis utility. In two of the nine studies, KT utility was higher than PD and hemodialysis utility, with PD and hemodialysis utility being equal. One study suggests that conflicting results of utility valuations existed among different valuation methods. For example, continuous ambulatory PD patients’ EQ-5D scores were higher than those of center hemodialysis patients, while continuous ambulatory PD patients’ SG and TTO scores were lower than those of center hemodialysis patients [43].
Resource use and cost-effectiveness
We did not identify primary studies addressing the resources required and cost-effectiveness to address this specific question. We report indirect evidence regarding the cost of different CKD interventions. The NICE guideline pointed out that more frequent review will be associated with more healthcare appointments leading to higher costs.
- Cost of interventions
Initial assessment clinic: annual cost per patient £2,537 (SAR 13,137), annual expenditure £6,421,018 (SAR 33,238,174). The mean total cost per hemodialysis session was calculated as 297 USD (1,114 SAR), and the mean total cost of dialysis per patient per year was 46,332 USD (173,784 SAR) [48]. One study conducted in Saudi Arabia described that an average annual cost of medical care per patient after transplantation in the first, second, third, and fourth year was US $133,291, US $14,233, US $5,536, and US $4,402; respectively. The average 4-year actual total cost per patient was US $210,779 and US $317,186.3 in the kidney transplant group and the hemodialysis group; respectively (p=0.017) [49].
In terms of cost-effectiveness, one study assessed the value for money and budget impact of offering hemodialysis as a first-line treatment, or the hemodialysis-first policy, and the PD first policy compared to a supportive care option in patients with ESKD in Indonesia [66]. The PD-first policy was found to be more cost-effective compared to the hemodialysis-first policy. Budget impact analysis provided evidence on the enormous financial burden for the country if the current practice, where hemodialysis dominates PD, continues for the next five years.
-
Costs:
- ○
-
Life years saved
- ▪
- Supportive care option: 0.21
- ▪
- PD first option: 5.93
- ▪
- Hemodialysis first option: 5.93
- ○
-
Quality-adjusted life years
- ▪
- Supportive care option: 0.076
- ▪
- PD first option: 4.40
- ▪
- Hemodialysis first option: 4.34
- ○
-
Incremental cost-effectiveness ratio
- ▪
- Supportive care: Not reported
- ▪
- PD first option: 193.2 million IDR
- ▪
- Hemodialysis first option: 2017.4 million IDR
- ○
-
Cost-effectiveness acceptability
- ▪
- At the threshold of willingness to pay 43 million IDR (1 GDP), supportive care was the best option (probability = 1.00)
- ▪
- At willingness to pay >190million IDR, PD first was the most cost-effective option (probability >0.5)
- ▪
- Hemodialysis first was not the best cost-effective option at any level of willingness to pay.
A CADTH Review [67] demonstrated the results from the cost-effectiveness acceptability curve. Supportive care remained the most cost-effective option up to a threshold of < 200 million IDR, after which PD first option was the most cost effective. Hemodialysis first option was not the best cost-effective option at any level of willingness to pay (43 million IDR equates roughly to $4,000 CAD).
Other contextual factors
- Equity: We did not identify direct evidence to address equity for this question.
- Acceptability: We did not identify direct evidence to address acceptability for this question. Indirect evidence from one study provided information on the survival of patients who have chosen to forego dialysis. The study demonstrated that in patients aged >75 years with high extra-renal comorbidity, the survival advantage conferred by KRT over conservative management is likely to be small [65].
- Feasibility: We did not identify direct evidence to address feasibility for this question.
- Implementation: We did not identify direct evidence to address implementation for this question.
Our update search conducted in October 2021 identified a protocol for a pilot RCT aiming to explore the feasibility and acceptability of Conservative Kidney Management Options and Advance Care Planning Education—COPE, change in communication of preferences and differences in the intervention’s effects on knowledge and communication of preferences by race (Stallings et al., 2021).
For additional details, please see the EtD framework and SoF table in (Supplementary material, Document S1).
Research needs for recommendation 11
The NICE guideline [20] identified the following research needs, confirmed by the CKD Task Force:
- What is the most clinical and cost-effective frequency of review for people on PD, hemodiafiltration, hemodialysis or conservative management? [20]
- Could a CKD Frailty Index be used to identify clinically important changes over time in individuals before dialysis and after initiation of dialysis? [68]
- Are the changes different with hemodialysis versus PD? [68]
- Is it possible to predict which patients improve and which get worse? [68]
- To what extent do uremic symptoms change after initiation of dialysis? [68]
Additional considerations
In order to enable patients, their families and caregivers to make informed decisions, the NICE guideline recommended to offer balanced and accurate information about
-
Treatments including KRT, conservative management and dietary intervention:
- What they involve, for example, availability of assistance, time that treatment takes place, and number of sessions per day/week
- Potential benefits
- The benefits of adherence to treatment regimens and the potential consequences of non-adherence
- Potential adverse effects, their severity and how they may be managed
- The likely prognosis on dialysis, after transplant or with conservative management
- The transplant listing process (when appropriate)
- Switching the modality of KRT and the possible consequences (that is, the impact on the person's life or how this may affect future treatment or outcomes)
- Reviewing treatment decisions
- Stopping treatment and planning end of life care.
