Submitted:
22 September 2025
Posted:
24 September 2025
You are already at the latest version
Abstract
Therapies targeting human epidermal growth factor receptor 2 (HER2) have substantially improved overall survival in patients with HER2-positive metastatic breast cancer. Approximately 31% of these patients develop brain metastases, representing a significant therapeutic challenge. This review classifies anti-HER2 therapies into three categories: monoclonal antibodies (MABs), antibody-drug conjugates (ADCs), and tyrosine kinase inhibitors (TKIs). The mechanisms of action and clinical impacts of these agents are examined, with particular attention to intracranial efficacy. The introduction of trastuzumab increased overall survival (OS) from 20.3 to 25.1 months compared to chemotherapy alone. The addition of pertuzumab further extended survival to 57.1 months, as demonstrated in the CLEOPATRA trial. Among ADCs, T-DM1 improved OS to 29.9 months versus 25.9 months in the EMILIA trial, while T-DXd extended OS to 52.6 months in DESTINY-Breast03. T-DXd also demonstrated notable intracranial activity, achieving a 64.9% objective response rate in patients with active brain metastases. In the HER2CLIMB trial, tucatinib reduced intracranial progression by 68% and improved OS (24.7 vs. 19.2 months) in patients with active brain metastases. Recent advances have increased median OS from approximately 20 months prior to trastuzumab to over 50 months with current therapies. Future research should focus on optimizing treatment sequencing, refining biomarker-driven approaches, and developing targeted strategies for brain metastases to further improve long-term survival outcomes.
Keywords:
HER2-positive breast cancer
; metastatic breast cancer
; anti-HER2 therapies
; brain metastases
; overall survival
; monoclonal antibodies
; antibody-drug conjugates
; tyrosine kinase inhibitors
Introduction
Breast cancer is the most commonly diagnosed malignancy and the leading cause of cancer-related mortality among women worldwide [1]. HER2-positive breast cancer accounts for approximately 20% of all cases [2]. Both HER2-positive and triple-negative subtypes are associated with poor prognoses, characterized by early and frequent recurrences and metastasis. However, the prognosis for HER2-positive disease is more favorable than for triple-negative breast cancer, primarily due to the benefits of targeted therapies [3]. The identification of EGFR in 1978 and HER2 in 1984, as well as the recognition of HER2 overexpression as a negative prognostic factor, facilitated the development of targeted therapies that have transformed breast cancer management [4]. In recent decades, significant advances in targeted therapies have markedly improved outcomes for these patients. The FDA approved trastuzumab, a humanized monoclonal antibody, for HER2-positive metastatic breast cancer in 1998. This major advance improved survival and established drug-diagnostic development [5]. Trastuzumab’s success greatly influenced cancer drug development, spurring advances in HER2-targeted therapy. Pertuzumab is an anti-HER2 antibody that binds a distinct domain of the HER2 receptor compared to trastuzumab. When combined with trastuzumab and other therapies, pertuzumab can help overcome resistance and enhance treatment efficacy. It is also associated with a favorable safety profile [6]. Small-molecule kinase inhibitors, such as lapatinib and tucatinib, target HER2 and have emerged as effective treatments for HER2-positive breast cancer. These drugs have significantly improved survival outcomes for patients with advanced disease, especially when used in combination with other therapies [7]. HER2-targeting Antibody-Drug Conjugates (ADCs) mark a significant advancement in breast cancer treatment. These therapies use antibody specificity to deliver potent cytotoxic payloads directly to cancer cells. HER2-targeting ADCs, such as Trastuzumab Emtansine (T-DM1) and Trastuzumab Deruxtecan (T-DXd), use varying mechanisms of action. They show promise in treating both HER2-positive and HER2-low breast cancer, offering improved efficacy and expanding treatment options [8]. This review provides a comprehensive update on anti-HER2-targeted therapies and their impact on overall survival. The mechanisms of action of these agents are examined, and results from recent clinical trials, including phase III studies, are analyzed with respect to progression-free and overall survival. Toxicity profiles and side effects are considered to evaluate the benefit-to-risk ratio and inform strategies for optimizing clinical use. Future research perspectives are also discussed, with emphasis on novel agents, therapeutic combinations, and intracranial activity.
Anti-HER2 Therapies
Monoclonal Antibodies (MAB)
Trastuzumab and pertuzumab, two monoclonal antibodies, have revolutionized the treatment of HER2-positive breast cancer. Both target the HER2 receptor in distinct ways. Trastuzumab was the first monoclonal antibody developed. De et al. explored how trastuzumab works, highlighting three main mechanisms. First, it disrupts the HER2–HER3 heterodimerization that drives tumor growth in HER2-overexpressing cancers. Second, it prevents the cleavage of the HER2 extracellular domain, stopping the production of the active p95HER2 fragment associated with aggressive tumor behavior. Lastly, trastuzumab activates the immune system by inducing antibody-dependent cellular cytotoxicity (ADCC), where immune cells target and destroy HER2-positive tumor cells [9]. At present, trastuzumab is used in the neoadjuvant, adjuvant, and metastatic settings in the treatment of HER2-positive breast cancer. The H0648g trial, a pivotal phase 3 study, investigated the impact of adding trastuzumab to standard chemotherapy regimens in patients with early-stage HER2-positive breast cancer. Compared to chemotherapy alone, the addition of trastuzumab demonstrated a significant improvement in key clinical outcomes in terms of progression-free survival (PFS) (median 7.4 vs. 4.6 months; p < .001) and overall survival (OS) (median 25.1 vs. 20.3 months; p =.01) [10]. A multicenter randomized trial was conducted in 2025 that demonstrated the efficacy of trastuzumab, in combination with docetaxel, in the metastatic setting of HER2-positive breast cancer. The combination resulted in higher response rates, longer overall survival (median of 31.2 months versus 22.7 months; P = .0325), and longer time to disease progression and treatment failure, with additional manageable toxicity [11]. A prospective observational study conducted in Germany evaluated the impact of continuing trastuzumab treatment beyond disease progression in patients with advanced or metastatic breast cancer. The findings indicated that patients who received trastuzumab beyond progression experienced improved survival outcomes compared to those who did not continue the treatment. This suggests that maintaining trastuzumab therapy, even after disease progression, may offer survival benefits for patients with advanced or metastatic breast cancer [12]. In HER2-positive hormone receptor (HR)-co-positive tumors, the TAnDEM trial demonstrated improved progression-free survival with trastuzumab plus anastrozole versus anastrozole alone (4.8 vs. 2.4 months), although overall survival was not significantly different (Median OS was 28.5 months in the trastuzumab plus anastrozole arm and 23.9 months in the anastrozole alone arm, log-rankP= .325), likely due to cross-over [10] Pertuzumab primarily works by binding to the HER2 dimerization domain, blocking HER2 from associating with other HER receptors, especially HER2/HER3 complexes driven by ligands like heregulin. While it induces ADCC, this is not essential for its action, and it does not prevent HER2 shedding [13]. The combination of trastuzumab and pertuzumab represents a significant advancement in the treatment of HER2-positive breast cancer. Their synergistic action effectively targets the HER2 receptor, improving clinical outcomes with an acceptable safety profile [14]. The CLEOPATRA trial is a phase 3, randomized, double-blind trial that compared pertuzumab plus trastuzumab and docetaxel with placebo plus trastuzumab and docetaxel in patients with HER2+ metastatic breast cancer. The median OS was 57.1 months (95% CI: 50 - 72) in the pertuzumab group compared with 40.8 months (95% CI: 36 - 48) in the placebo group, with a benefit of 16.3 months for pertuzumab. One serious adverse event that occurred in the pertuzumab treatment arm was congestive heart failure. Therefore, the final results of the phase 3 CLEOPATRA study reveal that first-line treatment of HER2+ metastatic breast cancer with pertuzumab plus trastuzumab and docetaxel offers an advantage in overall survival even in the long term (37% chance of being alive in 8 years vs. 23% with placebo plus trastuzumab and docetaxel), changing the natural history of this disease [15]. The Phase IIIb PERUSE study further evaluated the double anti-HER2 blockade with trastuzumab and pertuzumab, combined with different taxane backbones, in the first-line setting. Among 1436 treated patients, median PFS was 20.7 months, with similar efficacy across hormone receptor subgroups. Paclitaxel, used in 41% of patients, showed comparable efficacy to docetaxel and nab-paclitaxel, with median PFS of 23, 19.6, and 18 months, respectively. The overall response rates (ORRs) were 83%, 79%, and 77% with paclitaxel, docetaxel, and nab-paclitaxel, respectively [16]. Median OS reached 65.3 months, particularly favorable in hormone receptor–positive patients. These findings confirm the robustness of pertuzumab-based regimens and support paclitaxel as a valid alternative to docetaxel, offering a more favorable toxicity profile with preserved efficacy [17]. These results suggest that paclitaxel is a viable alternative to docetaxel, leading to similar PFS and ORR results with a predictable toxicity profile [18]. The PHEREXA trial evaluated the benefit of adding pertuzumab to trastuzumab and capecitabine in patients with HER2-positive metastatic breast cancer who had progressed on prior trastuzumab-based therapy [19]. While the primary endpoint of progression-free survival did not reach statistical significance, the final analysis revealed a significant improvement in overall survival for patients receiving the combination of trastuzumab and pertuzumab compared to trastuzumab alone. Although the study did not meet its primary endpoint, these findings suggest that dual HER2 inhibition may offer a survival benefit in the second-line setting for patients with HER2-positive metastatic breast cancer [20]. The PERTAIN study demonstrated that the addition of pertuzumab to therapy with trastuzumab and aromatase inhibitors improved progression-free survival in patients with HER2-positive, hormone receptor-positive breast cancer, particularly in those who had not received prior chemotherapy (median 20.6 months vs. 15.8 months). In the final analysis, no significant difference in overall survival was observed between the two treatment arms. [21].
