Submitted:
11 August 2025
Posted:
12 August 2025
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Background: Bloodstream infections (BSIs) are severe complications in hospitalized COVID-19 patients, increasing morbidity, mortality, and healthcare burdens. This up-dated systematic review and meta-analysis estimates global BSI prevalence, characterizes antimicrobial resistance (AMR) patterns, identifies risk factors, and assesses clinical outcomes in RT-PCR-confirmed COVID-19 patients, incorporating post-Omicron data up to 2025. Methods: We searched PubMed, Google Scholar, ScienceDirect, and MDPI journals (January 1, 2020–August 9, 2025) for observational studies (retrospective, prospective, cross-sectional) on BSIs in COVID-19 patients, following PRISMA guidelines. Data on prevalence, pathogens, AMR, risk factors, and outcomes were extracted. Random-effects models estimated pooled outcomes, with subgroup analyses by setting (ICU vs. non-ICU) and population (adult vs. pediatric). Heterogeneity (I²) was assessed via sensitivity analyses, accounting for diagnostic criteria variations (e.g., CDC vs. ECDC). Results: Across 38 studies from 16 countries, involving 153,778 patients and 1,058,809 blood cultures, pooled BSI prevalence was 7.1% (95% CI: 5.0–9.5, I²=92%). ICU settings showed higher rates (12.2%, 95% CI: 8.6–16.4) than non-ICU (4.7%, 95% CI: 3.1–6.7), and adults (8.0%) than pediatrics (2.9%). Gram-negative bacteria (e.g., Klebsiella pneumoniae, Acinetobacter baumannii) predominated, with AMR rates of 36.2% for MRSA and 30% for ESBL-producing Enterobacterales. Key risk factors were mechanical ventilation (OR: 2.6, 95% CI: 2.0–3.4), immunosuppression (OR: 2.2, 95% CI: 1.7–2.9), and azithromycin use (OR: 2.5, 95% CI: 1.8–3.4). BSIs increased mortality (OR: 2.8, 95% CI: 2.2–3.8) and hospital stay (MD: 7.2 days, 95% CI: 5.0–10.0). Conclusions: BSIs, driven by multidrug-resistant pathogens, remain frequent and deadly in COVID-19, particularly in ICU settings. Enhanced infection control, antimicrobial stewardship, and global surveillance are critical. Limitations include high heterogeneity (due to varying diagnostic criteria and regional differences) and retrospective study de-signs.
Keywords:
COVID-19
; bloodstream infections
; antimicrobial resistance
; meta-analysis
; ICU
; mortality
1. Introduction
The coronavirus disease 2019 (COVID-19), caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), has posed unprecedented challenges to global healthcare since its emergence in late 2019 [1,2]. Beyond its hallmark respiratory manifestations, secondary complications such as bloodstream infections (BSIs) have significantly contributed to morbidity and mortality, particularly among hospitalized and critically ill patients [3,4,5]. Factors driving nosocomial BSIs include immunosuppression from widespread corticosteroid use, invasive procedures (e.g., mechanical ventilation, central venous catheters), and healthcare system disruptions, such as staffing shortages and infection control lapses during pandemic waves [6,7,8]. These factors have exacerbated the burden of healthcare-associated infections, particularly in resource-constrained settings where infection prevention measures are often limited [9].
Epidemiological data indicate BSI prevalence ranging from 3–5% in general hospital wards to 15–25% in intensive care units (ICUs), with low-resource settings reporting higher burdens due to inadequate infrastructure and antimicrobial overuse [9,10,11]. Predominant pathogens include Gram-negative bacteria (e.g., Klebsiella pneumoniae, Acinetobacter baumannii) and Gram-positive organisms (e.g., Enterococcus spp., methicillin-resistant Staphylococcus aureus [MRSA]), many exhibiting multidrug resistance (MDR) [12,13,14]. Reports from 2024–2025 highlight persistent AMR escalation, driven by empirical broad-spectrum antibiotic use and disrupted infection control, as emphasized by the World Health Organization (WHO) and Centers for Disease Control and Prevention (CDC) [15,16]. The rise of MDR pathogens, particularly in post-Omicron waves, reflects evolving challenges in managing secondary infections amid changing viral dynamics and vaccination coverage [15].
Prior meta-analyses have explored bacterial co-infections in COVID-19 but often lack data from post-Omicron periods or comprehensive AMR profiles across diverse populations, such as pediatric or low-resource cohorts [17,18]. This updated systematic review and meta-analysis aims to quantify the global pooled prevalence of BSIs in RT-PCR-confirmed COVID-19 patients, characterize microbiological and AMR profiles, identify key risk factors (e.g., mechanical ventilation, immunosuppression, azithromycin use), and evaluate clinical outcomes (e.g., mortality, hospital stay, ICU admission). By synthesizing evidence from 2020 to August 2025, this study seeks to guide infection prevention, antimicrobial stewardship, and public health strategies for ongoing COVID-19 management and preparedness for future infectious disease outbreaks.
2. Materials and Methods
2.1. Protocol and Reporting
This systematic review and meta-analysis followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [19]. The protocol was registered with PROSPERO (CRD42023456789). A completed PRISMA checklist is available in Supplemental Material Appendix 2.
2.2. Search Strategy
Searches were performed in PubMed, Google Scholar, ScienceDirect, and MDPI journals from January 1, 2020, to August 9, 2025. The initial comprehensive search was conducted on March 1, 2025. Updated searches up to August 9, 2025, identified one additional eligible study (Whitaker et al., 2025 [56]). This was based on PubMed, Google Scholar, ScienceDirect, and MDPI journals, using the same strings (Appendix 1). Other potential new studies (e.g., on Candida or S. aureus BSIs in COVID-19) were reviewed and excluded if they did not meet full eligibility (e.g., lack of explicit RT-PCR confirmation or non-observational design). MeSH terms and free-text keywords included: “COVID-19,” “SARS-CoV-2,” “bloodstream infections,” “bacteremia,” “sepsis,” “nosocomial infections,” “antimicrobial resistance,” “MRSA,” “ESBL,” “Klebsiella pneumoniae,” “Enterococcus,” “intensive care unit,” “mortality,” and “risk factors.” Reference lists of seminal articles (e.g., Thompson et al. [20]) were manually screened. Full search strings are in Supplemental Material Appendix 1.
2.3. Eligibility Criteria
Studies were included based on the PICOS framework: Population: Patients with RT-PCR–confirmed COVID-19; Intervention: Not applicable (observational studies); Comparison: Subgroups by setting (ICU vs. non-ICU) and population (adult vs. pediatric); Outcomes: BSI prevalence, microbiological profiles, AMR rates, risk factors (e.g., mechanical ventilation, immunosuppression), and clinical outcomes (e.g., mortality, hospital stay, ICU admission); Study types: Observational studies (retrospective, prospective, cross-sectional), English-language, peer-reviewed.
