Submitted:
05 December 2025
Posted:
09 December 2025
You are already at the latest version
Abstract
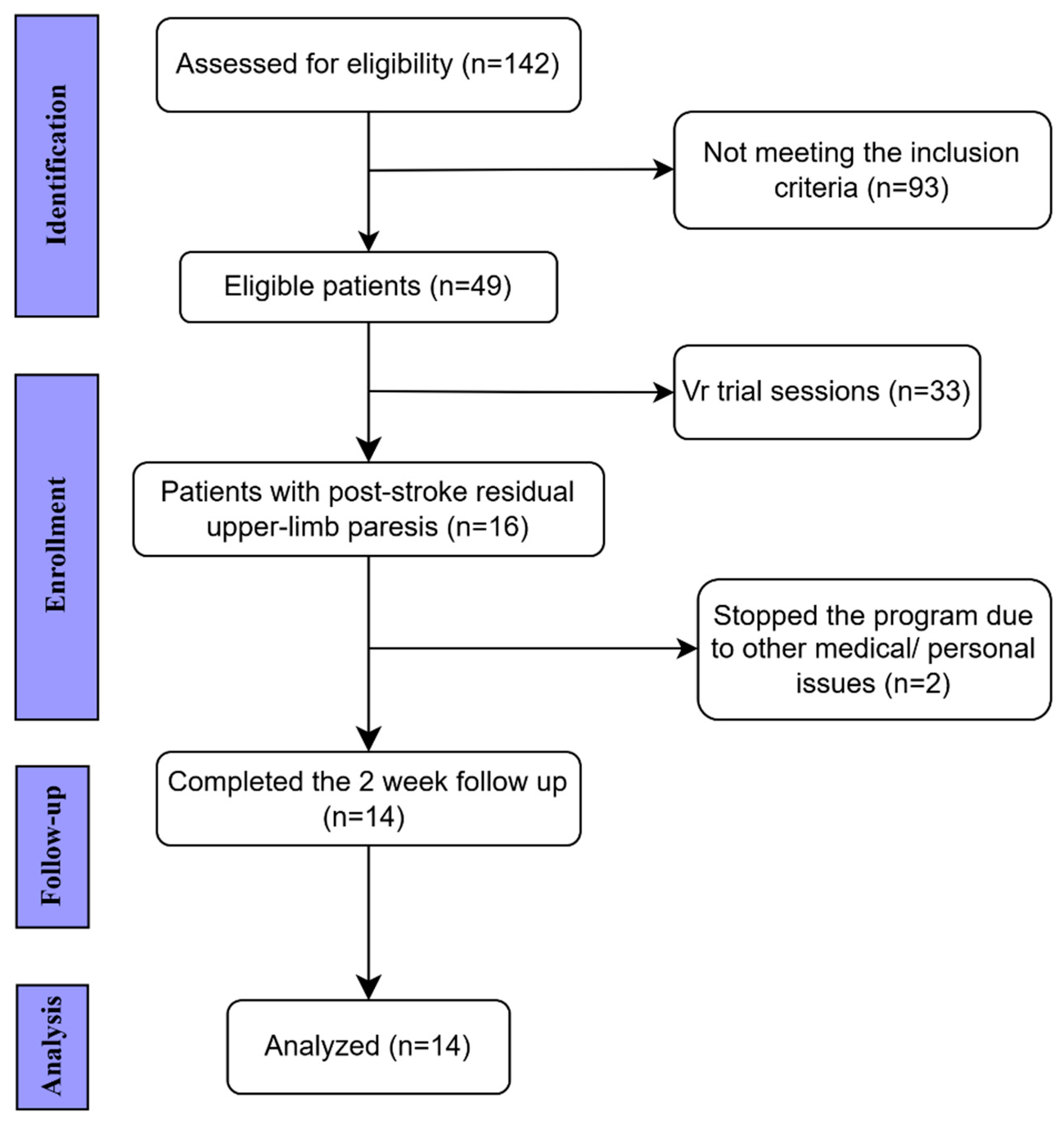
Background: Immersive virtual reality (VR) has emerged as a promising tool to enhance neuroplasticity, motivation, and engagement during post-stroke motor rehabilitation. However, evidence on its feasibility and data-driven integration into clinical practice remains limited. Objective: This pilot study aimed to evaluate the feasibility, usability, and short-term motor outcomes of an immersive VR-assisted rehabilitation program using the Travee-VR system. Methods: Fourteen adults with post-stroke upper-limb paresis completed a 10-day hybrid rehabilitation program combining conventional therapy with immersive VR sessions. Feasibility and tolerability were assessed through adherence, adverse events, the System Usability Scale (SUS), and the Simulator Sickness Questionnaire (SSQ). Motor outcomes included active and passive range of motion (AROM, PROM) and a derived GAP index (PROM–AROM). Correlations between clinical changes and in-game performance metrics were explored to identify potential digital biomarkers of recovery. Results: All participants completed the program without adverse events. Usability was rated as high (mean SUS = 79 ± 11.3), and cybersickness remained mild (SSQ < 40). Significant improvements were observed in shoulder abduction (+7.3°, p < 0.01) and elbow flexion (+5.8°, p < 0.05), with moderate-to-large effect sizes. Performance gains in the Fire and Fruits games correlated with clinical improvement in shoulder AROM (ρ = 0.45, p = 0.041). Cluster analysis identified distinct responder profiles, reflecting individual variability in neuroplastic adaptation. Conclusions: The Travee-VR system proved feasible, well tolerated, and associated with measurable short-term improvements in upper-limb function. By linking clinical outcomes with real-time kinematic data, this study supports the role of immersive, feedback-driven VR as a catalyst for data-informed neuroplastic recovery. These results lay the groundwork for adaptive, clinic-to-home rehabilitation models integrating clinical and digital biomarkers.
