Submitted:
17 November 2025
Posted:
18 November 2025
You are already at the latest version
Abstract
Chronic kidney disease (CKD) is a growing global health burden for which there are no curative treatments; therefore, it is essential to implement preventive and kidney-protective strategies. The renal kallikrein-kinin system (KKS) is a vasodilator, anti-inflammatory, and antifibrotic pathway located in the distal nephron, whose decline contributes to hypertension and CKD progression. A thorough evaluation of both experimental and clinical data was undertaken to ascertain the interactions between dietary potassium, renal KKS activity, and kidney protection. A particular focus was placed on animal models of proteinuria, tubulointerstitial damage, and salt-sensitive hypertension, in conjunction with human studies on potassium intake and renal outcomes. Experimental models show that potassium-rich diets stimulate renal kallikrein synthesis, increase urinary kallikrein activity, and up-regulate kinin B₂ receptor expression, leading to reduced blood pressure, oxidative stress, apoptosis, inflammation, and fibrosis. These effects are lost with B₂ receptor blockade. In humans, higher potassium intake enhances kallikrein excretion and lowers cardiovascular and renal risk, independently of aldosterone, and low potassium intake has the potential to exacerbate CKD progression. Notwithstanding the concerns that have been raised regarding the potential necessity of increasing potassium intake in cases of advanced CKD, extant evidence would appear to indicate that potassium excretion persists until late disease stages. Activation and preservation of the renal KKS through a potassium-rich diet represents a rational, low-cost renoprotective strategy. Combined with sodium reduction and nutritional education, this approach could mitigate CKD progression and improve cardiovascular health on a population scale.
Keywords:
potassium
; kallikrein
; kinins
; kidney
; renoprotection
Introduction
Chronic kidney disease has been identified as a significant public health concern on a global scale. The prevalence of end-stage renal disease has increased by 40% between 2003 and 2016 [1], and this trend will continue to rise, driven by obesity, hypertension, and diabetes pandemic, coupled with increased life expectancy and lower mortality. This will ensure the ongoing increase in the number of patients requiring renal replacement therapies [2]. In light of the present circumstances, wherein a cure remains elusive for numerous acquired kidney diseases and accessible gene therapy for genetic forms of nephropathy is not yet available, it is imperative to prioritize prevention and kidney protection. Considering these aspects, it is imperative to formulate optimal strategies that comprehensively support our patients throughout their arduous journey to dialysis and that are aimed at preserving their kidney function to the greatest extent possible [3].
Proteinuric glomerulopathies are a primary cause of chronic kidney damage. They primarily affect the glomerulus by altering the selectivity of the glomerular filtration barrier and resulting in proteinuria, which is associated with progressive deterioration of kidney function. A substantial body of research has evidenced the nephrotoxicity of proteinuria and its underlying mechanisms, encompassing the activation of transcription factors in renal tubular cells, the production of proinflammatory cytokines, the recruitment of leukocytes, the development of tubulointerstitial inflammation, and the production of profibrogenic factors [4]. The result is the established correlation between proteinuria, tubulointerstitial damage, and fibrosis, a finding with full applicability to human kidney disease [5,6,7].
The process of interstitial fibrosis is preceded by several distinct biological events, including leukocyte infiltration, the release of inflammatory mediators, the differentiation of resident cells, the proliferation of interstitial fibroblasts, tubular dilation, local activation of the renin-angiotensin system (RAS), and the release of vasoconstrictive substances. These events collectively result in increased protein deposition in the extracellular matrix [8,9]. In addition to the damage to the tubulointerstitium and the activation of vasopressor mechanisms, there would be a reduction in the activity of vasodilator systems. It is now widely accepted that the extent of tubulointerstitial damage plays a pivotal role in the progression of chronic kidney disease. Its damage has been identified as a reliable marker of a worse prognosis, particularly with regard to accelerated functional decline [10]. Consequently, it appears rational to concentrate available efforts on achieving effective protection of the tubulointerstitium.
The Renal Kallikrein-Kinin System
The renal kallikrein-kinin system (KKS) is an important vasodilator system located precisely in the renal tubulointerstitial compartment [11]. It is a multienzymatic complex in which their major components are an enzyme (renal kallikrein, KLK1), its substrates (renal high- and low-molecular-weight kininogens), effector bioactive peptides (kinins: lys-bradykinin and bradykinin), the kinin metabolizing enzymes (angiotensin-converting enzyme and neutral endopeptidase, among others), the kinin receptors (B1 and B2) and several activators/inhibitors of the system [12]. Kallikrein production occurs in connecting tubule cells in the renal cortex [13], whereas its substrates, the kininogens, are synthesized downstream in collecting tubule cells [14]. The anatomic vicinity of cells responsible for the synthesis of both components makes possible kinin formation and action at the luminal side of the distal nephron cells as well as in the peritubular space [15] affecting renal blood flow and electrolyte and water excretion. Another important anatomical feature is the close proximity that exist in the human and rat kidney between connecting tubule cells and the glomerular vascular pole and specifically with the afferent arteriole, the site of renin synthesis and storage (Figure 1); this anatomical proximity points to a key physiological relationship between vasopressor and vasodepressor systems in regulating renal blood flow. The kinin B2R, which has been revealed to be constitutively expressed not just in the kidney but also in a variety of different cell types [11], is the primary mechanism by which kinin peptides produced within the kidney operate in a paracrine manner [16]. One of the key targets of kinin action is the collecting duct cell that expresses kinin B2R on both basolateral and luminal cell membranes. Selective antagonists are available for this ligand, with the most widely used in experimental settings being Icatibant (JE049), formerly known as HOE140 [17].
A substantial body of research involving animal models has demonstrated the critical role of the renal KKS in regulating blood pressure. A decline in kallikrein activity has been repeatedly observed in various hypertension models [18,19]. These findings align with the observations made in human subjects, where a decrease in urinary kallikrein levels has been documented in individuals diagnosed with essential hypertension [20], salt-dependent hypertensive individuals who show reduced urinary kallikrein levels compared to salt-resistant individuals [21], and evidence of the hypotensive effect of pharmacological administration of KKS components to hypertensive subjects. Without ignoring the influence of hypertension on the progressive course of chronic kidney disease, the significance of proper KKS function extends beyond its role in regulating blood pressure. It is imperative to acknowledge the diverse array of biological functions exhibited by kinins, which encompasses the inflammatory process [22]. These peptides have been observed to possess an anti-inflammatory effect that appears to be contingent upon the B2R, thereby reducing cell migration [23].
Our group has been conducting research into the role of renal KKS in the pathogenesis of hypertension associated with kidney damage. To this end, experimental models of non-immune tubulointerstitial damage that lead to salt sensitivity, such as 5/6 nephrectomy, inhibition of nitric oxide (NO) synthesis with L-NAME, and the model of proteinuria due to intraperitoneal albumin overload, have been used [24]. In the various models examined, particularly in the albumin overload model [25], we have successfully demonstrated a significant downregulation of KKS [24,25,26,27]. This deficiency, which manifests during the induction of damage and persists for an extended period, has been substantiated through both histological examinations (employing immunohistochemical techniques specific for renal kallikrein) and urinary kallikrein enzyme activity measurements. The alteration is most likely associated with the tubulointerstitial damage induced by proteinuria, which involves the structures where the key enzyme is produced, resulting in a reduction of the immunoreactive kallikrein detected by immunohistochemistry. So far, there are no studies addressing the levels of renal kininogens in any of these experimental models.
Therefore, it is crucial to comprehend the relationship between proper function, or the necessary preservation of the KKS, in order to achieve a possible renoprotective effect. Reduced kallikrein levels in patients with mild or advanced renal failure are of particular relevance [28,29], as are human data associating a higher incidence of chronic renal failure to the presence of polymorphisms in the kallikrein [30] and kinin B2R genes [31].
Relations Between KKS and Renin-Angiotensin Aldosterone System
In recent years, there have been notable research efforts aimed at understanding the role of RAS in hypertension and also in the progressive nature of chronic kidney disease [32]; however, equal attention has not been paid to counter-regulatory systems, particularly the KKS. This is surprising, given that both systems are located in the kidney, share some components, are anatomically close to each other, and even act on similar effectors [33].
An important consideration regarding the potential renoprotective role of kinins arises from the postulate that these peptides may play a role in the effect of angiotensin-converting enzyme (ACE) inhibitor drugs. ACE inhibitors, which reduce angiotensin levels while increasing kinin levels by reducing their catabolism, are capable of reducing proteinuria, the severity of glomerulosclerosis, the intensity of tubulointerstitial damage, and fibrosis in several experimental models [34]. These drugs, used in diabetic nephropathy and cardiovascular diseases [35,36], can lose much of their effect if kinin receptors are blocked with specific antagonists [37]. This approach is particularly pertinent given the widespread use of ACE inhibitors in contemporary medicine, which has demonstrated efficacy in reducing proteinuria and the risk of developing end-stage renal disease in human diseases [38]. ACE inhibitors protect against the development of glomerulosclerosis through mechanisms unrelated to their antihypertensive action by reducing fibronectin production, an effect that can be attenuated by the use of HOE 140, a kinin B2R antagonist [39]. A potential antifibrotic role for KKS has been proposed through the use of kallikrein siRNA, demonstrating increases in the production of tissue plasminogen activator, fibronectin, and transforming growth factor-beta (TGF-b) [40].
It is worth mentioning that ACE is also known as kininase II, an enzyme capable of inactivating kinins in the circulation [41]. Notwithstanding the previous description that genetic changes associated with ACE hyperactivity, and therefore lower availability of kinins due to increased catabolism, may accentuate organ damage in diabetes mellitus or situations of cardiac or renal ischemia [42,43]; the genetic inactivation of KLK1 kallikrein and kinin receptors has shown similar effects [42,43,44,45,46].
ACE inhibitors were initially designed to treat high blood pressure by blocking angiotensin II formation. They were later found to be beneficial in conditions involving excessive vasoconstriction, such as heart failure and diabetic nephropathy. ACE inhibitors are now recognized as having a general cardiovascular protective role in high-risk individuals [47]. Studies performed on both experimental models and humans have documented an increase in circulating kinin levels during the use of ACE inhibitors. Additionally, a loss of the tissue-protective effect has been observed in animals deficient in kallikrein, kinins, or kinin receptors, as well as in those treated concomitantly with a kinin B2R antagonist [48,49]. These experiments strongly suggest that kinins may be involved in the multiple beneficial effects of ACE inhibitors in the cardiorenal sphere [50] although this has been called into question by a few researchers [51]. Angiotensin II AT1 receptor antagonists, widely used for the treatment of hypertension, heart failure, and diabetes-related kidney disease, appear to have similar benefits to ACE inhibitors in terms of organ protection. While it was initially hypothesized that ACE inhibitors would demonstrate superior cardiovascular benefits due to their capacity to augment kinin levels, it was subsequently revealed that “sartans” could also increase kinin levels, potentiating the kinin B2R activity. Indeed, the cardiac, renal, and vascular effects of angiotensin AT1 receptor blockade are not observed in animals deficient in kallikrein or the kinin B2R, nor in those with pharmacological B2R blockade [52,53,54,55]. It has been demonstrated that other pharmaceuticals employed in the domain of cardiovascular medicine, which were originally developed for the treatment of heart failure to protect against natriuretic peptide catabolism, such as neprilysin metallopeptidase inhibitors, have been observed to elevate kinin levels; this is due to the fact that neprilysin is also an effective kininase [56]. Furthermore, pharmacological activation of KLK1 kallikrein synthesis was demonstrated for aliskiren, a direct renin inhibitor, in experimental models of heart failure [57].
Renoprotective Potential of the KKS
Observations in mice lacking the kinin B2R (B2-KO) have yielded intriguing findings regarding renal and cardiovascular alterations. A first strain of this type, studied by Madeddu and colleagues, showed slightly higher blood pressure, dilation of the heart chambers, and reparative fibrosis when compared to control animals, under baseline conditions, and marked salt sensitivity [58]. These findings were discussed by other authors who did not find the same results when working with other strains of animals carrying the same defect [59]. The renal and cardiovascular benefits induced by the kinins are mediated by NO, formerly known as endothelium-derived vasorelaxant factor, and it explains its potentialities as a therapeutic option for hypertension and its main consequences, left ventricular hypertrophy and renal disease [122].
