Submitted:
11 September 2025
Posted:
12 September 2025
You are already at the latest version
Abstract
Hemp-derived cannabinoids (CBDs) such as Δ8- and Δ10-tetrahydrocannabinol (THC) in cannabis e-cigarettes have been growing in popularity among youth, causing a great concern for their health effects. Previous novel lung injury outbreaks, namely E-cigarette or Vaping Use-Associated Lung Injury (EVALI), were associated with the rising use of e-cigarettes and vaping products. Toxicological studies have revealed that chronic exposure to cannabis vapor can cause adverse brain and pulmonary effects. Federal regulatory policies like the United States 2018 Farm Bill classify hemp as cannabis and set a limit of no more than 0.3% Δ9-THC, while products containing more than 0.3% are defined as ‘marijuana.’ This regulatory loophole has led to the proliferation of hemp-derived intoxicating cannabinoids, such as Δ8- and Δ10-THC, in addition to cannabidiol (CBD), cannabinol (CBN), cannabigerol (CBG) and Δ9-THC appearing in combination products on the market. This phenomenon poses significant health risks to youth because these newer THC isomers and products are currently unregulated and not well-researched, yet they are still widely available. Therefore, we have examined the potential therapeutical uses, toxicity, pharmacology, and possible health risks of several THC and hemp-derived cannabinoids. This review also draws insightful highlights to the public health consequences of secondary exposures to CBD and THC, and their molecular mechanisms of actions. It underscores the urgency for a strict regulatory oversight over unregulated cannabinoid markets to prevent other vaping-related health crises and other rapidly emerging cannabis health disorders, like the cannabinoid hyperemesis syndrome (CHS).
Keywords:
cannabis
; CBD
; THC
; EVALI
; vaping
; lungs
1. Introduction
In recent years, as hemp-derived cannabinoids (CBDs) are legal in most states, cannabis vaping has surged in popularity amongst many young adults and teenagers. Hence, there has been prominent attention surrounding the purity and unlabeled additives in cannabis e-cigarettes (CECs) that can pose a threat to health [1]. In adolescents specifically, the prevalence of lifetime CEC usage has doubled from 6.1% in 2013-2016 to 13.6% in 2019-2020 [2]. The increase in usage has mainly been due to the growing perception of cannabis being less harmful than traditional smoking methods, drawn from extensive reports highlighting the potential therapeutic efficacies for medical purposes [3]. However, CEC causes great concern to medical communities as they have been associated with an inflammatory lung disease, namely, E-cigarette or Vaping Use-Associated Lung Injury (EVALI) [3]. According to the Centers for Disease Control (CDC), as of February 2020, there have been a total of 2,668 hospitalizations and deaths throughout the U.S. associated with e-cigarettes and EVALI [4].
In addition to respiratory issues like EVALI, habitual cannabis usage, especially through unregulated and high-potency cannabis products, have been associated with the cannabinoid hyperemesis syndrome (CHS) [5]. The symptoms of CHS, often characterized by episodes of abdominal pain, nausea, and vomiting can easily be overlooked [6], due to overlapping symptoms with other common diseases. In one report, an increase of 134-175% was expected for annual prevalence rates of CHS [7]. The rise of this syndrome is also suspected to be closely linked with the proliferation of cannabis products amongst young adults, and the rapid emergence of newer unregulated THC products, synthetic cannabinoids, and newer THC isomers [8], amid regulatory gaps. The lack of regulation and oversight for newer products may contribute to increased risk to public health. Even worse, although current systematic literature and empirical studies show some promising treatments for CHS [9], current scientific evidence for pharmacologic treatment is still limited, underscoring the importance of awareness and health risks associated with cannabinoid consumption, and the need for more clinical trials to define optimal treatment to address this emerging public health concern.
Generally, CECs contain three primary chemical constituents, including tetrahydrocannabinol (THC), medium-chain triglycerides (MCT), and vitamin E acetate [10]. Although many recent studies have identified vitamin E acetate as the primary potential causative agent in CECs linked to lung injuries like EVALI, other unlabeled aerosol components and direct effects of aerosolized THC cannot be unnoticed. CECs can be tainted with vitamin E acetate, but there have also been reports before 2019 suggesting that many lung injuries continue to stem from cannabis inhalation, indicating that other unlabeled cannabis components or additives may be responsible [3]. Many CECs associated with the EVALI have also been found to contain unnatural cannabinoid distributions and synthetic forms of vitamin E acetate, often added to tetrahydrocannabinol (THC) containing e-liquids [1].
In other studies involving in vitro mouse cells, when examining the effect of vitamin E acetate, MCT, and CBD/counterfeit vape cartilages on cytotoxicity and inflammatory responses, it was observed that increasing exposure to these constituents elicits a differential inflammatory response on both the epithelial cells and monocytes [10]. Specifically, it was found that infiltration of neutrophils and lymphocytes correlates with increased levels of exotoxin, interleukin-6 (IL-6), and granulocyte colony-stimulating factor (G-CSF) in the bronchoalveolar lavage fluid (BALF), which are all well-known inflammatory markers implicated in lung inflammation. Notably, exposing cells to CBD or counterfeit vape aerosols had a more toxic effect than exposure to vitamin E acetate and MCT [10]. These findings highlight how THC vaping products can pose serious health risks, which can be further exacerbated by regulatory loopholes and inaccurate commercial labeling.
Current federal regulations surrounding the US 2018 Farm Act Bill contain some loopholes, theoretically allowing vaping manufacturers to sell hemp-derived cannabinoids other than Δ9-THC and for the capitalization and marketing of Δ8-THC products [3]. In fact, as of May 2023, recent data show that some of the most common product type across retail websites are composed of 43% disposable vapes, 29% edibles, 18% cartridges, 7 pre-rolls, 2% flower, 1% dabs, and <1% vape pods (101). In addition, recent data also identified 26 toxic compounds in the products, with Δ8-THC, Δ9-THC, Δ10-THC, Δ11-THC, HHC, and others being the most common (101). Worse yet, in another study analyzing 27 products from 10 brands using NMR, GC-MS, ICP-MS, none were found to have accurate labeling, with 11 products containing unlabeled cutting agents [1]. Side products of these cannabis vapes also include heavy metals, olivetol, Δ4-iso-tetrahydrocannabinol, and 9-ethoxyhexahydrocannabional [1]. Many cannabis vape users, particularly young adults, may be at potential risk for adverse health effects from inhaling high quantities of unknown additives [11,12]. As the cannabinoid market continues to expand, there will be even more synthetic cannabinoids beyond the commonly known Δ8-THC (50). Other unknown compounds, such as THC-O-acetate can also be a potential public health threat as it is linked to pulmonary toxicity (50). This underscores the urgent need for further research on unlabeled additives and stricter regulatory oversight of unregulated vaping manufacturers to prevent another vaping-related health crises.
CBD and THC are the two major classes of cannabinoids isolated from cannabis plants, differing in their psychoactive effects and receptor interactions [3]. Currently, there are over 100 phytocannabinoids and over 500 chemical compounds derived from cannabis plants [13]. Presently, CBD and Δ9-THC are the most researched phytocannabinoids [14]. The endocannabinoid system, critical for homeostasis and neuroplasticity, consists of two main receptors: cannabinoid 1 receptor (CB1) and cannabinoid 2 receptor (CB2), which are primarily responsible for the physiological and psychoactive effects of cannabis [15]. CB1 is located on multiple neurons in the central nervous system. At the same time, CB2 is primarily found in glial cells and enteric nervous systems, and CB1 typically shows a higher expression than CB2 in human lungs [3,4,5,6,7,8,9,10,11,12,13,14,15]. THC produces more psychotomimetic effects by activating CB1 and can have other immunologic effects by activating CB2 [15]. In addition, the administration of Δ9-THC is most potent compared to other forms of THC like Δ8- and 10- THC, producing the feeling of ‘high,’ perceptual alterations, delusions, cognitive memory deficits, and verbal complications at higher doses [13,15].
On the other hand, CBD is often well tolerated, with only a few to no psychoactive effects, as it acts as an antagonist with low affinity at CB1 and CB2 cannabinoid receptors but is readily capable of antagonizing them in the presence of THC (103). CBD is non-intoxicating while having antipsychotic effects influencing many physiological processes [15]. Indeed, recent reports have noted that CBD may have potential clinical benefits for alleviating anxiety and movement disorders, cancers, epilepsy, and neuropathic pain [13,16].
However, recent studies have also examined that when CBD and THC are combined in pharmaceutical preparations or clinical uses in a 1:1 ratio, CBD acts as an antagonist to psychoactive outcomes and counteracts adverse effects from high doses of THC without interfering with relaxation effects [13,17]. There have also been contradictory studies arising from differences in dose ratios, analyses, and administration methods leading to several discrepancies [18]. Nonetheless, research shows that CBD decreases the psychotomimetic effects of cannabis by lowering the THC effects [15]. Despite potential therapeutic applications, loopholes in current federal regulations cannot be unseen.
As discussed earlier, current federal regulations that are highly tolerant of hemp-derived products have led to rapid growth in the usage of Δ8-THC and other newer THC isomers, available to customers through online sources. Other novel cannabis vaporizer ingredients, such as Δ10-THC, hexahydrocannabinol, which emerged on the market known as “legal highs,” continue to be a rising concern for medical communities as their toxicology and pharmacology have not been fully researched [19]. In this review, we analyzed hemp-derived cannabinoids and different types of tetrahydrocannabinol, as well as their toxicology and potential health benefits and risks. This review also aims to highlight the public health consequences of secondary exposures to CBD and THC while discussing the urgency to close the current loophole in federal regulations.
2. Methods
A comprehensive literature review was conducted through freely accessible papers published across PubMed and Google Scholar from 2014 to 2025 through a combination of the following key terms: “cannabis,” “cannabidiol,” “tetrahydrocannabinol,” “hemp,” “toxicity,” “delta 8-THC,” “delta 9-THC,” “delta 10-THC,” “cannabis hyperemesis syndrome,” “inflammation,” “THC isomers,” “THC pharmacology,” “secondary exposure,” “NF-kappaB,” and “biotoxicity.” Inclusion criteria comprised peer-reviewed articles, federal regulatory documents, and empirical studies relevant to cannabinoid toxicology and regulation. Due to the lack of attention to regulatory loopholes in recent years, there are limited regulatory publications regarding this focus, and hence selected cited literature and federal regulatory documents published prior to 2014 were also included. Each abstract, methods, and discussion were screened for relevance, followed by a full-text review. The literature search was then used to compile evidence surrounding reports on toxicants in E-cigarettes; toxicology and chemistry of different cannabinoids; pharmacology gaps THC isomers; present loopholes in cannabinoid FDA frameworks; harmful and beneficial effects of CBD/THC; cannabinoid hyperemesis syndrome’s link to THC use and its underlying biological mechanism; biomarkers of CBD/THC toxicity; current public health concern on CBD/THC use and secondary exposures; further regulatory recommendations; and present policies surrounding cannabis and cannabis research.
