Submitted:
28 September 2025
Posted:
29 September 2025
You are already at the latest version
Abstract
Background: Stroke leads to lasting disability by disrupting the connectivity of functional brain networks. Although several rehabilitation methods are promising, our full understanding of how these strategies restore network function is still limited. Methods: This scoping review adhered to PRISMA guidelines and searched PubMed, Cochrane, and Medline from January 2015 to January 2025 for clinical trials focused on stroke rehabilitation with functional connectivity outcomes. Included studies used conventional therapy, neuromodulation, or feedback-based interventions. Results: Twenty-three studies fulfilled the inclusion criteria, covering interventions like robotic training, transcranial stimulation (tDCS/TMS), brain–computer interfaces, virtual reality, and cognitive training. Motor impairments were linked to disrupted interhemispheric sensorimotor connectivity, while cognitive issues reflected changes in frontoparietal and default mode networks. Combining neuromodulation with feedback-based methods showed better network recovery than standard therapy alone, with clinical improvements closely associated with connectivity alterations. Conclusions: Effective stroke rehabilitation depends on targeting specific disrupted networks through various modalities. Robotic interventions focus on restoring structural motor pathways, feedback-enhanced methods improve temporal synchronization, and cognitive training aims to enhance higher-order network integration. Future research should work toward standardizing connectivity assessment protocols and conducting multicenter trials. This will help develop evidence-based, network-focused rehabilitation guidelines that effectively translate mechanistic insights into personalized clinical treatments.
Keywords:
stroke rehabilitation
; functional connectivity
; neuromodulation
; brain-computer interface
; motor recovery
1. Introduction
Stroke is a primary cause of long-term disability, impacting millions and resulting in notable motor, cognitive, and sensory impairments [1,2]. These impairments stem from disruptions in brain connectivity, which hinder communication between essential neural networks responsible for coordinated actions and cognitive functions [3,4]. Functional connectivity involves synchronized activity between brain regions, supporting the execution of complex tasks. Following a stroke, disconnection of networks—particularly the motor, default mode, and salience networks—significantly limits recovery prospects [5,6].
The motor network, which is crucial for carrying out voluntary movements, often faces significant disruption due to stroke-related damage, leading to impaired motor control and coordination [7,8]. Similarly, the default mode network (DMN), responsible for self-referential thought and cognitive processing, often shows altered connectivity in stroke survivors, contributing to deficits in memory and attention [9,10]. The salience network, which plays a key role in processing and prioritizing environmental stimuli, is also frequently affected, resulting in difficulties adapting to changing demands [11,12]. These disruptions highlight the importance of functional connectivity in post-stroke recovery and underscore the need for targeted interventions to restore network synchronization.
Advances in neuroimaging and electrophysiology have enhanced our understanding of post-stroke disconnection and its effects on outcomes [13,14]. Research indicates that rehabilitation techniques can help realign disrupted networks. Strategies like task-specific training and neurostimulation are promising for restoring connectivity and improving recovery. For example, task-specific therapies foster plasticity in motor networks, while non-invasive brain stimulation methods such as transcranial magnetic stimulation (TMS) and transcranial direct current stimulation (tDCS) support interhemispheric communication and network reorganization [15,16]. Recent studies involving brain-computer interfaces and neurofeedback offer innovative ways to modulate connectivity in real-time, allowing for personalized interventions that support recovery progress.
Post-stroke rehabilitation increasingly aims to restore functional connectivity to boost neuroplasticity and support motor recovery. Neuromodulatory tools like tDCS, TMS, and brain-computer interfaces (BCIs) are promising for influencing cortical activity and improving motor results. Traditional physical rehab remains widely used, though it often lacks real-time feedback. Integrating advanced feedback methods, such as quantitative electroencephalography (qEEG), with standard therapy could enhance recovery by directly addressing the neural pathways involved in functional connectivity.
tDCS has been shown to improve motor learning and increase total coherence (TotCoh), indicating better brain synchronization after stroke [17,18]. It is especially effective in upper limb rehabilitation when combined with functional electrical stimulation (FES). In FES, precisely timed electrical pulses are applied to paralyzed or weakened muscles via surface electrodes placed over targeted muscles. These pulses cause muscle contractions aligned with the patient’s voluntary movements or brain-computer interface signals, aiding motor relearning and strengthening neural pathways [19]. Likewise, brain-computer interfaces (BCIs) use neural signals to provide real-time feedback, boosting motor recovery and cognitive functions [20,21]. Unlike conventional rehabilitation, which may not fully activate neuroplasticity due to limited neural reinforcement, these interventions harness neural mechanisms more effectively.
While neuromodulatory methods are gaining attention, physical rehabilitation remains crucial for stroke recovery. Its effectiveness can be improved by combining neurostimulation and feedback mechanisms [22,23]. This review discusses integrating feedback-based therapies with traditional physical therapy to find the most effective interventions for restoring functional connectivity after stroke.
Current rehabilitation methods, like traditional physical therapy, often have limitations in addressing neurobiological disruptions caused by stroke and neurological injury [24,25]. These include inadequate targeting of impaired cortical excitability, persistent neuroinflammation, and reduced neuroplasticity, all of which are crucial for optimal functional recovery [24,25,26]. Conventional therapies frequently result in plateaued motor gains, long-term compensatory movements, and incomplete motor function restoration [24,27]. Combining neuromodulatory interventions, such as repetitive transcranial magnetic stimulation (rTMS), with standard physical therapy helps address this clinical gap by encouraging neurophysiological adaptation in affected motor pathways. Neuromodulation boosts cortical plasticity and synaptic connectivity, thereby increasing the effectiveness of traditional rehabilitation and improving both motor and cognitive outcomes [24,25,28].
This review hypothesizes that combining neurostimulation and feedback interventions with conventional stroke rehabilitation can restore functional connectivity. Disrupted neural networks, specifically the motor, default mode, and salience networks, can be reconnected to improve motor, cognitive, and sensory outcomes [29]. We assert that stroke-induced disconnections are a key factor in functional impairments and that targeted neuromodulatory strategies can boost neuroplasticity when paired with standard physical therapy.
To evaluate this hypothesis, the review addresses two primary research questions:
- What are the specific patterns of functional connectivity disruption in the motor, default mode, and salience networks following a stroke, and how do these relate to different functional impairments?
- Which rehabilitation protocols, including task-specific motor training, cognitive exercises, or neuromodulatory interventions, are most effective in enhancing network-specific connectivity and promoting functional recovery?
2. Method
This review employs a scoping approach to capture the range of rehabilitative strategies for restoring network-level function after a stroke. We utilized the PRISMA framework to guide the literature search, selection, and data extraction. By focusing on interventions (robotic, neuromodulatory, and feedback-driven) and outcomes (motor, cognitive, vascular, and neuroimaging), a scoping review design ensures that heterogeneous or preliminary studies, which contribute to our understanding of post-stroke connectivity disruptions, are not excluded.
Search Strategy and Selection Criteria
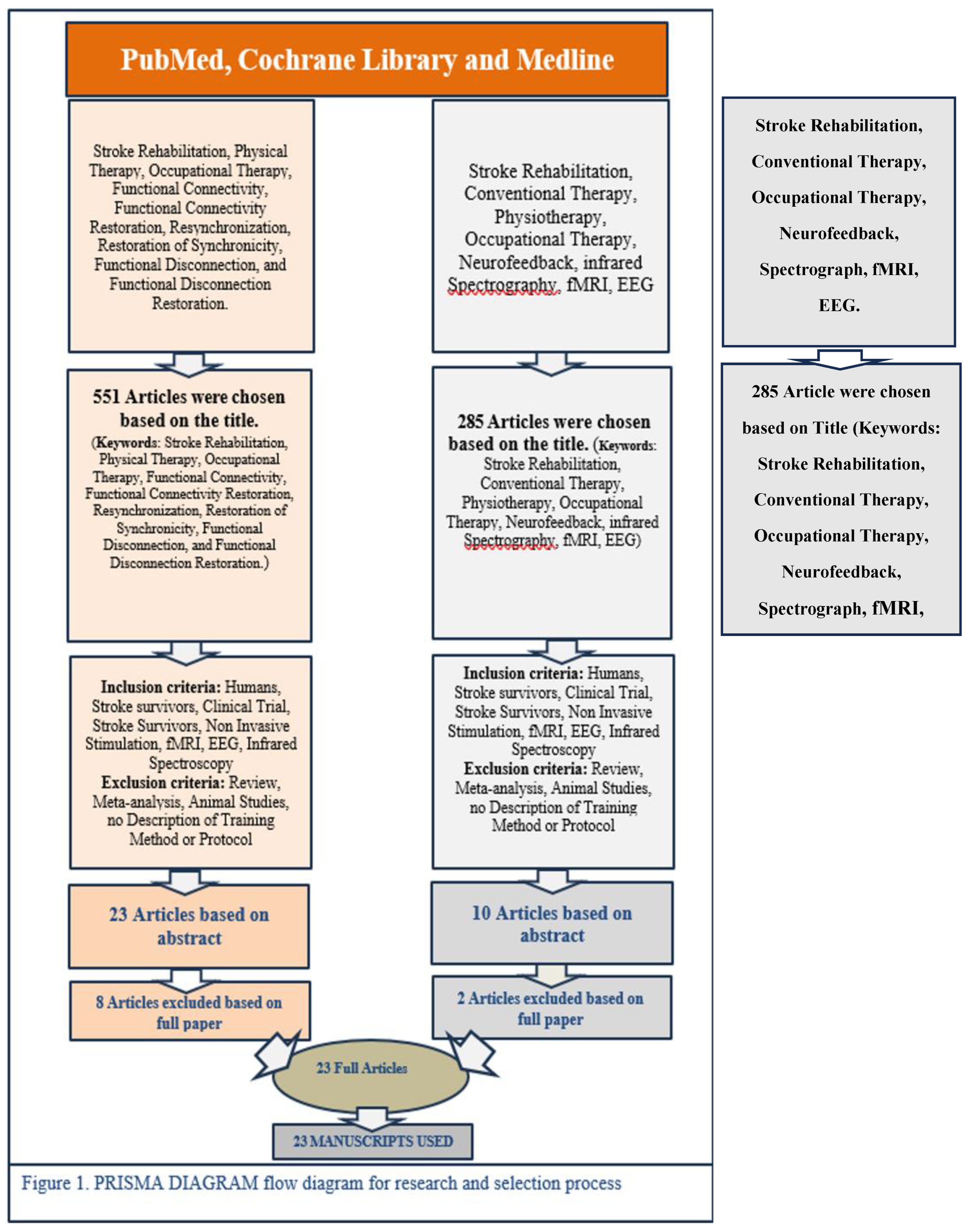
We searched PubMed, Cochrane, and Medline for articles published between January 2015 and January 2025, a ten-year period chosen to reflect recent advances in neuroimaging and neuromodulatory rehabilitation. After removing duplicates, two reviewers independently screened titles and abstracts, with a third reviewer resolving discrepancies. Full-text screening determined eligibility based on the criteria outlined below. The study selection process is summarized in Table 1.
A comprehensive literature search was performed to identify relevant studies on stroke rehabilitation and functional connectivity. An initial search focusing on stroke, connectivity, and therapy (including physical and occupational therapy, neurofeedback, fMRI, and EEG) yielded 551 articles. A second search, emphasizing conventional therapy, neurofeedback, and imaging, returned 285 results. Both sets were filtered to include only human studies and narrowed further by limiting to clinical trials and non-invasive protocols. Reviews, meta-analyses, animal studies, and articles without explicit protocols were excluded, reducing the first group to 23 abstracts and the second to 10. After full-text review, 15 and 8 articles, respectively, were considered suitable, totaling 23 articles. Additional refinements finalized the corpus for review.

Table 1.