Keywords:
1. Introduction
1.1. Virtual Reality in Post-Stroke Rehabilitation
1.2. The Travee-VR System
1.3. Rationale and Objectives
1.4. Significance of the Study
2. Materials and Methods
2.1. Study Design, Objectives and Ethical Approval
- 1.
- Determine feasibility through adherence and session completion;
- 2.
- Assess usability and tolerability using standardized questionnaires (SUS and SSQ);
- 3.
- Evaluate pre–post changes in upper-limb motor function (AROM, PROM);
- 4.
- Characterize VR performance trajectories across games;
- 5.
- Explore correlations between VR and clinical outcomes.
2.2. Participants
2.2.1. Inclusion Criteria
- Ischemic or hemorrhagic stroke confirmed by CT/MRI;
- Upper-limb paresis with residual voluntary movement sufficient to interact with the VR interface;
- No cognitive deficits as assessed by Mini-Mental State Examination (MMSE ≥ 25);
- Cooperative behavior and ability to understand instructions during VR tasks;
- Time from stroke onset ≥ 2 months;
- Age < 80 years and >18 years.
2.2.2. Exclusion Criteria
- Other neurological conditions causing upper-limb paresis;
- Unstable cardiovascular status or uncontrolled hypertension;
- MMSE ≤ 25 or severe cognitive/psychiatric disorders limiting participation;
- Epilepsy or seizure history;
- Severe visual or severe vestibular disorders, chronic vertigo, or other conditions associated with intolerance to visual motion (e.g., migraine with aura, Ménière’s disease);
- Inability to attend the full 10-day rehabilitation program.
2.3. Timing of Assessments
2.4. Rehabilitation Protocol
2.4.1. VR Task Selection
- Rocket and Fires: large-amplitude shoulder abduction and flexion;
- Cooking: internal/external rotation control;
- Fruits to Basket: elbow flexion/extension and forearm supination/pronation;
- Road: isolated forearm rotation with sustained trajectory tracking;
- Piano and Diorama: distal wrist and finger extension with visuomotor precision.
2.4.2. VR Performance Metrics
2.5. Outcome Measures
2.5.1. Motor Function
2.5.2. Muscle Tone Assessment
2.5.3. Cognitive Screening
2.5.4. Usability and Tolerability
2.6. Statistical Analysis
2.7. Data Management and Confidentiality
2.8. Summary of Methodological Rationale
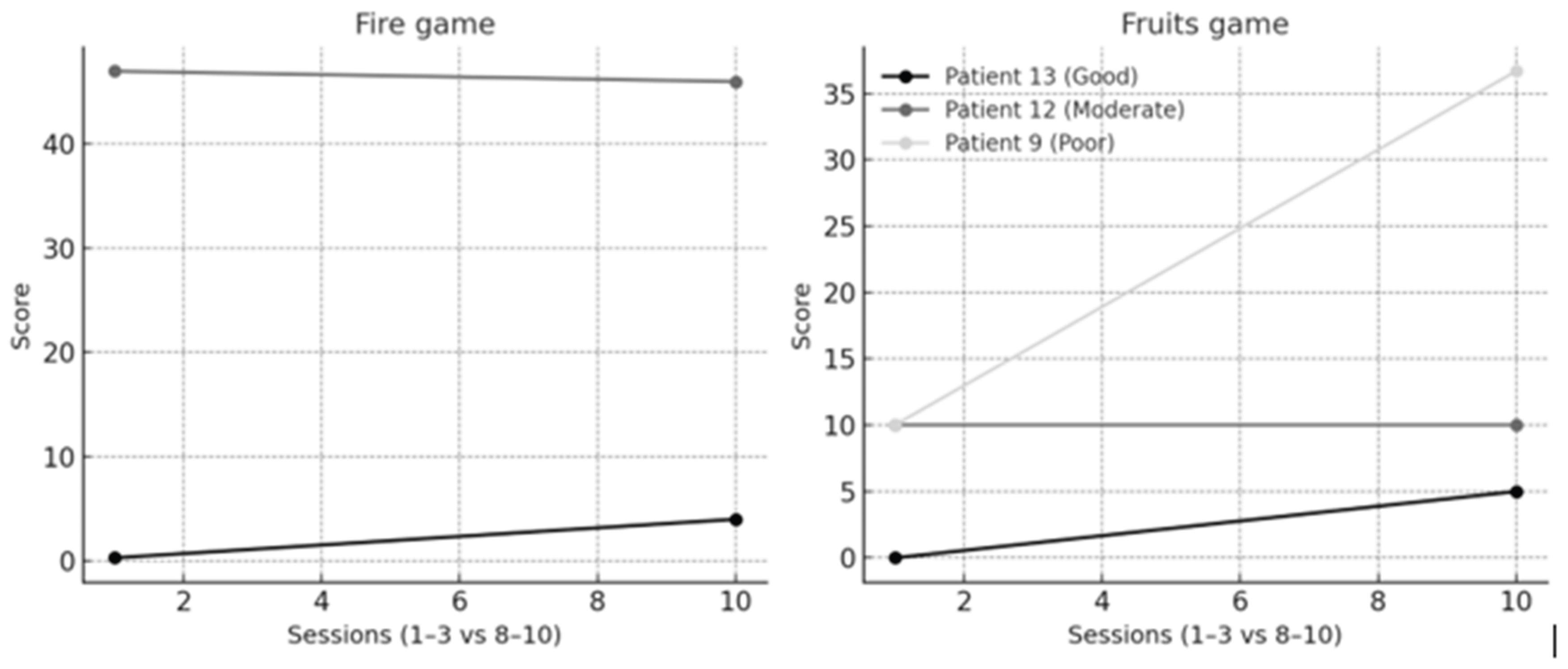
3. Results
- Good responder
- Moderate responder
- Poor responder
4. Discussion
4.1. Feasibility and Usability
4.2. Mechanisms of Motor Improvement
4.3. Functional Outcomes and Spasticity Considerations
4.4. Individual Variability and Digital Biomarkers
4.5. Cognitive Engagement and Motivational Aspects
4.6. Translational Implications
4.7. Limitations and Future Directions
5. Conclusions
Author Contributions
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Potter, T.B.H.; Tannous, J.; Vahidy, F.S. A Contemporary Review of Epidemiology, Risk Factors, Etiology, and Outcomes of Premature Stroke. Curr Atheroscler Rep. 2022, 24, 939–948. [Google Scholar] [CrossRef]
- Feigin, V.L.; Brainin, M.; Norrving, B.; Martins, S.O.; Pandian, J.; Lindsay, P.; et al. World Stroke Organization: Global Stroke Fact Sheet 2025. International Journal of Stroke 2025, 20, 132–144. [Google Scholar] [CrossRef]
- Tsao, C.W.; Aday, A.W.; Almarzooq, Z.I.; Anderson, C.A.M.; Arora, P.; Avery, C.L.; et al. Heart Disease and Stroke Statistics—2023 Update: A Report From the American Heart Association. Circulation 2023, 147. [Google Scholar] [CrossRef] [PubMed]