3. Toxicants in E-Cigarettes Containing THCs
While it is well known that cannabinoids in e-cigarettes pose potential health risks, counterfeit CECs, which consist of electronic parts that are often unlawfully replicated or altered from original manufacturers, can also especially cause great harm due to the presence of various unknown chemical toxicants. In one study, apart from vitamin E acetate being well-known as the primary causative agent in CECs linked in lung injuries, other potential toxicants were also found, such as metals, pesticides/plasticizers, solvent-derived hydrocarbons, silicon-linked compounds, and other terpenes in counterfeit cartridges [20]. Interestingly, these toxicants are primarily found in counterfeit cartridges because cutting agents such as seized drugs like butane hash oil, and legal substances like MCT oil, and vitamin E acetate are used for production. All these chemicals induce oxidative stress and several lung inflammatory responses [45]. Several solvents, such as n-butane and dimethoxyethane, have been present in both the liquid and vapor phases of counterfeit CECs [20]. The butane derivative is likely due to cartridge production’s “dabbing” extraction process. Case reports have revealed that when butane hash oil is heated at high temperatures, harmful derivatives and byproducts like methacrolein and benzene are produced, which are also pulmonary irritants and carcinogens [92].
Other compounds, such as undecane and decane hydrocarbons commonly found in CECs, can lead to respiratory tract irritations and central nervous system depression. If hydrocarbons are aspirated into the lungs, chemical pneumonitis may also be induced, causing lesions and destruction to alveolar and capillary membranes [20]. Significant levels of silica and tetramethyl silicates were also found in counterfeit cartridges. When inhaled at elevated levels, silicon compounds can cause acute lung damage, including pulmonary edema and lesions, through the formation of highly toxic secondary products from silicon dioxide and methanol [20]. Additional compounds found in e-cigarette counterfeit cartridges, including isoprene, toluene, acrolein, benzene, acetaldehyde, and ethylbenzene, are identified as harmful constituents by the FDA [20]. These chemical constituents, when inhaled, can react to form peroxides and self-polymerize upon exposure to oxygen, which can further catalyze the formation of other secondary harmful byproducts. Collectively, the presence of these harmful constituents in counterfeit CEC cartridges can emphasize their strong toxic role in severe respiratory injuries and chemical-induced pneumonitis, as evidenced in cases of EVALI.
3.1. Toxicology and Chemistry of Different Cannabinoid Structures
Δ8-, 9-, and 10- are three positional isomers that interact with the endocannabinoid system in humans, leading to psychoactive effects [22]. However, they vary in potency and toxicological effects. Δ8-THC has its double bond at the 8th carbon. This structural change reduces the potency and is associated with effects such as dizziness, confusion, sedation, and anxiety [21,22]. Animal studies have also brought up more toxicological concerns. For example, when Δ8-THC was administered to rats, there were dose-dependent reductions in body weight and relative organ weights such as the epididymis, heart, liver, lung, and spleen [23]. These findings may prove that exposure to high doses of Δ8-THC may interfere with metabolic processes and/or organ functions [23].
Unlike Δ8-THC, Δ9-THC is biosynthetically produced and is identified as the main potent psychoactive component of cannabis sativa plant [94]. Although the toxicity of Δ9-THC can generally cause side effects such as dizziness and cognitive impairments, serious adverse events are claimed to be typically rare and reversible [99]. In one recent study, it was found that Δ9-THC can significantly alter a brain’s dopamine level by stimulation of mesolimbic dopamine neurons. In turn, this can lead to elevated striatal dopamine, linked to neurological interference and addictive potential [94]. Other preclinical studies have also shown that exposure to (−)-Δ9-THC during pregnancy can also lead to fetal toxicity and potential neurodevelopmental deficits [95]. Similarly observed, other studies have found that when both prenatal maternal immune activation and Δ9-THC exposure co-occur, it can potentially lead to long lasting neuroanatomical and behavioral changes in adulthood [96]. Specifically, in Guma et al.’s study, when researchers performed behavioral tests and utilized longitudinal MRI to observe discrepancies in mice brain after exposure to THC, maternal immune activation, or both, it was found that densities of CB1 and CB2 receptors have decreased significantly [96], which can lead to risks of altered neuroanatomical developments. Even worse, other studies in mice show that even just a single dose of THC administered during a critical brain development period can decrease transcription levels in the parietal cortex and hippocampus, providing evidence that exposure to THC during a sensitive period of brain development can not only disrupt neurotropic signaling, but also increase oxidative stress and even apoptosis [97]. On the other hand, previous research has shown that exposure to Δ9-THC can change immune response in blood cells, yet the mechanisms underlying the changes in gene expression remains limited [98]. All taken together, these literatures suggest that Δ9-THC exposure can pose significant neurodevelopmental and immunological risks, especially during critical developmental periods of the brain.
Unlike Δ8- and Δ9-THC, there is very limited research on the toxicology of Δ10-THC, including its isomers (trans- and cis- Δ10-THC) [32]. Δ10-THC isomers are primarily created synthetically or semi-synthetically via isomerization from hemp-derived CBD [32]. At present, most information about Δ10-THC is derived from its structural similarity to Δ8- and Δ9-THC, such as, having relatively low toxicity [25]. Recent studies, however, suggest that Δ10-THC is generally less potent at CB1 receptors [32], likely producing milder psychoactive effects. Recent effects reported from cases related to Δ10-THC include mild nervous system depression, agitation, and more [100].
While all Δ8-, 9-, and 10- share a foundation as positional isomers, their toxicology and effects differ due to structural variations and potency. Δ9-THC remains the most potent isomer with documented therapeutic benefits. Δ8- and 10- may exhibit lower potency and toxicity, but Δ8- can raise metabolic concerns at higher doses [24,25].

Table 1.
Chemical analog, molecular formula, characteristics, and structure of Δ8-THC, Δ9-THC, and Δ10-THC.
Table 1.
Chemical analog, molecular formula, characteristics, and structure of Δ8-THC, Δ9-THC, and Δ10-THC.
| THC | Chemical Properties/ Origin | Characteristics | Structure |
|
Δ8- Tetrahydrocannabinol |
Molecular formula: [26] Molecular Weight: 314.5 g/mol [26] While Δ8-THC is naturally present in only trace amounts in cannabis plants, nearly all commercial Δ8-THC is often artificially synthesized from CBD via acid-catalyzed isomerization [24]. |
Δ8-THC is more stable than Δ9-THC due double bond positioning on the 8th carbon, causing lower reactivity [27]. Less binding to CB1 receptors compared to Δ9-, as such causes less psychoactive effects [27]. |
 |
|
Δ9- Tetrahydrocannabinol |
Molecular Formula: [28] Molecular Weight: 314.5 g/mol [28] Naturally abundant and directly isolated from cannabis plants [29]. |
Less stable under light and heat due to double bond being on ninth carbon. Has a higher reactivity with electrophiles and oxidation agents leading to a faster degradation over time. [27] |
 |
|
Δ10- Tetrahydrocannabinol (trans- and cis-) |
Molecular Formula: [30,31] Molecular Weight: 314.5 g/mol [30,31] Δ10-THC isomers are primarily created synthetically or semi-synthetically via isomerization from hemp-derived CBD [32]. |
Potentially similar stability as Δ8-THC Limited data on potency and psychoactive effects |
 cis-Δ-10-THC (S configuration) cis-Δ-10-THC (S configuration) trans-Δ-10-THC (R configuration) trans-Δ-10-THC (R configuration)
|
3.2. Pharmacology of THC Isomers
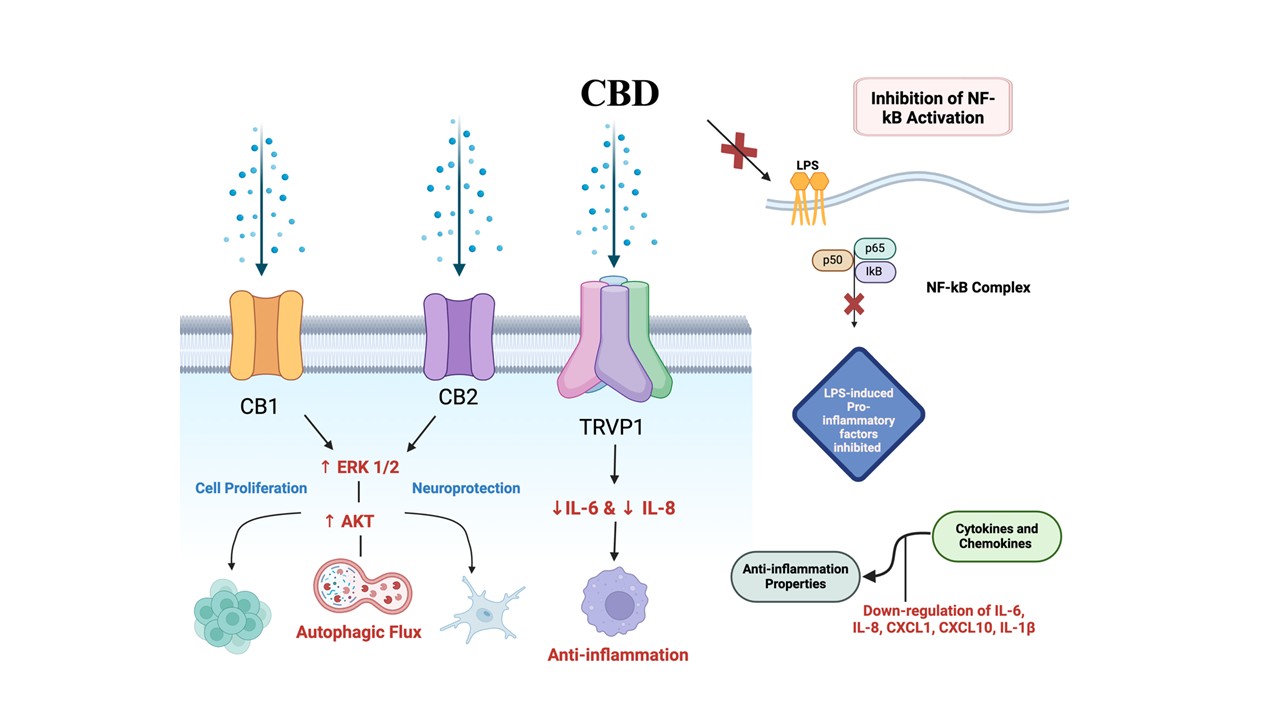
THC can exist in multiple isomeric forms, including Δ9- (the primary psychoactive component), Δ8-, and Δ10-THC. Beyond these, several cis- and trans-stereoisomers also exist, each with a different complex pharmacological property. Recent pharmaco-toxicological studies have highlighted considerable gaps and our limited understanding of different THC isomers, particularly regarding their binding affinity, psychoactivity and potency, toxicity profiles, and metabolism [33]. It is well known that while Δ9-THC serves as a strong CB1 cannabinoid receptor agonist, Δ8-THC and Δ10-THC show a weaker affinity to CB1, accounting for reduced psychoactivity [32]. In fact, studies have highlighted that for emerging Δ10-THC isomers (specifically trans-, cis-, HHC, and others), may even serve as an antagonist for CB1 [32]. Additionally, recent findings indicate that it can also interact with other receptors, including directly or indirectly with the GR alpha (GRα), to override the effect of steroid via CB1/CB2-GRα interaction, thereby rendering steroid ineffective in human macrophages [102] (Figure 1). Furthermore, CBD can differentially regulate basal pro-inflammatory response and attenuate both lipopolysaccharide (LPS)-induced cytokine release and NF-κB activity in monocytes, similar to dexamethasone [102]. However, the full spectrum of receptor binding profiles and functional activities for many isomers, particularly those produced synthetically, remains uncharacterized, unclear, and unstudied in humans.