A second approach in this regard was used by Uehara et al. [60,61], who, by administering sub-pressor doses of purified rat urinary kallikrein, managed to attenuate renal injury in Dahl salt-sensitive rats, with a reduction in proteinuria and improvement in glomerular filtration. This effect would be mediated by kinin B2R, as the use of Icatibant (HOE140) completely abolished it [62].
A third and very powerful approach was carried out by those who inoculated the kallikrein gene into rats with chronic kidney damage induced by 5/6 subtotal nephrectomy, achieving attenuation of hypertension, reduction of albuminuria, and protection against kidney damage (sclerosis and tubulointerstitial damage) and cardiac remodeling [63]. Urinary kinin levels increased and peripheral vascular resistance decreased, same as in the purified enzyme infusion tests. A similar outcome was observed in Dahl salt-sensitive rats, which was attributed to a reduction in oxidative stress and TGF-b1 expression [64,65,66]. From this same perspective, experiments in transgenic mice that overexpress the human kinin B2R are also relevant because these mice exhibited a propensity for hypotension and enhanced renal function in comparison to the control group. This phenomenon is attributed to the mediation of NO and can be abolished by a B2R antagonist [67].
In light of the available evidence, it is worthwhile investigating the potential of oxidative stress inhibition as a mediator of renal protection. A number of studies [66,68] have examined the role of oxidative stress in the pathophysiology of kidney damage, with some findings indicating a link between salt sensitivity and oxidative stress, as well as intrarenal angiotensin activation [69].
It is imperative to acknowledge that renal fibrosis is an inevitable consequence of excessive extracellular matrix accumulation that occurs in virtually any type of progressive kidney disease [70] and that, from a simplistic point of view, renal fibrosis represents a failed healing process. This process, which includes several pathways such as mesangial and fibroblastic activation and epithelial-mesenchymal transformation EMT), is centrally regulated by TGF-β [71,72]. They may play a significant role in the pathogenesis of acute and chronic nephropathies altering the degree of renal dysfunction, modifying the degree of cell proliferation, and the accumulation of extracellular matrix proteins. As previously documented, the renal protection achieved through tissue kallikrein (KLK1) transfection is accompanied by a reduction in TGF-β expression [66]. At the same time, an anti-inflammatory effect of the KKS in models of acute and chronic renal damage has been demonstrated by reducing inflammatory cells and proinflammatory cytokines [73], although it has not yet been clearly demonstrated that stimulation of kinins reduces TNF-α production [74]. It is tempting to hypothesize that the anti-inflammatory effect seen in several models of renal injury following kallikrein administration or enhancement of kinin activity may result from a primary involvement in reducing the effects of TGF-β in the inflammatory milieu, given the well-known proinflammatory activity of kinins in numerous animal models.
The mechanisms explaining how the KKS may reduce oxidative stress and apoptosis have been well described elsewhere [75]. Kinins stimulate the production of NO and cGMP, both relaxing factors that reduce vascular tone and enhance renal hemodynamics [11]. Increased renal NO levels in association with reduced NADH/NADPH oxidase activity and superoxide anion formation are involved in a reduction of oxidative stress [66], an effect that seems to be mediated via kinin B2R [76]. Kinins, by activating endothelial NO synthase (eNOS/NOS3) lead to low and transient production of NO and activates inducible NOS (iNOS/NOS2), facilitating higher and prolonged release of NO. Oxidative stress is also responsible for the induction of tubular epithelial cell death, which is mediated by caspases and/or endonucleases [77] and involves the activation of p38 MAPK specifically in the case of cisplatin-associated renal damage [78]. A relationship has been established between kinins and hemoxygenase-1 in hearts submitted to ischemia/reperfusion, where bradykinin pretreatment improves post-ischemic performance and infarct size, which is partially abrogated by the previous use of an HO-1 inhibitor [79]. In other cells (brain astrocytes) bradykinin induced HO-1 expression and enzymatic activity via a kinin B2R activated ROS-dependent signaling pathway [80].
In the course of functional renal parenchyma loss and fibrosis establishment, it is required to comprehend the role of cellular apoptosis, given its protagonism in preserving cellular homeostasis under both physiological and pathological conditions [81]. There is evidence linking apoptosis to the phenomenon of renal damage progression [82,83,84,85] and evidence of the pleiotropic effects of the KKS on the central nervous system [68] and myocardium [86] reducing apoptosis in tissue ischemia models. At the same time, it is postulated that oxidative stress may directly promote programmed cell death in experimental models [87]. Evidence of the relationship between apoptosis and oxidative stress in experimental models of hypertension is also available [88] and there are reports showing that strict antihypertensive control can reduce apoptosis during kidney damage [89]. Therefore, we believe it is important to clarify whether stimulation of the KKS is capable of modifying the apoptosis demonstrated in proteinuria models [90], its involvement in the phenomenon of fibrotic transformation and its relationship with oxidative stress, as has been demonstrated in experimental hypertension.
The renoprotective effect of KKS has been also suggested from observations in experimental models of acute renal injury. Rats that were administered gentamicin exhibited a significant decrease in urinary kallikrein levels, indicating that this downregulation may be relevant for the development of acute renal failure [91]. In addition, tissue kallikrein (KLK1) administration prevents and promotes recovery of gentamicin-induced renal injury by inhibiting apoptosis, inflammatory cell recruitment, and fibrotic lesions by suppressing oxidative stress and production of proinflammatory mediators [73]. Suppression of oxidative stress has also been associated with diminished C-jun N-terminal kinase activation, intercellular adhesion molecule-1 and TGF-β, through a kinin B2R-mediated signaling [75].
KKS Intervention and Kidney Protection
The physiological role of endogenous kinins has been thoroughly documented in the cardiovascular system and the kidney in both animal models and humans [92]. In various situations related to ischemia or chronic hypoglycemia, kinins have been shown to have an organ-protective effect, particularly in the heart and kidneys. In a variety of pathological circumstances, a deficiency of kallikrein, kinins, or kinin B2R has been demonstrated to be a contributing factor to tissue damage [50]. Kinins exert their protective effect through the kinin B2R, inducing collateral vasodilation, reducing oxidative stress, and stimulating angiogenesis [93,94,95,96]. Using models of loss of function, it has been possible to demonstrate a reduction in the area of infarction, prevention of ventricular remodeling in the heart, and tissue protection in the kidney under conditions of ischemia-reperfusion [92]. In lupus nephritis, the KKS may play a dual role, protecting tissue from ischemia and fibrosis, and modulating inflammation. In an interesting line of research, Liu et al. [97] showed that certain strains with upregulation of renal and urinary kallikreins exhibited less severe disease; furthermore, antagonizing the KKS increased disease severity, while agonist use attenuated it.
The issue of the use of pharmacological intervention to enhance the activity of the kallikrein-kinin system and its therapeutical value has been studied for a long time [98]. Gene therapy with human KLK1 has demonstrated benefits in cardiac and renal ischemia and diabetes [99,100,101,102,103,104]. Although there is currently insufficient evidence in nephrology, the use of kallikrein as a therapeutic agent is challenging due to pharmacokinetic reasons [105] and the manipulation of kinin B1 and B2 receptors with drugs [106,107] in cases of cardiac or cerebral ischemia appears to have some clinical utility [50].
It is noteworthy that the human phenotype of mutations that induce renal KLK1 dysfunction has not been associated with cardiovascular or renal diseases. This could be explained by the low frequency of these alleles, meaning that only subjects with partial functional deficiency and heterozygosity may have been studied [92].
Studies with experimental models involving kinin B2R-deficient animals or pharmacologically blocked receptors have established that the cardiovascular benefits of kinins are primarily mediated by the kinin B2R, something that has mainly been investigated in models of renal and cardiac ischemia. Studies of diabetic animals and their renal complications indicate that diabetic nephropathy generally worsens in the absence of kinin B2R stimulation because of genetic deletion or deficiency in animals without kallikrein [108]. Similarly, the beneficial effect of ACE inhibitors on diabetic nephropathy can be suppressed in mice and rats with the use of a kinin B2R antagonist such as Icatibant (HOE140) [109,110]. The significance of kinin B2R activation has prompted research and development of new agonists, especially since bradykinin is rapidly catabolized by peptidases [41]. However, these agonists have not yet reached clinical use due to the high rate of adverse effects, including angioedema, pain, and hypotension [44,48,50,111,112], though these adverse effects might be related to dosage or potency. Although it is not yet confirmed, it is a matter of concern that there are some suggestions of a potential carcinogenic effect associated with the activation of the kinin B2R in relation to the use of ACE inhibitors [113].
Experiments in salt-sensitive hypertension have shown that taurine, a conditionally essential amino acid, used pharmacologically, is capable of stimulating kallikrein synthesis, lowering atrial pressure, and inducing a renoprotective effect evidenced by a reduction in proteinuria [114].
Stimulation of the KKS Through Potassium-Rich Diets
The effect of potassium administration in the diet and its stimulating effect on kallikrein synthesis and kinin B2R expression is a known fact (Figure 2). This non-pharmacological maneuver has been shown to be very useful to up-regulate the system under experimental conditions [25,27,115].
Remarkably, potassium is actively secreted via ROMK by the connecting tubule cell, which is the site where renal kallikrein (KLK1) is synthesized and secreted [116]. By releasing kallikrein into the tubule lumen and interstitium, this cell's duality enables it to concurrently contribute to the regulation of potassium and the production of kinins [117]. Similarly, collecting duct cells that also participate in potassium excretion are the source of kininogen production. However, there are so far no studies addressing the levels of renal kininogen under a high-potassium diet.
Administration of potassium stimulates kallikrein secretion [118], which is accompanied by hypertrophy and hyperplasia of the cells that produce it, including hypertrophy of the Golgi apparatus and rough endoplasmic reticulum, and an increased number of kallikrein-containing secretory vesicles, suggesting that the increase in excretion is due to an increase in enzyme synthesis [115]. A diet with a high potassium content has been shown to increase renal kallikrein mRNA expression by 2.7 times, urinary kallikrein excretion by up to 70%, and kinin B2R density in the kidney by 40% [119]. High potassium intake can stimulate renal kallikrein synthesis by two major mechanisms: one that is aldosterone dependent and involves protein synthesis, and another that is fast and aldosterone independent. In the first pathway, potassium stimulates the adrenal cortex to release aldosterone, which then binds to receptors in the connecting tubule cell, activating transcription genes that enhance kallikrein synthesis. In the second pathway, excessive potassium depolarizes the membranes of connecting tubule cells, resulting in a calcium influx that stimulates the secretion of kallikrein-containing vesicles into the tubular lumen and possibly the tubulointerstitium[120]. Human studies show that potassium salts included in the diet can increase kallikrein excretion and simultaneously reduce blood pressure levels [121,122]; other researchers have shown a decrease in renal tissue injury, but this is unrelated to the antihypertensive effect in spontaneously hypertensive rats [123].
