Submitted:
13 October 2025
Posted:
14 October 2025
You are already at the latest version
Abstract
Periprosthetic joint infection (PJI) is a serious complication following total joint replacement, with methicillin-resistant Staphylococcus aureus (MRSA) being the primary pathogen. The treatment challenges posed by MRSA's antibiotic resistance further highlight the critical importance of research in this field. Current antibiotic therapies for periprosthetic joint infection caused by Methicillin-Resistant Staphylococcus aureus (MRSA-PJI) are limited by considerable side effects, such as high costs and the development of resistance. Therefore, there is an urgent need to explore novel alternative or adjunctive therapies. This review provides a comprehensive overview of several innovative therapeutic strategies. These include monoclonal therapies that target specific bacterial components; phage therapy, which can either independently or synergistically degrade biofilms and enhance antimicrobial efficacy, characterized by its high specificity; antimicrobial peptides, capable of disrupting bacterial membrane integrity and exhibiting dual antibiofilm activity, with a reduced tendency to induce resistance; as well as nanoparticles and hydrogels, which function as drug delivery systems for sustained release, thereby improving both preventive and therapeutic outcomes. However, these novel therapies also face challenges such as high production costs and limited stability, underscoring the need for further research and optimization. Future efforts should focus on additional studies, clinical trials, and the development of robust regulatory frameworks to fully realize the potential of these treatments for MRSA-PJI.
Keywords:
prosthetic joint infection
; methicillin-resistant Staphylococcus aureus
; enhanced therapy
; new therapy
1. Introduction
Total joint replacement (TJR) is considered one of the most successful surgical interventions in medical history and remains the optimal treatment for end-stage large joint diseases. The number of such surgeries is expected to double in the next decade [1]. However, the rising volume of total joint arthroplasty is associated with a corresponding increase in the incidence of postoperative complications [2].
Periprosthetic joint infection (PJI) is one of the most severe complications following TJR and represents a major challenge in contemporary orthopedics [3]. The percentages of PJI attributed to Total Knee Arthroplasty and total hip arthroplasty are very high [4]. A key feature of PJI is the presence of bacterial biofilms on the joint prosthesis, and the core of clinical treatment focuses on eradicating the biofilms formed by bacterial infections [5,6]. Research has shown that methicillin-resistant Staphylococcus aureus (MRSA) is one of the leading pathogens responsible for PJI, accounting for 25% of all pathogenic microorganisms involved [7]. Its multidrug-resistant characteristics significantly complicate treatment, leading to high recurrence rates and prosthesis removal rates. Furthermore, MRSA is also a significant risk factor for multiple artificial joint heterotopic PJIs [8].
Staphylococcus aureus is a predominant opportunistic pathogen in both healthcare and community environments and is implicated in a broad spectrum of clinically relevant infections, ranging from superficial skin conditions to severe invasive diseases [9]. Since the 1960s, MRSA has emerged and spread globally, becoming a major cause of bacterial infections [10]. The emergence of MRSA is due to the acquisition of the mec gene on the Staphylococcus chromosome(SCC mec), a mobile genetic element capable of encoding either the mecA or mecC genes [11] (Figure 1). The penicillin-binding protein 2a (PBP2a) encoded by the mecA gene is an enzyme responsible for cross-linking the peptidoglycan in bacterial cell walls. Unlike the PBPs produced by methicillin-sensitive Staphylococcus aureus (PBP1, PBP2, PBP3, and PBP4), PBP2a produced by MRSA has a lower affinity for β-lactam antibiotics, making it ineffective as a target for these drugs (penicillin, cephalosporin and carbapenems) [12]. PBP2a replaces the biosynthetic functions of other PBPs, allowing cell wall synthesis to continue and enabling the bacteria to evade the bactericidal and lytic effects of antibiotics [13]. MRSA causes severe infections, and due to the high incidence and mortality and its antibiotic resistance, the treatment of MRSA infections has become a pressing global public health issue [14].
The treatment of MRSA-induced PJI (MRSA-PJI) primarily involves two approaches: antibiotic therapy and surgical intervention. Surgical procedures, while effective, cause significant physical trauma to patients and increase their financial burden to a certain extent. Additionally, the failure rate of PJI treatment remains high even with the use of one- or two-stage revision surgery following prosthetic joint replacement [15]. These challenges underscore the urgent need for non-surgical therapeutic alternatives. Currently, the most commonly used antibiotics for MRSA-PJI are vancomycin, linezolid, and daptomycin [16,17,18,19,20]. However, these traditional targeted antibiotics have significant drawbacks, including high costs, toxic side effects, complex treatment regimens, and the exacerbation of resistance development, all of which negatively impact patient prognosis. The development and approval for marketing of new antibiotics is costly and eventually subject to the onset of resistance. Therefore, the exploration of novel alternative or adjunct therapies is necessary.
This review provides a thorough and critical analysis of current literature on emerging therapies for MRSA-PJI (Figure 2), with the aim of fostering innovation in their clinical application and further development. The significance of these novel therapeutic strategies extends well beyond clinical implementation. Not only do these novel strategies could offer opportunities for healthcare professionals to refine existing treatment protocols or introduce groundbreaking approaches for eradication of MRSA-PJI, but they also hold the promise of improved cure rates, better long-term outcomes, enhanced quality of life, and reduced socioeconomic burdens for patients. Moreover, the successful translation of these therapies may effectively integrate foundational research with clinical applications, thereby stimulating interdisciplinary innovation across areas including molecular medicine, clinical infectiology, pharmaceutical sciences, and biomaterials engineering.
2. Novel Therapeutics
2.1. Monoclonal Antibody Therapy
Therapeutic monoclonal antibodies (mAbs) typically belong to the class of γ-immunoglobulins (IgG). IgG is a Y-shaped 150 kDa immunoglobulin composed of two identical heavy and light chains linked by disulfide bonds [21]. The variable regions of each heavy and light chain form antigen-binding sites, known as the antigen-binding fragments (Fab), while the crystallizable fragment (Fc), responsible for the effector function, is composed of two constant structural domains. The antibody selectively binds to the antigen via its variable region, playing a pivotal role in its pharmacological function. Due to its pH-dependent recycling via the neonatal Fc receptor, this bivalent IgG molecule exhibits a long serum half-life.
The mechanism of monoclonal antibodies against MRSA primarily involves specific targeting, localization, bacterial killing, and toxin neutralization. For example, the monoclonal antibody MEDI4893* targeting α-toxin, binds with high affinity to a critical overlapping epitope on the α-toxin, specifically blocking the assembly of the monomer into the heptameric pore structure. This disrupts the critical steps in pore formation, reducing the damage caused by the toxin to lung and immune cells and thereby mitigating the severity of the infection [22]. In a model of influenza-associated MRSA pneumonia, MEDI4893* administered five days after influenza infection (24 hours prior to MRSA infection) significantly improved survival rates when used alone, with even greater efficacy when combined with the anti-influenza hemagglutinin mAb FY1 [23].
Monoclonal antibodies, such as mAb4461 and mAb4497, directed against wall teichoic acid (WTA) in Staphylococcus aureus, specifically recognize and bind to glycosylated GlcNAc residues on the WTA structure. These antibodies recognize the sugar moieties, phosphate groups, and ribitol phosphate backbone units of WTA, thereby binding to the bacterial surface (Figure 3). mAb4461 preferentially binds to the internal sugar moiety of α-1,4-GlcNAc-modified WTA, while mAb4497, due to the flexibility of the ribitol phosphate backbone, cross-recognizes β-1,3/β-1,4-GlcNAc-modified WTA [24]. Wang developed a conjugate by cross-linking the antigen-binding fragments of monoclonal antibodies against WTA with poly-sialic acid (PSA), forming mAbs-PSA conjugates. This conjugate effectively targets and induces calcification on the surface of MRSA, eliminating the bacteria by disrupting MRSA’s energy metabolism and several essential metabolic pathways. Furthermore, the bacterial calcification leads to increased expression of the calcium-binding proteins S100A8/S100A9 in macrophages and monocytes, triggering the activation of these cells to an inflammatory state, thereby promoting bacterial eradication [25].
Monoclonal antibody therapy has demonstrated significant progress in combating MRSA-PJI. Bruce developed a diagnostic-therapeutic monoclonal antibody by conjugating 4497-IgG1 with a radioactive isotope [26]. This mAb specifically targets the site of infection, assisting in imaging while simultaneously binding to the MRSA biofilm and eliminating bacteria via alpha radiation (e.g., bismuth-213). In addition to the aforementioned monoclonal antibody, several others targeting MRSA are currently under investigation.
Based on these studies, monoclonal antibodies exhibit high target specificity, a favorable safety profile, and broad therapeutic windows, underscoring their potential for clinical use in MRSA treatment. Further evaluation in in vivo models of MRSA-PJI is warranted to accelerate their translation from basic research to clinical practice, thereby expanding the range of effective therapeutic strategies for MRSA-PJI. Monoclonal antibodies are commonly delivered to the periprosthetic tissue and mature biofilms of MRSA via intravenous injection [26,27,28], where they specifically accumulate on infected joint prostheses over time [26]. Although antibodies may exhibit high specificity, the required dosage for effective treatment is typically large [29]. Subcutaneous administration of monoclonal antibodies, however, is hindered by low bioavailability and potential immunogenicity. Furthermore, Bruce van Dijk et al. reported that the biological half-life of free monoclonal antibodies reaches a plateau between 24 to 72 hours [26]. In contrast, liposome-encapsulated monoclonal antibodies exhibit sustained release properties, with continuous release observed even at 42 days [30]. Moreover, liposome-encapsulated monoclonal antibodies effectively protect the subcutaneously administered antibodies from degradation. Future work should focus on further optimizing liposomal formulations to enhance their loading capacity, stability, and release kinetics.
