Submitted:
27 August 2025
Posted:
28 August 2025
You are already at the latest version
Abstract
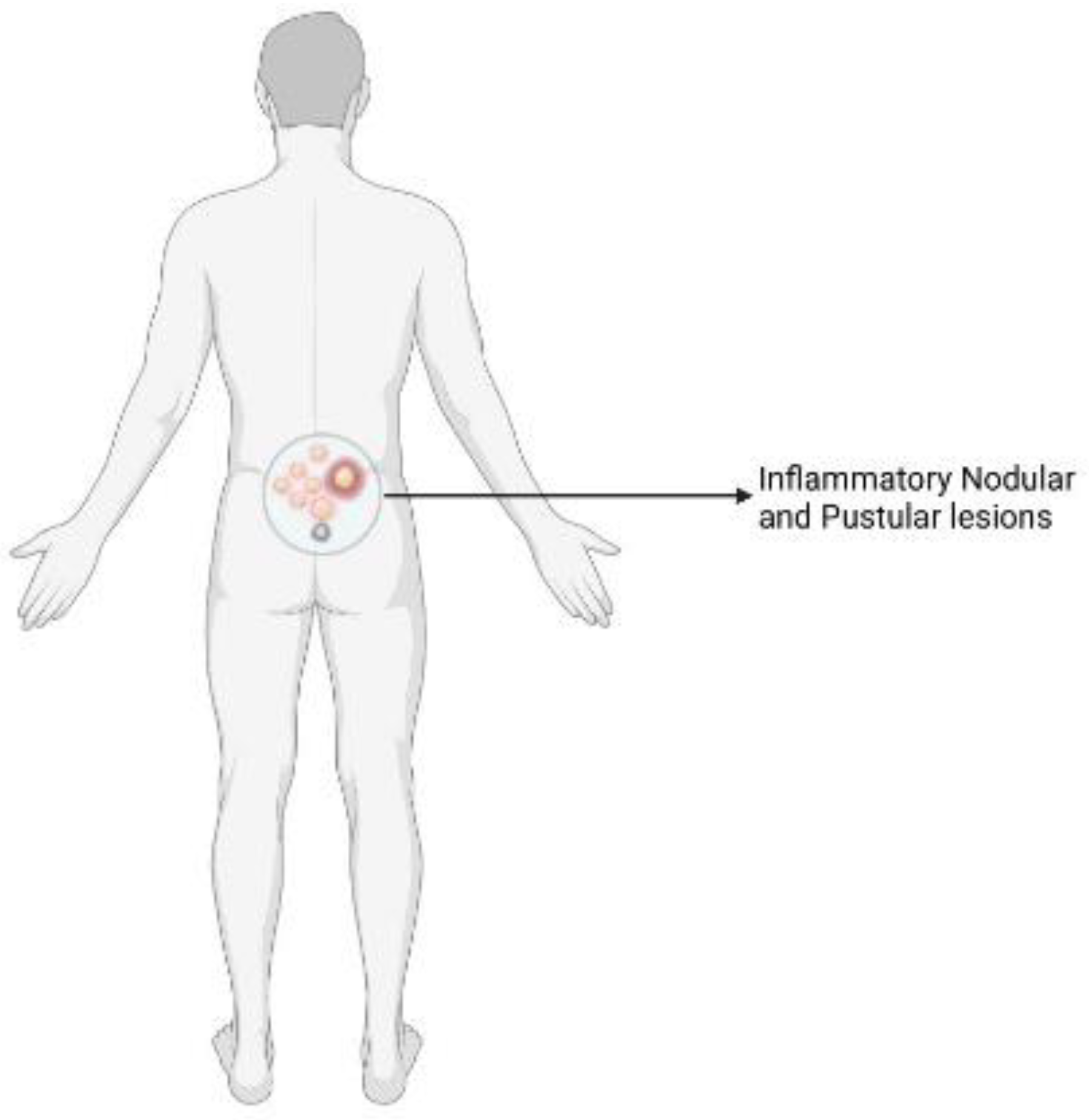
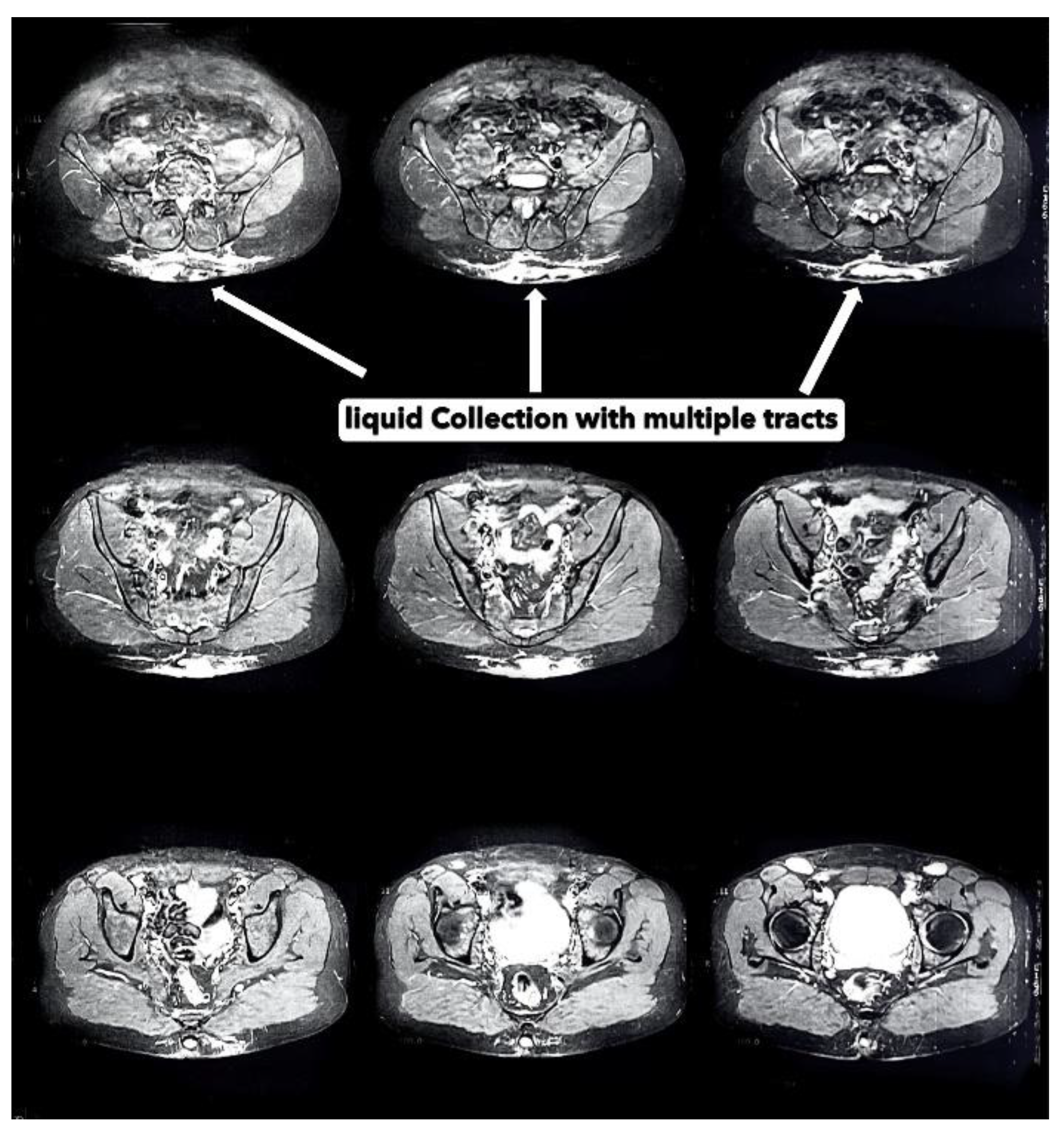
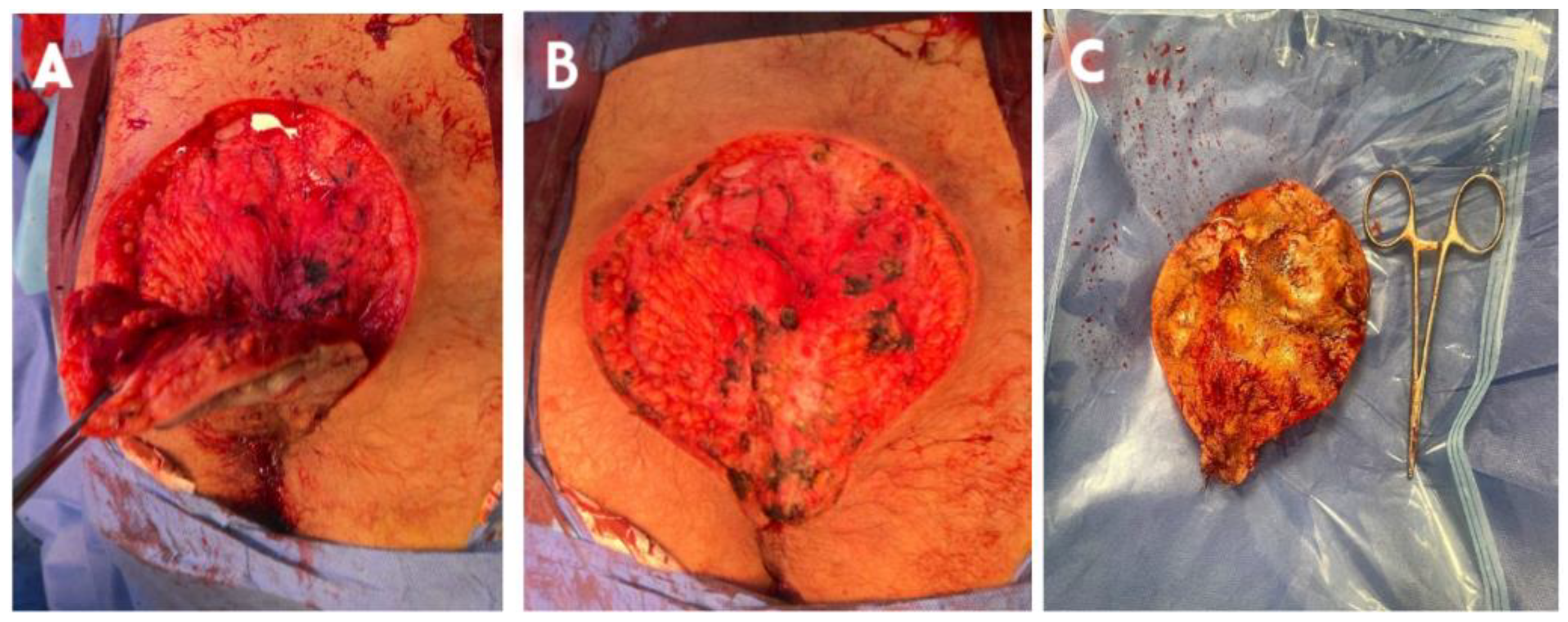
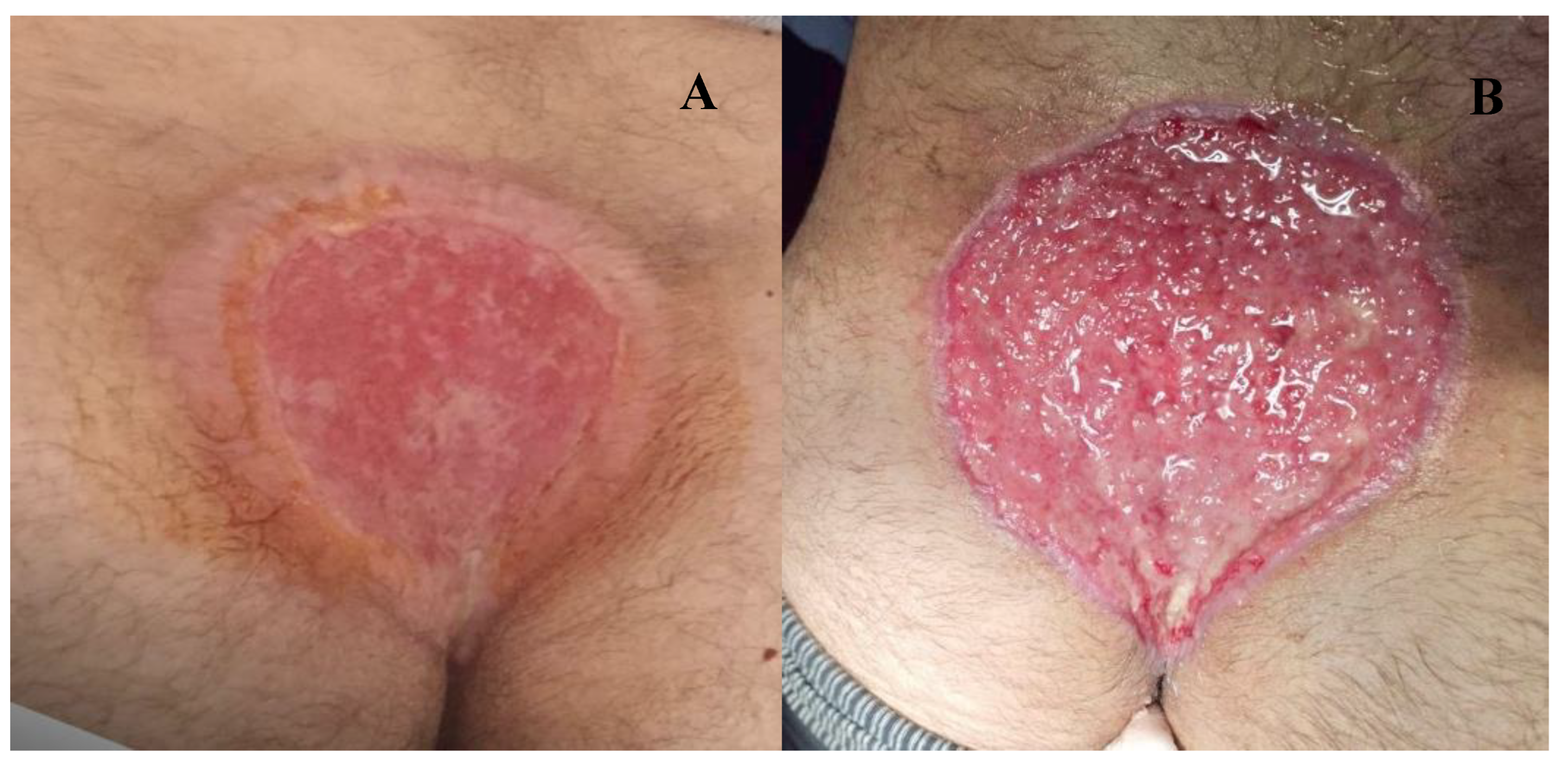
Introduction: Hidradenitis suppurativa (HS) is a rare painful, chronic inflammation of the apocrine glands. It is characterized by painful, inflamed cutaneous lesions causing nodules, sinus tracts and abcesses. This condition typically manifests in intertriginous areas such as axillae, groin, perineum and submammary regions. However, sacrococcygeal HS is an atypical localization and scarcely reported in the literature. Case presentation: We report a clinical case involving a 34-year-old young North-African male with no prior medical or surgical history or known predisposing factors. He presented an unusual anatomical presentation of hidradenitis suppurativa evolving in the last year prior to day clinic consultation. The patient self-took non documented oral antibiotics with no results before consultation. The lesion presented lower back pain and malodorant discharge. The evolution of the lesion although antibiotics motivated consultation. Our patient benefited a large surgical resection of the lesion with good evolution from week 7 post-surgery. Conclusion: Sacrococcygeal localization of HS is atypical but should be considered. This case illustrates the problems raised by a seemingly trivial disease. Surgery with adjuvant therapy may be the option in extensive lesion.