Experiments conducted in our laboratory during the induction stage of the proteinuria damage model have reproduced the stimulating effect of potassium chloride on renal kallikrein both in the tissue and in its urinary activity, which was accompanied by a hypotensive effect [13]. Subsequently, we have been able to demonstrate that a potassium-rich diet can significantly reduce the salt sensitivity observed after tubulointerstitial damage [27]. Utilizing this animal model, we were able to induce significant tubulointerstitial damage, which encompasses the components of the KKS located in this area. In a first approach, in the acute phase of overload proteinuria, we observed that potassium induced a significant increase in both urinary activity and renal kallikrein expression, associated with a significant reduction in blood pressure [25]. In a second series of experiments, in the late phase of the same animal model and challenged with a high salt diet, we found that stimulation of the system with a high potassium diet resulted in increased synthesis and excretion of tissue kallikrein (Klk1/rKlK1), accompanied by a significant reduction in blood pressure and attenuation of renal fibrosis. In those experiments, we could find downregulation of renal TGF-β mRNA and protein in comparison with rats that did not receive potassium. Evidence for the participation of the kinin B2R was provided by the fact that all beneficial effects were lost in the presence of a kinin B2R antagonist. Concurrent in vitro experiments utilizing the HK-2 proximal tubule cell line showed that the administration of bradykinin to tubular cells resulted in a reduction in EMT and albumin-induced production of TGF-β; the effects produced by bradykinin were counteracted by pretreatment with a kinin B2R antagonist. These experiments not only provide further evidence to support the hypothesis that the kinin pathway plays a pathogenic role in salt sensitivity but also evidence of its role as a renoprotective, antifibrotic paracrine system that modulates renal levels of TGF-β [27]. A study comparing animals that were pretreated with a potassium-rich diet and then exposed to intraperitoneal albumin overload to induce proteinuria under a normal sodium diet versus controls that did not receive a high potassium diet prior to the protein challenge was carried out in order to support this theory. The high potassium group showed reduction of tubulointerstitial fibrosis, decreased renal expression of alpha-smooth muscle actin and vimentin, reduced Smad3 phosphorylation, and increased Smad7, effects that were reversed by the kinin B2R antagonist HOE140, administered during the overload protein phase (Figure 3). In vitro experiments, conducted on the HK-2 cell line, revealed that elevated concentrations of albumin resulted in the expression of mesenchymal biomarkers, concomitant with augmented levels of TGF-β1 mRNA and its functionally active peptide, TGF-β1. We could also demonstrate that pretreatment of the cells with bradykinin inhibited the albumin-induced changes, thereby reducing alpha-smooth muscle actin and vimentin and recovering cytokeratin, accompanied by an increase in Smad7 levels and a decrease in type II TGF-β1 receptor, TGF-β1 mRNA, and its active fragment; the protective changes produced by bradykinin in vitro were blocked by the HOE140 antagonist (Figure 4) [124].
Of particular interest was the demonstration of the hypotensive effect achieved by administering potassium chloride, which stimulated kallikrein production and reduced blood pressure both during the induction of damage and during the period of salt sensitivity in the animal model of protein overload. It is well established that the effect of potassium is not limited to the increase of kallikrein levels since it also augments the expression of the kinin B2R. The latter is the most effective effector of vasoactive functions [118,119].
The evolution of the human diet can give us some clues as to the importance of adequate potassium intake. Early humans in the Paleolithic era ate fruits and vegetables, which provided low amounts of sodium (690 mg/day) and large amounts of potassium (11 g/day) [125]. With population growth, agricultural development, the need to preserve food, and changes in eating habits, we currently consume no less than 5 grams of sodium per day (8 grams of common salt) and only 2.5 grams of potassium [126]. The association between sodium chloride intake and hypertension, and its consequences, is widely recognized [127], and the clinical feature of blood pressure changes induced by changes in salt intake has been aptly termed as “salt sensitivity” [128]. Based on the above, research has been conducted into the possible beneficial role of potassium intake on salt sensitivity [129], and randomized studies have demonstrated the hypotensive effect of a potassium-rich diet in the general population, with a more pronounced effect in hypertensive individuals [130]. This is achieved by a natriuretic effect, independent of aldosterone (and preceding its secretion), which is mediated by acute dephosphorylation of NCC, the sodium-chloride cotransporter, in the distal tubule [131]. Many authors suggest that the relationship between potassium and sodium in the diet is more important than either of them individually; higher sodium and lower potassium intakes, as measured in multiple 24-hour urine samples, have been associated in a dose-response manner with a higher cardiovascular risk [132]. On the other hand, both higher potassium and a lower sodium-to-potassium ratio are associated with a lower risk of cardiovascular disease [133].
Given that these are observational studies that do not establish causality, it is conceivable that higher potassium intake could be associated with better dietary habits, including more fruits and vegetables, lower sodium intake, and lower incidence of hypertension.
There is reasonable doubt regarding the administration of potassium-rich diets to individuals with chronic kidney disease, considering that potassium is almost exclusively excreted by the kidney (80 to 90% of the daily intake). In this regard, it is noteworthy that the excretory function of potassium persists until advanced stages of renal failure [134]. It is worth noting that studies have indicated a correlation between low potassium intake and an increased risk of developing chronic kidney disease [135] as well as a heightened risk of its progression [136,137]. Other studies show that increased potassium intake could reduce both the incidence and progression of chronic kidney disease [138], and the results of ongoing clinical studies are awaited [139].
Concluding Remarks
The hypothesis that the stimulation and preservation of the renal KKS can act as a strategy for renal protection is a rational approach, given the established mechanisms by which an active and healthy system can mitigate renal damage. Despite the pharmacological potential of drugs that increase the activity of the system, a non-pharmacological approach is a viable prospect. This approach involves stimulating kallikrein synthesis, kinin production, and kinin B2R expression through a potassium-rich diet, which has also been demonstrated to reduce cardiovascular risk. A renal environment rich in kinins, obtained through a potassium-rich diet, could enable people to better cope with the various nephrotoxic challenges we face throughout our lives. Additionally, it is predicted that this could slow the progression to advanced kidney damage once the injury has been established. This straightforward approach, when implemented in conjunction with a reduction in sodium intake, can be accomplished through comprehensive nutritional education and adopted without compromising quality of life. Indeed, it can be incorporated into a patient's diet at an early stage of kidney disease and maintained until renal function and potassium excretion allow it, with a high cost-benefit ratio and therefore scalable to a large scale.
Funding
The authors declare that no financial support was received for the research, authorship, and/or publication of this article.
Acknowledgments
This work is dedicated to the memory of Dr. Kanti Bhoola, in recognition of his invaluable contributions to science and his enduring impact on our field. The present manuscript was produced as part of the activities of the International Society of Nephrology's Renal Training Center at the Universidad Austral de Chile in Valdivia. During the preparation of this manuscript/study, the authors used ChatGPT 5 for the purposes of creating the Graphical Abstract. The authors have reviewed and edited the output and take full responsibility for the content of this publication.
Conflicts of Interest
The authors declare that they have no conflict of interest.
References
- Thurlow, J. S., M. Joshi, G. Yan, K. C. Norris, L. Y. Agodoa, C. M. Yuan and R. Nee. "Global epidemiology of end-stage kidney disease and disparities in kidney replacement therapy." Am J Nephrol 52 (2021): 98-107. https://www.ncbi.nlm.nih.gov/pubmed/33752206. [CrossRef]
- McCullough, K. P., H. Morgenstern, R. Saran, W. H. Herman and B. M. Robinson. "Projecting esrd incidence and prevalence in the united states through 2030." J Am Soc Nephrol 30 (2019): 127-35. [CrossRef]
- Schieppati, A. and G. Remuzzi. "The june 2003 barry m. Brenner comgan lecture. The future of renoprotection: Frustration and promises." Kidney Int 64 (2003): 1947-55. https://www.ncbi.nlm.nih.gov/pubmed/14633117. [CrossRef]
- Eddy, A. A. "Protein restriction reduces transforming growth factor-beta and interstitial fibrosis in nephrotic syndrome." Am J Physiol 266 (1994): F884-93. https://www.ncbi.nlm.nih.gov/pubmed/8023968. [CrossRef]
- Remuzzi, G. "Nephropathic nature of proteinuria." Curr Opin Nephrol Hypertens 8 (1999): 655-63. https://www.ncbi.nlm.nih.gov/pubmed/10630809. [CrossRef]
- Eddy, A. A. "Expression of genes that promote renal interstitial fibrosis in rats with proteinuria." Kidney Int Suppl 54 (1996): S49-54. https://www.ncbi.nlm.nih.gov/pubmed/8731195.
- Eddy, A. A. "Molecular insights into renal interstitial fibrosis." J Am Soc Nephrol 7 (1996): 2495-508. https://www.ncbi.nlm.nih.gov/pubmed/8989727. [CrossRef]
- Bertani, T., F. Cutillo, C. Zoja, M. Broggini and G. Remuzzi. "Tubulo-interstitial lesions mediate renal damage in adriamycin glomerulopathy." Kidney Int 30 (1986): 488-96. https://www.ncbi.nlm.nih.gov/pubmed/3784288. [CrossRef]
- Largo, R., D. Gómez-Garre, K. Soto, B. Marrón, J. Blanco, R. M. Gazapo, J. J. Plaza and J. Egido. "Angiotensin-converting enzyme is upregulated in the proximal tubules of rats with intense proteinuria." Hypertension 33 (1999): 732-9. [CrossRef]
- Gómez-Garre, D., R. Largo, N. Tejera, J. Fortes, F. Manzarbeitia and J. Egido. "Activation of nf-kappab in tubular epithelial cells of rats with intense proteinuria: Role of angiotensin ii and endothelin-1." Hypertension 37 (2001): 1171-8. https://www.ncbi.nlm.nih.gov/pubmed/11304520. [CrossRef]
- Bhoola, K. D., C. D. Figueroa and K. Worthy. "Bioregulation of kinins: Kallikreins, kininogens, and kininases." Pharmacol Rev 44 (1992): 1-80. https://www.ncbi.nlm.nih.gov/pubmed/1313585.
- Vio, C. P., S. Loyola and V. Velarde. "Localization of components of the kallikrein-kinin system in the kidney: Relation to renal function. State of the art lecture." Hypertension 19 (1992): II10-6. https://www.ncbi.nlm.nih.gov/pubmed/1735562. [CrossRef]
- Vío, C. P. and C. D. Figueroa. "Subcellular localization of renal kallikrein by ultrastructural immunocytochemistry." Kidney Int 28 (1985): 36-42. https://www.ncbi.nlm.nih.gov/pubmed/3900530. [CrossRef]
- Figueroa, C. D., A. G. MacIver, J. C. Mackenzie and K. D. Bhoola. "Localisation of immunoreactive kininogen and tissue kallikrein in the human nephron." Histochemistry 89 (1988): 437-42. https://www.ncbi.nlm.nih.gov/pubmed/3170266. [CrossRef]
- Siragy, H. M., M. M. Ibrahim, A. A. Jaffa, R. Mayfield and H. S. Margolius. "Rat renal interstitial bradykinin, prostaglandin e2, and cyclic guanosine 3',5'-monophosphate. Effects of altered sodium intake." Hypertension 23 (1994): 1068-70. https://www.ncbi.nlm.nih.gov/pubmed/8206596. [CrossRef]
- Figueroa, C. D., C. B. Gonzalez, S. Grigoriev, S. A. Abd Alla, M. Haasemann, K. Jarnagin and W. Müller-Esterl. "Probing for the bradykinin b2 receptor in rat kidney by anti-peptide and anti-ligand antibodies." J Histochem Cytochem 43 (1995): 137-48. https://www.ncbi.nlm.nih.gov/pubmed/7822771. [CrossRef]
- Wirth, K., F. J. Hock, U. Albus, W. Linz, H. G. Alpermann, H. Anagnostopoulos, S. Henk, G. Breipohl, W. König and J. Knolle. "Hoe 140 a new potent and long acting bradykinin-antagonist: In vivo studies." Br J Pharmacol 102 (1991): 774-7. https://www.ncbi.nlm.nih.gov/pubmed/1364852. [CrossRef]
- Katori, M. and M. Majima. "The renal kallikrein-kinin system: Its role as a safety valve for excess sodium intake, and its attenuation as a possible etiologic factor in salt-sensitive hypertension." Crit Rev Clin Lab Sci 40 (2003): 43-115. https://www.ncbi.nlm.nih.gov/pubmed/12627748. [CrossRef]
- Glasser, R. J. and A. F. Michael. "Urinary kallikrein in experimental renal disease." Lab Invest 34 (1976): 616-22. https://www.ncbi.nlm.nih.gov/pubmed/933467.