-
Information about how treatments may affect lifestyle:
- The person or caregiver's ability to carry out and adjust the treatment themselves
- The possible impact of dietary management and management of fluid allowance
- How treatment may fit in with daily activities such as work, school, hobbies, family commitments and travel for work or leisure
- How treatment may affect sexual function, fertility, and family planning
- Opportunities to maintain social interaction
- How treatment may affect body image
- How treatment may affect physical activity (for example, whether contact sports should be avoided after transplantation, whether swimming should be avoided with PD)
- Whether a person's home will need to be modified to accommodate treatment
- How much time and travel treatment or training will involve
- The availability of transport
- The flexibility of the treatment regimen
- Whether any additional support or services might be needed.
The guideline also advised to offer oral and written information in an accessible format early enough to allow time for patients to fully understand their treatment options and make informed decisions; to direct patients to other sources of information and support such as online resources, pre-dialysis classes and peer support; to remember that some decisions must be made months before KRT is needed (e.g. fistula creation); to take into account information the patient has obtained from other sources such as family members and caregivers, and how this has influenced their decision; to ensure that healthcare professionals offering information have specialist knowledge about late-stage CKD and the skills to support shared decision making; and to offer patients who have presented late, or who started dialysis in an unplanned way, the same information as to those presenting at an earlier stage.
Evidence summary
The literature search conducted for the NICE guideline [20] identified thirty-nine qualitative studies (2018). Four of these studies were in children between the ages of 2 and 16 (and their parents), thirty-three studies included people aged 25 to 70 and two studies evaluated people aged 70 and over. Two studies focused on the pre-KRT population, two studies involved a mix of people before and during KRT. Five studies involved patients with any form of KRT, eight studies those undergoing either hemodialysis or PD (two with the input of caregivers) and eight studies patients who had received a transplant. Twelve studies involved patients undergoing hemodialysis only (two with the input of caregivers). One study involved those who had opted for conservative management. In our update search conducted in October 2021, we found an additional nineteen studies relevant to this question that dealt with the content of information, preferred format of information, decision making, psychological support, barriers and facilitators to good care, and modality of KRT.
Benefits and harms
Themes identified from the qualitative studies:
- Content of Information: Content of information should cover symptoms, prognosis, mode of access, benefits, and harms of different modalities of KRT and conservative management, services, adherence, how to approach living donors, acute situations, kidney function and CKD, Information around transitions between forms of KRT, and end-of-life care.
- Format of information provision: Patients reported the depth and timing of information, personalized information, delivery via classes and tours, and in multiple formats, and the target of education/information as important themes to be addressed. Decision making was also identified as an important topic for education.
- Stress/support: People noted that the availability of transport affected their ability to engage with KRT and was a significant psychological stressor during KRT. Psychological support was identified as one of the support systems.
- Barriers/problems: Barriers to home dialysis were lack of a care partner, lack of home space, and patient preference (El Shamy et al., 2021). Some of the participants encountered periods of limited funds. Some of the participants experienced the effects of the hidden costs of dialysis, such as specific dietary requirements including specific, more costly food groups (Small, 2010). Further problems described by patients included lack of information and dissatisfaction with their healthcare providers regarding perceptions of their care, lack of explanation of results, not being completely honest, kept in the dark about the seriousness of the problem, and not being clear about when dialysis would occur (Harwood et al., 2005).
- Facilitators of good care: Patients thought 1:1 time with transplant team members was helpful, and they wanted additional information sources as well, without losing 1:1 time (Korus et al., 2011).
- Impact of treatment on lifestyle: Patients mentioned that information on any modality choice, including limitations on travel, and sexual activity as areas they appreciated or would have appreciated.
- Information sources: These include sources other than healthcare professionals such as support groups and online resources.
Certainty in the evidence
We rated the overall certainty in the evidence of effects as moderate based on the lowest certainty in the evidence for the critical outcomes, owing to methodological limitations and concerns regarding adequacy for the assessment of outcomes.
Values
A retrospective cohort study evaluated whether a pre-dialysis education program (PDEP) was an acceptable tool for increasing the rates of PD in ESKD patients (Alghamdi et al., 2020). It showed that PDEP significantly reduced hemodialysis rates [OR (95% CI) = 0.11 (0.05-0.24); P-value < 0.001]. The PDEP positively impacted the rate of PD, while PD was associated with favorable outcomes and lower infection rates, emphasizing the importance of the educational program. Another study found that a series of structured PDEP sessions for the patients progressing to ESKD facilitated their selection of KRT (Mirza et al., 2020). Two studies showed that educating health promotion strategies were effective in improving self-esteem and quality of life in patients undergoing hemodialysis (Ghadam et al., 2015; Poorgholami et al., 2015).
Resource use and cost-effectiveness
We did not identify primary studies addressing the resources required to provide information, education and support to CKD patients.
Other contextual factors
- Equity: We did not identify direct evidence to address equity for this question.
- Acceptability: One study reported that quality-of-life issues for people with CKD include depression and anxiety, which are prevalent among people undergoing hemodialysis (Musa et al., 2018). Several small studies addressed whether screening, counseling or education might support social interactions (Kazemi et al., 2011), self-esteem (Poorgholami et al., 2015), or the families of children undergoing PD (Alhameedi and Collier, 2016).
- Feasibility: We did not identify direct evidence to address feasibility for this question. Studies that examined areas for improvement in the delivery of care included a cross-sectional study in Palestine that found self-reported adherence to diet, fluid restriction, medications, and hemodialysis sessions to be optimal in about 56% of 220 people with end-stage renal disease (Naalweh et al., 2017). A record review in New York found that lack of motivation, dialysis dependence, and comorbidities predicted failure to complete pre-transplantation preparation (Siskind et al., 2014). The authors suggested that interventions such as timely referral, educational resources, counseling, and support might increase workup completion rates or improve therapeutic outcomes.