Notably, one interesting finding regarding Δ9-THC isomers reported in Schafroth et al.’s study highlighted that (−)-Δ9-cis-THC acts as a partial agonist with lower binding affinities to cannabinoid receptors compared to the more prevalent (−)-Δ9-trans-THC. On the other hand, (+)-Δ9-cis-THC enantiomer largely appeared inactive at cannabinoid receptors. However, it showed evidence of selective inhibition of different endocannabinoid-degrading enzymes [34], which can indicate potential pharmacological activities and an inability to produce THC-like effects. This finding may introduce a further nuanced pharmacological profile of (+)-Δ9-cis-THC and its potential scaffold for novel therapeutics targeting the endocannabinoid system beyond the classical receptor-mediated effects if further research is conducted.
Furthermore, there is also a limited understanding of the toxicity and safety profiles of different THC isomers. As discussed in (Table 1), Δ8-THC can be readily derived synthetically from CBD via acid-catalyzed reactions. However, during this chemical process, various reaction conditions, such as temperature changes, reaction duration, type of solvent, and atmospheric exposure, can affect the overall yield of Δ8-THC and result in a mixture of toxic byproducts [35]. In addition to Δ8-THC, the catalytic process could also generate other non-natural THC isomers including, Δ-7 THC, Δ10-THC, and Δ-11 THC [35]. Nevertheless, many of these non-natural compounds have not been thoroughly evaluated for their pharmacological or toxicological effects on humans. This raises significant concern about the safety of commercially accessible Δ8-THC products on the market produced via the synthetic route. Hence, the pharmacological uncertainty of THC further underscores the need for a stricter regulatory oversight and toxicological studies on byproducts in Δ8-THC products.
Above all, analytical challenges are a further complication as the metabolites of many isomers are difficult to distinguish through traditional standard laboratory techniques. Because THC isomers have nearly identical structures, traditional laboratory methods such as chromatography and mass spectrometry remain a challenge when accurately quantifying different isomer metabolites since similar isomers tend to overlap in retention times and result in similar mass spectra [91]. However, recent advances in analytical chemistry, such as cyclic ion mobility spectrometry-mass spectrometry (IMS-MS) combined with silver ions, help amplify the subtle structural differences between different isomers by observing unique ways cannabinoids interact with silver ion particles [91]. Despite these advances, growing diversity in cannabinoid isomer structures would likely outpace current testing capabilities. Thus, the need for specific and accurate analytical methods is essential, as synthetic isomers of THC appear on the market.
4. Biological Actions of THC/CBD via Receptor Interaction and NF-κB Pathways
Interestingly, current literature searches show that THC does not significantly affect the NF- κB signaling pathway in BV-2 microglial cells, unlike CBD. However, THC does generally exhibit several anti-inflammatory properties [36]. As previously discussed, THC primarily acts on CB1 and CB2 receptors, which are both G-protein coupled receptors [37]. CB1 is more ubiquitous in cortical areas of the brain involved in motor functions, whereas CB2 is predominantly found in some neurons, and glial cells in the brain, most associated with immune function [38,39]. The binding of ligands to the G-protein domains induces a conformational change for the receptors, initiating different cellular processes. Different molecular dynamic studies have shown that ligand binding to CB1 and CB2 receptors occurs through a lateral insertion from a lipid bilayer [37]. Activation of CB1 is strongly linked to GABAergic and glutamergic cells, suppressing the release of glutamate and gamma-aminobutyric acid (GABA). It has also been discovered that activation of the CB1 receptor increases the activity of potassium and calcium ion channels and inhibition of adenylate cyclase, leading to decreased cyclic adenosine monophosphate (cAMP) levels [37].
On the other hand, CB2 receptor activation inhibits adenylyl cyclase through the Gi/Go subunits, affecting mature and neoteric tissues [37]. Other studies have also shown that CB2 activation can increase pro-inflammatory cytokine levels like IL-6 and IL-8 [40]. All taken together, the release of glutamate and GABA could possibly suggest THC’s potential anti-inflammatory benefits for neuroprotection, mood regulation, and neuroprotection. In addition, excessive activation could also potentially alter immune response and affect cognition and memory. This wide variety of receptor target could account for diverse pharmacological effects across different tissues at present.
CBD, the major non-psychotomimetic phytocannabinoid, shares neuroprotective, anti-oxidative, anti-emetic, and anti-carcinogenic qualities with THC and has been shown to counteract some of THC’s adverse effects, such as sedation and intoxication [41]. Similar to THC, CBD interacts with CB1, CB2, and TRPV1 (Transient Receipt Potential Channel Vanilloid Type 1) receptor antagonists, which plays a role in its anti-inflammatory effects. Similarly, it can interact with other receptors like GRα to override the effect of steroid via CB1/CB2-GRα interaction, thereby rendering steroids ineffective [102]. (Figure 1).
Recent studies discovered that CBD mediates an autophagic flux through ERK1/2 and AKT suppression activation, which is associated with neuroprotection, cell proliferation, and survival [36] (Figure 1). Remarkably, CBD also reduces NF-κB dependent pathways, a central inflammatory regulator, and upregulates STAT3, a transcription factor that induces anti-inflammatory processes [42]. Mechanistically, recent studies suggest that CBD, not THC, inhibits NF-κB regulations by inhibiting IκB degradation, IRAK-1 degradation, and NF-κB p65 phosphorylation [41] (Figure 1). However, CBD and THC reduce the activation of the LPS, STAT1 transcription factor, a significant unit in another proinflammatory activity, IFNβ [41]. Other studies have also further elucidated CBD’s potent anti-inflammatory effects in human microglial cells. In a recent study using HIV-infected human microglial cells, results demonstrated significant anti-inflammatory properties from CBD [42]. Anti-inflammatory properties were mainly due to reducing various cytokines and chemokines, including IL-6, IL-8, CXCL1, CXCL10, and IL-1β in microglial cells [42] (Figure 1). These findings can further highlight potential CBD therapeutic applications involving neuroinflammation.
5. Current Cannabinoid FDA Regulations
As discussed before, current cannabinoid regulations, namely the 2018 Farm Act Bill detailed significant changes in U.S. agricultural and regulatory policies, particularly in hemp production. Once signed into law, the 2018 Farm Bill legalized the general commercial cultivation of hemp by amending the Controlled Substances Act (CSA) to exclude “hemp” from the definition of “marijuana” [43]. This distinction was made by classifying hemp as cannabis (Cannabis sativa L.) and derivatives of cannabis with no more than 0.3% of the psychoactive compound, Δ9-THC. Other cannabis plants or derived products with greater than 0.3% Δ9-THC are defined as “marijuana” under the legislation and continue to be federally illegal. Additionally, the US 2018 Farm Bill removed hemp from being considered a Schedule I substance by removing the phrase “[THC] in hemp” from THC listings in Schedule I [43].
The repercussions of this framework include the expansion of hemp cultivation, which is detailed in Section 10113 of the 2018 Farm Bill. Section 10113 provides a framework for state and tribal authorities to submit their plans for monitoring and regulating hemp production to the US Department of Agriculture (USDA). If a state does not submit a plan or it is not approved, then the USDA will implement its plan [43]. Additionally, the legality of the non-psychoactive cannabidiol (CBD) products was clarified, an issue that many legal experts describe as a highly misinterpreted matter in the cannabis industry. The Bill specifically legalizes any cannabinoid derived from hemp plants, thus classifying any marijuana-derived CBD as an illegal Schedule I substance [44].
Other current federal guidelines remain fragmented, particularly regulations concerning novel cannabinoids like Δ8-THC and Δ10-THC. Inadvertently, the specificity of the legal threshold for a substance to be below 0.3% Δ9-THC has facilitated the rise of novel cannabinoids not explicitly addressed by federal law. Examples of these psychoactive THC isomers currently sold as “legal hemp derivatives” include Δ8-THC, Δ10-THC, THC-O-acetate derivatives, hexahydrocannabinol (HHC), cannabinol (CBN), tetrahydrocannabiphorol (THCP), and tetrahydrocannabivarin (THCV) [45].
This federal “loophole” arises due to the terminology utilized in defining hemp. By specifying a THC threshold, other potentially psychoactive hemp-derived cannabinoids that do not have the chemical structure of THC, like CBN, are inadvertently legalized [46]. Although Δ8-THC and Δ9-THC both naturally occur in cannabis, Δ8- and Δ9- can be synthesized through a series of chemical reactions from CBD, derived from either hemp or marijuana. Despite Δ9-THC levels being federally restricted; the legislation, alongside most state laws, does not provide regulation of hemp-derived THC isomers, like Δ8-THC. Consequently, a regulatory loophole now exists, where a lack of regulation of these THC isomers equates to no federal marketing or safety regulations of such products [47], though state-licensed dispensaries are established. Other hemp-derived THC isomers are misleadingly marketed as “diet weed” or “marijuana light,” leaving a false impression of safety [46].
The health consequences of this inconsistent regulation have already been noted. According to LoParco et al., Δ8-THC is easily accessible online, lower in price compared to Δ9-THC, and is marketed in such a way that appeals more towards children and teenagers. Also, a lack of safety regulations on the production of such substances has resulted in contaminated products and inconsistent effects, as well as calls to emergency services due to accidental Δ9-THC exposure among minors [48]. Already, poison control centers across the US are encountering incidents of adults mistaking Δ8-THC products to be CBD products and minors consuming Δ8-THC gummies believing them to be candy [49].
Another rising concern with the proliferation of novel cannabinoids is the potential for Δ9-THC and other THC isomers as a reaction by-product. A study conducted by the US Cannabis Council found that in a sample of products labeled as Δ8-THC, byproduct Δ9-THC concentrations were, on average, 10 times above the 0.3% limit. A lack of regulation and inaccurate labeling of such products has also revealed invalid certificates of product analysis for byproducts since the techniques utilized failed to distinguish specific isomers like iso-THCBF (isotetrahydrocannabifuran) from Δ8-THC. An additional study commissioned by CBD Oracle corroborated these differences in results, similar to the previously mentioned study, but in a different sample of products marketed with Δ8-THC. In this group, 76% of products contained a Δ9-THC level beyond 0.3%, and most samples failed to report reaction side products, heavy metals, or pesticides [50]. There is a cause for concern for marketing regulation beyond Δ8-THC products as well since other novel cannabinoids like THCP and THC-O-acetate derivatives require more complex reactions for synthesis, potentially resulting in more undisclosed and undiscovered side products [50]. Further, the regulatory loophole has led to the proliferation of hemp-derived intoxicating cannabinoids like Δ8-THC and Δ10-THC and other analogs in their various combinations along with the combinations of CBD/CBN/CBG and Δ9-THC with different flavors in the market.