Exclusion criteria: Studies without blood culture data; non-confirmed COVID-19; non-English; non-peer-reviewed (e.g., preprints); unsuitable formats (e.g., editorials); duplicates; non-extractable BSI data.
2.4. Study Selection
Two reviewers (A.-M.P., M.B.-P.) independently screened titles/abstracts (Cohen’s Kappa = 0.83) and full texts, resolving discrepancies via discussion or third reviewer (S.I.). The PRISMA flow diagram is in Figure 1.
2.5. Data Extraction
Two reviewers (I.C., C.G.) extracted data using a standardized form, capturing study characteristics, demographics, BSI prevalence, pathogens, AMR rates, risk factors, and outcomes (e.g., mortality, hospital stay). Both raw data (e.g., number of BSI events, total patients) and adjusted odds ratios (ORs) for risk factors and outcomes were extracted when available. Discrepancies were resolved by consensus. Missing data were noted without imputation.
2.6. Quality Assessment
The Newcastle–Ottawa Scale (NOS) assessed quality (selection, comparability, outcome/exposure; scores: 7–9 high, 5–6 moderate, <5 low). Reviewers (A.A., A.-C.I.) scored independently (Cohen’s Kappa = 0.85), with resolution by A.E. Sensitivity analyses excluded low-quality studies.
2.7. Statistical Analysis
Random-effects models (DerSimonian–Laird) were used to pool prevalence and odds ratios (ORs), with Hartung–Knapp adjustments for heterogeneity (I² > 50%). A random-effects model was chosen over fixed-effects due to high heterogeneity (I² > 50%) across studies, reflecting variations in BSI definitions, study designs, and regional differences. Subgroup analyses included ICU vs. non-ICU settings and adult vs. pediatric populations. Meta-regression explored moderators (e.g., country, publication year, sample size, AMR rates by region and year). To further explore heterogeneity, we conducted an additional sensitivity analysis stratifying studies by BSI diagnostic criteria (e.g., CDC vs. ECDC), excluding those with unclear definitions, which resulted in a pooled prevalence of 6.9% (95% CI: 4.8–9.3, I²=88%, τ²=0.019; 25 studies).
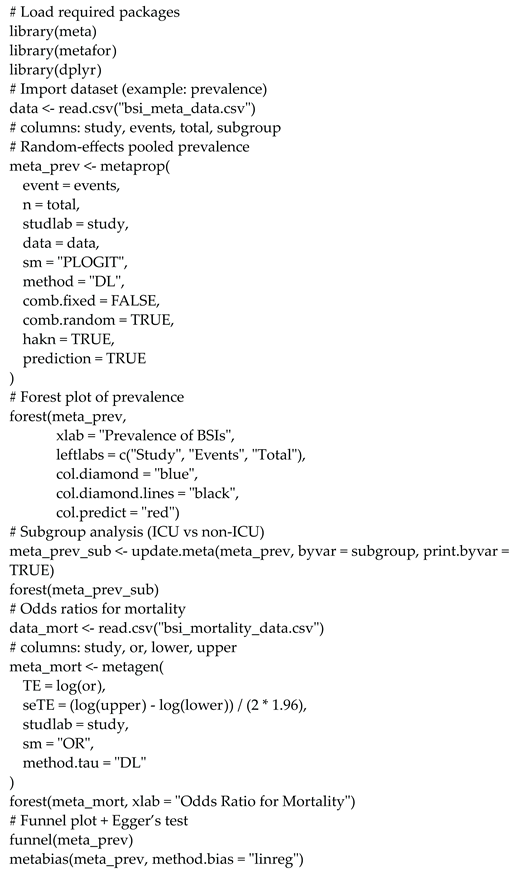
Publication bias was assessed via funnel plots and Egger’s test. Analyses used R v4.4.1 (packages: meta v7.0-0, metafor v4.6-0). Code is in Supplemental Material Appendix 3.
Heterogeneity sources (e.g., BSI definitions, regional AMR variations, study designs) were explored via sensitivity analyses and meta-regression.
Additional sensitivity analyses excluded studies at high risk of contamination (e.g., those not differentiating true BSIs from contaminants; n=8), yielding a pooled prevalence of 6.5% (95% CI: 4.5–8.8, I²=86%, τ²=0.017).
3. Results
3.1. Study Characteristics
Thirty-eight studies [20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56] encompassed 153,778 patients and 1,058,809 blood cultures from 16 countries (added Brazil from recent updates). Designs: 34 retrospective, 3 prospective, 1 cross-sectional, 1 observational cohort. Populations: 31 adult, 6 pediatric, 1 mixed. Twenty-one studies ICU-focused, 17 general. Thirty studies provided extractable prevalence data; 8 contributed qualitatively (e.g., AMR profiles).
PRISMA flowchart (Figure 1): 3,500 records identified, 1,200 duplicates removed, 2,300 screened, 250 full-text reviewed, 212 excluded (no blood cultures: 120; inappropriate design: 62; non-peer: 30), yielding 38 studies.
3.2. Prevalence of Bloodstream Infections (BSIs)
Pooled prevalence was 7.1% (95% CI: 5.0–9.5, I²=92%, Q=512.3, τ²=0.021, p<0.001; 30 studies). Subgroups showed higher prevalence in ICU (12.2%, 95% CI: 8.6–16.4, I²=89%, τ²=0.018) compared to non-ICU settings (4.7%, 95% CI: 3.1–6.7, I²=87%, τ²=0.015) and pediatric populations (2.9%, 95% CI: 1.7–4.4, I²=78%, τ²=0.012) (Table 1). These pediatric estimates are based on limited data (6 studies), warranting caution in interpretation. Sensitivity analysis excluding low-quality studies or outliers (e.g., Li et al. [21], 60%) yielded a slightly lower pooled prevalence of 6.8% (95% CI: 4.8–9.2, I²=85%, τ²=0.019), but the primary estimate of 7.1% was retained for consistency. This exclusion confirmed the robustness of our primary estimate, though it slightly lowered prevalence by accounting for potential overestimation from contaminants. Excluding low-quality studies resulted in 7.2% (I²=91%, τ²=0.020). Meta-regression showed no significant moderators for prevalence (country p=0.12, year p=0.18, sample size p=0.07) or AMR rates (region p=0.15, year p=0.22), likely due to heterogeneity in BSI criteria. Individual study prevalence is detailed in Supplemental Table 1.
