
Submitted:
31 October 2025
Posted:
03 November 2025
You are already at the latest version
Abstract
Refugee-serving primary health centres/clinics (PHCs) provide culturally safe, integrated care for refugee children, yet little is known about how their health conditions and outcomes are assessed. This scoping review examined the health conditions and outcomes of refugee children aged 0-5 years and how they are measured in refugee-serving PHCs in Canada. Conducted in partnership with the New Canadians Health Centre and guided by Joanna Briggs Institute methodological guidelines, we systematically searched Medline, CINAHL, Scopus, and Embase. Included studies focused on refugee children in Canada and reported health conditions, outcomes, and their measurements within PHCs. Twenty-five studies (2008–2024) met the inclusion criteria, most from Ontario (n=11), followed by Alberta and Saskatchewan (n=4 each). Reported health conditions or outcomes (n=24) spanned physical (n=19), developmental, and mental health domains (n=5). Communicable (e.g., gastrointestinal infections, hepatitis) and non-communicable conditions (e.g., malnutrition, vitamin D deficiency) were mostly reported. Although some standardized approaches were used, variability exists across provinces and conditions or outcomes measured. Findings reveal disproportionate focus on physical health and notable variability and gaps in child health measures, limited cultural adaptation, and lack of longitudinal data. Standardized, culturally responsive, and age-appropriate measurement approaches are needed to enhance health equity and inform evidence-based policy for refugee children in Canada.
Keywords:
refugee
; children
; health
; outcomes
; conditions
; measurement tools
; refugee serving
; primary health centre
; Canada
1. Introduction
By the end of 2024, it was estimated that over 123.2 million people were forcibly displaced worldwide [1] due to armed conflict, human rights violations, and climate-driven displacement [1,2]. As global crises intensify, an increasing number of people are forced to flee their homes, further escalating the global emergency. In 2024, just four countries accounted for 94% of global resettlement arrivals: the United States (105,500), Canada (49,300), Australia (17,200), and Germany (5,600) [1]. Among countries with universal healthcare coverage, Canada plays a vital role in welcoming asylum claimants and refugees, receiving approximately 200,000 in 2023. While the country provides essential healthcare support to refugees, greater attention is needed to fully address the complex and evolving health needs of this population.
The majority of refugees, specifically, government-assisted refugees (GARs), are eligible for universal healthcare access upon arrival in Canada through the Interim Federal Health Program coverage [3]. This coverage includes essential and urgent medical services, immunizations, diagnostic testing, hospital care, prescription medications, and limited dental and vision care until they become eligible for provincial or territorial health insurance. Although GARs and Canadian citizens are eligible for the same healthcare, refugees face unique barriers, such as language, unfamiliarity with the healthcare system, and navigation challenges, which create healthcare access disparities.
The disparity in healthcare access is particularly consequential for refugee children, especially those younger than six years, due to their increased vulnerability, which is often attributed to missed immunizations, vitamin D deficiency, developmental delays, and malnutrition, including stunting, wasting, and underweight [4,5,6,7]. Given the heightened risks for refugee children, addressing their healthcare needs requires a unique approach to service delivery to mitigate the long-term consequences of unmet healthcare needs.
System-level perspectives and corresponding policies that consider health needs across time and context are required for effective refugee healthcare access and system delivery [8,9,10]. Additionally, being able to clearly define and measure these needs and outcomes is critical for effectively addressing the health disparities and informing equitable service delivery. Throughout the literature, several terminologies are used to denote health needs, health conditions, health issues, disorders, and health status, and are used interchangeably. For this study, health condition is used as an overarching term to include all of these terminologies and to mean the gap between an individual’s current health status and/or a standard level of health, often shaped by social determinants such as housing, education, and income [11,12,13,14,15]. Health conditions can vary from higher rates of communicable diseases and malnutrition to mental health conditions [16,17,18]. Similarly, health outcome is also used interchangeably in literature, and for this study, health outcome refers to the results of healthcare interventions or lack thereof, and broader social and environmental influences, which include changes in health status, behaviour, or knowledge due to healthcare or public health efforts [15,24]. These two broad terminologies, health conditions and outcomes, allow for a system-level understanding of refugee children's health that integrates clinical, social, and policy dimensions and reflects the complex interactions between individual health experiences and structural determinants.
Within the Canadian universal healthcare system, refugee-serving primary healthcare centres/clinics (PHCs) play a critical role in delivering care tailored to the unique healthcare conditions and outcomes of refugee children and their families. Examples of refugee-serving PHCs in Canada include the New Canadian Clinic in British Columbia, the Sanctuary Refugee Health Centre in Ontario, Mosaic Refugee Health Clinic and the New Canadian Health Centre (NCHC) in Alberta [19,20]. PHCs adopt systems-level approaches grounded in three key principles: a holistic view of health, a life-course approach, and culturally safe care [21,22,23,24]. Holistic view of health, which is linked with a life-course approach emphasizes that refugee children’s health is shaped by both clinical conditions and outcomes, and the social determinants of health, including socioeconomic status, language barriers, access to social services, and cultural beliefs about health, as well as their interactions with the healthcare system [12,24,25]. This approach highlights the importance of early intervention during the critical early developmental periods to support optimal development and long-term well-being [22,23,24]. Culturally safe care ensures that healthcare is respectful, equitable, and responsive to the cultural identities and lived experiences of refugee families, while promoting patient empowerment and involvement in decisions about their care [26,27,28,29,30]. Together, these integrated approaches can mitigate systemic barriers and improve healthcare access for refugee children [19,29].
Despite the growing recognition of refugee children’s complex and urgent health conditions and outcomes, most research remains disproportionately focused on adolescents, leaving infants and preschool-aged children underrepresented in the literature [11,12,17,31]. Significant gaps also persist in the measurement of health conditions and outcomes [31,32,33,34]. Furthermore, measurement of refugee children's health conditions or outcomes remains underdeveloped in the Canadian literature, with few studies offering systematic approaches [33].
A recent review by Higgins et al. [35] examined the health conditions of refugee children aged 0–6 years in high-income countries, identifying a high prevalence of infectious diseases, nutritional deficiencies, and developmental delays. While Higgins et al.'s review provides valuable insights into the types of health conditions affecting refugee children, it does not address how these conditions are identified, measured, or tracked within PHC settings. This scoping review addresses these critical gaps by describing health conditions and outcomes of refugee children from birth to five years old and how they are measured in refugee-serving PHCs in Canada. It focuses specifically on the Canadian context and the refugee-serving PHC environment. By capturing both the types of health conditions and outcomes, and measurement approaches, including methodologies, techniques, and tools, this review provides a more targeted analysis of the structural and procedural dimensions of refugee child health measurement in Canada and extends the contributions of Higgins et al. Understanding these measurement approaches is critical, as they influence clinical care, policy decisions, resource allocation, and long-term health planning. Moreover, by systematically mapping the current evidence, this review identifies inconsistencies and gaps, highlights best practices, and proposes approaches to improve the measurement of refugee child health conditions and outcomes. This study is especially timely given the growing refugee population in Canada and the need for a coordinated, systems-level response that ensures equitable and effective care.
2. Materials and Methods
The review followed the methodological guidelines from the Joanna Briggs Institute (JBI) for scoping reviews [36,37] and was reported according to PRISMA extensions for scoping reviews (PRISMA-ScR); designing, conducting, and reporting results [37,89]. This review was conducted in partnership with the New Canadians Health Centre (NCHC), a refugee-serving PHC, located in Edmonton, Canada, that has a vested interest in learning about the health conditions and outcomes measured and reported by other refugee-serving PHCs in Canada. The NCHC provides culturally safe healthcare services to government-assisted refugees, and its operations are grounded in principles of social justice, equity, and inclusion [20]. The centre’s Research and Evaluation Committee (REC), composed of interdisciplinary researchers, healthcare practitioners, and refugees with lived experience, played a central role in guiding this review. The REC was equitably involved in all stages of the review, including the interpretation of the findings, enhancing its relevance and benefit to the community as well as ensuring the review reflected both academic rigour and community priorities [38,39].
The review protocol was registered in Open Science Framework (https://doi.org/10.17605/OSF.IO/5C2PN) on November 5, 2024, ensuring transparency and methodological rigour. The data used in this study were all publicly available, and ethics approval was not required. In the section that follows, we outline the key steps of this protocol.
2.1. Identifying the Research Question
Through consultation with the REC, two research questions to guide the scoping review were identified: (1) What are the current refugee child health conditions and outcomes described in the literature in Canada, and (2) How are refugee child health conditions and outcomes measured by refugee-serving PHCs.
2.2. Identifying Relevant Studies
2.2.1. Search Strategy
Search terms were defined according to the Patient, Intervention Comparison and Outcome (PICO) criteria [40]. Relevant search terms for each aspect of PICO were gathered and applied in our systematic search. A health science librarian assisted in refining our search strategy and in conducting the search. In May 2024, we systematically searched the following databases: EMBASE, Global Health, Medline, CINAHL Plus with full text via Ebscohost, and Scopus Advanced Search for literature published from 1949 to 2024. The wide period ensured an inclusive understanding of the evolving health conditions and outcomes within refugee-serving PHCs in Canada. Slight adaptations of the search string were made for each database’s specific requirements.
We subsequently completed a grey literature search in November 2024. Grey literature was identified through targeted Google Advanced Search, Google Scholar, and relevant refugee and immigrant-serving PHC websites searches using the keywords applied in our database search. Further, systematic reference and citation screening were performed on the retrieved full texts. To capture the most recent studies, an updated search was conducted on May 17, 2025.
2.2.2. Eligibility Criteria
Inclusion and exclusion criteria were defined by population, age, setting, phenomena of interest, study design, publication type, country, and language. To be eligible, studies needed to include: (i) refugee children 0-5 years old in the population, (ii) child health outcomes or conditions, or (iii) health condition or outcome measurement tools, or (iv) primary healthcare centres or clinics providing services to refugees/immigrants. Studies addressing health conditions and outcome measurement tools were included only if they were specific to the target population (i.e., refugee children aged 0–5). Exceptions were made for studies that explicitly focused on developmental delays or disabilities, mental health, or behaviour-related issues in children, even if the population was broader. This is because these health conditions and outcome measurements are generally developed for the pediatric population, 0-18 years old. Two independent reviewers (AB and NA) screened the articles using these criteria and refined them through an iterative process. The full final inclusion and exclusion criteria are presented in Table 1.
2.3. Study Selection
All identified studies were imported into Covidence software [41], a web-based platform for systematic review collaboration and duplicates were removed automatically. Screening and full-text review were conducted independently and in duplicate by two researchers (AB and NA). Titles and abstracts were screened based on predefined inclusion and exclusion criteria, with an initial agreement rate of 82%. Disagreements were resolved through discussion and consensus. Full-text articles of included studies were then reviewed using the same process - AB and NA independently assessed each study against the criteria, and any disagreements were again resolved by consensus. Following the full-text review, both researchers independently conducted citation and reference searches of the included studies. These additional records were screened and reviewed using the same procedures described above.
Additional studies were identified through searches of Google Scholar and grey literature. These were screened using the same inclusion criteria and review process described above. However, none of the grey literature sources met the inclusion criteria, and the studies found through Google Scholar were duplicates of those already included.
