
Submitted:
27 October 2025
Posted:
28 October 2025
You are already at the latest version
Abstract
Background/Objectives: Creatine monohydrate (Cr) supplementation may serve as an effective first-line nutritional intervention to enhance gut metabolism and preserve lean body mass, specifically fat-free mass, thereby improving functional capacity and quality of life in individuals with Crohn’s disease (CD). This paper aims to explore the potential mechanisms through which creatine supplementation may benefit CD patients and review the current literature on this topic. Methods: Study identification was conducted in accordance with the PRISMA-P guidelines. A total of 120,639 studies were initially identified using the selected keywords. After removing duplicates and excluding articles with irrelevant content, the remaining full-text studies were screened for eligibility. Results: Five studies were analyzed to assess the relationship between creatine supplementation and Crohn’s disease. Preliminary evidence suggests potential therapeutic benefits, although data remain limited. Conclusions: Creatine supplementation warrants further investigation through clinical trials and cohort studies. Emerging data from both in vitro and in vivo models indicate that Cr may help mitigate intestinal mucosal degradation. Additionally, its demonstrated benefits in other inflammatory conditions highlight its promise as a therapeutic strategy for promoting disease remission in CD. As a foundational step, further analysis of National Health and Nutrition Examination Survey (NHANES) data to document creatine-rich food sources and daily intake patterns is recommended before initiating clinical trials in Crohn’s disease cohorts.
Keywords:
inflammatory bowel disease
; NHANES
; clinical studies
; foods
1. Introduction
Creatine (Cr) is synthesized endogenously from the amino acids arginine, glycine, and methionine, primarily in the liver, kidneys, and pancreas [1]. The synthesis pathway involves two primary enzymes: L-arginine: glycine amidinotransferase and guanidinoacetate N-methyltransferase [2]. However, creatine is delivered as a supplement primarily as creatine monohydrate (95% of clinical trials), and is the only supplemental source of creatine approved for sale in countries worldwide. It has a pivotal role in energy homeostasis, particularly during high-intensity activities and metabolically stressful conditions (e.g., mitochondrial dysfunction, ischemia, etc.) [2]. The chemical structure of creatine comprises a methylguanidine-acetic acid moiety, enabling it to readily accept a phosphate group. Energy liberated from the degradation of the high-energy phosphate bond in phosphocreatine is crucial for the rapid regeneration of Triphosphoric Adenosine (ATP) from Diphosphoric Adenosine (ADP) inside the muscles, thereby sustaining muscle power and delaying fatigue [3,4,5].
Creatine monohydrate supplements have been extensively on athletes’ samples, depicting their beneficial role in performance, enhancing muscular strength, power [6], and high-intensity exercise capacity by facilitating ATP regeneration [7]. Specifically, its effect is particularly pronounced in activities involving short bursts of maximal effort, such as weightlifting, sprinting, and jumping, and in some cases endurance (>~3 min in duration) [8]. Prolonged creatine ingestion (0.3 grams/kg/day for 5–7 days and 0.03 to 0.15 grams/kg/day thereafter) [9,10] induces an increase in fat-free mass [11], stimulating protein synthesis and potentially leading to increased muscle mass and strength gains over time [12]. Consequently, there is an increasing number of studies that utilize creatine monohydrate supplements in the general population, from infants to the elderly, seeking to augment their creatine stores and, by extension, lean body mass. Of course, its beneficial role extends to factors such as injury and neurocognitive disorders prevention, neuroprotection (concussion, traumatic brain injury (TBI), spinal cord injuries), and improvements in cognitive function, pointing to creatine’s necessity throughout the lifespan [10]. Most studies show creatine is helpful for neuromuscular diseases affecting muscle, but not if neural damage has occurred [13]. For this reason, many authors are searching for creatine’s beneficial influence on pathological conditions [13] or, on rare occasions, the side effects [14,15].
Creatine has been shown to play a crucial role in preserving intestinal mucosal integrity and cellular energy during stress conditions. Supplementation with creatine in a novel intraluminal preservation solution significantly enhanced energy levels, including ATP and Cr, and improved mucosal structure and function. In rodent models, creatine treatment-maintained barrier integrity, reduced oxidative injury, and preserved electrophysiological properties compared to controls [16]. Genetic studies revealed that mutations in the Glycine Amidinotransferase (Gatm) gene, which is involved in creatine biosynthesis, led to increased susceptibility to colitis, while creatine supplementation reversed the damage [17]. Creatine also supports epithelial cell metabolism and tight junction integrity through its creatine transporter, which was found to be reduced in patients with inflammatory bowel disease (IBD) [18]. Overall, creatine’s ability to regulate energy balance and barrier function underscores its therapeutic potential in both organ preservation and intestinal diseases, and by extension, in pathological conditions such as Crohn’s disease.
In general, IBD encompasses a complex and severe group of gastrointestinal disorders characterized by chronic or relapsing inflammation, which significantly affects patients’ overall health, quality of life, and healthcare costs [19]. The two principal forms of IBD are CD and Ulcerative Colitis (UC), which are distinguished by their distinct anatomical involvement and histopathological patterns [20]. Although the precise etiology of IBD remains uncertain, it is widely recognized as a multifactorial condition involving genetic susceptibility, dysbiosis of the gut microbiota, and various environmental influences [21]. Accumulating evidence suggests that dietary patterns—particularly those associated with a Western diet—can adversely affect the gut microbiome, immune responses, and mucosal integrity, thereby contributing to the pathogenesis of IBD [22,23].
