Submitted:
22 August 2025
Posted:
22 August 2025
You are already at the latest version
Abstract
Background: ST-elevation myocardial infarction (STEMI) involving the left main coronary artery is frequently complicated by cardiogenic shock. We sought to compare in-hospital outcomes of coronary bypass grafting (CABG) vs. percutaneous coronary intervention (PCI) in left main STEMI complicated with cardiogenic shock using a large national inpatient database.
Method: We identified patients aged >18 years with STEMI involving the left main coronary artery complicated by cardiogenic shock, who underwent revascularization with either PCI or CABG, from 2016 to 2020 using the Nationwide Inpatient Sample (NIS) database.
Results: A total of 1,050 weighted patients with left main STEMI and cardiogenic shock underwent revascularization (about 68% with PCI and 32% with CABG). Some comorbidities, such as diabetes, smoking, chronic kidney disease, COPD, and hyperlipidemia, were more prominent in the PCI cohort, including higher use of mechanical support except for intra-aortic balloon pump use. In-hospital mortality was markedly higher in the PCI group (55.0% vs. 15.7%; p< 0.001). To adjust for confounding factors, we included numerous high-risk characteristics, including the use of mechanical support, in the multivariate analysis. Despite adjustment for high-risk characteristics, the utilization of PCI remained significantly associated with a more than 5-fold mortality (OR: 5.47, CI 1.67-17.95, p=0.005). Patients undergoing CABG had longer hospitalizations (median length of stay, 10.5 days vs. 4 days for PCI; p < 0.001) and higher median total hospital charges.
Conclusion: In this national analysis of the left main STEMI with cardiogenic shock, CABG was associated with dramatically lower in-hospital mortality despite multivariate adjustment than PCI.
Keywords:
cardiogenic shock
; acute coronary syndrome
; ST-elevation myocardial infarction
; coronary bypass grafting
; cardiac surgery
; percutaneous coronary intervention
; coronary revascularization
; three vessel coronary artery disease
; coronary artery disease
; myocardial infarction
; PCI
; CABG
Introduction
Acute myocardial infarction complicated by cardiogenic shock remains one of the most lethal scenarios in cardiovascular care. Cardiogenic shock (CS) is a state of critical end-organ hypoperfusion resulting from cardiac pump failure, classically defined by sustained hypotension (systolic blood pressure <90 mmHg for ≥30 minutes or requiring vasopressors) accompanied by elevated filling pressures and tissue hypoxia [1]. Cardiogenic shock occurs in ~5–10% of acute MI cases and is associated with in-hospital mortality rates of 40–50% in contemporary series [2,3,4,5]. When the infarction involves the left main coronary artery, an entity sometimes termed “left main shock syndrome”, mortality rates are even higher, reported in the range of 55–80% [6]. Left main ST-elevation myocardial infarction (STEMI) is a catastrophic event due to the large ischemic territory, often resulting in acute pump failure and hemodynamic collapse. Rapid restoration of coronary perfusion is critical for survival in this setting.
Early revascularization has been proven to improve outcomes in myocardial infarction with CS. The landmark SHOCK trial demonstrated a significant survival benefit of prompt revascularization via either percutaneous coronary intervention (PCI) or coronary artery bypass graft (CABG) over medical therapy alone in cardiogenic shock, leading to a Class I recommendation for emergency revascularization in these patients [3]. In practice, primary PCI is the most common reperfusion strategy in STEMI, including in shock, due to its wide availability and speed of initiation. CABG as a primary reperfusion method in STEMI is uncommon, estimated to be utilized in only a small minority of cases, generally reserved for patients with anatomy not amenable to PCI or mechanical complications of MI [7,8,9]. This is particularly relevant in left main occlusion, where emergent PCI is often performed as a life-saving measure given the time and logistical constraints of assembling a surgical team.
Despite PCI being more readily employed in left main STEMI with shock, it is not definitively established that PCI provides superior outcomes to CABG in this scenario. On the contrary, there are reasons to consider the potential benefits of surgical revascularization. In patients with multivessel coronary disease (including left main or triple-vessel disease), CABG can achieve more complete revascularization and may protect more myocardium by bypassing multiple critical stenoses, which could be advantageous in the setting of shock [7,10,11]. Moreover, PCI in the context of cardiogenic shock has a lower procedural success rate and higher risk of complications (e.g. no-reflow, acute stent thrombosis) compared to non-shock interventions [12,13,14,15,16,17]. On the other hand, performing CABG during ongoing MI and shock is extraordinarily challenging, and historically, surgical outcomes in this context were poor, so it has traditionally been avoided as first-line therapy unless PCI is not possible [18,19]. Thus, a grey area remains regarding the optimal strategy for LM STEMI complicated by shock, since no randomized trials specifically address this question, and prior clinical studies have been limited.
Data from randomized trials in hemodynamically stable left main disease (e.g. EXCEL and NOBLE) indicate that PCI and CABG yield similar mortality rates at 5 years, although CABG may provide fewer repeat revascularizations at the cost of higher peri-procedural risk [20,21,22]. However, patients in cardiogenic shock represent a very different clinical scenario, and the relative outcomes of CABG vs. PCI in this high-risk group may diverge from the stable patient population. Notably, an analysis of patients with STEMI, cardiogenic shock, and three-vessel coronary disease (excluding left main) suggests that those treated with CABG had significantly lower in-hospital mortality than those treated with multivessel PCI [10].
Given the paucity of direct evidence specific to left main STEMI in shock, we undertook a comprehensive analysis using a large nationwide inpatient database. We aimed to compare the clinical outcomes of patients with left main STEMI and cardiogenic shock undergoing emergent PCI versus CABG. In particular, we focused on in-hospital mortality as the primary endpoint. We also analyzed secondary endpoints, including hospital length of stay and total costs, to contextualize the resource utilization of each strategy. By leveraging real-world data from a broad sample, we sought to provide insight into the contemporary outcomes of these two revascularization strategies and inform the management of this highly lethal condition.
Methods
Data Source
This study is deemed institutional review board exempt as the NIS is a publicly available de-identified database. The NIS database includes weighted discharge information for about 35 million patients each year, 20% of all inpatient admissions to nonfederal hospitals in the United States.
