Submitted:
26 September 2025
Posted:
29 September 2025
You are already at the latest version
Abstract
Acute Systemic Antimicrobial Prophylaxis (ASAP) is the standard of care for managing open fractures. There is concern that protocols do not address the modern open fracture bioburden. Online databases were searched to estimate the effect size in reducing the risk of postoperative infections in open fracture management stratified by regimen and fracture classification. 2,031 patients from 17 studies were analyzed. Meta-analysis of Type III open fractures suggested that Flucloxacillin + Benzylpenicillin had a lower infection rate than Cefazolin + Gentamicin; furthermore, the duration of hospitalization was extended by four days with Cefazolin + Gentamicin in Type II/III open fractures. No one antibiotic prophylactic regimen can be recommended over another in the management of open fractures with the current available data. We offer methodological guidelines for future trials that will allow robust evidence for future studies.
Keywords:
antibiotics
; open fractures
; Gustilo-Anderson
; fracture related infection
; surgical site infection
; systemic
; intravenous
1. Introduction
Infection rates after open extremity fracture range from 1.8% in Gustilo-Anderson Type I to 40.5% in Type IIIB.[1,2,3,4] Surgical site Infections (SSI) require multifaceted management with the potential for complications that result in a significant clinical burden to patients and high cost to the healthcare system.[5] SSI alone may increase healthcare costs by 1.2 to 6-fold.[6]
Open fracture SSI rates have remained high and relatively unchanged for decades despite the widespread use of accelerated prophylactic antibiosis.[7] Acute systemic antimicrobial prophylaxis (ASAP) regimens have evolved and frequently change depending on geography, hospital system standards, or surgeon practice. There is also concern that traditional and even current antibiotic regimens are not accounting for the modern open fracture bioburden.[8]
Antibiotic stewardship in open fractures has primarily been guided by Gustilo and Anderson’s studies[3,9,10,11,12,13] conducted in 1976, in which they showed that prophylactic antibiotics such as penicillin, streptomycin, chloramphenicol, oxacillin, and kanamycin reduced deep infections from 10% to 5%.[12,13] In 1990, Gustilo et al. recommended two grams of cefazolin or cefamandole upon admission and one gram three times daily for up to 72 hours for Type I injuries. Further recommendations for Gustilo-Anderson (GA) Type II and III open fractures included the addition of 1.5 mg/kg of tobramycin upon admission and 3-5 mg/kg daily for 72 hours.[10]
The Surgical Infection Society (SIS) and the Eastern Association for the Surgery of Trauma (EAST) have also developed literature-based guidelines for ASAP regimens. In 2006, SIS recommended first-generation cephalosporin for 24-48 hours perioperatively for Type I open fractures and 48 hours for Type II and III open fractures. Additionally, the SIS guidelines reported a lack of evidence for gram-negative prophylaxis. A few years later, the EAST guidelines recommended a first-generation cephalosporin for all GA types for no longer than 24 hours after soft tissue coverage for type I and II open fractures and 72 hours for type III open fractures. Additionally, when indicated, an aminoglycoside for gram-negative coverage for GA type III fractures and high-dose penicillin for Clostridium spp. should be added. However, EAST guidelines discouraged using Fluoroquinolones for their non-superiority compared to the cephalosporin/aminoglycoside regimen.[14,15]
Despite these guidelines, there continues to be a lack of standardized ASAP regimens in the open fracture setting. Our meta-analysis aims to delineate which regimen is most effective in preventing SSI and to propose a minimum reporting standard for future studies to minimize evidence heterogeneity.
2. Materials and Methods:
2.1. Protocol
2.2. Search Methodology
A detailed, comprehensive literature search for all relevant studies was performed using several online databases on October 21, 2022: PubMed, MEDLINE via Ovid, Web of Science, Cochrane database, and Science-Direct. The search strategy combined subject headings and free text words such as “open fracture” and “antibiotics” in Ovid MEDLINE, topic searching in Web of Science, and free text words in the other databases. The references of relevant studies (reviews and meta-analyses) were manually examined for any that met our inclusion criteria to ensure the inclusion of all potentially eligible studies.
2.3. Study Selection and Eligibility Criteria
Two independent reviewers scoped the studies’ titles, abstracts, and full-text articles that were in English for their eligibility PICO criteria:
2.4. Population, Intervention, Comparison, and Outcome (PICO) Criteria
- Population: An eligible study should have at least five subjects with Gustilo-Anderson (GA) Type I, II, or III open extremity fractures.
-
Intervention: Any of the following acute systemic antimicrobial prophylaxis (ASAP) protocols.
- Cefazolin alone (Cef)
- Cefazolin + Gentamicin (Cef+Gent)
- Tobramycin + Cefazolin (Tobra+Cef)
- Piperacillin + Tazobactam (Pip+Tazo)
- Ampicillin + Sulbactam (Amp+Sulb)
- Cefazolin + Ciprofloxacin (Cef+Cipro)
- Flucloxacillin + Benzylpenicillin (Flu+Benz)
- Two doses of Cefazolin + Gentamicin (2Cef+Gent)
- Cefamandole + Gentamicin (Cefam+Gent)
- Ciprofloxacin (Cipro)
- Clindamycin (Clinda)
- Cloxacillin (Clox)
- Flucloxacillin (Flu)
- Cephradine (Ceph)
-
Comparison: Each intervention was compared to each other, and the following groups were specified:
-
Single dose of Cefazolin plus Gentamicin (Cef+Gent) versus:
- ➢
- Cefazolin alone (Cef)
- ➢
- Piperacillin plus Tazobactam (Pip+Tazo)
- ➢
- Ampicillin plus Sulbactam (Amp+Sulb)
- ➢
- Cefazolin plus Ciprofloxacin (Cef+Cipro)
- ➢
- Flucloxacillin plus Benzylpenicillin (Flu+Benz)
- ➢
- Two doses Cefazolin plus Gentamicin (2Cef+Gent)
- Cefazolin alone versus Piperacillin plus Tazobactam (Cef vs Pip+Tazo)
- Cefazolin plus Clindamycin versus Piperacillin plus Tazobactam (Cef/Clinda vs Pip+Tazo)
- Clindamycin versus Cloxacillin (Clinda vs Clox)
- Penicillin versus Cephradine (Pen vs Ceph)
- Cefamandole plus Gentamicin versus Ciprofloxacin (Cefa+Gent vs Cipro)
-
- Outcome: Outcome analyses of the included studies must report the post-fixation incidence of surgical site infection (SSI) and acute kidney injury (AKI). The length of hospital stay was considered as our secondary outcome.
2.5. Inclusion Criteria
Inclusion criteria included randomized controlled trials (RCTs), non-randomized prospective, and retrospective observational cohort studies published in English comparing different ASAP protocols following an open fracture.
2.6. Exclusion Criteria
Exclusion criteria included language other than English, article unavailable, or duplicate data/study. Some articles were excluded by reviewing the inclusion criteria in the title or abstract. All other studies required full-text review to determine relevance. Disagreements were resolved by direct communication between the reviewers.
2.7. Data Extraction
The reviewers extracted the required information from all eligible studies included. A data collection spreadsheet was established to analyze quantitative and qualitative data. The data was extracted from clinical studies using the following data variables: 1) demographics and characteristics (author, study design, year of publication, country of study, patient number, age, and female sex), 2) Gustilo-Anderson fracture type, and 3) antibiotic regimens used.
2.8. Quality Assessment of Included Studies (MINORS)
The methodological index for nonrandomized studies (MINORS) was used to assess the quality of the included studies. Full-text versions of included nonrandomized studies were reviewed for methodological quality analysis using the MINORS score. Twelve items were scored as “0” (not reported), “1” (reported but inadequate), or “2” (reported and adequate). Two reviewers independently assessed the quality of the included studies.[18]
2.9. Risk of Bias Assessment of Randomized Controlled Trials
Cochrane Collaboration’s assessment tool for risk of bias from the Cochrane Handbook for systematic reviews was used to assess included RCTs for methodological bias.[17] The following items were considered as ‘low risk,’ ‘high risk,’ or ‘unclear risk’ of bias: (1) random sequence generation (selection bias), (2) allocation concealment (selection bias), (3) blinding of participants and personnel (performance bias), (4) blinding of outcome assessment (detection bias), (5) incomplete outcome data (attrition bias), (6) selective reporting addressed (reporting bias).
