
Submitted:
26 September 2025
Posted:
22 October 2025
You are already at the latest version
Abstract
Background/Objectives: Pressure ulcers are an important patient safety healthcare concern. While staging frameworks guide clinical management, the association of the anatomical site, stage, and multiple PU presence, with outcomes such as length of stay (LOS) and mortality in Medicare patients has not been fully characterized. The study objective is to examine the relationship between PU site, stage, and multiplicity with inpatient LOS and mortality among hospitalized Medicare patients. Methods: This cross-sectional study was conducted with 1,123,121 inpatient Medicare admissions from a CMS medical claims dataset. PUs were identified using ICD-10-CM codes, classified by anatomical site and stage (1 though 4, unstageable, unspecified). Multivariate models examined associations of PU characteristics with LOS and mortality, adjusting for age, sex, primary diagnosis, and hospital transfer. Results: Overall, 3.7% of admissions included at least one PU (n=41,525). Stage 2 ulcers were the most common (28.6%), while unstageable or unspecified ulcers were frequent in heels and head. The sacral region was the most common anatomical site, followed by buttocks and heels. LOS gradually increased from Stage 1 (9.4 days) to Stage 4 (15.2 days). While death rate did not increase consistently with stage, it was highest for upper back (14%), head (12.8%), and unspecified hip (12.8%) sites. Multivariate analyses found sacral, hip, head, buttock, upper back ulcers and ulcers to be associated with prolonged LOS and increased mortality. Conclusions: PU anatomical site and multiple PU presence were stronger predictors of adverse outcomes than stage alone. These findings emphasize the importance of systematic documentation, early detection, and patient safety protocols to reduce the clinical and systemic burden of PUs.
Keywords:
patient safety
; pressure ulcers
; Medicare
; length of stay
; hospital mortality
1. Introduction
Pressure ulcers (PUs) are a significant challenge for health systems, extending beyond the immediate concerns of wound management, and include broader patient safety issues [1]. PUs are injuries to the skin and underlying tissues and result from long mechanical loading, typically over bony prominences such as the sacrum, heels, and hips. PUs are more frequent in patients with limited mobility. The etiology of PUs includes patient factors such as comorbidities, age-related tissue fragility, and nutritional deficiencies, as well as external factors such as mechanical forces, medical devices, and hospital care environment characteristics [4,5,6,7,8,9]. While largely preventable, PUs occur frequently in healthcare settings, showing prevention practice inefficiencies and the need for effective monitoring and quality improvement. The occurrence of PUs is therefore both a clinical concern and a quality-of-care indicator, emphasizing the responsibility of health providers to prevent injury and to mitigate adverse outcomes [1,2].
The prevalence of PUs varies across healthcare settings. Intensive care units (ICUs), long-term care acute settings, and nursing homes have higher PU incidence rates, likely due to patient acuity, hospital care practices, and issues with staffing, lack of educational initiatives or prevention protocols [2,3]. Older age is a significant risk factor, because of age-related skin changes, tissue integrity, reduced mobility, and the higher prevalence of comorbidities such as cardiovascular disease and diabetes [3,4]. Among younger populations those mostly affected are patients with prolonged mechanical ventilation, or extensive surgical interventions [3,6]. This variation in PU prevalence emphasized the need to map the frequency, anatomical site, and stage of PUs in hospitalized patients to understand risk stratification and resource allocation.
The pathophysiology of PUs involves an interplay of mechanical, cellular, and systemic factors. Prolonged pressure over bony prominences impairs tissue perfusion, leading to hypoxia, metabolic dysfunction, and ultimately cellular necrosis [4]. This is the reason patients with conditions such as compromised cardiovascular function, and diabetes are particularly vulnerable [4,5]. Comorbidities often require prolonged immobilization and sometimes medications that can slow tissue repair [5]. In addition, hospital environmental factors play a critical role. Patients in critical care settings experience extended immobility, sedation, and exposure to medical devices such as mechanical ventilators, catheters, and vascular access devices, all of which can contribute to tissue damage and delayed healing [6,7,8]. Staffing adequacy, nursing education, and institutional culture also influence PU outcomes, with insufficient knowledge of prevention protocols or lack of systematic risk assessment contributing to higher incidence rates [9,15].
Evidence-based strategies for PU prevention include evidence-driven risk assessment, targeted interventions, and continuous monitoring. Validated instruments such as the Braden Scale and Norton Scale are available to measures the risk and facilitate early identification of high-risk patients and the focus of preventive resources to specific anatomical sites [10,11]. Repositioning protocols and the use of pressure-relieving surfaces reduce mechanical loading and forces, lowering the likelihood of tissue injury [12,13,14]. Positioning techniques (e.g., 30-degree lateral rotation method) can be particularly effective in reducing pressure over bony prominences [14]. Nutritional status further influences PU risk by affecting tissue repair, immune function, and overall skin integrity. Malnutrition also increases susceptibility to PUs and this emphasizes the need for nutritional assessment as part of PU prevention programs [17].
Health provider education is important in PU prevention efforts. Educational interventions have been shown to improve knowledge, attitudes about patient safety, which in turn contribute to safer clinical practices related to PU prevention [15,16]. Training programs must prioritize professional development, documentation, and quality monitoring for adherence to evidence-based protocols. Quality monitoring includes process measures (e.g., completion rates of risk assessments, preventive interventions), and outcome measures (e.g., PU incidence, stage, and severity) as well [18,19,20].
The clinical consequences of PUs extend beyond local tissue injury, affecting patient quality of life, functional status, and mental health. Patients report pain, sleep disturbances, mobility limitations, and anxiety, depression, and reduced self-efficacy [21,30,31,32,35]. These impacts often influence long-term recovery and rehabilitation outcomes and extend beyond the hospital stay. Patients with advanced-stage PUs have higher risk for infection, sepsis, and delayed recovery from underlying medical conditions, and have been associated with increased morbidity and mortality [22,24,25,26,29]. In addition, multiple coexisting PUs create compound challenges, reflecting underlying vulnerability, nutritional compromise, and complex care needs, further straining healthcare resources [4,33,34]. The psychological and social implications of multiple PUs, including body image, social withdrawal, and caregiver strain, emphasize the importance of patient-centered approaches that address physical and psychosocial dimensions of care [35,36].
PU staging provides a framework for assessing injury severity, guiding treatment decisions, and evaluating clinical outcomes. Stage I PUs involve non-blanchable erythema of intact skin and with significant opportunities for early intervention to prevent progression [26,27]. Stage II injuries involve partial-thickness tissue loss and requires specialized wound care. There is still substantial healing potential [28]. Stage III and IV PUs, represent full-thickness tissue loss, and may extend into muscle, bone, or supporting structures. They are associated with increased risk for infection, sepsis, and prolonged recovery [29]. Advanced-stage PUs also increase resource utilization, and increased economic burden, emphasizing the critical need for early recognition and prevention [24,26,31].
The anatomical site and multiplicity of PUs also influence clinical outcomes. The sacrum, heels, buttocks, hips, and elbows are the most affected regions, and multiple coexisting ulcers indicate compounded clinical challenges [4,33]. Multiple PUs are frequently linked with malnutrition, or advanced frailty, and limited healing capacity, increased risk for infection, prolonged hospitalization, and increased mortality risk [4,33,34]. The psychological burden of multiple ulcers compounds patient vulnerability and interventions that address mental health alongside physical wound care [35,36].
