Submitted:
05 September 2025
Posted:
08 September 2025
You are already at the latest version
Abstract
Vascular pain encompasses a heterogeneous group of clinical conditions characterized by pain arising from arterial, venous, microvascular, or vasculitic mechanisms. Unlike classical nociceptive pain, vascular pain often displays mixed nociceptive, neuropathic, and nociplastic components, reflecting ischemia, endothelial dysfunction, neuroinflammation, and maladaptive central sensitization. Clinically, vascular pain is encountered in chronic limb-threatening ischemia (CLTI), venous leg ulcers (VLU), sickle cell disease (SCD), and systemic vasculitides, imposing a major burden on quality of life, functionality, and health systems. Its recognition remains challenging due to overlapping mechanisms and atypical pain presentations. Advances in pathophysiological understanding and the development of targeted interventions—ranging from revascularization and spinal cord stimulation to novel pharmacological and bioengineering approaches—are reshaping management. This narrative review synthesizes current evidence on mechanisms, clinical manifestations, diagnostic approaches, and therapeutic strategies for vascular pain, highlighting gaps in knowledge and directions for future research.
Keywords:
vascular pain
; chronic leg ulcers
; venous ulcers
; pain
Introduction
Pain of vascular origin represents a distinct yet underrecognized clinical entity. Chronic venous disease (CVD) and its most debilitating complication, venous leg ulcers (VLUs), represent a prevalent and underappreciated source of vascular pain distinguished by complex pathophysiology and significant impact on quality of life. Venous leg ulcers, which account for approximately 70–90 % of all chronic leg ulcers, affect about 1 % of the Western population during their lifetime, with prevalence rising to 3–5 % among individuals above 65 years of age [1,2].
Patients with VLUs commonly experience persistent wound-related pain, with reported prevalence ranging broadly from 50 % to as high as 87 %, reflecting varying methodologies and patient populations [3]. This pain is multifactorial in origin. Venous hypertension resulting from valve incompetence or obstruction leads to extravasation of plasma proteins, leukocyte trapping, chronic inflammation, and microvascular ischemia. This milieu promotes extracellular matrix degradation and impaired wound healing, while sensitizing both nociceptive and neuropathic pathways [4]. Biochemically, the persistent inflammatory state is characterized by elevated proinflammatory cytokines and proteases, compounding nociceptor activation and contributing to perceptual variability and central sensitization [5].
Clinically, pain associated with VLUs often manifests as dull, aching, or burning sensations that may worsen during movement or depend on limb position and can be constant or intermittent [6]. Qualitative studies highlight the profound psychosocial burden of VLU-associated pain: patients report embarrassment, interrupted sleep, impaired mobility, and emotional distress, all of which exacerbate pain perception and amplify central nociplastic mechanisms [7].
Despite these profound tribulations, vascular pain in the context of VLUs remains underrepresented within pain taxonomy frameworks and is often inadequately addressed in clinical practice. Standard management strategies for VLUs, including compression therapy, leg elevation, wound dressings, and corrective vascular interventions, primarily target ulcer healing but frequently fail to provide adequate analgesia. Moreover, comorbidities such as obesity, immobility, or lipodermatosclerosis may further exacerbate both ulcer chronicity and pain severity [8,9].
Emerging therapeutic avenues integrating multimodal approaches offer promise. For instance, addressing both underlying vascular pathology (via compression or endovenous procedures) and neuropathic or inflammatory pain pathways (through pharmacotherapy or neuromodulation) may yield superior outcomes [10]. However, mechanistic studies specific to VLU pain remain scarce, and well-designed clinical investigations are lacking.
In summary, pain originating from venous leg ulcers seems a complex, multifaceted phenomenon encompassing nociceptive, neuropathic, and nociplastic components. The high prevalence and substantial morbidity associated with VLU pain underscore the critical need for enhanced recognition, refined pathophysiological delineation, and targeted therapeutic research. This review endeavors to synthesize current knowledge and illuminate avenues for future innovation in this neglected arena.
Methods
This review was conceived as a narrative synthesis aimed at providing a comprehensive overview of the epidemiology, pathophysiology, clinical manifestations, diagnostic approaches, and therapeutic strategies related to vascular pain, with particular emphasis on chronic venous disease and VLUs. The methodological approach followed the recommendations of the Scale for the Assessment of Narrative Review Articles (SANRA), which encourages clarity of scope, transparent literature selection, scientific reasoning, and appropriate referencing [11].
Literature Search Strategy
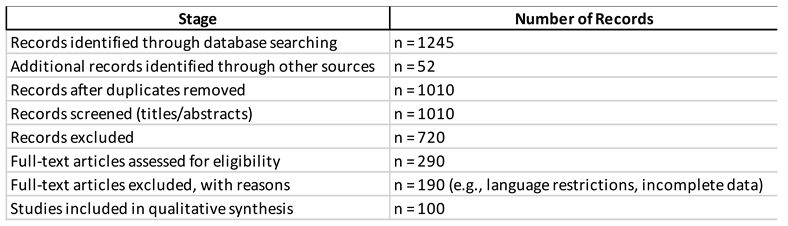
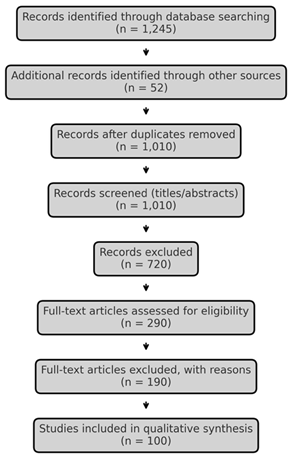
A non-systematic but comprehensive literature search was conducted across multiple databases, including PubMed/MEDLINE, Scopus, Embase, and Web of Science, covering publications from January 2015 to July 2025. Search terms combined controlled vocabulary (MeSH) and free-text keywords related to vascular pain and chronic venous disorders. The primary search string included combinations of the following terms: “vascular pain”, “chronic venous disease”, “venous leg ulcer”, “ulcer pain”, “nociceptive”, “neuropathic”, “nociplastic”, and “pathophysiology”. Boolean operators and filters were applied to refine results for peer-reviewed original studies, reviews, and clinical guidelines. Reference lists of retrieved articles were also screened to identify additional relevant publications.
