Submitted:
27 May 2026
Posted:
28 May 2026
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
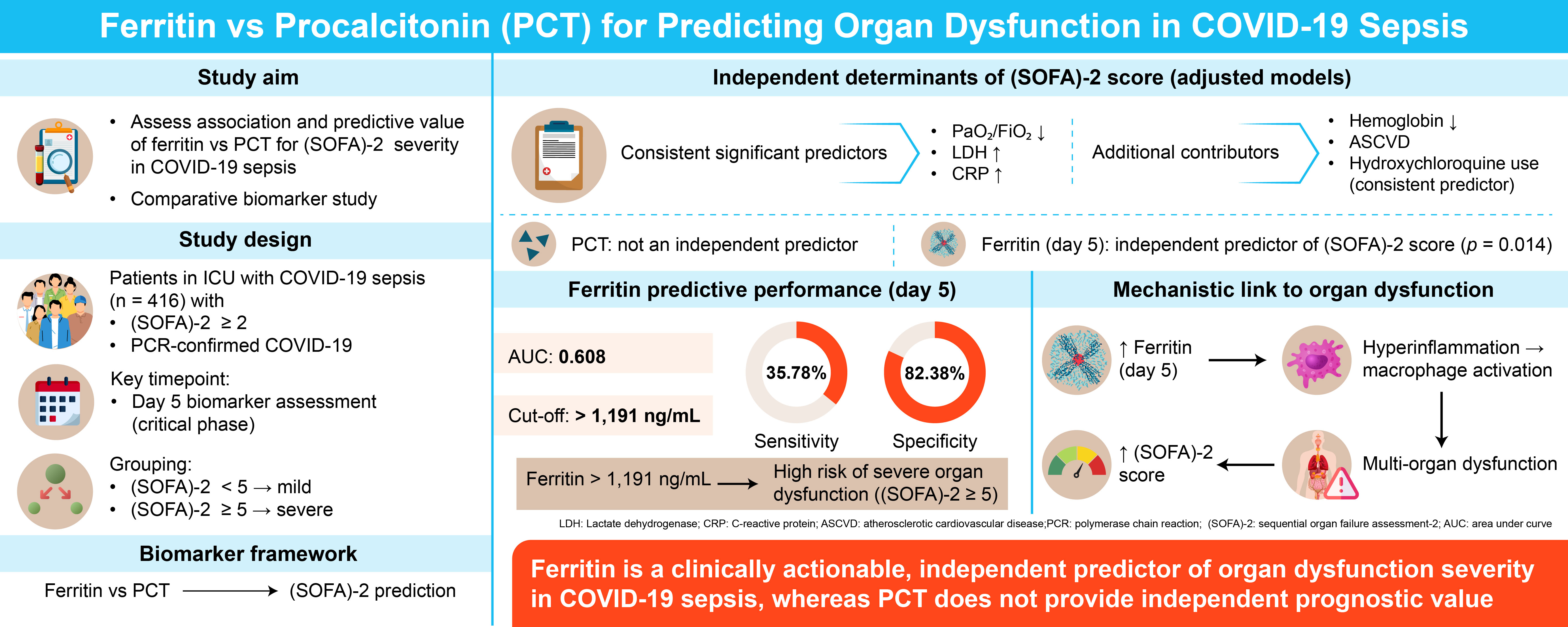
Background/Objectives: To our knowledge, this is the first study to simultaneously investigate the prognostic value of serum ferritin and procalcitonin (PCT) in relation to (SOFA)-2 score-based organ dysfunction severity in intensive care patients diagnosed with COVID-19-associated sepsis. Methods: Patients were stratified based on day 5 ferritin (ng/mL) and PCT levels (μg/L). Prognostic performance was analysed across severity groups defined by (SOFA)-2 score of <5 (mild) and ≥5 (severe). Results: Day 5 PCT levels did not significantly predict (SOFA)-2 score (p > 0.05). The optimal day 5 ferritin cut-off was >1,191 ng/mL, with 35.78% sensitivity and 82.38% specificity (AUC = 0.608). Elevated ferritin levels may help identify patients at higher risk of adverse outcomes who may benefit from closer monitoring or intensive care escalation. By contrast, PCT did not provide additional predictive value for organ dysfunction severity in COVID-19 beyond existing inflammatory markers, consistent with its known suppression during primary viral infections. Conclusions: Serum ferritin showed a significant positive association with (SOFA)-2 score, supporting its role as a clinically relevant biomarker for disease stratification in COVID-19-associated sepsis. These findings may extend to non-COVID sepsis populations where macrophage activation and iron dysregulation drive organ dysfunction.
Keywords:
COVID-19
; sepsis
; ferritin
; procalcitonin
; SOFA score
1. Introduction
In December 2019, a novel disease caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), later termed COVID-19, was first reported in Wuhan, China. The infection spread rapidly worldwide and was declared a pandemic by the World Health Organization (WHO) in March 2020, coinciding with the admission of critically ill patients to intensive care units (ICUs) across Europe [1]. Patients with COVID-19 requiring ICU care typically present with progressive respiratory failure secondary to severe pulmonary involvement. In addition to respiratory compromise, SARS-CoV-2 affects extrapulmonary systems—including the liver, kidneys, and haematological components—thereby increasing the risk of multi-organ failure [2]. The virus can infect both ciliated and secretory epithelial cells in the respiratory tract, contributing to its high transmissibility and pathogenicity compared with other coronaviruses [3].
In critically ill patients, clinical scoring systems support the assessment of disease severity and guide therapeutic decision-making [4]. The Sepsis-related Organ Failure Assessment (SOFA)-2 score evaluates the extent of organ dysfunction across multiple systems and may provide valuable prognostic information regarding disease progression and mortality risk, making it a practical tool for risk stratification at admission and during daily follow-up of critically ill patients with COVID-19 and COVID-19-associated sepsis. Previous work by Raschke et al. reported that the (SOFA)-2 score did not predict mortality in patients with COVID-19 pneumonia requiring mechanical ventilation [5]; however, their analysis was limited to a specific patient subset. In contrast, our study categorised patients according to disease severity and included a broader ICU population, allowing evaluation of the association between (SOFA)-2 score and mortality across severity groups.
Cytokine storm—an uncontrolled immune response—plays a central role in the immunopathogenesis of COVID-19, characterised by excessive release of pro-inflammatory cytokines, including tumour necrosis factor-α (TNF-α), interleukin (IL)-6, IL-12, and IL-8, which may lead to acute respiratory distress syndrome (ARDS) and multi-organ failure [6]. Emerging evidence indicates that biomarkers such as serum ferritin (ng/mL), D-dimer, lactate dehydrogenase (LDH; U/L), and IL-6 increase with disease progression and are associated with higher mortality risk [7]. In particular, hyperferritinemia—reflecting severe inflammation—has been linked to ICU admission and increased mortality, and may serve as a useful marker for identifying high-risk patients and guiding anti-inflammatory therapeutic strategies [8,9,10]. Hyperferritinemia is a hallmark of haemophagocytic lymphohistiocytosis (HLH)—a recognised complication of viral infections—and is closely associated with poor outcomes in patients with COVID-19 [11]. In adult-onset Still’s disease (AOSD), elevated ferritin levels are linked to macrophage activation syndrome (MAS), the most frequent life-threatening complication, and are associated with higher mortality [12]. Similarly, in sepsis, elevated ferritin levels correlate with greater disease severity and poorer prognosis [13], supporting the concept of a hyperferritinemic syndrome shared across inflammatory conditions [14]. Ferritin production by the liver and macrophages is upregulated during inflammatory states, driven by cytokines such as IL-1β, IL-6, and interferon (IFN)-γ [15]. Given its proposed role in immune activation, targeting ferritin or its regulatory pathways may represent a potential therapeutic strategy in hyperinflammatory conditions, including severe COVID-19 [16,17].
Several biomarkers have been proposed to predict disease severity in COVID-19, among which PCT (μg/L) is frequently investigated [18]. PCT, the prohormone of calcitonin, is normally produced by thyroid C cells under physiological conditions. During systemic inflammation, its production is upregulated in multiple tissues. Although elevated PCT levels are typically associated with bacterial infections, their synthesis can also be triggered by inflammatory mediators such as IL-6 and TNF-α, which are increased in severe COVID-19 [19]. In patients with COVID-19 and pulmonary involvement such as ARDS, PCT may reflect the degree of hyperinflammation [20] and can assist in identifying concurrent bacterial infections, supporting antibiotic stewardship decisions [21,22,23]. However, studies in isolated viral COVID-19—similar to other viral infections—have shown that PCT often remains within normal limits (≤0.5 μg/L), possibly due to viral suppression of TNF-α through macrophage-mediated IFN-γ production [23]. As an early biomarker of systemic inflammation [24], PCT has been linked to prognosis in infection-related diseases and has been identified as an independent risk factor in sepsis. Several studies have also reported associations between elevated PCT and COVID-19 severity [25,26,27].