2.4. Data Extraction
A data extraction spreadsheet was created in Covidence, which captured key study details, including publication information (authors, title, and year), study aim, participant demographic (age, gender, and country/region of origin), provinces where the study was conducted, study design, health conditions or outcomes, and their measurement (where applicable). After piloting the spreadsheet on a few articles, it was refined to include additional fields such as data sources, type of refugee or immigrant population, detailed descriptions of outcome measurements, key findings, and discussion points (see Supplementary Material Table 2).
Two researchers (AB and NA) independently extracted data into Covidence. Each entry was cross-checked by the other researcher to ensure accuracy before finalizing. Countries of origin for study participants were categorized using the World Health Organization’s regional groupings (WHO, n.d.).
2.5. Synthesis of Extracted Results
Extracted data were synthesized and organized according to the study’s research questions. A descriptive summary of study characteristics was first developed, followed by a thematic analysis focused on child health conditions and outcomes, and how they are measured. The analysis began with familiarization with the data, followed by inductive coding of text related to health conditions, outcomes, and measurement approaches. These codes were grouped into broader themes that reflected recurring patterns across studies. Themes were refined through iterative comparison and validation between researchers (AB and NA) to ensure consistency and relevance. The final themes captured key insights into the types of child health conditions and outcomes reported, such as developmental and mental health (e.g., behavioural difficulties, ADHD, emotional dysregulation, aggression, anxiety, and depression), as well as physical health. The methods used to assess these outcomes included clinical assessments, parental reports, standardized tools, and consideration of contextual factors influencing health.
3. Results
The results are presented in two sections; the first section describes the demographics of study characteristics, including participants' age, gender, country or region of origin, and the health conditions and outcomes identified across the studies. The second section presents the thematic analysis, identifying themes on physical, developmental, and mental health conditions or outcomes and measurements. This second section is organized by research questions.
3.1. Studies Included
A total of 818 articles, including Google Scholar articles, were retrieved based on our systematic search strategy. After removing duplicates, title and abstract screening, and full text review, a total of 25 articles were included in the review. See Figure 1 for the PRISMA flow diagram.
3.2. Study Characteristics
The studies were published between 2008 and 2024, with nearly half being published within the last five years. See supplementary Material Tables 2 and 3, which present summaries of studies included, study aim, their design, population characteristics, health conditions and outcome categories, and their measurement. Most studies were conducted in Ontario (n=11), followed by Alberta and Saskatchewan (n=4 each), Quebec (n=2), British Columbia (n = 1), national-level studies (n = 2), and one study spanning Ontario and Quebec, all provinces in Canada. Twenty-two of the studies were cross sectional studies, and three were cohort studies. Of 25 studies, 20 employed quantitative methods, four used mixed-methods, and one was a qualitative study. Most of the studies were retrospective designs (n = 24), with only one prospective study. A total of 21 of the 25 included studies presented information on health condition or outcome measurements (Supplementary Material Table 2). Electronic medical record (EMR) chart reviews were the predominant data source for assessing health conditions or outcomes (n = 15), followed by surveys (n = 3), health screenings (n = 3), administrative databases (n = 2), and clinical assessments (n = 2).
Thirteen studies reported disaggregated outcomes for children aged 0–5, while 19 included children older than six. Gender was reported in 22 of the 25 studies, with female representation ranging from 40% to 57% (mean = 49%, SD = 5.0). Two studies included refugees and claimants, one included refugees and asylum seekers, and the remaining 22 focused solely on refugees. Half of the studies (n = 12) did not specify refugee categories. Among the 13 that did, eight involved Government-Assisted Refugees (GARs), four included both GARs and Privately Sponsored Refugees (PSRs), and one included GARs, PSRs, and Blended Visa Office-Referred refugees. Twenty studies reported participants’ countries of origin, representing 28 countries, primarily from the Middle East, Asia, and sub-Saharan Africa.
3.3. Refugee Child Health Conditions and Outcomes in Canada
A thematic analysis of extracted data found 24 distinct health conditions and outcomes across the 25 included studies. Although many studies reported conditions and outcomes at various age ranges, we specifically focus on those relevant to children from birth to five years. The 24 health conditions and outcomes were further categorized into physical health (n=20), developmental, and mental health (n=5). Of the 20 studies on physical health, 21 unique health conditions and outcomes were identified and categorized into communicable and non-communicable diseases/conditions.
3.3.1. Communicable Diseases
The most commonly reported communicable diseases included gastrointestinal infections (n = 6) [13,35,51,52,54,60], parasitic infections (n = 5) [35,51,55,60,62], and hepatitis (n = 4) [35,51,60,62]. Gastrointestinal infections, including Giardiasis and Cryptosporidiosis, and parasitic infections, including worms, Strongyloides stercoralis, and Schistosoma species, were often interrelated, and typically a result of contaminated food and water, conditions frequently encountered in refugee camps or during migration journeys. Hepatitis, particularly type B, is likely due to the lack of or missed childhood immunizations [62]. Three studies [35,56,62] reported on Tuberculosis or Latent tuberculosis infections (LTBI).
3.3.2. Non-Communicable Diseases
A total of 19 different non-communicable diseases/conditions were identified across the included studies [35,36,37,46,47,48,49,50,51,53,54,55,58,59,62,63,64,65,66]. The most commonly reported were malnutrition and bone density (n = 10) [35,37,47,48,49,50,51,55,58,62,65], which often co-occurred. Malnutrition included both undernutrition and micronutrient deficiencies, often linked to food insecurity and inadequate dietary intake. Bone health conditions such as rickets were associated with insufficient vitamin D and calcium levels. Heamatological conditions, including anemia (n=5) [35,51,55,62,64], were also prevalent. While anaemia [35,51,55,62,64] and iron deficiency [35,62] were sometimes reported separately, anaemia in children was attributed to chronic illness and genetic conditions. Immunization status (n=4) [35,47,59,63], with incomplete, delayed, or no immunization, was identified as a contributing factor to the persistence of preventable infectious diseases. Oral health conditions (n = 4) [35,36,37,66], included dental caries and periodontal disease, frequently linked to poor oral hygiene practices and limited access to dental care services. Lastly, vitamin deficiencies (n = 4) [35,50,53,64], particularly vitamin A, D, and B complex, were associated with a range of health conditions including impaired immunity, vision problems, and neurological symptoms.
3.3.3. Developmental and Mental Health of Refugee Children
A total of five studies [35,45,49,54,57,58,61] reported on the developmental and mental health of refugee children. These health conditions focused primarily on neurodevelopmental delays and disabilities, behavioural difficulties including attention-deficit/hyperactivity disorder (ADHD) and emotion dysregulation, aggression, anxiety, and depression. These studies described the effects of child developmental and mental health conditions through neurodevelopmental delays and disabilities, behavioural and emotional dysregulation, such as irritability, excessive or aggressive behaviours, tantrums, social withdrawal, and loss of interest in daily activities or difficulty with attention. This complex interplay of these conditions and their effects on child developmental outcomes was also noted.
3.4. Measurement of Refugee Child Health Conditions and Outcomes by Refugee-Serving PHCs
Using the overarching categories of communicable and non-communicable diseases and developmental and mental health, the specificity of how health conditions and outcomes are measured varied considerably, as detailed below. Generally, most articles did not specify the age range that is appropriate for each tool. Therefore, it is assumed that measurement approaches, including methodologies, techniques, and tools, are used for children five years or younger, unless otherwise stated.
Among the studies included, only one study [58] provided the measurement approach for all three categories: communicable, non-communicable, and developmental and mental health. The study authors utilized electronic medical records as a secondary data source, and reviewers manually diagnosed clinical conditions and outcomes per the International Classification of Diseases and Related Health Problems, the 10th Revision, Canada (ICD-10-CA).
3.4.1. Communicable Diseases
Six studies [51,52,55,56,60,62] reported on the approaches used to measure various communicable diseases, including intestinal parasites and respiratory infections. All studies that reported on their parasite detection method used the stool ova and parasites test 51,52,55,60]. Specific approaches varied across laboratories. In one study [55], conducted in Quebec, Canada, positive microscopy results were used for initial detection, followed by enzyme immunoassay to differentiate Entamoeba species, whereas in another study [52], conducted in Alberta, Canada, enzyme immunoassay was used initially to screen for Giardia and Cryptosporidium, followed by microscopic examination of all specimens. While both studies employed microscopy and enzyme immunoassay, the order and purpose of the tools varied.
In addition to approach variations, some studies differentiated between active infections and prior exposure. In a study [51] conducted in Ontario, hepatitis B surface antigen (HBsAg) was tested to detect active infection, and for hepatitis B core antibody (anti-HBc) to assess prior exposure. Prior exposure to varicella was measured through an Immunoglobulin G (IgG) positive test. Lastly, a study conducted in Saskatchewan, Canada [56] provided information on measuring latent Tuberculosis infection through two different methods: Interferon-Gamma Release Assay (IGRA) and Tuberculin Skin Test. Interferon-Gamma Release Assay was for children older than two years, while Tuberculin Skin Test is for children between 6 months and 2 years.
3.4.2. Non-Communicable Diseases
Growth/Malnutrition/Bone Density
Ten studies [44,47,49,50,51,53,55,62,63,64,65] reported on the measurement approaches used to assess children’s growth. Although there were a variety of measures used, the most common was a simple measurement of height and weight to determine body mass index, based on the World Health Organization’s (WHO) criteria. One study [62] used both the Centers for Disease Control and Prevention Clinical Growth Charts and the WHO Child Growth Standards to norm-reference height and weight. Comparatively, Guttman6 categorized birth weight by predetermined criteria: very low (400-1499 g), low (1500-2499 g), and normal (32500 g). Another study [65] used the dual energy X-ray absorptiometry (DXA) machine, which measured body composition, bone mineral content, and density of total body, hip, and lumbar spine. Although all children (3-13) underwent the DXA scan, clinical reference standards were not available for children younger than 8 years. Weight was interpreted using the American anthropometric standards for children aged 5–13 and DXA-specific standards for those aged 8–13. Waist circumference was measured using the American standards for children 5 years and older, and the Canadian standards were applied for those aged 11–13.
Across the six studies [44,49,50,53,64,65] that measured vitamin D, most measured serum 25-hydroxyvitamin D (25[OH]D), the primary circulating form of vitamin D. However, interpretation of serum levels varied, with some studies referencing the Institute of Medicine, Osteoporosis Canada, or the Canadian Pediatric Society guidelines. There was no consensus on the threshold for sufficiency, with some studies using 50 nmol/L and others 75 nmol/L as the cutoff. In one study3, in addition to serum measurement, researchers also administered the Vitamin D Food Frequency Questionnaire (Baxter-Jones et al., 2010), which collected data on the type and frequency of foods and drinks consumed. Another study [49] indirectly measured vitamin D status by reporting whether infants received vitamin D supplements, as recommended by Health Canada (2012) for infants and young children.
Anaemia/Heamatological Conditions
Immunization Status
Immunization status was measured in two papers [47,63]. One of the two studies6 categorized immunization rates by the percentage of complete immunization, but did not define the exact vaccines required. The other study [63] defined complete immunization as three doses of Diptheria/Pertussis/Tetanus/Polio/Haemophilys influenza B (DPTP/Hib) with a booster and one dose of measles, mumps, and rubella vaccine.