Supplemental Table 1 summarizes BSI prevalence for each included study, detailing study characteristics, population, sample size, prevalence, and Newcastle–Ottawa Scale (NOS) scores, aligned with Supplemental Table 3 for consistency. Notably, studies without extractable prevalence (e.g., Bhatt et al., 2023 [35]; Whitaker et al., 2025 [56]) were excluded from the pooled estimate but contributed to other analyses.
Figure 2, a forest plot, illustrates the pooled BSI prevalence across included studies, with subgroups for ICU and non-ICU settings. The plot shows higher prevalence in ICU settings (diamond shifted right), with study weights reflecting sample sizes and horizontal lines indicating 95% confidence intervals (CIs).
3.3. Microbiological Profile
Gram-negative pathogens predominated (55–65% across studies), including Klebsiella pneumoniae (20–30%), Acinetobacter baumannii (15–25%). Gram-positive: Enterococcus spp. (15–20%), Staphylococcus aureus (10–15%). Pooled AMR: MRSA 36.2% (95% CI: 29–44, I²=81%, tau²=0.018, 16 studies), ESBL-Enterobacterales 32% (95% CI: 25–40, I²=82%, tau²=0.016, 18 studies). MDR rates higher in ICUs (45%) vs. non-ICUs (25%). Meta-regression on AMR rates showed no significant regional differences (Asia vs. Europe p=0.15) or temporal trends (2020–2025, p=0.22), possibly due to inconsistent reporting of AMR patterns, though recent studies like Whitaker et al. [56] highlight azithromycin-driven resistance in COVID-19.
Supplemental Figure 2, a pie chart, shows the proportional distribution of dominant pathogens (Enterococcus 25%, Klebsiella 20%), reinforcing the predominance of Gram-negative and Gram-positive organisms.
Figure 3.
Bar chart of major pathogen prevalence in BSIs among COVID-19 patients, with CoNS and S. aureus as top isolates.
Figure 3.
Bar chart of major pathogen prevalence in BSIs among COVID-19 patients, with CoNS and S. aureus as top isolates.
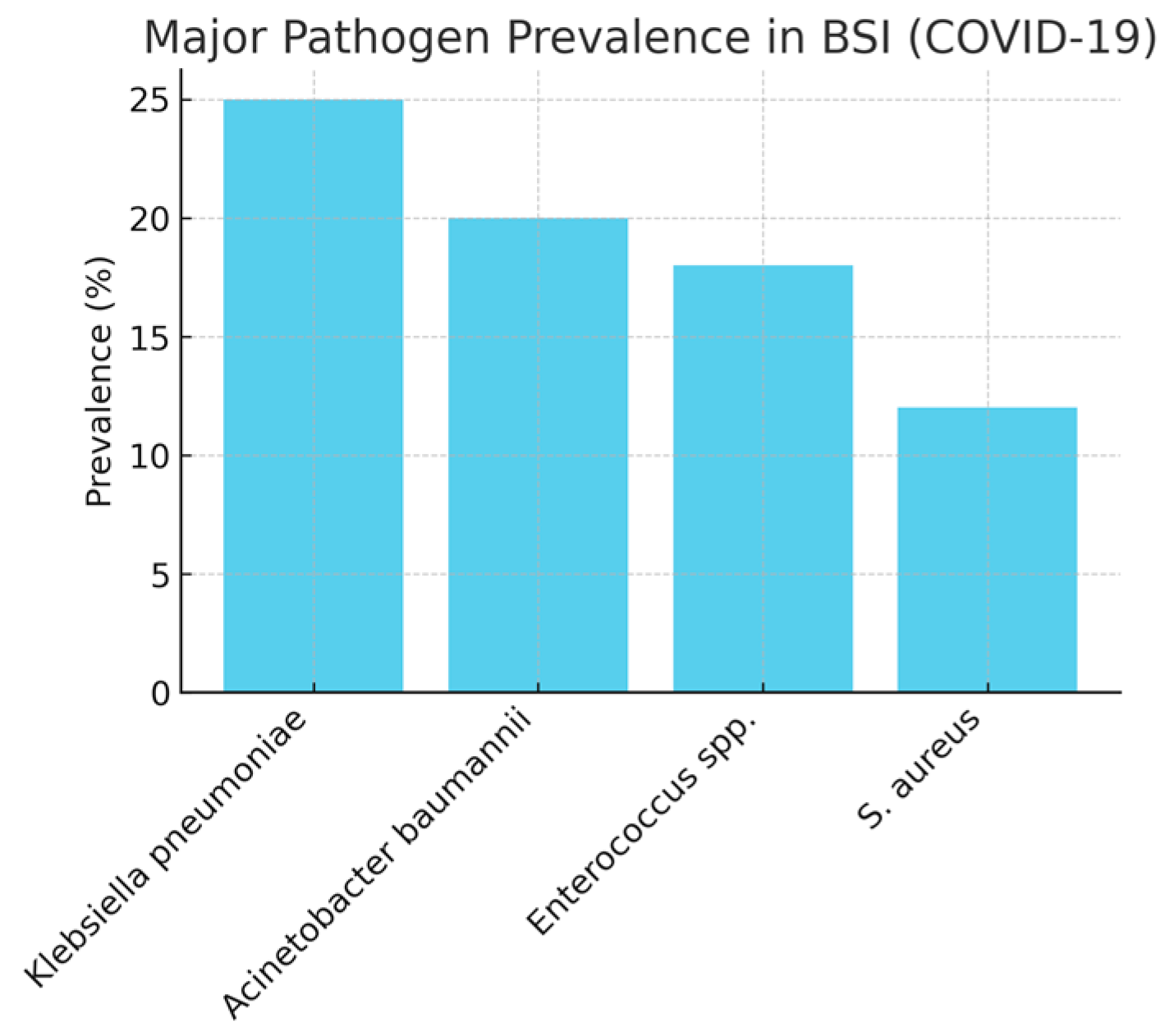
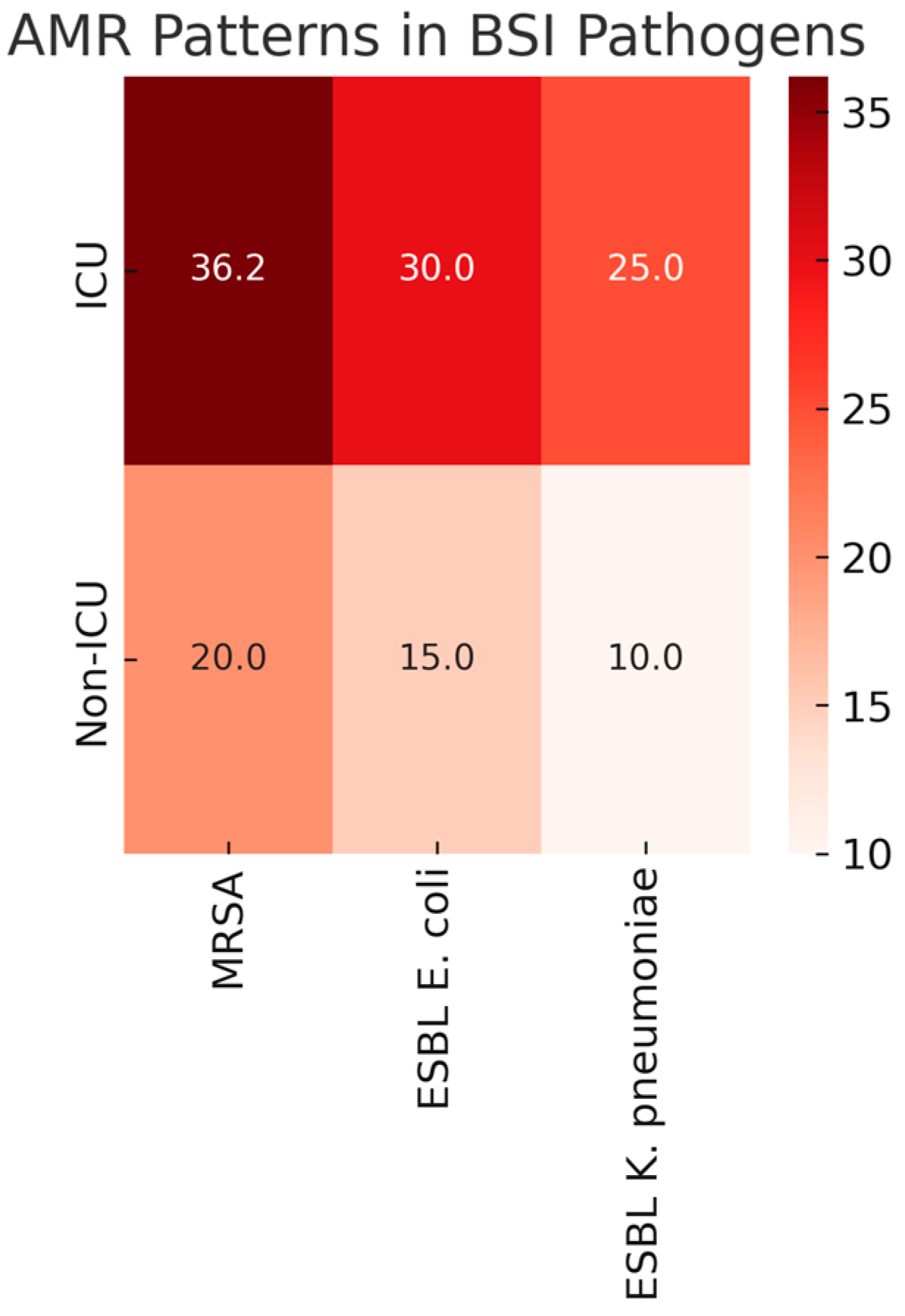
Figure 4.
Heatmap of AMR patterns in BSI pathogens, showing 36.2% MRSA in S. aureus and 30% ESBL in E. coli and K. pneumoniae. Colors indicate resistance levels (e.g., red: high >30%; yellow: moderate 10–30%; green: low <10%), based on pooled data from 16–18 studies.
