Submitted:
30 August 2025
Posted:
01 September 2025
You are already at the latest version
Abstract
Background Violence against women and girls (VAWG) remains a critical public health challenge globally and in Asia, where it is rooted in entrenched socio-cultural, economic, and legal inequities. Despite increasing awareness, the drivers of VAWG in Asian contexts remain poorly consolidated across disciplines.Objective To systematically identify and report the socio-cultural, economic, and legal determinants of VAWG in Asia.Methods An evidence synthesis protocol was systematic developed and registered in PROSPERO (CRD420241046281). Comprehensive searches were conducted across PubMed, Science Direct, and the Cochrane Gynaecology and Fertility Group Specialised Register for English-language peer-reviewed articles published between April 1980 and April 2025. The analysis was conducted using contextual and thematic approaches. Results From 16,473 records screened, 34 studies met inclusion criteria. Studies spanned South, Southeast, and East Asia, and included diverse methodologies. Thematic analysis revealed five dominant themes: socio-cultural determinants, economic constraints, legal and institutional weaknesses, regional and demographic variations, and emerging forms of violence. The total population represented across the studies was 193,429 women and girls.Conclusion VAWG in Asia is perpetuated by intersecting systems of gender inequality, economic deprivation, and weak legal enforcement. Multisectoral, culturally sensitive interventions are urgently needed to address the structural roots of violence. Future research should prioritise underrepresented regions and emerging modalities of violence, such as cyber abuse.
Keywords:
violence against women
; Asia
; socio-cultural factors
; economic abuse
; legal systems
; patriarchy
; gender-based violence
; systematic review
Background
Violence against women and girls (VAWG) constitutes a profound public health emergency and a grave violation of human rights, with far-reaching consequences for individuals, families, and societies [1]. In Asia home to nearly 60% of the global population, VAWG remains deeply embedded within social, economic, and legal systems that systematically disempower women [2,3]. Across the region, VAWG takes varied forms including intimate partner violence, dowry-related abuse, child marriage, honour killings, human trafficking, and workplace harassment, reflecting the breadth and complexity of structural gender violence [4,5].
Underpinning these manifestations is a common thread: persistent patriarchy and systemic gender inequality [6,7]. Socio-cultural norms across many Asian societies reinforce male authority and female subordination, often defining women’s roles exclusively within the domestic sphere as daughters, wives, and mothers rather than as autonomous individuals [8,9]. In many parts of Asia, women are subjected to violence beginning within their natal homes, where entrenched son preference—shaped by patrilineal notions of lineage continuity—positions daughters as less valued. This systemic bias manifests as discrimination and gender-based violence, often commencing even before birth [10].
Harmful cultural practices, including forced marriage, gender-selective abortion, and domestic servitude, are frequently justified through religious or traditional frameworks, normalising control, and violence [11,12]. Survivors of violence are commonly blamed, shamed, or silenced, creating substantial barriers to reporting and justice-seeking [3,6].
Economically, structural disadvantage and gendered poverty are key risk factors for VAWG. Limited access to education, formal employment, and financial resources leaves many women dependent on male family members and unable to escape abusive circumstances [13,14]. In lower-income contexts, the interplay between poverty, labour migration, and economic instability intensifies vulnerability, especially for rural, displaced, or marginalised women [15,16]. In some regions, dowry demands, informal labour conditions, and intergenerational debt further entrench this cycle [17,18].
Legally, while progress has been made in criminalising aspects of VAWG, significant gaps remain in implementation. Many countries in Asia suffer from weak legal frameworks, inconsistent enforcement, corruption, and entrenched bias within policing and judicial systems [19,20]. Survivors often face stigma, delayed investigations, and minimal legal redress [2,21]. In areas affected by conflict or displacement, militarised or collapsed legal systems leave women especially vulnerable to sexual and gender-based violence with little to no recourse [14].
A unifying factor behind these patterns is the enduring presence of patriarchy and entrenched gender inequality [6,7]. In many Asian societies, prevailing socio-cultural norms uphold male dominance and female subservience, frequently restricting women to domestic roles, such as daughters, wives, and mothers, rather than acknowledging them as independent individuals [8,9].
Despite decades of programming and advocacy, responses remain fragmented and inconsistently informed by context-specific evidence [22,23]. A comprehensive, interdisciplinary review is therefore essential to understand and address the intersecting socio-cultural, economic, and legal factors that drive VAWG in Asia.
VAWG is a global public health crisis and within Asian, bring together social, cultural, economic and legal factors that should be considered in line with the local, as well as international human rights standards, as well as the sustainable development goals deployed by the United Nations. In light of this, we explore the current published evidence landscape to identify trends within Asia in the first instance, to better identify available knowledge insights and gaps.
Methods
Study Design
This review followed a systematic methodology and adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA 2020) guidelines to ensure transparency and rigour. The study protocol was prospectively registered with PROSPERO (CRD420241046281).
Aims
The primary aim was to critically appraise and synthesise empirical evidence on the socio-cultural, economic, and legal determinants of VAWG across Asia.
Eligibility Criteria
Studies were eligible for inclusion if they were published in English between 30 April 1980 and 30 April 2025, employed empirical methods (quantitative, qualitative, or mixed-methods), focused on any form of violence affecting women and girls in Asia, and involved female participants of any age group. Studies were excluded if they were conducted outside Asia, were non-empirical in nature (e.g., editorials, opinion pieces), or focused exclusively on male victims of violence.
Search Strategy
Systematic searches were conducted across three electronic databases: PubMed, Science Direct, and the Cochrane Gynaecology and Fertility Group (CGF) Specialised Register of Controlled Trials. Keywords and Medical Subject Headings (MeSH) included combinations of:“violence against women,” “gender-based violence,” “intimate partner violence,” “socio-cultural factors,” “economic determinants,” “legal factors,” and “Asia” or specific country names. Boolean operators (AND, OR) were used to optimise search results. Additional studies were identified by manual reference checks of key reviews and relevant articles.
Study Selection
Records were imported into EndNote software for duplicate removal. Titles and abstracts were screened for relevance. A primary reviewer then reviewed full-text articles independently to determine eligibility. Any discrepancies in study inclusion were resolved through discussion with all reviewers until consensus was reached.
Data Extraction
A standardised data extraction form was developed to capture key study characteristics, including author(s), year of publication, and country; study design and setting; participant characteristics and sample size; type(s) of violence examined; and identified socio-cultural, economic, or legal determinants. Outcome measures and main findings were also recorded. The extracted data informed a thematic synthesis of the key drivers of VAGW in Asia.
Data Analysis
A contextual and thematic analysis was used to analyse the final sample. Thematic analysis categorised findings into three principal domain of socio-cultural determinants such as patriarchal norms, religious beliefs, gendered family roles; economic determinants such as poverty, financial dependence, employment restrictions and legal and institutional determinants such as legal protection, access to justice, enforcement gaps. This approach enabled the examination of both prevalence patterns and the interplay between structural and contextual risk factors.
Risk of Bias Assessment
The quality of included studies was appraised using two validated tools:
-
The Newcastle–Ottawa Scale (NOS) was applied to observational studies (cohort and case-control designs). Studies were rated based on selection, comparability, and outcome/exposure domains. Studies were classified as:
- ○
- Low risk: 7–9 stars;
- ○
- Moderate risk: 5–6 stars;
- ○
- High risk: 0–4 stars.