Diabetes
Three studies [51,59,65] measured diabetes by measuring glucose levels. One of the three studies [65] measured serum glucose using a random capillary blood glucose test and classified levels ≥ 7.8 mmol/L as high. Another study18 followed the 2013 Canadian Diabetes Association guidelines, identifying prediabetes or diabetes based on fasting glucose ≥6.1 mmol/L, random glucose ≥11.1 mmol/L, or HbA1c ≥6.0%. Similarly, one of the studies10 used fasting glucose, random glucose, and HbA1c to define impaired glucose metabolism, with thresholds of ≥7.0 mmol/L, ≥11.1 mmol/L, and ≥6.5%, respectively.
Oral Health
Two studies [43,66] measured children’s oral health through clinical examinations. Clinical examinations were used to measure multiple oral health indicators, including dental caries, oral hygiene, gingival health, and malocclusion status. Dental caries was diagnosed according to the WHO standard criteria, which counted the number of decayed, missing, and filled primary and permanent teeth (dmft/DMFT). Oral hygiene was measured based on the amount of plaque accumulation and quantified using the Simplified Oral Hygiene Index. Gingivitis and malocclusion were both measured through visual inspection, based on signs of redness, swelling, and spontaneous bleeding, and the appearance of cross bite, open bite, overbite and overjet. Additionally, urgent treatment needs were recorded for pain and infection, extractions, restorations, orthodontics, plaque control instructions, scaling, and root planning.
Eye Health
Only one study [46] reported eye health, specifically ocular health status. Data collection included self-reported medical history, including ocular histories, clinical assessments, and interviews assessing subjective visual acuity and access to eye care. The clinical assessments involved visual screening, slit-lamp examinations, direct dilated fundoscopy, and refractive index measurements.
3.4.3. Developmental and Mental Health
Overall, six studies [35,45,49,57,60] reported on developmental and mental health conditions with varying foci and measurement tools. Three studies [45,47,49] reported information on the measurement of child development. One study [47] in Ontario, Canada reported on the uptake of the enhanced 18-month well-child visit (EWCV), a developmental check-up to evaluate expected milestones. In the two other studies, several measures were used to assess developmental disabilities and delays, including the Nipissing District Assessment tool; the Rourke Baby Record; the Parents Evaluation of Developmental Status; Ages and Stages Questionnaire, the Autism Diagnostic Observation Schedule, the Modified Checklist for autism in toddlers, and the Childhood Autism Rating Scale screening tools. These tools are recommended by both the Canadian Pediatric Society and the American Academy of Pediatrics. The current standard of care for children includes Surveillance and Standardized Developmental and Behavioural Screening (Council on Children with Disabilities et al., 2006; Guevara et al., 2013; Lipkin & Macias, 2020; Rourke et al, 2019; Sheldrick & Perrin, 2013). The Nipissing District Assessment Tool, a standardized developmental screening tool, was used to monitor the developmental progress of children from one month to six years of age for early intervention. The tool includes a series of age-based questionnaires (e.g., 2 months, 6 months, 12 months, etc.) that assess a child’s development across key domains. This tool is widely used in Canada and internationally by health professionals, early childhood educators, and parents. The Rourke Baby Record is used for children from birth to five years and provides guidelines on developmentally appropriate milestones (Rourke et al., 2009). Similarly, the Parents' Evaluation of Developmental Status and the Ages and Stages Questionnaire are used for children from birth to 11 years and four months to five years, respectively. Several tools are also used for the screening and measurement of autism. The Autism Diagnostic Observation Schedule, the Modified Checklist for Autism in Toddlers, or the Childhood Autism Rating Scale Questionnaire screening tools are used. However, for autism spectrum disorder (ASD), the Autism Diagnostic Observation Schedule, the Modified Checklist for Autism in Toddlers, or the Childhood Autism Rating Scale is preferred.
All the studies [35,45,49,57,60] that measured mental health conditions and outcomes utilized different measurement tools, based on the availability of local data. One study [57] leveraged the 2014 Ontario Child Health Study Emotional Behavioural Scales, which is a parent/caregiver-report tool that evaluates internalizing and externalizing symptoms to measure seven mental health disorders (using the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders - 5). Internalizing behaviours include measuring symptoms of generalized anxiety disorder, separation anxiety disorder, major depressive disorder, and social phobia/social anxiety disorder, while externalizing behaviours include measuring symptoms of attention deficit hyperactivity disorder (ADHD), oppositional defiant disorder, and conduct disorder. Another study [61] relied on the use of multiple databases to investigate cases of ADHD, conduct disorders, and mood/anxiety disorders among immigrant, refugee, and nonimmigrant children in the province of British Columbia in Canada. The authors based their indicators on another Canadian provincial health policy, the Manitoba Centre for Health Policy’s operational definitions, which were developed using International Classification of Diseases (ICD-9 and ICD-10) codes. Diagnoses were determined through a combination of drug dispensation and diagnoses of several different types of disorders. For instance, children diagnosed with hyperkinetic syndrome and prescribed ADHD medication were classified as having ADHD.
4. Discussion
This section first discusses the key findings describing health conditions and outcomes in the current literature, then examines the measurement approaches for the conditions and outcomes. Next, the methodological and contextual gaps in measurement practices are discussed, followed by an exploration of the implications of the review findings for research, clinical practice, and policy. To conclude, recommendations to enhance the measurement and delivery of refugee child health services in Canada are proposed.
4.1. Refugee Child Health Conditions and Outcomes
The findings from this review align with global data but also bring to the fore unique challenges in the Canadian healthcare and research context. Many studies aggregate data across broad pediatric age ranges (0–18 years) or focus specifically on adolescents (13–18 years), which obscures the unique developmental and health barriers faced by younger. refugee children, limiting the ability to generate age-specific insights and interventions. Communicable diseases, particularly hepatitis A and B, remain a significant concern. Globally, hepatitis B alone causes approximately 800,000 deaths annually for all age groups (Lavanchy & Kane, 2015), and recent studies confirm its continued burden in vulnerable populations (Xiao et al., 2024). The review finding aligns with the global trend, indicating that viral hepatitis remains a major contributor to global morbidity and mortality, particularly in regions with limited access to vaccination and treatment programs [67,68]. In Canada, refugee children are at heightened risk due to pre-migration exposures and post-migration conditions such as overcrowded shelters and poor sanitation [17,56,58]. While Canada has strong vaccination programs, the re-emergence of vaccine-preventable diseases suggests gaps in immunization coverage, follow-up care, and surveillance, not just among refugee populations but the general population. This calls for enhanced early screening, catch-up vaccination, and monitoring to prevent outbreaks.
Non-communicable diseases are also prevalent. These often co-occur, shaped by both pre- and post-migration factors. While these findings are consistent with broader Canadian child health data, refugee children face compounded risks due to systemic barriers in accessing care [17,20,69]. The literature supports the need for nutrition-sensitive, integrated, culturally safe healthcare approaches, yet evidence on long-term outcomes and effectiveness of intervention remains limited, indicating a critical area for future research.
Despite growing recognition of the psychological toll of forced migration, few Canadian studies focus specifically on young refugee children’s developmental and mental health. This gap is consistent with findings from Higgins et al. [35] and supported by the findings from the Centre for Addiction and Mental Health and the Canadian Medical Association Journal (CMAJ) [6]. The co-occurrence of anxiety and depression combined with the diagnostic challenges in assessing young children, and cultural stigma associated with mental health, may have contributed to the underreporting and underdiagnosis [70,71]. While tools like the CMAJ-endorsed screening checklist [6,72,73] offer guidance, Bhayana & Bhayana [45] emphasize the need to integrate these tools into broader clinical guidelines from the Canadian Pediatric Society and the Centre for Disease Control (CDC) to ensure trauma-informed, culturally safe care.
This review confirms what is already known globally: refugee children are at risk for both infectious and chronic conditions. However, in the Canadian context, the literature remains fragmented, with limited longitudinal data, inconsistent reporting on developmental outcomes, and a lack of studies on tropical or parasitic diseases that may be unfamiliar to Canadian clinicians. This raises concerns about the preparedness of the healthcare system to manage conditions that are rare in the general population but increasingly relevant due to global migration and global climate change. Addressing these challenges requires Canada to strengthen its early screening programs, ensure equitable access to vaccinations, expand culturally safe care, particularly for mental health services, and invest in longitudinal research that captures the evolving health conditions of young refugee children.
4.2. Measurement Inconsistencies and Their Implications for Refugee Child Health Assessment
This review highlights the lack of age-specific details and raises questions about the appropriateness and accuracy of some measurement approaches for young children, particularly in the context of refugee health, where developmental and cultural considerations are critical, yet often overlooked. Additionally, this study identified the heterogeneity in the measurement of health conditions and outcomes among refugee children in Canada. While some measurement practices align with established clinical guidelines, others differ widely between provinces and institutions, reflecting broader systemic inconsistencies in pediatric health assessment. These inconsistencies stem from a lack of standardization in measurement techniques and tools, protocols, and reference criteria. These findings raise critical questions about the reliability, comparability, and clinical utility of current practices. This is especially concerning in refugee health, where early and accurate measurement is essential, and the preparedness of the Canadian healthcare system is vital.
For communicable diseases, while some measurement techniques and tools, such as those used to detect latent Tuberculosis infection, are standardized across Canada, others show significant variations. For example, the detection of stool ova and intestinal parasites differs notably between provinces due to the variations in public health guidelines, laboratory infrastructure and protocols, and test availability. These differences are driven more by provincial systems than by refugee-specific considerations. In Müller et al.'s [55] study in Toronto, Ontario, and DeVetten et al.'s [52] study in Calgary, Alberta, though both tested for parasitic infections, the order and purpose used for the microscopy and enzyme immunoassay were different. Müller et al. [55] followed Public Health Ontario’s recommendations [74] by using microscopy first, followed by enzyme immunoassay (EIA) to differentiate or confirm Entamoeba species. In contrast, [52] prioritized EIA or multiplex PCR for initial screening, with microscopy as a secondary method, consistent with Alberta Health Service protocols [75]. Such variability, while not unique to refugee populations, has greater implications for them. Refugee children may present with infections uncommon in the general Canadian population, such as tropical parasites or vaccine-preventable diseases. Inconsistent diagnostic sensitivity across measurements can lead to missed or delayed diagnoses [76], emphasizing the need for Canadian standardized protocols for refugee health screening.
In contrast, measurement practices of non-communicable diseases were more consistent with minor variations. Most studies used body mass index and growth charts from the World Health Organization (WHO) or CDC to assess height and weight. However, more advanced assessments, such as dual-energy X-ray absorptiometry (DXA), revealed gaps in normative data, particularly for children under age eight. The International Society for Clinical Densitometry [77] notes the absence of validated reference standards for children under three, limiting the interpretability of DXA results in younger age groups. While this limitation is not exclusive to refugee children, it is especially problematic in this population, where growth delays and nutritional deficiencies are more prevalent and early intervention is critical.
For assessment of development and mental health in young children, tools like the Ages and Stages Questionnaire, the Parents' Evaluation of Developmental Status, and Rourke Baby Record are recommended by the Canadian Pediatrics Society and American Academy of Pediatrics; their applications vary, and age ranges are often unspecified. Moreover, few studies used multi-informant or culturally informed tools, despite evidence that refugee children may express anxiety and depression differently due to trauma and cultural norms [78]. Bernhardt et al. [78] found that refugee children exhibited lower levels of social-interactive play and higher instances of traumatic reenactment play, behaviours linked to parental distress and adverse experiences. These findings emphasize the need for developmentally appropriate, culturally safe, and trauma-informed assessments. Yet, the literature remains sparse, and there is no clear gold standard for evaluating mental health in refugee children, particularly in early childhood.