New Anti-HER2 mAB (Monoclonal Antibody)
Margetuximab is an Fc-engineered anti-HER2 immunoglobulin G monoclonal antibody that targets the same epitope as trastuzumab, with similar antiproliferative effects but a higher binding affinity for the receptor [22,23]. The SOPHIA trial showed no significant overall survival (OS) difference between margetuximab and trastuzumab in HER2-positive advanced breast cancer (21.6 vs. 21.9 months; HR 0.95); safety profiles were similar [24]. Exploratory analysis suggested OS benefits for margetuximab in CD16A-158FF patients and trastuzumab in CD16A-158VV patients. Safety profiles were similar; further studies on CD16A allelic variants are needed, like the MARGOT trial. Margetuximab is approved in the USA for HER2-positive MBC after two or more prior anti-HER2 therapies, based on SOPHIA trial data [25].
Antibody-Drug Conjugate (ADCs)
- -
- Old Generation ADCs
T-DM1 is an antibody-drug conjugate (ADC) that targets the HER2 receptor. It is composed of trastuzumab, a monoclonal antibody, coupled with a cytotoxic molecule called DM1. T-DM1 acts by binding to the HER2 receptor, resulting in the internalization of the HER2-T-DM1 complex within the cell. Stable binding ensures that DM1 is released only when the antibody is degraded in the lysosome. Once released, DM1 metabolites inhibit microtubule assembly, leading to cell death. T-DM1 combines the antitumor action of trastuzumab with the cytotoxic activity of DM1 metabolites within cells [26]. Some key clinical trials have demonstrated the efficacy of T-DM1 in overall survival. The phase 3 EMILIA trial showed that T-DM1 significantly improved progression-free survival and overall survival compared with lapatinib plus capecitabine in patients with HER2-positive metastatic breast cancer who had progressed on previous trastuzumab-based therapy (29-9 months [95% CI 26-3-34-1] vs 25-9 months [95% CI 22-7-28-3]; hazard ratio 0-75 [95% CI 0-64-0-88]) [27]. The phase 3 TH3RESA trial compared the efficacy of T-DM1 with the physician’s choice of treatment in patients with HER2-positive advanced breast cancer previously treated and with progression after at least two HER2-directed regimens. Median overall survival was significantly longer with trastuzumab emtansine (22.7 months) compared to the physician’s choice (15.8 months), with a hazard ratio of 0.68 (p = 0.0007) [28]. The final results confirm that trastuzumab emtansine significantly improves overall survival in these patients.
- -
- New Generation ADCs
Trastuzumab deruxtecan (T-DXd) is a HER2-targeted antibody-drug conjugate consisting of a humanized IgG1 monoclonal antibody against HER2, a cleavable tetrapeptide-based linker, and a highly potent topoisomerase I inhibitor as its cytotoxic payload [29]. T-DXd is an internationally approved, guideline-recommended treatment for patients with HER2-positive metastatic breast cancer following progression on taxane and trastuzumab or recurrence within six months of completing neoadjuvant and/or adjuvant therapy [30]. The phase 2 DESTINY-Breast01 study evaluated the significant antitumor activity of T-DXd in patients with HER2-positive metastatic breast cancer previously treated with T-DM1 [31]. The DESTINY-Breast02 trial evaluated T-DXd versus the physician’s choice treatment (trastuzumab/capecitabine or lapatinib/capecitabine) in patients with unresectable or metastatic HER2-positive breast cancer previously treated with T-DM1. T-DXd significantly improved median PFS and showed superior efficacy with a manageable safety profile. The median overall survival, a key secondary endpoint, was 39.2 months with trastuzumab deruxtecan compared to 26.5 months with the physician’s choice of treatment [32].
These studies demonstrated substantial and durable antitumor efficacy, laying the foundation for the pivotal phase 3 DESTINY-Breast03 (DB03) trial.
The approval of T-DXd in this setting was based on the results of the DB03 trial, designed to evaluate the efficacy and safety of T-DXd compared to T-DM1. Based on the outcomes of this study, T-DXd has replaced T-DM1 as the preferred treatment in this setting [33]. At the data cutoff of November 20, 2023, the DB03 study demonstrated that T-DXd improved mOS (52.6 vs. 42.7 months; HR 0.73, 95% CI 0.56–0.94) [34]. T-DXd has shown significant overall survival benefits in HER2-positive metastatic breast cancer.
Tyrosine Kinase Inhibitor (TKI)
- -
- Old Generation TKI
Lapatinib is a small-molecule tyrosine kinase inhibitor that targets EGFR and HER2, with unclear effects on pyruvate kinase type M2 (PKM2), and is used in the treatment of advanced HER-2-positive breast cancers [35,36]. In 2017, a systematic review analyzed 12 studies involving 799 patients with HER2-positive breast cancer and brain metastases (BMs) treated with lapatinib (L), alone or with capecitabine (C). The pooled overall response rate (ORR) was 21.4% (95% CI 11.7–35.9) and increased to 29.2% (95% CI 18.5–42.7) for L + C. The pooled median progression-free survival (PFS) was 4.1 months (95% CI 3.1–6.7), and overall survival (OS) was 11.2 months (95% CI 8.9–14.1) [37]. The phase II VITAL study found that lapatinib plus vinorelbine (lap+vin) had comparable efficacy and safety to lap+cap, with a median OS of 23.3 vs. 20.3 months and similar death rates (56-57%), supporting lap+vin as a treatment option for HER2-positive MBC [38].
Neratinib is a pan-HER tyrosine kinase inhibitor that blocks HER signaling, induces cell cycle arrest, downregulates HER2, and reverses multidrug resistance [39]. The phase III NALA trial demonstrated that neratinib plus capecitabine (N+C) significantly improved progression-free survival (PFS) and reduced central nervous system (CNS) disease; however, overall survival (OS) was not significantly different (HR 0.88; P = .2098) compared to lapatinib plus capecitabine (L+C) in patients with HER2-positive metastatic breast cancer [40].