2.10. Synthesis of Results
GraphPad Prism (version 9.4.1) was used to calculate the descriptive analysis and perform a linear regression analysis between the publication year and the MINORS score.[19] In cases where the standard deviation was not reported, we calculated the mean, sample size, and range as described in previous literature.[20,21] Continuous variables were presented as mean ± standard deviation (SD), while categorical variables were reported as percentages. Using standard meta-analytic techniques, the authors calculated overall effect size estimates and forest plots based on all studies that provided sufficient data. To estimate the heterogeneity across studies, the I2 values were calculated. If the homogeneity of studies was identified with an I2 <50%, we used the fixed effects model to estimate the overall effects using the RevMan 5.3 software.[22]
3. Results
3.1. Literature Search and Study Selection
Upon the conclusion of our search strategy, there were 5,300 articles. After duplicates were removed, 144 records of full-text articles were screened for eligibility to the inclusion criteria. After screening, 4,189 studies were excluded for not meeting our PICO criteria. After eligibility screening, 17 clinical studies met the inclusion criteria for a qualitative descriptive and quantitative meta-analysis (Supplemental Figure S1).[23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39]
3.2. Characteristics of Included Studies
From 1988 to 2022, 17 studies (4 RCTs, 3 prospective studies, and 10 retrospective studies) were analyzed. These studies included 2,031 patients (70% males), with an average age of 40.0 ± 5.9 years old, ranging from 30-50.7 years old. The average follow-up duration was 9.12 ± 6.40 months, (1.5 – 24 months.)[28,38] 14 unique antibiotic regimens were analyzed in the 17 studies. The average infection rate across all studies was 18.0% (SD=18.0%, range [0-70%]). The feature diagnosis of the CDC definition of surgical site infection (SSI) is found in Supplemental Table S1. The number of patients and the associated dose and duration of antibiotic regimens are outlined in Table 1. There were 482 patients included in studies that did not stratify open fractures and antibiotic regimens by type (Table 2).[23,33,39] 88% of studies reported the duration of antibiotic type, ranging from 1 to 12.7 days.[23,24,25,26,28,29,30,31,32,34,35,36,37,38,39] 88% of the studies reported the fracture location either partially or completely (Table S3). [23,24,25,26,27,28,29,30,31,32,33,36,37,38,39] 35% of studies reported the fixation method in total.[24,30,32,33,36,38] 47% of the studies did not report their fixation method completely (Supplemental Table S2).[23,25,26,27,29,31,37,39] 75% of the studies were performed at a Level 1 Trauma Center; 33% and 8% were at academic and pediatric Level 1 trauma centers, respectively.[24,26,27,28,30,31,32,33,34,35,36,39] 29% of the studies did not report the study center.[23,25,29,37,38]
3.3. Geographical Distribution of the Included Studies
The 17 studies included in this meta-analysis were conducted in 7 countries. 65% of the studies were performed in the United States,[25,26,27,28,30,31,32,33,34,35,36] 11% were performed in Japan,[37,38], and 24% were completed in Finland,[39] the United Kingdom,[23] Germany,[24] and Iran,[29] respectively (Table 2, Supplemental Figure S2A).
3.4. Risk of Bias Assessment of Randomized Control Trials
All four RCTs were analyzed [23,33,36,39], each providing a brief or detailed discussion of the random sequence generation methodology. Sorger et al. did not report allocation concealment.[36] Three RCTs reported allocation concealment in detail.[23,33,39] Two RCTs could not blind the participants or personnel.[23,36] Three could not blind the outcome assessment.[23,36,39] All four RCTs had incomplete outcome data and demonstrated high bias in selective reporting (Supplemental Figure S2B&D).
3.5. Methodological Index for Nonrandomized Studies (MINORS)
There was no significant correlation between publication year and MINORS total score (r2=0.2020, p=0.1233, Supplemental Figure S2C). Any deduction in the MINORS score was given due to methodological limitations, such as using mostly retrospective comparative studies (Supplemental Figure S2C). The average MINORS score was 17.23 ± 2.89 out of 24, ranging from 10 to 20 (Supplemental Table S1). The following parameters were most likely to receive a low score: “a prospective collection of data,” “unbiased assessment of the study endpoint,” “follow-up period appropriate to the aim of the study,” and “prospective calculation of the study size.”
3.6. Synthesis of Results
- 1.
-
Surgical Site Infection (SSI)
- ➢
- Type I Gustilo-Anderson Open Fractures
The pooled results of 3 studies (169 patients) utilizing 3 ASAP protocols (Clinda vs. Cef, Clinda vs. Cloxa, and Cipro vs. Cefam+Gent) showed no significant difference between groups with regard to SSI (OR = 2.24, p=0.52, Figure 1).[28,33,39]
- ➢
- Type II Gustilo-Anderson Open Fractures
The pooled results of 4 studies (429 patients) utilizing 6 ASAP protocols (Cef + Gent vs. Cef, Cef + Gent vs. Pip+Tazo, Pip+Tazo vs. Cef alone OR Pip+Tazo vs. Cef+Clinda, 2Cef+Gent vs. 1Cef+Gent, and Clinda vs. Clox) demonstrated no significant differences between other groups. (OR=1.19, p=0.52, Figure 2).[26,30,36,39]
- ➢
- Type III Gustilo-Anderson Open Fractures
Our pooled results of 11 studies (1,232 patients) using 12 ASAP protocols demonstrated no significant difference in the rate of SSI between the following regimens including: (Cef+Gent vs. Cef, Cef+Gent vs. Pip+Tazo, Cef+Gent vs. Amp+Sulb, Cef+Gent vs. Cef+Cipro, Cef+Gent vs. Flu+Benz, and 2Cef+Gent vs. Cef+Gent) (OR=1.07, p=0.68). However, Flu+Benz had a lower SSI rate than Cef+Gent (OR=2.49, p=0.05, Figure 3).[24,25,26,27,29,31,32,34,36,37,38]
- ➢
- Open fracture, regardless of the type.
The pooled data from three studies (426 patients) investigating infection rate after open fracture without stratification by type demonstrated a lower infection rate with the use of Cloxacillin compared to Clindamycin (OR=0.43, p=0.03, Figure 4).[23,33,39]
- 2.
-
Acute Kidney Injury (AKI)
- ➢
- Type III Gustilo-Anderson Open Fractures
The results based on a pooled sample of four studies and five comparisons (471 patients) showed no significant difference in AKI with the use of Cef+Gent vs. Cef, Cef+Gent vs. Pip+Tazo, or Cef+Gent vs. Amp+Sulb in Type III open fractures (OR=0.74, p=0.43, Figure 5A).[24,26,32,36]
- ➢
- Type II & III Gustilo-Anderson Open Fractures
The pooled results of two studies and four comparisons (367 patients) demonstrated no significant difference in the rate of AKI in GA Type II or III fractures with the use of Cef+Gent vs. Pip+Tazo, Cef+Gent vs. Cef, Cef vs Pip+Tazo, or Cef+Gent vs. 2Cef+Gent (OR=1.14, p=0.66, Figure 5B).[26,36]
- 3.
-
Length of Hospital Stay (LOHS)
- ➢
- Type II Gustilo-Anderson Open Fractures
Our pooled results of two studies and three comparisons (230 patients) demonstrated a four-day longer LOHS with the use of Cef+Gent compared to Cef monotherapy (OR=4.00, p<0.00001, Figure 6A).[26,30]
- ➢
- Type III Gustilo-Anderson Open Fractures
When comparing different antibiotics and the length of hospital stay, our results from five studies and six comparisons (576 patients) showed no significant difference in LOHS comparing Cef+Gent to Pip+Tazo (OR=-2.39, p=0.25).[24,25,26,31,35] However, on subgroup analysis, there was around a four-day increased hospital stay using Cef+Gent compared to Cefazolin alone (OR=3.78, p<0.00001), Figure 6B.
4. Discussion
The risks of open fractures are well-known, with infection causing significant morbidity to patients and increasing health care costs. Despite efforts to reduce infection rates, SSI remains high in this patient population. To our knowledge, this is the largest meta-analysis on this topic to date, including 17 clinical studies with 2,031 patients comparing prophylactic antibiotic regimens in open fractures. This meta-analysis has identified poor and inconsistent reporting across previous studies, which contributes to the lack of standardized initial open fracture management protocols across practices and hospital systems.
Our meta-analysis demonstrated that Cef+Gent, Cef, Pip/Tazo, and Amp/Sulb antibiotics did not affect AKI in open fracture patients without pre-existing renal problems in GA Type II or III fractures. Cef+Gent was associated with an increased length of hospital stay in Type II and III fractures when compared to Cef alone. This supports the use of Cefazolin alone for Type II open fractures as infection rates were not significantly different with the addition of Gentamicin. The original GA paper’s conclusions on infection rates with Cef+Gent in Type III fractures were supported. However, a stratified meta-analysis of articles describing GA Type III fractures demonstrated that Flu+Benz had a lower infection rate than Cef+Gent. Overall, no recommendations can be made regarding the most effective antibiotic regimen for open fractures, given the inconsistencies between studies and overall poor-quality evidence within studies. Treatment should be tailored to the patient’s needs, as they vary based on severity of injury, contamination of wound, bacterial resistance, and regional/seasonal factors.[40,41,42]
Given the continued high infection rate in open fractures despite intravenous antibiosis, the orthopedic trauma community is increasingly using local intrawound antibiotic therapies. Soft tissue trauma around the open fracture site can limit the effectiveness of prophylactic systemic antibiotics, leading to the investigation of local antibiotics as an adjunct.[41] Local antibiotic powder is safe and affordable for open fractures, but its efficacy and impact on antibiotic resistance require further study.[42] O’Toole et al. found that applying intrawound vancomycin powder before closure reduced gram-positive surgical site infections in high-risk tibial plateau and pilon fractures. Yet, there are no large randomized controlled trials demonstrating the efficacy of powered in open fractures, but there have been studies supporting its use. [43] Future research should explore these methods and collaborate with systemic antibiotic use to establish new guidelines. [39,44]
This meta-analysis was constrained by the available evidence of the included studies. The heterogeneous protocols for the dosages and durations of described antibiotic regimens are evident in Table 2. Pooled subgroup analysis of GA Type I fractures failed to show significant differences in infection rates despite Vasenius et al. reporting a lower infection rate with Clindamycin compared to Cloxacillin and Iobst et al. reporting no infections in pediatric GA Type I fractures.[28,39] Insufficient data prevented analysis of AKI rates in GA Type I or II fractures alone or when combined with GA Type III fractures. Comparison of LOHS between GA Type I, II, and III fractures was also limited by available data. Limited data on BMI, comorbidities, number of irrigation and debridement procedures, mortality, and readmission also precluded subgroup analysis of this data. Recent studies lacked stratification by GA type and antibiotic regimen.[44]
4.1. Recommendations and Guidelines for Future Trials
After a review of the current literature, standardized methods are needed to compare antibiotic regimens in open fracture management. This review provides key information for future trials analyzing outcomes (Figure 7). Future trials should report categorical variables with mean, range, and standard deviation.