Study selection process.
| Search Terms | Filters | Inclusion Criteria | Exclusion Criteria |
|---|---|---|---|
| (“stroke rehabilitation” OR “post-stroke rehabilitation”) AND (“physical therapy” OR “occupational therapy” OR “neuromodulation” OR “neurofeedback” OR “infrared spectrography” OR “fMRI” OR “quantitative EEG”) AND (“functional disconnection” OR “functional connectivity” OR “resynchronization” OR “restoration of synchronicity”) | Date range: 2015–2025 Human studies English language |
Humans with a stroke Original clinical or real-world trials Non-invasive stimulation, imaging, or feedback-based interventions Focus on disruptions or restoration of functional connectivity |
Reviews, meta-analyses Animal studies No described intervention No mention of connectivity/disconnection |
A scoping review framework was selected because of the wide range of interventions (such as transcranial direct current stimulation, repetitive transcranial magnetic stimulation, robotic-assisted therapies, and brain–computer interfaces) and diverse outcome measures (including motor performance, executive function, imaging-based connectivity indices, and cerebrovascular parameters). This scope would be challenging to compile in a more restrictive systematic review or meta-analysis; however, a scoping approach enables mapping the evidence and pinpointing research gaps without excluding heterogeneous designs.
Two reviewers conducted a standardized data extraction using a structured form to record the study design, sample characteristics (including stroke type, sample size, and time since stroke), intervention details (frequency, intensity, and duration), and networks examined (motor, default mode, and salience). They also documented the methods used for connectivity assessment (fMRI, EEG, fNIRS), reported outcomes (motor and cognitive measures, clinical scales), and summarized key findings related to connectivity changes and recovery patterns. This information was then used to link specific patterns of network disruption to functional impairments and assess the effectiveness of interventions in restoring connectivity.
Both reviewers assessed methodological quality using validated appraisal tools to evaluate bias risk and study rigor. Disagreements were resolved through consensus. Due to the methodological diversity of the included studies, no quantitative meta-analysis or funnel-plot-based publication bias assessment was performed; instead, a qualitative synthesis identified common themes and notable gaps.
Because of differences in study environments, some interventions took place in tightly controlled clinical trials with higher internal validity. Others were part of real-world rehabilitation programs with more varied patient populations, offering greater external validity. By recording treatment intensity, frequency, and patient adherence, we could compare how these factors affected the recovery of functional connectivity. Subgroup analyses distinguished protocols performed in strict laboratory conditions from more flexible, patient-centered, or home-based approaches like tele-rehabilitation. This helped clarify how dosage, feedback type, and concurrent interventions might differently influence connectivity outcomes. Overall, this approach provides a thorough and systematic overview of current knowledge on rehabilitative strategies aimed at restoring disrupted neural networks post-stroke, while also identifying areas for future research. The overall study identification and selection process is depicted in the PRISMA flow diagram (Figure 1).
Figure 1.
The Prisma Flow diagram.
3. Findings and Thematic Synthesis
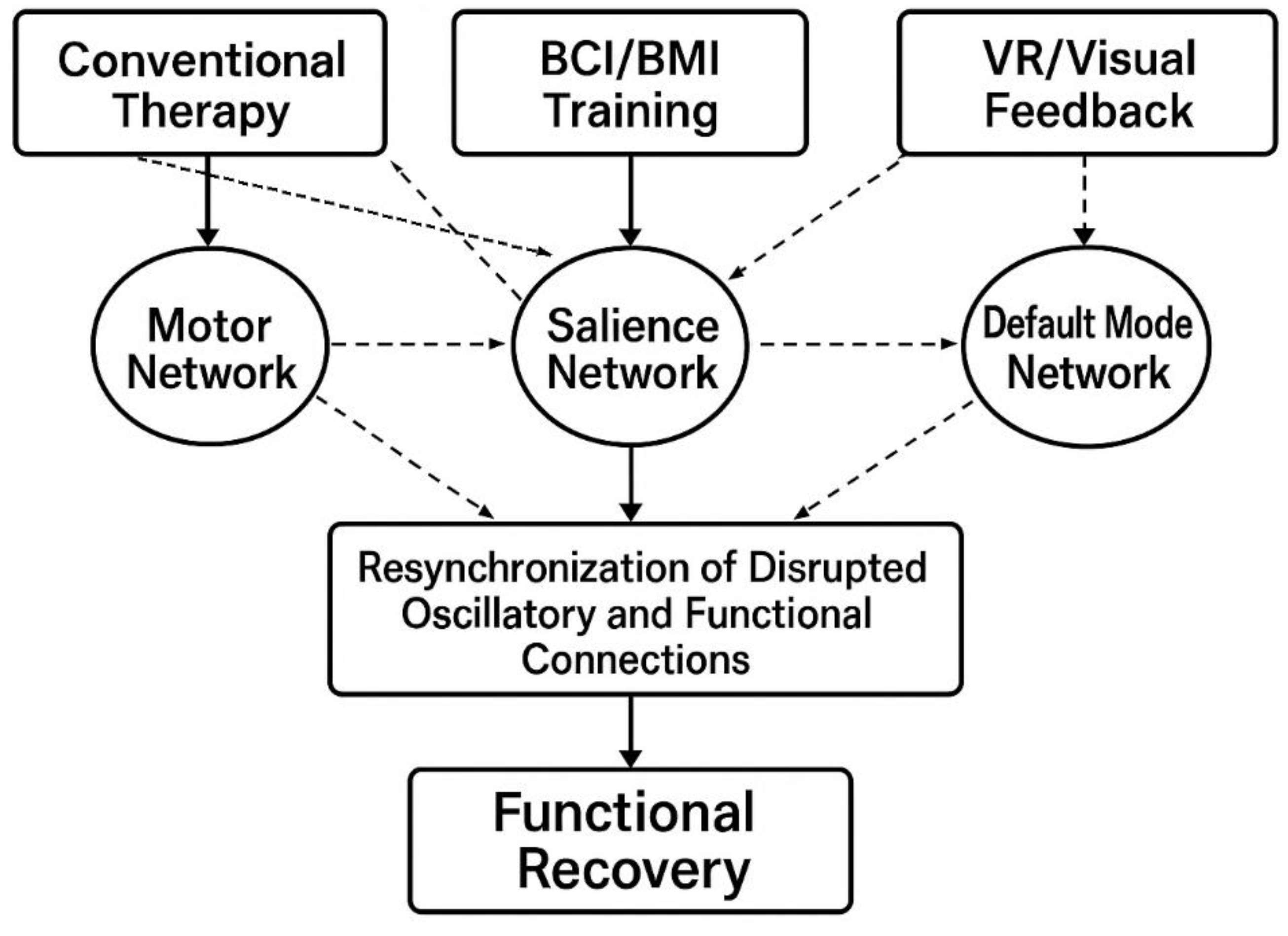
This section offers insights synthesized solely from secondary sources, not new empirical data. Highlighting “Findings and Thematic Synthesis” emphasizes that the goal of the scoping review is to identify and interpret patterns, themes, and gaps across various published studies, rather than presenting original experimental findings. An overview of this framework is illustrated in Figure 2.
Figure 2.
Conceptual Framework for Post-Stroke Network Resynchronization Through Rehabilitation Interventions.
Figure 2.
Conceptual Framework for Post-Stroke Network Resynchronization Through Rehabilitation Interventions.
3.1. Cognitive Training
Cognitive deficits such as attention, memory, executive function, and spatial awareness often reduce the quality of life and independence of stroke survivors [30,31]. Recent advances in neuroscience emphasize the importance of functional connectivity—the temporal correlation between different brain regions—as crucial for cognitive recovery after stroke [7,32]. Therefore, cognitive training interventions that target neural plasticity and connectivity are becoming more popular as potential therapies to improve cognitive deficits following a stroke.
Disruptions in functional connectivity following a stroke often lead to changes in communication within major brain networks such as the default mode network (DMN), dorsal attention network (DAN), and executive control network (ECN). These alterations are directly linked to the severity of cognitive impairments seen in clinical settings [4,10]. fMRI research consistently indicates that improvements in cognitive functions through specific training are associated with the restoration or reorganization of these affected networks [5,33]. Notably, increased functional connectivity within cognitive networks after intervention may serve as a biomarker for cognitive recovery and treatment success [34,35].
Recent advances in cognitive training emphasize personalized methods that combine adaptive training, virtual reality, and brain stimulation techniques such as transcranial magnetic stimulation (TMS) and transcranial direct current stimulation (tDCS). These approaches have been demonstrated to improve functional connectivity and promote neuroplasticity [36,37]. Evidence indicates that integrating cognitive training with neurostimulation results in greater cognitive improvements compared to single-modality strategies, highlighting the importance of comprehensive therapeutic protocols [38,39]. The included studies and their connectivity-related outcomes are summarized in Table 2.
Table 2.
Summary of Post-Stroke Functional Connectivity: Disruption, Stroke Rehabilitation Effects, and Relation to Motor, Sensory, and Cognitive Deficits.
Table 2.
Summary of Post-Stroke Functional Connectivity: Disruption, Stroke Rehabilitation Effects, and Relation to Motor, Sensory, and Cognitive Deficits.
