Submitted:
31 December 2022
Posted:
04 January 2023
You are already at the latest version
Abstract
Staphylococci sp. have become the primary pathogens implicated in infective endocarditis, especially within high-income nations. Coupled with the increasing burden of healthcare with aging populations and the protracted course the infections may take, these infections contribute to a significant challenge for healthcare. A systematic review was conducted using relevant search criteria from PubMed, Ovid’s version of MEDLINE, and EMBASE, and data were tabulated from randomized controlled trials (RCT), observational cohort studies, meta-analysis, and basic research articles. The review was registered with the OSF register of systematic reviews and followed the PRISMA reporting guidelines. 35 studies met the inclusion criteria and were included in the final systematic review. The role of Staphylococcus aureus and its interaction with the protective shield and host protection functions is identified and highlighted in several studies. The interaction between infective endocarditis pathogens, vascular endothelium, and blood constituents is also explored giving rise to the potential use of antiplatelets as preventative and/or curative agents. Several factors allow Staphylococcus aureus infections to proliferate within the host with numerous promoting and perpetuating agents. The complex interaction with the hosts' innate immunity also potentiates its virulence. Ameliorating these molecular pathways may serve as a therapeutic avenue for the prevention and treatment of these infections in the near future.
Keywords:
infective endocarditis
; staphylococcus aureus infection
; staphylococcus aureus immunity
; staphylococcus aureus cytotoxin
; biofilm resistance
1. Introduction
In many high-income countries, virulent staphylococci have become the primary pathogens in infective endocarditis (IE) and have overtaken the penicillin-sensitive streptococci. [1,2,3]. Similarly, the subjects at risk of contracting an IE by staphylococcus bacteremia have increased the burden on healthcare facilities, and tackling this infection represents one of the paramount challenges to infection in the 21st century [4,5,6]. This concern is related to the biomolecular characteristics of Staphylococcus aureus infection, which often has increased resistance to many antibiotics, constituting a major conundrum in modern health care [7,8,9]. Staphylococcus aureus interacts with the host’s innate immunity, playing a pivotal role in sustaining and maintaining the infectious state. The pathogen generates a protective shield that interferes with the host's protective mechanisms by means of two coagulases, von Willebrand factor binding protein (vWFbp) and Coagulase (Coa), leading to its critical virulence [10,11,12,13,14,15]. These proteins constitute a functionally intricate structure that S. aureus utilizes to form a protective shield formed of fibrinogen/fibrin surrounding the pathogen and conferring the ability to generate large vegetations. A substantial concern for staphylococcal infection is related to the specific characteristics of these vegetations. These may be large, mobile, and very frequently located in the mitral valve that has been linked with a notable augmentation of risk of symptomatic embolic events [16,17,18,19]. Although in 50% of patients, embolic events occur subtly and asymptomatically, up to 80% of patients’ systematic magnetic resonance imaging (MRI) of the brain may highlight cerebral injuries, [20,21,22]. The former condition may generate mycotic aneurysm lesions resulting from a septic arterial embolism that has migrated to the intraluminal space or vasa vasorum, followed then by the spread of infection through the vessel wall. The mycotic aneurysm was recorded in 5% of IE older patients with weak contrast immunity to S. aureus infection. Recently the detection of lesions are more frequently recorded through the increasing use of advanced imaging methods [24,25,26].
2. Methods
2.1. Search Strategy
In October 2022, PubMed, Ovid’s version of MEDLINE, and EMBASE the systematic review has been designed, and the database was investigated using the terms “Staphylococcus Aureus Infection (9.716 to the present)” “Staphylococcus aureus immunity (1.102 to the present)” “Staphylococcus aureus cytotoxin (300 to the present)” “Staphylococcus aureus coagulation (455 to the present)” and “Staphylococcus aureus biofilm (884 to the present)”. The search was directed to the identification of data from randomized controlled trials (RCT), observational cohort studies, meta-analysis and basic research articles. The review was registered with the OSF register of systematic reviews and followed the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) reporting guidelines. A DOI is available for the project online (https://osf.io/mnu9s)
2.2. Study Selection and Data Extraction
Searches retrieved 11, 573 relevant abstracts, and after deduplication 4 722 relevant citations were screened by 2 reviewers on their own (F.N, SSAS). Inconsistency was resolved by the first author who performed the conceptualization (F.N). The predefined inclusion criteria guided the review of titles and abstracts. The articles included were in English and were very impressive research articles based on the of infective endocarditis, S aureus. infection, S aureus immunity-related mechanisms, S aureus cytotoxin function, and pathophysiology and biofilm resistance to staphylococcus aureus infection. Relevant animal studies were included because they were of higher impact on the emerged role of S aureus as a causative pathogen in supporting infection and related interaction with immune response and coagulation process. Case reports, conference presentations, editorials, and expert opinions were excluded. A total of 280 citations were evaluated of which 40 studies met inclusion criteria and were included in the final systematic review. In Figure 1 is reported PRISMA Flowchart. PRISMA 2020 checklist in supplementary material
2.3. Endpoints and Effect Summary
The endpoints evaluated the effects of the emerging role of Staphylococcus aureus immunity, conferring particular attention to host innate immunity, immune modulation, B-cell vs T-cell cooperation, as well as immune response and vaccine. We also investigated new evidence from the infectious array of Staphylococcus aureus focusing on the involvement of the protective shield and host protection functions, the interaction between infective endocarditis pathogens, vascular endothelium, and blood constituents. Again, the role of biofilm formation has been discussed. Included studies that meet inclusion criteria and reported are reported in Table 1, Table 2 and Table 3.
3. Results
80–90% of infective endocarditis is caused by the gram-positive cocci of the staphylococcus, streptococcus, and enterococcus species. Among these causative bacteria, S aureus is the most frequently isolated pathogen associated with IE in high-income countries reaching up to 30% of cases of infection [1,2,3,4,5,6,27,28,29]. The family of coagulase-negative staphylococci, including Staphylococcus epidermidis, Staphylococcus lugdunensis, and Staphylococcus capitis, stands out as far-reaching skin commensals. Coagulase-negative staphylococci have specific characteristics involving frequent colonization of indwelling lines, CIEDs; Again, they are the most common causative bacteria discovered in patients suffering from early prosthetic valvular endocarditis [30,31,32,33,34]. These pathogens are often accountable as the cause of hospital-acquired native valvular endocarditis. [35,36,37] Furthermore, coagulase-negative staphylococci express the worrying function of generating biofilms that can lead to high rates of abscess formation and multi-antibiotic resistance [36]. Given the specificity of the immune response to infection and the ability to develop a marked resistance to antibiotics, IE caused by staphylococcal outbreaks affects particular populations of individuals. Included in the at-risk cohorts are hemodialysis patients and intravenous drug users and others who may become infected from native valves, prostheses, and cardiac implantable electronic devices (CIEDs) [38,39,40,41,42,43]. Staphylococcus cocci have a deep-seated propensity to acquire antibiotic resistance, thus methicillin-resistant strains have emerged and are a serious concern worldwide. [2,44,45]
3.1. Staphylococcus aureus immunity
In the immune response induced by external agents, in the absence of cardiac pathology, the endothelium of the heart is not subject to recurrent bacteremia. However, the latter can be induced by common daily activities, the most frequently represented by chewing and brushing the teeth. [46] Bacterial fastening to the tissue constitutes one of the crucial steps in the pathophysiological process of infective endocarditis. Once the endothelial injury is initiated, bacterial adhesion is promoted through two main steps. Initially, the release of inflammatory cytokines associated with tissue factors is recorded while in the second time the expression of fibronectin, which leads to the formation of a thrombus composed of platelets and fibrin occurs [47,48,49]. Common causative pathogens implicated in the development of ED can colonize heart valves either with pre-existing sterile vegetations or in the presence of minimal endothelial lesions. The intervening inflammatory response induces the production of cytokines, integrins, and tissue factors, which in turn attract monocytes and platelets. The associated production of fibronectin occurs due to the effect induced by chemokines. The crucial action of the chemokines allows the bacteria to adhere further favoring the activation of the inflammatory cascade which offers, through the incorporation of the bacteria, an anomalous protection mechanism by the host defenses. [48,49]. Figure 2
The pathoanatomy of IE is characterized by three substantial harmful factors that are addressed towards the endothelium: the direct activity of the bacterial pathogen, valvular sclerosis, and/or rheumatic valvulitis. The former is markedly caused by the interaction of Staphylococcus aureus in the infectious field. [50].
The pathophysiological and clinical assessments of IE, involving heterogeneous cohorts of subjects, allowed to range from individuals treated successfully without experiencing adverse events, to subjects who instead showed serious complications up to a high mortality event. As there has been a change in the temporal trend in the pattern of IE in high-income countries over the past 5 decades, the study of pathophysiology and clinics has involved increasingly aging subjects. These contract IE with increasing incidence of Staphylococcus aureus as the causative bacterium and often the infection develops in the health care setting. From this, physicians have acquired a greater understanding of the mechanisms that support the formation, growth, and embolization of vegetation that occur on damaged or inflamed heart valves on cardiac devices. A better understanding of these mechanisms has led to greater knowledge of how to tackle the growing problem of antimicrobial resistance.
From a pathophysiological point of view, two mechanisms causing IE have been shown to play a substantial role in its treatment: the immune response in elderly patients with IE and the new transcatheter valve implantation-based procedure for the disease of the aortic valve, the mechanisms that trigger septic shock. The latter leads to a substantially increased risk of death in patients with IE [51,52,53,54,55].
3.1.1. Staphylococcus aureus and host innate immunity
The peculiar characteristic of virulence of S aureus is due to the presence of virulence factors both on the surface of the bacterium and by their secretory molecules, which once activated offer a high capacity to counteract the host's immune defense mechanisms [56,57]. S. aureus has a crucial virulence program, the Accessory Gene Regulatory System (Agr), which works for the quorum detection of pathogens. Our knowledge supports that Agr works on the control of the expression of phenol-soluble modulins (PSM) which are active against immune cells and keratinocytes (KC). However, it has not yet been demonstrated how this mechanism can be triggered at the right moment [58]. The innate immune response supports a response by dead KCs, which generate a physical barrier that depends on the release of antimicrobial peptides such as human β-defensins 2 and 3, cathelicidins, and RNAse 7 and also favoring a bacteriostatic action against S aureus infection. It has been suggested that the antibacterial role of KCs is also mediated by pattern recognition receptors (PRRs) such as toll-like receptors (TLRs) and nucleotide-binding oligomerization domain (NOD) proteins. Molecular patterns associated with invading pathogens (PAMPs) are recorded in these two surveillance systems, thus promoting timely defense against S. aureus. [59,60] The innate immune response is also supported by the action of other cells such as dendritic cells, B and T cells, macrophages, mast cells, natural killer (NK) cells, plasma cells and fibroblasts located in the dermis [61,62].
It has been shown that S aureus infection is crucially promoted by a number of mechanisms by which the violation of innate immune system triggers is established. Two other stages have also been observed to fuel the infection of the pathogen, by entering the bloodstream and spreading into the host tissue once it has left the bloodstream. These two phases are closely related to the function of specific molecules expressed by S Aureus which interact with the endothelium, the blood, and the extracellular matrix. With a well-defined role, FnBPA and FnBPB bind fibronectin and interact with α5β1 integrin on the surface of the vascular endothelium, thereby triggering cell invasion and transmigration. Subsequently, the wall teichoic acid (WTA) and lipoteichoic acid (LTA) of S aureus, polymers that characterize the bacterial envelope, work to favor the staphylococcal invasion of the host cells. In the second phase, during S aureus infection the formation of fibrin thrombi is promoted, through the activation of the agglutination process mediated by Coa/vWbp and ClfA and binds to von Willebrand factor (vWF) on endothelial surfaces, generating the formation of polymers such as vWF Ultra Large (ULVWF). In the third phase, the secretion of Hla by S. Aureus can be observed. Hla is a toxin that interacts with the ADAM10 receptor favoring the cessation of the physiological barrier functions of the endothelial vascular system. Finally, the Trojan horse model is triggered, whereby neutrophils containing intracellularly incorporated S. aureus for phagocytosis lose their ability to deliver bacteria into host tissues [10,11,12,13,14,63].
3.1.2. Staphylo-cytotoxins: A Trojan horse for excellent immune modulating.
Since S Aureus targets a wide variety of immune cells during infection, the pathogen's release of cytotoxins is crucial. It releases leukocidins, hemolysins, and PSM. Leukocidins include leukotoxins such as LukED and LukAB, gamma hemolysin which comprises of HlgAB and HlgCB, and Panton-Valentine Leukocidin (PVL). Three independent studies have clearly described the role played by leukotoxins [64,65,66]. Malachova et al [64] suggested that LukAB was effective only on human polymorphonuclear leukocytes (PMNs) and can kill dendritic cells, monocytes and macrophages. This evidence was corroborated by Alonzo et al [65,66] who demonstrated that LukED recognizes C-C chemokine receptor 5 expressed on the cell resulting in the killing of dendritic cells, macrophages, and lymphocytes.
Likewise, at the micromolar level, a substantial role is offered by the intervention of PSM and alpha-hemolysin (Hla). The latter operates with a noticeable ability to kill neutrophils after phagocytosis. [67] Furthermore, it can modulate the action of disintegrin A and metalloprotease 1 (ADAM1) thus promoting the killing process of monocytes, macrophages, neutrophils, and T cells [68]. A substantial role is offered by cytotoxins that serve functionally as a Trojan horse to promote the spread of S aureus, which is separate from the role offered by S Aureus in evading the host's immune response. Cytotoxins govern by significantly dampening both the innate and adaptive immune responses, allowing protection of S aureus during its movement in the host [69].
3.1.3. Inconsistent cooperation between B and T lymphocytes due to cumulative effects of B lymphocyte deletion. Lack of help from T lymphocytes exacerbates infection
The mechanism by which Staphylococcus aureus evades host immune surveillance is mediated by the protein suppressor of phytochrome A-105 (SpA proteins), which are integrated into the wall structure of the S aureus. These molecules are released during the growth of the pathogen. Silverman et al [70] demonstrated the presence of five domains in the SpA, which are involved with the binding of immunoglobulins. The five immunoglobulin-binding domains bind to the IgG Fcγ domain and the Fab domain of the VH3 IgG and IgM clan. This activity is driven by the cross-links of the B-cell receptors which lead to the polyclonal proliferation of the B cells thus favoring the activity of the superantigen SpA. It is important to underline that during the different steps of the infection, a different growth response was observed arousing a varying expression of SpA. This event leads to the secretion of the Hla toxin which activates specific B lymphocytes located in sites distant from the S aureus. The described phenomenon is the immunological explanation for which humans generally generate antibodies against Hla despite most of the expressed SpA strains. Another important point to consider is related to the fact that the Hla release function is also mediated from the cell wall of the pathogen [70].
The superantigenic activity exerted by SpA proteins can exert an effect at a distance from the site of infection providing a crucial point for vaccine development. A specific effect of SpA proteins that evade recognition by B cells has been suggested by promoting a state called "lethargy" - a normal initial response to antigen. In this case, the B lymphocytes may not pick up a secondary signal to support their activation leading to a state of shock called "anergy". Anergy is a process that occurs in the colonization of S. aureus, in the persistence of its infection, and in the weakening of the defensive protection of T lymphocytes, caused by an impairment of their recruitment by superantigens and cytotoxins which leads to a reduced affinity for antibodies [71,72]. Figure 3
3.1.4. Immuno-Response and Vaccine
The development of a vaccine against staphylococcus aureus is a crucial challenge that would allow the emergence of antibiotic-resistant strains to be tackled with suitable weapons. Resistance to antibiotic therapy has made it possible to direct research toward alternative treatments, such as the use of immunotherapeutic drugs. However, better knowledge of the mechanisms driving the immune response during S aureus infection and the production of an active vaccine can be considered as two parallel paths. In several published reports, based on infected mouse models, the ability of a S. aureus vaccine antigen has been evaluated to elicit an immune response that can be scaled up to protect multiple mouse models infected with different strains of the pathogen. This procedure allowed us to evaluate cross-immune protection between different models in the presence of different strains of S Aureus [73,74,75,76].
Concerns due to the development of effective immuno-humoral response may be mitigated by converging immune-evasion mechanisms of S aureus. Given the experiences accumulated to date regarding the immune response to staphylococcal infection, there is no doubt that the progress needed to obtain a vaccine promising in terms of efficacy and safety against S aureus depends on an even better understanding of the immunity, both innate and adaptive. We learned that the immune response to S aureus is articulated on the effectiveness of the humoral response, T-cell work, blocking complement factors, and killing immune players by its toxins. The main contrast mechanism exerted by S. aureus to the host concerns the ability of the pathogen to hinder the immune action. Precisely, this peculiar characteristic epitomizes the main factor responsible for the failure of the development of targeted vaccines. Thus, the core of the problem may be the development of immunological interventions that are capable of effectively hampering the mechanisms by which S. aureus counteracts immunity. This process could ensure future success in vaccine development [73,74,75,76].
