Submitted:
01 September 2025
Posted:
02 September 2025
You are already at the latest version
Abstract
Background: Preterm infants are at high risk of osteopenia of prematurity (OOP) due to interrupted third-trimester mineral accretion and early postnatal deficits. Aim: To synthesize recent evidence on nutritional strategies—especially early, fortified enteral feeding—to prevent OOP, with emphasis on early fortified enteral feeding. Design: Narrative review (SANRA‑guided) with a structured, reproducible search of PubMed, Scopus, and Google Scholar (January 2010 – June 2025); English/Polish; human neonatal data prioritized; mechanistic/animal data used for context. Findings: Across cohorts, early fortified human milk (typical Ca:P ≈ 1.6–1.8 with adequate protein and vitamin D) correlates with improved biochemical markers and lower OOP incidence versus unfortified feeds; prolonged PN (Parenteral Nutrition) and delayed enteral advancement are linked to higher OOP risk; unit‑level protocols that optimize Ca:P delivery from day 1 and routine HMF (Human Milk Fortifier) use reduce MBD incidence. Evidence is heterogeneous in definitions and outcomes, precluding meta‑analysis. Conclusions: Timely transition to fortified enteral nutrition with judicious mineral/vitamin D supplementation is central to OOP prevention. Standardized definitions, multicenter protocols, and longitudinal follow‑up are needed to clarify long‑term skeletal benefits.
Keywords:
preterm infants
; osteopenia of prematurity
; enteral nutrition
; parenteral nutrition
; human milk fortifier
; calcium-to-phosphorus ratio
; vitamin D
; narrative review
1. Introduction
Nutritional treatment, often referred to as clinical nutrition, is a medical approach that involves delivering tailored nutritional formulations based on biochemical assessments and the patient’s overall health condition. This process also encompasses the monitoring of the patient’s nutritional status using appropriate medical equipment. Clinical nutrition is particularly crucial for individuals who are malnourished or at risk of malnutrition, especially in cases where oral intake is either not feasible or compromised [1].
Preterm infants – especially those with very low birth weight – are at high risk for osteopenia of prematurity, also known as metabolic bone disease of prematurity. This condition arises from inadequate mineral accretion due to the interruption of third-trimester calcium and phosphate transfer, compounded by postnatal nutritional deficits [2]. Even with advances in neonatal care, radiographic evidence of bone demineralization is observed in up to ~40% of infants born before 28 weeks’ gestation. Recent reports indicate that the incidence of metabolic bone disease reaches ~32% in very low birth weight (VLBW) preterm infants and over 50% in those of extremely low birth weight. Osteopenia in these infants can lead to fractures and rickets in early life and may have longer-term consequences such as impaired skeletal growth and suboptimal peak bone mass, underscoring the need for effective preventive strategies [3].
Optimal nutrition in the neonatal period is widely recognized as a key modifiable factor in preventing osteopenia of prematurity. The primary approach to prevention and treatment centers on ensuring adequate mineral intake – principally calcium (Ca), phosphorus (P), and vitamin D – to approximate in utero accretion rates and support bone mineralization. However, unfortified human milk alone contains insufficient quantities of Ca and P to meet preterm infants’ needs. Thus, current practice relies on human milk fortification and the use of mineral-enriched preterm formulas to provide the necessary nutrient density. These nutritional interventions have markedly reduced the incidence of severe metabolic bone disease (for example, lowering the frequency of spontaneous fractures), yet mild to moderate osteopenic changes on X-rays remain common. Furthermore, there is no consensus on the optimal monitoring or bedside assessment of bone mineral status in preterm infants, reflecting persistent uncertainty in clinical management despite standard supplementation protocols [4,5].
Recent research and reviews highlight both progress and continuing gaps in our understanding of nutritional strategies to prevent osteopenia in preterm infants. Notably, expert consensus guidelines now advocate for earlier and more aggressive nutritional fortification. For example, it is recommended to initiate enteral fortification early, adding supplemental phosphate within the first days of feeding and introducing multi-component human milk fortifiers as soon as minimal feed volumes are tolerated, to support bone mineral accrual better. Early transition from parenteral nutrition to fortified enteral feeds is also emphasized, as high protein and caloric intake without adequate phosphate provision can precipitate increased cellular phosphate utilization and mineral deficiency. At the same time, the evidence base guiding these practices remains limited. Only a single randomized trial has followed preterm infants into adulthood after differing neonatal mineral intakes, and it found no significant effect of higher calcium/phosphorus intake on adult bone mineral content. Important knowledge gaps persist regarding nutrient interactions and optimal fortification methods: for instance, how the interplay of macronutrient intake with mineral supply affects bone deposition, or how best to individualize fortification to an infant’s needs, are questions that existing studies have not fully answered. In addition, long-term skeletal outcomes of current nutritional interventions are poorly documented. These gaps point to the need for a dedicated analysis of current evidence and an updated framework for nutritional care focused on bone health [6].
In light of the above, a focused review of nutritional strategies to prevent osteopenia in preterm infants is warranted. The present review critically examines recent advances and unresolved issues in the nutritional management of at-risk preterm neonates – including mineral supplementation regimens, human milk fortification strategies, and the timing of enteral feeding – with an emphasis on aspects that have been underrepresented in prior literature (such as nutrient–nutrient interactions, fortification protocols, and long-term outcomes). The objective is to elucidate effective early nutritional interventions and inform best practices for reducing osteopenia of prematurity. We hypothesize that the early introduction of enteral feeding enriched with human milk fortifier (HMF) in preterm infants will reduce the prevalence of osteopenia, thereby improving both immediate and long-term skeletal health outcomes in this vulnerable population.
2. Materials and Methods
Methods — Design and reporting: This narrative review follows SANRA recommendations to enhance transparency. We implemented structured, reproducible search methods (without claiming a PRISMA-compliant systematic review), prespecified eligibility criteria, duplicate screening, and an explicit search flow diagram labeled ‘Search flow diagram (narrative review)’. Given substantial heterogeneity in populations, interventions, and OOP definitions/outcomes, no meta-analysis was undertaken. A concise, design-appropriate quality appraisal using JBI/NOS-style domains is summarized in Table S2 to aid interpretation.
Design rationale: This review was planned as a narrative synthesis rather than a systematic review because the topic integrates heterogeneous designs (clinical cohorts, QI initiatives, animal models, and guidelines). We followed SANRA to enhance transparency and quality. To aid reproducibility, we provide a PRISMA-style flow diagram with counts of records at each stage and explicitly separate human from non-human evidence. No formal risk-of-bias tool was applied; key limitations are discussed (Figure 1).
Literature Search Strategy
We performed a structured literature search to identify relevant publications on nutrition and osteopenia of prematurity. The primary databases searched were PubMed/MEDLINE, Scopus, and Google Scholar, covering both medical indexing sources and broad academic search engines. The search spanned articles published from January 2010 up to June 2025. We used various combinations of keywords related to preterm infants, bone health, and nutrition. For example, search terms included “osteopenia of prematurity”, “nutritional treatment”, “enteral nutrition in preterm”, “calcium to phosphorus ratio”, “vitamin D supplementation in premature neonates”, “ω3 fatty acids and bone density”, “zinc and vitamin D in preterm infants”, and “maternal factors of osteopenia in neonates”. These terms were applied in different combinations using Boolean operators to capture studies on nutritional interventions (e.g., human milk fortifiers, specialized formulas, parenteral nutrition regimens) and their effects on bone mineralization in preterm or low birth weight infants. We restricted the search to English and Polish language publications (as the authors are proficient in these languages) and excluded papers in other languages. To ensure the review was up-to-date and inclusive, we also manually screened the reference lists of key articles identified in the database search for any additional relevant studies that may have been missed by the keyword search. This snowball strategy allowed us to include pertinent articles cited in the literature, including important older studies or specialized documents not easily found via database queries.
Inclusion and Exclusion Criteria
We established clear criteria for selecting studies a priori to maintain focus and relevance. Inclusion criteria were defined as follows:
- Time frame: Publications from 2010 onwards (January 2010 through June 2025) to capture the last 15 years of research and current knowledge.
- Population focus: Studies involving preterm infants (typically <37 weeks gestation or low birth weight neonates) with outcomes related to bone health, osteopenia of prematurity, or metabolic bone disease.
- Intervention/Exposure: Research examining nutritional factors or interventions – including enteral nutrition (e.g., breast milk fortification, preterm formulas, nutritional supplements), parenteral nutrition strategies, or specific nutrients (calcium, phosphorus, vitamin D, etc.) – and their impact on bone mineralization or the risk of osteopenia/rickets in the target population.
- Article types: Given the narrative scope, a wide range of scientific literature was eligible. This included peer-reviewed original research articles (randomized trials, observational cohort or case–control studies, cross-sectional studies), clinical reviews and meta - analyses, relevant animal studies providing mechanistic insight, clinical guidelines or protocols, and other authoritative sources (such as textbook chapters or official reports on neonatal nutrition), provided they contained pertinent data on nutrition and bone outcomes.
- Availability: Full-text access had to be available for assessment (through academic databases or institutional access), to ensure we could thoroughly review the methods and results.
- Exclusion criteria were applied to omit sources that were not relevant or of insufficient quality:
- Outside time frame: Articles published before 2010 (older than 15 years) were generally excluded, to focus on up-to-date evidence (unless identified as a seminal study in reference scanning).
- Language: Publications in languages other than English or Polish were excluded, due to the feasibility of analysis and to avoid translation-related biases.
- Non-peer-reviewed literature: We excluded letters to the editor, editorials, opinion pieces, and other non–non-peer-reviewed reports, as well as anecdotal case reports lacking robust data.
- Out-of-scope content: Studies that did not directly address the interplay between nutrition and bone health in preterm infants were excluded. For example, we omitted papers focused on technical complications of feeding (such as intravenous extravasation injuries during parenteral nutrition administration or methods of drug delivery via feeding tubes) and studies examining unrelated outcomes of enteral feeding (e.g., gastrointestinal complications not tied to bone metabolism). Such topics were beyond the scope of this review.
- Quality concerns: If a study’s methodology or data quality was notably poor or if essential details were unavailable, we chose to exclude it in order to base our review on reliable evidence. In practice, all included sources were screened to ensure they met a minimum standard of scientific credibility (clear objectives, appropriate methodology, and reasonable sample size or rationale).
Study Selection and Data Extraction
The process of article selection followed recommended practices to enhance reliability. After executing the searches, all retrieved records were imported into a reference management tool, and duplicates were removed. Two authors independently screened the titles and abstracts of the remaining records to identify articles that potentially met the inclusion criteria. Studies that clearly did not match the inclusion criteria (based on title/abstract) were excluded at this stage. For records that appeared relevant or ambiguous, we obtained and reviewed the full-text articles. Each full text was assessed in detail by at least two reviewers against the inclusion/exclusion criteria. Any disagreements or discrepancies in study inclusion were resolved through discussion and consensus among the reviewing authors, with consultation of a third author when necessary. This collaborative selection process helped minimize bias in choosing the literature for review.
