
Submitted:
07 January 2023
Posted:
09 January 2023
You are already at the latest version
Abstract
This study aimed to clarify the relationship between the joint and ligament structures of the subtalar joint and degeneration of the subtalar articular facet. We examined 50 feet from 25 Japanese cadavers. The number of articular facets, joint congruence, and intersecting angle were measured for the joint structure of the subtalar joint, and the footprint areas of the ligament attachments of the cervical ligament, interosseous talocalcaneal ligament (ITCL), and anterior capsular ligament were measured for the ligament structure. Also, subtalar joint facets were classified into Degeneration (+) and (-) groups according to degeneration of the talus and calcaneus. No significant relationship was identified between the joint structure of the subtalar joint and degeneration of the subtalar articular facet. In contrast, footprint area of the ITCL was significantly higher in the Degeneration (+) group than in the Degeneration (-) group for the subtalar joint facet. These results suggest that the joint structure of the subtalar joint may not affect degeneration of the subtalar articular facet. Degeneration of the subtalar articular facet may be related to the size of the ITCL.
Keywords:
subtalar joint instability
; chronic ankle instability
; footprint osteoarthritis
1. Introduction
Recently, subtalar joint instability has been reported to occur in 10–80% of patients with chronic lateral ankle instability [1], but the problem is very difficult to diagnose [1,2]. Reasons for this include that the subtalar joint comprises anatomically complex structures and subtalar joint instability is similar to chronic ankle instability [2,3]. In a report on a mouse model of combined injury to the talocrural and subtalar joints, cartilage degeneration of the talocrural and subtalar joints was observed at 12 weeks after the ligament was cut, suggesting the possibility of progression to osteoarthritis [4]. Elucidation of detailed anatomical findings is therefore imperative to allow accurate diagnosis and evaluation of subtalar joint instability.
Previous studies have suggested that nerves, articular facets and ligaments, and muscles are involved in foot stability [5]. The anatomy of the subtalar joint involves multiple bony articular facets and ligaments [6]. Furthermore, since no muscles attach to the talus, movement of the talus is considered dependent on the forces applied to the joint [7]. These joint and ligament structures are thus considered to be highly involved in stability of the subtalar joint.
The relationships between joint structure of the subtalar joint facet (morphology of the articular facet, joint congruence, and intersecting angle) and degeneration of the subtalar articular facet have long been investigated. In addition, the presence of degeneration of the subtalar articular facet had been considered to indicate that the joint is unstable [8]. Previous studies using bleached bone have revealed that a two-facet configuration for the morphology of the articular facet of the calcaneus, which involves continuity between the anterior facet (AF) and middle facet (MF) and isolation of the posterior facet (PF), is prone to degeneration of the articular facet [8,9]. In terms of joint congruence, the foot with congruence of the subtalar joint facet of the talus and calcaneus has been considered more stable than the foot with incongruence of the subtalar joint facet of the talus and calcaneus [10]. The intersecting angle is the angle between the AF and MF of the calcaneus. The calcaneus with a two-facet configuration has been reported to show a larger intersecting angle and more frequent degeneration of the subtalar articular facet than that with a three-facet configuration [8,9]. Intersecting angle may therefore also be related to degeneration of the subtalar articular facet [8,9]. However, recent reports on bones with residual soft tissue, including cartilage, have found significant associations between morphology of the articular facet, joint congruence, or intersecting angle and degeneration of the subtalar articular facet [11], and agreement has been lacking among previous studies.
The ligaments involved in the braking of the subtalar joint include the calcaneofibular ligament [12,13], cervical ligament (CL) [14,15], interosseous talocalcaneal ligament (ITCL) [15,16,17], and anterior capsular ligament (ACaL) [15,16,17]. The calcaneofibular ligament is reportedly important in braking the subtalar joint, but the CL, ITCL, and ACaL have not been adequately studied. Jotoku et al. [16] considered that the size of the ligament may reflect mechanical demands on the involved structures. Ligamentous structures may thus be greater in area where the joint is unstable and loaded, but the relationship between joint and ligamentous structures of the subtalar joint and degeneration of the subtalar articular facet remains unclear.
The present study aimed to clarify relationships between joint and ligament structures of the subtalar joint and degeneration of the subtalar articular facet. We hypothesized that the joint structure of the subtalar joint facet is independent of the presence or absence of degeneration of the subtalar articular facet and that ligaments are larger in feet with degeneration of the subtalar articular facet.
2. Materials and Methods
2.1. Cadavers
This investigation examined 50 feet from 25 Japanese fixed cadavers (mean age at death, 79.4 ± 10.8 years; 26 sides from men, 24 sides from women, 25 right sides, 25 left sides) donated to Nippon Dental University School of Life Dentistry at Niigata. All cadavers had been fixed in 10% formalin that was then replaced with alcohol. Inclusion criteria were no history of surgery on the foot or ankle joint. This investigation was conducted with the approval of the Ethics Committee at our institution (approval no. 18867-220720). This study complied with the Declaration of Helsinki and was conducted after informed consent was obtained from all donor families.