In the context of nutritional status, patients with CD are particularly vulnerable to malnutrition due to factors such as inadequate dietary intake, nutrient malabsorption, increased gastrointestinal losses, and medication-related side effects [24,25]. The degree of malnutrition in CD patients varies, depending on the extent and severity of intestinal involvement and other contributory factors [26]. Consequently, malnutrition may lead to reductions in muscle mass and function. This raises the question of whether creatine monohydrate supplementation, which in typical population, its oral ingestion is nearly 100% bioavailable [2], could serve as an effective first-line nutritional intervention aimed at enhancing gut metabolism, maintaining lean body mass, specifically through the preservation or augmentation of fat-free mass, thereby improving both the functional capacity and quality of life in individuals with CD. The present review seeks to explore the potential mechanisms through which creatine supplementation may benefit CD patients and to review the current body of studies on this topic.
2. Materials and Methods
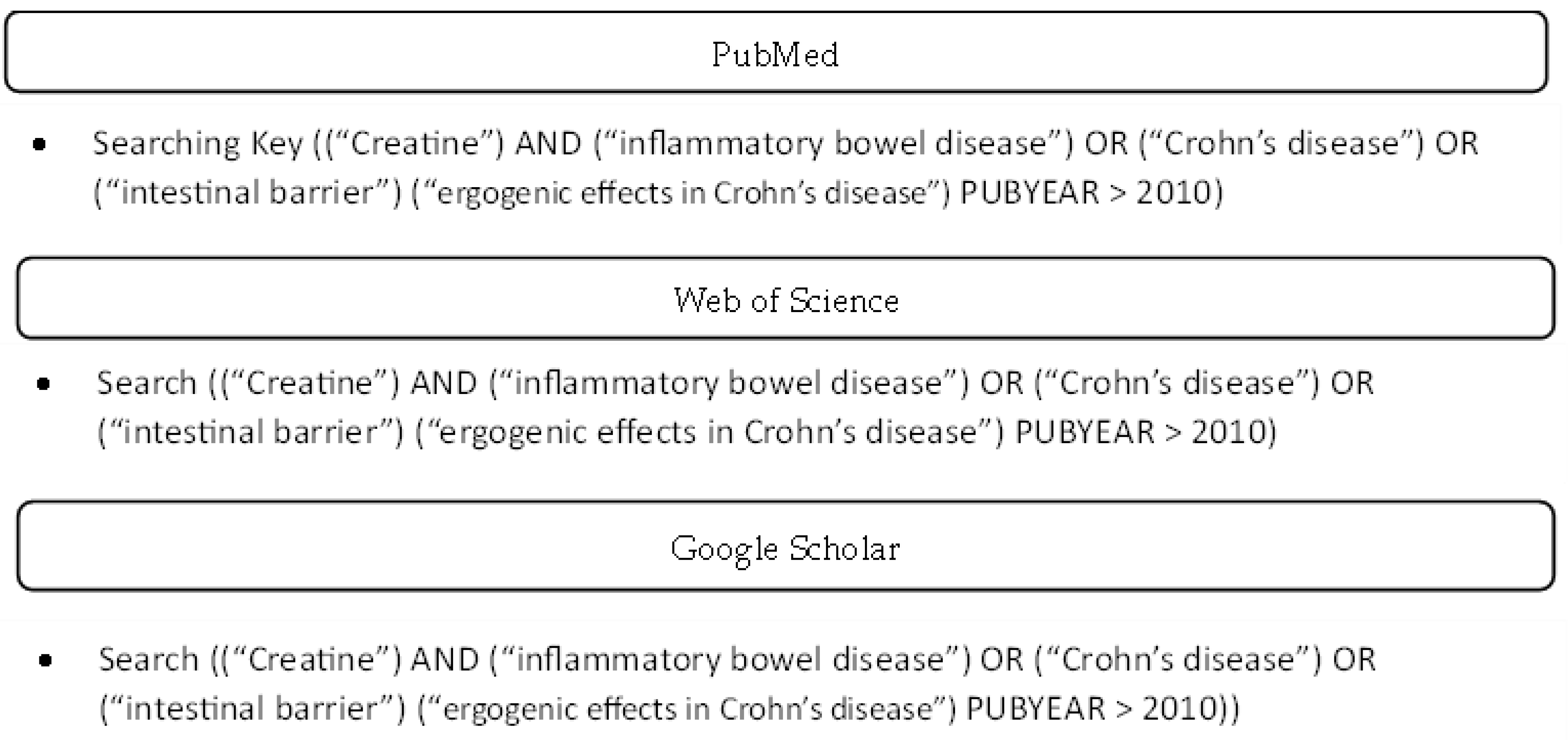
A search of the literature was conducted, with no registration number, to find the most relevant articles on Cr and CD from 1st January until 1st May 2025. Also, the included and excluded studies were conducted according to the PRISMA-P document [27]. The article search was conducted using the most robust databases, including PubMed, Web of Science, and Google Scholar. The search strategy comprised “creatine” AND “inflammatory bowel disease” OR “Crohn’s disease” OR “intestinal barrier” OR “ergogenic effects in Crohn’s disease. Each database’s systematic equations are presented in Appendix A. For a study to be included, the following were checked: 1. manuscripts in the English language, 2. full text availability, 3. human or animal participants, 4. acute or intervention effects of creatine, and 6. all study types (original, narrative reviews, systematic reviews and case reports, and studies). The exclusion criteria were 1. not meeting the inclusion criteria.
