Submitted:
11 September 2025
Posted:
12 September 2025
You are already at the latest version
Abstract
Background: Total hip and knee arthroplasty are widely performed procedures for end-stage osteoarthritis, with postoperative rehabilitation crucial in achieving optimal outcomes. Traditional in-person rehabilitation, however, faces limitations such as accessibility, cost, and logistical barriers. In this context, telerehabilitation has emerged as a promising digital alternative.Objective: This narrative review aims to synthesize current literature on telerehabilitation following total joint arthroplasty, evaluating its clinical effectiveness, cost-efficiency, patient satisfaction, and implementation challenges in comparison to conventional rehabilitation.Materials and Methods: A comprehensive literature search was conducted in Medline, Web of Science, and Scopus through April 2025. Studies included randomized controlled trials and longitudinal research involving telerehabilitation in total knee or hip arthroplasty. Data were extracted on outcomes, complications, technology integration, and patient-reported measures.Results: Evidence suggests that telerehabilitation—delivered via mobile apps, wearable sensors, virtual reality, and AI-enhanced platforms—can achieve functional outcomes comparable to traditional rehabilitation in terms of pain reduction, range of motion, and muscle strength. Patient satisfaction, adherence, and health-related quality of life are often superior in digitally supported programs, especially when remote coaching is included. Cost analyses indicate favorable economic benefits. However, challenges persist related to digital literacy, infrastructure, regulatory gaps, and the need for standardized protocols.Conclusion: Telerehabilitation represents a clinically valid, economically sustainable, and patient-centered alternative to traditional rehabilitation after total joint arthroplasty. Future research should focus on long-term outcomes, optimization of remote monitoring tools, and development of evidence-based implementation guidelines.
Keywords:
telerehabilitation
; total hip arthroplasty
; total knee arthroplasty
; PROMs
; digital health
; virtual reality
; postoperative rehabilitation
1. Introduction
Osteoarthritis (OA) is a degenerative joint disease, characterized by loss of cartilage, joint space narrowing, formation of osteophytes and synovial inflammation. It affects primarily weight-bearing joints such as hips and knees leading to pain, stiffness, reduced range of motion and functional impairment [1]. Risk factors include age, obesity, joint injury, genetic predisposition, and mechanical stress [2]. Current management of OA is a combination of non-pharmacological and pharmacological therapies aimed at symptom relief and functional improvement. These are conservative methods such as physical therapy, weight management, NSAIDs, and intra-articular injections [3]. In the end-stages of OA, when the conservative measures fail, total joint arthroplasty is the gold standard treatment [4]. In the last decades there has been a substantial increase of hip and knee replacement procedures particularly in the developed countries. This rise is due to the aging global population and advances in surgical techniques that have expanded indications to younger and more active individuals [5,6]. Moreover, the integration of robotic assistance in knee arthroplasty has contributed to improved surgical accuracy and better implant positioning. Nevertheless, the adoption of these technologies requires overcoming a learning curve, as outlined in recent systematic reviews. However, the success of joint replacement depends not only on the surgical procedure itself but also on a well-structured and effective postoperative rehabilitation program. Postoperative rehabilitation plays an essential role in obtaining optimal recovery after joint replacement surgery. It helps to restore joint function, recover muscle strength, mobility and facilitates the return to occupational and activities of daily living [7]. However, traditional face-to-face rehabilitation programs often present several limitations, including restricted access in rural or underserved areas, long travel distances, high costs, and limited availability of specialized professionals [8] In this context, telerehabilitation has emerged as a promising alternative to conventional in-person therapy. Telerehabilitation enables remote assessment, supervision, and monitoring through various technologies such as videoconferencing, mobile applications, web platforms, and wearable sensors. It may be delivered synchronously or asynchronously through recorded instructions and periodic feedback, and can be fully remote or integrated into a hybrid model combining in-person and virtual sessions [10,11]. Additionally, it offers advantages including increased accessibility, reduced travel time and costs, better adherence to home exercise programs, and greater flexibility for both patients and providers. Recent systematic reviews and meta-analyses support the efficacy and safety of telerehabilitation as a cost-effective and scalable solution for postoperative care [9,12]. Telerehabilitation has been used with great success in many areas of medicine and is becoming popular in the orthopedic field, particularly in the postoperative care of patients who underwent hip or knee joint replacement. This narrative review aims to explore and synthesize the current literature on the use of telerehabilitation in patients following total hip or knee arthroplasty. The review will examine its effectiveness, safety, cost-efficiency, and patient outcomes in comparison to traditional rehabilitation models, and highlight both its benefits and limitations.
2. Materials and Methods
This work was designed as a narrative review. No formal protocol registration (e.g., PROSPERO) was performed, and the PRISMA checklist was not applied. Nevertheless, a structured search and selection process was adopted to ensure transparency and reproducibility.
A comprehensive literature search was carried out up to April 2025 using Medline (via PubMed), Web of Science, and Scopus. The following combination of keywords and Boolean operators was employed: (“telerehabilitation” OR “tele-rehabilitation”) AND (“total hip arthroplasty” OR “hip replacement” OR “total knee arthroplasty” OR “knee replacement”). Only articles published in English were considered. In addition, the reference lists of the selected studies were manually screened to identify potentially relevant publications that were not retrieved during the initial database search.
Eligible studies included randomized controlled trials as well as prospective or retrospective longitudinal research. The target population consisted of adult patients undergoing total hip or knee arthroplasty. Interventions of interest were postoperative telerehabilitation programs delivered through mobile applications, web-based platforms, videoconferencing, wearable sensors, or virtual reality. Outcomes of relevance included clinical and functional recovery, patient-reported outcome measures (PROMs), cost-effectiveness, adherence, satisfaction, and complications. Studies such as case reports, expert opinions, editorials, letters, previous systematic reviews, and conference abstracts were excluded, as well as any publications not directly addressing telerehabilitation in joint arthroplasty [Table 1].
The study selection process was performed in two steps. First, titles and abstracts were screened to remove studies that did not meet the eligibility criteria. Second, full-text articles were retrieved and assessed for final inclusion. Two reviewers independently conducted the selection and data extraction; disagreements were resolved by discussion with a senior author. For each included study, the following information was extracted: study design, sample size, type of telerehabilitation intervention, comparator (if any), clinical and functional outcomes, patient-reported measures, complications, and implementation-related factors.
The extracted evidence was synthesized thematically, grouping studies according to the type of technology used, outcomes assessed, and key findings. Emphasis was placed on the level of clinical evidence, barriers to implementation, and potential economic implications. Although this review is not systematic, a simplified PRISMA-style flow diagram was developed to illustrate the study selection process, thereby increasing methodological transparency (Figure 1).
3. Results
The integration of digital technologies in healthcare has contributed to significant changes in the delivery of postoperative rehabilitation following total hip and knee arthroplasty. This section presents the available evidence on the technologies, clinical outcomes, and economic aspects of telerehabilitation.