- Implementation: We did not identify direct evidence to address implementation for this question.
For additional details, please see the EtD framework and SoF table in (Supplementary material, Document S1).
Research needs for recommendation 12
The NICE guideline [20] identified the following research needs, which were confirmed by the CKD Task Force:
- What is the clinical and cost-effectiveness of having keyworkers present in the context of KRT? [20]
- What is the clinical and cost-effectiveness of using decision aids in the context of KRT? [20].
- Can an integrated care model improve quality and decrease costs for patients with kidney disease as they transition from CKD G5 to G5D? [68].
- What is the preferred timing for educating patients regarding dialysis modalities? Does the optimal time vary based on patient characteristics? [68].
- What is the optimal content and format for educating patients regarding the advantages and disadvantages of each modality? How do we check their understanding? [68]
The CKD Task Force proposes that researchers develop studies (RCTs) to assess the impact of interventions, namely education and support to patients, families, and caregivers to evaluate the effectiveness and impact on outcomes like morbidity and mortality.
4.2. Performance measures
Performance measures (also known as key performance indicators, or KPIs) are quantifiable objectives that assess structures, processes, and outcomes. They define numerator and denominator definitions in order to assess how well a population of patients adheres to a specific clinical practice guideline [69].
A goal of guideline development is to create KPIs that work in tandem with evidence-based recommendations. Methodological rigor and relevance to guideline development have frequently been limited [70].
Searches were conducted to identify literature that might provide KPIs relevant to the questions and recommendations in this CKD guideline (for details on the search strategies see (Supplementary material, Document S1)). The resulting literature was shared with the team at King Saud University Medical City's Corporate Quality Management Department in Riyadh, who developed a long list of KPI candidates. The CKD Task Force submitted these for voting via a survey and a 1-to-9-point rating scale. In total, the CKD Task Force rated 14 KPIs, six of which were chosen for inclusion in the CKD guideline (for details on the KPIs please refer to the KPI sheets in the full CPG document (Supplementary material, Document S1).
4.3. Limitations of these guidelines
In comparison to previous efforts, this guideline adheres to the rigorous GRADE-ADOLOPMENT methodology, which is aimed at evaluating not only the quality of the evidence, but also the numerous factors that influence healthcare decisions, such as locally available intervention options, the balance of benefits and harms, the certainty of the evidence, the impact of patient characteristics, circumstances, values, and preferences on clinical decisions, and the impact of social, economic, or other practical cons.
4.4. Guideline dissemination and implementation
This guideline's multifaceted interventions to increase clinical adoption will include: Dissemination by website and app with content feeds from the associated GRADEpro account via API. Moreover, Implementation tools will include customized computerized provider order entry (CPOE) with order sets integrated into electronic health record systems at selected pilot sites throughout Saudi Arabia. Local guideline implementation strategies/interventions may also include: leadership commitment and engagement, dissemination and communication, regular training and education, regular audit and feedback to identify facilitators and barriers, and patients as change champions [71,72,73,74].
4.5. Updating or adapting of the guideline recommendations
The National Guidelines Center will review the guideline no later than 5 years after its publication, with an earlier review prompted by new substantial evidence and results of audit and feedback after implementation. The Checklist for the Reporting of Updated Guidelines (CheckUp) will guide the guideline update process [75].
4.6. The format of this Guideline Publication
Supplementary Materials
The following supporting information can be downloaded at: Preprints.org, Document S1: The CKD Guideline Full Document; Table S1: AGREE Reporting Checklist; Table S2: RIGHT-Ad@pt Checklist.
Author Contributions
Conceptualization, K.A.A., Z.A.M., and K.B.; methodology, J.J.Y.N., J.S.V., X.A., K.B., R.C., S.F., S.B., K.B.; validation, K.A.A., Y.S.A.; investigation, all authors; resources, K.A.A., K.B.; data curation, J.J.Y.N., J.S.V., X.A., S.F., S.B., K.B.; writing—original draft preparation, Y.S.A., K.A.A.; writing—review and editing, K.B., X. A.; supervision, K.A.A, K.B.; project administration, K.A.A, K.B.; funding acquisition, K.A.A, K.B.;. All authors have read and agreed to the published version of the manuscript.
Funding
The funding for this guideline project was reported in details in the Methods section.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not Applicable.
Acknowledgments
The authors would like to thank the other members of the CKD Guideline Task force including Mohammed Alrasheed, Abdulrahman Alqahtani, and Shatha Abuzinada; of the Guideline Support Team including: Hannu Gutt, Hema Jagota, Majed Sweis, Jennifer Goldstein, Maura Sostack, Naresh Goli, Sai Prasanna Vangapelly (Elsevier), and Maher A. Titi (King Saud University Medical City). Moreover, we would like to extend our gratitude to the Peer review and approval panel including: Faissal Shaheen (WHO Task Force for Organ and Tissue Donation and Transplantation and International Society for Organ Donation and Procurement), Rupesh Raina (American Kidney Institute), Ali Alrehaily, and Mohamad Saeedi (Saudi Health Council). Roles and responsibilities of all groups were reported in detail in the full guideline document (Supplementary material, Document S1).