To address this legal flaw, the Drug Enforcement Administration (DEA) released a statement to clarify that Schedule I controlled substances still include synthetically derived tetrahydrocannabinol. However, there has yet to be evidence of enforcement by the FDA. Also, there is no guarantee that judicial authorities will find Δ8- to be a “synthetically derived tetrahydrocannabinol” since it is already naturally occurring in the cannabis plant in small amounts [51]. More recently, the FDA released warning letters to five companies for misleading packaging of their food products containing Δ8-THC that were introduced into the marketplace in violation of the Federal Food, Drug, and Cosmetic Act [52]. While the federal government’s reaction towards novel cannabinoids has been limited, at least 21 States have blocked the sale of Δ8-, with other states enforcing more restrictive measures against Δ8- products in recent years [51]. Yet, it remains unclear whether existing regulations apply to State-licensed dispensaries with regard to these products.
Federal actions also apply outside of Δ8- products. In 2023, the US Drug Enforcement Agency (DEA) clarified that THC-O acetate derivatives are classified as Schedule I drugs due to their synthetic and non-naturally occurring nature, thus not falling under the definition of hemp-derived [46]. THC-O acetate derivatives are almost three times as potent as traditional THC [53]. Similarly, in April 2024, the US DEA determined that HHC does not naturally occur in the Cannabis sativa L. plant, thus not falling under the definition of hemp. Although earlier studies have indeed reported detecting small amounts of HHC in cannabis using gas chromatography-mass spectrometry, indicating that HHC can occur naturally, typically in trace amounts [54]. Despite this, concentrations found in cannabis are generally too low to be considered for commercial extraction [54]. Hence, nearly all HHC products available on the market are produced synthetically or semi-synthetically. Due to HHC’s predominant synthetic origin, it marks the most recent novel cannabinoid to be excluded from the Bill’s legalization [93]. This exclusion is now officialized by H.R. 8467, the Farm Bill’s extension for the 2025 fiscal year. The US Congress enacted this extension on December 21, 2024, and signed into law in December 2024 [55]. Additionally, this bill intends to redefine the current definition of hemp to be based on the “total tetrahydrocannabinol” concentration as opposed to Δ9-THC [56]. Despite several state attempts at closing the regulatory loophole, the ambiguity in the current framework with novel cannabinoids still poses serious health concerns.
6. Health Effects of CBD/THC
6.1. Harmful Health Effects of CBD/THC
Due to the lack of strict regulatory control over cannabinoids, health risks will continue to emerge. This concern is particularly relevant when the thermal degradation of flavored e-cigarettes can generate oxidants, heavy metals, and volatile organic compounds [57]. Not only has Cannabis e-cigarettes raise great concerns within the medical community through public health and secondary exposure concern as previously discussed, the misuse of THC and CBD can also lead to various complications affecting brain tissue and inducing pulmonary effects [3,58]. Specifically, Chan et al. found that lung sample from EVALI patients exposed to excessive inhalation of THC showed abnormal lipid macrophages and symptoms such as shortness of breath, dyspnea, nausea, chest pain, vomiting, fever, diarrhea, and weight loss [59]. Similarly, studies involving mouse models and in vitro experiments with human cells have demonstrated that cannabinoid vaping products can alter immune response and result in severe lung damage. Specifically, in tissues exposed to higher levels of CBD aerosol inhalation, myeloperoxidase activity and neutrophil elastase levels were significantly elevated compared to regular nicotine aerosol, resulting in more pronounced inflammatory changes and lung injury caused by oxidative stress [60].
CEC and THC can also cause complications affecting biochemical and molecular processes in brain tissue. As discussed previously, CB1 receptors are more readily expressed in the cortical areas of the brain involved in motor functions, while CB2 receptors can be found in some neurons and glial cells in the brain that is most associated with immune function [38,39]. Many past neuroimaging studies also reveal that morphological abnormalities associated with the amount of cannabis exposure. High levels of CB1 receptors are present in the cerebellum, neocortex, and temporal lobe, but they are expressed at lower levels in other brain regions [11]. Within the temporal lobe, studies have shown that elevated CB1 levels coincide with reduced hippocampal size in 14 young adults with a history of heavy CEC use (5.8 joints/day) for over 6 months [11,12]. Other research indicates that individuals dependent on cannabis exhibit significant abnormalities in hippocampal volume, where long-term users are more likely to have a smaller amygdala and hippocampal volume [11]. Nevertheless, numerous findings suggest that when CB1 levels are densely expressed in the temporal lobe, hippocampal volume can be significantly altered, potentially leading to long-term functional memory deficits and brain damage [12]. In addition to volume abnormalities, studies have discovered that frequent cannabis exposure is particularly detrimental to the adolescent brain, where the right hippocampus shows negative correlations with the number of cannabis joints smoked. This finding indicates that lower hippocampal volumes and impaired neural connectivity are associated with greater cannabis use, especially among adolescents (11, 12, 61).
Aside from the previously mentioned concerns, the existing loopholes in federal cannabinoid regulations, along with colorful packaging and flavorful marketing strategies from manufacturers in vaping products and fruity flavors, can serve as a gateway and significantly increase underage consumption [1]. Numerous pre-clinical and epidemiological data have indicated that excessive use of CECs may lead to various addictive behaviors over time. Furthermore, it is linked to higher risks of anxiety, depression, and lung cancer [61]. One study found that exposing juvenile rodents to cannabinoids decreased dopamine reactivity in the brain’s reward region [61,62]. If early exposure to CBD indeed diminishes dopamine levels during adolescence, this likely explains the consistent pattern of heightened vulnerability to addiction and substance abuse later in life [61].
Table 2.
Different forms of THC and their associated health effects.
| Form of THC | Common Health Effects |
| Δ8-THC |
|
| Δ9-THC | |
| Δ10-THC |
6.2. Beneficial Health Effects of CBD/THC
Despite the toxicity and harmful concerns, the therapeutic potential, when used appropriately under medical supervision, is also notable. In addition to the various health effects of different forms of THC, as shown in Table 2, the beneficial effects of CBD and THC can also depend on dosage, often resulting in different biological outcomes. Currently, although only Δ9-THC and CBD are well-studied forms of cannabinoids—responsible for intoxicated states and a range of therapeutic properties, respectively—cannabis has historically been valued for its pain-relieving, anti-inflammatory, and calming effects [64,65]. Recent literature findings indicate that substantial clinical trial evidence supports the use of high oral doses of CBD, specifically 10-50 mg/kg, for treating childhood epilepsies [64]. In a study assessing the efficacy and tolerability of oral CBD doses through clinical trials, researchers found that the therapeutic benefits of CBD become apparent only when doses are ≥ 300 mg [64]. Furthermore, while there appears to be no increase in adverse effects for doses between 60-400 mg/day, evidence suggests that at doses of 300-400 mg/day, reduced anxiety and anti-addiction effects occur in drug-dependent individuals [64].
Other studies have also shown cannabinoids to have significant effects on managing chronic pain, seizures, convulsions, nausea, peripheral neuropathy, inhibiting cell cancer growth, inflammatory bowel disorders, and lowering blood glucose levels [65]. As previously discussed, CBD mitigates some of the adverse psychotropic effects of THC by acting as a negative allosteric modulator against CB1, giving rise to its anti-inflammatory properties like anti-seizures [66]. Other chronically high levels of THC lower the efficiency of parts of the brain that control planning and cognitive tasks [67]. Despite all the potential benefits under medical supervision, when cannabis overuse occurs, the risk of psychotic symptoms can also be readily apparent in later life [65]. At present, the explicit ratio of THC: CBD for medical therapeutic purposes has not yet been identified in the literature search and requires further research.
6.3. Cannabinoid Hyperemesis Syndrome Link to THC
Aside from the previously mentioned concerns and benefits of CBD/THC, the present loopholes in federal cannabinoid regulations, along with colorful and flavorful marketing strategies, can serve as a gateway to increase consumption among young adults significantly. Studies have found that chronic and habitual cannabis usage, especially high-potency cannabis that is THC-rich, has been linked with cannabinoid hyperemesis syndrome (CHS) [5,8]. For example, in one study, an extensive survey conducted of all CHS patients, 89% highlighted that they used 4 grams of THC-predominant cannabis daily on average, with THC concentrations higher than 15% [8]. Hallmarks of CHS are often characterized by continued episodes of severe nausea, cyclic vomiting, and abdominal pain [6]. Because of such overlapping symptoms with other common diseases, CHS can often be overlooked and underdiagnosed [6]. Even worse, hallmarks of CHS are well known to be resistant to standard antiemetics [9]. Hence, patients often exhibit compulsive patterns of bathing and showering for simple symptomatic relief [68]. As cannabis use increases, especially with the current regulatory loopholes, user numbers can possibly rise over time, as well as the number of CHS cases.
Presently, although the complete pathophysiology of CHS has not been fully understood, several literatures have proposed strong links between CHS and different factors, including CB1 and CB2 receptors, TRPV1, and inflammation control via the release of specific pro-inflammatory mediators (e.g., interleukins). One possible mechanism explains that THC can act as a partial agonist and CB1 and CB2 receptors. Specifically, at lower doses of THC, activation of CB1 can suppress nausea and vomiting signals [69], whereas at chronic high levels of THC exposure, CB1 receptors can be downregulated, and THC can accumulate in the cerebral fat tissues, triggering vomiting during the stress of fasting [69,70]. Furthermore, as previously mentioned, CB2 receptors play a great role in inflammation control, and hence, chronic cannabinoid exposure can dysregulate the gut and immune function, further contributing to CHS symptoms [69]. Other genomic studies have identified mutations in the TRPV1 gene amongst patients with CHS, which encodes the capsaicin receptor involved in sensing heat and pain. When TRPV1 is activated by capsaicin, it leads to an emetic response (vomiting) [71].