3.1. Technologies and Modalities of Telerehabilitation
Telerehabilitation has gradually emerged as an effective alternative to traditional in-person rehabilitation, thanks to the integration of digital technologies that can support remote interventions. Early implementations were based on synchronous modalities, such as videoconferencing and telephone calls. This approach allows for direct contact, which is useful because of observation, immediate correction of exercises, and building a therapeutic alliance. Synchronous sessions are particularly suitable for initial assessments, supervised sessions, or for patients with ongoing support needs. However, these tools require a stable connection, simultaneous availability, and sometimes technical support for installation and management, limiting their accessibility [13,14]. With the expansion of mobile networks, there has been a rapid transition to asynchronous modes, based on mobile applications, web platforms and messaging systems. These tools allow patients to receive personalised exercises, educational materials and clinical feedback without simultaneous communication, offering greater flexibility [15]. Particularly relevant are mobile apps, which have become a focus of research in recent years. These apps allow autonomous use of demonstration videos, reminders, progress tracking and asynchronous interaction with the clinical team. This evolution is accompanied by the introduction of wearable devices (accelerometers, inertial measurements units - IMUs, gyroscopes) and rehabilitation robotics, which allow precise movement detection and active patient interaction with simulated environments [14]. Virtual reality has also found increasing application, offering motivating immersive scenarios for motor and cognitive training. Finally, the use of artificial intelligence represents the most advanced stage of telerehabilitation, allowing for the analysis of large volumes of clinical and biometric data, dynamic personalization of treatments, identification of early clinical deviations and support of therapeutic decision-making. The Vital Health Remote Rehabilitation system, for instance, combines user apps, wearable sensors and clinical portals to provide real-time biofeedback by adapting exercises through artificial intelligence algorithms [16]. In recent years, the development of digital technologies has enabled the integration of Patient-Reported Outcome Measures (PROMs) within telerehabilitation platforms, improving the ability to monitor post-operative recovery in a personalised and continuous manner. Among the most studied applications, myMobility (Zimmer Biomet) represents an established example. It provides educational content, guided rehabilitation exercises and collects physical activity data through integration with wearable devices, as well as including the regular administration of PROMs such as HOOS, Knee Injury and Osteoarthritis Outcome score (KOOS) and SF-36. Integrating digital health technologies in orthopedic surgery has fostered a synergistic relationship between the myMobility platform and the ROSA Robotic Surgical Assistant, both developed by Zimmer Biomet. MyMobility is a mobile health solution that facilitates pre- and postoperative management through remote education, tailored exercise programs, and continuous collection of PROMs. In parallel, ROSA provides robotic assistance during total joint arthroplasty, enhancing the precision of component alignment and bone preparation via real-time intraoperative data and preoperative planning [17]. The interoperability of these platforms enables a seamless continuum of care: ROSA delivers personalized surgical accuracy, while myMobility supports longitudinal tracking of functional recovery. Early evidence suggests that patients undergoing ROSA-assisted procedures, when managed postoperatively through myMobility, demonstrate increased adherence to rehabilitation protocols, improved early functional outcomes, and reduced dependence on in-person follow-up [18]. This digital-robotic integration enables standardized data collection for clinical registries, facilitating outcome-based and patient-centered decision-making in orthopedic care [19]. However, it has been shown that data collected passively from mobile devices (e.g. number of daily steps) do not show a strong correlation with subjective PROMs, highlighting the need to combine them with objective measurements of functional performance [20]. In this sense, systems such as StepApp, validated for patients undergoing total hip and knee arthroplasty, have shown a strong correlation between telemonitored data (e.g., 6-Minute Walk Test, 10-Meter Walk Test, 30-Second Sit-to-Stand Test) and those collected in-person, suggesting high reliability and clinical utility. These tests provide objective metrics on endurance, walking speed and muscle strength, with a high correlation to direct assessment by the therapist and are particularly effective in supporting a holistic and remote assessment of functional recovery, combining PROMs and performance data [21]. Nevertheless, it is important to emphasise that adherence to telerehabilitation strongly depends on individual factors such as caregiver support, digital literacy, and the presence of comorbidities [14,21].
3.2. Evidence of Effectiveness
The transition to telerehabilitation entails, at the same time, an evolution in the assessment of Patient-Reported Outcome Measures (PROMs): whereas in the past the focus was only on biomechanical parameters (e.g. pain, strength, range of motion), today increasing attention is being paid also to indicators such as patient satisfaction, self-efficacy, health-related quality of life (HRQoL) and cost-benefit analysis, reflecting a more holistic approach to evaluating rehabilitation effectiveness [14]. Patient-Reported Outcome Measures (PROMs) are standardised instruments used to collect information directly from patients about their perception of their health status, physical function, pain, quality of life and satisfaction with the treatment received. They are used in clinical and research settings to evaluate the effectiveness of therapeutic and rehabilitation interventions. PROMs can be categorised into: 1) functional outcomes (e.g., TUG, 6MWT), 2) autonomy in daily activities (e.g., FIM, Barthel), 3) pain (e.g., VAS, NRS), 4) mental health and self-efficacy (e.g., HADS, SEMCD), 5) quality of life (e.g., EQ-5D, SF-36), 6) specific joint outcomes (e.g., HOOS, KOOS, WOMAC, HHS), and 7) perceived satisfaction (e.g., GPE).
3.3. Physical Function and Motor Performance
The assessment of physical performance is one of the fundamental pillars for measuring the effectiveness of post-operative rehabilitation programmes. The PROMs used in this context provide objective information on the recovery of mobility, strength and balance. The studies analysed confirm that telerehabilitation is at least equivalent, and often superior, to conventional rehabilitation in terms of motor function.
Timed Up and Go (TUG): Assesses the time it takes a patient to get up from a chair, walk 3 metres, turn around, walk back and sit down. It measures functional mobility, balance and fall risk [22]. The TUG has been used in numerous studies to assess functional mobility. In the retrospective comparison trial published by Venosa et al. [23], the telerehabilitation group showed an improvement from 20 ± 2 to 12 ± 1.5 seconds (Δ -8.0 ± 2.6), whereas the group with in-person rehabilitation improved from 18 ± 1.5 to 13.1 ± 2 seconds (Δ -4.9 ± 2.5), with a statistically significant difference (p < 0.01).
Five Times Sit-to-Stand Test (FTSST): Measures the time it takes to stand up and sit down five consecutive times from a chair. It reflects lower limb strength, postural stability and autonomy in transfers [24]. In the study by Wijnen et al. [25], the tablet-app-treated group achieved 11.7 seconds at 6 months, compared to 14.7 and 14.0 seconds in the two control groups (p = 0.05), indicating a better recovery of lower limb strength.
6-Minute Walk Test (6MWT): Evaluates the distance travelled by walking for 6 minutes on a flat surface. It is an indicator of aerobic capacity and functional endurance [24]. In the Step-App® validation article by Lippi et al. [26], patients increased the distance walked from 128.0 m to 210.0 m after the rehabilitation cycle 10-Meter Walk Test (10MWT): Measures walking speed over 10 metres in normal and fast conditions. It is used to estimate walking autonomy and motor safety. [27]. The same study by Lippi et al. reported an increase in slow walking speed from 0.37 to 0.40 m/s and fast walking speed from 0.60 to 0.90 m/s (p < 0.0001), with values highly correlated with clinical standards.
30-Second Sit-to-Stand Test (30SST): Calculates how many times the patient can stand up completely from a chair in 30 seconds. Assesses lower limb strength and endurance [27]. In Lippi et al. [26], the number of repetitions increased from 6.0 to 8.0 (p < 0.0001), confirming the recovery of strength and endurance in the lower limbs.
