Submitted:
28 August 2025
Posted:
29 August 2025
You are already at the latest version
Abstract
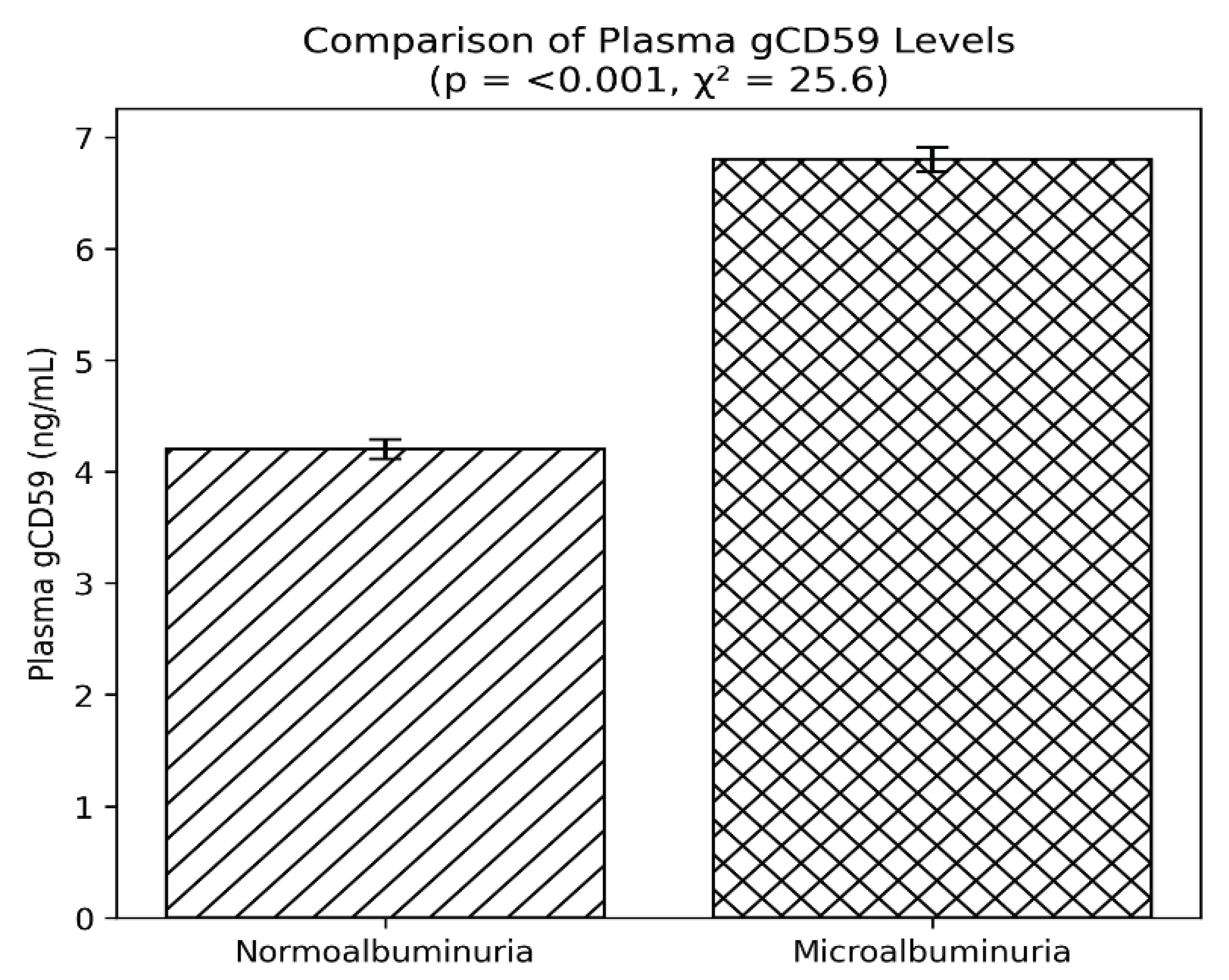
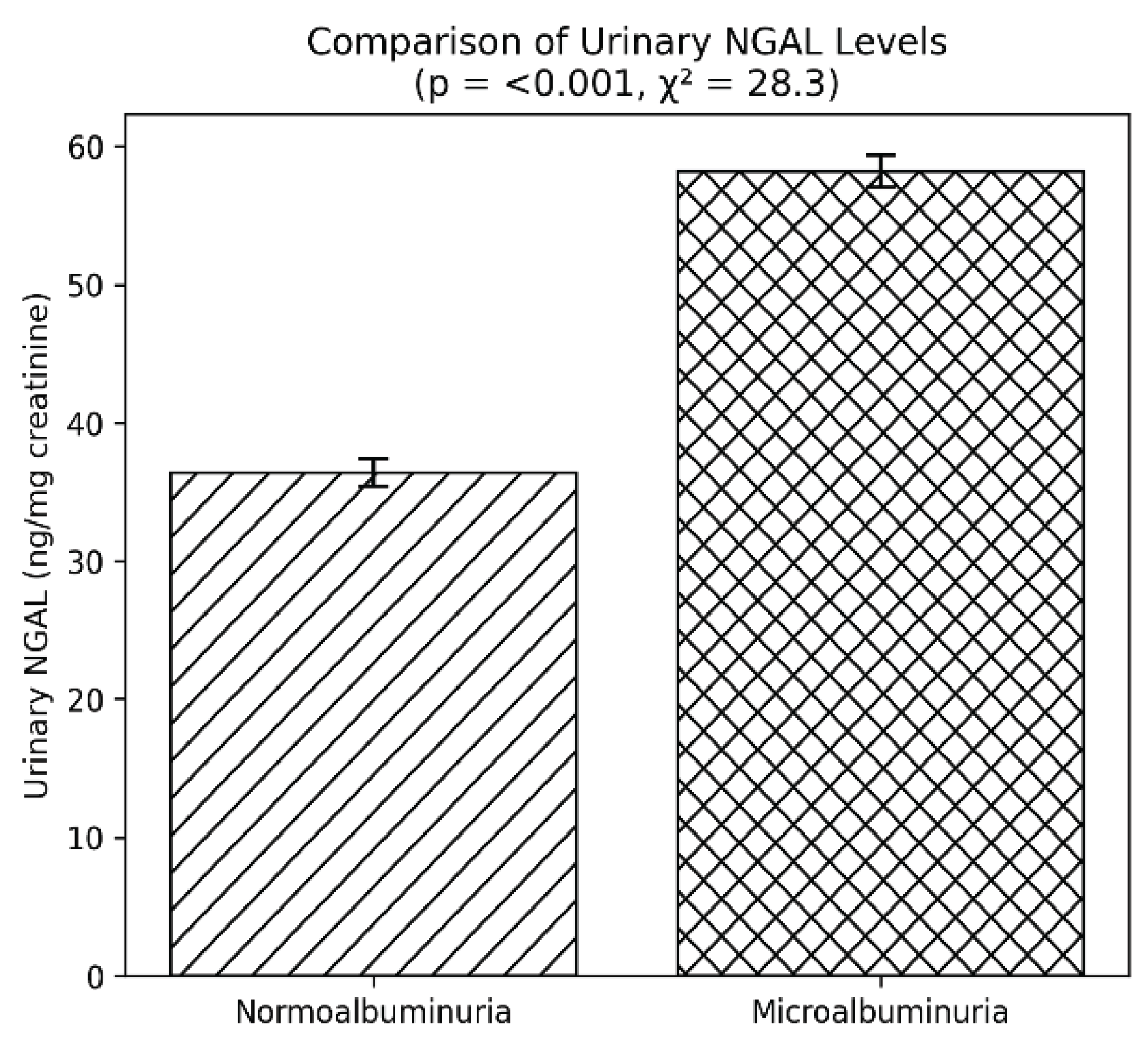
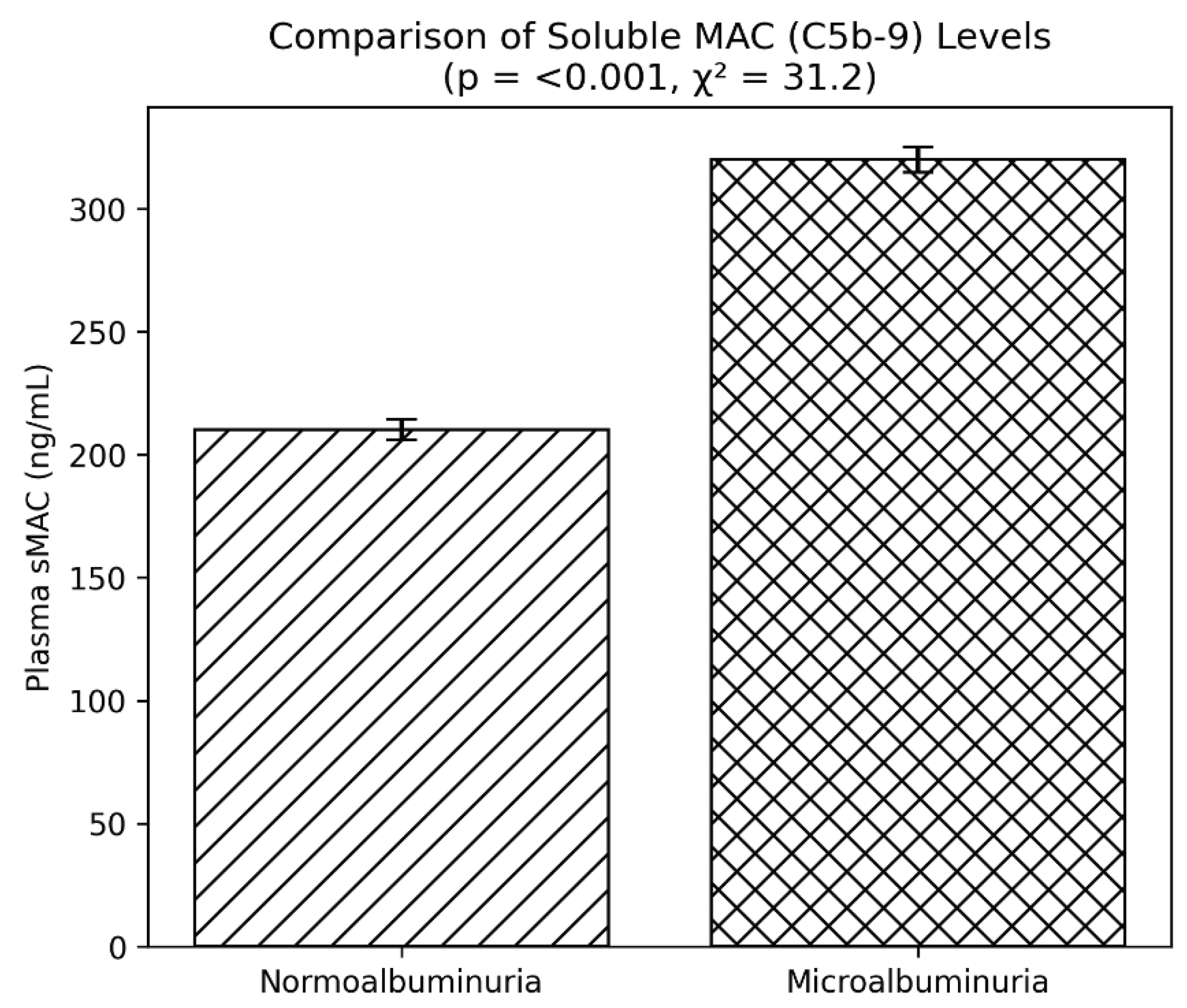
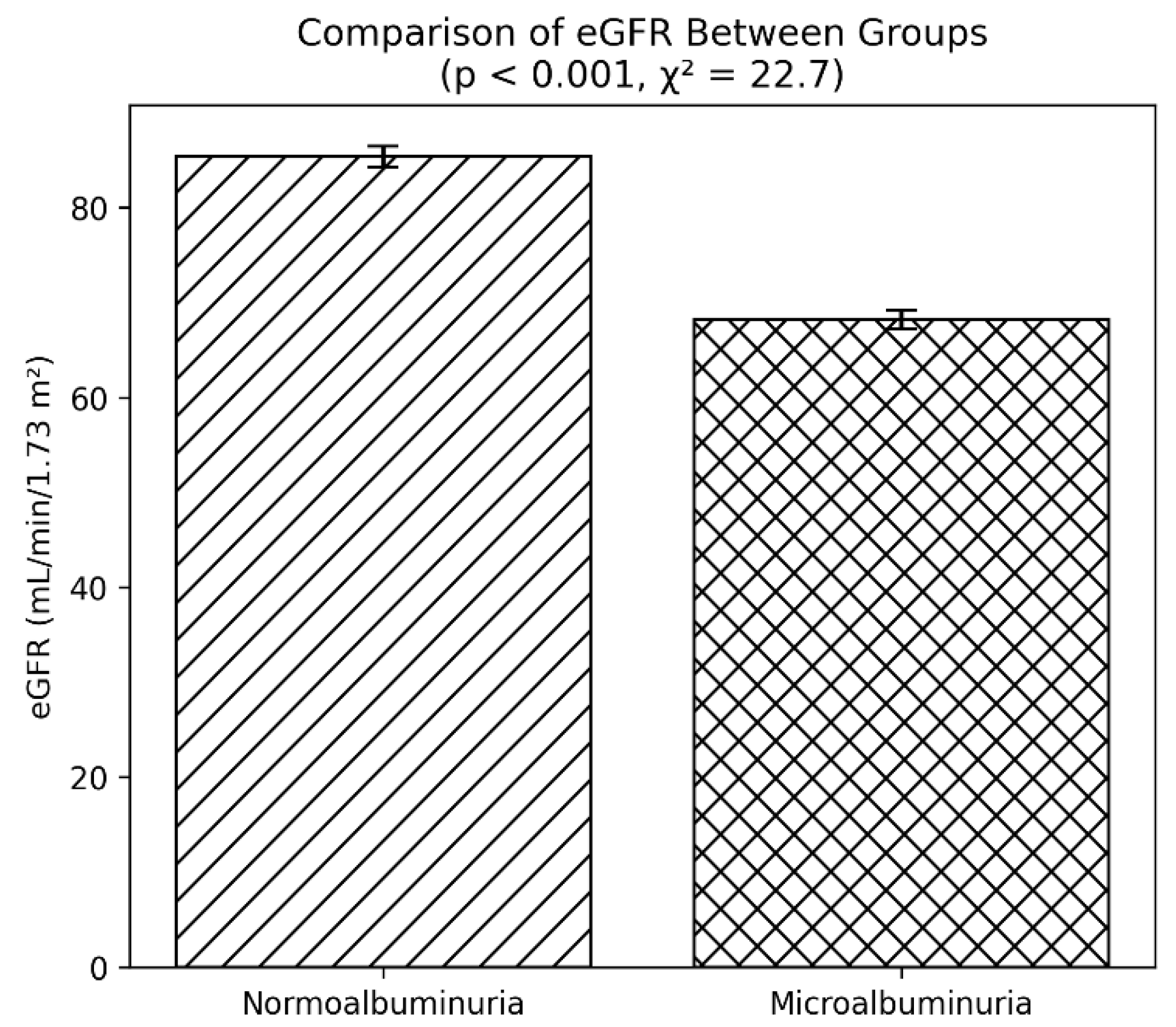
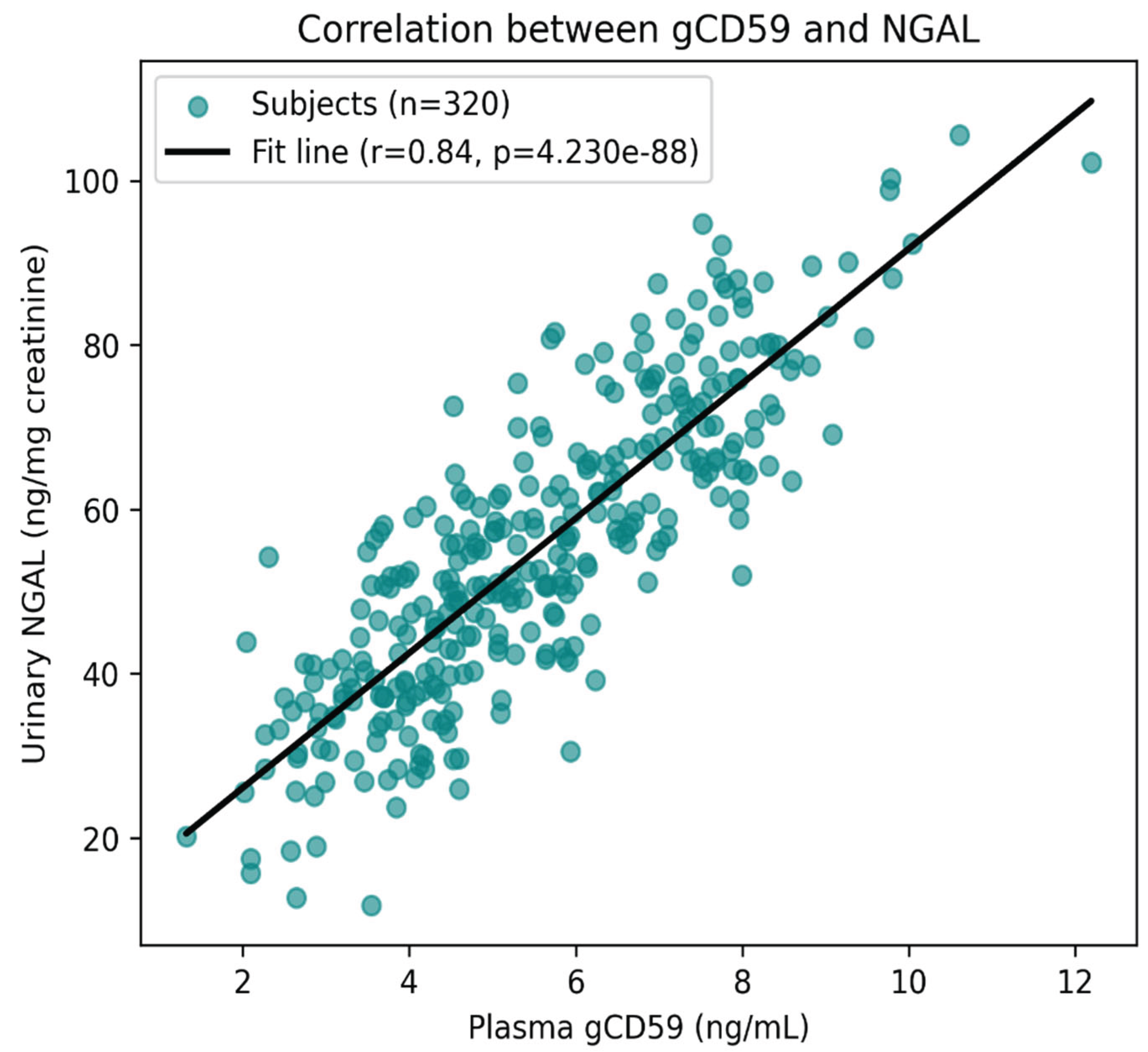
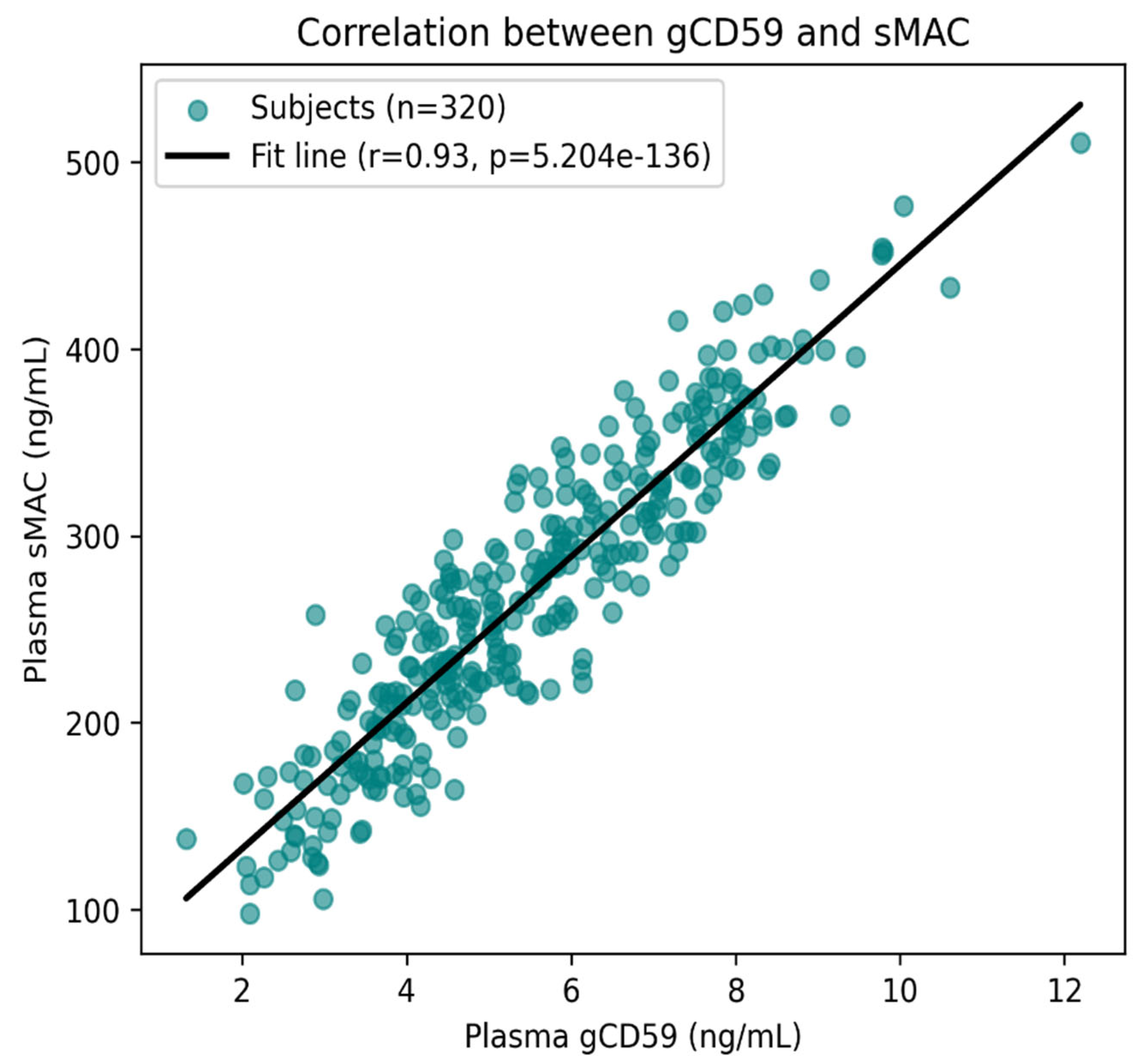
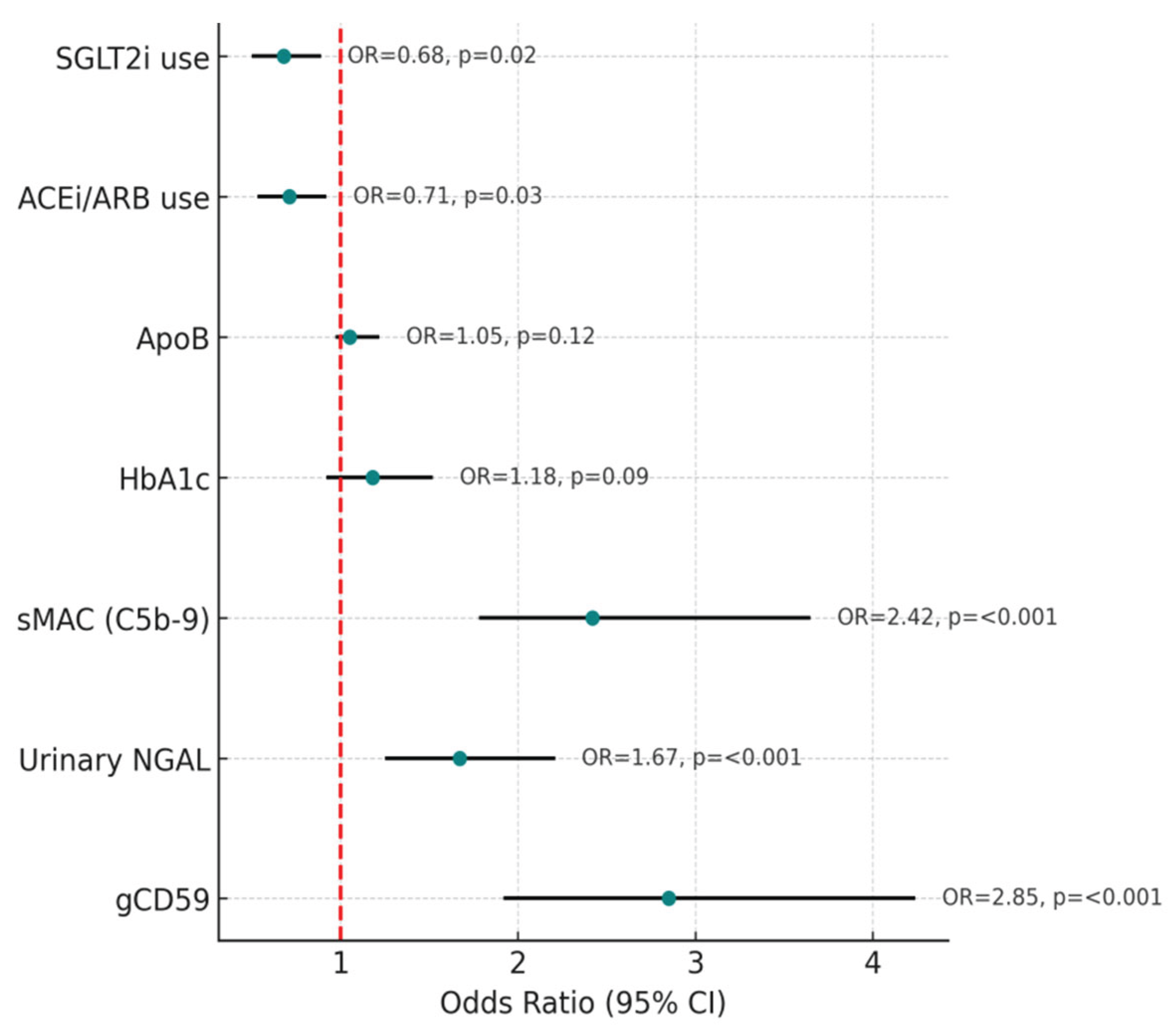
Background: Diabetic nephropathy (DN) is a major complication of type 2 diabetes (T2D). Conventional markers such as