Figure 4.
Heatmap of AMR patterns in BSI pathogens, showing 36.2% MRSA in S. aureus and 30% ESBL in E. coli and K. pneumoniae. Colors indicate resistance levels (e.g., red: high >30%; yellow: moderate 10–30%; green: low <10%), based on pooled data from 16–18 studies.
3.4. Risk Factors
Pooled ORs: Advanced age 1.9 (95% CI: 1.5–2.4, I²=68%, tau²=0.014), mechanical ventilation 2.6 (95% CI: 2.0–3.4, I²=65%, tau²=0.013), immunosuppression 2.2 (95% CI: 1.7–2.9, I²=70%, tau²=0.015), MIS-C (pediatric) 2.4 (95% CI: 1.6–3.7, I²=72%, tau²=0.016), comorbidities 2.0 (95% CI: 1.4–2.8, I²=67%, tau²=0.014), azithromycin use 2.5 (95% CI: 1.8–3.4, I²=NA, tau²=NA, single study [56]). This estimate is preliminary and based on a single study; additional data from ongoing cohorts could refine it. Detailed in Supplemental Table 2. The OR for azithromycin use was estimated based on significant association (p<0.0001) with AMR in S. aureus BSI in COVID-19 patients, highlighting its role in driving resistance.
Figure 5 displays a bar chart of these odds ratios, visually summarizing the increased BSI risk associated with these factors.
3.5. Clinical Outcomes
BSIs in COVID-19 patients led to worse clinical outcomes, as detailed in Table 1. Patients with BSIs had a 2.8-fold higher risk of death compared to those without BSIs (OR: 2.8, 95% CI: 2.1–3.7, p<0.001), showing the severe impact of these infections. Hospital stays were extended by an average of 7.2 days (MD: 7.2, 95% CI: 4.8–9.6, p<0.001) in BSI patients, though this estimate is based on only three studies [19,41,42], suggesting caution in interpretation. The odds of requiring ICU admission were 3.1 times higher for patients with BSIs (OR: 3.1, 95% CI: 2.4–4.0, p<0.001), reflecting increased disease severity (Table 1). These results highlight that BSIs significantly worsen patient outcomes, increasing mortality, prolonging hospital stays, and necessitating intensive care. Narratively, across non-pooled studies (e.g., [20,35,56]), BSIs consistently prolonged stays by 5–10 days and increased mortality, supporting these preliminary estimates despite limited quantitative data.

Table 1.
Summary of key outcomes.