2.2. Measurement procedures
The dissection procedure consisted of amputation of the donor foot 10 cm above the ankle joint, followed by dissection of the skin, subcutaneous tissue, inferior extensor retinaculum, and lower leg muscle and tendons from the isolated foot specimen. In addition, to transect the talus at the subtalar joint, ligaments were cut in the following order: calcaneofibular ligament, lateral talocalcaneal ligament, CL, dorsal talonavicular ligament, ACaL, posterior talocalcaneal ligament, deltoid ligament, and ITCL. To disarticulate the calcaneus at the transverse tarsal joint, ligaments were cut in the following order: bifurcated ligament, dorsal calcaneocuboid ligament, plantar calcaneonavicular ligament, short plantar ligament, long plantar ligament, and plantar calcaneocuboid ligament. Based on previous studies [8,11,18,19,20,21], the morphology of articular facets was classified by the number of articular facets in each talus and calcaneus according to the morphology of AF and MF. A morphology in which AF and MF were continuous and PF was isolated was considered a two-facet configuration, and a morphology in which AF, MF, and PF were isolated was considered a three-facet configuration (Figure 1). Joint congruence was evaluated based on whether the number of articular facets of the talus and calcaneus were the same or different, using the classification of articular facets described above [10]. Presence of the same number of articular facets for the talus and calcaneus was considered as congruence, while any difference was taken as incongruence (Figure 2). Intersecting angle was measured by placing a protractor (Stainless Steel Protractor and Angle Finder; General Tools, China) just above the articular facet of the calcaneus and measuring the angle between the AF and MF. Only a single measurement was taken (Figure 3). The footprint area of the ligament attachment was used to evaluate ligament structure. Footprint areas were analyzed for CL, ITCL, and ACaL. These ligaments were carefully exposed from the disarticulated talus and calcaneus, and each ligament was detached from each bone. The detached areas were then colored with a pen to identify the footprint area for each ligament attachment. A three-dimensional (3D) scanner (EinScan Pro HD; SHINING 3D, Hangzhou, China) (specifications from the manufacturer: measurement precision, 0.04 mm) was used to create 3D models of the talus and calcaneus. The 3D model data were transferred to Geomagic Freeform 2021 design software (3D SYSTEMS), and curves were drawn on the boundaries of the footprint area using a pen-type device (Touch; 3D SYSTEMS). Afterward, footprint areas on the talar and calcaneal sides were calculated using Rhinoceros7 3D software (McNeel) (Figure 4). Footprint area was taken as the sum of footprint areas of the talus and calcaneus sides, with one measurement taken for each footprint area of each ligament. Degeneration of the subtalar articular facet of the talus and calcaneus AF, MF, and PF was evaluated with a gross anatomical method based on the classification of Hirose et al. [22]. This method classifies joint facet degeneration into four grades: grade 1, no pathology; grade 2, swelling or fibrillation as a pre-degenerative change; grade 3, fissure or distinct erosion; or grade 4, cartilage defect. In addition, a previous study showed that osteophyte formation is observed in severe joint degeneration [23]. Therefore, in this study, in addition to the aforementioned grades 3 and 4, osteophyte formation was evaluated as a characteristic feature of degeneration of the subtalar articular facet. Feet with degeneration of any of the articular facets of the talus, articular facets of the calcaneus, or degeneration of the talus and calcaneus were assigned to the Degeneration (+) group. Feet without any degeneration of the talus or calcaneus were assigned to the Degeneration (-) group (Figure 5). The number of articular facets, joint congruence, intersecting angle, footprint area, and degeneration of the subtalar articular facet were evaluated and measured by one examiner.
2.3. Reliability of measurements of intersecting angle and footprint area
The reliabilities of intersecting angle and footprint area measurements were examined for 10 feet from 5 Japanese fixed cadavers (mean age at death, 72.8 ± 15.9 years; 3 sides from men, 2 sides from women, 5 right sides, 5 left sides) with no history of ankle or ankle joint surgery. Intersecting angles were measured as described above, and re-measurements were taken on the same day as the first measurement. The footprint area was measured by the method described above, and re-measurements were taken the next day or later.
2.4. Statistical analysis
Statistical analyses were performed using IBM SPSS Statistics Version 28.0 (IBM, NY, USA). The intraclass correlation coefficient (ICC) was used to examine the reliability, and intra-examiner reliability (1,1) was calculated for each intersecting angle and footprint area. Relationships between number of articular facets of the talus, joint congruence, and degeneration of the subtalar articular facet were examined using Fisher's exact test. The relationship between the number of articular facets of the calcaneus and degeneration of the subtalar articular facet was examined using the Chi-square test. After performing the Shapiro–Wilk test and Levene's test on the intersecting angle and footprint area, Welch's t-test was used for the footprint area of the ACaL, and a two-sample t-test was used for the total footprint area of the CL, ITCL, and ACaL in comparisons of the Degeneration (+) and Degeneration (-) groups of the subtalar joint facet. Intersecting angle and footprint areas of CL and ITCL were compared between the Degeneration (+) and Degeneration (-) groups of the subtalar joint facet using the Mann–Whitney U test. The significance level was set at 5%.
3. Results
3.1. Reliability of measurements of intersecting angle and footprint area
ICC (1,1) values for measurement of the intersecting angle and footprint area were 0.989 and 0.975, respectively. According to the criteria of Landis et al. [24], an ICC greater than 0.81 reflects “almost perfect” reliability of the measurement. Therefore, the reliability of measurements of intersecting angle and footprint area in this study were almost perfect.
3.2. Joint and ligament structure and degeneration of the subtalar articular facet
In terms of the number of articular facets of the talus, 76% (38/50) showed a two-facet configuration and 24% (12/50) had a three-facet configuration. Joint congruence was seen in 88% (44/50), with 12% (6/50) incongruent. Mean intersecting angle for the 50 feet was 138.4 ± 8.6° (Table 1). Mean footprint area for the 50 feet was 112.2 ± 43.6 mm2 for CL, 48.4 ± 24.3 mm2 for ITCL, and 48.3 ± 25.1 mm2 for ACaL. Total footprint area of the CL, ITCL, and ACaL was 208.9 ± 68.8 mm2 (Table 2). Degeneration of the subtalar articular facet was seen in 40% of feet (20/50; Degeneration (+) group), with 60% (30/50) in the Degeneration (-) group.
3.3. Relationship between joint and ligament structures and degeneration of the subtalar articular facet
In terms of joint structure, no significant differences were seen in number of articular facets of the talus and calcaneus, joint congruence, or intersecting angle between the Degeneration (+) and Degeneration (-) groups (Table 1). In terms of ligament structure, only footprint area of the ITCL was significantly higher in the Degeneration (+) group compared to the Degeneration (-) group (p = 0.036). No significant group differences between Degeneration (+) and Degeneration (-) groups were seen in footprint areas of the CL ACaL, or total footprint area for the CL, ITCL, and ACaL (Table 2).
4. Discussion
This study examined the relationship between joint and ligament structures of the subtalar joint and degeneration of the subtalar articular facet in Japanese fixed cadavers. To the best of our knowledge, this represents the first study to examine the relationship between joint and ligament structure of the subtalar joint and degeneration of the subtalar articular facet. Two main findings were obtained from this study. First, no significant relationship was apparent between joint structure of the subtalar joint (number of articular facets of the talus and calcaneus, joint congruence, and intersecting angle) and degeneration of the subtalar articular facet. Second, in terms of the ligamentous structure of the subtalar joint, footprint area of the ITCL was significantly higher in the Degeneration (+) group than in the Degeneration (-) group.