Study Population
Patient data was drawn for all patients over the age of 18 with a diagnosis of STEMI involving the left main coronary artery complicated by cardiogenic shock, who underwent revascularization with either PCI or CABG, from the Nationwide Inpatient Sample (NIS) from the 2016-2020 database years. Both International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM) and the International Classification of Diseases, Tenth Revision, Procedure Coding System (ICD-10-PCS) codes were used to query the NIS database and develop the study cohort. The target population of patients having undergone PCI was identified using the ICD-10-PCS codes 0270340 and 02170341. The target population of patients having undergone CABG was identified using the ICD-10-PCS codes 02100Z9, 02100ZA, and 02100ZJ. These populations were further stratified using the ICD-10-CM codes I21.01 for Left main STEMI and R57.0 for CS. Cohort demographic data were calculated using age, sex, and race. After performing multivariate analysis on high-risk baseline features and characteristics, we added any characteristics that were significantly different between the 2 groups in the multivariate analysis.
Study Outcomes
The patient outcome examined was inpatient total mortality. In multivariate analysis, we adjusted mortality for baseline characteristics and all high-risk features, including age, race, diabetes, gender, chronic kidney disease, hyperlipidemia, chronic obstructive pulmonary disease, smoking status, left ventricular assist devices, peripheral vascular disease, cardiomyopathy, history of systolic heart failure, cachexia, morbid obesity, obesity, chronic liver disease, atrial Fibrillation/Flutter, valvular heart disease, history of stroke, acute lactic acidosis, cardiac arrest, mechanical ventilation, renal replacement therapy, presence of aortocoronary bypass grafts and right ventricular infarction.
Statistical Analysis
Patient demographic, clinical, and hospital characteristics are reported as means, with 95% confidence intervals for continuous variables and proportions, and 95% confidence intervals for categorical variables. Trend analysis over time was assessed using Chi-squared analysis for categorical outcomes and univariate linear regression for continuous variables. Multivariable logistic regression ascertained the odds of binary clinical outcomes relative to patient and hospital characteristics as well as the odds of clinical outcomes over time. All analyses were conducted following the implementation of population discharge weights. All P-values are 2-sided, and P < .05 was considered statistically significant. Data were analyzed using STATA 17 (StataCorp LLC, College Station, Texas).
Results
Patient Population
From 2016–2020, we identified approximately 1,050 weighted hospitalizations meeting criteria for STEMI of the left main coronary artery with cardiogenic shock who underwent revascularization. Of these, about 700 (66.7%) underwent primary PCI and 350 (33.3%) underwent CABG during the hospitalization.
Baseline Demographic and Clinical Characteristics
The mean age was 66.4±11.9 years in the PCI group and 65.1±12.6 years in the CABG group (median 66 years in both), and this difference was not statistically significant (p=0.47). The majority of patients in both groups were men (approximately 63% of PCI vs. 69% of CABG patients were male; p=0.41). Racial distribution was similar: for example, about 60% of patients were White in each group, with smaller proportions Black (~11%), Hispanic (~12% in PCI vs. ~9.5% in CABG), and other races, and no significant differences in race/ethnicity between groups (p>0.2 for comparisons). Prevalence of major comorbid conditions between the PCI and CABG cohorts can be seen in Table 1.
In-Hospital Mortality
The overall in-hospital mortality rate for the entire cohort was extremely high, reflecting the severity of left main MI with shock. However, there was a striking difference in survival between the two revascularization strategies. In unadjusted analysis, inpatient mortality was 55% among patients who underwent PCI, compared with 15.7% among those who underwent CABG (OR: 6.56, CI: 3.19-13.46, p<0.001). On multivariate logistic regression analysis adjusting for all above-mentioned comorbidities, baseline characteristics, and high-risk features, PCI revascularization strategy remained the strongest independent predictor of more than 5-fold in-hospital mortality (OR: 5.47, CI: 1.67-17.95, p=0.005). Age showed a positive association with mortality. Sex (female vs. male) was not a significant predictor (OR ~0.89, p=0.72 after adjustment), suggesting no strong gender-based mortality difference in this cohort. The adjusted odds ratios for in-hospital mortality predicted from the multivariable model can be seen in the Figure.
Secondary Outcomes – Length of Stay and Cost
Among hospital survivors and non-survivors combined, the length of hospital stays (LOS) differed significantly between the two groups. Patients in the CABG group had a substantially longer LOS compared to those in the PCI group. The median LOS was 10.5 days (IQR 7–21) for CABG patients versus 4 days (IQR 1–9) for PCI patients (p<0.001). The mean LOS showed a similar gap (14±10 days for CABG vs. 7±9 days for PCI). With regard to hospital charges, CABG was associated with higher total charges than PCI. The median total hospital charge for the CABG group was approximately $307,400 (in 2016–2020 US dollars), compared to $224,700 for the PCI group (p=0.006). Table 2 summarizes the key outcomes for the two groups. In addition to the mortality difference, it includes data on hospital length of stay and total charges, as described below.
Discussion
In this retrospective analysis of a large national inpatient cohort, we found that for patients presenting with STEMI of the left main coronary artery complicated by cardiogenic shock, those who underwent emergent CABG had a far superior in-hospital survival compared to those who underwent PCI. The difference in mortality, 15.7% vs 55.0% is striking. Even after adjusting for baseline differences and comorbidities, CABG was associated with a significant reduction in the odds of in-hospital death. These results suggest a profound survival benefit with surgical revascularization in this specific context of left main coronary occlusion with shock.
Our findings must be interpreted in light of prior knowledge and the unique pathophysiology of left main myocardial infarction. The left main coronary artery supplies a huge proportion of the myocardium (via the left anterior descending and circumflex branches), so an acute left main occlusion often causes extensive infarction and immediate, severe depression of left ventricular function. In the absence of revascularization, left main STEMI in shock is usually rapidly fatal [3,14]. The standard approach per guideline is to perform immediate revascularization, if possible, typically with PCI, since it can be initiated within minutes in the catheterization lab, whereas organizing an emergency CABG takes time and surgical resources. Historically, urgent CABG has been less commonly used as the reperfusion strategy in STEMI except in cases of failed PCI or mechanical complications. Our analysis challenges the use of PCI as the default strategy in cases of left main shock. The data indicate that, among patients who did receive CABG, outcomes were dramatically better. This echoes findings from other studies that have compared CABG and PCI in patients with myocardial infarction complicated by CS, which also demonstrated lower mortality with CABG [10].