From each included article, we then extracted key data to inform our narrative synthesis. The extracted information included the publication details (authors, year, journal), the study design and setting (e.g., RCT, observational cohort, animal experiment, guideline, etc.), the characteristics of the population (for clinical studies, such as sample size, gestational age and birth weight of infants), the specifics of the nutritional intervention or exposure (e.g., type of feeding regimen, nutrient supplementation levels, duration of nutrition given), and the relevant outcomes related to bone health (such as bone mineral density measurements, incidence of osteopenia or rickets, biochemical markers of bone metabolism, or fracture rates). We also noted the main findings and conclusions of each study with respect to how nutrition influenced skeletal outcomes in preterm infants. This information was tabulated and thematically organized to facilitate comparison across studies during the write-up of results.Throughout the extraction and synthesis, we paid special attention to the level of evidence provided by different sources – distinguishing, for instance, outcomes supported by clinical trials in human preterm infants from those observed only in animal models or inferred from adult data – to appropriately contextualize the strength of evidence. No formal quantitative meta-analysis was attempted, given the narrative scope and the anticipated heterogeneity in study designs and outcome measures across the literature.
3. Results—Focus and Human Evidence
We present human neonatal studies first (summarized in Table 1 and Table 2), followed by a brief mechanistic context (moved to Supplementary where peripheral).
Three consistent signals emerge: (i) early fortified enteral feeding improves bone markers/outcomes; (ii) prolonged PN and delayed enteral advancement are associated with OOP; (iii) optimized mineral delivery (Ca:P from day 1; routine HMF) reduces MBD incidence.
A total of 115 full-text articles meeting the eligibility criteria were included in the narrative synthesis. For presentation, findings are organized into clinical (human) studies and animal/experimental evidence. Definitions of osteopenia/metabolic bone disease varied across studies (e.g., biochemical thresholds such as ALP (alkaline phosphatase) > 500 IU/L or ALP > 900 IU/L, radiographic rickets, or DXA-based bone mineral content), which we note when reporting results.
Human Studies: Nutritional Interventions and Bone Outcomes
Across clinical studies (Table 1), three signals were consistent:
- Early fortified enteral feeding improves bone outcomes. In a comparison of preterm infants fed unfortified breast milk vs fortified/supplemented feeds, rickets occurred in 40% without fortification vs 16% with fortification; serum phosphate was lower in the unfortified group (Bandara 2010). In a NICU cohort, 41% had osteopenia at 1 month (ALP > 900 IU/L); lack of HMF and irregular/no vitamin D use were over-represented among osteopenic infants (Bijari 2019).
- Prolonged parenteral nutrition and delayed enteral advancement are associated with osteopenia. In a prospective series of <1250 g infants, osteopenia cases had longer TPN (Total Parenteral Nutrition) (≈ 11 vs 6 days), later transition to enteral feeding (≈ 27 vs 32 days) of enteral nutrition by 6 weeks), and lower protein intake (Mohamed 2020). A larger cohort of <30 weeks’ gestation infants reported 30.9% MBD with lower early Ca, P, vitamin D, and protein intakes, more PN exposure, and greater illness burden (Viswanathan 2014).
- Optimizing mineral delivery reduces MBD incidence. A unit-level quality-improvement program introducing higher Ca:P in TPN from day 1 and routine HMF from ~day 14 reduced MBD from 35% to <20% (Sureshchandra 2025).
Biochemical and clinical correlates were concordant: lower serum 25(OH)D (≈ 21 vs 39 ng/mL), higher ALP, and lower early Ca:P and protein intakes tracked with osteopenia; adverse outcomes included longer hospitalization and higher mortality in affected cohorts (e.g., 14.1% vs 4.4%, Viswanathan 2014). Where reported, nutrient targets associated with favorable markers included a Ca:P ratio ~1.6–1.8 in fortified feeds and protein ~3.5–4 g/kg/day.
Animal and Experimental Evidence
Experimental models provide mechanistic support for clinical observations. Diets enriched with ω-3 fatty acids (EPA/DHA) reduced urinary calcium losses and improved mineral retention vs control fats, consistent with lower prostaglandin-mediated renal calcium excretion. Protein–mineral interactions were also evidenced: whey protein facilitates intestinal zinc uptake; zinc inhibited osteoclastogenesis in vitro, supporting a role in reducing bone resorption. Vitamin D acted synergistically with minerals (and influenced zinc transporters), and severe vitamin D deficiency produced rachitic phenotypes unless calcium intake was adequate. Together, these studies reinforce the importance of balanced Ca:P delivery, adequate vitamin D, sufficient high-quality protein, and potentially ω-3 fatty acids for bone mineralization in the neonatal context. As these are non-human or non-preterm data, they should be interpreted as supporting mechanisms rather than direct clinical estimates.
3.1. Nutritional Treatment - Definition, Classification, Characteristics
Nutritional therapy is a form of treatment for patients who are unable to eat orally or do not consume adequate amounts of food. The two common types of nutritional treatment are enteral feeding, which involves delivering nutrients directly to the stomach or intestine, and parenteral feeding, which is administered intravenously [7].
Parenteral nutrition remains necessary in cases where enteral feeding is contraindicated, such as in necrotizing enterocolitis, congenital intestinal anomalies, or acute critical illness. Patients who are unable to eat orally but have a functional gastrointestinal tract, such as premature infants, receive their nutrition through a nasogastric tube, which is inserted through the nose into the stomach [2,7].
3.2. Osteopenia of Prematurity - Symptoms, Risk, Factors, Diagnosis
Osteopenia of prematurity is characterized by low levels of calcium and phosphorus in the bones. Infants with severe osteopenia may experience limited movement or swelling in an arm or leg due to bone fractures [8]. Osteopenia in premature infants raises the risk of osteoporosis in adulthood. This condition leads to an increase in the resorption activity of osteogenic cells compared to osteoblasts, which are responsible for bone formation. As a result, this imbalance can contribute to a higher incidence of bone fractures, particularly in the vertebrae, radius, and femoral head. The development of osteoporosis is often linked to disabilities that manifest as chronic pain, which can, in turn, lead to depression [27].
The use of nutritional formulas that are not intended for premature infants leads to a deficiency of cholecalciferol, which is essential for the normal absorption of calcium and phosphorus in the intestines and kidneys. Low birth weight, preterm infants excrete more phosphorus in their urine compared to term-born infants [8]. Restricted intrauterine growth in infants born before 28 weeks’ gestation leads to impaired nutrient absorption [9]. Low serum phosphate levels in preterm infants receiving parenteral nutrition are due to an inadequate supply of phosphorus. This deficiency contributes to Metabolic Bone Disease of Prematurity (MBD), which is characterized by the demineralization of bone tissue and can lead to fractures [10]. A study by Cho et al. indicates that extended parenteral nutrition and insufficient breast milk intake significantly contribute to vitamin D deficiency in children born before 32 weeks of gestation [11]. The study by Nabiel et al. indicates a positive correlation between vitamin D deficiency and hypocalcemia in preterm infants [12]. Zinc deficiency may contribute to the death of osteoblast cells [13]. Medications commonly prescribed to preterm infants increase the risk of osteopenia through various mechanisms. Furosemide, caffeine citrate, and glucocorticoids (GCs) lead to increased calcium excretion [14,15,16,17,18]. As a result, hypercalciuria caused by the previously mentioned medications inhibits the formation of bone [19]. Phenobarbital and phenytoin induce the cytochrome enzyme system and contribute to increased breakdown of 25(OH) vitamin D3 [20].
Monitoring the nutritional status of preterm infants is crucial for adjusting both pharmacological and nutritional therapies, aiming to reduce the risk of osteopenia. To effectively monitor this nutritional status, appropriate medical equipment is essential. The lancet and Microtainer BD serum sampler (yellow) are used to collect capillary blood samples for measuring serum phosphate and calcium levels [21,22,23]. This yellow test tube contains an acrylate gel that forms a barrier between the serum and clotted blood, ensuring the stability of the elements being measured [22,23].
3.3. The Role of Nutritional Intervention in Preterm Infants
It is important to avoid overheating and do not microwave; use gentle thawing/warming per milk-bank/NICU protocol. Doing so can destroy essential nutrients, probiotic bacteria (which help reduce the risk of cow’s milk protein allergy), and immune cells like immunoglobulins (types A, G, and M), as well as B and T lymphocytes, all of which are crucial for the baby’s health. Additionally, heating breast milk in these ways can potentially burn the baby’s digestive tract [24,25]. This food alone does not completely meet the energy and nutrient needs of preterm infants. Combining it with an HMF that provides additional nutrients can help prevent nutritional deterioration and support the health of preterm infants. Ready-to-feed preterm infant formula (RTF) is designed for preemies who cannot be breastfed. These formulations contain essential nutrients and whey proteins in higher quantities than those found in standard milk formulas intended for full-term newborns [26]. Fortification provides bioavailable calcium (salt form varies by product); adequate Ca and P are key to bone accretion. The absorption of calcium lactate is not significantly influenced by stomach acidity, unlike inorganic calcium carbonate [27].
3.4. The Significance of Nutrients Found in Milk Mixtures for Preemies
3.4.1. Nutrients That Improve the Bioavailability of
3.4.1.1. Calcium
HMF and RTF are characterized by a calcium/phosphorus (Ca:P) ratio within the recommended range of 1.6 to 1.8 [28]. A suitable calcium-to-phosphorus ratio in both HMF and RTF helps prevent calcium loss from bones, thereby reducing the risk of osteopenia [28]. Additionally, it is essential for the process of proper bone formation [29]. Research by Abrams et al. suggests that lactose in milk mixtures enhances calcium absorption in infants [30].
3.4.1.2. Zinc
3.4.1.3. Phosphorus
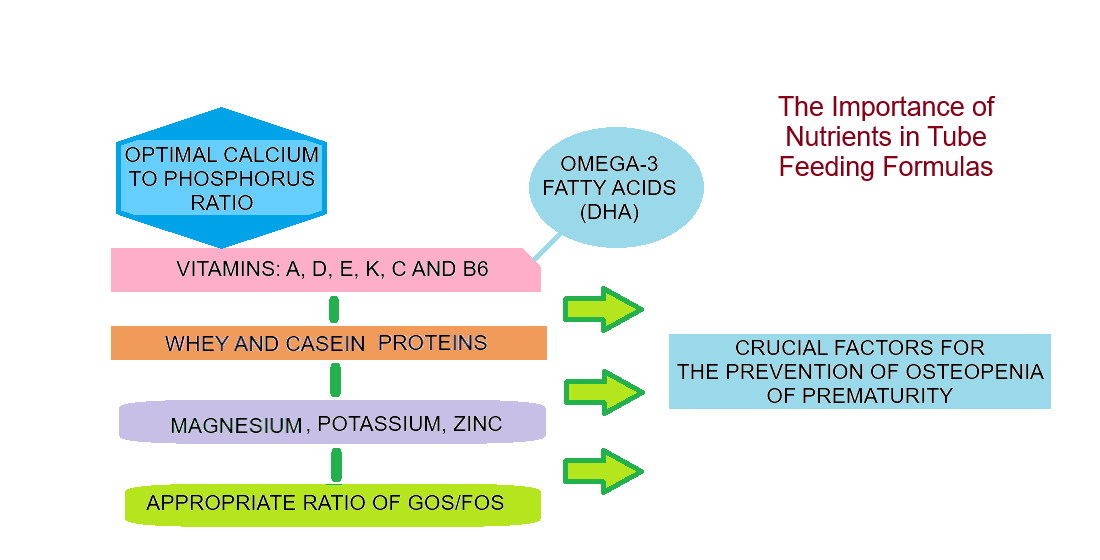
The presence of whey and casein proteins helps reduce the risk of hypophosphatemia caused by caffeine [33]. These ingredients enhance the absorption of phosphorus by binding to the element [34]. Nutrients that enhance the bioavailability of phosphorus are illustrated in Figure 2.