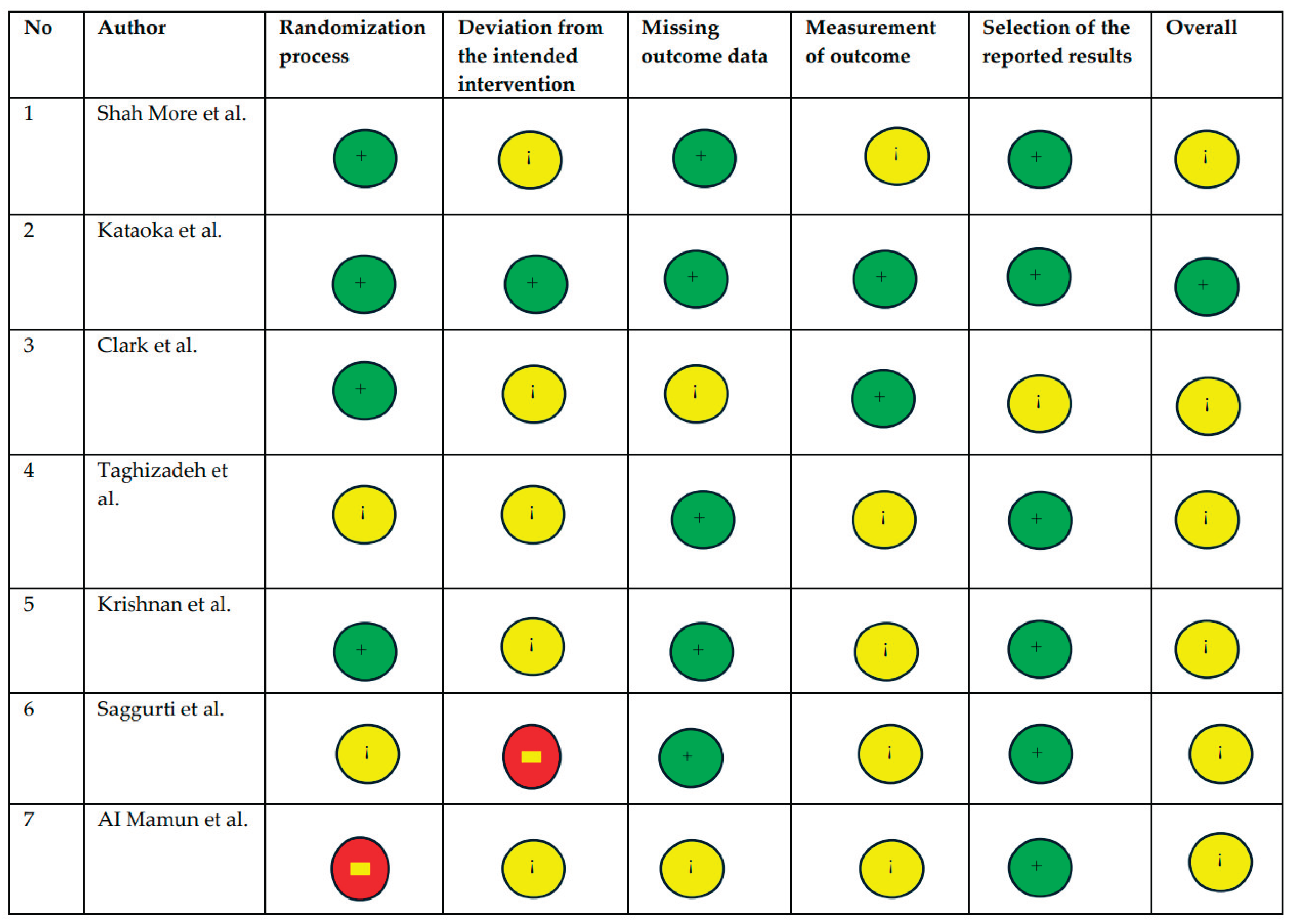
- The Cochrane Risk of Bias 2.0 (ROB-2) tool was used for randomised controlled trials (RCTs). Risk was assessed across five domains including randomisation, deviations from intended interventions, missing data, outcome measurement, and selective reporting.
Results
Study Selection
A total of 16,473 records were identified through database searches, and an additional 165 records were retrieved through manual screening. After the removal of duplicates (n = 15,803), 670 records remained for title and abstract screening. Of these, 505 were excluded based on relevance. Full-text assessment was conducted on 165 articles, and 131 were excluded for the following reasons conducted outside Asia (n = 123), not published in English (n = 8); and non-empirical (n = 4). The final sample comprised of 34 studies. The study selection process is detailed in the PRISMA flow diagram (Figure 1).
Study Characteristics
The included studies encompassed diverse geographical settings across South and South-east Asia and West Asia. Study contexts ranged from rural villages and urban slums to clinical facilities, factories, and refugee or conflict-affected areas. Designs included cross-sectional surveys (n = 26), randomised controlled trials (n = 6), prospective cohort studies (n = 2), and mixed-methods or qualitative studies (n = 2). Sample sizes ranged from 30 to over 89,000 participants, with a total pooled sample of 193,429 women and girls. Detailed study characteristics are summarised in Table 1.
Across 34 included studies conducted between 1980 and 2025, research spanned diverse Asian contexts, including South Asia (India, Nepal, Bangladesh, Sri Lanka), Southeast Asia (Vietnam), East Asia (China, Japan), and West Asia (Iran, Turkey, Afghanistan). Study designs ranged from large-scale population-based surveys to randomised controlled trials, qualitative interviews, and prospective cohort studies, with sample sizes varying from 20 to over 89,000 participants.
Legal and Institutional Gaps
Weak legal protections and limited institutional responsiveness were evident across settings. Studies from conflict-affected [14] and resource-limited regions [7] highlighted barriers to accessing justice, including gender-insensitive policing and absence of survivor services. Kataoka et al. found self-administered IPV screening to be more effective than interviews, suggesting potential for low-cost, scalable detection strategies in healthcare settings.
Health Impacts and Intergenerational Effects
IPV was consistently associated with adverse physical, sexual, and mental health outcomes. Bondade et al. linked IPV to psychiatric comorbidities in infertile women, while Pun et al. demonstrated associations between IPV and poor maternal and neonatal outcomes, including preterm birth. Gautam and Jeong, using national survey data, reported significant public health implications, including reproductive health complications and psychological morbidity.
Intervention Evidence and Prevention Strategies
Several RCTs [21,22,24,25] provided evidence for effective prevention and response strategies, including problem-solving skills training, community engagement, and empowerment of women and their families. Such interventions reduced IPV incidence, improved marital relationships, and strengthened resilience. However, coverage remained geographically uneven, and marginalised groups such as adolescents, migrants, and elderly women were underrepresented in intervention studies.
Contextual Variations and Emerging Forms of Violence
Urban women were more likely to disclose IPV and report cyber-harassment [20], whereas rural women often normalised abuse due to cultural expectations [16]. Workplace IPV and elder neglect [26] were under-recognised yet prevalent. In conflict and displacement contexts [14], IPV intersected with militarisation, food insecurity, and forced sexual exploitation.
Thematic Analysis
Several sub-themes and themes were identified across the data sample which has been summarised in Table 2.
Socio-Cultural Determinants
Across regions, socio-cultural norms anchored in patriarchal family structures, traditional gender roles, and religious interpretations were consistently identified as structural drivers of VAWG. In South Asia, dowry-related abuse and honour-based violence were particularly prevalent, reflecting entrenched gendered power hierarchies. Studies reported that victim-blaming, shame, and fear of social ostracisation inhibited help-seeking and reinforced the silence surrounding abuse. Cultural justifications for male dominance, often reinforced by religious or customary beliefs, perpetuated tolerance of intimate partner violence (IPV) and sexual coercion. In several settings, infertile women and elder housewives faced heightened emotional control and neglect due to rigid gender expectations, while women in rural communities frequently normalised violence as part of marital life.
Economic Determinants
Economic dependency emerged as a critical barrier to autonomy and safety. Limited access to education and formal employment increased women’s vulnerability to abuse and reduced their capacity to leave violent relationships. Financial stress, unemployment particularly among male partners and dowry demands were linked with elevated IPV risk. Women engaged in informal or low-wage labour, including garment factory work, were at heightened risk of workplace harassment, economic coercion, and exploitation. Several studies demonstrated that economic empowerment interventions, such as microfinance programmes or employment support, were associated with reductions in IPV, underscoring the interplay between economic security and gendered power dynamics.