2.2. Phage Therapy
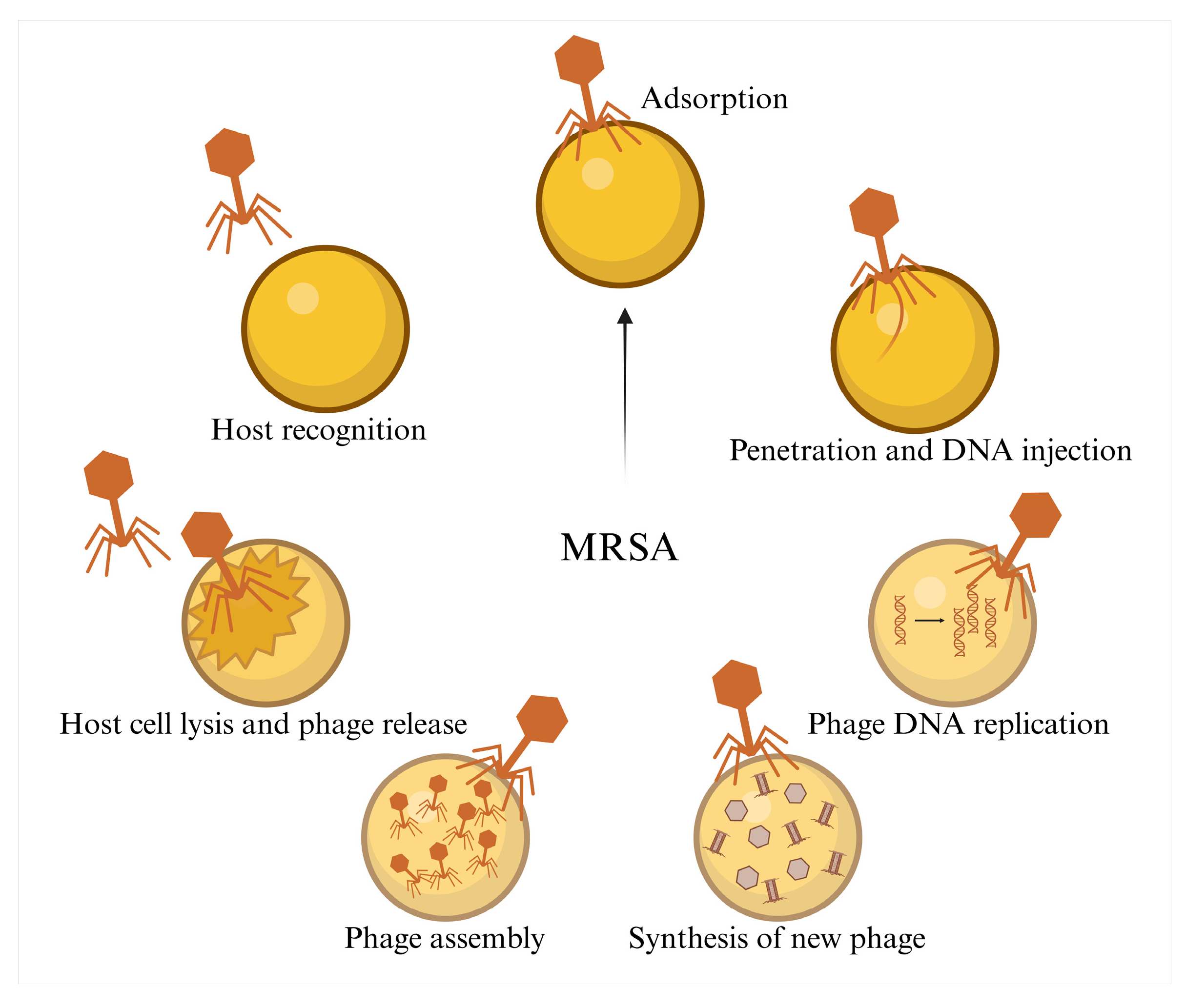
Bacteriophages are viruses with all the common characteristics of viruses and are widely found in various environments [31,32]. The core mechanism of phage therapy against MRSA in the treatment of PJI involves the specific binding of phage tail proteins to bacterial surface receptors, such as the cell wall proteins and teichoic acids of MRSA, or the capsular polysaccharides of PJI-associated bacteria. This binding facilitates the injection of genetic material into the bacterial cell, hijacking the bacterial metabolic system to replicate the phage. Ultimately, the phage mediates bacterial lysis via endolysins (peptidoglycan-hydrolyzing enzymes) and holins (disrupting the cell membrane), releasing progeny phages that continue to infect the surrounding bacteria [33] (Figure 4). Unlike antibiotics, bacteriophages can self-amplify at the site of infection, providing sustained bacterial clearance [34]. One of the therapeutic challenges in treating MRSA-PJI is the formation of biofilms on joint prosthetics, which increase antibiotic resistance. Some phages contain polysaccharide depolymerases in their tail structures, which can degrade the extracellular matrix of biofilm-associated bacteria, effectively disrupting the biofilm and aiding in the colonization of phages around the MRSA biofilm on the prosthetic [35,36].
Phage therapy shows particular promise in treating MRSA-PJI. Zhong isolated a bacteriophage targeting MRSA, called StAP1 [37], which can effectively infect all SCC mec types present in MRSA strains and has shown significant therapeutic efficacy in a murine model of MRSA infection. In a separate study, researchers showed that bacteriophage ØK, which possesses anti-MRSA activity, could be successfully loaded onto orthopedic carbon scaffolds and continuously released over a period of seven days [38]. Additionally, a novel inhalable dry powder formulation has been developed, consisting of porous PLGA microspheres encapsulating heat-resistant phages conjugated with indocyanine green [39]. This formulation has demonstrated potent bactericidal effects against MRSA. Phage therapy is generally well-tolerated. In a treatment study involving 20 patients with drug-resistant mycobacterial infections, no adverse reactions were observed as a result of phage therapy, regardless of the pathogen, the administered phage, or the delivery route [40]. In a Phase 1 clinical trial, researchers administered a phage mixture (AB-SA01) intranasally to nine patients with persistent chronic sinusitis who tested positive for Staphylococcus aureus. The phage therapy was well tolerated, and no deaths were recorded in any group [41]. Furthermore, studies have shown that infection eradication was observed in nine patients, indicating that the treatment is effective.
Figure 4.
The mechanism of phages in combating MRSA.
Moreover, many studies have shown that combining phages with antibiotics results in synergistic effects, reducing the minimum inhibitory concentration (MIC) of resistant strains and improving bacterial clearance efficiency [42,43,44]. For instance, Coyne investigated the synergy between the Romulus bacteriophage and humanized doses of daptomycin and cefazolin. The results demonstrated that the combination of phage and antibiotics exhibited bactericidal activity against MRSA strains without increasing antibiotic resistance post-treatment [45].
Phages offer a promising therapeutic strategy against MRSA-PJI. Currently, direct phage delivery (including intravenous administration and local application) remains the most extensively studied form of phage therapy, particularly in the context of prosthetic joint infections. Compared to antibiotics, phages, when used in combination with antibiotics, not only help eradicate the infection but also prevent its persistence and re-infection [46]. In a murine model of MRSA-induced implant-associated infections, local administration of phages in combination with antibiotics provided sustained effects and eradicated MRSA by day 10 [47]. Additionally, certain phages are capable of degrading biofilms, addressing a core challenge in the treatment of MRSA-PJI. Phage therapy not only has fewer adverse reactions but also exerts less negative impact on the human microbiota compared to antibiotics, which often disrupt the microbial community extensively. Current research has sufficiently demonstrated the potential of phage therapy in treating MRSA-PJI.
2.3. Antimicrobial Peptide Therapy
Antimicrobial peptides (AMPs) are a class of small peptides typically composed of 12 to 50 amino acid residues [48,49]. As biologics, AMPs, identified in a wide range of animal, insect, and plant species, function as host defense peptides and are essential components of innate immunity [50]. AMPs, which have antibiofilm and immunomodulatory properties, are less prone to induce resistance, positioning them as promising candidates for next generation of antimicrobial agents [51,52]. AMPs possess a complex mechanism of action, targeting the cell wall, cell membrane, and various intracellular components, as well as inhibiting biofilm formation and modulating host immune system activity [53].
AMPs have shown promising efficacy in combating MRSA and have been applied in animal models of PJI. GN1 is a potent and non-toxic antimicrobial peptide that counteracts resistance mechanisms in MRSA by inhibiting both the production and enzymatic activity of key resistance determinants. By reversing these resistance traits, GN1 restores the susceptibility of MRSA to low concentrations of multiple β-lactam antibiotics [54]. Additionally, Songnaka isolated a novel antimicrobial peptide from the soil bacterium Brevibacillus sp. SPR-20, which inhibits MRSA at concentrations ranging from 2-32 μg/mL by inducing bacterial membrane damage [55]. Pavel demonstrated, in animal models, that embedding antimicrobial peptides into bone cement effectively prevents MRSA attachment and inhibits over 80% of biofilm formation on the implant surface [56]. In a rabbit PJI model infected with Staphylococcus aureus, the antimicrobial peptide PR-39 exhibited strong antibacterial effects [57]. On days 7 and 14 post-PJI, the treated group showed significantly reduced erythrocyte sedimentation rates and C-reactive protein levels compared to the control group, which did not receive antimicrobial peptide treatment.