- Colamarino, E.; Morone, G.; Toppi, J.; Riccio, A.; Cincotti, F.; Mattia, D.; et al. A Scoping Review of Technology-Based Approaches for Upper Limb Motor Rehabilitation after Stroke: Are We Really Targeting Severe Impairment? J Clin Med. 2024, 13, 5414. [Google Scholar] [CrossRef] [PubMed]
- Takeuchi, N.; Izumi, S.I. Rehabilitation with poststroke motor recovery: a review with a focus on neural plasticity. Stroke Res Treat. 2013, 2013, 128641. [Google Scholar] [CrossRef] [PubMed]
- Ceradini, M.; Losanno, E.; Micera, S.; Bandini, A.; Orlandi, S. Immersive VR for upper-extremity rehabilitation in patients with neurological disorders: a scoping review. J Neuroeng Rehabil. 2024, 21, 75. [Google Scholar] [CrossRef]
- Chen, J.; Or, C.K.; Chen, T. Effectiveness of Using Virtual Reality–Supported Exercise Therapy for Upper Extremity Motor Rehabilitation in Patients With Stroke: Systematic Review and Meta-analysis of Randomized Controlled Trials. J Med Internet Res. 2022, 24, e24111. [Google Scholar] [CrossRef]
- Kenea, C.D.; Abessa, T.G.; Lamba, D.; Bonnechère, B. Immersive Virtual Reality in Stroke Rehabilitation: A Systematic Review and Meta-Analysis of Its Efficacy in Upper Limb Recovery. J Clin Med. 2025, 14, 1783. [Google Scholar] [CrossRef]
- Aderinto, N.; Olatunji, G.; Abdulbasit, M.O.; Edun, M.; Aboderin, G.; Egbunu, E. Exploring the efficacy of virtual reality-based rehabilitation in stroke: a narrative review of current evidence. Ann Med. 2023, 55, 2285907. [Google Scholar] [CrossRef]
- Khan, A.; Imam, Y.Z.; Muneer, M.; Al Jerdi, S.; Gill, S.K. Virtual reality in stroke recovery: a meta-review of systematic reviews. Bioelectron Med. 2024, 10, 23. [Google Scholar] [CrossRef]
- Cardile, D.; Arena, C.; Corallo, F.; Giuffrida, G.M.; Giustiniani, A.; Maggio, M.G.; et al. A systematic review on the use of virtual reality in post-stroke patients: exploring when modalities make the difference in executive and motor recovery. Front Virtual Real. 2025, 6. [Google Scholar] [CrossRef]
- Zhang, J.; Jiang, X.; Xu, Q.; Cai, E.; Ding, H. Effect of Virtual Reality-Based Training on Upper Limb Dysfunction during Post-Stroke Rehabilitation: A Meta-Analysis Combined with Meta-Regression. J Integr Neurosci. 2024, 23. [Google Scholar] [CrossRef]
- Ferche, O.; Moldoveanu, A.; Cinteza, D.; Toader, C.; Moldoveanu, F.; Voinea, A.; et al. From neuromotor command to feedback: A survey of techniques for rehabilitation through altered perception. In: 2015 E-Health and Bioengineering Conference (EHB). IEEE; 2015. p. 1–4. [CrossRef]
- Moldoveanu, A.; Ferche, O.M.; Moldoveanu, F.; Lupu, R.G.; Cinteza, D.; Constantin Irimia, D.; et al. The TRAVEE System for a Multimodal Neuromotor Rehabilitation. IEEE Access. 2019, 7, 8151–8171. [Google Scholar] [CrossRef]
- Huygelier, H.; Mattheus, E.; Vanden Abeele, V.; Van Ee, R.; Gillebert, C.R. The Use of the Term Virtual Reality in Post-Stroke Rehabilitation: A Scoping Review and Commentary. Psychol Belg 2021, 61. [Google Scholar] [CrossRef]
- Caraiman, S.; Stan, A.; Botezatu, N.; Herghelegiu, P.; Lupu, R.G.; Moldoveanu, A. Architectural Design of a Real-Time Augmented Feedback System for Neuromotor Rehabilitation. In: 2015 20th International Conference on Control Systems and Computer Science. IEEE; 2015. p. 850–5. [CrossRef]
- Norkin CC; WDJ. Measurement of Joint Motion: A Guide to Goniometry. 5th ed. F.A. Davis Company; 2016.