Measurement variability, from the findings, is typical across Canadian pediatric care, not just in refugee contexts. However, the consequences of the variability are amplified in refugees due to their complex health profiles and increased vulnerability. This scoping review findings also extends existing knowledge by revealing how systemic inconsistencies intersect with cultural and developmental complexities, shaping the health experiences and outcomes of refugee children in Canada. While some measurement approaches are well-established, others lack age-appropriate norms, cultural adaptability, or diagnostic sensitivity. What remains unknown is how these inconsistencies affect clinical outcomes, service access, and long-term health trajectories for refugee children, which we propose future research could focus on.
4.3. Inconsistent Data Collection and Its Consequences for Refugee Children
This review reveals substantial gaps in the literature regarding both the health conditions and outcomes affecting refugee children in Canada and the measurement methodologies. While a wide range of physical, and developmental and mental health conditions and outcomes were identified, the depth, consistency, and cultural relevance of measurement practices remain limited. These gaps have significant implications for clinical care, research, and policy development.
4.3.1. Gaps in Health Conditions and Outcomes
Research and practice on health conditions and outcomes are heavily skewed toward communicable and non-communicable diseases, despite the known prevalence of developmental and mental health conditions and outcomes in refugee children. Moreover, the review highlights the lack of disaggregated data on refugee-specific subgroups, such as gender, age, or ethnicity. For example, although several studies noted the vulnerability of ethnic minority girls to vitamin D deficiency, current measurement frameworks do not account for gender or ethnic disparities in bone health outcomes. Similarly, oral and vision health, which are critical components of child well-being, are rarely studied, and no standardized Canadian data exists for newly arrived refugee children.
4.3.2. Measurement Gaps and Methodological Limitations
A key limitation across studies was the inconsistent and often retrospective nature of data collection. Most studies relied on chart reviews, which introduced missing or incomplete data, particularly affecting pediatric-specific insights. The lack of prospective protocols and longitudinal follow-up limits our ability to assess the long-term health impacts of early conditions, especially for communicable diseases. For example, the absence of a formal Canadian screening and management program for latent tuberculosis infection (LTBI) has led to inconsistent practices across provinces, hindering data comparability and standardization on refugee-specific subgroups [79]. Similarly, while adequate measures exist for assessing non-communicable diseases such as growth and vitamin D levels, the lack of longitudinal, culturally contextualized data prevents meaningful monitoring of refugee children’s health over time. The exclusion of qualitative data further constrained the ability to assess nuanced contextual factors influencing treatment uptake and completion in this population.
This review revealed significant gaps in measuring developmental and mental health conditions and outcomes among refugee children. Many screening tools rely heavily on parent-reported data, which can be influenced by cultural norms, perceptions, and expectations, potentially affecting the accuracy and appropriateness of assessments [80,81]. Additionally, these cultural differences have implications for how developmental conditions and outcomes are recognized as well as how screening tools function across diverse populations - the measurement invariance of the tools. Tools such as the Parents' Evaluation of Developmental Status, which have been translated into other languages, for example, may suffer from measurement invariance, compromising their validity and reliability [82]. As a result, culturally nuanced developmental conditions or outcomes often go undetected. Language barriers and low health literacy further complicate the interpretation of developmental screening results, often leading to underdiagnosis or delayed identification of conditions. These challenges are compounded by the lack of comprehensive epidemiological data on developmental disabilities and delays among refugee children in Canada. Existing data are limited and based on small, non-representative samples, making it difficult to understand the true scope of need.
Mental health measurement was similarly fragmented. The lack of standardized Canadian screening protocols for mental health conditions and outcomes in newly arrived refugee children in Canada contributes to variability in diagnostic practices and potential underreporting. Our findings align with the findings of [32] on cross-cultural invalidity of screening and measurement tools and the lack of consensus on theoretical frameworks or constructs for measuring trauma and mental health, especially among young refugee children. Furthermore, most studies relied on symptom-based diagnoses during early resettlement, which can obscure chronic or trauma-related conditions. Moreover, the use of Western diagnostic frameworks is not able to fully capture culturally specific expressions of mental health. Few tools have been validated for use with immigrants, refugees, and asylum seekers. This finding is in line with the Canadian Collaboration for Immigrant and Refugee Health, for example, which recommends against routine Post-Traumatic Stress Disorder PTSD screening due to the potential for harm and lack of validated tools [73].
4.4. Implications for Practice, Research, and Policy
This scoping review offers novel insight into health measurement approaches for refugee-serving PHCs with implications for how research is conducted and how policies can guide healthcare. A key learning from this review is that current literature pays limited attention to social determinants of health, which significantly influence refugee child health outcomes. Despite evidence that refugee children and their families face compounded barriers, these are often underrepresented in existing data systems [83]. Their omission limits the ability to contextualize health conditions and outcomes within the lived realities of refugee families. To fully understand refugee child health conditions and outcomes, future research must adopt a system perspective that goes beyond biomedical indicators to include ecological factors at the micro, meso, and macro levels and how they interact to impact a child’s health outcomes [84,85,86,87]. This system perspective includes cultural preferences, family and community involvement, migration-specific experiences, and collaborative decision-making [84,88]. Furthermore, mixed-methods research that integrates both qualitative and quantitative data is essential to capture the complex interactions of the factors and to inform more equitable and contextually relevant health interventions.
4.4.1. Practice
The findings from the review pointing to evidence of many inconsistencies suggest the need to standardize and strengthen health measurement approaches in refugee-serving PHCs. Providers should adopt evidence-based tools such as the Rourke Baby Record and the Ages and Stages Questionnaire, which are evidence-based and already widely used in Canadian pediatric care. These tools provide a strong foundation for implementing consistent, age-appropriate, and culturally safe assessments for refugee children. To further improve diagnostic accuracy and support early intervention, the Canadian healthcare system should implement prospective data collection protocols. Standardized data practices would enhance the ability to improve the accuracy of diagnoses, to measure health outcomes, allocate resources effectively, and tailor services to the unique needs of refugee populations. By doing so, providers can deliver more equitable, responsive, and high-quality care to refugee children and their families.
4.4.2. Research
Future research should prioritize the development and validation of culturally and linguistically safe tools tailored to refugee populations. Future studies must employ longitudinal and mixed-method designs to measure how early health conditions and measurement variability affect long-term outcomes. To improve transparency and comparability, researchers should report age ranges, reference standards, and tool selection criteria. Additionally, integrating qualitative methods to capture the lived experiences, health behaviours, and care-seeking patterns of refugee families, insights that are essential for designing responsive and inclusive health systems.
4.4.3. Policy
The study findings revealed critical systemic gaps that hinder equitable health service delivery in Canada. Policymakers must address the systemic gaps by coordinating national efforts to standardize screening and assessment protocols, especially for developmental and mental health conditions. Current provincial inconsistencies in diagnostic criteria and data collection practices undermine care quality and equity. Federal leadership should coordinate developing and enforcing culturally appropriate measurement protocols and equip providers with the relevant training and resources needed for effective implementation. Strengthening the Canadian data systems to capture disaggregated, refugee-specific health conditions or outcomes will enable more targeted, evidence-based policy decisions and promote health equity across jurisdictions.
4.5. Limitations
The study has several limitations. First, the majority of included studies employed retrospective or cross-sectional designs, limiting our ability to draw causal inference or assess long-term health outcomes. Second, most studies relied on chart reviews and electronic medical records, which can be incomplete or inconsistently documented, particularly for pediatric-specific data. Third, the quality of the included studies was not formally assessed, which may affect the conclusions drawn. Additionally, the underrepresentation of qualitative studies limits understanding of contextual and cultural factors influencing health outcomes and care-seeking behaviours. There was also notable variability in measurement tools used across studies, compounded by the absence of standardized Canadian protocols for refugee child health measurement. Lastly, the strict focus on studies on health conditions and outcomes of refugee children aged from birth to 5 and the measurement of these conditions and outcomes limited the pool of available studies. Future research could focus on conducting longitudinal and mixed-methods studies to better understand the long-term impacts of resettlement on physical, mental, and developmental health
5. Conclusions
This review highlights the disproportionate focus on physical health, particularly non-communicable diseases, and reveals significant gaps and variability in measurement approaches for young refugee children. While the measurement challenges identified in this review are not unique to refugee children, their impact is more pronounced in this vulnerable population. The findings extend existing knowledge on gaps in the measurement of child health conditions and outcomes. It also reveals how systemic inconsistencies intersect with cultural and developmental complexities, shaping the health experiences of young refugee children in Canada. Addressing these gaps through coordinated clinical and policy efforts ensures all children, regardless of origin, receive accurate, timely, and equitable care in Canada.
Author Contributions
Conceptualization, A.B.; methodology, A.B and N.A.; validation, A.B., N.A., and R.G.; formal analysis, A.B. and N.A.; supervision, R.G., C.P., and S.Y.; project administration, A.B.; Visualization, A.B. and N.A.; writing—original draft preparation, A.B and N.A.; writing—review and editing, A.B., N.A., R.G., C.P., and S.Y.; All authors have read and agreed to the published version of the manuscript.
Funding
We are grateful to the Social Sciences and Humanities Research Council Partnership Grant (SSHRC), and the Stollery Children’s Hospital Foundation and the Alberta Women’s Health Foundation through the Women and Children’s Health Research Institute (WCHRI) through Dr Gokiert’s funding for supporting this research activities. We are also grateful to the Izaak Walton Killam Memorial Scholarship, administered by the University of Alberta and the WCHRI through a graduate studentship for the graduate funding to Augustine Botwe to support this research.
Institutional Review Board Statement
Note applicable
Informed Consent Statement
Not applicable.
Data Availability Statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Acknowledgments
We are grateful to Liz Dennett, a health science librarian at the Sperber Library, University of Alberta, for her assistance in refining our search strategy and searching the databases. We are also grateful for the feedback we received from Shelly Jun, Jessica Haight, Emma Monaghan, and Mary Honardar.
Conflicts of Interest
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Abbreviations
The following abbreviations are used in this manuscript:
| ADHD | Attention Deficit/Hyperactivity Disorder |
| ASD | Autism Spectrum Disorder |
| CDC | Centre for Disease Control |
| CINAHL | Cumulative Index to Nursing and Allied Health Literature |
| CMAJ | Canadian Medical Association Journal |
| DPTP | Diptheria/Pertussis/Tetanus/Polio |
| DXA | Dual Energy X-ray Absorptiometry |
| EIA | Enzyme Immunoassay |
| EMR | Electronic Medical Record |
| GARs | Government-Assisted Refugees |
| Hib | Haemophilys influenza B |
| ICD-10-CA | International Classification of Diseases and Related Health Problems, the 10th Revision, Canada |
| IGRA | Interferon-Gamma Release Assay |
| IgG | Immunoglobulin G |
| LTBI | Latent tuberculosis infections |
| NCHC | New Canadians Health Centre |
| PHCs | Primary Health Centres/Clinics |
| PICO | Patient, Intervention Comparison and Outcome |
| PRISMA-ScR | Preferred Reporting Items for Systematic Reviews and Meta-Analyses for Scoping Reviews |
| PSRs | Privately Sponsored Refugees |
| REC | Research and Evaluation Committee |
| WHO | World Health Organization |
Appendix
Appendix A.1
Box A1. Full Search String.