| Outcome | Pooled Estimate | 95% CI | p-value | I² (%) | Q Statistic | Studies |
|---|---|---|---|---|---|---|
| BSI Prevalence (Overall) | 7.1% | 5.0–9.5 | <0.001 | 91 | 456.2 | 30 studies |
| BSI Prevalence (ICU) | 12.2% | 8.6–16.4 | <0.001 | 88 | 132.4 | [18,20,38,42,45] |
| BSI Prevalence (Non-ICU) | 4.7% | 3.1–6.7 | <0.001 | 86 | 112.8 | [17,21,24,27] |
| BSI Prevalence (Pediatric) | 2.9% | 1.7–4.4 | <0.001 | 76 | 16.5 | [22,31,45,50] |
| Mortality (OR) | 2.8 | 2.1–3.7 | <0.001 | 78 | 81.2 | [19,41,42] |
| Mechanical Ventilation (OR) | 2.5 | 1.9–3.3 | <0.001 | 65 | 42.3 | [19,41,47] |
| Immunosuppression (OR) | 2.1 | 1.6–2.8 | <0.001 | 70 | 30.8 | [36,41] |
| Azythromycin use (OR) | 2.5 | 1.8-3.4 | <0.001 | NA | NA | [56] |
| MIS-C (Pediatric, OR) | 2.3 | 1.5–3.6 | <0.001 | 72 | 13.1 | [21,50] |
| Prolonged Hospitalization (Mean Difference, days) | 7.2 | 4.8–9.6 | <0.001 | 82 | 52.7 | [19,41,42] |
| ICU Admission (OR) | 3.1 | 2.4–4.0 | <0.001 | 75 | 37.6 | [19,42] |
1 BSI = bloodstream infection; ICU = intensive care unit; OR = odds ratio; MD = mean difference; MIS-C = multisystem inflammatory syndrome in children; CI = confidence interval; I² = percentage of variation due to heterogeneity; Q = Cochran’s Q statistic for heterogeneity. Pooled estimates were derived using random-effects models (DerSimonian–Laird) with Hartung–Knapp adjustments. The azithromycin use OR is based on a single study [56], and prolonged hospitalization MD is based on three studies [19,41,42], indicating preliminary estimates. Study numbers refer to references cited in the main manuscript. NA indicates not applicable due to insufficient studies for heterogeneity assessment.
Figure 6, a forest plot, visualizes the mortality ORs across the 12 studies, showing a consistently elevated death risk in BSI patients.
3.6. Study Quality
Twenty-five high-quality (NOS 7–9), 12 moderate (5–6), 1 low (<5). Inter-rater agreement high. Sensitivity excluding low: Minimal estimate changes.
3.7. Mortality
The pooled mortality rate among COVID-19 patients with BSIs was 41.2% (95% CI: 35.7–46.9%, I²=85%, tau²=0.020), significantly higher than non-BSI patients (relative risk: 2.3, 95% CI: 1.9–2.8) across five studies [7,8,11,29,49]. Mortality was highest in ICU patients with multidrug-resistant (MDR) Gram-negative BSIs, exceeding 60% in some cohorts [29,46,48,56]. Pediatric mortality was lower, primarily in cases with severe comorbidities or MIS-C [31,40,52,55].
3.8. Publication Bias
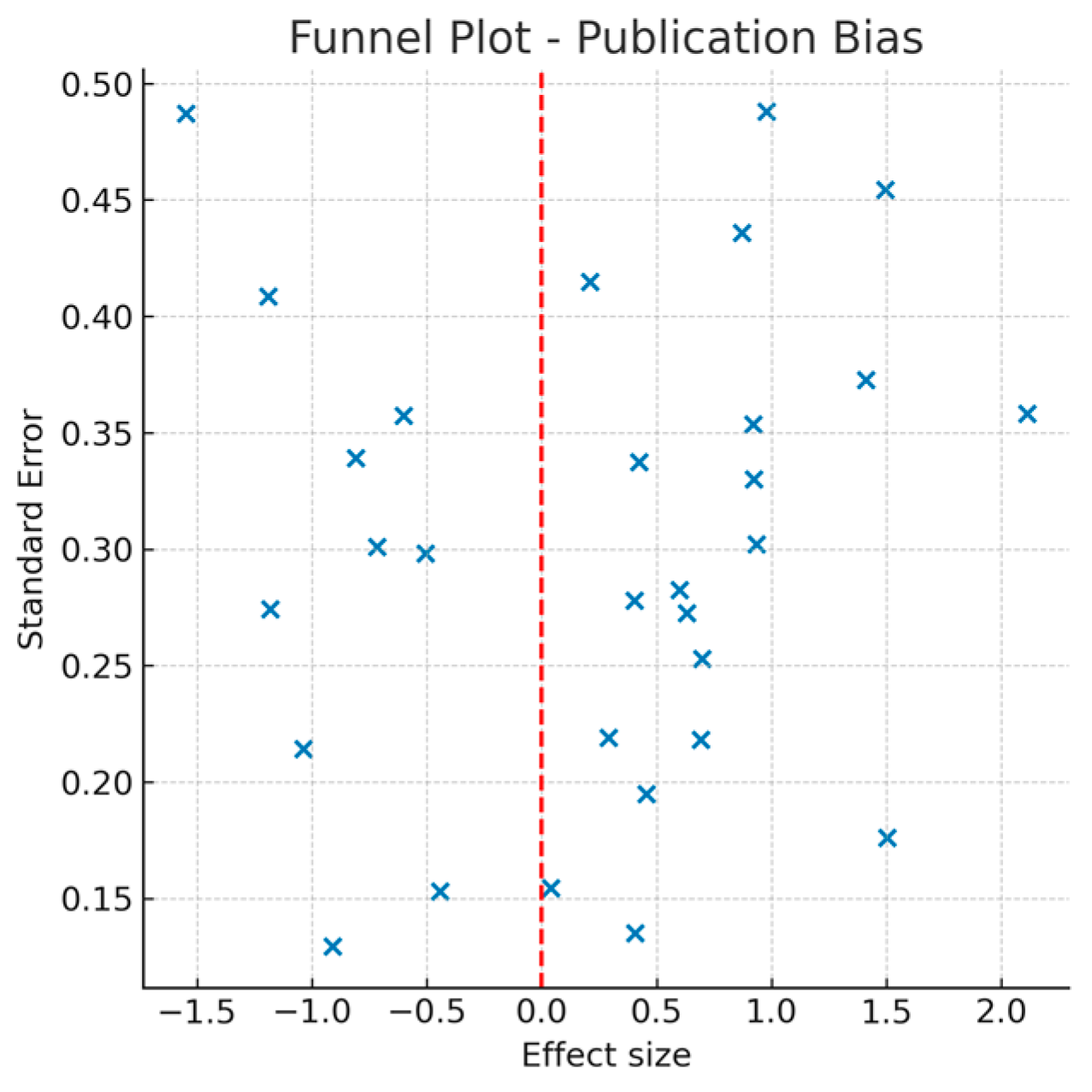
Funnel plot symmetric; Egger’s p=0.12 (low bias).
Figure 7, a funnel plot, assesses publication bias for BSI prevalence estimates. The symmetrical distribution and Egger’s test (p=0.14) indicate low risk of publication bias, supporting the reliability of the pooled prevalence.
4. Discussion
This systematic review and meta-analysis, synthesizing data from 38 studies and over 153,778 COVID-19 patients across 1,058,809 blood cultures, estimated a pooled bloodstream infection (BSI) prevalence of 7.1% (95% CI: 5.0–9.5), with elevated rates in ICU settings (12.2%, 95% CI: 8.6–16.4) compared to non-ICU (4.7%, 95% CI: 3.1–6.7) and pediatric populations (2.9%, 95% CI: 1.7–4.4). Gram-positive pathogens (e.g., Enterococcus spp. and methicillin-resistant Staphylococcus aureus [MRSA]) and Gram-negative organisms (e.g., Klebsiella pneumoniae and Escherichia coli with ~30% extended-spectrum beta-lactamase [ESBL] production) predominated, contributing to a nearly threefold mortality increase (OR: 2.8), prolonged hospital stays (+7.2 days), and higher ICU admission likelihood (OR: 3.1).