- -
- New Generation TKI
Tucatinib is a selective and reversible inhibitor of HER2 protein tyrosine kinase activity, with minimal impact on EGFR inhibition, that has become a valuable treatment option for patients with HER2-positive MBC who have progressed on prior therapies [41]. The pivotal HER2CLIMB trial evaluated the efficacy and safety of tucatinib combined with trastuzumab and capecitabine in patients with HER2-positive metastatic breast cancer, including those with brain metastases- a population historically excluded from clinical trials. Final analysis showed that the tucatinib combination significantly improved overall survival (OS) compared to the placebo combination, with a median OS of 24.7 months versus 19.2 months (hazard ratio [HR]: 0.73, P = 0.004) and a 2-year OS rate of 51% versus 40%. Progression-free survival (PFS) was also notably extended [42]. The study confirmed that tucatinib, when combined with trastuzumab and capecitabine, provides a clinically meaningful survival benefit for patients with HER2-positive metastatic breast cancer. An exploratory analysis of HER2CLIMB data focusing on patients who experienced isolated CNS progression and continued on study-assigned treatment after local intervention demonstrated a prolonged median time to second progression (either intracranial or systemic) of 15.9 months in the tucatinib arm versus 9.7 months in the control group (HR: 0.29) [43]. Overall, HER2CLIMB represents the first randomized clinical trial to demonstrate an OS benefit in patients with active brain metastases from HER2-positive breast cancer. These results firmly support the therapeutic positioning of tucatinib, in combination with trastuzumab and capecitabine, as an effective option for patients with CNS-involved disease [44].
Intracranial Efficacy of Anti-HER2 Therapies
Brain metastases (BMs) represent the most lethal subset of metastatic breast cancer, highlighting the need for greater focus after diagnosis and underscoring the importance of developing individualized management strategies for these high-risk patients [45]. The incidence of BMs among patients with HER2-positive breast cancer was 31% [46]. HER2-positive patients had the longest median survival after CNS metastases (16 months), and HER2 positivity emerged as an independent prognostic factor for improved outcomes (HR 0.60, P = 0.007) [47]. Local therapies help control breast cancer brain metastases, while systemic treatments, including chemotherapy and targeted agents, are increasingly essential due to the cognitive risks of whole-brain radiotherapy [48]. Surgery is recommended for single BMs and may be considered for multiple resectable BMs; stereotactic radiosurgery (SRS) is the preferred option for 1–4 BMs and may be considered for 5–10 BMs with limited tumor volume. Whole-brain radiotherapy (WBRT) should be avoided after surgery or SRS but may be considered for multiple unresectable BMs when CNS-active systemic therapy is unavailable [49]. Highlighted by Fontanella et al., therapeutic progress in this area has long lagged behind extracranial disease management, leaving patients with brain metastases underrepresented in clinical trials and often without effective systemic options [50]. This unmet need has gradually prompted the development of CNS-active anti-HER2 agents and the inclusion of patients with brain metastases in pivotal studies, reshaping the current treatment paradigm. Two retrospective studies evaluated the efficacy of first-line trastuzumab plus pertuzumab (TP) and a taxane in HER2-positive mBC with BMs. The Reper study (n=21) reported an ORR of 52.4% and a median PFS of 20 months, while the Bergen et al. study (n=26) showed a higher ORR of 92.9%, but with a shorter PFS of 8 months and a median OS of 44 months [51,52]. However, both studies had a high risk of bias due to their retrospective design and the use of local therapies. The phase II PATRICIA study assessed high-dose trastuzumab (HDT) plus pertuzumab after progression on standard trastuzumab in pretreated patients (n=39), showing a low CNS-ORR of 11% but confirming the safety of HDT [53]. The EMILIA trial T-DM1 demonstrated a significant overall survival advantage (26.8 vs. 12.9 months; HR = 0.38; P = 0.008) over capecitabine–lapatinib (XL), despite similar progression-free survival between the groups. The incidence of CNS progression was higher among those with baseline brain metastases but remained comparable between treatments [54]. The objective-response rate was higher in the T-DM1 group (43.6%; 95% CI, 38.6 to 48.6) than in the lapatinib–capecitabine group (30.8%; 95% CI, 26.3 to 35.7; P<0.001), and the median duration of response was longer (12.6 months vs. 6.5 months). The KAMILLA phase IIIb study confirmed T-DM1’s activity in HER2-positive MBC with BMs, supporting further research. Notably, in patients with previously untreated, asymptomatic BMs, T-DM1 achieved an intracranial objective response rate (ORR-IC) of 49.3%, highlighting its potential efficacy in this subgroup [55]. A pooled analysis of the DEBBRAH, TUXEDO-1, and DFCI/Duke/MDACC studies confirmed the significant intracranial efficacy of T-DXd in HER2-positive breast cancer with active brain metastases, achieving an ORR-IC of 64.9% and a clinical benefit rate of 81.1%. T-DXd maintained a stable quality of life and presented no new safety concerns, supporting its use regardless of brain metastasis status [56]. The DESTINY-Breast12 study confirmed T-DXd as a highly effective treatment for HER2-positive breast cancer, with BMs overcoming the blood-brain barrier, achieving a CNS-specific PFS of 58.9% and an ORR of 71.7%, which significantly improved patient outcomes [57]. The HER2CLIMB study showed that adding tucatinib to trastuzumab and capecitabine significantly improved outcomes in HER2-positive breast cancer with BMs, reducing intracranial progression or death by 68% and doubling the intracranial objective response rate (47.3% vs. 20.0%), establishing its role as an effective treatment option [58].
The intracranial efficacy of anti-HER2 therapies has improved substantially over time, as demonstrated by increasing objective response rates (ORR-IC) in recent studies such as HER2CLIMB and DESTINY-Breast12 (see Figure 1). These findings highlight significant advancements in systemic therapies for HER2-positive breast cancer with brain metastases. The expanding role of targeted treatments has improved survival and quality of life, yet further research is needed to refine therapeutic strategies for this high-risk population.
