Submitted:
15 August 2025
Posted:
18 August 2025
You are already at the latest version
Abstract
Background/Objective: To test the feasibility of a pilot, randomised controlled trial of mistletoe therapy (MT) with an embedded qualitative study in the UK National Health Service (NHS) setting. Methods: 45 patients were recruited via an NHS oncology centre with a diagnosis of early or locally advanced breast cancer. Participants were allocated to: Iscador® Malus, Iscador® Pinus or physiological saline (placebo). Diaries and Quality of life questionnaires were administered. Qualitative interviews were con-ducted with participants, oncologists, and nurses. Feasibility was assessed by recruitment, retention, adherence, blinding and safety. Results: Sixty-seven patients approached August 2019-March 2020, and 15 gave consent. 14 participants were randomised, two withdrew during the trial. Ten participants and five staff were interviewed. Barriers to recruitment were the additional treatments/time, extra injections, and the possibility of placebo allocation. Adherence was very good. Diaries and interviews indicated that some participants struggled with injections and skin reactions. Participants perceived MT as natural, immune-boosting and promoting self-healing. There were 22 adverse events due to the MT, related to the injections or skin reactions. Conclusion: It is feasible in the UK to recruit breast cancer patients into a randomised controlled trial of MT versus placebo, for them to adhere, and provide follow-up data.
Keywords:
Viscum album
; mistletoe
; breast cancer
; feasibility
; pilot randomised controlled trial
; quality of life
1. Introduction
Mistletoe (Viscum album) has been used medicinally since prehistoric times. Anthroposophic use of mistletoe has developed using specific mistletoe formulations and regimes with a focus on supportive cancer care. [1] In Europe, mistletoe is a commonly used therapy by patients with cancer and it is integrated into oncology care via health insurance schemes in Germany, and Switzerland. [1]
A recent Health Technology Assessment report that focused on adjunct mistletoe therapy (MT) for breast cancer patients concluded that improvements in health-related quality of life compared to the control group were small to moderate, but that the risk of bias within efficacy trials was high. [2] This evidence is based on seven clinical trials (three were randomised controlled trials (RCTs)) using mistletoe as an adjunct therapy to standard treatment of chemotherapy and or radiotherapy in patients with breast cancer. Local skin reactions of low and moderate severity were reported in a median of 25% (range 5 to 94%) of patients, and mild to moderate systemic reactions in a median of 2% (range 0 to 8%) of patients.
Observational studies, cross-sectional studies and an ethical evaluation were also included in this HTA report. A comparative cost analysis from Germany reported significantly lower medical costs within 5 years after surgery for patients with MT than for patients without it, however there was no control for systematic bias. From studies conducted in Germany, it was calculated that a median of 25% (range 7-46) of patients with breast cancer and 29% of treatment providers use MT. The main motivations to use MT cited by patients in these studies were to reduce side effects, strengthen the immune system and take an active role in the treatment process. It was also reported in these studies that patients felt insufficiently advised about MT.
Whilst MT is prescribed in the UK, this is through the private sector, and predominantly in primary or community care. [3] The lack of a robust, relevant evidence base for MT in supportive cancer care prohibits progress in this field, despite its potential to improve the patient experience of cancer care, a major priority of the National Health Service (NHS) cancer plan. [4] As MT is not available within the NHS, the UK population is generally unaware of MT, and its application as a supportive adjunct therapy for cancer. This potentially enhances participant blinding to treatment allocation in a randomised clinical trial in the UK as they are less likely to understand MT appearance and its effects.
Our aim was to test the feasibility of a pilot, mixed phase, mixed methods, and placebo controlled RCT of MT in patients with breast cancer in the UK NHS setting.
2. Materials and Methods
2.1. Design and Setting.
We conducted a pilot, placebo controlled RCT of MT with an embedded qualitative study in patients with breast cancer, in a UK NHS setting. [5] There were three groups in the trial: Iscador Malus (M), Iscador Pinus (P) MT and physiological saline as the placebo. The feasibility of the trial was assessed in terms of recruitment, retention, adherence, blinding and safety. [EudraCT number: 2018-000279-34] The MAB study adheres to CONSORT guidelines outlined at https://www.equator-network.org/reporting-guidelines/consort/.
2.2. Sample Size and Site
The aim was to recruit 45 adult patients via one site, the Bristol Haematology and Oncology Centre (BHOC) at University Hospitals Bristol and Weston NHS Foundation Trust. This was a feasibility study with the sample size chosen to allow fair assessment of the aims of recruitment, retention, and completion of outcomes and an assessment of the viability of blinding.
2.3. Inclusion and Exclusion Criteria
Participants were adults 18 years or over with histologically confirmed early or locally advanced invasive breast cancer who, following surgery, were to receive adjuvant chemotherapy, with or without radiotherapy and able to be randomised within 12 weeks of surgery. Patients could be included if they were also scheduled to receive biological therapies such as trastuzumab or endocrine therapy. Patients who received only radiotherapy were excluded as this treatment is generally well tolerated and of short duration. They had to be willing to self-administer or have a nominated person administer their injections. Their Eastern Cooperative Oncology Group (ECOG) performance status was 0 or 1 and they could have no active, uncontrolled infection. [6] Full inclusion and exclusion criteria are available in Appendix A.
2.4. Randomisation and Blinding
The patient randomisation list and the medication block randomisation lists were produced by an in-house statistician at Iscador AG. Randomisation of patients was conducted by University Hospitals Bristol Pharmacy (UHBP). Allocation of participants to Iscador® M/ Iscador® P/placebo in a 1:1:1 ratio was performed by UHBP. A separate randomisation list was held by UHBP for individual emergency unblinding. In the case of a serious adverse event and unblinding being required, the pharmacist would have been asked by the principal investigator to look at the unblinding randomisation list. Both participants and healthcare professionals were uninformed about the allocation of the trial therapies.
Participants took MAB therapy for approximately six months, The first study therapy was given within a week of randomisation to the study and, ideally, prior to the start of chemotherapy. If participants had a skin reaction larger than 5cm diameter, they stopped the MAB therapy for one week, then resumed with a step down in dose. Participants or participant-nominated individuals (e.g., spouse or partner) were taught to administer the MAB therapy by the research nurse – once by nurse demonstration and then by administering the therapy themselves under nurse observation.
2.5. Mistletoe Therapy (Intervention Group)
Participants received mistletoe preparations Iscador® M or Iscador® P in 1ml ampoules for sub-cutaneous injection. The standard therapy regime was devised from the manufacturer’s recommendation in conjunction with the MAB advisory group. [Appendix B]
2.6. Placebo (Control Group)
Placebo participants underwent the same regime as those in the intervention group, and the placebo ampoules had identical external packaging and labelling to the MT ampoules. The placebo was physiological saline 0.90% w/v of sodium chloride, 308 mOsm/L or 9.0 g per litre. [Appendix B]
2.7. Data Collection
Feasibility was measured using clinical study data and qualitative interview data to assess the following objectives:
2.7.1. Recruitment
- Recruitment rate
- Obstacles to recruitment
2.7.2. Retention and Adherence
- Attrition rate with reasons if possible
- Acceptability of regular sub-cutaneous injections
- Adherence to the study therapy schedule
- Assessment of therapy related symptoms and health related quality of life in the sample population
- Completion of outcome measures
2.7.3. Blinding
- Assessment of blinding of patients
2.7.4. Adverse Events
- Adverse events from MT and placebo subcutaneous injections
2.8. Clinical Study Data
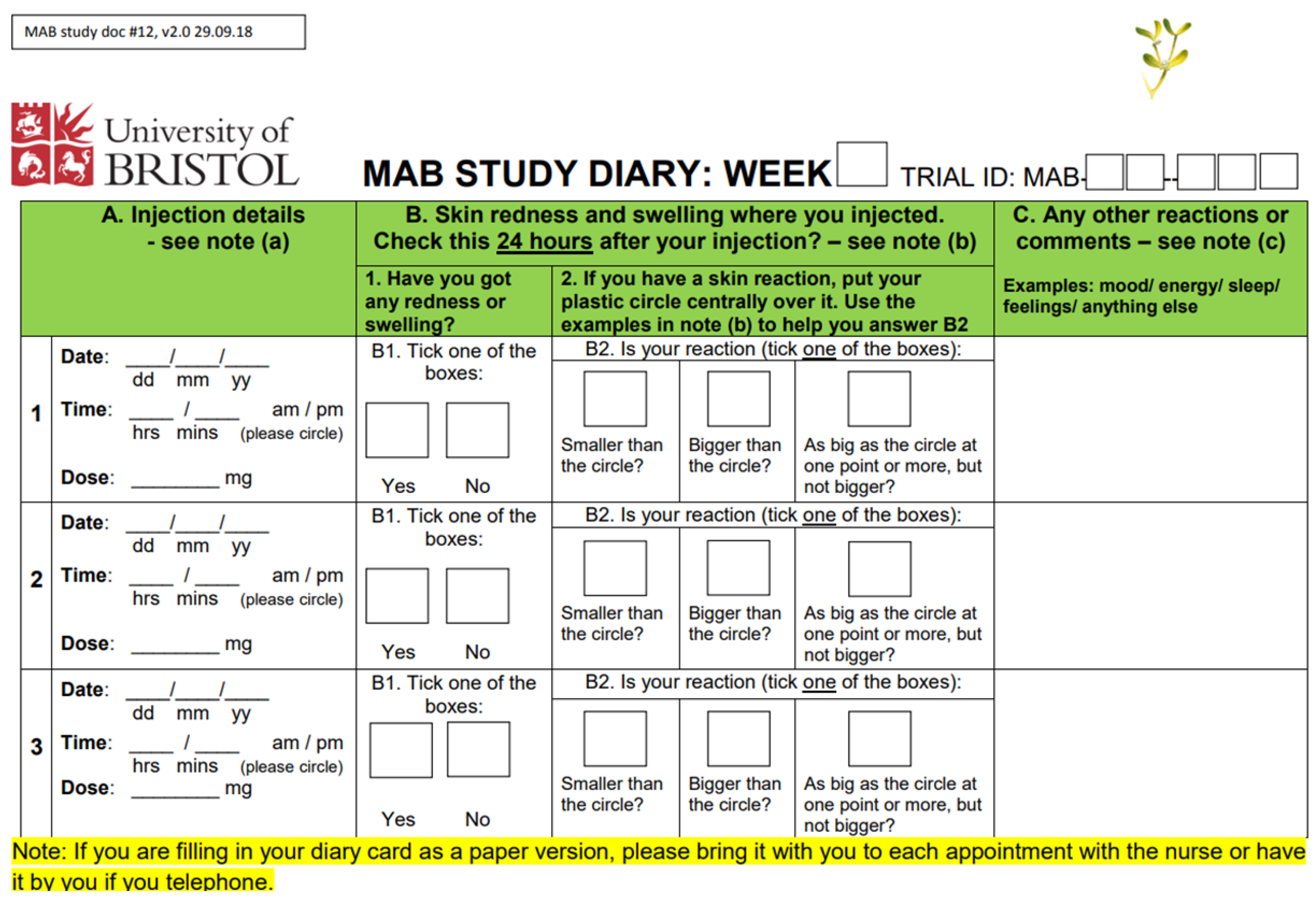
2.8.1. Participant Diaries
Participants received a diary card pack to record their thrice weekly MAB study therapy administration, the reaction to the injection, and any comments they wanted to add. [Appendix C]
2.8.2. Questionnaire Pack
This comprised six questionnaires: European Organisation for Research and Treatment of Cancer Quality of Life (EORTC- QLQ-C30), European Organisation for Research and Treatment of Cancer Quality of Life- Breast Cancer (EORTC QLQ-BR23), Functional Assessment of Cancer Therapy-Neutropenia (FACT-N) scale, Cancer Fatigue Scale, Autonomic Regulation Scale-State (ARS-S), and CompleMentary and Alternative Beliefs Inventory (CAMBI). [7,8,9,10,11,12] These were administered at three time points: Time point 0 or baseline (T0) - following randomisation and before the start of the chemotherapy regime; Time point one (T1) - following the 3rd cycle of chemotherapy; and Time point two (T2) - four weeks after last standard treatment (chemotherapy with or without radiotherapy), on the day of the last study (MAB therapy) treatment.