1 Refugees/ or (refugee* or asylum seeker* or asylee* or "displaced person*" or (claimant* and asylum)).mp.
2 (refugee clinic* or asylum clinic or refugee health program* or asylum health program*).mp. or Community Health Centers/ or Community Mental Health Services/ or Community health services/ or (community networks/ and ("health service*" or "health care" or healthcare or "primary care" or "migrant health" or "primary health*" or "public health").mp.) or (("community health" or "neighborhood health" or "primary health" or "primary care" or "public health" or "migrant health" or "refugee health" or "asylum seeker health" or "asylum health" or "claimant* health") adj3 (center* or centre* or clinic? or service* or network*)).mp. or ((health or healthcare) adj3 (center* or centre* or clinic? or service*)).mp. or (("community health" or "neighborhood health" or "primary health" or "primary care" or "public health") adj5 (refugee* or asylum seeker*)).mp.
3 Child/ or exp infant/ or exp pediatrics/ or (pediatric* or paediatric* or newborn* or congenital* or infan* or baby or babies or neonat* or pre-term or preterm* or premature birth* or child* or preschool* or pre-school* or kindergarten* or kindergarden* or nursery school* or ((day care* or daycare*) not adult*) or toddler* or boy or boys or girl* or grade-1* or grade-one* or m*-old* or 1-y*-old* or one-y*-old* or 2-y*-old* or two-y*-old* or 3-y*-old* or three-y*-old* or 4-y*-old* or four-y*-old* or 5-y*-old* or five-y*-old*).mp.
4 ("health status" or "nutritional status" or "vaccination status" or "immunization status" or "health screening" or "disease screening" or "Health outcome*" or "outcome measure*" or PROM or PROMs or "health needs" or "health concerns" or "health issues" or "health conditions" or "healthcare access" or "healthcare utilization" or (health* adj (need* or require*))).mp.
5 (malnutrition* or bone density* or health or "mental health" or anxiety or depress* or ptsd or trauma* or posttraumatic or post-trauma* or autis* or ADHD or "attention deficit" or "neurodevelpmental disorder*" or anemia or "iron deficienc*" or "vitamin deficienc*" or "infectious diseases" or "intestinal infection*" or "malaria" or parasite* or "upper respiratory infection*" or pneumonia or measles or mumps or rubella or "whooping cough" or hepatitis or polio* or diptheria or pertussis or varicella or tetanus or HIV or "HIV/AIDS" or tuberculosis or "human immunodeficiency virus" or obesity or overweight or underweight or wasting or "dental health" or "oral health" or "gum disease*" or "dental caries" or "blood elevated levels" or rickets or "stunt* growth").mp.
6 (Vitamin or iron or lead or calcium).mp.
7 ("Child development indicators" or ((child* or infant* or neonat* or toddler*) adj4 milestone)).mp.
8 4 or 5 or 6
9 1 and 2 and 3 and 8
10 (Canad* or British Columbia* or Alberta* or Saskatchewan or Manitoba* or Yukon or Northwest Territories or NWT or Nunavut or Ontario or Quebec* or Nova Scotia or Prince Edward Island or Newfoundland or Labrador or New Brunswick or Toronto or Vancouver or Montreal or Edmonton or Calgary or Winnipeg or Ottawa or Halifax).mp,in.
11 9 and 10
Appendix B.1

Table A1.
Summary of population characteristics of papers included in the review (n=25).
| Study ID | Study Aim | Study Design | Province | Population Age | Country/Region of Origin |
| Higgins 2023 | A systematic review which describes the extent, quality and cultural appropriateness of current research on the health conditions of refugee children aged 0-6 years settled in high-income countries | Systematic Review | Not Canadian specific, but includes papers in Canada | 0-6 | High income countries |
| Hoover 2017 | To identify the risk determinants of caries and record oral hygiene status in recent immigrant and refugee children | Cross sectional | Saskatchewan | Refugee children: 3-6 years; 6-14 years; 14-16 years Immigrant children: 3-6 years; 6-14 years; 14-16 years |
Indian subcontinent, Asia, and rest of the world |
| Lane 2019 | To characterize the health and nutritional status of immigrant and refugee children in Canada, specifically focusing on their bone mineral content and vitamin D status | Cross sectional; Mixed-methods research | Saskatchewan | 3-4 years; 5-7 years; 8-10 years; 11-13 years | Immigrants: Middle East (e.g., Iran, Iraq, Pakistan); Asia (e.g., Burma, India, Philippines); Africa; Latin America; Eastern Europe; Western Europe and United States Refugees: Middle East (e.g., Iran, Iraq, Pakistan); Asia (e.g., Burma, India, Philippines); Africa; Latin America; Eastern Europe |
| Bhayana 2018 | To provide a framework for primary care providers to approach developmental disabilities in both refugee and nonrefugee immigrant populations | Review | NA | NA | NA |
| BinYameen 2019 | To assess the ocular health status of Syrian pediatric refugees in Canada and report the prevalence of vision impairment within this population | Multi-methods Cross sectional study, | Ontario | <1 year; 1-3 years; 4-6 years; 7-9; 10-12; 13-15; 15-18 | Syria |
| Guttmann 2020 | To evaluate factors associated with uptake of a financial incentive for developmental screening at an enhanced 18-month well-child visit (EWCV) in Ontario, Canada. | Cross sectional study; Retrospective chart review | Ontario | 17-24 months. | Not specified |
| Suppiah 2023 | To assess growth indicators for resettled Yazidi and non-Yazidi pediatric refugees from Syria and Iraq. | Retrospective chart review cohort study | Alberta | < 5 years and 5 years or older | Iraq and Syria |
| Gagnon 2013 | To determine whether refugee or asylum-seeking women or their infants experience a greater number or a different distribution of professionally identified health concerns after birth than immigrant or Canadian-born women. | Quantitative research; Longitudinal (cohort study), Retrospective study | Ontario and Quebec | Infants | Refugees: Africa; Asia; Europe; Latin America Asylum-Seekers: Africa; Asia; Europe; Latin America Immigrants Africa; Asia; Europe; Latin America; Northern America |
| Aucoin 2013 | To determine the 25-hydroxyvitamin D (25[OH]D) serum levels in refugee women of childbearing age and in refugee children; to compare their 25(OH)D levels with the recommended levels in order to determine the prevalence of deficiency; to compare their 25(OH)D levels with those in the general Canadian population in the appropriate age and sex groups; and to investigate the association of vitamin D deficiency with potential risk factors | Cross sectional study; Retrospective chart review | Alberta | 0-5 years; 6-11 years; 12-19 years; 20-39 years; 40-45 years | Africa; Asia; Middle East; South America; Other |
| Dorman 2017 | Characterize the demographics and health status of North Korean refugees who have accessed care at a refugee clinic in Toronto | Retrospective chart review; cross sectional, Other: Community Based Participatory Research (CBPR) methodology | Ontario | All | North Korea; Swaziland; Saudi Arabia; Croatia; Iran; Afghanistan; Eritrea; Ethiopia; Nigeria; North Korea; Hungary; Other |
| DeVetten 2017 | To determine the prevalence of intestinal parasites and rates of stool testing compliance, as well as associated patient characteristics | Retrospective chart review, cross sectional | Alberta | < 6 years; 6-18 years; 19-39 years and 40 years | Sub-Saharan Africa; North Africa; Middle East; Asia; Latin America; Europe or North America |
| Taseen 2017 | To determine the level of serum 25-hydroxyvitamin D (25-(OH) D) in the paediatric refugee population residing in Sherbrooke, Quebec, Canada and to determine variables predicting vitamin D levels including age, sex, BMI, influence of season, ethnicity, previous country of residence and duration of stay in Canada from time of arrival. | Cross sectional study; Retrospective chart review | Quebec | <3 years; 3 - <6 years; 6 - <12 years; 12 years | Afghanistan; Iraq; Bhutan, Columbia, Guatemala; and Central African Republic |
| Darwish 2020 | To describe the population of Syrian refugees who received care at temporary triage clinics, the health issues addressed, and the health services used in the clinics | Non-randomized experimental study; Cross sectional study; Retrospective chart review | Ontario | 1 month - 62 years (55% children) | Syria |
| Muller 2022 | This study aims to investigate the prevalence and species of intestinal parasites identified in stool ova and parasite (O&P) specimens in a sample of newly arrived refugees in Toronto, Canada. | Retrospective chart review, cross sectional | Ontario | 0-9 years; 10-19 year; 20-29 years; 30-39 years; 40-49 year; 50-59 years; 60-69 years; 70+ | East Asia & Pacific; Europe & Central Asia; Latin America & Caribbean; Middle East & North Africa; North America; South Asia; and Sub-Saharan Africa |
| Harwood-Johnson 2023 | To measure LTBI treatment acceptance and completion outcomes of LTBI treatment at the REACH clinic in Saskatoon | Retrospective chart review, cross sectional | Saskatchewan | 6 months or older | Africa; Eastern Europe, Mediterranean; Southeast Asia |
| Kamali 2023 | To examine differences in mental health-related service contacts between immigrant, refugee, racial and ethnic minoritized children and youth, and the extent to which social, and economic characteristics account for group differences | Other: Retrospective correlational analysts (cross sectional) | Ontario | 4 - 17 yrs | NA |
| Smati 2024 | To conduct a detailed retrospective cohort investigation of the sociodemographic characteristics, health conditions, and clinic utilization patterns of Afghan refugee patients resettled in Calgary, Canada between 2011 and 2020 | Retrospective chart review; Other: community-engaged | Alberta | 0-4 years; 5-11 years; 12-17 years | Afghanistan |
| Redditt 2015b | To determine the prevalence of selected chronic diseases among newly arrived refugee patients and explore associations with key demographic factors | Retrospective chart review, cross-sectional | Ontario | 0-4 years; 5-14 years; 15-24 years; 25-34 years; 35-44 years; 45-54 years; 55-64 years; 65+ years | Africa; Americas; Asia; Eastern Mediterranean; Europe; North America |
| Redditt 2015 | To determine the prevalence of selected infectious diseases among newly arrived refugee patients and whether there is variation by key demographic factors | Retrospective chart review, cross-sectional | Ontario | 0-4 years; 5-14 years; 15-24 years; 25-34 years; 35-44 years; 45-54 years; 55-64 years; 65+ years | Africa; Americas; Asia; Eastern Mediterranean; Europe |
| Gadermann 2022 | Estimate the administrative data-derived diagnostic prevalence of mental disorders (conduct, attention-deficit/hyperactivity disorder [ADHD], and mood/anxiety) for refugee, immigrant, and nonimmigrant children and youth in British Columbia, Canada. | Retrospective chart review, cross sectional | British Columbia | 0-19 years | NA |
| Salehi 2015 | To describe selected anthropometric and health status variables among immigrant and refugee children ≤6 years of age within an inner-city clinic in Toronto, Ontario | Cross sectional; Retrospective chart review | Ontario | 0-6 years | Afghanistan; Myanmar; and Columbia |
| Guttmann 2008 | To investigate access to effective primary health care services in children of new immigrants to Canada by assessing immunization coverage at age 2 | Longitudinal (Cohort study) | Ontario | 17-24 months | Latin/Central America, Western Europe, North America; Eastern Europe; Middle East; Africa; Southeast and Northeast Asia, Oceania; South Asia |
| Beukeboom 2018 | To examine the variation among ethnic populations in the prevalence of anemia, vitamin D and B12 deficiencies among refugee children. The study aims to determine the frequency and distribution of these deficiencies among refugee children, stratified by country of origin and age group |
Cross sectional study; Retrospective chart review | Ontario | 0-4 year; 5-11 years; 12-16 years | Iraq; Somalia; Myanmar; Afghanistan; Other |
| Lane 2018 | Explore the health and nutritional status of immigrant and refugee children in Canada, identifying chronic disease risks and health inequities influenced by socioeconomic and lifestyle factors, to inform public health interventions for newcomer families. | Retrospective, Cross sectional study; Mixed-methods research | 3-13 years | ||
| Moreau 2019 | To assess the oral health status of refugee children in comparison with that of Canadian children and investigate the extent to which demographic factors are associated with caries experience in this population | Retrospective chart review | Quebec | 1-14 years | Africa; Latin America; North America; Middle East; Europe; and Asia |
Appendix B.2
Table A2.
