
Submitted:
22 September 2025
Posted:
23 September 2025
You are already at the latest version
Abstract
We report a rare case of precursor B-cell lymphoblastic leukemia presenting as thyrotoxic goiter, highlighting the diagnostic challenges posed by the overlapping symptomatology of acute leukemia and hyperthyroidism. Such presentations may arise from direct leukemic thyroid infiltration or hematologic complications of antithyroid medications. Our patient, a 32-year-old woman with untreated hyperthyroidism, developed classic thyrotoxic features with hematological abnormalities that ultimately led to a leukemia diagnosis. This case underscores the importance of heightened vigilance when evaluating thyroid abnormalities in patients with hematologic manifestations.
Keywords:
precursor B-cell lymphoblastic leukemia
; grave’s disease
; thyrotoxic goiter
1. Introduction
Acute leukemia, encompassing acute myeloid leukemia (AML) and acute lymphoblastic leukemia (ALL), represents a heterogeneous group of rapidly progressive hematologic malignancies marked by the uncontrolled proliferation of immature hematopoietic blasts in the bone marrow. AML is the most common acute leukemia in adults, with a median age at the time of diagnosis being 68. Furthermore, males have a higher incidence compared to the female population, with a ratio of 5:3 [1]. ALL predominates in the pediatric population, the risk for developing ALL is highest in children younger than 5 years, further the risk then declines slowly until the mid-20s, and begins to rise again gradually after the age of 50. Overall, about 4 of every 10 cases of ALL are in adults [2]. Clinically, patients present with manifestations of bone marrow failure—fever, fatigue, recurrent infections, and bleeding tendencies—resulting from cytopenias. Diagnosis relies on morphology, immunophenotyping, cytogenetics, and molecular testing to differentiate it from other marrow disorders.
Thyrotoxicosis, most frequently secondary to Graves’ disease, has a prevalence in the general population that is estimated to range roughly from 0.2% to 1.2% globally. Subclinical hyperthyroidism, a related mild form, affects about 0.7% to 1.4% of people, increasing to 2-3% among those aged 65 and older. Thyrotoxicosis affects women disproportionately, with female-to-male ratios between 7:1 and 10:1 [3]. It is characterized by excessive thyroid hormone levels, causing tachycardia, weight loss, tremors, and heat intolerance. Causes include Graves’ disease, toxic multinodular goiter, subacute thyroiditis, and drug-induced thyroid dysfunction. Accurate diagnosis necessitates a combination of biochemical thyroid function tests and imaging modalities.
Although rare, an association between acute leukemia and hyperthyroidism has been documented. These may arise from direct leukemic infiltration of the thyroid gland, leading to structural and functional alterations, or from adverse hematologic effects of antithyroid medications such as agranulocytosis and, in extreme cases, acute leukemia. Such overlap in symptomatology can delay diagnosis and complicate management, emphasizing the necessity for heightened clinical vigilance.
2. Case Presentation
A 32-year-old woman with a 2-year history of hyperthyroidism and goitre, with poor medication adherence, presented with 15 days of progressive odynophagia and increased swelling in the front of the neck. Dysphagia was more pronounced for solids than liquids, and a moderate-grade fever was also reported, which was relieved with antipyretics. She reported worsening palpitations and tremors over the past 45 days, during which she was started on carbimazole; low-grade fever, throat pain, and painful swallowing developed shortly thereafter. She noted a recent increase in the size of the neck swelling. Family history was negative for thyroid or other endocrine disorders. She was taking a mixed diet, with reduced appetite and disturbed sleep, with normal bowel and bladder habits.
On systemic examination, the patient was tachycardic and well-saturated with normal vesicular breath sounds bilaterally. Examination of the neck revealed a midline swelling, more prominent on the right side than the left, with the lower border visible. The right lobe swelling measured approximately 6 × 3 cm, while a discrete swelling on the left measured approximately 3 × 2 cm. The swelling moved with deglutition. On palpation, there was increased local temperature; the swelling was non-tender, firm in consistency, and had a smooth surface. A palpable thrill was appreciated at the right lower pole. Auscultation revealed a bruit over the right inferior pole.
Initial laboratory evaluation revealed anemia, thrombocytopenia, and marked leukocytosis with 80% blasts on the differential count. Red cell indices showed microcytosis and hypochromia. Peripheral smear demonstrated markedly elevated WBCs with large blast cells, three to four times the size of mature lymphocytes, having a high nuclear–cytoplasmic ratio, irregular nuclear membranes, open chromatin, scant cytoplasm, and one to two prominent nucleoli. Liver function tests and urinalysis were unremarkable except for trace proteinuria as seen in Table 1 and Table 2. Thyroid profile showed elevated FT4 (2.99 ng/dL) and FT3 (5.50 pg/mL) with suppressed TSH (<0.005 μIU/mL). Abdominal ultrasonography demonstrated hepatomegaly (17.5 cm) and splenomegaly (17.9 × 6.5 cm) without intrahepatic biliary dilatation.