Eligibility Criteria
Eligible studies were those that provided information on:
- Pathophysiology of vascular pain (ischemia, microvascular dysfunction, neuroinflammation, nociplastic mechanisms).
- Clinical characteristics of pain in VLUs, including prevalence, severity, and patient-reported outcomes.
- Diagnostic approaches integrating vascular and pain assessment.
- Management strategies, including conservative, pharmacological, interventional, and bioengineering-based approaches.
Both clinical and translational studies were considered. Publications not written in English, conference abstracts without full text, and case reports without broader contextual discussion were excluded.
Data Extraction and Synthesis
Two authors independently (MLGL, GF) reviewed titles and abstracts for relevance. Full texts of eligible studies were then examined, and relevant data were extracted into structured tables that included study design, population characteristics, main findings, and implications for vascular pain management. Emphasis was placed on identifying recurrent themes across studies rather than conducting quantitative synthesis, in line with the objectives of a narrative review.
Quality Considerations and Scientific Reasoning
Although no formal risk-of-bias assessment was performed (consistent with the narrative design), care was taken to prioritize high-quality peer-reviewed sources, recent systematic reviews, clinical practice guidelines, and original studies with robust methodology. In accordance with SANRA item 3 (scientific reasoning), studies were critically appraised in terms of internal validity, external applicability, and consistency with existing evidence. Where contradictory findings emerged, these were explicitly discussed with a third researcher (GV) to avoid selective reporting.
Referencing and Transparency
All references were managed using a citation software, and reporting adhered to Vancouver style. Following SANRA item 6 (appropriate referencing), priority was given to recent (2020–2025) publications indexed in major scientific databases. When earlier landmark studies were cited, their relevance was justified in the context of historical or mechanistic insights.
Limitations of Methodology
As this is a narrative rather than a systematic review, potential limitations include selection bias, the absence of quantitative meta-analysis, and possible underrepresentation of non-English language studies. Nevertheless, the adoption of SANRA criteria, transparent description of the search process, and integration of multidisciplinary perspectives mitigate these concerns and strengthen the scientific validity of the review.
Results
Epidemiology and Patient-Reported Burden
Venous leg ulcers (VLUs), which comprise approximately 60–80% of all lower-limb ulcers, are closely linked to pain, impaired sleep, psychological morbidity, and functional limitations [12,13,14,15,16]. The impact of these symptoms is increasingly assessed using disease- and wound-specific patient-reported outcome measures (PROMs), including VEINES-QOL/Sym, VLU-QoL, Wound-QoL, and the Cardiff Wound Impact Schedule. These instruments capture pain-related interference and broader consequences on daily living, with measurement properties that, while variable, are generally acceptable for comparative analyses at the group level [17,18,19].
Pathophysiology of VLU Pain
Ambulatory venous hypertension propagates excessive pressure into the microcirculation, leading to capillary dilatation, leukocyte adhesion and degranulation, fibrin cuff deposition, and repeated episodes of hypoxia–reperfusion injury, which collectively maintain a state of chronic inflammation [20,21,22,23,24]. Mechanistic studies demonstrate that these processes increase local concentrations of protons, bradykinin, prostanoids, and proinflammatory cytokines, thereby sensitizing peripheral nociceptors and amplifying pain signaling. Over time, persistent inflammation, tissue edema, and repeated procedural trauma such as dressing changes perpetuate both continuous “background” and activity-related “incident” pain. Prolonged ulcer chronicity further contributes to neuropathic alterations and central sensitization, aggravating the pain phenotype [20,21,22,23,24,25,26,27].
Clinical Phenotype and Assessment
Patients with venous leg ulcers typically report a spectrum of pain manifestations, including persistent aching or burning sensations representing “background” pain, movement-evoked or position-dependent “incident” pain, and procedure-related exacerbations during interventions such as debridement or dressing changes [26]. Standardized numeric or visual analog scales remain the most widely applied tools to quantify intensity, while neuropathic screening instruments such as DN4 assist in identifying neuropathic descriptors when present [28]. Comprehensive pain assessment should be integrated with vascular evaluation, including CEAP classification, duplex ultrasonography, and objective arterial indices such as the ankle–brachial pressure index (ABPI), to ensure safe prescription of compression therapy [29,30,31]. Patient-reported outcome measures (PROMs) such as VEINES-QOL/Sym, the Cardiff Wound Impact Schedule (CWIS), and Wound-QoL are frequently employed in active VLUs to capture pain-related interference and broader quality-of-life impact [17,18,19].