Discussion
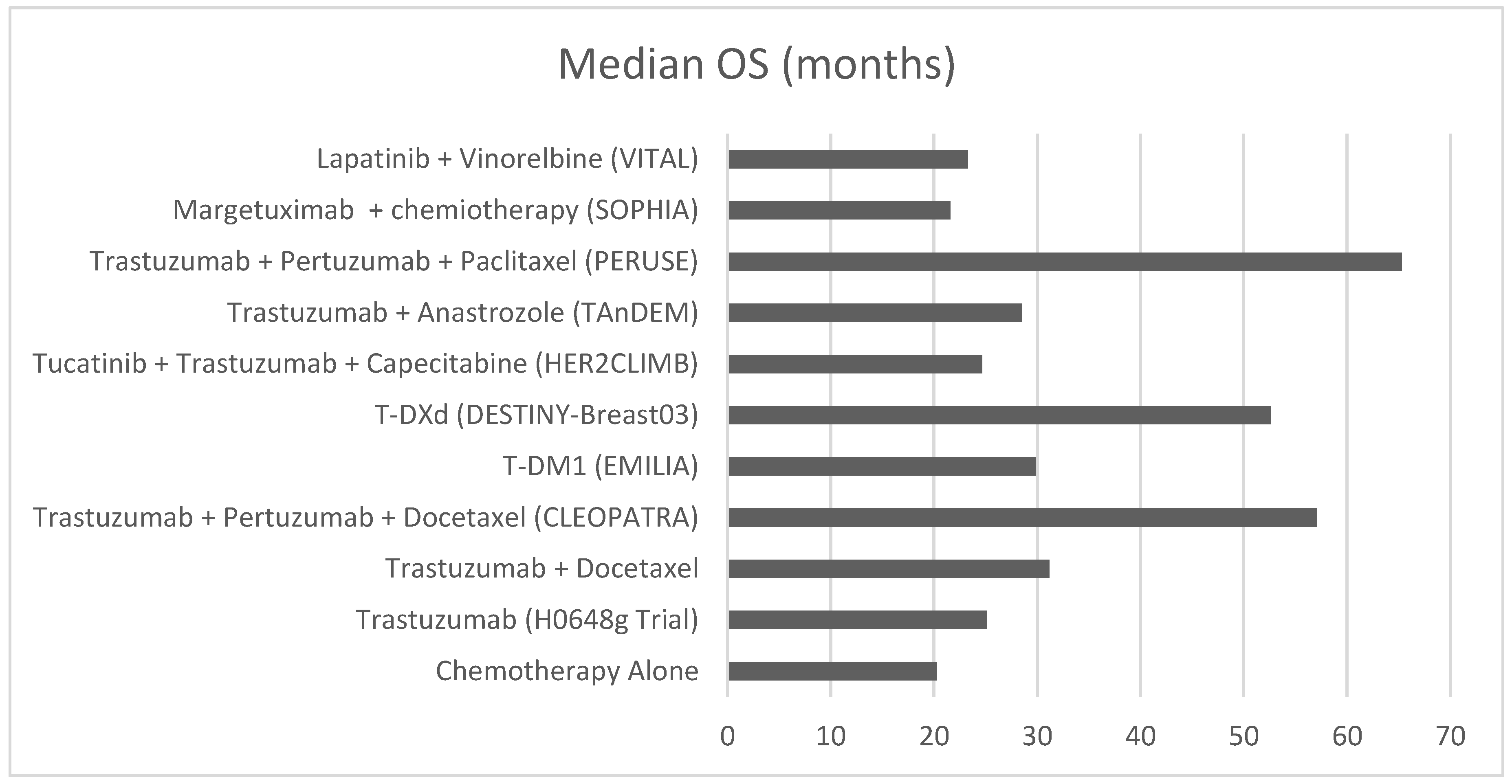
The evolution of anti-HER2 therapies has dramatically transformed the treatment landscape for HER2-positive breast cancer, with successive generations of treatments demonstrating increasingly impressive survival benefits. This progression highlights both the remarkable advances in targeted therapy and areas requiring further investigation. The introduction of trastuzumab marked the first significant improvement in overall survival (OS), extending median OS from 20.3 to 25.1 months compared to chemotherapy alone. The addition of pertuzumab to trastuzumab and docetaxel (CLEOPATRA trial) further elevated the survival benchmark, achieving a median OS of 57.1 months compared to 40.8 months with trastuzumab and docetaxel. This 16.3-month improvement represented a paradigm shift in HER2-positive metastatic breast cancer treatment, with 37% of patients surviving at 8 years versus 23% in the control arm. The development of antibody-drug conjugates (ADCs) has further extended survival benefits. T-DM1 demonstrated superior efficacy compared to lapatinib plus capecitabine, with a median OS of 29.9 months versus 25.9 months in the EMILIA trial. More recently, trastuzumab deruxtecan (T-DXd) has shown remarkable results in the DESTINY-Breast03 trial, achieving a median OS of 52.6 months compared to 42.7 months with T-DM1. This evolution from trastuzumab to T-DXd reflects a steady and meaningful improvement in OS, now exceeding 50 months with optimal sequencing. While survival has improved significantly, challenges remain—particularly in patients with brain metastases. From 1998 to 2024, each new therapeutic approach has contributed to extending patient survival, with the most recent data showing an unprecedented duration of survival for metastatic disease. This advancement demonstrates not only the success of targeted therapy development but also the importance of continued innovation in the field. A critical advancement in anti-HER2 therapy has been the increasing focus on intracranial efficacy. Brain metastases, affecting approximately 31% of HER2-positive breast cancer patients, have historically represented a significant therapeutic challenge. Recent developments, particularly with newer agents, have shown promising intracranial activity. T-DXd has demonstrated remarkable efficacy in patients with brain metastases, achieving an intracranial objective response rate of 64.9% and maintaining quality of life. Similarly, the addition of tucatinib to trastuzumab and capecitabine reduced intracranial progression or death by 68%, representing a significant advance in managing this challenging patient population. These findings underscore the critical importance of including patients with brain metastases in clinical trials. Historically, these patients have often been excluded from pivotal studies, which has limited our understanding of treatment efficacy in this high-risk population. The success of newer agents in treating brain metastases underscores the importance of systematically including these patients in future clinical trials to enhance understanding of therapeutic options and optimize treatment strategies. Beyond intracranial control, a deeper understanding of tumor biology may unlock personalized strategies. Despite these advances, predictive biomarkers remain crucial to optimizing treatment selection and outcomes. The recognition of CD16A polymorphisms has emerged as a potential predictor of response to trastuzumab-based therapies, as seen in the SOPHIA trial with margetuximab. Refining patient selection through biomarker integration is the next frontier in personalizing HER2-positive mBC therapy. Expanding on this, the optimization of treatment selection based on tumor biology is essential for achieving durable responses in HER2-positive metastatic breast cancer. Individualized management strategies should incorporate HER2 heterogeneity, hormone receptor co-expression, ERBB2 mutations, and features of the tumor microenvironment. These factors influence treatment sensitivity and resistance and can guide the sequencing of anti-HER2 agents. Integrating molecular profiling and multidisciplinary decision-making will be key to personalizing care and improving long-term outcomes. The GIM14 BIO-META study highlighted that HER2 IHC score 3+, non-visceral metastases, and a single metastatic site are associated with radiologic complete response (rCR) to first-line anti-HER2 therapy. Among long responders (TTD > 18 months), median OS reached 12.7 years, with a 5-year survival rate of 92%, supporting the potential for treatment de-escalation in selected patients. Liquid biopsy and MRD assessment may further refine this approach, as explored in the STOP-HER2 trial [59]. Future research should focus on validating these biomarkers to enable more personalized treatment strategies. Additionally, real-world evidence (RWE) is crucial for understanding how clinical trial results are applied in routine clinical practice. Retrospective analyses and large observational studies can provide insights into treatment effectiveness across diverse patient populations, including those typically underrepresented in trials, such as elderly patients and those with brain metastases. Integration of RWE into treatment guidelines could further refine therapeutic decision-making. The availability of multiple effective anti-HER2 therapies underscores the critical importance of developing optimal treatment sequencing strategies, as the choice and order of therapies can significantly impact patient outcomes. A well-planned sequential approach, considering factors such as prior treatments, resistance patterns, and the presence of brain metastases, is fundamental for maximizing survival benefits and maintaining quality of life. Looking forward, several key areas require attention. First, while survival improvements have been substantial, there remains a need for biomarker-driven approaches to better predict treatment response and resistance. Second, the optimal sequencing of available therapies needs further investigation, particularly given the expanding therapeutic arsenal. Finally, the development of strategies to prevent or delay the onset of brain metastases represents an important area for future research. The remarkable progress in anti-HER2 therapy exemplifies the success of targeted approaches in oncology. A longitudinal comparison of median overall survival (OS) across pivotal clinical trials demonstrates the steady improvement in outcomes with successive generations of anti-HER2 therapies (Figure 2). These findings highlight the importance of translating clinical trial results into routine clinical practice. Observational data from the GIM14/BIOMETA study support this need by documenting a progressive improvement in overall survival for patients with HER2-positive metastatic breast cancer over time, in parallel with the introduction of novel anti-HER2 therapies and evolving treatment strategies in real-world settings. Bridging the gap between clinical trials and real-world implementation remains crucial to translate the benefits of anti-HER2 therapies into tangible outcomes for diverse patient populations. However, continued research efforts are essential to further improve outcomes, particularly for patients with brain metastases. Future clinical trials should prioritize the inclusion of these high-risk patients to ensure that emerging therapies are effective across the full spectrum of disease presentations.