A radioiodine uptake scan and a 111 MBq pertechnetate thyroid scan demonstrated a nodular goitre with a hyperfunctioning nodule replacing the right lobe and a hypoplastic left lobe, consistent with a nodular Graves’ pattern. ENT evaluation showed normal vocal cord mobility; upper gastrointestinal endoscopy was advised for dysphagia. Review of prior investigations (15/12/2022) showed T3 2.64 ng/mL, T4 18.30. µg/dL, TSH < 0.008 µIU/mL, and thyroid ultrasound revealing a 4.4 × 3.6 × 3.7 cm right lobe and a 1.9 × 1.4 × 1.6 cm left lobe, suggestive of nodular goiter.
During the hospital stay, the patient developed bilateral shin pain and subsequently a fever of 104 °F. Blood cultures were obtained, which were negative. Bone marrow biopsy and flow cytometry were performed following oncology consultation. Flow cytometry of bone marrow aspirate demonstrated medium- to large-sized blasts with a high nuclear–cytoplasmic ratio, round to oval or notched nuclei, and 1–3 nucleoli as shown in Figure 1. Immunophenotyping revealed a distinct CD45+ blast population characterized by low side scatter, positivity for CD34, TdT, HLA-DR, CD19, CD10, CD22, cytoplasmic CD79a, CD38, and CD58, and aberrant expression of myeloid markers CD13 and CD33. Following flow cytometry results, a diagnosis of precursor B cell lymphoblastic leukemia with CD 13 and CD 33 was made.
The patient, diagnosed with precursor B-cell acute lymphoblastic leukemia, was initiated on the MCP-841 induction protocol with rituximab on January 16, 2023. Induction therapy consisted of vincristine, daunorubicin, intrathecal methotrexate, L-asparaginase, and oral prednisolone, along with prophylactic allopurinol and supportive antimicrobial agents (acyclovir, fluconazole, and cotrimoxazole). Baseline laboratory investigations showed anemia with preserved platelet and leukocyte counts, and serial monitoring of hematologic and biochemical parameters was planned. During hospitalization, she tolerated induction chemotherapy with scheduled doses of rituximab and L-asparaginase and was discharged on January 21, 2023, with continuation of methimazole and propranolol for coexisting thyrotoxicosis. She was advised to follow up for thyroid function tests, fine-needle aspiration cytology of the thyroid, and repeat hematologic and biochemical investigations.

Table 3.
Flow Cytometry Results.
| Test Name | Results | Units | Bio. Ref. Interval |
|---|---|---|---|
| LEUKEMIA DIAGNOSTIC PANEL (Flow Cytometry) | |||
| MARKERS | RESULT (%) | INTENSITY | INTERPRETATION |
| T cell markers | |||
| CD3 (cyto) | 3.8 | Negative | Negative |
| CD5 | 20.2 | Dim pos | Positive |
| CD7 | 11.9 | Negative | Negative |
| B cell markers | |||
| CD19 | 94.0 | Moderate | Positive |
| CD20 | 4.6 | Negative | Negative |
| CD22 | 52.6 | Dim to mod | Positive |
| CD22 (cyto) | 23.4 | Dim pos | Positive |
| CD79a (cyto) | 96.8 | Mod to bright | Positive |
| CD58 | 71.1 | Dim to mod | Positive |
| Myeloid markers | |||
| CD13 | 64.0 | Partial dim to mod | Positive |
| CD15 | 0.4 | Negative | Negative |
| CD33 | 56.0 | Partial dim to mod | Positive |
| CD66c | 0.0 | Negative | Negative |
| MPO | 5.1 | Negative | Negative |
| Precursor markers | |||
| CD34 | 36.8 | Dim to mod | Positive |
| CD117 | 0.2 | Negative | Negative |
| TdT | 89.6 | Moderate | Positive |
| CD99 | 98.8 | Moderate | Positive |
| Other markers | |||
| CD45 | 99.3 | Dim pos | Positive |
| CD9 | 3.1 | Negative | Negative |
| CD10 | 97.9 | Mod to bright | Positive |
| HLA-DR | 96.4 | Mod to bright | Positive |
| CD38 | 94.1 | Dim to mod | Positive |
3. Discussion
The coexistence of hyperthyroidism, especially Graves’ disease (GD), and acute leukemia is rare but increasingly reported in the literature. Our case describes a 32-year-old woman with previously diagnosed but untreated hyperthyroidism who presented with classic thyrotoxic symptoms as well as hematological findings that led to a diagnosis of precursor B-cell lymphoblastic leukemia. This case provides an opportunity to review potential associations, shared mechanisms, and important clinical considerations in such presentations.
