Submitted:
17 November 2025
Posted:
18 November 2025
You are already at the latest version
Abstract
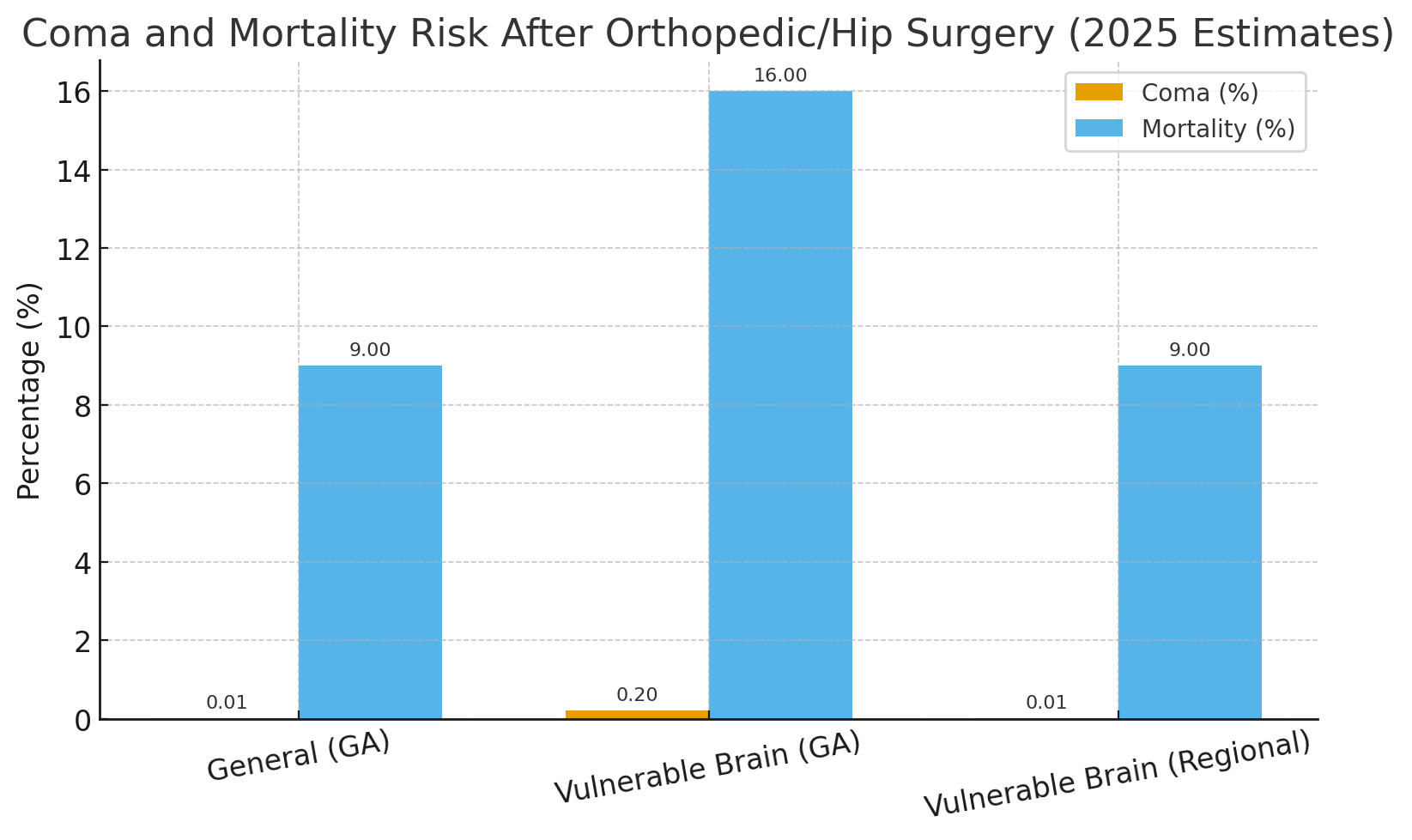
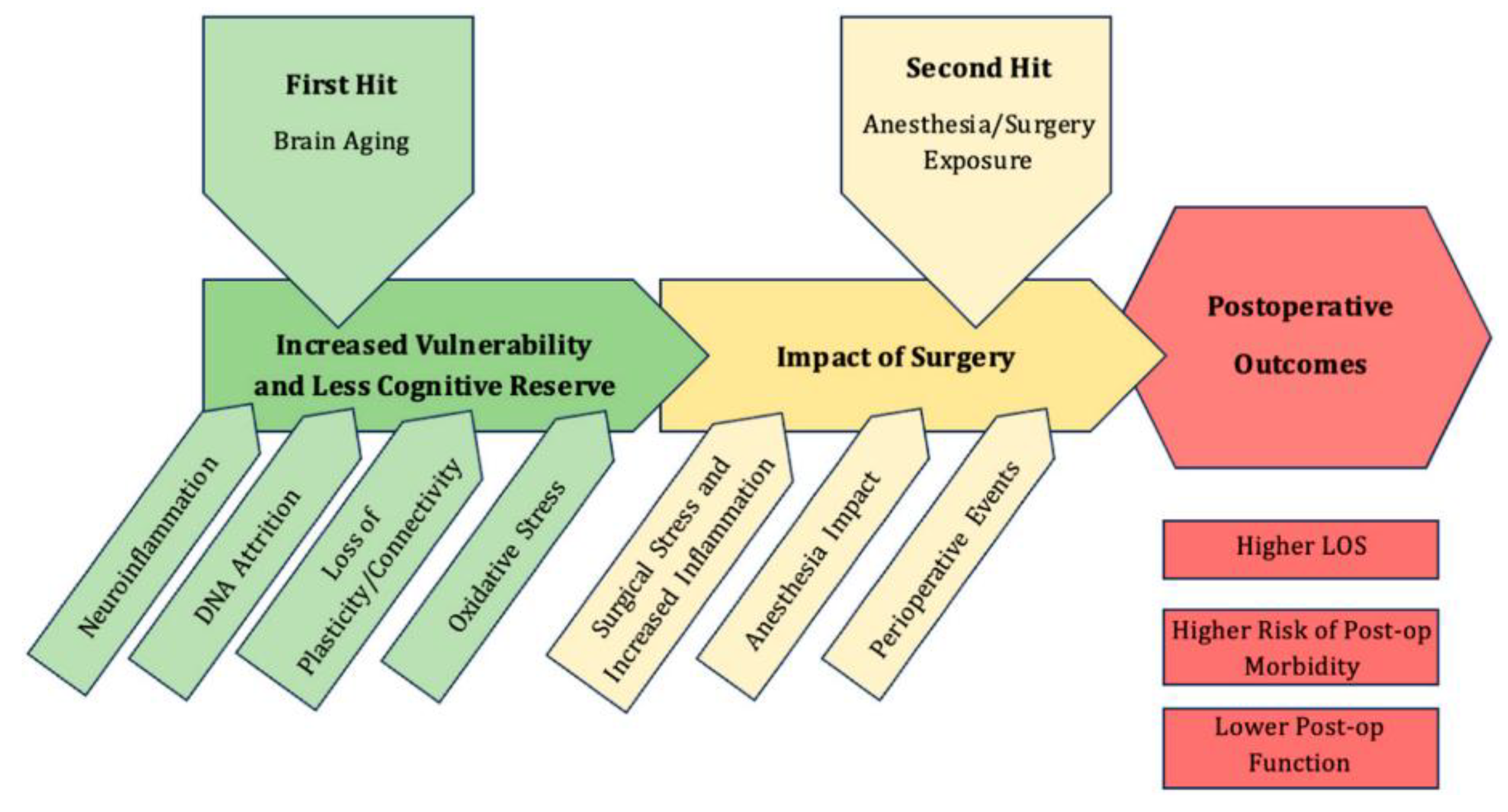
Orthopedic and lower limb fracture surgeries are among the most frequent emergency procedures and are commonly performed under general anesthesia (GA); Background and clinical significance: Epidemiologically, postoperative coma after GA is rare (0.005–0.08%), but delayed awakening (2–4%) and postoperative delirium or postoperative cognitive dysfunction (POCD) (15–40%) remain significant. These neurological complications increase markedly in vulnerable brain patients with psychiatric, cerebrovascular, or neurodegenerative disorders; Methods: This mechanistic narrative review synthesizes evidence from clinical and experimental studies (1990–2025) comparing the effects of general versus Regional (RA)/local (LA) or spinal anesthesia in vulnerable neuropsychiatric populations “with pre-existing brain illness” undergoing orthopedic surgery. Domains analyzed include: Neuropsychiatric medications effects and interactions with GA process and with general anesthetic agents, alongside alterations in neurotransmitter modulation, cerebrovascular autoregulation, mitochondrial dysfunction, oxidative stress, redox imbalance and neuroinflammatory activation. The review summarizes evidence on how the choice of anesthesia type influences postoperative brain outcomes in patients with known brain neurological conditions; Results: From previous studies, patients with psychiatric and/or chronic brain illness have 3-5-fold increased risk of delayed emergence and up to 60% incidence of postoperative delirium. Pathophysiological mechanisms involve GABAergic over inhibition, impaired perfusion, mitochondrial energy failure, and inflammatory amplification. Regional/local and spinal anesthesia preserve cerebral perfusion and are associated with significantly lower neurological complication rates; Conclusion: General anesthesia may exacerbate pre-existing brain vulnerability, converting reversible neural suppression into irreversible dysfunction. Therefore, whenever possible, regional/local or spinal anesthesia with or without sedation should be prioritized to reduce the length of hospital stay (LOS) and to lower postoperative neurological complications and risks in psychiatric and neurologically unstable patients.
