Submitted:
30 June 2026
Posted:
01 July 2026
You are already at the latest version
Abstract
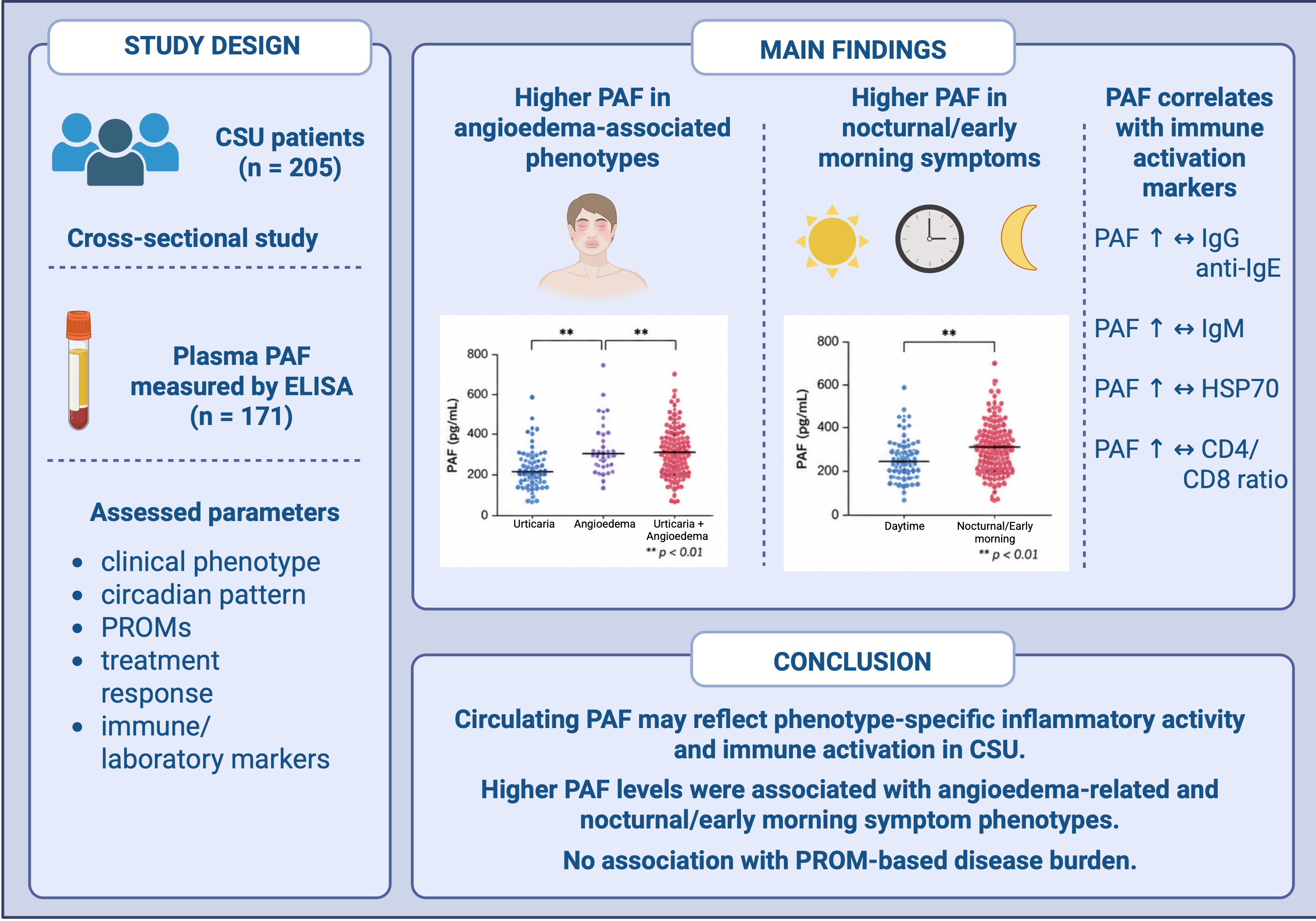
Background/Objectives: Chronic spontaneous urticaria (CSU) is a heterogeneous immune-mediated condition involving multiple inflammatory pathways. The clinical utility of platelet-activating factor (PAF) as a biomarker in CSU remains insufficiently defined. This study aimed to evaluate serum PAF levels in patients with CSU and to investigate their associations with clinical characteristics, disease activity, and laboratory and immunological parameters. Methods: This cross-sectional study included 205 adult patients diagnosed with CSU between January 2016 and May 2023. Clinical data, patient-reported outcome measures (PROMs), and extensive laboratory parameters were collected. Serum PAF levels were measured using ELISA in 171 patients. Associations were analyzed using appropriate statistical methods. Results: The cohort was predominantly female (77.6%), with a mean age of 42.6 ± 15.3 years. Most patients had uncontrolled disease (76.9%). The median UAS7 indicated moderate disease activity. PAF levels differed significantly across clinical subgroups. Higher PAF levels were observed in patients with angioedema (alone or in combination with urticaria) compared to those with urticaria alone (p = 0.002), and in patients with predominantly nocturnal and early morning symptoms (p = 0.018). No associations were found between PAF levels and disease activity scores or treatment response. PAF levels showed positive correlations with age, age at symptom onset, IgM, IgG anti-IgE, HSP70, and the CD4/CD8 ratio (all p < 0.05). Conclusions: Circulating PAF levels are associated with specific clinical phenotypes, circadian symptom patterns, and selected immunological markers in CSU, supporting a role for PAF in disease heterogeneity and immune activation. PAF may reflect underlying biological processes not captured by patient-reported disease severity.