Macrophages play a central role in sepsis through pathogen recognition, signalling pathway activation, cytokine production, and immunomodulation. Using surface toll-like receptors (TLRs), macrophages detect pathogen-associated molecular patterns and activate the TLR4/MyD88/NF-κB signalling cascade, leading to the robust release of pro- and anti-inflammatory cytokines. Figure 1 depicts the pathophysiological mechanisms underlying hyperferritinemia and elevated PCT in sepsis [28].
In summary, this study aimed to evaluate the relationship between serum ferritin (ng/mL), serum PCT (μg/L), and (SOFA)-2 score in patients with COVID-19-associated sepsis, and to assess their prognostic value for disease severity and clinical outcomes.
2. Materials and Methods
2.1. Study Design and Setting
This retrospective study included patients treated in the COVID-19 ICU at Afyonkarahisar University of Health Sciences Hospital who were diagnosed with COVID-19-associated sepsis and received favipiravir therapy between March 1, 2020, and June 30, 2021. COVID-19 diagnosis was confirmed via SARS-CoV-2 PCR-RNA testing using nasopharyngeal swabs or bronchoalveolar lavage (BAL) samples. The (SOFA)-2 score was calculated for all patients retrospectively in 2026, by re-applying the (SOFA)-2 criteria published by Ranzani et al. [29] to clinical and laboratory variables prospectively recorded during routine ICU care in 2020–2021. All variables required for SOFA-2 calculation (respiratory, cardiovascular, hepatic, coagulation, renal, and neurological domains) were available from the electronic medical record; those with a score of <2 were excluded. Ferritin (ng/mL) and PCT (μg/L) levels were evaluated in patients with a (SOFA)-2 score of ≥2.
Data from 461 patients meeting the inclusion criteria were initially screened. A total of 45 patients were subsequently excluded: two patients aged 92 years, one patient aged under 18 years, and 42 patients with a (SOFA)-2 score below 2. Ultimately, 416 patients were included in the analysis. The study exclusion criteria algorithm is presented in Figure 2.
The COVID-19 disease severity index was developed based on the WHO’s classification of COVID-19-related clinical syndromes. Sepsis is defined as life-threatening organ dysfunction caused by a dysregulated host response to a suspected or confirmed infection, with key indicators including altered mental status, tachypnea, hypoxemia, oliguria, tachycardia, hypotension, peripheral circulatory abnormalities, coagulopathy, thrombocytopenia, hyperlactatemia, and hyperbilirubinemia [30].
Patient data were extracted from electronic medical records. Laboratory data collected at admission included fasting plasma glucose (mmol/L), serum creatinine (μmol/L), estimated glomerular filtration rate (eGFR; mL/min/1.73 m2), white blood cell count (WBC; /μL) with differential, haemoglobin (g/dL), platelets (/μL), C-reactive protein (CRP; mg/dL), PCT (μg/L), ferritin (ng/mL), erythrocyte sedimentation rate (ESR; mm/h), D-dimer (μg/mL), ALT and AST (U/L), total and indirect bilirubin (μmol/L), electrolytes (mmol/L), albumin (g/dL), serum lactate (mmol/L), and PaO2/FiO2 ratio (mmHg). The same parameters were repeated on day 5. Antibiotic treatment data were not included because bacterial infections were not present in all patients and treatment protocols varied.
PCT levels were measured using the E801 Elecsys BRAHMS PCT assay on the COBAS 8000 system (Roche Diagnostics, Switzerland). Patients were grouped based on PCT levels as <2, 2–10, and ≥10.01 μg/L, using established cutoffs [31]. Ferritin levels (ng/mL) were categorised as 0–499, 500–1,000, and ≥1,001 ng/mL. For the 80 patients who died before day 5 and lacked day 5 measurements, analysis was restricted to the 336 patients with available data. Plasma ferritin (ng/mL) was measured using the ECLIA method on the Cobas E601 device. Patients with hereditary haemochromatosis or CKD (eGFR < 60 mL/min/1.73 m2) were excluded. A (SOFA)-2 score cut-off of ≥5 was used to classify high severity, consistent with the severity stratification framework of the (SOFA)-2 validation study by Ranzani et al. [29] and applied in COVID-19 ICU cohort studies [32].
2.2. Statistical Analysis
Continuous variables are presented as mean ± SD for normally distributed data (Shapiro–Wilk test) and as median (IQR) for non-normal data. Categorical variables are expressed as counts and percentages. Normally distributed variables were compared using the Student’s t-test; non-normally distributed variables with the Mann–Whitney U test; and groups of three or more with the Kruskal–Wallis test, with results reported as median (IQR). Categorical variables were compared using the chi-squared or Fisher’s exact test. Multivariate logistic regression was performed using a stepwise model (entry probability 0.05). ROC curve analysis was used to evaluate ferritin’s diagnostic accuracy, with AUC calculated and the Youden index applied to determine optimal cut-off values. Model calibration was assessed using the Hosmer–Lemeshow test. Given the exploratory nature of multiple comparisons across biomarker subgroups, results are interpreted in the context of the overall model rather than applying post-hoc correction; findings with p < 0.05 are considered statistically significant and are presented as ORs with 95% CIs. Statistical analyses were performed using SPSS version 17.0 (SPSS Inc., Chicago, IL, USA).
2.3. Ethics Approval
The study was conducted in accordance with the 1964 Declaration of Helsinki and its later amendments. Patient data were originally collected during routine clinical care between March 2020 and June 2021. The present retrospective analysis, which included re-calculation of the (SOFA)-2 score using its 2025 definition [29], was reviewed and approved by the Afyonkarahisar Health Sciences University Clinical Research Ethics Committee (Decision dated 06.03.2026, Meeting number 2026/3) under the framework for retrospective use of de-identified clinical data. Informed consent was waived by the ethics committee for this retrospective study. Clinical trial registration is not applicable.
3. Results
A total of 416 patients were included in the study. Of these, 284 (68.3%) were male and 132 (31.7%) were female, with a median age of 69 years (IQR: 62–76). Overall, 287 patients (69.0%) had a (SOFA)-2 score of 0–4 and 129 patients (31.0%) had a score of ≥5. Patient characteristics, clinical outcomes, comorbidities, and treatments stratified by (SOFA)-2 score group are presented in Table 1. Mean laboratory parameters for the entire cohort are summarised in Table 2. The overall mean PCT at admission was 2.4 ± 11.34 μg/L, increasing to 3.6 ± 13.4 μg/L on day 5.
ICU mortality was significantly higher in the severe group: 44.3% (SOFA 0–4) versus 86.8% (SOFA ≥5) (p < 0.001). Mechanical ventilation was required by 31.0% and 65.1% of patients in the mild and severe groups, respectively (p < 0.001). The severe group also had substantially higher rates of renal replacement therapy (23.3% vs. 7.3%; p < 0.001) and greater burden of heart failure, CKD, and ASCVD (Table 1). Day 5 ferritin was 854 ng/mL in the mild group versus 1,110 ng/mL in the severe group (p = 0.001), and day 5 CRP was 8.11 versus 12.62 mg/dL (p < 0.001). The distribution of key biomarkers across severity groups at admission and day 5 is illustrated in Figure 3 (box-plots); serial changes in ferritin and PCT are depicted in Figure 4.
Comparison of laboratory parameters by (SOFA)-2 score group is shown in Table 3. Patients with SOFA ≥5 had significantly higher day 5 PCT (6.44 ± 19.06 vs. 2.23 ± 9.31 μg/L; p < 0.001), day 5 ferritin (1,110 ± 816 vs. 854 ± 682 ng/mL; p = 0.001), and day 5 CRP (12.62 ± 9.25 vs. 8.11 ± 7.67 mg/dL; p < 0.001), while PaO2/FiO2 ratio (111 ± 24 vs. 126 ± 35 mmHg; p < 0.001) and haemoglobin (12.03 ± 2.28 vs. 12.58 ± 2.04 g/dL; p = 0.009) were significantly lower.
Among comorbidities, heart failure (38.0% vs. 20.6%; p < 0.001), CKD (14.7% vs. 6.3%; p = 0.005), and ASCVD (34.9% vs. 19.5%; p = 0.001) were significantly more prevalent in the SOFA ≥5 group (Table 4).