Short Physical Performance Battery (SPPB): Test consisting of three tests (static balance, walking, standing up from a chair). It provides a global score (0-12) of physical performance in the elderly [28]. Also in the work of Lippi et al. [26], the SPPB score increased from 5.0 to 7.0 points after treatment (p < 0.0001). Again, there was no direct comparison, but the results confirm the effectiveness of digitally tracked rehabilitation.
Range of Motion (ROM): Measures the active range of motion of the affected joint (e.g. flexion, extension, abduction). Assesses joint mobility and functional limitation. In particular, active and passive ROM are crucial indicators of joint recovery, while strength and pain are monitored to adapt the rehabilitation load [29]. In the post-operative setting, an active ROM ≥90° for knee flexion is considered functional for daily activities, while a passive ROM >120° represents a good rehabilitation target. Although passive ROM is more difficult to detect by telemonitoring, some studies also report reliable results by remote observation or caregiver support [28].
In the RCT trial of Correia et al. [30] on hip arthroplasty, active flexion in the standing position at 6 months was 97.4° in the digital group vs 89.9° in the conventional group (p = 0.018), while abduction was 51.7° vs 43.8° (p = 0.024).
Peak Torque (PT): Measures the maximum isometric force of muscle groups using a dynamometer (e.g. abductors, extensors). It is an objective indicator of residual or recovered muscle strength [31]. Correira et al. [30] found that hip abductor strength increased by +69.6 Nm/kg×10 in the telerehabilitation group vs. +62.6 in the conventional group (p = 0.028), with a very pronounced effect (Cohen’s d = 2.4).
3.4. Autonomy and Activities of Daily Living (ADL)
The recovery of autonomy in activities of daily living (ADL) is one of the central goals of post-surgical rehabilitation, especially after hip or knee arthroplasty. In this context, PROMs assess the patient’s level of functional independence in performing actions such as dressing, washing, walking, climbing stairs or managing household activities. The following instruments were used in the work analysed:
Functional Independence Measure (FIM): Assesses the degree of independence in 18 motor and cognitive activities, with a score ranging from 18 (total dependence) to 126 (complete independence) [32]. In the study by Cottrell et al. [33], patients undergoing telerehabilitation achieved an average FIM score of 111.7 ± 3.13 at 6 months, significantly higher than the 98.64 ± 5.12 in the control group (telephone rehabilitation); the difference was highly significant (p < 0.001).
Barthel Index: Measures independence in daily activities on a scale from 0 to 100 [34]. In the work of Fascio et al. [34], both groups (VRRS vs. traditional) reported high scores, with final values of 98.6 ± 2.8 for the telerehabilitation group and 99.2 ± 1.3 for the traditional group (p non-significant). The scores indicate that the patients achieved almost full functional independence by the end of follow-up.
3.5. Pain
Pain reduction is one of the primary goals of post-operative rehabilitation, especially following hip or knee arthroplasty. The PROMs used for pain assessment are validated, easy-to administer instruments capable of detecting clinically relevant changes in the subjective perception of pain at rest and during movement.
Visual Analogue Scale (VAS): The VAS is a continuous scale from 0 to 10 (or 0 to 100) that measures the intensity of perceived pain, where 0 indicates “no pain” and 10 “unbearable pain” [35]. In the trial by Venosa et al. [23], patients in the telerehabilitation group showed an average reduction in pain at rest from 2.2 ± 0.1 to 0.8 ± 0.2, while the control group reduced from 1.7 ± 0.4 to 0.6 ± 0.1. The difference between the groups was significant (p < 0.01). For pain during movement, both groups showed an improvement of -2.0 points, with no significant difference between the two (p = 0.93).
Numerical Rating Scale (NRS/NPRS): Similar to the VAS, the NRS employs a numeric scale from 0 to 10 [33]. In the study by Lippi et al. [26], patients treated with Step-App® reported a reduction in pain from 2.0 to 1.0 in the immediate post-operative period (p = 0.0421). Although there was no direct comparison group, the improvement was considered clinically significant.
WOMAC Pain Subscale: The WOMAC (Western Ontario and McMaster Universities Osteoarthritis Index) includes a pain-specific subscale consisting of 5 items [36]. In the randomised controlled trial by Peng et al. [37] on early rehabilitation with virtual reality, the WOMAC pain score improved by -188.42 in the VR group and by -187.95 in the traditional group (p = 0.98), without significant differences. In another study, Salaffi et al. [36] found a mean WOMAC pain score of 2.93 ± 4.55 in the digital group and 6.27 ± 4.55 in the traditional group at 6 months, with a favourable difference that was not statistically significant (p = 0.215), but with a mean effect (η² = 0.136).
HOOS Pain / KOOS Pain: These subscales of the HOOS/KOOS questionnaires measure specific joint pain [38], the HOOS Pain subscale showed an average improvement from 12.5 to 70.0 in the telerehabilitation group and from 12.5 to 67.5 in the in-presence group, with p = 0.09. Although the difference was not statistically significant, the trend favoured the digital intervention.
3.6. Psychological State and Self-Efficacy
The psychological component plays a crucial role in functional recovery after major orthopaedic surgery. Anxiety, depression and low perception of self-efficacy may hinder adherence to the rehabilitation programme and slow down recovery. For this reason, some studies have included PROMs dedicated to the assessment of psychological well-being and confidence in managing one’s condition (self-efficacy).
Self-Rating Anxiety Scale (SAS): The SAS is a self-rating scale that measures anxiety symptoms on 20 items [39] on elderly hip fracture patients treated with home telerehabilitation, the mean SAS score decreased from 42.40 ± 3.07 to 29.26 ± 1.63 in the telerehabilitation group and from 46.21 ± 3.53 to 33.81 ± 2.62 in the traditional group (p < 0.001). The data indicate a significantly greater reduction in anxiety in the digital group.
Self-Efficacy for Managing Chronic Disease Scale (SEMCD): Measures patients’ confidence in managing their chronic condition on a scale from 1 to 10 [40]. In the RCT by Sun et al. [41], the SEMCD score increased in both groups, with improvement from 5.2 to 7.3 in the telerehabilitation group and from 5.1 to 6.8 in the standard group. The differences between the two groups were not statistically significant (p > 0.4), but the digital group showed a more pronounced increase in the medium to long term.
Self-Efficacy for Rehabilitation Outcome Scale (SER): Validated instrument to measure the perception of personal efficacy in the rehabilitation context [42]. In Wang et al. [43], the SER scale was used to assess patients’ motivational change. The data reported a cntinuous improvement in self-efficacy, particularly in patients with high platform adherence.
3.7. Quality of Life (QoL)
Health-related quality of life (HRQoL) is a multidimensional indicator that integrates subjective perceptions of physical, psychological and social status. In post-operative rehabilitation pathways, the assessment of HRQoL allows the global impact of treatment on patient well-being to be measured [44]. The most commonly used PROMs are the EQ-5D, SF-36/SF-12 scales, and the HOOS and KOOS quality of life specific subscales.
EQ-5D (EuroQol-5Dimensions): A generic instrument that measures 5 dimensions of health (mobility, personal care, activities of daily living, pain, anxiety/depression) and includes a health index and a visual scale (VAS)[45]. Lin DY et al. [46], the EQ-5D VAS score at 6 months was 82.9 ± 4.3 in the digital group and 68.7 ± 4.6 in the standard group, with a clinically relevant difference (Δ +14.2), although not statistically significant (p = 0.093), but with a large effect size (η² = 0.217).