Keywords:
platelet activating factor
; chronic urticaria
; biomarkers
; disease progression
; inflammation
1. Introduction
Chronic spontaneous urticaria (CSU) is a chronic inflammatory skin disease characterized by the recurrent occurrence of pruritic wheals, angioedema, or both for at least six weeks in the absence of identifiable external triggers [1,2,3,4]. It is primarily driven by activation and degranulation of skin mast cells, leading to the release of inflammatory mediators responsible for wheal formation, angioedema, and pruritus [4].
CSU is increasingly recognized as a heterogeneous immune-mediated condition involving multiple inflammatory pathways. Skin biopsies demonstrate infiltration of mast cells, basophils, eosinophils, and T lymphocytes, along with increased expression of adhesion molecules and pro-inflammatory cytokines [3,5]. These mechanisms contribute to persistent inflammation and may explain variability in disease activity, clinical presentation, and response to therapy among patients [5,6].
Although histamine is the principal mediator of pruritus via activation of histamine H1 receptors, a substantial proportion of patients show inadequate response to antihistamine therapy, suggesting involvement of additional mediators. These include prostaglandins, leukotrienes, neuropeptides, and platelet-activating factor (PAF) [7]. This has prompted increasing interest in non-histamine pathways that may contribute to disease persistence and therapeutic refractoriness.
PAF is a potent bioactive phospholipid involved in inflammation and immune regulation [8,9]. It is produced by multiple immune cells, including mast cells, basophils, eosinophils, neutrophils, and macrophages, and exerts its effects via the platelet-activating factor receptor (PAFR), promoting leukocyte activation, mediator release, and increased vascular permeability [5,10,11]. These properties suggest that PAF may act as an amplifier of inflammatory responses in CSU [5,12].
Clinical evidence indicates that PAF may be associated with disease activity and treatment response in CSU. Elevated serum PAF levels, together with reduced activity of platelet-activating factor acetylhydrolase (PAF-AH), have been linked to increased disease severity and reduced responsiveness to antihistamine therapy [5,6,12]. Furthermore, PAF has been proposed as a potential predictor of antihistamine refractoriness [6].
Despite these observations, the clinical utility of PAF as a biomarker in CSU remains insufficiently defined. In particular, its relationship with clinical characteristics and laboratory markers of disease activity has not been fully elucidated. Given the need for reliable biomarkers to improve disease stratification and guide treatment decisions in CSU, further investigation of PAF is warranted.
This study aimed to evaluate serum PAF levels in patients with CSU and to investigate their relationship with clinical characteristics, circadian symptom patterns, laboratory and immunological markers, and treatment response.
2. Materials and Methods
2.1. Study Population
The study cohort was identified through the electronic medical records system of Pauls Stradiņš Clinical University Hospital, including patients diagnosed with CSU between January 2016 and May 2023. Additional participants were recruited from the Allergic Diseases Diagnosis and Treatment Center, a specialized referral centre for allergic diseases in Latvia.
Adult patients (≥18 years) were invited to participate. All participants received detailed information about the study and provided written informed consent. The study was approved by the Ethics Committee of Rīga Stradiņš University (Approval No. 2-PĒK-4/68/2023).
2.2. Clinical Data Collection
A total of 205 patients were included and evaluated by a board-certified allergologist. During study visits, participants completed validated disease-specific questionnaires, including the chronic urticaria quality of life questionnaire (CU-Q2oL), urticaria control test (UCT), urticaria activity score over 7 days (UAS7), urticaria severity score (USS), and angioedema-related instruments (AE-QoL, AAS, AECT), as well as a visual analogue scale (VAS).
