Submitted:
11 September 2025
Posted:
12 September 2025
You are already at the latest version
Abstract
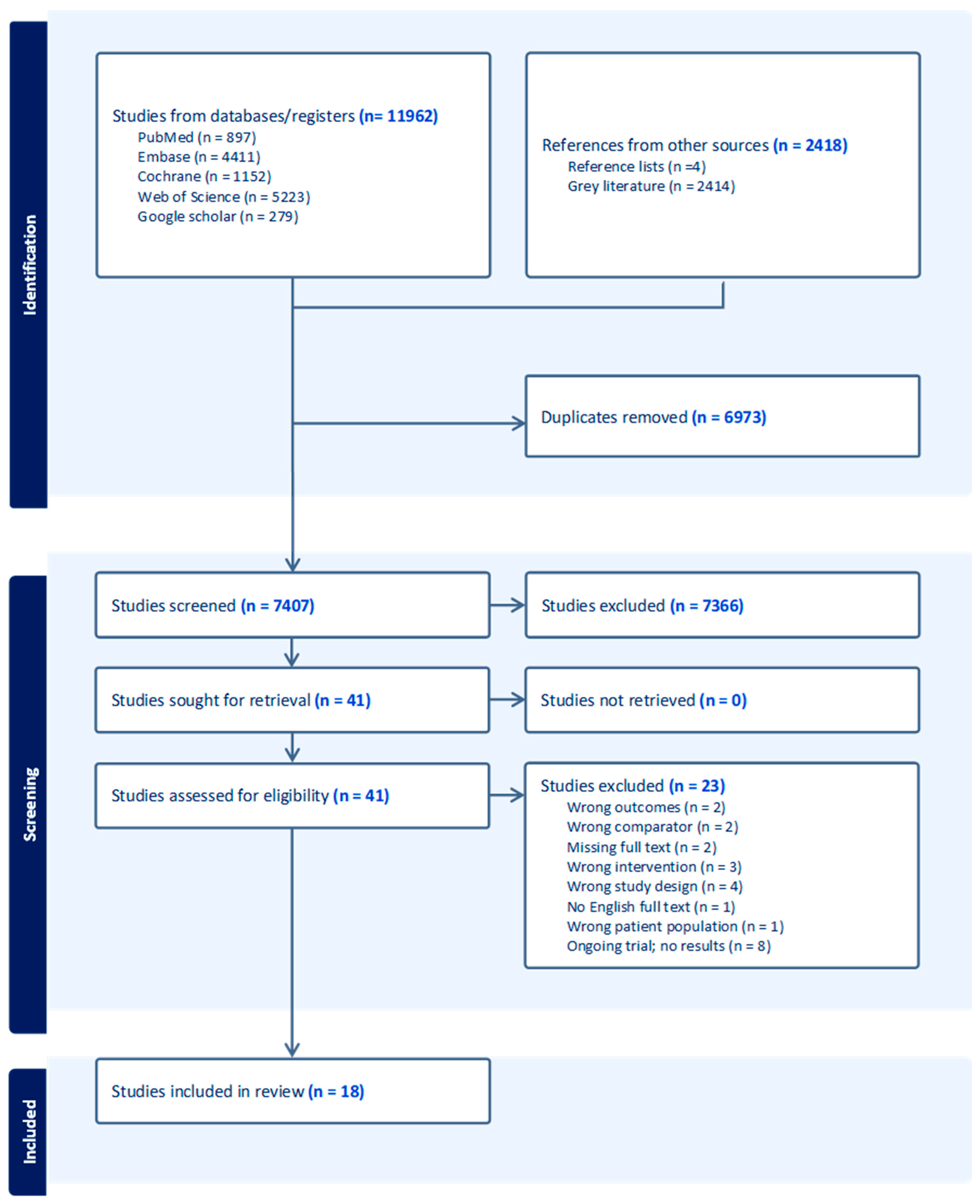
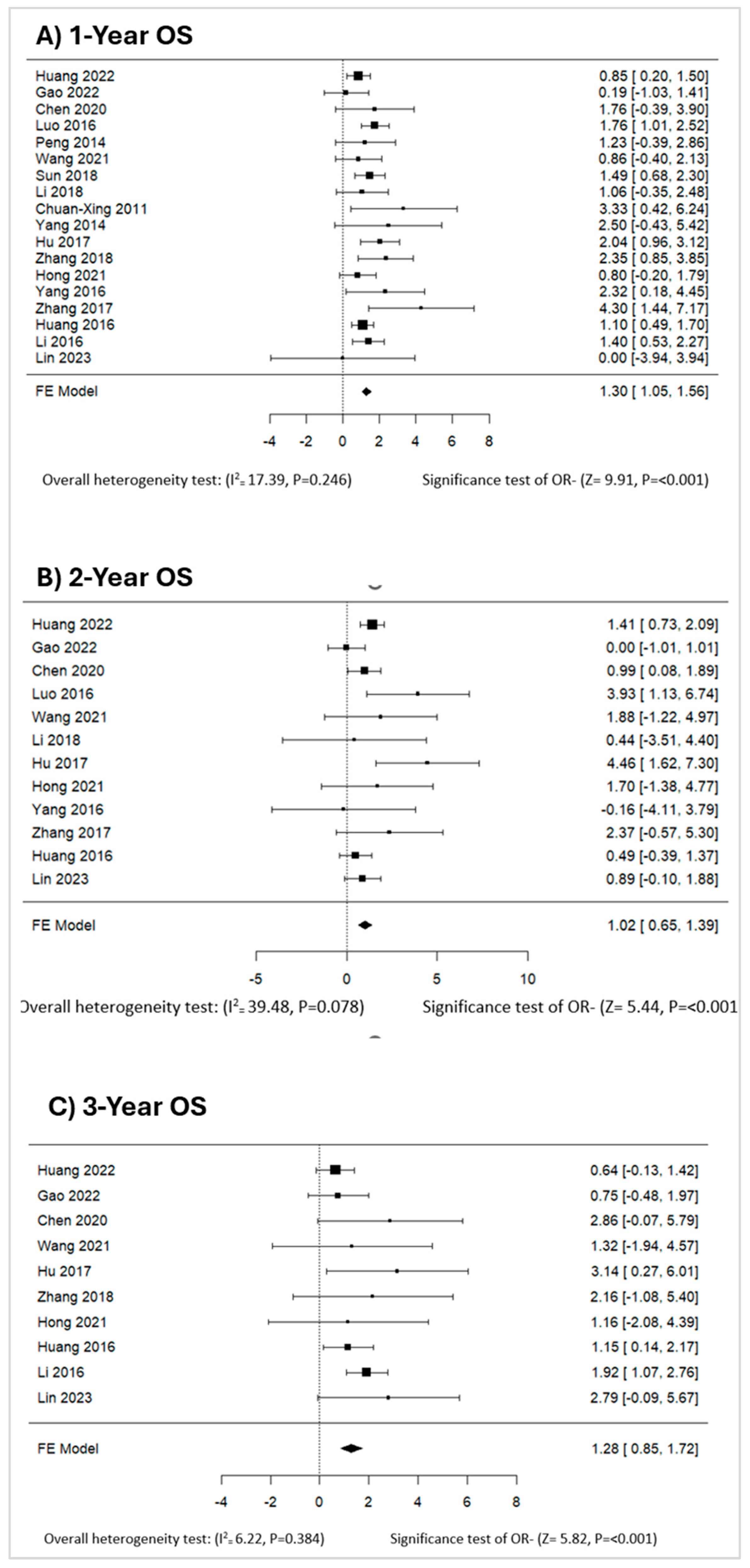
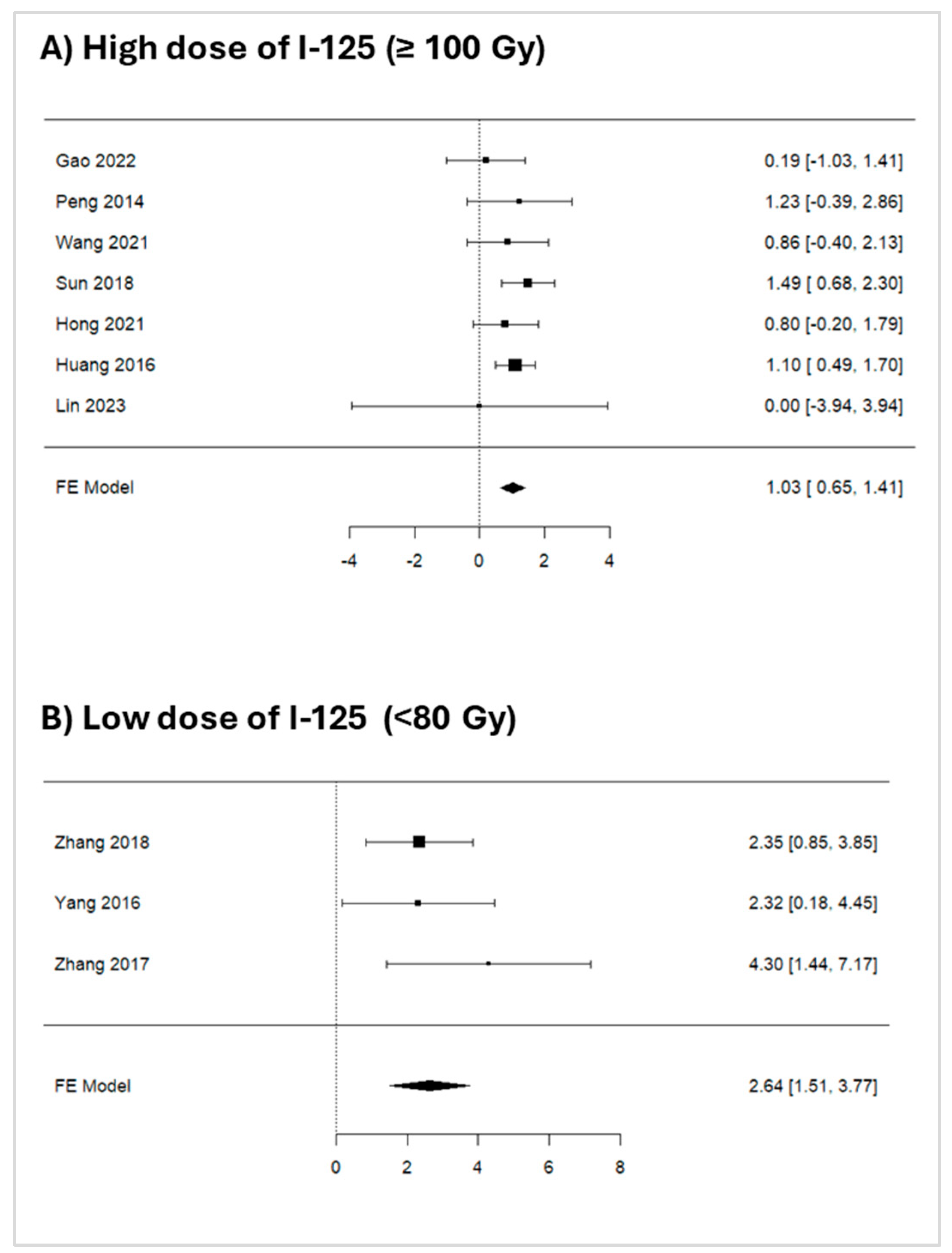
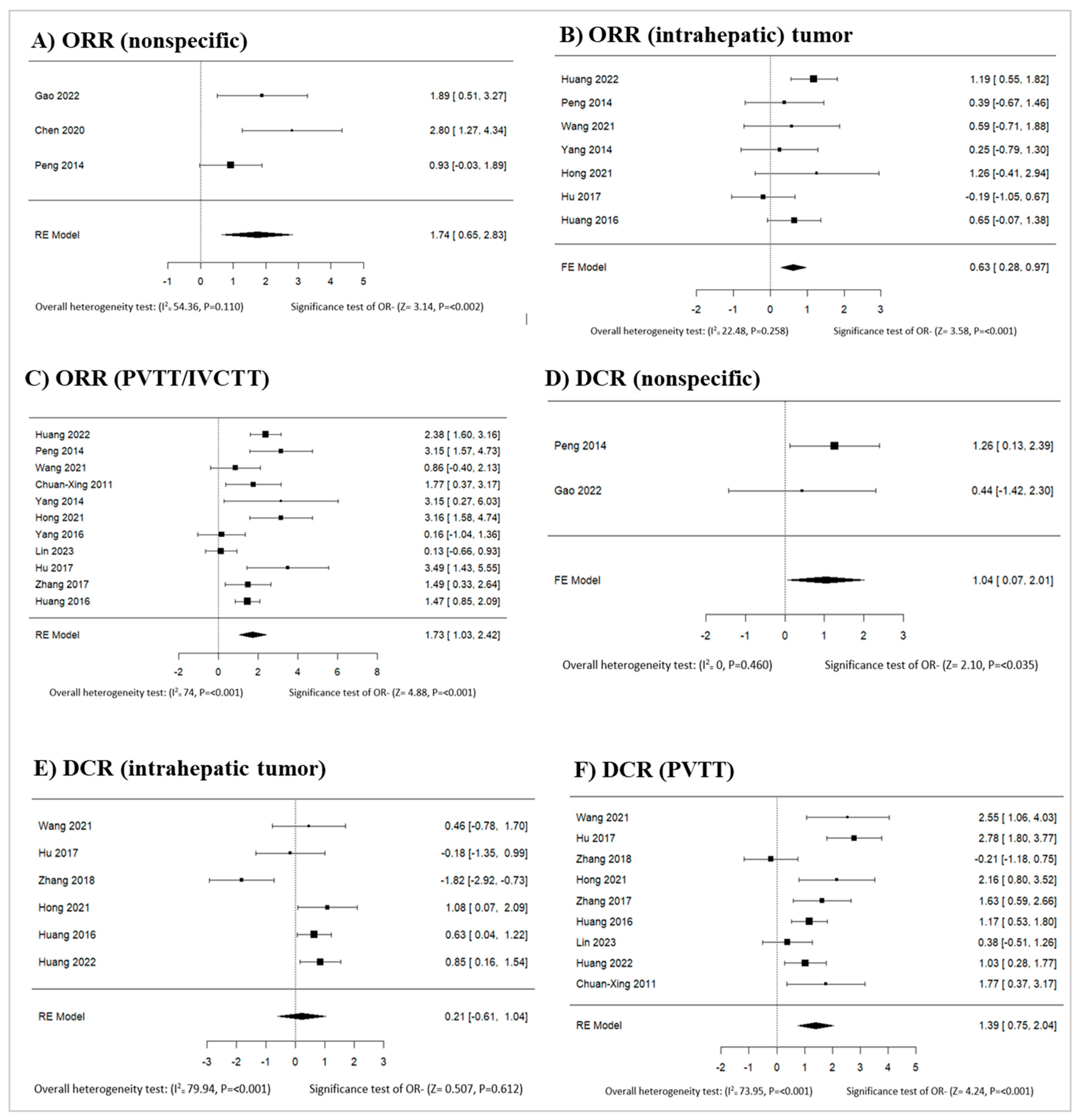
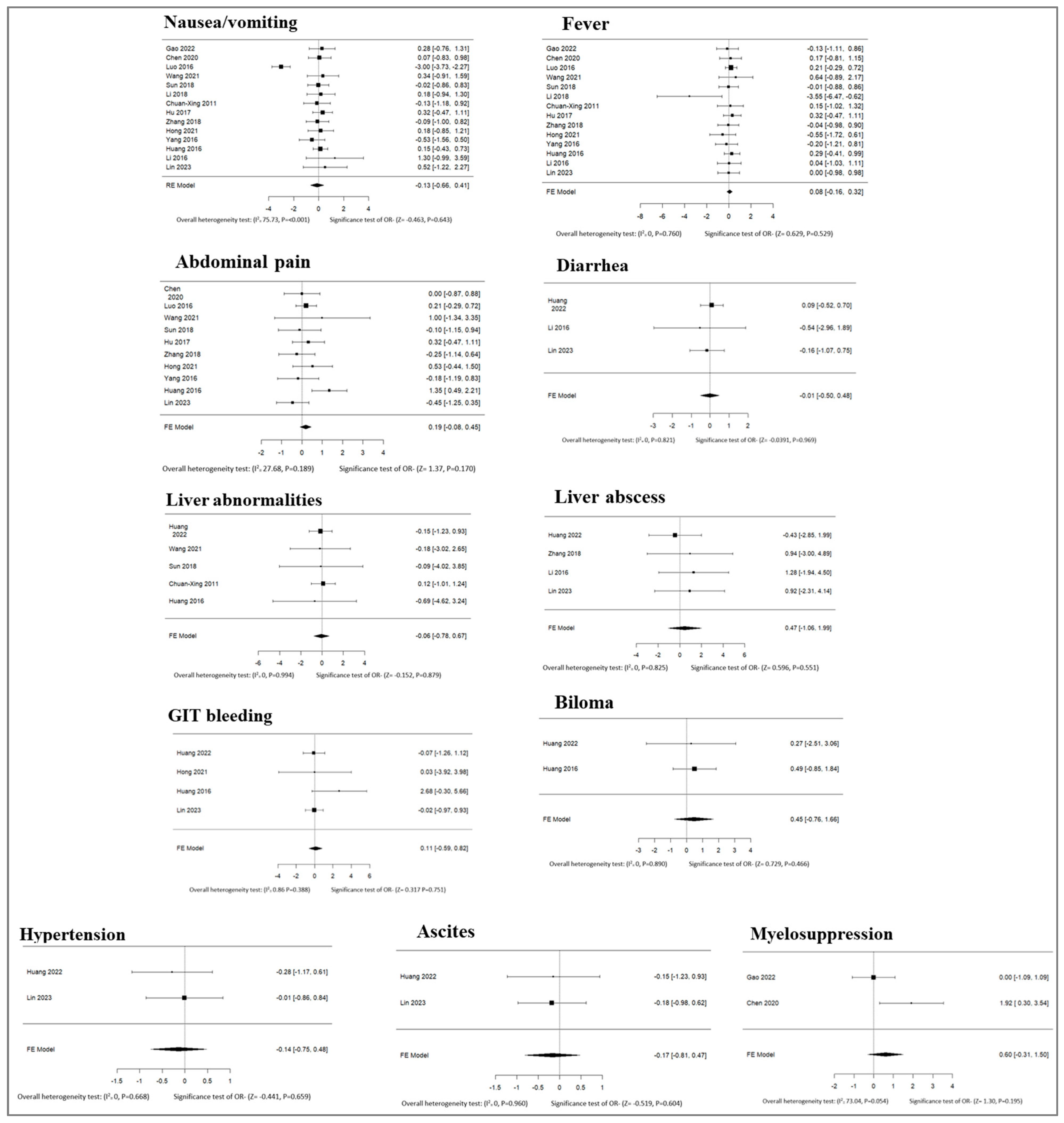
Introduction This systematic review and meta-analysis aimed to evaluate the efficacy and safety of TACE combined with I-125 brachytherapy versus TACE alone in Hepatocellular carcinoma (HCC) patients. Methods Following the PRISMA guidelines, we searched databases, including PubMed, EMBASE, the Cochrane Library, Scopus, Web of Science, and grey literature, for articles published between January 1, 2010 and November 30, 2023. Eligible studies compared TACE with and without I-125 brachytherapy, from randomized controlled trials (RCTs) and non-randomized comparative studies. Primary outcomes were overall survival (OS) at 1, 2, and 3 years. Secondary outcomes comprised progression-free survival (PFS), overall response rate (ORR), disease control rate (DCR), and adverse events. Data extraction and quality assessment were conducted using Covidence software and validated risk-of-bias tools. Meta-analyses were performed using Stata. Results Eighteen studies (n=1,872 patients) were included. TACE + I-125 brachytherapy significantly improved OS at 1 year (OR: 1.30, 95%; CI: 1.05–1.56), 2 years (OR: 1.02, 95%; CI: 0.65–1.39), and 3 years (OR: 1.28, 95%; CI: 0.85–1.71) compared to TACE alone. Tumor response rates, including overall response rate (ORR: 1.74, 95%; CI: 0.65–2.83) and disease control rate (DCR: 1.04, 95%; CI: 0.07–2.01), were also significantly higher in the combination group. Subgroup analyses showed consistent OS outcomes between higher and lower doses of I-125. Adverse event rates were insignificant and comparable between groups. Conclusion TACE combined with I-125 brachytherapy enhances survival and tumor response without increasing adverse events, offering a promising strategy for managing advanced HCC. Further RCTs are warranted to confirm these findings.
Keywords:
1. Introduction
2. Methods
2.1. Protocol and Registration
2.2. Search Strategy
2.3. Eligibility Criteria
- The population included adult patients (≥18 years old) diagnosed with HCC. Studies with similar baseline characteristics were included.
- Intervention: TACE combined with I-125 implantation (I-125 brachytherapy) was used. No limitations concerning agent, dose, methods, or duration of administration were imposed.
- Comparator: TACE monotherapy.
- Primary outcomes: overall survival (after at least one year)
- The secondary outcomes included at least one of the following efficacy outcome measures reported after at least one year: overall survival, progression-free survival, and the tumor response rate assessed by the modified RECIST criteria [24]. At least one of the following safety outcome measures was used: serious adverse events, treatment-related mortality, or liver function impairment.
- Study design: RCTs and nonrandomized comparative studies (i.e., non-RCTs, case-control studies, or cohort studies) were considered.