A line of investigative speculation has been the role of ESAT-6-like proteins secreted by S aureus, designed as S aureus EsxA (SaEsxA) and SaEsxB, which have been studied as possible targets for a vaccine. Although high titers of anti-SaEsxA and anti-SaEsxB antibodies were generated in mouse models vaccinated with the administration of purified proteins, a finding revealing an antibody-mediated immune response, S aureus infection was not prevented. On the other hand, mice treated with the use of recombinant SaEsxA (rSaEsxA) and rSaEsxB recorded sustained immunity to Th1 and Th17. Additionally, this cohort was observed to have substantially improved survival rates when subjected to S. aureus compared to the control cohort. This evidence elucited the functioning of SaEsxA and SaEsxB as two promising Th1 and Th17 antigen candidates, with the potential to expand towards the development of multivalent and serotype-independent vaccines against S. aureus infection [74].
Brady et al [75] focused on the genetically inactivated mutant HlaH35L of toxin alpha and analyzed the protection afforded by this antigen in three infection models using the same vaccine dose, regimen, immunization route, adjuvant, and challenge strain. The use of a systemic infection model challenged by HlaH35L immunized mice revealed a small but statistically significant decrease in bacterial colonization compared to that observed in control mice. In contrast, using a prosthetic implant model of chronic biofilm infection, the researchers observed no significant differences in bacterial levels compared to controls. These results suggest that although vaccines may protect one form of S. aureus disease, they are not active in providing protection against several manifestations of the disease, thus underscoring the significant challenge that exists in vaccine development against S. aureus. [75]
Epidemiological studies have revealed the high colonization potential that characterizes S. aureus, reaching 20 to 80% in humans. This implies the potential to generate a variety of diseases that constitute a nightmare for healthcare-associated and community-associated bacterial infections [73,76]. It is evident that in such a context the development of the vaccine against S aureus has been burdened by abortion, producing failures every time its application has been attempted to date. However, it is possible that the reason for this failure is due to incomplete knowledge of the mechanisms that support the immune defense against this pathogen. In humans, S aureus causes bacteremia, meningitis, endocarditis, pneumonia, osteomyelitis, sepsis, and skin and soft tissue infections. People who are carriers of S Aureus are at increased risk of infection and transmission to others. The spread of multidrug-resistant strains of S aureus limits optimal medical treatment with the use of antibiotic administration options. [73,76]
Recently the awareness of gaping a window on the future vaccine progress against S. aureus strains provided considerable insights. Zhang et al suggested the importance to generate multipronged B-cell, Th1-, and Th17-mediated that are effective to trigger a response against S aureus antigens. Likewise, this accurate immune response gives enhanced and wide protection against S aureus and prevents invasive infection, mucosal colonization as well as skin and soft tissue infection. [76]
Today the impact immunotherapy has is continuously more fostered and supported, which in particular can be conferred by the administration of the vaccine against S aureus infection. A crucial key role is offered by S aureus manganese transport protein C (MntC). This protein is a highly-conserved cell surface molecule that may evoke protective immunity against S. aureus and Staphylococcus epidermidis. Wei et al evaluated the humoral immune response and CD4+ T cell-mediated immune responses disclosing vital protection for mice to decrease the invasion of S. aureus that was evoked by MntC-specific antibodies. The evidence strongly underpinned the definite function of MntC-induced immunity response revealing that Th17 played a remarkable role in counteracting S aureus infection. Again, the evidence noted that MntC-specific antibodies and MntC-specific Th17 cells work synergistically in preventing S aureus infection. In fact, MntC-induced protective immunity decreased after neutralization of IL-17 by the antibody in vivo and adoptive Th17 transferred from mice may not be fully resistant to the S. aureus challenge [77]. Table 1.

Table 1.
Characteristics of the Included Studies.
| First Author/Year Ref | Type of Study | Cohort | Aims | Finding |
|---|---|---|---|---|
| Lockhart et al (2008) Circulation [46] |
Human RCT Single Center (USA) |
290 pts Brushing Gro 98 Vs Extraction-Amoxicillin 96 Vs Extraction-Placebo 96 |
To compare the incidence, duration, nature, and magnitude of IE related bacteremia from single-tooth extraction and toothbrushing. To determine the impact of amoxicillin prophylaxis on single-tooth extraction. |
Amoxicillin has a significant impact on bacteremia resulting from a single-tooth extraction. Toothbrushing may be a greater threat for individuals at risk for infective endocarditis. |
| Mancini et al (2018) Virulence [49] |
Animal (Switzerland pilot) |
Rat with catheter-induced aortic vegetations | To investigate the role of Coa and vWbp in IE initiation | Coa does not support the initial colonization of IE (in L. lactis). vWbp contributes to initiation of IE (in L. lactis) however is marginal in the present of ClfA. |
| Reguiero et al (2019) Circ Cardiovasc Interv [51] |
Human Comparative Multicenter (Canada pilot) |
245 pts SEV 115 Vs BEV 130 |
To determine the incidence, clinical characteristics, and outcomes of patients with IE post-TAVR | IE post-TAVR did not reveal early or late mortality |
| Rodríguez-Vidigal et al (2019) Enferm Infecc Microbiol Clin [52] |
Human Observational Retrospective (Spain) |
200 pts with TAVI | To evaluate single-centre experience of incidence, mortality and associated factors of IE after TAVI. | Incidence of IE post TAVI greater than other series. |
| Di Carluccio et al (2021) RSC Chem Biol. [20] |
Human Multicenter (Italy pilot) |
Collected anatomical specimen | To evaluate the mechanism of interaction of SLBR-B and SLBR-H from S. gordonii in causing IE | Streptococcal Siglec-like adhesins sparks the development of tailored synthetic inhibitors and therapeutics specific for Streptococcal adhesins to counteract IE. No impairment the interplay between Siglecs and glycans. |
| Manukumar et al (2017) Sci Rep [56] |
Human Single Center (India) |
Collected blood draws | To characterize MRSA strain using MALDI-Biotyper multiplex PCR to distinguish between MRSA and MSSA. To screen PCR-SSCP | PCR-SSCP technique for rapid detection of MSSA and MRSA strains was developed |
| Mempel et al (2002) Br J Dermatol. [57] |
Human Single Center (Germany) |
†S. aureus DU 5720 Vs S. aureus DU 8325-4 Vs S. aureus DU 5883 |
To investigate haemolysin-independent virulence to human keratinocytes. | Staphylococcal invasion of human keratinocytes independently of alpha- and beta-hemolysins, leads to necrotic and apoptotic cell damage. |
| Nakagawa et al (2017) Cell Host Microbe J [58] |
Animal Multicenter Center (Japan pilot) |
Murine epicutaneous infection model | To evaluate how S. aureus trigger inflammation | Increased production of IL-1α, IL-36α and Il 17 via IL-1R and IL-36R. Increased γδ T cells, ILC3 and neutrophil. Keratinocyte* Myd88 signaling in response to S. aureus PSMα drives an IL-17-mediated skin inflammatory response to epicutaneous S. aureus infection. |
| Schwarz et al (2021) Virulence [63] |
Human in vitro and in vivo Multicenter (Germany) |
34 S. aureus Pts with S. aureus endocarditis Vs healthy individuals |
To evaluate pathomechanisms in the induction of IE | in vitro assays did not correlate with the severity of IE. i S. aureus isolates differed in the activation and inhibition of pathways connected to the extracellular matrix and inflammatory response |
| Malachowa et al (2011) PLoS One [64] |
Human/Animal Single center (USA) |
S. aureus LAC Vs S. aureus LACΔhlgABC |
To study the S. aureus USA300 transcriptome | Limited contribution of any single two-component leukotoxin lukS-PV and lukF-PV to USA300 immune evasion and virulence. |
| Alonso et al (2013) Nature [65] |
Animal Single center (USA) |
CCR5-deficient mice | To study activity of S. aureus leukotoxin ED (LukED) | CCR5-deficient mice are resistant to lethal S. aureus infection |
| Kim et al (2010) J Exp Med. [71] |
Animal Single center (USA) |
ℷ Mice with SpA (KKAA) | To study S. aureus protective immunity. | SpA (KKAA) immunization enabled MRSA-challenged mice to organize antibody responses to many different staphylococcal antigens. |
| Becker et al (2014) Proc Natl Acad Sci U S A. [72] |
In vitro Single center (USA) |
S. aureus Newman cultures | To demonstrate that SpA is released with murein tetrapeptide-tetraglycyl [L-Ala-D-iGln-(SpA-Gly5) L-Lys-D-Ala-Gly4] linked to its C-terminal threonyl | SpA, a B cell superantigen, is released with peptidoglycan linked to its C terminus. Murein hydrolases cleave the anchor structure of released SpA to modify host immune responses. |
| Zhang et al (2015) Infect Immun. [74] |
Animal Single center (China) |
Mice SaEsxA and SaEsxB Vs Mice rSaEsxA and rSaEsxB |
To investigate SaEsxA and SaEsxB, as possible targets for a vaccine. | SaEsxA and SaEsxB are effective toward Th1 and Th17 candidate antigens. |
| Brady et al (2013) PLoS One [75] |
Animal Single center (USA) |
Mice HlaH35L Vs Control Vs Prosthetic implant model of chronic biofilm |
To evaluate the ability of one S. aureus vaccine antigen to protect in three mouse models of infection | Vaccines may confer protection against one form of S. aureus disease without conferring protection against other disease presentations |
| Zhang et al (2018) mBio [76] |
Animal Multicenter (USA pilot) |
C57BL/6 mice | To study the role of adaptive immunity induced by an S. aureus vaccine in protection against S. aureus bacteremia | Multipronged humoral and cellular (B-cell, Th1, Th17) responses to S. aureus antigens may be critical to achieve effective and comprehensive immune defense |
| Yu et al (2018) Sci Rep [77] |
Animal Single center (China) |
Mouse peritonitis model | To evaluate the humoral immune response and CD4+ T cell-mediated immune responses | The MntC-specific antibodies and MntC-specific Th17 cells play cooperative roles in the prevention of S. aureus infection. |
Abbreviations; BEV, balloon-expandable valve; C57BL/6 , C57 black 6; CCR5; C-C chemokine receptor type 5; ClfA, clumping factor A; Coa, plasma-clotting factors staphylocagulase; DU, S. aureus mutant; IE, infective endocarditis; γδ T cells, Gamma delta T cells; IL, interleukine; ILC3, group 3 innate lymphoid cells; HaCaT, aneuploid immortal keratinocyte cell; LAC, wild-type USA300 strain; LACΔhlgABC, hlgABC-deletion strain ; L. Lactis; Lactococcus lactis; lukS/F-PV, leukotoxin S/F -Panton-Valentine ; LukED, S. aureus leukotoxin ED; MntC, S. aureus manganese transport protein C; MRSA, methicillin resistant Staphylococcus aureus; MSSA, methicillin susceptible S. aureus; PCR, protein chain reaction; PCR-SSCP, PCR-coupled single strand conformation polymorphism; PSM, phenol-soluble modulin α; Pt, patient; PVL, Panton-Valentine Leukocidin; rSaEsx, recombinant; SaEsx, S. aureus Esx; SEV, self-expanding valve; SLBR, Siglec-like binding region; SpA, staphylococcal protein A; TAVI, transcatheter aortic valve implantation; Th17, T helper 17 cells, TSB, trypticase soy broth. †S. aureus mutant DU 5720 alpha-haemolysin, beta-haemolysin double-negative ; S. aureus mutant virulent strain DU 8325-4 ; S. aureus variant DU 5883 isogenic fibronectin-binding protein A/B-negative. .* Myd88, keratinocyte-specific deletion of the IL-1R and IL-36R ; ℷ variant KKAA staphylococcal protein A
4. New evidence from the infectious array of Staphylococcus aureus. Involvement of the protective shield and host protection functions
Staphylococcus aureus infections have been extensively studied with the use of different animal models, especially adapted to invasive infections of this pathogen, suggesting the fundamental role of two coagulases, von Willebrand factor binding protein (vWbp) and coagulase (Coa), which lead to critical virulence. These proteins constitute a functionally intricate architecture that S. aureus uses to generate a protective fibrinogen/fibrin shield that surrounds it. The creation of this shield gives the microorganism the ability to evade the main defense mechanisms implemented by the host's phagocytic cells. One of the key functions of coagulases leads to the non-proteolytic activation of the zymogen prothrombin to convert fibrinogen into fibrin, thus promoting the formation of the fibrinogen/fibrin protective shield.
There are several key functions of coagulases. One of these induces the non-proteolytic activation of the prothrombin zymogen to convert fibrinogen to fibrin, thus promoting the formation of the protective fibrinogen/fibrin shield. Another function offered by coagulases is to serve as a link with fibrinogen, whose interactions substantially support infection. The mechanism or mechanisms that allow the binding between vWbp and Coa and fibrinogen involve distinct interactions of the two proteins with the molecule, although they show a similar structure. Coa binding to soluble fibrinogen has a significantly higher affinity than fibrinogen coated on a plastic surface. The vWbp, on the other hand, did not show any preference between the two forms of fibrinogen [10,11,12,13,14]. Figure 4
Thomas et al investigated the complex interactions between fibrinogen and S. aureus suggesting a different action exerted by vWbp and Coa targeting different sites on fibrinogen, demonstrating an absence of competition between the two molecules in fibrinogen binding. Both Coa and vWbp have N- and C-terminal halves that drive fibrinogen binding activity [13,14]. These vWbp coagulases have the greatest fibrinogen binding affinity in the vWbp-N region, in contrast to Coa in which the greatest bias towards the fibrinogen binding site has been related to the C-terminal region. It has been reported that the peptides constituting the previously identified Fibrinogen Coa/Efb1 binding motif do not inhibit the vWbp-C component from binding to fibrinogen. Therefore, the absence of a functional homologue to this motif has been suggested for vWbp-C. It was also observed that although the N-terminal prothrombin-binding domains of both coagulases recognize the β-chain of fibrinogen, they nevertheless appear to interact with several sequence motifs in the host protein. It is therefore possible to speculate that the interaction of the two coagulases appears to be expressed with different sequence motifs in the host protein. The findings reported by Thomas et al provide insight into the complex interactions between Fg and S. aureus coagulases [14].
Multidrug-resistant Staphylococcus aureus strains are responsible for life-threatening diseases deploying a worldwide public health problem. The limitations for dealing with Staphylococcus aureus infection depend on both the treatment and the lack of an effective vaccine. As previously reported S aureus develops complex and accurate mechanisms that defend it through the protection of a shield by fibrinogen/fibrin. This coating serves two purposes: 1) it allows the pathogen to survive in the blood making it invisible to the host's immune protection and 2) it offers the possibility of spreading and giving rise to invasive diseases. Modifying this process represents a promising goal for new antistaphylococcal treatment strategies, however, the mechanisms that regulate the phenomena are not yet completely explored. S. aureus expresses many proteins that bind to fibrinogen. A redundant action exerted by some of these proteins with vWbp can limit its function. Indeed, in the presence of proteins expressing similar functions, a sharing between them in the structural or functional motif has often been suggested.
Thomas et al [14] proved the expression of a protein homologue (vhp) corresponding to the C-terminus of the von Willebrand factor binding protein (vWbp) providing an elucidation in both shield assembly and fibrinogen binding. Investigators identified a common Fg binding motif between vhp and vWbp.
Recently Schwartz et al [63 described the potential pathomechanisms involved in promoting infective endocarditis. In vitro and in vivo models of 34 isolates of Staphylococcus aureus were studied by collecting pathogens from patients with S. aureus endocarditis and healthy subjects. [63] The strains of S. aureus isolated were tested in vitro to evaluate cytotoxicity, the function of invading and interacting with platelets typically expressed by these pathogens. In order to correlate the ability of S. aureus to promote the development of vegetations on the aortic valves in vivo, the virulence factor expression profiles and cellular response were also studied and tested using an animal model. The presence of IE involving valves was assessed in vivo with the use of magnetic resonance imaging at 9.4 T. Histological evaluation with enrichment gene expression analysis was also performed. S. aureus isolated and tested in vivo recorded potentiality to give rise to IE, reliably inducing inflammatory responses associated with the aortic valve’s injuries. However, the differentiation and classification of IE as well as the characterization of inflammation based on the measurement of in vitro virulence profiles and cytotoxicity were not established [63].
Importantly, Schwartz et al suggested that in vitro test results did not correlate with EI severity. However, the researchers observed that the Staphylococcus isolates differed substantially in the degree of activation and inhibition of pathoanatomical processes related to the extracellular matrix and in the characteristics of the inflammatory response. It was therefore suggested that the pathogenic capacity of bacteria did not confer a uniform response and that more comprehensive approaches to host-pathogen interactions were needed for its assessment. Furthermore, this approach promoted new insights into the corresponding immune pathways to highlight differences in host/pathogen interaction [63].