3. Results
The literature was reviewed by examining the studies’ titles and abstracts to match the searched keywords. A total of 120639 studies (PubMed=167; Science Direct = 11693 and Scholar = 108779) were found using the included general keywords (creatine and inflammatory bowel disease). Then, removing duplicates (11) and articles with different content (120573), the remaining full-text studies were selected, screened, and compared to determine inclusion in the narrative review (55). Finally, five (5) studies were found and described the influence or/ and the mechanisms between Cr and IBD or CD. Also, in two (2) out of five (5) studies, there was a clear reference in the title for both the keywords Cr and CD (PRISMA flowchart, Figure 1).
4. Discussion
Unique scientific data regarding creatine supplementation in individuals with Crohn’s disease have been reported in a case study involving a 33-year-old patient who received 1.034 g/day of creatine hydrochloride (Cr-HCl) [28]. By the way, Kreider, Jäger, and Purpura [29] concluded that Cr-HCl does not offer superior absorption or muscle creatine retention compared to creatine monohydrate (Cr-M). Also, the manufacturers of C-HCl claimed that Cr-HCl is more bioavailable in tested doses of 1.5 and 5 g/day; however, without any substantiated clinical evidence. Furthermore, the review highlighted that Cr-HCl does not outperform Cr-M in enhancing physical performance, hormonal responses, or body composition. As a result, the researchers classified Cr-HCl as having limited evidence supporting its efficacy compared to a placebo.
In the case study, the authors do not clearly describe how the patient decided to initiate supplementation, nor do they state whether a physician prescribed it. Notably, creatine’s potential beneficial effects were observed only after four months, during which the patient discontinued creatine supplementation and began treatment with mesalamine (Salix Pharmaceuticals, Raleigh) at a dose of 1.5 g/day. During this time, the patient’s symptoms worsened, characterized by progressively more frequent and severe abdominal pain, extensive ulceration, worsening symptoms, and mucosal ulceration/inflammation, ultimately leading the patient to resume creatine supplementation. Upon resumption, symptom remission was reported, indicating that one of the probable mechanisms is the altered expression of mitochondrial and cytosolic CK enzymes and an overall decrease in transcript levels of CK. These findings highlight the important role played by creatine metabolism in intestinal mucosal function and colitis resolution [28].
Nevertheless, even during the period before discontinuing creatine, the patient had a two-year history of hematochezia and anal pain, thought to be secondary to non-healing anal fissures, as well as rectal bleeding, chronic cramping abdominal pain, and loose stools. Thus, two hypotheses can be proposed: (a) long-term supplementation with creatine hydrochloride contributed to the manifestation of the two-year history of symptoms (null hypothesis); (b) the patient’s adaptation to 1.034 g/day of creatine hydrochloride established a stable condition, suggesting that creatine supplementation contributed to symptom remission (research hypothesis).
4.1. The Null Hypothesis
In the null hypothesis, long-term supplementation with Cr-HCl is proposed as the cause of the two-year history of symptoms. Studies on CD’s and macro- and micronutrient consumption have indicated that imbalances in food intake may be positively correlated with the manifestation of symptoms [30]. This suggestion was first introduced in a case report involving a 22-year-old elite male endurance athlete, who, despite the absence of a family history of CD’s—unlike the 33-year-old patient—was noted to have unbalanced dietary habits, characterized by a high-fat diet and a lack of micronutrients [31].
In the current case, it is plausible that excessive creatine supplementation (1.034 g/day) combined with an unknown dietary pattern created an imbalanced intestinal environment, leading to gut microbiota dysbiosis [32], degradation of the mucosal layer, and subsequent symptom manifestation [33]. Additionally, two scientific reports have indicated that creatine may inhibit colon cancer growth [34,35], suggesting a potential role for creatine in modulating inflammatory processes associated with CD’s. On the other hand, Li and Yang [36] revealed that creatine supplementation enhances antitumor T cell immunity in multiple preclinical mouse tumor models, improving antitumor efficacy.
Although the contradictory reports, Gkikas et al. [32] propose a different explanation. Specifically, they support that dietary triggers act differently across populations, with the microbiome serving as a critical modifier of dietary influences on the development of IBD. This variability likely explains why the 33-year-old patient requested the resumption of creatine supplementation after four months. In other words, a systematic dietary imbalance (e.g., high intake of processed foods and red meat) can trigger gut microbiota dysbiosis and contribute to CD’s onset (Papadimitriou et al., 2025). However, following this trigger phase, the organism may adapt to the altered environment, and efforts to return to a balanced diet might paradoxically exacerbate symptoms [32].
In CD, the muscle mass degradation has many theories and misconceptions, making it difficult for the authors to precisely depict its mechanisms. However, this multifactorial disease seems to be focused on the small intestine, observing the degradation of the mucosa’s layer structure. This degradation induces epithelial cell exposure to luminal bacteria [37]. The epithelial cells’ exposure causes injury in many parts of the intestine [38]. As a result, it is observed that intestinal dysregulation in food absorption causes insufficient energy intake [30,39] and consequently, macronutrient depletion in the blood circulation, inducing muscle atrophy [31]. However, how can creatine supplementation remiss or reverse this degradation mechanism?
Regarding creatine supplementation, Cr-M is widely considered the gold standard for its ergogenic benefits, with a strong safety profile [10]. Specifically, the phosphocreatine (PCr)/Cr) shuttle system supports mucosal barrier function and wound healing by improving cellular energetics and stabilizing adherent junctions [40,41,42]. During active inflammation, such as in IBD, low oxygen (O₂) levels stabilize hypoxia-inducible transcription factors (HIFs), leading to the upregulation of creatine kinase (CK) isoenzymes and the creatine transporter (CrT1), belonging to the X-linked gene solute carrier family 6 member 8 (SLC6A8) [40], as a member of a solute carrier family, in intestinal epithelial cells. CK localizes to epithelial junctions, where it interacts with the actin cytoskeleton to maintain structural integrity. In the context of epithelial disruption, large amounts of ATP are required to support cytoskeletal reorganization, including acto-myosin ATPase activity at cellular junctions. Under these conditions, CK and CrT1 work coordinately to promote wound healing and barrier function by generating ATP from PCr, thereby maintaining epithelial homeostasis [40,41,42]. Therefore, the null hypothesis is rejected.