These examples highlight that AMPs possess broad-spectrum antibiofilm activity, making them highly suitable for the treatment of MRSA-PJI. Moreover, AMPs can synergize with antibiotics, reducing dosage and toxicity. Given their potential for structural modification, AMPs offer great promise for optimizing their activity and stability. Antimicrobial peptide therapy shows broad potential for the treatment of MRSA-PJI, and future research should focus on in vivo testing of AMPs in clinically representative MRSA-PJI models.
3. Emerging Therapeutic Approaches
3.1. Nanoparticles
Nanoparticles are materials with particle sizes ranging from 1 to 100 nanometers in diameter [58]. Due to their high surface-to-volume ratio, nanoparticles exhibit a variety of novel properties, including mechanical, chemical, electrical, optical, and magnetic characteristics. These properties enable nanoparticles to target multiple bacterial sites, thereby enhancing their antimicrobial efficacy against both resistant and susceptible bacteria [59]. Furthermore, nanoparticle-based materials can serve as carriers to improve the bioavailability and effectiveness of antibiotics [60].
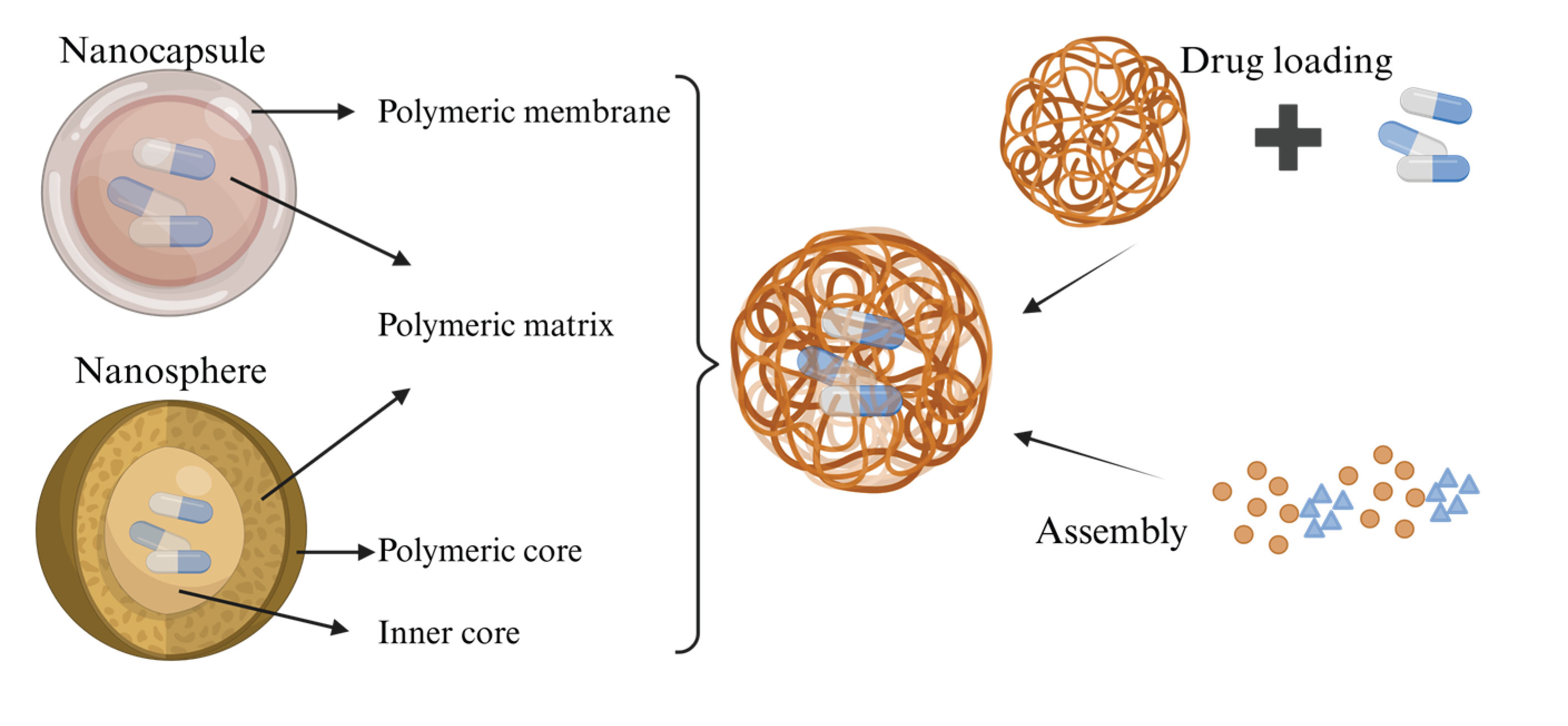
Nanoparticles encompass both nanocapsules and nanospheres, which differ in their morphology. Nanocapsules consist of an oily core in which the drug is typically dissolved, surrounded by a polymer shell that regulates the release profile of the drug from the core [61]. Nanospheres, on the other hand, are based on a continuous polymer network, within which the drug may be retained internally or adsorbed onto the surface. When used as carriers, strategies for synthesizing nanoparticle polymers include post-loading and co-loading approaches [62] (Figure 5).
Nanoparticles have demonstrated exceptional performance as delivery systems in combating MRSA infections. Guevara reported a formulation of PLGA nanoparticles loaded with antibiotics, which can induce sustained and controlled antibiotic release, resulting in prolonged antimicrobial activity against MRSA and Pseudomonas aeruginosa. This controlled and sustained antimicrobial effect is precisely what is urgently needed for the prevention and treatment of MRSA-PJI. Beyond its use in post-infection treatment, local delivery following joint replacement surgery can enable the sustained release of antibiotics around the prosthetic joint, offering a preventative strategy against the development of MRSA-PJI. In animal models, nanoparticles triggered by infection microenvironments, along with thermal-enhanced chemokinetic therapy and M1 macrophages, were effective in controlling MRSA-induced infections [63]. These findings highlight the promising potential of nanoparticles as a new enhancement therapy, demonstrating remarkable prospects in MRSA treatment. However, nanoparticle therapy carries the potential for adverse local tissue reactions. For instance, nanoparticles are prone to recognition and uptake by the mononuclear phagocyte system (MPS), leading to localized toxicity in organs such as the liver and spleen [64]. Macrophages in the liver, spleen, and bone marrow, which constitute the core of the MPS, are the primary sites for nanoparticle clearance. Upon intravenous injection, serum proteins (e.g., opsonins) adsorb onto the surface of nanoparticles, which are then recognized and internalized by scavenger receptors on macrophages, causing the particles to be cleared from circulation. Nanoparticles that are unPEGylated, charged (especially negatively charged), or possess abnormal sizes (either 250 nm) are more readily cleared by the MPS [65]. The half-life of nanoparticles is primarily determined by their physicochemical properties (e.g., particle size, surface modifications, composition) and the route of administration. The core function is to enhance accumulation in target tissues (such as tumors) by prolonging circulation time. For example, nanoparticles within the 10-200 nm size range can avoid renal filtration while reducing recognition and clearance by the MPS (macrophages in the liver and spleen). Particles larger than 200 nm may activate the complement system, triggering rapid clearance. Thus, the 10-200 nm range is optimal for achieving extended half-lives [66]. As research progresses in understanding the impact of nanoparticle size on interactions with the human body, the occurrence of adverse local tissue reactions can be minimized. Researchers are advancing towards establishing nanoparticles as a standard tool for clinical diagnostic imaging and drug delivery.
3.2. Hydrogels
Hydrogels have emerged as pivotal drug delivery vehicles owing to their highwater content, excellent biocompatibility, and three-dimensional network structure. These attributes not only improve drug stability but also enable sustained release profiles through strong interfacial adhesion. Stimuli-responsive hydrogels facilitate precise and targeted drug release, allowing localized delivery to specific sites such as areas of inflammation or the gastrointestinal tract. This site-specific approach markedly reduces systemic toxicity [67].
The use of hydrogels as drug delivery systems has shown promise in addressing MRSA infections. Researchers reported a copper-containing chitosan hydrogel that, when applied in 3D-printed scaffolds, significantly accelerated bone repair and eradicated MRSA-associated infections in both the cranial bone defect repair model and the ectopic MRSA infection model in Sprague-Dawley rats [68]. Another hybrid antimicrobial gel, designed for chronic wound healing, not only promoted cell proliferation and macrophage polarization to the M2 phenotype but also exhibited strong antibacterial activity against Gram-positive bacteria. This hydrogel accelerated skin regeneration in diabetic and burn patients with MRSA infections by enhancing the regenerative responses of M2 macrophages, reducing inflammation, and promoting angiogenesis [69]. Tu developed a multifunctional hydrogel by crosslinking hyperbranched poly(L-lysine)-modified manganese dioxide nanocatalysts with hydrophilic polymer (PEGMA-co-GMA-co-AAm), which effectively inhibited bacterial quorum sensing systems, downregulated virulence genes, and disrupted bacterial metabolism. This hydrogel killed 94.1%–99.5% of MRSA even at 10^9 CFU/mL [70]. Additionally, a FABA hydrogel, made by self-crosslinking Si-Ca-Cu nanoglass modified with F127-CHO (FA) and sodium alendronate, significantly inhibited MRSA growth in vitro, while demonstrating excellent cell and blood compatibility [71]. Furthermore, a multifunctional hydrogel wound dressing was evaluated in vivo, showing excellent hemostatic, antibacterial, and healing-promoting effects in rat models of brain ventricle perforation and full-thickness skin defects infected with MRSA [72]. Two case reports on the use of antibiotic-loaded hydrogels for the treatment of PJI/MRSA-associated orthopedic device infections employed a local delivery approach (targeting the infection site to minimize systemic side effects and enhance therapeutic efficacy). The results demonstrated that hydrogels significantly increased local antibiotic concentrations and achieved sustained-release effects [73,74]. Hydrogels not only facilitate sustained drug release to prolong therapeutic half-lives but also allow for targeted delivery, rendering them highly suitable for the management of MRSA-PJI.