This schematic summarizes mechanisms in preterm enteral nutrition that support P availability and bone mineralization: (i) Milk proteins (whey, casein) form soluble protein–phosphate complexes that support luminal solubility and uptake and may mitigate caffeine-related hypophosphatemia; (ii) Adequate vitamin D status facilitates intestinal P handling and acts synergistically with calcium (Ca) when the dietary Ca:P ratio is balanced (~1.6–1.8); (iii) Prebiotic oligosaccharides (GOS/FOS) and probiotic Lactobacillus spp. promote short-chain fatty acid production, lowering luminal pH and improving mineral solubility; (iv) Sufficient protein and magnesium support transport and downstream bone deposition. Abbreviations: Ca, calcium; P, phosphorus; HMF, human milk fortifier; GOS, galacto-oligosaccharides; FOS, fructo-oligosaccharides; SCFAs, short-chain fatty acids.
3.5. The Role of Phosphorus in Calcium Absorption
Phosphorus enhances the bioavailability of calcium when the Ca:P ratio is appropriately balanced. It promotes the reabsorption of calcium ions in the distal part of the nephron and their incorporation into bone. If phosphorus supply surpasses calcium intake, it hinders calcium ion absorption in the small intestine, leading to increased elimination in the feces [34].
3.6. The Importance of ω-3 Fatty Acids for the Bioavailability of Calcium and Phosphorus
DHA, an ω-3 polyunsaturated fatty acid, supports bone health by enhancing osteoblast formation and reducing bone resorption through its positive effects on calcium balance and the activity of bone-forming cells [35]. The study conducted by Maditz K.H. and colleagues demonstrates a positive correlation between the consumption of oils rich in ω-3 fatty acids, such as soybean oil and salmon oil, and the retention of calcium (Ca) and phosphorus (P). This consumption helps prevent deficiencies of these essential elements, attributed to the significant amounts of ω-3 fatty acids found in these oils [36].
3.7. Vitamin D3: Factors That Increase Its Uptake and Its Role
Fats in nutritional formulations for preterm infants enhance the bioavailability of cholecalciferol by creating a hydrophobic phase in which the vitamin dissolves [37]. Vitamin D3 regulates cellular zinc levels, enhancing zinc uptake [38]. Cholecalciferol supplementation is especially crucial for preemies receiving GCs, as these medications accelerate the metabolism of this vitamin [39].
3.8. Research Findings Highlighting the Significance of Nutrients in the Nutritional Treatment of Preterm Infants
Bijari B.B. et al. conducted a cross-sectional study involving 100 premature infants admitted to the NICU of Afzalipour Medical Centre in Kerman between 2017 and 2018 [40]. The study aimed to determine alkaline phosphatase (ALP) levels, which are used as a screening criterion for osteopenia, in one-month-old infants. It also examined the relationship between ALP levels and various factors, including birth weight, weight gain, length of hospitalization, the amount of parenteral nutrition administered, formula volume, and supplementation provided. Results showed that among the 100 preterm infants, 41 were diagnosed with osteopenia based on the criterion of ALP levels exceeding 900 U/L. It was found that infants who were exclusively fed breast milk without nutrient-rich breast milk fortifiers were more likely to have preterm osteopenia. Additionally, the average length of hospitalization and total parenteral nutrition for those with osteopenia was significantly longer compared to infants without the condition. Notably, 78% (32 out of 41) of the preterm infants with osteopenia did not receive any additional calcium and phosphate supplementation beyond what was provided in breast milk. In contrast, most of their peers without osteopenia received breast milk fortifiers. Furthermore, cholecalciferol in drop form was administered irregularly to 61% (25 out of 41) of the infants with osteopenia, and 7% (3 out of 41) did not receive it at all. On the other hand, a significant 88.1% (52 out of 59) of preterm infants without osteopenia received regular vitamin D supplementation [40]. Abrams’ research indicates that breast milk fortifiers, which provide additional doses of calcium, phosphorus, and vitamin D dissolved in breast milk, as well as vitamin D3 supplementation, have positive effects on bone density in preterm infants [41].
Mohamed et al. (2020) conducted a prospective case-control study to evaluate the significance of protein and vitamin D intake in osteopenia among preterm infants with a birth weight of less than 1250 grams [42]. Serum vitamin D levels were measured six weeks after birth, and wrist X-rays were taken at that time to diagnose osteopenia. Of the 26 preterm infants included in the study, 13 (50%) developed osteopenia, indicated by a loss of bone mass observed in the DEXA examination. The average vitamin D3 concentration in the group with osteopenia was significantly lower (mean 21 ng/ml) compared to those without osteopenia, who had an average serum cholecalciferol concentration of 39.3 ng/ml. Alkaline phosphatase (ALP) levels exceeding 619 IU/L showed a sensitivity of 76.9% and a specificity of 75%, indicating the presence of osteopenia at six weeks after birth. Daily protein intake among the study participants varied between 2,2 and 3,6 g/kg of body weight. In preterm infants who developed osteopenia, the protein supply was significantly lower and deviated from the daily recommended intake for infants, which is 3.5-4 g/kg of body weight. Premature infants with osteopenia were on total parenteral nutrition for an average of 11 days and had significantly shorter durations of enteral nutrition (tube feeding of breast milk supplemented with HMF), lasting only 27 days. In contrast, infants without osteopenia averaged 6 days on total parenteral nutrition and 32 days on enteral nutrition at 120 ml/kg of body weight. Infants born prematurely with bone mineral density (BMD) had an average of 32 days on parenteral nutrition (11 days total, with 21 days of partial tube feeding). In comparison, the group without BMD received parenteral nutrition for an average of 27 days (6 days total, with 21 days of partial and total parenteral feeding). The results of this study suggest that parenteral nutrition lasting longer than four weeks, delayed introduction of partial and total enteral feeding, as well as deficiencies in cholecalciferol and protein, contribute to the development of osteopenia in preterm infants. The findings of the study indicate that early initiation of enteral feeding in premature infants may help prevent MBD, including osteopenia [42].
The earliest symptom of mineral metabolism disturbance appears one to two weeks after birth and is characterized by hypophosphatemia. In infants exclusively fed breast milk, a serum phosphate concentration of less than 3.6 mg/dL (1.16 mmol/L) indicates mineral depletion and an increased risk of developing metabolic bone disease (MBD). A serum phosphate concentration below 5.6 mg/dL (<1.8 mmol/L) has been strongly correlated with the occurrence of radiographically apparent rickets in preterm infants, who have a mean gestational age of 30.3 weeks (ranging from 24.7 to 33.0 weeks) and a mean birth weight of 1490 g (within the range of 735 to 2250 g). The bioavailability of calcium varies from 40% (for modified milk) to 70% (for breast milk), while phosphate bioavailability ranges from 60% to 95% for fully enteral-fed preterm infants. A study by Bandara S. et al. (2010) showed that newborns who did not receive formula milk added to their breast milk had lower phosphate levels compared to preterm infants who received breast milk fortifiers or phosphate supplementation. Furthermore, among preterm infants exclusively fed breast milk, rickets, resulting from osteopenia, occurred in 40% of cases, compared to only 16% of preterm infants who received nutritional supplements providing phosphorus, which is essential for bone development [43]. Viswanathan S. et al. demonstrated that infants born before 30 weeks of gestation who received lower average weekly amounts of calcium, phosphorus, cholecalciferol, and protein during their first eight weeks of life were more likely to develop metabolic bone disease compared to a control group [44]. Of the 230 infants included in the study, 71 (30.9%) experienced MBD. Compared to the control group, these infants had lower average birth weights, were born at earlier gestational ages, and had a higher frequency of requiring mechanical ventilation. They also had increased incidences of chronic lung disease and cholestasis, a longer duration of parenteral nutrition, and more frequent use of furosemide, corticosteroids, and antibiotics. As a result, the mortality rate in the MBD group was significantly higher at 14.1% compared to 4.4% in the control group, and their hospital stays were longer. This analysis indicates that insufficient nutrient supply, along with these other factors, significantly increases the risk of death and disability [44].
Krithika et al. report that early supplementation of Ca and P in TPN, as well as the enrichment of breast milk with HMF rich in these elements, helps counteract insufficient bone mineralization caused by Ca and P deficiency [45]. The implementation of parenteral nutrition, supplemented with calcium and phosphorus from the first day of life, followed by the introduction of enteral nutrition starting at day 14 for preterm infants, was included as part of the quality improvement (QI) initiatives. This approach involved adding a human milk fortifier to breast milk to provide additional calcium and phosphorus supplementation. As a result of these QI efforts, the incidence of metabolic bone disease in preterm infants decreased from 35% to less than 20%.
The beneficial effects of polyunsaturated fatty acids in reducing urinary calcium excretion were demonstrated in a study conducted by Baggio et al. [46]. Participants in the study group received three capsules containing 0.85 grams of fish oil each, totaling 2.55 grams per day for 30 days. This dosage provided 1.29 grams of eicosapentaenoic acid (EPA) and 0.99 grams of docosahexaenoic acid (DHA) daily. Daily urine collections were performed for all participants, including those in the control group who did not receive the capsules. The results showed a significant reduction in calcium excretion among those taking fish oil capsules compared to the control group [46]. The administration of EPA and DHA leads to a reduction in the synthesis of pro-inflammatory prostaglandin E2 (PGE2), which is known to contribute to calcium reabsorption in the renal tubules, thereby decreasing its elimination [46]. A study conducted by Sun et al. revealed that rats consuming fish oil had significantly lower calcium ion excretion compared to those given soybean oil. The differences in results likely stem from the higher linoleic acid content and the lack of EPA and DHA in soybean oil compared to fish oil. The presence of the polyunsaturated fatty acids EPA and DHA in fish oil is due to their very low melting points, which are below -40°C, allowing them to thrive in cold aquatic environments [47]. Therefore, the findings of studies mentioned in this review suggest that EPA and DHA may help prevent the adverse effects of GCs on decreased intestinal absorption of calcium and phosphate, as well as enhanced elimination of calcium [47]. As a result, ω-3 fatty acids can help prevent bone degradation by increasing bone density [48].