Legal and Institutional Determinants
Weaknesses in legal systems and institutional responses were documented across multiple contexts. Survivors frequently encountered gender-insensitive policing, protracted judicial processes, and insufficient legal protections. In conflict-affected or post-disaster settings, legal recourse was often absent, militarised, or inaccessible. Gaps in shelter provision, psychosocial care, and legal aid were repeatedly cited as barriers to survivor recovery and justice. Institutional apathy and inadequate screening in healthcare settings limited opportunities for early intervention. Interventions incorporating structured community engagement or problem-solving training demonstrated measurable reductions in IPV incidence, highlighting the potential for targeted, context-sensitive institutional reforms.
Regional and Demographic Variations
Distinct patterns emerged by region and demographic group. Honour-based violence and dowry-related femicide were disproportionately reported in South Asia, while Southeast Asia exhibited higher prevalence of trafficking and sexual exploitation. Urban women were more likely to report IPV and cyber-harassment, whereas rural women often internalised violence as culturally normative. Vulnerable groups including adolescents, elderly women, migrants, and ethnic minorities experienced compounded marginalisation and were frequently excluded from formal support systems. In conflict zones, displaced women faced heightened risk of sexual violence, exacerbated by institutional absence.
Emerging Forms of Violence
Beyond physical and sexual IPV, studies identified emerging forms of violence, including cyber-violence (digital harassment, online blackmail, and non-consensual image sharing) and economic abuse (restriction of financial resources, education, and employment opportunities). These forms disproportionately affected adolescent girls, unmarried women, and urban populations. Workplace violence and elder neglect, which is often invisible in policy frameworks, were documented as significant yet under-recognised threats. In militarised contexts, sexual violence as a weapon of war persisted, with survivors facing near-total impunity for perpetrators.
Interplay Between Determinants of Violence Against Women and Girls
The analysis revealed a dynamic interplay between socio-cultural, economic, and legal determinants, where structural inequalities reinforced individual vulnerabilities. For example, patriarchal norms not only legitimised male control over household finances but also influenced institutional reluctance to enforce protective laws. Economic dependency both resulted from and contributed to legal and social marginalisation, while emerging forms of violence exploited gaps in legal frameworks and digital safety policies. Understanding these intersecting determinants is critical for designing integrated prevention and response strategies tailored to regional realities.
Sub-group Analysis
Psychological Intimate Partner Violence
Psychological IPV manifests in various emotionally abusive behaviours. Public humiliation, insults, intimidation, and threats of expulsion were widely reported. For instance, Yount et al. documented that between 9% and 27% of women reported lifetime exposure to different forms of psychological IPV. Satheesan et al. found that such abuse was associated with infertility, leading to lower marital satisfaction and psychological distress. Similarly, Deuba et al. and Gautam & Jeong highlighted how fear-inducing behaviours and threats impacted women’s physical and emotional well-being, especially during pregnancy [1,6].
Physical Intimate Partner Violence
This theme includes a spectrum of violent acts. Yount et al. identified slapping and striking as common, with 29% reporting lifetime exposure [13]. Shoving, observed by Pun et al., was a significant contributor to poor maternal and neonatal outcomes. Studies by Pun et al. and Bondade et al. linked physical IPV to adverse maternal and neonatal outcomes and psychiatric morbidity, particularly among infertile women. Additionally, Adhikari & Tamang found that 58% of married women experienced physical coercion, often used as a tool of control, while Gibbs et al. emphasized that threats of violence were a common feature, underlining the importance of economic interventions to mitigate such abuse [14]. Punching, as noted by Al Mamun et al., was common among garment workers, linking IPV to workplace stress and partner control. Beating, described by Adhikari & Tamang, frequently accompanied sexual coercion. Choking, reported by Bondade et al., was more prevalent among infertile women, leading to psychiatric conditions [15]. Threatening with physical harm, according to Gibbs et al., underscores the need for economic interventions to mitigate IPV [14]. Collectively, these forms reflect how physical violence is used to enforce control and exert dominance.
Sexual Intimate Partner Violence
Sexual IPV often overlaps with physical abuse. Adhikari & Tamang highlighted that coerced sex affected nearly 58% of married women, emphasizing how consent is undermined in intimate settings [3]. Pregnancy-related abuse, as shown by Taghizadeh et al., demonstrated the effectiveness of problem-solving training in reducing violence, offering a pathway for targeted interventions during vulnerable periods like pregnancy [24].
Economic Coercion
Economic dependency emerged as a critical enabler of IPV. Across several studies [13,15,22,27] women reported being denied financial autonomy and facing IPV linked to financial dependence. Clark et al. found that economic empowerment interventions significantly reduced IPV, highlighting the protective role of economic independence [28].
Dowry-related abuse was another economic sub-theme. Shah More et al. documented that IPV consultations were often related to economic expectations and dowry demands, indicating that monetary pressures and gender norms intersect to sustain abuse. Furthermore, employment restrictions were common. Dhungel et al. and Al Mamun et al. reported that factory-working women faced harassment and coercion, while Krishnan et al. noted that empowering both women and their mothers-in-law helped reduce IPV during pregnancy [4,25,29].
Socio-Cultural Factors
Socio-cultural structures deeply influence IPV dynamics. Patriarchal norms and gender roles were persistent drivers of violence. Studies by Sheikhan et al., Silwal et al., and Adhikari & Tamang highlighted how male dominance, stigma related to infertility, and expectations of female submission sustained IPV [3,8,9]. Leung et al. documented victim blaming health professionals, exacerbating women’s trauma [30].
Religious influences and gendered family roles also reinforced IPV. Deuba et al. indicated that alcohol use and denial of sex, framed through cultural or religious expectations, often triggered violence [6]. Studies by Yount et al., Satheesan et al., and Atilla & Akkus revealed that traditional family expectations, especially among elder housewives, led to neglect and psychological control [13,17,31].
Legal and Institutional Factors
Weak institutional frameworks and underperforming legal systems were major enablers of IPV. Clark et al. and Saggurti et al. emphasized the potential of community-based strategies and legal reforms to reduce IPV [21,28]. Yet, Deuba et al. and Nongrum et al. found that lack of police responsiveness, counselling services, and stigma severely limited women’s access to justice, especially in conflict-affected or remote regions [6,7].
Institutional responsiveness remains inconsistent. Taghizadeh et al. showed that training women in problem-solving skills during pregnancy helped prevent IPV [24]. Kataoka et al. introduced self-administered IPV screening, enhancing identification in clinical settings. However, Shah More et al. exposed ongoing gaps in institutional action, especially in cases involving dowry or cyber harassment [20].
Demographic Variations
IPV experiences vary by location and context. Rural versus urban disparities, studied by Bourey et al. and Nongrum et al., show that rural women face normalized traditional abuse, while urban women confront modern forms like cyber-harassment [7,16]. In conflict zones, highlighted by Gibbs et al., displaced women experience heightened IPV, compounded by a lack of state protection and services [14].
Emerging Forms of Intimate Partner Violence
New forms of IPV are gaining prominence. Cyber violence, reported by Shah More et al., is increasingly prevalent among young women in urban slums, revealing the digital extension of traditional abuse. Workplace violence, as found by Al Mamun et al., is closely tied to women’s economic vulnerability in informal labour settings. Lastly, elder neglect, identified by Atilla & Akkus, reflects how patriarchal norms persist across generations, leading to emotional abuse and isolation among older women [31].