While prevention strategies and risk assessment tools are well-established, there remains a need to quantify the frequency, stage, and anatomical characteristics of PUs and evaluate their association with clinical outcomes. Mapping PU prevalence and PU characteristics can offer a useful tool to understand early risk detection, preventive interventions, and improved resource allocation. Moreover, understanding the relationship between PUs and adverse outcomes provides evidence to support quality improvement initiatives and patient safety policies. The present study aims to addresses this knowledge gap (i) mapping the frequency, anatomical site, stage, and characteristics of PUs, and (ii) examine their association with inpatient LOS and hospital mortality among hospitalized elderly patients. By combining descriptive analyses of PU patterns with outcome associations, this study aims to improve understanding of PU burden in hospital settings. Findings could also guide prevention strategies, inform clinical risk stratification (and help healthcare providers prioritize high-risk patients), optimize care processes and support evidence-based patient safety interventions.
2. Materials and Methods
2.1. Study Design
A retrospective cross-sectional study using secondary administrative data was designed to examine hospitalized Medicare patients with documented Pressure Ulcers. The first goal of the research is to create a mapping of the PUs, including their frequency, the most frequent combinations, and their stages. Goal 2 is to examine the association of PU site, stage and multiple PU presence with two critical hospital outcomes: inpatient mortality, and LOS. After bivariate analysis is completed, the study furthermore controls for demographics, primary Dx and source of admission. Figure 1 shows a diagrammatic representation of the study design.
2.2. Dataset and Study Variables
The study used a dataset of 1,123,121 Medicare beneficiary inpatient admissions. The CMS Limited Data Set (LDS) Inpatient dataset is a de-identified claims dataset that includes information on inpatient hospital stays for Medicare patients. It contains data on patient demographics, diagnoses (ICD-10-CM codes), procedures, LOS, discharge status, hospital charges, and other administrative details. Although patient identifiers are removed, the dataset has important variables that enable health services and outcomes research at a national level in the United States.
Several deriving variables were created from the dataset, as appropriate to examine how the PU characteristics of (i) locality, (ii) stage, and (iii) multiple PU presence, are associated with the hospital mortality and LOS. All admissions were reviewed for the presence of PUs using ICD-10-CM Dx codes. Each unique PU ICD-10-CM code was extracted and coded as a dichotomous variable (present/absent) for analysis. A total of 25 groups of ICD-10-CM PU codes were identified. These codes included anatomical site-specific designations (e.g., sacral, heel, back) and were further detailed using secondary billable ICD-10-CM codes that captured the stage of the PU, classified as Stage 1, Stage 2, Stage 3, Stage 4, or unstageable. A summary of all extracted codes, along with their frequency of occurrence in the dataset, is provided in Table 1.
In addition to analyzing individual PU anatomical sites, composite constructs representing the presence of two or more co-existing PU anatomical sites during the same hospitalization were developed. These constructs were created by identifying admissions in which multiple distinct ICD-10-CM PU codes (indicating different anatomical sites) were documented simultaneously. Dichotomous variables were generated to indicate the presence of multisite PUs, allowing for comparisons between patients with single versus multi-site PUs.
Therefore, with these data transformation it becomes possible for the present study to examine three different PU characteristics: (i) PU anatomical site (ii) PU stage, and (iii) multi-site PU presence (more than 1 PU site code).
This approach enabled the evaluation of the cumulative burden of PUs on inpatient outcomes. The presence of multiple PU anatomical sites was analyzed as an independent variable in the regression models assessing the two key outcomes: hospital LOS, and inpatient mortality. By including these multisite constructs, the study aimed to determine whether patients with multiple PU anatomical sites experienced worse clinical outcomes compared to those with ulcers at a single site, after adjusting for covariates as shown on Table 1, which presents all the variables that the study used from the CMS dataset, their operational definitions, and role in the research.
2.3. Statistical Analysis
Initial descriptive statistics were calculated, including the mean LOS, mortality rate, and distribution of PU stages and anatomical sites. To examine the relationship between PU characteristics and inpatient outcomes, multivariable regression analyses were conducted. Specifically linear regression models were used to evaluate the association between PU anatomical site and hospital LOS. A logistic regression model was used to assess the association between PU anatomical site and inpatient mortality. All regression models controlled for potential confounders, including primary Dx, age group, sex, and admission transfer from another setting/SNF. Statistical analyses were performed using IBM SPSS Statistics for Windows, Version 29.0 (IBM Corp., Armonk, NY). A two-tailed alpha level of 0.05 was used to determine statistical significance.
3. Results
3.1. Mapping of Pressure Ulcers
Out of 1,123,121 patient admissions, 41,525 patients (3.69%) had at least one documented PU. Among these, 29,460 patients (70.94%) had a PU at a single site, 7,630 patients (18.37%) had two PUs, 2,954 patients (7.11%) had three PUs, and 912 patients (2.19%) had four PUs. Only 569 patients (1.37%) had five or more PUs. In total, 60,877 unique PU codes were recorded in the dataset. Regarding ulcer stage distribution, 12.31% of PUs were Stage 1, 28.64% Stage 2, 15.83% Stage 3, and 15.87% Stage 4. Additionally, 12.73% were classified as unstageable and 14.76% as unspecified. The distribution of stages varied significantly across anatomical sites. Table 2 highlights, for each PU site, the most frequent stage. For several sites, the “unstageable” or “unspecified stage” ICD-10-CM code was more frequent code. As expected, PUs recorded at unspecified sites (e.g., unspecified elbow, heel, hip, or ankle) had the highest proportion of unstageable or unspecified cases. The right heel, left heel, and head followed, with nearly half of the cases at these sites lacking a definitive stage classification (See: Table 2).
To summarize the severity of PUs by anatomical site, a “Pressure Ulcer Locality-Stage score” (PULS) was calculated as the weighted average stage for each site, excluding unstageable and unspecified cases. The PULS was defined as:
PULS=(1×k1+2×k2+3×k3+4×k4)/100
Where kj represents the percentage of cases at stage j. PULS ranges from 1 (all cases Stage 1) to 4 (all cases Stage 4). The last column on Table 2 presents PULS values across anatomical sites. With respect to the PULS score, the highest mean PU stage values were observed for Contiguous Site PUs (3.09), followed by Left Hip (3.07) and Right Hip (3.02). In contrast, the lowest scores were found for the head, left heel, and right heel (Table 2).
*back/buttock/hip.
3.2. Bivariate Associations Between PU Properties and Study Outcomes
3.2.1. Pressure Ulcer Site vs Study Outcomes
The distribution of PU sites, mean LOS and mortality rates are presented in Table 3. The sacral region was the most frequent site, with 23.5 cases per 1,000 hospital admissions, followed by the right buttock (4.3 per 1,000) and left buttock (4.2 per 1,000). Mean LOS varied by site, with the longest hospitalizations observed for head PUs (16.22 days), left upper back PUs (16.03 days), and contiguous site PUs involving the back, buttock, or hip (15.26 days). Mortality rates were highest for left upper back PUs (14.04%), head PUs (12.82%), and unspecified hip PUs (12.80%).
3.2.2. Pressure Ulcer Stage vs Study Outcomes
Without considering the PU site, but only the stage, those with any PU of Stage 1 had a mean LOS of 9.4 days (+/- 11.15), which increased to 10.33 days (+/- 12.09) for stage 2 PUs, up to 12.88 days (+/-43.40) for stage 3, and 15.24 days for stage 4 PUs. For inpatient mortality, those with any PU of stage 1 had a mortality rate of 7.12%, increased to 7.91% for stage 2 PUs, 8.66% for stage 3. Interestingly, stage 4 PU patients did not have a higher mortality rate than stage 3 (8.62%).