In the future, through continuous optimization of material design, exploration of underlying mechanisms, and collaborative progress in clinical translation, nanoparticle and hydrogel-based therapies will realize their full clinical potential in the fight against MRSA-PJI.
4. Discussion
PJI is a highly destructive complication following total joint replacement, with a high incidence and disability rate that not only severely impairs patients' quality of life but also poses a significant challenge to clinical diagnosis and treatment [75]. Clinical practice has shown that the core issue in PJI treatment failure lies in the formation of biofilms by bacteria colonizing the surface of the joint prosthesis [76]. It is noteworthy that MRSA, one of the primary pathogens responsible for PJI, poses an even greater therapeutic challenge due to its intrinsic multi-drug resistance. This characteristic has made MRSA as a focal point of concern in both orthopedic and microbiological research [77]. Currently, the traditional treatment approach for MRSA-PJI has clear limitations. Although surgical intervention remains essential to remove infectious foci, it is often associated with substantial tissue trauma and prolonged postoperative recovery. Moreover, the prevailing antibiotic strategies face multiple challenges: existing anti-MRSA agents are generally costly and exhibit notable side effects, which not only elevate the economic burden on patients but may also compromise clinical outcomes due to adverse drug reactions. The development process and marketing approval by regulatory agencies involve long timelines, making it difficult to rapidly meet clinical demands. Given these treatment limitations, this review explores new therapeutic strategies for MRSA-PJI, aiming to provide insights and references for overcoming current clinical bottlenecks and optimizing treatment regimens.
Monoclonal antibody therapy has already seen widespread application in the medical field. According to Umabs Antibody Therapy Database, China has 653 institutions engaged in monoclonal antibody drug development, ranking first in Asia and second globally, following the United States. To date, at least 212 monoclonal antibody therapies have been approved worldwide, benefiting millions of patients and demonstrating the transformative impact of monoclonal antibodies [78]. Moreover, the discovery of phage display technology has greatly accelerated the process of discovering therapeutic monoclonal antibodies. Phage display enables the identification of antibodies targeting nearly any target or epitope, including those that are toxic or non-immunogenic in animal immunity [79]. Amid the ongoing global COVID-19 pandemic, Ji Woong Kim used phage display to develop four specific human monoclonal antibodies targeting the receptor-binding domain of the SARS-CoV-2 spike protein [80]. Mary R. Ferguson utilized phage display to develop a monoclonal antibody targeting Treponema pallidum BamA protein, demonstrating superior activity [81]. Monoclonal antibodies, as specific agents against resistant bacteria, offer strong targeting capabilities with minimal side effects. As clinical research progresses, they are expected to play an increasingly important role in the treatment of various infections and diseases.
However, compared to small molecule drugs, monoclonal antibodies generally have low to moderate bioavailability, which may be due to their degradation by proteases in tissue fluids or the lymphatic system [82] (Table 1). Researchers could focus more on utilizing biomaterials such as nanoparticles and hydrogels for drug delivery, which would improve bioavailability and enhance drug stability. In such delivery systems, synergistic use of novel drugs and antibiotics could be achieved to improve therapeutic outcomes and reduce toxicity. Additionally, the high cost of monoclonal antibodies remains a challenge (Table 1). Future research may focus on phage expression systems, which could lower the cost of monoclonal antibodies through in vitro production, thus increasing the potential for clinical translation. This would help reduce the economic burden on patients and their overall quality of life.
Currently, research on phage therapy is progressing rapidly, with applications expanding into fields such as medical diagnostics, biological control, agriculture, nanotechnology, and drug discovery [83]. Phage therapy’s high specificity for target bacteria provides a promising new approach for treating MRSA-PJI. Claudia Ramirez-Sanchez et al. reported a successful case in which a two-stage exchange surgery for persistent methicillin-sensitive Staphylococcus aureus prosthetic joint infection was successfully treated following a second round of phage therapy [84]. The therapeutic application of phage therapy in MRSA-PJI is highly promising.
However, incorporating phage therapy into standard MRSA-PJI treatment protocols faces significant challenges (Table 1). The integration of genomics with machine learning-driven bioinformatics has already seen widespread use in cancer and other biomedical fields, and the latest advancements in machine learning-driven synthetic biology may further promote phage therapy as a viable clinical treatment option. Additionally, developing broad-spectrum phages is a potential solution. CRISPR technology could be used to engineer phages to expand their host range (e.g., knocking out receptor-binding protein genes). Immunogenicity also remains a concern, as the immune system could neutralize phages over time. Some researchers suggest engineering receptor-binding proteins and related domains through genomic techniques to redirect phage specificity and avoid resistance [85].
Although AMP therapy has shown several advantages for treating MRSA-PJI, it still faces limitations (Table 1). While AMPs have unique mechanisms of action, prolonged use may induce bacterial resistance (e.g., MRSA may resist peptides by upregulating efflux pumps or altering membrane phospholipid composition), necessitating monitoring of resistant strains and the development of new mechanisms targeting specific pathogens to reduce resistance risk [86,87]. AMPs also encounter challenges such as limited bioavailability and short half-lives. Researchers need to explore material science to address these issues, potentially by delivering AMPs through biomaterial carriers to improve bioavailability and extend half-lives [88,89]. For instance, designing nanoparticle carriers (e.g., liposomes or polymer micelles) for MRSA infections could enable targeted delivery of AMPs to the infection site, extending their half-life and improving bioavailability. High clinical translation barriers remain for AMP therapy. Researchers need to conduct more clinical trials to evaluate the safety and efficacy of AMPs for MRSA-PJI treatment. Overall, as emerging antimicrobial agent, AMPs offer distinct advantages and open new avenues for the management of infections.

Table 1.
Mechanisms and Advantages/Disadvantages of Three Novel Drugs.
| Treatment Strategy | Mechanism | Advantages | Disadvantages |
|---|---|---|---|
| Monoclonal Antibodies | Specific antibodies targeting resistant bacteria | Strong specificity, low side effects | High production cost, low bioavailability |
| Phage Therapy | Utilizing viruses to directly kill resistant bacteria | Strong targeting, effective against resistant bacteria | Narrow host range, potential for immune rejection |
| Antimicrobial Peptides | Disrupting cell membranes or cell walls leading to cell lysis | Low toxicity, strong thermal stability | Long-term use may induce bacterial resistance, Poor bioavailability, short half-life |
Nanoparticles and hydrogels, as novel enhancement therapies, have already been widely applied across multiple therapeutic areas and have shown great potential in treating MRSA-PJI [90]. However, several challenges remain for these emerging therapeutic approaches, particularly the “delivery efficiency - safety - efficacy persistence” bottleneck. Liang et al. reported the development of VZZ-8 NPs, which in vitro studies demonstrated to effectively eradicate 93.84 ± 7.38% of MRSA and inhibit biofilm formation by 95.36 ± 0.13%. In a murine model of MRSA-induced PJI, VZZ-8 NPs exhibited robust antibacterial efficacy, concurrently suppressing local TNF-α and IL-6 expression, and preventing infection-induced osteolysis, highlighting their comprehensive therapeutic potential for PJI treatment [91]. Additionally, locally administered daptomycin-loaded nanoparticles were shown to sterilize infection sites in MRSA-infected rabbit osteomyelitis models after a single dose, with effective outcomes at both 4 and 14 days post-treatment [92]. Similarly, Boot et al. reported that a hyaluronic acid hydrogel loaded with gentamicin and vancomycin successfully eradicated chronic methicillin-resistant Staphylococcus aureus orthopedic infections in a sheep model through local administration [93]. Future research should focus on clinically relevant studies, including the development of MRSA-PJI animal models that closely mimic clinical conditions, and systematically evaluating the safety and antimicrobial efficacy of these therapies. This will pave the way for their clinical application.
The field of prosthetic joint infection management is at a pivotal juncture, with an unprecedented wave of clinical research challenging fundamental therapeutic assumptions and introducing novel treatment paradigms [94]. Currently, emerging technologies such as artificial intelligence (AI) are being widely applied across various fields. The development, optimization, and application of AI-enabled novel therapies may herald a promising direction for future therapeutic innovation. Researchers have already proposed machine learning-based methods that successfully predict AMPs within the global microbiome, identifying nearly a million prokaryotic AMP sequences and providing a rich resource for antimicrobial peptide synthesis [95]. With the integration of artificial intelligence, the design of hydrogels is undergoing significant transformation, driven by advances in human–machine interaction, machine learning, neural networks, and 3D/4D printing technologies [96]. Additionally, various biomaterials, including platelet-derived materials, plant fibers, and synthetic analogs of natural antimicrobial peptides, have demonstrated remarkable antimicrobial properties [97,98,99]. It is foreseeable that combining novel drugs with these biomaterials, together with the integration of advanced tools like AI will provide more diverse and effective treatment options for MRSA-PJI. In addition, the novel therapies discussed in this article represent potential treatment strategies for a variety of diseases, including COVID-19 [100], cancer [101], and refractory bacterial infections [102], offering broad prospects for clinical application.
Author Contributions
X.X. & X.J. were responsible for the main writing and formatting of the manuscript. Q.Y. and L.Z. conducted the collection, organization, and illustration of the data. Y.W. and T.W. performed the preliminary review and revisions of the article. X.S. was in charge of resource acquisition and the review and revision of the manuscript. All authors have reviewed the final version of the manuscript and agree to its publication.