Summary of papers included in review (n=25).
| Study ID | Outcomes | Measurement Approach Defined | ||
| Communicable | Non- communicable | Developmental and mental health | ||
| Higgins 2023 | X | X | X | NA |
| Hoover 2017 | X | Clinical Examinations - Assessment of the presence of the number of decayed, missing and filled teeth (dmft/DMFT). Oral hygiene status evaluated by Simplified Oral Hygiene Index (OHIS). | ||
| Lane 2019 | X | Physical exam: Dual energy X-ray absorptiometry (DXA). Blood sample for serum vitamin D analysis. Questionnaire: Modified version of the Canadian Community Health Survey (CCHS) 2008 socio-economic and demographic questionnaire, the CCHS Food security Questionnaire, Statistics Canada's Children's Physical Activity questionnaire, and serial 24 h dietary recalls. |
||
| Bhayana 2018 | X | NA | ||
| BinYameen 2019 | X | Visual screening, slit-lamp examination, direct dilated fundoscopy, and refractive index measurements. | ||
| Guttmann 2020 | X | Immunization Rates (Categorized as 85%, 90%, or >95% complete immunizations) and birth weight | ||
| Suppiah 2023 | X | Height and Weight | ||
| Gagnon 2013 | X | X | Project nurse assessment post-birth, 7-10 days and four months. Assessed for the presence of health concerns based on a list developed from standards for postpartum care. Nipissing Assessment Tool Vitamin D supplements Infant weight |
|
| Aucoin 2013 | X | Laboratory measurement using the standard DiaSorin Liaison 25(OH)D vitamin D assay. | ||
| Dorman 2017 | X | X | Glucose (fasting blood sugar, random blood sugar, and hemoglobin A1c), hepatitis B serology (surface antigen, surface antibody, core antibody), BMI | |
| DeVetten 2017 | X | Stool ova and parasite test - All specimens were first screened for Giardia lamblia and Cyptospokidium using an enzyme immunoassay, then positives were confirmed with direct fluorescent antibody testing. | ||
| Taseen 2017 | X | Laboratory measurements of 25-(OH)D levels determined by Elecsys Vitamin D Total Assay. | ||
| Darwish 2020 | X | X | X | NA |
| Muller 2022 | X | X | BMI, WHO Anemia guidelines, height, weight | |
| Harwood-Johnson 2023 | X | QuantiFERON-TB Gold Plus 4-tube assay (IGRA) and Mantoux method (TST) | ||
| Kamali 2023 | X | Questionnaire tool: 2014 Ontario Child Health Study (OCHS) | ||
| Smati 2024 | X | X | X | Based on the ICD-10 |
| Redditt 2015b | X | Hemoglobin Levels and diabetes screening test results (fasting blood glucose, random blood glucose, or hemoglobin A1c [HbA1c] measurement) |
||
| Redditt 2015 | X | HIV serology, hepatitis B serology (surface antigen and surface antibody), hepatitis C antibody, Strongyloides serology, Schistosoma serology, stool ova and parasites, gonorrhea and chlamydia testing (culture or nucleic acid amplification test), syphilis testing, and varicella immune status (varicella immunoglobulin G antibody) | ||
| Gadermann 2022 | X | Identified Indicators using symptoms |
||
| Salehi 2015 | X | X | Height and weight abnormalities, determined by the WHO Child Growth Standards (using a cut-off z-score of ≤−2, which indicates a percentile measurement of approximately ≤2.3). Data were also collected regarding the presence of: iron deficiency (defined as ferritin levels below the age-specific laboratory lower reference limits); anemia (defined as hemoglobin levels below the age-specific laboratory lower reference limits); parasitic enteric infections (positive stool culture for ova and parasites); hepatitis B (positive hepatitis B surface antigen levels); HIV (positive ELISA test); and elevated lead levels (lead levels ≥ 0.48 μmol/L). |
|
| Guttmann 2008 | X | Five immunizations given after age 7 weeks as being up to date, representing the recommended 3doses and 1booster of Diptheria/Pertussis/Tetanus/Polio/ Haemophilys influenza B (DPTP/Hib) given at 2, 4, 6, and 18 months, and 1 combined dose of measles, mumps, and rubella given after age 12 months. |
||
| Beukeboom 2018 | X | "Hemoglobin Levels: Hemoglobin levels were measured to evaluate anemia among refugee children. The cut-off levels for anemia were based on age and sex-specific guidelines from the World Health Organization (WHO). Vitamin D Levels: Serum 25(OH)D levels were measured to assess vitamin D status. Vitamin D is crucial for bone health, immune function, and overall physical development. Vitamin B12 Levels: Serum vitamin B12 levels were measured to determine the prevalence of vitamin B12" |
||
| Lane 2018 | X | Physical exam: Dual energy X-ray absorptiometry (DXA). Blood sample for serum vitamin D analysis. Questionnaire: Modified version of the Canadian Community Health Survey (CCHS) 2008 socio-economic and demographic questionnaire, the CCHS Food security Questionnaire, Statistics Canada's Children's Physical Activity questionnaire, and serial 24h dietary recalls. Blood sample to assess serum glucose, total cholesterol, and serum vitamin D. Anthropometric measurements including height, weight, and waist circumference |
||
| Moreau 2019 | X | Dental caries diagnosis (dmft/DMFT) for primary and permanent teeth. Oral hygiene was scored using the simplified oral hygiene index. Gingival health status was measured visually without probing. Patients' malocclusion assessment looked at crossbite, open bite, overbite, and overjet. | ||
References
- UNHCR. (2025). Global trends: Forced displacement in 2024. United Nations High Commissioner for Refugees. https://www.unhcr.org/global-trends-report-2024. (accessed on 9 April 2025).
- Concern Worldwide. (2025). The global refugee crisis, explained. Concern Worldwide. https://www.concern.net/news/global-refugee-crisis-explained. (accessed on 12 June 2025).
- IRCC. (2024). 2024 annual report to Parliament on immigration. https://www.canada.ca/content/dam/ircc/documents/pdf/english/corporate/publications-manuals/annual-report-2024-en.pdf. (accessed on 12 August 2025).
- Dowell, A., & Turner, N. Child health indicators: From theoretical frameworks to practical reality? The British Journal of General Practice, 2014, 64(629), 608–609. [CrossRef]
- Khan, I., & Leventhal, B. L. Developmental Delay. In StatPearls. StatPearls Publishing., 2023. http://www.ncbi.nlm.nih.gov/books/NBK562231/.
- Kirmayer, L., & Jarvis, G. Culturally Responsive Services as a Path to Equity in Mental Healthcare. HealthcarePapers, 2019, 18(2), 11–23. [CrossRef]
- Sim, A., Ahmad, A., Hammad, L., Shalaby, Y., & Georgiades, K. Reimagining mental health care for newcomer children and families: A qualitative framework analysis of service provider perspectives. BMC Health Services Research, 2023, 23(1), 699. [CrossRef]
- Eruyar, S., Huemer, J., & Vostanis, P. Review: How should child mental health services respond to the refugee crisis? Child and Adolescent Mental Health, 2018. 23(4), 303–312. [CrossRef]
- Hong, J., Ruacho, H. C., Zeng, X., & Franklin, C. A Scoping Review of Family-Based Interventions for Immigrant/Refugee Children: Exploring Intergenerational Trauma. Community Mental Health Journal 2025. [CrossRef]
- Mahon, D. A Scoping Review of Interventions Delivered by Peers to Support the Resettlement Process of Refugees and Asylum Seekers. Trauma Care 2022, 2(1), Article 1. [CrossRef]
- Baauw, A., Kist-van Holthe, J., Slattery, B., Heymans, M., Chinapaw, M., & Van Goudoever, H. Health needs of refugee children identified on arrival in reception countries: A systematic review and meta-analysis. BMJ Paediatrics Open, 2019a, 3(1), e000516. [CrossRef]
- Frounfelker, R. L., Miconi, D., Farrar, J., Brooks, M. A., Rousseau, C., & Betancourt, T. S. Mental Health of Refugee Children and Youth: Epidemiology, Interventions, and Future Directions. Annual Review of Public Health, 41 2020, 159–176. [CrossRef]
- Gibson, J., & Evennett, J. The health needs of asylum-seeking children. The British Journal of General Practice, 2018, 68(670), 238. [CrossRef]
- Horne, M. Identifying the Health Needs of Communities and Populations. In Public Health and Society 2003, pp. 119–132). Palgrave, London. [CrossRef]
- WHO. (2021, October 21). Common health needs of refugees and migrants: Literature review. https://www.who.int/publications/i/item/9789240033108. (accessed on 12 July 2025).
- Refugee Health Coalition . (2020). Refugee health community engagement: Project report. Available online at: https://www.refugeehealthcoalition.ca/_files/ugd/fda787_0f3b634eff7c42d29ca35dcb57c9cff7.pdf. (accessed on 12 May 2025).
- Salami, B., Olukotun, M., Vastani, M., Amodu, O., Tetreault, B., Obegu, P. O., Plaquin, J., & Sanni, O. Immigrant child health in Canada: A scoping review. BMJ Global Health, 2022, 7(4). [CrossRef]
- Scharf, R. J., Zheng, C., Briscoe Abath, C., & Martin-Herz, S. P. Developmental Concerns in Children Coming to the United States as Refugees. Pediatrics, 2021, 147(6), e2020030130. [CrossRef]
- Gold, A. W., Perplies, C., Biddle, L., & Bozorgmehr, K. Primary healthcare models for refugees involving nurses: A systematic review and narrative synthesis. BMJ Global Health, 2025, 10(3), e018105. [CrossRef]
- Haight, J., Kruth, M., Gokiert, R., Botwe, A., Dzunic-Wachilonga, A., Neves, C., Velasquez, A., Whalen-Browne, M., Ladha, T., & Rogers, C. A principles-based community health center for addressing refugee health: The New Canadians Health Centre. Frontiers in Public Health, 2024, 12. [CrossRef]
- Marmot, M., Allen, J., Bell, R., Bloomer, E., & Goldblatt, P. WHO European review of social determinants of health and the health divide. The Lancet, 2012, 380(9846), 1011–1029. [CrossRef]
- Matlin, S. A., Depoux, A., Schütte, S., Flahault, A., & Saso, L. Migrants’ and refugees’ health: Towards an agenda of solutions. Public Health Reviews, 2018, 39(1), 27. [CrossRef]
- Pottie, K., Hui, C., Rahman, P., Ingleby, D., Akl, E. A., Russell, G., Ling, L., Wickramage, K., Mosca, D., & Brindis, C. D. Building Responsive Health Systems to Help Communities Affected by Migration: An International Delphi Consensus. International Journal of Environmental Research and Public Health, 2017, 14(2), 144. [CrossRef]
- World Health Organization. Regional Office for Europe. (2018). The life-course approach: from theory to practice: case stories from two small countries in Europe. World Health Organization. Regional Office for Europe. https://iris.who.int/handle/10665/342210. (accessed on 12 June 2025).