Diagnostic Framework (Vascular and Wound)
Accurate diagnostic assessment is fundamental to the safe and effective management of venous leg ulcers (VLUs). All patients should undergo clinical staging using the CEAP classification (Clinical–Etiological–Anatomical–Pathophysiological), which provides a standardized framework for documenting disease severity and guiding intervention. Duplex ultrasonography remains the gold standard for mapping venous reflux and obstruction, enabling precise identification of superficial, deep, or perforator incompetence and informing decisions regarding endovenous or surgical correction [32,33]. In parallel, arterial evaluation is indispensable, as undiagnosed peripheral arterial disease (PAD) can render compression unsafe and increase the risk of ischemic complications [34]. The ankle–brachial pressure index (ABPI) is the most widely used screening tool, supplemented by toe pressure or transcutaneous oxygen tension in cases of arterial calcification, diabetes, or inconclusive results [35].
The European Society for Vascular Surgery (ESVS) 2022 guideline recommends target ankle interface pressures ≥40 mmHg for active VLUs, recognizing this as the therapeutic threshold for promoting venous return and accelerating healing [29]. In patients with mixed arterial–venous disease, modified or reduced compression is advised, while sustained compression is contraindicated if ankle pressure is <60 mmHg, toe pressure <30 mmHg, or ABPI <0.6 [24,26]. Evidence syntheses highlight inter-guideline variability in safety thresholds, with some recommendations adopting a more conservative cutoff of 0.8 for ABPI [30]. This variation underscores the need for individualized clinical judgment, close patient monitoring, and periodic reassessment during compression therapy.
Emerging studies suggest that dynamic pressure monitoring and novel smart textiles may improve safety and adherence, offering real-time feedback on interface pressures [36]. In addition, structured vascular assessment protocols that integrate duplex and ABPI testing into wound care pathways have been associated with earlier diagnosis of mixed disease and improved healing trajectories [37]. Overall, thorough vascular staging and arterial assessment remain cornerstones of evidence-based VLU care, ensuring that compression, the mainstay of therapy, is both safe and optimally effective.
Management Strategies for Pain in VLUs
1) Treat the cause to treat the pain
Pain in venous leg ulcers (VLUs) is intimately linked with underlying venous hypertension and superficial reflux. Thus, addressing the root pathology is central to alleviating pain. Early correction of superficial venous incompetence, whether by thermal (endovenous laser ablation, radiofrequency ablation) or non-thermal (mechanochemical ablation, cyanoacrylate closure) techniques, has been shown to accelerate healing and prolong ulcer-free survival when compared with deferred intervention. The landmark EVRA trial demonstrated that early ablation shortened time to ulcer healing and increased ulcer-free days, while subsequent cost-utility analyses in both UK and US healthcare contexts confirmed its cost-effectiveness [32,38,39,40]. Importantly, improvements in ulcer healing correlated with significant reductions in wound-related pain and meaningful gains in health-related quality of life (QoL) [41,42]. For patients in whom conventional compression is not tolerated or proves insufficient, intermittent pneumatic compression (IPC) has been identified as a useful adjunct, enhancing venous return and promoting healing while also providing symptomatic relief [29].
2) Compression: the cornerstone
Compression therapy remains the cornerstone of both ulcer healing and pain relief in VLU management. High-pressure multilayer or inelastic compression, achieving ankle interface pressures of approximately 40 mmHg, has consistently been associated with accelerated healing, reduced edema, and subsequent pain relief [29]. A range of systems is available, including multilayer wraps, short-stretch bandages, adjustable Velcro® devices, and two-piece compression garments [43,44,45]. The choice of modality should be guided not only by hemodynamic efficacy but also by patient comfort, mobility, and lifestyle factors, as adherence is the primary determinant of treatment success. Barriers to consistent wear include discomfort in hot weather, difficulty with donning and doffing, and dermatologic irritation. Structured patient education, individualized garment selection, and provision of donning/doffing aids have been shown to enhance adherence [46,47,48,49]. Exercise programs designed to improve calf-muscle pump function represent a valuable adjunct to compression, contributing modestly to improved ulcer healing and symptom reduction, though their long-term role in preventing recurrence remains insufficiently defined [29,50].
3) Local wound care to minimize procedure-related pain
Beyond background and incident pain, procedure-related pain, particularly during debridement and dressing changes, constitutes a significant burden for patients with VLUs. Topical anesthetic agents, most notably eutectic lidocaine–prilocaine cream (EMLA), applied 30–60 minutes before sharp or mechanical debridement, have demonstrated significant analgesic benefit in multiple randomized controlled trials [51,52,53,54]. Similarly, the use of ibuprofen-releasing foam dressings has been associated with clinically relevant reductions in pain intensity during wear, without compromising wound healing, with pooled analyses estimating numbers-needed-to-treat between five and seven [55,56,57]. Also, the use of an inhalational anesthetic has been suggested as topical analgesic in these patients [58]. Conversely, routine systemic antibiotic therapy is not recommended for uninfected ulcers, as it neither enhances healing nor alleviates pain, and carries unnecessary risks of resistance and adverse effects [29].
4) Systemic and adjuvant analgesia
For patients with persistent pain, a multimodal pharmacological approach is warranted. Baseline analgesia may include short-course non-steroidal anti-inflammatory drugs (NSAIDs) when tolerated. Weak opioids can be considered for short-term management of severe background or procedure-related pain but should always be prescribed with exit strategies to avoid dependence [59]. Importantly, some patients develop neuropathic pain features, in which case gabapentinoids or serotonin–norepinephrine reuptake inhibitors (e.g., duloxetine), together with lidocaine patch, may be beneficial [60]. Although high-quality, ulcer-specific analgesic trials are scarce, the extrapolation of general neuropathic pain management strategies is currently justified [18,26,48]. Non-pharmacological adjuncts, including leg elevation, optimization of sleep hygiene, and cognitive-behavioral interventions, provide additional benefit, highlighting the need for individualized, multidisciplinary care [8,61].