Previous studies have demonstrated an increased incidence of thyroid diseases, predominantly autoimmune disorders such as Graves’ disease and Hashimoto’s thyroiditis, among patients with acute leukemia compared to the general population. One such study found a threefold higher prevalence of thyroid disease in patients with acute leukemia, with most cases involving acute myeloid leukemia (AML), but also acute lymphoblastic leukemia (ALL) and chronic myeloid leukemia in the accelerated phase. [4]
Table 4 summarises reported cases worldwide, describing the coexistence of hyperthyroidism and acute leukemias. Graves’ disease was the most frequent thyroid condition, though toxic goiter, autoimmune or infectious thyroiditis, and thyroid carcinomas treated with radioiodine were also reported. The leukemias observed encompassed both lymphoid and myeloid lineages, including ALL, AML subtypes (M1, M2, M3/APL, M6), and myelomonocytic or monocytic variants. Treatments for hyperthyroidism frequently involved thionamides or radioiodine, both of which have been implicated in marrow toxicity or genotoxicity, and several cases developed acute leukemia following prolonged drug exposure or repeated radioiodine therapy.
5. Conclusions
The concurrent occurrence of hyperthyroidism, particularly autoimmune Graves’ disease, and acute leukemia, though rare, represents a clinically significant intersection that warrants careful attention. The overlap of shared autoimmune and molecular mechanisms, coupled with the potential adverse effects of antithyroid therapy, highlights the intricate interplay between endocrine and hematological disorders. Recognizing these associations is essential, as it not only aids in timely diagnosis and comprehensive management but also opens avenues for further research into the pathophysiological links and therapeutic strategies at this intersection.
6. Limitations
The patient didn’t have any additional workup, like imaging with FDG PET or surgical biopsy, which was not pursued due to a lack of any severe compressive symptoms. Also, the patient didn’t undergo scheduled FNAC as she improved with chemotherapy; therefore, the possibility of infiltration of the thyroid by blast cells could not be ruled out.
References
- Vakiti A, Reynolds SB, Mewawalla P. Acute Myeloid Leukemia. [Updated 2024 Apr 27]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-.
- Key statistics for acute lymphocytic leukemia [Internet]. [cited 2025 Sept 21]. Available from: https://www.cancer.org/cancer/types/acute-lymphocytic-leukemia/about/key-statistics.html?
- Blick C, Nguyen M, Jialal I. Thyrotoxicosis. [Updated 2025 Jan 18]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK482216/?
- JIANG, YAJIAN, KEYUE HU, WANZHUO XIE, et al. 2014. “Hyperthyroidism with Concurrent FMS-like Tyrosine Kinase 3-Internal Tandem Duplication-Positive Acute Promyelocytic Leukemia: A Case Report and Review of the Literature.” Oncology Letters 7 (2): 419–22. [CrossRef]
- Bishnoi, Komal, Ralph Emerson, Girish Kumar Parida, Prapti Acharya, Somanath Padhi, and Kanhaiyalal Agrawal. 2023. “Acute Myeloid Leukemia Following Radioactive Iodine Therapy for Metastatic Follicular Carcinoma of the Thyroid.” Indian Journal of Nuclear Medicine 38 (1): 56–58. [CrossRef]
- Nehara HR, Gupta BK, Parmar S, Kumar V, and Sihag D, Beniwal S. 2025. “(PDF) Antithyroid Drug-Induced Pancytopenia Followed by Acute Lymphoblastic Leukemia: A Rare Case.” ResearchGate, ahead of print, May 24. [CrossRef]
- Oka, Satoko, Taiji Yokote, Tetuya Hiraiwa, et al. 2006. “Hyperthyroidism Associated With Philadelphia-Chromosome-Positive–Positive Acute Lymphoblastic Leukemia.” Journal of Clinical Oncology 24 (21): 3500–3502. [CrossRef]
- Tsabouri, S. E., A. Tsatsoulis, Chr. Giannoutsos, and K. L. Bourantas. 2000. “Acute Lymphoblastic Leukaemia Presenting as an Enlarged Goitre in a Pregnant Woman with Graves’ Disease.” European Journal of Haematology 65 (1): 84–85. [CrossRef]
- Niles, Denver, Juri Boguniewicz, Omar Shakeel, et al. 2019. “Candida Tropicalis Thyroiditis Presenting With Thyroid Storm in a Pediatric Patient With Acute Lymphocytic Leukemia.” Pediatric Infectious Disease Journal 38 (10): 1051–53. [CrossRef]
- Fadlalbari, Ghassan Faisal, Samar Sabir Hassan, Asmahan T Abdallah, Samar Omer Abusamra, Abeer Mohamed Abdalrhman, and Mohamed Ahmed Abdullah. 2021. “Acute Lymphoblastic Leukemia Complicating Graves’ Disease in a Sudanese Adolescent Girl: A Case Report and Exploration of the Underlying Mechanism Possibilities.” Preprint, In Review, August 18. [CrossRef]
- Perillat-Menegaux, Florence, Jacqueline Clavel, Marie-Françoise Auclerc, et al. 2003. “Family History of Autoimmune Thyroid Disease and Childhood Acute Leukemia1.” Cancer Epidemiology, Biomarkers & Prevention 12 (1): 60–63.