- Language: English.
- The study focused on non-HCC patients.
- Patients diagnosed with multiple cancers were included.
- Different brachytherapy isotopes were used.
- Authors did not report any of the specified efficacy or safety outcomes.
- These studies are noncomparative single-arm studies; case series; case reports; abstracts; reviews; commentaries; and animal studies.
2.4. Search and Selection Process
2.5. Data Extraction and Quality Assessment
2.6. Outcome
2.7. Data Synthesis and Statistical Analysis
3. Results
3.1. Study Selection
3.2. Study Characteristics
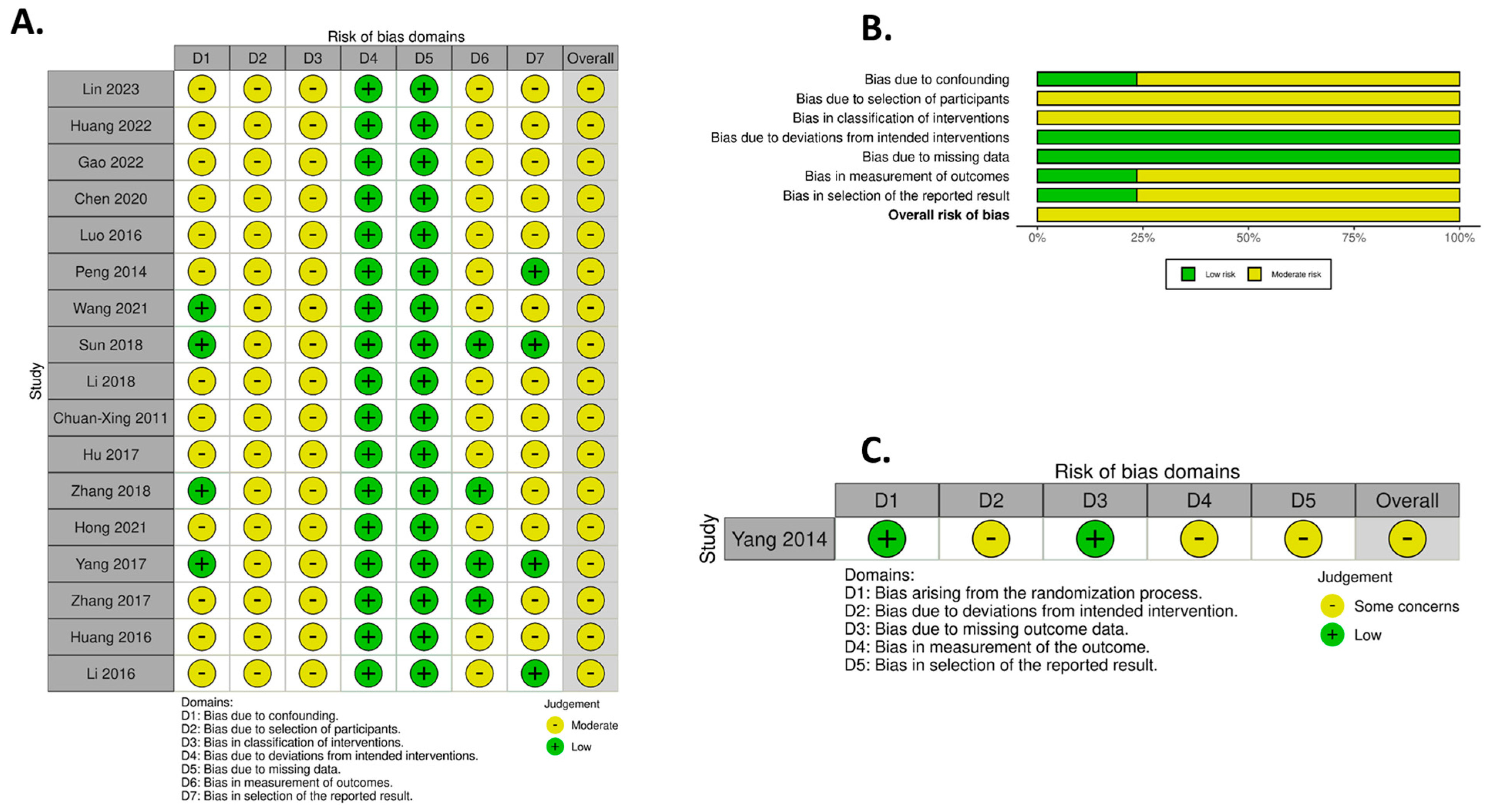
3.3. Risk of Bias in the Included Studies
3.4. Meta-Analysis
3.4.1. Primary Outcomes
Overall Survival at 1 Year
Overall Survival at 2 Years
Overall Survival at 3 Years
3.4.2. Secondary Outcomes
Cancer Response Rates and Survival Data
3.5. Non-Specific ORR
3.6. Intrahepatic Tumor ORR
3.7. PVTT/IVCTT ORR
Meta-Analysis of DCR
3.8. Intrahepatic Tumor DCR
3.9. PVTT/IVCTT DCR
3.9.1. Progression Free Survival (PFS)
3.9.2. Nonspecific PFS
3.9.3. Intrahepatic Tumor PFS
3.9.4. PVTT PFS
4. Discussion
4.1. Meta-Analysis Findings
4.1.1. Overall Survival (OS)
4.1.2. Objective Response Rate (ORR) and Disease Control Rate (DCR)
4.1.3. Progression-Free Survival (PFS)
4.1.4. Safety Analysis
4.2. Strengths and Limitations
4.3. Implications for Clinical Practice
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gao FL, Wang Y, Huang XZ, Pan TF, Guo JH. I-125 seeds brachytherapy with transcatheter arterial chemoembolization for subcapsular hepatocellular carcinoma. BMC Gastroenterol. 2022 Dec 1;22(1). [CrossRef]