5) Venoactive drugs (adjuncts)
Venoactive drugs, particularly micronized purified flavonoid fraction (MPFF), have demonstrated modest benefits in reducing venous symptoms such as pain, heaviness, and swelling. Randomized controlled trials and meta-analyses suggest that MPFF, when added to compression, may slightly increase ulcer healing rates and improve patient-reported symptoms [62,63,64]. However, guideline recommendations remain cautious, advocating their use only as adjuncts rather than replacements for compression and definitive reflux correction [29].

Quality of Life, Adherence, and Person-Centered Care
Pain in VLUs is not only a localised problem but also a systemic driver of functional decline, contributing to immobility, sleep disturbance, psychological distress, and social isolation [14,15,17,18,19]. Quality of life (QoL) has been shown to improve in parallel with ulcer healing and adequate symptom control, underscoring the importance of integrated pain management [18]. Patient-centered approaches, such as shared decision-making in compression modality, addressing practical barriers including footwear compatibility, climate-related discomfort, and donning/doffing challenges, and scheduling analgesia before dressing changes, have been shown to enhance adherence [46,47,48,49]. Structured self-care education, digital adherence tools, and multidisciplinary support further improve patient engagement, long-term outcomes, and recurrence prevention [65,66].
Special Populations and Comorbidity
Older adults living with VLUs frequently present with multidimensional symptom clusters, most notably persistent pain, chronic fatigue, and sleep disturbance, which interact synergistically to exacerbate disability and psychological distress. These clinical manifestations are often accompanied by elevated systemic inflammatory markers, reflecting the interplay between local ulcer pathology and systemic immune activation. Such complexity highlights the necessity for holistic, multidisciplinary management, integrating vascular care, targeted pain control, rehabilitation strategies, and psychosocial support to optimize healing, maintain functional independence, and enhance quality of life in this vulnerable population [35,67].
Evidence Gaps and Future Directions
Despite advances in the management of VLUs, several important research gaps persist. First, there is a striking lack of rigorous randomized controlled trials specifically addressing neuropathic and nociplastic pain phenotypes in VLUs, despite evidence that a subset of patients displays neuropathic descriptors and central sensitization [18,26,48]. Second, current VLU trials rarely incorporate standardized pain endpoints, limiting comparability across studies and hindering the development of evidence-based analgesic strategies [54,56]. Third, the comparative effectiveness of different compression modalities on pain outcomes remains poorly defined; while multilayer and inelastic bandages are widely studied, data on adjustable devices and smart compression garments are scarce [29,48,50]. Equally important is the need for scalable adherence interventions, such as digital adherence coaching, remote monitoring, and sensor-enabled compression systems, which may improve long-term engagement and outcomes [66,68]. Finally, further validation of wound-specific patient-reported outcome measures (PROMs), including their responsiveness to pain change in active VLUs, is required to ensure accurate assessment in both clinical practice and trials [18,21,29]. Addressing these gaps through targeted research will be crucial to advancing patient-centered, mechanism-based care.
Limitations of This Review
This narrative review has several important limitations that must be acknowledged. First, by design, it does not employ the systematic methodology of a meta-analysis; therefore, risks of selection bias and incomplete retrieval of relevant studies cannot be excluded, despite a broad search strategy and transparent reporting in accordance with SANRA criteria. Second, the inclusion of predominantly English-language publications may have introduced language bias and underrepresentation of valuable evidence from non-English sources. Third, although emphasis was placed on recent high-quality guidelines, randomized controlled trials, and systematic reviews, the heterogeneity of available data, particularly regarding pain endpoints, limits the ability to draw firm conclusions about comparative efficacy. Fourth, most studies addressing VLUs pain are secondary analyses of healing-focused trials, rather than rigorously designed pain studies, resulting in underpowered or inconsistent pain outcomes. Similarly, variability in outcome measures and patient-reported instruments hinders comparability across studies. Finally, while multidisciplinary perspectives were integrated, this review inevitably reflects the interpretive synthesis of the authors and may not encompass all nuances of clinical practice globally. Future systematic reviews and dedicated trials with standardized pain outcomes are required to confirm and extend the findings summarized herein.
Conclusions
VLU pain is prevalent, mechanistically complex, and clinically consequential. Effective pain control hinges on treating venous pathophysiology (compression, early ablation), minimizing procedure-related pain (topical local anesthetics, atraumatic care), and individualizing systemic/adjunctive therapy—all delivered within a person-centered program that optimizes adherence. Embedding robust pain endpoints in future VLU trials will sharpen guidance and improve patient-level outcomes.
Author Contributions
GV had the initial idea; bibliographic research and first draft are due to MLGL, GF, GV; the revision of the initial manuscript was made by AAAA and MRG. All the authors have equally participated to obtain the final version and accepted it for the submission.
Acknowledgments
The authors are grateful to Fondazione Paolo Procacci for the support during the publication phases. Secretarial support and coordination were possible because of it.
Conflicts of Interest
None of the authors has conflict of interest to declare, in relation to this manuscript.
Ethical approval
Not necessary for this research.