With regards to the etiology of Staphylococcus aureus-induced infective endocarditis, Schwarz et al opened a window to improve discernment of the interaction between virulence factors and immune response in S. aureus-borne infective endocarditis, so as to favour the development of innovative therapeutic strategies and specific diagnostic imaging markers [63].
4.1. Pathogen-Host Interaction in Determining Inflammation
Particular attention is paid to the substantial pathogenic action of Staphylococcus Aureus, which is mediated by adhesion proteins such as the fibronectin-binding protein and staphylococcal aggregation factors A and B, which play the role of bacterial mediators of adhesion and are the key determinants of pathogenicity [78,79,80,81]. Findings in an animal model with induced experimental endocarditis proved that the expression of Staphylococcus aureus adhesins in Lactococcus lactis suggested a crucial role of clumping factor A (ClfA) and fibronectin-binding protein A (FnBPA) for valve colonization. [78]
Que et al [78] evaluated the role of the progression of infective endocarditis in animals that were followed for three days. Investigators noted that ClfA-positive lactococci successfully colonized damaged valves, nevertheless, the eradication of infection was spontaneously observed over 48 h. As for FnBPA-positive lactococci, pathogens titers progressively increased both in vegetations and in spleens. Imaging findings revealed that while ClfA-positive lactococci were limited to vegetations, FnBPA-positive lactococci also overran to the adjacent endothelium. This process explained the ability of FnBPA to trigger cell internalization in vitro. FnBPA carries both fibrinogen and fibronectin binding domains, so the role of these two selective functionalities in causing infection was assessed by depriving FnBPA of the fibrinogen binding domain and integrating it with the fibrinogen binding domain of ClfA in cis. or in trans. Although the abrogation of the fibrinogen binding domain of FnBPA did not change fibronectin binding and cellular internalization in vitro; however, it completely led to the elimination of valve infectivity in vivo. Interested, the ability to induce infection was restored in cis with the insertion of the fibrinogen binding domain of ClfA into truncated FnBPA while in trans was obtained by co-expressing full-length ClfA and truncated FnBPA, by using two separate plasmids. Therefore, it can be inferred that in S. Aureus infection the binding of fibrinogen and fibronectin could cooperate for valve colonization and in vivo endothelial invasion. [78]
Staphylococcus aureus infection is supported by bacteremia which not only leads to complications such as infective endocarditis, and osteomyelitis but promotes the pathogen's exit from the bloodstream to cause metastatic abscesses. The bacterium's interaction process with endothelial cells plays a substantial role in causing these complications. At this stage of the infection, several bacterial proteins are involved. A fundamental role is offered by the extracellular adhesion protein(Eap) of S. aureus which has many functions including that of binding various host glycoproteins. [82,83,84,85,86]
It has also been shown to have both pro and anti-inflammatory activity. Difficulties have emerged in robustly testing the role of Eap in vivo, due to the difficulties expressed in defining its activity in mutant strains. Substantial evidence has been reported on the pro-inflammatory role of Eap and on the activity that purified native adhesion protein of S. aureus has in triggering the release of TNFα in human whole blood in a dose-dependent manner. TNFα production promotes S. aureus adhesion to endothelial cells with a 4-fold increase through a mechanism involving protein A on the bacterial surface and gC1qR / p33 on the surface of endothelial cells. This finding suggested that Eap's contribution to disease severity during S. aureus bacteremia is crucial. It was genetically engineered for an isogenic set of strains, in which the Eap gene was inactivated and integrated after inserting an intact copy of the gene elsewhere on the bacterial chromosome. Using a mouse bacteremia model, it was shown that Eap-expressing strains cause a more severe infection, suggesting the major role of Eap in invasive disease. [83,85,86]
Bacterial colonization offers the trigger for additional cycles of endothelial damage and thrombus deposition resulting in the implantation of infected vegetation. In this phase, the production of a biofilm which is formed by a multilayer with a bacterial aggregate containing a polysaccharide associated with a protein matrix assists bacterial persistence and contributes to antibiotic tolerance [87]. Figure 5
5. Interaction between infective endocarditis pathogens, vascular endothelium, and blood constituents
Staphylococcus aureus surface molecules work crucially to promote colonization of the vascular endothelium which is considered to be a key primary event in the pathogenesis of infective endocarditis. The ability of these molecules to elicit combined endothelial procoagulant and proinflammatory responses, leading to the development of ED, has been well established [78,88,89,90,91]. Heying et al [88] evaluated the peculiar role of three important molecules expressed by S aureus surface. Fibronectin-binding protein A (FnBPA) and B (FnBPA) as well as clumping factor A (ClfA) act to induce a bacterial adherence process that identifies the cultured human endothelial cells (ECs) interacting with Staphylococcus aureus. Likewise, these molecules promote the phenotypic and functional changes in ECs. The investigators used non-invasive surrogate bacterium Lactococcus lactis. Lactococcus lactis, by gene transfer, expressed staphylococcal molecules FnBPA, FnBPA, or ClfA. In this way, the recombinant Lactococci positive for FnBPA or FnBPB revealed an increase in the incidence of infection at the EC level up to 50-100 times the baseline threshold. Another piece of evidence highlighted a provoked inflammatory response with activation of the EC characterized by an increased expression of ICAM-1 and VCAM-1 on the surface, and production of interleukin-8 associated with the concomitant adhesion of monocytes. On the contrary, infection determined by ClfA-positive lactococci did not activate EC. The prominent action of FnBPA-positive L. lactis promoted a notable inflammatory response that was enhanced by cell-bound monocytes and mediated by tissue factor-dependent endothelial coagulation. Evidence suggested that S. aureus FnBPs, but not ClfA, promoted the invasiveness and pathogenicity of nonpathogenic L. lactis microorganisms, indicating that the bacterium-EC interactions mediated by these adhesins were strongly prone to favor both inflammation and procoagulant activity at infected endovascular sites [88].
Studies carried out on experimental endocarditis induced by Staphylococcus aureus have highlighted two important phases of the infection. The function of sequential fibrinogen binding responsible for valve colonization and the pivotal action of fibronectin-binding promoting endothelial invasion was demonstrated. These processes were supported by peptidoglycan-linked adhesins. The role played by fibronectin-binding protein A (FnBPA) promoted a synthesis between these two specific properties, combined with the binding of elastin, in leading experimental endocarditis.
Piroth et al [89] reported the substantial role played by the minimal subdomain of FnBPA responsible for fibrinogen and fibronectin binding in promoting cell invasion in endocarditis in vivo. FnBPA was expressed in Lactococcus lactis and was tested in vitro and in animals. Of note that the needful subdomain to induce infective endocarditis consisted of 127 amino acids that represented the hub of the fibrinogen- and fibronectin-binding regions of FnBPA and were sufficient to confer the charge of these properties. Although in animals evidence raised the belief about the crucial role of fibrinogen binding to determine endocarditis induction; however, the role exerted by fibronectin binding was not significantly associated with endocarditis induction. On the contrary, as for disease severity, both fibrinogen binding and fibronectin binding were of substantial importance. Besides, the synergistic combination of fibrinogen binding and fibronectin binding suggested a considerable increase in the infectious foray of cultured cell lines, emphasizing a decisive feature to be linked with endocarditis severity. Accordingly, the concept based on sequential action offered by fibrinogen binding and fibronectin binding in promoting colonization and invasion fell in support of the unexpectedly intertwined role offered in endocarditis by fibrinogen binding and fibronectin binding in terms of both functional anatomy and pathogenetic mechanism. Consequently, this refined and unexpected feature of FnBPA paves the way for the development of anti-adhesin strategies [89]. Figure 6
Bacterial proteins such ClfA and FnBPA intercede for the adhesion of S aureus to EC surface molecules. This function is shared with subendothelial matrix proteins involving fibrinogen, fibrin, fibronectin, and von Willebrand factor (vWF) [90]. It is important to underline the work of Pappelbaum et al [91] who suggested ultra-large von Willebrand factor (ULVWF) substantially concurred with the inceptive pathogenic step of S aureus-induced endocarditis in subjects disclosing an intact endothelium. The synergistic role of ClfA, FnBPA, and von Willebrand factor (vWF) in determining the adhesion of Staphylococcus aureus to endothelial cells (ECs) has been investigated in three recent reports that markedly endorse the fundamental importance of these molecules in IE [92,93,94]. Evidence pointed out that ultra-large von Willebrand factor (ULVWF) substantially promoted the initial pathogenic phase of S aureus-induced endocarditis in patients who revealed an undamaged endothelium. The use of heparin and ADAMTS13 allowed for decreasing the ULVWF formation and may suggest novel therapeutic choices to avoid IE [91].
Recently Claes et al [92] revealed the interaction between vWbp and staphylococcal surface protein that moderated S aureus adhesion to VWF and to vascular endothelium under shear stress. The investigators used Sortase A (SrtA) deficient mutants and SrtA-dependent surface proteins, as well as Lactococcus lactis conveying single staphylococcal surface proteins. In detail, S. aureus firstly tied to the endothelium via VWF, afterwards secreted VWF-binding protein (vWbp) that finalized the adhesion of S. aureus to VWF under shear stress and ultimately, vWbp interacted with VWF and the Sortase a ClfA dependent surface protein. So, it is possible to assert that VWF-vWbp-ClfA anchored S. aureus to the vascular endothelium under shear stress [92]. In another report, the same authors evaluated the effect of shear flow and plasma on the binding of ClfA and FnBPA, including its sub-domains A, A16+, ABC, CD, vWF, fibrinogen/fibrin, fibronectin or confluent ECs. With the use of a genetically engineered Lactococcus lactis that expressed these adhesins heterologously, Claes et al [93] found that global adherence profiles were similar in static and flow conditions. The degree of adhesion of L. lactis- FnBPA to EC-bound fibronectin and of L. lactis- ClfA to EC-bound fibrinogen was similar to that of L. lactis- ClfA to coated vWF domain A1, in the presence of vWF-binding protein (vWbp). To focus the evidence that in plasma, the adhesion of L. lactis-ClfA to activated EC-vWF / vWbp was reduced by 80% within the time limit of 10 minutes and was related to the crucial role of disintegrin-mediated and metalloproteinase-mediated vWF hydrolysis with thrombospondin motif type 1, member 13. Likewise, in lacking plasma components the adhesion of L. lactis- FnBPA was reduced by > 70% compared. In contrast, plasma fibrinogen supported high L. lactis- ClfA binding to resting and activated ECs. These findings suggested that in plasma S aureus adhesion to active endothelium was dependent mostly on two complementary pathways: a rapid but short-lived vWF/vWbp pathway and a stable integrin-coupled - fibrinogen pathway. Observations derived from these results confirmed that pharmacological inhibition of ClfA-fibrinogen interactions may constitute a valuable adjunctive treatment in infective endocarditis. [93]
Staphylococcus aureus actively invades the endothelium promoting detrimental action that led to apoptosis and endothelial damage. A vast body of literature supports the knowledge of the crucial role of Staphylococcus in causing IE through the pivotal role mediated by protein clotting factor A (ClfA), which is associated with the cell wall of S. aureus. Concerning the role exerted by secreted plasma coagulation factors staphylocagulase (Coa) and by the protein binding von Willebrand factor (vWbp), several studies have recently clarified their mechanisms. Mancini et al [94] studied rat models with catheter-induced aortic vegetations. They investigated the role of staphylococcal secreted coagulase (Coa-positive staphylococci) and Staphylococcus aureus encoded a von Willebrand factor binding protein (vWbp) in the institution of infective endocarditis. As previously described a model based on Lactococcus lactis mutants expressing coa, vWbp, ClfA or vWbp / clfA and S. aureus Newman Δcoa, ΔvWbp, ΔclfA or Δcoa / ΔvWbp / ΔclfA was used. Investigators observed that vWbp expression statistically increased L. lactis-induced valve infection as compared with parental and coa-expressing strains. Likewise, the expression of ClfA recorded increased infectivity of L. lactis, which was not further affected by the co-expression of vWbp. Of note the finding that deletion of the Coa or vWbp genes in S aureus did not reduce infectivity while deletion of ClfA dramatically decreased valve infection. A crucial observation supported that the activity of clfA was not affected by the triple deletion of Δcoa / ΔvWbp / ΔclfA. This result allowed for speculation that Coa did not promote inceptive IE colonization by using L. lactis as the pathogen without other key virulence factors. Unquestionably, the presence of vWbp concurred with the onset of IE induced by L. lactis, nevertheless, its role was borderline in the presence of ClfA [94].
A vast body of proven evidence has shown the markedly extracellular pathogen role worked by Staphylococcus aureus, however, this causative pathogen has also the ability to be integrated by host cells, including nonprofessional phagocytes. Hence, it can be a deterrent inside endothelial cells, epithelial cells, or osteoblasts. The intracellular S aureus location concurs to the establishment of infection. The entry gate of the bacterium is umpired by the binding of integrin α5β1 expressed on the membrane of the host cell which recognizes fibronectin. This bridge encourages the recognition between pathogen and host cell promoting subsequent cell integration. [95,96,97,98]. Although the osteoblasts revealed tall expression of α5β1-integrin and fibronectin with demonstrated high ability of the pathogen to adhere to osteoblasts; however, Niemann et al [99] suggested, using internalization tests and immunofluorescence microscopy, that S aureus was less swallowed in osteoblasts compared to epithelial cells. During cell infection adding exogenous fibronectin in presence of S aureus, authors found increased uptake of the pathogen in epithelial cells that was not recorded in osteoblasts. This finding offered understandable contrast to previous claims regarding the pathogen uptake mechanism, which gave integrin and fibronectin expression a pivotal role in causing bacterial uptake in host cells. Importantly, the organization of extracellular fibronectin surrounding osteoblasts and epithelial cells was different, revealing in the former a structure typically organized in a fibrillar network. The uptake enhancement of S aureus was significant, resulting in the inhibition of fibril formation, brief reduction of RNA-mediated fibronectin expression, and disruption of the fibronectin-fibril network. The work of Nieman et al highlighted that the fibronectin fibril network seemed to strongly decrease the uptake of S aureus into a given host cell, indicating that the supramolecular structure of fibronectin may direct the different ability of particular host cells to internalize the pathogen [99]. The results reported by Niemann et al [99] suggested the non-determining role exerted by the crude quantity of fibronectin but rather the substantial role established by the supramolecular structure of the fibronectin molecules. Once deposited on the eukaryotic cell surface, they play a fundamental role in bacterial uptake by host cells. This evidence can describe the considerable inconstancy expressed in the efficacy of S aureus absorption considering different types of host cells. Furthermore, differences have been shown in vivo between bacterial infection courses and bacterial localization in different clinical settings [99].
From a molecular point of view, the pathogenicity of S aureus is related to the expression of a variety of virulence factors, including proteins that moderate the process of adhesion to host plasma molecules and extracellular matrix proteins. Among these, numerous shreds of evidence have demonstrated a marked ability of IsdB-expressing bacteria to bind to both soluble and immobilized vWF [100]. A recent report by Alfeo et al [101] suggested that the iron-regulated surface determinant B (IsdB) protein, besides being involved in iron transport and vitronectin binding, interacted with von Willebrand Factor (vWF). The binding between IsdN and recombinant vWF was disrupted by heparin and was also decreased due to the high ionic strength. Furthermore, the use of administered ristocetin, an allosteric agent that induced exposure of the A1 domain of vWF, evoked the substantial effect of enhancing the binding between IsdB and vWF. It was permissible to speculate that IsdB binding and S. aureus adhesion were markedly inhibited by a monoclonal antibody against the A1 domain as well as IsdB reactive IgG isolated from patients experiencing staphylococcal endocarditis. Therefore, this evidence suggested two obvious conclusions: the importance of IsdB in favoring the adhesion of S. aureus, and its role in the colonization of the endothelium by S aureus. The potential role of IsdB in serving as therapeutic target could be offered [101].
5.1. Infective Endocarditis and Platelets
In patients with high-risk of infective endocarditis, the use of antibiotic prophylaxis is currently recommended, given the difficulty in treating IE and its inherent mortality. It should be underlined that the concerns related to the administration of antibiotics are confronted with their unquestionable low efficacy for certain strains of Staphylococcus aureus alongside perpetuating increasing multidrug-resistant strains of infection. Given this worrying clinical scenario, the need to find new therapeutic options remains a priority against IE. The role played by platelets is crucial in the early phase of infective endocarditis, making them first-line immune responders. [80,81,102]
Important results have been observed in mechanistic in vitro studies which have highlighted the early action of contrasting the infection supported by platelets during the first phase of the Staphylococcus aureus infection involving cardiac structures. Thus, a first front of the platelet-dependent immune response can be configured in directing an initial antimicrobial contrast action mediated by the interaction of platelets with the pathogen. This is the proposed case for the therapeutic use of acetylsalicylic acid.