- WHO. (2018b). The life-course approach: From theory to practice. Case stories from two small countries in Europe. World Health Organization. Regional Office for Europe. https://iris.who.int/handle/10665/342210. (accessed on 12 June 2025).
- Australian Institute of Health and Welfare. (2023, July 7). Cultural safety in health care for Indigenous Australians: Monitoring framework, Summary. Australian Institute of Health and Welfare. https://www.aihw.gov.au/reports/indigenous-australians/cultural-safety-health-care-framework/contents/summary. (accessed on 12 July 2025).
- Baba, L. Cultural Safety in First Nations, Inuit and Métis Public Health. 2013.
- Browne, A. J., Varcoe, C., Ford-Gilboe, M., Nadine Wathen, C., Smye, V., Jackson, B. E., Wallace, B., Pauly, B. (Bernie), Herbert, C. P., Lavoie, J. G., Wong, S. T., & Blanchet Garneau, A. Disruption as opportunity: Impacts of an organizational health equity intervention in primary care clinics. International Journal for Equity in Health, 2018, 17(1), 154. [CrossRef]
- Curtis, E., Jones, R., Tipene-Leach, D., Walker, C., Loring, B., Paine, S.-J., & Reid, P. Why cultural safety rather than cultural competency is required to achieve health equity: A literature review and recommended definition. International Journal for Equity in Health, 2019, 18(1), 174. [CrossRef]
- Schäfer, I., Oltrogge, J. H., Pruskil, S., Mews, C., Schlichting, D., Jahnke, M., Wagner, H.-O., Lühmann, D., & Scherer, M. Referrals to secondary care in an outpatient primary care walk-in clinic for refugees in Germany: Results from a secondary data analysis based on electronic medical records. BMJ Open, 2020, 10(10), e035625. [CrossRef]
- Klas, J., Grzywacz, A., Kulszo, K., Grunwald, A., Kluz, N., Makaryczew, M., & Samardakiewicz, M. Challenges in the Medical and Psychosocial Care of the Paediatric Refugee-A Systematic Review. International Journal of Environmental Research and Public Health, 2022, 19(17), 10656. [CrossRef]
- Gadeberg, A. K., Montgomery, E., Frederiksen, H. W., & Norredam, M. Assessing trauma and mental health in refugee children and youth: A systematic review of validated screening and measurement tools. European Journal of Public Health, 2017, 27(3), 439–446. [CrossRef]
- Gervais, C., Daoust-Zidane, N., Thomson-Sweeny, J., Campeau, M., & Côté, I. Safety at the Heart of Well-Being of Migrant-Background Children in Canada. Child Indicators Research, 2025. [CrossRef]
- Prior, A., Vestergaard, C. H., Vedsted, P., Smith, S. M., Virgilsen, L. F., Rasmussen, L. A., & Fenger-Grøn, M. Healthcare fragmentation, multimorbidity, potentially inappropriate medication, and mortality: A Danish nationwide cohort study. BMC Medicine, 2023, 21(1), 305. [CrossRef]
- Higgins, C., Gartland, D., Yelland, J., Brown, S., Szwarc, J., Kaplan, I., Paxton, G., & Riggs, E. Refugee child health: A systematic review of health conditions in children aged 0–6 years living in high-income countries. Global Health Promotion, 2023, 30(4), 45–55. [CrossRef]
- Peters, M. D. J., Marnie, C., Tricco, A. C., Pollock, D., Munn, Z., Alexander, L., McInerney, P., Godfrey, C. M., & Khalil, H. Updated methodological guidance for the conduct of scoping reviews. JBI Evidence Synthesis, 2020, 18(10), 2119–2126. [CrossRef]
- Peters, M. D. J., Marnie, C., Colquhoun, H., Garritty, C. M., Hempel, S., Horsley, T., Langlois, E. V., Lillie, E., O’Brien, K. K., Tunçalp, Ӧzge, Wilson, M. G., Zarin, W., & Tricco, A. C. Scoping reviews: Reinforcing and advancing the methodology and application. Systematic Reviews, 2021, 10(1), 263. [CrossRef]
- Wallerstein, N., & Duran, B. Community-Based Participatory Research Contributions to Intervention Research: The Intersection of Science and Practice to Improve Health Equity. American Journal of Public Health, 2010, 100(Suppl 1), S40–S46. [CrossRef]
- Minkler, M., & Wallerstein, N. Community-based participatory research for health: From process to outcomes (2nd ed.). Jossey-Bass. 2008.
- Schardt C, Adams MB, Owens T, Keitz S, Fontelo P. Utilization of the PICO framework to improve searching PubMed for clinical questions. BMC Med Inform Decis Mak. 2007;7:16. Published 2007 Jun 15. [CrossRef]
- Covidence systematic review software, (2025). Veritas Health Innovation, Melbourne, Australia. Available at www.covidence.org. (accessed on 10 February 2025).
- World Health Organization. Country groupings [Internet]. Geneva: WHO. Available from: https://www.who.int/observatories/global-observatory-on-health-research-and-development/classifications-and-standards/country-groupings. [accessed June 17 2025].
- Hoover, Jay et al. “Risk Determinants of Dental Caries and Oral Hygiene Status in 3-15 Year-Old Recent Immigrant and Refugee Children in Saskatchewan, Canada: A Pilot Study.” Journal of immigrant and minority health 2017, vol. 19,6: 1315-1321. [CrossRef]
- Lane, Ginny et al. “Canadian newcomer children's bone health and vitamin D status.” Applied physiology, nutrition, and metabolism = Physiologie appliquee, nutrition et metabolisme 2019, vol. 44,7: 796-803. [CrossRef]
- Bhayana A, Bhayana B. Approach to developmental disabilities in newcomer families. Can Fam Physician. 2018, 64(8):567-573.
- Bin Yameen, Tarek Abdullah et al. “Visual impairment and unmet eye care needs among a Syrian pediatric refugee population in a Canadian city.” Canadian journal of ophthalmology. Journal canadien d'ophtalmologie 2019, vol. 54,6: 668-673. [CrossRef]
- Guttmann, Astrid et al. “Implementation of a Physician Incentive Program for 18-Month Developmental Screening in Ontario, Canada.” The Journal of pediatrics 2020, vol. 226: 213-220.e1. [CrossRef]
- Suppiah, Roopa et al. “Stunting and Overweight Prevalence Among Resettled Yazidi, Syrian, and Iraqi Pediatric Refugees.” JAMA pediatrics 2023, vol. 177,2: 203-204. [CrossRef]
- Gagnon AJ, Dougherty G, Wahoush O, et al. International migration to Canada: the post-birth health of mothers and infants by immigration class. Soc Sci Med. 2013, 76(1):197-207. [CrossRef]
- Aucoin, Michael et al. “Vitamin D status of refugees arriving in Canada: findings from the Calgary Refugee Health Program.” Canadian family physician Medecin de famille canadien 2013, vol. 59,4: e188-94.
- Dorman, Katie et al. “Health Status of North Korean Refugees in Toronto: A Community Based Participatory Research Study.” Journal of immigrant and minority health 2017, vol. 19,1: 15-23. [CrossRef]
- DeVetten G, Dirksen M, Weaver R, et al. Parasitic stool testing in newly arrived refugees in Calgary, Alta. CFP 2017, 63:e518–e525.
- Taseen K, Beaulieu G. Vitamin D levels and influencing predictors in refugee children in Sherbrooke (Quebec), Canada. J Paediatr Child Health 2017; 22:307–311. [CrossRef]
- Darwish, Wais. and Laura Muldoon. “Acute primary health care needs of Syrian refugees immediately after arrival to Canada” Canadian Family Physician 2020, vol. 66,1: e30–e38.
- Müller, Frank et al. “Intestinal parasites in stool testing among refugees at a primary care clinic in Toronto, Canada.” BMC infectious diseases 2022, vol. 22,1 249. [CrossRef]
- Harwood-Johnson, Emily et al. “Community treatment of latent tuberculosis in child and adult refugee populations: outcomes and successes.” Frontiers in public health 2023, vol. 11 1225217. [CrossRef]
- Kamali, Mahdis et al. “Social Disparities in Mental Health Service Use Among Children and Youth in Ontario: Evidence From a General, Population-Based Survey.” Canadian journal of psychiatry. Revue canadienne de psychiatrie 2023, vol. 68,8: 596-604. [CrossRef]
- Smati, Hannah & Hassan, Nour & Essar, Mohammad & Abdaly, Fawzia & Noori, Shayesta & Grewal, Rabina & Norrie, Eric & Talavlikar, Rachel & Bietz, Julia & Kimball, Sarah & Coakley, Coakley & Chatterjee, Avik & Fabreau, Gabriel. Health status and care utilization among Afghan refugees newly resettled in Calgary, Canada between 2011-2020. 2024. 10.1101/2024.06.21.24309182.
- Reddit V, Granziano D, Janakiram P, et al. Health status of newly arrived refugees in Toronto, Ont: Part 2: chronic diseases: CFP 2015; 61:e310-e315.
- Redditt V, Janakiram P, Graziano D, et al. Health status of newly arrived refugees in Toronto, Ont: Part 1: infectious diseases. CFP 2015; 61:e303–e309.
- Gadermann, Anne M et al. “Prevalence of Mental Health Disorders Among Immigrant, Refugee, and Nonimmigrant Children and Youth in British Columbia, Canada.” JAMA network open 2022, vol. 5,2 e2144934. [CrossRef]
- Salehi L, Lofters AK, Hoffmann SM, Polsky JY, Rouleau KD. Health and growth status of immigrant and refugee children in Toronto, Ontario: a retrospective chart review. Paediatrics & child health. 2015, 20(8):e38-42. [CrossRef]
- Guttmann, Astrid et al. “Immunization coverage among young children of urban immigrant mothers: findings from a universal health care system.” Ambulatory pediatrics : the official journal of the Ambulatory Pediatric Association 2008, vol. 8,3: 205-9. [CrossRef]
- Beukeboom C, Arya N. Prevalence of Nutritional Deficiencies Among Populations of Newly Arriving Government Assisted Refugee Children to Kitchener/Waterloo, Ontario, Canada. J Immigr Minor Health 2018, 20:1317–1323. [CrossRef]
- Lane, Ginny et al. “Chronic health disparities among refugee and immigrant children in Canada.” Applied physiology, nutrition, and metabolism = Physiologie appliquee, nutrition et metabolisme 2018, vol. 43,10: 1043-1058. [CrossRef]
- Moreau, Anne-Marie et al. “Oral Health Status of Refugee Children in Montreal.” Journal of immigrant and minority health 2019, vol. 21,4: 693-698. [CrossRef]
- Lavanchy D, Kane M. Global epidemiology of hepatitis B virus infection. In Hepatitis B virus in human diseases 2016 (pp. 187-203). Cham: Springer International Publishing.