- Ferri, C., C. Bellini, A. Carlomagno, A. Perrone and A. Santucci. "Urinary kallikrein and salt sensitivity in essential hypertensive males." Kidney Int 46 (1994): 780-8. https://www.ncbi.nlm.nih.gov/pubmed/7996800. [CrossRef]
- Sanchez, R., M. I. Gimenez, F. Ramos, H. Baglivo and A. J. Ramirez. "Non-modulating hypertension: Evidence for the involvement of kallikrein/kinin activity associated with overactivity of the renin-angiotensin system. Successful blood pressure control during long-term na+ restriction." J Hypertens 14 (1996): 1287-91. https://www.ncbi.nlm.nih.gov/pubmed/8934356. [CrossRef]
- Margolius, H. S. "Theodore cooper memorial lecture. Kallikreins and kinins. Some unanswered questions about system characteristics and roles in human disease." Hypertension 26 (1995): 221-9. https://www.ncbi.nlm.nih.gov/pubmed/7635529. [CrossRef]
- Chao, J. and L. Chao. "Kallikrein-kinin in stroke, cardiovascular and renal disease." Exp Physiol 90 (2005): 291-8. https://www.ncbi.nlm.nih.gov/pubmed/15653716. [CrossRef]
- Ardiles, L. G., C. D. Figueroa and S. A. Mezzano. "Renal kallikrein-kinin system damage and salt sensitivity: Insights from experimental models." Kidney Int Suppl (2003): S2-8. https://www.ncbi.nlm.nih.gov/pubmed/12969120. [CrossRef]
- Ardiles, L. G., F. Loyola, P. Ehrenfeld, M. E. Burgos, C. A. Flores, G. Valderrama, I. Caorsi, J. Egido, S. A. Mezzano and C. D. Figueroa. "Modulation of renal kallikrein by a high potassium diet in rats with intense proteinuria." Kidney Int 69 (2006): 53-9. https://www.ncbi.nlm.nih.gov/pubmed/16374423. [CrossRef]
- Ardiles, L. G., P. Ehrenfeld, Y. Quiroz, B. Rodriguez-Iturbe, J. Herrera-Acosta, S. Mezzano and C. D. Figueroa. "Effect of mycophenolate mofetil on kallikrein expression in the kidney of 5/6 nephrectomized rats." Kidney Blood Press Res 25 (2002): 289-95. https://www.ncbi.nlm.nih.gov/pubmed/12435874. [CrossRef]
- Ardiles, L., A. Cardenas, M. E. Burgos, A. Droguett, P. Ehrenfeld, D. Carpio, S. Mezzano and C. D. Figueroa. "Antihypertensive and renoprotective effect of the kinin pathway activated by potassium in a model of salt sensitivity following overload proteinuria." Am J Physiol Renal Physiol 304 (2013): F1399-410. https://www.ncbi.nlm.nih.gov/pubmed/23552867. [CrossRef]
- Price, R. G. "Urinary enzymes, nephrotoxicity and renal disease." Toxicology 23 (1982): 99-134. https://www.ncbi.nlm.nih.gov/pubmed/6126019. [CrossRef]
- Naicker, S., S. Naidoo, R. Ramsaroop, D. Moodley and K. Bhoola. "Tissue kallikrein and kinins in renal disease." Immunopharmacology 44 (1999): 183-92. https://www.ncbi.nlm.nih.gov/pubmed/10604543. [CrossRef]
- Yu, H., D. W. Bowden, B. J. Spray, S. S. Rich and B. I. Freedman. "Identification of human plasma kallikrein gene polymorphisms and evaluation of their role in end-stage renal disease." Hypertension 31 (1998): 906-11. https://www.ncbi.nlm.nih.gov/pubmed/9535413. [CrossRef]
- Jozwiak, L., A. Drop, K. Buraczynska, P. Ksiazek, P. Mierzicki and M. Buraczynska. "Association of the human bradykinin b2 receptor gene with chronic renal failure." Mol Diagn 8 (2004): 157-61. https://www.ncbi.nlm.nih.gov/pubmed/15771553. [CrossRef]
- Rodríguez-Iturbe, B., H. Pons, Y. Quiroz, K. Gordon, J. Rincón, M. Chávez, G. Parra, J. Herrera-Acosta, D. Gómez-Garre, R. Largo, et al. "Mycophenolate mofetil prevents salt-sensitive hypertension resulting from angiotensin ii exposure." Kidney Int 59 (2001): 2222-32. https://www.ncbi.nlm.nih.gov/pubmed/11380825. [CrossRef]
- Shen, B. and S. S. El-Dahr. "Cross-talk of the renin-angiotensin and kallikrein-kinin systems." Biol Chem 387 (2006): 145-50. https://www.ncbi.nlm.nih.gov/pubmed/16497145. [CrossRef]
- Imamura, A., H. S. Mackenzie, E. R. Lacy, F. N. Hutchison, W. R. Fitzgibbon and D. W. Ploth. "Effects of chronic treatment with angiotensin converting enzyme inhibitor or an angiotensin receptor antagonist in two-kidney, one-clip hypertensive rats." Kidney Int 47 (1995): 1394-402. https://www.ncbi.nlm.nih.gov/pubmed/7637269. [CrossRef]
- Nishiyama, K., T. Igari, S. Nanba and M. Ishii. "Long-term effects of delapril on renal function and urinary excretion of kallikrein, prostaglandin e2, and thromboxane b2 in hypertensive patients." Am J Hypertens 4 (1991): 52S-53S. https://www.ncbi.nlm.nih.gov/pubmed/2009149. [CrossRef]
- Kramer, H. J., K. Glänzer, H. Meyer-Lehnert, M. Mohaupt and H. G. Predel. "Kinin- and non-kinin-mediated interactions of converting enzyme inhibitors with vasoactive hormones." J Cardiovasc Pharmacol 15 Suppl 6 (1990): S91-8. https://www.ncbi.nlm.nih.gov/pubmed/1697369.
- Hutchison, F. N., X. Cui and S. K. Webster. "The antiproteinuric action of angiotensin-converting enzyme is dependent on kinin." J Am Soc Nephrol 6 (1995): 1216-22. https://www.ncbi.nlm.nih.gov/pubmed/8589289. [CrossRef]
- Ruggenenti, P., A. Perna, G. Gherardi, F. Gaspari, R. Benini and G. Remuzzi. "Renal function and requirement for dialysis in chronic nephropathy patients on long-term ramipril: Rein follow-up trial. Gruppo italiano di studi epidemiologici in nefrologia (gisen). Ramipril efficacy in nephropathy." Lancet 352 (1998): 1252-6. https://www.ncbi.nlm.nih.gov/pubmed/9788454. [CrossRef]
- Pawluczyk, I. Z., S. R. Patel and K. P. Harris. "The role of bradykinin in the antifibrotic actions of perindoprilat on human mesangial cells." Kidney Int 65 (2004): 1240-51. https://www.ncbi.nlm.nih.gov/pubmed/15086463. [CrossRef]
- Pawluczyk, I. Z., E. K. Tan, D. Lodwick and K. Harris. "Kallikrein gene 'knock-down' by small interfering rna transfection induces a profibrotic phenotype in rat mesangial cells." J Hypertens 26 (2008): 93-101. https://www.ncbi.nlm.nih.gov/pubmed/18090545. [CrossRef]
- Erdös, E. G. "Angiotensin i converting enzyme and the changes in our concepts through the years. Lewis k. Dahl memorial lecture." Hypertension 16 (1990): 363-70. https://www.ncbi.nlm.nih.gov/pubmed/2170273. [CrossRef]
- Murphey, L. J., J. V. Gainer, D. E. Vaughan and N. J. Brown. "Angiotensin-converting enzyme insertion/deletion polymorphism modulates the human in vivo metabolism of bradykinin." Circulation 102 (2000): 829-32. [CrossRef]
- Marre, M., B. Bouhanick, G. Berrut, Y. Gallois, J. J. Le Jeune, G. Chatellier, J. Menard and F. Alhenc-Gelas. "Renal changes on hyperglycemia and angiotensin-converting enzyme in type 1 diabetes." Hypertension 33 (1999): 775-80. [CrossRef]
- Desposito, D., L. Waeckel, L. Potier, C. Richer, R. Roussel, N. Bouby and F. Alhenc-Gelas. "Kallikrein(k1)-kinin-kininase (ace) and end-organ damage in ischemia and diabetes: Therapeutic implications." Biol Chem 397 (2016): 1217-22. [CrossRef]
- Waeckel, L., L. Potier, C. Richer, R. Roussel, N. Bouby and F. Alhenc-Gelas. "Pathophysiology of genetic deficiency in tissue kallikrein activity in mouse and man." Thromb Haemost 110 (2013): 476-83. [CrossRef]
- Kakoki, M. and O. Smithies. "The kallikrein-kinin system in health and in diseases of the kidney." Kidney Int 75 (2009): 1019-30. [CrossRef]
- Yusuf, S., P. Sleight, J. Pogue, J. Bosch, R. Davies and G. Dagenais. "Effects of an angiotensin-converting-enzyme inhibitor, ramipril, on cardiovascular events in high-risk patients." N Engl J Med 342 (2000): 145-53. [CrossRef]
- Alhenc-Gelas, F., N. Bouby, C. Richer, L. Potier, R. Roussel and M. Marre. "Kinins as therapeutic agents in cardiovascular and renal diseases." Curr Pharm Des 17 (2011): 2654-62. https://www.ncbi.nlm.nih.gov/pubmed/21728987. [CrossRef]
- Rhaleb, N. E., X. P. Yang and O. A. Carretero. "The kallikrein-kinin system as a regulator of cardiovascular and renal function." Compr Physiol 1 (2011): 971-93. https://www.ncbi.nlm.nih.gov/pubmed/23737209. [CrossRef]
- Girolami, J.-P., N. Bouby, C. Richer-Giudicelli and F. Alhenc-Gelas. "Kinins and kinin receptors in cardiovascular and renal diseases." Pharmaceuticals 14 (2021): 240. [CrossRef]
- Kohzuki, M., M. Yasujima, M. Kanazawa, K. Yoshida, T. Sato and K. Abe. "Do kinins mediate cardioprotective and renoprotective effects of cilazapril in spontaneously hypertensive rats with renal ablation?" Clin Exp Pharmacol Physiol Suppl 22 (1995): S357-9. https://www.ncbi.nlm.nih.gov/pubmed/9072427. [CrossRef]
- Bergaya, S., R. H. Hilgers, P. Meneton, Y. Dong, M. Bloch-Faure, T. Inagami, F. Alhenc-Gelas, B. I. Lévy and C. M. Boulanger. "Flow-dependent dilation mediated by endogenous kinins requires angiotensin at2 receptors." Circ Res 94 (2004): 1623-9. https://www.ncbi.nlm.nih.gov/pubmed/15131008. [CrossRef]
- Messadi-Laribi, E., V. Griol-Charhbili, A. Pizard, M. P. Vincent, D. Heudes, P. Meneton, F. Alhenc-Gelas and C. Richer. "Tissue kallikrein is involved in the cardioprotective effect of at1-receptor blockade in acute myocardial ischemia." J Pharmacol Exp Ther 323 (2007): 210-6. [CrossRef]
- Liu, Y. H., X. P. Yang, V. G. Sharov, O. Nass, H. N. Sabbah, E. Peterson and O. A. Carretero. "Effects of angiotensin-converting enzyme inhibitors and angiotensin ii type 1 receptor antagonists in rats with heart failure. Role of kinins and angiotensin ii type 2 receptors." J Clin Invest 99 (1997): 1926-35. [CrossRef]
- Abadir, P. M., A. Periasamy, R. M. Carey and H. M. Siragy. "Angiotensin ii type 2 receptor-bradykinin b2 receptor functional heterodimerization." Hypertension 48 (2006): 316-22. [CrossRef]
- Bozkurt, B., A. P. Nair, A. Misra, C. Z. Scott, J. H. Mahar and S. Fedson. "Neprilysin inhibitors in heart failure: The science, mechanism of action, clinical studies, and unanswered questions." JACC: Basic to Translational Science 8 (2023): 88-105. https://www.sciencedirect.com/science/article/pii/S2452302X22002212. [CrossRef]
- Koid, S. S., J. Ziogas and D. J. Campbell. "Aliskiren reduces myocardial ischemia-reperfusion injury by a bradykinin b2 receptor- and angiotensin at2 receptor-mediated mechanism." Hypertension 63 (2014): 768-73. [CrossRef]
- Madeddu, P., M. V. Varoni, D. Palomba, C. Emanueli, M. P. Demontis, N. Glorioso, P. Dessì-Fulgheri, R. Sarzani and V. Anania. "Cardiovascular phenotype of a mouse strain with disruption of bradykinin b2-receptor gene." Circulation 96 (1997): 3570-8. https://www.ncbi.nlm.nih.gov/pubmed/9396457. [CrossRef]
- Milia, A. F., V. Gross, R. Plehm, J. A. De Silva, M. Bader and F. C. Luft. "Normal blood pressure and renal function in mice lacking the bradykinin b(2) receptor." Hypertension 37 (2001): 1473-9. https://www.ncbi.nlm.nih.gov/pubmed/11408397. [CrossRef]
- Uehara, Y., N. Hirawa, A. Numabe, Y. Kawabata, T. Ikeda, T. Gomi, A. Gotoh and M. Omata. "Long-term infusion of kallikrein attenuates renal injury in dahl salt-sensitive rats." Am J Hypertens 10 (1997): 83S-88S. https://www.ncbi.nlm.nih.gov/pubmed/9160787.