microalbuminuria and HbA1c provide limited predictive value. Glycated CD59 (gCD59), a complement-regulatory protein modified under hyperglycaemia, may serve as a novel biomarker. This study evaluated the relationship of gCD59 with renal function, tubular injury, inflammation, endothelial dysfunction, and complement activation in T2D patients. Methods: A total of 320 T2D patients were enrolled and divided equally into groups with and without microalbuminuria (n = 160 each). Laboratory parameters included HbA1c, estimated glomerular filtration rate (eGFR; creatinine ± cystatin C), and plasma gCD59. Urinary neutrophil gelatinase-associated lipocalin (NGAL) or kidney injury molecule-1 (KIM-1) were measured as tubular injury markers. High-sensitivity C-reactive protein (hs-CRP), soluble ICAM-1/VCAM-1, apolipoprotein B (ApoB), and soluble membrane attack complex (sMAC, C5b-9) were assessed. Data on reno-protective medications (ACEi/ARB, SGLT2i) were recorded. Correlation and multivariate regression analyses were performed. Results: Compared with patients without microalbuminuria, those with microalbuminuria showed higher gCD59, HbA1c, urinary NGAL/KIM-1, hs-CRP, ApoB, sICAM-1/VCAM-1, and sMAC levels (all p < 0.01). Mean eGFR was significantly lower in the microalbuminuria group (p < 0.001). gCD59 correlated positively with sMAC (r = 0.62, p < 0.001), urinary NGAL/KIM-1 (r = 0.58, p < 0.001), and HbA1c (r = 0.55, p < 0.001). In multivariate regression, gCD59, urinary NGAL/KIM-1, and sMAC emerged as independent predictors of microalbuminuria after adjustment for HbA1c, lipid profile, and medication use. Use of ACEi/ARB and SGLT2i was associated with lower biomarker levels and better renal function. Conclusions: gCD59 is closely linked with microalbuminuria, tubular injury, endothelial dysfunction, and complement activation in T2D. Its integration with conventional and novel biomarkers may improve early detection and risk stratification of DN, supporting more targeted interventions.