Demographic and clinical data were collected, including age, sex, education, occupational status, smoking, comorbidities, disease duration, symptom distribution, disease severity, circadian variation, triggers, and treatment history.
2.3. Laboratory Data Acquisition
Laboratory test results, including leukocyte subpopulations (Leu, Neu, Ly, Mo, Eo, Ba), inflammatory markers (CRP, D-dimer, IL-6, RF, ASO, ECP), thyroid and metabolic parameters (TSH, FT4, PTH, vitamin D), immunoglobulins (IgG, IgA, IgM, IgE), complement components (C1 inhibitor concentration and activity, C3c, C4), and autoantibodies (IgG-anti-TPO, IgG-anti-TG, IgG-anti-TSH receptor, IgG-anti-C1q, IgG-anti-dsDNA, and anti-cardiolipin IgG/IgM/IgA, ANA, ENA, pANCA, and cANCA), as well as tumour markers (CA 19-9, CEA, CA15-3, CA125), were obtained from the Latvian electronic medical information system, DataMed. This system integrates laboratory and imaging data from multiple certified laboratories across the country, ensuring standardized and reliable measurements.
2.4. Sample Collection and Measurement of PAF
Venous blood samples were collected under standardized conditions. Plasma was obtained using EDTA tubes and centrifugation at 1,500 × g for 10 minutes. Samples were aliquoted and stored at −80 °C until analysis.
PAF concentrations were measured using a competitive enzyme-linked immunosorbent assay (ELISA) kit (Platelet Activating Factor ELISA Kit, Antibodies-online, Germany; catalogue no. ABIN6969371) according to the manufacturer’s instructions. Plasma samples were analysed in duplicate, and concentrations were calculated using standard curves. All measurements were performed under standardized laboratory conditions.
2.5. Measurement of HSP70 and Autoantibodies
Serum levels of HSP70 and anti-HSP70 antibodies were measured using commercially available ELISA kits (Enzo Life Sciences, USA; catalogue no. ADI-EKS-715; catalogue no. ADI-EKS-750) according to the manufacturer’s protocols.
IgG autoantibodies against FcεRIα and IgE were measured using ELISA with recombinant human antigens. Serum samples were analyzed in duplicate, and detection was performed using chemiluminescence-based methods.
2.6. Statistical Analysis
Data distribution was assessed using the Shapiro–Wilk test. Continuous variables are presented as mean ± standard deviation (SD) or median (interquartile range, IQR), as appropriate. Categorical variables are expressed as counts and percentages.
Comparisons between groups were performed using Student’s t-test or one-way ANOVA for normally distributed data, and Mann–Whitney U test or Kruskal–Wallis test for non-normally distributed data. Associations between variables were assessed using Spearman’s rank correlation. A p-value < 0.05 was considered statistically significant. All analyses were performed using Jamovi (version 2.7.5).
3. Results
3.1. Clinical and Disease Characteristics
The study included 205 patients with CSU, of whom 77.6% (n = 159) were female. The mean age was 42.6 ± 15.3 years. Detailed clinical characteristics and treatment patterns are presented in Table 1.
3.2. Disease Activity, Severity and Control
Disease activity, severity, and control were assessed using validated patient-reported outcome measures (PROMs), including VAS, UCT, UAS7, CU-Q2oL, AAS7, AECT-3mo, and AE-QoL. The results are summarized in Table 2.
Overall, the study population demonstrated a high disease burden and suboptimal disease control. Based on UCT scores, only 1.4% (n = 2) of patients had completely controlled CSU, 20.8% (n = 29) had well-controlled disease, and 76.9% (n = 107) had uncontrolled CSU.
The median UAS7 score was 14 (IQR 4–28), indicating overall moderate disease activity. While 12.1% (n = 17) of patients were urticaria-free, 28.6% (n = 40) experienced severe disease.
Among patients with angioedema, disease control was generally poor, with only four patients achieving controlled disease according to AECT-3mo.
3.3. Serum PAF Levels Across Patient Subgroups
PAF measurements were available for 171 patients included in the study. Significant differences in PAF levels were observed across circadian symptom patterns (p = 0.018, η² = 0.07) and clinical presentation (p = 0.002, η² = 0.07). Patients with symptoms predominantly during the night and early morning exhibited higher PAF levels (median 17.3 [15.8–19.2] ng/mL) compared with other circadian symptom pattern subgroups, especially patients who were asymptomatic on waking (13.1 [8.9–17.0] ng/mL) (Figure 1).