Funding (Acknowledgments)
Hubei Provincial Natural Science Foundation (2025AFD256);.Yichang Medical and Health project Project (A24-2-056);.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| TJR | Total joint replacement |
| PJI | Periprosthetic Joint Infection |
| MRSA | Methicillin-Resistant Staphylococcus Aureus |
| PBP2a | The mec gene on the Staphylococcus chromosome |
| MRSA-PJI | Periprosthetic Joint Infection caused by Methicillin-Resistant Staphylococcus Aureus |
| mAbs | Monoclonal Antibodies |
| IgG | Gamma Immunoglobulin |
| Fab | Antigen-Binding Fragment |
| Fc | Crystallizable Fragment |
| AMP | Antimicrobial Peptides |
| MPS | mononuclear phagocyte system |
| PSA | Poly-sialic acid |
| AI | artificial intelligence |
References
- Baratta, J. L., Deiling, B., Hassan, Y. R., et al. (2023). Total joint replacement in ambulatory surgery. Best practice & research. Clinical anaesthesiology, 37(3), 269-284. [CrossRef]
- Vrancianu, C. O., Serban, B., Gheorghe-Barbu, I., et al. (2023). The Challenge of Periprosthetic Joint Infection Diagnosis: From Curren t Methods to Emerging Biomarkers. International journal of molecular sciences, 24(5), 4320. [CrossRef]
- Magruder, M. L., Heckmann, N. D., Lieberman, J. R., et al. Novel Technologies in Periprosthetic Joint Infections: Emerging Therap eutics. The Journal of arthroplasty, S0883-5403(0825)00837-X. [CrossRef]
- Tornero, E., García-Ramiro, S., Martínez-Pastor, J. C., et al. Prophylaxis with teicoplanin and cefuroxime reduces the rate of prosth etic joint infection after primary arthroplasty. Antimicrobial agents and chemotherapy, 59(2), 831-837. [CrossRef]
- Tillander, J. A. N., Rilby, K., Svensson Malchau, K., et al. Treatment of periprosthetic joint infections guided by minimum biofilm eradication concentration (MBEC) in addition to minimum inhibitory co ncentration (MIC): protocol for a prospective randomised clinical tria l. BMJ open, 12(9), e058168. [CrossRef]
- Hieda, Y., Choe, H., Maruo, A., et al. Clinical outcomes of continuous local antibiotic perfusion in combinat ion with debridement antibiotics and implant retention for periprosthe tic hip joint infection. Scientific reports, 15(1), 26017. [CrossRef]
- Hu, L., Fu, J., Zhou, Y., et al. (2023). Microbiological profiles and antibiotic resistance of periprosthetic j oint infection after hip replacement in patients with fracture or non- fracture: A comparative study. Journal of back and musculoskeletal rehabilitation, 36(1), 147-154. [CrossRef]
- Li, Y., Quan, X., Zhou, C., et al. Risk factors for metachronous periprosthetic joint infection in patien ts with multiple prosthetic joints: a systematic review and meta-analy sis. Journal of orthopaedic surgery and research, 20(1), 293. [CrossRef]
- Xu, Z. 1,2,3-Triazole-containing hybrids with potential antibacterial activit y against methicillin-resistant Staphylococcus aureus (MRSA). European journal of medicinal chemistry, 206, 112686. [CrossRef]
- Lee, A. S., de Lencastre, H., Garau, J., et al. Methicillin-resistant Staphylococcus aureus. Nature reviews. Disease primers, 4, 18033. [CrossRef]
- Peacock, S. J., Paterson, G. K. Mechanisms of Methicillin Resistance in Staphylococcus aureus. Annual review of biochemistry, 84, 577-601. [CrossRef]
- Sun, Z., Hu, L., Sankaran, B., et al. (2018). Differential active site requirements for NDM-1 β-lactamase hydrolysis of carbapenem versus penicillin and cephalosporin antibiotics. Nature Communications, 9(1), 4524. [CrossRef]
- Lai, L.-Y., Satishkumar, N., Cardozo, S., et al. Altered PBP4 and GdpP functions synergistically mediate MRSA-like high -level, broad-spectrum β-lactam resistance in Staphylococcus aureus. mBio, 15(5), e0288923. [CrossRef]
- Ju, Y., An, Q., Zhang, Y., et al. Recent advances in Clp protease modulation to address virulence, resis tance and persistence of MRSA infection. Drug discovery today, 26(9), 2190-2197. [CrossRef]
- Piuzzi, N. S., Klika, A. K., Lu, Q., et al. Periprosthetic joint infection and immunity: Current understanding of host-microbe interplay. Journal of orthopaedic research : official publication of the Orthopae dic Research Society, 42(1), 7-20. [CrossRef]
- Liang, S., Pan, Y., Wang, J., et al. Bone-targeting ZIF-8 based nanoparticles loaded with vancomycin for th e treatment of MRSA-induced periprosthetic joint infection. Journal of controlled release : official journal of the Controlled Rel ease Society, 385, 113965. [CrossRef]
- Joel, J., Graham, S. M., Peckham-Cooper, A., et al. Clinical results of linezolid in arthroplasty and trauma MRSA related infections. World journal of orthopedics, 5(2), 151-157. [CrossRef]
- Jiang, G., Wang, W., Yang, Y., et al. Organism profiles and empirical treatments for periprosthetic joint in fections. Journal of orthopaedic surgery and research, 20(1), 698. [CrossRef]
- Chang, Y.-J., Lee, M. S., Lee, C.-H., et al. Daptomycin treatment in patients with resistant staphylococcal peripro sthetic joint infection. BMC infectious diseases, 17(1), 736. [CrossRef]
- Kuo, F.-C., Yen, S.-H., Peng, K.-T., et al. Methicillin-resistant Staphylococcal periprosthetic joint infections c an be effectively controlled by systemic and local daptomycin. BMC infectious diseases, 16, 48. [CrossRef]
- Buss, N. A. P. S., Henderson, S. J., McFarlane, M., et al. Monoclonal antibody therapeutics: history and future. Current opinion in pharmacology, 12(5), 615-622. [CrossRef]
- Tkaczyk, C., Hua, L., Varkey, R., et al. Identification of anti-alpha toxin monoclonal antibodies that reduce t he severity of Staphylococcus aureus dermonecrosis and exhibit a corre lation between affinity and potency. Clinical and vaccine immunology : CVI, 19(3), 377-385. [CrossRef]
- Robinson, K. M., Ramanan, K., Tobin, J. M., et al. Survival during influenza-associated bacterial superinfection improves following viral- and bacterial-specific monoclonal antibody treatment. JCI insight, 4(14), e125554. [CrossRef]
- Di Carluccio, C., Soriano-Maldonado, P., Berni, F., et al. Antibody Recognition of Different Staphylococcus aureus Wall Te ichoic Acid Glycoforms. ACS central science, 8(10), 1383-1392. [CrossRef]
- Zhang, W., Liu, L., Zhang, Q., et al. Inducing bacterial calcification for systematic treatment and immunomo dulation against methicillin-resistant Staphylococcus aureus. Nature biotechnology, 10.1038/s41587-41025-02736-41583. [CrossRef]
- van Dijk, B., Hooning van Duyvenbode, J. F. F., de Vor, L., et al. Evaluating the Targeting of a Staphylococcus-aureus-Infected Im plant with a Radiolabeled Antibody In Vivo. International journal of molecular sciences, 24(5), 4374. [CrossRef]
- Qin, L., Hu, N., Zhang, Y., et al. Antibody-antibiotic conjugate targeted therapy for orthopedic implant- associated intracellular S. aureus infections. Journal of advanced research, 65, 239-255. [CrossRef]
- Hansel, T. T., Kropshofer, H., Singer, T., et al. The safety and side effects of monoclonal antibodies. Nature reviews. Drug discovery, 9(4), 325-338. [CrossRef]
- Daugherty, A. L., Mrsny, R. J. Formulation and delivery issues for monoclonal antibody therapeutics. Advanced drug delivery reviews, 58(5-6), 686-706. [CrossRef]
- Karimi, M., Aslanabadi, A., Atkinson, B., et al. Subcutaneous liposomal delivery improves monoclonal antibody pharmacok inetics in vivo. Acta biomaterialia, 195, 522-535. [CrossRef]
- Kakasis, A., Panitsa, G. Bacteriophage therapy as an alternative treatment for human infections . A comprehensive review. International journal of antimicrobial agents, 53(1), 16-21. [CrossRef]
- Strathdee, S. A., Hatfull, G. F., Mutalik, V. K., et al. Phage therapy: From biological mechanisms to future directions. Cell, 186(1), 17-31. [CrossRef]