Interestingly, recent studies have also suggested that certain genetic polymorphisms such as variants in the dopamine D2 receptor (DRD2), cytochrome P450 enzymes (CYP2C9), ATP-binding cassette transporter (ABCA1), and catechol-O-methyltransferase (COMT), have been linked to increased CHS susceptibility [8]. Particularly, mutations in DRD2 genes are a great indication of drug addiction beyond cannabis, also suspectable to chronic pain, psychosis, and anxiety [8]. On the other hand, the enzyme CYP2C9 helps facilitate THC metabolism by converting THC into 11-hydroxy-THC (active metabolite) and then into inactive 11-nor-9-carboxy-THC [71]. However, a mutation that causes hypoactivity of CYP2C9 can have toxic effects due to slowing down the rate of THC metabolism as the rate of catabolism of 11-hydroxy-THC becomes impaired [71]. Finally, other literatures have found that variants in ABCA1 transporter can increase the risk of dementia, abnormal brain protein depositions, and coronary artery diseases [8]. COMT facilitates dopamine breakdown; hence when mutations of COMT are suspected, patients may be linked to poor antidepressant responses, psychosis, anxiety, and addiction [71]. Above all, as previously mentioned, the complete pathophysiology of CHS is limited and not fully understood; further research is needed to define the complete mechanisms underlying CHS, especially if user numbers are expected to increase over the years due to the regulatory loophole.
At present, complete cessation of cannabis use appears to be the most effective treatment for CHS since conventional antiemetics are ineffective in relieving symptoms [72]. Recent literature also suggests various promising treatments for CHS, including capsaicin, haloperidol, benzodiazepines, and olanzapine [9]. As previously discussed with capsaicin’s link to TRPV1, treatments like capsaicin creams are reported to help relieve some patients with CHS [9]. Otherwise, benzodiazepines and haloperidol have been reported effective, as supported by many trials and case reports. For instance, in one case study, four patients with CHS who had been emitted to the emergency department failed all standard therapy for CHS; however, after receiving haloperidol, they all remarkably showed improvement in symptoms and were discharged 8 hours after [68]. The mechanism behind haloperidol draws from its role as an antagonism at D2 receptors in the central nervous system. High concentrations of D2 cause the drug’s antiemetic properties for CHS [68]. Recent animal studies have also highlighted complex interactions between CB1 and dopamine [73], which may explain haloperidol’s antiemetic properties as well. On the other hand, benzodiazepine primarily enhances the action of GABA at the GABA-A receptor, leading to reduction in anxiety, nausea, and vomiting [9]. Likewise, olanzapine, an antipsychotic drug, helps block neurotransmitter receptors such as serotonin and dopamine, leading to antiemetic effects as well [9]. Despite current studies highlighting different promising treatment drugs, the current scientific evidence for pharmacologic treatment is still limited. This underscores the importance of awareness and health risks associated with cannabinoid consumption, and the need for more clinical trials to define optimal treatment.
7. Biomarkers of Toxicity
In addition to the positive and negative health effects of CBD and THC, recent literature also highlights the biomarkers of their toxicity, which may help identify e-cigarette users with respiratory complications. Many findings show that biomarkers of toxicity for CBD/THC include elevated liver enzymes: alanine aminotransferase (ALT) and aspartate aminotransferase (AST), neurological biomarkers, and endocrine markers. In one clinical study conducted by Florian et al., 201 healthy participants were recruited and subjected to a randomized, double-blind, and placebo-controlled trial that investigated the effects of CBD dose (2.5 mg/kg/d twice a day) on endocrine hormones and liver enzymes [104]. After 4 weeks, 8 of 151 participants (5.6%) had liver enzymes of ALT or AST 3 times the upper limit, while 50 placebo participants showed no concerning results. Additionally, increased eosinophil counts were observed in 7 of 8 participants with elevated ALT levels [104]. ALT and AST play a crucial role in detecting liver cell injury, inflammation, and toxicity [105], which suggests that CBD exposure can result in immune-related hepatic responses, further underscoring the need for better CBD regulations.
Other in vitro animal cases also show that CBD-related toxicities include central nervous system inhibition, liver damage, toxic thyroid hormone levels, embryo-fetal mortality, hypotension, developmental toxicity, and alterations to the male reproductive system with higher doses of CBD than normal human pharmacotherapies [104,106]. Other than hepatic abnormalities as previously mentioned, human clinical studies for epilepsy have reported CBD to be associated with symptoms like vomiting, fatigue, and somnolence [106]. Finally, in recent studies using fluorescence microscopy, it was discovered that CBD can significantly increase levels of reactive oxygen species (ROS) and calcium, and decrease bound NADPH fluorescence, suggesting risks for oxidative stress and inhibition of the electron transport chain, respectively [107,108]. All taken together, biomarkers for CBD such as elevation of liver enzymes, eosinophilia, oxidative stress, and mitochondrial dysfunction, reflect on the systemic toxicity, neurotoxicity, and hepatotoxicity associated with CBD exposures.
Moreover, there are also biomarkers of toxicity of cannabis vaping-associated injuries. For instance, one study by McGraw et al. identified a potential noninvasive biomarker for EVALI: plasma phosphatidylethanolamines [74]. In the study, plasma samples with LC-MS/MS revealed over 500 molecular features, demonstrating that phosphatidylethanolamine levels were significantly lower in both EVALI users and e-cigarette users compared to the healthy group [74]. Since phosphatidylethanolamines are classified as a type of plasmalogen in human cells and are the third most abundant phospholipid in pulmonary surfactants, they play a crucial role in homeostasis via maintenance of surfactant equilibrium and reducing surface tension [74,75]. Overall, phosphatidylethanolamines could serve as a viable biomarker for other surfactant-mediated diseases and respiratory environmental exposure, as many specific alterations can be observed in conditions such as ATP-binding cassette transporter A3 deficiency (ABCA3) and pulmonary fibrosis [75].
In addition to phosphatidylethanolamine, various noninvasive systemic biomarkers related to e-cigarette-induced lung injuries, including THC metabolites, oxidative stress markers, lipid mediators, and inflammation indicators, have also been identified in numerous pilot studies [76]. In one study, researchers collected and compared plasma and urine samples from EVALI patients and non-vape users, utilizing Luminex-based assays along with ELISA/EIA biomarkers for analysis. The results demonstrated that EVALI subjects commonly exhibit higher levels of the THC metabolite (11-nor-9-carboxy-Δ9-THC) in their plasma samples compared to non-vape users [76]. Other mediators, such as resolving D1 (EvD1) and prostaglandin E2 (PGE2), were found to be significantly lower in EVALI samples. Elevated levels of 8-hydroxy-2′-deoxyguanosine (8-OHdG) and 8-isoprostane were identified in EVALI urine samples, representing an oxidative DNA damage biomarker and an oxidative stress marker, respectively [76]. Lastly, several pro-inflammatory biomarkers, including GM-CSF, TNF-α, and MIP-1β, showed decreased levels in affected plasma samples, which suggest a dysregulated inflammatory response due to e-cigarette use [76]. Overall, these biomarkers of toxicity can serve as effective indicators for earlier diagnosis of cannabinoid-associated respiratory complications and for guiding clinical intervention and treatments for CBD/THC.
8. Current Public Health Concerns and Secondary Exposures to CBD/THC/Nicotine
Given the toxicity of cannabinoids, cannabis vaping (along with nicotine vaping) can pose a significant public health concern if its prevalence is high. Unfortunately, we are witnessing an increase in cannabis vaping among adults, particularly young adults (ages 18 – 24). For adults overall, the rate of past-30-day cannabis vaping doubled from 1% in 2017 to 2% in 2019 [77]. Among young adults, the increase was even more pronounced (from 1.2% to 3.9%) [77]. Another study analyzing trends among adolescents found a six-fold rise in the prevalence of past-30-day cannabis vaping, increasing from 1.6% in 2013 to 8.4% in 2020 [2]. This significant rise among adolescents and young adults may be attributed to a lower perceived risk and the misconception that cannabis vaping is a safer alternative to other forms of substance use [78]. The relatively recent emergence of cannabis vaping raises serious public health concerns, especially for youth, due to the limited understanding of its long-term health effects on developing lungs, insufficient regulations, and the prevalence of more potent cannabinoid forms in e-liquids. These issues are compounded by the high rates of use among young people. Additionally, cannabis vaping has seen a more considerable increase among males than females, as well as among heterosexuals compared to homosexuals. Meanwhile, there are no significant differences observed among ethnic, educational, and socioeconomic groups [77].
Similar to cannabis smoke, second-hand exposure to cannabis aerosols can also pose a public health risk [79]. Particles are emitted by e-cigarette users at levels comparable to those of traditional cigarette users, suggesting that while cannabis vaping produces fewer particulates than cannabis smoking, it may still adversely affect air quality around the user [80,81]. The decline in air quality can increase the risk of bronchial problems among young adults (the demographic with the highest rate of cannabis vaping), particularly in those who lack awareness of how to avoid such exposures [82]. One recent controlled study involving simulated cannabis vaping aerosols observed that particle emissions from cannabis vape greatly decrease indoor air quality while also exposing pollutants to other non-vape users [83]. Degraded indoor air quality was evident as Tang et al. found that second-hand particle concentrations (PN) ranged from 0.7 x 106 to 13 x 106 per cm3 and mass concentrations ranged from 65 to 1191μg/m3 [83]. These peak levels indicate that emission from cannabis vape exposure can expose non-users to hazardous and high levels of toxicants, especially when emitted concentrations can be comparable to severe air pollution events [83]. Furthermore, second-hand exposure may also worsen existing airway conditions, including asthma [84]. Although there is no direct data regarding cannabinoid content in second-hand cannabis e-cigarette emissions, pharmacokinetic studies on cannabinoid absorption via inhalation indicate an efficiency of 10 to 35% for THC and 31% for CBD [85]. This suggests that the user might not absorb a significant amount of cannabinoids in the aerosol, allowing them to be exhaled as second-hand exposure, potentially exhibiting the toxicities discussed previously. Such second-hand exposure to cannabinoids can also raise public health concerns.
9. Regulatory Policies on Cannabis and Cannabis Research
Cannabis availability has significantly increased over the last two decades, as previously discussed. It is now accessible for medical purposes in most states, and in nearly half of the states, adults are permitted to purchase it for recreational use [86]. The rapid changes in cannabis availability and policy have outpaced our understanding and scientific research of its effects, despite the current literature and studies. Given the swiftly evolving landscape of cannabis, cannabis policy is crucial for guiding informed public health decisions. According to the National Survey on Drug Use and Health, it was reported that in 2022, 15.1% of individuals is currently using cannabis, and young adult (age 18-25) cannabis use rose from 19.47% to 23.03% between 2012 and 2019 [87]. This increase can be attributed to vape packaging, vibrant colors, and flavors designed to attract young adolescents [57]. However, various cannabis and vaping industries have continuously introduced an array of products with very high concentrations of THC [88]. Following an independent consensus study conducted by the National Academies of Sciences, Engineering, and Medicine, the NIH’s comprehensive roadmap for cannabis research report currently outlines the public health consequences of changes in cannabis policy, different regulatory frameworks for research and marketing approaches in other states, and enumerates recommendations for research to be conducted at the federal, state, and tribal levels to better inform policy [89].
Additionally, the roadmap discussed evaluations of various health programs that promote health and social equity, the impacts of the high potency of synthetic cannabinoid products, the therapeutic benefits of cannabis for health, and the interactions with prescription drugs. Other recommendations aim for the development of better tests to detect cannabis impairment, stricter and improved surveillance of cannabis cultivation and product sales, and wider adoption of a standard 5 mg THC unit in research studies [89]. Despite this new roadmap, public awareness and health initiatives focused on prevention are still absolutely necessary to prevent common misconceptions about cannabis vaping being safer than traditional smoking methods.