Multivariate logistic regression analyses evaluating the independent predictive roles of day 5 PCT and day 5 ferritin on (SOFA)-2 score are presented in Table 5. In Model A, day 5 PCT added in Step 2 was not a statistically significant predictor (OR = 1.001; 95% CI 0.981–1.022; p = 0.887), despite the significance of PaO2/FiO2 ratio, LDH, day 5 CRP, ASCVD, and hydroxychloroquine in Step 1. In Model B, day 5 ferritin added in Step 2 remained a statistically significant independent predictor (OR = 1.000 per unit; 95% CI 1.000–1.001; p = 0.014), above and beyond PaO2/FiO2 ratio (p = 0.004), LDH (p = 0.005), day 5 CRP (p = 0.002), and hydroxychloroquine use (p = 0.014).
On day 5, ROC curve analysis of ferritin showed an AUC of 0.608 (SE = 0.034), with an optimal cut-off of >1,191 ng/mL (sensitivity 35.78%, 95% CI 26.8–45.5; specificity 82.38%, 95% CI 76.8–87.1) (Table 6; Figure 5).
Laboratory parameters across day 5 PCT subgroups are presented in Table 7. Patients with PCT ≥10.01 μg/L had significantly lower day 5 lymphocyte counts [488 (228–836) vs. 752 (374–1,108) /μL; p = 0.027] and significantly higher day 5 ferritin [1,102 (704–1,568) vs. 724 (320–1,256) ng/mL; p = 0.001] and day 5 CRP [14.6 (8.4–24.2) vs. 6.4 (2.8–11.4) mg/dL; p < 0.001]. No significant association was found between day 5 PCT group and chronic disease or treatment parameters (Table 8).
Laboratory parameters across day 5 ferritin subgroups are presented in Table 9. Patients with ferritin ≥1,001 ng/mL had significantly higher LDH [578 (388–836) vs. 398 (280–560) U/L; p < 0.001], day 5 WBC [14,280 (8,660–20,480) vs. 9,860 (6,880–13,200) /μL; p < 0.001], and day 5 CRP [10.0 (4.4–18.6) vs. 5.6 (2.0–10.6) mg/dL; p < 0.001]. No significant association with chronic disease or treatment parameters was found (Table 10).
4. Discussion
This retrospective study evaluated the prognostic value of serum ferritin (ng/mL) and PCT (μg/L) in relation to (SOFA)-2 score-based organ dysfunction severity in patients with COVID-19-associated sepsis. Our central findings are: (i) day 5 serum ferritin independently predicted (SOFA)-2 score after full adjustment for respiratory, haematological, inflammatory, comorbidity, and treatment variables; and (ii) day 5 PCT did not provide independent predictive value for (SOFA)-2 score, a finding that is biologically coherent with PCT’s known suppression during primary viral infections. To our knowledge, this is the first study to simultaneously examine the relationship between both biomarkers and (SOFA)-2 score in patients specifically diagnosed with COVID-19-associated sepsis. Previous studies have explored a range of clinical and laboratory variables to improve prognostic assessment in critically ill patients with COVID-19, including D-dimer, prothrombin time, haematological indices, and ferritin, but none has simultaneously evaluated both PCT and ferritin against (SOFA)-2 score in a sepsis-defined ICU cohort [33,34,35,36].
4.1. Ferritin as an Independent Predictor of Organ Dysfunction Severity
Ferritin has established predictive value for sepsis severity and outcomes. Nonlinear associations between serum ferritin and mortality have been described, with each 1,000 ng/mL increment corresponding to higher mortality rates at 28 days, 90 days, and one year [37]. Elevated ferritin is also associated with an increased incidence of sepsis [38], and levels > 1,000 ng/mL have been linked to hyperinflammatory states including sepsis, HLH, and MAS [39]. Under physiological conditions, serum ferritin ranges from 30 to 300 ng/mL in men and 10 to 200 ng/mL in women, with a plasma half-life of approximately 30 hours; its circulating levels rise markedly during viral infections and may reflect viral replication kinetics [40,41,42].
In our cohort, day 5 ferritin was significantly lower in patients with SOFA 0–4 (854 ± 682 ng/mL) than in those with SOFA ≥5 (1,110 ± 816 ng/mL; p = 0.001). Multivariate logistic regression confirmed day 5 ferritin as a statistically significant independent predictor (p = 0.014) even after adjusting for CRP, LDH, PaO2/FiO2 ratio, haemoglobin, and comorbidities. This is particularly noteworthy because CRP was itself a significant predictor in Step 1. Although both are acute-phase reactants, their induction pathways differ: CRP is a rapid, IL-6-driven hepatic response, whereas circulating ferritin originates predominantly from activated macrophages and reflects iron-mediated immunopathology—including MAS, oxidative tissue damage, and ferroptosis—through mechanisms that are at least partially CRP-independent [43,44].
The timing of day 5 measurement is clinically relevant. Day 5 represents a transitional phase between initial viral replication and the immune-mediated inflammatory amplification driving severe COVID-19. Ferritin levels at this point capture both the initial inflammatory response and the evolving cytokine storm. Consistent with prior literature, the optimal cut-off of >1,191 ng/mL showed a high-specificity, low-sensitivity profile (specificity 82.38%; sensitivity 35.78%), positioning ferritin as a rule-in rather than rule-out marker [45,46,47]. The development of ARDS—the primary cause of death when COVID-19 progresses to respiratory failure—is driven by cytokine storm and exaggerated host immune responses, in which elevated ferritin plays a central role [48].
These findings are consistent with the broader concept of a hyperferritinemic syndrome shared across AOSD, MAS, sepsis, and catastrophic antiphospholipid syndrome [14]. SARS-CoV-2 provokes macrophage activation with release of IL-6, IL-1β, and TNF-α, which directly stimulate ferritin synthesis; emerging evidence further implicates ferroptosis—an iron-dependent cell death pathway—in multi-organ injury, with ferroptosis markers correlating with lung injury severity [44]. Ferritin’s ability to predict (SOFA)-2 score beyond PaO2/FiO2 ratio suggests it captures organ-level injury extending beyond the lungs, consistent with systemic macrophage activation and iron toxicity.
4.2. PCT and (SOFA)-2 Score: Biological Context of a Negative Finding
After engaging Toll-like receptors, SARS-CoV-2 triggers an inflammatory cascade through pro-inflammatory cytokines such as IL-1 and IL-6, which can upregulate PCT production [49]. In severe COVID-19, cytokine storm and immunological hyperactivation may elevate PCT even in the absence of bacterial co-infection [50]. Nevertheless, PCT synthesis is typically induced by bacterial lipopolysaccharide and cytokines—chiefly IL-1β and TNF-α—but is physiologically suppressed during viral infections by IFN-γ. Consistent with findings from prior coronavirus epidemics (SARS, MERS) and influenza H1N1, PCT remains ≤0.5 μg/L in most patients with uncomplicated viral COVID-19, rising primarily in severe cases or fatal outcomes [51,52,53]. Meta-analytic evidence has reported a positive association between elevated PCT and increased risk of severe COVID-19 [54], yet this elevation reflects secondary bacterial superinfection or extreme hyperinflammation rather than the primary viral inflammatory cascade.
In multivariate logistic regression, neither baseline nor day 5 PCT significantly predicted (SOFA)-2 score after adjustment. PCT’s non-significance arose in a model that already included day 5 CRP (p = 0.004) and LDH—biomarkers capturing the bulk of the virally driven inflammatory signal. This statistical attenuation within a comprehensive model does not imply that PCT lacks biological relevance; rather, it indicates that PCT does not provide independent discriminatory information for organ dysfunction severity beyond what is already conveyed by these markers in COVID-19-associated sepsis. This interpretation is consistent with reports showing that PCT does not reliably identify bacterial coinfection or independently stratify viral disease severity in this population [55,56], although some observational studies have reported an association between elevated PCT and in-hospital mortality in specific COVID-19 cohorts [57,58]. The age-dependent variation in PCT’s predictive performance is also relevant for hospitalised elderly cohorts [56]. Clinically, PCT remains most valuable in its primary validated role: guiding antibiotic stewardship and identifying secondary bacterial complications in patients whose deterioration exceeds what the viral illness alone would explain.
4.3. Clinical Implications and Applicability Beyond COVID-19
The finding that day 5 ferritin independently predicts (SOFA)-2 score has direct clinical implications. First, it supports the inclusion of serial ferritin measurements—particularly around day 5—in standardised COVID-19 monitoring protocols to identify patients at risk of progressing to multi-organ dysfunction. Second, ferritin may serve as a dynamic marker of treatment response: a lack of decline by day 5 could indicate ongoing macrophage activation, prompting consideration of immunomodulatory therapies such as corticosteroids or IL-6 pathway inhibitors. Third, in resource-limited settings, ferritin’s independent predictive value—demonstrated even after adjusting for standard clinical and laboratory parameters—makes it a high-value, cost-effective tool for severity stratification.