- Onsea, J., Wagemans, J., Pirnay, J. P., et al. Bacteriophage therapy as a treatment strategy for orthopaedic-device-r elated infections: where do we stand? European cells & materials, 39, 193-210. [CrossRef]
- Young, J., Lee, S. W., Shariyate, M. J., et al. Bacteriophage therapy and current delivery strategies for orthopedic i nfections: A SCOPING review. The Journal of infection, 88(3), 106125. [CrossRef]
- Pires, D. P., Oliveira, H., Melo, L. D. R., et al. Bacteriophage-encoded depolymerases: their diversity and biotechnologi cal applications. Applied microbiology and biotechnology, 100(5), 2141-2151. [CrossRef]
- Kim, S. G., Giri, S. S., Yun, S., et al. (2020). Synergistic phage–surfactant combination clears IgE-promoted Staphylococcus aureus aggregation in vitro and enhances the effect in vivo. International journal of antimicrobial agents, 56(1). [CrossRef]
- Lu, Y., Lu, Y., Li, B., et al. StAP1 phage: an effective tool for treating methicillin-resistant Staphylococcus aureus infections. Frontiers in microbiology, 14, 1267786. [CrossRef]
- Arens, D. K., Rodriguez, A. R., Huh, E. Y., et al. Enhancing orthopedic infection control: carbon scaffold-mediated phage therapy for methicillin-resistant staphylococcus aureus in fracture-r elated infections. Biomedical physics & engineering express, 11(1), 10.1088/2057-1976/ad1089c1087b. [CrossRef]
- Liu, M.-Y., Liu, X., Wang, C.-Y., et al. Inhalable Polymeric Microparticles for Phage and Photothermal Synergis tic Therapy of Methicillin-Resistant Staphylococcus aureus Pneu monia. Nano letters, 24(28), 8752-8762. [CrossRef]
- Dedrick, R. M., Smith, B. E., Cristinziano, M., et al. Phage Therapy of Mycobacterium Infections: Compassionate Use of Phages in 20 Patients With Drug-Resistant Mycobacterial Disease. Clinical infectious diseases : an official publication of the Infectio us Diseases Society of America, 76(1), 103-112. [CrossRef]
- Ooi, M. L., Drilling, A. J., Morales, S., et al. Safety and Tolerability of Bacteriophage Therapy for Chronic Rhinosinu sitis Due to Staphylococcus aureus. JAMA otolaryngology-- head & neck surgery, 145(8), 723-729. [CrossRef]
- Gu Liu, C., Green, S. I., Min, L., et al. Phage-Antibiotic Synergy Is Driven by a Unique Combination of Antibact erial Mechanism of Action and Stoichiometry. mBio, 11(4), e01462-01420. [CrossRef]
- Li, X., He, Y., Wang, Z., et al. (2021). A combination therapy of Phages and Antibiotics: Two is better than one. International Journal of Biological Sciences, 17(13), 3573-3582. [CrossRef]
- Tagliaferri, T. L., Jansen, M., Horz, H.-P. (2019). Fighting Pathogenic Bacteria on Two Fronts: Phages and Antibiotics as Combined Strategy. Frontiers in Cellular and Infection Microbiology, 9. [CrossRef]
- Kunz Coyne, A. J., Stamper, K., Bleick, C., et al. Synergistic bactericidal effects of phage-enhanced antibiotic therapy against MRSA biofilms. Microbiology spectrum, 12(4), e0321223. 0321. [CrossRef]
- Young, J., Lee, S. W., Shariyate, M. J., et al. (2024). Bacteriophage therapy and current delivery strategies for orthopedic infections: A SCOPING review. Journal of Infection, 88(3). [CrossRef]
- Kaur, S., Harjai, K., Chhibber, S. In Vivo Assessment of Phage and Linezolid Based Implant Coatings for T reatment of Methicillin Resistant S. aureus (MRSA) Mediated Orthopaedi c Device Related Infections. PloS one, 11(6), e0157626. [CrossRef]
- Antonelli, B., Chen, A. F. Reducing the risk of infection after total joint arthroplasty: preoper ative optimization. Arthroplasty (London, England), 1(1), 4. [CrossRef]
- Luo, Y., Song, Y. Mechanism of Antimicrobial Peptides: Antimicrobial, Anti-Inflammatory and Antibiofilm Activities. International journal of molecular sciences, 22(21), 11401. [CrossRef]
- Deo, S., Turton, K. L., Kainth, T., et al. Strategies for improving antimicrobial peptide production. Biotechnology advances, 59, 107968. [CrossRef]
- Bin Hafeez, A., Jiang, X., Bergen, P. J., et al. Antimicrobial Peptides: An Update on Classifications and Databases. International journal of molecular sciences, 22(21), 11691. [CrossRef]
- Luo, Y., Song, Y. Mechanism of Antimicrobial Peptides: Antimicrobial, Anti-Inflammatory and Antibiofilm Activities. International journal of molecular sciences, 22(21), 11401. [CrossRef]
- Li, X., Zuo, S., Wang, B., et al. Antimicrobial Mechanisms and Clinical Application Prospects of Antimic robial Peptides. Molecules (Basel, Switzerland), 27(9), 2675. [CrossRef]
- Shi, J., Chen, C., Kong, P., et al. Non-Membrane Active Peptide Resensitizes MRSA to β-Lactam Antibiotics and Inhibits S. aureus Virulence. Advanced science (Weinheim, Baden-Wurttemberg, Germany), 12(15), e2416260. [CrossRef]
- Songnaka, N., Lertcanawanichakul, M., Hutapea, A. M., et al. Purification and Characterization of Novel Anti-MRSA Peptides Produced by Brevibacillus sp. SPR-20. Molecules (Basel, Switzerland), 27(23), 8452. [CrossRef]
- Melicherčík, P., Kotaška, K., Jahoda, D., et al. Antimicrobial peptide in polymethylmethacrylate bone cement as a proph ylaxis of infectious complications in orthopedics-an experiment in a m urine model. Folia microbiologica, 67(5), 785-791. [CrossRef]
- Zhu, Y., Weng, X., Zhang, J., et al. Protective effect of additional cathelicidin antimicrobial peptide PR- 39 on prosthetic-joint infections. Journal of orthopaedic surgery (Hong Kong), 31(2), 10225536231175237. [CrossRef]
- Baetke, S. C., Lammers, T., Kiessling, F. Applications of nanoparticles for diagnosis and therapy of cancer. The British journal of radiology, 88(1054), 20150207. [CrossRef]
- Chen, C.-W., Hsu, C.-Y., Lai, S.-M., et al. Metal nanobullets for multidrug resistant bacteria and biofilms. Advanced drug delivery reviews, 78, 88-104. [CrossRef]
- Salatin, S., Bazmani, A., Shahi, S., et al. Antimicrobial Benefits of Flavonoids and their Nanoformulations. Current pharmaceutical design, 28(17), 1419-1432. [CrossRef]
- Zielińska, A., Carreiró, F., Oliveira, A. M., et al. Polymeric Nanoparticles: Production, Characterization, Toxicology and Ecotoxicology. Molecules (Basel, Switzerland), 25(16), 3731. [CrossRef]
- Liu, Y., Yang, G., Jin, S., et al. Development of High-Drug-Loading Nanoparticles. ChemPlusChem, 85(9), 2143-2157. [CrossRef]
- Fu, S., Yi, X., Li, Y., et al. Berberine and chlorogenic acid-assembled nanoparticles for highly effi cient inhibition of multidrug-resistant Staphylococcus aureus. Journal of hazardous materials, 473, 134680. [CrossRef]
- Hong, Q., Zhang, W., Liu, Z., et al. (2024). Infection microenvironment-triggered nanoparticles eradicate MRSA by thermally amplified chemodynamic therapy and M1 macrophage. Journal of Nanobiotechnology, 22(1), 448. [CrossRef]
- Foster, A. L., Boot, W., Stenger, V., et al. Single-stage revision of MRSA orthopedic device-related infection in s heep with an antibiotic-loaded hydrogel. Journal of orthopaedic research : official publication of the Orthopae dic Research Society, 39(2), 438-448. [CrossRef]
- Bédouet, L., Beilvert, A., Servais, E., et al. Degradable Hydrophilic Poly(ethylene glycol) Microspheres for the Sust ained Delivery of Peptide-Based Antibiotics for Local Anti-infective T herapies. ACS infectious diseases, 11(6), 1673-1685. [CrossRef]
- Yang, Q., Xiang, X., Wang, H., et al. Oral natural material hydrogels: a new strategy for enhancing oral dru g delivery efficiency. Journal of biomaterials science. Polymer edition, 1-28. [CrossRef]
- Zhang, J., Ye, X., Li, W., et al. Copper-containing chitosan-based hydrogels enabled 3D-printed scaffold s to accelerate bone repair and eliminate MRSA-related infection. International journal of biological macromolecules, 240, 124463. [CrossRef]
- Liu, W., Gao, R., Yang, C., et al. ECM-mimetic immunomodulatory hydrogel for methicillin-resistant Staphylococcus aureus-infected chronic skin wound healing. Science advances, 8(27), eabn7006. [CrossRef]