SF-36 / SF-12 (Short Form Health Survey): Instrument to assess physical and mental well-being in 8 domains [47]. In the work of Wijnen et al. [25], the SF-36 score for physical function increased from 61.4 ± 20.2 to 89.0 ± 10.6 in the telerehabilitation group, compared to 62.1 ± 18.9 to 74.6 ± 15.8 in the controls (p = 0.07; Cohen’s d = 1.5).
HOOS QoL / KOOS QoL: These are subsections of the joint questionnaires measuring the impact of the pathology on autonomy, perceived safety and well-being [48,49]. In the RCT by Zhou et al. [50], the HOOS QoL score at 6 months was 68.7 in the telerehabilitation group vs. 68.7 in the standard group (p = 0.70). Although the scores overlapped, both groups achieved a high quality of life.
3.8. Functionality
To assess the clinical outcome in patients undergoing total hip or knee replacement, joint function-specific PROMs are commonly used. These include:
Harris Hip Score (HHS): The HHS is one of the most widely used instruments to measure clinical outcome after total hip arthroplasty. It is widely used to assess the effectiveness of treatment in terms of functional recovery and quality of joint motion. The total score ranges from 0 to 100 points, with higher values indicative of better function. It consists of four main sections: Pain (0-44 points), Function (0-47 points), Absence of deformity (0-4 points), Range of motion (0-5 points) [51]. In the study by Wu et al. [52], geriatric patients undergoing telerehabilitation after hip replacement achieved significantly higher HHS scores than the group with conventional rehabilitation. The mean values recorded were: at 1 month: 66.35 ± 4.63 (telerehabilitation) vs 63.48 ± 4.49 (control); at 3 months: 76.33 ± 4.52 (TR) vs 71.81 ± 3.84; at 6 months: 84.23 ± 3.13 (TR) vs 77.29 ± 4.95. All differences were statistically significant (p < 0.001.
Hip Disability and Osteoarthritis Outcome Score (HOOS): The HOOS is an extension of the WOMAC, specifically for patients with hip disorders. It assesses symptoms, pain, function in daily activities, sports and leisure, and quality of life related to hip health [53]. In the study by Wijnen et al. [25], conducted on hip arthroplasty patients followed with a tablet app and remote coaching, participants in the TR group reported significantly higher HOOS scores in the domains “sport/recreation” and “quality of life” than controls. For example, the sports domain showed an average increase of +8.7 points at 12 weeks in the TR group compared to the conventional group (p < 0.05).
Knee Injury and Osteoarthritis Outcome Score (KOOS): Similar to the HOOS, but dedicated to the knee, the KOOS measures pain, symptoms, ADL, sport, and QoL [43]. In various studies that included telemonitoring systems (e.g. StepApp®) [26], KOOS scores were comparable or slightly higher in the TR group compared to patients who underwent rehabilitation in attendance.
Oxford Knee Score (OKS): The OKS is a specific scale for patients undergoing total knee arthroplasty, and assesses pain and perceived function in daily life [54]. A study conducted in 2023 [55] showed that patients followed with telerehabilitation achieved greater improvement than those followed with conventional physiotherapy. The OKS results were: Baseline: 22 ± 1.3 (TR) vs 23 ± 2.1 (conventional); After 12 weeks: 36 ± 2.7 (TR) vs 35.1 ± 4.2; Delta: +14 points (TR) vs +12 points (conventional rehab) With statistical significance in favour of the TR group (p < 0.01).
3.9. Satisfaction and Subjective Perception
In addition to objective and functional indicators, the assessment of patient satisfaction and subjective perception plays a key role in measuring the overall effectiveness of post-arthroplasty rehabilitation.
GPE (Global Perceived Effect): a 7-point scale with which patients express their global perception of improvement after a therapeutic intervention. It varies from ‘strongly worsened’ to ‘completely recovered. [56]. In the randomised controlled trial by Fascio et al. [34], traditional home rehabilitation was compared with an early virtual reality rehabilitation programme (VRRS) after total hip replacement (THA). GPE scores were significantly higher in the VRRS group as early as postoperative day 15: GPE at day 15: 4.76 ± 0.43 (VRRS) vs 3.96 ± 0.65 (control), with p < 0.001. This finding suggests a higher perception of efficacy and subjective improvement by telerehabilitation patients.
Self-Administered Patient Satisfaction Scale: assesses the level of satisfaction with the course of treatment and the results obtained, often on a Likert or visuo-analogue scale [57]. In the study conducted by Rossi et al. [19] on the application of a care management system on a smartphone, the overall satisfaction reported by patients was high. Approximately 85% of the users stated that the rehabilitation experience via the app was “very satisfactory” or “satisfactory”, while more than 70% indicated that they would prefer this approach to an entirely face-to-face rehabilitation. Despite some reported limitations (technical problems or need for initial assistance), the overall perception was strongly positive.
3.10. Proprioception and Digital Engagement
Telerehabilitation is not limited to reproducing motor exercises at a distance, but can be enriched with advanced sensory components through the integration of systems such as virtual reality. A crucial element in post-arthroplasty recovery is proprioception, i.e. the patient’s ability to perceive the position and movement of the joint in space, which is crucial for stability, coordination and fall prevention. A controlled study by Gianola et al. [58] objectively assessed proprioception in patients undergoing total knee replacement using the Virtual Reality Rehabilitation System (VRRS). The test used was a proprioceptive reaching test, performed on a stabilometric platform, in which the degree of similarity (in percent) between the path taken by the patient and an ideal reference trajectory was measured. Measurements were taken at two points in time: at 3-4 days post-operative (baseline) and at discharge (approximately 10 days). The parameter measured was the proprioceptive similarity index: a percentage indicator of movement accuracy. The results showed a significant increase in the VRRS group compared to the conventional group, with an average improvement from 47.3% to 62.8% in the VRRS group (Δ = +15.5%), compared to a marginal increase in the control group (Δ = +3.2%). The intergroup difference was statistically significant (p = 0.0020).
3.11. Economic and Accessibility Aspects
One of the aspects in favour of telerehabilitation is the reduction of direct and indirect healthcare costs. Several studies show that home programmes result in significant cost savings compared to traditional rehabilitation, due to reduced transport costs, lost working time and the need for therapists to be physically present. Nelson et al. [56] have shown in a trial-based economic analysis that telerehabilitation after total hip arthroplasty is more cost-effective than standard in-patient care. Use of telerehabilitation optimises the resources of healthcare personnel, reducing the direct workload without compromising clinical outcomes, especially in post-pandemic settings where it is necessary to ensure continuity of care at a distance. According to Zhou et al. [50], the possibility to deliver services remotely reduces systemic costs related to the shortage of physiotherapists in rural or disadvantaged areas, contributing to a better distribution of available resources. Wijnen et al. [25], while not providing a formal economic analysis, hypothesise that tablet-assisted home-based programmes are more sustainable for national healthcare systems due to the lower work intensity of therapists and the scalability of the technology platform.Recent evidence shows that digital telerehabilitation devices can offer favourable cost-effectiveness, especially when compared to standard in-patient rehabilitation. The GaitSmart system, a sensorised device integrated with a customised exercise application, has been shown to be clinically more effective and less costly than standard of care (SoC) in the elderly population undergoing hip or knee arthroplasty. In particular, it generated an average saving of £450.56 per patient and an increase of 0.02 QALYs, thus proving to be a dominant strategy [55]. In parallel, a meta-analysis of 14 studies showed that telerehabilitation has a 90% probability of being cost-effective at a willingness-to-pay (WTP) threshold of $30,000 per QALY, with an average saving of between $1,200 and $6,500 per patient. The most effective devices were found to be those integrating sensors, remote monitoring and digital coaching platforms [56]. However, some methodological heterogeneity among the studies is reported, making more standardisation necessary for more robust comparisons. According to Calabrò et al. [16], the integration of artificial intelligence into telerehabilitation systems has the potential to improve overall accessibility to care, particularly for patients with limited mobility or living in remote regions, reducing delays in recovery and improving functional outcomes.