- Faridah, A.A.; Noor Istiqomah, I.; Kurnianto, S.; Khovifah, N. The Effectiveness of Range of Motion (ROM) on Increasing Muscle Strength in Stroke Patients: Literature Review. Nursing and Health Sciences Journal (NHSJ) 2022, 2, 137–142. [Google Scholar] [CrossRef]
- Harb AMKKS. Modified Ashworth Scale. In StatPearls [Internet]; StatPearls Publishing: Treasure Island (FL), 2025. [Google Scholar]
- Truong, Q.C.; Cervin, M.; Choo, C.C.; Numbers, K.; Bentvelzen, A.C.; Kochan, N.A.; et al. Examining the validity of the Mini-Mental State Examination ( MMSE ) and its domains using network analysis. Psychogeriatrics 2024, 24, 259–271. [Google Scholar] [CrossRef] [PubMed]
- Peres, S.C.; Pham, T.; Phillips, R. Validation of the System Usability Scale (SUS). Proceedings of the Human Factors and Ergonomics Society Annual Meeting 2013, 57, 192–196. [Google Scholar] [CrossRef]
- Uğur, E; Kurter, A; Aydın, Ç; Konukseven, BÖ. Novel Approach to the Simulator Sickness Questionnaire. J Audiol Otol. 2025, 29, 57–63. [Google Scholar] [CrossRef] [PubMed]
- Garro, F.; Chiappalone, M.; Buccelli, S.; De Michieli, L.; Semprini, M. Neuromechanical Biomarkers for Robotic Neurorehabilitation. Front Neurorobot [Internet]. 2021;Volume 15-2021. Available online: https://www.frontiersin.org/journals/neurorobotics/articles/10.3389/fnbot.2021.742163.
- Cipolla, M.J.; Liebeskind, D.S.; Chan, S.L. The importance of comorbidities in ischemic stroke: Impact of hypertension on the cerebral circulation. J Cereb Blood Flow Metab. 2018, 38, 2129–2149. [Google Scholar] [CrossRef]
- Zhang, Y.; Wang, C.; Liu, D.; Zhou, Z.; Gu, S.; Zuo, H. Association of total pre-existing comorbidities with stroke risk: a large-scale community-based cohort study from China. BMC Public Health 2021, 21, 1910. [Google Scholar] [CrossRef]
- Potcovaru, C.G.; Cinteză, D.; Săndulescu, M.I.; Poenaru, D.; Chiriac, O.; Lambru, C.; et al. The Impact of Virtual Reality as a Rehabilitation Method Using TRAVEE System on Functional Outcomes and Disability in Stroke Patients: A Pilot Study. Biomedicines 2024, 12, 2450. [Google Scholar] [CrossRef]
- Roussou, G.; Despoti, A.; Patsaki, I.; Tzoumi, D.; Leventakis, N.; Dimitriadi, N.; et al. Suitability, usability and safety of fully immersive Virtual Reality applications for motor and cognitive rehabilitation in stroke patients preliminary data. Health & Research Journal. 2024, 10, 193–205. [Google Scholar]
- Bargeri, S.; Scalea, S.; Agosta, F.; Banfi, G.; Corbetta, D.; Filippi, M.; et al. Effectiveness and safety of virtual reality rehabilitation after stroke: an overview of systematic reviews. EClinicalMedicine 2023, 64, 102220. [Google Scholar] [CrossRef]
- Diriba Kenea, C.; Gemechu Abessa, T.; Lamba, D.; Bonnechère, B. Technological Features of Immersive Virtual Reality Systems for Upper Limb Stroke Rehabilitation: A Systematic Review. Sensors 2024, 24, 3546. [Google Scholar] [CrossRef] [PubMed]
- Mares, K.; del Rocio Hidalgo Mas, M.; Watt, A.; Gregoriou, E.; Clark, A. Technical feasibility of the implementation of an intensive upper-limb rehabilitation system (NeuroVirt) intervention for stroke survivors. BMC Digital Health 2025, 3, 27. [Google Scholar] [CrossRef]
- Hsieh, Y.W.; Howe, T.H.; Lee, M.T.; Tai, R.Y.; Chen, C.C. Design and usability evaluation of an immersive virtual reality mirrored hand system for upper limb stroke rehabilitation. Sci Rep. 2025, 15, 5781. [Google Scholar] [CrossRef]
- Olana, D.D.; Abessa, T.G.; Lamba, D.; Triccas, L.T.; Bonnechere, B. Effect of virtual reality-based upper limb training on activity of daily living and quality of life among stroke survivors: a systematic review and meta-analysis. J Neuroeng Rehabil. 2025, 22, 92. [Google Scholar] [CrossRef] [PubMed]
- Lazem, H.; Harris, D.; Hall, A.; Mansoubi, M.; Pontes, R.G.; de Mello Monteiro, C.B.; et al. Validity, safety, usability, and user experience of virtual reality gamified home-based exercises in stroke. Clin Rehabil. 2025, 39, 1527–1540. [Google Scholar] [CrossRef]
- Ferrer Costa, J.; Ciudad, M.J.; González Abad, M.; Rodríguez García, J.L. Virtual Reality in Cognitive Rehabilitation: A Pilot Study on Usability and Preliminary Clinical Outcomes in Seniors with Mild Cognitive Impairment. Journal of Medical Extended Reality [Internet] 2025, 2, 30–42. Available online: https://liebertpub.com/doi/abs/10.1089/jmedxr.2024.0051.