For most anatomical sites, advancing PU stage did not correspond to higher mortality. Simple linear regression analyses indicated a moderate to strong positive trend for Sacral PUs (R² = 0.882, p = 0.06) and PUs of Unspecified Site (R² = 0.896, p = 0.05). Conversely, several PU sites demonstrated an inverse association, with higher-stage ulcers linked to lower mortality (Table 3).
In contrast, LOS exhibited a more consistent pattern. For most PU sites, LOS increased progressively from stage 1 through stage 4. Notably, Sacral PUs (R² = 0.96, p = 0.01) and Left Hip PUs (R² = 0.99, p < 0.01) demonstrated near-perfect linear relationships between ulcer stage and hospital LOS. Results for all PU sites are summarized on Table 4.
3.2.3. Multiple Site Pressure Ulcers vs Study Outcomes
A significant increase in both LOS and hospital mortality was observed among patients with PUs at multiple anatomical sites. The correlation between LOS and the total number of PU codes was statistically significant (Pearson’s r = 0.088, p < 0.01). An independent samples t-test demonstrated a significant difference in the mean number of PU codes between patients who died in the hospital and those discharged alive (t = –56.127, p < 0.001). Mean LOS increased progressively with the number of PU sites: 10.58 days for patients with one PU, 11.63 days for two, 12.34 days for three, and 23.46 days for eight or more. A similar trend was observed for mortality, with death rates of 8.13% for one PU, 8.24% for two, 9.51% for three, and 12.50% for eight or more (Figure 2).
The most frequent combinations of multiple co-existing PU sites were found to be: {right heel, left heel} (2059 cases), and {sacral, left heel} (1939 cases), followed by {sacral, right heel} (1858 cases} and {sacral, other site} (1671 cases). Some multiple-PPU-site combinations were found to be associated with especially prolonged hospital stays and high hospital morality rate. Table 5 presents the top 10 combinations of PU sites with the highest hospital inpatient mortality rate and LOS, for combinations appearing in at least 1 in 10,000 cases.
3.3. Multivariate Analysis
3.3.1. Length of Stay
To assess the association between PU anatomical site and hospital LOS, a multiple linear regression analysis was performed. Twenty-five dichotomous variables representing distinct PU sites were entered into the model using the stepwise elimination method. The total number of different PU Dx’s and the PU staging information were also inserted into the model. Control variables included primary Dx (categorized using the Clinical Classifications Software [CCS]), patient transfer status (from a different unit or another hospital or a SNF), sex, and age group.
Several PU anatomical sites were significantly associated with hospital LOS. Specifically, the total number of PUs was positively associated with longer stays (β = 0.93, p < 0.001). The presence of ulcers at the following sites also showed a positive association with LOS: head (β = 4.17, p < 0.001), sacral (β = 2.18, p < 0.001), right hip (β = 2.09, p < 0.001), right buttock (β = 0.92, p < 0.001), left buttock (β = 1.02, p < 0.001), left upper back (β = 2.88, p < 0.001), and contiguous site (β = 2.08 p = 0.03).
In addition, the presence of a PU of a stage other than stage 1 was found to be associated with prolonged hospital stay, by 0.29 days for stage 2 (p=0.02), 2.12 days for stage 3 (p<0.001) and by 4.09 days for stage 4 PUs. A negative association with LOS was observed for left hip PUs (β = -2.14, p < 0.001), left elbow (β = -2.10, p = 0.01), right elbow (β = -2.06, p = 0.014), right lower back (β = -2.99, p = 0.01), and right ankle PUs (β = -1,34, p = 0.001). Among the control variables, transfer from another hospital or from a different unit of the same hospital was associated with longer hospital stays. In contrast, younger age and female gender were both associated with shorter hospital stays (see Table 6).
3.3.2. In-Patient Mortality
Binary Logistic Regression was used to examine the association between PU site, stage and complexity with inpatient mortality. After controlling for the primary Dx, age group, sex, and transfer from other settings, it was found that several PU sites are associated with an increased likelihood for hospital death. These include the left upper back PU (OR=2.32, 1.38-3.89), Sacral (OR=2.19, 1.79-2.68), left buttock (OR=1.39, 1.12-1.73), right heel (OR=1.36, 1.07-1.72), right hip (OR=1.32, 1.00-1.75), and head (OR=1.64, 1.07-2.52). Unspecified buttock, unspecified hip, other site and unspecified site codes were also found to be statistically associated with an increased likelihood for hospital death.
Of the control variables, age (OR=1.16, 1.16-1.17), transfer from another hospital (OR=1.80, 1.74-1.86), or SNF (OR=1.60, 1.52-1.68) were found to be associated with increased likelihood for inpatient death. PU stage was not found to be a predictor of inpatient mortality. Table 7 presents the statistically significant variables.
4. Discussion
This study shows the clinical significance of pressure ulcers (PUs) in hospitalized Medicare patients. Overall PU prevalence was found to be 3.7%, consistent with prior national estimates showing PUs being a problem in acute care settings [21]. The sacral region was the most frequent site, followed by buttocks and heels. These anatomical sites are most prone to immobility-related pressure [4]. Stage 2 ulcers were the most common overall. This is likely because they represent the point at which early skin damage progresses to partial tissue loss, making them clinically visible. Stage 1 ulcers, although more frequent in practice, are often underreported since they involve only redness of intact skin, sometimes subtle. By contrast, Stage 2 PUs present with clear skin breaks, prompting recognition, and coding.
A high proportion of PUs are unstageable or unspecified ulcers, particularly in the right heel, left heel, and head, where nearly half of the cases lacked a definitive stage classification. While it is not clear whether these represent limitations in documentation or a distinct clinical profile, there are some reasonable explanations. Heel ulcers, for instance, are often covered with eschar that prevents accurate staging until debridement, while head ulcers in elderly patients may present atypically. It is also possible that hospitals with resource or training gaps contribute to inconsistent staging practices. This assumption can be furthermore explored in studies conducted at a hospital level, to account for organizational, and structural hospital characteristics. Unstageable ulcers may also hold clinical significance, because they may be proxies of overall patient vulnerability, where patient frailty and overall severity is more determinative of outcomes than wound severity. Addressing this uncertainty will require improved training in staging frameworks and standardized documentation practices. Accurate classification is required to inform appropriate treatment, and prevention strategies.
Hospital LOS was strongly correlated with PU stage and anatomical site. LOS increased from 9.4 days in Stage 1 to 15.2 days in Stage 4, showing the resource burden associated with advanced ulcers. In contrast, inpatient mortality rose modestly from Stage 1 through Stage 3 and plateaued at Stage 4, indicating that severity by stage may not be a direct mortality predictor.
PU severity, measured by locality stage score, was highest in hips and contiguous back/buttock/hip sites, while lowest in heels and head, and unstageable or unspecified ulcers were most frequent in the hip, heel, ankle, and elbow. Certain ulcer anatomical sites, such as the head, sacral area, hips, upper back, and contiguous back/buttock/hip sites, were associated with substantially longer LOS, while mortality was highest for left upper back (14%), head (12.8%), and unspecified hip (12.8%). The association of sacral, hip, head, and upper back ulcers with longer LOS and higher mortality suggests that these anatomical sites are markers of systemic frailty and serious comorbidities, where immobility, poor perfusion, and challenges in wound care would worsen outcomes.
Regression analyses identified specific sites, sacral, hip, head, buttock, and upper back, as independent risk factors for both longer hospitalization and higher mortality. These findings echo reports that ulcer anatomical site may reflect systemic illness severity and frailty rather than wound severity alone [26].