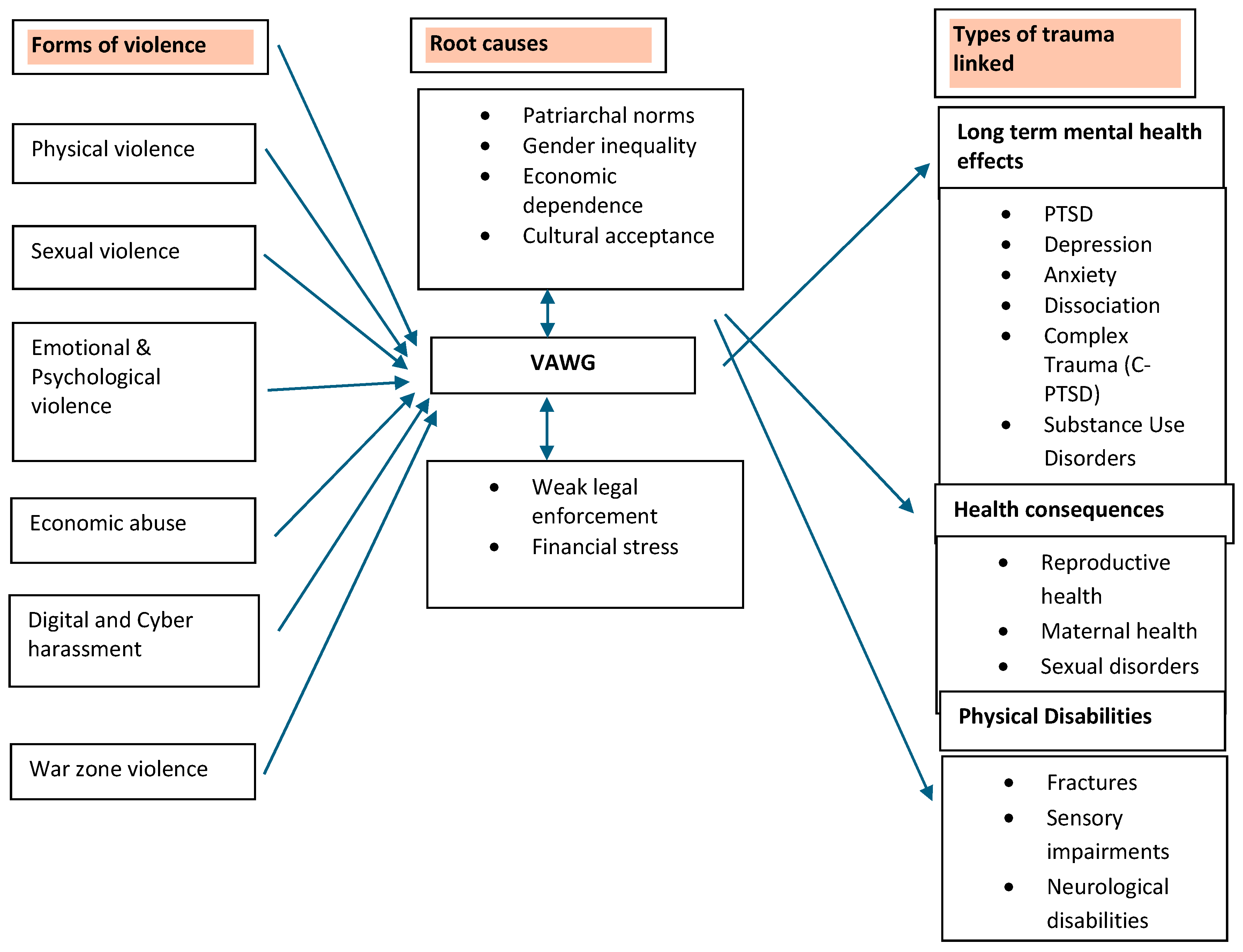
Figure 2.
Impact of trauma and causation tree in Violence Against Women and Girls (VAWG) in Asia.
Risk of Bias
Discussion
This systematic review reinforces the multifactorial and intersectional nature of VAGW in Asia. The findings reveal that VAWG is not merely the result of individual pathology or isolated incidents, but rather the product of deeply embedded socio-cultural, economic, and institutional structures. Each domain plays a distinct yet interrelated role in sustaining an environment in which violence is normalised, underreported, and often unaddressed.
Socio-Cultural Determinants: Entrenched Patriarchy and Harmful Norms
Patriarchal norms continue to be the dominant organising principle of gender relations across much of Asia. Women are expected to conform to rigid gender roles, with cultural and religious narratives often reinforcing male authority and female subordination [3,6]. In some contexts, violence is regarded as a private family matter rather than a social or legal issue [1]. The fear of shame, social exclusion, and dishonour discourages survivors from disclosing abuse or seeking support [7,22]. Additionally, polygamy and practices such as child marriage and dowry perpetuate women’s disempowerment, while framing their suffering as culturally or religiously acceptable sacrifices [14]
Intergenerational transmission of gendered norms emerged as a critical theme. Children raised in violent households often internalise these dynamics, perpetuating a cycle of abuse and normalisation [17,27]. The findings call for culturally grounded, community-based strategies that empower women while also engaging men and youth in challenging harmful norms.
Economic Dependency: Structural Poverty as an Enabler of Violence
Economic dependence and gendered poverty were consistently identified as risk factors for both experiencing and remaining in abusive relationships [13,14]. Limited access to education, vocational training, or secure employment confines women’s autonomy and reinforces their reliance on male partners. In some contexts, particularly in South Asia, dowry-related expectations continue to drive violence, coercion, and even femicide [9,15].
The findings also suggest that economic empowerment alone is insufficient if not accompanied by broader structural change. For instance, women employed in informal or low-wage sectors remained highly vulnerable to harassment, coercion, and violence,often without access to protection or recourse [4,29]. Programmes that combine financial literacy, legal awareness, and social support are more likely to create sustained improvements in safety and autonomy [16,19].
Legal and Institutional Gaps: Protection Without Enforcement
While legislative reforms have been enacted in many Asian countries, the review identifies a significant gap between law and practice. Survivors of violence frequently face systemic barriers, including gender bias among law enforcement officers, lack of timely investigations, and inadequate judicial outcomes [20,21]. Even in cases where women do seek justice, stigma and re-traumatisation are common (Krishnan et al., 2010; [30]].
In rural or conflict-affected areas, the legal vacuum is even more pronounced. Women rely on informal or customary justice mechanisms, which often prioritise family preservation over survivor safety [24,31]. Without coordinated support systems such as shelters, legal aid, and trauma-informed counselling—many survivors remain trapped in cycles of abuse [5,32].
Demographic and Regional Variations: Intersectionality of Risk
This systematic review highlights that VAWG is not experienced uniformly. Rural women face higher barriers to accessing services, while urban women report higher levels of emerging forms of violence, such as cyber abuse [16,20]. Conflict-affected populations, including refugees and displaced women, are at elevated risk of rape, trafficking, and impunity-driven abuse [14].
Strengths and Limitations
This review’s strengths include its comprehensive coverage of studies from diverse socio-economic and geopolitical contexts across Asia, and its integration of perspectives from public health, sociology, gender studies, and law to offer a holistic understanding of VAWG. The structured thematic synthesis enabled both the identification of common patterns and the recognition of context-specific drivers, while the intersectional lens allowed for focused analysis of particularly vulnerable groups. However, the exclusion of non-English language publications may have omitted valuable region-specific insights, and the heterogeneity in study design and quality limited the feasibility of quantitative synthesis. Geographic representation was uneven, with notable gaps in Central Asia and conflict-affected regions. Furthermore, the predominance of cross-sectional studies constrained causal inferences, underscoring the need for longitudinal, regionally inclusive, and methodologically robust research to guide effective policy and practice.
Implications for Policy and Practice
The persistent drivers of VAWG in Asia call for integrated, multisectoral approaches. Legal reform must be backed by institutional accountability, gender-sensitive training, and survivor-centred service delivery. Economic interventions must address the structural constraints that limit women’s autonomy. Community engagement including the participation of men, religious leaders, educators, and survivors is essential to shift harmful social norms.