| Author & Year | Participants (Age, Sex, N) | Key Measures | Intervention | Connectivity Disruption | Effect of Intervention |
Domain(s) |
|---|---|---|---|---|---|---|
| 1. Yin [38] | 34 (rTMS grp 16 M/2 F; no-stim grp 16 M/2 F; ≈57 y) | MoCA, VST, RBMT, MBI; ALFF, FC | 10 Hz rTMS (L-DLPFC) + CACT (4 wk) | ↓ DMN (MPFC–hippocampus) | ↑ ALFF (L-MPFC), ↑ FC (R-MPFC→rACC) correlating with MoCA & VST improvements | Cognitive |
| 2. Qin et al. [40] | 49 (31 M/18 F; ≈59 y) | MAS, FMA-UE, MBI | 1 Hz rTMS + 10 Hz rPMS (8 wk) | Reticulospinal ↑ excitability; ↓ inhibition | ↑ ALFF (rSMA, rMFG, rCereb); ↓ ALFF (rPCG, lPrCG); improved spasticity & motor function | Motor |
| 3. Middag-Van Spanje et al. [41] | 22 (16 M/6 F; median ≈ 61 y) | SCT, CVDT, MLBT-d, SLBT, CBS, SNQ | 10 Hz tACS + VST (6 wk) | Disrupted lateralized spatial attention | ↑ Alpha synchronization; better contralesional detection; reduced visuospatial neglect | Cognitive/Spatial Attention |
| 4. Chen et al. [42] | 5 (3 M/2 F; 47–77 y) | UE-FM; rs-fMRI | Bihemispheric tDCS (1.5 mA) + PT/OT (2 wk) | ↓ Interhemispheric motor connectivity | ↑ Ipsilesional motor → contralesional premotor & precuneus connectivity → improved motor function | Motor |
| 5. Sinha et al. [43] | 23 (13 M/10 F; ≈62 y) | rs-fMRI; ARAT; 9-HPT; SIS; BI | EEG-BCI + FES (~15 sessions) | ↓ Interhemispheric M1 connectivity | ↑ M1–M1 and broader motor network rsFC; improved SIS (ADL, mobility) | Motor/ADL |
| 6. Mekbib et al. [44] | 8 stroke, 13 HC (≈57 y) | FM-UE; rs-fMRI | VR-LMT + conventional (1 h/day, 2 wk) | Bilateral M1 connectivity disrupted | ↑ Interhemispheric M1 connectivity; correlated with FM-UE gains | Motor |
| 7. Wittenberg et al. [45] | 13 (12 M/1 F; 44–81 y) | TMS (MEP); MRI (FA, BOLD); FM; WMFT | Intensive robotic vs. conventional (6–12 wk) | Affected M1–PMAd connectivity changes | ↑ M1–PMAd connectivity; correlated with improved motor outcomes | Motor |
| 8. Fan et al. [46] | 10 (8 M/2 F; ≈52 y) | FMA-UL; WMFT; FIM; rs-fMRI | Robot-assisted bilateral arm therapy (4 wk) | ↓ Interhemispheric SMC connectivity | ↑ M1–M1 rs-FC; improved FMA, WMFT, ADLs | Motor/ADL |
| 9. Hu et al. [47] | 19 stroke (14 M/5 F; ≈54 y), 11 HC | ALFF; ReHo; FC; FMA | MI-BCI ± tDCS (1 mA, 20 min; ~2 wk) | ↓ SMN, disrupted DMN | MI-BCI only: ↑ ALFF in contralesional SMN; ↓ ALFF/ReHo in posterior DMN; better FMA | Motor/Cognitive |
| 10. Wada et al. [48] | 9 (6 M/3 F; ≈64 y) | EEG (ERD strength); physio data | DMB-based neurofeedback (14 d) + conventional | Impaired motor cortical connectivity → weaker ERD | 22.9% ↑ ERD strength → reorganized motor pathways; improved spasticity | Motor |
| 11. Sebastian et al. [37] | 32 HC (42 y), 34 stroke (65 y) | EEG (BSI, LC); FMA; BBT; 9HPT | MI-BCI: VR avatar + FES (~25 sess) | Lateralization asymmetry (BSI, LC) → motor deficits | ↑ Symmetry (BSI, LC); correlated with better FMA and function | Motor |
| 12. Phang et al. [49] | 10 (6 M/4 F; 39–80 y) | EEG (MRCP, FC); IMU; classification accuracy | Lower-limb motor tasks BCI (17 min) | PFCC disconnection | ↑ PFCC strength hemiplegic side; marker of recovery | Motor/Sensorimotor Integration |
| 13. Li et al. [50] | 7 (5 HC, 2 stroke) | EEG–EMG (SPMI); isometric push/pull | GNN approach to EEG–EMG data | Traditional CMC inadequate | GNN: 88.9% accuracy; robust connectivity measure | Motor Intention Detection |
| 14. Gangemi et al. [51] | 30 (15 Exp/15 Ctrl; M = 20 F = 10; ≈58 y) | EEG (θ, α, β); clinical | Neurocognitive VR training (2D/3D) | (presumed) reduced α/β power | ↑ α/β band power; enhanced connectivity; neural improvements | Cognitive/Motor |
| 15. Ray et al. [52] | 30 (18 M/12 F; ≈50 y) | cFMA; SMR; ERD (EEG) | BMI + physiotherapy (several wk) | Possible interhemispheric inhibition → ↓ α desync | ↑ α desync ipsilesional; correlated with better motor recovery | Motor |
| 16. Phang et al. [53] | 11 (age ≈ 25 y) | EEG (frontoparietal corr.); BCI accuracy | Bipedal motor-prep BCI + neurofeedback | ↓ Frontoparietal α → poor classification | Lowering α improved BCI performance; enhanced synchronization | Motor |
| 17. Carino-Escobar et al. [54] | 9 (5 M/4 F; 43–85 y) | EEG (α, β ERD/ERS); FMA-UE | BCI + robotic hand orthosis (4 wk) | β-band disruptions; nonhomologous hemispheres | ↑ β power; correlated with motor recovery; cortical activation | Motor |
| 18. Chen et al. [55] | 46 (18–65 y) | BBS; TIS; balance tests; sEMG; fNIRS; FMA-LE; BI | Cerebellar vermis iTBS (3 wk) + PT | (implicit) vermis–cortical disruption | Hypothesized ↑ SMA excitability; better trunk/lower-limb activation | Motor/Balance |
| 19. Ramos-Murguialday et al. [56] | 28 (18–80 y) | cFMA; GAS; MAL; Ashworth; EMG; fMRI; LI | BMI + physiotherapy (1 h + 1 h/day, 4 wk) | (no long-term connectivity change) | Motor learning observed; EEG reorganization | Motor |
| 20. Cheng et al. [42] | 10 (4 M/6 F; ≈52 y) | fNIRS (OxyHb); sEMG; MSS | Robot-assisted hand therapy | (not specified) | ↑ prefrontal & SMC OxyHb; improved muscle synergy/activation | Motor |
| 21. Min Li et al. [57] | 8 (M = 8; age ≈24.5 y) | Behavioral (accuracy, RT); P300 (ERP) | Exoskeleton hand + fingertip haptics | Disrupted motor–perception loop | ↑ P300 amplitude; stronger M1/PM/S1 activation | Motor/Sensory Feedback |
| 22. Ripollés et al. [58] | 20 stroke (≈59 y), 14 Ctrl (≈56 y) | ARAT; APS; BBT; 9HPT; Barthel; neuropsych; fMRI | Music-supported therapy (4 wk) | ↓ auditory–motor network (SMA–PRG, PAC–IFG) | ↑ intrahemispheric connectivity (SMA–PRG, etc.); normalized network; gains in motor, sensory, some cognition | Motor/Sensory/Cognitive |
| 23. Chen et al. [59] | 72 (18–80 y; 4 groups) | MoCA; IADL; TCD (CBFV, PI, BHI) | CCT, tDCS, CACT, or CACT + tDCS (3 wk) | ↓ DMN–FP correlation | CACT + tDCS: ↑ cerebrovascular reactivity; bilateral prefrontal excitability | Cognitive |
Legend Table 2: Clinical assessments: MoCA, Montreal Cognitive Assessment; VST, Victoria Stroop Test; RBMT, Rivermead Behavioral Memory Test; MBI, Modified Barthel Index; MAS, Modified Ashworth Scale; FMA-UE, Fugl-Meyer Assessment—Upper Extremity; UE-FM, Upper-Extremity Fugl-Meyer; ARAT, Action Research Arm Test; 9-HPT, Nine-Hole Peg Test; SCT, Star Cancellation Task; CVDT, Computerized Visual Detection Task; MLBT-d, Manual Line Bisection Task (difficult); SLBT, Standard Line Bisection Task; CBS, Catherine Bergego Scale; SNQ, Subjective Neglect Questionnaire; SIS, Stroke Impact Scale; BBT, Box & Block Test; FIM, Functional Independence Measure; IADL, Instrumental Activities of Daily Living; GAS, Goal Attainment Scale. Neurophysiology & imaging: EEG, electroencephalography (including ERD/ERS, MRCP, BSI, LC); ERP, event-related potential (e.g., P300); rs-fMRI, resting-state fMRI; fNIRS, functional near-infrared spectroscopy; TMS/MEP, transcranial magnetic stimulation/motor evoked potential; BOLD, blood-oxygenation-level-dependent signal; ALFF, amplitude of low-frequency fluctuations; ReHo, regional homogeneity; FC, functional connectivity; CMC, cortico-muscular coherence; FA, fractional anisotropy; CBFV, cerebral blood-flow velocity; PI, pulsatility index; BHI, breath-holding index; LI, laterality index; sEMG, surface electromyography. Interventions & technologies: rTMS, repetitive transcranial magnetic stimulation (10 Hz, 1 Hz); tDCS, transcranial direct current stimulation; tACS, transcranial alternating current stimulation; iTBS, intermittent theta-burst stimulation; rPMS, repetitive peripheral magnetic stimulation; BCI/BMI, brain-computer (or-machine) interface; FES, functional electrical stimulation; VR/VR-LMT, virtual reality (limb movement training); robot-assisted therapy; CACT, computer-assisted cognitive training; PT/OT, physical/occupational therapy; neurofeedback. ↑ Increased; ↓ Decreased. Brain networks & regions: DMN, default mode network; SMN, sensorimotor network; Salience Network; PFCC, parieto-frontocentral connectivity; Motor Network (M1/PM/S1); MPFC, medial prefrontal cortex; rACC, right anterior cingulate cortex; SMA, supplementary motor area.
To understand how these interventions restore function, it is essential first to examine the specific patterns of network disruption that underlie post-stroke cognitive and motor deficits.
3.1.1. Functional Disconnection Patterns Underlying Cognitive and Accompanying Physical Dysfunction
Analyzing functional disconnectivity patterns in chronic stroke patients provides insights into the neural mechanisms underlying impaired motor and cognitive functions. A key study by Ripollés et al. highlighted disruptions in the auditory–motor network, showing decreased connectivity between the supplementary motor area (SMA) and the precentral gyrus (PRG) [58]. Chen et al. observed improved vasomotor reactivity in certain patient groups, suggesting partial recovery of connectivity, though the exact network effects remain unclear [42]. Gangemi et al. supported these findings with EEG assessments, revealing reduced activation in motor areas before therapy [51]. Although initial tests showed similar auditory activation to healthy controls, there was a marked decrease in activity in the affected hemisphere’s precentral gyrus and bilateral SMA, confirming significant auditory-motor disconnection consistent with Ripollés et al. The studies consistently show disrupted connectivity, especially in auditory-motor pathways, emphasizing its role in chronic stroke. Increased bilateral motor network activity indicates compensatory mechanisms due to ipsilesional disconnections [58]. Furthermore, impaired interhemispheric connectivity in motor regions highlights extensive neural disruptions in chronic stroke [58]. Persistent cerebrovascular changes reported by Chen et al. point to vascular factors in these disconnectivity patterns [42]. Recognizing these disruptions allows exploration of how cognitive training can promote network restoration and recovery.
3.1.2. Connectivity and Synchronization Mechanisms Underpinning Cognitive Training Intervention Outcomes
Connectivity and synchronization mechanisms are increasingly understood as essential to evaluating the success of cognitive training in chronic stroke rehab. Music-supported therapy (MST), as studied by Ripollés et al., vividly shows how auditory–motor synchronization can be restored, reinstating functional connectivity within the SMA–PRG loop, normalizing disrupted activation, and promoting bilateral motor activity [58]. Similarly, Chen et al. indirectly supported network synchronization through combined computer-aided cognitive training (CACT) and transcranial direct current stimulation (tDCS) [59]. Although they did not directly measure functional connectivity, improvements in MoCA scores and BHI suggest vascular and cortical contributions to network recovery. They hypothesized that bilateral prefrontal stimulation via tDCS could enhance oxygenation and diffusion, accelerating functional healing. These studies underscore how targeted cognitive or neuromodulatory treatments can foster synchrony at cortical and subcortical levels. Gangemi et al. further explored VR cognitive training using EEG to track connectivity changes; following VR therapy, patients showed increased alpha and beta power—indicative of better attention, cognitive resource use, and motor planning—with alpha elevations in occipital areas and beta increases frontally, suggesting improved regional synchronization [51]. Gangemi et al. argued that VR-based interventions promote neurocognitive and motor restructuring by modifying connectivity across multiple networks. Collectively, these studies point to recurring mechanisms—such as enhanced auditory-motor coupling [51,58] and increased frontal activation and connectivity [42,51,58]—which underpin post-stroke cognitive and motor recoveries. The role of vascular health, highlighted by Chen et al., adds another layer of importance to connectivity restoration [42]. Overall, these insights confirm that neuroplastic reorganization supports the success of various cognitive rehab methods by restoring network functions, advancing our comprehension of how different interventions work at the network level.
3.2. Conventional Therapy
Despite ongoing technological advances, traditional therapies remain the main rehabilitation method because of their practicality and proven effectiveness [27,60].
Recent advances in neuroimaging have enhanced understanding of the neural mechanisms involved in recovery through traditional rehabilitation. Functional connectivity, an important biomarker, reflects the effectiveness of these interventions [7,12]. Conventional therapy encourages adaptive changes in functional connectivity within brain networks related to motor and cognitive functions, improving recovery outcomes [61,62].
Repetitive practice in traditional rehabilitation promotes reorganization within motor regions and interconnected networks, positively affecting motor functions [8,63]. Likewise, cognitive rehabilitation exercises can modify functional connectivity in attentional networks, leading to cognitive gains after stroke [10,64]. Research frequently investigates the mechanisms behind conventional therapy, which vary greatly depending on clinical settings and available patient resources [27,60]. In many cases, task-specific practice remains essential: therapists engage patients in daily activities like reaching or sit-to-stand transitions to promote meaningful recovery [22,65]. For example, inpatient programs might include 45-min sessions targeting repetitive motor tasks, assessed using tools such as the Functional Independence Measure (FIM) [66] and the Berg Balance Scale [67]. Correlating improvements in these assessments with neuroimaging can reveal links between recovery progress and brain coherence changes.
Home-based rehabilitation may also include scheduled therapist visits and customized exercise plans [68,69]. Patients might perform arm or balance exercises in front of a mirror, with weekly check-ins for support, especially in areas with limited resources [27]. Some clinics incorporate telehealth and wearable sensors for real-time monitoring of therapy intensity [69].
Case studies demonstrate the effectiveness of traditional therapy approaches. For example, a 62-year-old stroke patient might undergo six weeks of constraint-induced movement therapy (CIMT) combined with task-specific training, leading to improvements in Fugl-Meyer scores and increased motor cortex synchronization [70,71]. Another patient could focus on postural stabilization and gait training with the assistance of balance aids [72]. These routines can promote neuroplasticity, boosting neural connectivity, as shown in periodic assessments.