The present study did not find any relationship between joint structure of the subtalar joint (number of articular facets of the talus and calcaneus, joint congruence, or intersecting angle) and degeneration of the subtalar articular facet. These results were similar to those described by Kleipool et al. [11], who examined relationships between the number of articular facets, joint congruence, intersecting angle and degeneration of the subtalar articular facet in bone specimens with residual soft tissue. Kleipool et al. [11] also considered that the degeneration of the subtalar articular facet observed in bleached bone may reflect secondary features of degeneration, while bone with remaining soft tissue may allow detection of early-stage degeneration of the articular cartilage. In this study, articular cartilage degeneration and osteophyte formation were analyzed as degeneration of the subtalar articular facet, which may have allowed more comprehensive evaluation than in previous studies. In a review article [25] reporting risk factors for osteoarthritis, systemic factors such as sex, ethnicity, genetics, obesity, diet, bone density and bone mass, and joint-level factors such as bone morphology, muscle strength, joint alignment, occupation, and sports activities, and joint injury were reported as risk factors for osteoarthritis. The degeneration of the subtalar articular facet observed in the present study may thus have been induced by influences other than the joint structure of the subtalar joint.
In the present study, among the ligamentous structures of the subtalar joint, only the footprint area of the ITCL showed significantly higher values in the Degeneration (+) group compared to the Degeneration (-) group for the subtalar joint facet. Previous studies have suggested that the CL, ITCL, and ACaL in the subtalar joint are each important for stability of the subtalar joint [12,15,16]. In addition, the main function of the ITCL has been considered to be connection of the talus and calcaneus and maintenance of the subtalar joint axis [26,27]. Furthermore, Jotoku et al. [16] considered that the size of the ligament may reflect the magnitude of mechanical demands. Therefore, unstable joints would be expected to show the adaptation of ligament structures to the mechanical loading. Based on such considerations, the footprint area of the ITCL may have been larger in the Degeneration (+) group for the subtalar articular facet due to the loading that caused malalignment of the talus and calcaneus.
Several limitations to this study need to be kept in mind. The first is that the lifestyles, medical history, and history of sprains for donors remained unknown. In previous studies, osteoarthritis has been reported to show many risk factors [25]. Thickening of the anterior talofibular ligament has also been shown to occur after a lateral ankle sprain [28]. We therefore cannot rule out the possibility that the lifetime contributions of donor lifestyle, lower extremity alignment, medical history, and history of sprains may have caused changes in ligament structure and degeneration of the subtalar articular facet. Second, we did not include the calcaneofibular ligament or inferior extensor retinaculum in our study. The calcaneofibular ligament and inferior extensor retinaculum have been suggested as potentially important for stability of the subtalar joint [12,29,30]. However, the structure and function of the CL, ITCL, and ACaL in the subtalar joint have not been fully investigated. We therefore prioritized evaluation of the CL, ITCL, and ACaL in this study. Future studies should include the calcaneofibular ligament and inferior extensor retinaculum to evaluate in detail the structures and functions of the subtalar joint. Third, this study was conducted only on Japanese fixed cadavers. In a previous study, the morphology of the subtalar articular facet has been shown to vary markedly between ethnicities [31]. Such differences may have similar effects on ligament structure. The fourth point is that no biomechanical studies were conducted. In the present study, we investigated the relationship between joint and ligament structures of the subtalar joint and degeneration of the subtalar articular facet. Since ancient times, the relationship between morphology of the subtalar articular facet and degeneration of the subtalar articular facet has been reported along with the interpretation that the presence of degeneration of the subtalar articular facet indicates joint instability [8]. The same interpretation was used in the present study. However, the relationship between subtalar joint motion and variations in morphology of the subtalar articular facet, as well as detailed function of the ligaments of the subtalar joint, are not yet clear. Detailed investigations using biomechanical methods are clearly needed.
5. Conclusions
In this study, no significant relationship was identified between joint structure and the presence of degeneration of the subtalar articular facet. In terms of ligament structure, only footprint area of the ITCL was significatly higher in the Degeneration (+) group than in the Degeneration (-) group of the subtalar joint facet. The present results suggest that the joint structure of the subtalar joint may not affect degeneration of the subtalar articular facet. In the ligament structure of the subtalar joint, the footprint area of the ITCL was significantly larger in the group with degeneration of the subtalar joint facet, suggesting that degeneration of the subtalar joint facet may be related to the size of the ITCL. Further studies using biomechanical methods are needed to clarify the relationship between subtalar joint motion and variations in subtalar articular facet morphology, as well as the detailed functions of the ligaments of the subtalar joints.
Author Contributions
R.T. contributed to conceptualization, data and formal analysis, investigation and methodology and writing—original draft; M.E. contributed to conceptualization, funding acquisition, supervision and writing—original draft; M.S. and H.O. contributed to validation and writing—review and editing; H.Y., R.H., C.S., T.I., H.A., Y.Y., and T.T contributed to writing—review and editing of the manuscript; I.K. supervised the study, contributed to writing—original draft of the manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Ethics Committee of Niigata University of Health and Welfare (approval no. 18867-220720).
Informed Consent Statement
Informed consent was obtained from the families of all subjects.
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Acknowledgments
The authors would like to acknowledge and thank those anonymous individuals who generously donated their bodies so that this study could be performed. This study was supported by the Japan Society for the Promotion of Science (JSPS) KAKENHI Grant Number JP22K19739 and a Grant-in-Aid program from Niigata University of Health and Welfare.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Michels, F.; Clockaerts, S.; Van Der Bauwhede, J.; Stockmans, F.; Matricali, G. Does subtalar instability really exist? A systematic review. Foot Ankle Surg 2020, 26, 119–127. [CrossRef]
- Pereira BS, Andrade R, Espregueira-Mendes J, Marano RPC, Oliva XM, Karlsson J: Current concepts on subtalar instability. Orthopaedic Journal of Sports Medicine, 9: 23259671211021352, 2021. [CrossRef]
- Aynardi M, Pedowitz DI, Raikin SM: Subtalar instability. Foot and Ankle Clinics, 20: 243-252, 2015. [CrossRef]
- Liu P, Chen K, Wang S, Hua C, Zhang H, Yu J: A mouse model of ankle-subtalar joint complex instability induced post-traumatic osteoarthritis. J Orthop Surg Res, 16: 541, 2021. [CrossRef]
- McKeon PO, Hertel J, Bramble D, Davis I: The foot core system: a new paradigm for understanding intrinsic foot muscle function. Br J Sports Med, 49: 290, 2015. [CrossRef]
- Budny A: Subtalar joint instability: current clinical concepts. Clinics in Podiatric Medicine and Surgery, 21: 449-460, 2004. [CrossRef]
- Stagni R, Leardini A, O'Connor JJ, Giannini S: Role of passive structures in the mobility and stability of the human subtalar joint: a literature review. Foot & Ankle International, 24: 402-409, 2003. [CrossRef]
- Drayer-Verhagen F: Arthritis of the subtalar joint associated with sustentaculum tali facet configuration. J Anat, 183 (Pt 3): 631-634, 1993.