Conclusions
The development of anti-HER2 therapies has markedly improved overall survival in HER2-positive metastatic breast cancer, increasing median survival from 20 months to over 50 months with current treatments. Recent innovations, such as T-DXd (DESTINY-Breast03) and tucatinib-based regimens (HER2CLIMB), have further enhanced survival, particularly for patients with brain metastases. However, challenges persist regarding optimal therapy sequencing, resistance mechanisms, and early intervention strategies. As the therapeutic landscape evolves, the effective translation of clinical trial findings into routine practice and the addressing of resistance will be critical for further improving patient outcomes and advancing personalized treatment approaches. Ongoing integration of molecular diagnostics, real-world evidence, and patient-focused trial design will be essential to fully realize the potential of anti-HER2 therapy in metastatic breast cancer.
References
- Lei S, Zheng R, Zhang S, Wang S, Chen R, Sun K, Zeng H, Zhou J, Wei W. Global patterns of breast cancer incidence and mortality: A population-based cancer registry data analysis from 2000 to 2020. Cancer Commun (Lond). 2021 Nov;41(11):1183-1194. Epub 2021 Aug 16. [CrossRef] [PubMed] [PubMed Central]
- Mercogliano MF, Bruni S, Mauro FL, Schillaci R. Emerging Targeted Therapies for HER2-Positive Breast Cancer. Cancers (Basel). 2023 Mar 26;15(7):1987. [CrossRef] [PubMed] [PubMed Central]
- Li J, Chen Z, Su K, Zeng J. Clinicopathological classification and traditional prognostic indicators of breast cancer. Int J Clin Exp Pathol. 2015 Jul 1;8(7):8500-5. [PubMed] [PubMed Central]
- Swain SM, Shastry M, Hamilton E. Targeting HER2-positive breast cancer: advances and future directions. Nat Rev Drug Discov. 2023 Feb;22(2):101-126. Epub 2022 Nov 7. [CrossRef] [PubMed] [PubMed Central]
- Jørgensen JT. Twenty-five years with HER2 targeted therapy. Ann Transl Med. 2024 Jun 10;12(3):53. Epub 2023 Jun 25. [CrossRef] [PubMed] [PubMed Central]
- Malenfant SJ, Eckmann KR, Barnett CM. Pertuzumab: a new targeted therapy for HER2-positive metastatic breast cancer. Pharmacotherapy. 2014 Jan;34(1):60-71. Epub 2013 Aug 5. [CrossRef] [PubMed]
- Bansal I, Pandey AK, Ruwali M. Small-molecule inhibitors of kinases in breast cancer therapy: recent advances, opportunities, and challenges. Front Pharmacol. 2023 Aug 30;14:1244597. [CrossRef] [PubMed] [PubMed Central]
- Mark C, Lee JS, Cui X, Yuan Y. Antibody-Drug Conjugates in Breast Cancer: Current Status and Future Directions. Int J Mol Sci. 2023 Sep 6;24(18):13726. [CrossRef] [PubMed] [PubMed Central]
- De P, Hasmann M, Leyland-Jones B. Molecular determinants of trastuzumab efficacy: what is their clinical relevance? Cancer Treat Rev. 2013;39:925–34.
- Stanowicka-Grada M, Senkus E. Anti-HER2 Drugs for the Treatment of Advanced HER2 Positive Breast Cancer. Curr Treat Options Oncol. 2023 Nov;24(11):1633-1650. Epub 2023 Oct 25. [CrossRef] [PubMed] [PubMed Central]
- Marty M, Cognetti F, Maraninchi D, Snyder R, Mauriac L, Tubiana-Hulin M, Chan S, Grimes D, Antón A, Lluch A, Kennedy J, O’Byrne K, Conte P, Green M, Ward C, Mayne K, Extra JM. Randomized phase II trial of the efficacy and safety of trastuzumab combined with docetaxel in patients with human epidermal growth factor receptor 2-positive metastatic breast cancer administered as first-line treatment: the M77001 study group. J Clin Oncol. 2005 Jul 1;23(19):4265-74. Epub 2005 May 23. [CrossRef] [PubMed]
- Jackisch C, Welslau M, Schoenegg W, et al. Impact of trastuzumab treatment beyond disease progression for advanced/metastatic breast cancer on survival - results from a prospective, observational study in Germany. Breast. 2014;23:603–8. [CrossRef]
- Rocca A, Andreis D, Fedeli A, Maltoni R, Sarti S, Cecconetto L, Pietri E, Schirone A, Bravaccini S, Serra P, Farolfi A, Amadori D. Pharmacokinetics, pharmacodynamics and clinical efficacy of pertuzumab in breast cancer therapy. Expert Opin Drug Metab Toxicol. 2015;11(10):1647-63. Epub 2015 Aug 26. [CrossRef] [PubMed]
- Jagosky M, Tan AR. Combination of Pertuzumab and Trastuzumab in the Treatment of HER2-Positive Early Breast Cancer: A Review of the Emerging Clinical Data. Breast Cancer (Dove Med Press). 2021 Jun 14;13:393-407. [CrossRef] [PubMed] [PubMed Central]
- Swain SM, Miles D, Kim SB, Im YH, Im SA, Semiglazov V, Ciruelos E, Schneeweiss A, Loi S, Monturus E, Clark E, Knott A, Restuccia E, Benyunes MC, Cortés J; CLEOPATRA study group. Pertuzumab, trastuzumab, and docetaxel for HER2-positive metastatic breast cancer (CLEOPATRA): end-of-study results from a double-blind, randomised, placebo-controlled, phase 3 study. Lancet Oncol. 2020 Apr;21(4):519-530. Epub 2020 Mar 12. [CrossRef] [PubMed]
- Bachelot T, Ciruelos E, Schneeweiss A, et al. on behalf of the PERUSE investigators. Preliminary safety and efficacy of first-line pertuzumab combined with trastuzumab and taxane therapy for HER2-positive locally recurrent or metastatic breast cancer (PERUSE). Ann Oncol 2019; 30: 766-73. [CrossRef]
- Miles D, Ciruelos E, Schneeweiss A, Puglisi F, Peretz-Yablonski T, Campone M, Bondarenko I, Nowecki Z, Errihani H, Paluch-Shimon S, Wardley A, Merot JL, Trask P, du Toit Y, Pena-Murillo C, Revelant V, Klingbiel D, Bachelot T; PERUSE investigators. Final results from the PERUSE study of first-line pertuzumab plus trastuzumab plus a taxane for HER2-positive locally recurrent or metastatic breast cancer, with a multivariable approach to guide prognostication. Ann Oncol. 2021 Oct;32(10):1245-1255. Epub 2021 Jul 2. [CrossRef] [PubMed]
- del Mastro L, De Laurentiis M. Applicazioni cliniche del trastuzumab nel trattamento del carcinoma mammario HER2+ Recenti Prog Med 2019;110(12):594-603. [CrossRef]
- Urruticoechea A, Rizwanullah M, Im SA et al. Final overall survival (OS) analysis of PHEREXA: A randomized phase III trial of trastuzumab (H) + capecitabine (X) ± pertuzumab (P)in patients with HER2-positive metastatic breast cancer (MBC)who experienced disease progression during or after H-based therapy. J Clin Oncol. 2018;36(Suppl.15):Abst. 1013.