These examples highlight how structured exercises and goal-oriented tasks are essential for reconnecting disrupted networks [24]. Therapists modify protocols—whether Bobath [73], neurodevelopmental techniques, or resistance exercises—based on each patient’s functional level and environment. Although less advanced than virtual reality or brain–computer interfaces, conventional methods are broadly accessible and can incorporate connectivity principles into stroke rehabilitation. To understand conventional therapies, it is important to examine the specific network disruptions they aim to address.
3.2.1. Functional Disconnection Patterns Underlying Sensory, Motor, and Cognitive Dysfunction
Post-stroke motor and sensory deficits are seen as disruptions in key brain regions’ functional connectivity. The disconnection between parietal and frontocentral areas is strongly linked to motor impairments. This connectivity change appears during movement-related cortical potentials (MRCPs) in two-legged gait tasks, indicating a breakdown in the timing needed for effective sensorimotor integration. Specifically, the parietal cortex, crucial for motor planning, fails to synchronize well with frontal premotor areas responsible for movement execution [49].
Specific motor-related disconnection patterns have been identified. Stroke often causes an imbalance between hemispheres, with increased alpha-band synchronization in the ipsilesional motor cortex and decreased activity in the contralesional hemisphere. These changes, especially in the motor cortices and cerebellum, are positively linked to motor recovery, highlighting the importance of restoring hemispheric balance for functional gains [49]. Corticomuscular coherence (CMC), which reflects the connection between the motor cortex and muscle activity, is another critical factor affected. Stroke-related reductions in CMC could serve as biomarkers for motor impairments and recovery prospects. Recent studies support using CMC measurements in brain-computer interface (BCI) systems to monitor recovery and guide targeted therapy. Additionally, a new sequential learning model utilizing graph neural networks (GNNs) has been created to combine EEG and EMG signals, enabling the detection of complex spatiotemporal patterns for personalized rehabilitation [50].
Furthermore, disrupted cerebellar–cortical circuits, especially those involving the cerebellar vermis, are linked to balance and postural control deficits. The vermis coordinates muscles crucial for stability, and impaired communication with cortical areas can hinder recovery [55,74]. These findings highlight the importance of focusing on cerebellar connectivity in interventions for balance and gait training.
Together, these insights highlight that stroke is not just a lesion-based disorder but also involves extensive functional disconnectivity. Connectivity studies show that focal lesions lead to changes in remote network activity, and abnormal interactions among motor regions are linked to impaired behavior and recovery prospects [7].
Rehabilitation strategies that include this connectivity perspective—such as targeted gait training for fronto-central-parietal synchrony restoration [7], neuromodulation targeting cerebellar pathways [2], and advanced EEG–EMG integrated systems for decoding movement intent [7]—may offer more effective, personalized approaches to recovery after stroke. Recognizing these disruption patterns helps us examine how traditional rehabilitation interventions restore affected neural pathways through connectivity and synchronization mechanisms.
3.2.2. Connectivity and Synchronization Mechanisms Underpinning Conventional Intervention Outcomes
Recent studies emphasize the crucial role of neural connectivity in the success of traditional stroke rehabilitation. Parietal-frontocentral connectivity (PFCC) links sensory integration regions with motor execution areas and is synchronized with motor-related cortical potentials (MRCPs) during lower limb tasks in post-stroke patients. The timing of PFCC activation highlights its important role in planning and executing motor tasks. Variations in PFCC strength are linked to lower limb performance, indicating that improving this connectivity could lead to better functional recovery [49].
Corticomuscular coherence (CMC) measures the connection between motor cortex activity and muscle output, offering insights into brain-muscle interactions during voluntary movement. Recognized as a dynamic biomarker, CMC monitors motor recovery and cortical involvement in rehabilitation processes. Recent advances allow for precise modeling of these interactions, such as edge concatenation methods using symmetric partial mutual information (SPMI), providing a detailed analysis of corticomuscular communication. These methods quantify recovery progress and identify functional deficits, guiding targeted interventions [75].
Stimulating the cerebellar vermis is increasingly being explored for restoring posture and balance. Chen et al. investigated cerebellar vermis iTBS to activate the trunk and lower limbs, hypothesizing it modulates supplementary motor areas via cerebellospinal pathways [55]. These methods complement gait-focused therapies and may help improve balance and trunk control by influencing subcortical and cortical pathways. Ongoing research will reveal if combining cerebellar stimulation with traditional exercises produces better motor recovery. A promising advancement involves integrating EEG and EMG to analyze brain-muscle connectivity during rehab. This multimodal technique captures cortical intent and muscle activity, offering deeper insights into motor processes. Additionally, a graph neural network (GNN) model encodes sequential movements, allowing phase-specific analysis of intent and output. This supports more interpretable evaluations of movement complexity and neurofeedback, potentially leading to more personalized rehab plans [50].
These findings highlight the importance of using connectivity and synchronization mechanisms to improve rehabilitation strategies. Strengthening PFCC may enhance planning, while CMC metrics act as biomarkers for therapy adjustments. Cerebellar stimulation shows potential for improving postural control, and EEG-EMG integration offers a framework for recovery assessment. This connectivity-based perspective signals a shift toward individualized approaches in stroke rehabilitation, demonstrating how traditional therapies utilize neuroplasticity to improve functional connectivity and boost motor and cognitive outcomes.
3.3. Robot-Assisted Enhanced Conventional Therapy
Integrating robotic technologies in neurorehabilitation offers intensive, high-repetition therapy for individuals recovering from neurological injuries. Robot-Assisted Enhanced Conventional Therapy (RAECT) combines the consistency and accuracy of robotics with the adaptability of traditional therapy. This method aims to restore motor function and stimulate neuroplasticity essential for long-term recovery [76,77].
Robot-assisted therapies facilitate activity-dependent plasticity by guiding goal-oriented movements that impact cortical excitability and foster neural reorganization [78]. Neuroimaging and neurophysiological research demonstrate that these therapies activate dormant neural pathways, enhance ipsilesional corticospinal function, and reestablish the balance of interhemispheric inhibition [79,80]. Increasingly, recovery is seen as a process of restoring and strengthening existing neural networks rather than forming new ones [8,81].
RAECT can improve recovery by engaging network mechanisms, reactivating peri-infarct regions, recruiting secondary motor areas, and dynamically altering connectivity [82]. These changes happen through Hebbian learning, synaptic strengthening, and axonal sprouting, especially in high-intensity, feedback-rich settings provided by robotic systems. To understand how these interventions promote neuroplasticity, it is important to analyze the network disconnections they aim to address.
3.3.1. Functional Disconnection Patterns Underlying Sensory, Motor, and Cognitive Dysfunction
Recent evidence indicates that integrating robotic systems with traditional therapy helps address disconnections by fostering network-level neuroplasticity [42,83]. Reduced interhemispheric connectivity is common in post-stroke hemiparesis [46]. Fan et al. discovered that patients showed decreased resting-state functional connectivity between ipsilesional and contralesional primary motor cortices (M1), which correlated with the severity of motor impairment [46]. Likewise, Wittenberg et al. reported asymmetrical intrahemispheric connectivity, with less synchrony in the lesioned hemisphere, indicating that stroke impacts broader motor networks [45]. Robotic assistance improves traditional rehabilitation by enabling high-intensity, task-specific, and repetitive movement training—key factors for experience-dependent plasticity [42,46]. When combined with conventional therapy, robotic systems enhance motor network reorganization [40,56]. For example, Fan et al. showed that four weeks of robot-assisted bilateral arm training increased M1–M1 functional connectivity, linked to improved upper limb function [46]. Wittenberg et al. found that after upper limb therapy, patients exhibited increased connectivity between affected M1 and areas like contralesional M1, suggesting recovery within a distributed sensorimotor network [45]. Multimodal methods confirm these neuroplastic improvements [42]. Cheng et al. used synchronized fNIRS and surface EMG to demonstrate that robot-assisted hand therapy activates motor-related cortical areas and enhances muscle output, supporting cortico-muscular integration [42]. Qin et al. showed that exoskeleton-assisted hand rehabilitation with fingertip haptic stimulation results in stronger sensorimotor cortex activation, emphasizing the importance of multisensory feedback in therapy [40].
Recovery also involves cognitive systems related to planning and control, especially in patients with severe impairments [54,56]. Ramos-Murguialday et al. demonstrated that BMI training combined with conventional therapy increased activation in the prefrontal and premotor cortices, indicating recruitment of higher-order resources during motor learning [56]. Carino-Escobar et al. found that beta-band EEG activity was linked to better motor outcomes, reflecting broader network engagement [54]. Khademi et al. showed that proprioceptive neurofeedback in the beta-band frequency modulated cortico-muscular control, supporting the idea that robotics and neurofeedback target motor and cognitive domains [84].
The intensity and repetition of task-specific practice promote neural reorganization, regardless of the type of therapy [45]. Wittenberg et al. found no significant differences in brain connectivity outcomes between robotic and traditional therapy, indicating similar plasticity mechanisms [45]. However, robotic systems improve therapy delivery through consistent movement guidance, real-time feedback, and adjustable intensity, providing advantages within traditional frameworks [40,46]. Ramos-Murguialday et al. highlighted that BMI training combined with standard physiotherapy resulted in superior motor gains compared to sham controls, supporting the potential of hybrid interventions [56]. Several studies examined whether changes in brain connectivity can predict treatment response [45,46]. Wittenberg et al. found that baseline connectivity between affected M1 and dorsal premotor cortex could predict functional outcomes [45]. Fan et al. showed that increases in M1–M1 connectivity mediated the relationship between therapy and motor recovery [46]. Cheng et al. also supported this by demonstrating that real-time neurophysiological data monitored cortical engagement and muscular response, suggesting avenues for personalized intervention strategies [42]. Overall, these findings demonstrate that robot-assisted conventional therapy restores functional connectivity and advances stroke recovery [42,46,56]. This approach facilitates the reorganization of sensorimotor and cognitive networks by combining the adaptive elements of conventional therapy with the precision and feedback of robotics [40,45]. Ongoing research may pave the way for personalized rehabilitation protocols that enhance recovery by tailoring interventions to neural responsiveness [54,84]. Recognizing these disconnection patterns allows exploration of how robot-assisted interventions can restore network connectivity and improve recovery.
3.3.2. Connectivity and Synchronization Mechanisms Underpinning Robotics Enhanced Conventional Intervention Outcomes
Emerging evidence highlights the potential of robotics-enhanced interventions to improve functional recovery in stroke rehabilitation through network connectivity and cortico-muscular synchronization. These neuroplastic changes reinforce behavioral improvements, driven by robotic precision and task-specific engagement characteristic of conventional therapy.
Fan et al. studied how robot-assisted bilateral arm therapy (RBAT) affects brain connectivity in people with chronic stroke [46]. They found that RBAT notably boosts interhemispheric connectivity between the ipsilesional and contralesional primary motor cortices (M1–M1), which correlates with improved motor skills and functional ability [46]. Additionally, RBAT promotes connectivity across multiple brain regions, showing that robotics-based therapies can foster large-scale reorganization of motor and associative networks. Changes in M1–M1 connectivity significantly mediated therapy success and recovery, indicating that restoring communication between the motor cortices across hemispheres is key to achieving functional improvements [46].
Wittenberg et al. found that intensive upper limb rehabilitation, combining robotic and conventional therapy, improved synchronization between the affected M1 and various motor-related cortical areas [45]. They observed no significant differences in connectivity outcomes between the therapies, suggesting that the intensity and repetition in both methods may mainly drive reorganization.
Ramos-Murguialday et al. investigated how brain-machine interface (BMI) training impacts motor control networks in conjunction with physiotherapy [56]. Their findings showed that BMI training increased the influence of nonprimary motor areas, particularly the premotor cortex, on finger extensor muscles, indicating adaptive cortical changes. Additionally, they observed a positive link between increased beta-band cortico-muscular coherence and clinical progress, underscoring the importance of synchronization in recovery.