- Chen L, Sun T, Kan X, Chen S, Ren Y, Cao Y, et al. Transarterial chemoembolization combined with iodine-125 seed implantation for patients with hepatocellular carcinoma: a retrospective controlled study. Journal of International Medical Research. 2020;48(10). [CrossRef]
- Lin LW, Yan LY, Ke K, Yang WZ, Lin JQ, Huang N. Efficacy and safety of transarterial chemoembolization combined with lenvatinib, programmed death-1 inhibitor, and iodine-125 seed brachytherapy for hepatocellular carcinoma with portal vein tumor thrombosis. Brachytherapy. 2023 Nov 1;22(6):858–71. [CrossRef]
- Li CX, He X, Hu BS, Li Y, Shao PJ, Yu XY, et al. Efficacy of therapy for hepatocellular carcinoma with portal vein tumor thrombus: Chemoembolization and stent combined with iodine-125 seed. Cancer Biol Ther. 2011 Nov 15;12(10):865–71.
- Huang M, Lin Q, Wang H, Chen J, Bai M, Wang L, et al. Survival benefit of chemoembolization plus Iodine125 seed implantation in unresectable hepatitis B-related hepatocellular carcinoma with PVTT: a retrospective matched cohort study. Eur Radiol. 2016 Oct 1;26(10):3428–36. [CrossRef]
- Huang J, Cai M, Huang W, Guo Y, Zhou J, Liang L, et al. Transarterial chemoembolization combined with sorafenib and iodine-125 seed brachytherapy for hepatocellular carcinoma with portal vein tumor thrombus: a retrospective controlled study. Vol. 135, Chinese Medical Journal. Lippincott Williams and Wilkins; 2022. p. 113–5. [CrossRef]