Zhou et al. [50] also emphasise that infrastructural and socio-economic barriers - including low levels of education and limited internet connectivity - represent a challenge for patients in disadvantaged areas, but reiterate that mobile-based home programmes can fill this gap. Telerehabilitation can facilitate the participation of patients with difficulties in reaching rehabilitation centres for geographical or physical reasons, reducing costs and travel time [52]. These advantages are particularly relevant for elderly patients, often with walking problems or without stable family support for transfers.
4. Discussion
Telerehabilitation represents one of the most promising applications of the digital transformation in healthcare, offering a patient-centered and cost-effective alternative to conventional in-person therapy.
Despite its many advantages, telerehabilitation presents technological barriers that may compromise the effectiveness of treatment, especially in the elderly population. Among the most frequent problems are unfamiliarity with digital devices, the need for stable, high-speed connections, and difficulty in configuring and maintaining systems. Many users, especially those with physical or cognitive disabilities, may face significant obstacles in using keyboards, software or video devices, aggravated by a lack of technical support and non-intuitive interfaces [15].
Further critical issues concern the need for software updates, the management of multiple peripheral devices (cameras, sensors, remote controls), and the intervention of clinical staff not always trained in technology, which may slow down or compromise patient interaction. Furthermore, the sensory and cognitive problems typical of older individuals - such as visual impairment or memory difficulties - necessitate a simplified and inclusive design of user interfaces.
The implementation of tele-neurorehabilitation is hindered by practical problems such as uneven access to smart devices, network interruptions, poor lighting, and difficulties in receiving timely technical assistance, with a significant impact on acceptance and perceived effectiveness, especially among elderly patients [19].
Telerehabilitation can serve as a key resource for patients living in peripheral or underserved areas, often affected by poor healthcare facilities, economic constraints, and limited mobility [53]. Several studies indicate that it enables better allocation of healthcare personnel, ensures continuity of care, and reduces systemic costs, especially in post-pandemic contexts [52,53].
The adherence of elderly patients is a crucial dimension for the clinical effectiveness of the intervention. Recent studies show that most patients can follow the programme at a distance, but hindering factors related to age, educational level, presence of comorbidities and family support remain. For example, Wang et al. [14] showed that at least secondary education level, coexistence with family members and a good level of perceived self-efficacy are associated with more frequent access to the programme, higher exercise completion and active interactions in digital forums. In contrast, older age correlates negatively with activity in forums and communication channels with therapists, indicating a greater vulnerability to digital isolation.
However, adherence to telerehabilitation strongly depends on individual factors such as caregiver support, digital literacy, and the presence of comorbidities [14,22].
Wijnen et al. [25] also observed good adherence in moderately elderly patients (up to 75 years) to a programme supported by tablet and telephone coaching, but emphasised the need for initial onboarding for the correct use of the technology. Weekly exercise frequency (more than 5 days) and participation in telephone coaching contributed to a higher clinical improvement than controls. However, Chen et al. [21], in a qualitative study, point out that significant barriers remain in patients over the age of 65, including a lack of understanding of the treatment pathway, fears related to pain or complications, and logistical difficulties (e.g. absence of environmental modifications, such as aids in bathrooms). These factors often result in reduced rehabilitation efforts. In this sense, caregiver involvement and continuous support by healthcare professionals are indicated as key determinants of adherence.
Finally, the use of mobile apps and social messaging systems (e.g. WeChat) was perceived positively in terms of accessibility, but digital literacy is still a limitation for some elderly people, especially in the absence of personalised technical guidance [57]. Although mobile-based and sensor-integrated platforms can reduce infrastructural barriers, socioeconomic disparities and limited digital competence remain challenges to be addressed to fully realise the potential of remote rehabilitation [20].
Currently, there is no universally accepted protocol for the administration of telerehabilitation programmes, which limits the replicability of studies, comparability of clinical outcomes and integration into healthcare systems. Telerehabilitation applications are often described in a way that is limited to specific types of technology or individual populations, making it difficult to generalise the evidence and define shared guidelines [15].In addition, the need for greater clarity in the implementation modalities is noted, especially in the transition between hospital and home settings, and in the definition of the healthcare professionals involved. The literature also points to the variability in the duration, intensity, content and mode of administration of the protocols, which prevents the establishment of precise and comparable therapeutic thresholds. This has also been recognised in more recent studies, such as that of Fascio et al. [34], in which it is observed that the adoption of home VR systems is effective, but difficult to compare with other interventions that are not equivalent in terms of frequency or supervision.
One of the main issues raised in the literature concerns the protection of personal data and the confidentiality of digitally transmitted information. Many concerns are related to privacy, security, professional liability and the risk of malpractice, especially in resource-limited settings [19].
The lack of transparency of algorithms in artificial intelligence-based system, and the risk of systematic errors, pose challenges in terms of clinical liability, requiring strict guidelines to ensure safe and responsible use of the technology [20].
5. Conclusions
Telerehabilitation has emerged as a safe and clinically valid modality for delivering post-arthroplasty rehabilitation, with outcomes that are largely equivalent to conventional face-to-face rehabilitation. It promotes joint mobility, muscles strength and pain control while also considering patient-reported outcomes like satisfaction, adherence, and health-related quality of life. The integration of digital tools, such as virtual reality, smart wearable systems, mobile applications, and AI platforms, enables customization, monitoring, and patient engagement, turning telerehabilitation into an adaptive and innovative solution for several users, including older adults and those living in rural areas. From an economic point of view, telerehabilitation is significant cost savings compared to traditional rehabilitation, due to reduced transport costs, lost working time and the need for therapists to be physically present and, as such, it offers a viable and sustainable solution for health systems, particularly in the post-pandemic era, despite it shows several limitations that may compromise the effectiveness of treatment, especially in the elderly population. Moreover, future research should prioritize the development of evidenced-based clinical practice guidelines, refinement of remote assessment tools, and robust trial examining long-term effects. Furthermore, ethical and legal issues encompassing privacy and clinician accountability must be resolved to ensure the safe deployment of AI-enhanced telerehabilitation. With coordinated efforts in terms of technology design, policy, and education, telerehabilitation holds the potential to redefine rehabilitation protocols making it more accessible, patient-centered, and a sustainable solution.
Author Contributions
All authors have contributed to the conception and design of this study, acquisition of data, in drafting the article, in its revision, and all the authors approved the final draft of the submitted article.