- Bartsch R, Bergen E. ASCO 2018: highlights in HER2-positive metastatic breast cancer. Memo. 2018;11(4):280-283. Epub 2018 Oct 11. [CrossRef] [PubMed] [PubMed Central]
- Arpino G, de la Haba Rodríguez J, Ferrero JM, De Placido S, Osborne CK, Klingbiel D, Revelant V, Wohlfarth C, Poppe R, Rimawi MF; PERTAIN Study Group. Pertuzumab, Trastuzumab, and an Aromatase Inhibitor for HER2-Positive and Hormone Receptor-Positive Metastatic or Locally Advanced Breast Cancer: PERTAIN Final Analysis. Clin Cancer Res. 2023 Apr 14;29(8):1468-1476. [CrossRef] [PubMed] [PubMed Central]
- Nordstrom JL, Gorlatov S, Zhang W, et al.: Anti-tumor activity and toxicokinetics analysis of MGAH22, an anti-HER2 monoclonal antibody with enhanced Fcgamma receptor binding properties. Breast Cancer Res 13:R123, 2011. [CrossRef]
- Liu L, Yang Y, Burns R, et al.: Margetuximab mediates greater Fc-dependent anti-tumor activities than trastuzumab or pertuzumab in vitro. Cancer Res 79:1538, 2019 (abstr 1538). [CrossRef]
- Rugo HS, Im SA, Cardoso F, Cortes J, Curigliano G, Musolino A, Pegram MD, Bachelot T, Wright GS, Saura C, Escrivá-de-Romaní S, De Laurentiis M, Schwartz GN, Pluard TJ, Ricci F, Gwin WR 3rd, Levy C, Brown-Glaberman U, Ferrero JM, de Boer M, Kim SB, Petráková K, Yardley DA, Freedman O, Jakobsen EH, Gal-Yam EN, Yerushalmi R, Fasching PA, Kaufman PA, Ashley EJ, Perez-Olle R, Hong S, Rosales MK, Gradishar WJ; SOPHIA Study Group. Margetuximab Versus Trastuzumab in Patients With Previously Treated HER2-Positive Advanced Breast Cancer (SOPHIA): Final Overall Survival Results From a Randomized Phase 3 Trial. J Clin Oncol. 2023 Jan 10;41(2):198-205. Epub 2022 Nov 4. [CrossRef] [PubMed] [PubMed Central]
- Gradishar WJ, O’Regan R, Rimawi MF, Nordstrom JL, Rosales MK, Rugo HS. Margetuximab in HER2-positive metastatic breast cancer. Future Oncol. 2023 May;19(16):1099-1112. Epub 2023 May 12. [CrossRef] [PubMed]
- Barok M, Joensuu H, Isola J. Trastuzumab emtansine: mechanisms of action and drug resistance. Breast Cancer Res. 2014 Mar 5;16(2):209. [CrossRef] [PubMed] [PubMed Central]
- Diéras V, Miles D, Verma S, Pegram M, Welslau M, Baselga J, Krop IE, Blackwell K, Hoersch S, Xu J, Green M, Gianni L. Trastuzumab emtansine versus capecitabine plus lapatinib in patients with previously treated HER2-positive advanced breast cancer (EMILIA): a descriptive analysis of final overall survival results from a randomised, open-label, phase 3 trial. Lancet Oncol. 2017 Jun;18(6):732-742. Epub 2017 May 16. Erratum in: Lancet Oncol. 2017 Aug;18(8):e433. doi: 10.1016/S1470-2045(17)30527-2. Erratum in: Lancet Oncol. 2018 Dec;19(12):e667. doi: 10.1016/S1470-2045(18)30848-9. PMID: 28526536; PMCID: PMC5531181. [CrossRef]
- Krop IE, Kim SB, Martin AG, LoRusso PM, Ferrero JM, Badovinac-Crnjevic T, Hoersch S, Smitt M, Wildiers H. Trastuzumab emtansine versus treatment of physician’s choice in patients with previously treated HER2-positive metastatic breast cancer (TH3RESA): final overall survival results from a randomised open-label phase 3 trial. Lancet Oncol. 2017 Jun;18(6):743-754. Epub 2017 May 16. [CrossRef] [PubMed]
- Meric-Bernstam F, Makker V, Oaknin A, Oh DY, Banerjee S, González-Martín A, Jung KH, Ługowska I, Manso L, Manzano A, Melichar B, Siena S, Stroyakovskiy D, Fielding A, Ma Y, Puvvada S, Shire N, Lee JY. Efficacy and Safety of Trastuzumab Deruxtecan in Patients With HER2-Expressing Solid Tumors: Primary Results From the DESTINY-PanTumor02 Phase II Trial. J Clin Oncol. 2024 Jan 1;42(1):47-58. Epub 2023 Oct 23. [CrossRef] [PubMed] [PubMed Central]
- Daiichi Sankyo Co. Ltd. ENHERTU® Approved in the U.S. for Patients with HER2 Positive Metastatic Breast Cancer Treated with a Prior Anti-HER2-Based Regimen daiichisankyo.us/press-releases/-/article/enhertu-approved-in-the-u-s-for-patients-with-her2-positive-metastatic-breast-cancer-treated-with-a-prior-anti-he r2-based-regimen (2022).
- Modi S, Saura C, Yamashita T, Park YH, Kim SB, Tamura K, Andre F, Iwata H, Ito Y, Tsurutani J, Sohn J, Denduluri N, Perrin C, Aogi K, Tokunaga E, Im SA, Lee KS, Hurvitz SA, Cortes J, Lee C, Chen S, Zhang L, Shahidi J, Yver A, Krop I; DESTINY-Breast01 Investigators. Trastuzumab Deruxtecan in Previously Treated HER2-Positive Breast Cancer. N Engl J Med. 2020 Feb 13;382(7):610-621. Epub 2019 Dec 11. [CrossRef] [PubMed] [PubMed Central]
- André F, Hee Park Y, Kim SB, Takano T, Im SA, Borges G, Lima JP, Aksoy S, Gavila Gregori J, De Laurentiis M, Bianchini G, Roylance R, Miyoshi Y, Armstrong A, Sinha R, Ruiz Borrego M, Lim E, Ettl J, Yerushalmi R, Zagouri F, Duhoux FP, Fehm T, Gambhire D, Cathcart J, Wu C, Chu C, Egorov A, Krop I. Trastuzumab deruxtecan versus treatment of physician’s choice in patients with HER2-positive metastatic breast cancer (DESTINY-Breast02): a randomised, open-label, multicentre, phase 3 trial. Lancet. 2023 May 27;401(10390):1773-1785. Epub 2023 Apr 20. Erratum in: Lancet. 2023 Dec 9;402(10418):2196. doi: 10.1016/S0140-6736(23)02709-5. Erratum in: Lancet. 2024 Mar 9;403(10430):912. doi: 10.1016/S0140-6736(24)00420-3. PMID: 37086745. [CrossRef]
- Hurvitz SA, Hegg R, Chung WP, Im SA, Jacot W, Ganju V, Chiu JWY, Xu B, Hamilton E, Madhusudan S, Iwata H, Altintas S, Henning JW, Curigliano G, Perez-Garcia JM, Kim SB, Petry V, Huang CS, Li W, Frenel JS, Antolin S, Yeo W, Bianchini G, Loi S, Tsurutani J, Egorov A, Liu Y, Cathcart J, Ashfaque S, Cortés J. Trastuzumab deruxtecan versus trastuzumab emtansine in patients with HER2-positive metastatic breast cancer: updated results from DESTINY-Breast03, a randomised, open-label, phase 3 trial. Lancet. 2023 Jan 14;401(10371):105-117. Epub 2022 Dec 7. Erratum in: Lancet. 2023 Feb 18;401(10376):556. doi: 10.1016/S0140-6736(22)00045-9. PMID: 36495879. [CrossRef]