The applicability of these findings extends beyond the COVID-19 population studied. Elevated ferritin in COVID-19 shares a common pathophysiological substrate with hyperferritinemic states in non-COVID bacterial sepsis, MAS, and septic shock—all characterised by dysregulated macrophage activation, excessive cytokine release, and iron-mediated immunopathology. Understanding the pathogenesis of sepsis and identifying therapeutic targets—including immunomodulatory approaches—remains an active area of research that may further clarify the role of ferritin and related pathways in clinical outcomes [59,60]. In non-COVID sepsis populations, ferritin has consistently emerged as an independent predictor of 28-day mortality with nonlinear dose-response relationships [37,46]. The parallel finding that PCT provides limited independent predictive value for organ dysfunction severity within a comprehensive inflammatory marker panel may also have relevance in mixed ICU populations. Clinicians managing sepsis of any aetiology may therefore consider serial ferritin measurement as a complement to existing organ dysfunction scoring systems, interpreting PCT primarily in the context of suspected bacterial co-infection rather than as a standalone severity marker.
4.4. Limitations
Several limitations should be acknowledged. First, the retrospective design limits causal inference. Second, as a retrospective study, a formal a priori power calculation was not performed; the sample size of 416 reflects real-world clinical availability. The adequacy of statistical power for the primary multivariate analyses is supported by the observation of significant effects, but subgroup analyses should be interpreted with appropriate caution. Third, day 5 ferritin and PCT values were unavailable for 80 patients who died before day 5 (17.3% of the cohort), introducing potential survivorship bias; the direction of this bias is likely conservative, as excluded patients represent the most severe cases, potentially underestimating the association between elevated biomarkers and adverse outcomes. Formal multiple imputation was not performed; analyses are therefore restricted to the 336 patients with available day 5 data. Fourth, antibiotic treatment data were not systematically included because bacterial infections were not present in all patients and no standardised regimen was administered. Fifth, patients with hereditary haemochromatosis or CKD (eGFR < 60 mL/min/1.73 m2) were excluded, limiting generalisability to these subgroups. Sixth, given the exploratory nature of multiple comparisons across biomarker subgroups, results should be interpreted in the context of the overall model, and prospective validation in independent cohorts is warranted. Seventh, the SOFA-2 score was applied retrospectively in 2026 to data collected before the score’s 2025 publication [29]. Although all variables required for (SOFA)-2 score calculation were available in the original electronic medical records, prospective application of the score may yield slightly different operating characteristics, and our findings should be re-examined in cohorts in which SOFA-2 is collected prospectively. Eighth, the diagnostic performance of day 5 ferritin at the optimal cut-off (>1,191 ng/mL) was modest (AUC 0.608; sensitivity 35.78%), reflecting a high-specificity, low-sensitivity profile. This indicates that ferritin elevation above this threshold is informative as a rule-in marker for severe organ dysfunction but cannot, in isolation, rule out severity in patients with lower ferritin levels; clinical use should therefore be as an adjunct to—not a replacement for—established multi-parameter scoring systems. Ninth, all included patients received favipiravir as part of contemporary local treatment protocols; generalisability to cohorts treated with other antiviral or immunomodulatory regimens (e.g., remdesivir, tocilizumab, baricitinib, or dexamethasone-based protocols) requires further validation, particularly given the substantial evolution of standard care during and after the study period. Finally, while the study period (2020–2021) captures an important phase of the pandemic, treatment protocols have evolved substantially, and findings may not fully generalise to later variant epochs.
5. Conclusions
Serum ferritin measured on day 5 of hospitalisation is an independent predictor of (SOFA)-2 score-based organ dysfunction severity in patients with COVID-19-associated sepsis, supporting its role as a clinically relevant adjunctive biomarker for disease stratification. A cut-off of >1,191 ng/mL provides high specificity (82.38%) but modest sensitivity (35.78%; AUC 0.608), positioning it as a rule-in rather than a rule-out marker that should prompt early escalation of monitoring and therapeutic intervention when values exceed this threshold, while not reassuring against severity when below it. In contrast, PCT did not provide independent predictive value for organ dysfunction severity in this context, consistent with its known suppression during primary viral infection; its primary utility remains in guiding antibiotic stewardship and detecting secondary bacterial complications. These findings support the consideration of serial ferritin measurement as a complement to established organ-dysfunction scoring in COVID-19 ICU monitoring protocols, pending prospective validation, and suggest broader relevance in sepsis management where macrophage activation and iron dysregulation contribute to organ failure.
Author Contributions
M.A. (Murat Ay): conceptualisation, investigation, methodology, data analysis, interpretation, writing—original draft, writing—review and editing; S.O.: discussion, writing, review, and editing; N.D.: discussion, review, and editing; E.B.: discussion, review, and editing; A.S.: discussion, review, and editing; M.A. (Merve Ay): review and editing. All authors have read and approved the published version of the manuscript.
Funding
This research did not receive any specific grants from funding agencies in the public, commercial, or not-for-profit sectors.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Clinical Research Ethics Committee of Afyonkarahisar Health Sciences University (Meeting number 2026/3; date of approval 06 March 2026)) for the retrospective re-analysis of de-identified clinical data originally collected during routine ICU care between March 2020 and June 2021. Clinical trial registration is not applicable.
Informed Consent Statement
Informed consent was waived by the ethics committee for this retrospective study. All authors have provided written consent for publication.
Data Availability Statement
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
Acknowledgments
None. AI-assisted technologies were not used in the preparation of this article.
Conflicts of Interest
The authors declare no competing financial interests or personal relationships that could have influenced the work reported in this study.
Abbreviations
The following abbreviations are used in this manuscript:
| Abbreviation | Definition |
| AOSD | Adult-Onset Still’s Disease |
| ARDS | Acute Respiratory Distress Syndrome |
| ASCVD | Atherosclerotic Cardiovascular Disease |
| AUC | Area Under the Curve |
| BAL | Bronchoalveolar Lavage |
| CI | Confidence Interval |
| CKD | Chronic Kidney Disease |
| COVID-19 | Coronavirus Disease 2019 |
| CRP | C-Reactive Protein |
| eGFR | Estimated Glomerular Filtration Rate |
| HF | Heart Failure |
| HFNO | High-Flow Nasal Oxygen |
| HLH | Haemophagocytic Lymphohistiocytosis |
| ICU | Intensive Care Unit |
| IFN | Interferon |
| IL | Interleukin |