T0 questionnaires were completed during an initial visit to BHOC. T1 and T2 were either generated by the REDCAP database (for four participants) or administered by BHOC staff at the appropriate time for those participants working on paper.
2.8.3. Adverse Events
All adverse events experienced by the participants during the MAB trial were collected independent of their causal relationship with MT. The manual of the Common Terminology Criteria for Adverse Events (CTCAE) grading of toxicity was used to classify the adverse events. [13]
2.8.4. Qualitative Interviews
Semi-structured interviews were conducted by LD with participating patients, oncologists, and research nurses. All patient participants who had consented to being interviewed were contacted. In addition, three research nurses working on the MAB study and two oncologists were interviewed.
Initial interviews in the first few weeks of MAB therapy were conducted in person with five participants between October 2019 and February 2020. All remaining interviews were undertaken remotely in compliance with COVID-19 pandemic restrictions, and interviewees selected either telephone or online options. Thus, all staff interviews, five initial participant interviews and all ten second interviews, which took place up to one month after all treatment was completed, were conducted remotely. Written consent was obtained, and topic guides were used to aid questioning whilst allowing interviewees to discuss additional issues. [Appendices D and E] Topics considered included (i) awareness of MT; (ii) recruitment (iii) retention and adherence; (iv) blinding; (vi) perspectives on complementary and alternative therapies; and (vi) availability of complementary and alternative therapies within the NHS (staff only).
Interviews were transcribed and anonymised, then analysed thematically by LD assisted by MG and PG using NVivo qualitative data analysis software (version 12). [14] A subset of transcripts was coded inductively to establish an initial analysis framework (LD, AH), and differences were discussed during the process between LD, MG, and PG to ensure coding consensus. [15]
2.9. Data Analysis
The recruitment rate is expressed using descriptive statistics, as are all questionnaires completed by the participants. Retention is summarised by recording the number of participants in each study group at the pre-specified worst toxicity time point (T1) and 4 weeks post standard treatment (T2). A questionnaire was considered completed if data could be used. For example, the EORTC QLQ-C30 data was included if at least half the questions from the factors of interest were complete in accordance with the manual of the EORTC Quality of Life group. Blinding was assessed by asking the patient at T2 to assess which study treatment they had received or to register a “don’t know” option.
2.10. MAB Management
The core MAB management team members were SB, LD, AH and GF working in conjunction with the BHOC team led by JB. In the development and approval process of the MAB study this core team worked with a wider team of co-applicants, an advisory group and BHOC colleagues detailed within the acknowledgement section. The core MAB team met monthly during the MAB trial with additional attendance by patient and public involvement (PPI) members and advisory members as required.
The MAB Trial Steering, Data Monitoring and Ethics Committee comprised clinical, statistical, and patient representation (see acknowledgement section). The committee met regularly (every 4-5 months) prior to trial start up until the end, remaining available beyond that time if needed.
2.11. Patient and Public Involvement
Bristol-based MT research was formally launched in September 2010 with a public education event led by GF, AH, ME and the Cancer research network (CRN) of West of England cancer lead Catherine Carpenter Clawson, and involved the public, patients, and health professionals. This event contributed to our protocol development and the initial development of our topic guide for our qualitative interviews, with ME and SB piloting questions with health professionals. The MAB PPI group was convened in September 2017 by LD and AH and comprised four women with the experience of a breast cancer diagnosis, treatment and beyond. This initial work contributed to the refinement of our patient interview topic guide and patient facing documents, and to the use of a transparent disc to aid measurement of anticipated skin reactions during the trial. Two of our PPI members remained actively involved (JB and SB) throughout the trial, joining team meetings and the trial steering group meetings.
3. Results
3.1. Recruitment
Sixty-seven potential participants were approached, screened (25 were not eligible) and if appropriate recruited by the research nurses between August 1st 2019 and March 19th, 2020. Following screening, 15 were eligible and gave their consent. Participant 15 dropped out prior to randomisation.
Characteristics are available for 14 of the participants. All were women and had a mean age of 49 (range 36-76) years. They identified as White British (n=11), White other background (n=2) and Chinese (n=1). (Breast cancer status was stage 1-3, and 10 /14 participants were Estrogen Receptor Positive (ER+). [Table 1]
Ten of the 14 participants agreed to be interviewed both at the beginning and end of the study (20 interviews). The mean age of those interviewed was 46 years (range 36-63), and eight participants described themselves as White British and the remaining two as White other background. Five interviews were also undertaken with staff – two consultant oncologists involved in recruitment to the study, and three research nurses who were the day-to-day points of contact for the MAB participants.
All patient participants and staff interviewees were asked what they had known about MT before learning of the trial. The unanimous response from participants in the qualitative interviews was that they had not heard of the therapy before although everyone was familiar with the mistletoe plant; all were surprised to hear of its therapeutic use. [Table 2, A1 & A2]
The nurses were also unfamiliar with MT, although one said patients often spoke of complementary therapies with her and that mistletoe might have been mentioned. One of the oncologists was aware of patients who had used MT in private practice. [Table 2, A3]
3.1.1. Barriers to Recruitment
In the first five months of recruitment (August-December 2019), 43 potential participants were approached and 6 (14%) gave their consent. From January 1st to March 19th, 2020, 24 potential participants were approached and nine (38%) gave their consent. The difference in these recruitment rates was related to an initial ambiguity in the inclusion criteria around the human epidermal growth factor receptor 2 (HER2) status of patients, for which a major protocol amendment was made, improving recruitment from January 2020 onwards.
Reasons for non-participation can be grouped into four categories: not meeting the screening criteria (25), patient decision (22), healthcare professional decision (1), and practical barriers (4). [Figure 1] By 19th March 2020, 15 participants were consented, and 14 were randomised to treatment allocation. The 15th participant withdrew before randomisation citing the COVID-19 pandemic as the reason.
The most common reasons recorded on the recruitment log for women not accepting invitation into the trial (82%) were the injections or the related additional visits to BHOC. These concerns were echoed in the qualitative interviews. [Table 2,A4 & A5]
Other, more generic reasons included not wishing to be part of a trial or to receive the placebo, or the presence of other health issues.
In the January-March 2020 period of recruitment, seven in ten patient refusals were due to the extra hospital visits, and although not formally recorded these may also have been linked to the imminent COVID-19 pandemic.
3.1.2. Enablers to recruitment
Despite the potential barriers discussed above, several factors identified by our participant interviewees acted to outweigh them. These included the possibility that MAB therapy may enable participants to continue supporting their home life whilst undergoing chemotherapy. [Table 2, A6]
The idea of mistletoe as a natural product was also viewed favourably by some, as well as the accepted use of this therapy in other countries. Several participants also indicated they had altruistic reasons for taking part. [Table 2, A7 & A8] Some participants spoke of the appeal of regaining a sense of self-empowerment which they felt had been lost to cancer, surgery, chemotherapy and radiotherapy. [Table 2, A9]
Staff interviewed also spoke of the enthusiasm they noted for the study in participants, one commenting that some had asked whether they could take part despite not having been approached about the study. The oncologists also noted the positivity generated amongst participants by the trial. [Table 2, A10 & A11]
3.2. Retention & adherence
Fourteen participants were randomised and allocated to their MAB therapy. [Figure 2] Two of the 14 participants withdrew during the trial. Both remained in the study for around five of the anticipated six months’ duration. The first participant withdrew after 4 months and 27 days, and the nurse recorded ‘participant reported “forgot” to take/give injections for approximately 1 month and described feeling no better/no worse so made the decision to stop the treatment.' After unblinding, it was revealed this participant was on placebo.
The second participant withdrew at 5 months 5 days, and the nurse reported ‘Patient is currently emotionally distressed and unable to cope with the extra injections [due to Covid-19 outbreak].’ After unblinding, it was revealed that this participant was on Iscador M.
Adherence was measured by analysis of patient diaries and questionnaires. Participants were asked at the eligibility stage whether they wanted to complete these online or on paper, four of 14 participants opted for online.
The diary data shows that six participants took the MAB therapy for ≥26 weeks and five participants for ≥20 weeks. The remaining three participants returned diaries for 9,12 and 16 weeks respectively. 50% of the participants had one break in MAB therapy, and two participants had two breaks. All participants that had breaks were on MT and as per the MAB protocol which stated that a skin reaction of ≥5cm should result in one weeks break from MAB therapy, these participants had a step down to a lower dose. [Appendix B]
The free text section in the diaries allowed participants to express how they were coping with the MAB therapy on a weekly basis. Comments around this were focused on issues with methods of self-administration, pain and discomfort upon administration, difficulty in maintaining the routine of injections, and the impact of the COVID-19 pandemic. There were no comments around the increasing colour and viscosity of the solutions for the active MT as dosages increased nor any comments on a lack of change in appearance as dosages ‘increased’ in the placebo.
All 14 participants completed the baseline (T0) questionnaire. Twelve questionnaires were returned after the third chemotherapy cycle (T1), and 12 after the last MAB therapy treatment (T2). The loss of two T1 questionnaires was related to one of the participants who withdrew, and for the other questionnaire, it was unclear why it was not received. At T2, the missing questionnaires were both due to the participants that withdrew.
3.2.1. Barriers to retention and adherence
The factors indicated above by the participants who withdrew were also apparent in the interviews, along with other barriers identified by participants who remained on the study: Self-injection remained a challenge to the participants.