References
- Stanek A, Mosti G, Nematillaevich TS, Valesky EM, Planinšek Ručigaj T, Boucelma M, Marakomichelakis G, Liew A, Fazeli B, Catalano M, Patel M. No More Venous Ulcers-What More Can We Do? J Clin Med. 2023 Sep 23;12(19):6153. [CrossRef]
- Attaran RR, Edwards ML, Arena FJ, Bunte MC, Carr JG, Castro-Dominguez Y, Espinoza A, Feldman DN, Firestone S, Fukaya E, Harth K. 2025 SCAI Clinical Practice Guidelines for the Management of Chronic Venous Disease: This statement was endorsed by the Society for Vascular Medicine (SVM). J Soc Cardiovasc Angiogr Interv. 2025 Jun 30:103729. [CrossRef]
- Sussman C, Bates-Jensen B. Management of wound pain. Wound Care: A Collaborative Practice Manual for Health Professionals. 3rd ed. Philadelphia, PA: Lippincott Williams & Wilkins. 2007.
- O’Donnell TF Jr, Passman MA, Marston WA, Ennis WJ, Dalsing M, Kistner RL, Lurie F, Henke PK, Gloviczki ML, Eklöf BG, Stoughton J, Raju S, Shortell CK, Raffetto JD, Partsch H, Pounds LC, Cummings ME, Gillespie DL, McLafferty RB, Murad MH, Wakefield TW, Gloviczki P; Society for Vascular Surgery; American Venous Forum. Management of venous leg ulcers: clinical practice guidelines of the Society for Vascular Surgery ® and the American Venous Forum. J Vasc Surg. 2014 Aug;60(2 Suppl):3S-59S. [CrossRef]
- Hofmann AG, Deinsberger J, Oszwald A, Weber B. The Histopathology of Leg Ulcers. Dermatopathology (Basel). 2024 Jan 29;11(1):62-78. [CrossRef]
- Probst S, Schobinger E, Saini C, Larkin P, Bobbink P. Unveiling the hidden pain and daily struggles of individuals with a venous leg ulcer: a thematic analysis. J Tissue Viability. 2025 Aug;34(3):100906. [CrossRef]
- Weir D, Davies P. The impact of venous leg ulcers on a patient’s quality of life: considerations for dressing selection. Wounds Int. 2023 Feb 7;14(1):36-41. Available at: https://www.molnlycke.co.nz/SysSiteAssets/master-and-local-markets/documents/master/wound-care-documents/vlu/wint14-1_davies-web.pdf.
- Todd M. Assessment and management of older people with venous leg ulcers. Nurs Older People. 2018 Jul 26;30(5):39-48. [CrossRef]
- Jia H, Tan Y, Li H, Bu X, Li L, Lei X. A nomogram model for predicting risk factors and the outcome of skin ulcer. Ann Med. 2025 Dec;57(1):2525404. [CrossRef]
- Ketteler E, Cavanagh SL, Gifford E, Grunebach H, Joshi GP, Katwala P, Kwon J, McCoy S, McGinigle KL, Schwenk ES, Shutze WP, Vaglienti RM, Rossi P. The Society for Vascular Surgery expert consensus statement on pain management for vascular surgery diseases and interventions. J Vasc Surg. 2025 Jul;82(1):1-31.e2. [CrossRef]
- Baethge C, Goldbeck-Wood S, Mertens S. SANRA-a scale for the quality assessment of narrative review articles. Res Integr Peer Rev. 2019 Mar 26;4:5. [CrossRef]
- Lim CS, Baruah M, Bahia SS. Diagnosis and management of venous leg ulcers. BMJ. 2018 Aug 14;362:k3115. [CrossRef]
- Liu S, Team V, Qiu Y, Weller CD. Measurement properties of quality of life instruments for adults with active venous leg ulcers: a systematic review protocol. Wound Practice & Research: J Austr Wound Man Ass. 2021 Jun 1;29(2):104-9. [CrossRef]
- Liu S, Team V, Qiu Y, Weller CD. Investigating quality of life instrument measurement properties for adults with active venous leg ulcers: A systematic review. Wound Repair Regen. 2022 Jul;30(4):468-486. [CrossRef]
- Olsson M, Wadin L, Åhlén J, Friman A. A qualitative study of patients’ experiences of living with hard-to-heal leg ulcers. Br J Community Nurs. 2023 Jun 1;28(Sup6):S8-S13. [CrossRef]
- Probst S, Saini C, Gschwind G, Stefanelli A, Bobbink P, Pugliese MT, Cekic S, Pastor D, Gethin G. Prevalence and incidence of venous leg ulcers-A systematic review and meta-analysis. Int Wound J. 2023 Nov;20(9):3906-3921. [CrossRef]
- Price P, Harding K. Cardiff Wound Impact Schedule: the development of a condition-specific questionnaire to assess health-related quality of life in patients with chronic wounds of the lower limb. Int Wound J. 2004 Apr;1(1):10-7. [CrossRef]
- Bland JM, Dumville JC, Ashby RL, Gabe R, Stubbs N, Adderley U, Kang’ombe AR, Cullum NA. Validation of the VEINES-QOL quality of life instrument in venous leg ulcers: repeatability and validity study embedded in a randomised clinical trial. BMC Cardiovasc Disord. 2015 Aug 11;15(1):85. [CrossRef]
- Granado-Casas M, Martinez-Gonzalez D, Martínez-Alonso M, Dòria M, Alcubierre N, Valls J, Julve J, Verdú-Soriano J, Mauricio D. Psychometric Validation of the Cardiff Wound Impact Schedule Questionnaire in a Spanish Population with Diabetic Foot Ulcer. J Clin Med. 2021 Sep 6;10(17):4023. [CrossRef]