Notably, the mortality we observed in the CABG group (12.5%) is substantially lower than even the usual expectations for cardiogenic shock. For perspective, the original SHOCK trial reported ~47% 30-day mortality in the early revascularization arm (which included a mix of PCI and CABG), and contemporary shock registries often report 40–60% in-hospital mortality despite prompt PCI [13,14,15,23]. A mortality of only 12.5% in the CABG group is remarkably low for this population. This suggests that the patients selected (or able) to undergo CABG in left main shock might have had factors in their favor, for example, perhaps they were stabilized with mechanical support or had slightly less severe shock, allowing them to survive in order to undergo surgery and then benefited greatly from definitive surgical revascularization. It also likely reflects excellent surgical and perioperative care in the centers that attempted CABG in such critically ill patients.
One must consider selection bias when interpreting these results. This was not a randomized comparison; clinicians decided the revascularization strategy based on patient condition and other factors. It is highly likely that patients who were deemed too unstable to survive surgery were triaged to PCI, whereas those who maintained perfusion (perhaps with the help of an intra-aortic balloon pump or percutaneous left ventricular assist devices) and had surgical backup available were taken to CABG. This could create a scenario where the CABG group inherently had a better prognosis (even before the procedure) than the PCI group. Indeed, the baseline clinical variables we measured (age, comorbidities) were similar between groups, but we did not have data on hemodynamic parameters like blood pressure, lactate levels, use of mechanical circulatory support, or infarct size before revascularization. It is conceivable that the CABG cohort represents a subset of patients who responded better to initial stabilization, making it to surgery, whereas the sickest of the sick either could only get PCI or died despite PCI. Such unmeasured confounders could exaggerate the apparent benefit of CABG. We attempted to mitigate confounding by multivariate adjustment; notably, none of the measured comorbidities explained away the mortality difference. But unmeasured factors (shock severity, timing delays, etc.) remain.
Despite these caveats, it is important to highlight that even after adjustment, the OR for mortality with CABG vs PCI was 0.16, which is a massive effect size rarely seen in observational studies. This suggests that selection bias alone is unlikely to account for the entirety of the difference; it hints at a true benefit of the surgical approach in many cases. There are plausible biological reasons why CABG could improve survival in left main shock patients. First, CABG provides complete revascularization in a single session: a surgeon can graft not only the left main (LAD and circumflex territories) but also any coexisting right coronary disease, ensuring all major myocardial territories are re-perfused. In acute PCI for shock, the current best practice per guidelines is to treat only the culprit lesion (the left main in this case) and not necessarily other lesions acutely [14]. Even if the left main is stented, patients might have residual critical disease (e.g. severe RCA stenosis) that remains untreated in the acute setting, potentially compromising recovery. CABG, by revascularizing multiple vessels, might rescue more myocardium and provide hemodynamic stability that a single culprit PCI cannot [10,24,25,26]. Second, CABG can be more effective if the culprit lesion is not amenable to good PCI outcomes for instance, an occluded left main with high thrombus burden and low flow after stenting might still result in poor perfusion, whereas surgical bypass can restore flow beyond the occlusion [7,27]. There is evidence that PCI in unprotected left main shock has high failure rates prior studies have noted that if TIMI 3 flow is not quickly achieved, mortality increases significantly [28,29,30]. CABG, while requiring longer initial time, once established, can provide robust flow to both the LAD and circumflex. Third, there may be a benefit of surgical revascularization in shock by bypassing severely diseased segments and providing more durable patency. Stents in the setting of shock and a pro-thrombotic state may occlude or thrombose, whereas grafts (especially an internal mammary graft to LAD) might remain patent. Additionally, mechanical support devices (IABP, Impella, ECMO) can be deployed to bridge patients to CABG; while we do not have NIS data on device use, it is likely that many of the CABG patients received such support. The use of combined Impella and ECMO (ECpella) or other shock protocols at advanced centers has shown improved survival in shock patients [31,32,33].
Another notable finding in our analysis is the association of hyperlipidemia with better survival. This counterintuitive result has been observed in other critical illness contexts; higher cholesterol or the presence of treated hyperlipidemia has been linked to improved outcomes in acute heart failure and shock, possibly reflecting the effects of chronic statin therapy or a selection bias where those with hyperlipidemia have more chronic disease adaptation [34,35,36,37]. It is plausible that patients with known hyperlipidemia were more likely to be on statins or other cardioprotective medications before the MI, which might have conferred some resilience (for example, statins have pleiotropic benefits like improving endothelial function and reducing inflammatory responses during acute MI). This “lipid paradox” should not overshadow the main findings, but it is an interesting corroboration of prior studies and suggests that aggressive preventative therapy (like statins) in those at risk might incidentally improve acute MI/shock outcomes. Age showed a trend toward higher mortality (which is expected, as older patients have less physiological reserve), but many older patients did survive with CABG, indicating that chronological age alone should not exclude consideration of surgery if otherwise appropriate. We did not find significant differences in outcome by sex or race, although our sample size may limit the detection of such differences.
The length of stay and cost findings deserve comment from a health systems perspective. We observed that CABG survivors stayed a median of 6 days longer than PCI patients. This is logical given the nature of recovery from open-heart surgery. From a cost standpoint, the CABG strategy was more expensive acutely (median ~$307k vs $225k). However, if we consider cost per survivor, the picture changes dramatically. With 87.5% mortality in PCI, essentially for every 8 PCI patients treated, only 1 survives (on average), at a collective cost of 8 * $284k (average cost of PCI) ≈ $2.27 million per survivor. In contrast, for CABG, for every 8 patients treated, 7 survive, at a collective cost of 8 * $423k (average cost of CABG) ≈ $3.38 million, which per survivor is about $0.48 million. Thus, CABG appears far more cost-effective in terms of lives saved, despite higher upfront costs per patient. This is a rough illustrative calculation, but it underscores that resource utilization should be interpreted alongside clinical outcomes Of course, a formal cost-effectiveness analysis would require long-term outcome data, quality-of-life assessment, and inclusion of costs beyond the hospitalization, which is beyond our scope.