- Thomson, John A. 1963. “ACUTE LEUKÆMIA FOLLOWING ADMINISTRATION OF RADIOIODINE FOR THYROTOXICOSIS.” The Lancet 282 (7315): 978–79. [CrossRef]
- Al-Anazi, Khalid A., Sohail Inam, MT Jeha, and R Judzewitch. 2005. “Thyrotoxic Crisis Induced by Cytotoxic Chemotherapy.” Support Care Cancer 13 (3): 196–98. PubMed (15459765). [CrossRef]
- McBride, J. A. 1964. “Acute Leukaemia After Treatment for Hyperthyroidism with Radioactive Iodine.” British Medical Journal 2 (5411): 736.
- Aksoy, Muzaffer, Sakir Erdem, Hikmet Tezel, and Tuna Tezel. 1974. “ACUTE MYELOBLASTIC LEUKÆMIA AFTER PROPYLTHIOURACIL.” The Lancet 303 (7863): 928–29. [CrossRef]
- Johnson, John E., Jr. 1962. “Acute Myelomonocytic Leukemia After Radioiodine Therapy of Hyperthyroidism.” JAMA 179 (7): 572–73. [CrossRef]
- Imai, Chihaya, Toshio Kakihara, Akihiro Watanabe, et al. 2002. “ACUTE SUPPURATIVE THYROIDITIS AS A RARE COMPLICATION OF AGGRESSIVE CHEMOTHERAPY IN CHILDREN WITH ACUTE MYELOGENEOUS LEUKEMIA.” Pediatric Hematology and Oncology 19 (4): 247–53. [CrossRef]
- Kolade, Victor O., Timothy J. Bosinski, and Enrico L. Ruffy. 2005. “Acute Promyelocytic Leukemia After Iodine-131 Therapy for Graves’ Disease.” Pharmacotherapy: The Journal of Human Pharmacology and Drug Therapy 25 (7): 1017–20. [CrossRef]
- Fadilah, SAW, I Faridah, and S K Cheong. 2000. Transient Hyperthyroidism Following L-Asparaginase Therapy for Acute Lymphoblastic Leukemia. 55 (4).
- Laurenti, L., P. Salutari, S. Sica, et al. 1998. “Acute Myeloid Leukemia after Iodine-131 Treatment for Thyroid Disorders.” Annals of Hematology 76 (6): 271–72. [CrossRef]
- McCormack, Kenneth R., and Glenn E. Sheline. 1963. “LEUKEMIA AFTER RADIOIODINE THERAPY FOR HYPERTHYROIDISM.” California Medicine 98 (4): 207–9.
- Burns, Thomas W. 1960. “Acute Leukemia After Radioactive Iodine (I131) Therapy for Hyperthyroidism.” Archives of Internal Medicine 106 (1): 97. [CrossRef]
- Kennedy, William M., and Robert G. Fish. 1959. “Acute Granulocytic Leukemia after Radioactive-Iodine Therapy for Hyperthyroidism.” New England Journal of Medicine 260 (2): 76–77. [CrossRef]
- Mittal, Lalchand, and Sandeep Jasuja. 2025. “Carbimazole-Induced Acute Myeloid Leukemia: A Very Rare Case Report and Review of the Literature.” Indian Journal of Cancer 62 (1): 142–44. [CrossRef]
- Khanna G, Damle NA, Agarwal S, et al. Mixed Phenotypic Acute Leukemia (mixed myeloid/B-cell) with Myeloid Sarcoma of the Thyroid Gland: A Rare Entity with Rarer Asssociation - Detected on FDG PET/CT. Indian J Nucl Med. 2017;32(1):46-49. [CrossRef]
- Goldenberg D, Joshi M, Malysz J, Claxton D, Cottrill EE. Myeloid sarcoma of the thyroid. Ear Nose Throat J. 2017;96(12):460-461.