- Xiao, W., Zhao, J., Chen, Y., Liu, X., Xu, C., Zhang, J., Qian, Y., & Xia, Q. Global burden and trends of acute viral hepatitis among children and adolescents from 1990 to 2019: A systematic analysis of the Global Burden of Disease Study 2019. Hepatology International, 2024, 18(3), 917–928. [CrossRef]
- Baauw, A., Kist-van Holthe, J., Slattery, B., Heymans, M., Chinapaw, M., & Van Goudoever, H. Health needs of refugee children identified on arrival in reception countries: A systematic review and meta-analysis. BMJ Paediatrics Open, 2019b, 3(1), e000516. [CrossRef]
- Carpenter, K.L.H, Sprechmann, P., Calderbank, R., Sapiro G, Egger H. L. Quantifying Risk for Anxiety Disorders in Preschool Children: A Machine Learning Approach. PLOS ONE 2016, 11(11): e0165524. [CrossRef]
- Wichstrøm L, Belsky J, Berg-Nielsen TS. Preschool predictors of childhood anxiety disorders: a prospective community study. J Child Psychol Psychiatry. 2013, 54(12):1327-1336. [CrossRef]
- Centre for Addiction and Mental Health. Evidence snapshots [Internet]. Toronto (ON): CAMH. Available from: https://www.camh.ca/en/professionals/professionals--projects/immigrant-and-refugee-mental-health-project/newsletter/evidence-snapshots. (accessed 2024 Jun 22).
- Pottie, K., Greenaway, C., Feightner, J., Welch, V., Swinkels, H., Rashid, M., Narasiah, L., Kirmayer, L. J., Ueffing, E., MacDonald, N. E., Hassan, G., McNally, M., Khan, K., Buhrmann, R., Dunn, S., Dominic, A., McCarthy, A. E., Gagnon, A. J., Rousseau, C., … Health, coauthors of the C. C. for I. and R. Evidence-based clinical guidelines for immigrants and refugees. CMAJ, 2011, 183(12), E824–E925. [CrossRef]
- Public Health Ontario. (n.d.). Parasite – Faeces. https://www.publichealthontario.ca/en/laboratory-services/test-information-index/parasite-faeces. (accessed on 15 July 2025).
- Alberta Precision Laboratories. (n.d.). Ova and parasite exam (O&P). https://www.albertahealthservices.ca/webapps/labservices/indexAPL.asp?id=8538&tests=&zoneid=1&details=true. (accessed on 15 July 2025).
- Herrick JA, Nordstrom M, Maloney P, Rodriguez M, Naceanceno K, Gallo G, Mejia R, Hershow R. Parasitic infections represent a significant health threat among recent immigrants in Chicago. Parasitology research. 2020, Mar;119(3):1139-48.
- International Society for Clinical Densitometry. 2019 ISCD official positions – Pediatric. 2019. https://www.iscd.org.
- Bernhardt, K., Le Beherec, S., Uppendahl, J., Baur, M.-A., Klosinski, M., Mall, V., & Hahnefeld, A. Exploring Mental Health and Development in Refugee Children Through Systematic Play Assessment. Child Psychiatry & Human Development, 2025, 56(3), 629–639. [CrossRef]
- Sterling, T. R., Bethel, J., Goldberg, S., Weinfurter, P., Yun, L., & Horsburgh, C. R. The Scope and Impact of Treatment of Latent Tuberculosis Infection in the United States and Canada. American Journal of Respiratory and Critical Care Medicine, 2006, 173(8), 927–931. [CrossRef]
- King, J. S. H., Low, P. S., Chan, Y. H., & Neihart, M. Interpreting Parents’ Concerns About Their Children’s Development with the Parents Evaluation of Developmental Status: Culture Matters. Journal of Developmental & Behavioral Pediatrics, 2012, 33(2), 179. [CrossRef]
- Kroening, A. L. H., Moore, J. A., Welch, T. R., Halterman, J. S., & Hyman, S. L. Developmental Screening of Refugees: A Qualitative Study. Pediatrics, 2016, 138(3), e20160234. [CrossRef]
- Zhu, Z., Jiao, D., Li, X., Zhu, Y., Kim, C., Ajmal, A., Matsumoto, M., Tanaka, E., Tomisaki, E., Watanabe, T., Sawada, Y., & Anme, T. Measurement invariance and country difference in children’s social skills development: Evidence from Japanese and Chinese samples. Current Psychology, 2023, 42(24), 20385–20396. [CrossRef]
- McKenzie K, Ashraf A, Tuck A, di Tomasso L, Thompson L, Varga B. (2019). Immigrant, refugee, ethnocultural and racialized populations and the social determinants of health: A review of 2016 census data. Toronto: Centre for Addiction and Mental Health. Available from: https://www.camh.ca/en/professionals/professionals--projects/immigrant-and-refugee-mental-health-project/newsletter/evidence-snapshots/es-nov-2019---immigrant-refugee-ethnocultural-and-racialized-populations. (accessed on 10 June 2025).
- de Freitas Girardi, J., Miconi, D., Lyke, C., & Rousseau, C. Creative expression workshops as Psychological First Aid (PFA) for asylum-seeking children: An exploratory study in temporary shelters in Montreal. Clinical Child Psychology and Psychiatry, 2020, 25(2), 483–493. [CrossRef]
- McDonald, J. T., & Kennedy, S. Insights into the ‘healthy immigrant effect’: Health status and health service use of immigrants to Canada. Social Science & Medicine, 2004, 59(8), 1613–1627. [CrossRef]
- Morteza H, Boleyn T. Health ecology: health, culture and human-environment interactions. Routledge London, New York. 1999.
- von Schirnding, Y. Health ecology. Health, culture and human-environment interaction. Bulletin of the World Health Organization, 2000, 78(2), 276–276.
- Berman H, Mulcahy G, Forchuk C, et al. Uprooted and displaced: a critical narrative study of homeless, Aboriginal, and newcomer girls in Canada. Issues Ment. Health Nurs 2009, 30:418–430. [CrossRef]
- Tricco, A. C., Lillie, E., Zarin, W., O’Brien, K. K., Colquhoun, H., Levac, D., Moher, D., Peters, M. D. J., Horsley, T., Weeks, L., Hempel, S., Akl, E. A., Chang, C., McGowan, J., Stewart, L., Hartling, L., Aldcroft, A., Wilson, M. G., Garritty, C., … Straus, S. E. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Annals of Internal Medicine, 2018, 169(7), 467–473. [CrossRef]
Figure 1.
Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) Flow Diagram.
Figure 1.
Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) Flow Diagram.
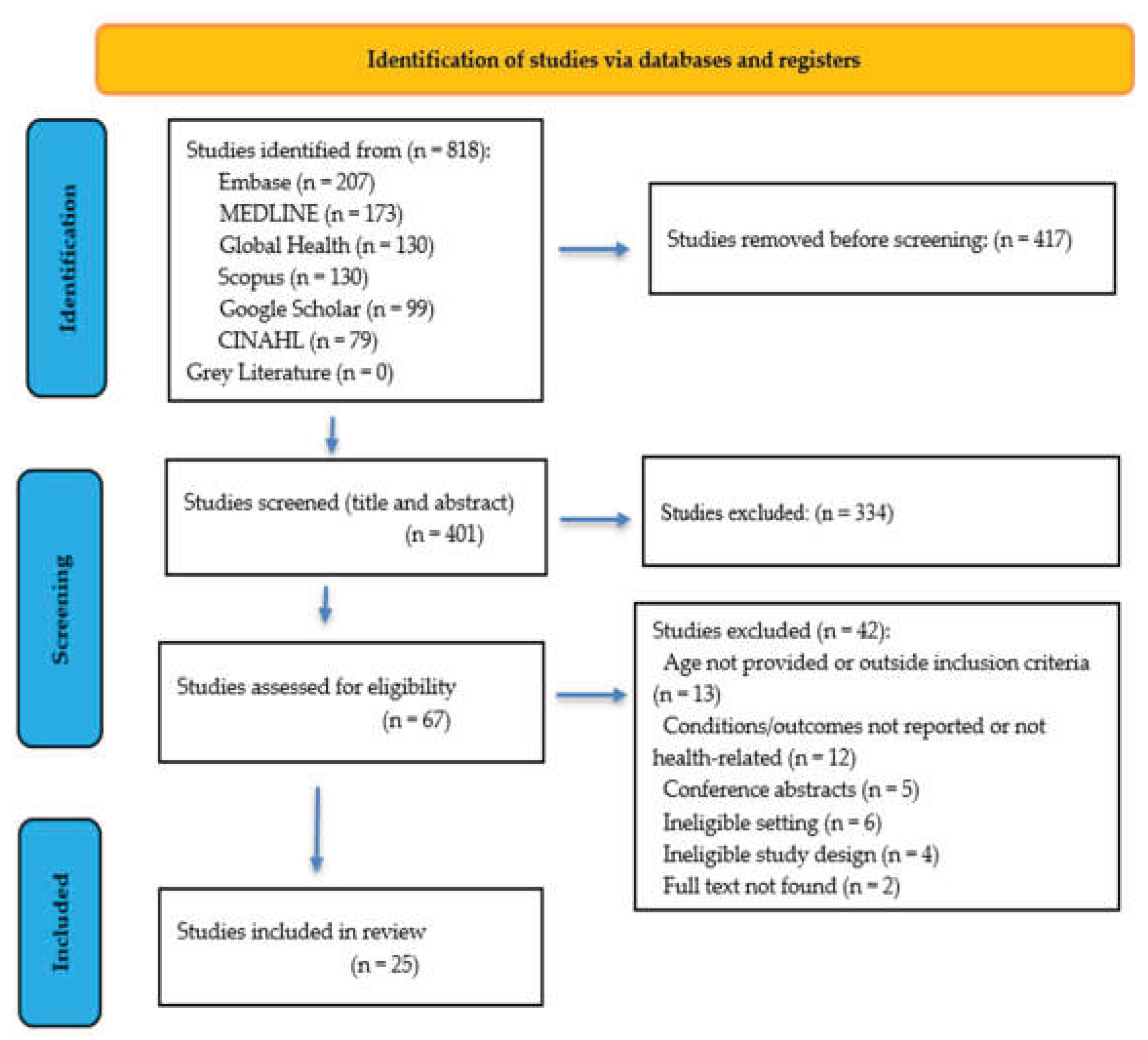
Table 1.
Inclusion and Exclusion Criteria Based on PICOs Framework.
| Criteria | Inclusion (study meets all criteria) | Exclusion (study meets any criteria) |
| Population | Focus on refugees, asylum seekers, or displaced persons | Immigrants, Adolescents, youth and adults, Newcomers |
| Age | A sample of refugee children birth to 5 years old in the population | Adolescents, youth and adults |
| AND | ||
| Setting (Context) | Refugee-receiving Primary healthcare clinic/centre providing services to refugee/immigrant | |
| AND | ||
| Phenomena of Interest (Concept) | Health conditions or outcomes of young children and/or health conditions or outcomes measurement techniques and tools | Focus on acute/emergency health issues |
| Study design/ types of publication | Quantitative, qualitative, mixed methods studies, Interventional studies/ RCTs, Review articles, Secondary data analysis, Grey literature, Conference proceedings, preprints, and research letter | Opinion papers or commentaries or pieces, Books, presentations, and conference abstracts, case studies |
| Results of studies | Results presented for Canadian children < 6 years. Health outcomes must be disaggregated for this population but not health measurements | |
| AND | ||
| Country | Canada | Any study does not include Canada |
| Language | English language | Published in any language other than English |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