- Tu, C., Lu, H., Zhou, T., et al. Promoting the healing of infected diabetic wound by an anti-bacterial and nano-enzyme-containing hydrogel with inflammation-suppressing, ROS -scavenging, oxygen and nitric oxide-generating properties. Biomaterials, 286, 121597. [CrossRef]
- Zhang, L., Niu, W., Lin, Y., et al. Multifunctional antibacterial bioactive nanoglass hydrogel for normal and MRSA infected wound repair. Journal of Nanobiotechnology, 21(1), 162. [CrossRef]
- Cheng, J., Wang, H., Gao, J., et al. First-Aid Hydrogel Wound Dressing with Reliable Hemostatic and Antibac terial Capability for Traumatic Injuries. Advanced healthcare materials, 12(25), e2300312. [CrossRef]
- Indelli, P. F., Iannotti, F., Ferretti, A., et al. "Recommendations for periprosthetic joint infections (PJI) prevention: the European Knee Associates (EKA)-International Committee American A ssociation of Hip and Knee Surgeons (AAHKS)-Arthroplasty Society in As ia (ASIA) survey of members". Knee surgery, sports traumatology, arthroscopy : official journal of t he ESSKA, 30(12), 3932-3943. [CrossRef]
- Brooks, J. R., Dusane, D. H., Moore, K., et al. Pseudomonas aeruginosa biofilm killing beyond the spacer by ant ibiotic-loaded calcium sulfate beads: an in vitro study. Journal of bone and joint infection, 6(5), 119-129. [CrossRef]
- Indelli, P. F., Iannotti, F., Ferretti, A., et al. "Recommendations for periprosthetic joint infections (PJI) prevention: the European Knee Associates (EKA)-International Committee American A ssociation of Hip and Knee Surgeons (AAHKS)-Arthroplasty Society in As ia (ASIA) survey of members". Knee surgery, sports traumatology, arthroscopy : official journal of t he ESSKA, 30(12), 3932-3943. [CrossRef]
- Brooks, J. R., Dusane, D. H., Moore, K., et al. <i>Pseudomonas aeruginosa</i> biofilm killing beyond the spacer by ant ibiotic-loaded calcium sulfate beads: an in vitro study. Journal of bone and joint infection, 6(5), 119-129. [CrossRef]
- Antonelli, B., Chen, A. F. Reducing the risk of infection after total joint arthroplasty: preoper ative optimization. Arthroplasty (London, England), 1(1), 4. [CrossRef]
- han, A. C., Martyn, G. D., Carter, P. J. Fifty years of monoclonals: the past, present and future of antibody t herapeutics. Nature reviews. Immunology, 10.1038/s41577-41025-01207-41579. [CrossRef]
- Zhang, Y. Evolution of phage display libraries for therapeutic antibody discover y. mAbs, 15(1), 2213793. [CrossRef]
- Kim, J. W., Min, S. W., Lee, J., et al. Development and Characterization of Phage-Display-Derived Novel Human Monoclonal Antibodies against the Receptor Binding Domain of SARS-CoV- 2. Biomedicines, 10(12), 3274. [CrossRef]
- Ferguson, M. R., Delgado, K. N., McBride, S., et al. Use of Epivolve phage display to generate a monoclonal antibody with o psonic activity directed against a subdominant epitope on extracellula r loop 4 of Treponema pallidum BamA (TP0326). Frontiers in immunology, 14, 1222267. [CrossRef]
- Keizer, R. J., Huitema, A. D. R., Schellens, J. H. M., et al. Clinical pharmacokinetics of therapeutic monoclonal antibodies. Clinical pharmacokinetics, 49(8), 493-507. [CrossRef]
- Kortright, K. E., Chan, B. K., Koff, J. L., et al. Phage Therapy: A Renewed Approach to Combat Antibiotic-Resistant Bacte ria. Cell host & microbe, 25(2), 219-232. [CrossRef]
- Ramirez-Sanchez, C., Gonzales, F., Buckley, M., et al. Successful Treatment of <i>Staphylococcus aureus</i> Prosthetic Joint Infection with Bacteriophage Therapy. Viruses, 13(6), 1182. [CrossRef]
- Lenneman, B. R., Fernbach, J., Loessner, M. J., et al. Enhancing phage therapy through synthetic biology and genome engineeri ng. Current opinion in biotechnology, 68, 151-159. [CrossRef]
- Erdem Büyükkiraz, M., Kesmen, Z. Antimicrobial peptides (AMPs): A promising class of antimicrobial comp ounds. Journal of applied microbiology, 132(3), 1573-1596. [CrossRef]
- Xuan, J., Feng, W., Wang, J., et al. Antimicrobial peptides for combating drug-resistant bacterial infectio ns. Drug resistance updates : reviews and commentaries in antimicrobial an d anticancer chemotherapy, 68, 100954. [CrossRef]
- Gao, N., Sun, J., Li, X., et al. Overcoming delivery challenges of antimicrobial peptides for clinical translation: From nanocarriers to molecular modifications. Drug resistance updates : reviews and commentaries in antimicrobial an d anticancer chemotherapy, 83, 101289. [CrossRef]
- Sharma, L., Bisht, G. S. Short Antimicrobial Peptides: Therapeutic Potential and Recent Advance ments. Current pharmaceutical design, 29(38), 3005-3017. [CrossRef]
- Gutierrez, A. M., Frazar, E. M., X Klaus, M. V., et al. Hydrogels and Hydrogel Nanocomposites: Enhancing Healthcare through Hu man and Environmental Treatment. Advanced healthcare materials, 11(7), e2101820. [CrossRef]
- Liang, S., Pan, Y., Wang, J., et al. (2025). Bone-targeting ZIF-8 based nanoparticles loaded with vancomycin for the treatment of MRSA-induced periprosthetic joint infection. Journal of Controlled Release, 385, 113965. [CrossRef]
- Jacqueline, C., Caillon, J., Meyer, O., et al. (2021). Efficacy of Nanoencapsulated Daptomycin in an Experimental Methicillin-Resistant Staphylococcus aureus Bone and Joint Infection Model. Antimicrobial agents and chemotherapy, 65(12), 10.1128/aac.00768-00721. [CrossRef]
- Boot, W., Schmid, T., D'Este, M., et al. (2021). A Hyaluronic Acid Hydrogel Loaded with Gentamicin and Vancomycin Successfully Eradicates Chronic Methicillin-Resistant Staphylococcus aureus Orthopedic Infection in a Sheep Model. Antimicrobial agents and chemotherapy, 65(4). [CrossRef]
- Isler, B., Welyczko, Z., Jorgensen, N., et al. Advancing the management of prosthetic joint infections: a review of r andomized controlled trials and emerging evidence. Antimicrobial agents and chemotherapy, 69(10), e0033825. [CrossRef]
- Santos-Júnior, C. D., Torres, M. D. T., Duan, Y., et al. Discovery of antimicrobial peptides in the global microbiome with mach ine learning. Cell, 187(14), 3761-3778.e3716. [CrossRef]
- Li, F., Gan, L., Yang, X., et al. Progress of AI assisted synthesis of polysaccharides-based hydrogel an d their applications in biomedical field. International journal of biological macromolecules, 287, 138643. [CrossRef]
- Jian, T., Wang, M., Hettige, J., et al. Self-Assembling and Pore-Forming Peptoids as Antimicrobial Biomaterial s. ACS nano, 18(34), 23077-23089. [CrossRef]
- Shariati, A., Moradabadi, A., Azimi, T., et al. Wound healing properties and antimicrobial activity of platelet-derive d biomaterials. Scientific reports, 10(1), 1032. [CrossRef]
- Zamora-Mendoza, L., Guamba, E., Miño, K., et al. Antimicrobial Properties of Plant Fibers. Molecules (Basel, Switzerland), 27(22), 7999. [CrossRef]
- Kelley, B., De Moor, P., Douglas, K., et al. Monoclonal antibody therapies for COVID-19: lessons learned and implic ations for the development of future products. Current opinion in biotechnology, 78, 102798. [CrossRef]
- Garfall, A. L. New Biological Therapies for Multiple Myeloma. Annual review of medicine, 75, 13-29. [CrossRef]
- Hatfull, G. F., Dedrick, R. M., Schooley, R. T. Phage Therapy for Antibiotic-Resistant Bacterial Infections. Annual review of medicine, 73, 197-211. [CrossRef]
Figure 1.
The mechanism of MRSA resistance. PBP2a, encoded by the mecA gene, has low affinity for β-lactam antibiotics, making it ineffective as a target for these drugs.
Figure 1.
The mechanism of MRSA resistance. PBP2a, encoded by the mecA gene, has low affinity for β-lactam antibiotics, making it ineffective as a target for these drugs.
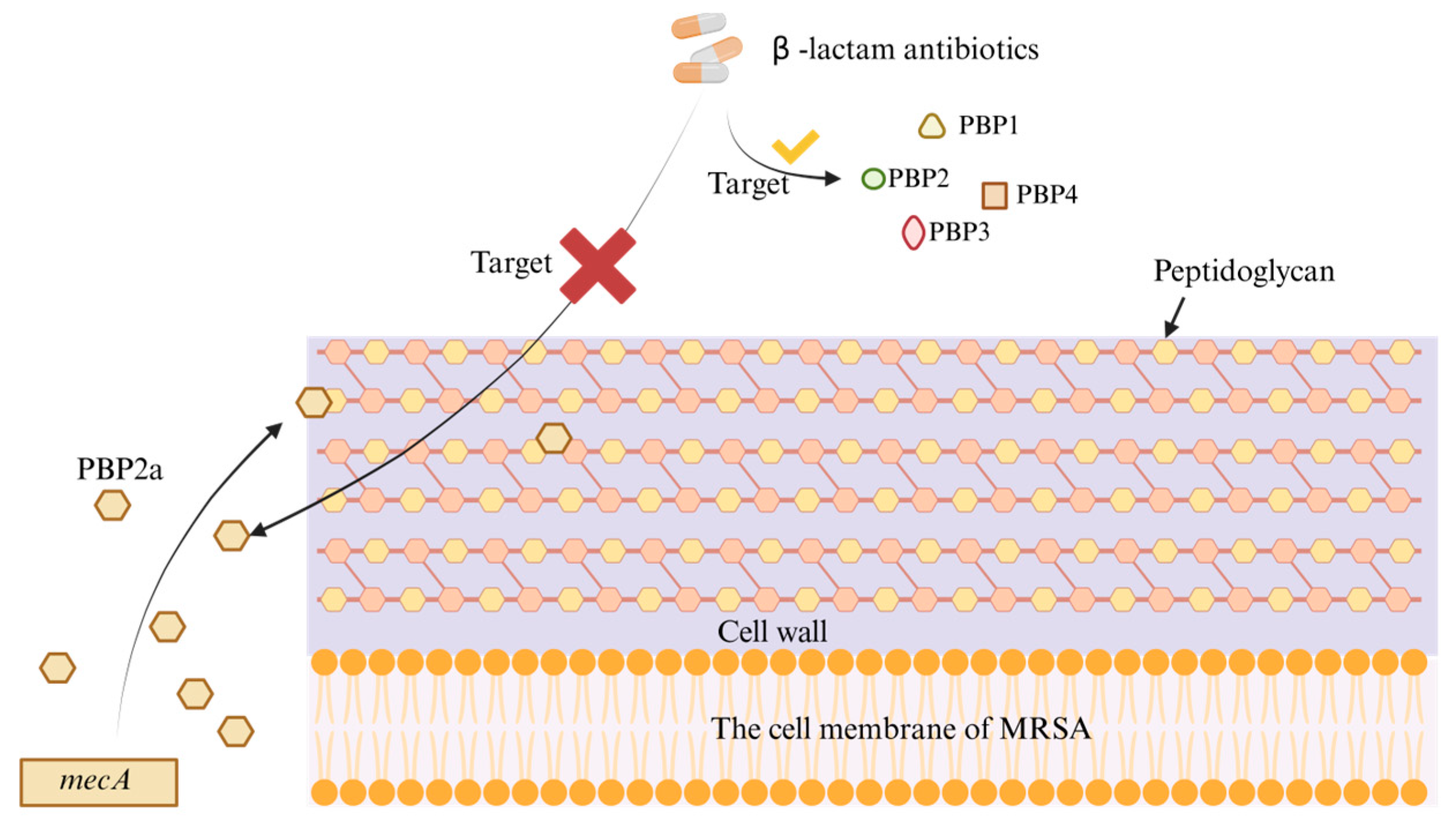
Figure 2.