Conflicts of Interest
The authors declare no conflict of interest (further details were mentioned in the methods section). The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- Memish, Z.A.; Alqahtani, A.S.; Al-Azemi, N.; Abu Alhamayel, N.; Saeedi, M.; Abuzinada, S.; Albarakati, R.G.; Natarajan, S.; Alvira, X.; Bilimoria, K.; et al. A New Era of National Guideline Development in Saudi Arabia. J. Epidemiology Glob. Health 2022, 12, 373–379. [Google Scholar] [CrossRef] [PubMed]
- Afiatin; Khoe, L.C.; Kristin, E.; Masytoh, L.S.; Herlinawaty, E.; Werayingyong, P.; Nadjib, M.; Sastroasmoro, S.; Teerawattananon, Y. Economic evaluation of policy options for dialysis in end-stage renal disease patients under the universal health coverage in Indonesia. PLoS ONE 2017, 12, e0177436. [CrossRef]
- Agarwal, A.; Cheung, A.K.; Ma, J.; Cho, M.; Li, M. Effect of Baseline Kidney Function on the Risk of Recurrent Stroke and on Effects of Intensive Blood Pressure Control in Patients With Previous Lacunar Stroke: A Post Hoc Analysis of the SPS3 Trial (Secondary Prevention of Small Subcortical Strokes). J. Am. Hear. Assoc. 2019, 8, e013098. [Google Scholar] [CrossRef] [PubMed]
- Qaseem, A.; Forland, F.; Macbeth, F.; Ollenschläger, G.; Phillips, S.; van der Wees, P. Guidelines International Network: toward international standards for clinical practice guidelines. Annals of Internal Medicine 2012, 156, 525–531. [Google Scholar] [CrossRef] [PubMed]
- Guyatt, G.H.; Oxman, A.D.; Vist, G.E.; Kunz, R.; Falck-Ytter, Y.; Alonso-Coello, P.; Schünemann, H.J. GRADE: An emerging consensus on rating quality of evidence and strength of recommendations. BMJ 2008, 336, 924–926. [Google Scholar] [CrossRef] [PubMed]
- Schünemann, H.J.; Wiercioch, W.; Etxeandia, I.; Falavigna, M.; Santesso, N.; Mustafa, R.; Ventresca, M.; Brignardello-Petersen, R.; Laisaar, K.-T.; Kowalski, S.; et al. Guidelines 2.0: systematic development of a comprehensive checklist for a successful guideline enterprise. Can. Med Assoc. J. 2013, 186, E123–E142. [Google Scholar] [CrossRef] [PubMed]
- Schünemann, H.J.; Wiercioch, W.; Brozek, J.; Etxeandia-Ikobaltzeta, I.; Mustafa, R.A.; Manja, V.; Brignardello-Petersen, R.; Neumann, I.; Falavigna, M.; Alhazzani, W.; et al. GRADE Evidence to Decision (EtD) frameworks for adoption, adaptation, and de novo development of trustworthy recommendations: GRADE-ADOLOPMENT. J. Clin. Epidemiology 2017, 81, 101–110. [Google Scholar] [CrossRef]
- Cheung, A.K.; Chang, T.I.; Cushman, W.C.; Furth, S.L.; Hou, F.F.; Ix, J.H.; Knoll, G.A.; Muntner, P.; Pecoits-Filho, R.; Sarnak, M.J.; et al. KDIGO 2021 Clinical Practice Guideline for the Management of Blood Pressure in Chronic Kidney Disease. Kidney Int. 2021, 99, S1–S87. [Google Scholar] [CrossRef]
- Levin, A.S.; Bilous, R.W.; Coresh, J. Chapter 1: Definition and classification of CKD. Kidney Int. Suppl. 2013, 3, 19–62. [Google Scholar] [CrossRef]
- Ariceta, G. Clinical practice. Eur. J. Pediatr. 2010, 170, 15–20. [Google Scholar] [CrossRef]
- Bhalla, K.; Singh, R.; Nanda, S.; Gupta, A.; Mehra, S. Correlation of spot urinary protein: Creatinine ratio and quantitative proteinuria in pediatric patients with nephrotic syndrome. J. Fam. Med. Prim. Care 2019, 8, 2343–2346. [Google Scholar] [CrossRef] [PubMed]
- NICE-NG203, 2021. Chronic kidney disease: assessment and management NICE guideline [NG203] [WWW Document]. Available online: https://www.nice.org.uk/guidance/ng203 (accessed on 29 November 2021).
- Rovin, B.H.; Adler, S.G.; Barratt, J.; Bridoux, F.; Burdge, K.A.; Chan, T.M.; Cook, H.T.; Fervenza, F.C.; Gibson, K.L.; Glassock, R.J.; et al. KDIGO 2021 Clinical Practice Guideline for the Management of Glomerular Diseases. Kidney Int. 2021, 100, S1–S276. [Google Scholar] [CrossRef] [PubMed]
- Al-Sayyari, A.A.; Shaheen, F.A. End stage chronic kidney disease in Saudi Arabia. A rapidly changing scene. Saudi Med. J. 2011, 32, 339–346. [Google Scholar] [PubMed]
- Ahmed, H.G.; Ginawi, I.A.; Haridi, H.K.; Eltom, F.M.; Al-Hazimi, A.M. Distribution of CKD and Hypertension in 13 Towns in Hail Region, KSA. Egypt. Acad. J. Biol. Sci. C, Physiol. Mol. Biol. 2014, 6, 39–45. [Google Scholar] [CrossRef]
- Al-Homrany, M.; Abolfotoh, M. Incidence of treated end-stage renal disease in asir region, southern saudi arabia. Saudi J. Kidney Dis. Transpl. 1998, 9, 425–430. [Google Scholar] [PubMed]
- Alsuwaida, A.O., Farag, Y.M.K., Al Sayyari, A.A., Mousa, D., Alhejaili, F., Al-Harbi, A., Housawi, A., Mittal, B.V., Singh, A.K., 2010. Epidemiology of chronic kidney disease in the Kingdom of Saudi Arabia (SEEK-Saudi investigators) - a pilot study. Saudi journal of kidney diseases and transplantation : an official publication of the Saudi Center for Organ Transplantation, Saudi Arabia 21.