PAF levels also differed across CSU clinical presentations (p = 0.002). Patients with both urticaria and angioedema (17.2 [15.1–18.8] ng/mL) and those with angioedema only (17.1 [14.3–17.9] ng/mL) had higher PAF levels than patients with urticaria alone (14.1 [10.6–17.4] ng/mL) (Figure 2).
No significant associations were observed between PAF levels and demographic or clinical variables, including sex, place of residence, allergic comorbidity, disease-triggering factors, accompanying symptoms, or treatment effectiveness (all p > 0.05).
Comparisons of serum PAF levels across patient subgroups are presented in Table 3.
Higher levels were observed in patients with predominantly night and early morning symptoms compared with other circadian symptom pattern subgroups. Abbreviations: PAF – platelet-activating factor
Higher PAF levels were observed in patients with angioedema (alone or with urticaria) compared with those with urticaria alone. Abbreviations: PAF – platelet-activating factor, CSU – chronic spontaneous urticaria, AE – angioedema.
3.4. Correlation of PAF Levels with Clinical and Laboratory Parameters
Serum PAF levels showed significant positive correlations with age (r = 0.202, p = 0.008), age at symptom onset (r = 0.208, p = 0.007), IgG anti-IgE (r = 0.186, p = 0.015), IgM (r = 0.215, p = 0.012), HSP70 (r = 0.171, p = 0.029), and the CD4/CD8 index (r = 0.369, p < 0.001).
No significant correlations were observed with disease duration, BMI, PROMs, or other laboratory parameters (all p > 0.05).
Correlations between serum PAF levels and clinical and laboratory parameters are shown in Table 4.
4. Discussion
This study shows that circulating PAF levels are associated with clinical characteristics and selected immunological markers in CSU, supporting a role for PAF as a marker of immune activation and disease heterogeneity.
PAF is a pro-inflammatory phospholipid mediator involved in allergic inflammation and immune signaling and is produced by multiple cell types relevant to CSU pathogenesis, including mast cells and basophils [5,9,10]. Given its role in inflammatory processes, PAF has been explored as a biomarker in chronic inflammatory diseases [5,8].
CSU is a heterogeneous disease with distinct autoimmune endotypes, including type I (autoallergic) and type IIb (autoimmune) CSU, defined by different autoantibody profiles and immune mechanisms [1,3,4]. In this context, the observed correlation between PAF levels and anti-IgE IgG antibodies may suggest an association with type IIb autoimmune CSU. This interpretation is consistent with previously reported features of type IIb CSU, such as nocturnal symptoms, eosinopenia, and reduced IgA levels [13,14,15].
We also identified associations between PAF levels and IgM antibodies, HSP70, and the CD4/CD8 ratio. Although direct evidence linking these markers to PAF in CSU is limited, these findings may reflect broader immune dysregulation. IgM autoantibodies have been described in CSU, although their specificity remains unclear [13], while alterations in the CD4/CD8 ratio and increased HSP70 levels have been associated with chronic immune activation and inflammatory stress responses [14,15]. These observations support the concept that PAF may be linked to multiple overlapping immune pathways rather than a single pathogenic mechanism.
In a large study by Ulambayar et al., PAF and PAF-acetylhydrolase levels were evaluated in CSU, with no association observed with age or disease activity, although correlations with metabolic parameters and antihistamine refractoriness were reported[6]. In contrast, we observed positive associations between PAF levels and age, age at symptom onset, circadian symptom patterns, and clinical presentation, but not with antihistamine response. These differences may be explained by differences in population characteristics (e.g., demographic or clinical profiles), variations in study design and sample size, as well as underlying biological heterogeneity of CSU.
Consistent with previous reports demonstrating elevated PAF levels in CSU and in severe allergic reactions [6,16,17], we found higher PAF levels in patients with angioedema, either alone or in combination with urticaria, compared with those with urticaria alone. This pattern suggests that increased PAF levels may be associated with more severe or systemic disease manifestations. Given the established role of PAF in vascular permeability and inflammatory signaling, these findings may have implications for identifying patients who could benefit from targeted anti-PAF strategies.
Circadian variation is a recognized feature of CSU, with symptoms often worsening during the evening and night [18,19,20,21,22]. In our study, higher PAF levels were observed in patients with predominantly nocturnal and early morning symptoms, suggesting a potential contribution of PAF to circadian disease activity. Although direct evidence for circadian regulation of PAF synthesis is limited [23,24,25], indirect data suggest that PAF-related pathways may be influenced by circadian mechanisms [24,25,26]. This may reflect circadian variation in mast cell activity and mediator release, including histamine and potentially PAF, as well as fluctuations in upstream immunological processes. In addition, circadian patterns in immune regulation, including possible variation in autoantibody-mediated activation, may further contribute to the observed symptom patterns.