Multiplicity of ulcers was a determinant of adverse outcomes. Patients with ≥8 ulcers had a mean LOS of 23.5 days and mortality of 12.5%, compared to 10.6 days and 8.1% for those with a single ulcer. This trend shows the compounding effect of multisite ulceration, likely because of compromised healing capacity and overall systemic vulnerability [36]. High-risk combinations, such as bilateral heels with sacral or hip involvement, were associated with especially poor outcomes, suggesting potential “red flag” patterns for clinical monitoring.
Our findings indicate that higher stage PUs were not directly associated with greater mortality risk. This somewhat counterintuitive result may reflect the reality that patients with the most severe underlying illnesses often do not survive long enough to develop advanced-stage ulcers. Another interpretation is that hospitals consistently coding higher stage ulcers may also be those with greater clinical vigilance and more robust prevention practices, which can lessen their impact on mortality. At the same time, it should be acknowledged that our study did not account for comorbidities or procedures that may contribute to ulcer development and severity. Exploring these relationships would offer a more nuanced understanding of which patient groups are most vulnerable. Still, recognizing certain combinations of ulcer anatomical site and stage as “red flags” for risk has practical value, as such awareness can help clinicians prevent avoidable harm.
When examining hospital LOS, we found that severe and multi-site ulcers are linked with longer admissions. Yet, this association may be circular: patients with prolonged hospitalizations are at higher risk of developing serious ulcers, and once ulcers appear, they tend to further extend recovery time. This feedback loop shows the importance of timely preventive strategies, consistent documentation, and early intervention.
Equally important, our findings reinforce that PUs themselves are strongly associated with extended hospital stays and, in some cases, increased inpatient mortality, regardless of primary Dx. Patients with multiple or advanced ulcers experienced markedly prolonged admissions, underscoring the dual role of PUs as both a cause and a consequence of longer hospitalizations. Certain ulcer sites, such as sacral, hip, and head, were independent predictors of poor outcomes, suggesting that anatomical site conveys additional risk beyond stage alone.
5. Conclusions
Findings show both the clinical and health system attributes of PU care, pointing to the need for more studies that take into consideration comorbidities, therapeutic pathways, and hospital practices to better understand patient risk and outcomes. Our findings emphasize the importance of prevention, early recognition, and systematic documentation. They also highlight the need for risk models that integrate ulcer anatomical site and multiplicity rather than relying on stage alone. Transfers from skilled nursing facilities or other hospitals further amplified risks, pointing to transitions of care as a vulnerable period for PU management [24]. PU anatomical site and multiplicity were found to be stronger predictors of negative outcomes than the PU stage itself. emphasizing that prevention must extend beyond staging frameworks.
We would like to emphasize the need for patient safety protocols that prioritize not just prevention but also early detection. Validated risk assessments, pressure redistribution intervention, and staff education remain central to limiting PU progression. Clinical training should focus on early recognition of subtle skin changes for prompt intervention. This is especially important in high-risk groups such as patients transferred from nursing facilities or those with multiple comorbidities. These preventive approaches can reduce patient suffering and lessen the effects of PUs on hospital resource use and system-level outcomes.
Author Contributions
Conceptualization, D.Z.; methodology, D.Z.; formal analysis, D.Z.; resources, D.Z and P.E.; data curation, D.Z.; writing—original draft preparation, D.Z and P.E.; writing—review and editing, D.Z and P.E.; supervision, D.Z. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding
Institutional Review Board Statement
Not applicable. Secondary de-identified administrative data was used
Informed Consent Statement
Not applicable.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| PU | Pressure Ulcer |
| CMS | Centers for Medicare and Medicaid Services |
| ICD-10 | International Classification of Diagnoses, 10th edition |
| LOS | Length of Stay |
| ICU | Intensive Care Unit |
References
- Hu D., Ning J., Sun Y., Wang S., Jin N., Chen Y. et al. Construction and application of a three-level linkage system for the prevention and treatment of pressure sores in geriatric patients in Henan Province, China. Iranian Journal of Public Health 2022. [CrossRef]
- AYYILDIZ A. and Yelken B. Evaluation of pressure sores in intensive care; what situation are we in? Cukurova Anestezi Ve Cerrahi Bilimler Dergisi 2021;4(1):61-65. [CrossRef]
- Tsai, Y., Lin, C., Yen, Y., Wu, C., Carvajal, C. J., Molte, N. F., … & Hsieh, C. (2023). Risk factors for pressure ulcer recurrence following surgical reconstruction: a cross-sectional retrospective analysis. Frontiers in Surgery, 10. [CrossRef]
- Jaul E., Barron J., Rosenzweig J., & Menczel J. An overview of comorbidities and the development of PUs among older adults. BMC Geriatrics 2018;18(1). [CrossRef]
- Bekele H., Zemene W., & Tesfaye E. PU and associated factors among adult patients admitted to the surgical wards in the comprehensive specialized hospital of the northwest Amhara regional state, Ethiopia. 2024. [CrossRef]
- Hossain B., Mamun A., Razi H., & Raisul N. Evaluation of PUs among critically ill patients admitted to a tertiary hospital. Journal of Bangladesh College of Physicians and Surgeons 2022;40(1):23-30. [CrossRef]