An additional concern related to the injections was that the syringes were not pre-loaded. Most participants were required to self-inject Filgrastim during their chemotherapy to stimulate white blood cell production. This was provided in a pre-prepared format and some participants compared their MAB therapy unfavorably. [Table 2, B1 & B2]
The absence of a visible skin reaction to MAB therapy was also a potential barrier to retention and adherence. A research nurse had anticipated that participants randomised to the placebo treatment might withdraw for this reason. [Table 2, B3] Practical considerations also played a part in participants’ thinking. The additional hospital visits were an issue, particularly with a lack of available parking nearby. [Table 2, B4]. The emerging COVID-19 pandemic also impacted and caused additional stress for the participants. [Table 2, B5]
For those participants whose treatment regimens included both chemotherapy and radiotherapy, the duration of their MAB therapy was also a potential barrier to carrying on with it. In some cases, adherence to the MAB therapy regime decreased somewhat after completion of chemotherapy. Some interviewees explained that, as they had understood that MT was helpful with chemotherapy side effects, it could seem less important either during radiotherapy or during the additional month of MAB therapy required post chemotherapy/ radiotherapy. [Table 2, B6]
Another interviewee offered an additional perspective. When she was able to ring the bell signaling completion of her final radiotherapy session, her MAB therapy, which was to continue for a further month, became less important. [Table 2, B7]
3.2.2. Enablers to retention and adherence
The skin reaction around the injection site to the MAB therapy, although not pleasant, made participants feel they could be receiving active MT. [Table 2, B8]
Engagement from family and friends was a further enabler for some participants and one participant wrote a blog about mistletoe with very positive feedback. [Table 2, B9] Personal investment in the trial by participants was also identified by the staff. [Table 2, B10] Some interviewees found their own unique ways of remembering their MAB therapy such as using a mistletoe-themed song for their morning alarm. [Table 2, B11]
The response of the participants to the MAB trial also influenced staff perspectives, some having their reservations over-ridden on seeing that participants were accepting the therapy and happy with it. [Table 2, B12,13]
3.3. Assessment of blinding
Ten participants were on an active MT (Iscador M (n=5) Iscador P (n=5) and four participants were on the placebo treatment. In the final questionnaire (T2) the 12 remaining participants were asked for their thoughts regarding which intervention they thought they had received and were given the options 'don't know', 'active' or 'placebo'. They were also asked to briefly explain their reasoning. [Appendix F]
Of the twelve participants, nine were on active mistletoe treatment and three were allocated to placebo. Of the nine participants on active treatment, four said they did not know their allocation, four said active and one said placebo. Of the three on placebo treatment, two said that they were on placebo, and one said they did not know. Eleven of the twelve participants gave their reasoning, and all gave an explanation relating either to how they felt during chemotherapy, or to whether they had skin reactions.
Among the ten participants interviewed, it was clear that most had spent considerable amounts of time thinking about whether they were receiving active or placebo therapy whilst on the trial and their opinions could fluctuate.
As with the questionnaire responses, interviewees indicated that the presence or absence of skin reactions and/ or their response to chemotherapy influenced their thoughts around this. [Table 2, C1-C3]
Some interviewees, though, said they were unable to decide which study therapy they had received as they did not know how their response to chemotherapy would have been in either case. [Table 2, C4] Whatever their thoughts on this however, the research nurses noted that participants were keen to discuss their possible therapy allocation throughout their treatment. [Table 2, C5]
One of the nurses indicated they could make a visual distinction between some MT doses and the placebo. [Table 2, C6] However, while the nurses were able to see both the placebo and MT ampoules, the participants saw only their own trial ampoules. it is of note that no participants on active MT commented on the increasing colour and viscosity of the solutions as dosages increased either in the final question around blinding in the T2 questionnaire, the qualitative interviews or the diaries.
3.4. Adverse Events
All adverse events (AEs) experienced by the participants during the MAB trial were collected. 23/218 were related to MAB therapy injections and experienced by 11 of the 14 participants. [Appendix G] Two of three remaining participants who did not have AEs related to injections were allocated to the placebo group. 13/23 AEs related to skin reactions to the injections, and as expected were experienced by the participants receiving MT.
18 of the 23 AEs were defined as Definitely related to the MAB therapy, with one Probably, one Possibly and three as Unrelated. All 23 AEs were linked to the injections and the skin response to these and were identified as: pain/discomfort with injection’ [n=7]; ‘bruising/hematoma at injection site’ [n=3]; skin reaction, ’redness/itchiness, rash/induration/lumps’ [n=13].
All AE were given a CTCAE score of 1 and were described as ‘not serious’ and ‘expected’. Reporting of intensity was not consistently made, but when reported it was described as ‘mild’. The exception was one AE report with a CTCAE of 5. This is considered as a reporting error due to other information describing the AE as ‘not serious’ and ‘expected’. Cross-referencing with the concomitant medications log and the qualitative interviews, this participant was on blood thinning agents and was vulnerable to excess bruising. Hence causality is reported as ‘not related’.
The free text section in the participant diaries included reflections on these AEs as indicated in the ‘retention and adherence’ section above, with one of the main themes focusing on pain and discomfort upon administration. The participant quotes in Table 2 also describe the impacts of these AEs and as already mentioned, could be viewed as either barriers or as facilitators to retention and adherence by different interviewees. [Table 2, E]
3.5. Quality of Life Questionnaire
3.5.1. Acceptability
Five of the six questionnaires were used to assess quality of life and signs & symptoms associated with cancer treatment. Item completion was high, with the only exception being questions 13 & 14 in the EORTC BR23 and questions 15 &16 in the FACT-N which focused on the individual’s sex life or intimate relationships.
Participants often did not respond (completely) to these particularly in the T1 and T2 questionnaires, and in one case a participant described a relationship breakdown in an annotation on the form. These questions were also identified as ‘odd’ or ‘interesting’ by some participants in the qualitative interviews. [Table 2, E1 & 2]
3.6. Outcome Data
This study was not powered to prove the efficacy of MT on quality of life, and symptoms of cancer treatment, and as such no differences were seen within or between groups for these measures. We have presented the EORTC QLQ-C30 global quality of life scores with a data box which shows similar trend for all three groups across the duration of the study. [Figure 3]

Data box:.
| Time /group | Placebo (n=4) | Iscador P (n=5) | Iscador M (n=5) |
| T0 | 90 ±12.5 | 78±24 | 71±18 |
| T1 | 73±8.0 | 58±27* | 60±23* |
| T2 | 72±20.9 | 65±10 | 67±17* |
*data from n=4 participants.
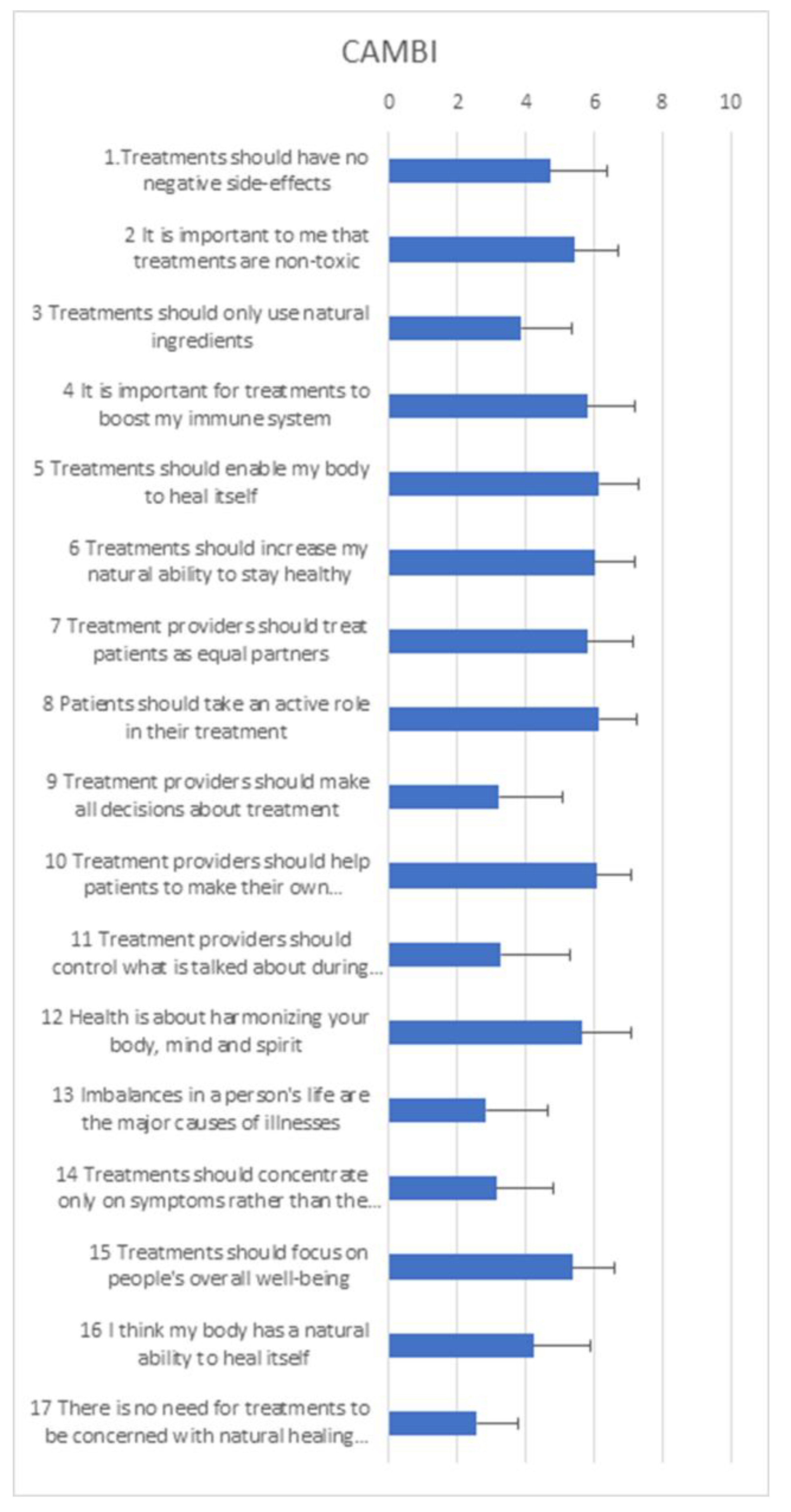
3.7. Complementary and Alternative Medicine Beliefs
The sixth questionnaire was the CAMBI questionnaire in which participants were asked to rate their opinions on a wide range of statements broadly around complementary and alternative approaches to health using a 0-7 scale (‘completely disagree’ to ‘completely agree’). [Appendix H] The results of this questionnaire at T0 suggest that overall participants were in favour of interventions that allow them to be involved in their own treatment, are considered natural and may promote immune-boosting and self-healing.