4.2. Study Design
When reporting data for randomized controlled trials and observational studies, the CONSORT and STROBE checklist items must be implemented and adhered to for increasing the quality of articles on this topic and maintain validity and reproducibility.
4.3. Patient’s Characteristics
Patient matching of demographics is essential for reporting differences. Comorbidities like substance abuse, diabetes, hypertension, and immunosuppression increase infection risk. Osteoporotic and immunosuppressive drugs can impair bone healing. Previous orthopedic surgery may increase wound healing issues. We recommend stratifying groups by antibiotic regimen, fracture type, age, sex, BMI, income, comorbidities, previous fractures/surgery, substance abuse, and immunosuppressive medication use.[45,46,47,48,49]
4.4. Fracture Characteristics
A thorough history and identification of the injury mechanism determines treatment aggressiveness. Fracture characteristics such as location and AO/OTA classification should be reported for reproducibility. Stratifying patients by antibiotic and GA type is essential. The GA type is an independent predictive risk factor for infection.[33,47] Fracture bioburden varies by location and season, as shown in a study by Sagi et al. Reporting the geographic region and month of injury is recommended.[50]
4.5. Treatment Characteristics
4.5.1. Antibiotics
Details of antibiotics used, including type, frequency, duration, and time of treatment initiation is recommended. The timing of antibiotics within three hours of injury and the longer duration of antibiotics have been debated regarding their effect on reducing SSI.[33,51] While a recent meta-analysis found no benefit in using antibiotics after 72 hours, a multicenter retrospective cohort study suggested that prolonged antibiotic duration may benefit high-contamination open fractures.[51,52,53,54] The use of intrawound therapy (antibiotic beads, powder) should also be reported, as this local strategy of additional prophylaxis is being commonly adopted in the trauma community.
4.5.2. Irrigation & Debridement
Conflicting evidence exists regarding the time to debridement for open fractures.[55,56] Type III open fractures with delayed time to debridement greater than 8 hours have an increased risk of infection.[55] Irrigation and debridement procedures, the type of irrigation used, the amount of solution used, and the method have been shown to affect infection rates. Alternative irrigation solutions may damage tissue.[57] Reporting the time to debridement and the type of irrigation used is recommended for future trials.[28,55,56,57]
4.5.3. Would Closure
Wound closure for open fractures varies by GA type and closure method, as shown by one of our analyzed studies.[25] Delayed wound closure, external fixation, free flap, and bone graft use should be reported and stratified by fracture type. Negative pressure wound therapy, which reduced infection rates, should also be noted, along with the timing of wound closure.[58]
4.5.4. Post-operative Assessment
Aminoglycosides are commonly used in contaminated fractures but have potential consequences such as AKI. Conflicting studies have reported on this effect, so we recommend reporting it as well as any pre-existing renal impairment.[13,27,29,59] Post-operative antibiotics should be reported to accurately determine infection rates and treatment reproducibility, with a minimum follow-up of one year to evaluate nonunion and its definition.[60] MRI should be performed and reported for suspected infection and septic nonunion and to rule out osteomyelitis.
5. Conclusion
This meta-analysis is unable to definitively recommend one prophylactic antibiotic regimen over another with confidence to reduce open fracture-related infection. We offer methodological guidelines for future trials that will allow robust evidence for future studies describing antibiotic prophylaxis for open fracture management.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Craig, J., et al., Systematic review and meta-analysis of the additional benefit of local prophylactic antibiotic therapy for infection rates in open tibia fractures treated with intramedullary nailing. Int Orthop, 2014. 38(5): p. 1025-30. [CrossRef]
- Lack, W.D., et al., Type III open tibia fractures: immediate antibiotic prophylaxis minimizes infection. J Orthop Trauma, 2015. 29(1): p. 1-6.
- Gustilo, R.B., R.M. Mendoza, and D.N. Williams, Problems in the management of type III (severe) open fractures: a new classification of type III open fractures. J Trauma, 1984. 24(8): p. 742-6.
- Kortram, K., et al., Risk factors for infectious complications after open fractures; a systematic review and meta-analysis. Int Orthop, 2017. 41(10): p. 1965-1982. [CrossRef]
- Foster, A.L., et al., Fracture-related infection: current methods for prevention and treatment. Expert Rev Anti Infect Ther, 2020. 18(4): p. 307-321. [CrossRef]
- O'Connor, O., A. Thahir, and M. Krkovic, How Much Does an Infected Fracture Cost? Arch Bone Jt Surg, 2022. 10(2): p. 135-140. [CrossRef]
- Castillo, I.A., et al., Where Are We in 2022? A Summary of 11,000 Open Tibia Fractures Over 4 Decades. J Orthop Trauma, 2023. 37(8): p. e326-e334. [CrossRef]
- Polmear, M., et al., Deep Infections After Open and Closed Fractures. J Bone Joint Surg Am, 2025. 107(Suppl 1): p. 71-79. [CrossRef]
- Agel, J., et al., The OTA open fracture classification: a study of reliability and agreement. J Orthop Trauma, 2013. 27(7): p. 379-84; discussion 384-5.
- Gustilo, R.B., The Management of Open Fractures. Journal of Bone and Joint Surgery, 1990. 72-A(2): p. 299-304.
- Gustilo, R.B. and J.T. Anderson, JSBS classics. Prevention of infection in the treatment of one thousand and twenty-five open fractures of long bones. Retrospective and prospective analyses. J Bone Joint Surg Am, 2002. 84(4): p. 682. [CrossRef]
- Gustilo, R.B. and J.T. Anderson, Prevention of infection in the treatment of one thousand and twenty-five open fractures of long bones: retrospective and prospective analyses. J Bone Joint Surg Am, 1976. 58(4): p. 453-8.
- Gustilo, R.B., et al., Analysis of 511 Open Fractures. Clinical Orthopaedics and Related Research®, 1969. 66. [CrossRef]
- Hoff, W.S., et al., East Practice Management Guidelines Work Group: update to practice management guidelines for prophylactic antibiotic use in open fractures. J Trauma, 2011. 70(3): p. 751-4. [CrossRef]
- Hauser, C.J., et al., Surgical Infection Society guideline: prophylactic antibiotic use in open fractures: an evidence-based guideline. Surg Infect (Larchmt), 2006. 7(4): p. 379-405.
- Moher, D., et al., Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ, 2009. 339: p. b2535.
- Higgins, J.P.T. and Cochrane Collaboration, Cochrane handbook for systematic reviews of interventions. Second edition. ed. Cochrane book series. 2020, Hoboken, NJ: Wiley-Blackwell. pages cm.
- Slim, K., et al., Methodological index for non-randomized studies (minors): development and validation of a new instrument. ANZ J Surg, 2003. 73(9): p. 712-6. [CrossRef]
- GraphPad Prism version www.graphpad.com [9.4.1] 2022.
- Hozo, S.P., B. Djulbegovic, and I. Hozo, Estimating the mean and variance from the median, range, and the size of a sample. BMC Medical Research Methodology, 2005. 5(1): p. 13. doi:10.1186/1471-2288-5-13.
- Wan, X., et al., Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Medical Research Methodology, 2014. 14(1): p. 135. [CrossRef]
- Collagboration, T.C., Review Manager Web 2020.