- Madhavi C, Madhuri V, George VM, Antonisamy B: South Indian calcaneal talar facet configurations and osteoarthritic changes. Clin Anat, 21: 581-586, 2008. [CrossRef]
- Badalahu, Qin B, Luo J, Zeng Y, Fu S, Zhang L: Classification of the subtalar articular surface and its matching situation: an anatomical study on Chinese subtalar joint. Surg Radiol Anat, 42: 1133-1139, 2020. [CrossRef]
- Kleipool RP, Vuurberg G, Stufkens SAS, van der Merwe AE, Oostra R-J: Bilateral symmetry of the subtalar joint facets and the relationship between the morphology and osteoarthritic changes. Clinical Anatomy, 33: 997-1006, 2020. [CrossRef]
- Pellegrini MJ, Glisson RR, Wurm M, Ousema PH, Romash MM, Nunley JA, 2nd, Easley ME: Systematic quantification of stabilizing effects of subtalar joint soft-tissue constraints in a novel cadaveric model. J Bone Joint Surg Am, 98: 842-848, 2016. [CrossRef]
- Li L, Gollhofer A, Lohrer H, Dorn-Lange N, Bonsignore G, Gehring D: Function of ankle ligaments for subtalar and talocrural joint stability during an inversion movement – an in vitro study. Journal of Foot and Ankle Research, 12: 16, 2019. [CrossRef]
- Edama M, Takabayashi T, Inai T, Hirabayashi R, Ikezu M, Kaneko F, Matsuzawa K, Kageyama I: Morphological features of the cervical ligament. Surg Radiol Anat, 42: 215-218, 2020. [CrossRef]
- Michels F, Matricali G, Vereecke E, Dewilde M, Vanrietvelde F, Stockmans F: The intrinsic subtalar ligaments have a consistent presence, location and morphology. Foot Ankle Surg, 27: 101-109, 2021.
- Jotoku T, Kinoshita M, Okuda R, Abe M: Anatomy of ligamentous structures in the tarsal sinus and canal. Foot Ankle Int, 27: 533-538, 2006. [CrossRef]
- Li SY, Hou ZD, Zhang P, Li HL, Ding ZH, Liu YJ: Ligament structures in the tarsal sinus and canal. Foot Ankle Int, 34: 1729-1736, 2013. [CrossRef]
- Jung M-H, Choi BY, Lee JY, Han CS, Lee JS, Yang YC, Cho BP: Types of subtalar joint facets. Surgical and Radiologic Anatomy, 37: 629-638, 2015. [CrossRef]
- Bruckner J: Variations in the human subtalar joint. J Orthop Sports Phys Ther, 8: 489-494, 1987. [CrossRef]
- Nozaki S, Watanabe K, Katayose M: Three-dimensional morphometric analysis of the talus: implication for variations in kinematics of the subtalar joint. Surgical and Radiologic Anatomy, 39: 1097-1106, 2017. [CrossRef]
- Cho H-J, Kwak D-S, Kim I-B: Analysis of movement axes of the ankle and subtalar joints: Relationship with the articular surfaces of the talus. Proceedings of the Institution of Mechanical Engineers, Part H: Journal of Engineering in Medicine, 228: 1053-1058, 2014. [CrossRef]
- Hirose K, Murakami G, Kura H, Tokita F, Ishii S: Cartilage degeneration in talocrural and talocalcaneal joints from Japanese cadaveric donors. J Orthop Sci, 4: 273-285, 1999. [CrossRef]
- Kellgren JH, Lawrence JS: Radiological assessment of osteo-arthrosis. Ann Rheum Dis, 16: 494-502, 1957. [CrossRef]
- Landis JR, Koch GG: The measurement of observer agreement for categorical data. Biometrics, 33: 159-174, 1977. [CrossRef]
- Vina ER, Kwoh CK: Epidemiology of osteoarthritis: literature update. Curr Opin Rheumatol, 30: 160-167, 2018. [CrossRef]
- Tochigi Y, Amendola A, Rudert MJ, Baer TE, Brown TD, Hillis SL, Saltzman CL: The role of the interosseous talocalcaneal ligament in subtalar joint stability. Foot & Ankle International, 25: 588-596, 2004. [CrossRef]
- Tochigi Y, Takahashi K, Yamagata M, Tamaki T: Influence of the interosseous talocalcaneal ligament injury on stability of the ankle-subtalar joint complex — a cadaveric experimental study. Foot & Ankle International, 21: 486-491, 2000. [CrossRef]
- Liu K, Gustavsen G, Royer T, Wikstrom EA, Glutting J, Kaminski TW: Increased ligament thickness in previously sprained ankles as measured by musculoskeletal ultrasound. J Athl Train, 50: 193-198, 2015. [CrossRef]
- Stephens MM, Sammarco GJ: The stabilizing role of the lateral ligament complex around the ankle and subtalar joints. Foot Ankle, 13: 130-136, 1992. [CrossRef]
- Weindel S, Schmidt R, Rammelt S, Claes L, Campe Av, Rein S: Subtalar instability: a biomechanical cadaver study. Archives of Orthopaedic and Trauma Surgery, 130: 313-319, 2010. [CrossRef]
- Bunning PS, Barnett CH: A comparison of adult and foetal talocalcaneal articulations. J Anat, 99: 71-76, 1965.
Figure 1.
Procedure for classifying the number of subtalar articular facets. (a, c) Plantar view of the right talus (b, d) Dorsal view of the right calcaneus. M: medial side; L: lateral side. A morphology in which the anterior facet (AF) and middle facet (MF) are continuous, and the posterior facet (PF) is isolated is considered as a two-facet configuration. A morphology in which AF, MF, and PF are all isolated is considered as a three-facet configuration.