| IQR | Interquartile Range |
| LDH | Lactate Dehydrogenase |
| MAS | Macrophage Activation Syndrome |
| OR | Odds Ratio |
| PCT | Procalcitonin |
| ROC | Receiver Operating Characteristic |
| SARS-CoV-2 | Severe Acute Respiratory Syndrome Coronavirus 2 |
| SD | Standard Deviation |
| SOFA | Sepsis-related Organ Failure Assessment |
| TLR | Toll-Like Receptor |
| TNF-α | Tumour Necrosis Factor-Alpha |
| WBC | White Blood Cell Count |
| WHO | World Health Organization |
References
- Ferrando, C.; Mellado-Artigas, R.; Gea, A.; Arruti, E.; Aldecoa, C.; Bordell, A.; Adalia, R.; Zattera, L.; Ramasco, F.; Monedero, P.; et al. Patient characteristics, clinical course and factors associated to ICU mortality in critically ill patients infected with SARS-CoV-2 in Spain: A prospective, cohort, multicentre study. Rev. Esp. Anestesiol. Reanim. (Engl. Ed.) 2020, 67, 425–437. [Google Scholar] [CrossRef] [PubMed]
- Xu, J.; Yang, X.; Yang, L.; Zou, X.; Wang, Y.; Wu, Y.; Zhou, T.; Yuan, Y.; Qi, H.; Fu, S.; et al. Clinical course and predictors of 60-day mortality in 239 critically ill patients with COVID-19: A multicenter retrospective study from Wuhan, China. Crit. Care 2020, 24, 394. [Google Scholar] [CrossRef] [PubMed]
- Zhu, N.; Wang, W.; Liu, Z.; Liang, C.; Wang, W.; Ye, F.; Huang, B.; Zhao, L.; Wang, H.; Zhou, W.; et al. Morphogenesis and cytopathic effect of SARS-CoV-2 infection in human airway epithelial cells. Nat. Commun. 2020, 11, 3910. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.; Yao, N.; Qiu, Y.; He, C. Predictive performance of SOFA and qSOFA for in-hospital mortality in severe novel coronavirus disease. Am. J. Emerg. Med. 2020, 38, 2074–2080. [Google Scholar] [CrossRef]
- Raschke, R.A.; Agarwal, S.; Rangan, P.; Heise, C.W.; Curry, S.C. Discriminant accuracy of the SOFA score for determining the probable mortality of patients with COVID-19 pneumonia requiring mechanical ventilation. JAMA 2021, 325, 1469–1470. [Google Scholar] [CrossRef]
- Moore, J.B.; June, C.H. Cytokine release syndrome in severe COVID-19. Science 2020, 368, 473–474. [Google Scholar] [CrossRef]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Kernan, K.F.; Carcillo, J.A. Hyperferritinemia and inflammation. Int. Immunol. 2017, 29, 401–409. [Google Scholar] [CrossRef]
- Bennett, T.D.; Hayward, K.N.; Farris, R.W.; Ringold, S.; Wallace, C.A.; Brogan, T.V. Very high serum ferritin levels are associated with increased mortality and critical care in pediatric patients. Pediatr. Crit. Care Med. 2011, 12, e233–e236. [Google Scholar] [CrossRef]
- Carcillo, J.A.; Sward, K.; Halstead, E.S.; Telford, R.; Jimenez-Bacardi, A.; Shakoory, B.; Simon, D.; Hall, M. A systemic inflammation mortality risk assessment contingency table for severe sepsis. Pediatr. Crit. Care Med. 2017, 18, 143–150. [Google Scholar] [CrossRef]
- Al Maqbali, M.; Al Badi, K.; Al Sinani, M.; Madkhali, N.; Dickens, G.L. Clinical features of COVID-19 patients in the first year of pandemic: A systematic review and meta-analysis. Biol. Res. Nurs. 2022, 24, 172–185. [Google Scholar] [CrossRef]
- Di Benedetto, P.; Cipriani, P.; Iacono, D.; Pantano, I.; Caso, F.; Emmi, G.; Grembiale, R.D.; Cantatore, F.P.; Atzeni, F.; Perosa, F.; et al. Ferritin and C-reactive protein are predictive biomarkers of mortality and macrophage activation syndrome in adult onset Still’s disease. PLoS ONE 2020, 15, e0235326. [Google Scholar] [CrossRef] [PubMed]
- Kyriazopoulou, E.; Leventogiannis, K.; Norrby-Teglund, A.; Dimopoulos, G.; Pantazi, A.; Orfanos, S.E.; Rovina, N.; Tsangaris, I.; Gkavogianni, T.; Botsa, E.; et al. Macrophage activation-like syndrome: An immunological entity associated with rapid progression to death in sepsis. BMC Med. 2017, 15, 172. [Google Scholar] [CrossRef]
- Rosário, C.; Zandman-Goddard, G.; Meyron-Holtz, E.G.; D’Cruz, D.P.; Shoenfeld, Y. The hyperferritinemic syndrome: Macrophage activation syndrome, Still’s disease, septic shock and catastrophic antiphospholipid syndrome. BMC Med. 2013, 11, 185. [Google Scholar] [CrossRef]
- Recalcati, S.; Invernizzi, P.; Arosio, P.; Cairo, G. New functions for an iron storage protein: The role of ferritin in immunity and autoimmunity. J. Autoimmun. 2008, 30, 84–89. [Google Scholar] [CrossRef]
- Perricone, C.; Bartoloni, E.; Bursi, R.; Cafaro, G.; Guidelli, G.M.; Shoenfeld, Y.; Gerli, R. COVID-19 as part of the hyperferritinemic syndromes: The role of iron depletion therapy. Immunol. Res. 2020, 68, 213–224. [Google Scholar] [CrossRef]
- Gómez-Pastora, J.; Weigand, M.; Kim, J.; Wu, X.; Strayer, J.; Palmer, A.F.; Zborowski, M.; Yazer, M.; Chalmers, J.J. Hyperferritinemia in critically ill COVID-19 patients—is ferritin the product of inflammation or a pathogenic mediator? Clin. Chim. Acta 2020, 509, 249–251. [Google Scholar] [CrossRef] [PubMed]
- Danwang, C.; Endomba, F.T.; Nkeck, J.R.; Wouna, D.L.A.; Robert, A.; Noubiap, J.J. A meta-analysis of potential biomarkers associated with severity of coronavirus disease 2019 (COVID-19). Biomark. Res. 2020, 8, 37. [Google Scholar] [CrossRef]
- Maruna, P.; Nedelníková, K.; Gürlich, R. Physiology and genetics of procalcitonin. Physiol. Res. 2000, 49 (Suppl. 1), S57–S61. [Google Scholar] [PubMed]
- Camporota, L.; Chiumello, D.; Busana, M.; Gattinoni, L.; Marini, J.J. Pathophysiology of COVID-19-associated acute respiratory distress syndrome. Lancet Respir. Med. 2021, 9, e1. [Google Scholar] [CrossRef]
- Schuetz, P.; Wirz, Y.; Sager, R.; Christ-Crain, M.; Stolz, D.; Tamm, M.; Bouadma, L.; Luyt, C.E.; Wolff, M.; Chastre, J.; et al. Procalcitonin to initiate or discontinue antibiotics in acute respiratory tract infections. Cochrane Database Syst. Rev. 2017, 10, CD007498. [Google Scholar] [CrossRef]
- Briel, M.; Schuetz, P.; Mueller, B.; Young, J.; Schild, U.; Nusbaumer, C.; Périat, P.; Bucher, H.C.; Christ-Crain, M. Procalcitonin-guided antibiotic use vs a standard approach for acute respiratory tract infections in primary care. Arch. Intern. Med. 2008, 168, 2000–2007. [Google Scholar] [CrossRef] [PubMed]
- Burkhardt, O.; Ewig, S.; Haagen, U.; Giersdorf, S.; Hartmann, O.; Wegscheider, K.; Hummers-Pradier, E.; Welte, T. Procalcitonin guidance and reduction of antibiotic use in acute respiratory tract infection. Eur. Respir. J. 2010, 36, 601–607. [Google Scholar] [CrossRef]
- Becker, K.L.; Nylén, E.S.; White, J.C.; Müller, B.; Snider, R.H., Jr. Procalcitonin and the calcitonin gene family of peptides in inflammation, infection, and sepsis: A journey from calcitonin back to its precursors. J. Clin. Endocrinol. Metab. 2004, 89, 1512–1525. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef]
- Zeng, Z.; Yu, H.; Chen, H.; Qi, W.; Chen, L.; Chen, G.; Yan, W.; Chen, T.; Ning, Q.; Han, M.; et al. Longitudinal changes of inflammatory parameters and their correlation with disease severity and outcomes in patients with COVID-19. Crit. Care 2020, 24, 525. [Google Scholar] [CrossRef] [PubMed]
- Su, W.; Qiu, Z.; Zhou, L.; Hou, J.; Wang, Y.; Huang, F.; Zhang, Y.; Jia, Y.; Zhou, J.; Liu, D.; et al. Sex differences in clinical characteristics and risk factors for mortality among severe patients with COVID-19. Aging 2020, 12, 18833–18843. [Google Scholar] [CrossRef]
- Xu, W.; Hou, H.; Yang, W.; Tang, W.; Sun, L. Immunologic role of macrophages in sepsis-induced acute liver injury. Int. Immunopharmacol. 2024, 143, 113492. [Google Scholar] [CrossRef]
- Ranzani, O.T.; Singer, M.; Salluh, J.I.F.; Shankar-Hari, M.; Pilcher, D.; Berger-Estilita, J.; Coopersmith, C.M.; Juffermans, N.P.; Laffey, J.; Reinikainen, M.; et al. Development and validation of the Sequential Organ Failure Assessment (SOFA)-2 Score. JAMA 2025 2025. [Google Scholar] [CrossRef]