Schemes of new therapies for MRSA-PJI. The new therapy consists of two parts: new drugs and new enhanced therapies. New drugs include: monoclonal antibodies, bacteriophages, and antimicrobial peptides. New enhanced therapies include nanoparticle delivery and hydrogel delivery.
Figure 2.
Schemes of new therapies for MRSA-PJI. The new therapy consists of two parts: new drugs and new enhanced therapies. New drugs include: monoclonal antibodies, bacteriophages, and antimicrobial peptides. New enhanced therapies include nanoparticle delivery and hydrogel delivery.
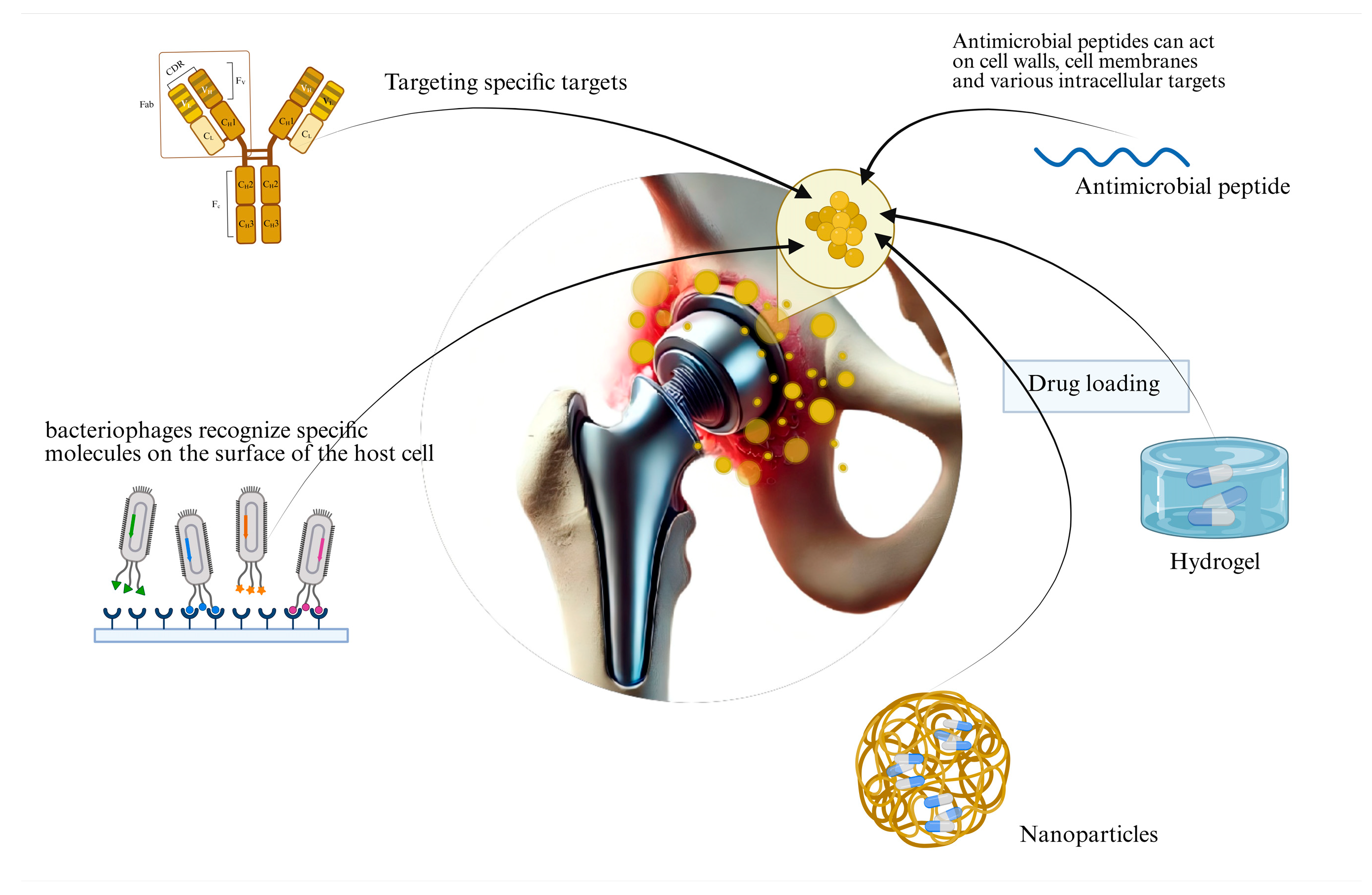
Figure 3.
Schematic diagram of the mechanism of AMPs against WTA.
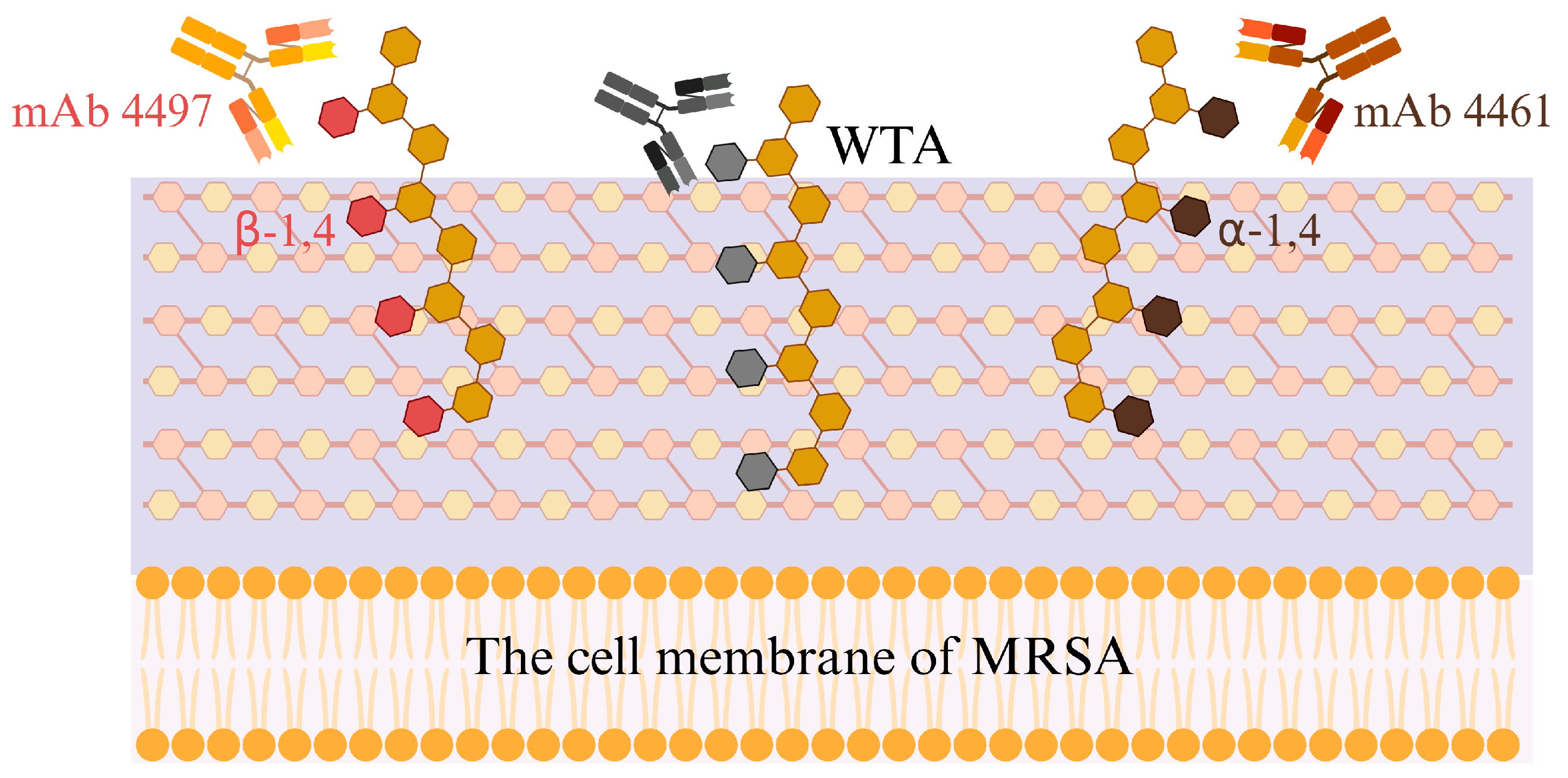
Figure 5.
Synthesis strategies of nanoparticle polymers.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