Despite the high disease burden observed in our cohort, PROMs did not correlate with PAF levels. This may suggest that circulating PAF reflects underlying biological activity that is not directly aligned with patients’ subjective perception of symptoms. Patient-reported outcomes are influenced by multiple factors, including symptom perception, psychological burden, and individual variability, whereas PAF may capture specific pathophysiological processes that do not translate proportionally into perceived disease severity.
Several limitations should be considered that may have influenced the observed associations. Although the overall sample size was adequate, subgroup analyses were limited by unequal group sizes and small numbers in some subgroups, which may have affected the robustness of the findings. In addition, the sex distribution was unbalanced. Some clinical data were based on patient-reported history, and not all laboratory parameters were available for all participants. PAF levels were assessed at a single time point, precluding evaluation of their temporal dynamics. PAF measurements were available for only a subset of the study population (n = 171).
5. Conclusions
Circulating PAF levels were associated with clinical phenotype, circadian symptom patterns, and selected immunological markers in CSU, suggesting a potential role for PAF in disease heterogeneity and immune activation.
Higher PAF levels in patients with predominantly night and early morning symptoms, as well as in those with angioedema, point to an association with specific clinical phenotypes rather than overall disease severity.
The absence of correlations with patient-reported outcomes suggests that PAF may reflect underlying biological processes not fully captured by subjective measures.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org. Table S1: Correlation of PAF levels with clinical and laboratory parameters.
Author Contributions
Conceptualization, L.L. and N.K.; methodology, L.L. and N.K.; formal analysis, L.L. and K.S.; investigation, L.L. and N.K.; resources, L.L. and N.K.; data curation, L.L., G.Z. and N.K.; writing—original draft preparation, L.L.; writing—review and editing, L.L., K.S., G.Z. and N.K.; supervision, N.K.; project administration, L.L. and N.K. All authors have read and agreed to the published version of the manuscript.
Funding
The authors report no funding for this work.
Institutional Review Board Statement
Ethical approval for the study was granted by the Ethics Committee of Riga Stradiņš University (Nr. 2-PĒK-4/68/2023).
Informed Consent Statement
Not applicable.
Data Availability Statement
All data generated or analyzed during this study are presented within this article. Additional information is available upon reasonable request by contacting the corresponding author.
Acknowledgments
The authors express their sincere gratitude to Anna Lauva, Sindija Papirte, Līga Ciekure, Egīls Mauliņš, Līga Lielmane, Petra Kriķe, Marija Selicka, and Signe Puriņa for their valuable assistance and support in data collection and patient coordination throughout this study. Their contributions were essential to the successful completion of the research.
Conflicts of Interest
All authors declare no conflicts of interest in relation to this work.
Abbreviations
The following abbreviations are used in this manuscript:
| AECT-3mo | Angioedema control test over 3 months |
| AAS | Angioedema activity score over 7 days |
| AE-QoL | Angioedema quality of life questionnaire |
| BMI | Body mass index |
| CSU | Chronic spontaneous urticaria |
| CU-Q2oL | Chronic urticaria quality of life questionnaire |
| ELISA | Enzyme-linked immunosorbent assay |
| IQR | Interquartile range |
| PAF | Platelet-activating factor |
| PAF-AH | Platelet-activating factor acetylhydrolase |
| PAFR | Platelet-activating factor receptor |
| PROMs | Patient-reported outcome measures |
| SD | Standard deviation |