- Li M, He J, Pan M, Yu Y, Pan Z, Xu B, et al. Iodine-125 implantation plus transarterial chemoembolization for the treatment of hepatocellular carcinoma of 3–5 cm: A propensity score matching study. Digestive and Liver Disease. 2016 Sep 1;48(9):1082–7. [CrossRef]
- Peng S, Yang QX, Zhang T, Lu MJ, Yang G, Liu ZY, et al. Lobaplatin-TACE combined with radioactive 125I seed implantation for treatment of primary hepatocellular carcinoma. Asian Pacific Journal of Cancer Prevention. 2014;15(13):5155–60. [CrossRef]
- Li S, He X, Dang L, Xu F, Fang J, Li F, et al. Efficacy of 125I Versus Non-125I Combined with Transcatheter Arterial Chemoembolization for the Treatment of Unresectable Hepatocellular Carcinoma with Obstructive Jaundice. Vol. 63, Digestive Diseases and Sciences. Springer New York LLC; 2018. p. 321–8. [CrossRef]
- Luo JJ, Zhang ZH, Liu QX, Zhang W, Wang JH, Yan ZP. Endovascular brachytherapy combined with stent placement and TACE for treatment of HCC with main portal vein tumor thrombus. Hepatol Int. 2016 Jan 1;10(1):185–95. [CrossRef]
- Wang W, Wang C, Shen J, Ren B, Yin Y, Yang J, et al. Integrated I-125 Seed Implantation Combined with Transarterial Chemoembolization for Treatment of Hepatocellular Carcinoma with Main Portal Vein Tumor Thrombus. Cardiovasc Intervent Radiol. 2021 Oct 1;44(10):1570–8. [CrossRef]
- Yang Q hui, Zhang W, Liu Q xin, Liu L xiao, Wu L lin, Wang J hua, et al. TACE Combined with Implantation of Irradiation Stent Versus TACE Combine with Bare Stent for HCC Complicated by IVCTT. Cardiovasc Intervent Radiol. 2016 Sep 1;39(9):1280–8.