Health systems can play a pivotal role by embedding violence screening in routine care, training staff in survivor-centred approaches, and linking women to legal and social support. Prevention efforts should address patriarchal attitudes at both household and community levels, while targeting emerging forms of violence that reflect changing social and technological landscapes.
Additionally, greater investment is needed in data systems and research infrastructure to monitor VAWG, especially in underrepresented and high-risk areas. The lack of longitudinal data, particularly from Central Asia and conflict zones, remains a critical gap.
Conclusions
This systematic review reinforces that VAGW in Asia is sustained by intersecting socio-cultural, economic, and institutional determinants. While legal and programmatic interventions exist, their impact is undermined by persistent patriarchal ideologies, structural poverty, and weak enforcement. Addressing VAWG demands an integrated approach that combines legislative reform, survivor-centred services, economic empowerment, and transformative community engagement. Sustained, multisectoral action is essential to dismantle systemic inequities, challenge harmful norms, and protect the rights and safety of women and girls.
Author Contributions
GD developed the ELEMI program and conceptualised the ANULA project. NW conducted the data extraction and wrote the first draft. The analysis was conducted by NW, JQS and GD. The manuscript was critically appraised and furthered by all other authors. All authors reviewed and commented on all versions of the manuscript. All authors read and approved the final manuscript.
Funding
NIHR Research Capability Fund.
Institutional Review Board Statement
Not applicable.
Consent to Participate
Not applicable.
Consent for Publication
All authors consented to publication.
Availability of Data and Material
All data included in the manuscript is publicly available.
Code Availability
Not applicable.
Acknowledgements
ELEMI Consortium.
Conflicts of Interest
None declared.
References
- Gautam, S.; Jeong, H.S. Intimate Partner Violence in Relation to Husband Characteristics and Women Empowerment: Evidence from Nepal. Int J Environ Res Public Health 2019, 16. [Google Scholar] [CrossRef]
- Ackerson, L.K.; Kawachi, I.; Barbeau, E.M.; Subramanian, S.V. Effects of individual and proximate educational context on intimate partner violence: A population-based study of women in India. Am J Public Health 2008, 98, 507–514. [Google Scholar] [CrossRef] [PubMed]
- Adhikari, R.; Tamang, J. Sexual coercion of married women in Nepal. BMC Womens Health 2010, 10, 31. [Google Scholar] [CrossRef] [PubMed]
- Dhungel, S.; Dhungel, P.; Dhital, S.R.; Stock, C. Is economic dependence on the husband a risk factor for intimate partner violence against female factory workers in Nepal? BMC Womens Health 2017, 17, 82. [Google Scholar] [CrossRef] [PubMed]
- Chandra, P.S.; Satyanarayana, V.A.; Carey, M.P. Women reporting intimate partner violence in India: Associations with PTSD and depressive symptoms. Arch Womens Ment Health 2009, 12, 203–209. [Google Scholar] [CrossRef]
- Deuba, K.; Mainali, A.; Alvesson, H.M.; Karki, D.K. Experience of intimate partner violence among young pregnant women in urban slums of Kathmandu Valley, Nepal: A qualitative study. BMC Womens Health 2016, 16, 11. [Google Scholar] [CrossRef]
- Nongrum R, Thomas E, Lionel J, Jacob KS. Domestic violence as a risk factor for maternal depression and neonatal outcomes: A hospital-based cohort study. Indian J Psychol Med. 2014, 36, 179–181. [CrossRef]
- AU - Silwal A, AU - Thapa B, 2020/06/30 P-, 2025/08/17 Y-, Article S-O, 10.31729/jnma.4886 D-; et al. Prevalence of Domestic Violence among Infertile Women attending Subfertility Clinic of a Tertiary Hospital. J Nepal Med Assoc. 58(226).
- Sheikhan, Z.; Ozgoli, G.; Azar, M.; Alavimajd, H. Domestic violence in Iranian infertile women. Medical Journal of the Islamic Republic of Iran (MJIRI) 2014, 28, 152. [Google Scholar]
- Hesketh, T.; Lu, L.; Xing, Z.W. The consequences of son preference and sex-selective abortion in China and other Asian countries. Cmaj 2011, 183, 1374–1377. [Google Scholar] [CrossRef]
- Aygül Akyüz GŞ, Memnun Seven, Bilal Bakır. The Effect of Marital Violence on Infertility Distress among A Sample of Turkish Women. International Journal of Fertility and Sterility. 2014, 8.
- Ardabily HE, Moghadam ZB, Salsali M, Ramezanzadeh F, Nedjat S. Prevalence and risk factors for domestic violence against infertile women in an Iranian setting. Int J Gynaecol Obstet. 2011, 112, 15–17. [CrossRef]
- Yount KM, Krause KH, VanderEnde KE. Economic Coercion and Partner Violence Against Wives in Vietnam: A Unified Framework? J Interpers Violence. 2016, 31, 3307–3331. [CrossRef] [PubMed]
- Gibbs A, Corboz J, Jewkes R. Factors associated with recent intimate partner violence experience amongst currently married women in Afghanistan and health impacts of IPV: A cross sectional study. BMC Public Health 2018, 18, 593.
- Bondade S, Iyengar RS, Shivakumar BK, Karthik KN. Intimate Partner Violence and Psychiatric Comorbidity in Infertile Women - A Cross-Sectional Hospital Based Study. Indian J Psychol Med. 2018, 40, 540–546. [CrossRef] [PubMed]
- Bourey C, Stephenson R, Hindin MJ. Reproduction, functional autonomy and changing experiences of intimate partner violence within marriage in rural India. Int Perspect Sex Reprod Health. 2013, 39, 215–226. [CrossRef]
- Satheesan SC, Satyaranayana VA. Quality of marital relationship, partner violence, psychological distress, and resilience in women with primary infertility. International Journal Of Community Medicine And Public Health. 2018, 5(2).
- Coskuner Potur D, Onat G, Dogan Merih Y. An evaluation of the relationship between violence exposure status and personality characteristics among infertile women. Health Care Women Int. 2019, 40, 1135–1148. [CrossRef]
- Koenig MA, Stephenson R, Acharya R, Barrick L, Ahmed S, Hindin M. Domestic violence and early childhood mortality in rural India: Evidence from prospective data. Int J Epidemiol. 2010, 39, 825–833. [CrossRef]
- Neena Shah More SD, Ujwala Bapat, Mahesh Rajguru, Glyn Alcock, Wasundhara Joshi, Shanti Pantvaidya and David Osrin. Community resource centres to improve the health of women and children in Mumbai slums: Study protocol for a cluster randomized controlled trial. Bio med central.
- Saggurti N, Nair S, Silverman JG, Naik DD, Battala M, Dasgupta A; et al. Impact of the RHANI Wives intervention on marital conflict and sexual coercion. Int J Gynaecol Obstet. 2014, 126, 18–22. [CrossRef]
- Clark CJ, Ferguson G, Shrestha B, Shrestha PN, Batayeh B, Bergenfeld I; et al. Mixed methods assessment of women’s risk of intimate partner violence in Nepal. BMC Womens Health. 2019, 19, 20.
- Kalokhe A, Del Rio C, Dunkle K, Stephenson R, Metheny N, Paranjape A, Sahay S. Domestic violence against women in India: A systematic review of a decade of quantitative studies. Glob Public Health. 2017, 12, 498–513. [CrossRef]
- Taghizadeh Z, Pourbakhtiar M, Ghasemzadeh S, Azimi K, Mehran A. The effect of training problem-solving skills for pregnant women experiencing intimate partner violence: A randomized control trial. Pan Afr Med J. 2018, 30, 79.
- Suneeta Krishnan KS, Prabha Chandra3 and Krishnamachari Srinivasan. Minimizing risks and monitoring safety of an antenatal care intervention to mitigate domestic violence among young Indian women: The Dil Mil trial. BMC Public health. 2012.
- DilekAkkuş ASM. Domestic Violence Against 116 Turkish Housewives: A Field Study. Women & Health. 2004, Vol. 40(3).