- Mitwalli, A.H.; Al-Swailem, A.R.; Aziz, K.M.; Aswad, S.; Paul, T.; Mohammed, A.R.; Diwan, M.; Wafa, A.M. The incidence of end-stage renal disease in two regions of kingdom of saudi arabia. Saudi J. Kidney Dis. Transpl. 1995, 6, 280–285. [Google Scholar]
- Saudi Center for Organ Transplantation, 2020. Annual Report for the Saudi Center for Organ Transplantation in the Kingdom of Saudi Arabia (SCOT).
- NICE-NG107, 2018. Renal replacement therapy and conservative management NICE guideline [NG107] [WWW Document]. Available online: https://www.nice.org.uk/guidance/ng107 (accessed on 29 November 2021).
- Andrews, J.; Guyatt, G.; Oxman, A.D.; Alderson, P.; Dahm, P.; Falck-Ytter, Y.; Nasser, M.; Meerpohl, J.; Post, P.N.; Kunz, R.; et al. GRADE guidelines: 14. Going from evidence to recommendations: the significance and presentation of recommendations. J. Clin. Epidemiology 2013, 66, 719–725. [Google Scholar] [CrossRef]
- Brouwers, M.C.; Kerkvliet, K.; Spithoff, K. ; AGREE Next Steps Consortium The AGREE Reporting Checklist: a tool to improve reporting of clinical practice guidelines. BMJ 2016, 352, i1152. [Google Scholar] [CrossRef]
- Song, Y.; Alonso-Coello, P.; Ballesteros, M.; Cluzeau, F.; Vernooij, R.W.; Arayssi, T.; Bhaumik, S.; Chen, Y.; Ghersi, D.; Langlois, E.V.; et al. A Reporting Tool for Adapted Guidelines in Health Care: The RIGHT-Ad@pt Checklist. Ann. Intern. Med. 2022, 175, 710–719. [Google Scholar] [CrossRef]
- Hari, P.; Sahu, J.; Sinha, A.; Pandey, R.M.; Bal, C.S.; Bagga, A. Effect of enalapril on glomerular filtration rate and proteinuria in children with chronic kidney disease: A randomized controlled trial. Indian Pediatr. 2013, 50, 923–928. [Google Scholar] [CrossRef]
- Hanson, C.S.; Gutman, T.; Craig, J.C.; Bernays, S.; Raman, G.; Zhang, Y.; James, L.J.; Ralph, A.F.; Ju, A.; Manera, K.E.; et al. Identifying Important Outcomes for Young People with CKD and Their Caregivers: A Nominal Group Technique Study. Am. J. Kidney Dis. 2019, 74, 82–94. [Google Scholar] [CrossRef] [PubMed]
- Bress, A.P.; King, J.B.; Kreider, K.E.; Beddhu, S.; Simmons, D.L.; Cheung, A.K.; Zhang, Y.; Doumas, M.; Nord, J.; Sweeney, M.E.; et al. Effect of Intensive Versus Standard Blood Pressure Treatment According to Baseline Prediabetes Status: A Post Hoc Analysis of a Randomized Trial. Diabetes Care 2017, 40, 1401–1408. [Google Scholar] [CrossRef] [PubMed]
- Halbach, S. Practical application of ABPM in the pediatric nephrology clinic. Pediatr. Nephrol. 2019, 35, 2067–2076. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, R.; Sinha, A.D.; Pappas, M.K.; Abraham, T.N.; Tegegne, G.G. Hypertension in hemodialysis patients treated with atenolol or lisinopril: a randomized controlled trial. Nephrol. Dial. Transplant. 2014, 29, 672–681. [Google Scholar] [CrossRef] [PubMed]
- Hannedouche, T.; Landais, P.; Goldfarb, B.; Esper, N.E.; Fournier, A.; Godin, M.; Durand, D.; Chanard, J.; Mignon, F.; Suc, J.-M.; et al. Randomised controlled trial of enalapril and blockers in non- diabetic chronic renal failure. BMJ 1994, 309, 833–837. [Google Scholar] [CrossRef] [PubMed]
- PROCOPA Study Group. Dissociation between blood pressure reduction and fall in proteinuria in primary renal disease: a randomized double-blind trial. J. Hypertens. 2002, 20, 729–737. [Google Scholar] [CrossRef] [PubMed]
- Herlitz, H.; Harris, K.; Risler, T.; Boner, G.; Bernheim, J.; Chanard, J.; Aurell, M. The effects of an ACE inhibitor and a calcium antagonist on the progression of renal disease: the Nephros Study. Nephrol. Dial. Transplant. 2001, 16, 2158–2165. [Google Scholar] [CrossRef] [PubMed]
- Saruta, T.; Hayashi, K.; Ogihara, T.; Nakao, K.; Fukui, T.; Fukiyama, K.; for the CASE-J Study Group Effects of candesartan and amlodipine on cardiovascular events in hypertensive patients with chronic kidney disease: subanalysis of the CASE-J Study. Hypertens. Res. 2009, 32, 505–512. [CrossRef]
- Yilmaz, R.; Altun, B.; Kahraman, S.; Ozer, N.; Akinci, D.; Turgan, C. Impact of amlodipine or ramipril treatment on left ventricular mass and carotid intima-media thickness in nondiabetic hemodialysis patients. Ren. Fail. 2010, 32, 903–912. [Google Scholar] [CrossRef]
- Zucchelli, P.; Zuccalà, A.; Borghi, M.; Fusaroli, M.; Sasdelli, M.; Stallone, C.; Sanna, G.; Gaggi, R. Long-term comparison between captopril and nifedipine in the progression of renal insufficiency. Kidney Int. 1992, 42, 452–458. [Google Scholar] [CrossRef]