- Yang M, Fang Z, Yan Z, Luo J, Liu L, Zhang W, et al. Transarterial chemoembolisation (TACE) combined with endovascular implantation of an iodine-125 seed strand for the treatment of hepatocellular carcinoma with portal vein tumour thrombosis versus TACE alone: A two-arm, randomised clinical trial. J Cancer Res Clin Oncol. 2014;140(2):211–9.
- Zhang ZH, Zhang W, Gu JY, Liu QX, Ma JQ, Liu LX, et al. Treatment of Hepatocellular Carcinoma with Tumor Thrombus with the Use of Iodine-125 Seed Strand Implantation and Transarterial Chemoembolization: A Propensity-Score Analysis. Journal of Vascular and Interventional Radiology. 2018 Aug 1;29(8):1085–93. [CrossRef]
- Zhang ZH, Liu QX, Zhang W, Ma JQ, Wang JH, Luo JJ, et al. Combined endovascular brachytherapy, sorafenib, and transarterial chemobolization therapy for hepatocellular carcinoma patients with portal vein tumor thrombus. World J Gastroenterol. 2017;23(43):7735–45. [CrossRef]
- Sun H, Zhang M, Liu R, Liu Y, Hou Y, Wu C. Endovascular implantation of 125I seed combined with transcatheter arterial chemoembolization for unresectable hepatocellular carcinoma. Future Oncology. 2018 May 1;14(12):1165–76. [CrossRef]
- Hong D, Zhou Y, Wan X, Su H, Shao H. Brachytherapy with Iodine-125 seeds for treatment of portal vein-branch tumor thrombus in patients with hepatocellular carcinoma. BMC Cancer. 2021 Dec 1;21(1). [CrossRef]
- Hu HT, Luo JP, Li HL, Yang Guo C, Yao QJ, Geng X, et al. Transarterial chemoembolization combined with computed tomography-guided 125 iodine implantation enhances survival in hepatocellular carcinoma patients with portal vein tumor thrombus [Internet]. 2017. Available from: www.impactjournals.com/oncotarget. [CrossRef]
- Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021 Mar 29;n71.
- McGuinness LA, Higgins JPT. Risk-of-bias VISualization (robvis): An R package and Shiny web app for visualizing risk-of-bias assessments. Res Synth Methods. 2021 Jan 6;12(1):55–61.
- Lencioni R, Llovet J. Modified RECIST (mRECIST) Assessment for Hepatocellular Carcinoma. Semin Liver Dis. 2010 Feb 19;30(01):052–60. doi:10.1055/s-0030-1247132.
- Dhondt E, Lambert B, Hermie L, Huyck L, Vanlangenhove P, Geerts A, et al. 90 Y Radioembolization versus Drug-eluting Bead Chemoembolization for Unresectable Hepatocellular Carcinoma: Results from the TRACE Phase II Randomized Controlled Trial. Radiology. 2022 Jun;303(3):699–710.
- Kudo M, Ueshima K, Ikeda M, Torimura T, Tanabe N, Aikata H, et al. Randomised, multicentre prospective trial of transarterial chemoembolisation (TACE) plus sorafenib as compared with TACE alone in patients with hepatocellular carcinoma: TACTICS trial. Gut. 2020 Aug;69(8):1492–501. [CrossRef]
- Llovet JM, Vogel A, Madoff DC, Finn RS, Ogasawara S, Ren Z, et al. Randomized Phase 3 LEAP-012 Study: Transarterial Chemoembolization With or Without Lenvatinib Plus Pembrolizumab for Intermediate-Stage Hepatocellular Carcinoma Not Amenable to Curative Treatment. Cardiovasc Intervent Radiol. 2022 Apr 4;45(4):405–12. [CrossRef]
- Brown AM, Kassab I, Massani M, Townsend W, Singal AG, Soydal C, et al. <scp>TACE</scp> versus <scp>TARE</scp> for patients with hepatocellular carcinoma: Overall and individual patient level meta analysis. Cancer Med. 2023 Feb 9;12(3):2590–9.
- Liu L, Chen H, Wang M, Zhao Y, Cai G, Qi X, et al. Combination Therapy of Sorafenib and TACE for Unresectable HCC: A Systematic Review and Meta-Analysis. PLoS One. 2014 Mar 20;9(3):e91124. [CrossRef]
- Yang SB, Zhang JH, Fu YF, Wang R. TACE with portal vein radioactive seeds for HCC with portal vein tumor thrombus: a meta-analysis. Minimally Invasive Therapy & Allied Technologies. 2022 Aug 1;31(6):856–64. [CrossRef]
- Kang D, Shim S, Cho J, Lim HK. Systematic Review of Studies Assessing the Health-Related Quality of Life of Hepatocellular Carcinoma Patients from 2009 to 2018. Korean J Radiol. 2020;21(6):633. [CrossRef]
- Oliveri RS, Wetterslev J, Gluud C. Transarterial (chemo)embolisation for unresectable hepatocellular carcinoma. Cochrane Database of Systematic Reviews. 2011 Mar 16. [CrossRef]
- Chen J, Jin Z, Zhong B, Fan W, Zhang W, Luo B, et al. Locoregional therapies for hepatocellular carcinoma: The current status and future perspectives. United European Gastroenterol J. 2024 Mar 19;12(2):226–39. [CrossRef]
- Cerrito L, Annicchiarico BE, Iezzi R, Gasbarrini A, Pompili M, Ponziani FR. Treatment of hepatocellular carcinoma in patients with portal vein tumor thrombosis: Beyond the known frontiers. World J Gastroenterol. 2019 Aug 21;25(31):4360–82. [CrossRef]
- Yang SB, Zhang JH, Fu YF, Wang R. TACE with portal vein radioactive seeds for HCC with portal vein tumor thrombus: a meta-analysis. Minimally Invasive Therapy & Allied Technologies. 2022 Aug 1;31(6):856–64. [CrossRef]
- Khan AR, Wei X, Xu X. Portal Vein Tumor Thrombosis and Hepatocellular Carcinoma – The Changing Tides. J Hepatocell Carcinoma. 2021 Sep;Volume 8:1089–115. [CrossRef]
- Abdelhamed W, Shousha H, El-Kassas M. Portal vein tumor thrombosis in hepatocellular carcinoma patients: Is it the end? Liver Res. 2024 Sep;8(3):141–51.