Qin et al. examined the impact of exoskeleton-assisted hand rehabilitation with fingertip haptic stimulation, finding significantly greater activation in M1, premotor cortex (PM), and primary somatosensory cortex (S1) compared to robot assistance alone [40]. This approach increased the amplitude of the P300 component, signifying enhanced attentional and sensory processing, which suggests improved cortical engagement [57].
Carino-Escobar et al. examined EEG beta-band activity during a BMI intervention using robotic hand orthoses in stroke patients [54]. Their results showed that beta-band activity in frontal, central, and parietal regions was associated with motor recovery, indicating the involvement of broader cortical networks as a compensatory mechanism.
These studies collectively demonstrate that robotics-augmented interventions stimulate neuroplasticity by boosting both interhemispheric and intrahemispheric connectivity, as well as cortico-muscular coherence. This facilitates motor execution, advanced sensorimotor integration, and cognitive-motor coordination. The uniformity of results across different therapies suggests that recovery results from synchronized cortical activity within functional networks, enabled by the repetitive, feedback-rich, task-focused nature of these methods. Therefore, robotics-supported therapy offers a promising approach for motor function recovery by addressing both structural and dynamic brain connectivity, utilizing technology and neuroplasticity to achieve better outcomes than traditional therapy alone.
3.4. BMI, BCI, Virtual Reality, Visual Feedback-Enhanced Conventional Therapy
Recent advances in neurorehabilitation include the use of non-invasive brain-computer interfaces (BCIs), brain-machine interfaces (BMIs), virtual reality (VR), and therapies that utilize visual feedback. When combined with traditional treatments, these modalities provide feedback-driven interventions that target motor, perceptual, attentional, and cognitive functions [40,54,56]. Their integration aligns with key neuroplasticity principles—such as repetition, task specificity, sensory salience, and goal-directed learning [78]—creating a multisensory environment that encourages adaptive network reorganization in individuals post-stroke [54,56]. Unlike robotic systems that focus on movement, BMI and BCI techniques prioritize neural engagement and decoding of motor intent, enabling patients with severe motor deficits to operate devices through brain activity [54,56]. Ramos-Murguialday et al. showed that BMI training combined with physiotherapy improved movement and increased activation in brain regions, especially the ipsilesional premotor cortex, indicating effective voluntary control recovery [56].
EEG-based BCIs also interpret motor intentions and offer feedback to support neuroplasticity. Carino-Escobar et al. observed that using a robotic hand in a BCI intervention increased beta-band activity in certain brain areas, suggesting the engagement of compensatory networks in patients with limited function [54].
Similarly, virtual reality (VR) rehabilitation boosts patient engagement by offering interactive simulations that provide rich sensory feedback [85]. VR creates an immersive sensory environment and allows for intensive task repetition, which enhances brain activity through goal-oriented feedback, thereby strengthening motor and cognitive pathways [86]. The sense of presence fostered by VR activates cognitive networks crucial for engagement and learning [87].
Visual feedback-enhanced therapies use traditional methods like visual mirrors and augmented displays to correct movement errors and aid motor execution by activating relevant brain pathways [88]. This method is similar to mirror therapy, which stimulates motor-related brain regions through observational learning [88,89].
Neurofeedback and virtual interventions depend on real-time synchronization of brain activity with sensory input and motor output. Using various tools, they boost error-based learning, which is crucial for neuroplasticity [90]. Their flexibility allows integration into a wide range of therapy protocols, helping patients with different impairments [56,85].
Overall, BMI, BCI, VR, and visual-feedback therapies are neuroadaptive interventions that actively reshape brain connectivity. Their effectiveness depends on integrating advanced technology with conventional motor learning methods [78], supporting motor recovery by harnessing the brain’s ability to reorganize through feedback-based experiences [50,54,56]. To fully understand these interventions, it is important to analyze the complex network disconnection patterns they aim to target.
3.4.1. Functional Disconnection Patterns Underlying Sensory, Motor, and Cognitive Dysfunction
Several studies emphasize the disconnection between hemispheres in stroke survivors, especially those with severe motor impairments. Ramos-Murguialday et al. found that chronic stroke patients had decreased resting-state connectivity between primary motor cortices (M1) compared to healthy controls, linking this disconnection to motor deficits and targeting it in their BMI intervention, which linked motor intent with outcomes [56]. After therapy, M1–M1 connectivity increased and correlated with clinical recovery, highlighting the importance of restoring interhemispheric synchrony [56].
Sinha et al. observed that stroke patients undergoing BMI training with functional electrical stimulation exhibited intrahemispheric connectivity centered on the ipsilesional M1, which differs from the typical bilateral patterns seen in healthy individuals [43]. After the intervention, interhemispheric connectivity was enhanced and was associated with motor improvements. This indicates that stroke-related sensorimotor disconnection involves both structural and functional aspects, and technology-supported therapies can help restore cortical balance [43].
Functional disconnection impacts cognitive and attentional networks and is often overlooked in rehabilitation. VR-based cognitive therapies have been proven to boost cortical rhythms and connectivity in areas responsible for executive functions. Gangemi et al. found that stroke patients undergoing immersive VR training showed increased EEG alpha and beta power, unlike those in traditional therapy [51]. This suggests that VR might more effectively stimulate cognitive networks by providing multisensory immersion [51].
Phang et al. showed frontoparietal disconnection during motor imagery in stroke patients, which reduced BCI system performance [53]. Their findings indicate that disrupting the frontoparietal network impacts intention-driven interfaces, emphasizing the need for interventions to reactivate motor control regions.
Wada et al. developed a proprioceptive feedback-based BMI that uses event-related desynchronization (ERD) to interpret motor intentions [48]. This approach enhances synchronization between brain signals and sensory feedback, thereby improving motor learning. Such proprioceptive cues could also aid in restoring sensorimotor coupling after a stroke.
Ray et al. found that beta-band power serves as a biomarker for motor recovery, with patients exhibiting greater improvements showing unique EEG patterns during tasks [52]. This indicates that the return of rhythmic activity is linked to restored function, making it a promising target for neurofeedback and BMI-based rehabilitation.
Overall, research indicates that rehabilitation approaches using closed-loop feedback through BMI, BCI, VR, or visual augmentation more effectively activate disconnected neural networks than traditional therapies. Ramos-Murguialday et al. demonstrated that combining BMI with physiotherapy resulted in greater motor improvements and restored M1–M1 connectivity compared to physiotherapy alone [56]. Sinha et al. found that VR limb mirroring enhanced interhemispheric integration and patient outcomes beyond conventional therapy [43]. Additionally, Gangemi et al. observed that only VR training caused neuroplastic changes [51].
These results show that fixing functional disconnection by syncing motor intent and feedback is key for recovery. While traditional therapies are important, they might lack the neural precision needed for network reorganization. Innovations in BMI, VR, and neurofeedback effectively help restore disrupted networks, supporting coordinated movement and thinking. Once we identify these disconnection patterns, we can investigate how feedback-enhanced interventions restore connectivity and synchronization.
3.4.2. Connectivity and Synchronization Mechanisms Underpinning Feedback-Enhanced Conventional Intervention Outcomes
Ray et al. identified that alpha band oscillatory activity, particularly event-related desynchronization (ERD) during motor imagery, serves as a dependable biomarker for motor recovery in chronic stroke patients [52]. Patients exhibiting higher alpha ERD at baseline and greater desynchronization during training experienced more notable functional gains. A shift toward desynchronization in the ipsilesional hemisphere associated with clinical improvements suggests that restoring hemispheric balance is crucial for recovery. Similarly, Wada et al. developed a BCI system that utilized mu band ERD (8–13 Hz) to activate proprioceptive feedback for hand movements within a virtual environment [48]. This feedback loop, synchronized with motor imagery, likely promoted sensory-motor pathway reorganization by increasing cortical activity and enhancing the coupling of sensory input.
Connectivity within frontoparietal networks plays a vital role in stroke rehabilitation success. Phang et al. found that lower alpha-band connectivity between frontal and parietal areas is linked to better motor preparation-based BCI control [53]. This indicates that adjusting or even decoupling activity in frontoparietal circuits can enhance BCI performance by supporting motor intention encoding. Notably, stroke patients showed reduced frontoparietal connectivity compared to healthy individuals during motor preparation and execution, implying widespread disruptions in top-down motor planning.
Sinha et al. examined a virtual reality limb mirroring approach for patients in the subacute stroke phase, observing a transition in functional connectivity from within a single hemisphere to bilateral engagement [43]. They found that stronger connectivity between the primary motor cortices on both sides was linked to better motor function. The authors suggested that visual stimulation of the mirror neuron system through limb mirroring promoted reorganization between hemispheres, leading to improved synchronization.
Supporting this, Ramos-Murguialday et al. demonstrated that BMI training with functional electrical stimulation improved interhemispheric M1–M1 connectivity, which was linked to better upper limb function [56]. fMRI revealed a temporary normalization of contralateral M1 activation during paretic hand movements after the intervention. Although this shift in lateralization was not sustained at the six-month follow-up, it highlights the importance of early cortical re-engagement in recovery. The BMI system used sensorimotor rhythm desynchronization to provide proprioceptive and visual feedback, creating a feedback loop that likely encouraged sensorimotor reconnection.
EEG asymmetry measures, such as the Brain Symmetry Index (BSI), show a significant correlation with motor function; lower BSI scores, indicating better symmetry, are linked to improved performance. The Laterality Coefficient (LC), which assesses ERD asymmetry, also relates to upper limb function, implying that symmetric activation of the hemispheres improves outcomes. Sinha et al. found that BCI training with functional electrical stimulation enhanced interhemispheric connectivity within the motor network, resulting in improvements across various motor domains [43]. This indicates that BCI feedback can reorganize the overall motor network and boost its connectivity, promoting better cortical communication both locally and across the brain.
In cognitive research, Gangemi et al. found that VR-based cognitive training for chronic stroke patients increased alpha power in occipital regions and beta power in frontal areas, suggesting improved functional connectivity within visual and executive control networks [51]. The use of real-time audiovisual feedback probably supported multisystem reorganization by promoting task-specific, feedback-enhanced engagement.
Across these studies, converging mechanisms become apparent. Restoring interhemispheric balance in motor regions is linked to better clinical outcomes. Event-related desynchronization in alpha and mu bands acts as a neural marker for motor imagery engagement and encourages plasticity when combined with feedback. Additionally, multisensory feedback—whether visual, proprioceptive, or auditory—is essential for strengthening the connection between motor intention and execution. These findings suggest that feedback-enhanced interventions can effectively promote synchronization and plasticity in disrupted neural circuits, complementing traditional therapy in personalized, connectivity-focused stroke rehabilitation. This evidence indicates that feedback-based interventions produce improved therapeutic results by restoring the temporal alignment of disrupted neural networks through closed-loop mechanisms.
4. Discussion
This scoping review systematically addresses the two primary research questions posed in the introduction, offering critical insights into post-stroke network disruption and the efficacy of rehabilitation.
4.1. Mechanisms of Network Restoration
4.1.1. Addressing Research Question 1: Patterns of Functional Connectivity Disruption
Our analysis revealed distinct network-specific disruption patterns that correlate with particular functional impairments. In the motor domain, impaired interhemispheric communication—especially between primary motor cortices (M1–M1)—along with weakened intrahemispheric pathways, such as parietal–premotor coupling during gait and cortico-muscular coherence, represent the core neural substrates of persistent motor deficits [46,49]. Cognitive dysfunction arises from breakdowns in the auditory–motor loop (SMA–PRG, PAC–IFG) that disconnect sensory feedback from motor planning, intensifying perceptual challenges [51,58]. While early evidence indicates that frontoparietal, default mode, and salience networks are involved in post-stroke cognitive impairments, their precise contributions to functional deficits need further clarification.
4.1.2. Addressing Research Question 2: Rehabilitation Protocol Effectiveness
Our results indicate that different rehabilitation approaches promote network-specific recovery through unique mechanisms. Traditional high-repetition practices encourage gradual reorganization of the motor network, which is further enhanced by neuromodulation techniques like cerebellar iTBS or multimodal EEG–EMG feedback [55,63]. Robot-assisted therapies offer the intensity and precision needed for strong M1–M1 recoupling and the recruitment of perilesional areas by restoring structural connectivity [42]. Feedback-based methods—including BMI/BCI systems, immersive virtual reality, and visual feedback—use real-time brain–machine interaction to restore functional connectivity through precise timing of neural networks [43,56]. Cognitive training, from music-supported therapy to tDCS-enhanced exercises, normalizes auditory–motor and prefrontal connections, improving both cognitive abilities and vascular responsiveness [58,59].