- Pun KD, Rishal P, Darj E, Infanti JJ, Shrestha S, Lukasse M; et al. Domestic violence and perinatal outcomes - a prospective cohort study from Nepal. BMC Public Health. 2019, 19, 671.
- Clark CJ, Spencer RA, Shrestha B, Ferguson G, Oakes JM, Gupta J. Evaluating a multicomponent social behaviour change communication strategy to reduce intimate partner violence among married couples: Study protocol for a cluster randomized trial in Nepal. BMC Public Health. 2017, 17, 75.
- Al Mamun M, Parvin K, Yu M, Wan J, Willan S, Gibbs A; et al. The HERrespect intervention to address violence against female garment workers in Bangladesh: Study protocol for a quasi-experimental trial. BMC Public Health. 2018, 18, 512.
- Leung TW, Leung WC, Ng EH, Ho PC. Quality of life of victims of intimate partner violence. Int J Gynaecol Obstet. 2005, 90, 258–262. [CrossRef] [PubMed]
- Mayda AS, Akkus D. Domestic violence against 116 Turkish housewives: A field study. Women Health. 2004, 40, 95–108.
- Sis Celik A, Kirca N. Prevalence and risk factors for domestic violence against infertile women in a Turkish setting. Eur J Obstet Gynecol Reprod Biol. 2018, 231, 111–116. [CrossRef]
Figure 1.
PRISMA Flow diagram.
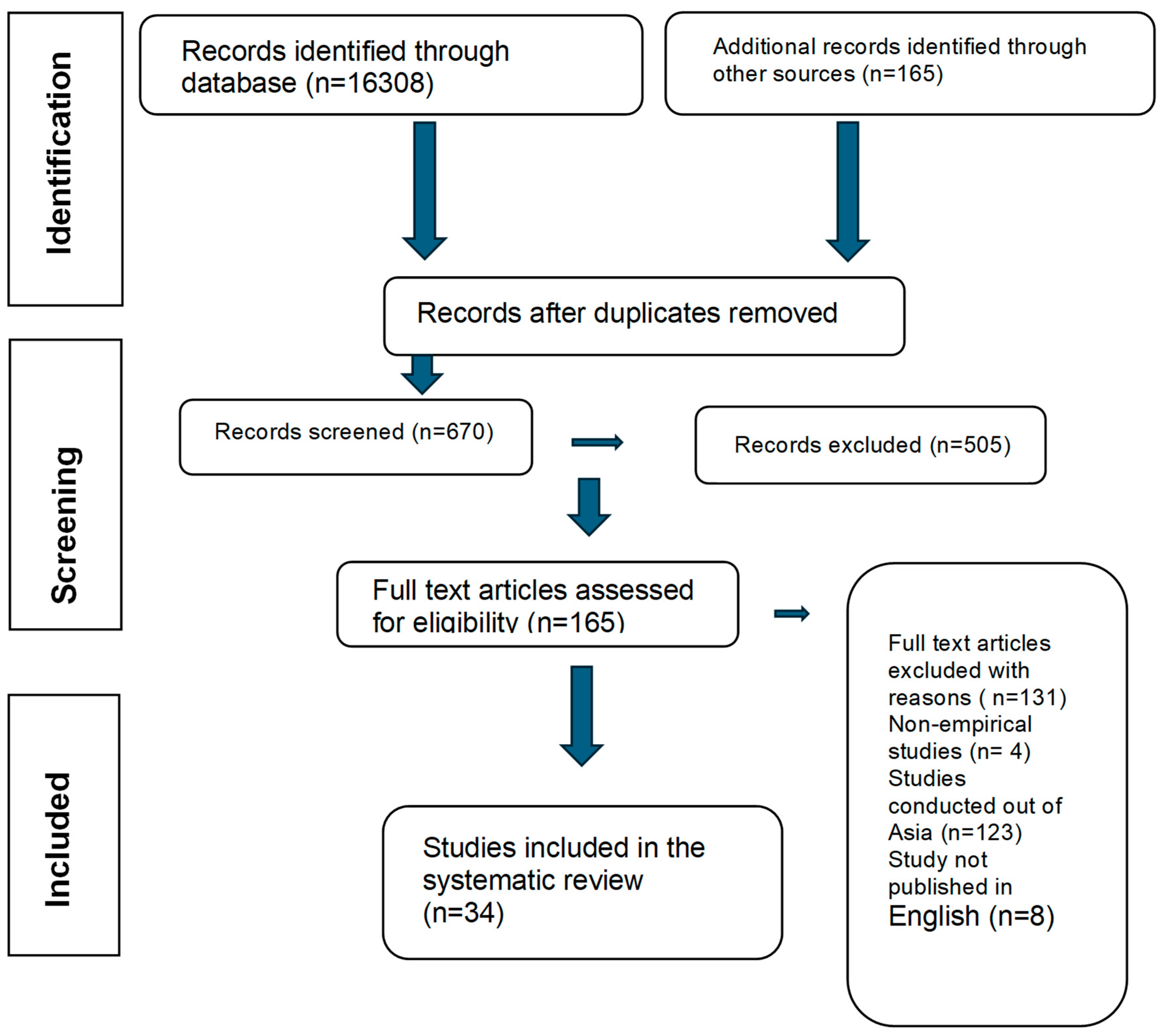

Table 1.
Characteristics of the studies included in the systematic review.
| Id | Author | Country | Study type | Methods | Setting | Population | Age | Sample size | Findings/ outcomes | Outcome measure |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Yount et al. | Vietnam | Population-based household | Survey | Community | Married women | 18-50 years | 533 | Determinants of economic coercion and common forms of IPV | Survey questionnaire |
| 2 | Silwal et al. | Nepal | Cross-sectional | Descriptive | Acute | Infertile women | 15-44 years | 112 | Women experiencing infertility are exposed to various forms of domestic violence | Standard tool used in Nepal demographic and health survey (NDHS),2016 |
| 3 | Z. Sheikhan, et al. | Iran | Cross- sectional | Descriptive | Fertility centre, (private) | Infertile women | Nr | 400 | Domestic violence and fertility | Researcher made questionnaire |
| 4 | Akyüz et al. | Turkey | Cross-sectional | Descriptive | In vitro fertilization (IVF) centre at military medical academy | Married women who applied to an in vitro fertilization | Nr | 139 | Marital violence is a factor increasing the distress of infertile women. | A descriptive questionnaire developed by the researcher |
| 5 | Bondade et al. | India | Cross-sectional | Descriptive | Oxford medical college hospital And research centre, Bangalore |
Women with primary infertility | 18 -45 years | 100 | A significant number of women who had infertility reported IPV. Women with IPV had higher psychiatric comorbidity and may require psychotherapeutic intervention. |
Psychiatric diagnosis-dsm-5. Hamilton anxiety rating scale (ham-a) and Hamilton depression rating scale (ham-d) IPV -who violence against women instrument. |
| 6 | Leung et al. | China | Case-control | Quantitative | Queen Mary Hospital | Patients seeking medical help from the department Of obstetrics and gynaecology |
Nr | 1614 |
Prevalence of intimate partner violence The quality of life of abused women. |
Structured questionnaire modified from the abuse assessment screen questionnaire |
| 7 | Pun et al. | Nepal | Prospective cohort study | Quantitative | Two hospitals in Nepal | Pregnant women | 1381 | Violence is a potential risk factor for severe morbidity and mortality in newborns. | The abuse assessment screen (modified) | |
| 8 | Satheesan SC et al. | India | Cross sectional | Quantitative | Infertility hospital in Bangalore | Adult women | 18+ years | 30 | High rates of intimate partner violence (47%) Poorer quality of marital relationship was associated with higher levels of psychological distress and lower resilience |
Marital quality scale, domestic violence Questionnaire, depression anxiety stress scale-21, and Connor Davidson resilience scale |
| 9 | Gibbs et al. | Afghanistan | Cross-sectional | Descriptive | Villages | Married women | 18 -49 years | 935 | Importance of economic empowerment interventions to reduce women’s experiences of IPV | Structured paper and pencil questionnaires |
| 10 | Al Mamun et al. | Bangladesh | Quasi-experimental | Quantitative | Factories | Garment workers | Nr | 800 | Evaluate the impact on IPV and WPV | |
| 11 | Kataoka et al. | Japan | Randomised control trial | Quantitative | Prenatal clinic | Pregnant women | 328 | Self-administered questionnaire versus interview as a screening method for intimate partner violence | Self-administered questionnaire and interviews | |
| 12 | Clark et al. | Nepal | Randomised control trial | Mixed methods | Community | Female participants | Nr | 1440 individuals | The effectiveness of a promising strategy to prevent IPV | Survey, focus group discussions, interviews |
| 13 | Taghizadeh et al., | Tehran | Randomised control trial | Quantitative | Health centres of Tehran | Pregnant women | Nr | 142 | The effectiveness of training problem-solving skills on IPV against pregnant women | Conflict tactics scale questionnaire |
| 14 | Shah more et al. | India | Randomised control trial | Quantitative | Urban slum areas | Women and children | Women-15 to 49 years Children undue age 5 |