- Wei S, Li C, Li M, Xiong Y, Jiang Y, Sun H, et al. Radioactive Iodine-125 in Tumor Therapy: Advances and Future Directions. Front Oncol. 2021 Sep 30;11. [CrossRef]
- Zhao XH, Yuan H, Xia WL, Zhang LL, Li Z, Cao GS, et al. Prospective study of TACE combined with sorafenib vs TACE combined with 125I seed implantation in the treatment of hepatocellular carcinoma with portal vein tumor thrombus and arterioportal fistulas. Front Oncol. 2022 Oct 5;12. [CrossRef]
- Zhang ZH, Zhang W, Gu JY, Liu QX, Ma JQ, Liu LX, et al. Treatment of Hepatocellular Carcinoma with Tumor Thrombus with the Use of Iodine-125 Seed Strand Implantation and Transarterial Chemoembolization: A Propensity-Score Analysis. Journal of Vascular and Interventional Radiology. 2018 Aug;29(8):1085–93. [CrossRef]
- Lin ZY, Lin J, Lin C, Li YG, Chen SM, Hu JP, et al. 1.5T conventional MR-guided iodine-125 interstitial implants for hepatocellular carcinoma: Feasibility and preliminary clinical experience. Eur J Radiol. 2012 Jul;81(7):1420–5. [CrossRef]
- Zhang ZH, Hou SN, Yu JZ, Zhang W, Ma JQ, Yang MJ, et al. Combined iodine-125 seed strand, portal vein stent, transarterial chemoembolization, lenvatinib and anti-PD-1 antibodies therapy for hepatocellular carcinoma and Vp4 portal vein tumor thrombus: A propensity-score analysis. Front Oncol. 2023 Jan 19;12. [CrossRef]
- Zhu ZX, Wang XX, Yuan KF, Huang JW, Zeng Y. Transarterial chemoembolization plus iodine-125 implantation for hepatocellular carcinoma: a systematic review and meta-analysis. HPB [Internet]. 2018;20(9):795–802. Available from: https://www.embase.com/search/results?subaction=viewrecord&id=L2000768368&from=export.
- Li S, Guo JH, Lu J, Wang C, Wu H, Wang H, et al. I125 irradiation stent for treatment of hepatocellular carcinoma with portal vein thrombosis: A meta-analysis. Cancer/Radiotherapie [Internet]. 2021;25(4):340–9. Available from: https://www.embase.com/search/results?subaction=viewrecord&id=L2010697123&from=export. [CrossRef]
- Qiu Z, Yu C, Qiu X, Li Q, Li J, Chen Z, et al. Safety and Efficacy of CT-Guided Iodine-125 Brachytherapy for Portal Vein Tumor Thrombus in Hepatocellular Carcinoma. Acad Radiol. 2023 Sep;30:S53–60. [CrossRef]
- Hong D, Zhou Y, Wan X, Su H, Shao H. Brachytherapy with Iodine-125 seeds for treatment of portal vein-branch tumor thrombus in patients with hepatocellular carcinoma. BMC Cancer. 2021 Dec 14;21(1):1020. [CrossRef]

| Author & Year | Patients (N) | Gender (M\F) | Age (Mean ±SD, years) | Tumor size (cm) | No. of tumors | Child-Pugh Class (A/B/C) |
Etiology (Hep B\Hep C\Other) |
I-125 dose (Gy) | TACE treatment drug & dose | |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Huang 2022 (6) | |||||||||
| Control | 97 | 86\11 | 51 ± 12.0 |
7.5 ± 2.4 |
1\≥2:34\63 | 70\27\0 | 84\8\5 | Sorafenib (400 mg) | ||
| Intervention | 74 | 68\6 | 49 ± 12.5 | 6.8 ± 2.0 | 1\≥2:23\51 | 56\18\0 | 65\5\4 | NR | AA | |
| 2 | Gao 2022 (1) | |||||||||
| Control | 32 | 26\6 | 62.1±13.3 | 5.8±2.7 | 1\≥2:19\12 | 25\7\0 | 31\0\1 | 5-fuorouracil (150 mg), mitomycin C (10 mg), epirubicin (50 mg) |
||
| Intervention | 32 | 26\6 | 62.7±11.8 | 5.5±1.9 | 1\≥2:25\7 | 26\6\0 | 22\0\10 | 100–140 | AA | |
| 3 | Chen 2020 (2) | |||||||||
| Control | 48 | 38\10 | 59.6 ± 10.1 | <3\≥3:13\35 | 1\≥2:24\24 | 35\13\0 | 27\0\21 | doxorubicin (10 - 20 mg) | ||
| Intervention | 35 | 26\9 | 58.1 ± 10.1 | <3\≥3:14\21 | 1\≥2:16\19 | 24\11\0 | 18\0\17 | 90–165 | AA | |
| 4 | Luo 2016 (10) | |||||||||
| Control | 94 | 82\12 | 55.1 ± 11.1 | >5\-<5:61\33 | NA | 86\8\0 | 74/10/10 | epirubicin (10–50 mg) | ||
| Intervention | 182 | 167\15 | 53.6 ±10.2 | >5\-<5:123\59 | NA | 160\22\0 | 154/16/12 | 37–180.7 | AA | |