- Ruggenenti, P.; Podestà, M.A.; Trillini, M.; Perna, A.; Peracchi, T.; Rubis, N.; Villa, D.; Martinetti, D.; Cortinovis, M.; Ondei, P.; et al. Ramipril and Cardiovascular Outcomes in Patients on Maintenance Hemodialysis. Clin. J. Am. Soc. Nephrol. 2021, 16, 575–587. [Google Scholar] [CrossRef] [PubMed]
- ESCAPE Trial Group; Wühl, E.; Trivelli, A.; Picca, S.; Litwin, M.; Peco-Antic, A.; Zurowska, A.; Testa, S.; Jankauskiene, A.; Emre, S.; et al. Strict Blood-Pressure Control and Progression of Renal Failure in Children. New Engl. J. Med. 2009, 361, 1639–1650. [CrossRef]
- Agarwal, A.; Cheung, A.K.; Ma, J.; Cho, M.; Li, M. Effect of Baseline Kidney Function on the Risk of Recurrent Stroke and on Effects of Intensive Blood Pressure Control in Patients with Previous Lacunar Stroke: A Post Hoc Analysis of the SPS3 Trial (Secondary Prevention of Small Subcortical Strokes). J. Am. Hear. Assoc. 2019, 8, e013098. [Google Scholar] [CrossRef] [PubMed]
- Appel, L.J.; Wright, J.T.J.; Greene, T.; Agodoa, L.Y.; Astor, B.C.; Bakris, G.L.; Cleveland, W.H.; Charleston, J.; Contreras, G.; Faulkner, M.L.; et al. Intensive Blood-Pressure Control in Hypertensive Chronic Kidney Disease. New Engl. J. Med. 2010, 363, 918–929. [Google Scholar] [CrossRef] [PubMed]
- Cheung, A.K.; Rahman, M.; Reboussin, D.M.; Craven, T.E.; Greene, T.; Kimmel, P.L.; Cushman, W.C.; Hawfield, A.T.; Johnson, K.C.; Lewis, C.E.; et al. Effects of Intensive BP Control in CKD. J. Am. Soc. Nephrol. 2017, 28, 2812–2823. [Google Scholar] [CrossRef] [PubMed]
- Klahr, S.; Levey, A.S.; Beck, G.J.; Caggiula, A.W.; Hunsicker, L.; Kusek, J.W.; Striker, G. The Effects of Dietary Protein Restriction and Blood-Pressure Control on the Progression of Chronic Renal Disease. New Engl. J. Med. 1994, 330, 877–884. [Google Scholar] [CrossRef] [PubMed]
- Winkelmayer, W.C.; Owen, W.F.; Levin, R.; Avorn, J. A Propensity Analysis of Late Versus Early Nephrologist Referral and Mortality on Dialysis. J. Am. Soc. Nephrol. 2003, 14, 486–492. [Google Scholar] [CrossRef] [PubMed]
- Controversies Conference on Early Identification & Intervention in CKD, 2019.
- Yang, F.; Liao, M.; Wang, P.; Yang, Z.; Liu, Y. The Cost-Effectiveness of Kidney Replacement Therapy Modalities: A Systematic Review of Full Economic Evaluations. Appl. Heal. Econ. Heal. Policy 2020, 19, 163–180. [Google Scholar] [CrossRef]
- Gadelkarim, H.; Alzayed, F.S.M.; Albluwe, H.K.A.; Alosayfir, Z.A.S.; Aljarallah, M.Y.J.; Alghazi, B.K.M.; Mohammed Ali Ghazai, A. Etiology of Chronic Kidney Disease (CKD) in Saudi Arabia. International Journal of Medical Research Health Sciences 2019, 8, 177–182. [Google Scholar]
- Jha, V.; Garcia-Garcia, G.; Iseki, K.; Li, Z.; Naicker, S.; Plattner, B.; Saran, R.; Wang, A.Y.-M.; Yang, C.-W. Chronic kidney disease: Global dimension and perspectives. Lancet 2013, 382, 260–272. [Google Scholar] [CrossRef]
- Cass, A.; Chadban, S.; Gallagher, M. The economic impact of end-stage kidney disease in Australia: Projections to 2020. Kidney Health Australia 2010, 1–68. [Google Scholar]
- Couser, W.G.; Remuzzi, G.; Mendis, S.; Tonelli, M. The contribution of chronic kidney disease to the global burden of major noncommunicable diseases. Kidney Int. 2011, 80, 1258–1270. [Google Scholar] [CrossRef] [PubMed]
- Al Saran, K.; Sabry, A. The cost of hemodialysis in a large hemodialysis center. Saudi J. Kidney Dis. Transpl. 2012, 23, 78–82. [Google Scholar] [PubMed]
- Hamawi, K.; Al-Jedai, A.; Alsultan, M.; Almeshari, K.; Alshaibani, K.; Elgamal, H.; Alkortas, D.; Khurshid, F.; Altalhi, M. Cost analysis of kidney transplantation in highly sensitized recipients compared to intermittent maintenance hemodialysis. Ann. Transplant 2012, 17, 82–91. [Google Scholar] [CrossRef] [PubMed]
- Mushi, L.; Marschall, P.; Fleßa, S. The cost of dialysis in low and middle-income countries: a systematic review. BMC Heal. Serv. Res. 2015, 15, 506. [Google Scholar] [CrossRef] [PubMed]
- Kwek, J.L.; Griva, K.; Kaur, N.; Chong, K.Y.; Chua, Z.Y.; Sim, G.H.A.; Ng, L.C.; Yong, P.W.; Tung, Y.-T.; Lim, L.W.W.; et al. Effectiveness and acceptability of a multidisciplinary approach in improving the care of patients with advanced chronic kidney disease: a pilot study. Int. Urol. Nephrol. 2021, 54, 917–926. [Google Scholar] [CrossRef] [PubMed]