- Hirawa, N., Y. Uehara, Y. Kawabata, A. Numabe, T. Gomi, T. Ikeda, T. Suzuki, A. Goto, T. Toyo-oka and M. Omata. "Long-term inhibition of renin-angiotensin system sustains memory function in aged dahl rats." Hypertension 34 (1999): 496-502. https://www.ncbi.nlm.nih.gov/pubmed/10489400. [CrossRef]
- Hirawa, N., Y. Uehara, T. Suzuki, Y. Kawabata, A. Numabe, T. Gomi, T. lkeda, K. Kizuki and M. Omata. "Regression of glomerular injury by kallikrein infusion in dahl salt-sensitive rats is a bradykinin b2-receptor-mediated event." Nephron 81 (1999): 183-93. https://www.ncbi.nlm.nih.gov/pubmed/9933754. [CrossRef]
- Wolf, W. C., H. Yoshida, J. Agata, L. Chao and J. Chao. "Human tissue kallikrein gene delivery attenuates hypertension, renal injury, and cardiac remodeling in chronic renal failure." Kidney Int 58 (2000): 730-9. https://www.ncbi.nlm.nih.gov/pubmed/10916096. [CrossRef]
- Chao, J., J. J. Zhang, K. F. Lin and L. Chao. "Adenovirus-mediated kallikrein gene delivery reverses salt-induced renal injury in dahl salt-sensitive rats." Kidney Int 54 (1998): 1250-60. https://www.ncbi.nlm.nih.gov/pubmed/9767541. [CrossRef]
- Chao, J., J. J. Zhang, K. F. Lin and L. Chao. "Human kallikrein gene delivery attenuates hypertension, cardiac hypertrophy, and renal injury in dahl salt-sensitive rats." Hum Gene Ther 9 (1998): 21-31. https://www.ncbi.nlm.nih.gov/pubmed/9458239. [CrossRef]
- Zhang, J. J., G. Bledsoe, K. Kato, L. Chao and J. Chao. "Tissue kallikrein attenuates salt-induced renal fibrosis by inhibition of oxidative stress." Kidney Int 66 (2004): 722-32. https://www.ncbi.nlm.nih.gov/pubmed/15253727. [CrossRef]
- Wang, D., H. Yoshida, Q. Song, L. Chao and J. Chao. "Enhanced renal function in bradykinin b(2) receptor transgenic mice." Am J Physiol Renal Physiol 278 (2000): F484-91. https://www.ncbi.nlm.nih.gov/pubmed/10710553. [CrossRef]
- Xia, C. F., G. Bledsoe, L. Chao and J. Chao. "Kallikrein gene transfer reduces renal fibrosis, hypertrophy, and proliferation in doca-salt hypertensive rats." Am J Physiol Renal Physiol 289 (2005): F622-31. https://www.ncbi.nlm.nih.gov/pubmed/15886273. [CrossRef]
- Alvarez, V., Y. Quiroz, M. Nava, H. Pons and B. Rodríguez-Iturbe. "Overload proteinuria is followed by salt-sensitive hypertension caused by renal infiltration of immune cells." Am J Physiol Renal Physiol 283 (2002): F1132-41. https://www.ncbi.nlm.nih.gov/pubmed/12372790. [CrossRef]
- Razzaque, M. S., N. Ahsan and T. Taguchi. "Role of apoptosis in fibrogenesis." Nephron 90 (2002): 365-72. https://www.ncbi.nlm.nih.gov/pubmed/11961393. [CrossRef]
- Liu, Y. "Renal fibrosis: New insights into the pathogenesis and therapeutics." Kidney Int 69 (2006): 213-7. https://www.ncbi.nlm.nih.gov/pubmed/16408108. [CrossRef]
- Iglesias-De La Cruz, M. C., P. Ruiz-Torres, J. Alcamí, L. Díez-Marqués, R. Ortega-Velázquez, S. Chen, M. Rodríguez-Puyol, F. N. Ziyadeh and D. Rodríguez-Puyol. "Hydrogen peroxide increases extracellular matrix mrna through tgf-beta in human mesangial cells." Kidney Int 59 (2001): 87-95. https://www.ncbi.nlm.nih.gov/pubmed/11135061. [CrossRef]
- Bledsoe, G., B. Shen, Y. Y. Yao, M. Hagiwara, B. Mizell, M. Teuton, D. Grass, L. Chao and J. Chao. "Role of tissue kallikrein in prevention and recovery of gentamicin-induced renal injury." Toxicol Sci 102 (2008): 433-43. https://www.ncbi.nlm.nih.gov/pubmed/18227104. [CrossRef]
- Oda, Y., H. Nishi and M. Nangaku. "Role of inflammation in progression of chronic kidney disease in type 2 diabetes mellitus: Clinical implications." Seminars in Nephrology 43 (2023): 151431. https://www.sciencedirect.com/science/article/pii/S0270929523001419. [CrossRef]
- Bledsoe, G., S. Crickman, J. Mao, C. F. Xia, H. Murakami, L. Chao and J. Chao. "Kallikrein/kinin protects against gentamicin-induced nephrotoxicity by inhibition of inflammation and apoptosis." Nephrol Dial Transplant 21 (2006): 624-33. https://www.ncbi.nlm.nih.gov/pubmed/16401625. [CrossRef]
- Kakoki, M., C. M. Kizer, X. Yi, N. Takahashi, H. S. Kim, C. R. Bagnell, C. J. Edgell, N. Maeda, J. C. Jennette and O. Smithies. "Senescence-associated phenotypes in akita diabetic mice are enhanced by absence of bradykinin b2 receptors." J Clin Invest 116 (2006): 1302-9. https://www.ncbi.nlm.nih.gov/pubmed/16604193. [CrossRef]
- Basnakian, A. G., G. P. Kaushal and S. V. Shah. "Apoptotic pathways of oxidative damage to renal tubular epithelial cells." Antioxid Redox Signal 4 (2002): 915-24. https://www.ncbi.nlm.nih.gov/pubmed/12573140. [CrossRef]
- Luo, J., T. Tsuji, H. Yasuda, Y. Sun, Y. Fujigaki and A. Hishida. "The molecular mechanisms of the attenuation of cisplatin-induced acute renal failure by n-acetylcysteine in rats." Nephrol Dial Transplant 23 (2008): 2198-205. https://www.ncbi.nlm.nih.gov/pubmed/18385389. [CrossRef]
- Dong, H. Z., Y. Y. Chen, L. Zhu, H. J. Xu, Y. Wang, F. R. Shen, Z. N. Cai and Y. L. Shen. "[cox-2 and ho-1 are involved in the delayed preconditioning elicited by bradykinin in rat hearts]." Zhejiang Da Xue Xue Bao Yi Xue Ban 36 (2007): 13-20. https://www.ncbi.nlm.nih.gov/pubmed/17290486. [CrossRef]
- Hsieh, H. L., H. H. Wang, C. Y. Wu and C. M. Yang. "Reactive oxygen species-dependent c-fos/activator protein 1 induction upregulates heme oxygenase-1 expression by bradykinin in brain astrocytes." Antioxid Redox Signal 13 (2010): 1829-44. https://www.ncbi.nlm.nih.gov/pubmed/20486760. [CrossRef]
- Ortiz, A. "Nephrology forum: Apoptotic regulatory proteins in renal injury." Kidney Int 58 (2000): 467-85. https://www.ncbi.nlm.nih.gov/pubmed/10886604. [CrossRef]
- Ortiz, A., S. González Cuadrado, C. Lorz and J. Egido. "Apoptosis in renal diseases." Front Biosci 1 (1996): d30-47. https://www.ncbi.nlm.nih.gov/pubmed/9159208. [CrossRef]
- Thomas, G. L., B. Yang, B. E. Wagner, J. Savill and A. M. El Nahas. "Cellular apoptosis and proliferation in experimental renal fibrosis." Nephrol Dial Transplant 13 (1998): 2216-26. https://www.ncbi.nlm.nih.gov/pubmed/9761500. [CrossRef]
- Yukawa, K., M. Kishino, M. Goda, X. M. Liang, A. Kimura, T. Tanaka, T. Bai, K. Owada-Makabe, Y. Tsubota, T. Ueyama, et al. "Stat6 deficiency inhibits tubulointerstitial fibrosis in obstructive nephropathy." Int J Mol Med 15 (2005): 225-30. https://www.ncbi.nlm.nih.gov/pubmed/15647835.
- Vaziri, N. D. "Roles of oxidative stress and antioxidant therapy in chronic kidney disease and hypertension." Curr Opin Nephrol Hypertens 13 (2004): 93-9. https://www.ncbi.nlm.nih.gov/pubmed/15090865. [CrossRef]
- Montanari, D., H. Yin, E. Dobrzynski, J. Agata, H. Yoshida, J. Chao and L. Chao. "Kallikrein gene delivery improves serum glucose and lipid profiles and cardiac function in streptozotocin-induced diabetic rats." Diabetes 54 (2005): 1573-80. https://www.ncbi.nlm.nih.gov/pubmed/15855348. [CrossRef]
- Allen, D. A., S. Harwood, M. Varagunam, M. J. Raftery and M. M. Yaqoob. "High glucose-induced oxidative stress causes apoptosis in proximal tubular epithelial cells and is mediated by multiple caspases." FASEB J 17 (2003): 908-10. https://www.ncbi.nlm.nih.gov/pubmed/12670885. [CrossRef]
- Quiroz, Y., J. Bravo, J. Herrera-Acosta, R. J. Johnson and B. Rodríguez-Iturbe. "Apoptosis and nfkappab activation are simultaneously induced in renal tubulointerstitium in experimental hypertension." Kidney Int Suppl (2003): S27-32. https://www.ncbi.nlm.nih.gov/pubmed/12969124. [CrossRef]
- Soto, K., D. Gómez-Garre, R. Largo, J. Gallego-Delgado, N. Tejera, M. P. Catalán, A. Ortiz, J. J. Plaza, C. Alonso and J. Egido. "Tight blood pressure control decreases apoptosis during renal damage." Kidney Int 65 (2004): 811-22. https://www.ncbi.nlm.nih.gov/pubmed/14871401. [CrossRef]
- Thomas, M. E., N. J. Brunskill, K. P. Harris, E. Bailey, J. H. Pringle, P. N. Furness and J. Walls. "Proteinuria induces tubular cell turnover: A potential mechanism for tubular atrophy." Kidney Int 55 (1999): 890-8. https://www.ncbi.nlm.nih.gov/pubmed/10027925. [CrossRef]
- Higa, E. M., N. Schor, M. A. Boim, H. Ajzen and O. L. Ramos. "Role of the prostaglandin and kallikrein-kinin systems in aminoglycoside-induced acute renal failure." Braz J Med Biol Res 18 (1985): 355-65. https://www.ncbi.nlm.nih.gov/pubmed/2424533.