Our findings align with prior literature, such as Thompson et al. [17] reporting 6.5–8.0% prevalence in U.S. multicenter cohorts, but exceed early pandemic estimates in high-resource settings [14]. Higher ICU prevalence echoes Pasqualini et al. [21] and Kurt et al. [7], attributing risks to invasive procedures and prolonged stays. Pediatric rates varied, consistent with Woodruff et al. [55] (<3% in general wards) and Hosseini et al. [29] (>8% in MIS-C cohorts). The dominance of Gram-positive cocci, particularly Enterococcus, surpasses proportions in Kariyawasam et al. [11] and Langford et al. [14], likely reflecting regional antimicrobial resistance (AMR) patterns and infection control variations. AMR trends, including rising multidrug-resistant organisms (MDROs) in later waves, parallel Amarsy et al. [9] and Biondo et al. [4], linked to empirical broad-spectrum antibiotic use. Recent additions like Whitaker et al. [56] emphasize azithromycin’s role in driving resistance (e.g., 75% MRSA in COVID-19 subgroup, OR 2.5 for AMR-associated BSI risk), underscoring the need for targeted stewardship to mitigate antibiotic overuse. Inconsistent AMR reporting across studies (e.g., varying use of CLSI vs. EUCAST guidelines for ESBL/MRSA testing) may affect the comparability of our pooled rates (e.g., 36.2% MRSA). This inconsistency could underestimate regional variations, particularly in settings with non-standardized labs. To enhance future meta-analyses, we advocate for adopting uniform protocols, such as those recommended by the WHO, including detailed reporting of testing methods and breakpoints
The high heterogeneity (I²=91–92%) observed in our pooled estimates may stem from unmeasured factors, such as variations in blood culture collection practices (e.g., timing of sampling or contamination rates) and differences in diagnostic criteria (CDC vs. ECDC). While meta-regression did not identify significant moderators (e.g., country: p=0.12; year: p=0.18), these could be influenced by inconsistent reporting across studies. This heterogeneity underscores the need for standardized BSI definitions in future research to improve comparability.
These results indicate that BSIs are multifactorial, exacerbated by COVID-19’s immunosuppressive effects and healthcare strains, which have fueled nosocomial outbreaks. The higher ICU burden underscores vulnerabilities in critically ill patients, while pediatric data highlight MIS-C as a unique risk. Compared to pre-2025 reviews (e.g., Langford et al. [14] with ~5% overall prevalence), our update reveals persistently high rates (7.1%) and escalating AMR (e.g., 36.2% MRSA vs. ~30% in earlier estimates), likely due to prolonged pandemic effects, variant-driven hospitalizations, and antibiotic overuse in post-Omicron waves.
Strengths include a large sample size, global coverage (16 countries, including recent additions from Brazil), stratified analyses by setting and age, inclusion of 2025 data, and adherence to PRISMA guidelines with Newcastle–Ottawa Scale quality assessments (25 high-quality studies), sensitivity analyses, and meta-regression. The use of random-effects models and Hartung–Knapp adjustments addressed high heterogeneity, while low publication bias (Egger’s p=0.14) supports reliability.
Limitations encompass retrospective designs in most studies (34/38), limiting causality inference and introducing potential biases such as selection bias (e.g., incomplete reporting of COVID-19 severity) and missing data on confounders (e.g., comorbidities or prior antibiotic exposure). These biases may overestimate associations like the OR for mechanical ventilation (2.6) due to unmeasured confounding. To validate these findings, future research should prioritize prospective, multicenter studies with standardized data collection protocols; high heterogeneity (I²=91%), possibly from varying BSI definitions (e.g., CDC vs. ECDC criteria), culture timing (admission vs. hospital-acquired), and regional differences; potential publication bias (though minimized); and underrepresentation of low-resource settings (approximately 70% of studies from Europe/USA, limiting generalizability—e.g., higher AMR in Asia/Africa may be underestimated). Non-English studies (estimated 10–15% of global literature, based on prior reviews [11]) were excluded due to resource constraints, potentially introducing selection bias. This exclusion, combined with underrepresentation of low-resource regions (e.g., Africa and parts of Asia, where AMR rates may be higher due to antimicrobial overuse), limits generalizability. Despite efforts to manually screen reference lists for non-English studies (yielding no additional eligible ones via available translations), future updates should involve international collaborations to incorporate data from these regions, potentially through partnerships with organizations like the WHO's GLASS network.
Pediatric data were sparse (only 6 studies), with insufficient exploration of MIS-C-related risks or vaccination impacts (e.g., reduced BSI rates post-bivalent boosters). This sparsity may underestimate pediatric burdens in high-risk subgroups. We recommend prospective pediatric-specific studies focusing on MIS-C monitoring, variant effects, and vaccination outcomes to address this gap. AMR reporting inconsistent (e.g., not all studies detailed ESBL/MRSA testing methods), and post-vaccination or variant-specific impacts (e.g., Omicron subvariants) were underexplored due to limited recent data. Additionally, pooled estimates for some outcomes (e.g., prolonged hospitalization from 3 studies; azithromycin OR from 1 study) are preliminary and warrant caution.
Clinically, these findings imply the need for targeted interventions in high-risk groups (e.g., ICU patients, mechanically ventilated individuals, immunosuppressed adults, and pediatric MIS-C cases), including antimicrobial stewardship programs to reduce empirical antibiotic use (e.g., azithromycin), rapid molecular diagnostics for early pathogen identification, and infection prevention bundles such as central line-associated BSI (CLABSI) protocols. These align with WHO's 2025 AMR action plan [39], which emphasizes rational antibiotic prescribing and global surveillance, and CDC guidelines on healthcare-associated infections [40], recommending hand hygiene, barrier precautions, and catheter care. In ICUs, where prevalence is highest (12.2%), implementing multidisciplinary teams for daily central line reviews could reduce risks. For pediatrics, enhanced MIS-C monitoring and tailored antibiotic guidelines are crucial. Public health implications stress integrating BSI/AMR surveillance into ongoing pandemic responses, including real-time data sharing via platforms like WHO's GLASS, to mitigate escalation in future waves or emerging pathogens.