4.2. The Research Hypothesis
In the research hypothesis, creatine hydrochloride could potentially remiss the symptoms. In the case of the 33-year-old patient, creatine hydrochloride improved him clinically, and the prior extensive ulceration and inflammation in the Terminal ileum appeared significantly improved, and only one small aphthous ulcer was seen. Observing the beneficial effects of creatine, the therapy was continued. However, what would happen in the case of the utilization of another more or equally effective creatine supplement, such as creatine monohydrate, whose influence has been proven more or equally beneficial than other creatine types [1,43].
Escalante et al. [44] reported the total creatine content per serving, form(s) of creatine in products, product claims, and prevalence of products third-party certified, they revealed that there is a total of 175 creatine supplements. However, Cr has been shown to have the most beneficial effects, enhancing during in vitro or in vivo studies. Specifically, a novel intraluminal preservation solution, tailored to address energy depletion and oxidative stress in stored intestines, was supplemented with creatine to improve mucosal integrity in rodent models. The tissues showed higher levels of creatine phosphate and ATP, preserved transepithelial resistance, and reduced permeability after 10 hours of cold storage compared to untreated controls. Histological analysis revealed substantially less tissue damage in creatine-loaded samples, suggesting that enhancing cellular energy reserves may be a viable strategy for maintaining intestinal viability during transplantation or storage [16].
Additionally, complementary studies on the CrT/SLC6A8 in intestinal epithelial cells have shown its crucial role in maintaining energy homeostasis and barrier function. CrT, which localizes at tight junctions, was found to regulate intracellular creatine levels, wound healing, and epithelial integrity. Knockdown or deficiency of CrT led to impaired barrier formation and increased reliance on glycolysis, contributing to tight junction dysfunction and cellular stress. Moreover, mucosal biopsies from patients with IBD exhibited significantly reduced CrT expression, potentially linking creatine metabolism deficiencies to compromised barrier integrity in IBD [18]. These findings align with broader insights into dietary creatine’s role in human physiology, highlighting its importance for energy metabolism and gastrointestinal health [46].
Roy & Lee [28], in their case study, noted that in future studies using 3–5 g of chemically pure creatine monohydrate per day, given for 3–6 months, either as a monotherapy or in combination with low dose metformin (0.5–1.0 g per day) would potentially be able to improve several quality-of-life parameters of patients with IBD. Considering the wide spectrum of beneficial effects of creatine with improvement in muscle mass and strength, mobility, and vital functions, with less fatigue and depression [46], its utilization seems important. However, since 1932, when Burrill B. Crohn [47] first published his report on CD (Crohn, Ginzburg, Oppenheimer, 1932), there have not been well-studied protocols. Possible, because the last decay has been answered more scientifically, the avoidance of any severe side effects after creatine supplementation [10,43].
4.3. How Can We Begin the Research Journey of Creatine Contribution?
It is well established that certain foods are notable for their creatine content (g/kg), including herring (6.5–10), beef (4.5), salmon (4.5), pork (5), cod (3), tuna (4), milk (0.1), cranberries (0.02), and shrimp (0.7) [48]. Therefore, the first step is determining whether individuals with CD consume such foods and, by extension, whether this contributes to symptom remission. According to the study by Papadimitriou et al. [30], foods most commonly associated with symptom relief and preferred by CD patients include yogurt, wine, bananas, dairy products, rice, kefir, olive oil, potatoes, fish, chicken, vegetables, fruits, and meat (primarily pork). Notably, many of these items contain moderate to high levels of creatine, suggesting that CD patients may indeed be consuming creatine-rich foods that could support symptom remission (Table 1).
Before evaluating the potential effects of creatine supplementation, it is essential to recognize that patients with CD may benefit from consuming foods naturally high in creatine. A National Health and Nutrition Examination Survey (NHANES) would be a significant first step for the recognition of the CD’s daily Cr intake through their food consumption [49]. Based on the cited studies, CD patients already prefer and tolerate many creatine-rich foods in their daily diet. Therefore, using creatine as a supplement appears feasible and unlikely to cause adverse reactions or symptom exacerbation. This assumption aligns with the hypotheses and recommendations of Roy & Lee [28] and Wallimann et al. [46]. Furthermore, considering creatine supplementation has been studied for its therapeutic potential in conditions such as sarcopenia [50], aging [51], cardiovascular disease, diabetes, neurodegenerative disorders, muscular dystrophy, and even in oncology [13], it is timely to explore its role in CD management.
Consistent with Roy & Lee’s [28] proposal, we also recommend assessing the expression of the creatine transporter CrT1 in intestinal epithelial cells via biopsy before prescribing creatine supplementation. This biomarker would serve as a critical parameter for determining the likelihood of treatment efficacy, as patients with active disease and significant ulceration may have impaired creatine absorption. Conversely, given creatine’s potential to accelerate tissue regeneration, it may offer a novel therapeutic avenue for inducing remission in CD disease, whose prevalence has increased markedly in recent decades.
5. Conclusions
Cr-M supplementation requires further investigation through clinical and cohort studies about its effects on intestinal metabolism in CD. Recent data from both in vitro and in vivo models suggest that Cr may help counteract the degradation of the intestinal mucosa. Moreover, its beneficial effects in other inflammatory conditions underscore its potential as a therapeutic standard in promoting disease remission. As a preliminary step, further NHANES studies documenting specific creatine-rich foods and patterns of daily intake are needed before launching clinical trials in CD cohorts.