- Saharay M, Shields DA, Porter JB, Scurr JH, Coleridge Smith PD. Leukocyte activity in the microcirculation of the leg in patients with chronic venous disease. J Vasc Surg. 1997 Aug;26(2):265-73. [CrossRef]
- Raffetto JD, Ligi D, Maniscalco R, Khalil RA, Mannello F. Why Venous Leg Ulcers Have Difficulty Healing: Overview on Pathophysiology, Clinical Consequences, and Treatment. J Clin Med. 2020 Dec 24;10(1):29. [CrossRef]
- Attaran RR, Carr JG. Chronic Venous Disease of the Lower Extremities: A State-of-the Art Review. J Soc Cardiovasc Angiogr Interv. 2022 Nov 26;2(1):100538. [CrossRef]
- Coelho GA, Secretan PH, Tortolano L, Charvet L, Yagoubi N. Evolution of the Chronic Venous Leg Ulcer Microenvironment and Its Impact on Medical Devices and Wound Care Therapies. J Clin Med. 2023 Aug 28;12(17):5605. [CrossRef]
- Krizanova O, Penesova A, Hokynkova A, Pokorna A, Samadian A, Babula P. Chronic venous insufficiency and venous leg ulcers: Aetiology, on the pathophysiology-based treatment. Int Wound J. 2023 Oct 19;21(2):e14405. [CrossRef]
- Hart O, Adeane S, Vasudevan T, van der Werf B, Khashram M. The utility of hyperspectral imaging in patients with chronic venous disorders. J Vasc Surg Venous Lymphat Disord. 2022 Nov;10(6):1325-1333.e3. [CrossRef]
- Leren L, Johansen E, Eide H, Falk RS, Juvet LK, Ljoså TM. Pain in persons with chronic venous leg ulcers: A systematic review and meta-analysis. Int Wound J. 2020 Apr;17(2):466-484. [CrossRef]
- Mayrovitz HN, Wong S, Mancuso C. Venous, Arterial, and Neuropathic Leg Ulcers with Emphasis on the Geriatric Population. Cureus. 2023 Apr 25;15(4):e38123. [CrossRef]
- Pan Q, Zhai X, Wang H, Du J, Shi Y, Yu X, Yan S, Wu X, Li HH, Sun T, Guo L, Zhao J, Fan B. Real-World Pharmacological Treatment Pattern of Neuropathic Pain in China: A Retrospective, Database, Multicenter Study (ReTARdant) Protocol. Pain Ther. 2025 Aug 11. [CrossRef]
- De Maeseneer MG, Kakkos SK, Aherne T, Baekgaard N, Black S, Blomgren L, Giannoukas A, Gohel M, de Graaf R, Hamel-Desnos C, Jawien A, Jaworucka-Kaczorowska A, Lattimer CR, Mosti G, Noppeney T, van Rijn MJ, Stansby G, Esvs Guidelines Committee, Kolh P, Bastos Goncalves F, Chakfé N, Coscas R, de Borst GJ, Dias NV, Hinchliffe RJ, Koncar IB, Lindholt JS, Trimarchi S, Tulamo R, Twine CP, Vermassen F, Wanhainen A, Document Reviewers, Björck M, Labropoulos N, Lurie F, Mansilha A, Nyamekye IK, Ramirez Ortega M, Ulloa JH, Urbanek T, van Rij AM, Vuylsteke ME. Editor’s Choice - European Society for Vascular Surgery (ESVS) 2022 Clinical Practice Guidelines on the Management of Chronic Venous Disease of the Lower Limbs. Eur J Vasc Endovasc Surg. 2022 Feb;63(2):184-267. Epub 2022 Jan 11. Erratum in: Eur J Vasc Endovasc Surg. 2022 Aug-Sep;64(2-3):284-285. doi: 10.1016/j.ejvs.2022.05.044. [CrossRef]
- Valesky EM, Hach-Wunderle V, Protz K, Zeiner KN, Erfurt-Berge C, Goedecke F, Jäger B, Kahle B, Kluess H, Knestele M, Kuntz A, Lüdemann C, Meissner M, Mühlberg K, Mühlberger D, Pannier F, Schmedt CG, Schmitz-Rixen T, Strölin A, Wilm S, Rabe E, Stücker M, Dissemond J. Diagnosis and treatment of venous leg ulcers: S2k Guideline of the German Society of Phlebology and Lymphology (DGPL) e.V. J Dtsch Dermatol Ges. 2024 Jul;22(7):1039-1051. [CrossRef]
- Weller CD, Team V, Ivory JD, Crawford K, Gethin G. ABPI reporting and compression recommendations in global clinical practice guidelines on venous leg ulcer management: A scoping review. Int Wound J. 2019 Apr;16(2):406-419. Epub 2018 Nov 28. Erratum in: Int Wound J. 2019 Aug;16(4):1074. doi: 10.1111/iwj.13165. [CrossRef]
- Gohel MS, Mora MSc J, Szigeti M, Epstein DM, Heatley F, Bradbury A, Bulbulia R, Cullum N, Nyamekye I, Poskitt KR, Renton S, Warwick J, Davies AH; Early Venous Reflux Ablation Trial Group. Long-term Clinical and Cost-effectiveness of Early Endovenous Ablation in Venous Ulceration: A Randomized Clinical Trial. JAMA Surg. 2020 Dec 1;155(12):1113-1121. [CrossRef]
- Shawa HJ, Dahle SE, Isseroff RR. Consistent application of compression: An under-considered variable in the prevention of venous leg ulcers. Wound Rep Reg. 2023 May;31(3):393-400. [CrossRef]
- Weller C, Richards C, Turnour L, Green S, Team V. Vascular assessment in venous leg ulcer diagnostics and management in Australian primary care: Clinician experiences. J Tissue Viability. 2020 Aug;29(3):184-189. [CrossRef]