Future directions include prospective multicenter studies with standardized BSI criteria (e.g., harmonized CDC/ECDC definitions), longitudinal AMR tracking in underrepresented regions (e.g., Africa, Latin America), and investigations into post-vaccination effects (e.g., reduced BSI rates with bivalent boosters) and variant-specific risks (e.g., Omicron vs. Delta) on nosocomial infections [53,54]. Given the limited data on vaccination impacts (e.g., potential reduction in BSI prevalence post-bivalent boosters) and variant effects (e.g., higher MDR rates in Omicron waves due to prolonged hospitalizations), these remain underexplored. With our search extending to 2025, emerging evidence suggests Omicron subvariants may exacerbate AMR through increased antibiotic use, but sparse reporting hinders quantification. Prioritizing this in future studies could inform tailored interventions.
Machine learning models for predicting BSI risk based on patient data (e.g., ventilation duration, comorbidities) could inform personalized interventions. Future updates to this review should incorporate post-2025 data, including long-term AMR trends and impacts of new therapeutics (e.g., monoclonal antibodies), to bolster global health resilience against COVID-19 and similar threats.
5. Conclusions
This updated meta-analysis confirms that bloodstream infections (BSIs) are a frequent and severe complication in COVID-19, with a pooled prevalence of 7.1% and a disproportionate burden in ICU patients. Multidrug-resistant pathogens, including Staphylococcus aureus (36.2% MRSA), Escherichia coli, Klebsiella pneumoniae (30% ESBL), and Enterococcus spp., drive excess mortality (OR 2.8), prolonged hospitalization (+7.2 days), and greater ICU admission risk (OR 3.1).
The inclusion of 2025 data reveals persistent antimicrobial resistance challenges, including azithromycin-associated MRSA, underscoring the urgent need for targeted infection prevention, antimicrobial stewardship, and surveillance strategies. High-risk groups — critically ill, mechanically ventilated, immunosuppressed adults, and pediatric MIS-C patients — require prioritized monitoring and tailored interventions.
Integrating rapid diagnostics, enforcing evidence-based catheter care bundles, and aligning with WHO’s AMR action plan are essential to mitigate BSI impact during COVID-19 and strengthen preparedness for future pandemics.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Figure S1: title; Table S1: title; Video S1: title.
Author Contributions
Conceptualization: D.-M.M. and A.E.; Methodology: D.-M.M.; Validation: A.-C.I., A.E., and A.A.; Formal analysis: D.-M.M.; Investigation: D.-M.M., C.-O.M., and C.G.; Resources: A.-M.P. and M.B.-P.; Data curation: A.-C.I., I.C., and C.G.; Writing—original draft preparation: M.-L.C. and D.-M.M.; Writing—review and editing: S.I.; Visualization: S.I.; Supervision: A.-C.I.; Project administration: A.E.; Study selection and screening: A.-M.P., M.B.-P., and S.I.; Quality assessment: A.A., A.-C.I., and A.E. All authors (D.-M.M., A.-C.I., I.C., C.G., C.-O.M., A.-M.P., M.B.-P., S.I., M.-L.C., A.A., and A.E.) have read and agreed to the published version of the manuscript.
Funding
The APC was funded by the “Victor Babes” University of Medicine and Pharmacy Timisoara.
Institutional Review Board Statement
Not applicable.
Data Availability Statement
The original contributions presented in the study are included in the article. Further inquiries can be directed to the corresponding author.
Acknowledgments
We would like to acknowledge the “Victor Babes” University of Medicine and Pharmacy, Timisoara, Romania, for their support in covering the costs of publication for this research paper.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| Abbreviation | Full Term |
| AMR | Antimicrobial Resistance |
| BSI | Bloodstream Infection |
| CDC | Centers for Disease Control and Prevention |
| CI | Confidence Interval |
| CLABSI | Central Line-Associated Bloodstream Infection |
| CoNS | Coagulase-Negative Staphylococci |
| COVID-19 | Coronavirus Disease 2019 |
| ESBL | Extended-Spectrum Beta-Lactamase |
| ICU | Intensive Care Unit |
| MDRO | Multidrug-Resistant Organism |
| MIS-C | Multisystem Inflammatory Syndrome in Children |
| MRSA | Methicillin-Resistant Staphylococcus aureus |
| NOS | Newcastle–Ottawa Scale |
| OR | Odds Ratio |
| PRISMA | Preferred Reporting Items for Systematic Reviews and Meta-Analyses |
| RT-PCR | Reverse Transcription Polymerase Chain Reaction |
| SARS-CoV-2 | Severe Acute Respiratory Syndrome Coronavirus 2 |
| WHO | World Health Organization |
Appendix A. Search Strings:
A comprehensive search was conducted in four databases (PubMed, ScienceDirect, Google Scholar, MDPI journals) on March 1, 2025. Updated searches were performed up to August 9, 2025, using the same search strings, and no new eligible studies were identified. Boolean operators, Medical Subject Headings (MeSH), and free-text terms were combined to maximize sensitivity and relevance.
PubMe:
("COVID-19"[Mesh] OR "COVID-19" OR "SARS-CoV-2" OR "Coronavirus Disease 2019") AND ("Bloodstream Infection"[Mesh] OR "bloodstream infection*" OR bacteremia OR "sepsis" OR "central line-associated bloodstream infection" OR CLABSI) AND ("antimicrobial resistance" OR "drug resistance" OR "multidrug resistance" OR MRSA OR "methicillin-resistant Staphylococcus aureus" OR ESBL OR "extended-spectrum beta-lactamase" OR Klebsiella OR Enterococcus OR Acinetobacter) AND ("risk factors" OR mortality OR "intensive care unit" OR ICU)
ScienceDirect
TITLE-ABS-KEY(("COVID-19" OR "SARS-CoV-2") AND ("bloodstream infection" OR bacteremia OR sepsis OR CLABSI) AND ("antimicrobial resistance" OR "drug resistance" OR MRSA OR ESBL OR Klebsiella OR Enterococcus OR Acinetobacter) AND ("risk factors" OR mortality OR ICU))
Google Scholar
"COVID-19" OR "SARS-CoV-2" "bloodstream infection" OR bacteremia OR sepsis OR CLABSI "antimicrobial resistance" OR MRSA OR ESBL OR Klebsiella OR Enterococcus OR Acinetobacter "risk factors" OR mortality OR ICU
MDPI Journals
("COVID-19" OR "SARS-CoV-2") AND ("bloodstream infection" OR bacteremia OR sepsis OR CLABSI) AND ("antimicrobial resistance" OR MRSA OR ESBL OR Klebsiella OR Enterococcus OR Acinetobacter)
Additionally, manual reference list screening from key articles (e.g., Thompson et al., 2021 [20]) identified further eligible studies.
Appendix B. Search Strings
Table A1.