- Kiper, P.; Godart, N.; Cavalier, M.; Berard, C.; Cieślik, B.; Federico, S.; et al. Effects of Immersive Virtual Reality on Upper-Extremity Stroke Rehabilitation: A Systematic Review with Meta-Analysis. J Clin Med. 2023, 13. [Google Scholar] [CrossRef]
- Soleimani, M.; Ghazisaeedi, M.; Heydari, S. The efficacy of virtual reality for upper limb rehabilitation in stroke patients: a systematic review and meta-analysis. BMC Med Inform Decis Mak. 2024, 24, 135. [Google Scholar] [CrossRef]
- Liu, Y.; Li, J.H.; Tao, J.Y.; Li, Y.Z.; Xiong, H. Virtual reality combined with task-oriented circuit training for upper limb rehabilitation in subacute stroke patients: A randomized controlled trial. Medicine 2025, 104, e43505. [Google Scholar] [CrossRef]
- Chen, L.; Chen, Y.; Fu, WBin; Huang, D.F.; Lo, W.L.A. The Effect of Virtual Reality on Motor Anticipation and Hand Function in Patients with Subacute Stroke: A Randomized Trial on Movement-Related Potential. Neural Plast. 2022, 2022, 7399995. [Google Scholar] [CrossRef]
- Nath, D.; Singh, N.; Saini, M.; Banduni, O.; Kumar, N.; Srivastava, M.V.P.; et al. Clinical potential and neuroplastic effect of targeted virtual reality based intervention for distal upper limb in post-stroke rehabilitation: a pilot observational study. Disabil Rehabil. 2024, 46, 2640–2649. [Google Scholar] [CrossRef]
- Connelly, N.; Welsby, E.; Lange, B.; Hordacre, B. Virtual Reality Action Observation and Motor Imagery to Enhance Neuroplastic Capacity in the Human Motor Cortex: A Pilot Double-blind, Randomized Cross-over Trial. Neuroscience 2024, 549, 92–100. [Google Scholar] [CrossRef]
- Alsubiheen, A.M.; Choi, W.; Yu, W.; Lee, H. The Effect of Task-Oriented Activities Training on Upper-Limb Function, Daily Activities, and Quality of Life in Chronic Stroke Patients: A Randomized Controlled Trial. Int J Environ Res Public Health 2022, 19, 14125. [Google Scholar] [CrossRef]
- Seki, M.; Hase, K.; Takahashi, H.; Liu, M. Comparison of three instruments to assess changes of motor impairment in acute hemispheric stroke: the Stroke Impairment Assessment Set (SIAS), the National Institute of Health Stroke Scale (NIHSS) and the Canadian Neurological Scale (CNS). Disabil Rehabil. 2014, 36, 1549–1554. [Google Scholar] [CrossRef] [PubMed]
- van der Groen, O.; Ghosh, M.; Norman, R.; Kuceyeski, A.; Tozlu, C.; Kimberley, T.J.; et al. Point of View on Outcome Prediction Models in Post-Stroke Motor Recovery. Neurorehabil Neural Repair. 2024, 38, 386–398. [Google Scholar] [CrossRef]
- Demeco, A.; Zola, L.; Frizziero, A.; Martini, C.; Palumbo, A.; Foresti, R.; et al. Immersive Virtual Reality in Post-Stroke Rehabilitation: A Systematic Review. Sensors 2023, 23, 1712. [Google Scholar] [CrossRef] [PubMed]
- Georgiev, D.; Georgieva, I.; Gong, Z.; Nanjappan, V.; Georgiev, G. Virtual Reality for Neurorehabilitation and Cognitive Enhancement. Brain Sci. 2021, 11, 221. [Google Scholar] [CrossRef] [PubMed]
- Feitosa, J.A.; Casseb, R.F.; Camargo, A.; Brandao, A.F.; Li, L.M.; Castellano, G. Graph analysis of cortical reorganization after virtual reality-based rehabilitation following stroke: a pilot randomized study. Front Neurol. 2023, 14, 1241639. [Google Scholar] [CrossRef]
- Choy, C.S.; Fang, Q.; Neville, K.; Ding, B.; Kumar, A.; Mahmoud, S.S.; et al. Virtual reality and motor imagery for early post-stroke rehabilitation. Biomed Eng Online 2023, 22, 66. [Google Scholar] [CrossRef]
- Dayan, E.; Cohen, L.G. Neuroplasticity Subserving Motor Skill Learning. Neuron 2011, 72, 443–454. [Google Scholar] [CrossRef]
- Huang, C.Y.; Chiang, W.C.; Yeh, Y.C.; Fan, S.C.; Yang, W.H.; Kuo, H.C.; et al. Effects of virtual reality-based motor control training on inflammation, oxidative stress, neuroplasticity and upper limb motor function in patients with chronic stroke: a randomized controlled trial. BMC Neurol. 2022, 22, 21. [Google Scholar] [CrossRef] [PubMed]
- Quan, W.; Liu, S.; Cao, M.; Zhao, J. A Comprehensive Review of Virtual Reality Technology for Cognitive Rehabilitation in Patients with Neurological Conditions. Applied Sciences 2024, 14, 6285. [Google Scholar] [CrossRef]
- Abd El-Kafy, E.M.; Alshehri, M.A.; El-Fiky, A.A.R.; Guermazi, M.A.; Mahmoud, H.M. The Effect of Robot-Mediated Virtual Reality Gaming on Upper Limb Spasticity Poststroke: A Randomized-Controlled Trial. Games Health J [Internet] 2022, 11, 93–103. [Google Scholar] [CrossRef] [PubMed]
- Abd El-Kafy, E.M.; Alshehri, M.A.; El-Fiky, A.A.R.; Guermazi, M.A.; Mahmoud, H.M. The Effect of Robot-Mediated Virtual Reality Gaming on Upper Limb Spasticity Poststroke: A Randomized-Controlled Trial. Games Health J. 2022, 11, 93–103. [Google Scholar] [CrossRef]
- Pelosi, A.D.; Roth, N.; Yehoshua, T.; Itah, D.; Braun Benyamin, O.; Dahan, A. Personalized rehabilitation approach for reaching movement using reinforcement learning. Sci Rep. 2024, 14, 17675. [Google Scholar] [CrossRef]
- Maier, M.; Ballester, B.R.; Verschure, P.F.M.J. Principles of Neurorehabilitation After Stroke Based on Motor Learning and Brain Plasticity Mechanisms. Front Syst Neurosci [Internet]. 2019;Volume 13-2019. Available online: https://www.frontiersin.org/journals/systems-neuroscience/articles/10.3389/fnsys.2019.00074.