| 5 | Peng 2014 (8) | |||||||||
| Control | 43 | 39\4 | ≥50\<50:21\22 | NA | 1-3\>3:26\17 | 38\5\0 | 31\1\11 | lobaplatin (10 - 50 mg) | ||
| Intervention | 32 | 31\1 | ≥50\<50:17\15 | NA | 1-3\>3:15\17 | 27\5\0 | 23\0\9 | 120 | AA | |
| 6 | Wang 2021 (11) | |||||||||
| Control | 25 | 23\2 | <50\≥50 : 12\13 | <5\≥5:5\20 | NA | 19\6\0 | 19\0\6 | pirarubicin (20–40 mg) | ||
| Intervention | 21 | 18\3 | <50\≥50 :11\10 | <5\≥ 5:6\15 | NA | 15\6\0 | 18\0\3 | 100 | AA | |
| 7 | Sun 2018 (16) | |||||||||
| Control | 70 | 58\12 | 55\≥55 :39\31 | 5\>5:15\55 | NA | 31\39\0 | 60\4\6 | piarubicin (30–40 mg),floxuridine (750–1000 mg) , mitomycin (10 mg). | ||
| Intervention | 64 | 45\19 | 55\≥55 : 30\34 | 5\>5:18\46 | NA | 25\39\0 | 49\6\9 | 100-120 | AA |
|
| 8 | Li 2018 (9) | |||||||||
| Control | 33 | 25\8 | 54.64 ± 11.58 | 4.763 ± 1.501 | NA | 7\26\0 | 22\4\7 | doxorubicin (20–40 mg ) | ||
| Intervention | 21 | 17\4 | 56.14 ± 9.82 | 4.809 ± 1.571 | NA | 4\17\0 | 14\3\4 | NR | AA | |
| 9 | Chuan-Xing 2011 (4) | |||||||||
| Control | 30 | 7\23 | 51 ± 2.3 | NA | NA | 17\13\0 | 21\0\9 | oxaliplatin (135 mg), epirubicin (30–40 mg) | ||
| Intervention | 26 | 9\17 | 48 ± 1.6 | NA | NA | 13\11\0 | 23\0\3 | > 40 | AA | |
| 10 | Yang 2014 (13) | |||||||||
| Control | 42 | 39\3 | ≥50\<50: 23\19 | ≥5\<5:29\13 | NA | 23\19\0 | 40\1\1 | Sorafenib (50–75 mg) | ||
| Intervention | 43 | 39\4 | ≥50\<50: 25\18 | ≥5\<5:28\15 | NA | 24\19\0 | 40\2\1 | NR | AA | |
| 11 | Hu 2017 (18) | |||||||||
| Control | 50 | 40\10 | 45.4±5.2 | >5\≤5: 31\19 | NA | 44\6\0 | 40\8\2 | doxorubicin (20–40 mg) | ||
| Intervention | 50 | 42\8 | 47.6±6.3 | >5\≤5: 30\20 | NA | 42\8\0 | 42\7\1 | NR | AA | |
| 12 | Zhang 2018 (14) | |||||||||
| Control | 56 | 48\8 | ≥ 55\< 55: 34\22 | ≥ 10\< 10: 17\39 | NA | 54\2\0 | 56\0\0 | Epirubcin (10–50 mg) | ||
| Intervention | 20 | 19\1 | ≥ 55\< 55: 11\9 | ≥ 10\< 10: 5\15 | NA | 18\2\0 | 20\0\0 | 58.3–64.0 | AA | |
| 13 | Hong 2021 (17) | |||||||||
| Control | 35 | 25\10 | 54.5 ± 8.4 | 8.7 ± 2.5 | Single\multiple: 20\14 | 32\3\0 | 33\1\1 | Epirubicin (40 mg) | ||
| Intervention | 34 | 29\5 | 58.1 ± 7.3 | 7.6 ± 3.0 | Single\multiple: 17\18 | 33\1\0 | 31\2\1 | 120 | AA | |
| 14 | Yang 2016 (12) | |||||||||
| Control | 28 | 25\3 | 50.86 ± 12.116 | ≥ 10\< 10: 13\15 | NA | 20\8\0 | 21\2\5 | Epirubicin (10–50 mg) | ||
| Intervention | 33 | 27\6 | 53.30 ± 8.640 | ≥ 10\< 10: 13\20 | NA | 22\11\0 | 22\2\9 | 60.6–76.6 | AA | |
| 15 | Zhang 2017 (15) | |||||||||
| Control | 31 | 26\5 | ≥ 55\< 55: 14\17 | ≥ 5\< 5: 19\12 | NA | 24\7\0 | 29\0\2 | Epirubicin (10–50 mg) | ||
| Intervention | 37 | 34\3 | ≥ 55\< 55: 18\19 | ≥ 5\ < 5: 26\11 | NA | 33\4\0 | 35\0\2 | 57.4-65.3 | AA | |
| 16 | Huang 2016 (5) | |||||||||
| Control | 140 | 127\13 | 51.6 ± 10.8 | <7\≥7: 83\57 | <3/≥3: 70/70 | 68\72\0 | 140\0\0 | doxorubicin (20–60 mg), lobaplatin (50 mg) | ||
| Intervention | 70 | 63\7 | 51.1 ± 11.1 | <7\≥7: 39\31 | <3/≥3: 30/40 | 31\39\0 | 70\0\0 | 120 | AA | |
| 17 | Li 2016 (7) | |||||||||
| Control | 78 | 67\11 | 48.1 ± 10.0 | 4.00 ± 0.55 | 1\2\3-4: 26\39\13 | 63\15\0 | 60\0\18 | Pirarubicin (20 mg) and cisplatin (50 mg) | ||
| Intervention | 66 | 56\10 | 48.8 ± 10.7 | 3.97 ± 0.58 | 1\2\3-4: 21\33\12 | 58\8\0 | 62\0\4 | 90–165 | AA | |
| 18 | Lin 2023 (3) | |||||||||
| Control | 45 | 42\3 | 57.0 ± 6.4 | 9.0 ±3.7 | ≤33/>3: 3/42 | (5-7)/(7-9): 28/17 | 42\0\3 | Lenvatinib (4-12 mg PO) and camrelizumab (200 mg IV) | ||
| Intervention | 55 | 48\7 | 54.2 ± 11.7 | 8.6 ±3.6 | ≤33/>3: 5/50 | (5-7)/(7-9): 33/32 | 50\0\5 | 110-140 | AA | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).