4.1.3. Key Finding: Modality-Specific Network Targeting
The evidence indicates that no single intervention can effectively target all disrupted networks. Instead, successful rehabilitation involves a strategic combination of approaches: robotic interventions are particularly good at repairing structural motor pathways, feedback-enhanced methods help restore functional timing and synchronization, and cognitive training focuses on higher-level network integration. This approach aligns with precision medicine, where individual connectivity profiles and specific network deficits inform the choice of interventions.
4.2. Clinical Translation
Translating network-based rehabilitation insights into clinical practice offers both promising opportunities and notable challenges. Robot-assisted therapies are the most widely adopted, with well-established protocols for restoring M1–M1 connectivity that lead to observable functional improvements within 4–6 weeks [45,46]. These interventions’ dose-dependent nature aligns with current rehabilitation standards, easing their integration into routine care. While feedback-enhanced modalities deliver higher precision in synchronizing the temporal network, they require specialized technical infrastructure and training. BMI/BCI systems that restore cortico-muscular coherence are effective clinically, but their deployment demands significant equipment and expertise [56]. Virtual reality therapies serve as a balanced option, offering immersive feedback environments that are adaptable across clinical settings without losing therapeutic accuracy [43,51]. Cognitive training methods, particularly music-supported therapy and tDCS-augmented protocols, hold immediate clinical promise because they can be implemented in various settings with moderate resources [58,59]. Combining traditional therapy with targeted neuromodulation provides a practical approach for embedding connectivity-based interventions into current rehabilitation frameworks.
4.3. Limitations of Current Evidence
Despite progress, turning mechanistic insights into routine clinical practice remains challenging due to methodological constraints. Researchers utilize a range of imaging and electrophysiological methods—such as fMRI, EEG, and fNIRS—with unique analytical approaches, making comparisons and data integration difficult. A major obstacle is the inconsistent definition and measurement of “functional connectivity” across these modalities: fMRI assesses BOLD signal correlations, EEG examines oscillatory coherence, and fNIRS measures hemodynamic coupling. This variability hampers efforts to develop standardized connectivity biomarkers useful for clinical decisions.
Small, single-center studies with limited randomization reduce statistical reliability and validity, especially for emerging treatments like RAECT and closed-loop neurofeedback. Additionally, the differences in stroke features, lesion sites, and timing after injury make it harder to apply findings broadly across diverse patient groups.
Limited assessment of the default mode and salience networks leaves gaps in understanding cognitive and emotional outcomes. Although motor network recovery has been explored, the contribution of higher-order cognitive networks is not well understood, restricting the development of comprehensive rehabilitation approaches.
Furthermore, the absence of long-term follow-up data limits insights into whether connectivity improvements and independence are maintained over time. Most research assesses results only weeks or months after treatment, so the long-term stability of network changes and their impact on quality of life remain unclear.
Economic barriers also hinder implementation because high costs, technical complexities, and the need for specialized training for robotics and neurofeedback systems limit their widespread use, especially in resource-limited settings.
4.4. Future Research Trajectories
To develop a precision-connectivity approach in stroke rehab, future research needs to overcome current limitations by following strategic steps. Standardizing methods should involve creating consensus protocols for data collection and analysis, allowing studies to be directly compared and supporting meta-analyses. Large, multicenter trials that classify patients by lesion location and severity will help confirm the effectiveness of treatments across different groups and aid in developing evidence-based, connectivity-focused rehab guidelines. These should include standardized outcome measures that accurately reflect improvements in network function and overall recovery.
Expanding assessments to include default mode and salience circuitry will clarify their roles in cognitive recovery and guide therapeutic strategies. Understanding how cognitive and motor networks interact during rehabilitation will support the development of comprehensive intervention methods.
Longitudinal studies lasting six to twelve months after intervention are crucial for assessing the durability of neural reorganization and its effects on everyday living. These studies should investigate how ongoing connectivity modifications are connected to long-term independence, quality of life, and caregiver strain.
Future protocols ought to utilize baseline connectivity profiling to guide intervention choices, dosing, and sequencing. Machine learning can detect connectivity signatures that forecast treatment response, enabling personalized rehabilitation tailored to each person’s neural architecture.
The creation of portable feedback platforms that include EEG, EMG, and fNIRS within intuitive virtual environments can make advanced treatments more accessible, enabling home-based and remote rehabilitation. These technologies should focus on ease of use and affordability to overcome barriers to access.
Targeted training programs that address economic and infrastructure barriers will improve clinical adoption. Implementation research should investigate strategies for integrating connectivity-based interventions into healthcare systems, ensuring they are both effective and cost-efficient.
By integrating detailed mechanistic research with scalable, patient-centered care models, the field can transition from proof-of-concept studies to sustainable strategies that restore network integrity and enhance the recovery potential of stroke survivors. Evidence supports a future where rehabilitation protocols are tailored to address functional deficits and specific patterns of network disconnection underlying each patient’s impairments.
5. Conclusions
This scoping review offers a comprehensive overview of how disruptions at the network level contribute to motor, sensory, and cognitive impairments following a stroke. It critically assesses the effectiveness of current rehabilitation methods in restoring network integrity. Analyzing 22 clinical studies published between 2015 and 2025, this analysis uncovers four key insights:
First, stroke should be viewed primarily as a disorder of large-scale brain-network integrity rather than solely as focal tissue damage. Throughout both acute and chronic stages, persistent deficits are most consistently associated with weakened inter- and intra-hemispheric sensorimotor connectivity (such as M1–M1 coupling, parietal–premotor interactions, corticospinal coherence), dys-synchrony in higher-order cognitive networks (like default-mode, fronto-parietal, and salience networks), and impaired cerebrovascular reactivity, which further disrupts functional connectivity. These network issues go beyond lesion location and timing, highlighting the need to include network-level assessments in both diagnosis and treatment planning.
Second, different intervention strategies target various aspects of network dysfunction. High-dose, task-specific practice gradually retrains residual corticospinal pathways, while robot-assisted therapy speeds up the structural reconnection of bilateral sensorimotor hubs. Non-invasive neuromodulation techniques such as TMS, tDCS, and iTBS temporarily adjust excitatory and inhibitory activity to prepare networks. Moreover, closed-loop feedback systems, such as BCI/BMI, VR, and neurofeedback, assist in optimizing oscillatory dynamics and corticomuscular coupling. Since there is no single “network fix,” this highlights the need for personalized, multimodal rehabilitation that adapts each approach to an individual’s specific connectivity profile.
Third, factors such as the amount of practice, quality of feedback, and timing between modalities have a more significant influence on outcomes than the specific technology brand. Patients showed clinically meaningful improvements after engaging in at least around 15 h of feedback-rich, task-specific practice over at least three weeks, whether it was facilitated by a robot, a therapist, or through self-guided practice.
Fourth, applying priming neuromodulation techniques early, such as cerebellar iTBS or bi-hemispheric tDCS, together with intensive training, consistently led to greater and more lasting network changes than using either method individually.
While methodological rigor and the quality of evidence are improving, variation in imaging techniques, cohort sizes, outcome metrics, and follow-up periods continues to hinder meta-analyses and accurate dose-response evaluations. To push the field forward, future studies should implement standardized protocols—such as combining resting-state fMRI with high-density EEG—and use uniform connectivity metrics along with multicenter randomized trials. These measures are essential to establish minimal effective “connectivity doses,” improve cost-efficiency, and facilitate the integration of network-based rehabilitation into everyday clinical practice.
Author Contributions
J.A.K.: Conceptualization, methodology, analysis, writing, original draft preparation, review and editing, project administration. N.H.: Analysis, writing, review, and editing. F.R.C.: Analysis, writing, review, and editing. M.J.: Conceptualization, methodology, analysis, writing, original draft preparation, review and editing, project administration, and supervision. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Johnson, C.O.; Nguyen, M.; Roth, G.A.; Nichols, E.; Alam, T.; Abate, D.; Abd-Allah, F.; Abdelalim, A.; Abraha, H.N.; Abu-Rmeileh, N.M.; et al. Global, regional, and national burden of stroke, 1990–2016: A systematic analysis for the global burden of disease study 2016. Lancet Neurol. 2019, 18, 439–458. [Google Scholar] [CrossRef]
- Feigin, V.L.; Stark, B.A.; Johnson, C.O.; Roth, G.A.; Bisignano, C.; Abady, G.G.; Abbasifard, M.; Abbasi-Kangevari, M.; Abd-Allah, F.; Abedi, V.; et al. Global, regional, and national burden of stroke and its risk factors, 1990–2019: A systematic analysis for the global burden of disease study 2019. Lancet Neurol. 2021, 20, 795–820. [Google Scholar] [CrossRef] [PubMed]