This was reflected in the qualitative interviews. Several participants had a positive view of complementary and alternative medicines (CAM) and had previously used them; however, others did not have a (strong) opinion on CAM approaches. [Table 2, F1 & 2]
Staff interviewees spoke of the possible benefits of complementary therapies for patients, although they indicated they themselves had not needed to use CAM. Although the perspectives of the oncologists interviewed were a little more circumspect, they also saw possible benefits in the use of CAM. [Table 2, F3 &4]
4. Discussion
4.1. Summary of Findings
The aim of the MAB study was to test the feasibility of a pilot placebo controlled, RCT of MT in patients with breast cancer in the UK NHS setting.
The recruitment rate was optimised during the study to just under 40% of people approached. Whilst the trial was open to both women and men participants our recruitment log indicated that only women participants were approached, this is not unsurprising as we know that breast cancer is rare in men, with around 400 new cases diagnosed each year in the UK. [16]
Most barriers to recruitment for potential participants were the extra treatment and time, unwelcome extra injections, and to a lesser extent being allocated to placebo. It is important to note that this decision was made in the context of physical and emotional challenges of diagnosis, need for chemotherapy, side effects of chemotherapy including intravenous treatments, use of granulocyte-colony stimulating factor (GCSF) injections and other supportive medications. There was a general lack of knowledge about MT expressed by both participants and health professionals.
Once recruited, over three quarters (12/15) of the participants completed the full trial therapy. Adherence to the therapy regimes was very good as measured by participant diaries, so too was the completion of the questionnaires at all three time points. Half of the participants said they did not know their therapy allocation. Both diary data and the qualitative interviews indicated that participants struggled with injections, and in some cases, also with the skin reactions. However, the qualitative interviews show a positive and enthusiastic attitude towards the MAB therapy with participants devising ways of coping with the negative aspects of regular self-injection. The number of adverse events related to MAB therapy were low and all were related to MAB therapy injections or skin reactions.
4.2. Strengths & Limitations
This was the first clinical trial of MT to be conducted in the UK, and in the NHS setting. It shows that MT can be provided and supported through the UK system of care. It also shows that participant adherence to the therapy (placebo or active) was good, as was completion of validated quality of life scales.
Whilst there were difficulties in recruiting to the trial, these were not all specific to the MAB therapy. Our recruitment was a third of that anticipated (15/45). Once optimal recruitment had been established in 2019, the remaining recruitment time was impacted by the impending COVID-19 situation and ultimate global lockdown in 2020. In addition to shortening the recruitment time, we feel the COVID-19 situation with national messages discouraging hospital attendance, as well as fears about infection risk and disruption of some chemotherapy treatment, impacted participation in early 2020.
It was our original thinking to interview people that declined to be involved. Unfortunately, this was not possible as it was not the researcher who recruited into the trial, rather the research nurse. Once the potential participant expressed that they were not interested in being involved, it did not seem fair to ask them to give their details about being contacted by the researcher and we suspect that our take up rate would have been low.
The trial was designed by primary and secondary care researchers, patients, and health professionals but on a day-to-day basis it was run by secondary care health professionals in an oncology research unit. Despite good communication between the University of Bristol (Principal investigators and Sponsor) and the Bristol Haematology and Oncology Centre this resulted in a lag in eliminating glitches in the trial start-up and in some practical aspects of data collection, which was further inhibited by the COVID-19 restrictions. For example, some participants changed diary records from online to paper without formal notification.
Whilst a significant number of potential participants declined involvement due to the extra hospital visits and injections, most who accepted were retained. This reflects both good initial patient information and good participant support from health professionals during the trial. We know from both the diaries and the qualitative interviews that participants struggled with the process of regular injections, and the skin reactions, yet they persevered with the therapy regime. It is possible that participants who perceived that they were allocated to placebo were less motivated.
The qualitative interviews suggest that some participants were less focused on their MAB therapy after their chemotherapy was complete. The Patient Information Sheet stated clearly that MT could be beneficial during both chemotherapy and radiotherapy. There is likely to be different reasons for wanting to stop the regular self-injections, but the qualitative interviews suggest some participants had just had enough of the injections and wanted to move on.
The lack of awareness of MT and its potential responses likely enhanced the blinding of participants to their therapy allocation. The increasing colour and viscosity of the solutions for the active mistletoe treatment as dosages increased was not commented on by the participants in the qualitative interviews, diaries, or in the final question around blinding. The appearance of the saline placebo would remain identical throughout, but due to the lack of knowledge around MT this equally may not have been a factor for participants.
Skin reactions and especially prolonged skin reactions are much less likely with the saline placebo. From the diary data, two of the four participants on placebo had at least one episode of minor skin reactions, and one participant also had a skin infection which may have been misinterpreted as a reaction.
While health professionals were not formally asked for their perspective on the allocated treatments, the qualitative interviews suggested that one nurse was aware of the increasing colouration of some participants’ therapies. The number of adverse events was low, and entirely related to self-injections and the skin reactions expected with MT. This is in line with adverse event monitoring in previous clinical trials. [17,18]
We used a range of quality-of-life measures and the CAMBI questionnaire. We have included access to the data with no comparative analysis, as appropriate to a feasibility study. Equally we cannot comment on the comparative effectiveness of the two Iscador products beyond the fact that having two active therapies may have enhanced recruitment. Of note, although overall the quality-of-life questionnaires were completed well, the questions relating to sexual feelings, sex life and interpersonal relationships appear to be inappropriate for our population at this point in their treatment.
4.3. Implications for Clinical Practice and Further Research
MT is integrated into oncology care via health insurance schemes in Germany and Switzerland. In the UK, it is predominately available via private practice although there is some NHS provision. An HTA report which focused on adjunct MT for breast cancer patients concluded that improvements in health-related quality of life compared to the control group are small to moderate but that the risk of bias within these efficacy trials is high. [2] Broader reviews across cancer types come to a similar conclusion. [19,20,21]
Our study design did not permit us to determine a primary endpoint, effect size or sample size. However, published full RCTs with a similar population conducted in other countries and settings suggest the use of EORTC- QLQ-C30 is preferable for quality of life measurement, and the two Semiglasnov RCTs of breast cancer patients provide estimates of effect size and calculate sample size. [17,22,23,24]
Whilst it is unlikely that MT will be made more widely available on the NHS in the near future, MT is used by cancer patients in the UK. MT is available across anthroposophic medicine centres in England and Scotland and is likely to be available through some individual General Practitioners. It is therefore important that we continue to add to the evidence–base of this safe adjunct therapy for cancer patients. Previous qualitative research, and the interviews within the MAB study suggest a perceived benefit for cancer patients. [25]
UK based research should focus on mistletoe provision within its countries, adding to the evidence base of efficacy within 21st century conventional cancer treatment. It is also important that different modes of application of mistletoe are examined bearing in mind the challenges of self-injection highlighted by this mixed methods trial. Other potential modes include pre-filled syringes, oral mistletoe, and hydrogels. Such modalities would further enhance the acceptability of mistletoe therapy by both patient and practitioner but to date there is little to no research on these approaches.
5. Conclusions
This pilot shows that it is feasible to recruit breast cancer patients into a randomised controlled trial of MT versus placebo within the UK National Health Service, for them to adhere to therapy, and provide follow-up data.
Author Contributions
For research articles with several authors, a short paragraph specifying their individual contributions must be provided. The following statements should be used Conceptualization, GF, DS, JPB, ALH; Methodology, GF, SB, ALH; Formal analysis, GF, LJD, MG, PG, ALH.; Investigation, GF, LJD, SB, ALH.; Data curation, LJD, SB, ALH.; Writing—original draft preparation, LJD, ALH; Writing—review and editing, all authors; Project administration, SB, ALH; Funding acquisition, GF, ALH. All authors have read and agreed to the published version of the manuscript.
Funding
The MAB study was funded by Verein für Krebsforschung (Society for Cancer Research), Arlesheim, Switzerland: for running costs and staff salaries (LD) Camphill Wellbeing Trust: for developmental work, running costs and staff salaries (AH, LD, SB) Claire Hunter Trust: for patient costs. Bristol University cancer fund: for staff salaries. (SB) School of Primary Care Research Grant (SPCR): for developmental work, running costs and staff salaries. (AH, ME, SB) Flexibility and sustainability funding from Avon Primary Care Research Collaborative: for developmental work and grant writing time for AH. Iscador AG: Iscador and placebo product. The funders were not involved in the design or conduct of the study, nor in the analysis of data, nor interpretation of our findings.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and all necessary research governance approvals were sought and approved including: Bristol REC reference: 18/SW/0045 / date of favourable opinion 12/04/2018 EudraCT number: 2018-000279-34 Date of registration on EudraCT 05/04/18 URL: https://www.clinicaltrialsregister.eu/ctr-search/search?query=+2018-000279-34++
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study. The patients were given at least 24 hours to consider whether they wanted to participate or not. If a patient was happy to take part, following written informed consent, they were randomised into either one of the two mistletoe therapies or a placebo therapy. There is no identifiable individual person’s data in the paper.
Data Availability Statement
Any further data not presented within the paper or supporting documents are available from the authors on reasonable request.
Acknowledgments
We would like to thank: Most importantly, all MAB participants, both patients and health professionals. The MAB co-applicants for their help in the development of the MAB project: Maggie Evans (researcher), Esther van der Werf (researcher), Sharon Love (statistician), Elizabeth Thompson (clinician), Ruth Randall (PPI), Broder von Laue (clinician). The MAB advisory group members who have provided extra expertise: Jo Beedell (patient representative, Sue Bell (patient representative) Stephen Falk (Consultant oncologist), Matthias Kröz (Mistletoe expert), Maurice Orange (mistletoe expert). CRN West of England cancer lead Catherine Carpenter Clawson for her initial public consultation support. Bristol Haematology and Oncology Centre Staff for clinical expertise and useful comments on the protocol. The MAB Trial Steering, Data Monitoring and Ethics Committee for their independent oversight: Willie Hamilton (Professor of cancer diagnosis in primary care and Chair) Sarah Pirrie (Independent Statistician) Jo Beedell (patient representative, Sue Bell (patient representative). Data entry and checking: The MAB team would like to thank Marie Platt and Alice Hagley for both assisting in entering and checking MAB data in the REDCAP database. The team would also like to thank Jemi Maliyil and Benjamin Roberto (Bristol undergraduate medical students) for their Student Choice project work on the MAB participant diaries.
Conflicts of Interest
Both SB and LJD received salary funding from the Verein für Krebsforschung (Society for Cancer Research), Arlesheim, Switzerland and the Camphill Wellbeing Trust. ALH received salary funding from the Camphill Wellbeing Trust. The authors declare no further conflict of interest.