- Hemminki, Kari, Wuqing Huang, Jan Sundquist, Kristina Sundquist, and Jianguang Ji. 2020. “Autoimmune Diseases and Hematological Malignancies: Exploring the Underlying Mechanisms from Epidemiological Evidence.” Autoimmune Disease and Comorbidity 64 (August): 114–21. [CrossRef]
- Umesono, Kazuhiko, Vincent Giguere, Christopher K. Glass, Michael G. Rosenfeld, and Ronald M. Evans. 1988. “Retinoic Acid and Thyroid Hormone Induce Gene Expression through a Common Responsive Element.” Nature 336 (6196): 262–65. [CrossRef]
- Dayton, A. I, J R Selden, G Laws, et al. 1984. “A Human C-erbA Oncogene Homologue Is Closely Proximal to the Chromosome 17 Breakpoint in Acute Promyelocytic Leukemia.” Proceedings of the National Academy of Sciences 81 (14): 4495–99. [CrossRef]
- Stunnenberg, Hendrik G., Custodia Garcia-Jimenez, and Joan L. Betz. 1999. “Leukemia: The Sophisticated Subversion of Hematopoiesis by Nuclear Receptor Oncoproteins.” Biochimica et Biophysica Acta (BBA) - Reviews on Cancer 1423 (1): F15–33. [CrossRef]
- Graupner, Gerhart, Ken N. Wills, Maty Tzukerman, Xiao-kun Zhang, and Magnus Pfahl. 1989. “Dual Regulatory Role for Thyroid-Hormone Receptors Allows Control of Retinoic-Acid Receptor Activity.” Nature 340 (6235): 653–56. [CrossRef]
- Kennedy, Vanessa E., and Catherine C. Smith. 2020. “FLT3 Mutations in Acute Myeloid Leukemia: Key Concepts and Emerging Controversies.” Frontiers in Oncology Volume 10-2020. https://www.frontiersin.org/journals/oncology/articles/10.3389/fonc.2020.612880.
Figure 1.
Peripheral Smear.
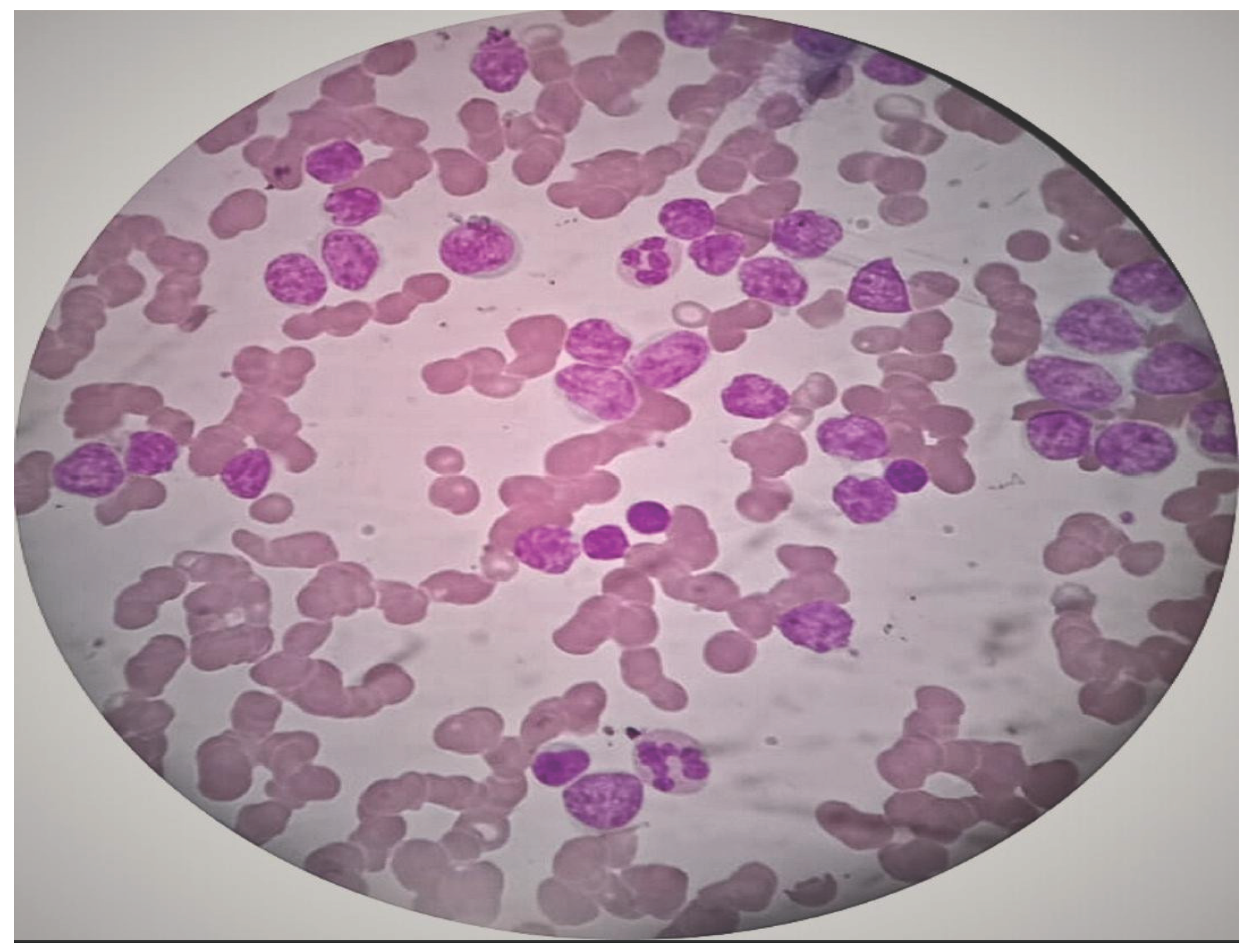
Table 1.
Laboratory Results.
| Parameter | Value | Units | Normal Range |
|---|---|---|---|
| Hemoglobin | 8.9 | g/dl | 12–16 (F), 13–17 (M) |
| Total Leukocyte Count (TLC) | 185,290 | /mm3 | 4,000–11,000 |