Figure 1.
Procedure for classifying the number of subtalar articular facets. (a, c) Plantar view of the right talus (b, d) Dorsal view of the right calcaneus. M: medial side; L: lateral side. A morphology in which the anterior facet (AF) and middle facet (MF) are continuous, and the posterior facet (PF) is isolated is considered as a two-facet configuration. A morphology in which AF, MF, and PF are all isolated is considered as a three-facet configuration.
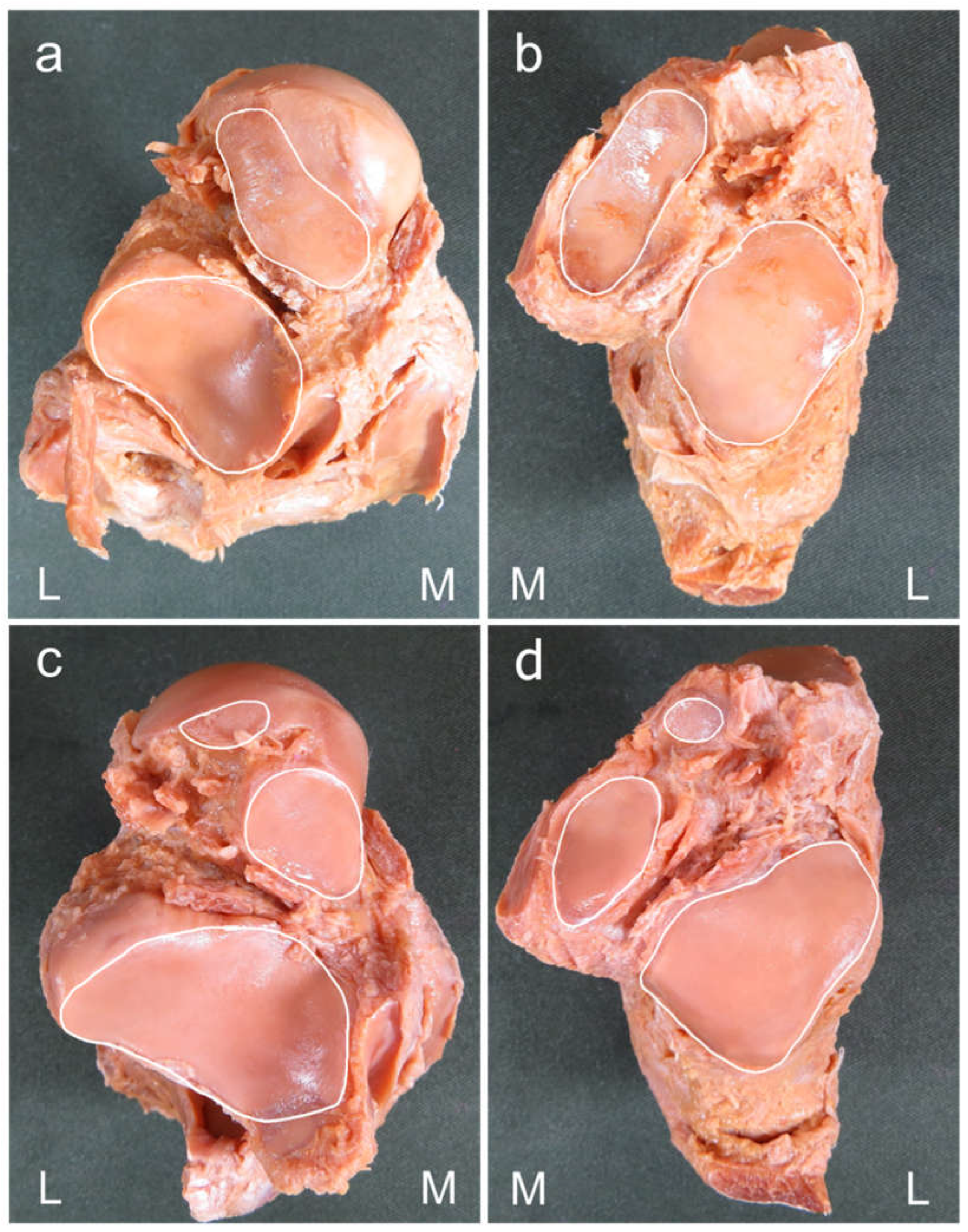
Figure 2.
Procedure for assessing joint congruence (a, c) Plantar aspect of the right talus; (b, d) Dorsal aspect of the right calcaneus. Joint congruence was evaluated based on whether the number of articular facets of the talus and calcaneus were the same or different based on the classification of the number of the articular facets. The same number of articular facets for both talus and calcaneus was considered to represent congruence (a, b) and a different number represented incongruence (c, d).
Figure 2.
Procedure for assessing joint congruence (a, c) Plantar aspect of the right talus; (b, d) Dorsal aspect of the right calcaneus. Joint congruence was evaluated based on whether the number of articular facets of the talus and calcaneus were the same or different based on the classification of the number of the articular facets. The same number of articular facets for both talus and calcaneus was considered to represent congruence (a, b) and a different number represented incongruence (c, d).