Experimental in vitro and animal models have suggested that the purpose of aspirin may restrict bacterial-platelet interactions promoting the prevention of vegetation spread and has revealed promising results. However, the data from clinical trials reporting outcomes in patients with IE who received additional aspirin to background therapy has not produced conclusive results. Therefore, conflicting evidence emerged shedding a veil of uncertainty about the benefit of antiplatelet drugs in the prevention of IE sustained by Staphylococcus aureus. In addition to aspirin, other drugs with anti-platelet action have been tested for which a therapeutic effect has been observed. For example, the P2Y12 platelet receptor antagonist ticagrelor could couple its potent and well-known antiplatelet activity with a marked antibacterial property. Furthermore, a recent study based on a mouse animal model reported a marked ability of ticagrelor to eradicate Staphylococcus aureus bacteraemia [103,104,105]. Table 2
Table 2.
Characteristics of the Included Studies.
| First Author/Year Ref | Type of Study | Cohort | Aims | Finding |
|---|---|---|---|---|
| Que et al (2005) J Exp Med [78] |
Animal model Single Center (Switzerland) |
Rat model of IE induced | To study valve colonization with experimental endocarditis. To evaluate the role of ClfA and FnBPA positive lactococci | Fibrinogen and fibronectin binding could cooperate for S. aureus valve colonization and endothelial invasion in vivo |
| Edwards et al (2012) PLoS One [79] |
Human Single Center (UK) |
Blood sample | To study in vivo role of Eap to interact with host glyco-proteins | Eap expressing strains cause a more severe infection, demonstrating its role in invasive disease. Increased level of TNFα and gC1qR/p33 expression |
| Veloso et al (2013) Infect Immun [81] |
Animal model Single Center (Switzerland) |
Rat model of IE induced 10(6) CFU L. lactis pIL253 Vs Recombinant L. lactis (ClfA, FnbpA, BCD, or SdrE) |
To explore the contributions of S. aureus virulence factors to the initiation of IE. | Fibrinogen binding in the initiation of S. aureus IE. Activation of platelet aggregation or an inflammatory response may contribute to or promote the development of EI |
| Thomas et al (2021) mBio [82] |
Animal model Single Center (USA) |
Rat model of IE induced | To identify proteins with significant amino acid identities to vWbp | Protein homologous to the C-terminal of vWbp was identified. Its role in Fg shield assembly and binds. |
| Hussain et al (2002) Infect Immun [83] |
In vitro Single center (Germany) |
S. aureus Newman cultures Vs Control mutant |
To investigate the role of Eap by constructing a stable eap::ermB deletion | Eap may contribute to pathogenicity by promoting adhesion of whole staphylococcal cells to complex eukaryotic substrates |
| Palankar et al (2018) Int J Med Microbiol. [84] |
In vitro Single center (Germany |
S. aureus Mu50 | To investigate Eap subdomain and interaction with platelet | Eap subdomain Eap D3D4 specifically interacts and rapidly activates human platelets |
| Hussain et al (2008) Infect Immun [85] |
In vitro Single center (Germany |
S. aureus Newman cultures Vs S. aureus Wood 46 |
To investigated the interactions of full-length Eap and five recombinant tandem repeat domains with host proteins. | More than one Eap tandem repeat domain is required for S. aureus agglutination, adherence, and cellular invasion but not for the stimulation of PBMC proliferation. |
| Heying et al (2007) Thromb Haemost. [88] |
Human Single Center (Germany) |
S. aureus L. lactis culture cultured human EC |
To investigate the role of FnBPA, FnBPB ClfA to promote bacterial adherence to cultured human ECs. | S. aureus FnBPs, but not ClfA, lead pathogenicity to non-pathogenic L. lactis. Adhesins (ICAM-1 and VCAM-1) evokes inflammation (interleukin-8) as well as procoagulant activity. |
| Piroth et al (2008) Infect Immun [89] |
Animal model Single Center (Switzerland) |
S. aureus L. lactis culture In vitro and in vivo |
To study subdomain of FnBPA responsible for fibrinogen and fibronectin binding, cell invasion, and in vivo endocarditis | Fb binding combined with fibronectin binding to synergize the invasion of cultured cell lines is correlate with IE severity |
| Pappelbaum et al (2013) Circulation. [91] |
Human/Animal Single center (Germany) |
6 WT mice with VWF vs 5 knockout mice vs Cultured human EC |
Whether ULVWF mediates bacterial adherence. | ULVWF contributes to the initial pathogenic step of S aureus-induced endocarditis in patients with an apparently intact endothelium. Heparin or ADAMTS13 intervenes in decreasing ULVWF adherence |
| Claes et al (2018) Thromb Haemost [93] |
Human/Animal Multicenter (Belgium pilot) |
L. lactis-clfA Vs L. lactis-fnbpA Vs Cultured human EC |
To study the influence of shear flow and plasma on the binding of ClfA and FnbpA | Pharmacological inhibition of ClfA-Fg interactions may constitute a valuable additive treatment in infective endocarditis. |
| Ko et al (2016) mBio [94] |
Animal model Single Center (USA) |
Rat model of IE induced | To identify variants of a linear Fg binding motif, present in Coa and Efb which are responsible for the Fg binding activities of these proteins | S. aureus coagulase can induce the formation of a fibrinogen shield in experimental abscess models which surrounds and protects bacteria in the microcolony from clearance. |
| Niemann et al (2021) mBio. [99] |
Animal Multicenter (Germany) |
Rat model of IE induced in osteoblasts vs epithelial cells |
To demonstrate that S. aureus was less engulfed in osteoblasts than in epithelial cells. | Large differences of S. aureus uptake efficacy in different host cell types. In vivo differences between courses of bacterial infections and the localization of bacteria in different clinical settings mediated by α5β1-integrin |
| Pietrocola et al (2020) J Biol Chem. [100] |
Animal Multicenter center (Italy pilot) |
Rat model of IE induced | To evaluate a variety of virulence factors that promote infection by S. aureus | Adherence to and invasion of epithelial and ECs by IsdB-expressing S. aureus cells was promoted by Vn, and an αvβ3 integrin-blocking mAb |
| Alfeo et al (2021) Sci Rep [101] |
Animal Multicenter center (Italy pilot |
Rat model of IE induced | To study IsdB protein and Vn binding Interacts with vWF. | Importance of IsdB in adherence of S. aureus to the endothelium colonization and as potential therapeutic target. |
| Ditkowski et al (2021) J Thorac Cardiovasc Surg [103] |
Human Multicenter (Belgium pilot) |
5 graft tissues | To investigate contributions by platelets and plasma fibrinogen to IE initiation on various grafts used for valve replacement | Binding of plasma Fg to especially BJV grafts enables adhesion of single platelets via αIIbβ3. S aureus attaches from blood to activated bound platelet αIIbβ3 via plasma fibrinogen. |
Abbreviations; ADAMTS13, a disintegrin and metalloproteinase with thrombospondin motifs 13; BJV, bovine jugular vein ; ClfA, clumping factor A; Eap, S. aureus extracellular adhesion protein ; EC, endothelial; cell; Fc, fibrinogen; FnBPA, fibronectin-binding protein A; IsdB, iron-regulated surface determinant B protein; IL, interleukine; L. lactis, Lactococcus lactis; SdrE; mAb, monoclonal antibody; PBMC, peripheral blood mononuclear cells; TNF, tumor necrosis factor; ULVWF, ultra large von Willebrand factor; Vn, extracellular matrix protein vitronectin ; vWbp, von Willebrand factor-binding protein ; vhp, vWbp homologous protein
6. Biofilm formation
Biofilms allow microorganisms to live by adapting to the functions and metabolism of the self-produced matrix which is made up of hydrated extracellular polymeric substances (EPS). Therefore, biofilms behave as an immediate functional environment formed directly by the bacteria. The main constituents that form EPS are molecules of polysaccharides, proteins, nucleic acids, and lipids. EPS performs multiple functions involving the conferral of mechanical stability of biofilms, mediating their adhesion to surfaces and forming a cohesive and three-dimensional polymeric network that interconnects and transiently immobilizes the biofilm cells. Regarding the function of the external digestive system offered by the biofilm matrix, it keeps the extracellular enzymes close to the cells which can be metabolized and dissolved into colloidal and solid biopolymers [87,106,107].
During infective endocarditis, the formation of bacterial biofilms is a basic stage for the fatal evolution of the disease. IE manifests itself as a minor lesion of the cardiac structure and the damage generated is then accompanied by a healing reaction, which promotes the recruitment of fibrin and immune cells. In the first cicatricial phase the vegetations are sterile but potentially at risk of inducing colonization during temporary bacteraemia, thus leading well established IE. In vitro, experimental models using a simulated IE vegetation model produced from venous whole blood have proven to be of great utility for studying biofilms during infective endocarditis. Likewise, these models allowed establishment of stable bacterial colonization after 24 hours. Once structured in biofilm aggregates, the pathogens showed greater tolerance to antibiotics [106,107].
Swartz et al. recently investigated the time required to generate biofilms and how these affect the development of antibiotic tolerance. Evidence suggested that reference strains of Staphylococcus aureus, as well as three clinical isolates of IE, generated biofilms modeled on IE vegetation 6 hours after the onset of infection. Furthermore, the earlier the antibiotic was administered, the more marked its pharmacological action in containing biofilm maturation, suggesting that early treatment was more effective in containing the development of the disease. The authors were able to follow the biofilm development under the microscope by observing the bacterial aggregates growing on the IE vegetation model and the interaction with the antibiotic. The formation of mature, antibiotic-resistant biofilms was recorded after 6 hours, thus accelerating screening for optimal treatment strategies for IE [108].
Biofilm formations raises concerns in patients requiring treatment of heart valves endocarditis (HVE) [109,110,111,112]. In this context the aggressiveness of Gram-positive bacteria become crucial due to the lack of an external membrane that is replaced by surrounding peptidoglycan, less sensitive to serum-induced killing. Subsequently to bacteria colonization and adhesion, pathophysiology of HVE is chacterized by bacterial proliferation cycles. In this phase local thrombotic processes, recruitment of monocytes, and inflammation, leading to the formation of mature vegetations occur [50]. As regard HVE, the production of biofilm is representative of numerous causative pathogens, including staphylococci, streptococci, and enterococci with other rarer germs, such as Pseudomonas aeruginosa and Candida species that promote bacterial incorporation into polysaccharide extracellular slime-like matrix. In patients who developed staphylococcal prothethic valve endocarditis (PVE), undergoing to valve replacement with the use of a homograft or autograft [109,110,111,112], the specificity of biofilms induces a cell-to-cell communication and synchronized gene expression that promotes the assembly and maturation of pathogens. In this population of patients once the biofilm arises, it protects the bacteria from the host’s immune system, reduces antimicrobial efficacy, while shielding the organisms [50].
The characteristics of the generating biofilm are now recognized as a virulent trait in the development of PVE especially related to Staphylococcus aureus, for which the use of allogeneic or autologous tissue as an ideal valve substitute is recommended. Aortic Homografts are widely used in prosthetic valve endocarditis (58.1% vs 28.8%, P =.002) and methicillin-resistant Staphylococcus infection (25.6% vs 12.1%, P = .002), compared to those who surgical correction was performed using conventional prostheses [113]. In another report 64% of patients with PVE involving the aortic valve received an aortic homograft in 56 (64%) patients while mechanical prosthesis was used 23% of cases and a bioprosthesis in 13%, respectively. Surgical correction using aortic homograft was independently associated with a reduced risk of infection relapse (P = 0.006) compared to conventional valves [114]. Active endocarditis supported by causative pathogens generating biofilm is often responsible of recurrence [115,116,117,118,119] and is a statistically significant univariable risk factor for increased early and late mortality as revealed by studies with short [113,118]. and long-term follow-up (over 20 years) [120,121,122,123,124,125]. As far as PVE is concerned, the use of Ao-H appears indisputable, unlike native valve endocarditis whereby the preference for conventional prosthesis and synthetic material is still prevailing [114].
We used homografts as substitute to replace aortic and mitral valve diseased in 56,2% and 21% of patients, in which abscess formation occurred. The process was sustained by causative pathogen generating biofilm and resistant to antibiotic treatment [18,116,119,120,122,125]. Sometimes in the presence of aggressive IE with extension to the aorto-mitral junction and mitral valve, we used a double homograft valve implant [18,120,125,126,127,128,129,130]. During the cryopreservation process the homograft was processed in combination with the application of antibiotics (gentamicin, vancomycin, metronidazole, piperacillin, flucloxacillin, tobramycin, meropenem, colistin and antifungal amphotericin-B) which promoted a significant influence on the resistance of the allogeneic tissue to infections. To note that ascending aortic homograft tissue revealed significantly improved resistance against S epidermidis and S aureus with a lower propensity for bacterial contamination than homograft aortic valves. For the latter, the highest risk of bacterial biofilm formation persists, especially induced by staphylococcus aureus, which appear to be difficult to perforate. Along the same lines, more effective resistance was observed against P aeruginosa using flucloxacillin and E coli using meropenem and colistin [131]. Table 3
Table 3.
Characteristics of the Included Studies.
| First Author/Year Ref | Type of Study | Cohort | Aims | Finding |
|---|---|---|---|---|
| Schwartz et al (2021) APMIS [106] |
In vitro patch enriched with platelet and leucocyte-rich fibrin Multicenter (Danemark) |
IE organoid-like model by colonization with IE-associated bacterial isolates S. aureus, S. mitis and Enterococcus faecalis (IE vegetation (IEV) | To establish an in vitro vegetation simulation IE model for fast screening of novel treatment strategies | The surface-associated bacteria displayed increased tolerance to antibiotics compared to planktonic bacteria. IE simulation model with the relevant pathogens S. aureus, S. mitis group, and E. faecalis was established and IE model mirrors the natural IE process. |
| Di Domenico et al (2019) BMC Microbiol [107] |
Human Multicenter (IT) |
Samples of infected heart tissue. S. s aureus 50%, Enterococcus faecalis 25% and Streptococcus gallolyticus 25% | To assess a rapid biofilm identification assay and a targeted antimicrobial susceptibility profile of biofilm-growing bacteria in patients with IE, which were unresponsive to antibiotic therapy. | Biofilm-producing bacteria, from surgically treated IE, display a high tolerance to antibiotics, which is undetected by conventional antibiograms. |
| Schwartz et al (2012) APMIS [108] |
Animal model Multicenter (Danemark) |
IE organoid-like model by colonization with IE-associated bacterial isolates S. aureus, S. mitis and Enterococcus faecalis (IEV) | To evaluate the time course of biofilm formation and the impact on antibiotic tolerance development. | The antibiotic effect was significantly higher than when treatment was started after the biofilm was allowed to mature. |
| Kim et al (2016) JTCVS [113] |
Human Single Center (USA) |
86 pts Homografts Vs 139 pts Xenograft prostheses Vs 79 pts Mechanical prostheses |
To evaluate resistance to infection | Homografts were more used in PVE (P = .002) and methicillin-resistant Staphylococcus (P = .002), compared with conventional prostheses. No significant benefit to use of homografts was demonstrable with regard to resistance to reinfection in the setting of IE. |
| Nappi et al (2018) JTCVS [120] |
Human Single center (France) |
210 pts | To evaluate long-term results of aortic allografts and to identify factors influencing long-term durability. | The use of allograft is a valid option in complex infective endocarditis and in women of childbearing age |
| Steffen et al (2016) JTCVS. [131] |
In vitro Single center (Germany) |
10 cryopreserved human allografts | To evaluate the in vitro antimicrobial activity of 3 antibiotic regimens | Allograft antibacterial activity despite long-term storage over 5 years. Antibiotic combinations applied during CHA processing have a significant influence on their infection resistance. Ascending aortic tissue shows a significantly enhanced bacterial resistance against staphylococcal bacteria compared with aortic valves. |
Abbreviations ; IEV, infective endocarditis vegetation ; pts, patients ; PVE, prosthetic valve endocarditis ; S. aureus, staphylococcus aureus ; S. mitis, Streptococcus mitis
7. Conclusion
Several factors allow Staphylococcus aureus infections to proliferate within the host with numerous promoting and perpetuating agents with direct bacterial pathogenic activity predominating other factors such as rheumatic heart disease. This is further supported by the roles of teichoic and lipoteichoic acids within teichoic acid which favour host cell invasion. The complex interaction with the hosts' innate immunity also potentiates its virulence. The role of vaccines have not been successfully translated to the clinical setting thus far. Ameliorating these molecular pathways may serve as a therapeutic avenue for the prevention and treatment of these infections in the near future with antiplatelet agents showing promising results.