| Red Blood Cells (RBC) | 4.05 | million/mm3 | 4.2–5.4 (F), 4.7–6.1 (M) |
| Packed Cell Volume (PCV) | 28.9 | % | 36–46 (F), 40–54 (M) |
| Mean Corpuscular Volume (MCV) | 71.4 | fL | 80–100 |
| Mean Corpuscular Hemoglobin (MCH) | 22 | pg | 27–32 |
| Mean Corpuscular Hemoglobin Concentration | 30.8 | g/dl | 32–36 |
| Red Cell Distribution Width (RDW) | 22.7 | % | 11.5–14.5 |
| Erythrocyte Sedimentation Rate | 40 | mm/hr | <20 (M), <30 (F) |
| Total Bilirubin | 0.7 | mg/dl | 0.3–1.2 |
| Direct Bilirubin |
0.4 | mg/dl | <0.3 |
| AST (SGOT) | 22 | U/L | 5–40 |
| ALT (SGPT) |
11 | U/L | 5–45 |
| Alkaline Phosphatase (ALP) | 96 | U/L | 44–147 |
| Total Protein | 7.7 | g/dl | 6.0–8.3 |
| Albumin | 3.5 | g/dl | 3.5–5.0 |
| Gamma Glutamyl Transferase(GGT) | 31 | U/L | 9–48 (M), 8–35 (F) |
| Urea | 20 | mg/dl | 15–40 |
| Creatinine | 0.9 | mg/dl | 0.6–1.3 |
| Uric Acid | 9.2 | mg/dl | 3.5–7.2 (M), 2.6–6.0 (F) |
| Sodium (Na+) | 131 | mmol/L | 135–145 |
| Potassium (K+) | 3.7 | mmol/L | 3.5–5.0 |
| Chloride (Cl−) | 99 | mmol/L | 98–106 |
| Test | Result | Reference/Normal Range | |
| Iron Profile | |||
| Serum Iron | 42 | 60 – 170 µg/dL | |
| TIBC | 220 | 240 – 450 µg/dL | |
| UIBC | 177 | 150 – 375 µg/dL | |
| Transferrin saturation | 19% | 20 – 50% | |
| Ferritin | Not reported | ||
| Vitamin Profile | |||
| Vitamin B12 | 481 | 200 – 900 pg/mL | |
| Folic Acid | 1.4 | 2.7 – 17 ng/mL | |
| Hematology | |||
| Reticulocyte count | 0.8 % | 0.5 – 1.5 % | |
| Corrected Reticulocyte Count | 0.34 % | 0.5 – 1.5 % | |
| Platelet | Pending | 150 – 400 ×109/L | |
| PCV | Pending | 36 – 46 % | |
| Serology | |||
| HIV | Negative | Negative | |
| HBsAg | Negative | Negative | |
| HEV | Negative | Negative | |
| VDRL | Pending | Negative |
Table 2.