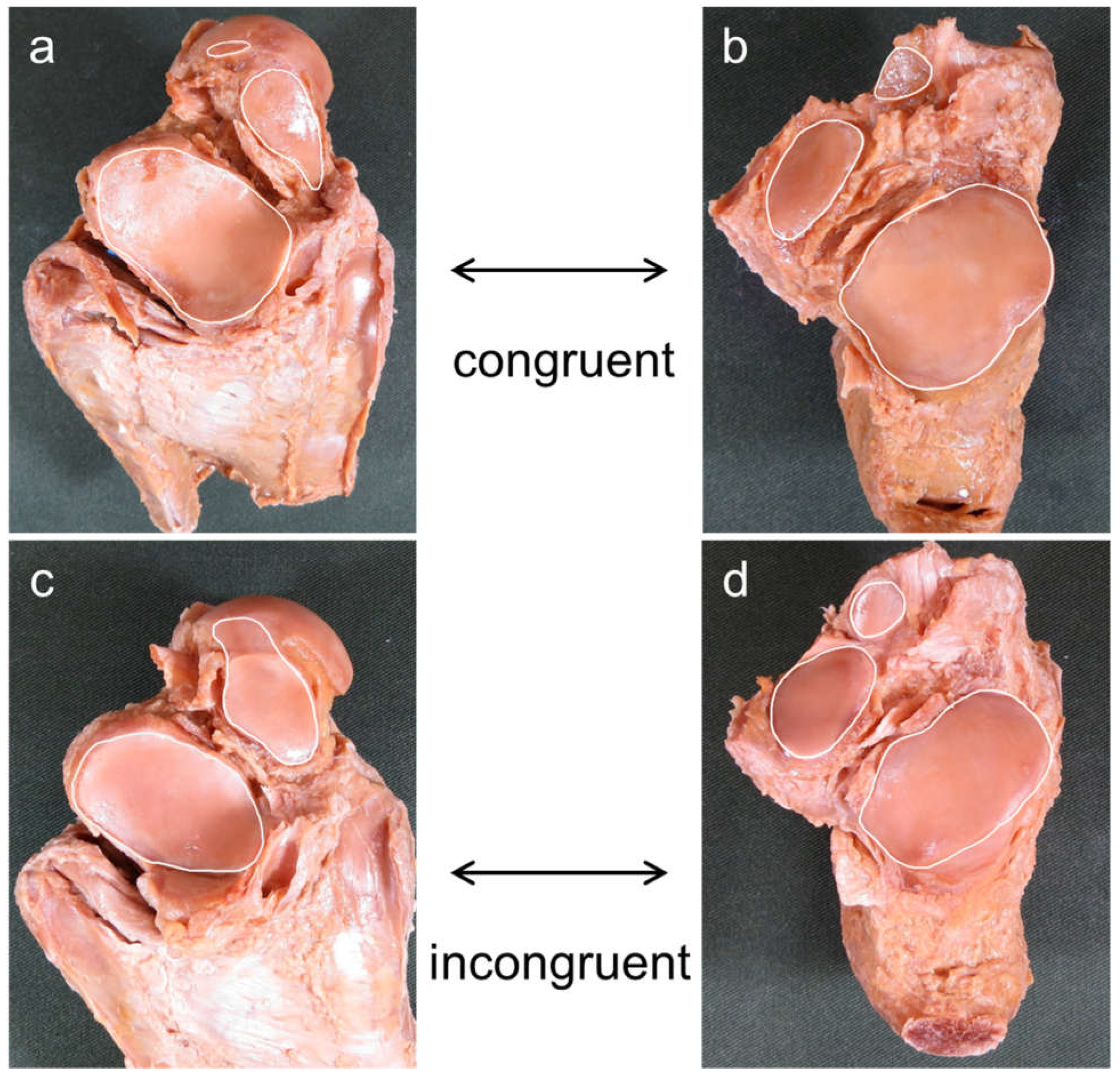
Figure 3.
Procedure for measuring the intersecting angle. (a) Dorsal view of the right calcaneus; (b) Anteromedial view of the right calcaneus. The intersecting angle was measured by placing the protractor just above the articular facet of the calcaneus and measuring the angle between the AF and MF.
Figure 3.
Procedure for measuring the intersecting angle. (a) Dorsal view of the right calcaneus; (b) Anteromedial view of the right calcaneus. The intersecting angle was measured by placing the protractor just above the articular facet of the calcaneus and measuring the angle between the AF and MF.
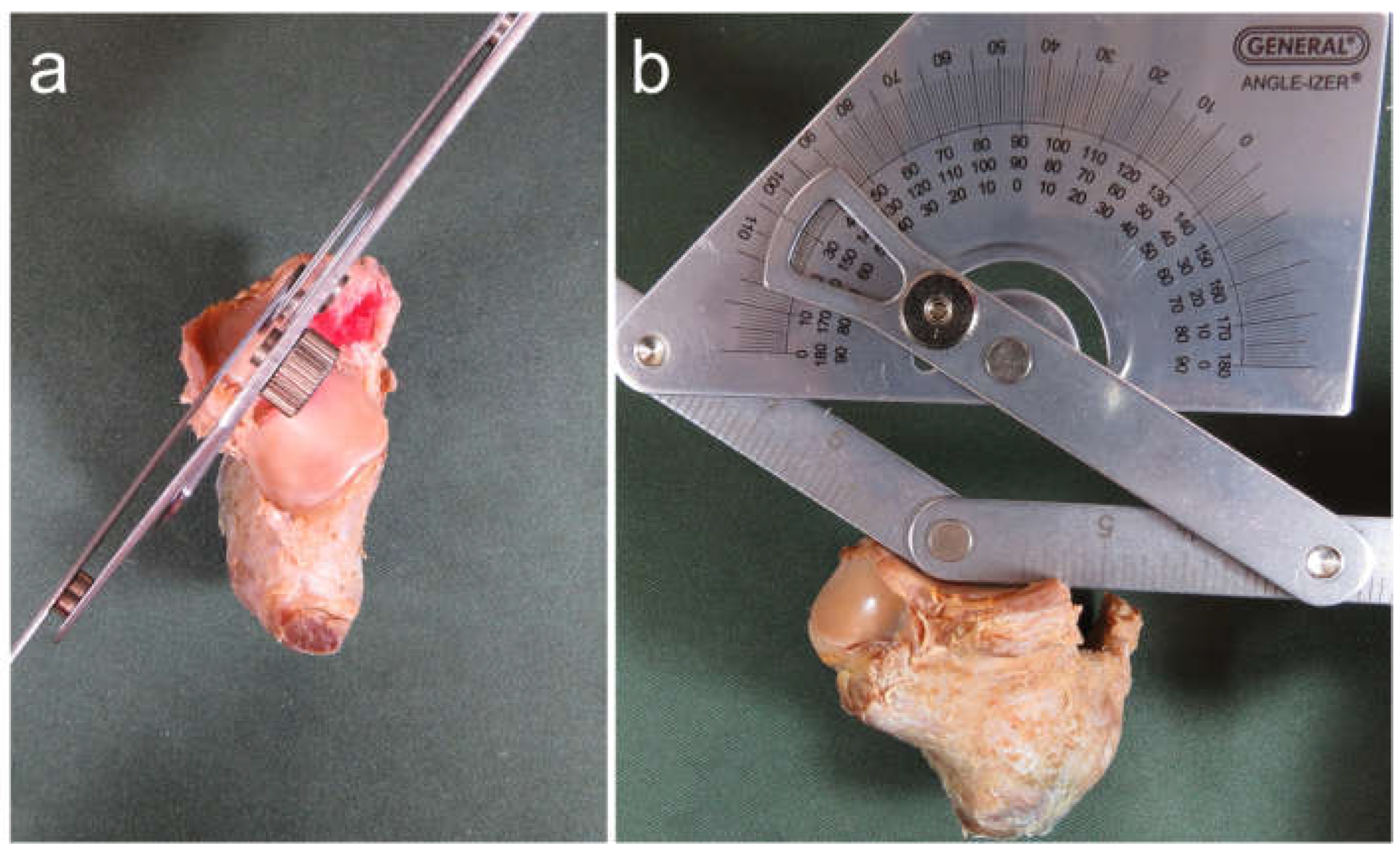
Figure 4.