9.1. Evolving Risks and Urge for Regulatory Oversight on Modern Cannabis Landscape
All taken together, although cannabis has been used since ancient times and traditionally cultivated in natural forms with low concentrations of active compounds like Δ9-THC, the current cannabis market has undergone substantial changes. Modern strains now contain much higher and potentially hazardous levels of THC, which may contribute to adverse health effects such as EVALI and CHS, as previously discussed. Alongside, the diversity of THC isomers and minor compounds has increased, many of which remain poorly understood in terms of pharmacological and toxicological profiles. Moreover, the rise of different synthetic cannabinoids implicates that recreational users are likely subjected to substances that are not naturally present in plants. These synthetic compounds often have greater drug potency and unpredictable effects, and their unregulated status raises further concerns about unknown health risks. This lack of oversight increases the risk that recreational users may encounter substances that are bacteriologically and chemically harmful. Hence, regulatory frameworks must be strictly strengthened and ensure that cannabis products are professionally handled and tested, overall promoting public health, and minimizing harm to users.
9.2. Further Recommendations for Regulatory Sciences
As discussed earlier, there are numerous issues with the current regulatory framework for cannabis vaping, including the lack of regulation of Δ8- and Δ10-THC, as well as inconsistencies in law enforcement across administrations and states. Therefore, robust regulatory updates should be implemented to address the public health concerns associated with these regulatory loopholes, particularly since such issues significantly impact the youth [48].
One way to address the issue is to broaden the scope of regulation beyond Δ9-THC in hemp derivatives. The current 0.3% THC limit for hemp products should instead focus on the concentration of total cannabinoids that exhibit similar effects to Δ9-THC, including Δ8-, Δ9-, Δ10-THC, and others. Furthermore, regulatory agencies must establish a cohesive regulatory framework for the prompt and consistent enforcement of regulations rather than the fragmented approach we are seeing now [51]. Given the rising popularity of cannabis vaping among young people [2,77], educating them about the risks associated with such products is also crucial. This education can be facilitated by regulating the messages presented on product packaging, which has demonstrated some educational effectiveness [90]. Furthermore, additional research on the properties of various cannabinoid forms is needed to provide a stronger scientific foundation and better inform the development of innovative regulatory strategies.
10. Conclusion
The emergence and growing popularity of cannabinoids and tetrahydrocannabinol, including Δ8-, 9-, and 10-THC present significant health risks and public health concerns. While cannabinoids and Δ9-THC do demonstrate some therapeutic medical potential according to medical reports, their widespread availability, especially regarding products like Δ8- and Δ10-THC, remains poorly regulated. Lack of consistent regulation enables misuse and raises significant public health concerns. Due to the existing loopholes in the regulation regarding hemp products, Δ8-THC and other THC forms are readily available through online platforms, where vibrant packaging and appealing marketing strategies target adolescents and young adults. Additionally, counterfeit e-cigarettes introduce a range of toxic substances, including solvent-derived hydrocarbons, silicon-linked chemicals, and vitamin E acetate. These compounds can contribute to oxidative stress and inflammatory responses leading to acute respiratory syndromes like EVALI as suggested by earlier studies. Beyond the toxicological risks, the pharmacological effects of THC and CBD through CB1 and CB2 receptors and NF-κB pathways reveal complex roles in neuroprotection, inflammation, and immune modulation. It has divergent pro- and anti-inflammatory properties based on dose and susceptibility factors. Although some literature suggests that young adults have the highest prevalence of cannabis vaping, this review emphasizes the critical need for regulatory reforms by mandating a more consistent cannabinoid regulation across states, more accurate labeling of cannabinoid content in e-cigarette products on the market, and expanding the scope of limited regulation beyond Δ9-THC. Establishing proactive measures is essential to safeguarding public health and mitigating health risks by reducing the rise of novel cannabinoids and exposure to harmful and unlabeled chemical additives. Public awareness and public health initiatives focusing on prevention are necessary to counteract common misconceptions about cannabis vaping being more ‘safe’ than traditional methods. Ultimately, this review underlines the urgency for further research and tighter regulatory frameworks to mitigate health risks among youth associated with cannabis vaping.
Author Contributions
KL, YS, RR, PS, FE, and IR designed, wrote, and edited the manuscript. IR provided conceptual ideas, layouts, and planning and edited the manuscript.
Institutional Review Board Statement
Not Applicable.
Data Availability Statement
None. All materials are provided in this manuscript.
Conflict of Interest
The authors have no financial disclosure or conflict of interest with the findings presented in this research article
References
- Meehan-Atrash J, Rahman I. Cannabis Vaping: Existing and Emerging Modalities, Chemistry, and Pulmonary Toxicology. Chem Res Toxicol. 2021;34(10):2169-79.
- Lim CCW, Sun T, Leung J, Chung JYC, Gartner C, Connor J, et al. Prevalence of Adolescent Cannabis Vaping: A Systematic Review and Meta-analysis of US and Canadian Studies. JAMA Pediatr. 2022;176(1):42-51.
- Meehan-Atrash J, Rahman I. Novel Δ(8)-Tetrahydrocannabinol Vaporizers Contain Unlabeled Adulterants, Unintended Byproducts of Chemical Synthesis, and Heavy Metals. Chem Res Toxicol. 2022;35(1):73-6.
- Prevention CfDCa. Outbreak of Lung Injury Associated with the Use of E-Cigarette, or Vaping, Products 2020 [updated 2.25.2020. Available from: https://archive.cdc.gov/www_cdc_gov/tobacco/basic_information/e-cigarettes/severe-lung-disease.html.
- Ruberto AJ, Sivilotti MLA, Forrester S, Hall AK, Crawford FM, Day AG. Intravenous Haloperidol Versus Ondansetron for Cannabis Hyperemesis Syndrome (HaVOC): A Randomized, Controlled Trial. Ann Emerg Med. 2021;77(6):613-9.
- Lee C, Greene SL, Wong A. The utility of droperidol in the treatment of cannabinoid hyperemesis syndrome. Clin Toxicol (Phila). 2019;57(9):773-7.
- Costales B, Lu Y, Young-Wolff KC, Cotton DM, Campbell CI, Iturralde E, et al. Prevalence and trends of suspected cannabinoid hyperemesis syndrome over an 11-year period in Northern California: An electronic health record study. Drug Alcohol Depend. 2024;263:112418.
- Russo EB, Whiteley VL. Cannabinoid hyperemesis syndrome: genetic susceptibility to toxic exposure. Front Toxicol. 2024;6:1465728.
- Richards JR, Gordon BK, Danielson AR, Moulin AK. Pharmacologic Treatment of Cannabinoid Hyperemesis Syndrome: A Systematic Review. Pharmacotherapy. 2017;37(6):725-34.
- Muthumalage T, Friedman MR, McGraw MD, Ginsberg G, Friedman AE, Rahman I. Chemical Constituents Involved in E-Cigarette, or Vaping Product Use-Associated Lung Injury (EVALI). Toxics. 2020;8(2).
- Burggren AC, Shirazi A, Ginder N, London ED. Cannabis effects on brain structure, function, and cognition: considerations for medical uses of cannabis and its derivatives. Am J Drug Alcohol Abuse. 2019;45(6):563-79.
- Ashtari M, Avants B, Cyckowski L, Cervellione KL, Roofeh D, Cook P, et al. Medial temporal structures and memory functions in adolescents with heavy cannabis use. J Psychiatr Res. 2011;45(8):1055-66.
- Boggs DL, Nguyen JD, Morgenson D, Taffe MA, Ranganathan M. Clinical and Preclinical Evidence for Functional Interactions of Cannabidiol and Δ(9)-Tetrahydrocannabinol. Neuropsychopharmacology. 2018;43(1):142-54.
- Jurga M, Jurga A, Jurga K, Kaźmierczak B, Kuśmierczyk K, Chabowski M. Cannabis-Based Phytocannabinoids: Overview, Mechanism of Action, Therapeutic Application, Production, and Affecting Environmental Factors. Int J Mol Sci. 2024;25(20).
- Boggs DL, Peckham A, Boggs AA, Ranganathan M. Delta-9-tetrahydrocannabinol and cannabidiol: Separating the chemicals from the “weed,” a pharmacodynamic discussion. Ment Health Clin. 2016;6(6):277-84.
- Nidadavolu P, Bilkei-Gorzo A, Effah F, Leidmaa E, Schürmann B, Berger M, et al. Dynamic Changes in the Endocannabinoid System during the Aging Process: Focus on the Middle-Age Crisis. Int J Mol Sci. 2022;23(18).
- Pennypacker SD, Cunnane K, Cash MC, Romero-Sandoval EA. Potency and Therapeutic THC and CBD Ratios: U.S. Cannabis Markets Overshoot. Front Pharmacol. 2022;13:921493.
- Wall MB, Freeman TP, Hindocha C, Demetriou L, Ertl N, Freeman AM, et al. Individual and combined effects of cannabidiol and Δ(9)-tetrahydrocannabinol on striato-cortical connectivity in the human brain. J Psychopharmacol. 2022;36(6):732-44.
- Graziano S, Varì MR, Pichini S, Busardo FP, Cassano T, Di Trana A. Hexahydrocannabinol Pharmacology, Toxicology, and Analysis: The First Evidence for a Recent New Psychoactive Substance. Curr Neuropharmacol. 2023;21(12):2424-30.
- Muthumalage T, Lucas JH, Wang Q, Lamb T, McGraw MD, Rahman I. Pulmonary Toxicity and Inflammatory Response of E-Cigarette Vape Cartridges Containing Medium-Chain Triglycerides Oil and Vitamin E Acetate: Implications in the Pathogenesis of EVALI. Toxics. 2020;8(3).
- Kruger JS, Kruger DJ. Delta-8-THC: Delta-9-THC’s nicer younger sibling? J Cannabis Res. 2022;4(1):4.
- Leas EC, Harati RM, Satybaldiyeva N, Morales NE, Huffaker SL, Mejorado T, et al. Self-reported adverse events associated with ∆(8)-Tetrahydrocannabinol (Delta-8-THC) Use. J Cannabis Res. 2023;5(1):15.
- Sjödén PO, Järbe TU, Henriksson BG. Influence of tetrahydrocannabinols (delta8-THC and delta9-THC) on body weight, food, and water intake in rats. Pharmacol Biochem Behav. 1973;1(4):395-9.
- Abdel-Kader MS, Radwan MM, Metwaly AM, Eissa IH, Hazekamp A, ElSohly MA. Chemistry and Pharmacology of Delta-8-Tetrahydrocannabinol. Molecules. 2024;29(6).
- Sharma P, Murthy P, Bharath MM. Chemistry, metabolism, and toxicology of cannabis: clinical implications. Iran J Psychiatry. 2012;7(4):149-56.