Ahmed et al. (2020) presented evidence on the prevalence of rickets in children in Bangladesh caused by calcium deficiency [49]. The authors reported that chronic low calcium intake leads to urinary phosphate loss, resulting in hypophosphatemia and active rickets. The results indicated that children under 6 years old in Group A consumed significantly less calcium and slightly less phosphorus compared to the control group. Furthermore, the ratio of calcium to phosphorus intake in Group A was significantly lower than in the control group. Children with active rickets in Group A also had lower body weight and growth rates, along with lower vitamin D levels, where more than half of the participants had vitamin D levels below 25 nmol/L, relative to the control group. The biochemical profile of participants in Group A was characteristic of active rickets induced by calcium deficiency, indicating reduced serum calcium, reduced serum phosphorus, and increased phosphate excretion during daily urine collection.
Additionally, cholecalciferol deficiency may contribute to calcium deficiency, particularly when calcium intake and the calcium-to-phosphorus ratio are low [49]. It is essential to maintain proper levels of vitamin D, calcium, and phosphorus to ensure the stability of bone tissue [50]. According to the recommendations by Embleton et al. (2022), the decision to transition from enteral to oral feeding should consider the health status of the preterm infant, including their nutritional status and gastrointestinal maturity. Additionally, the infant should have reached 32 weeks of gestation before this switch is made [51].
Future research should concentrate on comparing biochemical tests that measure levels of calcium, phosphorus, zinc, magnesium, potassium, and vitamin D in both preterm and term-born infants. This analysis aims to identify differences in their nutritional statuses. The clinical implications of these findings may lead to recommendations regarding the frequency of biochemical testing based on the nutritional treatments used in preterm infants.
Unfortunately, during our literature review, we identified some gaps, particularly the scarcity of studies focused on preterm infants and the mechanism by which vitamins A and E enhance zinc uptake. Only Vendolovich and colleagues address this issue: “Zinc absorption is enhanced by the presence of vitamins A and E.,, There is an urgent need for a publication on enteral feeding in preterm infants, which should also outline the interactions between enteral formulae, breast milk fortifiers, and human milk.
3.9. Interaction of Nutrients in Enteral Feeding for Preterm Infants
Enriching breast milk with human milk fortifiers is crucial for preventing osteopenia in preterm infants. Breast milk naturally contains synbiotics, which are a combination of probiotics and prebiotics. Prebiotics, primarily in the form of oligosaccharides, work alongside probiotics, such as lactic acid bacteria, to enhance the absorption of minerals that are essential for proper bone development [104]. Human milk has symbiotic properties that promote the production of short-chain fatty acids (SCFAs) such as acetate, butyrate, and propionate during bacterial fermentation. Short-chain fatty acids (SCFAs) lower the pH level in the gut, which improves the solubility and bioavailability of minerals such as divalent cations (e.g., calcium, magnesium). The symbiotic action that facilitates calcium and phosphorus absorption also stimulates enterocyte proliferation, contributing to the expansion of the gut’s absorption surface, with bacterial fermentation playing a role. Additionally, breast milk as a natural symbiotic agent prevents the formation of insoluble complex compounds that hinder the absorption of essential minerals such as calcium, magnesium, and zinc [105].
If breastfeeding is not possible, modified milk should be given for the enteral feeding of preterm infants, with an appropriate GOS/FOS oligosaccharide ratio of 9:1 [106]. The correct ratio of GOS/FOS can help prevent mineral deficiencies that lead to osteopenia by lowering the cecum’s pH, thus improving the levels of calcium, phosphorus, and magnesium in bone tissue. This improvement contributes to better bone development and helps prevent stunted growth and fractures related to osteopenia. The study conducted by Bryk found a positive correlation between the administration of a 9:1 GOS/FOS prebiotic mixture and the absorption of calcium (Ca), phosphorus (P), and magnesium (Mg) in the colon [107].
Our synthesis is limited by its narrative design, heterogeneity of included studies (populations, definitions of osteopenia/metabolic bone disease, and outcome measures), and lack of formal risk-of-bias scoring. To partially mitigate this, we applied SANRA, reported a transparent PRISMA-style search flow, separated neonatal-human evidence from animal/mechanistic findings, and provided comparative summary tables. Future work should employ standardized diagnostic criteria and formal quality appraisal across multicenter cohorts.
Our review demonstrates that targeted nutritional interventions play a pivotal role in managing osteopenia of prematurity. Strategies such as early human milk fortification, use of mineral-enriched preterm formulas, and supplementation with calcium, phosphate, and vitamin D were frequently associated with improved bone mineralization markers and reduced incidence of metabolic bone disease in preterm infants. These findings align with current practice recommendations that emphasize optimizing nutrition and mineral intake to support bone health. Importantly, practical implementation requires a multidisciplinary approach in the neonatal intensive care unit (NICU). Neonatologists must lead early identification and management of at-risk infants, while neonatal nurses ensure careful handling of fragile infants, vigilant monitoring of growth and biochemistry, and adherence to feeding protocols. In parallel, dietitians (clinical nutritionists) should tailor and adjust feeding plans to meet the high calcium and phosphate requirements of growing preterm infants, and pharmacists are integral in formulating parenteral nutrition and preparing supplementation (e.g., phosphate, calcium, vitamin D) to ensure safe and effective delivery [108,109,110]. The success of a recent quality-improvement initiative underscores this team - based approach: a multidisciplinary NICU team (including neonatologists, nurses, dietitians, and pharmacists) that standardized screening and nutritional management significantly reduced osteopenia-related fractures. These practical implications highlight that effective prevention and treatment of neonatal osteopenia depend on coordinated efforts across professions to implement nutritional strategies, monitor bone health, and minimize risk factors.
Despite generally positive trends, our analysis also revealed substantial heterogeneity in study methodologies and definitions, which complicates the interpretation of the evidence. The included studies varied widely in design and quality, ranging from small single-center trials to observational case series, and used inconsistent criteria to define osteopenia or metabolic bone disease of prematurity. For example, some researchers diagnosed osteopenia based on biochemical markers (such as alkaline phosphatase or serum phosphate thresholds), whereas others required radiological evidence of rickets or fractures; no single uniform diagnostic criterion was applied across all studies. This lack of consensus is well recognized in the field: neonatal units and authors employ different thresholds for alkaline phosphatase (from ~500 IU/L up to > 900 IU/L) and various imaging modalities, reflecting significant variability in definitions and diagnostic cut-offs. A focused review in one NICU found that “unclear definitions” were a key barrier leading to inconsistent diagnosis and management of osteopenia.
Moreover, the methodological quality of studies was inconsistent – many lacked control groups or had a high risk of bias – limiting the strength of conclusions. This variability in study populations, outcome measures, and quality makes it difficult to directly compare results or perform quantitative synthesis. Our findings must therefore be interpreted in light of these limitations. Standardization of definitions and high-quality study designs are needed to better delineate which nutritional interventions truly confer the greatest benefit.
Given these limitations, we recommend specific directions for future research to strengthen the evidence base. Prospective, multicenter studies should be conducted to evaluate nutritional strategies for preventing osteopenia in preterm infants under uniform protocols. Enrolling larger patient cohorts from multiple NICUs would increase the power and generalizability of findings, and a common set of diagnostic criteria (for example, agreed-upon biochemical thresholds and imaging assessments) should be used to reduce heterogeneity. In addition, longitudinal tracking of bone outcomes is essential. Future studies ought to follow preterm infants beyond the neonatal period – through infancy and into childhood – with appropriate measures (such as serial dual-energy X-ray absorptiometry scans or other bone density assessments) to determine whether early nutritional interventions translate into improved long-term bone health. Such longitudinal data would clarify if initial improvements (e.g., in alkaline phosphatase levels or early growth) lead to meaningful differences in outcomes like fracture incidence, bone mineral density at later ages, or attainment of peak bone mass. Some recent investigations have also highlighted the need to establish age-specific reference standards and refine diagnostic cut-offs (e.g., optimal alkaline phosphatase levels for different postnatal ages) through larger studies. Ultimately, well-designed multicenter trials and cohort studies with extended follow-up will help identify the most effective nutritional treatment protocols and inform evidence-based guidelines to reduce osteopenia of prematurity.
3.10. Practice Points for NICU Teams (Concise, Evidence-Informed)
- Initiate fortified human milk early once minimal feeds are tolerated; target Ca:P ≈ 1.6–1.8, adequate protein (~3.5–4 g/kg/day), and vitamin D per local guidance.
- Minimize duration of exclusive PN where feasible; ensure adequate Ca:P in PN from day 1 per unit protocol.
- Monitor phosphate and ALP using consistent thresholds; address low 25(OH)D and low P promptly.
- Standardize protocols (nutrition + monitoring) through multidisciplinary NICU teams; audit OOP/MBD incidence over time.
3.11. Research Agenda
- Consensus OOP/MBD definitions (biochemical cut-offs + imaging) for preterm infants.
- Multicenter protocols comparing fortification strategies and PN mineral targets.
- Longitudinal follow-up into childhood/adolescence to link early nutrition to bone mass/fracture outcomes.
4. Conclusions
In conclusion, appropriate nutritional management is a cornerstone of preventing and treating osteopenia in preterm infants, but current evidence is constrained by inconsistent methodologies and definitions across studies. Our review indicates that ensuring sufficient mineral intake – via fortified feedings and judicious supplementation of calcium, phosphorus, and vitamin D – can improve short-term indicators of bone health in vulnerable preterm neonates. However, the lack of standardized diagnostic criteria and the variable quality of available studies make it challenging to issue universal recommendations. There is a need to translate emerging evidence into consistent practice: neonatal units should consider adopting unified protocols for screening and nutritional care of at-risk infants, ideally developed by multidisciplinary teams and informed by the best available data.
Moving forward, rigorous multicenter research with long-term follow-up is warranted to confirm which interventions yield sustained improvements in bone outcomes. Rather than broad generalizations or calls for “urgent” action, we advocate for specific, evidence-based steps: develop consensus definitions, implement collaborative nutritional strategies in the NICU setting, and conduct prospective studies to guide optimal care. By doing so, the neonatal community can more effectively mitigate osteopenia of prematurity and improve the lifelong bone health of former preterm infants.
Author Contributions
Conceptualization, D.B., R.P., E.Ł.; methodology, D.B., R.P., Ł.O., A.S., E.Ł.; writing—original draft, D.B., R.P., E.Ł.; writing—review and editing, D.B., R.P., Ł.O., A.S., E.Ł.;. All authors have read and agreed to the published version of the manuscript.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
No new data were created or analyzed in this study.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Kłęk, S.; Kapała, A. Nutritional treatment. Varia Medica 2019, 3, 77–87. [Google Scholar]
- Ciborowska, H.; Rudnicka, A. Nutrition for preterm and low birth weight infants. Dietetics. Nutrition of healthy and sick man; Medical Publishing House PZWL Warsaw, Poland, 2016; 515-520.