- World Health Organization. Clinical management of severe acute respiratory infection (SARI) when COVID-19 disease is suspected: Interim guidance; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Hoeboer, S.H.; van der Geest, P.J.; Nieboer, D.; Groeneveld, A.B. The diagnostic accuracy of procalcitonin for bacteraemia: A systematic review and meta-analysis. Clin. Microbiol. Infect. 2015, 21, 474–481. [Google Scholar] [CrossRef]
- Azoulay, E.; Fartoukh, M.; Darmon, M.; Géri, G.; Voiriot, G.; Dupont, T.; Zafrani, L.; Girodias, L.; Labbé, V.; Dres, M.; et al. Increased mortality in patients with severe SARS-CoV-2 infection admitted within seven days of disease onset. Intensive Care Med. 2020, 46, 1714–1722. [Google Scholar] [CrossRef] [PubMed]
- Long, H.; Nie, L.; Xiang, X.; Li, H.; Zhang, X.; Fu, X.; Ren, H.; Liu, W.; Wang, Q.; Wu, Q. D-dimer and prothrombin time are the significant indicators of severe COVID-19 and poor prognosis. Biomed. Res. Int. 2020, 2020, 6159720. [Google Scholar] [CrossRef] [PubMed]
- Soraya, G.V.; Ulhaq, Z.S. Crucial laboratory parameters in COVID-19 diagnosis and prognosis: An updated meta-analysis. Med. Clin. (Barc.) 2020, 155, 143–151. [Google Scholar] [CrossRef]
- Liao, D.; Zhou, F.; Luo, L.; Xu, M.; Wang, H.; Xia, J.; Gao, Y.; Cai, L.; Wang, Z.; Yin, P.; et al. Haematological characteristics and risk factors in the classification and prognosis evaluation of COVID-19: A retrospective cohort study. Lancet Haematol. 2020, 7, e671–e678. [Google Scholar] [CrossRef]
- Para, O.; Caruso, L.; Pestelli, G.; Tangianu, F.; Carrara, D.; Maddaluni, L.; Tamburello, A.; Castelnovo, L.; Fedi, G.; Guidi, S.; et al. Ferritin as prognostic marker in COVID-19: The FerVid study. Postgrad. Med. 2022, 134, 58–63. [Google Scholar] [CrossRef]
- He, L.; Guo, C.; Su, Y.; Ding, N. The relationship between serum ferritin level and clinical outcomes in sepsis based on a large public database. Sci. Rep. 2023, 13, 8677. [Google Scholar] [CrossRef]
- Asrini, D.N.; Afriani, A. Association between ferritin levels and sepsis in patients with COVID-19 at Dr. M. Djamil Hospital. J. Respirologi Indones. 2024, 44, 18–27. [Google Scholar] [CrossRef]
- Taylor, M.D.; Allada, V.; Moritz, M.L.; Nowalk, A.J.; Sindhi, R.; Aneja, R.K.; Torok, K.; Morowitz, M.J.; Michaels, M.; Carcillo, J.A. Use of C-reactive protein and ferritin biomarkers in daily pediatric practice. Pediatr. Rev. 2020, 41, 172–183. [Google Scholar] [CrossRef]
- Cullis, J.O.; Fitzsimons, E.J.; Griffiths, W.J.H.; Tsochatzis, E.; Thomas, D.W. Investigation and management of a raised serum ferritin. Br. J. Haematol. 2018, 181, 331–340. [Google Scholar] [CrossRef]
- Li, Y.; Hu, Y.; Yu, J.; Ma, T. Retrospective analysis of laboratory testing in 54 patients with severe- or critical-type 2019 novel coronavirus pneumonia. Lab. Invest. 2020, 100, 794–800. [Google Scholar] [CrossRef]
- Baraboutis, I.G.; Gargalianos, P.; Aggelonidou, E.; Adraktas, A. Initial real-life experience from a designated COVID-19 centre in Athens, Greece: A proposed therapeutic algorithm. SN Compr. Clin. Med. 2020, 2, 689–693. [Google Scholar] [CrossRef] [PubMed]
- Lin, Z.; Long, F.; Yang, Y.; Chen, X.; Xu, L.; Yang, M. Serum ferritin as an independent risk factor for severity in COVID-19 patients. J. Infect. 2020, 81, 647–679. [Google Scholar] [CrossRef]
- Ahmed, S.; Ansar Ahmed, Z.; Siddiqui, I.; Haroon Rashid, N.; Mansoor, M.; Jafri, L. Evaluation of serum ferritin for prediction of severity and mortality in COVID-19—A cross-sectional study. Ann. Med. Surg. 2021, 63, 102163. [Google Scholar] [CrossRef]
- Kurian, S.J.; Mathews, S.P.; Paul, A.; Viswam, S.K.; Saravu, K.; Rao, M.; Miraj, S.S. Association of serum ferritin with severity and clinical outcome in COVID-19 patients: An observational study in a tertiary healthcare facility. Clin. Epidemiol. Glob. Health 2023, 21, 101295. [Google Scholar] [CrossRef]
- Liu, F.; Liu, Z. Association between ferritin to albumin ratio and 28-day mortality in patients with sepsis: A retrospective cohort study. Eur. J. Med. Res. 2023, 28, 414. [Google Scholar] [CrossRef]
- Chicamy, Y.A.; Safitri, A.; Nindrea, R.D. Serum ferritin levels for the prediction of mortality among COVID-19 patients in an Indonesia’s national referral hospital. Open Access Maced. J. Med. Sci. 2022, 10, 1056–1061. [Google Scholar] [CrossRef]
- Wu, C.; Chen, X.; Cai, Y.; Xia, J.; Zhou, X.; Xu, S.; Huang, H.; Zhang, L.; Zhou, X.; Du, C.; et al. Risk factors associated with acute respiratory distress syndrome and death in patients with coronavirus disease 2019 pneumonia in Wuhan, China. JAMA Intern. Med. 2020, 180, 934–943. [Google Scholar] [CrossRef] [PubMed]
- Conti, P.; Ronconi, G.; Caraffa, A.; Gallenga, C.E.; Ross, R.; Frydas, I.; Kritas, S.K. Induction of pro-inflammatory cytokines (IL-1 and IL-6) and lung inflammation by Coronavirus-19 (COVI-19 or SARS-CoV-2): Anti-inflammatory strategies. J. Biol. Regul. Homeost. Agents 2020, 34, 327–331. [Google Scholar]
- Mehta, P.; McAuley, D.F.; Brown, M.; Sanchez, E.; Tattersall, R.S.; Manson, J.J. COVID-19: Consider cytokine storm syndromes and immunosuppression. Lancet 2020, 395, 1033–1034. [Google Scholar] [CrossRef] [PubMed]
- Chen, N.; Zhou, M.; Dong, X.; Qu, J.; Gong, F.; Han, Y.; Qiu, Y.; Wang, J.; Liu, Y.; Wei, Y.; et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: A descriptive study. Lancet 2020, 395, 507–513. [Google Scholar] [CrossRef]
- Hu, R.; Han, C.; Pei, S.; Yin, M.; Chen, X. Procalcitonin levels in COVID-19 patients. Int. J. Antimicrob. Agents 2020, 56, 106051. [Google Scholar] [CrossRef] [PubMed]
- Samiullah, S.; Ahmad, A.; Patni, M.A. Unveiling the role of procalcitonin in COVID-19: A literature review. Int. J. Community Med. Public Health 2024, 11, 1011–1015. [Google Scholar] [CrossRef]
- Shen, Y.; Cheng, C.; Zheng, X.; Jin, Y.; Duan, G.; Chen, M.; Chen, S. Elevated procalcitonin is positively associated with the severity of COVID-19: A meta-analysis based on 10 cohort studies. Medicina 2021, 57, 594. [Google Scholar] [CrossRef]
- Relph, K.A.; Russell, C.D.; Fairfield, C.J.; Turtle, L.; de Silva, T.I.; Siggins, M.K.; Drake, T.M.; Thwaites, R.S.; Abrams, S.; Moore, S.C.; et al. Procalcitonin is not a reliable biomarker of bacterial coinfection in people with coronavirus disease 2019. Open Forum Infect. Dis. 2022, 9, ofac195. [Google Scholar] [CrossRef]
- Hussain, A.; Singh, L.; McAlister, J.; Jo, Y.; Makaryan, T.; Ghimire, S.; Bagchi, S.; Mehta, D.; Zheng, M.; Lipinski, J.; et al. Serum procalcitonin as a predictive biomarker in COVID-19: A retrospective cohort analysis. Cureus 2022, 14, e27816. [Google Scholar] [CrossRef]
- Liu, Z.M.; Li, J.P.; Wang, S.P.; Chen, D.Y.; Zeng, W.; Chen, S.C.; Huang, Y.H.; Huang, J.L.; Long, W.; Li, M.; et al. Association of procalcitonin levels with the progression and prognosis of hospitalized patients with COVID-19. Int. J. Med. Sci. 2020, 17, 2468–2476. [Google Scholar] [CrossRef]
- Orhan, S.; Tasdemir Mecit, B.B.; Dizen Kazan, E.; et al. The effect of acute phase reactants on the survival of COVID-19 patients in intensive care. Prog. Nutr. 2021, 23(S2), e2021268. [Google Scholar]
- Zhang, W.; Jiang, H.; Wu, G.; Huang, P.; Wang, H.; An, H.; Liu, S.; Zhang, W. The pathogenesis and potential therapeutic targets in sepsis. MedComm 2023, 4, e418. [Google Scholar] [CrossRef]
- Leventogiannis, K.; Kyriazopoulou, E.; Antonakos, N.; Kotsaki, A.; Tsangaris, I.; Markopoulou, D.; Grondman, I.; Rovina, N.; Theodorou, V.; Antoniadou, E.; et al. Toward personalized immunotherapy in sepsis: The PROVIDE randomized clinical trial. Cell Rep. Med. 2022, 3, 100817. [Google Scholar] [CrossRef]
Figure 1.