Supplementary Materials
https://www.mdpi.com/journal/biomedicines/special_issues/Endocarditis_IE. Supplementary Table S1: Prisma checklist 2020, reference [From: Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 2021;372: n71. doi: 10.1136/bmj. n71 http://www.prisma-statement.org/] is cited in supplementary materials.
Author Contributions
Conceptualization, F.N.; methodology, F.N. and S.S.A.S.; software, S.S.A.S.; validation, F.N. and S.S.A.S.; formal analysis, F.N. and S.S.A.S.; investigation, F.N.; data curation, F.N. and S.S.A.S.; writing—original draft preparation, F.N.; writing—review and editing, F.N. and S.S.A.S.; visualization, F.N. and S.S.A.S.; supervision, F.N. and S.S.A.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Selton-Suty C, Celard M, Le Moing V, Doco-Lecompte T, Chirouze C, Iung B, Strady C, Revest M, Vandenesch F, Bouvet A, Delahaye F, Alla F, Duval X, Hoen B; AEPEI Study Group. Preeminence of Staphylococcus aureus in infective endocarditis: a 1-year population-based survey. Clin Infect Dis 2012; 54: 1230–39. [CrossRef]
- Chen H, Zhan Y, Zhang K, Chen H, Zhan Y, Zhang K, Gao Y, Chen L, Zhan J, Chen Z, Zeng Z. The Global, Regional, and National Burden and Trends of Infective Endocarditis From 1990 to 2019: Results from the Global Burden of Disease Study 2019.Front Med (Lausanne). 2022 Mar 9 ;9 :774224. [CrossRef]
- Resende P Jr, Fortes CQ, do Nascimento EM, Sousa C, Querido Fortes NR, Thomaz DC, de Bragança Pereira B, Pinto FJ, de Oliveira GMM. In-hospital Outcomes of Infective Endocarditis from 1978 to 2015: Analysis Through Machine-Learning Techniques. CJC Open. 2021 Sep 11 ;4(2) :164-172. [CrossRef]
- Allegranzi B, Bagheri Nejad S, Combescure C, Graafmans W, Attar H, Donaldson L, Pittet D.. Burden of endemic health-care-associated infection in developing countries: systematic review and meta-analysis. Lancet 2011 ; 377 : 228–41. [CrossRef]
- Bagheri Nejad S, Allegranzi B, Syed SB, Ellis B, Pittet D. Health-care-associated infection in Africa: a systematic review. Bull World Health Organ. 2011 Oct 1 ;89(10):757-65. [CrossRef]
- Joubert D, Cullati S, Briot P, Righi L, Grauser D, Ourahmoune A, Chopard P. How to improve hospital admission screening for patients at risk of multidrug-resistant organism carriage: a before-and-after interventional study and cost-effectiveness analysis. BMJ Open Qual. 2022 Apr ;11(2): e001699. [CrossRef]
- Blair JMA, Webber MA, Baylay AJ, Ogbolu DO, Piddock LJV. Molecular mechanisms of antibiotic resistance. Nat Rev Microbiol 2015 ; 13 : 42–51.
- Martínez JL Antibiotics and antibiotic resistance genes in natural environments. Science. 2008 Jul 18 ;321(5887) :365-7.
- Yang M, Zhang J, Wei Y, Zhang J, Tao C Recent advances in metal-organic framework-based materials for anti-staphylococcus aureus infection. Nano Res. 2022 May 11 :1-23.
- McAdow M, Missiakas DM, Schneewind O. Staphylococcus aureus secretes coagulase and von Willebrand factor binding protein to modify the coagulation cascade and establish host infections. J Innate Immun. 2012 ;4(2) :141-8. [CrossRef]
- Thomer L, Schneewind O, Missiakas D. Multiple ligands of von Willebrand factor-binding protein (vWbp) promote Staphylococcus aureus clot formation in human plasma. J Biol Chem. 2013 Sep 27 ;288(39) :28283-92. [CrossRef]
- Nappi F, Martuscelli G, Bellomo F, Avtaar Singh SS, Moon MR Infective Endocarditis in High-Income Countries. Metabolites. 2022 Jul 25 ;12(8) :682. [CrossRef]
- Thomas S, Liu W, Arora S, Ganesh V, Ko YP, Höök. The Complex Fibrinogen Interactions of the Staphylococcus aureus Coagulases. Front Cell Infect Microbiol. 2019 Apr 16 ;9 :106. [CrossRef]
- Sinha B, Herrmann M. Mechanism and consequences of invasion of endothelial cells by Staphylococcus aureus. Thromb Haemost. 2005 Aug ;94(2) :266-77. [CrossRef]
- Thuny F, Di Salvo G, Belliard O, Avierinos JF, Pergola V, Rosenberg V, Casalta JP, Gouvernet J, Derumeaux G, Iarussi D, Ambrosi P, Calabró R, Riberi A, Collart F, Metras D, Lepidi H, Raoult D, Harle JR, Weiller PJ, Cohen A, Habib G.. Risk of embolism and death in infective endocarditis: prognostic value of echocardiography: a prospective multicenter study. Circulation 2005 ;112 :69-75. [Erratum, Circulation 2005 ;112(9) : e125.
- Di Salvo G, Habib G, Pergola V, Avierinos JF, Philip E, Casalta JP, Vailloud JM, Derumeaux G, Gouvernet J, Ambrosi P, Lambert M, Ferracci A, Raoult D, Luccioni R. Echocardiography predicts embolic events in infective endocarditis. J Am Coll Cardiol 2001 ;37 :1069-76. [CrossRef]
- Vilacosta I, Graupner C, San Román JA, Sarriá C, Ronderos R, Fernández C, Mancini L, Sanz O, Sanmartín JV, Stoermann W. Risk of embolization after institution of antibiotic therapy for infective endocarditis. J Am Coll Cardiol. 2002 May 1 ;39(9) :1489-95. [CrossRef]
- Nappi F, Spadaccio C, Dreyfus J, Attias D, Acar C, Bando K. Mitral endocarditis: A new management framework. J Thorac Cardiovasc Surg. 2018 Oct ;156(4) :1486-1495.e4. [CrossRef]
- Avtaar Singh SS, Costantino MF, D'Addeo G, Cardinale D, Fiorilli R, Nappi F. A narrative review of diagnosis of infective endocarditis-imaging methods and comparison. Ann Transl Med. 2020 Dec ;8(23) :1621. [CrossRef]
- Duval X, Iung B, Klein I, Thabut G, Arnoult F, Lepage L, Laissy JP, Wolff M, Leport C; IMAGE (Resonance Magnetic Imaging at the Acute Phase of Endocarditis) Study Group.. Effect of early cerebral magnetic resonance imaging on clinical decisions in infective endocarditis: a prospective study. Ann Intern Med 2010 ;152 :497-504.
- Béraud G, Tubiana S, Erpelding ML, Le Moing V, Chirouze C, Gorenne I, Manchon P, Tattevin P, Vernet V, Varon E, Hoen B, Duval X; AEPEI study group; COMBAT study group. . Combined Bacterial Meningitis and Infective Endocarditis: When Should We Search for the Other When Either One is Diagnosed? Infect Dis Ther. 2022 May 26.
- Vitali P, Savoldi F, Segati F, Melazzini L, et al. MRI versus CT in the detection of brain lesions in patients with infective endocarditis before or after cardiac surgery. Neuroradiology. 2022 May ;64(5) :905-913. [CrossRef]
- Corr P, Wright M, Handler LC. Endocarditis- related cerebral aneurysms: radiologic changes with treatment. AJNR Am J Neuroradiol 1995 ;16 :745-8.
- 24. Champey J, Pavese P, Bouvaist H, Maillet M, Kastler A, Boussat B, Francois P; and the investigator groups. Is brain angio-MRI useful in infective endocarditis management ? Eur J Clin Microbiol Infect Dis. 2016 Dec ;35(12) :2053-2058.
- Peters PJ, Harrison T, Lennox JL. A dangerous dilemma: management of infectious intracranial aneurysms complicating endocarditis. Lancet Infect Dis 2006 ;6 :742-8. [CrossRef]
- Serrano F, Guédon A, Saint-Maurice JP, et al. Endovascular treatment of infectious intracranial aneurysms complicating infective endocarditis: a series of 31 patients with 55 aneurysms. Neuroradiology. 2022 Feb ;64(2) :353-360. [CrossRef]
- Murdoch DR, Corey GR, Hoen B, Miró JM, Fowler VG Jr, Bayer AS, Karchmer AW, Olaison L, Pappas PA, Moreillon P, Chambers ST, Chu VH, Falcó V, Holland DJ, Jones P, Klein JL, Raymond NJ, Read KM, Tripodi MF, Utili R, Wang A, Woods CW, Cabell CH ; International Collaboration on Endocarditis-Prospective Cohort Study (ICE-PCS) Investigators. . Clinical presentation, etiology, and outcome of infective endocarditis in the 21st century: the International Collaboration on Endocarditis-Prospective Cohort Study. Arch Intern Med 2009; 169: 463–73.
- Liaqat W, Palaiodimos L, Li W, Karamanis D, Tahir A, Tzoumas A, Nagraj S, Tiwari N, Grushko M, Kokkinidis D, Gashi E, Leider J, Coyle C, Faillace RT. Epidemiologic and clinical characteristics of infective endocarditis: a single-center retrospective study in the Bronx, New York. Infection. 2022 Oct ;50(5):1349-1361. [CrossRef]
- Paul G, Ochs L, Hohmann C, Baldus S, Michels G, Meyer-Schwickerath C, Fätkenheuer G, Mader N, Wahlers T, Weber C, Jung N.. Surgical Procedure Time and Mortality in Patients with Infective Endocarditis Caused by Staphylococcus aureus or Streptococcus Species Clin Med. 2022 Apr 30 ;11(9):2538.
- Becker K, Heilmann C, Peters G. Coagulase-negative staphylococci. Clin Microbiol Rev 2014; 27: 870–926.
- López J, Revilla A, Vilacosta I, Villacorta E, González-Juanatey C, Gómez I, Rollán MJ, San Román JA.. Definition, clinical profile, microbiological spectrum, and prognostic factors of early-onset prosthetic valve endocarditis. Eur Heart J 2007; 28: 760–65. [CrossRef]
- Alonso-Valle H, Fariñas-Alvarez C, García-Palomo JD, et al. Clinical course and predictors of death in prosthetic valve endocarditis over a 20-year period. J Thorac Cardiovasc Surg 2010; 139: 887–93. [CrossRef]
- Xu Z, Chen L, Chen X, Tang A, Huang D, Pan Q, Fang Z. Prevalence and Molecular Characterization of Methicillin-Resistant Staphylococci Recovered from Public Shared Bicycles in China. Int J Environ Res Public Health. 2022 Apr 8 ;19(8) :4492. [CrossRef]
- Argemi X, Hansmann Y, Prola K, Prévost G. Coagulase-Negative Staphylococci Pathogenomics. Int J Mol Sci. 2019 Mar 11;20(5):1215. [CrossRef]
- Chu VH, Woods CW, Miro JM, Hoen B, Cabell CH, Pappas PA, Federspiel J, Athan E, Stryjewski ME, Nacinovich F, Marco F, Levine DP, Elliott TS, Fortes CQ, Tornos P, Gordon DL, Utili R, Delahaye F, Corey GR, Fowler VG Jr; International Collaboration on Endocarditis-Prospective Cohort Study Group. the International Collaboration on Endocarditis-Prospective Cohort Study Group. Emergence of coagulase-negative staphylococci as a cause of native valve endocarditis. Clin Infect Dis 2008; 46: 232–42.
- Chu VH, Miro JM, Hoen B, Cabell CH, Pappas PA, Jones P, Stryjewski ME, Anguera I, Braun S, Muñoz P, Commerford P, Tornos P, Francis J, Oyonarte M, Selton-Suty C, Morris AJ, Habib G, Almirante B, Sexton DJ, Corey GR, Fowler VG Jr. International Collaboration on Endocarditis-Prospective Cohort Study Group. Coagulase-negative staphylococcal prosthetic valve endocarditis--a contemporary update based on the International Collaboration on Endocarditis: prospective cohort study. Heart. 2009 Apr ;95(7) :570-6. [CrossRef]
- Alawad MJ, Ali GA, Goravey W. Underrecognized pathogen; Staphylococcus warneri-associated native mitral valve endocarditis in an immunocompetent host: A case report and literature review. Clin Case Rep. 2022 Apr 22 ;10(4): e05591. [CrossRef]
- Voigt A, Shalaby A, Saba S. Rising rates of cardiac rhythm management device infections in the United States: 1996 through 2003. J Am Coll Cardiol 2006 ;48 :590–1. [CrossRef]
- Traykov V, Blomström-Lundqvist C. Antibiotic-Eluting Envelopes for the Prevention of Cardiac Implantable Electronic Device Infections: Rationale, Efficacy, and Cost-Effectiveness. Front Cardiovasc Med. 2022 Mar 28 ;9 :855233. [CrossRef]
- Elad B, Perl L, Hamdan A, Yahav D, Atamna A, Shaked H, Rubchevsky V, Sharony R, Bernstine H, Shapira Y, Vaturi M, Ofek H, Sagie A, Kornowski R, Orvin K. The clinical value of the endocarditis team: insights from before and after guidelines implementation strategy. Infection. 2022 Feb ;50(1) :57-64. [CrossRef]
- Han HC, Hawkins NM, Pearman CM, Birnie DH, Krahn AD. Epidemiology of cardiac implantable electronic device infections: incidence and risk factors. Europace. 2021 Jun 23 ;23(23 Suppl 4): iv3-iv10. [CrossRef]
- Durante-Mangoni E, Bradley S, Selton-Suty C, et al, and the International Collaboration on Endocarditis Prospective Cohort Study Group. Current features of infective endocarditis in elderly patients: results of the International Collaboration on Endocarditis Prospective Cohort Study. Arch Intern Med 2008; 168: 2095–103.
- Zampino R, Iossa D, Ursi MP, Bertolino L, Karruli A, Molaro R, Esposito G, Vitrone M, D'Amico F, Albisinni R, Durante-Mangoni E, On Behalf Of The Monaldi Hospital CardiovascularInfection Group. Clinical Significance and Prognostic Value of Hemostasis Parameters in 337 Patients with Acute Infective Endocarditis. J Clin Med. 2021 Nov 18 ;10(22) :5386. [CrossRef]
- Molton JS, Tambyah PA, Ang BSP, Ling ML, Fisher DA. The global spread of healthcare-associated multidrug-resistant bacteria: a perspective from Asia. Clin Infect Dis 2013; 56: 1310–18. [CrossRef]
- Çaǧlayan Ç, Barnes SL, Pineles LL, Harris AD, Klein EY. A Data-Driven Framework for Identifying Intensive Care Unit Admissions Colonized With Multidrug-Resistant Organisms. Front Public Health. 2022 Mar 17; 10:853757. [CrossRef]
- Lockhart PB, Brennan MT, Sasser HC, Fox PC, Paster BJ, Bahrani-Mougeot FK. Bacteremia associated with toothbrushing and dental extraction. Circulation 2008; 117: 3118–25.
- Widmer E, Que YA, Entenza JM, Moreillon P. New concepts in the pathophysiology of infective endocarditis. Curr Infect Dis Rep 2006; 8: 271–79. [CrossRef]
- Moreillon P, Que YA, Bayer AS. Pathogenesis of streptococcal and staphylococcal endocarditis. Infect Dis Clin North Am. 2002 Jun ;16(2) :297-318. [CrossRef]
- Mancini S, Oechslin F, Menzi C, Que YA, Claes J, Heying R, Veloso TR, Vanassche T, Missiakas D, Schneewind O, Moreillon P, Entenza JM . Marginal role of von Willebrand factor-binding protein and coagulase in the initiation of endocarditis in rats with catheter-induced aortic vegetations. Virulence. 2018 ;9(1) :1615-1624. [CrossRef]
- Werdan K, Dietz S, Löffl B, Niemann S, Bushnaq H, Silber RE, Peters G, Müller-Werdan U.. Mechanisms of infective Endocarditis: pathogen-host interaction and risk states. Nat Rev Cardiol 2014; 11: 35–50. [CrossRef]
- Regueiro A, Linke A, Latib A, Urena M, Walther T, Husser O, Herrmann C, Nombela-Franco L, Cheema A, Le Breton H, Stortecky S, Kapadia S, Bartorelli L, Sinning JM, Amat-Santos I, Munoz-Garcia J, Lerakis S, Gutíerrez-Ibanes E, Abdel-Wahab M, Tchetche D, Testa L, Eltchaninoff H, et al. Infective Endocarditis Following Transcatheter Aortic Valve Replacement: Comparison of Balloon- Versus Self-Expandable Valves. Circ Cardiovasc Interv. 2019 Nov ;12(11): e007938.