- Westin, V.; Klevebro, S.; Domellöf, M.; Vanpée, M.; Hallberg, B.; Sjöström, E.S. Improved nutrition for extremely preterm infants - a population-based observational study. Clinical Nutrition ESPEN 2018, 23, 245–251. [Google Scholar] [CrossRef] [PubMed]
- Angelika, D.; Etika, R.; Mapindra, M. P.; Utomo, M. T.; Rahardjo, P.; Ugrasena, D. I. G. Associated neonatal and maternal factors of osteopenia of prematurity in low resource setting: A cross-sectional study. Annals of Medicine and Surgery 2021, 64, 102235. [Google Scholar] [CrossRef]
- Ratajczak, A.E.; Rychter, A.M.; Zawada, A.; Dobrowolska, A.; Krela-Kaźmierczak, I. Nutrients in the Prevention of Osteoporosis in Patients with Inflammatory Bowel Diseases. Nutrients 2020, 12, 1–18. [Google Scholar] [CrossRef]
- Freitas, B. C. F.; Lima, L. M.; Moreira, M. E. L.; Priore, S. E.; Henriques, B. D.; Carlos, C. F. L. V.; Sabino, J. S. N.; Franceschini, S. D. C. C. Micronutrient supplementation adherence and influence on the prevalences of anemia and iron, zinc and vitamin A deficiencies in preemies with a corrected age of six months. Clinics 2016, 71, 440–448. [Google Scholar] [CrossRef]
- Ciborowska, H.; Rudnicka, A. Nutritional treatment. Dietetics. Nutrition of healthy and sick man; Medical Publishing House PZWL Warsaw, Poland, 2016; 359-370.
- Osteopenia - premature infants. Neonatal rickets; Brittle bones - premature infants; Weak bones - premature infants; Osteopenia of prematurity. https://ssl.adam.com/content.aspx?productid=617&pid=1&gid=007231&site=makatimed.adam.com&login=MAKA1603 (06-01-2025).
- Pinto, M. R. C.; Machado, M. M. T.; de Azevedo, D. V.; Correia, L. L.; Leite, Á. J. M.; Rocha, H. A. L. Osteopenia of prematurity and associated nutritional factors: case–control study. BMC pediatrics 2022, 22, 1–11. [Google Scholar] [CrossRef]
- Sureshchandra, S.; Maheshwari, R.; Nowland, T.; Elhindi, J.; Rundjan, L.; D’Cruz, D.; Luig, M.; Shah, D.; Lowe, G.; Baird, J.; Jani, P.R. Implementation of Parenteral Nutrition Formulations with Increased Calcium and Phosphate Concentrations and Its Impacton Metabolic Bone Disease in Preterm Infants: A Retrospective Single-Centre Study. Children 2025, 12, 1–14. [Google Scholar] [CrossRef]
- Cho, H.; Lee, Y.; Oh, S.; Heo, J. S. Risk factors and outcomes of vitamin D deficiency in very preterm infants. Pediatrics and Neonatology 2025, 66, 31–36. [Google Scholar] [CrossRef]
- Nabiel, N.; Nugroho, H. W.; Moelyo, A. G. Vitamin D Deficiency is Associated with Hypocalcemia in Preterm Infants. Molecular and Cellular Biomedical Sciences 2024, 8, 90–95. [Google Scholar] [CrossRef]
- Fang, D.; Jiang, D.; Shi, G.; Song, Y. The association between dietary zinc intake and osteopenia, osteoporosis in patients with rheumatoid arthritis. BMC Musculoskeletal Disorders 2024, 25, 1–9. [Google Scholar] [CrossRef] [PubMed]
- FUROSEMIDE injection, for intravenous or intramuscular use Initial U.S. Approval: 1982 https://www.accessdata.fda.gov/drugsatfda_docs/label/2024/018267s029lbl.pdf (Revised: 10/2024).
- Mohn, E.S.; Kern, H.J.; Saltzman, E.; Mitmesser, S.H.; McKay, D.L. Evidence of Drug–Nutrient Interactions with Chronic Use of Commonly Prescribed Medications: An Update. Pharmaceutics 2018, 10, 1–45. [Google Scholar] [CrossRef]
- Kumar, M.; Ali, A.; Khan, M.A.; Sohail, S.; Saleem, S.M.; Khan, M.; Naz, F.; Khan, W.A.; Salat, M.S.; Hussain, K.; Ambreen, G. Relationship of caffeine regimen with osteopenia of prematurity in preterm neonates: a cohort retrospective study. BMC Pediatrics 2022, 22, 1–10. [Google Scholar] [CrossRef]
- Peyona 20 mg/mL solution for infusion and oral solution. Summary of product characteristics. https://www.ema.europa.eu/en/documents/product-information/peyona-epar-product-information_en.pdf (03-03-2014).
- Wada, Y.; Hisamatsu, T.; Naganuma, M.; Matsuoka, K.; Okamoto, S.; Inoue, N.; Yajima, T.; Kouyama, K.; Iwao, Y.; Ogata, H.; Hibi, T.; Abe, T.; Kanai, T. Risk factors for decreased bone mineral density in inflammatory bowel disease: A cross-sectional study. Clinical Nutrition 2015, 34, 1202–1209. [Google Scholar] [CrossRef]
- Hekimoğlu, B. S. Risk factors and clinical features of osteopenia of prematurity: Single-center experience. Trends in Pediatrics 2023, 4, 24–30. [Google Scholar] [CrossRef]
- Sivakova, N.A.; Abramova, I.V.; Rybasova, V.P.; Trukhina, I.Y.; Lukina, L.V.; Nasyrova, R.F.; Mikhailov, V.A.; Mazo, G.E. The Effect of Anticonvulsants on Bone Mineral Density: Brief Review. Personalized Psychiatry and Neurology 2023, 3, 32–37. [Google Scholar] [CrossRef]
- Lim, H.B.; Rhu, M.; Jung, J.; Jeon, G.W.; Sin, J. A Comparative Study of Two Different Heel Lancet Devices for Blood Collection in Preterm Infants. Journal of the Korean Society of Neonatology 2010, 17, 239–44. [Google Scholar] [CrossRef]
- Bowen, R.A.R.; Remaley, A.T. Interferences from blood collection tube components on clinical chemistry assays. Biochemia Medica 2014, 24, 31–44. [Google Scholar] [CrossRef]
- Kraszula, Ł.; Eusebio, M.; Pietruczuk, M.; Kuna, P. Serum stability of sodium, potasium and chloride concentration.
- in special tubes containing separator and clotting activator. Laboratory Diagnostics 2018, 54, 23–28.
- Lokossou, G.A.G.; Kouakaniu, L.; Schumacher, A.; Zenclussen, A.C. Human Breast Milk: From Food to Active Immune Response With Disease Protection in Infants and Mothers. Frontiers in Immunology 2022, 13, 1–19. [Google Scholar] [CrossRef]
- Stinson, L.F.; George, A.; Gridneva, Z.; Jin, X.; Lai, C.T.; Geddes, D.T. Effects of Different Thawing and Warming Processes on Human Milk Composition. The Journal of Nutrition 2024, 154, 314–324. [Google Scholar] [CrossRef]
- Królak-Olejnik, B.; Czosnykowska-Łukacka, M. Nutrition of a newborn born prematurely after discharge from a neonatal unit. Neonate born prematurely patient of a primary care physician; Wroclaw Scientific Publishers Atla 2, Poland, 2018, 23-34.
- Dobosz, A.; Smektala, A. Osteoporosis-pathophysiology, symptoms, prevention and treatment. Polish Pharmacy 2020, 76, 344–352. [Google Scholar] [CrossRef]
- Yan-Mei, C.; Xin-Zhu, L.; Rong, Z.; Xi-Hong, L.; Xiao-Mei, T.; Ping-Yang, C.; Zhi-Chun, F. Expert consensus on clinical management of metabolic bone disease of prematurity (2021). Chinese Journal of Contemporary Pediatrics 2021, 23, 761–772. [Google Scholar]
- Dardzińska, J.; Chabaj-Kędroń, H.; Małgorzewicz, S. Osteoporosis as a social and civilisation disease-methods of prevention. Hygeia Public Health 2016, 51, 23–30. [Google Scholar]
- Salomão, N.A.; Geraldes, A.A.; Lima-Silva, A.E. Influence of lactose intolerance and physical activity level on bone mineral density in young women. Revista Brasileira de Educação Física e Esporte 2017, 31, 787–796. [Google Scholar] [CrossRef]
- Talsma, E. F.; Moretti, D.; Ly, S. C.; Dekkers, R.; van den Heuvel, E. G.; Fitri, A.; Boelsma, E.; Stomph, T.J.; Zeder, C.; Melse-Boonstra, A. Zinc Absorption from Milk Is Affected by Dilution but Not by Thermal Processing, and Milk Enhances Absorption of Zinc from High-Phytate Rice in Young Dutch Women. The Journal of nutrition 2017, 147, 1086–1093. [Google Scholar] [CrossRef]
- Park, K.H.; Park, B.; Yoon, D.S.; Kwon, S.-H.; Shin, D.M.; Lee, J.W.; Lee, H.G.; Shim, J.-H.; Park, J.H.; Lee, J.M. Zinc inhibits osteoclast differentiation by suppression of Ca2+-Calcineurin-NFATc1 signaling pathway. Cell Communication and Signaling 2013, 11, 1–12. [Google Scholar] [CrossRef]
- Han, M.J.; Kim, S.H.; Shin, J.; Hwang, J.H. Caffeine-induced hypokalemia: a case report. BMC Nephrology 2021, 22, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Melse-Boonstra, A. Bioavailability of Micronutrients From Nutrient-Dense Whole Foods: Zooming in on Dairy, Vegetables, and Fruits. Frontiers in Nutrition 2020, 7, 1–12. [Google Scholar] [CrossRef]
- Lavado-García, J.; Roncero-Martin, R.; Moran, J.M.; Pedrera-Canal, M.; Aliaga, I.; Leal-Hernandez, O.; Rico-Martin, S.; Canal-Macias, M.L. Long-chain omega-3 polyunsaturated fatty acid dietary intake is positively associated with bone mineral density in normal and osteopenic Spanish women. PLoS One 2018, 13, 1–14. [Google Scholar] [CrossRef]
- Maditz, K.H.; Smith, B.J.; Miller, M.; Oldaker, C.; Tou, J.C. Feeding soy protein isolate and oils rich in omega-3 polyunsaturated fatty acids affected mineral balance, but not bone in a rat model of autosomal recessive polycystic kidney disease. BMC Nephrology 2015, 16, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Lavelli, V.; D’Incecco, P.; Pellegrino, L. Vitamin D Incorporation in Foods. Formulation Strategies, Stability, and Bioaccessibility as Affected by the Food Matrix. Foods 2021, 10, 1–19. [Google Scholar] [CrossRef] [PubMed]
- Amos, A.; Razzaque, M. S. Zinc and its role in vitamin D function. Current research in physiology 2022, 5, 203–207. [Google Scholar] [CrossRef] [PubMed]
- Balwierz, R.; Madej, A. How can you prevent vitamin and mineral deficiencies while taking medication. Pharmacotherapy. When Food Matters. Drug-Food Interactions in Dietetics; University Publishing House Opole, Poland, 2023; 1, 131-140.