Procedure for measuring footprint area (a) Site of attachment of the cervical ligament, interosseous talocalcaneal ligament, and anterior capsular ligament: right foot, dorsal view; (b) After detaching ligaments from bones, detached areas were colored with a pen to identify the footprint for each ligamentous attachment; (c) A three-dimensional (3D) scanner was used to create 3D models of the talus and calcaneus; (d) A curve was drawn on the boundaries of the footprint using a pen-type device; (e) Footprint area was then calculated using Rhinoceros7 3D software.
Figure 4.
Procedure for measuring footprint area (a) Site of attachment of the cervical ligament, interosseous talocalcaneal ligament, and anterior capsular ligament: right foot, dorsal view; (b) After detaching ligaments from bones, detached areas were colored with a pen to identify the footprint for each ligamentous attachment; (c) A three-dimensional (3D) scanner was used to create 3D models of the talus and calcaneus; (d) A curve was drawn on the boundaries of the footprint using a pen-type device; (e) Footprint area was then calculated using Rhinoceros7 3D software.
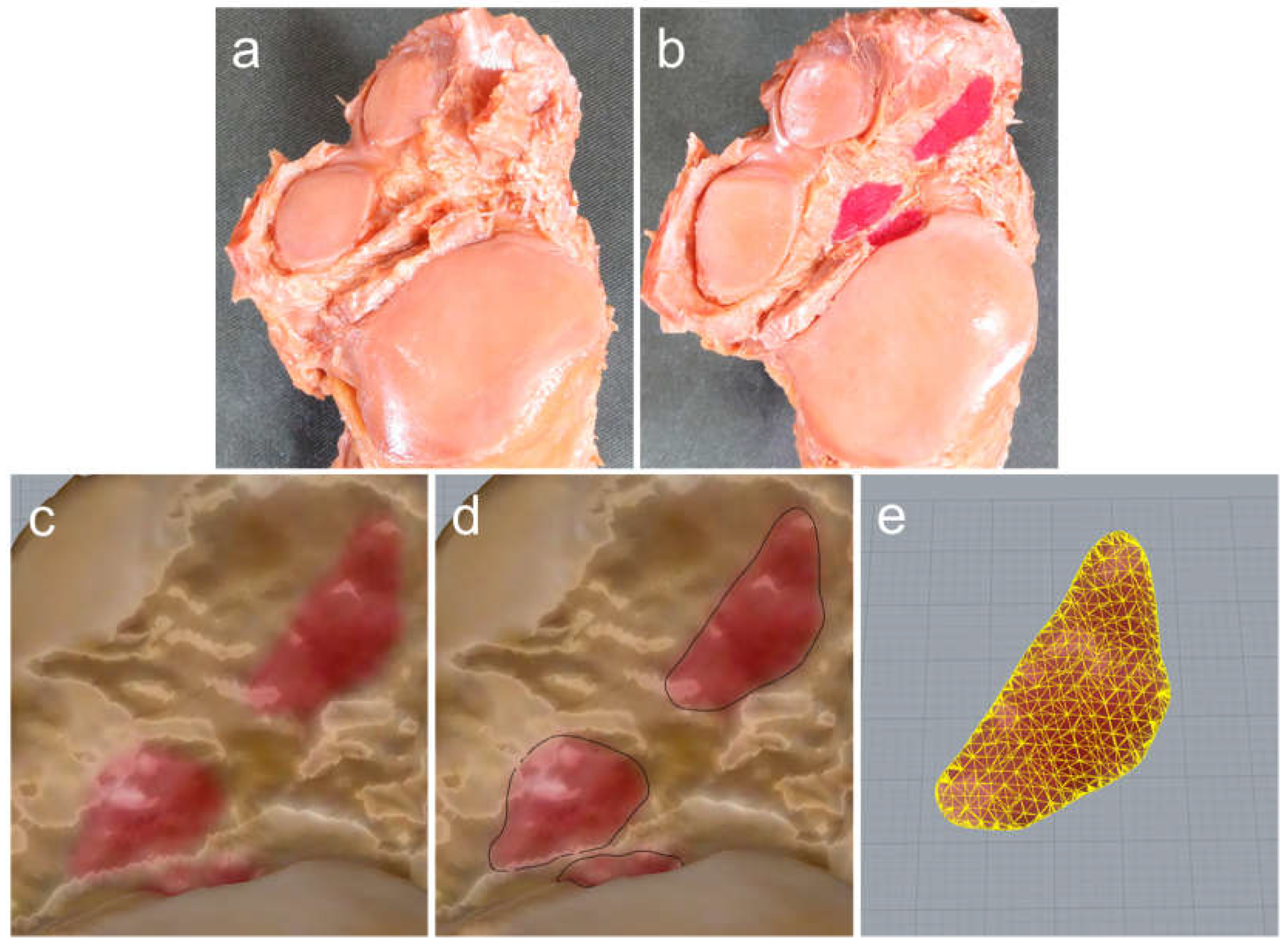
Figure 5.
Procedure for assessing degeneration of the subtalar articular facet (a, c) Plantar view of the right talus; (b, d) Dorsal view of the calcaneus. Arrow: Areas showing degeneration of the subtalar articular facet. M: medial side; L: lateral side. Joints showing degeneration of any of articular facets of the talus, calcaneus, or both were assigned to the Degeneration (+) group. Joints with no degeneration of the talus or calcaneus were assigned to the Degradation (-) group.
Figure 5.
Procedure for assessing degeneration of the subtalar articular facet (a, c) Plantar view of the right talus; (b, d) Dorsal view of the calcaneus. Arrow: Areas showing degeneration of the subtalar articular facet. M: medial side; L: lateral side. Joints showing degeneration of any of articular facets of the talus, calcaneus, or both were assigned to the Degeneration (+) group. Joints with no degeneration of the talus or calcaneus were assigned to the Degradation (-) group.