Our results contribute to a growing body of evidence that in the setting of acute myocardial infarction with cardiogenic shock, more aggressive or complete revascularization strategies might improve survival. The SHOCK trial two decades ago confirmed that revascularization is far better than medical management. Now, with modern data, we are exploring what kind of revascularization yields the best outcome. The concept of “shock teams” has emerged in advanced centers, multidisciplinary teams that rapidly evaluate shock patients and deploy a combination of PCI, mechanical support, and sometimes surgical intervention. Studies have suggested that dedicated shock protocols and teams can improve survival in cardiogenic shock [15,38]. Our findings strongly support involving cardiac surgeons early in the care of left main MI shock patients. Rather than defaulting to PCI only, the heart team (including interventional cardiology, cardiothoracic surgery, and critical care) should assess whether the patient could be a surgical candidate, especially if initial stabilization can be achieved. It may be that in the coming years, we see a paradigm shift for certain shock subsets (like left main occlusion), where immediate PCI is used as a bridge to definitive CABG, or even immediate surgical bypass is performed if surgical resources are on standby. Not all hospitals can provide this level of care, which is another possible explanation for our findings: the CABG cases likely happened at tertiary centers with surgical capability, whereas many PCI cases could have been at centers without surgery on-site (where CABG simply wasn’t an option emergently). Our data suggest that if CABG can be done in a timely fashion, the outcomes may be superior.
Finally, it’s useful to contrast our results with outcomes in stable left main revascularization trials. The EXCEL trial, which compared PCI with CABG for left main coronary artery disease, reported that at five years, all-cause mortality was slightly higher in the PCI arm compared to the CABG arm (13% vs. 9.9%) although this difference was not statistically significant (difference, 3.1 percentage points; 95% CI, 0.2 to 6.1) [20]. However, Bayesian analyses of the EXCEL trial data suggested a high probability that total mortality was increased with PCI compared to CABG, with the absolute difference likely small [39]. This highlights how patient context (shock vs. elective) completely changes the risk-benefit calculus. In stable patients, PCI avoids the operative morbidity and upfront risk of surgery and appears adequate for many; in shock patients, the immediate completeness of revascularization by CABG appears to outweigh its invasiveness. The NOBLE trial reported that the 5-year Kaplan-Meier estimates of MACCE were 28% for PCI and 19% for CABG, with a hazard ratio (HR) of 1.58 (95% CI 1.24-2.01), indicating that CABG was superior to PCI for the primary composite endpoint (p=0.0002) [40]. The rates of non-procedural myocardial infarction were 8% for PCI versus 3% for CABG (HR 2.99, 95% CI 1.66-5.39; p=0.0002), and the rates of repeat revascularization were 17% for PCI versus 10% for CABG (HR 1.73, 95% CI 1.25-2.40; p=0.0009) [40]. Importantly, the all-cause mortality was similar between the two groups, estimated at 9% for both PCI and CABG (HR 1.08, 95% CI 0.74-1.59; p=0.68) [40]. Thus, in the long term, survival converges in stable patients regardless of strategy, whereas in the acute shock setting, survival is determined in the first few days, and that’s where the surgical advantage manifested in our study.
Limitations
Despite the provocative findings, our study has important limitations. First, as an observational study using administrative data, unmeasured confounding is a major concern. We lacked detailed clinical data such as hemodynamic parameters (blood pressure, cardiac index), infarct size, angiographic complexity, success or failure of PCI, use of mechanical circulatory support (IABP, Impella, ECMO), timing from MI onset to revascularization, etc. Any of these factors could bias the selection of therapy and outcomes. Second, there is likely a survivor bias in that patients had to survive long enough to undergo CABG. If a patient dies early in the cardiac catheterization laboratory, they count in the PCI group’s mortality, whereas a patient who dies before reaching the OR might not even be captured in our CABG group (depending on coding). Third, the NIS database is an administrative dataset and is subject to coding errors or inconsistencies. It’s possible some cases were misclassified. Additionally, NIS does not allow linkage of revascularization timing; we know a CABG was done, but not if it was on hospital day 0, 1, or 3, which matters greatly in acute MI. Fourth, our outcome focus was in-hospital mortality; we do not have data on 30-day or longer-term mortality. It’s conceivable that some CABG patients who survived discharge might have had early post-discharge mortality that our analysis misses. However, it’s unlikely enough to bridge an enormous gap. Long-term outcomes would also be interesting: perhaps PCI survivors might have had different 6-month outcomes versus CABG survivors. But given how acute this syndrome is, in-hospital survival is a reasonable and clinically relevant endpoint. Fifth, we did not analyze neurologic outcomes or strokes explicitly. CABG in the setting of an acute MI carries a risk of stroke (on-pump surgery in a critically ill patient), which is an important outcome for survivors. The NIS data did not readily allow us to identify peri-procedural strokes in this specific subset. Finally, generalizability may be an issue: the CABG group in this study likely represents high-volume centers with cardiac surgery on-site. Outcomes at those centers may not mirror what could be achieved at all hospitals. If a community hospital attempted an emergent CABG without the experience or resources of a tertiary center, results might not be as favorable. Thus, our data should not be taken to mean that every left main shock patient can simply be sent to surgery and do well; it likely requires optimal care (including perhaps pre-operative support, surgical expertise, etc.).
Conclusion
For patients with left main STEMI complicated by cardiogenic shock, our study suggests that coronary artery bypass grafting is associated with significantly better in-hospital survival than percutaneous coronary intervention. While PCI remains the quicker and more readily available option in most acute MI cases, these findings highlight that, in the specific and dire circumstance of left main occlusion, an aggressive surgical approach, when feasible, can offer a life-saving benefit. CABG patients in our cohort had a much higher chance of leaving the hospital alive, albeit after a longer and costlier hospitalization. This marked survival advantage of CABG, even after accounting for baseline differences, indicates that the revascularization strategy may play a pivotal role in outcomes above and beyond the patient’s initial risk profile.
Clinicians managing cardiogenic shock from left main MI should consider early involvement of the heart team and assess the possibility of emergent CABG, especially at centers where advanced mechanical support and surgical capabilities are available. The decision must still be individualized, weighing the patient’s operative risk, co-morbidities, and available resources. Our results support the notion that with appropriate patient selection and systemic support, surgical revascularization can be done in shock with acceptable mortality. Moving forward, improving outcomes in left main shock will likely involve a multidisciplinary approach: rapid PCI for immediate stabilization when needed, prompt utilization of mechanical circulatory support to maintain perfusion, and definitive surgical revascularization to ensure complete restoration of coronary blood flow.