- Alhenc-Gelas, F., N. Bouby and J. P. Girolami. "Kallikrein/k1, kinins, and ace/kininase ii in homeostasis and in disease insight from human and experimental genetic studies, therapeutic implication." Front Med (Lausanne) 6 (2019): 136. https://www.ncbi.nlm.nih.gov/pubmed/31316987. [CrossRef]
- Kränkel, N., R. G. Katare, M. Siragusa, L. S. Barcelos, P. Campagnolo, G. Mangialardi, O. Fortunato, G. Spinetti, N. Tran, K. Zacharowski, et al. "Role of kinin b2 receptor signaling in the recruitment of circulating progenitor cells with neovascularization potential." Circ Res 103 (2008): 1335-43. https://www.ncbi.nlm.nih.gov/pubmed/18927465. [CrossRef]
- Kayashima, Y., O. Smithies and M. Kakoki. "The kallikrein-kinin system and oxidative stress." Curr Opin Nephrol Hypertens 21 (2012): 92-6. https://www.ncbi.nlm.nih.gov/pubmed/22048723. [CrossRef]
- Silvestre, J. S., S. Bergaya, R. Tamarat, M. Duriez, C. M. Boulanger and B. I. Levy. "Proangiogenic effect of angiotensin-converting enzyme inhibition is mediated by the bradykinin b(2) receptor pathway." Circ Res 89 (2001): 678-83. https://www.ncbi.nlm.nih.gov/pubmed/11597990. [CrossRef]
- Spinetti, G., O. Fortunato, D. Cordella, P. Portararo, N. Kränkel, R. Katare, G. B. Sala-Newby, C. Richer, M. P. Vincent, F. Alhenc-Gelas, et al. "Tissue kallikrein is essential for invasive capacity of circulating proangiogenic cells." Circ Res 108 (2011): 284-93. https://www.ncbi.nlm.nih.gov/pubmed/21164105. [CrossRef]
- Liu, K., Q. Z. Li, A. M. Delgado-Vega, A. K. Abelson, E. Sánchez, J. A. Kelly, L. Li, Y. Liu, J. Zhou, M. Yan, et al. "Kallikrein genes are associated with lupus and glomerular basement membrane-specific antibody-induced nephritis in mice and humans." J Clin Invest 119 (2009): 911-23. [CrossRef]
- Marceau, F. "Drugs of the kallikrein–kinin system: An overview." Drugs and Drug Candidates 2 (2023): 538-53. [CrossRef]
- Stone, O. A., C. Richer, C. Emanueli, V. van Weel, P. H. Quax, R. Katare, N. Kraenkel, P. Campagnolo, L. S. Barcelos, M. Siragusa, et al. "Critical role of tissue kallikrein in vessel formation and maturation: Implications for therapeutic revascularization." Arterioscler Thromb Vasc Biol 29 (2009): 657-64. [CrossRef]
- Emanueli, C., A. Minasi, A. Zacheo, J. Chao, L. Chao, M. B. Salis, S. Straino, M. G. Tozzi, R. Smith, L. Gaspa, et al. "Local delivery of human tissue kallikrein gene accelerates spontaneous angiogenesis in mouse model of hindlimb ischemia." Circulation 103 (2001): 125-32. [CrossRef]
- Pinto, Y. M., M. Bader, J. B. Pesquero, C. Tschöpe, E. Scholtens, W. H. van Gilst and H. Buikema. "Increased kallikrein expression protects against cardiac ischemia." Faseb j 14 (2000): 1861-3. [CrossRef]
- Silva, J. A., Jr., R. C. Araujo, O. Baltatu, S. M. Oliveira, C. Tschöpe, E. Fink, S. Hoffmann, R. Plehm, K. X. Chai, L. Chao, et al. "Reduced cardiac hypertrophy and altered blood pressure control in transgenic rats with the human tissue kallikrein gene." Faseb j 14 (2000): 1858-60. [CrossRef]
- Tschöpe, C., T. Walther, J. Königer, F. Spillmann, D. Westermann, F. Escher, M. Pauschinger, J. B. Pesquero, M. Bader, H. P. Schultheiss, et al. "Prevention of cardiac fibrosis and left ventricular dysfunction in diabetic cardiomyopathy in rats by transgenic expression of the human tissue kallikrein gene." Faseb j 18 (2004): 828-35. [CrossRef]
- Koch, M., F. Spillmann, A. Dendorfer, D. Westermann, C. Altmann, M. Sahabi, S. V. Linthout, M. Bader, T. Walther, H. P. Schultheiss, et al. "Cardiac function and remodeling is attenuated in transgenic rats expressing the human kallikrein-1 gene after myocardial infarction." Eur J Pharmacol 550 (2006): 143-8. [CrossRef]
- Kolodka, T., M. L. Charles, A. Raghavan, I. A. Radichev, C. Amatya, J. Ellefson, A. Y. Savinov, A. Nag, M. S. Williams and M. S. Robbins. "Preclinical characterization of recombinant human tissue kallikrein-1 as a novel treatment for type 2 diabetes mellitus." PLoS One 9 (2014): e103981. https://www.ncbi.nlm.nih.gov/pubmed/25100328. [CrossRef]
- Bélanger, S., V. Bovenzi, J. Côté, W. Neugebauer, M. Amblard, J. Martinez, B. Lammek, M. Savard and F. Gobeil. "Structure-activity relationships of novel peptide agonists of the human bradykinin b2 receptor." Peptides 30 (2009): 777-87. https://www.ncbi.nlm.nih.gov/pubmed/19111586. [CrossRef]
- Côté, J., M. Savard, V. Bovenzi, S. Bélanger, J. Morin, W. Neugebauer, A. Larouche, C. Dubuc and F. Gobeil. "Novel kinin b1 receptor agonists with improved pharmacological profiles." Peptides 30 (2009): 788-95. https://www.ncbi.nlm.nih.gov/pubmed/19150636. [CrossRef]
- Bodin, S., C. Chollet, N. Goncalves-Mendes, J. Gardes, F. Pean, D. Heudes, P. Bruneval, M. Marre, F. Alhenc-Gelas and N. Bouby. "Kallikrein protects against microalbuminuria in experimental type i diabetes." Kidney Int 76 (2009): 395-403. [CrossRef]
- Allard, J., M. Buléon, E. Cellier, I. Renaud, C. Pecher, F. Praddaude, M. Conti, I. Tack and J. P. Girolami. "Ace inhibitor reduces growth factor receptor expression and signaling but also albuminuria through b2-kinin glomerular receptor activation in diabetic rats." Am J Physiol Renal Physiol 293 (2007): F1083-92. [CrossRef]
- Buléon, M., J. Allard, A. Jaafar, F. Praddaude, Z. Dickson, M. T. Ranera, C. Pecher, J. P. Girolami and I. Tack. "Pharmacological blockade of b2-kinin receptor reduces renal protective effect of angiotensin-converting enzyme inhibition in db/db mice model." Am J Physiol Renal Physiol 294 (2008): F1249-56. https://www.ncbi.nlm.nih.gov/pubmed/18367657. [CrossRef]
- Cicardi, M., A. Banerji, F. Bracho, A. Malbrán, B. Rosenkranz, M. Riedl, K. Bork, W. Lumry, W. Aberer, H. Bier, et al. "Icatibant, a new bradykinin-receptor antagonist, in hereditary angioedema." N Engl J Med 363 (2010): 532-41. [CrossRef]
- Whalley, E. T., S. Clegg, J. M. Stewart and R. J. Vavrek. "The effect of kinin agonists and antagonists on the pain response of the human blister base." Naunyn Schmiedebergs Arch Pharmacol 336 (1987): 652-5. [CrossRef]
- Hicks, B. M., K. B. Filion, H. Yin, L. Sakr, J. A. Udell and L. Azoulay. "Angiotensin converting enzyme inhibitors and risk of lung cancer: Population based cohort study." Bmj 363 (2018): k4209. [CrossRef]
- Ideishi, M., S. Miura, T. Sakai, M. Sasaguri, Y. Misumi and K. Arakawa. "Taurine amplifies renal kallikrein and prevents salt-induced hypertension in dahl rats." J Hypertens 12 (1994): 653-61. https://www.ncbi.nlm.nih.gov/pubmed/7963490.
- Vío, C. P. and C. D. Figueroa. "Evidence for a stimulatory effect of high potassium diet on renal kallikrein." Kidney Int 31 (1987): 1327-34. https://www.ncbi.nlm.nih.gov/pubmed/3302506. [CrossRef]
- Welling, P. A. and K. Ho. "A comprehensive guide to the romk potassium channel: Form and function in health and disease." Am J Physiol Renal Physiol 297 (2009): F849-63. [CrossRef]
- El Moghrabi, S., P. Houillier, N. Picard, F. Sohet, B. Wootla, M. Bloch-Faure, F. Leviel, L. Cheval, S. Frische, P. Meneton, et al. "Tissue kallikrein permits early renal adaptation to potassium load." Proc Natl Acad Sci U S A 107 (2010): 13526-31. https://www.ncbi.nlm.nih.gov/pubmed/20624970. [CrossRef]
- Obika, L. F. "Urinary kallikrein excretion after potassium adaptation in the rat." Arch Int Physiol Biochim 95 (1987): 189-93. https://www.ncbi.nlm.nih.gov/pubmed/2446581.
- Jin, L., L. Chao and J. Chao. "Potassium supplement upregulates the expression of renal kallikrein and bradykinin b2 receptor in shr." Am J Physiol 276 (1999): F476-84. https://www.ncbi.nlm.nih.gov/pubmed/10070172. [CrossRef]
- Hayashi, I., T. Fujita, M. Majima and M. Katori. "A secretory mechanism of renal kallikrein by a high potassium ion; a possible involvement of atp-sensitive potassium channel." Immunopharmacology 44 (1999): 49-55. https://www.ncbi.nlm.nih.gov/pubmed/10604524. [CrossRef]
- Valdés, G., C. P. Vio, J. Montero and R. Avendaño. "Potassium supplementation lowers blood pressure and increases urinary kallikrein in essential hypertensives." J Hum Hypertens 5 (1991): 91-6. https://www.ncbi.nlm.nih.gov/pubmed/2072372.
- Overlack, A., K. O. Stumpe, B. Moch, A. Ollig, R. Kleinmann, H. M. Müller, R. Kolloch and F. Krück. "Hemodynamic, renal, and hormonal responses to changes in dietary potassium in normotensive and hypertensive man: Long-term antihypertensive effect of potassium supplementation in essential hypertension." Klin Wochenschr 63 (1985): 352-60. https://www.ncbi.nlm.nih.gov/pubmed/3923252. [CrossRef]
- Ellis, D., B. Banner, J. E. Janosky and P. U. Feig. "Potassium supplementation attenuates experimental hypertensive renal injury." J Am Soc Nephrol 2 (1992): 1529-37. https://www.ncbi.nlm.nih.gov/pubmed/1600125. [CrossRef]
- Cárdenas, A., J. Campos, P. Ehrenfeld, S. Mezzano, M. Ruiz-Ortega, C. D. Figueroa and L. Ardiles. "Up-regulation of the kinin b2 receptor pathway modulates the tgf-β/smad signaling cascade to reduce renal fibrosis induced by albumin." Peptides 73 (2015): 7-19. https://www.ncbi.nlm.nih.gov/pubmed/26256678. [CrossRef]
- Eaton, S. B. and M. Konner. "Paleolithic nutrition. A consideration of its nature and current implications." N Engl J Med 312 (1985): 283-9. https://www.ncbi.nlm.nih.gov/pubmed/2981409. [CrossRef]
- Agriculture, U. S. D. o. U.S. Department of agriculture; u.S. Department of health and human services. Dietary guidelines for americans, 2020–2025 . 9th ed. December 2020. Available from: Https://www.Dietaryguidelines.Gov. U.S.: 2020,.