- Zhao, J.; Guo, J.; Chen, Y.; Li, W.; Zhou, P.; Zhu, G.; et al. Improving rehabilitation motivation and motor learning ability of stroke patients using different reward strategies: study protocol for a single-center, randomized controlled trial. Front Neurol. 2024, 15, 1418247. [Google Scholar] [CrossRef]
- Kanzler, C.M.; Armand, T.; Simovic, L.; Sylvester, R.; Domnik, N.; Eilfort, A.M.; et al. Influence of virtual reality and task complexity on digital health metrics assessing upper limb function. J Neuroeng Rehabil. 2024, 21, 125. [Google Scholar] [CrossRef]
- Ceradini, M.; Losanno, E.; Micera, S.; Bandini, A.; Orlandi, S. Immersive VR for upper-extremity rehabilitation in patients with neurological disorders: a scoping review. J Neuroeng Rehabil. 2024, 21, 75. [Google Scholar] [CrossRef] [PubMed]
- Beard, J.; Williams, G.; Kahn, M.; Banky, M. The Modified Ashworth and Modified Tardieu Scales differ in their classification of lower limb spasticity. Clin Rehabil. 2025. [Google Scholar] [CrossRef] [PubMed]

| Game | Representative Metric Used in Analysis | Targeted Movements/ Functional Focus |
Game Objective |
|---|---|---|---|
| Fires | Targets extinguished | Shoulder abduction and flexion; proximal reach; visual–motor coordination | Extinguish virtual fires using upper-limb reaching movements |
| Rocket | In-game score (points) | Shoulder abduction and flexion; rapid activation and motor control | Control a rocket to intercept targets using shoulder elevation |
| Road | Checkpoints reached | Forearm pronation–supination; bilateral coordination; sustained control | Steer along a virtual road using forearm rotation |
| Fruits to Basket | Fruits caught | Elbow flexion–extension; forearm pronation–supination; grasp–release coordination | Catch and place fruits into baskets using coordinated reaching |
| Diorama | Completion rate (%) | Wrist flexion–extension; precision and fine-motor control | Interact with small virtual objects requiring fine control |
| Cooking | Participation only (qualitative) | Shoulder internal/external rotation; visuomotor planning | Simulate cooking gestures to train shoulder rotation |
| Piano | Participation only (qualitative) | Wrist flexion–extension; rhythmic and timing coordination | Press virtual piano keys using distal wrist/finger movement |
| Sex/Age | No. | Stroke type (Ischemic/Hemorrhagic) | Lesion location | Affected side (left/right) | Time from onset (months) | SIAS U/L Proximal |
|---|---|---|---|---|---|---|
| M/54 | 1 | Hemorrhagic | Right hemispheric hemorrhage | Left | 8 months | 4 |
| M/53 | 2 | Ischemic | Right MCA territory infarct | Left | 18 months | 3 |