References
- Heidenreich, P.A.; Bozkurt, B.; Aguilar, D.; Allen, L.A.; Byun, J.J.; Colvin, M.M.; Deswal, A.; Drazner, M.H.; Dunlay, S.M.; Evers, L.R.; Fang, J.C.; Fedson, S.E.; Fonarow, G.C.; Hayek, S.S.; Hernandez, A.F.; Khazanie, P.; Kittleson, M.M.; Lee, C.S.; Link, M.S.; Milano, C.A.; Nnacheta, L.C.; Sandhu, A.T.; Stevenson, L.W.; Vardeny, O.; Vest, A.R.; Yancy, C.W. 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J Am Coll Cardiol. 2022, 79, e263–e421, Erratum in: J Am Coll Cardiol. 2023, 81, 1551. 10.1016/j.jacc.2023.03.002. [Google Scholar] [CrossRef] [PubMed]
- Amsterdam, E.A.; Wenger, N.K.; Brindis, R.G.; Casey DEJr Ganiats, T.G.; Holmes DRJr Jaffe, A.S.; Jneid, H.; Kelly, R.F.; Kontos, M.C.; Levine, G.N.; Liebson, P.R.; Mukherjee, D.; Peterson, E.D.; Sabatine, M.S.; Smalling, R.W.; Zieman, S.J.; ACC/AHA Task Force Members. 2014 AHA/ACC guideline for the management of patients with non-ST-elevation acute coronary syndromes: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. 2014, 130, e344–426, Erratum in Circulation. 2014, 130, e433-e434. Dosage error in article text. [Google Scholar] [CrossRef] [PubMed]
- O'Gara, P.T.; Kushner, F.G.; Ascheim, D.D.; Casey DEJr Chung, M.K.; de Lemos, J.A.; Ettinger, S.M.; Fang, J.C.; Fesmire, F.M.; Franklin, B.A.; Granger, C.B.; Krumholz, H.M.; Linderbaum, J.A.; Morrow, D.A.; Newby, L.K.; Ornato, J.P.; Ou, N.; Radford, M.J.; Tamis-Holland, J.E.; Tommaso, C.L.; Tracy, C.M.; Woo, Y.J.; Zhao, D.X. 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2013, 61, e78–e140. [Google Scholar] [CrossRef] [PubMed]
- Berg, D.D.; Bohula, E.A.; Morrow, D.A. Epidemiology and causes of cardiogenic shock. Curr Opin Crit Care. 2021, 27, 401–408. [Google Scholar] [CrossRef] [PubMed]
- Lauridsen, M.D.; Rørth, R.; Lindholm, M.G.; Kjaergaard, J.; Schmidt, M.; Møller, J.E.; Hassager, C.; Torp-Pedersen, C.; Gislason, G.; Køber, L.; Fosbøl, E.L. Trends in first-time hospitalization, management, and short-term mortality in acute myocardial infarction-related cardiogenic shock from 2005 to 2017: A nationwide cohort study. Am Heart J. 2020, 229, 127–137. [Google Scholar] [CrossRef] [PubMed]
- Quigley, R.L.; Milano, C.A.; Smith, L.R.; White, W.D.; Rankin, J.S.; Glower, D.D. Prognosis and management of anterolateral myocardial infarction in patients with severe left main disease and cardiogenic shock. The left main shock syndrome. The left main shock syndrome. Circulation. 1993, 88(5 Pt 2), II65–70. [Google Scholar] [PubMed]
- Alexander, J.H.; Smith, P.K. Coronary-Artery Bypass Grafting. N Engl J Med. 2016, 374, 1954–1964. [Google Scholar] [CrossRef]
- Elbadawi, A.; Elzeneini, M.; Elgendy, I.Y.; et al. Coronary artery bypass grafting after acute ST-elevation myocardial infarction. J Thorac Cardiovasc Surg. 2023, 165, 672–683.e10. [Google Scholar] [CrossRef]
- Sandner, S.; Florian, A.; Ruel, M. Coronary artery bypass grafting in acute coronary syndromes: modern indications and approaches. Curr Opin Cardiol. 2024, 39, 485–490. [Google Scholar] [CrossRef] [PubMed]
- Smilowitz, N.R.; Alviar, C.L.; Katz, S.D.; Hochman, J.S. Coronary artery bypass grafting versus percutaneous coronary intervention for myocardial infarction complicated by cardiogenic shock. Am Heart J. 2020, 226, 255–263. [Google Scholar] [CrossRef]
- Mulukutla, S.R.; Gleason, T.G.; Sharbaugh, M.; et al. Coronary Bypass Versus Percutaneous Revascularization in Multivessel Coronary Artery Disease. Ann Thorac Surg. 2019, 108, 474–480. [Google Scholar] [CrossRef]
- Thiele, H.; Akin, I.; Sandri, M.; et al. PCI Strategies in Patients with Acute Myocardial Infarction and Cardiogenic Shock. N Engl J Med. 2017, 377, 2419–2432. [Google Scholar] [CrossRef]
- Samsky, M.D.; Morrow, D.A.; Proudfoot, A.G.; Hochman, J.S.; Thiele, H.; Rao, S.V. Cardiogenic Shock After Acute Myocardial Infarction: A Review. JAMA. 2021, 326, 1840–1850, Erratum in JAMA. 2021, 326, 2333. [Google Scholar] [CrossRef]
- Henry, T.D.; Tomey, M.I.; Tamis-Holland, J.E.; et al. Invasive Management of Acute Myocardial Infarction Complicated by Cardiogenic Shock: A Scientific Statement From the American Heart Association. Circulation. 2021, 143, e815–e829. [Google Scholar] [CrossRef]
- van Diepen, S.; Katz, J.N.; Albert, N.M.; et al. Contemporary Management of Cardiogenic Shock: A Scientific Statement From the American Heart Association. Circulation. 2017, 136, e232–e268. [Google Scholar] [CrossRef] [PubMed]