- Cortés J, Hurvitz SA, Im SA, Iwata H, Curigliano G, Kim SB, Chiu JWY, Pedrini JL, Li W, Yonemori K, Bianchini G, Loi S, Borges GS, Wang X, Bachelot T, Nakatani S, Ashfaque S, Liang Z, Egorov A, Hamilton E. Trastuzumab deruxtecan versus trastuzumab emtansine in HER2-positive metastatic breast cancer: long-term survival analysis of the DESTINY-Breast03 trial. Nat Med. 2024 Aug;30(8):2208-2215. Epub 2024 Jun 2. [CrossRef] [PubMed] [PubMed Central]
- Guan M, Tong Y, Guan M, Liu X, Wang M, Niu R, Zhang F, Dong D, Shao J, Zhou Y. Lapatinib Inhibits Breast Cancer Cell Proliferation by Influencing PKM2 Expression. Technol Cancer Res Treat. 2018 Jan 1;17:1533034617749418. [CrossRef] [PubMed] [PubMed Central]
- Chintalaramulu N, Vadivelu R, Nguyen NT, Cock IE. Lapatinib inhibits doxorubicin induced migration of HER2-positive breast cancer cells. Inflammopharmacology. 2020 Oct;28(5):1375-1386. Epub 2020 May 6. [CrossRef] [PubMed]
- Petrelli F, Ghidini M, Lonati V, Tomasello G, Borgonovo K, Ghilardi M, Cabiddu M, Barni S. The efficacy of lapatinib and capecitabine in HER-2 positive breast cancer with brain metastases: A systematic review and pooled analysis. Eur J Cancer. 2017 Oct;84:141-148. Epub 2017 Aug 12. [CrossRef] [PubMed]
- Janni W, Sarosiek T, Karaszewska B, Pikiel J, Staroslawska E, Potemski P, Salat C, Brain E, Caglevic C, Briggs K, Mahood K, DeSilvio M, Marini L, Papadimitriou C. Final overall survival analysis of a phase II trial evaluating vinorelbine and lapatinib in women with ErbB2 overexpressing metastatic breast cancer. Breast. 2015 Dec;24(6):769-73. Epub 2015 Sep 16. [CrossRef] [PubMed]
- Xuhong JC, Qi XW, Zhang Y, Jiang J. Mechanism, safety and efficacy of three tyrosine kinase inhibitors lapatinib, neratinib and pyrotinib in HER2-positive breast cancer. Am J Cancer Res. 2019 Oct 1;9(10):2103-2119. [PubMed] [PubMed Central]
- Saura C, Oliveira M, Feng YH, Dai MS, Chen SW, Hurvitz SA, Kim SB, Moy B, Delaloge S, Gradishar W, Masuda N, Palacova M, Trudeau ME, Mattson J, Yap YS, Hou MF, De Laurentiis M, Yeh YM, Chang HT, Yau T, Wildiers H, Haley B, Fagnani D, 101 Lu YS, Crown J, Lin J, Takahashi M, Takano T, Yamaguchi M, Fujii T, Yao B, Bebchuk J, Keyvanjah K, Bryce R, Brufsky A; NALA Investigators. Neratinib Plus Capecitabine Versus Lapatinib Plus Capecitabine in HER2-Positive Metastatic Breast Cancer Previously Treated With ≥ 2 HER2-Directed Regimens: Phase III NALA Trial. J Clin Oncol. 2020 Sep 20;38(27):3138-3149. Epub 2020 Jul 17. [CrossRef] [PubMed] [PubMed Central]
- Sirhan Z, Thyagarajan A, Sahu RP. The efficacy of tucatinib-based therapeutic approaches for HER2-positive breast cancer. Mil Med Res. 2022 Jul 13;9(1):39. [CrossRef] [PubMed] [PubMed Central]
- Curigliano G, Mueller V, Borges V, Hamilton E, Hurvitz S, Loi S, Murthy R, Okines A, Paplomata E, Cameron D, Carey LA, Gelmon K, Hortobagyi GN, Krop I, Loibl S, Pegram M, Slamon D, Ramos J, Feng W, Winer E. Tucatinib versus placebo added to trastuzumab and capecitabine for patients with pretreated HER2+ metastatic breast cancer with and without brain metastases (HER2CLIMB): final overall survival analysis. Ann Oncol. 2022 Mar;33(3):321-329. Epub 2021 Dec 23. Erratum in: Ann Oncol. 2023 Jul;34(7):630. doi: 10.1016/j.annonc.2022.12.005. PMID: 34954044. [CrossRef]
- Murthy RK, Loi S, Okines A, Paplomata E, Hamilton E, Hurvitz SA, Lin NU, Borges V, Abramson V, Anders C, Bedard PL, Oliveira M, Jakobsen E, Bachelot T, Shachar SS, Müller V, Braga S, Duhoux FP, Greil R, Cameron D, Carey LA, Curigliano G, Gelmon K, Hortobagyi G, Krop I, Loibl S, Pegram M, Slamon D, Palanca-Wessels MC, Walker L, Feng W, Winer EP. Tucatinib, Trastuzumab, and Capecitabine for HER2-Positive Metastatic Breast Cancer. N Engl J Med. 2020 Feb 13;382(7):597-609. Epub 2019 Dec 11. Erratum in: N Engl J Med. 2020 Feb 6;382(6):586. doi: 10.1056/NEJMx190039. PMID: 31825569.]. [CrossRef]
- Criscitiello C, Corti C, De Laurentiis M, Bianchini G, Pistilli B, Cinieri S, Castellan L, Arpino G, Conte P, Di Meco F, Gennari A, Guarneri V, Visani L, Livi L, Marchetti P, Puglisi F, Viale G, Del Mastro L, De Placido S, Curigliano G. Tucatinib’s journey from clinical development to clinical practice: New horizons for HER2-positive metastatic disease and promising prospects for brain metastatic spread. Cancer Treat Rev. 2023 Nov;120:102618. Epub 2023 Aug 22. [CrossRef] [PubMed]
- Wang R, Zhu Y, Liu X, Liao X, He J, Niu L. The Clinicopathological features and survival outcomes of patients with different metastatic sites in stage IV breast cancer. BMC Cancer. 2019 Nov 12;19(1):1091. [CrossRef] [PubMed] [PubMed Central]
- Kuksis M, Gao Y, Tran W, Hoey C, Kiss A, Komorowski AS, Dhaliwal AJ, Sahgal A, Das S, Chan KK, Jerzak KJ. The incidence of brain metastases among patients with metastatic breast cancer: a systematic review and meta-analysis. Neuro Oncol. 2021 Jun 1;23(6):894-904. [CrossRef] [PubMed] [PubMed Central]
- Lopes S, Vieira I, Abreu M, Pousa I, Ferreira A, Sousa S, Pereira D. Prognostic Factors and Survival According to Tumor Subtype in Women With Breast Cancer Brain Metastases. Curr Probl Cancer. 2022 Dec;46(6):100866. Epub 2022 Jun 11. [CrossRef] [PubMed]
- Raghavendra AS, Ibrahim NK. Breast Cancer Brain Metastasis: A Comprehensive Review. JCO Oncol Pract. 2024 Oct;20(10):1348-1359. Epub 2024 May 15. [CrossRef] [PubMed] [PubMed Central]
- E. Le Rhun, M. Guckenberger, M. Smits et al., on behalf of the EANO Guidelines Committee and the ESMO Guidelines Committee.