Keywords:
1. Introduction and Clinical Significance
2. Methodology
3. Clinical Perspective: A Fragile Mind in a Surgical Emergency
4. Pathophysiology
5. Clinical Evidence and Discussion
6. Clinical Recommendations and Future Directions
7. Conclusions
Abbreviations
| GA | General Anesthesia |
| LA | Local Anesthesia |
| RA | Regional Anesthesia |
| POCDs | Postoperative Cognitive Disorders |
| GABA | Gamma-Aminobutyric Acid (Inhibitory) |
| LOS | Length of stay |
| PNDs | Perioperative Neurocognitive Disorders |
| NMDA | N-Methyl-D-Aspartate receptor (Glutamate/excitatory) |
| EEG | Electro Enchephalo GRAM |
| IL | Interleukin-6 |
| TNF | Tumor Necrosis Factor |
| REDOX | Oxidation Reduction |
| ATP | Adenosin Tri-Phosphate |
References
- Mashour, G.A.; Hudetz, A.G. Neural correlates of unconsciousness in large-scale brain networks. Trends Neurosci. 2018, 41, 150–160. [Google Scholar] [CrossRef]
- Evered, L.; Silbert, B.; Knopman, D.S.; et al. Recommendations for the nomenclature of cognitive change associated with anaesthesia and surgery. Br J Anaesth. 2018, 121, 1005–1012. [Google Scholar] [CrossRef]
- Deiner, S.; Silverstein, J.H. Postoperative delirium and cognitive dysfunction. Br J Anaesth. 2009, 103 (Suppl. 1), i41–i46. [Google Scholar] [CrossRef]
- Sanders, R.D.; Tononi, G.; Laureys, S.; Sleigh, J.W. Unresponsiveness ≠ unconsciousness. Anesthesiology. 2012, 116, 946–959. [Google Scholar] [CrossRef]
- Neuman, M.D.; Feng, R.; Carson, J.L.; et al. Spinal anesthesia or general anesthesia for hip surgery in older adults. N Engl J Med. 2021, 385, 2025–2035. [Google Scholar] [CrossRef]
- Zhou, J.; Yang, L.; Chen, W.; et al. General versus regional anesthesia for hip fracture surgery: an updated meta-analysis of randomized controlled trials. J Orthop Surg Res. 2023, 18, 47. [Google Scholar] [CrossRef] [PubMed]
- Pisani, M.A.; Kong, S.Y.; Kasl, S.V.; et al. Days of delirium are associated with 1-year mortality in an older intensive care unit population. Am J Respir Crit Care Med. 2009, 180, 1092–1097. [Google Scholar] [CrossRef]
- Brown, E.N.; Lydic, R.; Schiff, N.D. General anesthesia, sleep, and coma. N Engl J Med. 2010, 363, 2638–2650. [Google Scholar] [CrossRef] [PubMed]
- Cibelli, M.; Fidalgo, A.R.; Terrando, N.; et al. Role of interleukin-1β in postoperative cognitive dysfunction. Ann Neurol. 2010, 68, 360–368. [Google Scholar] [CrossRef]
- Hachenberg, T.; Schneemilch, C.E. Anesthesia in patients with neurological or psychiatric disorders. Curr Opin Anaesthesiol. 2014, 27, 468–474. [Google Scholar]
- Radtke, F.M.; Franck, M.; Lendner, J.; et al. Monitoring depth of anaesthesia in a randomized trial decreases the rate of postoperative delirium but not postoperative cognitive dysfunction. Br J Anaesth. 2013, 110 (Suppl. 1), i98–i105. [Google Scholar] [CrossRef]
- Terrando, N.; Eriksson, L.I.; Ryu, J.K.; et al. Resolving postoperative neuroinflammation and cognitive decline. Ann Neurol. 2011, 70, 986–995. [Google Scholar] [CrossRef]
- Volkow, N.D.; Thomas, J.D.; Wang, G.J.; Fowler, J.S. Neurobiologic mechanisms of addiction: relevance to diagnosis and treatment. Nat Rev Neurosci. 2019, 20, 663–678. [Google Scholar]
- Wang, D.S.; Orser, B.A. Inhibition of learning and memory by general anesthetics. Can J Anaesth. 2011, 58, 167–177. [Google Scholar] [CrossRef]
- Meng, L.; Gelb, A.W. Regulation of cerebral autoregulation by carbon dioxide. Anesthesiology. 2015, 122, 196–205. [Google Scholar] [CrossRef]