- Ranganathan, D.; John, G.T.; Yeoh, E.; Williams, N.; O'Loughlin, B.; Han, T.; Jeyaseelan, L.; Ramanathan, K.; Healy, H. A Randomized Controlled Trial to Determine the Appropriate Time to Initiate Peritoneal Dialysis after Insertion of Catheter (Timely PD Study). Perit Dial Int. 2017, 37, 420–428. [Google Scholar] [CrossRef] [PubMed]
- Ishani, A.; Gilbertson, D.T.; Kim, D.; Bradbury, B.D.; Collins, A.J. Predialysis Care and Dialysis Outcomes in Hemodialysis Patients with a Functioning Fistula. Am. J. Nephrol. 2014, 39, 238–247. [Google Scholar] [CrossRef] [PubMed]
- Ravani, P.; Brunori, G.; Mandolfo, S.; Cancarini, G.; Imbasciati, E.; Marcelli, D.; Malberti, F. Cardiovascular Comorbidity and Late Referral Impact Arteriovenous Fistula Survival. J. Am. Soc. Nephrol. 2004, 15, 204–209. [Google Scholar] [CrossRef]
- Bello, A.K.; Levin, A.; Tonelli, M.; Okpechi, I.G.; Feehally, J.; Harris, D.; Jindal, K.; Salako, B.L.; Rateb, A.; Osman, M.A.; et al. Assessment of Global Kidney Health Care Status. JAMA 2017, 317, 1864–1919. [Google Scholar] [CrossRef]
- Alharbi, K.; Enrione, E.B. Malnutrition is prevalent among hemodialysis patients in Jeddah, Saudi Arabia. Saudi J Kidney Dis Transpl. 2012, 23, 598–608. [Google Scholar] [PubMed]
- Kiani, B.; Bagheri, N.; Tara, A.; Hoseini, B.; Hashtarkhani, S.; Tara, M. Comparing potential spatial access with self-reported travel times and cost analysis to haemodialysis facilities in North-eastern Iran. Geospat. Health 2018, 13, 240–246. [Google Scholar] [CrossRef] [PubMed]
- Cervantes, L.; Richardson, S.; Raghavan, R.; Hou, N.; Hasnain-Wynia, R.; Wynia, M.K.; Kleiner, C.; Chonchol, M.; Tong, A. Clinicians' Perspectives on Providing Emergency-Only Hemodialysis to Undocumented Immigrants. Ann. Intern. Med. 2018, 169, 78. [Google Scholar] [CrossRef] [PubMed]
- Chaiviboontham, S.; Phinitkhajorndech, N.; Tiansaard, J. Symptom Clusters in Patients with End-Stage Renal Disease Undergoing Hemodialysis. Int. J. Nephrol. Renov. Dis. 2020, 13, 297–305. [Google Scholar] [CrossRef] [PubMed]
- Akkina, S.K.; Connaire, J.J.; Snyder, J.J.; Matas, A.J.; Kasiske, B.L. Earlier Is Not Necessarily Better in Preemptive Kidney Transplantation. Am. J. Transplant. 2008, 8, 2071–2076. [Google Scholar] [CrossRef] [PubMed]
- Cooper, B.A.; Branley, P.; Bulfone, L.; Collins, J.F.; Craig, J.C.; Fraenkel, M.B.; Harris, A.; Johnson, D.W.; Kesselhut, J.; Li, J.J.; et al. A Randomized, Controlled Trial of Early versus Late Initiation of Dialysis. New Engl. J. Med. 2010, 363, 609–619. [Google Scholar] [CrossRef] [PubMed]
- Ishani, A.; Ibrahim, H.N.; Gilbertson, D.; Collins, A.J. The impact of residual renal function on graft and patient survival rates in recipients of preemptive renal transplants. Am. J. Kidney Dis. 2003, 42, 1275–1282. [Google Scholar] [CrossRef] [PubMed]
- Winnicki, E.; Johansen, K.L.; Cabana, M.D.; Warady, B.A.; McCulloch, C.E.; Grimes, B.; Ku, E. Higher eGFR at Dialysis Initiation Is Not Associated with a Survival Benefit in Children. J. Am. Soc. Nephrol. 2019, 30, 1505–1513. [Google Scholar] [CrossRef]
- Preka, E.; Bonthuis, M.; Harambat, J.; Jager, K.J.; Groothoff, J.W.; Baiko, S.; Bayazit, A.K.; Boehm, M.; Cvetkovic, M.; O Edvardsson, V.; et al. Association between timing of dialysis initiation and clinical outcomes in the paediatric population: an ESPN/ERA-EDTA registry study. Nephrol. Dial. Transplant. 2019, 34, 1932–1940. [Google Scholar] [CrossRef]
- Chandna, S.M.; Da Silva-Gane, M.; Marshall, C.; Warwicker, P.; Greenwood, R.N.; Farrington, K. Survival of elderly patients with stage 5 CKD: comparison of conservative management and renal replacement therapy. Nephrol. Dial. Transplant. 2010, 26, 1608–1614. [Google Scholar] [CrossRef]
- Afiatin; Khoe, L.C.; Kristin, E.; Masytoh, L.S.; Herlinawaty, E.; Werayingyong, P.; Nadjib, M.; Sastroasmoro, S.; Teerawattananon, Y. Economic evaluation of policy options for dialysis in end-stage renal disease patients under the universal health coverage in Indonesia. PLOS ONE 2017, 12, e0177436. [CrossRef]
- Subramonian, A., Frey, N., 2020. Conservative Management of Chronic Kidney Disease in Adult Patients: A Review of Clinical Effectiveness and Cost-Effectiveness, CADTH Rapid Response Reports. Canadian Agency for Drugs and Technologies in Health, Ottawa (ON).