- Alpar, E.K., Cephradine and flucloxacillin in the prophylaxis of infection in patients with open fractures. Journal of clinical pharmacy and therapeutics, 1988. 13(2): p. 117-20. [CrossRef]
- Bankhead-Kendall, B., et al., Antibiotics and open fractures of the lower extremity: less is more. EUROPEAN JOURNAL OF TRAUMA AND EMERGENCY SURGERY, 2019. 45(1): p. 125-129. [CrossRef]
- Depcinski, S.C., K.H. Nguyen, and P.T. Ender, Cefazolin and an aminoglycoside compared with cefazolin alone for the antimicrobial prophylaxis of type III open orthopedic fractures. International journal of critical illness and injury science, 2019. 9(3): p. 127-131. [CrossRef]
- Frantz, T.L., et al., Early complications of antibiotic prophylaxis with cefazolin protocols versus piperacillin-tazobactam for open fractures: a retrospective comparative study. CURRENT ORTHOPAEDIC PRACTICE, 2020. 31(6): p. 549-555. [CrossRef]
- Glass, G.E., et al., The microbiological basis for a revised antibiotic regimen in high-energy tibial fractures: Preventing deep infections by nosocomial organisms. JOURNAL OF PLASTIC RECONSTRUCTIVE AND AESTHETIC SURGERY, 2011. 64(3): p. 375-380. [CrossRef]
- Iobst, C.A., et al., A protocol for the management of pediatric type I open fractures. JOURNAL OF CHILDRENS ORTHOPAEDICS, 2014. 8(1): p. 71-76. [CrossRef]
- Janmohammadi, N. and M.R. Hasanjani Roshan, Comparison the efficacy of cefazolin plus gentamicin with cefazolin plus ciprofloxacin in management of Type-IIIA open fractures. Iranian Red Crescent medical journal, 2011. 13(4): p. 239-242.
- McMurtrie, T., et al., Extended Antibiotic Coverage in the Management of Type II Open Fractures. SURGICAL INFECTIONS, 2021. 22(7): p. 662-667. [CrossRef]
- O'Connell, C.R., et al., Evaluation of Piperacillin-Tazobactam for Antibiotic Prophylaxis in Traumatic Grade III Open Fractures. Surgical infections, 2022. 23(1): p. 41-46. [CrossRef]
- Patanwala, A.E., et al., Cefazolin Monotherapy Versus Cefazolin Plus Aminoglycosides for Antimicrobial Prophylaxis of Type III Open Fractures. AMERICAN JOURNAL OF THERAPEUTICS, 2021. 28(3): p. E284-E291. [CrossRef]
- Patzakis, M.J., et al., Prospective, randomized, double-blind study comparing single-agent antibiotic therapy, ciprofloxacin, to combination antibiotic therapy in open fracture wounds. Journal of orthopaedic trauma, 2000. 14(8): p. 529-533. [CrossRef]
- Redfern, J., et al., Surgical Site Infections in Patients With Type 3 Open Fractures: Comparing Antibiotic Prophylaxis With Cefazolin Plus Gentamicin Versus Piperacillin/Tazobactam. JOURNAL OF ORTHOPAEDIC TRAUMA, 2016. 30(8): p. 415-419. [CrossRef]
- Shawar, S.K., et al., Piperacillin/Tazobactam versus Tobramycin-Based Antibiotic Prophylaxis for Type III Open Fractures. Surgical infections, 2020. 21(1): p. 23-28. [CrossRef]
- Sorger, J.I., et al., Once daily, high dose versus divided, low dose gentamicin for open fractures. Clin Orthop Relat Res, 1999(366): p. 197-204. [CrossRef]
- Takahara, S., et al., Ampicillin/sulbactam versus cefazolin plus aminoglycosides for antimicrobial prophylaxis in management of Gustilo type IIIA open fractures: A retrospective cohort study. INJURY-INTERNATIONAL JOURNAL OF THE CARE OF THE INJURED, 2022. 53(4): p. 1517-1522. [CrossRef]
- Ukai, T., et al., Retrospective analysis of risk factors for deep infection in lower limb Gustilo-Anderson type III fractures. JOURNAL OF ORTHOPAEDICS AND TRAUMATOLOGY, 2020. 21(1). [CrossRef]
- Vasenius, J., et al., Clindamycin versus cloxacillin in the treatment of 240 open fractures. A randomized prospective study. Annales chirurgiae et gynaecologiae, 1998. 87(3): p. 224-228.
- OʼToole, R.V., et al., Local Antibiotic Therapy to Reduce Infection After Operative Treatment of Fractures at High Risk of Infection: A Multicenter, Randomized, Controlled Trial (VANCO Study). J Orthop Trauma, 2017. 31 Suppl 1: p. S18-s24. [CrossRef]
- Hanssen, A.D., D.R. Osmon, and R. Patel, Local antibiotic delivery systems: where are we and where are we going? Clin Orthop Relat Res, 2005(437): p. 111-4.
- Burbank, K.M., et al., Early application of topical antibiotic powder in open-fracture wounds: A strategy to prevent biofilm formation and infections. OTA International, 2020. 3(4): p. e091.
- Sajid, M.I., et al., Efficacy of Topical Antibiotic Powder Application in the Emergency Department on Reducing Deep Fracture-Related Infection in Type III Open Lower Extremity Fractures: A Multicenter Study. J Am Acad Orthop Surg, 2025. [CrossRef]
- Prebianchi, S., et al., Type of antibiotic but not the duration of prophylaxis correlates with rates of fracture-related infection. Eur J Orthop Surg Traumatol, 2022. [CrossRef]
- Li, J., Q. Zhang, and B. Su, Clinical characteristics and risk factors of severe infections in hospitalized adult patients with primary nephrotic syndrome. The Journal of international medical research, 2017. 45(6): p. 2139-2145. [CrossRef]
- Szymski, D., et al., Evaluation of Comorbidities as Risk Factors for Fracture-Related Infection and Periprosthetic Joint Infection in Germany. Journal of clinical medicine, 2022. 11(17): p. 5042. [CrossRef]
- Sudduth, J.D., et al., Open Fractures: Are We Still Treating the Same Types of Infections? SURGICAL INFECTIONS, 2020. 21(9): p. 766-772. [CrossRef]
- Duarte, P.M., et al., The effect of an immunosuppressive therapy and its withdrawal on bone healing around titanium implants. A histometric study in rabbits. J Periodontol, 2001. 72(10): p. 1391-7. [CrossRef]
- Hegde, V., et al., Effect of osteoporosis medications on fracture healing. Osteoporos Int, 2016. 27(3): p. 861-871. [CrossRef]
- Sagi, H.C., et al., Institutional and seasonal variations in the incidence and causative organisms for posttraumatic infection following open fractures. Journal of Orthopaedic Trauma, 2017. 31(2): p. 78-84. [CrossRef]
- Burke, J.F., The effective period of preventive antibiotic action in experimental incisions and dermal lesions. Surgery, 1961. 50: p. 161-8.
- Patzakis, M.J. and J. Wilkins, Factors influencing infection rate in open fracture wounds. Clin Orthop Relat Res, 1989(243): p. 36-40. [CrossRef]
- Messner, J., et al., Duration of Administration of Antibiotic Agents for Open Fractures: Meta-Analysis of the Existing Evidence. Surg Infect (Larchmt), 2017. 18(8): p. 854-867. [CrossRef]
- Stennett, C.A., et al., Effect of Extended Prophylactic Antibiotic Duration in the Treatment of Open Fracture Wounds Differs by Level of Contamination. JOURNAL OF ORTHOPAEDIC TRAUMA, 2020. 34(3): p. 113-120. [CrossRef]
- Rozell, J.C., K.P. Connolly, and S. Mehta, Timing of Operative Debridement in Open Fractures. Orthop Clin North Am, 2017. 48(1): p. 25-34. [CrossRef]
- Weber, D., et al., Time to initial operative treatment following open fracture does not impact development of deep infection: a prospective cohort study of 736 subjects. J Orthop Trauma, 2014. 28(11): p. 613-9.
- A Trial of Wound Irrigation in the Initial Management of Open Fracture Wounds. New England Journal of Medicine, 2015. 373(27): p. 2629-2641.
- Kumaar, A., A.H. Shanthappa, and P. Ethiraj, A Comparative Study on Efficacy of Negative Pressure Wound Therapy Versus Standard Wound Therapy for Patients With Compound Fractures in a Tertiary Care Hospital. Cureus, 2022. 14(4): p. e23727-e23727. [CrossRef]
- Kafisheh, H., et al., Characterization of antimicrobial prophylaxis and definitive repair in traumatic open fractures. Critical Care Medicine, 2022. 50(1 SUPPL): p. 771. [CrossRef]
- Thomas, J.D. and J.L. Kehoe, Bone Nonunion, in StatPearls. 2022: Treasure Island (FL).
Figure 1.
Forest Plot of Fracture Related Infection Comparing 3 Different Antibiotic Regimens In Type I Open Fractures.
Figure 1.
Forest Plot of Fracture Related Infection Comparing 3 Different Antibiotic Regimens In Type I Open Fractures.