Funding
This research received no external funding. None of the authors received any funds or has any financial interests to disclose.
Compliance with ethical standards
The study was conducted according to the principles expressed in the Declaration of Helsinki and its later amendments. The research protocol was approved by the Institutional Review Board of Fondazione Policlinico Universitario “A Gemelli” IRCCS – Rome.
Data Availability Statement
All the data we analysed and tables we compiled are available for any clarification.
Acknowledgments
Not applicable.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Hunter DJ, Bierma-Zeinstra S. (2019). Osteoarthritis. Lancet, 393(10182), 1745–1759.
- Loeser, RF; et al. (2012). Osteoarthritis: a disease of the joint as an organ. Arthritis Rheum, 64(6), 1697–1707. [CrossRef]
- Kolasinski, SL; et al. (2020). 2020 American College of Rheumatology guideline for the management of osteoarthritis. Arthritis Care Res, 72(2), 149–162.
- Evans, JT; et al. (2019). How long does a knee replacement last? A systematic review and meta-analysis of case series and national registry reports. Lancet, 393(10172), 655–663. [CrossRef]
- Sloan M, Premkumar A, Sheth NP. (2018). Projected volume of primary total joint arthroplasty in the U.S., 2014 to 2030. J Bone Joint Surg Am, 100(17), 1455–1460. [CrossRef]
- Pabinger C, Lothaller H, Geissler A. (2015). Utilization rates of hip arthroplasty in OECD countries. Osteoarthritis Cartilage, 23(10), 1664–1673. [CrossRef]
- Artz, N; et al. (2015). Effectiveness of physiotherapy exercise after hip arthroplasty: a systematic review. BMJ Open, 5(6), e005521.
- Russell, TG. (2007). Physical rehabilitation using telemedicine. J Telemed Telecare, 13(5), 217–220. [CrossRef]
- Cottrell, MA; et al. (2017). Real-time telerehabilitation for the treatment of musculoskeletal conditions is effective and comparable to standard practice: a systematic review and meta-analysis. Clin Rehabil, 31(5), 625–638.
- Kairy D, Lehoux P, Vincent C, Visintin M. (2009). A systematic review of clinical outcomes, clinical process, healthcare utilization and costs associated with telerehabilitation. Disabil Rehabil, 31(6), 427–447. [CrossRef]
- Mani, S; et al. (2017). Validity and reliability of internet-based physiotherapy assessment for musculoskeletal disorders: a systematic review. J Telemed Telecare, 23(3), 379–391.
- Jiang, S; et al. (2021). Effectiveness of telerehabilitation for patients after total knee arthroplasty: A meta-analysis of randomized controlled trials. Telemed J E Health, 27(3), 247–258.
- Pramuka, M., & van Roosmalen, L. (2009). Telerehabilitation technologies: Accessibility and usability. International Journal of Telerehabilitation, 1(1), 85–88.
- Wang, L., Zhang, L., & He, C. (2025). Research progress and hot topics in telerehabilitation for hip or knee arthroplasty. Orthopaedic Surgery, 17, 677–693. [CrossRef]
- Uddin, M. , Ganapathy, K., & Syed-Abdul, S. (2024). Digital technology enablers of tele-neurorehabilitation in pre- and post-COVID-19 pandemic era – A scoping review. International Journal of Telerehabilitation, 16(1). [CrossRef]
- Calabrò, R. S. , & Mojdehdehbaher, S. (2025). AI-driven telerehabilitation: Benefits and challenges of a transformative healthcare approach. AI, 6(62). [CrossRef]
- Capece, G., Andriollo, L., Sangaletti, R., Righini, R., Benazzo, F., & Rossi, S. M. P. (2024). Advancements and Strategies in Robotic Planning for Knee Arthroplasty in Patients with Minor Deformities. Life, 14(12), 1528. [CrossRef]
- Chambers, M. , & Goyal, N. (2022). Integration of digital health with robotic-assisted arthroplasty: A review of myMobility and ROSA Knee System. Journal of Orthopaedic Surgery and Research, 17(1), 114. [CrossRef]
- Rossi, S.M.P. et al. Problems and Opportunities of a Smartphone-Based Care Management Platform. Healthcare. 2024;12(2):153. https://doi.org/10.3390/healthcare12020153) (Zimmer Biomet. ROSA® Knee and myMobility® Digital Care Management System Integration White Paper. Warsaw, IN: Zimmer Biomet; 2021. [CrossRef]
- Lippi, L.; et al. System for tracking and Evaluating performance (Step-App®): validation and clinical application. Eur J Phys Rehabil Med. 2024;60(2):349–360. [CrossRef]
- Chen, J. , Zhu, X., Jiang, J., Qi, Y., & Shi, Y. (2019). Needs of Chinese patients undergoing home-based rehabilitation after hip replacement: A qualitative study. PLOS ONE, 14(7), e0220304. [CrossRef]
- Podsiadlo D, Richardson S. The timed “Up & Go”: a test of basic functional mobility for frail elderly persons. J Am Geriatr Soc. 1991 Feb;39(2):142-8. [CrossRef] [PubMed]
- Venosa M, Romanini E, Ciminello E, Cerciello S, Angelozzi M, Calvisi V. Telerehabilitation Is a Valid Option for Total Knee Arthroplasty Patients: A Retrospective Pilot Study Based on Our Experience during the COVID-19 Pandemic. Healthcare (Basel). 2023 Sep 7;11(18):2489. [CrossRef] [PubMed] [PubMed Central]
- Muñoz-Bermejo L, Adsuar JC, Mendoza-Muñoz M, Barrios-Fernández S, Garcia-Gordillo MA, Pérez-Gómez J, Carlos-Vivas J. Test-Retest Reliability of Five Times Sit to Stand Test (FTSST) in Adults: A Systematic Review and Meta-Analysis. Biology (Basel). 2021 Jun 9;10(6):510. [CrossRef] [PubMed] [PubMed Central]