Keywords:
Introduction
Materials and Methods
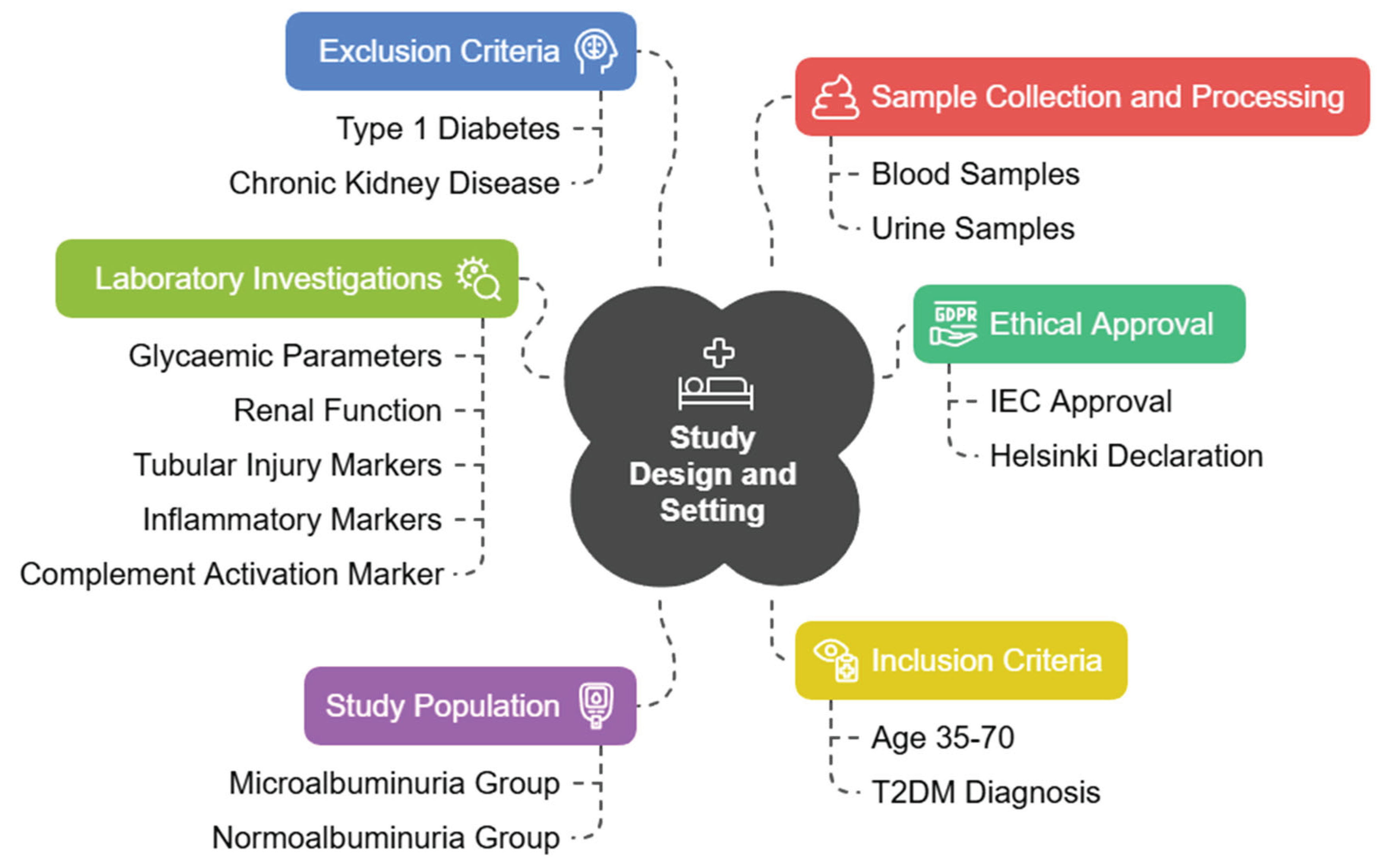
Study Design and Setting
Ethical Approval
Study Population
Inclusion Criteria
Exclusion Criteria
Sample Collection and Processing
Laboratory Investigations
Glycaemic and Renal Parameters
Measurement of Plasma gCD59
Tubular Injury Markers
Inflammatory and Endothelial Dysfunction Markers
Complement Activation Marker
Medication History
Statistical Analysis
Results
Baseline Characteristics
Biochemical and Biomarker Profile
Correlation Analysis
Multivariate Regression Analysis
Discussion
Strengths and Limitations
Clinical Implications
Conclusions
Acknowledgements
Conflict of Interest
Funding
References
- Forbes, J.M.; Cooper, M.E. Mechanisms of diabetic complications. Physiol Rev. 2013, 93, 137–188. [Google Scholar] [CrossRef]
- Alicic, R.Z.; Rooney, M.T.; Tuttle, K.R. Diabetic Kidney Disease: Challenges, Progress, and Possibilities. Clin J Am Soc Nephrol. 2017, 12, 2032–2045. [Google Scholar] [CrossRef]
- Inker, L.A.; Astor, B.C.; Fox, C.H.; et al. KDOQI US commentary on the 2012 KDIGO clinical practice guideline for the evaluation and management of CKD. Am J Kidney Dis. 2014, 63, 713–735. [Google Scholar] [CrossRef]
- Bus, P.; Chua, J.S.; Klessens, C.Q.F.; et al. Complement Activation in Patients With Diabetic Nephropathy. Kidney Int Rep. 2017, 3, 302–313, Published 2017 Oct 16. [Google Scholar] [CrossRef]
- Couves, E.C.; Gardner, S.; Voisin, T.B.; Bickel, J.K.; Stansfeld, P.J.; Tate, E.W.; Bubeck, D. Structural basis for membrane attack complex inhibition by CD59. Nat Commun. 2023, 14, 890. [Google Scholar] [CrossRef]
- Ghosh, P.; Vaidya, A.; Sahoo, R.; et al. Glycation of the complement regulatory protein CD59 is a novel biomarker for glucose handling in humans. J Clin Endocrinol Metab. 2014, 99, E999–E1006. [Google Scholar] [CrossRef]
- Yilmaz, O.; Erinc, O.; Gungordu, A.G.; Erdogan, M.; Algemi, M.; Akarsu, M. The Relationship of the Plasma Glycated CD59 Level with Microvascular Complications in Diabetic Patients and Its Evaluation as a Predictive Marker. J Clin Med. 2025, 14, 4588. [Google Scholar] [CrossRef] [PubMed]