Author Contributions
For research articles with several authors, a short paragraph specifying their individual contributions must be provided. The following statements should be used “Conceptualization, K.P.; methodology, K.P.; G.E.D.; SKP; validation, K.P. R.B.K. and S.K.P.; formal analysis, K.P.; investigation, K.P.; resources, K.P. R.B.K.; data curation, K.P. R.B.K. and S.K.P.; writing—original draft preparation, K.P. R.B.K.; writing—review and editing, K.P., R.B.K., G.E.D. and S.K.P.; visualization, K.P.; supervision, K.P.; project administration, K.P. All authors have read and agreed to the published version of the manuscript.” Please turn to the CRediT taxonomy for the term explanation. Authorship must be limited to those who have contributed substantially to the work reported.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Conflicts of Interest
R.B.K. has conducted industry-sponsored research on creatine, received financial support for presenting at conferences, and has served as an expert witness throughout his career. Additionally, he serves as Chair of the Scientific Advisory Board for AlzChem (a company that makes creatine monohydrate), is a co-founder of the non-profit International Society of Sports Nutrition (ISSN), and a member of the scientific advisory boards for Oath Nutrition and Trace Minerals. The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| Cr | Creatine |
| CD | Crohn’s disease |
| NHANES | National Health and Nutrition Examination Survey |
| ATP | triphosphoric adenosine |
| ADP | diphosphoric adenosine |
| TBI | Traumatic brain injury |
| StO2 | Oxygen saturation |
| Gatm | Glycine aminotransferase |
| IBD | Inflammatory bowel disease |
| UC | Ulcerative colitis |
| Cr-HCL | Creatine hydrochloride |
| Cr-M | Creatine monohydrate |
| PCr | phosphocreatine |
| O2 | Oxygen |
| HIF | hypoxia-inducible transcription factors |
| CK | creatine kinase |
| CrT1 | creatine transporter |
| SLC6A8 | solute carrier family 6 member 8 |
Appendix A
References
- Jäger, R.; Purpura, M.; Shao, A.; Inoue, T.; Kreider, R.B. Analysis of the Efficacy, Safety, and Regulatory Status of Novel Forms of Creatine. Amino Acids 2011, 40, 1369. [Google Scholar] [CrossRef] [PubMed]
- Kreider, R.B.; Jäger, R.; Purpura, M. Bioavailability, Efficacy, Safety, and Regulatory Status of Creatine and Related Compounds: A Critical Review. Nutrients 2022, 14, 1035. [Google Scholar] [CrossRef] [PubMed]
- Parise, G.; Mihic, S.; MacLennan, D.; Yarasheski, K.E.; Tarnopolsky, M.A. Effects of Acute Creatine Monohydrate Supplementation on Leucine Kinetics and Mixed-Muscle Protein Synthesis. J. Appl. Physiol. 2001, 91, 1041–1047. [Google Scholar] [CrossRef]
- Ruchalla, E. Nahrungsergänzungsmittel im Sport – Kreatinsupplementation Erhöht den Wassergehalt im Körper. Sportverletz. Sportschaden 2016, 30, 126–129. [Google Scholar] [CrossRef]
- Ellery, S.J.; Murthi, P.; Gatta, P.A.D.; May, A.K.; Davies-Tuck, M.; Kowalski, G.M.; Callahan, D.L.; Bruce, C.R.; Wallace, E.M.; Walker, D.W.; et al. The Effects of Early-Onset Pre-Eclampsia on Placental Creatine Metabolism in the Third Trimester. Int. J. Mol. Sci. 2020, 21, 806. [Google Scholar] [CrossRef]
- Fernández-Landa, J.; Calleja-González, J.; León-Guereño, P.; Caballero-García, A.; Córdova, A.; Mielgo-Ayuso, J. Effect of the Combination of Creatine Monohydrate Plus HMB Supplementation on Sports Performance, Body Composition, Markers of Muscle Damage and Hormone Status: A Systematic Review. Nutrients 2019, 11, 2528. [Google Scholar] [CrossRef]
- Beck, K.L.; Thomson, J.; Swift, R.J.; von Hurst, P.R. Role of Nutrition in Performance Enhancement and Postexercise Recovery. Open Access J. Sports Med. 2015, 6, 259–267. [Google Scholar] [CrossRef]
- Forbes, S.C.; Candow, D.G.; Neto, J.H.F.; Kennedy, M.D.; Forbes, J.L.; Machado, M.; Bustillo, E.; Gomez-Lopez, J.; Zapata, A.; Antonio, J. Creatine Supplementation and Endurance Performance: Surges and Sprints to Win the Race. J. Int. Soc. Sports Nutr. 2023, 20, 2204071. [Google Scholar] [CrossRef]
- Hall, M.; Trojian, T.H. Creatine Supplementation. Curr. Sports Med. Rep. 2013, 12, 240–244. [Google Scholar] [CrossRef]
- Kreider, R.B.; Jagim, A.R.; Antonio, J.; Kalman, D.S.; Kerksick, C.M.; Stout, J.R.; Wildman, R.; Collins, R.; Bonilla, D.A. Creatine Supplementation Is Safe, Beneficial throughout the Lifespan, and Should Not Be Restricted. Front. Nutr. 2025, 12, 1578564. [Google Scholar] [CrossRef] [PubMed]
- van Loon, L.J.C.; Oosterlaar, A.M.; Hartgens, F.; Hesselink, M.K.C.; Snow, R.J.; Wagenmakers, A.J.M. Effects of creatine loading and prolonged creatine supplementation on body composition, fuel selection, sprint and endurance performance in humans. Clin. Sci. 2003, 104, 153. [Google Scholar] [CrossRef]