- Murray, C. J. and A. D. Lopez. "Measuring the global burden of disease." N Engl J Med 369 (2013): 448-57. https://www.ncbi.nlm.nih.gov/pubmed/23902484. [CrossRef]
- Dahl, L. K. "Possible role of chronic excess salt consumption in the pathogenesis of essential hypertension." The American Journal of Cardiology 8 (1961): 571-75. https://www.sciencedirect.com/science/article/pii/0002914961901370. [CrossRef]
- Dahl, L. K., G. Leitl and M. Heine. "Influence of dietary potassium and sodium/potassium molar ratios on the development of salt hypertension." J Exp Med 136 (1972): 318-30. https://www.ncbi.nlm.nih.gov/pubmed/5043414. [CrossRef]
- Aburto, N. J., S. Hanson, H. Gutierrez, L. Hooper, P. Elliott and F. P. Cappuccio. "Effect of increased potassium intake on cardiovascular risk factors and disease: Systematic review and meta-analyses." BMJ 346 (2013): f1378. https://www.ncbi.nlm.nih.gov/pubmed/23558164. [CrossRef]
- Sorensen, M. V., S. Grossmann, M. Roesinger, N. Gresko, A. P. Todkar, G. Barmettler, U. Ziegler, A. Odermatt, D. Loffing-Cueni and J. Loffing. "Rapid dephosphorylation of the renal sodium chloride cotransporter in response to oral potassium intake in mice." Kidney International 83 (2013): 811-24. [CrossRef]
- Ma, Y., F. J. He, Q. Sun, C. Yuan, L. M. Kieneker, G. C. Curhan, G. A. MacGregor, S. J. L. Bakker, N. R. C. Campbell, M. Wang, et al. "24-hour urinary sodium and potassium excretion and cardiovascular risk." N Engl J Med 386 (2022): 252-63. [CrossRef]
- Gonçalves, C. and S. Abreu. "Sodium and potassium intake and cardiovascular disease in older people: A systematic review." Nutrients 12 (2020): 10.3390/nu12113447.
- Caravaca-Fontán, F., J. Valladares, R. Díaz-Campillejo, S. Barroso, E. Luna and F. Caravaca. "Renal potassium handling in chronic kidney disease: Differences between patients with or wihtout hyperkalemia." Nefrologia (Engl Ed) 40 (2020): 152-59. https://www.ncbi.nlm.nih.gov/pubmed/31353054. [CrossRef]
- Swift, S. L., Y. Drexler, D. Sotres-Alvarez, L. Raij, M. M. Llabre, N. Schneiderman, L. V. Horn, J. P. Lash, Y. Mossavar-Rahmani and T. Elfassy. "Associations of sodium and potassium intake with chronic kidney disease in a prospective cohort study: Findings from the hispanic community health study/study of latinos, 2008–2017." BMC Nephrology 23 (2022): 133. [CrossRef]
- Suenaga, T., S. Tanaka, H. Kitamura, K. Tsuruya, T. Nakano and T. Kitazono. "Estimated potassium intake and the progression of chronic kidney disease." Nephrol Dial Transplant 40 (2025): 1362-73. [CrossRef]
- Picard, K., M. I. Barreto Silva, D. Mager and C. Richard. "Dietary potassium intake and risk of chronic kidney disease progression in predialysis patients with chronic kidney disease: A systematic review." Adv Nutr 11 (2020): 1002-15. [CrossRef]
- Kim, H. J., H. B. Koh, G. Y. Heo, H. W. Kim, J. T. Park, T. I. Chang, T.-H. Yoo, S.-W. Kang, K. Kalantar-Zadeh, C. Rhee, et al. "Higher potassium intake is associated with a lower risk of chronic kidney disease: Population-based prospective study." The American Journal of Clinical Nutrition 119 (2024): 1044-51. https://www.sciencedirect.com/science/article/pii/S0002916524000716. [CrossRef]
- Gritter, M., L. Vogt, S. M. H. Yeung, R. D. Wouda, C. R. B. Ramakers, M. H. de Borst, J. I. Rotmans and E. J. Hoorn. "Rationale and design of a randomized placebo-controlled clinical trial assessing the renoprotective effects of potassium supplementation in chronic kidney disease." Nephron 140 (2018): 48-57. [CrossRef]
Figure 1.
Schematic representation of the human nephron (right) and the major characteristics of connecting tubule and cortical collecting duct (left). A human nephron is represented and its different segments are identified: G, glomerulus; EA, efferent arteriole; PT, proximal tubule; DCT, distal convoluted tubule; LH, loop of Henle; CNT, connecting tubule; CCD, cortical collecting duct. An anatomical relationship is established between the afferent arteriole (AA), the site of renin synthesis, the macula dense (MD), and the connecting tubule. In the distal nephron, cells of both CNT (CNTc) and CCD (CDc/PC) intermingle over a certain distance, whereas intercalated cells are present in both segments. CNTc produce and secrete renal kallikrein (KLK1) into the tubular lumen and the tubulointerstitium and CDc/PC produce the kininogens (KNGs) making feasible kinin production in both the urinary fluid and the interstitium. It is still unknown whether kininogens are secreted by CDc/PC or are filtered from interstitial capillaries into the interstitium. Once formed, kinins may stimulate the release of prostaglandin E2 (PGE2) from CDc/PC that in turn inhibits sodium and water absorption producing diuresis and natriuresis.
Figure 1.
Schematic representation of the human nephron (right) and the major characteristics of connecting tubule and cortical collecting duct (left). A human nephron is represented and its different segments are identified: G, glomerulus; EA, efferent arteriole; PT, proximal tubule; DCT, distal convoluted tubule; LH, loop of Henle; CNT, connecting tubule; CCD, cortical collecting duct. An anatomical relationship is established between the afferent arteriole (AA), the site of renin synthesis, the macula dense (MD), and the connecting tubule. In the distal nephron, cells of both CNT (CNTc) and CCD (CDc/PC) intermingle over a certain distance, whereas intercalated cells are present in both segments. CNTc produce and secrete renal kallikrein (KLK1) into the tubular lumen and the tubulointerstitium and CDc/PC produce the kininogens (KNGs) making feasible kinin production in both the urinary fluid and the interstitium. It is still unknown whether kininogens are secreted by CDc/PC or are filtered from interstitial capillaries into the interstitium. Once formed, kinins may stimulate the release of prostaglandin E2 (PGE2) from CDc/PC that in turn inhibits sodium and water absorption producing diuresis and natriuresis.
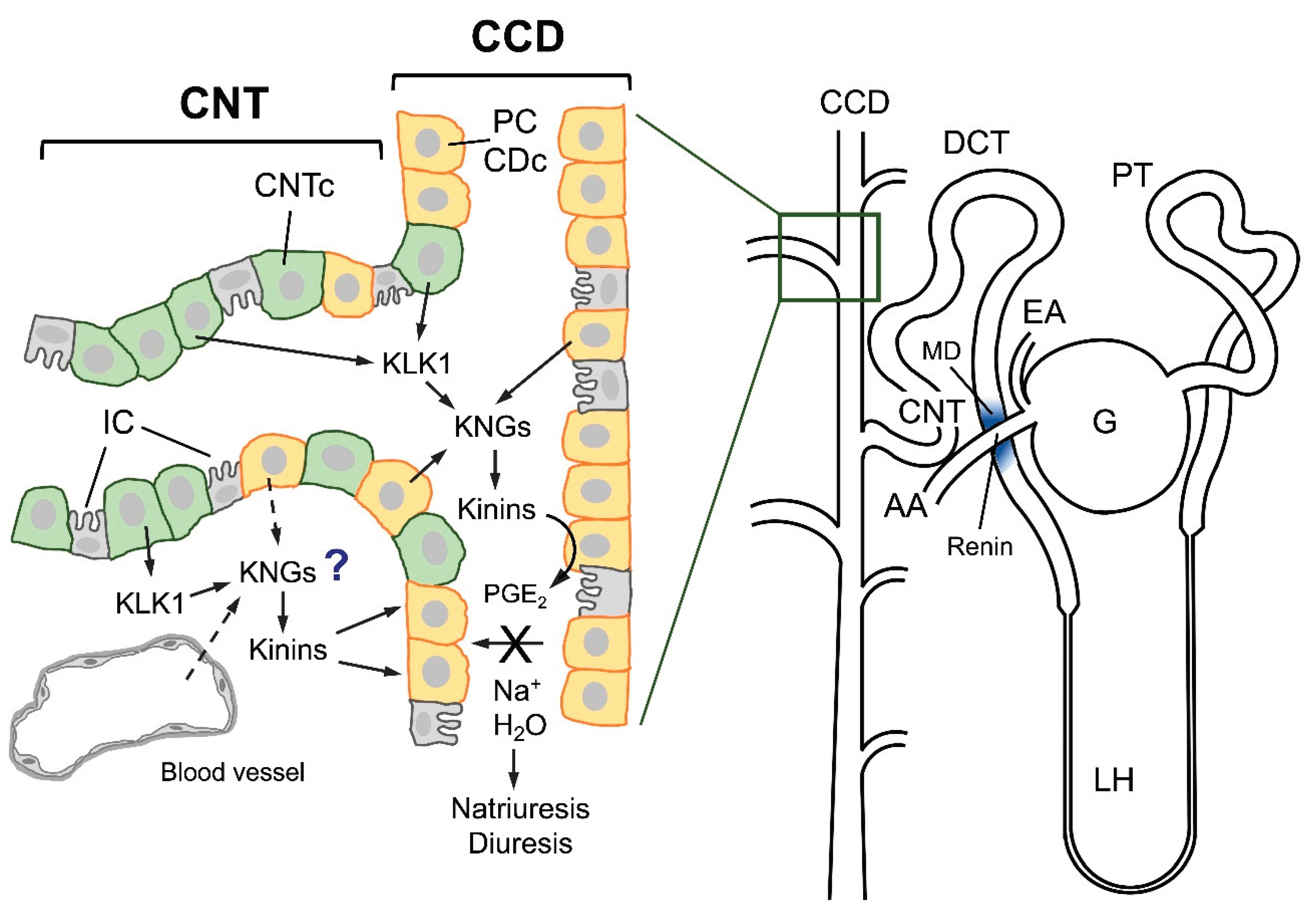
Figure 2.
Effect of a high potassium diet on the distal nephron (CNT-CCD). A high potassium diet induces hypertrophy and hyperplasia of CNTc and CDc/PC upregulating the synthesis and secretion of renal kallikrein (KLK1) by CNTc and the expression of kinin B2 receptor (B2R) in CNTc, and CDc/PC. So far, it is not known whether a high potassium diet also increases the synthesis and/or release on renal kininogens. Upregulation of the kinin system by a high potassium diet increases natriuresis and diuresis, and reduces fibrosis, oxidative stress, apoptosis, and blood pressure.
Figure 2.
Effect of a high potassium diet on the distal nephron (CNT-CCD). A high potassium diet induces hypertrophy and hyperplasia of CNTc and CDc/PC upregulating the synthesis and secretion of renal kallikrein (KLK1) by CNTc and the expression of kinin B2 receptor (B2R) in CNTc, and CDc/PC. So far, it is not known whether a high potassium diet also increases the synthesis and/or release on renal kininogens. Upregulation of the kinin system by a high potassium diet increases natriuresis and diuresis, and reduces fibrosis, oxidative stress, apoptosis, and blood pressure.