- Corbetta, M.; Siegel, J.S.; Shulman, G.L. On the low dimensionality of behavioral deficits and alterations of brain network connectivity after focal injury. Cortex 2018, 107, 229–237. [Google Scholar] [CrossRef] [PubMed]
- Corbetta, M.; Ramsey, L.; Callejas, A.; Baldassarre, A.; Hacker, C.D.; Siegel, J.S.; Astafiev, S.V.; Rengachary, J.; Zinn, K.; Lang, C.E.; et al. Common behavioral clusters and subcortical anatomy in stroke. Neuron 2015, 85, 927–941. [Google Scholar] [CrossRef] [PubMed]
- Siegel, J.S.; Ramsey, L.E.; Snyder, A.Z.; Metcalf, N.V.; Chacko, R.V.; Weinberger, K.; Baldassarre, A.; Hacker, C.D.; Shulman, G.L.; Corbetta, M. Disruptions of network connectivity predict impairment in multiple behavioral domains after stroke. Proc. Natl. Acad. Sci. USA 2016, 113, E4367–E4376. [Google Scholar] [CrossRef]
- Van Den Heuvel, M.P.; Sporns, O. A cross-disorder connectome landscape of brain dysconnectivity. Nat. Rev. Neurosci. 2019, 20, 435–446. [Google Scholar] [CrossRef]
- Grefkes, C.; Fink, G.R. Connectivity-based approaches in stroke and recovery of function. Lancet Neurol. 2014, 13, 206–216. [Google Scholar] [CrossRef]
- Rehme, A.K.; Grefkes, C. Cerebral network disorders after stroke: Evidence from imaging-based connectivity analyses of active and resting brain states in humans. J. Physiol. 2013, 591, 17–31. [Google Scholar] [CrossRef]
- Wang, L.; Yu, C.; Chen, H.; Qin, W.; He, Y.; Fan, F.; Zhang, Y.; Wang, M.; Li, K.; Zang, Y.; et al. Dynamic functional reorganization of the motor execution network after stroke. Brain 2010, 133, 1224–1238. [Google Scholar] [CrossRef]
- Baldassarre, A.; Ramsey, L.E.; Siegel, J.S.; Shulman, G.L.; Corbetta, M. Brain connectivity and neurological disorders after stroke. Curr. Opin. Neurol. 2016, 29, 706–713. [Google Scholar] [CrossRef]
- Heilman, K.M.; Valenstein, E.; Watson, R.T. Neglect and related disorders. Semin. Neurol. 2000, 20, 463–470. [Google Scholar] [CrossRef]
- Carter, A.R.; Astafiev, S.V.; Lang, C.E.; Connor, L.T.; Rengachary, J.; Strube, M.J.; Pope, D.L.W.; Shulman, G.L.; Corbetta, M. Resting interhemispheric functional magnetic resonance imaging connectivity predicts performance after stroke. Ann. Neurol. 2010, 67, 365–375. [Google Scholar] [CrossRef]
- Fox, M.D.; Halko, M.A.; Eldaief, M.C.; Pascual-Leone, A. Measuring and manipulating brain connectivity with resting state functional connectivity magnetic resonance imaging (fcmri) and transcranial magnetic stimulation (tms). Neuroimage 2012, 62, 2232–2243. [Google Scholar] [CrossRef] [PubMed]
- De Schotten, M.T.; Foulon, C.; Nachev, P. Brain disconnections link structural connectivity with function and behaviour. Nat. Commun. 2020, 11, 5094. [Google Scholar] [CrossRef] [PubMed]
- Lindenberg, R.; Renga, V.; Zhu, L.L.; Nair, D.; Schlaug, G. Bihemispheric brain stimulation facilitates motor recovery in chronic stroke patients. Neurology 2010, 75, 2176–2184. [Google Scholar] [CrossRef] [PubMed]
- Di Pino, G.; Pellegrino, G.; Assenza, G.; Capone, F.; Ferreri, F.; Formica, D.; Ranieri, F.; Tombini, M.; Ziemann, U.; Rothwell, J.C.; et al. Modulation of brain plasticity in stroke: A novel model for neurorehabilitation. Nat. Rev. Neurol. 2014, 10, 597–608. [Google Scholar] [CrossRef]
- Hamoudi, M.; Schambra, H.M.; Fritsch, B.; Schoechlin-Marx, A.; Weiller, C.; Cohen, L.G.; Reis, J. Transcranial direct current stimulation enhances motor skill learning but not generalization in chronic stroke. Neurorehabil. Neural Repair 2018, 32, 295–308. [Google Scholar] [CrossRef]
- Chowdhury, N.S.; Rogasch, N.C.; Chiang, A.K.I.; Millard, S.K.; Skippen, P.; Chang, W.-J.; Bilska, K.; Si, E.; Seminowicz, D.A.; Schabrun, S.M. The influence of sensory potentials on transcranial magnetic stimulation—electroencephalography recordings. Clin. Neurophysiol. 2022, 140, 98–109. [Google Scholar] [CrossRef]
- Devi, M.; Arumugum, N.; Midha, D. Combined effect of transcranial direct current stimulation (tdcs) and functional electrical stimulation (fes) on upper limb recovery in patients with subacute stroke. J. Neurol. Stroke 2019, 9, 140–145. [Google Scholar] [CrossRef]
- Gulati, T.; Won, S.J.; Ramanathan, D.S.; Wong, C.C.; Bodepudi, A.; Swanson, R.A.; Ganguly, K. Robust neuroprosthetic control from the stroke perilesional cortex. J. Neurosci. 2015, 35, 8653–8661. [Google Scholar] [CrossRef]
- Maier, M.; Ballester, B.R.; Verschure, P.F.M.J. Principles of neurorehabilitation after stroke based on motor learning and brain plasticity mechanisms. Front. Syst. Neurosci. 2019, 13, 74. [Google Scholar] [CrossRef]
- Veerbeek, J.M.; Van Wegen, E.; Van Peppen, R.; Van Der Wees, P.J.; Hendriks, E.; Rietberg, M.; Kwakkel, G. What is the evidence for physical therapy poststroke? A systematic review and meta-analysis. PLoS ONE 2014, 9, e87987. [Google Scholar] [CrossRef] [PubMed]
- McGlinchey, M.P.; James, J.; McKevitt, C.; Douiri, A.; McLachlan, S.; Sackley, C.M. The effect of rehabilitation interventions on physical function and immobility-related complications in severe stroke-protocol for a systematic review. Syst. Rev. 2018, 7, 197. [Google Scholar] [CrossRef] [PubMed]
- Dimyan, M.A.; Cohen, L.G. Neuroplasticity in the context of motor rehabilitation after stroke. Nat. Rev. Neurol. 2011, 7, 76–85. [Google Scholar] [CrossRef] [PubMed]
- Takeuchi, N.; Izumi, S.-I. Rehabilitation with poststroke motor recovery: A review with a focus on neural plasticity. Stroke Res. Treat. 2013, 2013, 1–13. [Google Scholar] [CrossRef]
- Pekna, M.; Pekny, M.; Nilsson, M. Modulation of neural plasticity as a basis for stroke rehabilitation. Stroke 2012, 43, 2819–2828. [Google Scholar] [CrossRef]
- Langhorne, P.; Bernhardt, J.; Kwakkel, G. Stroke rehabilitation. Lancet 2011, 377, 1693–1702. [Google Scholar] [CrossRef]
- Higgins, J.; Koski, L.; Xie, H. Combining rtms and task-oriented training in the rehabilitation of the arm after stroke: A pilot randomized controlled trial. Stroke Res. Treat. 2013, 2013, 539146. [Google Scholar] [CrossRef]
- Hummel, F.C.; Cohen, L.G. Non-invasive brain stimulation: A new strategy to improve neurorehabilitation after stroke? Lancet Neurol. 2006, 5, 708–712. [Google Scholar] [CrossRef]
- Cumming, T.B.; Marshall, R.S.; Lazar, R.M. Stroke, cognitive deficits, and rehabilitation: Still an incomplete picture. Int. J. Stroke 2013, 8, 38–45. [Google Scholar] [CrossRef]
- Pendlebury, S.T.; Rothwell, P.M. Prevalence, incidence, and factors associated with pre-stroke and post-stroke dementia: A systematic review and meta-analysis. Lancet Neurol. 2009, 8, 1006–1018. [Google Scholar] [CrossRef]
- Carter, A.R.; Patel, K.R.; Astafiev, S.V.; Snyder, A.Z.; Rengachary, J.; Strube, M.J.; Pope, A.; Shimony, J.S.; Lang, C.E.; Shulman, G.L.; et al. Upstream dysfunction of somatomotor functional connectivity after corticospinal damage in stroke. Neurorehabil. Neural Repair 2012, 26, 7–19. [Google Scholar] [CrossRef]
- Bai, Z.; Zhang, J.; Fong, K.N.K. Effects of transcranial magnetic stimulation in modulating cortical excitability in patients with stroke: A systematic review and meta-analysis. J. Neuroeng. Rehabil. 2022, 19, 24. [Google Scholar] [CrossRef]
- Ramsey, L.E.; Siegel, J.S.; Lang, C.E.; Strube, M.; Shulman, G.L.; Corbetta, M. Behavioural clusters and predictors of performance during recovery from stroke. Nat. Hum. Behav. 2017, 1, 38. [Google Scholar] [CrossRef] [PubMed]
- Van Meer, M.P.A.; Van Der Marel, K.; Wang, K.; Otte, W.M.; El Bouazati, S.; Roeling, T.A.P.; Viergever, M.A.; Berkelbach Van Der Sprenkel, J.W.; Dijkhuizen, R.M. Recovery of sensorimotor function after experimental stroke correlates with restoration of resting-state interhemispheric functional connectivity. J. Neurosci. 2010, 30, 3964–3972. [Google Scholar] [CrossRef] [PubMed]
- Miotto, E.C.; Bazán, P.R.; Batista, A.X.; Conforto, A.B.; Figueiredo, E.G.; Martin, M.d.G.M.; Avolio, I.B.; Amaro, E.; Teixeira, M.J. Behavioral and neural correlates of cognitive training and transfer effects in stroke patients. Front. Neurol. 2020, 11. [Google Scholar] [CrossRef] [PubMed]
- Sebastián-Romagosa, M.; Udina, E.; Ortner, R.; Dinarès-Ferran, J.; Cho, W.; Murovec, N.; Matencio-Peralba, C.; Sieghartsleitner, S.; Allison, B.Z.; Guger, C. Eeg biomarkers related with the functional state of stroke patients. Front. Neurosci. 2020, 14, 582. [Google Scholar] [CrossRef]
- Yin, M.; Liu, Y.; Zhang, L.; Zheng, H.; Peng, L.; Ai, Y.; Luo, J.; Hu, X. Effects of rtms treatment on cognitive impairment and resting-state brain activity in stroke patients: A randomized clinical trial. Front. Neural Circuits 2020, 14, 563777. [Google Scholar] [CrossRef]
- Lawrence, B.J.; Gasson, N.; Bucks, R.S.; Troeung, L.; Loftus, A.M. Cognitive training and noninvasive brain stimulation for cognition in parkinson’s disease: A meta-analysis. Neurorehabil. Neural Repair 2017, 31, 597–608. [Google Scholar] [CrossRef]
- Qin, Y.; Liu, X.; Zhang, Y.; Wu, J.; Wang, X. Effects of transcranial combined with peripheral repetitive magnetic stimulation on limb spasticity and resting-state brain activity in stroke patients. Front. Hum. Neurosci. 2023, 17, 992424. [Google Scholar] [CrossRef]
- Middag-van Spanje, M.; Nijboer, T.C.W.; Schepers, J.; Van Heugten, C.; Sack, A.T.; Schuhmann, T. Alpha transcranial alternating current stimulation as add-on to neglect training: A randomized trial. Brain Commun. 2024, 6, fcae287. [Google Scholar] [CrossRef]
- Cheng, C.; Liu, T.; Zhang, B.; Wu, X.; Song, Z.; Zhao, Z.; Ren, X.; Zhao, M.; Su, Y.; Wang, J. Effects of robot-assisted hand function therapy on brain functional mechanisms: A synchronized study using fnirs and semg. Front. Med. 2024, 11, 1411616. [Google Scholar] [CrossRef]
- Sinha, A.M.; Nair, V.A.; Prabhakaran, V. Brain-computer interface training with functional electrical stimulation: Facilitating changes in interhemispheric functional connectivity and motor outcomes post-stroke. Front. Neurosci. 2021, 15, 670953. [Google Scholar] [CrossRef] [PubMed]
- Mekbib, D.B.; Zhao, Z.; Wang, J.; Xu, B.; Zhang, L.; Cheng, R.; Fang, S.; Shao, Y.; Yang, W.; Han, J.; et al. Proactive motor functional recovery following immersive virtual reality–based limb mirroring therapy in patients with subacute stroke. Neurotherapeutics 2020, 17, 1919–1930. [Google Scholar] [CrossRef] [PubMed]
- Wittenberg, G.F.; Chen, R.; Ishii, K.; Bushara, K.O.; Taub, E.; Gerber, L.H.; Hallett, M.; Cohen, L.G. Constraint-induced therapy in stroke: Magnetic-stimulation motor maps and cerebral activation. Neurorehabil. Neural Repair 2003, 17, 48–57. [Google Scholar] [CrossRef] [PubMed]
- Fan, Y.T.; Wu, C.Y.; Liu, H.L.; Lin, K.C.; Wai, Y.Y.; Chen, Y.L. Neuroplastic changes in resting-state functional connectivity after stroke rehabilitation. Front. Hum. Neurosci. 2015, 9, 546. [Google Scholar] [CrossRef]