- Francaux, M.; Poortmans, J. Effects of training and creatine supplement on muscle strength and body mass. Eur. J. Appl. Physiol. Occup. Physiol. 1999, 80, 165. [Google Scholar] [CrossRef]
- Kreider, R.B.; Stout, J.R. Creatine in Health and Disease. Nutrients 2021, 13, 447. [Google Scholar] [CrossRef] [PubMed]
- Parsowith, E.J.; Stock, M.S.; Kocuba, O.; Schumpp, A.; Jackson, K.; Brooks, A.M.; Larson, A.; Dixon, M.; Fairman, C.M. Impact of short-term creatine supplementation on muscular performance among breast cancer survivors. Nutrients 2024, 16, 979. [Google Scholar] [CrossRef] [PubMed]
- Domingues, W.J.R.; Ritti-Dias, R.M.; Cucato, G.G.; Wolosker, N.; Zerati, A.E.; Puech-Leão, P.; Coelho, D.B.; Nunhes, P.M.; Moliterno, A.A.; Avelar, A. Effect of creatine supplementation on functional capacity and muscle oxygen saturation in patients with symptomatic peripheral arterial disease: A pilot study of a randomized, double-blind placebo-controlled clinical trial. Nutrients 2021, 13, 149. [Google Scholar] [CrossRef] [PubMed]
- Mueller, K.; Kokotilo, M.S.; Carter, J.M.; Thiesen, A.; Madsen, K.L.; Studzinski, J.; Khadaroo, R.G.; Churchill, T.A. Creatine-loading preserves intestinal barrier function during organ preservation. Cryobiology 2018, 84, 69–76. [Google Scholar] [CrossRef]
- Turer, E.; McAlpine, W.; Wang, K.W.; Lu, T.; Li, X.; Tang, M.; Zhan, X.; Wang, T.; Zhan, X.; Bu, C.H.; Murray, A.R.; Beutler, B. Creatine maintains intestinal homeostasis and protects against colitis. Proc. Natl. Acad. Sci. USA 2017, 114, E1273–E1281. [Google Scholar] [CrossRef]
- Hall, C.H.T.; Lee, J.S.; Murphy, E.M.; Gerich, M.E.; Dran, R.; Glover, L.E.; Abdulla, Z.I.; Skelton, M.R.; Colgan, S.P. Creatine transporter, reduced in colon tissues from patients with inflammatory bowel diseases, regulates energy balance in intestinal epithelial cells, epithelial integrity, and barrier function. Gastroenterology 2020, 159, 984–998e1. [Google Scholar] [CrossRef] [PubMed]
- Santiago, M.; Dias, C.C.; Alves, C.; Ministro, P.; Gonçalves, R.; Carvalho, D.; Portela, F.; Correia, L.; Lago, P.; Magro, F. The Magnitude of Crohn’s Disease Direct Costs in Health Care Systems (from Different Perspectives): A Systematic Review. Inflamm. Bowel Dis. 2022, 28, 1527–1536. [Google Scholar] [CrossRef]
- Chang, J.T. Pathophysiology of Inflammatory Bowel Diseases. N. Engl. J. Med. 2020, 383, 2652–2664. [Google Scholar] [CrossRef]
- Burisch, J.; Zhao, M.; Odes, S.; De Cruz, P.; Vermeire, S.; Bernstein, C.N.; Kaplan, G.G.; Duricova, D.; Greenberg, D.; Melberg, H.O.; et al. The cost of inflammatory bowel disease in high-income settings: A Lancet Gastroenterology & Hepatology Commission. Lancet Gastroenterol. Hepatol. 2023, 8, 458–492. [Google Scholar] [CrossRef]
- Huppertz-Hauss, G.; Høivik, M.L.; Langholz, E.; Odes, S.; Småstuen, M.; Stockbrugger, R.; Hoff, G.; Moum, B.; Bernklev, T. Health-Related Quality of Life in Inflammatory Bowel Disease in a European-Wide Population-Based Cohort 10 Years after Diagnosis. Inflamm. Bowel Dis. 2015, 21, 337–344. [Google Scholar] [CrossRef]
- Forbes, A.; Escher, J.; Hébuterne, X.; Kłęk, S.; Krznaric, Z.; Schneider, S.; Shamir, R.; Stardelova, K.; Wierdsma, N.; Wiskin, A.E.; et al. ESPEN Guideline: Clinical Nutrition in Inflammatory Bowel Disease. Clin. Nutr. 2017, 36, 321–347. [Google Scholar] [CrossRef]
- Jabłońska, B.; Mrowiec, S. Nutritional Status and Its Detection in Patients with Inflammatory Bowel Diseases. Nutrients 2023, 15, 1991. [Google Scholar] [CrossRef] [PubMed]
- Balestrieri, P.; Ribolsi, M.; Guarino, M.P.L.; Emerenziani, S.; Altomare, A.; Cicala, M. Nutritional Aspects in Inflammatory Bowel Diseases. Nutrients 2020, 12, 372. [Google Scholar] [CrossRef]
- Marcil, V.; Levy, E.; Amre, D.; Bitton, A.; Sant’Anna, A.M.G.A.; Szilagy, A.; Sinnett, D.; Seidman, E.G. A Cross-Sectional Study on Malnutrition in Inflammatory Bowel Disease: Is There a Difference Based on Pediatric or Adult Age Grouping? Inflamm. Bowel Dis. 2019, 25, 1428–1441. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2020, 372, n71. [Google Scholar] [CrossRef]
- Roy, A.; Lee, D. Dietary Creatine as a Possible Novel Treatment for Crohn’s Ileitis. ACG Case Rep. J. 2016, 3, e173. [Google Scholar] [CrossRef] [PubMed]
- Kreider, R.B.; Jäger, R.; Purpura, M. Bioavailability, Efficacy, Safety, and Regulatory Status of Creatine and Related Compounds: A Critical Review. Nutrients 2022, 14, 1035. [Google Scholar] [CrossRef]
- Papadimitriou, K.; Deligiannidou, G.-E.; Voulgaridou, G.; Giaginis, C.; Papadopoulou, S.K. Nutritional Habits in Crohn’s Disease Onset and Management. Nutrients 2025, 17, 559. [Google Scholar] [CrossRef]