- Wijnen A, Hoogland J, Munsterman T, Gerritsma CL, Dijkstra B, Zijlstra WP, Dekker JS, Annegarn J, Ibarra F, Slager GE, Zijlstra W, Stevens M. Effectiveness of a Home-Based Rehabilitation Program After Total Hip Arthroplasty Driven by a Tablet App and Remote Coaching: Nonrandomized Controlled Trial Combining a Single-Arm Intervention Cohort With Historical Controls. JMIR Rehabil Assist Technol. 2020 Apr 27;7(1):e14139. [CrossRef] [PubMed] [PubMed Central]
- Lippi L, Desimoni F, Canonico M, Massocco G, Turco A, Polverelli M, et al. System for Tracking and Evaluating Performance (Step-App®): Validation and Clinical Application of a Mobile Telemonitoring System in Patients with Knee and Hip Total Arthroplasty. A Prospective Cohort Study. European Journal of Physical and Rehabilitation Medicine. 2024;60(2):349-360. [CrossRef]
- Enright, PL. The six-minute walk test. Respir Care. 2003 Aug;48(8):783-5. [PubMed]
- De Baptista CRJA, Vicente AM, Souza MA, Cardoso J, Ramalho VM, Mattiello-Sverzut AC. Methods of 10-Meter Walk Test and Repercussions for Reliability Obtained in Typically Developing Children. Rehabil Res Pract. 2020 Aug 20;2020:4209812. [CrossRef] [PubMed] [PubMed Central]
- Jones CJ, Rikli RE, Beam WC. A 30-s chair-stand test as a measure of lower body strength in community-residing older adults. Res Q Exerc Sport. 1999 Jun;70(2):113-9. [CrossRef] [PubMed]
- Dias Correia F, Nogueira A, Magalhães I, Guimarães J, Moreira M, Barradas I, Molinos M, Teixeira L, Pires J, Seabra R, Lains J, Bento V. Digital Versus Conventional Rehabilitation After Total Hip Arthroplasty: A Single-Center, Parallel-Group Pilot Study. JMIR Rehabil Assist Technol. 2019 Jun 21;6(1):e14523. [CrossRef] [PubMed] [PubMed Central]
- Welch SA, Ward RE, Beauchamp MK, Leveille SG, Travison T, Bean JF. The Short Physical Performance Battery (SPPB): A Quick and Useful Tool for Fall Risk Stratification Among Older Primary Care Patients. J Am Med Dir Assoc. 2021 Aug;22(8):1646-1651. Epub 2020 Nov 13. [CrossRef] [PubMed] [PubMed Central]
- Osundolire, S. , Mbrah, A., Liu, S.-H., & Lapane, K. L. (2024). Association between patient and facility characteristics and rehabilitation outcomes after joint replacement surgery in different rehabilitation settings for older adults: A systematic review. Journal of Geriatric Physical Therapy, 47(1), E1–E18. [CrossRef]
- Cottrell MA, O’Leary SP, Raymer M, Hill AJ, Comans T, Russell TG. Does telerehabilitation result in inferior clinical outcomes compared with in-person care for the management of chronic musculoskeletal spinal conditions in the tertiary hospital setting? A non-randomised pilot clinical trial. J Telemed Telecare. 2021 Aug;27(7):444-452. Epub 2019 Nov 26. [CrossRef] [PubMed]
- Fascio, E. , Vitale, J. A., Sirtori, P., Peretti, G., Banfi, G., & Mangiavini, L. (2022). Early virtual-reality-based home rehabilitation after total hip arthroplasty: A randomized controlled trial. Journal of Clinical Medicine, 11(1766). [CrossRef]
- Cramer JT, Housh TJ, Evetovich TK, Johnson GO, Ebersole KT, Perry SR, Bull AJ. The relationships among peak torque, mean power output, mechanomyography, and electromyography in men and women during maximal, eccentric isokinetic muscle actions. Eur J Appl Physiol. 2002 Jan;86(3):226-32. [CrossRef] [PubMed]
- Salaffi F, Leardini G, Canesi B, Mannoni A, Fioravanti A, Caporali R, Lapadula G, Punzi L; Gonarthrosis and Quality Of Life Assessment (GOQOLA). Reliability and validity of the Western Ontario and McMaster Universities (WOMAC) Osteoarthritis Index in Italian patients with osteoarthritis of the knee. Osteoarthritis Cartilage. 2003 Aug;11(8):551-60. [CrossRef] [PubMed]
- Peng L, Zeng Y, Wu Y, Si H, Shen B. Virtual reality-based rehabilitation in patients following total knee arthroplasty: a systematic review and meta-analysis of randomized controlled trials. Chin Med J (Engl). 2021 Dec 13;135(2):153-163. [CrossRef] [PubMed] [PubMed Central]
- Davis AM, Perruccio AV, Canizares M, Hawker GA, Roos EM, Maillefert JF, Lohmander LS. Comparative, validity and responsiveness of the HOOS-PS and KOOS-PS to the WOMAC physical function subscale in total joint replacement for osteoarthritis. Osteoarthritis Cartilage. 2009 Jul;17(7):843-7. Epub 2009 Jan 31. [CrossRef] [PubMed]
- Olatunji BO, Deacon BJ, Abramowitz JS, Tolin DF. Dimensionality of somatic complaints: factor structure and psychometric properties of the Self-Rating Anxiety Scale. J Anxiety Disord. 2006;20(5):543-61. Epub 2005 Sep 29. In the RCT trial of Wu et al. (2023). [CrossRef] [PubMed]
- Ritter PL, Lorig K. The English and Spanish Self-Efficacy to Manage Chronic Disease Scale measures were validated using multiple studies. J Clin Epidemiol. 2014 Nov;67(11):1265.
- Sun S, Li Y, Zhang G, Zhang Y, Dong J. A randomized controlled Trial of telerehabilitation intervention for acute ischemic stroke patients Post-Discharge. J Clin Neurosci. 2025 Jun;136:111245. Epub 2025 Apr 30. [CrossRef] [PubMed]