- Chan, C.T.; Blankestijn, P.J.; Dember, L.M.; Gallieni, M.; Harris, D.C.; Lok, C.E.; Mehrotra, R.; Stevens, P.E.; Wang, A.Y.-M.; Cheung, M.; et al. Dialysis initiation, modality choice, access, and prescription: conclusions from a Kidney Disease: Improving Global Outcomes (KDIGO) Controversies Conference. Kidney Int. 2019, 96, 37–47. [Google Scholar] [CrossRef] [PubMed]
- Nothacker, M.; on behalf of the Guidelines International Network (G-I-N) Performance Measures Working Group; Stokes, T.; Shaw, B.; Lindsay, P.; Sipilä, R.; Follmann, M.; Kopp, I. Reporting standards for guideline-based performance measures. Implement. Sci. 2015, 11, 6. [CrossRef]
- Piggott, T.; Langendam, M.; Parmelli, E.; Adolfsson, J.; Akl, E.A.; Armstrong, D.; Braithwaite, J.; Brignardello-Petersen, R.; Brozek, J.; Gore-Booth, J.; et al. Bringing two worlds closer together: a critical analysis of an integrated approach to guideline development and quality assurance schemes. BMC Health Serv. Res. 2021, 21, 172. [Google Scholar] [CrossRef] [PubMed]
- Amer, Y.S.; Wahabi, H.A.; Elkheir, M.M.A.; Bawazeer, G.A.; Iqbal, S.M.; Titi, M.A.; Ekhzaimy, A.; Alswat, K.A.; Alzeidan, R.A.; Al-Ansary, L.A. Adapting evidence-based clinical practice guidelines at university teaching hospitals: A model for the Eastern Mediterranean Region. J. Evaluation Clin. Pr. 2018, 25, 550–560. [Google Scholar] [CrossRef]
- Fischer, F.; Lange, K.; Klose, K.; Greiner, W.; Kraemer, A. Barriers and Strategies in Guideline Implementation—A Scoping Review. Healthcare 2016, 4, 36. [Google Scholar] [CrossRef] [PubMed]
- Peters, S.; Sukumar, K.; Blanchard, S.; Ramasamy, A.; Malinowski, J.; Ginex, P.; Senerth, E.; Corremans, M.; Munn, Z.; Kredo, T.; et al. Trends in guideline implementation: an updated scoping review. Implement. Sci. 2022, 17, 50. [Google Scholar] [CrossRef] [PubMed]
- Paksaite, P.; Crosskey, J.; Sula, E.; West, C.; Watson, M. A systematic review using the Theoretical Domains Framework to identify barriers and facilitators to the adoption of prescribing guidelines. Int. J. Pharm. Pract. 2020, 29, 3–11. [Google Scholar] [CrossRef] [PubMed]
- Vernooij, R.W.M.; Alonso-Coello, P.; Brouwers, M.; García, L.M.; Panel, C. Reporting Items for Updated Clinical Guidelines: Checklist for the Reporting of Updated Guidelines (CheckUp). PLOS Med. 2017, 14, e1002207. [Google Scholar] [CrossRef]
- Nieuwlaat, R.; Wiercioch, W.; Brozek, J.L.; Santesso, N.A.M.; Kunkle, R.; Alonso-Coello, P.; Anderson, D.R.; Bates, S.M.; Dahm, P.; Iorio, A.; et al. How to write a guideline: a proposal for a manuscript template that supports the creation of trustworthy guidelines. Blood Adv. 2021, 5, 4721–4726. [Google Scholar] [CrossRef] [PubMed]
- Yang, N.; Zhao, W.; Qi, W.-A.; Yao, C.; Dong, C.-Y.; Zhai, Z.-G.; Chen, T.; Liu, E.-M.; Li, G.-B.; Long, Y.-L.; et al. Publishing clinical prActice GuidelinEs (PAGE): Recommendations from editors and reviewers. Chin. J. Traumatol. 2022, 25, 312–316. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