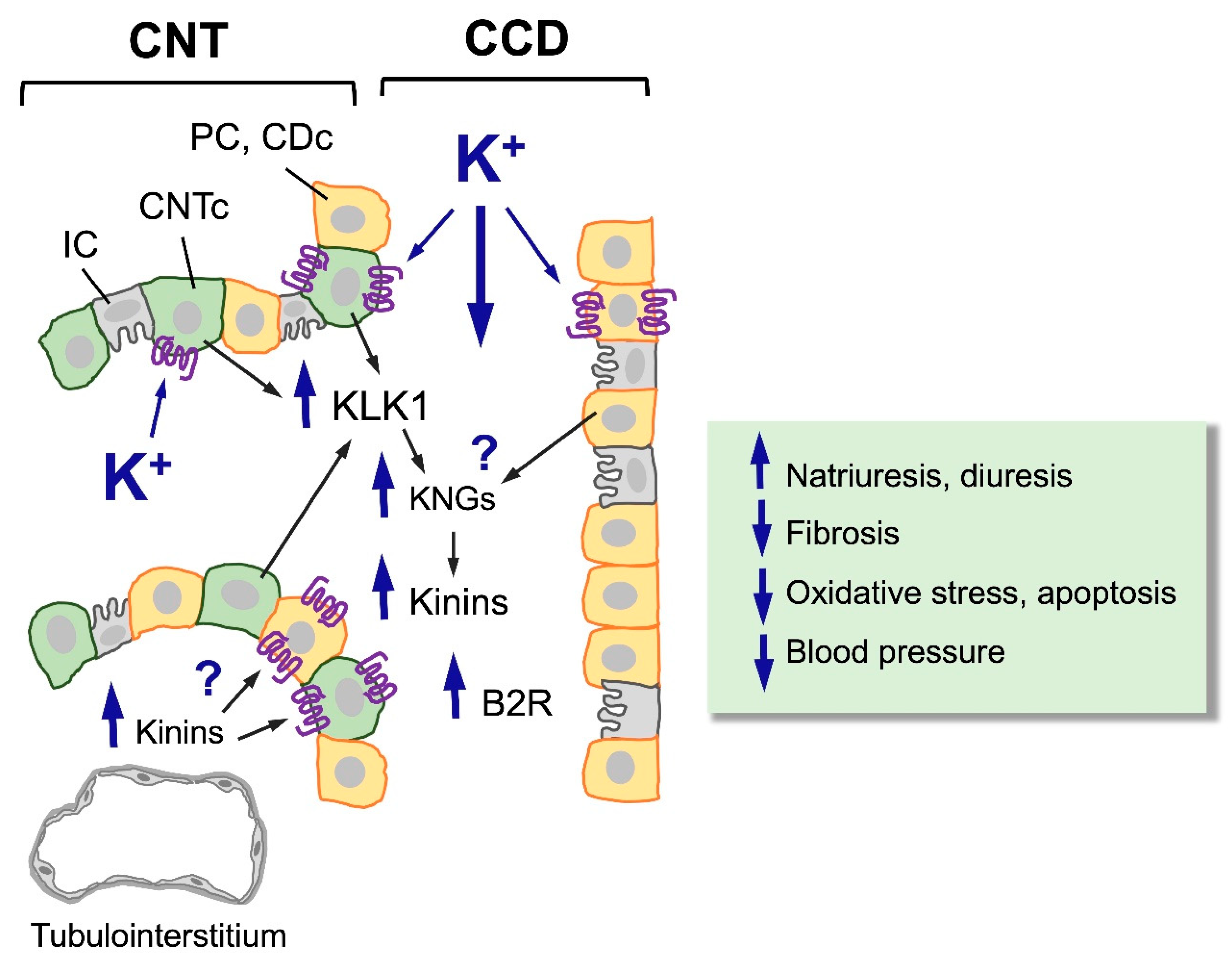
Figure 3.
Kinins and the kinin B2 receptor (B2R) counterbalance the effect of TGFbeta. TGFbeta is produced by various types of cells and is then secreted to the extracellular matrix (MEC) where it is activated and stimulate fibroblasts/myofibroblasts that accumulate in the tubulointerstitium and promote renal fibrosis. These cells may have different origin, including epithelial-mesenchymal transition (EMT) from damaged tubular cells that acquire a new phenotype characterized by high vimentin and alpha-smooth muscle actin (SMA). Kinins, through activation of the kinin B2 receptor (B2R) reduce EMT, myofibroblasts formation and renal fibrosis.
Figure 3.
Kinins and the kinin B2 receptor (B2R) counterbalance the effect of TGFbeta. TGFbeta is produced by various types of cells and is then secreted to the extracellular matrix (MEC) where it is activated and stimulate fibroblasts/myofibroblasts that accumulate in the tubulointerstitium and promote renal fibrosis. These cells may have different origin, including epithelial-mesenchymal transition (EMT) from damaged tubular cells that acquire a new phenotype characterized by high vimentin and alpha-smooth muscle actin (SMA). Kinins, through activation of the kinin B2 receptor (B2R) reduce EMT, myofibroblasts formation and renal fibrosis.
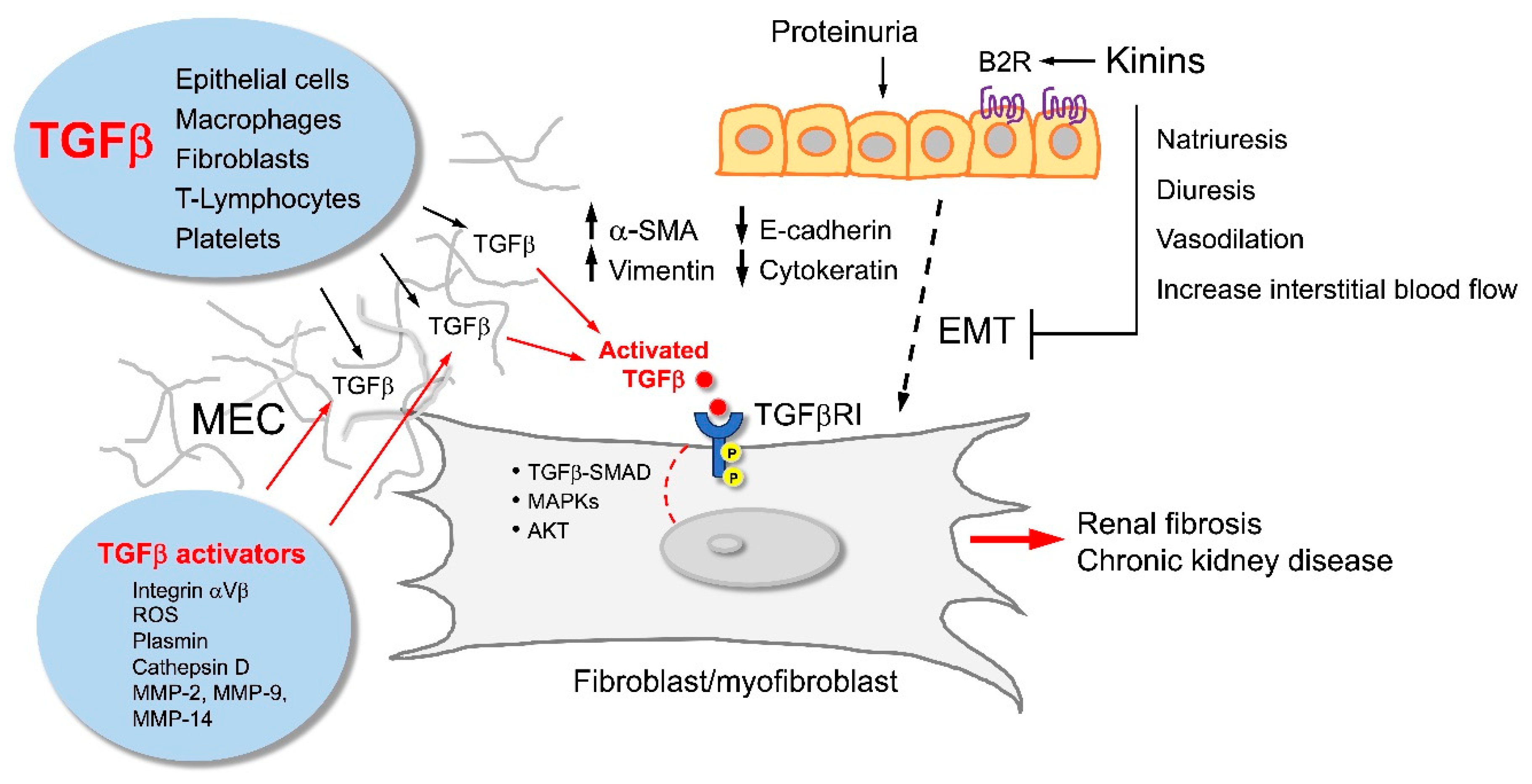
Figure 4.
Major signaling routes activated by TGFbeta and kinins in renal tubular cells. TGFbeta activates the Smad2/3/4 signaling pathway that favors epithelial-mesenchymal transition (EMT), myofibroblast differentiation and tubulointerstitial fibrosis. On the contrary, kinins and activation of the kinin B2 receptor (B2R) triggers the Smad7 pathway that reduces EMT and tubulointerstitial fibrosis. Potassium upregulates the kinin system enhancing the antifibrotic activity of renal kinins.
Figure 4.
Major signaling routes activated by TGFbeta and kinins in renal tubular cells. TGFbeta activates the Smad2/3/4 signaling pathway that favors epithelial-mesenchymal transition (EMT), myofibroblast differentiation and tubulointerstitial fibrosis. On the contrary, kinins and activation of the kinin B2 receptor (B2R) triggers the Smad7 pathway that reduces EMT and tubulointerstitial fibrosis. Potassium upregulates the kinin system enhancing the antifibrotic activity of renal kinins.
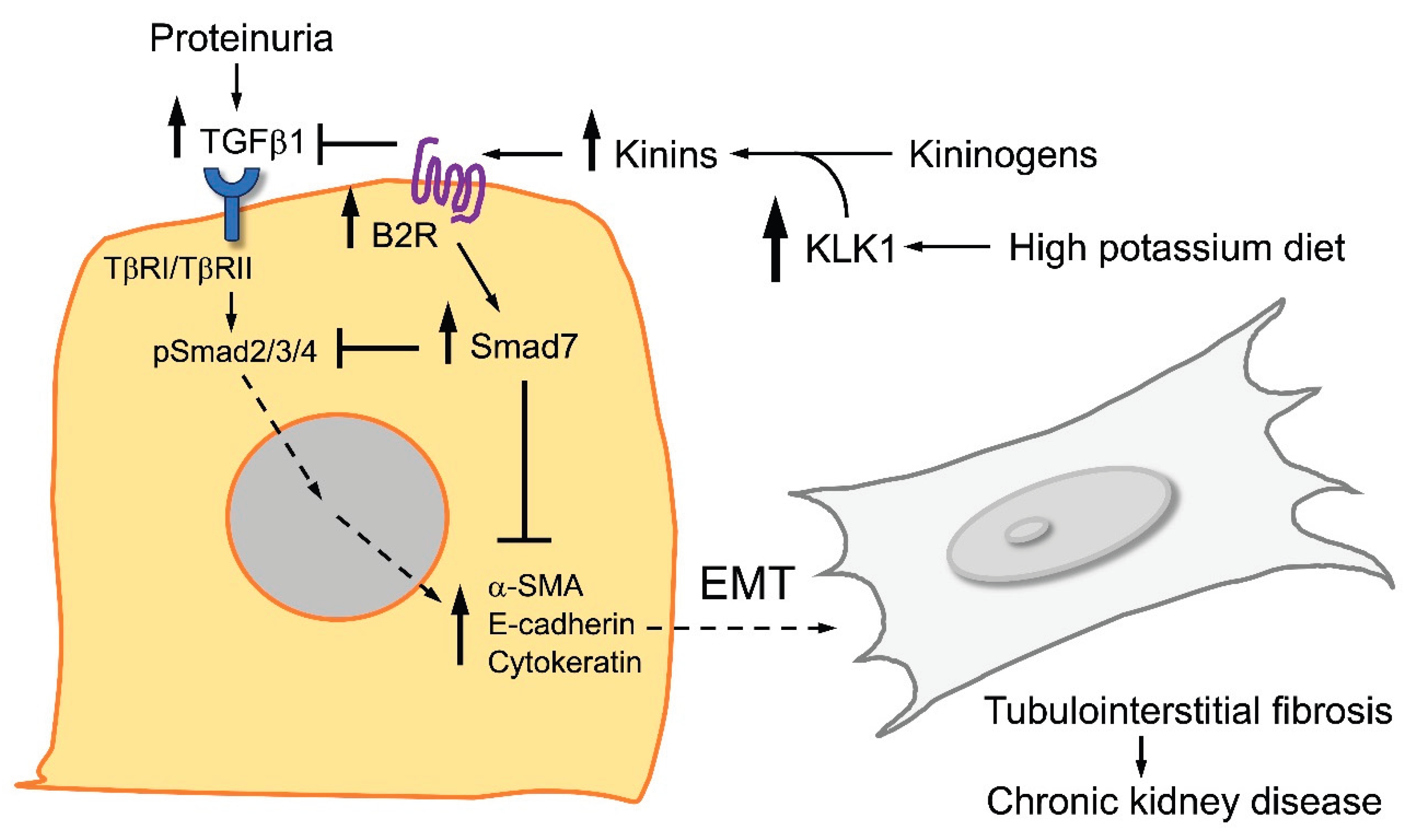
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