- Ghosh, P.; Sahoo, R.; Vaidya, A.; et al. A specific and sensitive assay for blood levels of glycated CD59: a novel biomarker for diabetes. Am J Hematol. 2013, 88, 670–676. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Xu, C.; Lu, X.; et al. Glycated CD59 is a potential biomarker for gestational diabetes mellitus. Front Endocrinol (Lausanne). 2024, 15, 1374253, Published 2024 Sep 16. [Google Scholar] [CrossRef] [PubMed]
- Bogdanet, D.; Luque-Fernandez, M.A.; Toth-Castillo, M.; Desoye, G.; O’Shea, P.M.; Dunne, F.P.; Halperin, J.A. The role of early pregnancy maternal pGCD59 levels in predicting neonatal hypoglycemia—subanalysis of the DALI study. J Clin Endocrinol Metab. 107, e4311–e4319. [CrossRef]
- World Medical Association. WMA declaration of Helsinki: ethical principles for medical research involving human subjects. First adopted in June 1964, and last amended in October 2013. Available at: https://www.wma.net/policies-post/wma-declaration-of-helsinki-ethical-principles-for-medical-research-involving-human-subjects (Accessed August 25, 2023).
- Kurihara, C.; Kerpel-Fronius, S.; Becker, S.; Chan, A.; Nagaty, Y.; Naseem, S.; Schenk, J.; Matsuyama, K.; Baroutsou, V. Declaration of Helsinki: ethical norm in pursuit of common global goals. Front Med (Lausanne). 2024, 11, 1360653. [Google Scholar] [CrossRef]
- Shrestha, B.; Dunn, L. The Declaration of Helsinki on Medical Research involving Human Subjects: A Review of Seventh Revision. J Nepal Health Res Counc. 2020, 17, 548–552. [Google Scholar] [CrossRef]
- American Diabetes Association Professional Practice Committee; 2. Diagnosis and Classification of Diabetes: Standards of Care in Diabetes—2025. Diabetes Care 2025, (Supplement_1), S27–S49. [CrossRef]
- Naidoo, D.P. The link between microalbuminuria, endothelial dysfunction and cardiovascular disease in diabetes. Cardiovasc J S Afr. 2002, 13, 194–199. [Google Scholar]
- Acosta, J.; Hettinga, J.; Flückiger, R.; et al. Molecular basis for a link between complement and the vascular complications of diabetes. Proc Natl Acad Sci U S A. 2000, 97, 5450–5455. [Google Scholar] [CrossRef]
- KDIGO2024 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease Stevens Paul, E. et al. Kidney International 105, S117–S314.