- Fontanella C, De Carlo E, Cinausero M, Pelizzari G, Venuti I, Puglisi F. Central nervous system involvement in breast cancer patients: Is the therapeutic landscape changing too slowly? Cancer Treat Rev. 2016 May;46:80-8. Epub 2016 Apr 1. [CrossRef] [PubMed]
- Gamucci, T.; Pizzuti, L.; Natoli, C.; Mentuccia, L.; Sperduti, I.; Barba, M.; Sergi, D.; Iezzi, L.; Maugeri-Saccà, M.; Vaccaro, A.; et al. A multicenter REtrospective observational study of first-line treatment with PERtuzumab, trastuzumab and taxanes for advanced HER2 positive breast cancer patients. RePer Study. Cancer Biol. Ther. 2019, 20, 192–200. [CrossRef]
- Bergen ES, Binter A, Starzer AM, Heller G, Kiesel B, Tendl-Schulz K, Bago-Horvath Z, Furtner J, Leitner J, Exner R, Fitzal F, Dieckmann K, Widhalm G, Preusser M, Berghoff AS, Bartsch R. Favourable outcome of patients with breast cancer brain metastases treated with dual HER2 blockade of trastuzumab and pertuzumab. Ther Adv Med Oncol. 2021 Apr 22;13:17588359211009002. [CrossRef] [PubMed] [PubMed Central]
- Lin NU, Pegram M, Sahebjam S, Ibrahim N, Fung A, Cheng A, Nicholas A, Kirschbrown W, Kumthekar P. Pertuzumab Plus High-Dose Trastuzumab in Patients With Progressive Brain Metastases and HER2-Positive Metastatic Breast Cancer: Primary Analysis of a Phase II Study. J Clin Oncol. 2021 Aug 20;39(24):2667-2675. Epub 2021 May 4. [CrossRef] [PubMed] [PubMed Central]
- Krop IE, Lin NU, Blackwell K, Guardino E, Huober J, Lu M, Miles D, Samant M, Welslau M, Diéras V. Trastuzumab emtansine (T-DM1) versus lapatinib plus capecitabine in patients with HER2-positive metastatic breast cancer and central nervous system metastases: a retrospective, exploratory analysis in EMILIA. Ann Oncol. 2015 Jan;26(1):113-119. Epub 2014 Oct 29. [CrossRef] [PubMed] [PubMed Central]
- Montemurro F, Delaloge S, Barrios CH, Wuerstlein R, Anton A, Brain E, Hatschek T, Kelly CM, Peña-Murillo C, Yilmaz M, Donica M, Ellis P. Trastuzumab emtansine (T-DM1) in patients with HER2-positive metastatic breast cancer and brain metastases: exploratory final analysis of cohort 1 from KAMILLA, a single-arm phase IIIb clinical trial☆. Ann Oncol. 2020 Oct;31(10):1350-1358. Epub 2020 Jul 5. [CrossRef] [PubMed]
- Bartsch R, Pérez-García JM, Furtner J, Berghoff AS, Marhold M, Starzer AM, Hughes M, Kabraji S, Sammons S, Anders C, Murthy RK, Van Swearingen AED, Pereslete A, Gion M, Vaz Batista M, Braga S, Pinto PBC, Sampayo-Cordero M, Llombart-Cussac A, Preusser M, Cortés J, Lin NU. Results of a patient-level pooled analysis of three studies of trastuzumab deruxtecan in HER2-positive breast cancer with active brain metastasis. ESMO Open. 2025 Jan;10(1):104092. Epub 2025 Jan 3. [CrossRef] [PubMed] [PubMed Central]
- Das G, Wong STC, Zhao H. Beyond Primary HER2 Expression: Trastuzumab Deruxtecan’s Efficacy in Brain Metastasis. Cancers (Basel). 2024 Oct 18;16(20):3525. [CrossRef] [PubMed] [PubMed Central]
- Lin NU, Borges V, Anders C, Murthy RK, Paplomata E, Hamilton E, Hurvitz S, Loi S, Okines A, Abramson V, Bedard PL, Oliveira M, Mueller V, Zelnak A, DiGiovanna MP, Bachelot T, Chien AJ, O’Regan R, Wardley A, Conlin A, Cameron D, Carey L, Curigliano G, Gelmon K, Loibl S, Mayor J, McGoldrick S, An X, Winer EP. Intracranial Efficacy and Survival With Tucatinib Plus Trastuzumab and Capecitabine for Previously Treated HER2-Positive Breast Cancer With Brain Metastases in the HER2CLIMB Trial. J Clin Oncol. 2020 Aug 10;38(23):2610-2619. Epub 2020 May 29. [CrossRef] [PubMed] [PubMed Central]
- Cucciniello L, Blondeaux E, Bighin C, Gasparro S, Russo S, Dri A, Pugliese P, Fontana A, Cortesi E, Ferzi A, Riccardi F, Sini V, Boni L, Fabi A, Montemurro F, De Laurentiis M, Arpino G, Del Mastro L, Gerratana L, Puglisi F. Clinico-pathological predictors of radiologic complete response to first-line anti-HER2 therapy in metastatic breast cancer. NPJ Breast Cancer. 2024 Dec 18;10(1):105. [CrossRef] [PubMed] [PubMed Central]
Figure 1.
Median Overall Survival with Anti-HER2 Therapies.
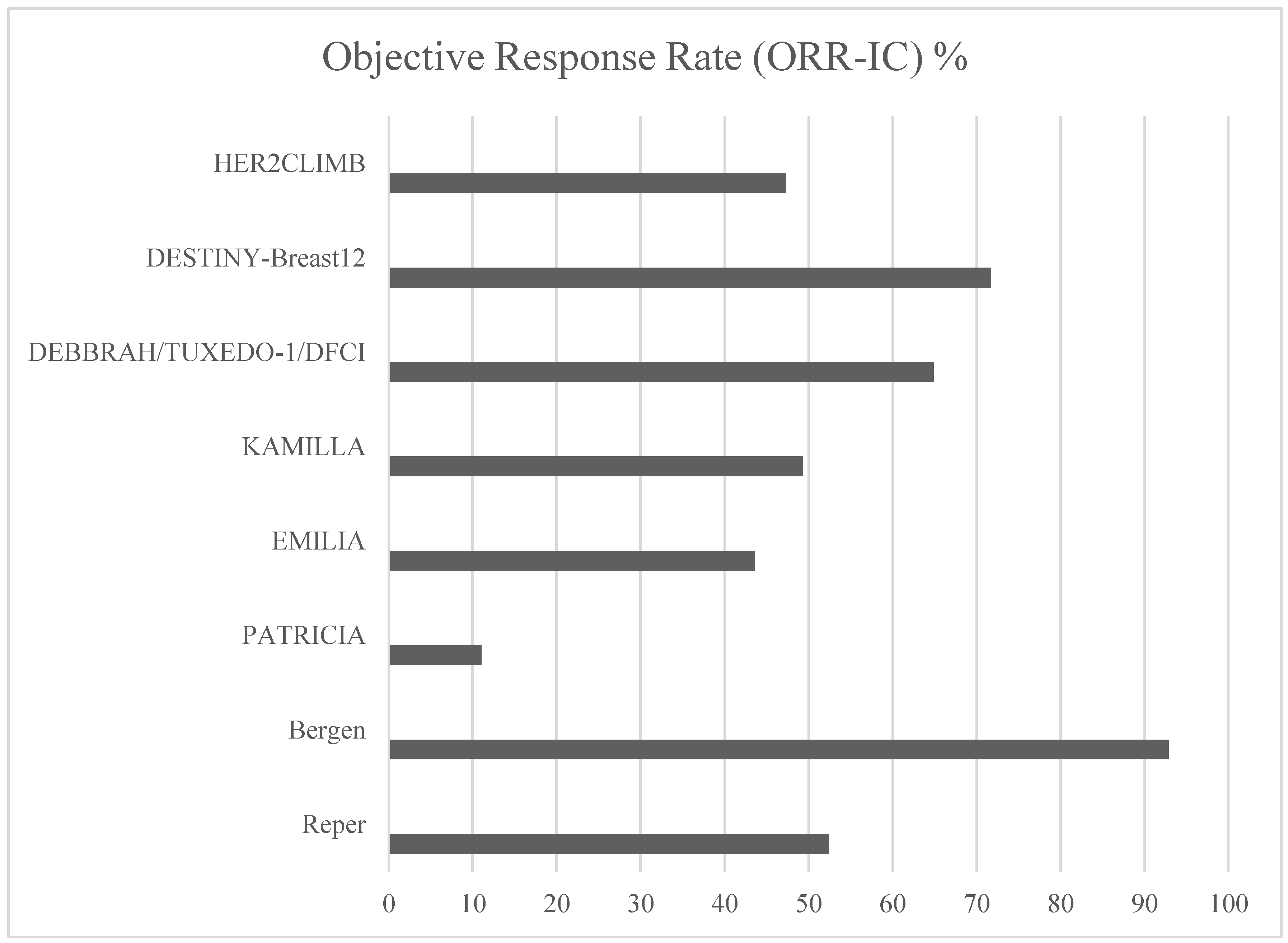
Figure 2.
Intracranial Objective Response Rates (ORR-IC) in HER2-Positive Breast Cancer.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