Urinalysis:.
| Test | Result | Normal/Reference range |
|---|---|---|
| Urinalysis | ||
| Specific Gravity | 1.010 | 1.005 – 1.030 |
| pH | 7 | 4.6 – 8.0 |
| Protein | Trace | Nil / Negative |
| Glucose | Nil | Nil / Negative |
| Ketone | Nil | Nil / Negative |
| Urobilinogen | Normal | Normal |
| Bilirubin | Nil | Nil / Negative |
| Microscopy | ||
| Pus cells | 1 /hpf | 0–5 /hpf |
| Epithelial cells | 1 /hpf | 0–5 /hpf |
| RBC | Nil | 0–2 /hpf |
| Casts | Nil | Negative |
| Crystals | Nil | Negative |
| Nitrite | Nil | Negative |
| Leukocyte esterase | Nil | Negative |
| Other tests | ||
| Dengue | Negative | Negative |
| Malaria | Negative | Negative |
Table 4.
Summary of Reported Cases.
| Sl no. | AUTHOR | Country | Age | Type of Hyperthyroidism |
Treatment Received |
Type Of Acute Leukemia |
Treatment Received For Leukemia |
|---|---|---|---|---|---|---|---|
| 1 | Jiang et al. [5] | China | 42/ M | The patient was initially treated with propylthiouracil (PTU) at the time of diagnosis; however, due to drug-induced leukopenia, the therapy was switched to methimazole (MMI) in 2010 | M3 leukemia harboring the FMS-like tyrosine kinase 3-internal tandem duplication. |
ATRA (25 mg/m 2 /d, per os) |
|
| 2 | Bishnoi et al. [6] | India | 52/ F | Follicular thyroid carcinoma | The patient underwent a total thyroidectomy in 2011. Between 2012 and 2016, she received 8 cycles of radioactive iodine (RAI) therapy (200 mCi per cycle), with a cumulative dose of 1600 mCi. Subsequently, she was given palliative radiotherapy foran L4 spinal metastasis | AML with myelodysplasia-related changes (WHO category II) as per the 2017 revised WHO classification | N/A |
| 3 | Nehara et al. [7] | India | 26/M | Graves disease | The patient was started on carbimazole 20 mg twice daily and propranolol 40 mg three times daily, followed by radioiodine ablation after achieving remission from acute lymphoblastic leukemia (ALL) | ALL with 85% blasts |
Multicentric protocol (MCP 841) chemotherapy for 2.5 years (Oka et al. 2006) |
| 4 | Oka S et al. [8] | Japan | 35/M | D/t to metastatic involvement | N/A | Philadelphiaa-chromosome-PPositive– acute lymphoblastic leukemia (ALL) | chemotherapy for ALL with lenograstim 5g/kg per day by subcutaneous injection |
| 5 | Tsabouri et al. [9] | Greece | 24/F Pregnant |
Graves’ disease | She was initially managed with carbimazole, which was later switched to propylthiouracil 50 mg/day during her pregnancy | Acute lymphoblastic leukaemia (ALL) |
Chemotherapy and 18 months later, achieved complete haematologic remission. Her current maintenance therapy for ALL |
| 6 | Niles D et al. [10] |
USA | 15/ M | Candia tropicalis thyroiditisisis | Started on methimazole, followed by propylthiouracil and eventually thyroidectomy after 9 weeks of treatment. | Acute lymphocytic leukemia | Induction chemotherapy with vincristine, daunorubicin, polyethylene glycol-asparaginase, and intrathecal methotrexate |
| 7 | Fadlalbari et al. [11] |
SUDAN | 16/F | Graves’ disease | The patient was initially started on carbimazole, and after 14 months, was transitioned to levothyroxine due to the development of hypothyroidism | ALL | N/A(Perillat-Menegaux et al. 2003) |
| 8 | Perillat-Menegaux F et al. [12] | France | Autoimmune thyroid diseases (Graves’ disease and/or hyperthyroidism and Hashimoto’s disease, and/or hypothyroidism) | N/A | ALL ANLL |
N/A | |
| 9 | Thomson [13] | Edinburgh | 40/ F | Thyrotoxicosis | Radioiodine therapy | Acute leukemia | treated with prednisone 40 mg daily and 6-mercaptopurine 50 mg. t.i.d. (Al-Anazi et al. 2005) |
| 10 | Al-Anazi et al. [14] |