- PubChem. DELTA8-Tetrahydrocannabinol [Available from: https://pubchem.ncbi.nlm.nih.gov/compound/638026.
- Tagen M, Klumpers LE. Review of delta-8-tetrahydrocannabinol (Δ(8) -THC): Comparative pharmacology with Δ(9) -THC. Br J Pharmacol. 2022;179(15):3915-33.
- PubChem. Dronabinol [Available from: https://pubchem.ncbi.nlm.nih.gov/compound/Dronabinol.
- Reyes-Resina I, Rivas-Santisteban R, Raïch I, del Torrent CL, Lillo J, Franco R, et al. Naturally occurring delta-9-tetrahydrocannabinol derivatives and binding to CB1 and CB2 receptors: Linking in the endocannabinoid system. Neurobiology and Physiology of the Endocannabinoid System: Elsevier; 2023. p. 379-94.
- PubChem. (6AR,9R)-Delta10-thc [Available from: https://pubchem.ncbi.nlm.nih.gov/compound/146639819.
- PubChem. (6AR,9S)-Delta10-thc [Available from: https://pubchem.ncbi.nlm.nih.gov/compound/6AR_9S_-Delta10-thc.
- Haghdoost M, Brumar D, Geiling B, Brunstetter M, Bonn-Miller MO. Chemistry, Crystal Structure, and In Vitro Receptor Binding of Δ10-THC Isomers. Cannabis Cannabinoid Res. 2023;8(S1):S1-s10.
- La Maida N, Di Giorgi A, Pichini S, Busardò FP, Huestis MA. Recent challenges and trends in forensic analysis: Δ9-THC isomers pharmacology, toxicology and analysis. J Pharm Biomed Anal. 2022;220:114987.
- Schafroth MA, Mazzoccanti G, Reynoso-Moreno I, Erni R, Pollastro F, Caprioglio D, et al. Δ(9)-cis-Tetrahydrocannabinol: Natural Occurrence, Chirality, and Pharmacology. J Nat Prod. 2021;84(9):2502-10.
- Geci M, Scialdone M, Tishler J. The Dark Side of Cannabidiol: The Unanticipated Social and Clinical Implications of Synthetic Δ(8)-THC. Cannabis Cannabinoid Res. 2023;8(2):270-82.
- Vrechi TAM, Leão A, Morais IBM, Abílio VC, Zuardi AW, Hallak JEC, et al. Cannabidiol induces autophagy via ERK1/2 activation in neural cells. Sci Rep. 2021;11(1):5434.
- Shahbazi F, Grandi V, Banerjee A, Trant JF. Cannabinoids and Cannabinoid Receptors: The Story so Far. iScience. 2020;23(7):101301.
- Howlett AC, Abood ME. CB(1) and CB(2) Receptor Pharmacology. Adv Pharmacol. 2017;80:169-206.
- Kendall DA, Yudowski GA. Cannabinoid Receptors in the Central Nervous System: Their Signaling and Roles in Disease. Front Cell Neurosci. 2016;10:294.
- Hytti M, Andjelic S, Josifovska N, Piippo N, Korhonen E, Hawlina M, et al. CB(2) receptor activation causes an ERK1/2-dependent inflammatory response in human RPE cells. Sci Rep. 2017;7(1):16169.
- Kozela E, Pietr M, Juknat A, Rimmerman N, Levy R, Vogel Z. Cannabinoids Delta(9)-tetrahydrocannabinol and cannabidiol differentially inhibit the lipopolysaccharide-activated NF-kappaB and interferon-beta/STAT proinflammatory pathways in BV-2 microglial cells. J Biol Chem. 2010;285(3):1616-26.
- Yndart Arias A, Kolishetti N, Vashist A, Madepalli L, Llaguno L, Nair M. Anti-inflammatory effects of CBD in human microglial cell line infected with HIV-1. Sci Rep. 2023;13(1):7376.
- Mattingly, KE. State Regulation of Hemp Cultivation: Using the 2018 Farm Bill to Ease the Regulatory Burden on Farmers. U Louisville L Rev. 2019;58:589.
- Smith, S. Hemp on the horizon: The 2018 Farm Bill and the future of CBD. NCL Rev Addendum. 2019;98:1503.
- Dotson, SJ. Cannabis Regulations Being Evaded by Use of Novel THC Isomers. American Psychiatric Publishing, Inc.; 2022.
- Rossheim ME, LoParco CR, Henry D, Trangenstein PJ, Walters ST. Delta-8, Delta-10, HHC, THC-O, THCP, and THCV: What Should We Call These Products? J Stud Alcohol Drugs. 2023;84(3):357-60.
- Babalonis S, Raup-Konsavage WM, Akpunonu PD, Balla A, Vrana KE. Δ(8)-THC: Legal Status, Widespread Availability, and Safety Concerns. Cannabis Cannabinoid Res. 2021;6(5):362-5.
- LoParco CR, Rossheim ME, Walters ST, Zhou Z, Olsson S, Sussman SY. Delta-8 tetrahydrocannabinol: a scoping review and commentary. Addiction. 2023;118(6):1011-28.
- Leas, EC. The Hemp Loophole: A Need to Clarify the Legality of Delta-8-THC and Other Hemp-Derived Tetrahydrocannabinol Compounds. Am J Public Health. 2021;111(11):1927-31.
- Zawatsky CN, Mills-Huffnagle S, Augusto CM, Vrana KE, Nyland JE. Cannabidiol-Derived Cannabinoids: The Unregulated Designer Drug Market Following the 2018 Farm Bill. Med Cannabis Cannabinoids. 2024;7(1):10-8.
- Flomberg, O. Legal High? The High Stakes Regulatory Questions about Delta-8 THC & Other Emerging Psychoactive Cannabinoids. Wash UJL & Pol’y. 2023;72:195.
- Administration USFD. Warning Letters for Cannabis-Derived Products 2025 [Available from: https://www.fda.gov/news-events/public-health-focus/warning-letters-cannabis-derived-products.
- Holt AK, Poklis JL, Peace MR. ∆8-THC, THC-O Acetates and CBD-di-O Acetate: Emerging Synthetic Cannabinoids Found in Commercially Sold Plant Material and Gummy Edibles. J Anal Toxicol. 2022;46(8):940-8.
- Qureshi MN, Kanwal F, Siddique M, Inayat-ur-Rahman A. Estimation of biologically active cannabinoids in Cannabis indica by gas chromatography-mass spectrometry (GC-MS). World Appl Sci J. 2012;19(7):918-23.
- Monke J, Stubbs M, Aussenberg RA. Expiration of the 2018 Farm Bill and Extension in 2024. Congressional Research Service. 2024;47659.
- Aussenberg RAB, Lisa S.; Bickell, Eleni G.; Billings, Kara Clifford; Biondo, Lia; Bracmort, Kelsi; Gatz, Laura; Gottron, Frank; Greene, Joel L.; Heflin, Jason O.; Johnson, Renée; Mickler, Alexandria K.; Monke, Jim; Riddle, Anne A.; Rosch, Stephanie; Rowan, Linda R.; Stubbs, Megan; Tsui, Benjamin; Whitt, Christine; Yen, Jerry H. The 2024 Farm Bill: H.R. 8467 Compared with Current Law 2024 [Available from: https://www.congress.gov/crs-product/R48167.
- Effah F, Sun Y, Lin K, Rahman I. A comparative toxicological evaluation of emerging nicotine analogs 6-methyl nicotine and nicotinamide: a scoping review. Arch Toxicol. 2025;99(4):1333-40.
- Archie SR, Cucullo L. Harmful Effects of Smoking Cannabis: A Cerebrovascular and Neurological Perspective. Front Pharmacol. 2019;10:1481.
- Chand HS, Muthumalage T, Maziak W, Rahman I. Pulmonary Toxicity and the Pathophysiology of Electronic Cigarette, or Vaping Product, Use Associated Lung Injury. Front Pharmacol. 2019;10:1619.
- Bhat TA, Kalathil SG, Goniewicz ML, Hutson A, Thanavala Y. Not all vaping is the same: differential pulmonary effects of vaping cannabidiol versus nicotine. Thorax. 2023;78(9):922-32.
- Volkow ND, Baler RD, Compton WM, Weiss SR. Adverse health effects of marijuana use. N Engl J Med. 2014;370(23):2219-27.
- Pistis M, Perra S, Pillolla G, Melis M, Muntoni AL, Gessa GL. Adolescent exposure to cannabinoids induces long-lasting changes in the response to drugs of abuse of rat midbrain dopamine neurons. Biol Psychiatry. 2004;56(2):86-94.
- Simon TA, Simon JH, Heaning EG, Gomez-Caminero A, Marcu JP. Delta-8, a Cannabis-Derived Tetrahydrocannabinol Isomer: Evaluating Case Report Data in the Food and Drug Administration Adverse Event Reporting System (FAERS) Database. Drug Healthc Patient Saf. 2023;15:25-38.
- Arnold JC, McCartney D, Suraev A, McGregor IS. The safety and efficacy of low oral doses of cannabidiol: An evaluation of the evidence. Clin Transl Sci. 2023;16(1):10-30.
- Leinen ZJ, Mohan R, Premadasa LS, Acharya A, Mohan M, Byrareddy SN. Therapeutic Potential of Cannabis: A Comprehensive Review of Current and Future Applications. Biomedicines. 2023;11(10).
- Lafaye G, Karila L, Blecha L, Benyamina A. Cannabis, cannabinoids, and health. Dialogues Clin Neurosci. 2017;19(3):309-16.
- Niesink RJ, van Laar MW. Does Cannabidiol Protect Against Adverse Psychological Effects of THC? Front Psychiatry. 2013;4:130.
- Witsil JC, Mycyk MB. Haloperidol, a Novel Treatment for Cannabinoid Hyperemesis Syndrome. Am J Ther. 2017;24(1):e64-e7.
- Perisetti A, Gajendran M, Dasari CS, Bansal P, Aziz M, Inamdar S, et al. Cannabis hyperemesis syndrome: an update on the pathophysiology and management. Ann Gastroenterol. 2020;33(6):571-8.
- Lu ML, Agito MD. Cannabinoid hyperemesis syndrome: Marijuana is both antiemetic and proemetic. Cleve Clin J Med. 2015;82(7):429-34.
- Russo EB, Spooner C, May L, Leslie R, Whiteley VL. Cannabinoid Hyperemesis Syndrome Survey and Genomic Investigation. Cannabis Cannabinoid Res. 2022;7(3):336-44.
- Burillo-Putze G, Richards JR, Rodríguez-Jiménez C, Sanchez-Agüera A. Pharmacological management of cannabinoid hyperemesis syndrome: an update of the clinical literature. Expert Opin Pharmacother. 2022;23(6):693-702.
- Schulze DR, Carroll FI, McMahon LR. Interactions between dopamine transporter and cannabinoid receptor ligands in rhesus monkeys. Psychopharmacology (Berl). 2012;222(3):425-38.