Appendix A. Inclusion and Exclusion Criteria for the MAB Study
- Inclusion criteria
- a)
- Adults 18 years or over
- b)
- Histologically verified early or locally advanced invasive breast cancer (T1 – 3, N0 – 3, M0) without clinical suspicion/evidence of distant metastases. Routine staging for distant metastases should be according to local practice.
- c)
- Planned adjuvant chemotherapy with or without radiotherapy regime
- d)
- Willing to self-administer or have a nominated person e.g., relative to administer
- subcutaneous injections
- e)
- Eastern Cooperative Oncology Group (ECOG) performance status 0 or 1
- f)
- All other aspects of management as per the local multi-disciplinary team (MDT) decision.
- g)
- No active, uncontrolled infection
- h)
- Randomisation within 12 weeks of surgery
- i)
- Applicable to female participants only: non-pregnant and non-lactating, with no intention of pregnancy during chemotherapy, and prepared to adopt adequate contraceptive measures if pre-menopausal and sexually active. Adequate contraceptive measures according to the Clinical Trial Facilitation Group (CTFG) guidance for women of child-bearing potential (WOCBP)1 state that WOCBP can be recruited after a negative highly sensitive pregnancy test and assurance of an acceptable, effective method of contraception as a minimum until treatment discontinuation. Additional pregnancy testing should not be required.
- j)
- Applicable to male participants and relevant to trial therapy only, the participant should follow the guidance given by the nurse in relation to chemotherapy: No contraception measures are needed for male subjects with pregnant or non-pregnant women of childbearing potential as the Iscador product and placebo can be classified as having no genotoxicity or demonstrated or suspected human teratogenicity/fetotoxicity at subtherapeutic systemic exposure levels, as per the criteria set in the CTFG recommendations related to contraception and pregnancy testing in clinical trials.1
- k)
- No concomitant medical, psychiatric, or geographic problems that might prevent
- completion of therapy or follow-up.
- l)
- There will be no restrictions on MAB participants being involved in concurrent clinical trial as long as the consultant in charge of their care considers it appropriate and the study protocols do not exclude participation in more than one trial.
- Exclusion criteria
- a)
- Additional immunomodulatory therapy - for example: Patients receiving immunotherapy or biological therapy for autoimmune disorders, for diseases such as inflammatory bowel disease, inflammatory arthropathies, multiple sclerosis, etc.
- b)
- Receiving endocrine therapy as a stand-alone treatment
- c)
- Patients with known chronic viral infection such as active Hepatitis B, Hepatitis C or HIV
- d)
- Previous invasive breast cancer or bilateral breast cancer (unless treated with surgery or
- radiotherapy >5 years ago).
- e)
- Patients not able or willing to give informed consent
- f)
- Known allergy to mistletoe preparations
- g)
- Previous use of mistletoe, in the last 5 years, or current use of mistletoe
- h)
- Acute inflammatory or pyrexial conditions
- i)
- Chronic granulomatous diseases, active auto-immune diseases
- j)
- Hyperthyroidism with tachycardia.
- 1.http://www.hma.eu/fileadmin/dateien/Human_Medicines/01-AboutHMA/WorkingGro ups/CTFG/2014_09_HMA_CTFG_Contraception.pdf
Appendix B. MAB Study Therapy Regimes
- A)
- Example of typical study therapy & maintenance regime for both ISCADOR® M
- (Maleus) and ISCADOR® P (Pinus)
- Induction phase
- Week 1 0.01 mg (1.0ml) x3 = total of 0.03 mg Iscador M or P
- Week 2 0.1mg (1.0ml) x3 =total of 0.3 mg of Iscador M or P
- Week 3 1mg (1.0ml) x3= total of 3 mg of Iscador M or P
- Week 4 10mg (1.0ml) x3= total of 30 mg of Iscador M or P
- Week 5 20mg (1.0ml) x3= total of 60 mg of Iscador M or P
- Classification of reactions
- No or minimal response = no or only marginal local skin reactions, maximally 1 cm in diameter.
- Optimal response = local skin reactions, maximum diameter between 1 and 5 cm.
- Excessive response = local skin reactions, maximum diameter more than 5cm.
- A patient mistletoe medication was increased from the lowest dose to their optimal dose. The optimal dose was defined as a dose to which they experience a sustained local skin reaction, still present 24 hours after the injection. Such a reaction determines the dose they remained on for the rest of trial treatment unless they had a skin reaction of ≥5cm. In cases of skin reactions of ≥5cm, the participants dropped to the dose below (table 1) and this became their optimal dose.
- B)
- Treatment & maintenance regime with placebo
- Week 1-5
- Physiological saline 0.90% w/v of sodium chloride, (1.0ml) x3
- There is unlikely to be a sustained local reaction with the saline placebo and the participants will continue the same physiological saline preparation for the remaining time of the study but essentially the same rule applies as for the mistletoe arm: the participant would continue the same physiological saline preparation in week five and this will be called the maintenance dose.
Appendix C. MAB Participant Diary
Appendix D. Topic Guides for Qualitative Interviews with Participants
- Mistletoe And Breast Cancer (MAB) Pilot Trial: Participant interview topic guides (A and B)
- Interview A
- Patients who are participating in the study will be interviewed early in the study therapy phase. The interview will begin with general questions regarding their current health, how their [non-trial] treatment is going generally and how long they have been taking their study therapy. The following topics will then be explored:
- Previous knowledge and understanding of mistletoe.
- Before you were recruited into this trial had you heard of mistletoe therapy (also called Viscum, Iscador, Helixor etc)?
- If you had heard of it, what do you know about it? Did this match up with the information you have been given for the trial?
- If you hadn’t heard of it, what do you think about mistletoe therapy based on the trial information you have been given?
- Patients’ expectations of the study therapy
- What made you decide to join the MAB trial?
- What do you hope the trial therapy may do for you/help you with?
- Acceptability of consenting and randomisation procedures
- How did you feel about being asked to join the mistletoe trial (the process)?
- What did you think about the nurse’s approach – the information, signing a consent form?
- It will have been explained by the nurse that you may be randomised to one of two mistletoe therapies or placebo. How do you feel about possibly taking a placebo? - do you think that may change over time?
- Experiences and attitudes towards Complementary and Alternative therapies in general and herbal treatments specifically
- Mistletoe could be described as a CAM therapy. Talking more generally about CAM
- Have you used any herbal remedies or any other complementary therapies?
- How about family and friends?
- Which other remedies/ therapies? / For what reason? / What or who influenced you to use that? / Did you find it helpful?
- If you have not used CAM remedies/ therapies, have you ever thought about them, or about using them?
- Quality of life outcome measures & patient experience
- The participant will have filled in the questionnaires at the start of the therapy. It is also possible they may have filled in the mid-point questionnaire.
- Do the questions ask you about the issues/symptoms/effects that are experiencing or concerning/worrying/ you at this point?
- Are there some issues/ symptoms/ effects that you feel are missed out by the questions?
- Any questions which seemed irrelevant?
- Acceptability of questionnaires & patient diary
- How do you feel generally about filling in the questionnaires?
- Prompts:
- Usefulness: useful/not useful /allows you to self-monitor
- Time & effect: too much /about right/ok
- Burdensome: difficult/complicated/repetitive
- Acceptable: intrusive or inappropriate
- Any particular questions those were hard to understand or answer? Or which were particularly helpful (e.g., for self-monitoring)?
- Repeat these questions in relation to the patient diary.
- Adherence to therapy
- The study therapy is taken three times a week by injection – how are you getting on with that? Have you used the ‘help’ sheets; if so, are they helpful?
- (Participant may still be getting nurses help)
- Difficult/easy/no real problem
- Burdensome
- Any practical issues? - injecting, remembering to do it, feeling well enough.
- Anything which might make it easier/ simpler for you?
- Thank you for taking part in this interview.
- Interview B
- A follow-up interview will be carried out towards the end, or following completion, of the study therapy. Participants who do not complete the study therapy regime will be interviewed shortly after stopping it. The interview will begin with general questions regarding the participant’s current health, how their [non-trial] treatment is going generally and how long they have been taking their study therapy/ how long ago they stopped their study therapy. The following topics will then be explored:
- Patients’ experience of the intervention and its perceived effects – positive and negative
- How have your experiences of the study therapy been?
- Acceptability and feasibility of the mode of study therapy delivery/
- How did the initial dose adjusting period go for you?
- Did the dispensing (dealing with pharmacy) of the study therapy go ok?
- How did the support you received from the study nurse(s) work?
- The study therapy was to be taken three times/ week by injection – how did you get on with that?
- Difficult/easy/no real problem
- Burdensome
- Any practical issues? (e.g., injecting, remembering to do it, feeling well enough)
- Could anything have been done to make it easier/ simpler?
- Acceptability of outcome questionnaires
- We may have asked you this at beginning of trial but can we ask again
- Do the questions ask you about the issues/symptoms/effects that are experiencing or concerning/worrying/ you at this point?
- Are there some issues/symptoms/effects that you feel are missed out by the questions?
- Any questions which seemed irrelevant? How do you feel generally about filling in the questionnaires?
- Prompts:
- Usefulness: useful/not useful /allows you to self-monitor
- Time & effect: too much /about right/ok
- Burdensome: difficult/complicated/repetitive
- Acceptable: intrusive or inappropriate
- Any particular questions those were hard to understand or answer? Or which were particularly helpful (e.g., for self-monitoring)?
- Repeat these questions in relation to the patient diary.
- Any other treatments or interventions used by the patient.
- Have you used any other herbal remedies/complementary therapies or different approaches during the trial period?
- Acceptability of participating in the trial
- What are your feelings generally about being involved in the MAB study?
- Time
- Emotions
- Self-care
- Health - symptoms
- Placebo/ or mistletoe therapy
- Do you think you know whether you were randomised to mistletoe or placebo?
- Why do you think that?
- Thank you for taking part in this interview.
Appendix E. Topic Guide for Qualitative Interviews with Healthcare Professionals
Mistletoe And Breast Cancer (MAB) Pilot Trial: Healthcare professional interview topic guide
- Professional role
- Please could you tell me your job title and give me a brief description of your professional role (length of time in current and other relevant roles)
- Do you have any training in complementary therapies or anthroposophical medicine?
- About the Mistletoe study
- What are your views about the likely recruitment (any obstacles to this)?
- How acceptable and feasible do you think the mode of delivery for the intervention will be (sub-cutaneous self-injection taught by a research nurse)?
- What is your view on the likely attrition rate?
- What do you think about the proposed placebo?
- What are your views on the potential for success in blinding?
- Views on Mistletoe
- We will be using mistletoe as an adjunct treatment to cancer in the MAB trial.
- What do you know about mistletoe as a treatment?
- We will be using extract of mistletoe, or ‘Viscum album,’ as a herbal medicine for people with breast cancer as it may help to ameliorate the side effects of chemotherapy and radiotherapy
- What are your views on this in terms of acceptability to healthcare professionals and patients?