- Bahman, B. B.; Salmeei, S.; Niknafs, P.; Jamali, Z.; Mousavi, H.; Sabzevari, F.; Daee, Z.; Mehdi, B. M. Osteopenia of prematurity and its meternal and nutrition-related factors among preterm infants admitted to the NICU department of Afzalipour Medical Center. Journal of Kerman University of Medical Sciences 2023, 30, 339–343. [Google Scholar] [CrossRef]
- Abrams, S.A. Vitamin D in Preterm and Full-Term infants. Annals of Nutrition and Metabolism 2020, 76, 6–14. [Google Scholar] [CrossRef]
- Mohamed, M.; Kamleh, M.; Muzzy, J.; Groh-Wargo, S.; Abu-Shaweesh, J. Association of Protein and Vitamin D Intake With Biochemical Markers in Premature Osteopenic Infants: A Case-Control Study. Frontiers in Pediatrics 2020, 8, 1–8. [Google Scholar] [CrossRef]
- Faienza, M.F.; D’Amato, E.; Natale, M.P.; Grano, M.; Chiarito, M.; Brunetti, G.; D’Amato, G. Metabolic Bone Disease of Prematurity: Diagnosis and Management. Frontiers in Pediatrics 2019, 7, 1–8. [Google Scholar] [CrossRef]
- Viswanathan, S.; Khasawneh, W.; McNelis, K.; Dykstra, C.; Amstadt, R.; Super, D.M.; Groh-Wargo, S.; Kumar, D. Metabolic bone disease: a continued challenge in extremely low birth weight infants. Journal of Parenteral and Enteral Nutrition 2014, 38, 982–990. [Google Scholar] [CrossRef]
- Krithika, M. V.; Balakrishnan, U.; Amboiram, P.; Shaik, M. S. J.; Chandrasekaran, A.; Ninan, B. Early calcium and phosphorus supplementation in VLBW infants to reduce metabolic bone disease of prematurity: a quality improvement initiative. BMJ Open Quality 2022, 11, 1–8. [Google Scholar] [CrossRef]
- Rodgers, A.L.; Siener, R. The Efficacy of Polyunsaturated Fatty Acids as Protectors against Calcium Oxalate Renal Stone Formation: A Review. Nutrients 2020, 12, 1–12. [Google Scholar] [CrossRef]
- Elbahnasawy, A.S.; Valeeva, E.R.; El-Sayed, E.M.; Stepanova, N.V. Protective effect of dietary oils containing omega-3 fatty acids against glucocorticoid-induced osteoporosis. Journal of Nutrition and Health 2019, 52, 323–331. [Google Scholar] [CrossRef]
- Martin - Bautista, E.M.; Muñoz - Torres, J.; Fonolla, M.; Quesada, A.; Poyatos, A.; Lopez – Huertas, E. Improvement of Bone Formation Biomarkers After 1- Year Consumption With Milk Fortified With Eicosapentaenoic Acid, Docosahexaenoic Acid, Oleic Acid, and Selected Vitamins. Nutrition Research 2010, 30, 320–326. [Google Scholar] [CrossRef]
- Ahmed, S.; Goldberg, G.R.; Raqib, R.; Roy, S.K.; Haque, S.; Braithwaite, V. S.; Pettifor, J.M.; Prentice, A. Aetiology of nutritional rickets in rural Bangladeshi children. Bone 2020, 136, 1–10. [Google Scholar] [CrossRef]
- Falbová, D.; Švábová, P.; Beňuš, R.; Hozáková, A.; Sulis, S.; Vorobeľová, L. Association Between Self-Reported Lactose Intolerance, Additional Environmental Factors, and Bone Mineral Density in Young Adults. American Journal of Human Biology 2025, 37, 1–12. [Google Scholar] [CrossRef]
- Embleton, N. D.; et al. Enteral nutrition in preterm infants (2022): a position paper from the ESPGHAN committee on nutrition and invited experts. Journal of pediatric gastroenterology and nutrition 2023, 76, 248–268. [Google Scholar] [CrossRef] [PubMed]
- Molenda, M.; Kolmas, J. K. The Role of Zinc in Bone Tissue Health and Regeneration—a Review. Biological Trace Element Research 2023, 201, 5640–5651. [Google Scholar] [CrossRef] [PubMed]
- Vázquez-Gomis, R.; Bosch-Gimenez, V.; Juste-Ruiz, M.; Vázquez-Gomis, C.; Izquierdo-Fos, I.; Pastor-Rosado, J. Zinc concentration in preterm newborns at term age, a prospective observational study. BMJ Paediatrics Open 2019, 3, 1–5. [Google Scholar] [CrossRef]
- Zhang, J.; Tang, L.; Qi, H.; Zhao, Q.; Liu, Y.; Zhang, Y. Dual function of magnesium in bone biomineralization. Advanced healthcare materials 2019, 8, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Mihatsch, W.; Fewtrell, M.; Goulet, O.; Molgaard, C.; Picaud, J. C.; Senterre, T. ESPGHAN/ESPEN/ESPR/CSPEN guidelines on pediatric parenteral nutrition: calcium, phosphorus and magnesium. Clinical Nutrition 2018, 37, 2360–2365. [Google Scholar] [CrossRef]
- Shahsavani, Z,; Asadi, A. H.; Shamshirgardi, E.; Akbarzadeh, M. Vitamin D, Magnesium and Their Interactions: A Review. International Journal of Nutrition Sciences 2021, 6, 113–118. [Google Scholar]
- Joseph, A. Correlation of serum magnesium and vitamin D levels in patients attending a tertiary care hospital. International Journal of Academic Medicine and Pharmacy 2025, 7, 216–220. [Google Scholar]
- Ahmed, F.; Mohammed, A. Magnesium: The Forgotten Electrolyte—A Review on Hypomagnesemia. Medical Sciences 2019, 7, 56. [Google Scholar] [CrossRef]
- Abate, V.; Vergatti, A.; Altavilla, N.; Garofano, F.; Salcuni, A.S.; Rendina, D.; De Filippo, G.; Vescini, F.; D’Elia, L. Potassium Intake and Bone Health: A Narrative Review. Nutrients 2024, 16, 3016. [Google Scholar] [CrossRef]
- Singh, W.; Kushwaha, P. Potassium: a frontier in osteoporosis. Hormone and Metabolic Research 2024, 56, 329–340. [Google Scholar] [CrossRef]
- Humalda, J. K.; et al. Effects of potassium or sodium supplementation on mineral homeostasis: a controlled dietary intervention study. The Journal of Clinical Endocrinology and Metabolism 2020, 105, e3246–e3256. [Google Scholar] [CrossRef] [PubMed]
- Yee, M.M.F.; Chin, K.-Y.; Ima-Nirwana, S.; Wong, S.K. Vitamin A and Bone Health: A Review on Current Evidence. Molecules 2021, 26, 1757. [Google Scholar] [CrossRef] [PubMed]
- Khojah, Q.; AlRumaihi, S.; AlRajeh, G.; Aburas, A.; AlOthman, A.; Ferwana, M. Vitamin A and its dervatives effect on bone mineral density, a systematic review. Journal of Family Medicine and Primary Care 2021, 10, 4089–4095. [Google Scholar] [CrossRef]
- Samedi, V.; Abdul Aziz, A.; AlJouburi, S.; Mugarab-Samedi, N. Does vitamin K deficiency aggravate osteopenia in preterm infants: Case report and literature review. Journal of Perinatal Medicine 2019, 47, 144. [Google Scholar]
- Rodríguez-Olleros Rodríguez, C.; Díaz Curiel, M. Vitamin K and Bone Health: A Review on the Effects of Vitamin K Deficiency and Supplementation and the Effect of Non-Vitamin K Antagonist Oral Anticoagulants on Different Bone Parameters. Journal of Osteoporosis 2019, 2019, 2069176. [Google Scholar] [CrossRef] [PubMed]
- Aaseth, J.O.; Finnes, T.E.; Askim, M.; Alexander, J. The Importance of Vitamin K and the Combination of Vitamins K and D for Calcium Metabolism and Bone Health: A Review. Nutrients 2024, 16, 2420. [Google Scholar] [CrossRef]
- Thaler, R.; Khani, F.; Sturmlechner, I.; et al. Vitamin C epigenetically controls osteogenesis and bone mineralization. Nature Communications 2022, 13, 5883. [Google Scholar] [CrossRef] [PubMed]
- Aghajanian, P.; Hall, S.; Wongworawat, M. D.; Mohan, S. The roles and mechanisms of actions of vitamin C in bone: new developments. Journal of Bone and Mineral Research 2015, 3, 1945–1955. [Google Scholar] [CrossRef]
- Russo, S.; Scotto di Carlo, F.; Gianfrancesco, F. The osteoclast traces the route to bone tumors and metastases. Frontiers in Cell and Developmental Biology 2022, 10, 886305. [Google Scholar] [CrossRef]
- Rondanelli, M.; Peroni, G.; Fossari, F.; Vecchio, V.; Faliva, M.A.; Naso, M.; Perna, S.; Di Paolo, E.; Riva, A.; Petrangolini, G.; et al. Evidence of a Positive Link between Consumption and Supplementation of Ascorbic Acid and Bone Mineral Density. Nutrients 2021, 13, 1012. [Google Scholar] [CrossRef]
- Britton, R.A.; Irwin, R.; Quach, D.; Schaefer, L.; Zhang, J.; Lee, T.; et al. Probiotic treatment with L. reuteri prevents bone loss in a menopausal ovariectomized mouse model. Journal of cellular physiology 2014, 229, 1822–30. [Google Scholar] [CrossRef]
- Mondal, K. C.; Samanta, S.; Mondal, S.; Mondal, S. P.; Mondal, K.; Halder, S. K. Navigating the frontiers of mineral absorption in the human body: Exploring the impact of probiotic innovations: Impact of probiotics in mineral absorption by human body. Indian Journal of Experimental Biology (IJEB) 2024, 62, 475–483. [Google Scholar]
- St-Jules, D. E.; Jagannathan, R.; Gutekunst, L.; Kalantar-Zadeh, K.; Sevick, M. A. Examining the proportion of dietary phosphorus from plants, animals, and food additives excreted in urine. Journal of Renal Nutrition 2017, 27, 78–83. [Google Scholar] [CrossRef] [PubMed]
- Stremke, E.R.; Hill Gallant, K.M. Intestinal Phosphorus Absorption in Chronic Kidney Disease. Nutrients 2018, 10, 1364. [Google Scholar] [CrossRef] [PubMed]
- Miller, A.; Mathew, S.; Patel, S.; Fordjour, L.; Chin, V.L. Genetic Disorders of Calcium and Phosphorus Metabolism. Endocrines 2022, 3, 150–167. [Google Scholar] [CrossRef]
- Bellavia, D.; Costa, V.; De Luca, A.; Maglio, M.; Pagani, S.; Fini, M.; Giavaresi, G. Vitamin D level between calcium-phosphorus homeostasis and immune system: new perspective in osteoporosis. Current osteoporosis reports 2024, 22, 599–610. [Google Scholar] [CrossRef]
- Dominguez, L.J.; Veronese, N.; Guerrero-Romero, F.; Barbagallo, M. Magnesium in Infectious Diseases in Older People. Nutrients 2021, 13, 180. [Google Scholar] [CrossRef] [PubMed]