- Papadimitriou, K. The Influence of Aerobic Type Exercise on Active Crohn’s Disease Patients: The Incidence of an Elite Athlete. Healthcare 2022, 10, 713. [Google Scholar] [CrossRef]
- Gkikas, K.; Svolos, V.; Hansen, R.; Russell, R.K.; Gerasimidis, K. Take-Home Messages from 20 Years of Progress in Dietary Therapy of Inflammatory Bowel Disease. Ann. Nutr. Metab. 2023, 79, 476–484. [Google Scholar] [CrossRef] [PubMed]
- Papadimitriou, K. Effect of Resistance Exercise Training on Crohn’s Disease Patients. Intest. Res. 2021, 19, 275–281. [Google Scholar] [CrossRef] [PubMed]
- Kirstensen, C.A.; Askenasy, N.; Jain, R.K.; Koretsky, A.P. Creatine and Cyclocreatine Treatment of Human Colon Adenocarcinoma Xenografts: 31P and 1H Magnetic Resonance Spectroscopic Studies. Br. J. Cancer 1999, 79, 278–285. [Google Scholar] [CrossRef]
- Wyss, M.; Kaddurah-Daouk, R. Creatine and Creatinine Metabolism. Physiol. Rev. 2000, 80, 1107–1133. [Google Scholar] [CrossRef]
- Li, B.; Yang, L. Creatine in T Cell Antitumor Immunity and Cancer Immunotherapy. Nutrients 2021, 13, 1633. [Google Scholar] [CrossRef] [PubMed]
- Abraham, C.; Cho, J.H. Inflammatory Bowel Disease. N. Engl. J. Med. 2009, 361, 2066–2078. [Google Scholar] [CrossRef]
- Beery, R.M.M.; Li, E.; Fishman, L.N. Impact of Pediatric Inflammatory Bowel Disease Diagnosis on Exercise and Sports Participation: Patient and Parent Perspectives. World J. Gastroenterol. 2019, 25, 4493–4501. [Google Scholar] [CrossRef]
- Papadimitriou, K.; Detopoulou, P.; Soufleris, K.; Voulgaridou, G.; Tsoumana, D.; Ntopromireskou, P.; Giaginis, C.; Chatziprodromidou, I.P.; Spanoudaki, M.; Papadopoulou, S.K. Nutritional Risk and Sarcopenia Features in Patients with Crohn’s Disease: Relation to Body Composition, Physical Performance, Nutritional Questionnaires, and Biomarkers. Nutrients 2023, 15, 3615. [Google Scholar] [CrossRef]
- Glover, L.E.; Bowers, B.E.; Saeedi, B.; Ehrentraut, S.F.; Campbell, E.L.; Bayless, A.J.; Dobrinskikh, E.; Kendrick, A.A.; Kelly, C.J.; Burgess, A.; Miller, L.; Kominsky, D.J.; Jedlicka, P.; Colgan, S.P. Control of Creatine Metabolism by HIF is an Endogenous Mechanism of Barrier Regulation in Colitis. Proc. Natl. Acad. Sci. USA 2013, 110, 19820–19825. [Google Scholar] [CrossRef]
- Glover, L.E.; Colgan, S.P. Epithelial Barrier Regulation by Hypoxia-Inducible Factor. Ann. Am. Thorac. Soc. 2017, 14, S233–S236. [Google Scholar] [CrossRef]
- Lee, J.S.; Wang, R.X.; Alexeev, E.E.; Colgan, S.P. Intestinal Inflammation as a Dysbiosis of Energy Procurement: New Insights into an Old Topic. Gut Microbes 2021, 13, 1–20. [Google Scholar] [CrossRef]
- Antonio, J.; Candow, D.G.; Forbes, S.C.; et al. Common Questions and Misconceptions about Creatine Supplementation: What Does the Scientific Evidence Really Show? J. Int. Soc. Sports Nutr. 2021, 18, 13. [Google Scholar] [CrossRef]
- Escalante, G.; Gonzalez, A.M.; St Mart, D.; Torres, M.; Echols, J.; Islas, M.; Schoenfeld, B.J. Analysis of the efficacy, safety, and cost of alternative forms of creatine available for purchase on Amazon.com: Are label claims supported by science? Heliyon 2022, 8, e12113. [Google Scholar] [CrossRef]
- Brosnan, M.E.; Brosnan, J.T. The Role of Dietary Creatine. Amino Acids 2016, 48, 1785–1791. [Google Scholar] [CrossRef]
- Wallimann, T.; Hall, C.H.T.; Colgan, S.P.; Glover, L.E. Creatine supplementation for patients with inflammatory bowel diseases: A scientific rationale for a clinical trial. Nutrients 2021, 13, 1429. [Google Scholar] [CrossRef]
- Crohn, B.B.; Ginzburg, L.; Oppenheimer, G.D. Regional ileitis; a pathologic and clinical entity. Am. J. Med. 1952, 13, 583–590. [Google Scholar] [CrossRef] [PubMed]
- Rasmussen, C.J. Nutritional Supplements for Endurance Athletes. In Nutritional Supplements in Sports and Exercise; Humana Press, 2008. [Google Scholar] [CrossRef]
- Xiong, N.; Zhang, W.; Zhang, Y.; Nie, C.; Dan, H. Association between nutrient intake and inflammatory bowel disease risk: Insights from NHANES data and dose-response analysis. Nutrition 2025, 131, 112632. [Google Scholar] [CrossRef]
- Dolan, E.; Artioli, G.G.; Pereira, R.M.R.; Gualano, B. Muscular atrophy and sarcopenia in the elderly: Is there a role for creatine supplementation? Biomolecules 2019, 9, 642. [Google Scholar] [CrossRef] [PubMed]
- Candow, D.G.; Forbes, S.C.; Chilibeck, P.D.; Cornish, S.M.; Antonio, J.; Kreider, R.B. Effectiveness of creatine supplementation on aging muscle and bone: Focus on falls prevention and inflammation. J. Clin. Med. 2019, 8, 488. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Prisma flow chart of selected studies.