600 households | The number of consultation for violence against women or children | Interviews |
| 15 | Krishnan et al. | India | Randomised control trial | Quantitative | Primary health centres and community | Young pregnant women in 1st or 2nd trimesters | Nr | 144 | Incidence of domestic violence, the empowerment of daughter-in -law and mother -in -law | Interview |
| 16 | Bourey et al., | India | Prospective cohort | Quantitative | Rural areas | Married women | Nr | 4,749 | Economic contribution, pregnancy, and violence | Survey |
| 17 | D. Cos¸kuner potur et al., | Turkey | Cross-sectional | Descriptive | Acute | Infertile women | Nr | 315 | Infertility treatment duration and violence | An introductory information form, The Eysenck personality questionnaire revised-abbreviated Form (EPQR-a), and the infertile women’s exposure to Violence determination scale (IWEVDS) |
| 18 | Atilla s. Mayda and Dilek akkus | Turkey | Cross-sectional | Survey | Community | Housewives | Nr | 116 | Prevalence and forms of domestic violence (physical, emotional, sexual); demographic correlates | Survey |
| 19 |
H.E. Ardabil et al. | Iran | Cross sectional | Survey | Valais reproductive health research centre, Tehran university of medical science | Infertile women | Nr | 400 | Infertility and domestic violence | Revised conflict tactics scales questionnaire |
| 20 | Adhikari and Tamang | Nepal | Cross sectional | Survey | Community | Married women | 15-49 years | 1536 | About three in five women (58%) had experienced some form of sexual coercion by them Husbands. |
Structured questionnaire |
| 21 | Deuba et al. | Nepal | Qualitative | Interview | Urban slums | Young pregnant women | 15-24 years | 20 | Having a husband who has alcohol use Disorder, identification of foetal gender, and refusal to Have sex were fuelling factors that instigated IPV among Young pregnant women in urban slums |
in depth interviews |
| 22 | Nongrum et al. | India | Cross sectional | Quantitative | Urban | Women | Nr | 126 | High IPV; lack of services in ne region | Edinburgh postnatal depression scale, abuse assessment screen, maternal and neonatal outcome pro forma |
| 23 | Gautam and Jeong | Nepal | Cross sectional | Survey | Community and hospital setting | Men and women | 15–49 years | 12,862 women and 4063 men | Gender-based violence (or IPV) produces significant public health concerns resulting in physical, Sexual and reproductive, and psychological health problems and presents a violation of women’s Human rights. |
Nepal demographic And health survey (NDHS) 2016 |
| 24 | Saggurti et al. | India | Randomised control trial | Quantitative | Low income community | Married women | 18–40 years | 220 | Community intervention reduced IPV significantly | Survey |
| 25 | Dhungel et al. | Nepal | Cross sectional | Quantitative | Factory | Working women | 15–49 years |
236 | Workplace harassment and economic coercion reported | A standardized, closed Ended questionnaire |
| 26 | Koenig et al. | India | Prospective cohort | Survey | Rural areas | Women | 15–49 years | 89199 | IPV prevalence tracked across regions and time |
Survey |
| 27 | A. Sis Celik, n. Kırca | Turkey | Cross sectional | IVF centre, community | Infertile women | 423 | High IPV rates among infertile women; stigma influences violence | Sociodemographic questionnaire” and “infertile women’s expo- Sure to violence determination scale |
||
| 28 | Chandra et al. | India | Cross sectional | Quantitative | Adult psychiatry outpatient unit of National institute of mental health and neurosciences |
Women | 18 to 49 years | 105 | 56% of this sample of Indian women seeking help for common Mental health problems reported at least one form of intimate partner violence. |
Structured interview Severity of abuse was assessed by the index of spouse abuse (isa; Hudson and McIntosh Sexual coercion was assessed using the sexual experiences scale (ses; Koss and Oros Depression was assessed using the beck depression inventory Post-traumatic symptom checklist |
| 29 | Ackerson et al. | India | Cross sectional | Descriptive | Community | Ever-married women | 15 To 49 years |
83627 |
Reporting IPV is high when women educational level is higher. | Survey |
| 30 | Ackerson and Subramanian | India | Cross sectional | Rural areas | Ever-married women | 15 To 49 years |
69,072 |
Domestic violence and malnutrition indicators | Survey | |
| 31 | Choudhary et al. | Nepal | Cross sectional | Quantitative | Urban and rural areas | Women | Nr | 3708 | Sub-optimal water access and the probability of IPV against Women. |
Interview |
| 32 | Bhatta, Assanangkornchai, & Rajbhandari, 2021 | Nepal | Cross sectional | Quantitative | Acute | Women in pregnancy | 15 To 49 years |
660 | DV is significantly associated with husband’s alcohol consumption, controlling behaviour | Validated questionnaire |
| 33 | Akar et al. | Turkey | Cross sectional | Quantitative | Primary care health centres affiliated with Gazi university, Ankara | Married women | Nr | 1178 | Lifetime IPV prevalence: 77.9% | Structure questionnaire |
| 34 | Bloom et al. | Eswatini | Cross sectional | Quantitative | Acute | Pregnant women | Nr | 406 | Women who were food insecure or reported constrained agency (e.g., sex due to poverty, pressure) were at greater risk of reporting IPV. | Who violence against women Scale |
Table 2.
Thematic Analysis Outcomes.