- Views on and experience of herbal remedies and complementary therapies
- Have you used herbal remedies or any other complementary therapies?
- How about family and friends?
- Which remedies/therapies? / For what reason? / What or who influenced you/ them to use that? / Did you find it helpful?
- If you have not used CAM remedies/therapies, have you ever considered using them? Why/ not?
- Local availability of complementary therapies
- Are you aware of any complementary therapy resources available in your unit / practice / locally?
- Role of complementary therapies in cancer
- What role, if any, do you feel complementary therapies might play in cancer care?
- Have any of your cancer patients ever requested information or advice about complementary therapies? How do you respond?
- Do patients ever tell you that they are using complementary therapies? How do you respond?
- Do you ever ask cancer patients whether or not they are using any complementary therapies?
- Have you offered advice or information about complementary therapies to a cancer patient or referred anyone for complementary therapy?
- If so, was that because you thought it would be a good idea or because they had asked?
- Complementary therapies and the NHS
- Do you feel complementary therapies should be integrated into the NHS?
- What do you see as the main barriers to integrating complementary therapies into conventional care?
- Are there any organisational / institutional / policy issues that might facilitate or impede such integration?
- Are some complementary therapies, in your view, better candidates for integration than others? Which ones and why?
- Do you think some complementary therapies are harmful? If so, in what way?
- Do you have any other comments?
- Thank you for taking part in this interview.
Appendix F. Treatment Allocation and Participant Opinion
| Patients’ opinion by allocation | What they said |
|
Iscador P Five responses |
Don’t know n=3 Some weeks because I felt strong and I had a redness after injections, I felt I could have the active part but some weeks, I've just had a feeling my body was in good shape before the diagnosis and I was really active with the kids and I barely reaction overall, I thought I could be on placebo. No text provided. I haven't been told which intervention I received. If I had to guess, I would say I received the Active intervention. This is because I feel I coped really well with chemo and hardly experienced any side effects and have been able to carry on with normal day to day activities - including looking after my 2 children. Active n=2 I had a red reaction most of the time after injecting. My family commented how well I looked and coped through chemo. I was able to be active around the house throughout the treatments. Bearing in mind I have been in lockdown since March and had to self-isolate from late January, some of the results have been warp by the isolation. I feel that the results would have been a lot better under normal circumstances but were a lot better than they would have been without mistletoe. Side effects of chemotherapy were mild and manageable for the majority of the 6 cycles of treatment. I felt well and was able to lead a normal life. Covid lockdown in cycle 3 was more of a hindrance and did affect my emotional wellbeing where I was unable to see friends or my partner. I feel that I 'got away' with chemotherapy side effects due to mistletoe injections. |
|
Iscador M 4 responses and 1 not complete T2 questionnaire. |
Don’t know n=1 Just do not know. I had a large reaction once and my partner said' you must be on the active intervention' but I felt that I could have had the reaction with… (incomplete) Active n=2 I felt I was having the active intervention. I did notice the difference in Cycles 2 and 3 of chemo, my energy levels had increased. Also, as the dose gradually increased to 10mg I encountered extreme reactions almost like hives. The area was raised, hot to touch and was large in diameter. I then went back to a reduced dose of 1mg for the rest of the trial. I have suffered with considerable fatigue during and post chemo and radiotherapy. I do not know if this was made better by receiving mistletoe injections hence my response to question 11 above. I would be very interested to learn whether I had the agent or a placebo, if it transpires it was the guess then I guess without it the fatigue would have been even worse. Placebo n=1 I may have been on the placebo as I had most of the symptoms given in the booklet, I read except that I did not get feeling sick. |
|
Placebo 3 responses and 1 did complete T2 questionnaire. |
Don’t know n=1 I don't know what I have been taking - active or placebo. Placebo n=2 I've not had any reaction to the injection which suggests placebo, but I have also been very lucky with mild symptoms to my treatment which suggests active. No skin reaction to injections |
Appendix G. Adverse Events
Adverse events from participants on Iscador P (n=5 participants)
| Participant | Description | CTCAE | Seriousness | Intensity | Expected | Causality |
| A | Pain on injection site | 1 | Not serious | Mild | 1 | Definite |
| Skin reaction of ≥5cm | 1 | Not serious | Mild | 1 | Definite | |
| B | Bruising | 1 | Not serious | Not reported | 1 | Not related |
| C | Pain at injection site | 1 | Not serious | Mild | 1 | Not related |
| Skin in duration @injection site | 1 | Not serious | Not reported | 1 | Definite | |
| D | Pain at injection site | 1 | Not serious | Not reported | 1 | Definite |
| Bruise at injection site | *5 | Not serious | Not reported | 1 | Not related | |
| Red patch 1cm, itchy & small lump | 1 | Scored as 5 | not reported | 1 | Definite | |
| Redness & itching at injection site | 1 | Not serious | Not reported | 1 | Definite | |
| E | Haematoma | 1 | Not serious | Not reported | 1 | Definite |
| Pain on injection site | 1 | Not serious | Not reported | Not reported | Definite | |
| Skin rash at injection site | 1 | Not serious | Not reported | 1 | Definite | |
| Cutaneous rash, skin reaction | 1 | Not serious | Not reported | 1 | Definite | |
| Cutaneous rash bilateral thigh | 1 | Not serious | Not reported | 1 | Definite |
*This is taken as an error in reporting due to other information given. Cross-referencing with concomitant medications log this participant was on blood thinning agents and was vulnerable to excess bruising hence causality is reported as not related.
- Adverse events from participants on Iscador M n=4/5 participants
| Participant | Description | CTCAE | Seriousness | Intensity | Expected (1) Not expected (2) |
Causality |
| F | Skin reaction | 1 | Not serious | Not reported | 1 | Probable |
| Lumps in stomach | 1 | Not serious | Not reported | 1 | Possible | |
| G | Skin reaction at injection site ≥5cm | 1 | Not serious | Not reported | 1 | Definite |
| H | Bruise at injection site | 1 | Not serious | Not reported | 1 | Definite |
| I | Pain on injection site | 1 | Not serious | Not reported | 1 | Definite |
| Local skin reaction | 1 | Not serious | Not reported | 1 | Definite |
- Adverse events from participants on placebo (n=2/4 participants)
| Participant | Description | CTCAE | Seriousness | Intensity | Expected | Causality |
| J | Discomfort at injection site | 1 | Not serious | Mild | 1 | Definite |
| Pain at injection site | 1 | Not serious | Mild | 1 | Definite | |
| K | Bruise at site of injection | 1 | Not serious | Not reported | 1 | Definite |
Appendix H. CAMBI Questionnaire at T0 (baseline)
References
- Mistletoe therapy: Information for doctors Accessed at Mistletoe therapy: Information for doctors (mistletoe-therapy.org) on 01.06.25.
- Schnell-Inderst P, Steigenberger C, Mertz M, Otto I, Flatscher-Thöni M, Siebert U. Additional treatment with mistletoe extracts for patients with breast cancer compared to conventional cancer therapy alone - efficacy and safety, costs and cost-effectiveness, patients and social aspects, and ethical assessment. Ger Med Sci 2022 Jul 14;20: Doc10. eCollection 2022. [CrossRef]
- Mistletoe centres in the UK Accessed at Centres – Mistletoe Therapy UK on 01.06.25.
- NHS Long Term Plan ambitions for cancer accessed at NHS England » NHS Long Term Plan ambitions for cancer on 01.06.23.
- Bryant S, Duncan L, Feder G, Huntley AL. A pilot study of the mistletoe and breast cancer (MAB) trial: a protocol for a randomised double-blind controlled trial. Pilot Feasibility Stud 2022 Apr 6;8(1):78. [CrossRef]
- The ECOG Performance Status Scale accessed at ECOG Performance Status Scale - ECOG-ACRIN Cancer Research Group on 01.06.25.
- Aaronson NK, Ahmedzai S, Bergman B, Bullinger M, Cull A, Duez NJ, Filiberti A, Flechtner H, Fleishman SB, de Haes JCJM et al. The European Organization for Research and Treatment of Cancer QLQ-C30: a quality-of-life instrument for use in international clinical trials in oncology. J Natl Cancer Inst 1993; 85(5):365-76. [CrossRef]
- Sprangers MA, Groenvold M, Arraras JI, Franklin J, te Velde A, Muller M, Franzini L, Williams A, de Haes HC, Hopwood P, Cull A, Aaronson NK. European Organization for Research & Treatment of Cancer breast cancer-specific quality-of-life questionnaire module: first results from a 3-country field study. J Clin Oncol 1996 Oct; 14(10):2756-68. [CrossRef]
- Wagner LI, Beaumont JL, Ding B, Malin J, Peterman A, Calhoun E, Cella D. Measuring health-related quality of life and neutropenia-specific concerns among older adults undergoing chemotherapy: validation of the Functional Assessment of Cancer Therapy Neutropenia (FACT-N). Support Care Cancer 2008 16(1):47-56. [CrossRef]
- Tanaka K, Akechi T, Okuyama T, Nishiwaki Y, Uchitomi Y. Development and validation of the cancer fatigue scale: a brief, three-dimensional, self-rating scale for assessment of fatigue in cancer patients. J Pain Symptom Manage 19 (1): 5-14, 2000. [CrossRef]
- Kröz M, Feder G, von Laue H, Zerm R, Reif M, Girke M, Matthes H, Gutenbrunner C, Heckmann C. Validation of a questionnaire measuring the regulation of autonomic function. BMC Complement Altern Med 2008; 8:26. [CrossRef]
- Bishop FL, Yardley L, Lewith G. Developing a measure of treatment beliefs: the complementary and alternative beliefs inventory. Comp Ther Med 2005; 13(2): 144-9. [CrossRef]
- Common Terminology Criteria for Adverse Events (CTCAE) Version 5.0, November 27, 2017, US Department of Health and Human Services, National Institutes of Health, National Cancer Institute.
- Braun V, Clarke V. What can “thematic analysis” offer health and wellbeing researchers? International Journal of Qualitative Studies in Health and Well-being 2014;9(1):26152. [CrossRef]
- Tracy SJ. Qualitative Quality: Eight “Big-Tent” Criteria for Excellent Qualitative Research. Qualitative Inquiry 2010;16(10):837-51. [CrossRef]
- UK breast cancer statistics in men accessed https://www.wcrf-uk.org/preventing-cancer/uk-cancer-statistics/ on 01.06.25.