- Rodríguez-Vidigal FF, Nogales-Asensio JM, Calvo-Cano A, et al. Infective endocarditis after transcatheter aortic valve implantation: Contributions of a single-centre experience on incidence and associated factors. Enferm Infecc Microbiol Clin (Engl Ed). 2019 Aug-Sep ;37(7):428-434. [CrossRef]
- Ciofu O, Moser C, Jensen PØ, Høiby N Tolerance and resistance of microbial biofilms. Nat Rev Microbiol. 2022 Feb 3.
- Annappah D, Saling M, Prodafikas J, Badie AN. Device-associated aortic valve endocarditis due to a complicated Enterobacter cloacae urinary tract infection. ID Cases. 2021 Dec 16 ;27: e01365. [CrossRef]
- Di Carluccio C, Forgione RE, Bosso A, et al.. Molecular recognition of sialoglycans by streptococcal Siglec-like adhesins: toward the shape of specific inhibitors. RSC Chem Biol. 2021 Oct 18 ;2(6) :1618-1630. [CrossRef]
- Manukumar H.M., Umesha S. MALDI-TOF-MS based identification and molecular characterization of food associated methicillin-resistant Staphylococcus aureus. Sci Rep. 2017 Sep 12 ;7(1) :11414. [CrossRef]
- Mempel M., Schnopp C., Hojka M, et al. Invasion of human keratinocytes by Staphylococcus aureus and intracellular bacterial persistence represent haemolysin-independent virulence mechanisms that are followed by features of necrotic and apoptotic keratinocyte cell death. Br J Dermatol. 2002 Jun ;146(6) :943-51. [CrossRef]
- Nakagawa S, Matsumoto M., Katayama, Y, et al. Staphylococcus aureus virulent PSMα peptides induce keratinocyte alarmin release to orchestrate IL-17-dependent skin inflammation. Cell Host Microbe 22, 667–677. 2017 Nov 8 ;22(5) :667-677.e5. [CrossRef]
- Fournier, B., Philpott, D.J. Recognition of Staphylococcus aureus by the innate immune system. Clin. Microbiol. Rev. 2005 Jul ;18(3) :521-40.
- Kawa T, Akira S. The role of pattern-recognition receptors in innate immunity: update on toll-like receptors. Nat. Immunol. 2010 May ;11(5) :373-84.
- Kupper T.S, Fuhlbrigge R.C. Immune surveillance in the skin: mechanisms and clinical consequences. Nat. Rev. Immunol. 2004 Mar ;4(3) :211-22. [CrossRef]
- Nestle F.O, Di M.P, Qin, J.Z., Nickoloff, B.J. Skin immune sentinels in health and disease. Nat. Rev. Immunol. 2009 Oct ;9(10) :679-91. [CrossRef]
- Schwarz C, Töre Y, Hoesker V, et al. Host-pathogen interactions of clinical S. aureus isolates to induce infective endocarditis. Virulence. 2021 Dec ;12(1) :2073-2087.
- 64. Malachowa N, Whitney A.R., Kobayashi S.D, et al. Global changes in Staphylococcus aureus gene expression in human blood. PLoS One 6, e18617. 2011 Apr 15 ;6(4) : e18617. [CrossRef]
- Alonzo 3rd F, Kozhaya, L., Rawlings S.A, et al. CCR5 is a receptor for Staphylococcus aureus leukotoxin ED. Nature 2013 Jan 3 ;493(7430):51-5.
- Alonzo 3rd F, Torres V.J. Bacterial survival amidst an immune onslaught: the contribution of the Staphylococcus aureus leukotoxins. PLoS Pathog. 2013 Feb ;9(2) : e1003143.
- Cheung G.Y, Joo H.S, Chatterjee S.S. et al. Phenol-soluble modulins–critical determinants of staphylococcal virulence. FEMS Microbiol. Rev. 2014 Jul ;38(4) :698-719. [CrossRef]
- Berube BJ, Bubeck Wardenburg J. Staphylococcus aureus α-toxin: nearly a century of intrigue. Toxins (Basel). 2013 Jun ;5(6) :1140-66. [CrossRef]
- Foster TJ. Immune evasion by staphylococci. Nat Rev Microbiol. 2005 Dec ;3(12) :948-58. [CrossRef]
- Silverman GJ, Goodyear CS. Confounding B-cell defences: lessons from a staphylococcal superantigen. Nat Rev Immunol. 2006 Jun ;6(6) :465-75. [CrossRef]
- Kim HK, Cheng AG, Kim HY, Missiakas DM, Schneewind O. Nontoxigenic protein A vaccine for methicillin-resistant Staphylococcus aureus infections in mice. J Exp Med. 2010 Aug 30 ;207(9) :1863-70. [CrossRef]
- Becker S, Frankel MB, Schneewind O, Missiakas D. Release of protein A from the cell wall of Staphylococcus aureus. Proc Natl Acad Sci U S A. 2014 Jan 28 ;111(4) :1574-9. [CrossRef]
- Zhang X, Marichannegowda MH, Rakesh KP, Qin HL. Master mechanisms of Staphylococcus aureus: consider its excellent protective mechanisms hindering vaccine development! Microbiol Res. 2018 Jul-Aug ;212-213 :59-66.
- Zhang BZ, Hua YH, Yu B, Cai JP, Zheng SY, Yam WC, Kao RY, Sze KH, Zheng BJ, Yuen KY, Huang JD. Recombinant ESAT-6-like proteins provoke protective immune responses against invasive Staphylococcus aureus disease in a murine model. Infect Immun. 2015 Jan ;83(1) :339-45. [CrossRef]
- Brady RA, Mocca CP, Prabhakara R, Plaut RD, Shirtliff ME, Merkel TJ, Burns DL. Evaluation of genetically inactivated alpha toxin for protection in multiple mouse models of Staphylococcus aureus infection. PLoS One. 2013 Apr 29 ;8(4): e63040. [CrossRef]
- Zhang F, Ledue O, Jun M, Goulart C, Malley R, Lu YJ. Protection against Staphylococcus aureus Colonization and Infection by B- and T-Cell-Mediated Mechanisms. mBio. 2018 Oct 16 ;9(5): e01949-18. [CrossRef]
- Yu W, Yao D, Yu S, Wang X, Li X, Wang M, Liu S, Feng Z, Chen X, Li W, Wang L, Liu W, Ma J, Yu L, Tong C, Song B, Cui Y. Protective humoral and CD4+ T cellular immune responses of Staphylococcus aureus vaccine MntC in a murine peritonitis model. Sci Rep. 2018 Feb 26 ;8(1) :3580. [CrossRef]
- Que Y-A, Haefliger J-A, Piroth L, François P, Widmer E, Entenza JM, Sinha B, Herrmann M, Francioli P, Vaudaux P, Moreillon P. Fibrinogen and fibronectin binding cooperate for valve infection and invasion in Staphylococcus aureus experimental endocarditis. J Exp Med 2005; 201: 1627–35. [CrossRef]
- Edwards AM, Bowden MG, Brown EL, Laabei M, Massey RC. Staphylococcus aureus extracellular adherence protein triggers TNFα release, promoting attachment to endothelial cells via protein A. PLoS One 2012; 7: e43046.
- Fitzgerald JR, Foster TJ, Cox D. The interaction of bacterial pathogens with platelets. Nat Rev Microbiol 2006; 4: 445–57.
- Veloso TR, Chaouch A, Roger T, Giddey M, Vouillamoz J, Majcherczyk P, Que YA, Rousson V, Moreillon P, Entenza JM. Use of a human-like low-grade bacteremia model of experimental endocarditis to study the role of Staphylococcus aureus adhesins and platelet aggregation in early endocarditis. Infect Immun 2013; 81: 697–703. [CrossRef]
- Thomas S, Arora S, Liu W, Churion K, Wu Y, Höök M. vhp Is a Fibrinogen-Binding Protein Related to vWbp in Staphylococcus aureus. mBio. 2021 Aug 31 ;12(4): e0116721. [CrossRef]
- Hussain M, Haggar A, Heilmann C, et al. Insertional inactivation of Eap in Staphylococcus aureus strain Newman confers reduced staphylococcal binding to fibroblasts. Infect Immun. 2002 Jun ;70(6) :2933-40. [CrossRef]
- Palankar R, Binsker U, Haracska B, et al. Interaction between the Staphylococcus aureus extracellular adherence protein Eap and its subdomains with platelets. Int J Med Microbiol. 2018 Aug ;308(6):683-691. [CrossRef]
- Hussain M, Haggar A, Peters G, et al. More than one tandem repeat domain of the extracellular adherence protein of Staphylococcus aureus is required for aggregation, adherence, and host cell invasion but not for leukocyte activation. Infect Immun. 2008 Dec ;76(12) :5615-23.
- Harraghy N, Hussain M, Haggar A, et al. The adhesive and immunomodulating properties of the multifunctional Staphylococcus aureus protein Eap. Microbiology (Reading). 2003 Oct ;149(Pt 10):2701-2707. [CrossRef]
- Flemming H-C, Wingender J. The biofilm matrix. Nat Rev Microbiol 2010; 8: 623–33.
- Heying R, van de Gevel J, Que YA, Moreillon P, Beekhuizen H Fibronectin-binding proteins and clumping factor A in Staphylococcus aureus experimental endocarditis: FnBPA is sufficient to activate human endothelial cells. Thromb Haemost. 2007 Apr ;97(4) :617-26.
- Piroth L, Que YA, Widmer E, et al. The fibrinogen- and fibronectin-binding domains of Staphylococcus aureus fibronectin-binding protein A synergistically promote endothelial invasion and experimental endocarditis. Infect Immun. 2008 Aug ;76(8) :3824-31. [CrossRef]
- Claes J, Vanassche T, Peetermans M, et al. Adhesion of Staphylococcus aureus to the vessel wall under flow is mediated by von Willebrand factor-binding protein. Blood. 2014 Sep 4 ;124(10) :1669-76. [CrossRef]
- Pappelbaum KI, Gorzelanny C, Grässle S, et al. Ultralarge von Willebrand factor fibers mediate luminal Staphylococcus aureus adhesion to an intact endothelial cell layer under shear stress. Circulation. 2013 Jul 2 ;128(1):50-9. [CrossRef]
- Claes J, Liesenborghs L, Peetermans M, et al. Clumping factor, A, von Willebrand factor-binding protein and von Willebrand factor anchor Staphylococcus aureus to the vessel wall. J Thromb Haemost. 2017 May ;15(5) :1009-1019.
- Claes J, Ditkowski B, Liesenborghs L, et al. Assessment of the Dual Role of Clumping Factor A in S. Aureus Adhesion to Endothelium in Absence and Presence of Plasma. Thromb Haemost. 2018 Jul ;118(7) :1230-1241. [CrossRef]
- Ko YP, Kang M, Ganesh VK, Ravirajan D, Li B, Höök M. Coagulase and Efb of Staphylococcus aureus Have a Common Fibrinogen Binding Motif. mBio. 2016 Jan 5 ;7(1) : e01885-15. [CrossRef]
- Foster TJ. The remarkably multifunctional fibronectin binding proteins of Staphylococcus aureus. Eur J Clin Microbiol Infect Dis. 2016 Dec ;35(12) :1923-1931. [CrossRef]
- Ahmed S, Meghji S, Williams RJ, Henderson B, Brock JH, Nair SP. Staphylococcus aureus fibronectin binding proteins are essential for internalization by osteoblasts but do not account for differences in intracellular levels of bacteria. Infect Immun. 2001 May ;69(5) :2872-7. [CrossRef]
- Massey RC, Kantzanou MN, Fowler T, Day NP, Schofield K, Wann ER, Berendt AR, Höök M, Peacock SJ.. Fibronectin-binding protein A of Staphylococcus aureus has multiple, substituting, binding regions that mediate adherence to fibronectin and invasion of endothelial cells. Cell Microbiol. 2001 Dec ;3(12) :839-51. [CrossRef]
- Ridley RA, Douglas I, Whawell SA. Differential adhesion and invasion by Staphylococcus aureus of epithelial cells derived from different anatomical sites. J Med Microbiol. 2012 Dec ;61(Pt 12) :1654-1661. [CrossRef]
- Niemann S, Nguyen MT, Eble JA, Chasan AI, Mrakovcic M, Böttcher RT, Preissner KT, Roßlenbroich S, Peters G, Herrmann M. More Is Not Always Better-the Double-Headed Role of Fibronectin in Staphylococcus aureus Host Cell Invasion. mBio. 2021 Oct 26 ;12(5): e0106221. [CrossRef]
- Pietrocola G, Pellegrini A, Alfeo MJ, Marchese L, Foster TJ, Speziale P.. The iron-regulated surface determinant B (IsdB) protein from Staphylococcus aureus acts as a receptor for the host protein vitronectin. J Biol Chem. 2020 Jul 17 ;295(29) :10008-10022. [CrossRef]
- Alfeo MJ, Pagotto A, Barbieri G, Foster TJ, Vanhoorelbeke K, De Filippis V, Speziale P, Pietrocola G. Staphylococcus aureus iron-regulated surface determinant B (IsdB) protein interacts with von Willebrand factor and promotes adherence to endothelial cells. Sci Rep. 2021 Nov 23 ;11(1) :22799. [CrossRef]
- Leeten K, Jacques N, Lancellotti P, Oury C Aspirin or Ticagrelor in Staphylococcus aureus Infective Endocarditis: Where Do We Stand? Front Cell Dev Biol. 2021 Oct 7 ;9 :716302.
- Ditkowski B, Bezulska-Ditkowska M, Jashari R, et al Antiplatelet therapy abrogates platelet-assisted Staphylococcus aureus infectivity of biological heart valve conduits. Congenital Cardiology and Cardiac Surgery Group. J Thorac Cardiovasc Surg. 2021 Jun ;161(6): e457-e472.
- Hannachi N, Habib G, Camoin-Jau L Aspirin Effect on Staphylococcus aureus-Platelet Interactions During Infectious Endocarditis. Front Med (Lausanne). 2019 Oct 15 ;6 :217.
- Park, E. Na HS, Song YR, Shin SY, Kim YM, Chung J. Activation of NLRP3 and AIM2 inflammasomes by Porphyromonas gingivalis infection. Infect Immun. 2014 Jan ;82(1):112-23. [CrossRef]
- Schwartz FA, Christophersen L, Laulund AS, Lundquist R, Lerche C, Rude Nielsen P, Bundgaard H, Høiby N, Moser C. Novel human in vitro vegetation simulation model for infective endocarditis. APMIS. 2021 Nov ;129(11) :653-662. [CrossRef]
- Di Domenico EG, Rimoldi SG, Cavallo I et al. Microbial biofilm correlates with an increased antibiotic tolerance and poor therapeutic outcome in infective endocarditis. BMC Microbiol. 2019 Oct 21 ;19(1) :228. [CrossRef]
- Schwartz FA, Nielsen L, Struve Andersen J, Bock M, Christophersen L, Sunnerhagen T, Lerche CJ, Bay L, Bundgaard H, Høiby N, Moser C. Dynamics of a Staphylococcus aureus infective endocarditis simulation model. APMIS. 2022 Apr 23. [CrossRef]
- Nappi F, Avtaar Singh SS, Timofeeva I. Learning From Controversy: Contemporary Surgical Management of Aortic Valve Endocarditis. Clin Med Insights Cardiol. 2020 Sep 28 ;14 :1179546820960729. [CrossRef]
- Nappi F, Singh SSA, Nappi P, Spadaccio C, Nenna A, Gentile F, Chello M. Heart Valve Endocarditis. Surg Technol Int. 2020 Nov 28 ;37 :203-215.
- Nappi F, Singh SSA, Spadaccio C, Acar C. Revisiting the guidelines and choice the ideal substitute for aortic valve endocarditis. Ann Transl Med. 2020 Aug;8(15):952. [CrossRef]
- Nappi F, Iervolino A, Singh SSA. The New Challenge for Heart Endocarditis: From Conventional Prosthesis to New Devices and Platforms for the Treatment of Structural Heart Disease. Biomed Res Int. 2021 Jun 14; 2021:7302165. doi: 10.1155/2021/7302165. eCollection 2021. [CrossRef]
- Kim JB, Ejiofor JI, Yammine M, Camuso JM, Walsh CW, Ando M, et al. The Journal of Thoracic and Cardiovascular Surgery. 2016;151(5):1239-48. e2. [CrossRef]
- Perrotta S, Jeppsson A, Fröjd V, Svensson G. Surgical Treatment of Aortic Prosthetic Valve Endocarditis: A 20-Year Single-Center Experience. The Annals of Thoracic Surgery. 2016;101(4):1426-32. [CrossRef]
- David TE, Gavra G, Feindel CM, Regesta T, Armstrong S, Maganti MD. Surgical treatment of active infective endocarditis: a continued challenge. J Thorac Cardiovasc Surg. 2007;133(1):144-9.