- Camargo W., Pereira R., Tanita M., Heko L., Grion I., Festti J. et al. The effect of support surfaces on the incidence of pressure injuries in critically ill patients: a randomized clinical trial. Critical Care Research and Practice 2018;2018:1-6. [CrossRef]
- Mathur M., Mutreja J., Gill N., Vyas K., Niranjan A., & Kale R. Prevalence, risk factors, and management of pressure sores in the teaching hospital -- medical and surgical treatment. International Journal of Contemporary Surgery 2019;7(2):132-141. [CrossRef]
- Aiman U., Saddique H., & Jabeen R. Nursing knowledge and practice regarding the prevention of PUs. Biological and Clinical Sciences Research Journal 2024;2024(1):1150. [CrossRef]
- Mwebaza I., Katende G., Groves S., & Nankumbi J. Nurses' knowledge, practices, and barriers in care of patients with PUs in a Ugandan teaching hospital. Nursing Research and Practice 2014;2014:1-6. [CrossRef]
- Truong B., Grigson E., Patel M., & Liu X. PU prevention in the hospital setting using silicone foam dressings. Cureus 2016. [CrossRef]
- Stuque A., Sasaki V., Teles A., Santana M., Rabeh S., & Sonobe H. Protocol for prevention of PU. Rev Rene 2017;18(2):272-282. [CrossRef]
- Antony L., Thelly A., & Mathew J. Evidence-based clinical practice guidelines for caregivers of palliative care patients on the prevention of PUs. Indian Journal of Palliative Care 2022;29:75-81. [CrossRef]
- Sulistiyawati A. and Cahyati Y. Comparison of the effect of 30° and 90° sloping position on PU incident on stroke patients. Indonesian Journal of Global Health Research 2020;2(1):73-82. [CrossRef]
- Karimian M., Khalighi E., Salimi E., Borji M., Tarjoman A., & Mahmoudi Y. The effect of educational intervention on the knowledge and attitude of intensive care nurses in the prevention of PUs. International Journal of Risk & Safety in Medicine 2020;31(2):89-95. [CrossRef]
- Horton-Jones M., Marsh E., Fumarola S., Wright-White H., McSherry W., & Rowson T. Using deep dive methodology to investigate an increased incidence of hospital-acquired avoidable category 2 and 3 PUs. Healthcare 2019;7(2):59. [CrossRef]
- Mobayen M., Zohrevandi B., Jorshari S., & Salari A. Prevalence of bed sores among patients referring to a medical center in Iran. Journal of Surgery and Trauma 2021:17-25. [CrossRef]
- Song Y., Ban K., Kim H., Kim S., Park S., & Kwon M. Development of PU management and fall prevention protocol. Journal of Korean Academy of Fundamentals of Nursing 2023;30(3):391-403. [CrossRef]
- Bulut A., Aksu Ç., Bulut A., & Aslan M. Investigating attitudes of nurses working in a state hospital towards preventing PUs. Genel Tıp Dergisi 2022;32(1):5-11. [CrossRef]
- Gunningberg L., Sving E., Hommel A., Ålenius C., Wiger P., & Bååth C. Tracking pressure injuries as adverse events: national use of the global trigger tool over a 4-year period. Journal of Evaluation in Clinical Practice 2018;25(1):21-27. [CrossRef]
- Li Z., Lin F., Thalib L., & Chaboyer W. Global prevalence and incidence of pressure injuries in hospitalized adult patients: a systematic review and meta-analysis. International Journal of Nursing Studies 2020;105:103546. [CrossRef]
- Shafipour V., Ramezanpour E., Gorji M., & Moosazadeh M. Prevalence of postoperative PU: a systematic meta-analytic review. Electronic Physician 2016;8(11):3170-3176. [CrossRef]
- Jackson D., Sarki A., Betteridge R., & Brooke J. Medical device-related PUs: a systematic review and meta-analysis. International Journal of Nursing Studies 2019;92:109-120. [CrossRef]
- Kim S., Medina M., Hotz K., Kim J., & Chang J. Vulnerability to decubitus ulcers and their association with healthcare utilization: evidence from the Nationwide Inpatient Sample dataset from 2016 to 2020 in us hospitals. Journal of Patient Safety 2023;20(3):164-170. [CrossRef]
- Lechner A., Kottner J., Coleman S., Muir D., Beeckman D., Chaboyer W. et al. Outcomes for PU trials (outputs) project: review and classification of outcomes reported in PU prevention research. British Journal of Dermatology 2020;184(4):617-626. [CrossRef]
- Alderden J., Zhao Y., Zhang Y., Thomas D., Butcher R., Zhang Y. et al. Outcomes associated with stage 1 pressure injuries: a retrospective cohort study. American Journal of Critical Care 2018;27(6):471-476. [CrossRef]
- Maida V., Ennis M., & Corban J. Wound outcomes in patients with advanced illness. International Wound Journal 2012;9(6):683-692. [CrossRef]
- Ahn H., Stechmiller J., Fillingim R., Lyon D., & Garvan C. Bodily pain intensity in nursing home residents with PUs: analysis of national minimum data set 3.0. Research in Nursing & Health 2015;38(3):207-212. [CrossRef]
- Jiao X., Cui C., Ng S., Jiang Z., Tu C., Zhou J. et al. The modified bilobed flap for reconstructing sacral decubitus ulcers. Burns & Trauma 2020;8. [CrossRef]
- Brem H., Maggi J., Nierman D., Rolnitzky L., Bell D., Rennert R. et al. High cost of stage iv PUs. The American Journal of Surgery 2010;200(4):473-477. [CrossRef]
- Smyczek D., Opyrchał J., Koszutski T., Dowgierd K., & Krakowczyk Ł. Reconstructive options for PUs in pediatric patients. Children 2024;11(6):691. [CrossRef]
- Jackson M., McKenney T., Drumm J., Merrick B., LeMaster T., & VanGilder C. PU prevention in high-risk postoperative cardiovascular patients. Critical Care Nurse 2011;31(4):44-53. [CrossRef]
- Sen C. Human wounds and its burden: an updated compendium of estimates. Advances in Wound Care 2019;8(2):39-48. [CrossRef]
- Chica J. and Hill J. Effectiveness of zinc therapy for the treatment of PUs. British Journal of Community Nursing 2023;28(Sup9):S32-S36. [CrossRef]
- Charalambous C., Vassilopoulos A., Koulouri A., Eleni S., Popi S., Farmakas A. et al. The impact of stress on PU wound healing process and on the psychophysiological environment of the individual suffering from them. Medical Archives 2018;72(3):362. [CrossRef]
- Jaul E, Calderon-Margalit R. Systemic factors and mortality in elderly patients with pressure ulcers. Int Wound J. 2015;12(3):254–259. [CrossRef]
Figure 1.
Diagrammatic representation of study design.
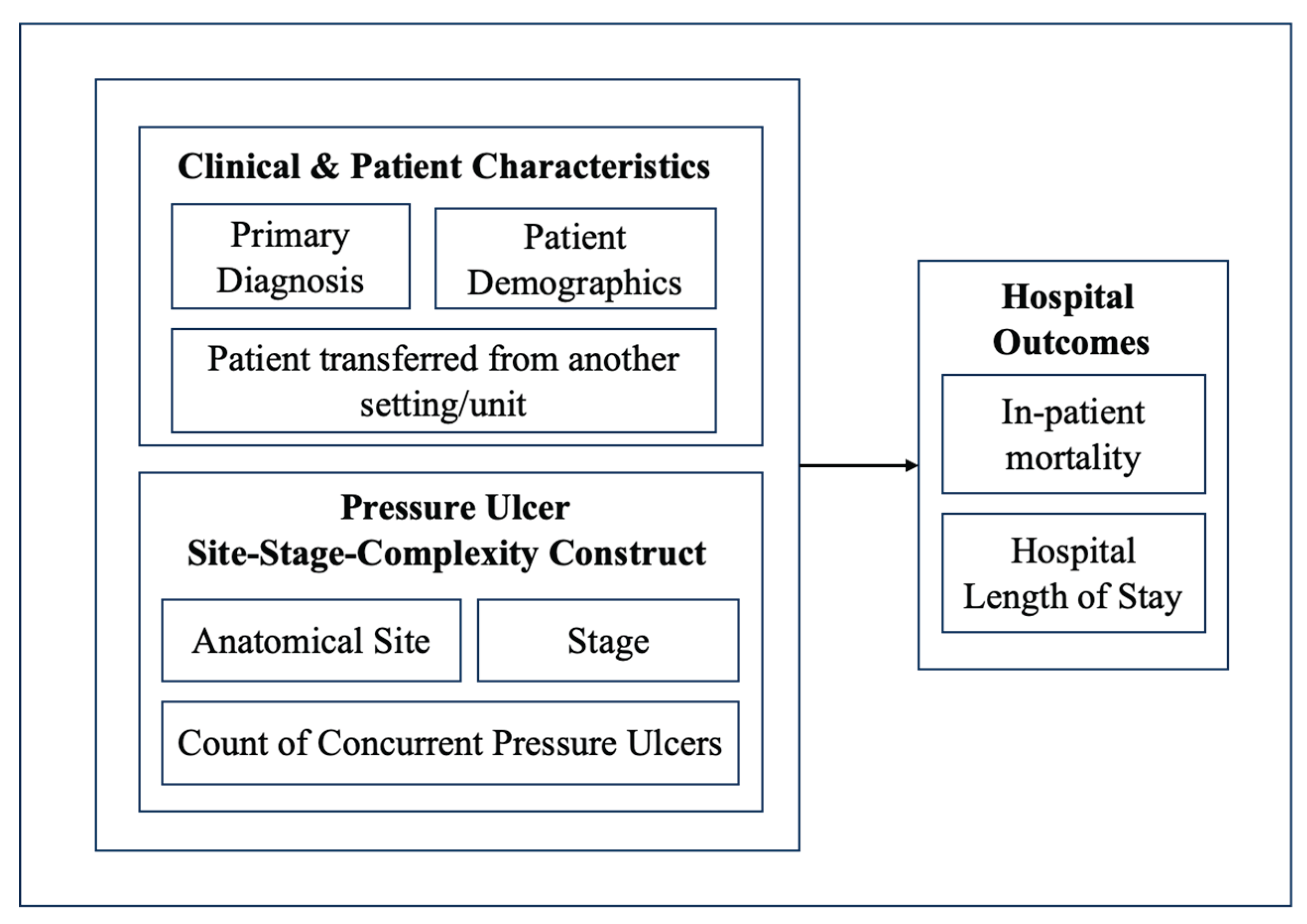
Figure 2.