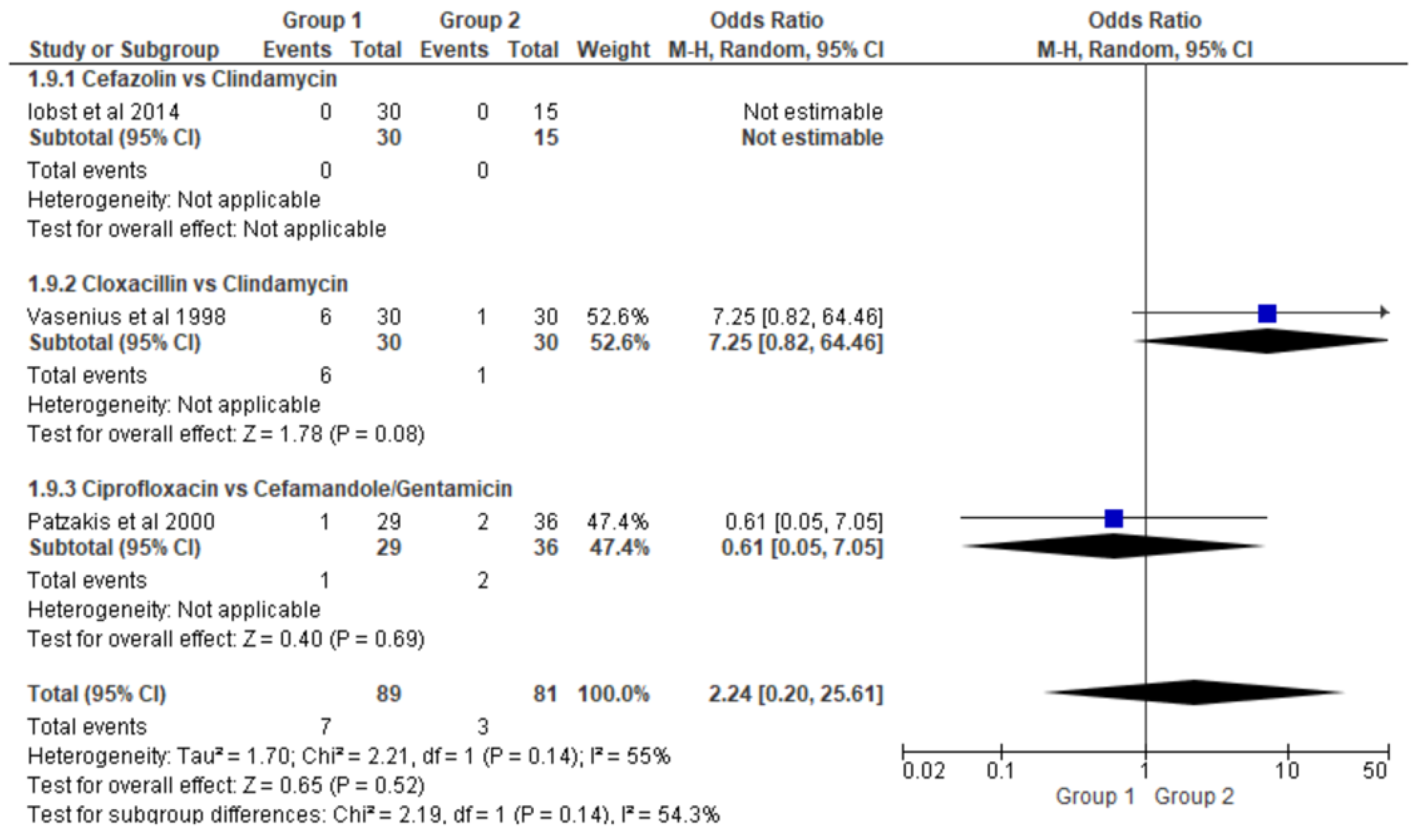
Figure 2.
Forest Plot of Fracture Related Infection Comparing 6 Different Antibiotic Regimens In Type II Open Fractures.
Figure 2.
Forest Plot of Fracture Related Infection Comparing 6 Different Antibiotic Regimens In Type II Open Fractures.
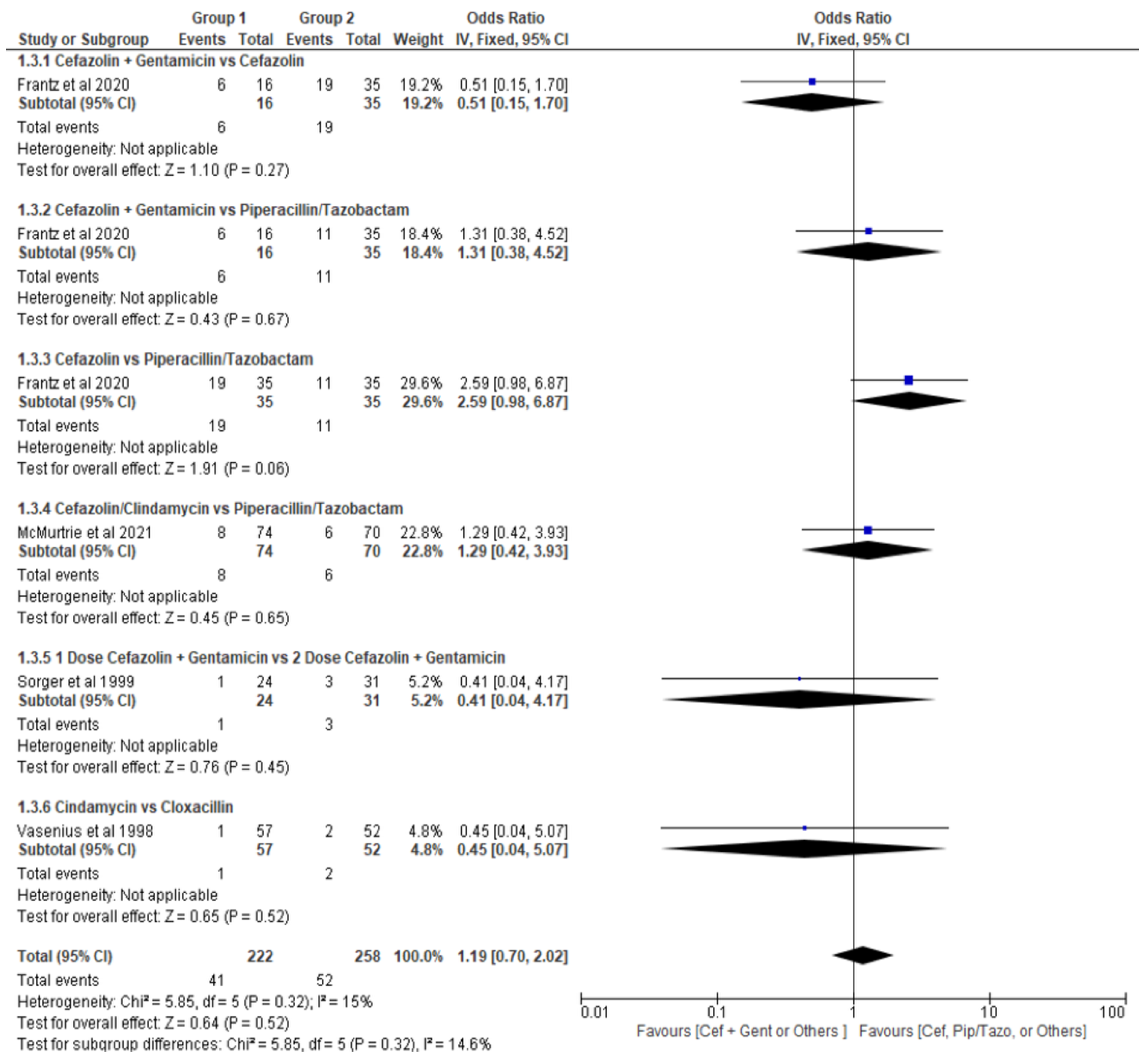
Figure 3.
Forest Plot of Fracture Related Infection Comparing 6 Different Antibiotic Regimens In Type III Open Fractures.
Figure 3.
Forest Plot of Fracture Related Infection Comparing 6 Different Antibiotic Regimens In Type III Open Fractures.