| M/57 | 3 | Ischemic | Right vertebrobasilar territory infarct | Left | 5 months | 4 |
| M/55 | 4 | Ischemic | Left vertebrobasilar territory infarct | Right | 6 months | 3 |
| F/53 | 5 | Ischemic | Right MCA territory infarct | Left | 48 months | 4 |
| M/67 | 6 | Ischemic | Right MCA territory infarct | Left | 2 months | 2 |
| F/73 | 7 | Ischemic | Right MCA territory infarct | Left | 18 months | 3 |
| M/52 | 8 | Ischemic | Right vertebrobasilar territory infarct | Left | 2 months | 4 |
| M/48 | 9 | Hemorrhagic | Right hemispheric hemorrhage | Right | 2 months | 4 |
| M/43 | 10 | Ischemic | Bilateral MCA territory infarct | Bilateral | 4 months | 4 |
| M/66 | 11 | Ischemic | Right MCA territory infarct | Left | 10 months | 3 |
| M/58 | 12 | Ischemic | Right MCA territory infarct | Left | 48 months | 3 |
| M/50 | 13 | Ischemic | Right MCA territory infarct | Left | 14 months | 2 |
| M/45 | 14 | Hemorrhagic | Right hemispheric hemorrhage | Left | 120 months | 4 |
| Outcome | Mean ± SD | Median | IQR | p-value |
|---|---|---|---|---|
| SUS_total | 79.0 ± 11.3 | 80.5 | 17.8 | - |
| SSQ_pre | 26.4 ± 11.6 | 24.3 | 16.8 | - |
| SSQ_post | 35.5 ± 14.4 | 37.3 | 22.3 | - |
| SSQ (Δ pre vs post) | - | - | - | p = 0.135 ns |
| Outcome | Pre (mean ± SD, median, IQR) | Post (mean ± SD, median, IQR) | Δ (Post–Pre) | N paired | p-value (Wilcoxon) |
|---|---|---|---|---|---|
| Shoulder abduction (AROM) | 98.6 ± 19.0 (median 100.0, IQR 86.2–110.0) | 102.3 ± 18.3 (median 102.0, IQR 90.0–113.8) | 3.7 ± 3.7 (median 5.0, IQR 0.0–5.0) | 14 | 0.0097 |
| Shoulder abduction (PROM) | 120.6 ± 17.0 (median 120.0, IQR 109.2–136.8) | 124.8 ± 15.4 (median 123.5, IQR 110.8–137.5) | 4.1 ± 4.1 (median 4.0, IQR 0.0–5.0) | 14 | 0.0074 |
| Shoulder abduction GAP | 22.1 ± 11.2 (median 20.0, IQR 16.2–24.0) | 22.5 ± 11.2 (median 20.0, IQR 19.2–22.2) | 0.4 ± 3.9 (median 0.0, IQR 0.0–0.0) | 14 | 0.6845 |
| Shoulder flexion (AROM) | 101.1 ± 31.9 (median 110.0, IQR 83.2–116.8) | 104.4 ± 30.9 (median 110.0, IQR 90.0–121.0) | 3.4 ± 3.0 (median 4.0, IQR 0.0–5.0) | 14 | 0.0065 |
| Shoulder external rotation (AROM) | 41.1 ± 28.1 (median 40.0, IQR 15.8–67.8) | 45.3 ± 26.3 (median 42.5, IQR 21.5–69.5) | 4.2 ± 3.3 (median 5.0, IQR 1.0–5.0) | 14 | 0.0045 |
| Elbow flexion (AROM) | 135.3 ± 16.2 (median 140.0, IQR 132.5–143.8) | 137.6 ± 14.8 (median 141.5, IQR 134.8–145.8) | 2.4 ± 2.6 (median 2.0, IQR 1.0–2.8) | 14 | 0.0020 |
| Elbow flexion (PROM) | 137.4 ± 14.9 (median 140.0, IQR 136.2–147.2) | 141.1 ± 10.9 (median 142.5, IQR 140.0–149.0) | 3.7 ± 5.4 (median 2.0, IQR 1.0–4.5) | 14 | 0.0032 |
| Elbow flexion GAP | 2.1 ± 3.2 (median 0.0, IQR 0.0–5.0) | 3.5 ± 7.5 (median 0.0, IQR 0.0–4.8) | 1.4 ± 4.8 (median 0.0, IQR 0.0–0.0) | 14 | 0.2850 |