Keywords:
Introduction
Case Presentation
Discussion
Conclusion
Author Contributions
Funding
Consent
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Zouboulis Cc Desai, N.; Emtestam, L.; Hunger Re Ioannides, D.; Juhász, I.; et al. European S1 guideline for the treatment of hidradenitis suppurativa/acne inversa. J Eur Acad Dermatol Venereol [Internet]. 2015, 29, 619–644. Available from: https://onlinelibrary.wiley.com/doi/abs/10.1111/jdv.12966 [cited 4 June 2025]. [CrossRef] [PubMed]
- Verneuil, A. Etudes sur les tumeurs de la peau; de quelques maladies des glandules sudoripares. Arch Gen Med. 1854, 447–468. [Google Scholar]
- McCarthy, S. Hidradenitis Suppurativa. Annu Rev Med [Internet]. 2025, 76, 69–80. Available from: https://www.annualreviews.org/content/journals/10.1146/annurev-med-051223-031234 [cited 8 June 2025]. [CrossRef] [PubMed]
- Ingram, J.R. The epidemiology of hidradenitis suppurativa. Br J Dermatol [Internet]. 2020, 183, 990–998. Available from: https://onlinelibrary.wiley.com/doi/abs/10.1111/bjd.19435 [cited 9 July 2025]. [CrossRef] [PubMed]
- Poli, F.; Wolkenstein, P.; Revuz, J. Back and Face Involvement in Hidradenitis Suppurativa. Dermatology [Internet]. 2010, 221, 137–141, [cited 2025 Jun 8]. [Google Scholar] [CrossRef] [PubMed]
- Harvey LM, Fortson JK. Hidradenitis Suppurativa at an Uncommon Site: A Review of Its Clinical Features, Diagnostic Difficulties, and Management. Cureus [Internet]. [cited 2025 Jun 23];13(10):e18704. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8584235/. [CrossRef]
- Fabbrocini G, De Vita V. Comorbidities and Complex Syndromes. In: Hidradenitis Suppurativa [Internet]. John Wiley & Sons, Ltd.; 2017 [cited 2025 Jul 9]. p. 55–64. Available from: https://onlinelibrary.wiley.com/doi/abs/10.1002/9781119424291.ch7.
- Bettoli V, Ruina G. Epidemiology and pathogenesis. In: Hidradenitis Suppurativa [Internet]. 2017 [cited 2025 Jun 26]. p. 3–5. Available from: https://login.research4life.org/tacsgr1onlinelibrary_wiley_com/doi/10.1002/9781119424291.ch2.
- Canoui-Poitrine, F.; Revuz, J.E.; Wolkenstein, P.; Viallette, C.; Gabison, G.; Pouget, F.; et al. Clinical characteristics of a series of 302 French patients with hidradenitis suppurativa, with an analysis of factors associated with disease severity. J Am Acad Dermatol. 2009, 61, 51–57. [Google Scholar] [CrossRef] [PubMed]
- Hurley H. Axiillairy hyperhidrosis, apocrine bromhidrosis, hidradenitis suppurativa, and familial benign 41. pemphigus: surgical approach. Dermatol Surg. :729–39.
- Sartorius, K.; Emtestam, L.; Jemec, G.B.E.; Lapins, J. Objective scoring of hidradenitis suppurativa reflecting the role of tobacco smoking and obesity. Br J Dermatol [Internet]. 2009, 161, 831–839, [cited 2025 Jul 9]. [Google Scholar] [CrossRef] [PubMed]
- Manfredini, M.; Garbarino, F.; Bigi, L.; Pellacani, G.; Magnoni, C. Surgical and postsurgical wound care in hidradenitis suppurativa. Dermatol Ther [Internet]. 2020, 33, e13282. Available from: https://onlinelibrary.wiley.com/doi/abs/10.1111/dth.13282 [cited 8 June 2025]. [CrossRef] [PubMed]
- Ezanno, A.C.; Guillem, P.; Gorin, C.; Gabison, G.; Malgras, B.; Fougerousse, A.C. What should a surgeon know about hidradenitis suppurativa? J Visc Surg [Internet]. 2023, 160, 444–455. Available from: https://www.sciencedirect.com/science/article/pii/S187878862300142X [cited 8 June 2025]. [CrossRef] [PubMed]


| Hurley score [10] |
|---|
|
Stage I: Abscess formation (single or multiple) without sinus tracts and cicatrization Stage II: One or more widely separated recurrent abscesses with tract formation and scars Stage III: Multiple interconnected tracts and abscesses throughout an entire area |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).