- Winders S, Lyon DE, Kelly DL, Weaver MT, Yi F, Rezende de Carvalho M, Stechmiller JK. Sleep, Fatigue, and Inflammatory Biomarkers in Older Adults with Chronic Venous Leg Ulcers Receiving Intensive Outpatient Wound Care. Adv Wound Care (New Rochelle). 2024 Oct;13(10):508-517. [CrossRef]
- Nair HK, Mosti G, Atkin L, Aburn R, Ali Hussin N, Govindarajanthran N, Narayanan S, Ritchie G, Samuriwo R, Sandy-Hodgetts K, Smart H, Sussman G, Ehmann S, Lantis J, Moffatt C, Naude L, Probst S, White W. Leg ulceration in venous and arteriovenous insufficiency: assessment and management with compression therapy as part of a holistic wound-healing strategy. J Wound Care. 2024 Oct 1;33(Sup10b):S1-S31. [CrossRef]
- Epstein DM, Gohel MS, Heatley F, Liu X, Bradbury A, Bulbulia R, Cullum N, Nyamekye I, Poskitt KR, Renton S, Warwick J, Davies AH; EVRA trial investigators. Cost-effectiveness analysis of a randomized clinical trial of early versus deferred endovenous ablation of superficial venous reflux in patients with venous ulceration. Br J Surg. 2019 Apr;106(5):555-562. [CrossRef]
- Gohel MS, Heatley F, Liu X, Bradbury A, Bulbulia R, Cullum N, Epstein DM, Nyamekye I, Poskitt KR, Renton S, Warwick J, Davies AH; EVRA Trial Investigators. A Randomized Trial of Early Endovenous Ablation in Venous Ulceration. N Engl J Med. 2018 May 31;378(22):2105-2114. [CrossRef]
- Zheng H, Magee GA, Tan TW, Armstrong DG, Padula WV. Cost-effectiveness of Compression Therapy With Early Endovenous Ablation in Venous Ulceration for a Medicare Population. JAMA Netw Open. 2022 Dec 1;5(12):e2248152. [CrossRef]
- Cai PL, Hitchman LH, Mohamed AH, Smith GE, Chetter I, Carradice D. Endovenous ablation for venous leg ulcers. Cochrane Database Syst Rev. 2023 Jul 27;7(7):CD009494. [CrossRef]
- Franks PJ, Morgan PA. Health-related quality of life with chronic leg ulceration. Expert Rev Pharmacoecon Outcomes Res. 2003 Oct;3(5):611-22. [CrossRef]
- Holloway S, Ahmajärvi K, Frescos N, Jenkins S, Oropallo A, Slezáková S, Pokorná A, Coaccioli S, Colwill A, Woo K. Holistic management of wound-related pain: an overview of the evidence and recommendations for clinical practice. J Wound Man. 2024 Apr 1;25(1). [CrossRef]
- Dissemond J, Schicker C, Breitfeld T, Keuthage W, Häuser E, Möller U, Thomassin L, Stücker M. An innovative multicomponent compression system in a single bandage for venous leg ulcer and/or oedema treatment: a real-life study in 343 patients. J Wound Care. 2025 Jan 2;34(1):31-46. [CrossRef]
- Ruiz MJS, Moll NV, Gálvez MM, Jiménez MG, Muñoz LA. Compression therapy in patients with venous leg ulcers: a best practice implementation project. JBI Evid Implement. 2025 Jul 1;23(3):256-264. [CrossRef]
- Nair HKR, Bin Othman AF, Hariz Bin Ramli AR, Bin Md Idris MA, Azmi NM, Jaafar MA. Utilizing the adjustable Velcro system Compreflex® for patients with chronic venous leg ulcers: An observational multicenter clinical follow-up study. Phlebology. 2025 Jul 20:2683555251357361. [CrossRef]
- Buset CS, Fleischer J, Kluge R, Graf NT, Mosti G, Partsch H, Seeli C, Anzengruber F, Kockaert M, Hübner M, Hafner J. Compression Stocking With 100% Donning and Doffing Success: An Open Label Randomised Controlled Trial. Eur J Vasc Endovasc Surg. 2021 Jan;61(1):137-144. [CrossRef]
- Weller CD, Richards C, Turnour L, Team V. Patient Explanation of Adherence and Non-Adherence to Venous Leg Ulcer Treatment: A Qualitative Study. Front Pharmacol. 2021 Jun 3;12:663570. [CrossRef]
- Bar L, Brandis S, Marks D. Improving Adherence to Wearing Compression Stockings for Chronic Venous Insufficiency and Venous Leg Ulcers: A Scoping Review. Pat Prefer Adher. 2021 Sep 17;15:2085-2102. [CrossRef]
- Perry C, Atkinson RA, Griffiths J, Wilson PM, Lavallée JF, Cullum N, Dumville JC. Barriers and facilitators to use of compression therapy by people with venous leg ulcers: A qualitative exploration. J Adv Nurs. 2023 Jul;79(7):2568-2584. [CrossRef]
- Turner BRH, Jasionowska S, Machin M, Javed A, Gwozdz AM, Shalhoub J, Onida S, Davies AH. Systematic review and meta-analysis of exercise therapy for venous leg ulcer healing and recurrence. J Vasc Surg Venous Lymphat Disord. 2023 Jan;11(1):219-226. [CrossRef]
- Holm J, Andrén B, Grafford K. Pain control in the surgical debridement of leg ulcers by the use of a topical lidocaine--prilocaine cream, EMLA. Acta Derm Venereol. 1990;70(2):132-6. PMID: 1969197.