Riyadh, Saudi Arabia | 25/F | Thyrotoxic crisis occurring in a patient with Graves’ disease induced by the course of chemotherapy given earlier. | The patient was started on carbimazole 20 mg twice daily, atenolol 100 mg per day, and hydrocortisone 100 mg intravenously, followed by 100 mg IV every 6 hours. By September 7, the thyrotoxic features had slightly improved; however, tachycardia had worsened with a pulse rate of 130/min. Consequently, the atenolol dose was increased to 600 mg/day, while the carbimazole dose was adjusted to 40 mg/day. | Acute myeloid leukaemia (AML, M2 type) | Induction course of chemotherapy (3+7 protocol) composed of cytarabine (Ara-C, Cytosar) 100 mg/m2 i.v. daily for 7 days and daunorubicin 60 mg/m2 i.v. daily for 3 days. |
| 11 | McBride [15] |
Edinburgh | 64/F | N/A | Carbimazole followed by radioactive iodine | Acute leukemia | Prednisolone 60mg followed by 6 6-mercaptopurine 100mg daily |
| 12 | Aksoy et al. [16] |
Istanbul, Turkey | 74/F | Grave’s disease | Propylthiouracil | Acute myeloblastic leukemia | Corticosteroid, mercaptopurine, vincristine |
| 13 | Johnson et al. [17] |
Texas | 55/M | Diffuse toxic goiter with congestive heart failure. | Methimazole and reserpine, followed by radioactive iodine | Acute myelomonocytic leukemia | N/A |
| 14 | Imai et al. [18] |
Niigata, Japan |
11/M 14/F |
Acute suppurative Thyroiditis with bacterial etiology Acute suppurative Thyroiditis with bacterial etiology |
Clindamycin Clindamycin |
AML (FAB classification: M1) AML (FAB classification: M2) |
High- does cytarabine (AraC) and etoposide (ETP) with intrathecal injection of methotrexate (MTX), AraC, and hydrocortisone (HDC), pirarubicin, vincristine, and 5 days’ continuous infusion of AraC |
| 15 | Kolade et al. [19] |
New york | 47/M | Graves disease | Propylthiouracil, propranolol, followed by radioactive iodine | Acute promyelocytic leukemia | All trans retinoic acid with anthracycline-based chemotherapy |
| 16 | Fadilah et al. [20] |
Kuala lumpur | 18/M 52/M |
Transient hyperthyroidism Transient hyperthyroidism |
No anti-thyroid therapy No anti-thyroid therapy |
Acute lymphoblastic leukemia Acute lymphoblastic leukemia |
L asparginase L asparginase |
| 17 | Laurenti et al. [21] | Italy | 48/F 44/F |
Nodular thyroid Medullary thyroid carcinoma |
Radioiodine therapy Radioiodine therapy |
AML M2, AML M6 |
Mitoxantrone 12 mg/m2 days 1, 3, and 5, VP16 100 mg/m2 days 1–5, and cytosine arabinoside 100 mg/m2 days 1–10. Complete remission was achieved, and consolidation chemotherapy- motherapy with mitoxantrone 12 mg/m2 days 4, 5, and 6 and cytosine arabinoside 500 mg/m2 days 1–6. Not considered eligible for aggressive chemotherapy |
| 18 | McCormack et al. [22] | San Francisco | 48/M | Radioiodine therapy | Acute myelomonocytic leukemia | N/A | |
| 19 | Burns et al. [23] | Missouri | 65/M 64/F |
Graves disease Goiter |
Radioiodine therapy | Acute monocytic leukemia | Prednisone, 20 mg per day, |
| 20 |
Kennedy et al. [24] | North Carolina | 38/M | Radioiodine therapy | Acute granulocytic leukemia | N/A | |
| 21 | Mittal et al. [25] | India | 34/M | Thyrotoxicosis | Carbimazole | Acute myeloid leukemia | Induction chemotherapy (daunorubicin and cytarabine) for 7 days and three cycles of high-dose cytarabine chemotherapy as consolidation chemotherapy. |
| 22 |
Khanna et al. [26] |
India | 58/F |
Clinically and biochemically euthyroid. Midline neck swelling that moved with deglutition. |
Mixed phenotypic Acute leukemia (mixed myeloid/B/B/cell) with myeloid sarcoma, involving the thyroid gland |
Hoelzer’s protocol, comprising daunorubicin, vincristine, methylprednisolone, and L-asparaginase, along with intrathecal methotrexate. |
|
| 23 | Dana Goldenberg et al. [27] | USA | 48/F | Myeloid sarcoma of the thyroid | Cladribine, cytarabine, and filgrastim with mitoxantrone |
Acute myeloid leukemia (AML) |
Allogeneic stem cell transplant |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