Mean LOS and inpatient mortality vs number of concurrent PU codes.
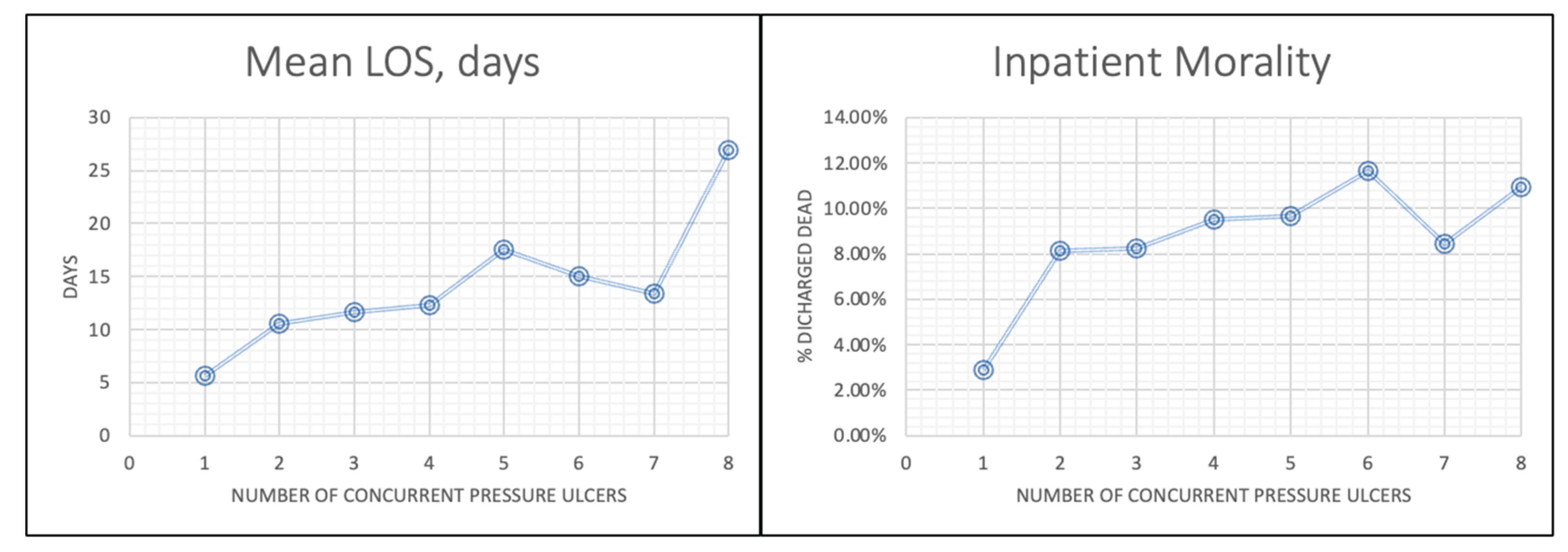

Table 1.
Variables used in the study and operational definitions
| Variable Name | How it is calculated | Definition | Values |
| Dependent Variables | |||
| Length of Stay (days) | Deriving, calculated as the difference of discharge-admission date | Total number of in-patient days | Integer. Length of Stay (days). |
| Died | Deriving from “Discharge Status” | Patient expired during the hospitalization | yes/no |
| Main Independent Variables | |||
| Presence of PUs by site | Deriving from secondary Dx list. | The anatomical site that the PU is present, using ICD-10. | One y/n variable per site/ stage combo |
| Pressure Ulcer Stage | Deriving, PU code of highest stage. For >1 PUs, it takes the value of the worst stage. | PU stage, as recognized by health providers. | 1, 2, 3, 4 |
| Number of concurrent PUs | Count of unique PUs regardless of stage/site | Sum of unique PU codes during the hospital stay | Integer. Sum of total PU codes |
| Control Variables | |||
| Age group | As it appears in the original dataset | Patient age based on the date of birth | 5-year-range groups |
| Patient sex | As it appears in the original dataset | Administrative sex in the admission file | male/female |
| Primary Dx | Categorical variable of the primary Dx | The patient Dx that led to need for hospitalization | 285 CCS codes |
| Patient transferred from… | |||
| Another hospital | Deriving from “Admission Source” | Patient transferred directly from another hospital | yes/no |
| Skilled Nursing Facility | Patient was transferred directly from SNF | yes/no | |
| Another unit (same hospital) | Internal transfer from another unit of the hospital | yes/no | |
Table 2.
PU frequency by stage & Pressure Ulcer Locality-Stage (PULS) score per anatomical site
| Stage 1 | Stage 2 | Stage 3 | Stage 4 | Unstageable/ Unspecified | PULS | |
| Unspec. Elbow | 16.67% (3) | 16.67% (3) | 5.55% (1) | 0% (0) | 61.07% (11) | 1.71 |
| Right Elbow | 15.34% (27) | 25.57% (45) | 19.32% (34) | 9.09% (16) | 30.68% (54) | 2.32 |
| Left Elbow | 15.89% (31) | 23.59% (46) | 16.41% (32) | 14.35% (28) | 29.73% (58) | 2.42 |
| Unspecified Back | 17.91% (141) | 32.4% (255) | 13.6% (107) | 6.73% (53) | 29.34% (231) | 2.13 |
| Right Upper Back | 13.29% (25) | 29.79% (56) | 23.4% (44) | 9.57% (18) | 23.92% (45) | 2.38 |
| Left Upper Back | 16% (28) | 24.57% (43) | 17.71% (31) | 9.71% (17) | 31.99% (56) | 2.31 |
| Right Low. Back | 12.22% (11) | 26.67% (24) | 23.33% (21) | 13.33% (12) | 24.44% (22) | 2.50 |
| Left Lower Back | 4.76% (4) | 28.57% (24) | 20.24% (17) | 16.66% (14) | 29.75% (25) | 2.69 |
| Sacral | 12.48% (3363) | 31.55% (8499) | 16.45% (4432) | 20.18% (5437) | 19.33% (5210) | 2.55 |
| Unspecified Hip | 6.34% (8) | 11.9% (15) | 11.11% (14) | 12.69% (16) | 57.93% (73) | 2.72 |
| Right Hip | 6.23% (108) | 17.96% (311) | 18.19% (315) | 32.39% (561) | 25.31% (437) | 3.03 |
| Left Hip | 6.01% (101) | 17.87% (300) | 17.33% (291) | 34.96% (587) | 23.81% (400) | 3.07 |
| Unspec. Buttock | 19.27% (328) | 34.67% (590) | 10.28% (175) | 5.99% (102) | 29.78% (507) | 2.04 |
| Right Buttock | 10.71% (529) | 41.37% (2042) | 15.94% (787) | 12.62% (623) | 19.33% (955) | 2.38 |
| Left Buttock | 11.01% (526) | 40.47% (1934) | 16.38% (783) | 12.15% (581) | 19.97% (955) | 2.37 |
| Contiguous Site* | 4.51% (6) | 20.30% (27) | 18.79% (25) | 36.84% (49) | 19.54% (26) | 3.09 |
| Unspec. Ankle | 9.58% (7) | 17.81% (13) | 8.22% (6) | 8.21% (6) | 56.15% (41) | 2.34 |
| Right Ankle | 9.04% (69) | 20.84% (159) | 19.4% (148) | 12.18% (93) | 38.52% (294) | 2.57 |
| Left Ankle | 9.74% (72) | 19.89% (147) | 19.22% (142) | 9.6% (71) | 41.54% (307) | 2.49 |
| Unspecified Heel | 10.93% (28) | 15.63% (40) | 7.81% (20) | 4.29% (11) | 61.31% (157) | 2.14 |
| Right Heel | 16.42% (729) | 15.23% (676) | 12.89% (572) | 7.61% (338) | 47.83% (2123) | 2.22 |
| Left Heel | 16.30% (780) | 15.49% (741) | 13.4% (641) | 7.04% (337) | 47.76% (2285) | 2.21 |
| Head | 15.16% (42) | 20.22% (56) | 13.36% (37) | 6.13% (17) | 45.11% (125) | 2.19 |
| Other Site | 8.60% (398) | 24.62% (1139) | 18.91% (875) | 10.74% (497) | 37.10% (1716) | 2.51 |
| Unspecified Site | 11.26% (133) | 21.68% (256) | 7.45% (88) | 6.68% (79) | 52.91% (625) | 2.20 |
Table 3.