Pathophysiological mechanism of hyperferritinemia and elevated PCT in sepsis. IL, interleukin; TNF-α, tumour necrosis factor-α; LPS, lipopolysaccharide; PCT, procalcitonin.
Figure 1.
Pathophysiological mechanism of hyperferritinemia and elevated PCT in sepsis. IL, interleukin; TNF-α, tumour necrosis factor-α; LPS, lipopolysaccharide; PCT, procalcitonin.

Figure 2.
Exclusion criteria flowchart.

Figure 3.
Biomarker distribution by (SOFA)-2 score severity group. Box-plots show median and IQR for ferritin (ng/mL), PCT (μg/L), and CRP (mg/dL) at admission and on day 5. *p < 0.05, **p < 0.01, ***p < 0.001, ns = not significant (Mann–Whitney U test).
Figure 3.
Biomarker distribution by (SOFA)-2 score severity group. Box-plots show median and IQR for ferritin (ng/mL), PCT (μg/L), and CRP (mg/dL) at admission and on day 5. *p < 0.05, **p < 0.01, ***p < 0.001, ns = not significant (Mann–Whitney U test).

Figure 4.
Serial biomarker levels at admission and day 5 by (SOFA)-2 severity group. Bars represent median values; error bars represent IQR/2. Ferritin (ng/mL) and PCT (μg/L) are shown for SOFA 0–4 (mild) and SOFA ≥5 (severe) groups.
Figure 4.
Serial biomarker levels at admission and day 5 by (SOFA)-2 severity group. Bars represent median values; error bars represent IQR/2. Ferritin (ng/mL) and PCT (μg/L) are shown for SOFA 0–4 (mild) and SOFA ≥5 (severe) groups.

Figure 5.
ROC curve of day 5 ferritin.


Table 1.
Patient characteristics by (SOFA)-2 score group.
| Characteristic | Total (n = 416) | SOFA 0–4 (n = 287) | SOFA ≥5 (n = 129) | p-value |
| Demographics | ||||
| Age, years [median (IQR)] | 69 (62–76) | 68 (60.5–76) | 69 (65–75) | 0.204 |
| Male sex, n (%) | 284 (68.3%) | 193 (67.2%) | 91 (70.5%) | 0.580 |
| Clinical outcomes | ||||
| ICU mortality, n (%) | 239 (57.5%) | 127 (44.3%) | 112 (86.8%) | <0.001 |
| Mechanical ventilation, n (%) | 173 (41.6%) | 89 (31.0%) | 84 (65.1%) | <0.001 |
| HFNO, n (%) | 116 (27.9%) | 98 (34.1%) | 18 (14.0%) | <0.001 |
| Renal replacement therapy, n (%) | 51 (12.3%) | 21 (7.3%) | 30 (23.3%) | <0.001 |
| Comorbidities | ||||
| Hypertension, n (%) | 195 (46.9%) | 129 (44.9%) | 66 (51.2%) | 0.285 |
| Diabetes mellitus, n (%) | 135 (32.5%) | 85 (29.6%) | 50 (38.8%) | 0.084 |
| Heart failure (HF), n (%) | 108 (26.0%) | 59 (20.6%) | 49 (38.0%) | <0.001 |
| Coronary artery disease, n (%) | 102 (24.5%) | 56 (19.5%) | 46 (35.7%) | 0.001 |
| CKD, n (%) | 37 (8.9%) | 18 (6.3%) | 19 (14.7%) | 0.009 |
| Malignancy, n (%) | 51 (12.3%) | 32 (11.1%) | 19 (14.7%) | 0.385 |
| Treatments | ||||
| Hydroxychloroquine, n (%) | 76 (18.3%) | 42 (14.6%) | 34 (26.4%) | 0.006 |
| Plasmapheresis, n (%) | 86 (20.7%) | 62 (21.6%) | 24 (18.6%) | 0.570 |
| Cytokine adsorption, n (%) | 38 (9.1%) | 22 (7.7%) | 16 (12.4%) | 0.172 |
| Cultures obtained, n (%) | 121 (29.1%) | 81 (28.2%) | 40 (31.0%) | 0.644 |
Chi-squared or Fisher’s exact test for categorical variables; Mann–Whitney U test for age. HFNO, high-flow nasal oxygen; ICU, intensive care unit; CKD, chronic kidney disease.
Table 2.
Mean ± SD of laboratory parameters (n = 416 unless stated).
| Parameter | n | Mean ± SD |
| Procalcitonin (μg/L) | 416 | 2.4 ± 11.34 |
| Day 5 procalcitonin (μg/L) | 336 | 3.6 ± 13.4 |
| Day 5 lymphocytes (/μL) | 336 | 781.68 ± 586.38 |
| Day 5 ferritin (ng/mL) | 336 | 937.42 ± 737.09 |
| PaO2/FiO2 ratio (mmHg) | 416 | 121.62 ± 32.36 |
| Haemoglobin (g/dL) | 416 | 12.41 ± 2.13 |
| LDH (U/L) | 416 | 512.49 ± 269.91 |
| WBC (/μL) | 416 | 9,832.34 ± 4,814.84 |
| Day 5 CRP (mg/dL) | 336 | 9.57 ± 8.47 |
LDH, lactate dehydrogenase; WBC, white blood cell count; CRP, C-reactive protein; PaO2/FiO2, partial oxygen pressure/inspiratory oxygen fraction.
Table 3.
Comparison of laboratory parameters by (SOFA)-2 score group.
| Parameter | SOFA 0–4 Mean ± SD | SOFA ≥5 Mean ± SD | p-value |
| Procalcitonin (μg/L) | 1.67 ± 8.84 | 4.03 ± 15.45 | 0.001 |
| Day 5 procalcitonin (μg/L) | 2.23 ± 9.31 | 6.44 ± 19.06 | <0.001 |
| Day 5 lymphocytes (/μL) | 824.64 ± 571.27 | 692.21 ± 609.66 | 0.009 |
| Day 5 ferritin (ng/mL) | 854.39 ± 682.35 | 1,110.36 ± 816.25 | 0.001 |
| PaO2/FiO2 ratio (mmHg) | 126.35 ± 34.57 | 111.11 ± 23.76 | <0.001 |
| Haemoglobin (g/dL) | 12.58 ± 2.04 | 12.03 ± 2.28 | 0.009 |
| LDH (U/L) | 488.08 ± 239.72 | 566.80 ± 321.71 | 0.010 |
| WBC (/μL) | 9,433.41 ± 4,244.61 | 10,719.88 ± 5,809.97 | 0.056 |
| Day 5 WBC (/μL) | 13,068.06 ± 15,445.32 | 14,368.07 ± 10,967.48 | 0.008 |
| Day 5 CRP (mg/dL) | 8.11 ± 7.67 | 12.62 ± 9.25 | <0.001 |
All comparisons: Mann–Whitney U test. LDH, lactate dehydrogenase; WBC, white blood cell count; CRP, C-reactive protein; PaO2/FiO2, partial oxygen pressure/inspiratory oxygen fraction.
Table 4.
Comorbidities and hydroxychloroquine therapy by (SOFA)-2 score group.
| Variable | SOFA 0–4 n (%) | SOFA ≥5 n (%) | p-value |
| Heart failure (HF) | <0.001 | ||
| No | 228 (79.4) | 80 (62.0) | |
| Yes | 59 (20.6) | 49 (38.0) | |
| CKD | 0.005 | ||
| No | 269 (93.7) | 110 (85.3) | |
| Yes | 18 (6.3) | 19 (14.7) | |
| ASCVD | 0.001 | ||
| No | 231 (80.5) | 84 (65.1) | |
| Yes | 56 (19.5) | 45 (34.9) | |
| Hydroxychloroquine | 0.004 | ||
| No | 245 (85.4) | 95 (73.6) | |
| Yes | 42 (14.6) | 34 (26.4) |
Chi-squared test. CKD, chronic kidney disease; ASCVD, atherosclerotic cardiovascular disease.
Table 5.
Multivariate logistic regression: predictive roles of day 5 PCT and day 5 ferritin on (SOFA)-2 score.
Table 5.