- Fiorentini, D.; Cappadone, C.; Farruggia, G.; Prata, C. Magnesium: Biochemistry, Nutrition, Detection, and Social Impact of Diseases Linked to Its Deficiency. Nutrients 2021, 13, 1136. [Google Scholar] [CrossRef]
- Pouteau, E.; Kabir-Ahmadi, M.; Noah, L.; Mazur, A.; Dye, L.; Hellhammer, J.; Pickering, G.; Dubray, C. Superiority of magnesium and vitamin B6 over magnesium alone on severe stress in healthy adults with low magnesemia: A randomized, single-blind clinical trial. PLoS One, 2018, 13, e0208454. [Google Scholar] [CrossRef]
- Maares, M.; Haase, H. A. Guide to Human Zinc Absorption: General Overview and Recent Advances of In Vitro Intestinal Models. Nutrients 2020, 12, 762. [Google Scholar] [CrossRef]
- Stiles, L.I.; Ferrao, K.; Mehta, K.J. Role of zinc in health and disease. Clinical and Experimental Medicine 2024, 24, 38. [Google Scholar] [CrossRef]
- Doğan, A.; Dumanoğlu Doğan, İ.; Uyanık, M.; Köle, M. T.; Pişmişoğlu, K. The clinical significance of vitamin D and zinc levels with respect to immune response in COVID-19 positive children. Journal of Tropical Pediatrics 2022, 68, fmac072. [Google Scholar] [CrossRef]
- Ge, X.; Zhang, J.; Regenstein, J. M.; Liu, D.; Huang, Y.; Qiao, Y.; Zhou, P. α-Lactalbumin: Functional properties and potential health benefits. Food Bioscience 2024, 60, 104371. [Google Scholar] [CrossRef]
- Ribeiro, D. C.; Neto, H. A.; Lima, J. S.; de Assis, D. C.; Keller, K. M.; Campos, S. V.; Oliveira, D.A.; Fonseca, L. M. Determination of the lactose content in low-lactose milk using Fourier-transform infrared spectroscopy (FTIR) and convolutional neural network. Heliyon 2023, 9, e12898. [Google Scholar] [CrossRef] [PubMed]
- Barone, M.; D’amico, F.; Brigidi, P.; Turroni, S. Gut microbiome–micronutrient interaction: The key to controlling the bioavailability of minerals and vitamins? Biofactors 2022, 48, 307–314. [Google Scholar] [CrossRef] [PubMed]
- Ratajczak, A.E.; Zawada, A.; Rychter, A.M.; Dobrowolska, A.; Krela-Kaźmierczak, I. Milk and Dairy Products: Good or Bad for Human Bone? Practical Dietary Recommendations for the Prevention and Management of Osteoporosis. Nutrients 2021, 13, 1329. [Google Scholar] [CrossRef]
- Wendołowicz, A.; Stefańska, E.; Ostrowska, L. Influence of selected dietary components on the functioning of the human nervous system. Annals of the National Institute of Hygiene 2018, 69, 15–21. [Google Scholar]
- Mada, S. B.; Garba, N. A. Effect of Omega-3 Fatty acid on Osteoanabolic Markers and Bone-resorbing Cytokines in Ovariectomized Rats. Journal of Innovative Research in Life Sciences 2024, 6, 12–24. [Google Scholar]
- Karageorgou, D.; Rova, U.; Christakopoulos, P.; Katapodis, P.; Matsakas, L.; Patel, A. Benefits of supplementation with microbial omega-3 fatty acids on human health and the current market scenario for fish-free omega-3 fatty acid. Trends in Food Science and Technology 2023, 136, 169–180. [Google Scholar] [CrossRef]
- Ali, Z.; Al-Ghouti, M.A.; Abou-Saleh, H.; Rahman, M.M. Unraveling the Omega-3 Puzzle: Navigating Challenges and Innovations for Bone Health and Healthy Aging. Marine Drugs 2024, 22, 446. [Google Scholar] [CrossRef] [PubMed]
- Aravind, T. Fat-soluble vitamins: Essential nutrients for human health. World Journal of Pharmaceutical Research 2024, 13, 71–97. [Google Scholar]
- Hu, B.; Lin, Z. Y.; Cai, Y.; Sun, Y. X.; Yang, S. Q.; Guo, J. L.; Zhang, S.; Sun, D. L. A cross-sectional study on the effect of dietary zinc intake on the relationship between serum vitamin D3 and HOMA-IR. Frontiers in Nutrition 2022, 9, 945811. [Google Scholar] [CrossRef] [PubMed]
- Bleizgys, A. Zinc, Magnesium and Vitamin K Supplementation in Vitamin D Deficiency: Pathophysiological Background and Implications for Clinical Practice. Nutrients 2024, 16, 834. [Google Scholar] [CrossRef] [PubMed]
- Ziemińska, M.; Sieklucka, B.; Pawlak, K. Vitamin K and D Supplementation and Bone Health in Chronic Kidney Disease—Apart or Together? Nutrients 2021, 13, 809. [Google Scholar] [CrossRef]
- Dingess, K.A.; Gazi, I.; van den Toorn, H.W.P.; Mank, M.; Stahl, B.; Reiding, K.R.; Heck, A.J.R. Monitoring Human Milk? - Casein Phosphorylation and O-Glycosylation Over Lactation Reveals Distinct Differences between the Proteome and Endogenous Peptidome. International journal of molecular sciences 2021, 22, 8140. [Google Scholar] [CrossRef]
- Lönnerdal, B. Bioactive proteins in human milk: Health, nutrition, and implications for infant formulas. The Journal of pediatrics 2016, 173, S4–S9. [Google Scholar] [CrossRef]
- Allawi, A. A. D.; Alwardi, M. A. W.; Altemimi, H. M. Effects of Omega-3 on vitamin D activation in Iraqi patients with chronic kidney disease treated by maintenance hemodialysis. Journal of Pharmaceutical Sciences and Research 2017, 9, 1812–1816. [Google Scholar]
- Rodzik, A.; Pomastowski, P.; Sagandykova, G.N.; Buszewski, B. Interactions of Whey Proteins with Metal Ions. International journal of molecular sciences 2020, 21, 2156. [Google Scholar] [CrossRef]
- Hall, A.G.; King, J.C. The Molecular Basis for Zinc Bioavailability. International journal of molecular sciences 2023, 24, 6561. [Google Scholar] [CrossRef]
- Wang, B.; Xiao, S.; Zhou, G.; Wang, J. Novel casein-derived peptide-zinc chelate: zinc chelation and transepithelial transport characteristics. Journal of agricultural and food chemistry 2023, 71, 6978–6986. [Google Scholar] [CrossRef] [PubMed]
- Mei, Z.; Yuan, J.; Li, D. Biological activity of galacto-oligosaccharides: A review. Frontiers in Microbiology 2022, 13, 993052. [Google Scholar] [CrossRef]
- Costa, G. T.; Vasconcelos, Q. D. J. S. .; Abreu, G. C.; Albuquerque, A. O.; Vilar, J. L.; Aragão, G. F. Systematic review of the ingestion of fructooligosaccharides on the absorption of minerals and trace elements versus control groups. Clinical nutrition ESPEN 2021, 41, 68–76. [Google Scholar] [CrossRef]
- Seijo, M.; Bryk, G.; Zeni Coronel, M.; et al. Effect of Adding a Galacto-Oligosaccharides/Fructo-Oligosaccharides (GOS/FOS®) Mixture to a Normal and Low Calcium Diet, on Calcium Absorption and Bone Health in Ovariectomy-Induced Osteopenic Rats. Calcified Tissue International 2019, 104, 301–312. [Google Scholar] [CrossRef] [PubMed]
- Mohanty, D.; Misra, S.; Mohapatra, S.; Sahu, P. S. Prebiotics and synbiotics: Recent concepts in nutrition. Food bioscience 2018, 26, 152–160. [Google Scholar] [CrossRef]
- Ilesanmi-Oyelere, B. L.; Kruger, M. C. The role of milk components, pro-, pre-, and synbiotic foods in calcium absorption and bone health maintenance. Frontiers in Nutrition 2020, 7, 578702. [Google Scholar] [CrossRef]
- Kadim, M.; Darma, A.; Kartjito, M.S.; Dilantika, C.; Basrowi, R.W.; Sungono, V.; Jo, J. Gastrointestinal Health and Immunity of Milk Formula Supplemented with a Prebiotic Mixture of Short-Chain Galacto-oligosaccharides and Long-Chain Fructo-Oligosaccharides (9:1) in Healthy Infants and Toddlers: A Systematic Review with Meta-Analysis. Pediatric Gastroenterology, Hepatology & Nutrition 2025, 28, 1–18. [Google Scholar]
- Bryk, G.; Coronel, M. Z.; Lugones, C.; et al. Effect of a mixture of GOS/FOS® on calcium absorption and retention during recovery from protein malnutrition: experimental model in growing rats. European journal of nutrition 2016, 55, 2445–2458. [Google Scholar] [CrossRef]
- Leonardi, R.; Mattia, C.; Decembrino, N.; Polizzi, A.; Ruggieri, M.; Betta, P. The Critical Role of Vitamin D Supplementation for Skeletal and Neurodevelopmental Outcomes in Preterm Neonates. Nutrients 2025, 17, 1381. [Google Scholar] [CrossRef] [PubMed]
- Grover, M.; Ashraf, A. P.; Bowden, S. A.; Calabria, A.; Diaz-Thomas, A.; Krishnan, S.; Miller, J.L.; Robinson, M.E.; DiMeglio, L. A. Invited mini review metabolic bone disease of prematurity: overview and practice recommendations. Hormone Research in Paediatrics 2025, 98, 40–50. [Google Scholar] [CrossRef] [PubMed]
- Saif, S.A.; Maghoula, M.; Babiker, A.; Abanmi, M.; Nichol, F.; Al Enazi, M.; Guevarra, E.; Sehlie, F.; Al Shaalan, H.; Mughal, Z. A Multidisciplinary and a Comprehensive Approach to Reducing Fragility Fractures in Preterm Infants. Current Pediatric Reviews 2024, 20, 434–443. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Search flow diagram (narrative review). Full texts included (n = 115). Main exclusion reasons at full-text: not preterm/neonatal population; outcomes not related to bone health; language other than English/Polish; insufficient data quality.
Figure 1.
Search flow diagram (narrative review). Full texts included (n = 115). Main exclusion reasons at full-text: not preterm/neonatal population; outcomes not related to bone health; language other than English/Polish; insufficient data quality.

Figure 2.
Factors that enhance intestinal phosphorus (P) availability relevant to the prevention of osteopenia of prematurity.
Figure 2.
Factors that enhance intestinal phosphorus (P) availability relevant to the prevention of osteopenia of prematurity.