Frequency of all-stage PU localities, and their mean LOS and mortality
| PU Anatomical site (any stage) | N | Cass per 1000 admissions | LOS (days) | % Died |
| Unspecified Elbow | 18 | 0.016 | 14.89 | 11.11% |
| Right Elbow | 175 | 0.156 | 11.05 | 8.52% |
| Left Elbow | 195 | 0.173 | 11.2 | 9.23% |
| Unspecified Back | 779 | 0.693 | 10.46 | 11.42% |
| Right Upper Back | 185 | 0.164 | 13.04 | 8.11% |
| Left Upper Back | 171 | 0.152 | 16.03 | 14.04% |
| Right Lower Back | 90 | 0.080 | 9.99 | 4.44% |
| Left Lower Back | 83 | 0.074 | 10.69 | 7.23% |
| Sacral | 26476 | 23.537 | 11.8 | 9.40% |
| Unspecified Hip | 125 | 0.111 | 10.84 | 12.80% |
| Right Hip | 1715 | 1.525 | 14.85 | 8.86% |
| Left Hip | 1666 | 1.481 | 12.33 | 8.58% |
| Unspecified Buttock | 1693 | 1.505 | 9.48 | 8.74% |
| Right Buttock | 4900 | 4.356 | 12.29 | 6.98% |
| Left Buttock | 4743 | 4.216 | 12.33 | 7.57% |
| Contiguous Site | 133 | 0.118 | 15.26 | 8.27% |
| Unspecified Ankle | 73 | 0.065 | 8.28 | 6.85% |
| Right Ankle | 760 | 0.676 | 11.27 | 8.16% |
| Left Ankle | 735 | 0.653 | 12.72 | 8.30% |
| Unspecified Heel | 256 | 0.228 | 10.54 | 6.64% |
| Right Heel | 4397 | 3.909 | 11.61 | 7.82% |
| Left Heel | 4752 | 4.224 | 11.29 | 7.18% |
| Head | 273 | 0.243 | 16.22 | 12.82% |
| Other Site | 4367 | 3.882 | 11.88 | 8.17% |
| Unspecified Site | 1172 | 1.042 | 7.99 | 9.22% |
Table 4.
Hospital Mortality and Length of Stay for PUs of different stages.
| Inpatient Mortality | Length of Stay (days) | |||||||||
| PU Stage | PU Stage | |||||||||
| 1 | 2 | 3 | 4 | r² (sig.) | 1 | 2 | 3 | 4 | r² (sig.) | |
| Unspecified Elbow | 33.3% | 0% | 0% | NA | 7 | 24 | 8 | NA | NA | |
| Right Elbow | 3.70% | 11.11% | 8.82% | 6.25% | 0.04 (0.78) | 11.15 | 9.91 | 15.62 | 11.31 | 0.10 (0.67) |
| Left Elbow | 12.90% | 6.52% | 6.25% | 10.71% | 0.07 (0.72) | 9 | 9.65 | 13.03 | 13 | 0.85 (0.07) |
| Unspecified Back | 9.22% | 11.76% | 9.35% | 9.43% | 0.03 (0.81) | 9.21 | 9.96 | 9.78 | 13.36 | 0.70 (0.15) |
| Right Upper Back | 12.00% | 7.14% | 9.09% | 5.56% | 0.65 (0.19) | 5.4 | 10.38 | 20.3 | 19.56 | 0.87 (0.06) |
| Left Upper Back | 7.14% | 16.28% | 6.45% | 23.53% | 0.39 (0.37) | 12.96 | 12.5 | 19.16 | 34.19 | 0.80 (0.10) |
| Right Lower Back | 9.09% | 8.33% | 0.00% | 0.00% | 0.83 (0.08) | 7.55 | 9.75 | 10.48 | 10.58 | 0.80 (0.10) |
| Left Lower Back | 25.00% | 4.17% | 11.76% | 0.00% | 0.62 (0.20) | 11.5 | 7.58 | 16.88 | 11.71 | 0.11 (0.66) |
| Sacral | 7.61% | 8.95% | 9.18% | 9.67% | 0.88 (0.06) | 8.92 | 10.57 | 12.49 | 15.97 | 0.96 (0.01) |
| Unspecified Hip | 25.00% | 20.00% | 7.14% | 12.50% | 0.67 (0.17) | 6.5 | 5.53 | 11.29 | 13.27 | 0.81 (0.09) |
| Right Hip | 7.41% | 9.32% | 8.89% | 7.84% | 0.01 (0.87) | 9.33 | 10.02 | 13.89 | 22.1 | 0.86 (0.07) |
| Left Hip | 5.94% | 9.00% | 9.62% | 7.33% | 0.13 (0.62) | 7.83 | 9.78 | 12.46 | 14.71 | 0.99 (<0.01) |
| Unspecified Buttock | 4.88% | 8.47% | 6.86% | 9.80% | 0.64 (0.19) | 9.17 | 9.04 | 11.1 | 14.02 | 0.85 (0.07) |
| Right Buttock | 5.67% | 6.02% | 8.39% | 4.98% | 0.001 (0.97) | 8.79 | 10.01 | 18.66 | 16.84 | 0.74 (0.13) |
| Left Buttock | 6.84% | 6.72% | 9.07% | 5.16% | 0.04 (0.78) | 8.24 | 10.25 | 18.84 | 16.2 | 0.71 (0.15) |
| Contiguous Site | 0.00% | 7.41% | 24.00% | 4.08% | 0.12 (0.64) | 5.5 | 11.89 | 14.44 | 13.14 | 0.68 (0.17) |
| Unspecified Ankle | 14.29% | 7.69% | 16.67% | 0.00% | 0.34 (0.41) | 4.57 | 7.58 | 7.5 | 9 | 0.84 (0.08) |
| Right Ankle | 11.59% | 7.55% | 8.78% | 4.30% | 0.77 (0.11) | 9.57 | 10.52 | 13.89 | 12 | 0.53 (0.26) |
| Left Ankle | 6.94% | 4.08% | 9.86% | 9.86% | 0.45 (0.32) | 11.65 | 11.96 | 14.12 | 14.14 | 0.85 (0.07) |
| Unspecified Heel | 3.57% | 10.00% | 5.00% | 9.09% | 0.22 (0.52) | 13.71 | 8.03 | 12.25 | 11.91 | 0.01 (0.93) |
| Right Heel | 7.13% | 7.40% | 6.64% | 7.69% | 0.07 (0.73) | 11.65 | 10.34 | 13.36 | 13.82 | 0.58 (0.23) |
| Left Heel | 8.08% | 5.80% | 4.99% | 6.82% | 0.19 (0.55) | 10.65 | 10.63 | 11.41 | 14.06 | 0.76 (0.12) |
| Head | 9.52% | 8.93% | 2.70% | 5.88% | 0.49 (0.29) | 13.02 | 12.14 | 17.76 | 27.18 | 0.81 (0.09) |
| Other Site | 8.79% | 7.11% | 8.34% | 9.46% | 0.17 (0.57) | 11.08 | 10.17 | 14.04 | 14.39 | 0.71 (0.15) |
| Unspecified Site | 3.01% | 7.42% | 7.95% | 10.13% | 0.89 (0.05) | 7.29 | 7.75 | 9.1 | 9.97 | 0.97 (0.01) |
Table 5.