- Nappi F, Spadaccio C, Acar C. Use of allogeneic tissue to treat infective valvular disease: Has everything been said? J Thorac Cardiovasc Surg. 2017;153(4):824-8.
- Brouqui P, Raoult D. Endocarditis due to rare and fastidious bacteria. Clin Microbiol Rev. 2001;14(1):177-207.
- Kim JB, Ejiofor JI, Yammine M, Ando M, Camuso JM, Youngster I, et al. Surgical outcomes of infective endocarditis among intravenous drug users. The Journal of Thoracic and Cardiovascular Surgery. 2016;152(3):832-41. e1. [CrossRef]
- Nappi F, Spadaccio C. Simplest solutions are not always the cleverest: Can we stitch in an infected annulus? Should we rethink the current guidelines? J Thorac Cardiovasc Surg. 2017;154(6):1899-900.
- Nappi F, Nenna A, Petitti T, Spadaccio C, Gambardella I, Lusini M, et al. Long-term outcome of cryopreserved allograft for aortic valve replacement. J Thorac Cardiovasc Surg. 2018 ;156(4) :1357-65 e6. [CrossRef]
- Arabkhani B, Bekkers JA, Andrinopoulou E-R, Roos-Hesselink JW, Takkenberg JJM, Bogers AJJC. Allografts in aortic position: Insights from a 27-year, single-center prospective study. The Journal of Thoracic and Cardiovascular Surgery. 2016;152(6):1572-9. e3. [CrossRef]
- Nappi F. CRT-721 The Cryopreserved Mitral Homograft Valve: 19 Years’ Experience. JACC: Cardiovascular Interventions. 2014;7(2 Supplement): S58. [CrossRef]
- Fukushima S, Tesar PJ, Pearse B, Jalali H, Sparks L, Fraser JF, et al. Long-term clinical outcomes after aortic valve replacement using cryopreserved aortic allograft. J Thorac Cardiovasc Surg. 2014;148(1):65-72. e2. [CrossRef]
- O'Brien MF, Harrocks S, Stafford EG, Gardner MA, Pohlner PG, Tesar PJ, et al. The homograft aortic valve: a 29-year, 99.3% follow up of 1,022 valve replacements. J Heart Valve Dis. 2001;10(3):334-44; discussion 5.
- Olivito S, Lalande S, Nappi F, Hammoudi N, D'Alessandro C, Fouret P, et al. Structural deterioration of the cryopreserved mitral homograft valve. J Thorac Cardiovasc Surg. 2012;144(2):313-20, 20.e1. [CrossRef]
- Nappi F, Singh SSA, Lusini M, Nenna A, Gambardella I, Chello M. The use of allogenic and autologous tissue to treat aortic valve endocarditis. Annals of Translational Medicine. 2019;7(18):68. [CrossRef]
- Nappi F, Acar C. Monobloc or Separate Aortic and Mitral Homografts for Endocarditis of the Intervalvular Fibrosa? Ann Thorac Surg. 2021 Oct;112(4):1382-1383. [CrossRef]
- Nappi F, Spadaccio C, Moon MR A management framework for left sided endocarditis: a narrative review. Ann Transl Med. 2020 Dec;8(23):1627. [CrossRef]
- Benedetto U, Spadaccio C, Gentile F, Moon MR, Nappi F. A narrative review of early surgery versus conventional treatment for infective endocarditis: do we have an answer? Ann Transl Med. 2020 Dec;8(23):1626. [CrossRef]
- Pollari F, Spadaccio C, Cuomo M, Chello M, Nenna A, Fischlein T, Nappi F. Sharing of decision-making for infective endocarditis surgery: a narrative review of clinical and ethical implications. Ann Transl Med. 2020 Dec;8(23):1624. [CrossRef]
- Steffen V, Marsch G, Burgwitz K, Kuehn C, Teebken OE. Resistance to infection of long-term cryopreserved human aortic valve allografts. J Thorac Cardiovasc Surg. 2016;151(5):1251-9. [CrossRef]
Figure 1.
PRISMA 2021 Flow diagram for new systematic review which include searches of database and registers only.
Figure 1.
PRISMA 2021 Flow diagram for new systematic review which include searches of database and registers only.
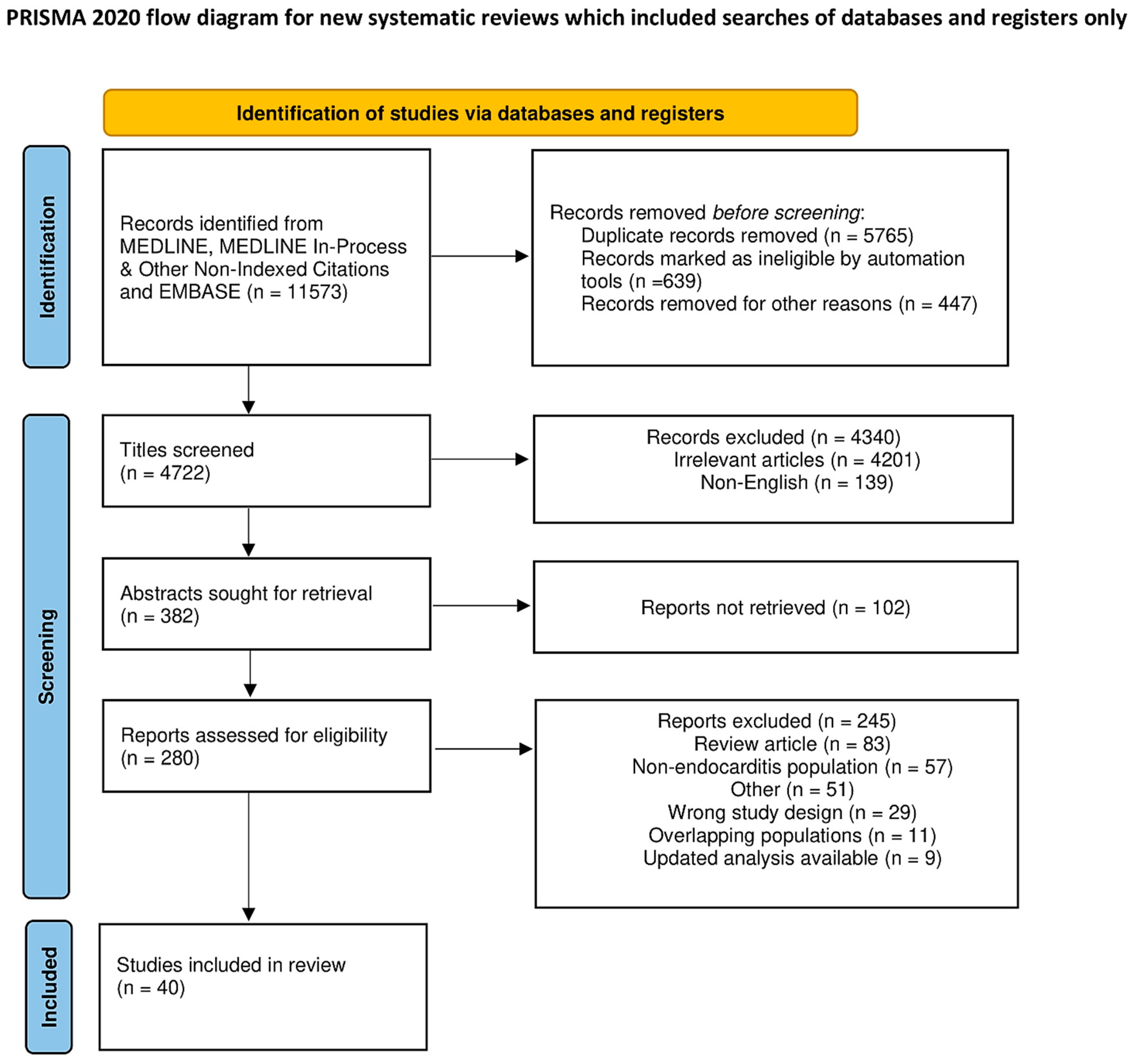
Figure 2.
The bacterial adhesion is the first pathophysiological process leading to IE. The involvement of inflammatory cells (PMN, monocyte, and macrophage) occurs in the first phase which is supported by the production of cytokines (TNF, α, interleukine 1,6 and 8), integrins, tissue factor, adhesion molecules (ICAM, VCAM). These mediators of inflammation attract monocytes and platelets with the associated production of fibronectin, due to the effect induced by chemokines. S Aureus releases cytotoxins that trigger the immune response both innate and mediate (T-cell and B- cell). Abbreviations; ICAM, IE, infective endocarditis; Inter Cellular Adhesion Molecule; S. Aureus, staphylococcus aureus; TNF, tumor necrosis factor; VCAM, vascular cell adhesion molecule.
Figure 2.
The bacterial adhesion is the first pathophysiological process leading to IE. The involvement of inflammatory cells (PMN, monocyte, and macrophage) occurs in the first phase which is supported by the production of cytokines (TNF, α, interleukine 1,6 and 8), integrins, tissue factor, adhesion molecules (ICAM, VCAM). These mediators of inflammation attract monocytes and platelets with the associated production of fibronectin, due to the effect induced by chemokines. S Aureus releases cytotoxins that trigger the immune response both innate and mediate (T-cell and B- cell). Abbreviations; ICAM, IE, infective endocarditis; Inter Cellular Adhesion Molecule; S. Aureus, staphylococcus aureus; TNF, tumor necrosis factor; VCAM, vascular cell adhesion molecule.
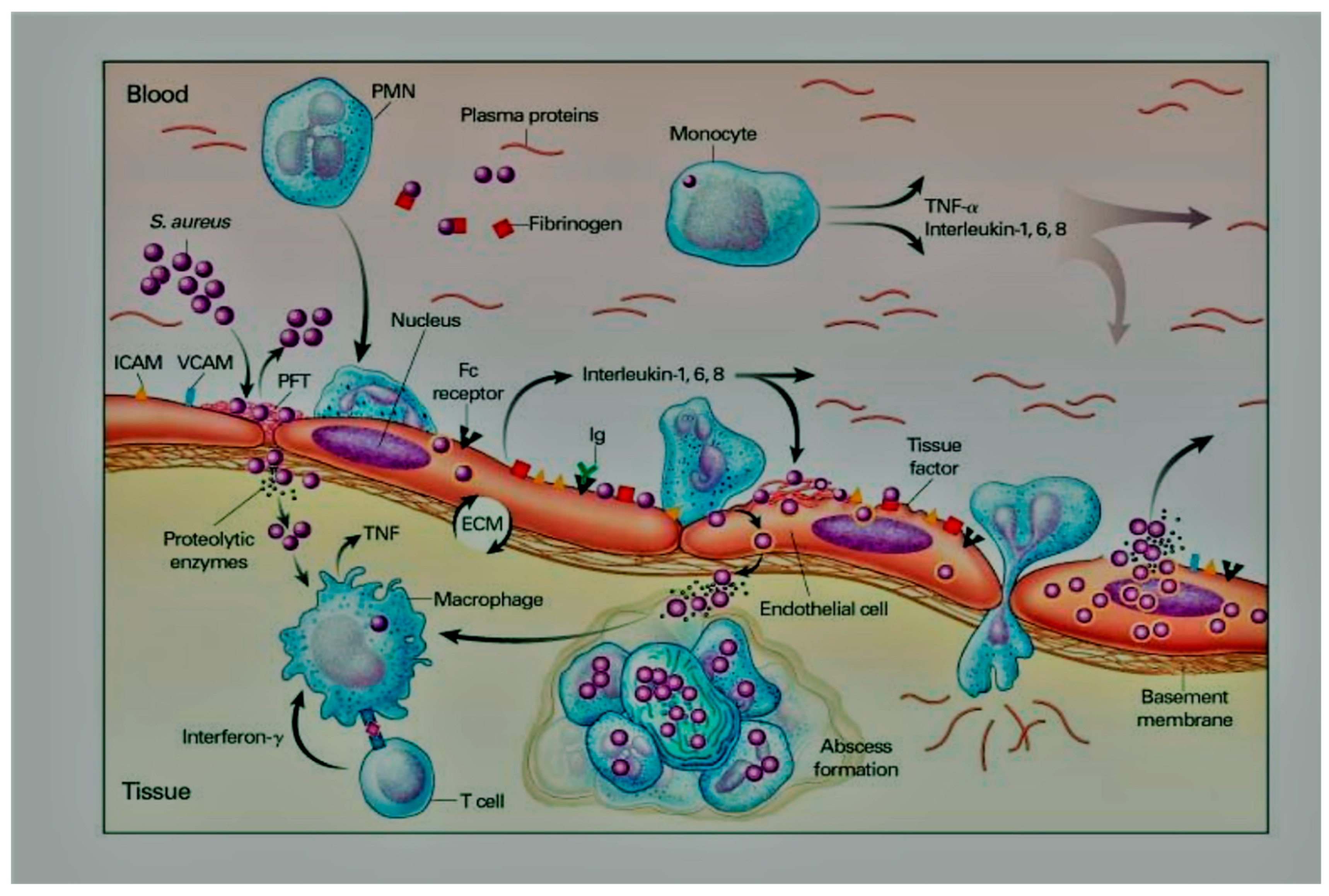
Figure 3.
Staphylocytotoxins interfere (great red arrow) with the cells of the innate (purple box) and adaptive (brown box) immune response. Cytotoxins (TSS-1, Staphylococcal endotoxin, and alpha toxin) can induce lysis of immune cells including PMN, monocytes, and macrophages involved in the clearance of S. aureus (small red arrow). Cytotoxins can also impair the function of adaptive immune cells (green arrows) represented by T and B lymphocytes. Finally, cytotoxins can impair the interaction between innate and adaptive immune cells (blue arrows). Abbreviation; PMN, polymorphonuclear; TSS-1, Toxic Shock Syndrome-1.
Figure 3.
Staphylocytotoxins interfere (great red arrow) with the cells of the innate (purple box) and adaptive (brown box) immune response. Cytotoxins (TSS-1, Staphylococcal endotoxin, and alpha toxin) can induce lysis of immune cells including PMN, monocytes, and macrophages involved in the clearance of S. aureus (small red arrow). Cytotoxins can also impair the function of adaptive immune cells (green arrows) represented by T and B lymphocytes. Finally, cytotoxins can impair the interaction between innate and adaptive immune cells (blue arrows). Abbreviation; PMN, polymorphonuclear; TSS-1, Toxic Shock Syndrome-1.
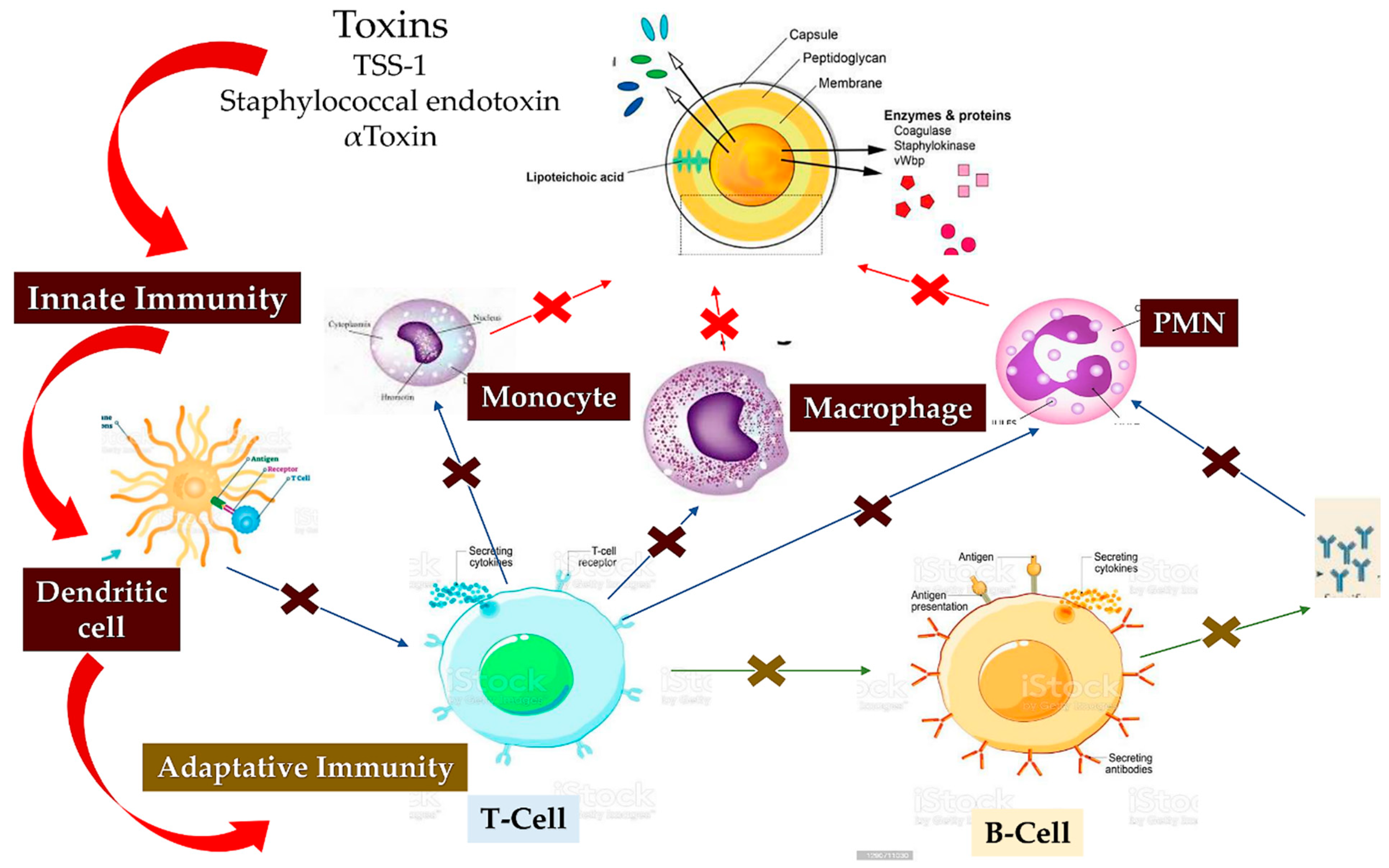
Figure 4.