Multivariate logistic regression: predictive roles of day 5 PCT and day 5 ferritin on (SOFA)-2 score.
| Variable | OR | 95% CI LL | 95% CI UL | p-value |
| Model A — Day 5 PCT (μg/L): Step 1 = covariates; Step 2 adds Day 5 PCT | ||||
| Step 1 — significant covariates | ||||
| PaO2/FiO2 ratio (mmHg) | 0.984 | 0.972 | 0.996 | 0.008 |
| Haemoglobin (g/dL) | 0.874 | 0.768 | 0.995 | 0.042 |
| LDH (U/L) | 1.001 | 1.000 | 1.002 | 0.006 |
| Day 5 CRP (mg/dL) | 1.049 | 1.015 | 1.084 | 0.004 |
| ASCVD | 2.509 | 1.011 | 6.225 | 0.047 |
| Hydroxychloroquine | 2.215 | 1.153 | 4.256 | 0.017 |
| Step 2 — Day 5 PCT added | ||||
| Day 5 PCT (μg/L) | 1.001 | 0.981 | 1.022 | 0.887 (ns) |
| Model B — Day 5 ferritin (ng/mL): Step 1 = covariates; Step 2 adds Day 5 ferritin | ||||
| Step 1 — significant covariates | ||||
| PaO2/FiO2 ratio (mmHg) | 0.982 | 0.969 | 0.994 | 0.004 |
| Haemoglobin (g/dL) | 0.876 | 0.770 | 0.998 | 0.046 |
| LDH (U/L) | 1.001 | 1.000 | 1.002 | 0.005 |
| Day 5 CRP (mg/dL) | 1.052 | 1.019 | 1.086 | 0.002 |
| Hydroxychloroquine | 2.287 | 1.185 | 4.413 | 0.014 |
| Step 2 — Day 5 ferritin added | ||||
| Day 5 ferritin (ng/mL) | 1.000 | 1.000 | 1.001 | 0.014 * |
OR, odds ratio; CI, confidence interval; LL, lower limit; UL, upper limit; ns, not significant. Non-significant covariates omitted for clarity. * p = 0.014 after full adjustment including CRP, LDH, PaO2/FiO2, haemoglobin, comorbidities, and treatment. LDH, lactate dehydrogenase; CRP, C-reactive protein; ASCVD, atherosclerotic cardiovascular disease.
Table 6.
Diagnostic performance of day 5 ferritin in predicting (SOFA)-2 score groups.
| Parameter | Cut-off (ng/mL) | AUC | Sensitivity % (95% CI) | Specificity % (95% CI) | +LR (95% CI) | −LR (95% CI) | +PV % (95% CI) | −PV % (95% CI) |
| Day 5 ferritin | >1,191 | 0.608 | 35.78 (26.8–45.5) | 82.38 (76.8–87.1) | 2.03 (1.4–3.0) | 0.78 (0.7–0.9) | 49.4 (37.9–60.9) | 72.8 (66.9–78.1) |
+PV, positive predictive value; −PV, negative predictive value; +LR, positive likelihood ratio; −LR, negative likelihood ratio; CI, confidence interval; AUC, area under the curve.
Table 7.
Laboratory parameters by day 5 PCT group [median (IQR)].
| Parameter | PCT <2 μg/L | PCT 2.01–10.00 μg/L | PCT ≥10.01 μg/L | p-value |
| Procalcitonin (μg/L) | 0.4 (0.2–0.7) | 4.6 (3.0–7.2) | 18.4 (11.4–33.8) | <0.001 |
| Day 5 lymphocytes (/μL) | 752 (380–1,108) | 582 (396–812) | 488 (228–836) | 0.027 |
| Day 5 ferritin (ng/mL) | 724 (320–1,256) | 1,094 (658–1,584) | 1,102 (704–1,568) | 0.001 |
| PaO2/FiO2 ratio (mmHg) | 114 (96–138) | 112 (88–148) | 106 (92–128) | 0.636 |
| Haemoglobin (g/dL) | 12.5 (11.0–13.8) | 12.2 (10.8–13.8) | 12.3 (11.2–13.4) | 0.938 |
| LDH (U/L) | 452 (320–628) | 544 (390–748) | 558 (382–848) | 0.052 |
| WBC (/μL) | 9,220 (6,170–12,480) | 9,440 (6,520–13,020) | 9,890 (6,040–14,140) | 0.987 |
| Day 5 WBC (/μL) | 10,520 (7,280–14,680) | 13,960 (10,060–19,260) | 14,360 (9,980–19,160) | <0.001 |
| Day 5 CRP (mg/dL) | 6.4 (2.8–11.4) | 15.2 (9.6–22.8) | 14.6 (8.4–24.2) | <0.001 |
Kruskal–Wallis test; results as median (IQR). LDH, lactate dehydrogenase; WBC, white blood cell count; CRP, C-reactive protein; PaO2/FiO2, partial oxygen pressure/inspiratory oxygen fraction.
Table 8.
Comorbidities and treatment by day 5 PCT group.
| Variable | PCT <2 μg/L n (%) | PCT 2.01–10 μg/L n (%) | PCT ≥10.01 μg/L n (%) | p-value |
| Heart failure (HF) | 0.426 | |||
| No | 203 (74.4) | 32 (76.2) | 13 (61.9) | |
| Yes | 70 (25.6) | 10 (23.8) | 8 (38.1) | |
| CKD | —ᵃ | |||
| No | 256 (93.8) | 38 (90.5) | 15 (71.4) | |
| Yes | 17 (6.2) | 4 (9.5) | 6 (28.6) | |
| ASCVD | 0.572 | |||
| No | 209 (76.6) | 31 (73.8) | 14 (66.7) | |
| Yes | 64 (23.4) | 11 (26.2) | 7 (33.3) | |
| Hydroxychloroquine | —ᵃ | |||
| No | 218 (79.9) | 32 (76.2) | 17 (81.0) | |
| Yes | 55 (20.1) | 10 (23.8) | 4 (19.0) |
ᵃ Chi-squared assumptions not met; p-values not calculated. CKD, chronic kidney disease; ASCVD, atherosclerotic cardiovascular disease.
Table 9.
Laboratory parameters by day 5 ferritin group [median (IQR)].
| Parameter | Ferritin 0–499 ng/mL | Ferritin 500–1,000 ng/mL | Ferritin ≥1,001 ng/mL | p-value |
| Procalcitonin (μg/L) | 0.4 (0.1–0.9) | 0.5 (0.2–1.4) | 1.0 (0.3–3.6) | <0.001 |
| Day 5 procalcitonin (μg/L) | 0.5 (0.2–1.1) | 1.1 (0.4–3.3) | 1.8 (0.6–5.2) | <0.001 |
| Day 5 lymphocytes (/μL) | 756 (374–1,166) | 724 (422–1,076) | 622 (290–1,028) | 0.118 |
| PaO2/FiO2 ratio (mmHg) | 116 (96–142) | 112 (90–140) | 108 (88–136) | 0.359 |
| Haemoglobin (g/dL) | 11.3 (9.8–13.0) | 12.7 (11.4–14.2) | 12.4 (10.8–14.0) | <0.001 |
| LDH (U/L) | 398 (280–560) | 442 (316–612) | 578 (388–836) | <0.001 |
| WBC (/μL) | 9,260 (5,820–12,620) | 8,780 (5,740–12,280) | 9,940 (6,600–13,740) | 0.201 |
| Day 5 WBC (/μL) | 9,860 (6,880–13,200) | 11,420 (7,360–15,380) | 14,280 (8,660–20,480) | <0.001 |
| Day 5 CRP (mg/dL) | 5.6 (2.0–10.6) | 6.8 (2.6–13.0) | 10.0 (4.4–18.6) | <0.001 |
Kruskal–Wallis test; results as median (IQR). LDH, lactate dehydrogenase; WBC, white blood cell count; CRP, C-reactive protein; PaO2/FiO2, partial oxygen pressure/inspiratory oxygen fraction.
Table 10.
Comorbidities and treatment by day 5 ferritin group.
| Variable | Ferritin 0–499 ng/mL n (%) | Ferritin 500–1,000 ng/mL n (%) | Ferritin ≥1,001 ng/mL n (%) | p-value |
| Heart failure (HF) | 0.772 | |||
| No | 71 (75.5) | 97 (74.6) | 80 (71.4) | |
| Yes | 23 (24.5) | 33 (25.4) | 32 (28.6) | |
| CKD | 0.359 | |||
| No | 89 (94.7) | 120 (92.3) | 100 (89.3) | |
| Yes | 5 (5.3) | 10 (7.7) | 12 (10.7) | |
| ASCVD | 0.837 | |||
| No | 73 (77.7) | 98 (75.4) | 83 (74.1) | |
| Yes | 21 (22.3) | 32 (24.6) | 29 (25.9) | |
| Hydroxychloroquine | 0.122 | |||
| No | 79 (84.0) | 96 (73.8) | 92 (82.1) | |
| Yes | 15 (16.0) | 34 (26.2) | 20 (17.9) |
Chi-squared analysis. CKD, chronic kidney disease; ASCVD, atherosclerotic cardiovascular disease.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