PU combinations with the highest inpatient mortality and longest hospital stay
| PU combination | N | LOS (days) | PU combination | N | % Died |
| {Right Hip, Left Buttock, Sacral} | 104 | 55.94 | {Unspecified Buttock, Other Site} | 108 | 18.52% |
| {Right & Left Buttock, Right Hip} | 101 | 55.69 | {Unspecified Back, Sacral} | 281 | 14.59% |
| {Right Hip, Right Buttock, Sacral} | 115 | 52.76 | {Right & Left Heel, Right Hip} | 102 | 13.73% |
| {Right Hip, Left Buttock} | 176 | 38.77 | {Right Buttock, Other Site, Sacral} | 202 | 13.37% |
| {Right Hip, Right Buttock} | 209 | 35.11 | {Right Ankle, Other Site, Sacral} | 100 | 13.00% |
| {Right Buttock, Other Site, Sacral} | 202 | 19.55 | {Sacral, Right Heel} | 146 | 12.90% |
| {Right & Left Buttock, Sacral} | 806 | 19.19 | {Right & Left Buttock, Right Hip} | 101 | 12.87% |
| {Left Buttock, Other Site, Sacral} | 215 | 18.56 | {Right & Left Ankle} | 159 | 12.58% |
| {Right Hip, Sacral} | 904 | 18.53 | {Left Elbow, Sacral} | 104 | 12.50% |
| {Left Hip, Left Buttock, Sacral} | 103 | 18.41 | {Right & Left Heel, Other Site} | 280 | 12.50% |
Table 6.
Multiple Linear Regression to examine the association between PU site & stage with LOS
| Variable | b | SE | t | p-value | 95% CI | |
| Total number of PU codes | 0.933 | 0.077 | 12.073 | <.001 | 0.78 - 1.08 | |
| PU Stage | ||||||
| Stage 1 | -0.609 | 0.165 | -3.695 | <.001 | -0.93 - -0.28 | |
| Stage 2 | 0.291 | 0.126 | 2.31 | 0.021 | 0.04 - 0.53 | |
| Stage 3 | 2.121 | 0.152 | 13.963 | <.001 | 1.82 - 2.41 | |
| Stage 4 | 4.099 | 0.165 | 24.907 | <.001 | 3.77 - 4.42 | |
| PU Site | ||||||
| Sacral | 2.189 | 0.116 | 18.925 | <.001 | 1.96 - 2.41 | |
| Left Hip | -2.146 | 0.308 | -6.958 | <.001 | -2.75 - -1.54 | |
| Right Buttock | 0.922 | 0.198 | 4.654 | <.001 | 0.53 - 1.31 | |
| Right Hip | 2.096 | 0.304 | 6.891 | <.001 | 1.50 - 2.69 | |
| Head | 4.175 | 0.679 | 6.151 | <.001 | 2.84 - 5.50 | |
| Left Buttock | 1.027 | 0.199 | 5.164 | <.001 | 0.63 - 1.41 | |
| Left Elbow | -2.108 | 0.822 | -2.565 | 0.01 | -3.71 - -0.49 | |
| Left Upper Back | 2.889 | 0.862 | 3.351 | <.001 | 1.19 - 4.57 | |
| Right Lower Back | -2.996 | 1.171 | -2.558 | 0.011 | -5.29 - -0.70 | |
| Right Elbow | -2.06 | 0.863 | -2.388 | 0.017 | -3.75 - -0.37 | |
| Contiguous Site (back/buttock/hip) | 2.081 | 0.963 | 2.16 | 0.031 | 0.19 - 3.96 | |
| Right Ankle | -1.343 | 0.421 | -3.191 | 0.001 | -2.16 - -0.51 | |
| Control variables | ||||||
| Age group | -0.058 | 0.006 | -9.305 | <.001 | -0.07 - -0.04 | |
| Female sex | -0.082 | 0.021 | -3.83 | <.001 | -0.12 - -0.04 | |
| Transfer from another hospital | 4.501 | 0.038 | 117.097 | <.001 | 4.42 - 4.57 | |
| Transfer from SNF | 0.643 | 0.069 | 9.335 | <.001 | 0.50 - 0.77 | |
| Transfer from Same Hospital | 2.375 | 0.089 | 26.694 | <.001 | 2.20 - 2.54 | |
| (Constant) | 4.386 | 0.039 | 113.506 | <.001 | 4.31 - 4.46 | |
Table 7.
Binary Logistic Regression analysis
| Variable name | B | S.E. | Sig. | OR | 95% CI OR | ||
| PU Stage | |||||||
| Stage 1 | -.258 | .060 | <.001 | .772 | .68 - .86 | ||
| Stage 2 | -.070 | .044 | .115 | .933 | .85 - 1.01 | ||
| Stage 3 | -.087 | .052 | .092 | .916 | .82 - 1.01 | ||
| Stage 4 | -.210 | .055 | <.001 | .811 | .72 - .90 | ||
| PU Anatomical Site | |||||||
| Left Upper Back | 0.84 | 0.27 | <.001 | 2.32 | 1.38 - 3.89 | ||
| Sacral | 0.78 | 0.1 | <.001 | 2.19 | 1.79 - 2.68 | ||
| Unspecified Hip | 0.67 | 0.31 | 0.03 | 1.95 | 1.06 - 3.58 | ||
| Right Hip | 0.28 | 0.14 | 0.05 | 1.32 | 1 - 1.75 | ||
| Unspecified Buttock | 0.62 | 0.14 | <.001 | 1.86 | 1.42 - 2.42 | ||
| Left Buttock | 0.33 | 0.11 | <.001 | 1.39 | 1.12 - 1.73 | ||
| Right Heel | 0.3 | 0.12 | 0.01 | 1.36 | 1.07 - 1.72 | ||
| Head | 0.5 | 0.22 | 0.02 | 1.64 | 1.07 - 2.52 | ||
| Other Site | 0.39 | 0.12 | <.001 | 1.47 | 1.16 - 1.86 | ||
| Unspecified Site | 0.72 | 0.15 | <.001 | 2.05 | 1.54 - 2.74 | ||
| Control Variables | |||||||
| Age Group | .156 | .003 | <.001 | 1.168 | 1.16 - 1.17 | ||
| Female Sex | -.135 | .011 | <.001 | .874 | .85 - .89 | ||
| Transferred from another hospital | .591 | .017 | <.001 | 1.806 | 1.74 - 1.86 | ||
| Transferred from SNF | .472 | .026 | <.001 | 1.603 | 1.52 - 1.68 | ||
| Transferred from same hospital | -.130 | .065 | .046 | .878 | .77 - .99 | ||
| Constant | -4.09 | 0.02 | <.001 | 0.02 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