| Wrist extension (AROM) | 32.9 ± 22.3 (median 40.0, IQR 11.2–48.8) | 35.2 ± 21.4 (median 40.0, IQR 16.2–49.2) | 2.3 ± 3.1 (median 1.0, IQR 0.0–3.0) | 14 | 0.0176 |
| Wrist extension (PROM) | 54.4 ± 18.2 (median 60.0, IQR 50.0–65.8) | 56.3 ± 17.1 (median 60.0, IQR 50.0–67.8) | 1.9 ± 2.2 (median 1.0, IQR 0.0–4.5) | 14 | 0.0158 |
| Wrist extension GAP | 21.4 ± 18.4 (median 15.0, IQR 10.0–23.8) | 21.1 ± 18.5 (median 14.0, IQR 10.0–22.5) | -0.4 ± 2.9 (median 0.0, IQR -1.8–0.0) | 14 | 0.6049 |
| Forearm pronation (AROM) | 80.1 ± 3.5 (median 80.0, IQR 80.0–80.0) | 80.3 ± 3.6 (median 80.0, IQR 80.0–80.0) | 0.2 ± 0.8 (median 0.0, IQR 0.0–0.0) | 14 | 0.3173 |
| Forearm pronation (PROM) | 90.0 ± 0.0 (median 90.0, IQR 90.0–90.0) | 90.0 ± 0.0 (median 90.0, IQR 90.0–90.0) | 0.0 ± 0.0 (median 0.0, IQR 0.0–0.0) | 14 | 1.0000 |
| Forearm pronation GAP | 9.9 ± 3.5 (median 10.0, IQR 10.0–10.0) | 9.7 ± 3.6 (median 10.0, IQR 10.0–10.0) | -0.2 ± 0.8 (median 0.0, IQR 0.0–0.0) | 14 | 0.3173 |
| Game | Metric | First 3 sessions | Last 3 sessions | Δ (mean) | p-value |
|---|---|---|---|---|---|
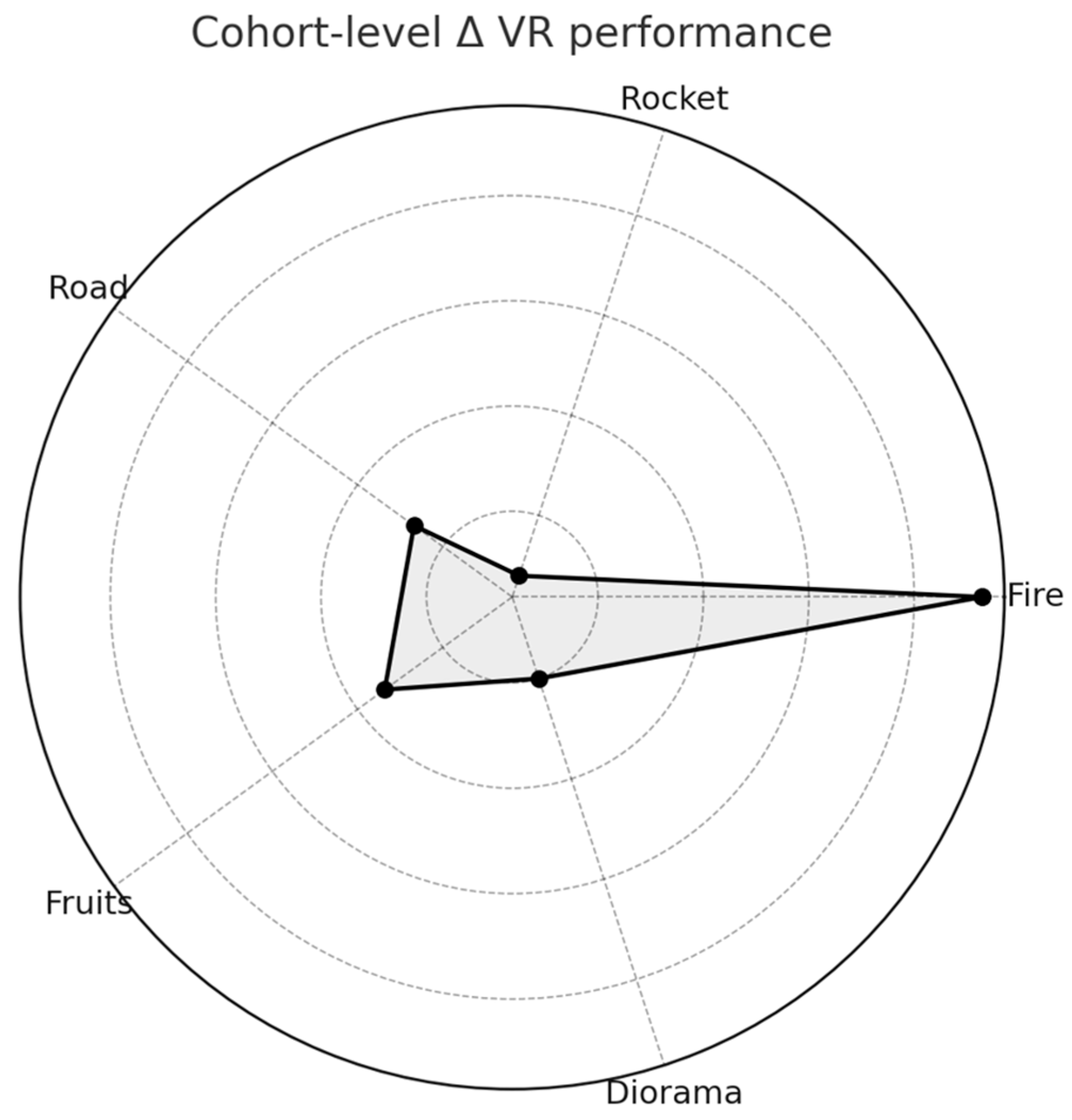
| Fire | Targets extinguished | 49.6 ± 39.8, 41.4 [37.4–50.8] | 86.1 ± 54.0, 89.3 [45.0–125.5] | 36.4 | 0.004 |
| Rocket | Score (points) | 35.9 ± 33.0, 25.0 [20.0–31.0] | 29.9 ± 13.4, 31.0 [23.0–36.5] | -6.0 | 0.310 ns |
| Road | Checkpoints reached | 86.4 ± 19.0, 98.3 [78.2–99.6] | 89.8 ± 29.9, 100.0 [99.7–100.0] | 3.4 | 0.161 ns |
| Fruits | Fruits caught | 8.7 ± 5.9, 10.0 [4.7–10.5] | 15.6 ± 9.6, 13.0 [10.0–20.0] | 6.8 | 0.034 |
| Diorama | Completion (%) | 12.6 ± 4.2, 14.0 [14.0–14.0] | 12.6 ± 4.2, 14.0 [14.0–14.0] | 0.0 | — |
| Piano | Played (Y/N) | — | — | Participated | — |
| Cooking | Played (Y/N) | — | — | Participated | — |
| Patient ID | Fire Δ (targets) | Rocket Δ (points) | Road Δ (checkpoints) | Fruits Δ (items) | Diorama Δ (pieces) | Composite VR score |
|---|---|---|---|---|---|---|
| 4 | 55 | 0 | 55.6 | 18 | — | 0.93 |
| 3 | 123.3 | 17.6 | — | — | 0 | 0.87 |
| 5 | 106 | 28 | 25 | 11 | 0 | 0.74 |
| VR Game | Clinical outcome (Δ AROM) | ρ (Spearman) | p-value | N |
|---|---|---|---|---|
| Fire | Shoulder abduction | 0.45 | 0.041 | 14 |
| Rocket | Shoulder abduction | 0.28 | 0.19 | 14 |
| Rocket | Shoulder flexion | 0.22 | 0.28 | 14 |
| Road | Forearm pronation | 0.05 | 0.82 | 13 |
| Road | Forearm supination | 0.11 | 0.65 | 13 |
| Fruits | Forearm pronation | 0.18 | 0.39 | 13 |
| Fruits | Forearm supination | 0.09 | 0.71 | 13 |
| Diorama | Wrist extension | 0.14 | 0.55 | 12 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).