- Chan, W.; Stub, D.; Clark, D.J.; et al. Usefulness of transient and persistent no reflow to predict adverse clinical outcomes following percutaneous coronary intervention. Am J Cardiol. 2012, 109, 478–485. [Google Scholar] [CrossRef]
- Ndrepepa, G.; Cassese, S.; Xhepa, E.; et al. Coronary no-reflow and adverse events in patients with acute myocardial infarction after percutaneous coronary intervention with current drug-eluting stents and third-generation P2Y12 inhibitors. Clin Res Cardiol. 2024, 113, 1006–1016. [Google Scholar] [CrossRef] [PubMed]
- Davierwala, P.M.; Leontyev, S.; Verevkin, A.; et al. Temporal Trends in Predictors of Early and Late Mortality After Emergency Coronary Artery Bypass Grafting for Cardiogenic Shock Complicating Acute Myocardial Infarction. Circulation. 2016, 134, 1224–1237. [Google Scholar] [CrossRef]
- Acharya, D.; Gulack, B.C.; Loyaga-Rendon, R.Y.; et al. Clinical Characteristics and Outcomes of Patients With Myocardial Infarction and Cardiogenic Shock Undergoing Coronary Artery Bypass Surgery: Data From The Society of Thoracic Surgeons National Database. Ann Thorac Surg. 2016, 101, 558–566. [Google Scholar] [CrossRef] [PubMed]
- Stone, G.W.; Kappetein, A.P.; Sabik, J.F.; et al. Five-Year Outcomes after PCI or CABG for Left Main Coronary Disease. N Engl J Med. 2019, 381, 1820–1830, Erratum in N Engl J Med. 2020, 382, 1078. 10.1056/NEJMx200004. [Google Scholar] [CrossRef]
- Holm, N.R.; Mäkikallio, T.; Lindsay, M.M.; et al. Percutaneous coronary angioplasty versus coronary artery bypass grafting in the treatment of unprotected left main stenosis: updated 5-year outcomes from the randomised, non-inferiority NOBLE trial. Lancet. 2020, 395, 191–199. [Google Scholar] [CrossRef]
- Sabatine, M.S.; Bergmark, B.A.; Murphy, S.A.; et al. Percutaneous coronary intervention with drug-eluting stents versus coronary artery bypass grafting in left main coronary artery disease: an individual patient data meta-analysis. Lancet. 2021, 398, 2247–2257, Erratum in Lancet. 2022, 399, 1606. 10.1016/S0140-6736(22)00701-2; Lancet. 2022, 400, 1304. 10.1016/S0140-6736(22)01944-4. [Google Scholar] [CrossRef]
- Hochman, J.S.; Sleeper, L.A.; Webb, J.G.; et al. Early revascularization in acute myocardial infarction complicated by cardiogenic shock. SHOCK Investigators. Should We Emergently Revascularize Occluded Coronaries for Cardiogenic Shock. N Engl J Med. 1999, 341, 625–634. [Google Scholar] [CrossRef]
- White, H.D.; Assmann, S.F.; Sanborn, T.A.; Jacobs, A.K.; Webb, J.G.; Sleeper, L.A.; Wong, C.K.; Stewart, J.T.; Aylward, P.E.; Wong, S.C.; Hochman, J.S. Comparison of percutaneous coronary intervention and coronary artery bypass grafting after acute myocardial infarction complicated by cardiogenic shock: results from the Should We Emergently Revascularize Occluded Coronaries for Cardiogenic Shock (SHOCK) trial. Circulation. 2005, 112, 1992–2001. [Google Scholar] [CrossRef] [PubMed]
- Omerovic, E.; Råmunddal, T.; Petursson, P.; Angerås, O.; Rawshani, A.; Jha, S.; Skoglund, K.; Mohammad, M.A.; Persson, J.; Alfredsson, J.; Hofmann, R.; Jernberg, T.; Fröbert, O.; Jeppsson, A.; Hansson, E.C.; Dellgren, G.; Erlinge, D.; Redfors, B. Percutaneous vs. surgical revascularization of non-ST-segment elevation myocardial infarction with multivessel disease: the SWEDEHEART registry. Eur Heart J. 2025, 46, 518–531. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Bakaeen FG, Gaudino M, Whitman G, Doenst T, Ruel M, Taggart DP, Stulak JM, Benedetto U, Anyanwu A, Chikwe J, Bozkurt B, Puskas JD, Silvestry SC, Velazquez E, Slaughter MS, McCarthy PM, Soltesz EG, Moon MR; American Association for Thoracic Surgery Cardiac Clinical Practice Standards Committee; Invited Experts. 2021: The American Association for Thoracic Surgery Expert Consensus Document: Coronary artery bypass grafting in patients with ischemic cardiomyopathy and heart failure. J Thorac Cardiovasc Surg. 2021, 162, 829–850.e1. [CrossRef] [PubMed]
- Lee, P.H.; Park, H.; Lee, J.S.; Lee, S.W.; Lee, C.W. Meta-Analysis Comparing the Risk of Myocardial Infarction Following Coronary Artery Bypass Grafting Versus Percutaneous Coronary Intervention in Patients With Multivessel or Left Main Coronary Artery Disease. Am J Cardiol. 2019, 124, 842–850. [Google Scholar] [CrossRef] [PubMed]