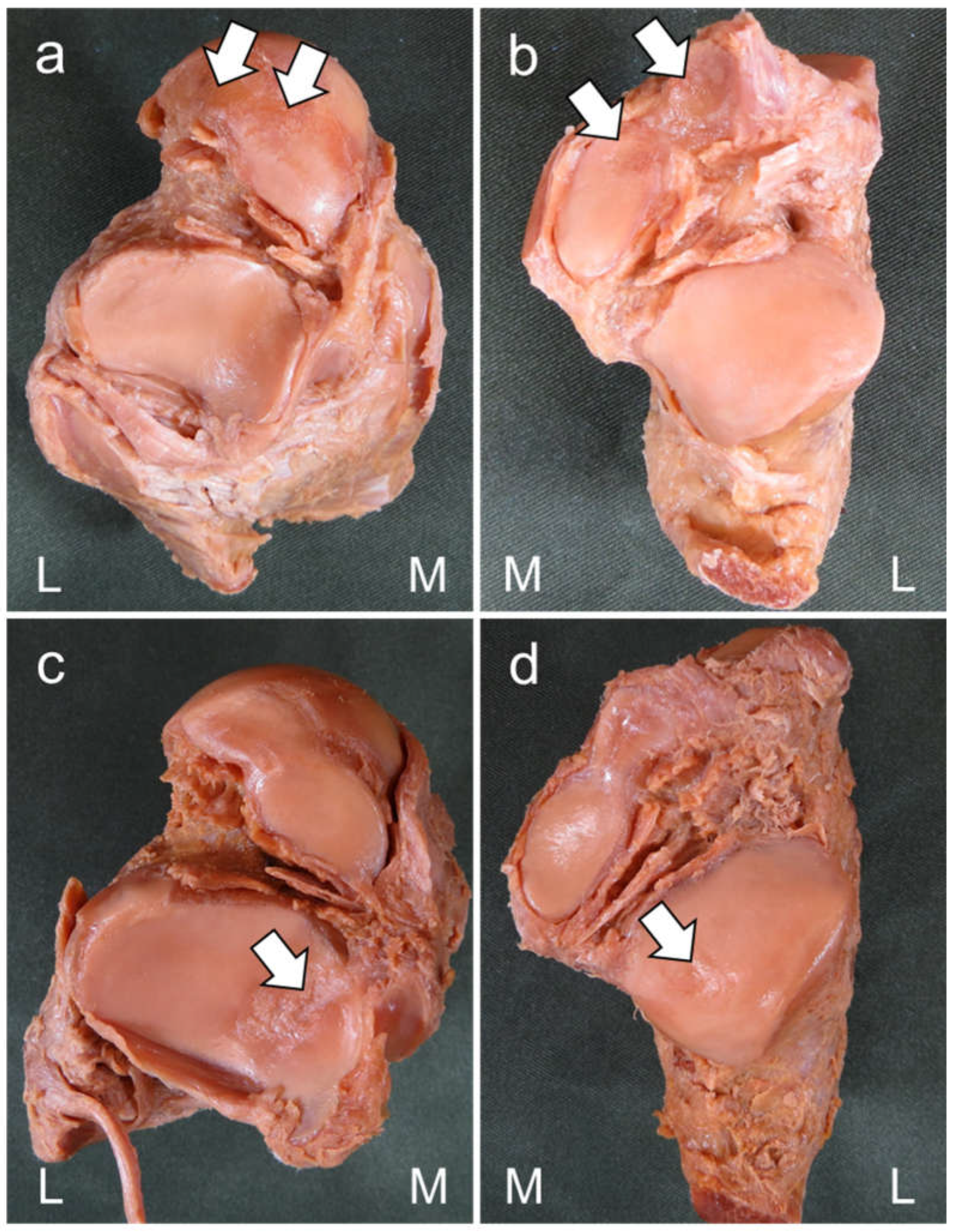

Table 1.
Relationship between joint structure of the subtalar joint and degeneration of the subtalar articular facet.
Table 1.
Relationship between joint structure of the subtalar joint and degeneration of the subtalar articular facet.
| Degeneration | |||
| (+) | (-) | Total | |
| Number of joint facets (n) | |||
| Talar two-facet configuration | 17 | 21 | 38 |
| Talar three-facet configuration | 3 | 9 | 12 |
| Calcaneal two-facet configuration | 15 | 17 | 32 |
| Calcaneal three-facet configuration | 5 | 13 | 18 |
| Joint congruence (n) | |||
| Congruent | 18 | 26 | 44 |
| Incongruent | 2 | 4 | 6 |
| Intersecting angle (°) | 137.8 ± 6.7 | 138.7 ± 9.7 | 138.4 ± 8.6 |
- Congruent: Specimens with the same number of articular facets for both talus and calcaneus.
- Incongruent: Specimens with a different number of articular facets for the talus and calcaneus.
- Degeneration (+): Specimen with degeneration of the subtalar articular facet.
- Degeneration (-): Specimens without degeneration of the subtalar articular facet.
Table 2.
Relationship between ligament structure of the subtalar joint and degeneration of the subtalar articular facet.
Table 2.
Relationship between ligament structure of the subtalar joint and degeneration of the subtalar articular facet.
| Degeneration | |||
| (+) | (-) | Total | |
| Footprint area (mm2) | |||
| CL | 110.1 ± 46.0 | 113.6 ± 42.8 | 112.2 ± 43.6 |
| ITCL | 55.0 ± 21.1 | 44.1 ± 25.7 * | 48.4 ± 24.3 |
| ACaL | 44.9 ± 17.9 | 50.5 ± 29.1 | 48.3 ± 25.1 |
| Total footprint of CL, ITCL, ACaL | 210.0 ± 61.8 | 208.2 ± 74.2 | 208.9 ± 68.8 |
- Values are given as mean ± standard deviation. CL: cervical ligament; ITCL: interosseous talocalcaneal ligament; ACaL: anterior capsular ligament.
- Degeneration (+): Specimen with degeneration of the subtalar articular facet.
- Degeneration (-): Specimen without degeneration of the subtalar articular facet.
- *p = 0.036 vs. Degeneration (+) for the subtalar articular facet.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