- Stevens M, van den Akker-Scheek I, van Horn JR. A Dutch translation of the Self-Efficacy for Rehabilitation Outcome Scale (SER): a first impression on reliability and validity. Patient Educ Couns. 2005 Aug;58(2):121-6. [CrossRef] [PubMed]
- Wang, Q., Lee, R. L.-T., Hunter, S., Zhu, A., & Chan, S. W.-C. (2024). Patient engagement in a mobile app–based rehabilitation program for total hip or knee arthroplasty: Secondary data analysis of a randomized controlled trial. JMIR Mhealth and Uhealth, 12, e57635. [CrossRef]
- Hernández-Segura N, Marcos-Delgado A, Pinto-Carral A, Fernández-Villa T, Molina AJ. Health-Related Quality of Life (HRQOL) Instruments and Mobility: A Systematic Review. Int J Environ Res Public Health. 2022 Dec 8;19(24):16493. [CrossRef] [PubMed] [PubMed Central]
- Balestroni G, Bertolotti G. The EuroQol-5D (EQ-5D): an instrument for measuring quality of life [EuroQol-5D (EQ-5D): an instrument for measuring quality of life]. Monaldi Arch Chest Dis. 2012 Sep;78(3):155-9. Italian. [CrossRef] [PubMed]
- Lin DY, Cheok TS, Kaambwa B, Samson AJ, Morrison C, Chan T, Kroon HM, Jaarsma RL. Evaluation of the EQ-5D-5L, EQ-VAS stand-alone component and Oxford knee score in the Australian knee arthroplasty population utilising minimally important difference, concurrent validity, predictive validity and responsiveness. Health Qual Life Outcomes. 2023 May 10;21(1):41. [CrossRef] [PubMed] [PubMed Central]
- Ware JE Jr, Sherbourne CD. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med Care. 1992 Jun;30(6):473-83. [PubMed]
- Nilsdotter AK, Lohmander LS, Klässbo M, Roos EM. Hip disability and osteoarthritis outcome score (HOOS)--validity and responsiveness in total hip replacement. BMC Musculoskelet Disord. 2003 May 30;4:10. Epub 2003 May 30. [CrossRef] [PubMed] [PubMed Central]
- Roos EM, Lohmander LS. The Knee injury and Osteoarthritis Outcome Score (KOOS): from joint injury to osteoarthritis. Health Qual Life Outcomes. 2003 Nov 3;1:64. [CrossRef] [PubMed] [PubMed Central]
- Zhou Y, Lyu Y, Wang Q, Ma Y, Huang L, Zhang X. Mobile-based in-home telerehabilitation compared with in-hospital face-to-face rehabilitation for elderly patients after total hip arthroplasty in China’s level 1 trauma center: a noninferiority randomized controlled trial. Front Surg. 2025 Jan 14;11:1536579. [CrossRef] [PubMed] [PubMed Central]
- Nilsdotter A, Bremander A. Measures of hip function and symptoms: Harris Hip Score (HHS), Hip Disability and Osteoarthritis Outcome Score (HOOS), Oxford Hip Score (OHS), Lequesne Index of Severity for Osteoarthritis of the Hip (LISOH), and American Academy of Orthopedic Surgeons (AAOS) Hip and Knee Questionnaire. Arthritis Care Res (Hoboken). 2011 Nov;63 Suppl 11:S200-7. [CrossRef] [PubMed]
- Wu WY, Zhang YG, Zhang YY, Peng B, Xu WG. Clinical Effectiveness of Home-Based Telerehabilitation Program for Geriatric Hip Fracture Following Total Hip Replacement. Orthop Surg. 2023 Feb;15(2):423-431. Epub 2022 Nov 29. [CrossRef] [PubMed] [PubMed Central]
- Williams DP, Blakey CM, Hadfield SG, Murray DW, Price AJ, Field RE. Long-term trends in the Oxford knee score following total knee replacement. Bone Joint J. 2013 Jan;95-B(1):45-51. [CrossRef] [PubMed]
- Kamper SJ, Ostelo RW, Knol DL, Maher CG, de Vet HC, Hancock MJ. Global Perceived Effect scales provided reliable assessments of health transition in people with musculoskeletal disorders, but ratings are strongly influenced by current status. J Clin Epidemiol. 2010 Jul;63(7):760-766.e1. Epub 2010 Jan 8. [CrossRef] [PubMed]
- Mahomed N, Gandhi R, Daltroy L, Katz JN. The self-administered patient satisfaction scale for primary hip and knee arthroplasty. Arthritis. 2011;2011:591253. Epub 2011 Jan 10. [CrossRef] [PubMed] [PubMed Central]
- Nelson, M. , Russell, T., Crossley, K., Bourke, M., & McPhail, S. (2021). Cost-effectiveness of telerehabilitation versus traditional care after total hip replacement: A trial-based economic evaluation. Journal of Telemedicine and Telecare, 27(6), 359-366. [CrossRef]
- Zanghelini, F., Ponzo, A., Xydopoulos, G., Fordham, R., & Khanal, S. (2024). Cost-effectiveness of GaitSmart and an artificial intelligence solution for rehabilitation of patients undergoing total hip arthroplasty (THA) and total knee arthroplasty (TKA) in older population in the United Kingdom. Geriatrics, 9(129).
- Gianola S, Stucovitz E, Castellini G, Mascali M, Vanni F, Tramacere I, Banfi G, Tornese D. Effects of early virtual reality-based rehabilitation in patients with total knee arthroplasty: A randomized controlled trial. Medicine (Baltimore). 2020 Feb;99(7):e19136. [CrossRef] [PubMed] [PubMed Central]
Figure 1.
PRISMA Flow-diagram.
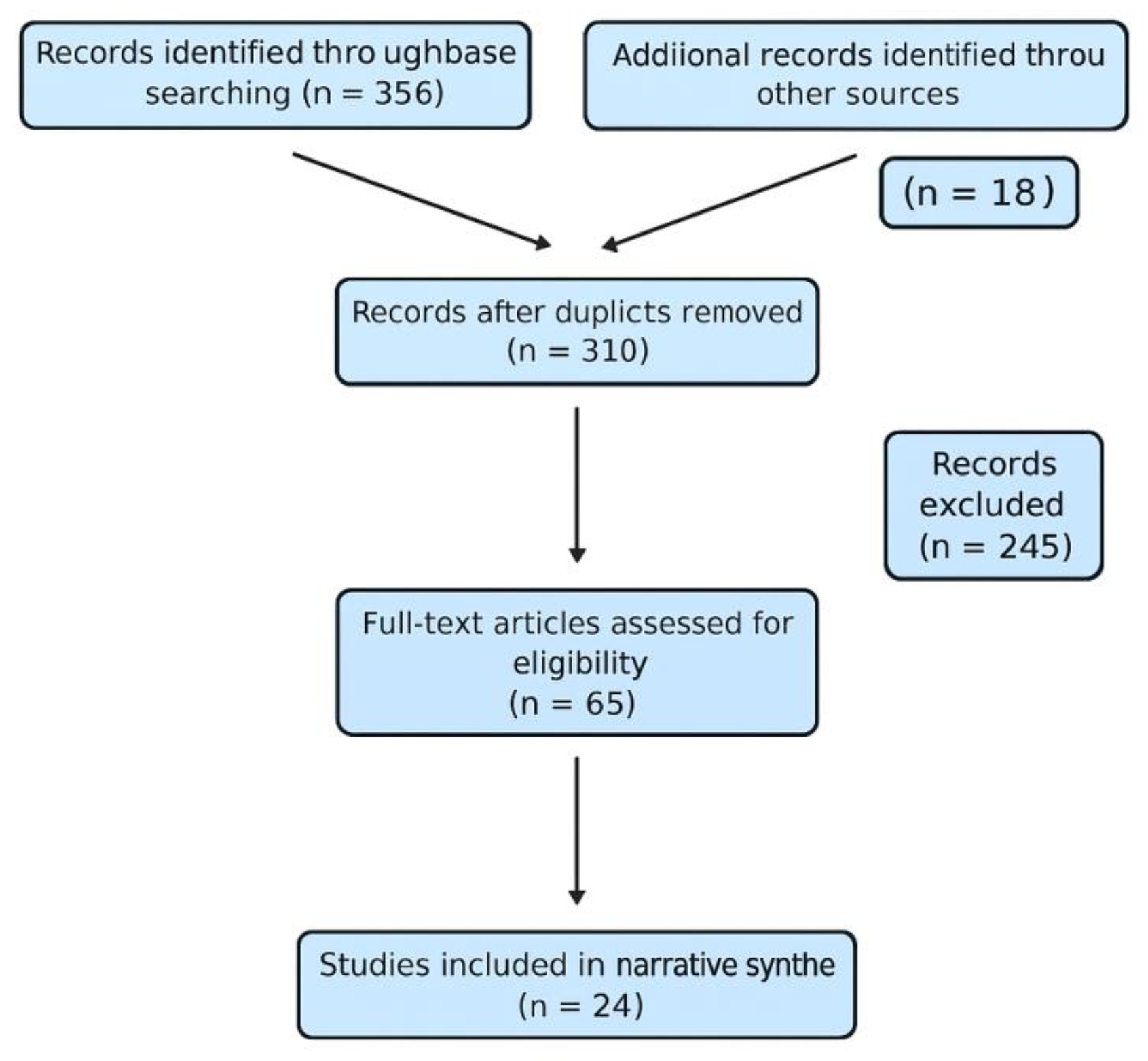

Table 1.
Inclusion and Exclusion Criteria.
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| Randomized controlled trials, prospective or retrospective longitudinal studies | Case reports, expert opinions, editorials, letters, systematic reviews or meta-analyses, conference abstracts without full data. |
| Adult patients undergoing total hip or knee arthroplasty | Studies not directly addressing telerehabilitation after joint arthroplasty. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