- Hu, M.; Cheng, H.-J.; Ji, F.; Chong, J.S.X.; Lu, Z.; Huang, W.; Ang, K.K.; Phua, K.S.; Chuang, K.-H.; Jiang, X.; et al. Brain functional changes in stroke following rehabilitation using brain-computer interface-assisted motor imagery with and without tdcs: A pilot study. Front. Hum. Neurosci. 2021, 15, 692304. [Google Scholar] [CrossRef]
- Wada, K.; Ono, Y.; Kurata, M.; (Imanishi) Ito, M.; (Tani) Minakuchi, M.; Kono, M.; Tominaga, T. Development of a brain-machine interface for stroke rehabilitation using event-related desynchronization and proprioceptive feedback. Adv. Biomed. Eng. 2019, 8, 53–59. [Google Scholar] [CrossRef]
- Phang, C.-R.; Su, K.-H.; Cheng, Y.-Y.; Chen, C.-H.; Ko, L.-W. Time synchronization between parietal–frontocentral connectivity with mrcp and gait in post-stroke bipedal tasks. J. Neuroeng. Rehabil. 2024, 21, 101. [Google Scholar] [CrossRef]
- Li, H.; Ji, H.; Yu, J.; Li, J.; Jin, L.; Liu, L.; Bai, Z.; Ye, C. A sequential learning model with gnn for eeg-emg-based stroke rehabilitation bci. Front. Neurosci. 2023, 17, 1125230. [Google Scholar] [CrossRef]
- Gangemi, A.; De Luca, R.; Fabio, R.A.; Lauria, P.; Rifici, C.; Pollicino, P.; Marra, A.; Olivo, A.; Quartarone, A.; Calabrò, R.S. Effects of virtual reality cognitive training on neuroplasticity: A quasi-randomized clinical trial in patients with stroke. Biomedicines 2023, 11, 3225. [Google Scholar] [CrossRef] [PubMed]
- Ray, A.M.; Figueiredo, T.D.C.; López-Larraz, E.; Birbaumer, N.; Ramos-Murguialday, A. Brain oscillatory activity as a biomarker of motor recovery in chronic stroke. Hum. Brain Mapp. 2020, 41, 1296–1308. [Google Scholar] [CrossRef] [PubMed]
- Phang, C.-R.; Chen, C.-H.; Cheng, Y.-Y.; Chen, Y.-J.; Ko, L.-W. Frontoparietal dysconnection in covert bipedal activity for enhancing the performance of the motor preparation-based brain–computer interface. IEEE Trans. Neural Syst. Rehabil. Eng. 2023, 31, 139–149. [Google Scholar] [CrossRef] [PubMed]
- Carino-Escobar, R.I.; Carrillo-Mora, P.; Valdés-Cristerna, R.; Rodriguez-Barragan, M.A.; Hernandez-Arenas, C.; Quinzaños-Fresnedo, J.; Galicia-Alvarado, M.A.; Cantillo-Negrete, J. Longitudinal analysis of stroke patients’ brain rhythms during an intervention with a brain-computer interface. Neural Plast. 2019, 2019, 7084618. [Google Scholar] [CrossRef]
- Chen, Y.; Su, W.; Gui, C.-F.; Guo, Q.-F.; Tan, H.-X.; He, L.; Jiang, H.-H.; Wei, Q.-C.; Gao, Q. Effectiveness of cerebellar vermis intermittent theta-burst stimulation in improving trunk control and balance function for patients with subacute stroke: A randomised controlled trial protocol. BMJ Open 2023, 13, e066356. [Google Scholar] [CrossRef]
- Ramos-Murguialday, A.; Curado, M.R.; Broetz, D.; Yilmaz, Ö.; Brasil, F.L.; Liberati, G.; Garcia-Cossio, E.; Cho, W.; Caria, A.; Cohen, L.G.; et al. Brain-machine interface in chronic stroke: Randomized trial long-term follow-up. Neurorehabil. Neural Repair 2019, 33, 188–198. [Google Scholar] [CrossRef]
- Li, M.; Chen, J.; He, B.; He, G.; Zhao, C.-G.; Yuan, H.; Xie, J.; Xu, G.; Li, J. Stimulation enhancement effect of the combination of exoskeleton-assisted hand rehabilitation and fingertip haptic stimulation. Front. Neurosci. 2023, 17, 1149265. [Google Scholar] [CrossRef]
- Ripollés, P.; Rojo, N.; Grau-Sánchez, J.; Amengual, J.L.; Càmara, E.; Marco-Pallarés, J.; Juncadella, M.; Vaquero, L.; Rubio, F.; Duarte, E.; et al. Music supported therapy promotes motor plasticity in individuals with chronic stroke. Brain Imaging Behav. 2016, 10, 1289–1307. [Google Scholar] [CrossRef]
- Chen, Y.; Zhao, Z.; Huang, J.; Wang, T.; Qu, Y. Computer-aided cognitive training combined with tdcs can improve post-stroke cognitive impairment and cerebral vasomotor function: A randomized controlled trial. BMC Neurol. 2024, 24, 132. [Google Scholar] [CrossRef]
- Pollock, A.; St George, B.; Fenton, M.; Firkins, L. Top 10 research priorities relating to life after stroke—consensus from stroke survivors, caregivers, and health professionals. Int. J. Stroke 2014, 9, 313–320. [Google Scholar] [CrossRef]
- Guggisberg, A.G.; Koch, P.J.; Hummel, F.C.; Buetefisch, C.M. Brain networks and their relevance for stroke rehabilitation. Clin. Neurophysiol. 2019, 130, 1098–1124. [Google Scholar] [CrossRef]
- Cassidy, J.M.; Wodeyar, A.; Srinivasan, R.; Cramer, S.C. Abstract tmp42: Coherent neural oscillations inform early stroke motor recovery. Stroke 2020, 51 (Suppl. S1), ATMP42. [Google Scholar] [CrossRef]
- Ward, N.S.; Brown, M.M.; Thompson, A.J.; Frackowiak, R.S.J. Neural correlates of outcome after stroke: A cross-sectional fmri study. Brain 2003, 126, 1430–1448. [Google Scholar] [CrossRef]
- Veldsman, M.; Curwood, E.; Pathak, S.; Werden, E.; Brodtmann, A. Default mode network neurodegeneration reveals the remote effects of ischaemic stroke. J. Neurol. Neurosurg. Psychiatry 2018, 89, 318. [Google Scholar] [CrossRef]
- Kwakkel, G.; Wagenaar, R.C.; Koelman, T.W.; Lankhorst, G.J.; Koetsier, J.C. Effects of intensity of rehabilitation after stroke: A research synthesis. Stroke 1997, 28, 1550–1556. [Google Scholar] [CrossRef] [PubMed]
- Granger, C.V.; Hamilton, B.B.; Keith, R.A.; Zielezny, M.; Sherwin, F.S. Advances in functional assessment for medical rehabilitation. Top. Geriatr. Rehabil. 1986, 1, 59–74. [Google Scholar] [CrossRef]
- Berg, K.O.; Wood-Dauphinee, S.L.; Williams, J.I.; Maki, B. Measuring balance in the elderly: Validation of an instrument. Can. J. Public Health. 1992, 83 (Suppl. S2), S7–S11. [Google Scholar] [PubMed]
- Cramer, S.C.; Dodakian, L.; Le, V.; See, J.; Augsburger, R.; McKenzie, A.; Zhou, R.J.; Chiu, N.L.; Heckhausen, J.; Cassidy, J.M.; et al. Efficacy of home-based telerehabilitation vs in-clinic therapy for adults after stroke: A randomized clinical trial. JAMA Neurol. 2019, 76, 1079. [Google Scholar] [CrossRef]
- Laver, K.E.; Adey-Wakeling, Z.; Crotty, M.; Lannin, N.A.; George, S.; Sherrington, C. Telerehabilitation services for stroke. Cochrane Database Syst. Rev. 2020, 1, CD010255. [Google Scholar] [CrossRef]
- Taub, E.; Miller, N.E.; Novack, T.A.; Cook, E.W., 3rd; Fleming, W.C.; Nepomuceno, C.S.; Connell, J.S.; Crago, J.E. Technique to improve chronic motor deficit after stroke. Arch. Phys. Med. Rehabil. 1993, 74, 347–354. [Google Scholar]
- Wolf, S.L.; Winstein, C.J.; Miller, J.P.; Taub, E.; Uswatte, G.; Morris, D.; Giuliani, C.; Light, K.E.; Nichols-Larsen, D.; Excite Investigators, F.T. Effect of constraint-induced movement therapy on upper extremity function 3 to 9 months after stroke: The excite randomized clinical trial. JAMA 2006, 296, 2095. [Google Scholar] [CrossRef]
- Bastian, A.J. Understanding sensorimotor adaptation and learning for rehabilitation. Curr. Opin. Neurol. 2008, 21, 628–633. [Google Scholar] [CrossRef]
- Bobath, B. Adult Hemiplegia: Evaluation and Treatment, 3rd ed.; Heinemann Medical Books: Oxford, UK, 1990. [Google Scholar]
- Konosu, A.; Matsuki, Y.; Fukuhara, K.; Funato, T.; Yanagihara, D. Roles of the cerebellar vermis in predictive postural controls against external disturbances. Sci. Rep. 2024, 14, 3162. [Google Scholar] [CrossRef]
- Li, X.; Qi, G.; Yu, C.; Lian, G.; Zheng, H.; Wu, S.; Yuan, T.-F.; Zhou, D. Cortical plasticity is correlated with cognitive improvement in alzheimer’s disease patients after rtms treatment. Brain Stimul. 2021, 14, 503–510. [Google Scholar] [CrossRef]
- Lo, A.C.; Guarino, P.D.; Richards, L.G.; Haselkorn, J.K.; Wittenberg, G.F.; Federman, D.G.; Ringer, R.J.; Wagner, T.H.; Krebs, H.I.; Volpe, B.T.; et al. Robot-assisted therapy for long-term upper-limb impairment after stroke. N. Engl. J. Med. 2010, 362, 1772–1783. [Google Scholar] [CrossRef] [PubMed]
- Mehrholz, J.; Pohl, M.; Platz, T.; Kugler, J.; Elsner, B. Electromechanical and robot-assisted arm training for improving activities of daily living, arm function, and arm muscle strength after stroke. Cochrane Database Syst. Rev. 2018, 2018, CD006876. [Google Scholar] [CrossRef] [PubMed]
- Kleim, J.A.; Jones, T.A. Principles of experience-dependent neural plasticity: Implications for rehabilitation after brain damage. J. Speech. Lang. Hear. Res. 2008, 51, S225–S239. [Google Scholar] [CrossRef] [PubMed]
- Nudo, R.J. Mechanisms for recovery of motor function following cortical damage. Curr. Opin. Neurobiol. 2006, 16, 638–644. [Google Scholar] [CrossRef]
- Ward, N.S. Restoring brain function after stroke—bridging the gap between animals and humans. Nat. Rev. Neurol. 2017, 13, 244–255. [Google Scholar] [CrossRef]
- Calautti, C.; Baron, J.-C. Functional neuroimaging studies of motor recovery after stroke in adults: A review. Stroke 2003, 34, 1553–1566. [Google Scholar] [CrossRef]
- Dancause, N.; Nudo, R.J. Shaping plasticity to enhance recovery after injury. In Progress in Brain Research; Elsevier: Amsterdam, The Netherlands, 2011; Volume 192, pp. 273–295. [Google Scholar]
- Ramos-Murguialday, A.; Broetz, D.; Rea, M.; Läer, L.; Yilmaz, Ö.; Brasil, F.L.; Liberati, G.; Curado, M.R.; Garcia-Cossio, E.; Vyziotis, A.; et al. Brain–machine interface in chronic stroke rehabilitation: A controlled study. Ann. Neurol. 2013, 74, 100–108. [Google Scholar] [CrossRef] [PubMed]
- Khademi, F.; Naros, G.; Nicksirat, A.; Kraus, D.; Gharabaghi, A. Rewiring cortico-muscular control in the healthy and poststroke human brain with proprioceptive β-band neurofeedback. J. Neurosci. 2022, 42, 6861–6877. [Google Scholar] [CrossRef] [PubMed]
- Laver, K.E.; Lange, B.; George, S.; Deutsch, J.E.; Saposnik, G.; Crotty, M. Virtual reality for stroke rehabilitation. Cochrane Database Syst. Rev. 2017, 11, CD008349. [Google Scholar] [CrossRef] [PubMed]
- Da Silva Cameirão, M.; Bermúdez, I.; Badia, S.; Duarte, E.; Verschure, P.F.M.J. Virtual reality based rehabilitation speeds up functional recovery of the upper extremities after stroke: A randomized controlled pilot study in the acute phase of stroke using the rehabilitation gaming system. Restor. Neurol. Neurosci. 2011, 29, 287–298. [Google Scholar] [CrossRef]
- Weiss, P.L.; Rand, D.; Katz, N.; Kizony, R. Video capture virtual reality as a flexible and effective rehabilitation tool. J. Neuroeng. Rehabil. 2004, 1, 12. [Google Scholar] [CrossRef]
- Thieme, H.; Morkisch, N.; Mehrholz, J.; Pohl, M.; Behrens, J.; Borgetto, B.; Dohle, C. Mirror therapy for improving motor function after stroke. Cochrane Database Syst. Rev. 2018, 2018, CD008449. [Google Scholar] [CrossRef]
- Ertelt, D.; Small, S.; Solodkin, A.; Dettmers, C.; McNamara, A.; Binkofski, F.; Buccino, G. Action observation has a positive impact on rehabilitation of motor deficits after stroke. Neuroimage 2007, 36, T164–T173. [Google Scholar] [CrossRef]
- Marchal-Crespo, L.; Reinkensmeyer, D.J. Review of control strategies for robotic movement training after neurologic injury. J. Neuroeng. Rehabil. 2009, 6, 20. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