| UAS7 | Urticaria activity score over 7 days |
| UCT | Urticaria control test |
| VAS | Visual analogue scale |
References
- Zuberbier, T.; Abdul Hameed Ansari, Z.; Abdul Latiff, A.H.; Abuzakouk, M.M.; Agcaoili-De Jesus, M.S.; Agondi, R.C.; Al-Ahmad, M.; Alangari, A.A.; Alhameli, H.; Alonso Bello, C.D.; et al. The International Guideline for the Definition, Classification, Diagnosis and Management of Urticaria. Allergy 2026. [Google Scholar] [CrossRef] [PubMed]
- Kolkhir, P.; Muñoz, M.; Asero, R.; Ferrer, M.; Kocatürk, E.; Metz, M.; Xiang, Y.K.; Maurer, M. Autoimmune chronic spontaneous urticaria. J. Allergy Clin. Immunol. 2022, 149, 1819–1831. [Google Scholar] [CrossRef] [PubMed]
- Oliver, E.T.; Saini, S.S. Chronic Spontaneous Urticaria: Etiology and Pathogenesis. Immunol. Allergy Clin. North Am. 2024, 44, 421–438. [Google Scholar] [CrossRef] [PubMed]
- Kolkhir, P.; Giménez-Arnau, A.M.; Kulthanan, K.; Peter, J.; Metz, M.; Maurer, M. Urticaria. Nat. Rev. Dis. Prim. 2022, 8, 61. [Google Scholar] [CrossRef] [PubMed]
- Choi, B.Y.; Ye, Y.-M. Role of Platelet-Activating Factor in the Pathogenesis of Chronic Spontaneous Urticaria. Int. J. Mol. Sci. 2024, 25, 12143. [Google Scholar] [CrossRef] [PubMed]
- Ulambayar, B.; Yang, E.M.; Cha, H.Y.; Shin, Y.S.; Park, H.S.; Ye, Y.M. Increased platelet activating factor levels in chronic spontaneous urticaria predicts refractoriness to antihistamine treatment: an observational study. Clin. Transl. Allergy 2019, 9, 33. [Google Scholar] [CrossRef] [PubMed]
- Su Küçük, Ö.; Yücel, M.B. Clinical and molecular aspects of managing chronic spontaneous urticaria: identifying endotypes, phenotypes, and determinants of treatment response and resistance. Front. Allergy 2026, 6–2025. [Google Scholar] [CrossRef] [PubMed]
- Upton, J.E.M.; Grunebaum, E.; Sussman, G.; Vadas, P. Platelet Activating Factor (PAF): A Mediator of Inflammation. Biofactors 2022, 48, 1189–1202. [Google Scholar] [CrossRef] [PubMed]
- Fan, W.; Xu, Y.; He, X.; Luo, P.; Zhu, J.; Li, J.; Wang, R.; Yuan, Q.; Wu, K.; Hu, W.; et al. Molecular basis for the activation of PAF receptor by PAF. Cell Rep. 2024, 43, 114422. [Google Scholar] [CrossRef] [PubMed]
- Ashraf, M.A.; Nookala, V. Biochemistry of Platelet Activating Factor. In StatPearls; StatPearls Publishing, Copyright © 2026, StatPearls Publishing LLC.: Treasure Island (FL), 2026. [Google Scholar]
- Sánchez Crespo, M.; Montero, O.; Fernandez, N. The role of PAF in immunopathology: From immediate hypersensitivity reactions to fungal defense. Biofactors 2022, 48, 1217–1225. [Google Scholar] [CrossRef] [PubMed]
- Yang, E.-M.; Ye, Y.-M.; Cha, H.-Y.; Ulambayar, B.; Shin, Y.; Park, H.-S. Serum platelet activating factor levels predicts refractoriness to antihistamine treatment in chronic spontaneous urticaria. World Allergy Organ. J. 2020, 13, 100235. [Google Scholar] [CrossRef]
- Altrichter, S.; Zampeli, V.; Ellrich, A.; Zhang, K.; Church, M.K.; Maurer, M. IgM and IgA in addition to IgG autoantibodies against FcɛRIα are frequent and associated with disease markers of chronic spontaneous urticaria. Allergy 2020, 75, 3208–3215. [Google Scholar] [CrossRef] [PubMed]
- McBride, J.A.; Striker, R. Imbalance in the game of T cells: What can the CD4/CD8 T-cell ratio tell us about HIV and health? PLoS Pathog. 2017, 13, e1006624. [Google Scholar] [CrossRef] [PubMed]
- Kasperska-Zając, A.; Damasiewicz-Bodzek, A.; Bieniek, K.; Skrzypulec-Frankel, A.; Tyrpien-Golder, K.; Grzanka, A. Elevated circulating heat shock protein 70 and its antibody concentrations in chronic spontaneous urticaria. Int. J. Immunopathol. Pharmacol. 2018, 31, 394632017750440. [Google Scholar] [CrossRef] [PubMed]
- Gomułka, K.; Mędrala, W. Serum Levels of Vascular Endothelial Growth Factor, Platelet Activating Factor and Eosinophil-Derived Neurotoxin in Chronic Spontaneous Urticaria—A Pilot Study in Adult Patients. Int. J. Mol. Sci. 2022, 23, 9631. [Google Scholar] [PubMed]