- Yilmaz, O.; Demir, S.; Arslan, U.; Koc, A.; Kaya, E. Plasma glycated CD59 and microvascular complications in type 2 diabetes mellitus: a cross-sectional study. International Journal of Clinical Practice. 2025, 79, e15672. [Google Scholar]
- Nielsen, S.E.; Andersen, S.; Zdunek, D.; Hess, G.; Parving, H.H.; Rossing, P. Tubular markers do not predict the decline in glomerular filtration rate in type 1 diabetic patients with overt nephropathy. Kidney Int. 2011, 79, 1113–1118. [Google Scholar] [CrossRef] [PubMed]
- Bolignano, D.; Donato, V.; Coppolino, G.; Campo, S.; Buemi, A.; Lacquaniti, A.; Buemi, M. Neutrophil gelatinase-associated lipocalin (NGAL) as a marker of kidney damage. American Journal of Kidney Diseases. 2008, 52, 595–605. [Google Scholar] [CrossRef] [PubMed]
- Vaidya, V.S.; Ramirez, V.; Ichimura, T.; Bobadilla, N.A.; Bonventre, J.V. Urinary kidney injury molecule-1: a sensitive quantitative biomarker for early detection of kidney tubular injury. Am J Physiol Renal Physiol. 2006, 290, F517–F529. [Google Scholar] [CrossRef]
- Mezzano, S.A.; Droguett, M.A.; Burgos, M.E.; et al. Overexpression of chemokines, fibrogenic cytokines, and myofibroblasts in human membranous nephropathy. Kidney Int. 2000, 57, 147–158. [Google Scholar] [CrossRef]
- Navarro-González, J.F.; Mora-Fernández, C. The role of inflammatory cytokines in diabetic nephropathy. J Am Soc Nephrol. 2008, 19, 433–442. [Google Scholar] [CrossRef]
- Perkins, B.A.; Ficociello, L.H.; Silva, K.H.; Finkelstein, D.M.; Warram, J.H.; Krolewski, A.S. Regression of microalbuminuria in type 1 diabetes. N Engl J Med. 2003, 348, 2285–2293. [Google Scholar] [CrossRef]
- Afkarian, M.; Sachs, M.C.; Kestenbaum, B.; Hirsch, I.B.; Tuttle, K.R.; Himmelfarb, J.; de Boer, I.H. Kidney disease and increased mortality risk in type 2 diabetes. Journal of the American Society of Nephrology. 2013, 24, 302–8. [Google Scholar] [CrossRef] [PubMed]
- Ruggenenti, P.; Perna, A.; Remuzzi, G. ACE inhibitors to prevent end-stage renal disease: when to start and why possibly never to stop: a post hoc analysis of the REIN trial results. Ramipril Efficacy in Nephropathy. J Am Soc Nephrol. 2001, 12, 2832–2837. [Google Scholar] [CrossRef]
- Perkovic, V.; Jardine, M.J.; Neal, B.; et al. Canagliflozin and Renal Outcomes in Type 2 Diabetes and Nephropathy. N Engl J Med. 2019, 380, 2295–2306. [Google Scholar] [CrossRef] [PubMed]
- Heerspink, H.J.L.; Stefánsson, B.V.; Correa-Rotter, R.; et al. Dapagliflozin in Patients with Chronic Kidney Disease. N Engl J Med. 2020, 383, 1436–1446. [Google Scholar] [CrossRef] [PubMed]
- Thomas, M.C.; Brownlee, M.; Susztak, K.; et al. Diabetic kidney disease. Nat Rev Dis Primers. 2015, 1, 15018, Published 2015 Jul 30. [Google Scholar] [CrossRef] [PubMed]
- Coca, S.G.; Nadkarni, G.N.; Huang, Y.; et al. Plasma Biomarkers and Kidney Function Decline in Early and Established Diabetic Kidney Disease. J Am Soc Nephrol. 2017, 28, 2786–2793. [Google Scholar] [CrossRef]
- Holtkamp, F.A.; de Zeeuw, D.; de Graeff, P.A.; et al. Albuminuria and blood pressure, independent targets for cardioprotective therapy in patients with diabetes and nephropathy: a post hoc analysis of the combined RENAAL and IDNT trials. Eur Heart J. 2011, 32, 1493–1499. [Google Scholar] [CrossRef]

| Parameter |
Normoalbuminuria (n = 160) |
Microalbuminuria (n = 160) |
p value |
| Age (years) | 55.1 ± 8.4 | 56.2 ± 8.0 | 0.21 |
| Male gender, n (%) | 83 (51.9) | 87 (54.3) | 0.64* |
| Duration of diabetes (y) | 8.2 ± 3.5 | 10.8 ± 3.9 | <0.001 |
| BMI (kg/m²) | 27.4 ± 3.2 | 27.9 ± 3.6 | 0.27 |
| HbA1c (%) | 7.8 ± 1.1 | 8.9 ± 1.3 | <0.001 |
| Systolic BP (mmHg) | 131 ± 14 | 138 ± 16 | 0.002 |
| Parameter | Normoalbuminuria (n=160) | Microalbuminuria (n=160) | p value |
|---|---|---|---|
| HbA1c (%) | 7.8 ± 1.1 | 8.9 ± 1.3 | <0.001 |
| eGFR (mL/min/1.73m²) | 85.4 ± 13.8 | 68.2 ± 12.5 | <0.001 |
| gCD59 (ng/mL) | 4.2 ± 1.1 | 6.8 ± 1.4 | <0.001 |
| NGAL (ng/mg creat.) | 36.4 ± 12.3 | 58.2 ± 14.9 | <0.001 |
| KIM-1 (ng/mg creat.) | 3.1 ± 0.9 | 5.2 ± 1.4 | <0.001 |
| hs-CRP (mg/L) | 2.7 ± 0.9 | 4.2 ± 1.3 | <0.001 |
| sICAM-1 (ng/mL) | 256 ± 35 | 320 ± 42 | <0.001 |
| sVCAM-1 (ng/mL) | 490 ± 78 | 640 ± 85 | <0.001 |
| ApoB (mg/dL) | 96 ± 15 | 110 ± 18 | <0.001 |
| sMAC (ng/mL) | 210 ± 52 | 320 ± 65 | <0.001 |
| Variable | Odds Ratio (OR) | 95% CI | p value |
|---|---|---|---|
| gCD59 | 2.85 | 1.92–4.24 | <0.001 |
| Urinary NGAL | 1.67 | 1.25–2.21 | <0.001 |
| sMAC (C5b-9) | 2.42 | 1.78–3.65 | <0.001 |
| HbA1c | 1.18 | 0.92–1.52 | 0.09 |
| ApoB | 1.05 | 0.97–1.22 | 0.12 |
| ACEi/ARB | 0.71 | 0.53–0.92 | 0.03 |
| SGLT2i | 0.68 | 0.50–0.89 | 0.02 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).