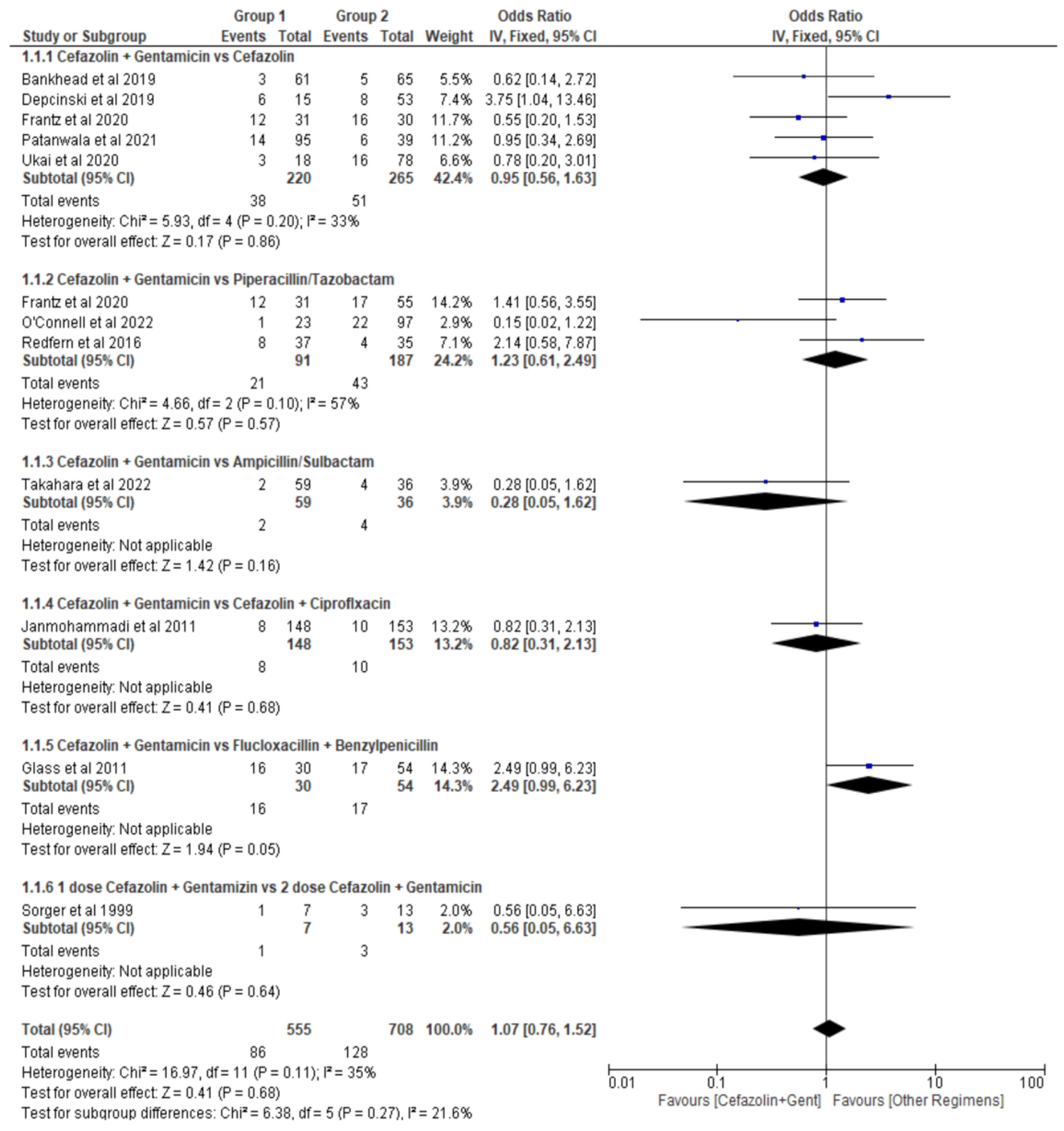
Figure 4.
Forest Plot of Fracture Related Infection Comparing 3 Different Antibiotic Regimens Regardless of Open Fracture Type.
Figure 4.
Forest Plot of Fracture Related Infection Comparing 3 Different Antibiotic Regimens Regardless of Open Fracture Type.
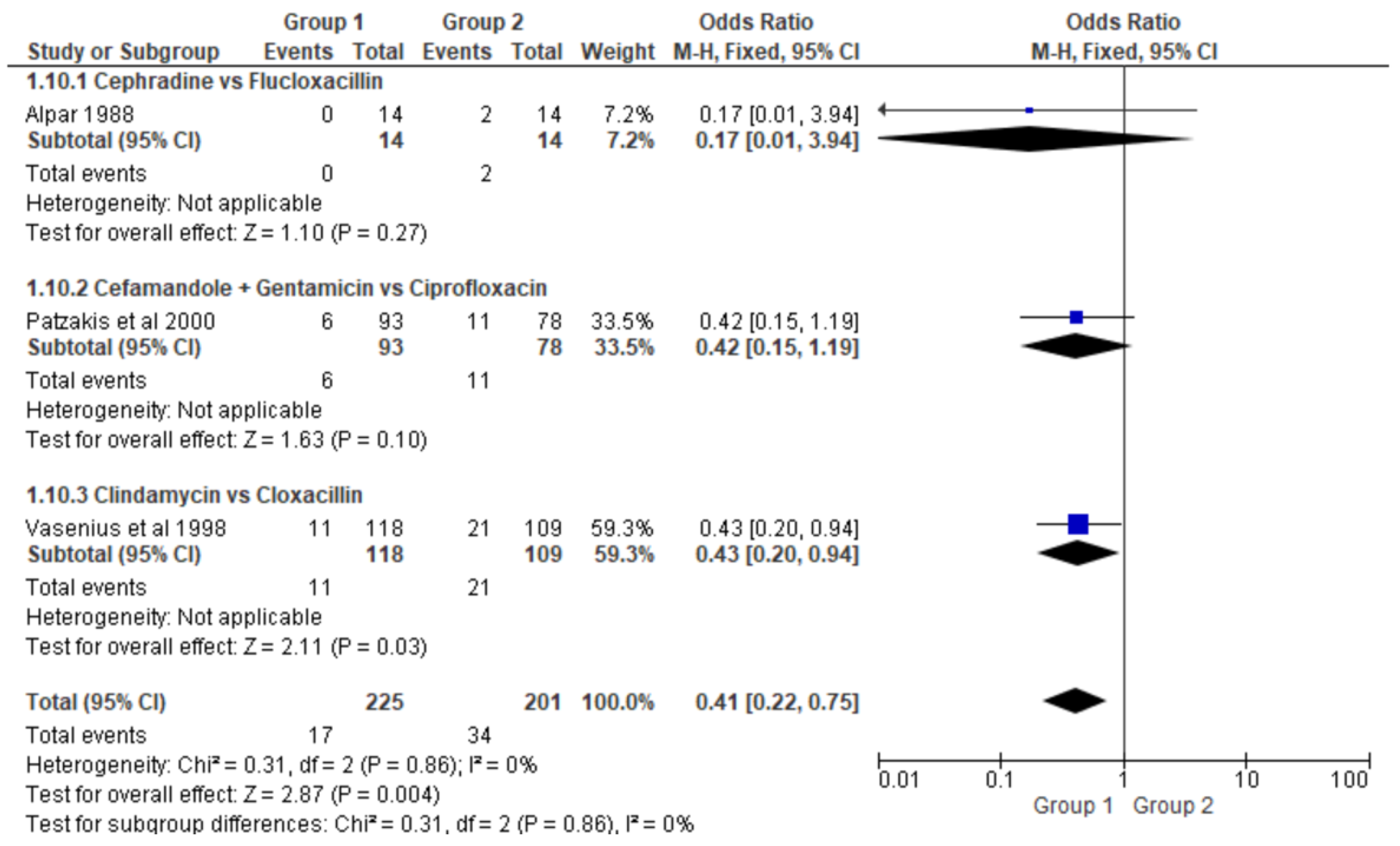
Figure 5.
(A) Forest Plot of Acute Kidney Injury Comparing 3 Different Antibiotic Regimens In Type II Open Fractures (B) Forest Plot of Acute Kidney Injury Comparing 4 Different Antibiotic Regimens In Type II & III Open Fractures.
Figure 5.
(A) Forest Plot of Acute Kidney Injury Comparing 3 Different Antibiotic Regimens In Type II Open Fractures (B) Forest Plot of Acute Kidney Injury Comparing 4 Different Antibiotic Regimens In Type II & III Open Fractures.