- Pałgan, K.; Bartuzi, Z. Platelet activating factor in allergies. Int. J. Immunopathol. Pharmacol. 2015, 28, 584–589. [Google Scholar] [CrossRef] [PubMed]
- Yosipovitch, G.; Ansari, N.; Goon, A.; Chan, Y.H.; Goh, C.L. Clinical characteristics of pruritus in chronic idiopathic urticaria. Br. J. Dermatol. 2002, 147, 32–36. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.; Jing, D.; Su, J.; Huang, Z.; Liu, H.; Tao, J.; He, M.; Chen, X.; Shen, M.; Xiao, Y. Association of Night Shift Work With Chronic Spontaneous Urticaria and Effect Modification by Circadian Dysfunction Among Workers. Front. Public Health 2021, 9–2021. [Google Scholar] [CrossRef] [PubMed]
- Paganelli, R.; Petrarca, C.; Di Gioacchino, M. Biological clocks: their relevance to immune-allergic diseases. Clin. Mol. Allergy 2018, 16, 1. [Google Scholar] [CrossRef] [PubMed]
- Maurer, M.; Ortonne, J.P.; Zuberbier, T. Chronic urticaria: an internet survey of health behaviours, symptom patterns and treatment needs in European adult patients. Br. J. Dermatol. 2009, 160, 633–641. [Google Scholar] [CrossRef] [PubMed]
- Smolensky, M.H.; Portaluppi, F.; Manfredini, R.; Hermida, R.C.; Tiseo, R.; Sackett-Lundeen, L.L.; Haus, E.L. Diurnal and twenty-four hour patterning of human diseases: acute and chronic common and uncommon medical conditions. Sleep Med. Rev. 2015, 21, 12–22. [Google Scholar] [CrossRef] [PubMed]
- Harishkumar, R.; Hans, S.; Stanton, J.E.; Grabrucker, A.M.; Lordan, R.; Zabetakis, I. Targeting the Platelet-Activating Factor Receptor (PAF-R): Antithrombotic and Anti-Atherosclerotic Nutrients. Nutrients 2022, 14, 4414. [Google Scholar] [PubMed]
- Scheer, F.; Michelson, A.; Frelinger, A.; Evoniuk, H.; Kelly, E.; McCarthy, M.; Doamekpor, L.; Barnard, M.; Shea, S. The Human Endogenous Circadian System Causes Greatest Platelet Activation during the Biological Morning Independent of Behaviors. PLoS ONE 2011, 6, e24549. [Google Scholar] [CrossRef] [PubMed]
- Misso, N.L.; Gillon, R.L.; Stewart, G.A.; Thompson, P.J. Lyso-PAF acetyltransferase activity in neutrophils of patients during acute asthma and after recovery. Eur. Respir. J. 1996, 9, 2243–2249. [Google Scholar] [CrossRef] [PubMed]
- Levin, A.M.; Wang, Y.; Wells, K.E.; Padhukasahasram, B.; Yang, J.J.; Burchard, E.G.; Williams, L.K. Nocturnal asthma and the importance of race/ethnicity and genetic ancestry. Am. J. Respir. Crit. Care Med. 2014, 190, 266–273. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
PAF levels according to circadian symptom pattern.

Figure 2.
PAF levels according to CSU clinical presentation.


Table 1.
Clinical and demographic characteristics of the study population (n = 205).
| Sex, n (%) | |
| Female | 159 (77.6) |
| Male | 46 (22.4) |
| Age, years (Mean, SD) | 42.6 (15.3) |
| Higher education, n (%) | 118 (57.6) |
| Place of residence, n (%) | |
| Urban | 181 (88.4) |
| Rural | 24 (11.7) |
| BMI, Median (IQR) | 25.5 (21.6 -30.9) |
| Smoking status, n (%) | |
| Non-smoker | 113 (55.1) |
| Smoker | 59 (28.8) |
| Former smoker | 33 (16.1) |
| Clinical presentation, n (%) | |
| Urticaria only | 81 (39.5) |
| Urticaria + angioedema | 98 (47.8) |
| Angioedema only | 26 (12.6) |
| Allergic comorbidity, n (%) | 94 (45.8) |
| Duration of CSU, months | Mean (SD) 57.4 (71.8) |
| Age of symptom onset, years | Mean (SD) 36.1 (15.2) |
| Circadian symptom pattern, n (%) | |
| No circadian pattern | 89 (43.4) |
| Only daytime | 37 (18.0) |
| Only nighttime | 11 (5.4) |
| Mostly at night and in the morning | 35 (17.1) |
| Asymptomatic on waking | 33 (16.1) |
| Accompanying symptoms, n (%) | 128 (62.4) |
| Disease-provoking factors, n (%) | 156 (76.1) |
| Therapy with antihistamines, n (%) | 191 (93.2) |
| Therapy with omalizumab, n (%) | 56 (27.3) |
| Therapy with cyclosporine, n (%) | 8 (3.9) |
Abbreviations: BMI- body mass index, CSU- chronic spontaneous urticaria, SD – standard deviation, IQR – interquartile range.