Virulent factors of S. aureus are reported. MSCRAMMs drive with a substantial key role in the initiation of endovascular, bone, and joint, alongside prosthetic-device infections. These structures can bind to molecules such as collagen (mostly via Cna), fibronectin (via FnbAB), and fibrinogen (with ClfAB and Fib) and thus evade the immune system. The development of infection is induced by Coa and von Willebrand factor binding protein that led to critical virulence. Coa binds preferentially soluble fibrinogen while vWbp did not disclose any preference between the two forms of fibrinogen. Abbreviations; Coa, coagulase; MSCRAMM, microbial surface components recognizing adhesive matrix molecules; vWbp, von Willebrand factor binding protein.
Figure 4.
Virulent factors of S. aureus are reported. MSCRAMMs drive with a substantial key role in the initiation of endovascular, bone, and joint, alongside prosthetic-device infections. These structures can bind to molecules such as collagen (mostly via Cna), fibronectin (via FnbAB), and fibrinogen (with ClfAB and Fib) and thus evade the immune system. The development of infection is induced by Coa and von Willebrand factor binding protein that led to critical virulence. Coa binds preferentially soluble fibrinogen while vWbp did not disclose any preference between the two forms of fibrinogen. Abbreviations; Coa, coagulase; MSCRAMM, microbial surface components recognizing adhesive matrix molecules; vWbp, von Willebrand factor binding protein.
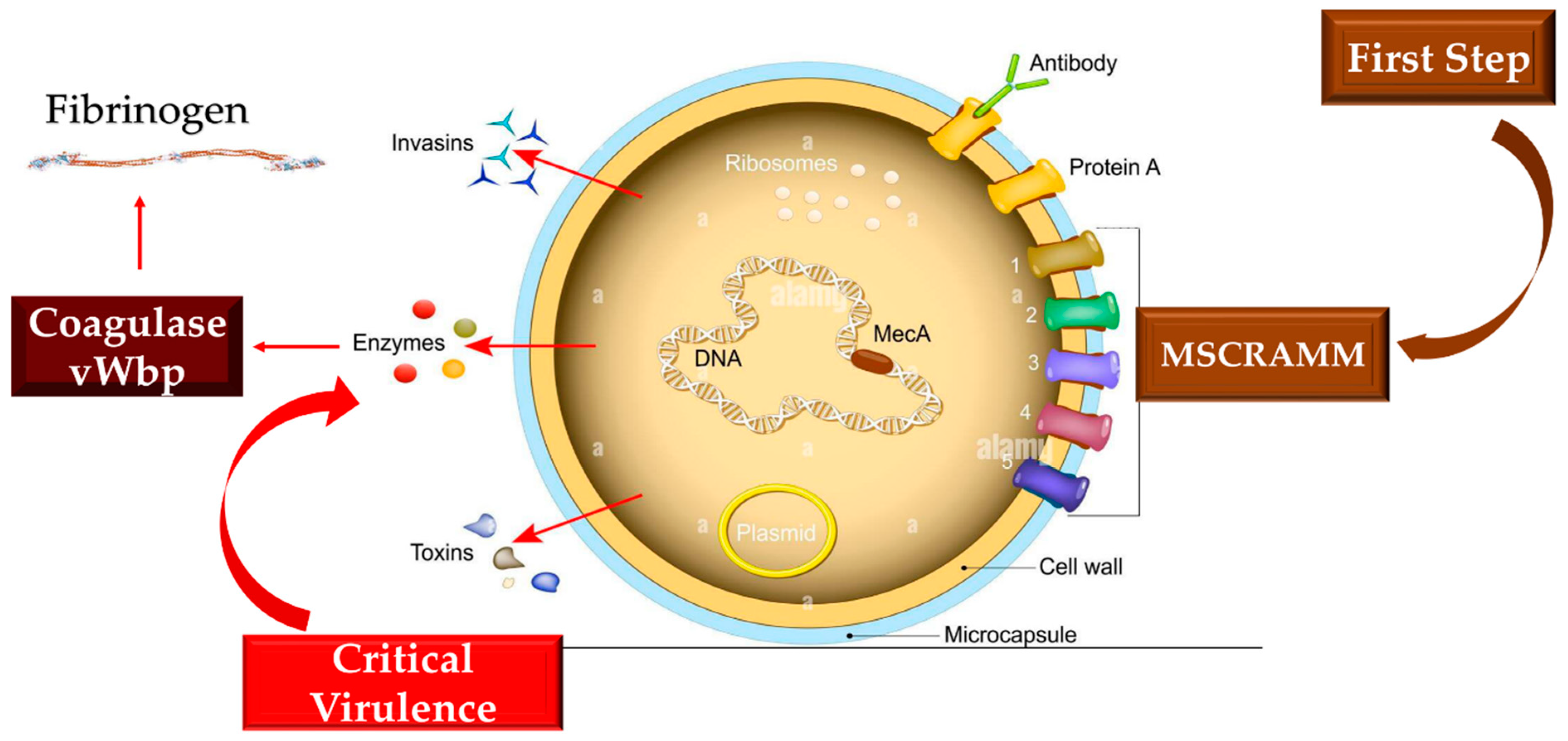
Figure 5.
The distinctive pathogenic action of Staphylococcus Aureus on the heart and endothelial cells is shown and involves three crucial stages: increased inflammatory response (blue box), adhesion and internalization of the pathogen (green box), and development of an active immune response (brown box). The external envelope of S Aureus, consisting of the cell wall and peptidoglycans, expresses the different molecules involved in the three pathophysiological processes. Abbreviations; αVβ3, integrin alpha V and integrin beta 3 (CD61); Atl, autolysin; Clfa, clumping factor A: FnBP, fibronectin-binding protein; Hsc70, Heat shock cognate; Hsp60, Heat shock protein; SdrD, Serine Aspartate repeat containing protein D; TLR2, Toll-like receptor 2; TNFR1, tumor necrosis factor receptor 1.
Figure 5.
The distinctive pathogenic action of Staphylococcus Aureus on the heart and endothelial cells is shown and involves three crucial stages: increased inflammatory response (blue box), adhesion and internalization of the pathogen (green box), and development of an active immune response (brown box). The external envelope of S Aureus, consisting of the cell wall and peptidoglycans, expresses the different molecules involved in the three pathophysiological processes. Abbreviations; αVβ3, integrin alpha V and integrin beta 3 (CD61); Atl, autolysin; Clfa, clumping factor A: FnBP, fibronectin-binding protein; Hsc70, Heat shock cognate; Hsp60, Heat shock protein; SdrD, Serine Aspartate repeat containing protein D; TLR2, Toll-like receptor 2; TNFR1, tumor necrosis factor receptor 1.
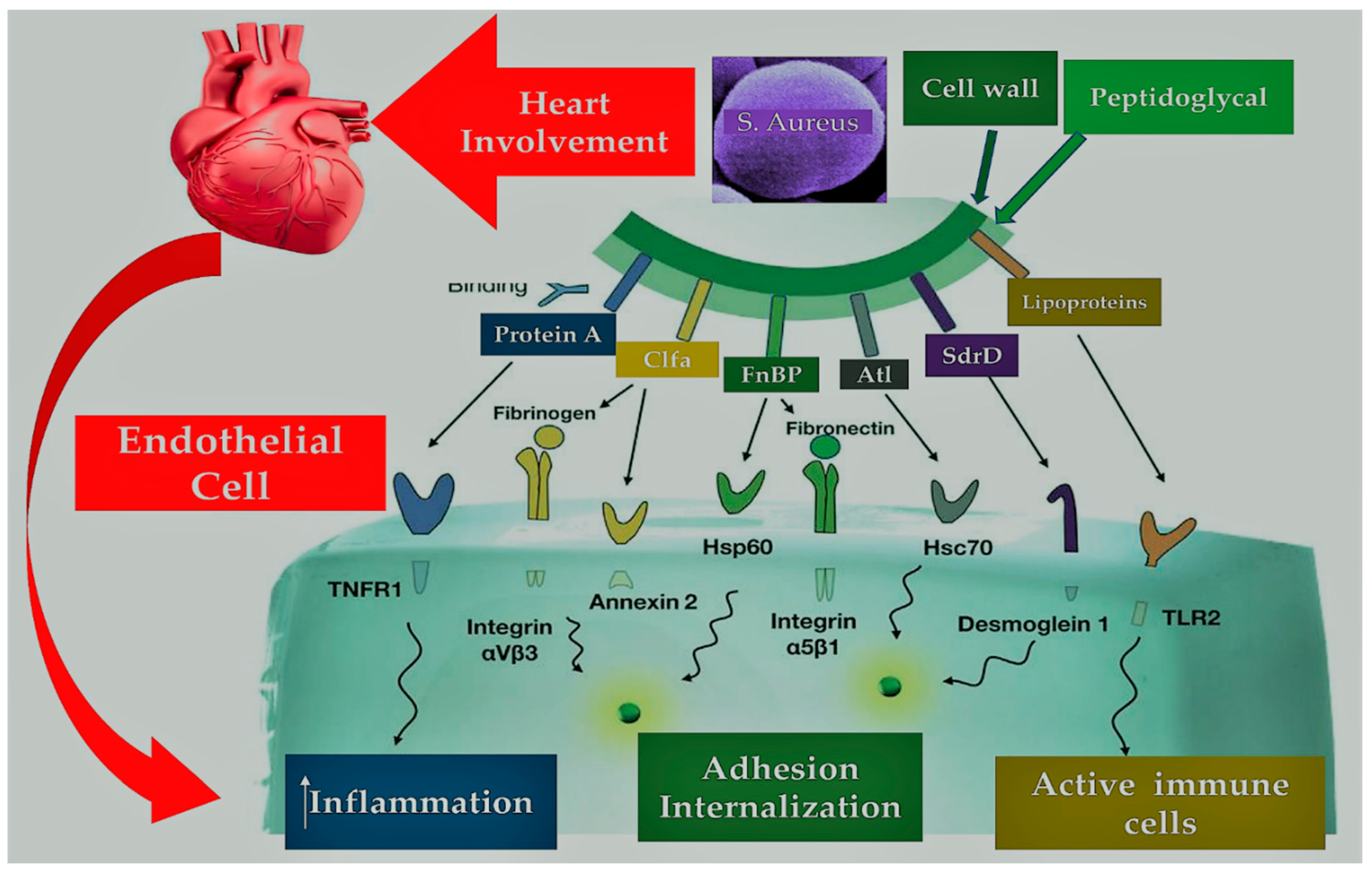
Figure 6.
Experimental endocarditis caused by Staphylococcus aureus marked the crucial function of sequential fibrinogen binding responsible for valve colonization and the paramount action of fibronectin-binding that promotes leading endothelial invasion. FnBPA responsible for fibrinogen and fibronectin binding may lead to cell invasion in vivo endocarditis. Abbreviations; Akt or PKB, protein kinase B, FAK, focal adhesion kinase; P13-k, Phosphoinositide 3-kinase; Src, proto-oncogene tyrosine-protein kinase.
Figure 6.
Experimental endocarditis caused by Staphylococcus aureus marked the crucial function of sequential fibrinogen binding responsible for valve colonization and the paramount action of fibronectin-binding that promotes leading endothelial invasion. FnBPA responsible for fibrinogen and fibronectin binding may lead to cell invasion in vivo endocarditis. Abbreviations; Akt or PKB, protein kinase B, FAK, focal adhesion kinase; P13-k, Phosphoinositide 3-kinase; Src, proto-oncogene tyrosine-protein kinase.
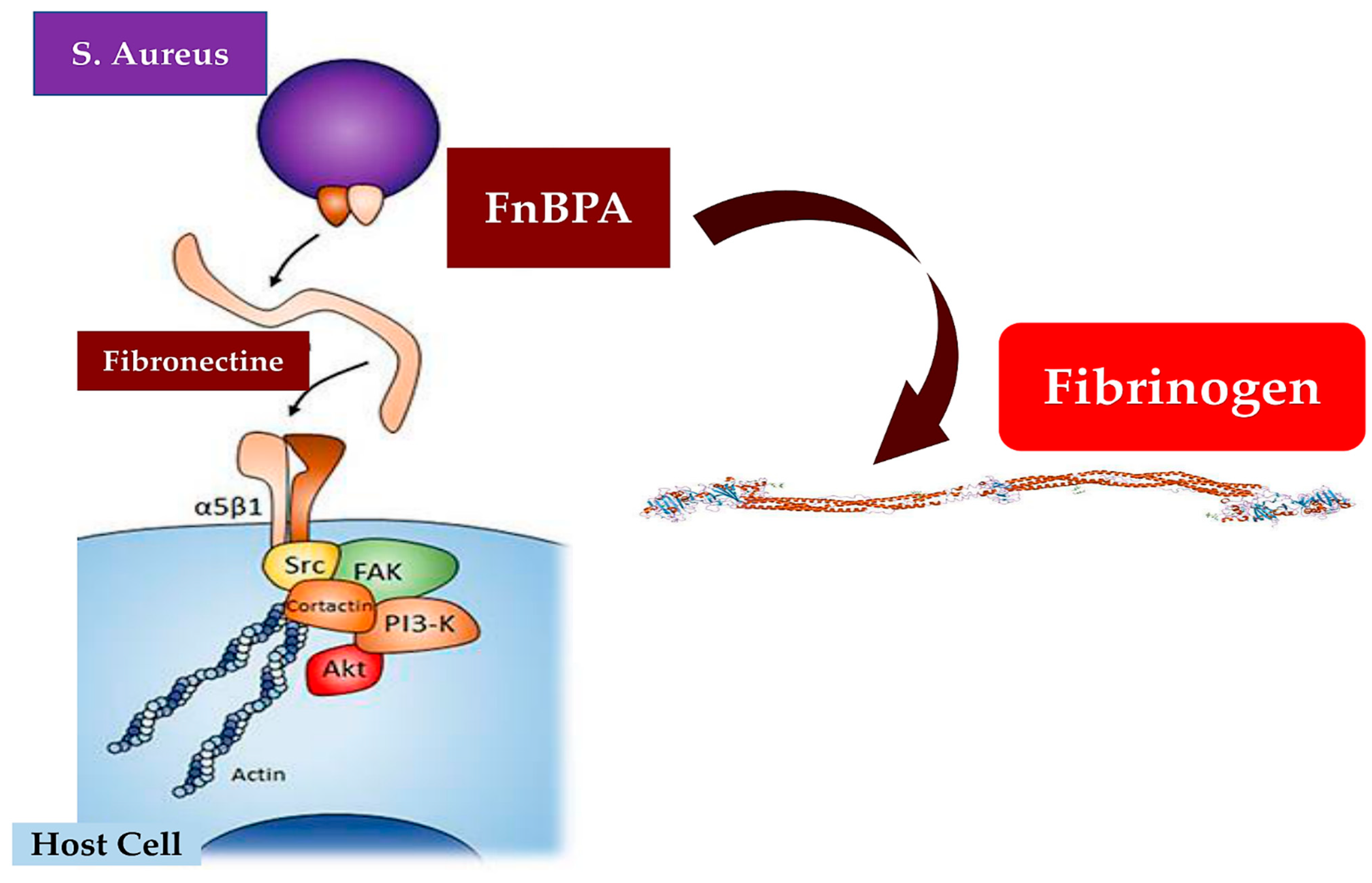
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