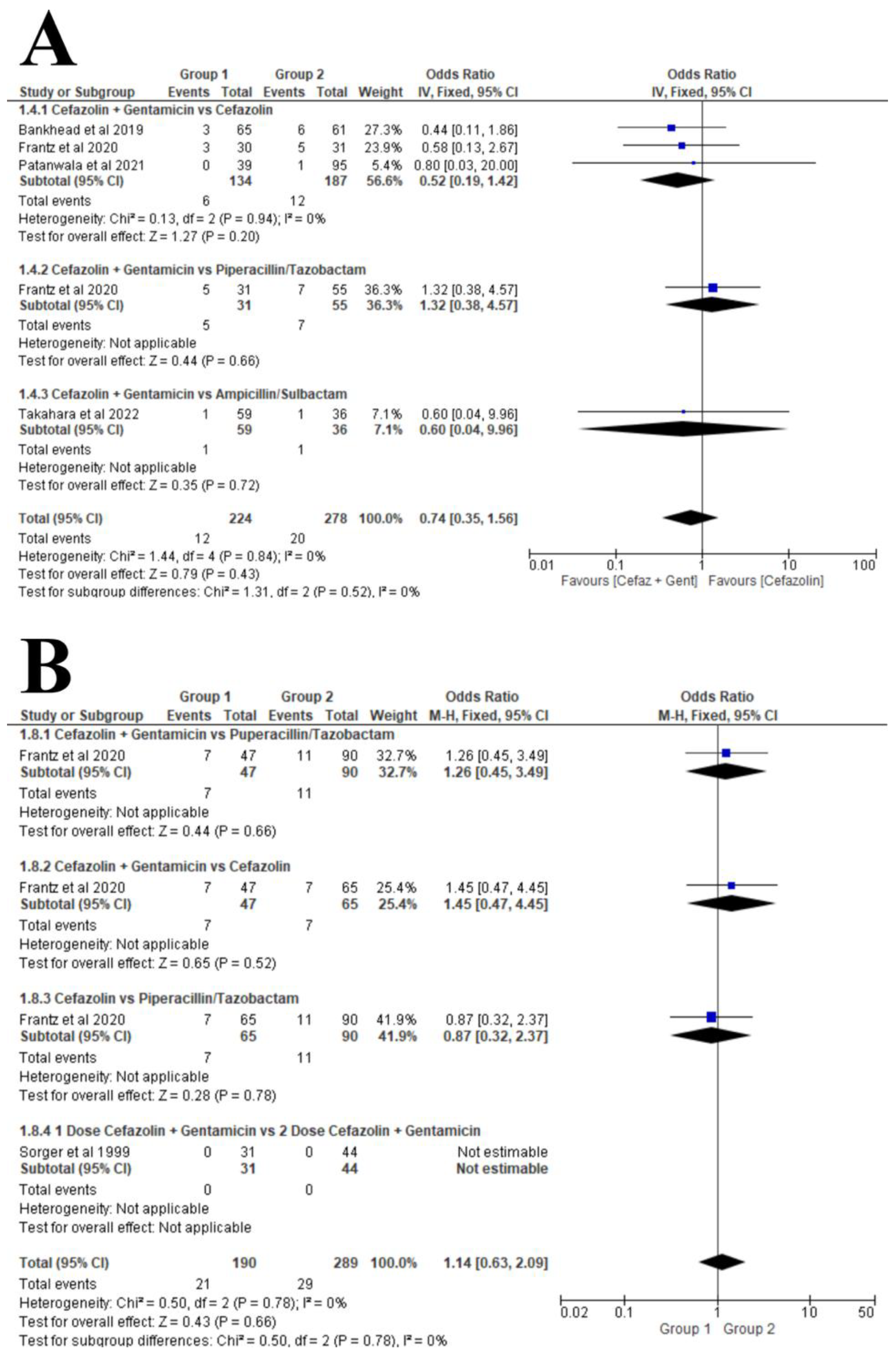
Figure 6.
(A) Length of Hospital Stay In Type II Open Fractures (B) Length of Hospital Stay In Type III Open Fractures.
Figure 6.
(A) Length of Hospital Stay In Type II Open Fractures (B) Length of Hospital Stay In Type III Open Fractures.
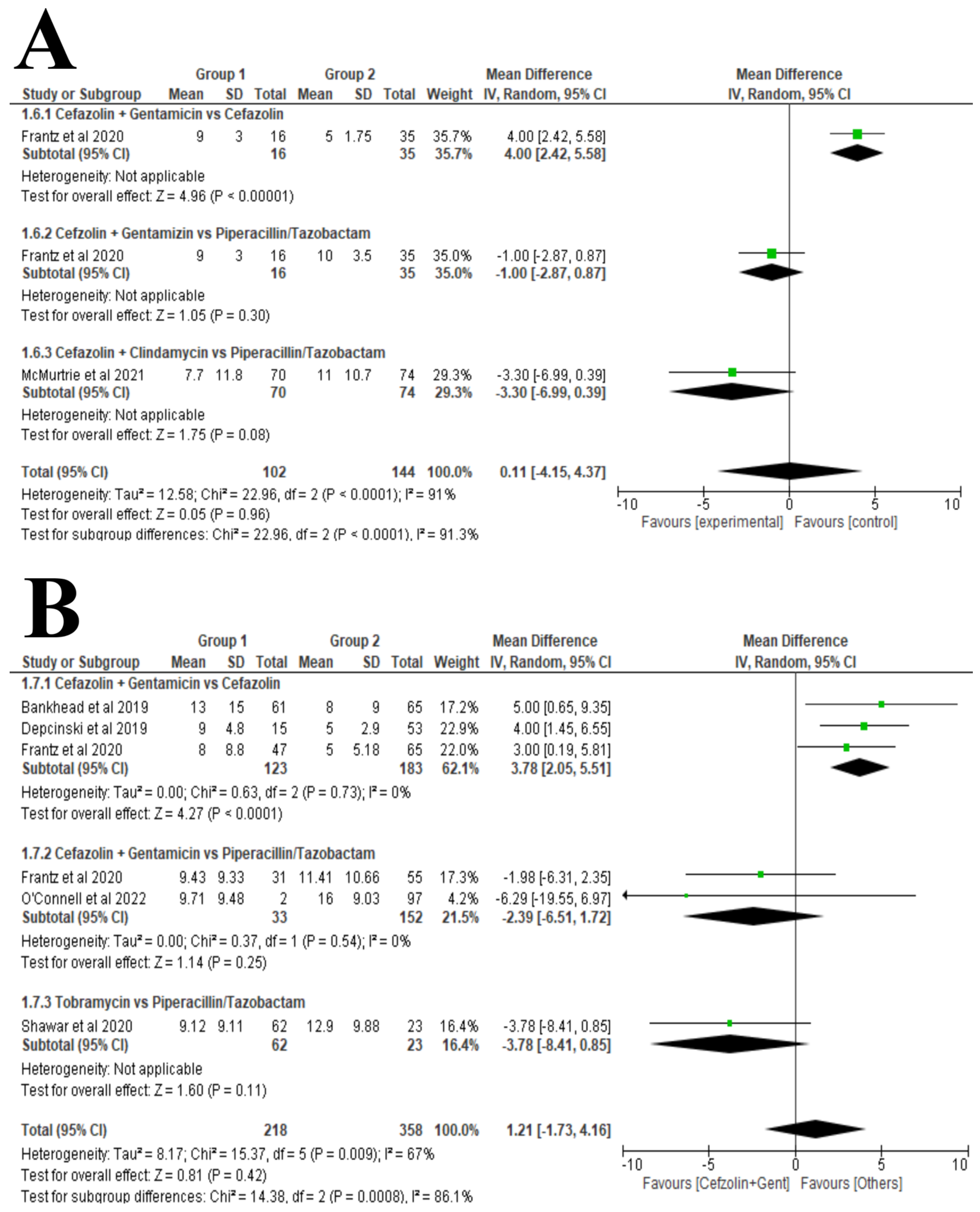
Figure 7.
Guideline chart for the minimum required data to be reported in future clinical trial.
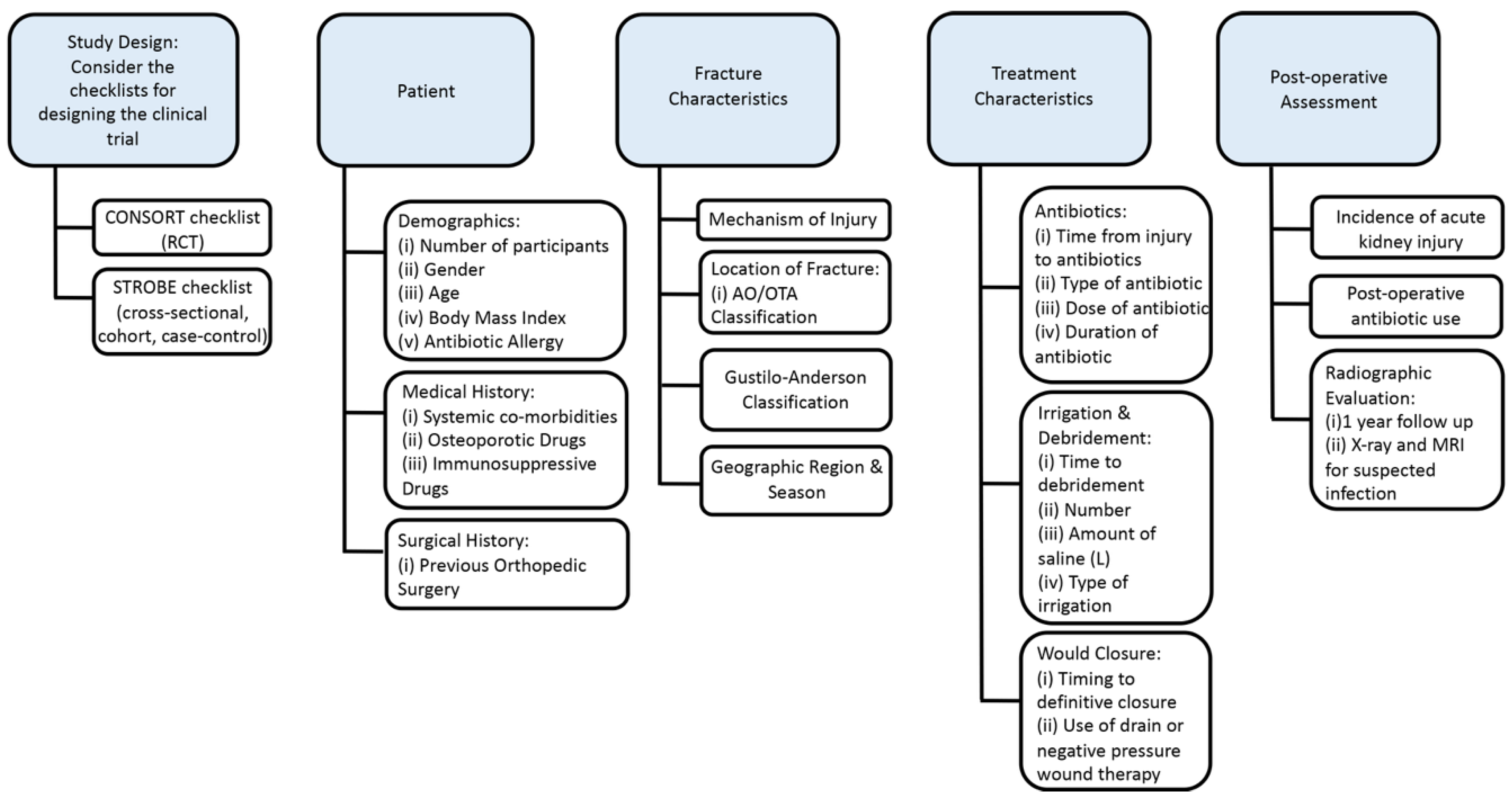

Table 1.