Table 2.
Patient-reported outcome measures (PROMs).
| Variable | n | Median (IQR) |
| VAS | 139 | 8 (2–10) |
| UCT | 139 | 8 (5.5–11) |
| UAS7 | 139 | 14 (4–28) |
| CU-Q2oL | 139 | 34 (21–51) |
| AAS7 | 20 | 10.0 (0–78.8) |
| AECT-3mo | 20 | 6.00 (3.75–9) |
| AE-QoL | 19 | 38.2 (22.8–77.2) |
Abbreviations: IQR – interquartile range, VAS - visual analogue scale, UCT - urticaria control test, UAS7 - urticaria activity score over 7 days, CU-Q2oL - chronic urticaria quality of life questionnaire, AAS – angioedema activity score over 7 days, AECT-3mo- angioedema control test over 3 months, AE-QoL – angioedema quality of life questionnaire.
Table 3.
Serum PAF levels across selected patient subgroups.
| Variable | Group | n | Median (IQR) | p |
|---|---|---|---|---|
| Sex | Female | 132 | 16.3 (12.1–18.6) | 0.887 |
| Male | 39 | 16.3 (13.3–18.3) | ||
| Place of residence | Urban | 151 | 16.0 (12.3–18.3) | 0.250 |
| Rural | 20 | 16.7 (13.9–18.6) | ||
| Allergic comorbidity | No | 85 | 15.8 (11.9–17.9) | 0.241 |
| Yes | 85 | 16.8 (13–18.7) | ||
| Disease-triggering factors | No | 51 | 16.0 (11.8–18.3) | 0.612 |
| Yes | 119 | 16.5 (11.8–18.3) | ||
| Circadian symptom pattern | No circadian pattern | 78 | 16.4 (13.1–18.5) | 0.018 |
| Only daytime | 6 | 15.4 (11.8–17.5) | ||
| Only nighttime | 8 | 16.6 (13.1–18.7) | ||
| Mostly at night and in the morning | 25 | 17.3 (15.8–19.2) | ||
| Asymptomatic on waking | 28 | 13.1 (8.9–17.0) | ||
| Response to antihistamine treatment | Effective | 99 | 16.3 (13.0–18.4) | 0.223 |
| Ineffective | 45 | 17.1 (11.9–18.6) | ||
| Partially effective | 14 | 16.1 (11.8–17.5) | ||
| Does not use | 12 | 14.4 (8.7–15.8) | ||
| Response to omalizumab treatment | Effective | 31 | 16.9 (11.6–17.9) | 0.351 |
| Ineffective | 9 | 17.9 (15.4–18.5) | ||
| Partially effective | 8 | 13.7 (10.2–16.6) | ||
| Does not use | 122 | 16.0 (13.0–18.5) | ||
| Clinical presentation | Urticaria only | 70 | 14.1 (10.6–17.4) | 0.002 |
| Angioedema only | 23 | 17.1 (14.3–17.9) | ||
| Urticaria + angioedema | 77 | 17.2 (15.1–18.8) | ||
| Accompanying symptoms | No | 62 | 14.8 (11.5–18.7) | 0.359 |
| Yes | 108 | 16.6 (13.5–18.0) |
Note: PAF measurements were available for 171 patients; subgroup totals vary because of missing data for selected variables. Abbreviations: PAF – platelet-activating factor; IQR – interquartile range.
Table 4.
Correlation of PAF levels with clinical and laboratory parameters.
| Variable | n | r | p-value |
|---|---|---|---|
| CD4/CD8 index | 92 | 0.369 | < 0.001 |
| IgM | 163 | 0.215 | 0.012 |
| Age at symptom onset | 205 | 0.208 | 0.007 |
| Age | 206 | 0.202 | 0.008 |
| IgG anti-IgE | 199 | 0.186 | 0.015 |
| HSP70 | 173 | 0.171 | 0.029 |
Note: Only statistically significant correlations are shown. Full results are available in Supplementary Table S1. Abbreviations: PAF – platelet-activating factor, HSP70 – heat shock protein 70.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