- Lok C, Paul C, Amblard P, Bessis D, Debure C, Faivre B, Guillot B, Ortonne JP, Huledal G, Kalis B. EMLA cream as a topical anesthetic for the repeated mechanical debridement of venous leg ulcers: a double-blind, placebo-controlled study. J Am Acad Dermatol. 1999 Feb;40(2 Pt 1):208-13. [CrossRef]
- Rosenthal D, Murphy F, Gottschalk R, Baxter M, Lycka B, Nevin K. Using a topical anaesthetic cream to reduce pain during sharp debridement of chronic leg ulcers. J Wound Care. 2001 Jan;10(1):503-5. [CrossRef]
- Briggs M, Nelson EA, Martyn-St James M. Topical agents or dressings for pain in venous leg ulcers. Cochrane Database Syst Rev. 2012 Nov 14;11(11):CD001177. [CrossRef]
- Jørgensen B, Friis GJ, Gottrup F. Pain and quality of life for patients with venous leg ulcers: proof of concept of the efficacy of Biatain-Ibu, a new pain reducing wound dressing. Wound Repair Regen. 2006 May-Jun;14(3):233-9. [CrossRef]
- Gottrup F, Jørgensen B, Karlsmark T, Sibbald RG, Rimdeika R, Harding K, Price P, Venning V, Vowden P, Jünger M, Wortmann S, Sulcaite R, Vilkevicius G, Ahokas TL, Ettler K, Arenbergerova M. Less pain with Biatain-Ibu: initial findings from a randomised, controlled, double-blind clinical investigation on painful venous leg ulcers. Int Wound J. 2007 Apr;4 Suppl 1(Suppl 1):24-34. [CrossRef]
- Fogh K, Andersen MB, Bischoff-Mikkelsen M, Bause R, Zutt M, Schilling S, Schmutz JL, Borbujo J, Jimenez JA, Cartier H, Jørgensen B. Clinically relevant pain relief with an ibuprofen-releasing foam dressing: results from a randomized, controlled, double-blind clinical trial in exuding, painful venous leg ulcers. Wound Repair Regen. 2012 Nov-Dec;20(6):815-21. [CrossRef]
- Imbernon-Moya A, Ortiz-de Frutos FJ, Sanjuan-Alvarez M, Portero-Sanchez I, Merinero-Palomares R, Alcazar V. Pain and analgesic drugs in chronic venous ulcers with topical sevoflurane use. J Vasc Surg. 2018 Sep;68(3):830-835. [CrossRef]
- Latina R, Varrassi G, Di Biagio E, Giannarelli D, Gravante F, Paladini A, D’Angelo D, Iacorossi L, Martella C, Alvaro R, Ivziku D, Veronese N, Barbagallo M, Marchetti A, Notaro P, Terrenato I, Tarsitani G, De Marinis MG. Chronic Non-cancer Pain Management in a Tertiary Pain Clinic Network: a Retrospective Study. Pain Ther. 2023 Feb;12(1):151-164. Epub 2022 Oct 17. Erratum in: Pain Ther. 2023 Jun;12(3):891-892. doi: 10.1007/s40122-023-00503-3. [CrossRef]
- Nalamachu S, Mallick-Searle T, Adler J, Chan EK, Borgersen W, Lissin D. Multimodal Therapies for the Treatment of Neuropathic Pain: The Role of Lidocaine Patches in Combination Therapy: A Narrative Review. Pain Ther. 2025 Jun;14(3):865-879. [CrossRef]
- Simon DA, Dix FP, McCollum CN. Management of venous leg ulcers. BMJ. 2004 Jun 5;328(7452):1358-62. [CrossRef]
- Scallon C, Bell-Syer SE, Aziz Z. Flavonoids for treating venous leg ulcers. Cochrane Database Syst Rev. 2013 May 31;2013(5):CD006477. [CrossRef]
- Li KX, Diendéré G, Galanaud JP, Mahjoub N, Kahn SR. Micronized purified flavonoid fraction for the treatment of chronic venous insufficiency, with a focus on postthrombotic syndrome: A narrative review. Res Pract Thromb Haemost. 2021 May 8;5(4):e12527. [CrossRef]
- Gianesini S, De Luca L, Feodor T, Taha W, Bozkurt K, Lurie F. Cardiovascular Insights for the Appropriate Management of Chronic Venous Disease: A Narrative Review of Implications for the Use of Venoactive Drugs. Adv Ther. 2023 Dec;40(12):5137-5154. [CrossRef]
- Pasek J, Szajkowski S, Cieślar G. Quality of Life in Patients with Venous Leg Ulcers Treated by Means of Local Hyperbaric Oxygen Therapy or Local Ozone Therapy-A Single Center Study. Medicina (Kaunas). 2023 Nov 24;59(12):2071. [CrossRef]
- Weller CD, Buchbinder R, Johnston RV. Interventions for helping people adhere to compression treatments for venous leg ulceration. Cochrane Database Syst Rev. 2016 Mar 2;3(3):CD008378. [CrossRef]
- Kim J, Stechmiller J, Weaver M, James G, Stewart PS, Lyon D. Associations Among Wound-Related Factors Including Biofilm, Wound-Related Symptoms and Systemic Inflammation in Older Adults with Chronic Venous Leg Ulcers. Adv Wound Care (New Rochelle). 2024 Oct;13(10):518-527. [CrossRef]
- Guest JF, Gerrish A, Ayoub N, Vowden K, Vowden P. Clinical outcomes and cost-effectiveness of three alternative compression systems used in the management of venous leg ulcers. Journal of wound care. 2015 Jul 2;24(7):300-10. [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