Dose and Duration of Antibiotic Regimens by Author.
| Author Year |
Patient No | Antibiotic | Dose/Duration | Antibiotic | Dose/Frequency | Mean Duration |
Mean Age | Female | ||
|---|---|---|---|---|---|---|---|---|---|---|
| Regimen 1 | Regimen 2 | (days) | ||||||||
|
Alpar 1988 |
60 | Cephradine | 1g IM q6h, then 500 mg BID for ten days | Flucloxacillin | 250 mg IM q6h for ten days or Oral 250mg QID | 10 | 30.5 | 15 | ||
|
Bankhead-Kendall 2019 |
126 | Cefazolin | N/A | Cefazolin + Aminoglycoside | N/A | 2.9 | 31.5 | 28 | ||
|
Depcinski 2019 |
68 | Cefazolin | N/A | Cefazolin + Aminoglycoside | 1.5 mg/kg q8h or 5 mg/kg q24h | 1 | 31.5 | 54 | ||
|
Frantz 2020 |
202 | Cefazolin | N/A | Piperacillin-Tazobactam | N/A | Cefazolin + Aminoglycoside | N/A | 3 | 43.5 | 56 |
|
Glass 2011 |
52 | Cephalosporin ± Gentamicin | N/A | Flucloxacillin ± Benzyl Penicillin | N/A | N/A | 40 | 11 | ||
|
Iobst 2014 |
45 | Cefazolin | 21.7 (range 11.9-45) mg/kg | Clindamycin | 12.1 (range 9.8-15.2) mg/kg | 1 | 10 | 9 | ||
|
Janmohammadi 2011 |
301 | Cefazolin + Gentamicin | 5g IV q8h + Gentamicin divided into 3 doses | Cefazolin + Ciprofloxacin | 1g IV q8h + 500 mg TID | 3 | 37 | 86 | ||
|
McMurtrie 2021 |
144 | Cefazolin or Clindamycin if allergy to cephalosporin | Upon arrival and a minimum of 24 h after I&D | Piperacillin/Tazobactam |
Upon arrival and a minimum of 24 h after I&D |
1 | 41 | 58 | ||
|
O’Connell 2022 |
120 | Cefazolin + Gentamicin | N/A | Piperacillin/Tazobactam | N/A | 5 | 46.3 | 37 | ||
|
Patanwala 2021 |
134 | Cefazolin | 2g IV q8h | Cefazolin + Aminoglycoside | 6 mg/kg QD or 2.5 mg/kg BID | 3 | 39 | 29 | ||
|
Patzakis 2000 |
163 | Ciprofloxacin | N/A | Cefamandole/Gentamicin | N/A | N/A | 30 | 29 | ||
|
Redfern 2016 |
72 | Cefazolin + Gentamicin | 1-2g every 8-12h + 1-2.5 mg/kg q8h or 7 mg/kg QD | Piperacillin/Tazobactam |
4.5g every 6-12h | 3.5 | 44.5 | 38 | ||
|
Shawar 2020 |
85 | Piperacillin/Tazobactam | 4.5 g q8h (1st dose over 30 minutes and later doses over 4h) | Tobramycin plus Cefazolin | 7 mg/kg plus 2g q8h |
1 | 41.1 | 26 | ||
|
Sorger 1999 |
71 | Twice Daily Dose of Cefazolin + Gentamicin | 5 mg/kg of body weight divided into two daily doses | Once Daily Dose of Cefazolin + Gentamicin | 6 mg/kg of body weight given once daily |
1 | 36 | 25 | ||
|
Takahara 2022 |
90 | Cefazolin plus Aminoglycoside (Amikacin or gentamicin) | 1-2 g q8h plus daily based on weight | Ampicillin/Sulbactam | 3g every 8 h | 1 | 50.65 | 30 | ||
|
Ukai 2020 |
110 | Cefazolin | 1g or 2g BID | Cefazolin + Gentamicin | Dosed based on therapeutic drug monitoring | 12.65 | 44.5 | 29 | ||
|
Vasenius 1998 |
227 | Clindamycin | 300-600 mg by patient weight q6h for 72 h | Cloxacillin | 2g IV every 6 h for 72 h | 3 | 38 | 80 | ||
Table 2.
Study Characteristics by Author.
| Author Year |
Country | Patient No | Mean Age | Female | Antibiotic | Antibiotic | Open Fracture Types | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Regimen 1 | Regimen 2 | Type I | Type II | Type IIIA | Type IIIB | Type IIIC | ||||||||||
|
Alpar 1988 |
United Kingdom | 60 | 30.5 | 15 | Cephradine | Flucloxacillin | 12 | 20 | 28 | |||||||
|
Bankhead-Kendall 2019 |
Germany | 126 | 31.5 | 28 | Cefazolin | Cefazolin + Aminoglycoside | N/A | N/A | 126 | |||||||
|
Depcinski 2019 |
USA | 68 | 31.5 | 54 | Cefazolin | Cefazolin + Aminoglycoside | N/A | N/A | 68 | |||||||
|
Frantz 2020 |
USA | 202 | 43.5 | 56 | Cefazolin | N/A | Cefazolin + Aminoglycoside | N/A | 86 | 116 | ||||||
|
Glass 2011 |
USA | 52 | 40 | 11 | Cephalosporin ± Gentamicin | Flucloxacillin ± Benzyl Penicillin | N/A | N/A | N/A | 52 | N/A | |||||
|
Iobst 2014 |
USA | 45 | 10 | 9 | Cefazolin | Clindamycin | 45 | N/A | ||||||||
|
Janmohammadi 2011 |
Iran | 301 | 37 | 86 | Cefazolin + Gentamicin | Cefazolin + Ciprofloxacin | N/A | N/A | 301 | N/A | N/A | |||||
|
McMurtrie 2021 |
USA | 144 | 41 | 58 | Cefazolin or Clindamycin if allergy to cephalosporin | Piperacillin/tazobactam |
N/A | 144 | N/A | N/A | N/A | |||||
|
O’Connell 2022 |
USA | 120 | 46.3 | 37 | Cefazolin + Gentamicin | Piperacillin/tazobactam | N/A | N/A | 120 | |||||||
|
Patanwala 2021 |
USA | 134 | 39 | 29 | Cefazolin | Cefazolin + Aminoglycoside | N/A | N/A | 134 | |||||||
|
Patzakis 2000 |
USA | 163 | 30 | 29 | Ciprofloxacin | Cefamandole/Gentamicin | 65 | 54 | 34 | 16 | 2 | |||||
|
Redfern 2016 |
USA | 72 | 44.5 | 38 | Cefazolin + Gentamicin | Piperacillin/tazobactam |
N/A | N/A | 72 | |||||||
|
Shawar 2020 |
USA | 85 | 41.1 | 26 | Piperacillin/tazobactam | Tobramycin plus Cefazolin | N/A | N/A | 85 | |||||||
|
Sorger 1999 |
USA | 71 | 36 | 25 | Twice Daily Dose of Cefazolin + Gentamicin | Once Daily Dose of Cefazolin + Gentamicin | N/A | 77 | 10 | 10 | 3 | |||||
|
Takahara 2022 |
Japan | 90 | 50.65 | 30 | Cefazolin plus Aminoglycoside (Amikacin or gentamicin) | Ampicillin/Sulbactam (ABPC/SBT) | N/A | N/A | 95 | N/A | N/A | |||||
|
Ukai 2020 |
Japan | 110 | 44.5 | 29 | Cefazolin | Cefazolin + Gentamicin | N/A | N/A | 77 | 37 | N/A | |||||
|
Vasenius 1998 |
Finland | 227 | 38 | 80 | Clindamycin | Cloxacillin | 60 | 109 | 33 | 15 | 10 | |||||
IV = Intravenous; IM = Intramuscular; I&D = Incision and drainage; h = hour; q8h = every 8 hours; QD = Once daily; TID = Three times a day; BID = Twice a day; USA = United States of America.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