- Horneber M, van Ackeren G, Linde K, Rostock M. Mistletoe therapy in oncology. Cochrane Database of Systematic Reviews 2008, Issue 2. Art. No.: CD003297. [CrossRef]
- Wider B, Rostock M, Huntley A, van Ackeren G, Horneber M. Mistletoe extracts for cancer treatment (Protocol). Cochrane Database of Systematic Reviews 2022, Issue 8. Art. No.: CD014782. [CrossRef]
- Loef M, Walach H. Quality of life in cancer patients treated with mistletoe: a systematic review and meta-analysis. BMC Complement Med Ther 2020 Jul 20;20(1):227. [CrossRef]
- Freuding M, Keinki C, Kutschan S, Micke O, Buentzel J, Huebner J. Mistletoe in oncological treatment: a systematic review: Part 2: quality of life and toxicity of cancer treatment. J Cancer Res Clin Oncol 2019 Apr;145(4):927-939. Epub 2019 Jan 2. [CrossRef]
- Chen Q, Wright F, Duncan LJ, Huntley AL. Profiling MT research and identifying evidence gaps: A systematic review of conditions treated, mode of application and outcomes. Eur J Integrat Med 2022 49: 101392. [CrossRef]
- Tröger W, Zdrale Z, Tišma N, Matijašević M. Additional Therapy with a Mistletoe Product during Adjuvant Chemotherapy of Breast Cancer Patients Improves Quality of Life: An Open Randomized Clinical Pilot Trial. Evid Based Complement Alternat Med 2014:2014:430518. [CrossRef]
- Semiglasov VF, Stepula VV, Dudov A, Lehmacher W, Mengs U. The Standardised Mistletoe Extract PS76A2 Improves QoL in Patients with Breast Cancer Receiving Adjuvant CMF Chemotherapy: A Randomised, Placebo-controlled,Double-blind, Multicentre Clinical Trial. Anticancer research 2004 24: 1293-1302.
- Semiglasov VF, Stepula VV, Dudov A, Lehmacher W, Mengs U. Quality of Life is Improved in Breast Cancer Patients by Standardised Mistletoe Extract PS76A2 during Chemotherapy and Follow-up: A Randomised, Placebo-controlled, Double-blind, Multicentre Clinical Trial. Anticancer Research 2006 26: 1519-1530.
- Evans M, Bryant S, Huntley AL, Feder G. Cancer Patients' Experiences of Using Mistletoe (Viscum album): A Qualitative Systematic Review and Synthesis. J Altern Complement Med 2016 22(2):134-44. [CrossRef]
Figure 1.
Screening & recruiting for MAB therapy.
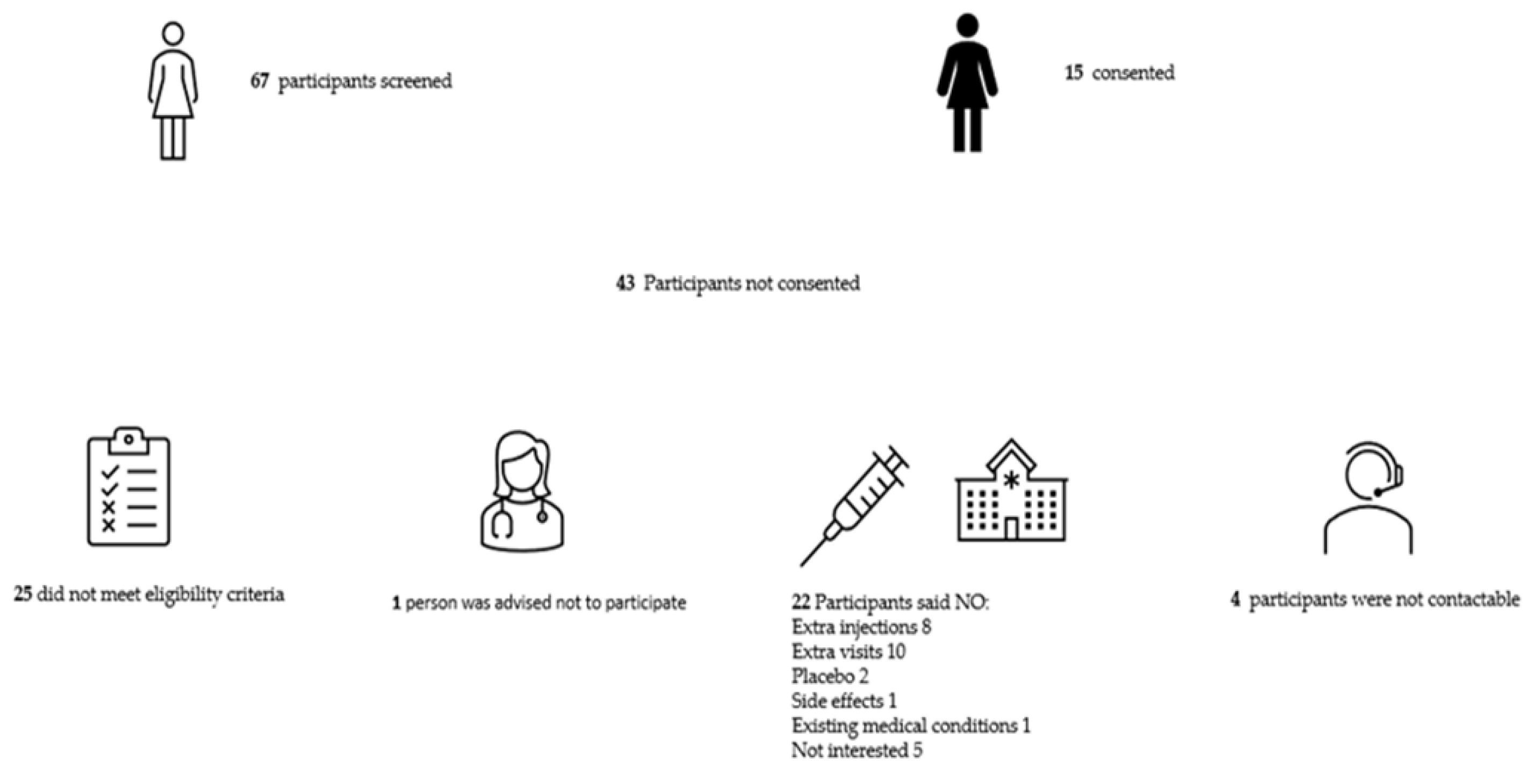
Figure 2.
Consort diagram.
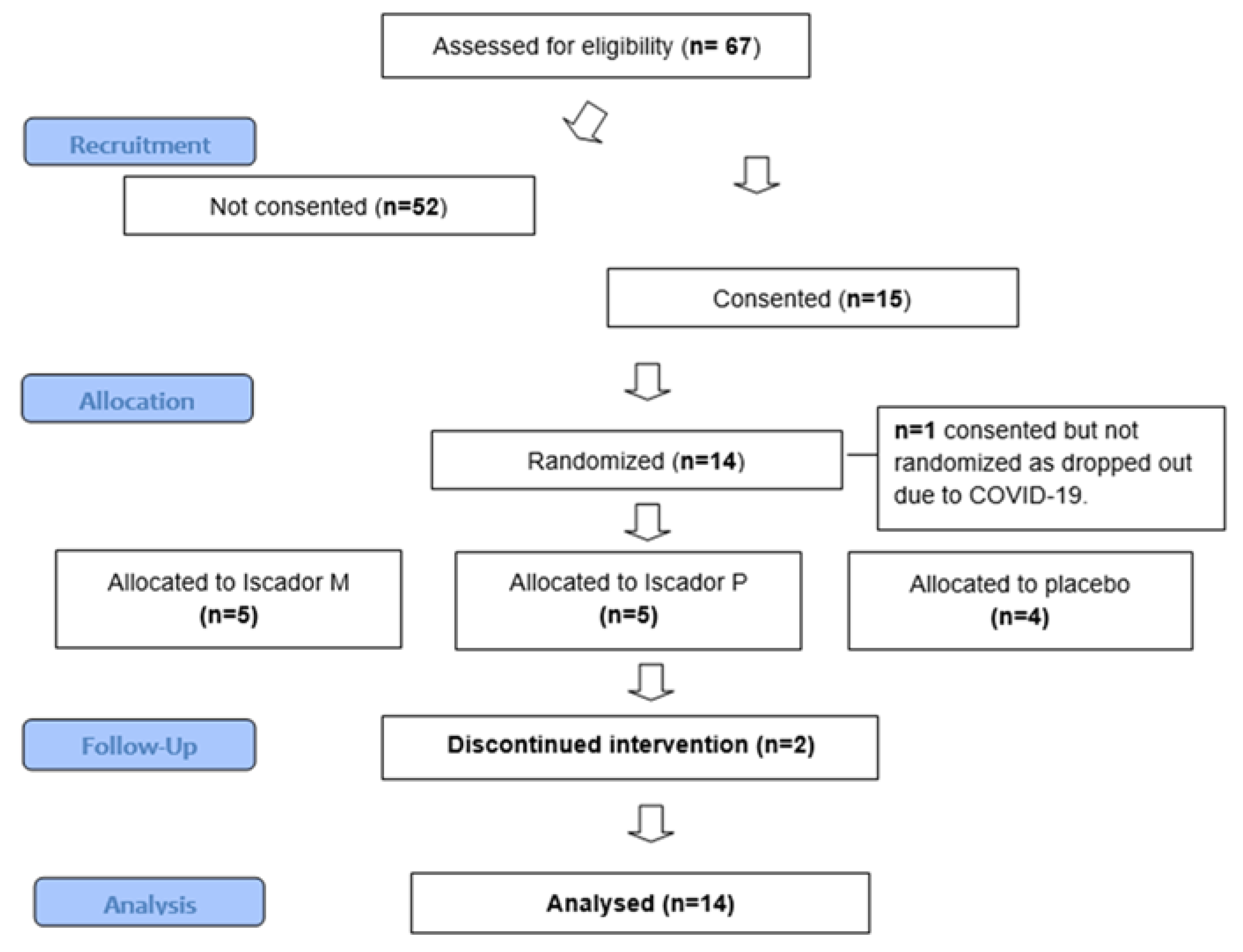
Figure 3.
Mean and SD of Global Quality of Life scores across the three MAB groups at T0, T1 and T2.
Figure 3.
Mean and SD of Global Quality of Life scores across the three MAB groups at T0, T1 and T2.