- McGraw MD, Croft DP, Nacca NE, Rahman I. Reduced plasma phosphatidylethanolamines in e-cigarette, or vaping, product use-associated lung injury (EVALI). Pediatr Pulmonol. 2022;57(5):1350-4.
- Rebuli ME, Rose JJ, Noël A, Croft DP, Benowitz NL, Cohen AH, et al. The E-cigarette or Vaping Product Use-Associated Lung Injury Epidemic: Pathogenesis, Management, and Future Directions: An Official American Thoracic Society Workshop Report. Ann Am Thorac Soc. 2023;20(1):1-17.
- Podguski S, Kaur G, Muthumalage T, McGraw MD, Rahman I. Noninvasive systemic biomarkers of e-cigarette or vaping use-associated lung injury: a pilot study. ERJ Open Res. 2022;8(2).
- Boakye E, Obisesan OH, Uddin SMI, El-Shahawy O, Dzaye O, Osei AD, et al. Cannabis vaping among adults in the United States: Prevalence, trends, and association with high-risk behaviors and adverse respiratory conditions. Prev Med. 2021;153:106800.
- Chadi N, Minato C, Stanwick R. Cannabis vaping: Understanding the health risks of a rapidly emerging trend. Paediatr Child Health. 2020;25(Suppl 1):S16-s20.
- Nguyen PK, Hammond SK. Fine Particulate Matter Exposure From Secondhand Cannabis Bong Smoking. JAMA Netw Open. 2022;5(3):e224744.
- Papaefstathiou E, Bezantakos S, Stylianou M, Biskos G, Agapiou A. Comparison of particle size distributions and volatile organic compounds exhaled by e-cigarette and cigarette users. Journal of Aerosol Science. 2020;141:105487.
- Ott WR, Zhao T, Cheng K-C, Wallace LA, Hildemann LM. Measuring indoor fine particle concentrations, emission rates, and decay rates from cannabis use in a residence. Atmospheric Environment: X. 2021;10:100106.
- Islam T, Braymiller J, Eckel SP, Liu F, Tackett AP, Rebuli ME, et al. Secondhand nicotine vaping at home and respiratory symptoms in young adults. Thorax. 2022;77(7):663-8.
- Tang X, Rapp VH, Chen S, Russell ML, Destaillats H. Secondhand Exposure to Simulated Cannabis Vaping Aerosols. Environ Sci Technol. 2025;59(20):10032-43.
- Bayly JE, Bernat D, Porter L, Choi K. Secondhand Exposure to Aerosols From Electronic Nicotine Delivery Systems and Asthma Exacerbations Among Youth With Asthma. Chest. 2019;155(1):88-93.
- Lucas CJ, Galettis P, Schneider J. The pharmacokinetics and the pharmacodynamics of cannabinoids. Br J Clin Pharmacol. 2018;84(11):2477-82.
- Crowley R, Cline K, Hilden D, Beachy M. Regulatory Framework for Cannabis: A Position Paper From the American College of Physicians. Ann Intern Med. 2024;177(8):1104-5.
- Mattingly DT, Richardson MK, Hart JL. Prevalence of and trends in current cannabis use among US youth and adults, 2013-2022. Drug Alcohol Depend Rep. 2024;12:100253.
- Freeman TP, Craft S, Wilson J, Stylianou S, ElSohly M, Di Forti M, et al. Changes in delta-9-tetrahydrocannabinol (THC) and cannabidiol (CBD) concentrations in cannabis over time: systematic review and meta-analysis. Addiction. 2021;116(5):1000-10.
- Volkow, N. National Institute on Drug Abuse. 2025. Available from: https://nida.nih.gov/about-nida/noras-blog/2025/01/new-roadmap-cannabis-cannabis-policy-research.
- Jones D, Morgan A, Moodie C, Alexandrou G, Ford A, Mitchell D. The Role of e-Cigarette Packaging as a Health Communications Tool: A Focus Group Study With Adolescents and Adults in England and Scotland. Nicotine Tob Res. 2025;27(4):705-13.
- Huang S, Righetti L, Claassen FW, Krishna A, Ma M, van Beek TA, et al. Ultrafast, Selective, and Highly Sensitive Nonchromatographic Analysis of Fourteen Cannabinoids in Cannabis Extracts, Δ8-Tetrahydrocannabinol Synthetic Mixtures, and Edibles by Cyclic Ion Mobility Spectrometry–Mass Spectrometry. Analytical Chemistry. 2024;96(25):10170-81.
- Anderson RP, Zechar K. Lung injury from inhaling butane hash oil mimics pneumonia. Respir Med Case Rep. 2019;26:171-3.
- Johnson, R. Hemp Provisions in the House Farm Bill and FY2025 Agriculture Appropriations Bill: Washington (DC): Congressional Research Service; 2024 [Available from: https://www.congress.gov/crs-product/IN12381.
- Chetia S, Borah G. Δ 9-Tetrahydrocannabinol Toxicity and Validation of Cannabidiol on Brain Dopamine Levels: An Assessment on Cannabis Duplicity. Natural Products and Bioprospecting. 2020;10(5):285-96.
- Kumar AR, Benson LS, Wymore EM, Phipers JE, Dempsey JC, Cort LA, et al. Quantification and prediction of human fetal (-)-Δ(9)-tetrahydrocannabinol/(±)-11-OH-Δ(9)-tetrahydrocannabinol exposure during pregnancy to inform fetal cannabis toxicity. Nat Commun. 2025;16(1):824.
- Guma E, Cupo L, Ma W, Gallino D, Moquin L, Gratton A, et al. Investigating the “two-hit hypothesis”: Effects of prenatal maternal immune activation and adolescent cannabis use on neurodevelopment in mice. Prog Neuropsychopharmacol Biol Psychiatry. 2023;120:110642.
- Philippot G, Forsberg E, Tahan C, Viberg H, Fredriksson R. A Single δ(9)-Tetrahydrocannabinol (THC) Dose During Brain Development Affects Markers of Neurotrophy, Oxidative Stress, and Apoptosis. Front Pharmacol. 2019;10:1156.
- Hu Y, Ranganathan M, Shu C, Liang X, Ganesh S, Osafo-Addo A, et al. Single-cell Transcriptome Mapping Identifies Common and Cell-type Specific Genes Affected by Acute Delta9-tetrahydrocannabinol in Humans. Sci Rep. 2020;10(1):3450.
- Černe, K. Toxicological properties of Δ9-tetrahydrocannabinol and cannabidiol. Arh Hig Rada Toksikol. 2020;71(1):1-11.
- Burgess A, Hays HL, Badeti J, Spiller HA, Rine NI, Gaw CE, et al. Delta-8 tetrahydrocannabinol, delta-10 tetrahydrocannabinol, and tetrahydrocannabinol-O acetate exposures reported to America’s Poison Centers. Clin Toxicol (Phila). 2024;62(4):256-66.
- Rossheim ME, Tillett KK, Vasilev V, LoParco CR, Berg CJ, Trangenstein PJ, et al. Types and Brands of Derived Psychoactive Cannabis Products: An Online Retail Assessment, 2023. Cannabis Cannabinoid Res. 2024;9(6):1478-81.
- Muthumalage T, Rahman I. Cannabidiol differentially regulates basal and LPS-induced inflammatory responses in macrophages, lung epithelial cells, and fibroblasts. Toxicol Appl Pharmacol. 2019;382:114713.
- Vučković S, Srebro D, Vujović KS, Vučetić Č, Prostran M. Cannabinoids and Pain: New Insights From Old Molecules. Front Pharmacol. 2018;9:1259.
- Florian J, Salcedo P, Burkhart K, Shah A, Chekka LMS, Keshishi D, et al. Cannabidiol and Liver Enzyme Level Elevations in Healthy Adults: A Randomized Clinical Trial. JAMA Internal Medicine. 2025;185(9):1070-8.
- McGill, MR. The past and present of serum aminotransferases and the future of liver injury biomarkers. Excli j. 2016;15:817-28.
- Huestis MA, Solimini R, Pichini S, Pacifici R, Carlier J, Busardò FP. Cannabidiol Adverse Effects and Toxicity. Curr Neuropharmacol. 2019;17(10):974-89.
- Mould RR, Botchway SW, Parkinson JRC, Thomas EL, Guy GW, Bell JD, et al. Cannabidiol Modulates Mitochondrial Redox and Dynamics in MCF7 Cancer Cells: A Study Using Fluorescence Lifetime Imaging Microscopy of NAD(P)H. Frontiers in Molecular Biosciences. 2021;Volume 8 - 2021.
- Chan JZ, Duncan RE. Regulatory Effects of Cannabidiol on Mitochondrial Functions: A Review. Cells. 2021;10(5).
Figure 1.
Potential Anti-inflammatory Pathways via CB1, CB2, and TRPV1 Receptors and NF-κB Activation. The major non-psychotomimetic phytocannabinoid, CBD, can share neuroprotective, anti-oxidative, anti-emetic, and anti-carcinogenic qualities through various mechanisms. CBD interacts with CB1 and CB2 receptors, activating ERK 1/2 and AKT suppression, ultimately mediating autophagic fluxes in the cell. AKT suppression activation is also associated with anti-inflammatory effects such as cell proliferation, neurological function, neuroprotection, and immune modulation. TRPV1 activation leads to a reduction in IL-6 and IL-8, promoting anti-inflammatory effects. Interestingly, CBD also reduces NF-κB-dependent pathways by inhibiting the NF-κB complex degradation, IRAK-1 degradation, and p65 phosphorylation. CBD also reduces activation of LPS and STAT1, inhibiting pro-inflammatory mediators. As shown above, other anti-inflammatory properties are also caused by reduced cytokines and chemokines. CB1/CB2 receptors can interact with glucocorticoid receptor (GR) alpha to override the effect of steroid, rendering ineffectively of steroids. This figure was created in Biorender.com.
Figure 1.
Potential Anti-inflammatory Pathways via CB1, CB2, and TRPV1 Receptors and NF-κB Activation. The major non-psychotomimetic phytocannabinoid, CBD, can share neuroprotective, anti-oxidative, anti-emetic, and anti-carcinogenic qualities through various mechanisms. CBD interacts with CB1 and CB2 receptors, activating ERK 1/2 and AKT suppression, ultimately mediating autophagic fluxes in the cell. AKT suppression activation is also associated with anti-inflammatory effects such as cell proliferation, neurological function, neuroprotection, and immune modulation. TRPV1 activation leads to a reduction in IL-6 and IL-8, promoting anti-inflammatory effects. Interestingly, CBD also reduces NF-κB-dependent pathways by inhibiting the NF-κB complex degradation, IRAK-1 degradation, and p65 phosphorylation. CBD also reduces activation of LPS and STAT1, inhibiting pro-inflammatory mediators. As shown above, other anti-inflammatory properties are also caused by reduced cytokines and chemokines. CB1/CB2 receptors can interact with glucocorticoid receptor (GR) alpha to override the effect of steroid, rendering ineffectively of steroids. This figure was created in Biorender.com.

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