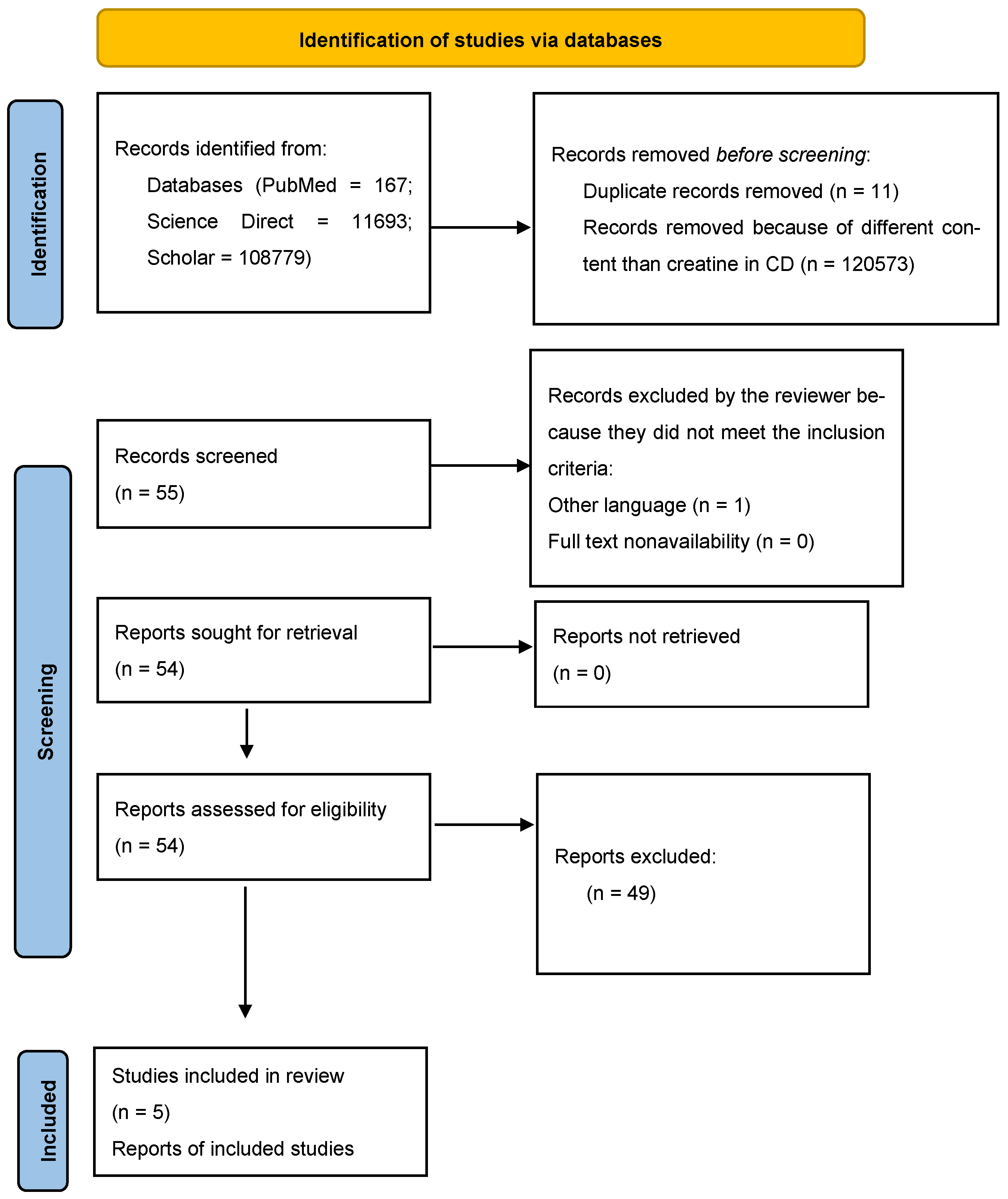

Table 1.
Foods and beverages that CD patients consume and their creatine content.
| Foods | Creatine Content (g· kg−1 mass) |
|---|---|
| Rice | ≈ 0.32 |
| Potatoes | ≈ 0.18 |
| Salmon | ≈ 4.5 |
| Chicken | ≈ 0.8 |
| Meat (Beef, pork) | ≈ 4.5-5 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