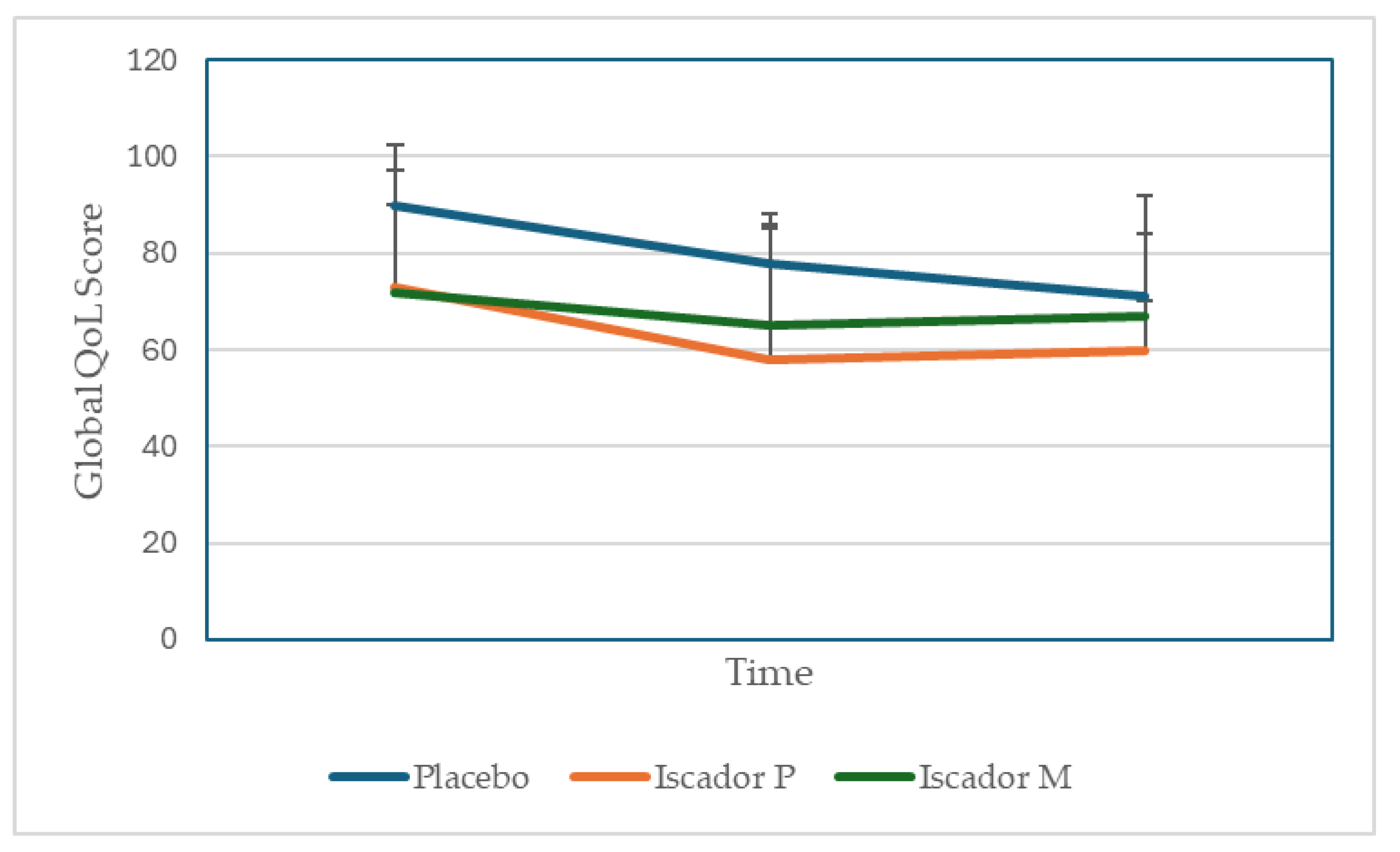
Table 1.
Characteristics of MAB participants (n=14).
| Participant characteristics |
Cancer characteristics |
|||||||||
|
Mean age (yrs) |
Age range (yrs) |
Identified as | Education | Occupation | Laterality | Stage | Tumour size | Nodes | ER status | |
| 49 | 36-76 | White British n=11 White other background n=3 Chinese n=1 |
No formal qualifications n=1 Secondary n=2 Further n=2 Higher n=9 |
Employed n=11 retired n=1 unemployed due to ill health n=1 |
Right =7 Left =7 |
Stage one = 3 Stage two =9 Stage three =2 |
T1= 2 T2=12 |
N0=7 N1=4 N2=2 N3=1 |
ER+= 10 ER-=4 |
Key: Secondary education ≤16yrs (level 2) Further education16-19yrs (level 3) Higher education 18yrs + (Level 4+) .
Table 2.
Illustrative quotes from participants interviews.
| Feasibility outcomes | Illustrative quotes |
| A Recruitment | |
| Awareness of mistletoe therapy |
A1 “Never heard of it before” Participant G. A2 “The berries are poisonous, so this was quite interesting. I was like ‘mistletoe?’ (laughs) Gosh, ok” Participant K. A3 “A while back it was quite a popular thing for people to try … for their metastatic cancer. A lot of patients were looking at getting that in the private sector” Oncologist A. |
| Barriers to recruitment |
A4 “If it will help me then I’ll have it, but I find it hard to inject myself.” Participant G. A5 “Initially I said no ‘cos of all the extra hospital appointments … with the little one and we live out at (village X) so getting to the hospital (is difficult)” Participant B. |
| Enablers to recruitment |
A6 “I thought it was a chance to maintain my family life by reducing my side effects” Participant H. A7 “Having a natural product that could alleviate something like a chemo treatment, I found the idea of that absolutely amazing” Participant J. A8 “I said ‘yes I’d like to go ahead with it’ because I did see that Germany, Switzerland and Holland had already started using it and I did a bit of research and people were paying for it privately in America and this country …. I just thought anything that will give me an edge as well is absolutely going to help. Help me and also other people for the future, so it’s win-win” Participant J. A9 “If I am finding this too much, I can say no… the other things I didn’t have control over” Participant C. A10 “[Patients] question if there is any trial they would be eligible for, having mistletoe, because I think they in a way are aware …. The thing is patients are interested; I find them to be more interested” Research Nurse A. A11 “[Patients were] clearly enthusiastic about potentially entering the study …. Happy to do any extra attendances that might be necessary” Oncologist A. |
| B Retention & adherence | |
| Barriers to retention and adherence |
B1 “When you don’t like needles then you’ll always be terrified by needles” Participant H. B2 “You have to build the injection up yourself … in some ways I found that quite difficult because you’ve got time to think about what you’re doing and I’d rather not, I’d rather just take something out of a packet and off. Yeah. So in a way it prolonged the agony” Participant J. B3 “I kind of feel like if someone notices that she’s not reacting then she probably will think she’s on placebo and may drop off. So far it didn’t happen but I can’t really say it’s not going to” Research Nurse A. B4 “It’s proven to be a bit tiresome, I must be honest with you, having to come into oncology … we have to keep going back weekly and it means coming into the city and it’s a nightmare to park and all of those things” Participant D. B5 “Well I have to say I didn’t like going [to the hospital]… it did make it more stressful because obviously the place you don’t want to go to is the place you’ve got to go to, but they temperature checked you at the door on the way in, I had a mask, I had gloves, they had masks and you just had to get on with it really” Participant F. B6 “I had the first week of radio and then .... I kept forgetting to take it” Participant A. B7 ““Once I’d finished the other treatment then the mistletoe became kind of secondary …. After my last radiotherapy I rang the bell and my husband and my daughter were there with me and that was a real kind of emotional moment and it felt like a real sense of closure and yet with the mistletoe, that was still going on, so it wasn’t a closure” Participant E. |
| Enablers to retention and adherence |
B8 “It was painful and it was irritating me, I was like ‘oh I can’t be doing with this’ and I did have thoughts ‘oh shall I just finish with it?’ And then in the back of my mind I just thought ‘well would I really be having these reactions if I was on placebo? I just kind of had to ride the storm basically and I’m glad I did because I ended up sort of talking to myself going right, ok, there are positives to this, this is uncomfortable at the moment but, you know, it’s not going to last’” Participant C. B9 “I had a blog page …. I told them all about the mistletoe on that and I got a very positive response” Participant D. B10 “Even if they’d said they got a skin reaction and we’d said ‘ok, tell us about that, is that problematic’, they were still really keen to kind of carry on and say ‘no, I really want to do this and it’s fine’ …. So once they’d signed up to it they really wanted to persevere and see it through” Research Nurse C. B11 “I’ve got an alarm on my phone that goes off in the morning, I’ve chosen Justin Bieber’s classic hit ‘Mistletoe’ to remind me!” Participant E. B12 “What we were concerned about is the injecting themselves. So they seem to be coping alright …[and] they all seem to be sort of happy to be carrying on with it which is actually more surprising” Research Nurse B. B13 “To begin with I was a bit uncertain, but when I saw they were accepting it quite easily I thought that was quite good and they didn’t have any side effects. And none of them complained to me about being tired, whereas 99% of the people, if you look at any of my letters …. would have toxicity and fatigue” Oncologist B. |
| C Assessment of blinding |
C1 “What makes me think I might have had the placebo because I’ve had no skin reactions at all” Participant F. C2 “I viewed [the skin reaction] as possibly having the actual mistletoe injection instead of a placebo so I was like this is good, I’ve actually got the mistletoe (laughs) so I was quite pleased.... I think with the reaction that I had and the way that I felt throughout chemotherapy, I would lean more towards thinking that I had had either mistletoes, but like I say you never know, maybe it was all in my mind. But I think, yeah, I think that I did have mistletoe.” Participant B. C3 “I feel very strongly that it was the mistletoe …. I was ready for the [chemotherapy] side effects and I didn’t have them … All I had was hunger” Participant K. C4 “I don’t know if it was the mistletoe that sort of helped or if it was just the frame of mind, I honestly couldn’t tell you” Participant A. C5 “Some people were saying I don’t think I had it because I still had some side effects or there were others that said I think I did have it because I felt great all the way through, but I think they definitely had an opinion as to whether they were on it” Research Nurse C. C6 “So the colour of the [mistletoe] liquid is probably a light yellow but the saline is … colourless.… I can say from week four I can see the difference” Research Nurse A. |
| D Adverse events | Relevant quotes in B and C e.g., B8, B9 & C2 |
| E Questionnaire data |
E1 "There was some slightly odder questions than others. There was a couple of questions about my sex life which I thought was interesting, a bit left-field." Participant E. E2 "... there were questions about kind of, you know, like your sex life and that sort of… Some of that obviously, yeah, ... I just put not applicable" Participant C. |
| F Complementary and alternative medicine beliefs |
F1 “I fully understand the power of plants ... But I don’t fully believe they can cure everything ‘cos I think there is a place for engineered drugs if you need them. I think it’s a complementary thing” Participant F. F2 “To be perfectly honest I don’t really think about it … just go with the flow” Participant A, who had not used CAM therapies previously. F3 “I think mainstream treatment should absolutely sit alongside kind of complementary or additional therapies because if it’s improving their general health, wellbeing, emotional and physical kind of health then that’s great” Research Nurse C. F4 “I tend to be fairly relaxed about patients taking …. complementary medicines because I think at the very least you’ll be harnessing a placebo and potential psychological benefits, and then there may be added benefits. Now if it’s got a very active ingredient or there’s something unknown about it then I’d be more cautious ‘cos I think we just don’t have any evidence about the interactions” Oncologist A. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