- Castro-Mejía, A.F.; Ortega-Armas, M.E.; Mejía-Rentería, H.; et al. Short-term clinical outcomes of percutaneous coronary intervention of unprotected left main coronary disease in cardiogenic shock. Catheter Cardiovasc Interv. 2020, 95, 515–521. [Google Scholar] [CrossRef]
- Bajaj, R.; Ramasamy, A.; Brown, J.T.; et al. Treatment Strategies and Outcomes of Emergency Left Main Percutaneous Coronary Intervention. Am J Cardiol. 2022, 177, 1–6. [Google Scholar] [CrossRef]
- El Nasasra, A.; Hochadel, M.; Zahn, R.; et al. Outcomes After Left Main Percutaneous Coronary Intervention in Patients With Acute Myocardial Infarction Complicated by Cardiogenic Shock (from the German ALKK PCI Registry). Am J Cardiol. 2023, 197, 77–83. [Google Scholar] [CrossRef]
- Bhatia, K.; Jain, V.; Hendrickson, M.J.; et al. Meta-Analysis Comparing Venoarterial Extracorporeal Membrane Oxygenation With or Without Impella in Patients With Cardiogenic Shock. Am J Cardiol. 2022, 181, 94–101. [Google Scholar] [CrossRef]
- Patel, S.M.; Lipinski, J.; Al-Kindi, S.G.; et al. Simultaneous Venoarterial Extracorporeal Membrane Oxygenation and Percutaneous Left Ventricular Decompression Therapy with Impella Is Associated with Improved Outcomes in Refractory Cardiogenic Shock. ASAIO J. 2019, 65, 21–28. [Google Scholar] [CrossRef]
- Pappalardo, F.; Schulte, C.; Pieri, M.; et al. Concomitant implantation of Impella® on top of veno-arterial extracorporeal membrane oxygenation may improve survival of patients with cardiogenic shock. Eur J Heart Fail. 2017, 19, 404–412. [Google Scholar] [CrossRef]
- Bozkurt, B.; Aguilar, D.; Deswal, A.; et al. Contributory Risk and Management of Comorbidities of Hypertension, Obesity, Diabetes Mellitus, Hyperlipidemia, and Metabolic Syndrome in Chronic Heart Failure: A Scientific Statement From the American Heart Association. Circulation. 2016, 134, e535–e578. [Google Scholar] [CrossRef] [PubMed]
- Horwich, T.B.; Hernandez, A.F.; Dai, D.; Yancy, C.W.; Fonarow, G.C. Cholesterol levels and in-hospital mortality in patients with acute decompensated heart failure. Am Heart J. 2008, 156, 1170–1176. [Google Scholar] [CrossRef] [PubMed]
- Greene, S.J.; Vaduganathan, M.; Lupi, L.; et al. Prognostic significance of serum total cholesterol and triglyceride levels in patients hospitalized for heart failure with reduced ejection fraction (from the EVEREST Trial). Am J Cardiol. 2013, 111, 574–581. [Google Scholar] [CrossRef]
- Jin, J.; Shi, Z.; Pang, X. Association between low-density lipoprotein cholesterol level and mortality in patients with cardiogenic shock: a retrospective cohort study. BMJ Open. 2021, 11, e044668. [Google Scholar] [CrossRef] [PubMed]
- Papolos, A.I.; Kenigsberg, B.B.; Berg, D.D.; et al. Management and Outcomes of Cardiogenic Shock in Cardiac ICUs With Versus Without Shock Teams. J Am Coll Cardiol. 2021, 78, 1309–1317. [Google Scholar] [CrossRef]
- Brophy, J.M. Bayesian Interpretation of the EXCEL Trial and Other Randomized Clinical Trials of Left Main Coronary Artery Revascularization. JAMA Intern Med. 2020, 180, 986–992. [Google Scholar] [CrossRef]
- Holm, N.R.; Mäkikallio, T.; Lindsay, M.M.; et al. Percutaneous coronary angioplasty versus coronary artery bypass grafting in the treatment of unprotected left main stenosis: updated 5-year outcomes from the randomised, non-inferiority NOBLE trial. Lancet. 2020, 395, 191–199. [Google Scholar] [CrossRef]
Figure.
Adjusted odds ratios (OR) for predictors of in-hospital mortality (with 95% confidence intervals) in patients with left main STEMI and shock. The analysis controls for age, sex, race, and comorbidities. Note the logarithmic scale on the x-axis. CABG (versus PCI) is associated with a dramatically lower odds of mortality (OR ~0.16, far to the left of the unity line), indicating significantly improved survival with surgical revascularization.
Figure.
Adjusted odds ratios (OR) for predictors of in-hospital mortality (with 95% confidence intervals) in patients with left main STEMI and shock. The analysis controls for age, sex, race, and comorbidities. Note the logarithmic scale on the x-axis. CABG (versus PCI) is associated with a dramatically lower odds of mortality (OR ~0.16, far to the left of the unity line), indicating significantly improved survival with surgical revascularization.
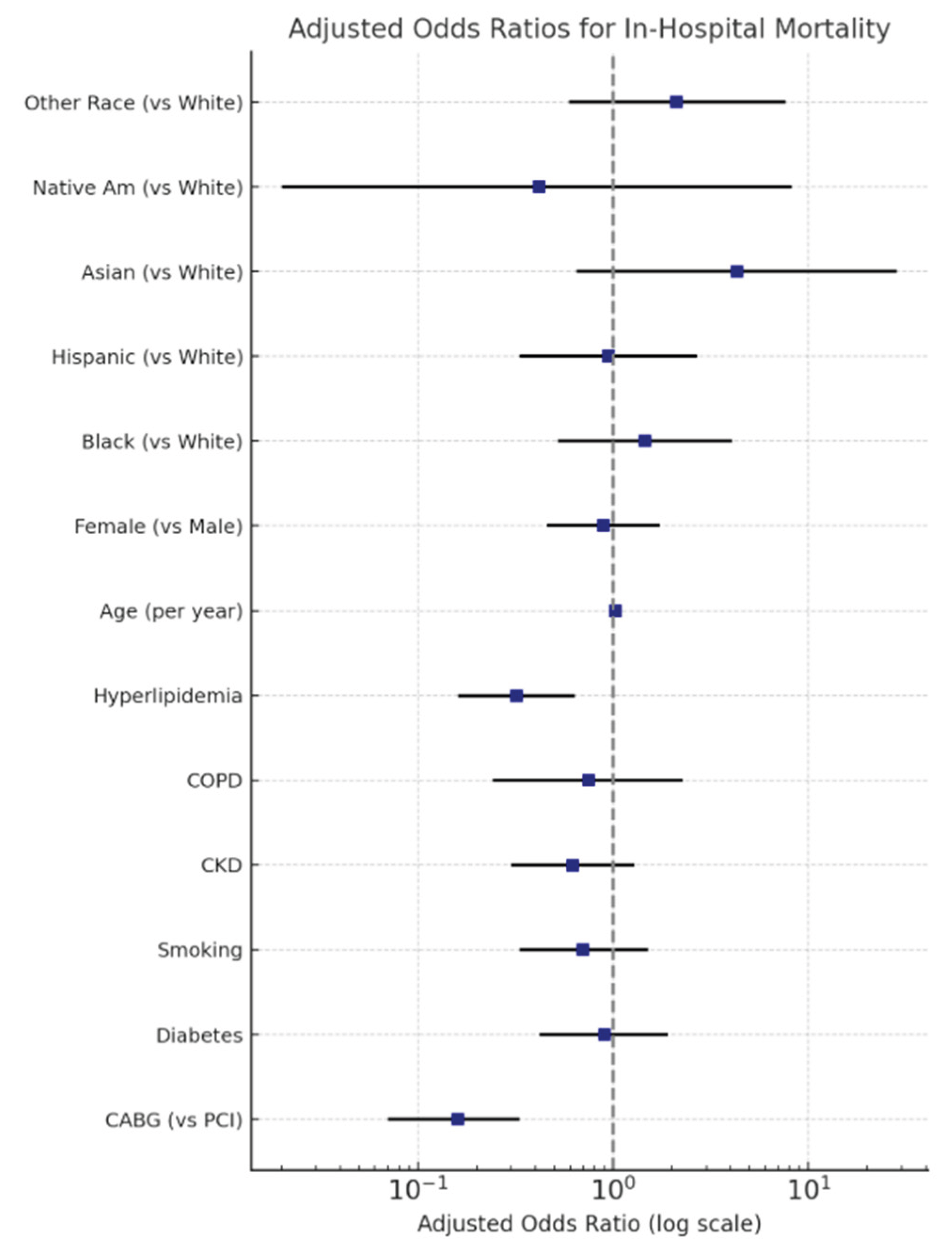

Table 1.