| Themes | Sub-themes | Study | Key findings |
|---|---|---|---|
| Psychological Intimate Partner Violence | Public humiliation | Yount et al. Choudhary et al. |
Between 9% and 15% of women reported lifetime exposure to specific forms of psychological IPV; 27% reported lifetime exposure to any psychological IPV. |
| Insult & Degradation | Satheesan et al. | Psychological IPV linked to lower marital quality and higher psychological distress in women facing infertility. | |
| Fear &Intimidation | Deuba et al. Pun et al. |
Alcohol use by husbands and sex refusal led to fear-inducing behaviour and violence against young pregnant women. Both violence and fear was significantly associated with giving birth to a preterm infant |
|
| Threat & Expulsion | Gautam & Jeong Atilla & Akkus Deuba et al. Satheesan et al. |
IPV produces long-term psychological, physical, and sexual health problems and violates women’s rights. | |
| Emotional abuse | Akyüz et al. Gibbs et al. T.W.Leung et al. |
Emotional abuse is prevalent, linked to depression and low marital satisfaction among Turkish women. Majority (61.5%) of the victims suffered from emotional or verbal abuse |
|
| Physical Intimate Partner Violence | Slap & strike | Yount et al. A. Sis Celik, N. Kırca Choudhary et al. |
29% reported lifetime exposure to any physical IPV. 30% expressed to be injured as a result of the violence |
| Shoving | Pun et al. Yount et al. |
IPV is a risk factor for poor maternal and neonatal health outcomes. | |
| Punching | Al Mamun et al. Choudhary et al. |
IPV prevalence remains high among garment workers, links to workplace stress and partner control | |
| Beating | Adhikari & Tamang Choudhary et al. H.E. Ardabily et al. |
58% of married women experienced sexual coercion; physical force commonly used to assert control. 8% of infertile women experienced injuries. |
|
| Chocking | Bondade et al. | Infertile women reported higher rates of physical IPV and associated psychiatric morbidity. | |
| Threatening | Gibbs et al. | Economic interventions are key to reducing IPV, which often includes physical threats. | |
| Sexual Intimate Partner Violence | Coerced sex | Adhikari & Tamang Saggurti et al. |
About 58% of women had experienced sexual coercion by their husbands. |
| Pregnancy-related abuse | Taghizadeh et al. | IPV against pregnant women decreased through problem-solving training, showing strong preventive potential. | |
| Economic Coercion | Financial control/ dependency | Yount et al. Bondade et al. Pun et al. Clark et al. Bourey et al., Deuba et al. |
3%–21% of women reported economic coercion such as being denied financial autonomy. Infertile women reported higher IPV and psychiatric morbidity due to dependency. IPV is a risk factor for poor maternal and neonatal outcomes, particularly in low-income settings. Economic interventions and empowerment programs effectively reduce IPV. Changes in financial autonomy and freedom of movement were reported by 38% and 44% of the women. |
| Dowry-related abuse | Shah More et al. Bourey et al. |
Consultations for IPV often related to dowry demands; economic expectations used to justify abuse. | |
| Employment restrictions | Dhungel et al. Al Mamun et al. Krishnan et al. Shah More et al. |
Working women in factories experienced harassment and economic coercion tied to gender roles. Workplace IPV is linked to economic vulnerability among garment workers. Empowerment of women (and mothers-in-law) can reduce IPV during pregnancy. Consultations for IPV were tied to economic factors like dowry demands. |
|
| Socio-Cultural Factors | Patriarchy & gender norms | Sheikhan et al. Silwal et al. Adhikari & Tamang |
Cultural beliefs reinforcing male dominance and stigma toward infertile women sustain IPV. 58% of married women experienced sexual coercion; physical force used to assert control. |
| Victim blaming | Leung et al. | Women reporting IPV had reduced quality of life and often faced judgment from health professionals. | |
| Religious influences | Deuba et al. | Alcohol use and sex refusal fuelled IPV; influenced by cultural and possibly religious values. | |
| Gendered family roles | Yount et al. Sheikhan et al. Satheesan et al. Gautam & Jeong Atilla & Akkus |
Lifetime exposure to psychological and physical IPV often stems from traditional roles. Infertility and IPV linked to poor marital quality and increased psychological distress. IPV leads to physical, sexual, and reproductive health issues, and violates human rights. Elder housewives face emotional control and neglect due to traditional expectations. |
|
| Legal & Institutional Factors | Weak justice systems | Clark et al. Saggurti et al. |
Legal reforms and community-based strategies can effectively reduce IPV incidence. RCT shows interventions can reduce IPV through structured community engagement. |
| Limited support services | Deuba et al. | Lack of counselling and police responsiveness discourages IPV reporting. | |
| Access to justice | Deuba et al. Nongrum et al. |
IPV is underreported due to stigma and lack of police responsiveness. Women in conflict-affected or remote areas struggle to access protection. |
|
| Institutional responsiveness | Taghizadeh et al. Kataoka et al. Shah More et al. |
Training in problem-solving skills effectively reduced IPV during pregnancy. IPV screening improved with self-administered questionnaires in clinical settings. IPV related to dowry and cyber harassment indicates gaps in institutional response. |
|
| Demographic Variations | Rural vs urban disparity | Bourey et al. Nongrum et al. | Rural women face normalized abuse due to tradition, while urban women are more exposed to cyber-harassment. |
| Conflict zones | Gibbs et al. | High IPV rates among displaced women; compounded by lack of institutional protection. | |
| Emerging Forms of Intimate partner Violence | Cyber violence | Shah More et al. | Digital harassment is increasingly reported among young and unmarried women in urban slums |
| Workplace violence | Al Mamun et al. | Workplace IPV is linked with economic vulnerability and informal labour settings | |
| Elder neglect | Atilla & Akkus | Elder housewives in patriarchal settings experience neglect and emotional control. |
Table 3.
Risk of bias assessing observational studies using Newcastle Ottawa Quality Assessment Scale.
Table 3.
Risk of bias assessing observational studies using Newcastle Ottawa Quality Assessment Scale.
| No | Authors | Selection (S) | Comparability (C) | Exposure / Outcome (E/O) | Total stars | Conclusion | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 1 | 2 | 3 | |||||
| 1 | Silwal et al.,2020 | * | * | ** | * | * | ****** | Moderate risk | |||
| 2 | Z.Sheikhan, et al.,2014 | * | * | * | ** | * | ****** | Moderate risk | |||
| 3 | Akyüz et al. | * | * | ** | * | * | ****** | Moderate risk | |||
| 4 | Bondade et al. | * | * | * | ** | * | * | * | ******** | Low risk | |
| 5 | T.W.Leung et al. | * | * | * | * | * | ***** | Moderate risk | |||
| 6 | Pun et al. | * | * | * | * | * | * | ****** | Moderate risk | ||
| 7 | Satheesan SC et al. | * | * | * | * | * | ***** | Moderate risk | |||
| 8 | Gibbs et al. | * | * | * | * | * | ***** | Moderate risk | |||
| 9 | Bourey et al. | * | * | * | ** | * | ****** | Moderate risk | |||
| 10 | D. Cos ̧Kuner Potur et al. | * | * | ** | **** | High risk | |||||
| 11 | Koenig et al. | * | * | * | ** | * | * | * | ******** | Low risk | |
| 12 | Yount et al. | * | * | * | * | * | * | * | ******* | Low risk | |
| 13 | H.E. Ardabily et al. | * | * | * | ** | * | ****** | Moderate risk | |||
| 14 | Chandra et al.,2009 | * | * | * | * | * | ***** | Moderate risk | |||
| 15 | Ackerson et al.,2008 | * | * | * | ** | * | ****** | Moderate risk | |||
| 16 | Ackerson and Subramanian | * | * | * | ** | * | ****** | Moderate risk | |||
| 17 | Atilla S. Mayda and Dilek Akkus | * | * | * | High risk | ||||||
| 18 | Gautam and Jeong | * | * | * | ** | * | ****** | Low risk | |||
| 19 | Choudhary et al. | * | * | * | ** | * | * | ******* | Low risk | ||
| 20 | A. Sis Celik, N. Kırca | * | * | * | * | * | * | ****** | Moderate risk | ||
| 21 | Dhungel et al. | * | * | * | * | * | * | * | ******* | Low risk | |
| 22 | Clark et al., 2019 | * | * | * | * | * | * | ****** | Moderate risk | ||
| 23 | Akar et al. (2010) | * | * | * | * | * | * | ****** | Moderate risk | ||
| 24 | Bhatta, Assanangkornchai, & Rajbhandari, 2021 | * | * | * | ** | * | * | ******* | Low risk | ||
| 25 | Bloom et al. | * | * | * | ** | * | * | ******* | Low risk | ||
| 26 | Nogrum et al. | * | * | * | * | ** | * | * | * | ********* | Low risk |
Table 4.
Risk of bias assessing randomised control trial using Cochrane Collaboration’s tool (Risk of bias assessment was carried out using the RoB 2 tool).
Table 4.
Risk of bias assessing randomised control trial using Cochrane Collaboration’s tool (Risk of bias assessment was carried out using the RoB 2 tool).
 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