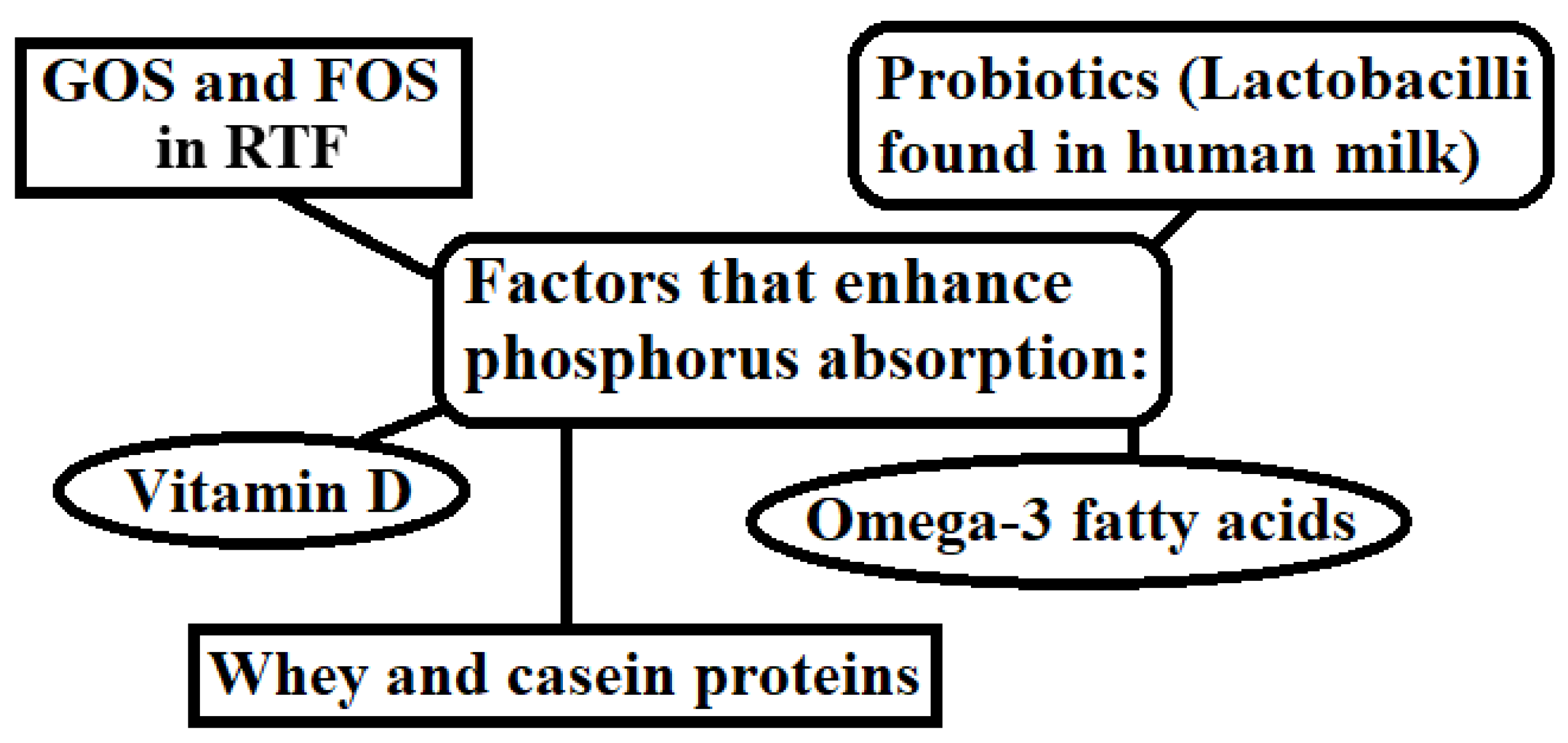

Table 1.
Summary of key clinical studies on nutritional interventions and osteopenia in preterm infants.
Table 1.
Summary of key clinical studies on nutritional interventions and osteopenia in preterm infants.
|
Study (Year) |
Design / Sample |
Intervention / Comparison |
Key findings |
| Bandara (2010) | Retrospective; preterm infants | Breast milk with vs without fortification/ supplementation |
Rickets: 40% without vs 16% with fortification; lower serum phosphate without fortification. |
| Bijari (2019) | Cross-sectional; NICU n = 100 | HMF use vs none among breast-fed | Osteopenia (ALP > 900 IU/L): 41%; 78% of osteopenic infants had no Ca:P supplements; vitamin D regular use 32% vs 88% in non-osteopenic. |
| Mohamed (2020) | Prospective case – control; <1250 g, n = 26 |
Early nutrition in osteopenia vs non-osteopenia |
TPN: 11 vs 6 days; enteral by 6 weeks: 27 vs 32 days; 25(OH)D: 21 vs 39 ng/mL; protein lower in osteopenia. |
| Viswanathan (2014) | Retrospective cohort; <30 weeks, n = 230 | Nutrient intake and outcomes (MBD vs no MBD) | MBD 30.9%; lower early Ca, P, vitamin D, protein; more PN, BPD, steroids/diuretics; mortality 14.1% vs 4.4%. |
| Sureshchandra (2025) | Pre–post QI in VLBW | Higher Ca:P in TPN day 1 + HMF by ~day 14 | MBD decreased from 35% to <20% after implementation. |
HMF, human milk fortifier; ALP, alkaline phosphatase; TPN, total parenteral nutrition; MBD, metabolic bone disease of prematurity; VLBW, very low birth weight; BPD, bronchopulmonary dysplasia; Ca, calcium; P, phosphorus.
Table 2.
Comparative baseline variables and outcomes across robust studies.
| Study | Osteopenia definition/ incidence |
Sample characteristics |
Nutrition exposure |
Outcomes (osteopenia vs comparison) |
| Bandara 2010 | Radiographic rickets: 40% (no fortifier) vs 16% (fortified) | Preterm infants (details not reported) |
Unfortified breast milk vs fortified/ supplemented |
Lower phosphate and higher rickets without fortification. |
| Bijari 2019 | ALP > 900 IU/L at 1 month: 41% |
NICU preterms n = 100 |
HMF absent vs present; vitamin D irregular/ none vs regular |
Higher osteopenia with no HMF; vitamin D regular 32% vs 88%. |
| Mohamed 2020 | DXA/radiographic evidence by 6 weeks: 50% | <1250 g, n = 26 | Longer TPN, lower protein, later enteral | TPN: 11 vs 6 days; 25(OH)D: 21 vs 39 ng/mL; shorter enteral duration. |
| Viswanathan 2014 | Radiographic MBD or ALP > 500 IU/L: 30.9% | <30 weeks, n = 230 | Lower early Ca/P/vit D/protein; more PN and meds | Higher mortality (14.1% vs 4.4%), BPD, cholestasis. |
| Sureshchandra 2025 | Unit incidence: 35% → <20% | VLBW infants (QI cohort) |
Early Ca:P in TPN + HMF protocol | Lower MBD after protocol adoption. |
HMF, human milk fortifier; ALP, alkaline phosphatase; TPN, total parenteral nutrition; MBD, metabolic bone disease of prematurity; VLBW, very low birth weight; BPD, bronchopulmonary dysplasia; Ca, calcium; P, phosphorus.
Table 3.
The impact of specific nutrients in gastric tube feeding formulations on bone development.
| Nutrient | Effects on Skeletal Development |
| Zinc | Zinc plays a crucial role in the deposition of citrate in bone apatite, which facilitates bone mineralization. This happens because citrate stabilizes liquid calcium phosphate precursors and enriches collagen fibers [52]. A study conducted by Vázquez-Gomis R. examined preterm infants and found a positive correlation between the z-score of bone mineral density relative to body length and serum Zn concentration at discharge. The results suggest that Zn plays a crucial role in bone growth [53]. |
| Magnesium | Crucial for growth and the mineralization of bone [54]. The release of parathormone (PTH) is triggered by conditions that prevent the occurrence of hypocalcemia [55]. It plays a role in the biosynthesis, transport, and activation of cholecalciferol as a cofactor [56]. Joseph A.’s research indicated a rise in serum magnesium levels that was directly proportional to vitamin D levels in humans [57]. Helps prevent the loss of potassium [58]. |
|
Potassium Citrate in RTF |
Jehle et al. demonstrated that potassium citrate significantly ↓ decreases the excretion of calcium in urine [59]. |
| Potassium | Encourages the development and maturation of cells responsible for bone formation [60]. The study by Humald J.K. et al. indicated that potassium supplementation led to increased phosphate reabsorption [61]. |
|
Retinol (Vitamin A) |
A study by Choi M.J. indicates a connection between osteopenia and retinol deficiency, suggesting that vitamin A may help protect against osteopenia [62]. Essential for bone development, as it promotes the differentiation of cells that form bone [63]. |
| Vitamin K | M-Samedi V. and colleagues demonstrate that vitamin K inhibits bone turnover in infants [64]. Vitamin K plays a key role in synthesizing osteocalcin, which regulates bone structure and growth [65]. Menaquinone K2 activates osteocalcin, which transports calcium from the blood to the bones, positively affecting bone mineralization [66]. |
|
Vitamin C (ascorbic acid, AA) |
AA plays a vital role in the differentiation of osteoblasts [67]. Vitamin C is essential for the apoptosis of osteoclasts, the cells that degrade bone tissue [68,69]. The research by Martínez-Ramírez M.J. reveals an inverse correlation between blood AA levels and the likelihood of bone fractures [70]. |
|
Probiotics (Lactobacilli found in human milk) |
The results of Britton’s study show that probiotics ↓ the quantity of osteoclasts [71]. Probiotic bacteria produce short-chain fatty acids, which increase the solubility of calcium, magnesium, and zinc, which are crucial for bone development [72]. |
| Prebiotics (GOS) in RTF | Galacto-oligosaccharides (GOS) reduce the pH in the large intestine, which enhances passive calcium absorption and stimulates bone mineralization [101]. |
Table 4.
Nutrients that enhance the bioavailability of vitamins and minerals in nasogastric tube feeding formulations for preterm infants.
Table 4.
Nutrients that enhance the bioavailability of vitamins and minerals in nasogastric tube feeding formulations for preterm infants.
| Nutrient | Factors that increase bioavailability | References |
| Potassium | Probiotics (Lactobacilli found in human milk) | [72] |
| Phosphorous | Vitamin D (Cholecalciferol) |
[73,74,75] |
| Calcium | [75,76] | |
| Magnesium | [77] | |
|
Magnesium |
Peptides from casein or whey | [78] |
| Vitamin B6 (Pyridoxine) | [79] | |
| Zinc | Citrates found in human milk | [80,81] |
| Vitamin D | Zinc | [82] |
| Calcium | Alpha-lactalbumin (alpha-LA) present in human milk | [83] |
|
Calcium Magnesium |
Lactose |
[84] |
|
Zinc Magnesium |
Probiotics (La[85,86ctobacilli found in human milk) | [85,86] |
| Calcium Phosphorus | [86] | |
| Zinc | Vitamin A and E | [87] |
| Calcium | ω-3 fatty acids | [88,89,90] |
| Vitamins: A, D, E, K | Lipids | [91] |
| Zinc | Vitamin D | [92] |
| Vitamin D | Magnesium | [93] |
| Calcium | Vitamin K | [94] |
|
Zinc Calcium |
Casein proteins in human milk/HMF | [95,96] |
| Vitamin D | ω-3 fatty acids | [97] |
| Zinc | Whey protein (alpha-LA), peptides from casein | [98,99,100] |
| Calcium | Galacto-oligosaccharides (GOS) in RTF | [101] |
|
Calcium Magnesium Zinc |
Fructooligosaccharides (FOS) in RTF | [102] |
|
Magnesium Phosphorus |
GOS and FOS in RTF | [103] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