Baseline Characteristics and Comorbidities.
| 2016-2020 | Left Main STEMI & PCI | Left Main STEMI & CABG | P-value | Odds Ratio (C.I) |
| Total Population | 700 | 350 | ||
| Age | 0.47 | |||
| Mean±SD | 66.42±11.89 | 65.11±12.63 | ||
| Median(IQR) | 66(59-74.5) | 66(57-74) | ||
| LOS | <0.001 | |||
| Mean±SD | 7±9 | 14±10 | ||
| Median(IQR) | 4(1-9) | 10.5(7-21) | ||
| Total Charges $ | 0.006 | |||
| Mean | 284432 | 423202 | ||
| Median | 224667 | 307426 | ||
| Gender | ||||
| Male | 62.86% | 68.57% | REF | |
| Female | 37.14% | 31.43% | 0.41 | 1.29(0.70-2.37) |
| Race | ||||
| White | 58.82% | 66.67% | REF | |
| Black | 11.03% | 11.11% | 0.81 | 1.12(0.42-3.01) |
| Hispanic | 14.71% | 9.52% | 0.27 | 1.75(0.64-4.76) |
| Asian/Pac Isl | 5.88% | 3.17% | 0.37 | 2.10(0.41-10.68) |
| Native American | 2.21% | 0.00% | NA | 1 |
| Others | 7.35% | 9.52% | 0.81 | 0.87(0.29-2.64) |
| Mortality | 55.00% | 15.71% | <0.001 | 6.56(3.19-13.46) |
| Diabetes | 40.71% | 35.71% | 0.48 | 1.24(0.68-2.23) |
| Smoking | 21.43% | 21.43% | 1 | 1.00(0.49-2.03) |
| CKD | 25.71% | 24.29% | 0.83 | 1.08(0.53-2.18) |
| COPD | 10.71% | 12.86% | 0.65 | 0.81(0.33-1.99) |
| Hyperlipidemia | 57.86% | 57.14% | 0.92 | 1.03(0.58-1.83) |
| Alcohol | 5.00% | 2.86% | 0.48 | 1.79(0.36-9.01) |
| ECMO | 9.29% | 5.71% | 0.38 | 1.69(0.52-5.46) |
| IABP | 37.86% | 71.43% | <0.001 | 0.24(0.13-0.45) |
| Impella | 42.14% | 11.43% | <0.001 | 5.65(2.55-12.51) |
| Peripheral Vascular Diseases | 5.00% | 5.71% | 0.83 | 0.87(0.24-3.17) |
| History of Cardiomyopathy | 0.00% | 1.43% | NA | 1 |
| History of Systolic Heart Failure | 40.71% | 38.57% | 0.77 | 1.09(0.61-1.97) |
| Cachexia | 1.43% | 0.00% | NA | 1 |
| Morbid Obesity | 4.29% | 8.57% | 0.22 | 0.48(0.15-1.55) |
| Obesity | 8.57% | 10.00% | 0.74 | 1.19(0.43-3.24) |
| Chronic Liver Disease | 27.14% | 21.43% | 0.36 | 1.37(0.70-2.68) |
| Atrial Fibrillation/Flutter | 24.29% | 31.43% | 0.29 | 0.70(0.36-1.35) |
| Valvular Heart Disease | 10.71% | 17.14% | 0.18 | 0.58(0.26-1.30) |
| History of Stroke | 0.71% | 0.00% | NA | 1 |
| Acute Lactic Acidosis | 42.14% | 37.14% | 0.48 | 1.23(0.69-2.20) |
| Cardiac Arrest | 12.86% | 7.14% | 0.19 | 1.92(0.73-5.07) |
| Mechanical Ventilation | 63.57% | 37.14% | 0.001 | 2.95(1.59-5.48) |
| Renal Replacement Therapy | 10.00% | 11.43% | 0.75 | 0.86(0.34-2.18) |
| Presence of Aortocoronary Bypass Graft | 3.57% | 1.43% | 0.4 | 2.56(0.29-22.66) |
| Right Ventricular Infarction | 2.14% | 1.43% | 0.72 | 1.51(0.15-15.03) |
Table 2.
Clinical outcomes for left main STEMI with shock, by revascularization strategy. Mortality is dramatically higher in PCI-treated patients. Length of stay and hospital charges are significantly greater for the CABG group. (★ indicates statistically significant differences).
Table 2.
Clinical outcomes for left main STEMI with shock, by revascularization strategy. Mortality is dramatically higher in PCI-treated patients. Length of stay and hospital charges are significantly greater for the CABG group. (★ indicates statistically significant differences).
| Outcome | PCI Group | CABG Group | P-value |
|---|---|---|---|
| In-hospital mortality | 55.0% | 15.7% | <0.001 ★ |
| Length of stay (days) | 7 ± 9 (median 4 [1,2,3,4,5,6,7,8,9]) | 14 ± 10 (median 10.5 [7,8,9,10,11,12,13,14,15,16,17,18,19,20,21]) | <0.001 ★ |
| Total hospital charges | $284,432 (median $224,667) | $423,202 (median $307,426) | 0.006 ★ |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