- Jensen, S.S.; Pedersen, A.B.; Vestergaard, P.; et al. Impact of dementia, depression, and other mental disorders on reoperation and mortality among hip fracture patients: a nationwide Danish cohort study. J Gerontol A Biol Sci Med Sci. 2025, 80, glaf074. [Google Scholar]
- Olofsson, E.; Gustafson, Y.; Odén, A.; et al. Factors associated with one-year mortality after hip fracture among very old adults (≥85 years): depressive disorders, history of stroke, and subtrochanteric fractures. Eur Geriatr Med. Epub ahead of print. 2025. [Google Scholar] [CrossRef]
- Olofsson, E.; Ohlen, G.; et al. Association of depressive disorders and dementia with long-term mortality after hip fracture. BMC Geriatr. 2023, 23, 383. [Google Scholar] [CrossRef] [PubMed]
- Jaruga, K.; Puścion-Jakubik, A.; Jakubów, P. Regional anesthesia: a narrative review of impact on oxidative stress biomarkers. J Clin Med. 2025, 14, 7503. [Google Scholar] [CrossRef] [PubMed]
- Stamenkovic, D.M.; Selvaraj, S.; Venkatraman, S.; Arshad, A.; Rancic, N.K.; Dragojevic-Simic, V.M.; Miljkovic, M.N.; Cattano, D. Anesthesia for patients with psychiatric illnesses: a narrative review with emphasis on preoperative assessment and postoperative recovery and pain. Minerva Anestesiol. 2020, 86, 1089–1102. [Google Scholar] [CrossRef] [PubMed]
- Crasta, C.M.; Hegde, D.; Chand, S.; Kolar, R.; Nandakumar, U.P. Critical evaluation of factors associated with pre-operative anxiety among patients scheduled for surgery in the orthopaedics department. Curr Probl Surg. 2024, 61, 101631. [Google Scholar] [CrossRef] [PubMed]
- Niu, Y.; Wang, Q.; Lu, J.; He, P.; Guo, H.T. Risk factors for postoperative delirium in orthopedic surgery patients: a systematic review and meta-analysis. Ann Med. 2025, 57, 2534520. [Google Scholar] [CrossRef] [PubMed]
- Bokhari, S.F.H.; Waseem, A.B.; Raza, H.; Javaid, S.; Idrees, B.; Saad, K.A.D.; Iqbal, A.; Bakht, D.; Dost, W. Impact of psychiatric disorders on surgical outcomes: a comprehensive review of preoperative screening and interventions. World J Surg Proced. 2025, 15, 104178. [Google Scholar] [CrossRef]
- Attri, J.P.; Bala, N.; Chatrath, V. Psychiatric patient and anaesthesia. Indian J Anaesth. 2012, 56, 8–13. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Garcia, P.S.; Kolesky, S.E.; Jenkins, A. General Anesthetic Actions on GABAA Receptors. Curr Neuropharmacol. 2010, 8, 2–9. [Google Scholar] [CrossRef] [PubMed Central]
- Mathew, C.; Wong, T.G.L.; Leong, R.W.L. Local anesthesia versus general anesthesia for surgical drainage of chronic subdural hematoma: a systematic review and meta-analysis. Can J Anaesth. 2024, 71, 870–882. [Google Scholar] [CrossRef] [PubMed]
- Levy, R.J. Carbon monoxide and anesthesia-induced neurotoxicity. Neurotoxicol Teratol. 2017, 60, 50–58. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Rengel, K.F.; Pandharipande, P.P.; Hughes, C.G. Special considerations for the aging brain and perioperative neurocognitive dysfunction. Anesthesiol Clin. 2019, 37, 521–536. [Google Scholar] [CrossRef] [PubMed]
- Ritiu, S.A.; Rogobete, A.F.; Sandesc, D.; Bedreag, O.H.; Papurica, M.; Popovici, S.E.; Toma, D.; Ivascu, R.I.; Velovan, R.; Garofil, D.N.; Corneci, D.; Bratu, L.M.; Pahontu, E.M.; Pistol, A. The impact of general anesthesia on redox stability and epigenetic inflammation pathways: crosstalk on perioperative antioxidant therapy. Cells. 2022, 11, 1880. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Tawfik, G.A.; Lu, M.; De La Hoz, M.; Crugnola, W.; Jin, Z.; Moller, D. Molecular and clinical considerations for anesthesia in the aging brain. Int J Mol Sci. 2025, 26, 10272. [Google Scholar] [CrossRef]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).