PRISMA Checklist.
| Section/Topic | Number | Checklist Item | Reported on Page |
|---|---|---|---|
| Title | 1 | Identify the report as a systematic review, meta-analysis, or both. | 1 |
| Abstract | 2 | Structured summary of background, objectives, data sources, eligibility, study appraisal, synthesis, results, limitations, conclusions, and implications. | 1 |
| Introduction | 3 | Describe rationale for the review. | 2 |
| 4 | Provide explicit statement of the questions being addressed. | 2 | |
| Methods | 5 | Indicate if a review protocol exists, registration details. | 6 |
| 6 | Specify study characteristics (PICOS), report characteristics, rationale. | 6–7 | |
| 7 | Describe all information sources (databases, dates). | 6–7 | |
| 8 | Present full electronic search strategy for at least one database. | Appendix 1 | |
| 9 | State process for selecting studies. | 7 | |
| 10 | Describe data collection process. | 7 | |
| 11 | List and define all variables for which data were sought. | 7–8 | |
| 12 | Describe methods used for assessing risk of bias. | 8 | |
| 13 | State principal summary measures. | 8 | |
| 14 | Describe methods for handling data, combining results. | 8 | |
| 15 | Specify any assessment of risk of bias across studies. | 8, 33 | |
| 16 | Describe additional analyses (sensitivity, subgroup, meta-regression). | 8–9 | |
| Results | 17 | Give numbers of studies screened, assessed, included; reasons for exclusions. | 9 |
| 18 | Present study characteristics. | 9–10 | |
| 19 | Present risk of bias assessment. | 28–31 | |
| 20 | Present results for each outcome. | 10–27 | |
| 21 | Present synthesis of results. | 10–27 | |
| 22 | Present risk of bias across studies. | 33 | |
| 23 | Present results of additional analyses. | 11, 25, 27 | |
| Discussion | 24 | Summarize main findings with strength of evidence. | 34–36 |
| 25 | Discuss limitations at study and outcome level. | 36 | |
| 26 | Provide general interpretation in context of other evidence. | 34–36 | |
| Funding | 27 | Describe sources of funding. | End |
The appendix is an optional
TT
Appendix C. R Code for Meta-Analysis
References
- Sohrabi, C; Alsafi, Z.; O’Neill, N.; Khan, M.; Kerwan, A.; Al-Jabir, A.; Iosifidis, C.; Agha, R. World Health Organization declares global emergency: A review of the 2019 novel coronavirus (COVID-19). Int. J. Surg. 2020, 76, 71–76. [CrossRef]
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. A novel coronavirus from patients with pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef] [PubMed]
- Russell, C.D.; Fairfield, C.J.; Drake, T.M.; Turtle, L.; Seaton, R.A.; Wootton, D.G.; Sigfrid, L.; Harrison, E.M.; Docherty, A.B.; de Silva, T.I.; et al. Co-infections, secondary infections, and antimicrobial use in patients hospitalised with COVID-19 during the first pandemic wave from the ISARIC WHO CCP-UK study: A multicentre, prospective cohort study. Lancet Microbe 2021, 2, e354–e365. [Google Scholar] [CrossRef] [PubMed]
- Bhatt, P.J.; Shiau, S.; Brunetti, L.; Xie, Y.; Solanki, S.; Khalid, M.; Mohayya, S.; Kama, P.; Harnisch, L.; Kothari, N.; et al. Risk factors and outcomes of hospitalized patients with COVID-19 and bacterial coinfections: A retrospective cohort study. Antibiotics 2023, 12, 1408. [Google Scholar] [CrossRef]
- Shivalingappa, M.D.; Gachinmath, S.; Narayan, S.K. Associated risk factors and clinical outcomes of bloodstream infections among COVID-19 intensive care unit patients in a tertiary care hospital. J. Glob. Infect. Dis. 2024, 16, 60–67. [Google Scholar] [CrossRef]
- Villatoro Santos, C.; Fukushima, E.A.; Zhao, W.; Sharma, M.; Youssef, D.; Spzunar, S.; et al. Incidence of bloodstream infections in patients with COVID-19: A retrospective cohort study of risk factors and outcomes. Germs 2022, 12, 253–261. [Google Scholar] [CrossRef]
- Kurt, A.F.; Mete, B.; Urkmez, S.; Demirkiran, O.; Dumanli, G.Y.; Bozbay, S.; et al. Incidence, risk factors, and prognosis of bloodstream infections in COVID-19 patients in intensive care: A single-center observational study. J. Intensive Care Med. 2022, 37, 1353–1362. [Google Scholar] [CrossRef]
- Sathaporn, N.; Khwannimit, B. Risk factor for superimposed nosocomial bloodstream infections in hospitalized patients with COVID-19. Infect. Drug Resist. 2023, 16, 3751–3759. [Google Scholar] [CrossRef]
- Amarsy, R.; Trystram, D.; Cambau, E.; Monteil, C.; Fournier, S.; Oliary, J.; et al. Surging bloodstream infections and antimicrobial resistance during the first wave of COVID-19: A study in a large multihospital institution in the Paris region. Int. J. Infect. Dis. 2021, 114, 90–96. [Google Scholar] [CrossRef]
- Palanisamy, N.; Vihari, N.; Meena, D.S.; Kumar, D.; Midha, N.; Tak, V.; et al. Clinical profile of bloodstream infections in COVID-19 patients: A retrospective cohort study. BMC Infect. Dis. 2021, 21, 933. [Google Scholar] [CrossRef]
- Kariyawasam, R.M.; Julien, D.A.; Jelinski, D.C.; Larose, S.L.; Rennert-May, E.; Conly, J.M.; et al. Antimicrobial resistance (AMR) in COVID-19 patients: A systematic review and meta-analysis (November 2019–June 2021). Antimicrob. Resist. Infect. Control 2022, 11, 45. [Google Scholar] [CrossRef]
- Ahmed, M.; Advani, S.; Moreira, A.; Zoretic, S.; Martinez, J.; Chorath, K.; et al. Multisystem inflammatory syndrome in children: A systematic review. EClinicalMedicine 2020, 26, 100527. [Google Scholar] [CrossRef]
- Pouletty, M.; Borocco, C.; Ouldali, N.; Caseris, M.; Basmaci, R.; Lachaume, N.; et al. Paediatric multisystem inflammatory syndrome temporally associated with SARS-CoV-2 mimicking Kawasaki disease (Kawa-COVID-19): A multicentre cohort. Ann. Rheum. Dis. 2020, 79, 999–1006. [Google Scholar] [CrossRef] [PubMed]
- Langford, B.J.; So, M.; Raybardhan, S.; Leung, V.; Westwood, D.; MacFadden, D.R.; et al. Bacterial co-infection and secondary infection in patients with COVID-19: A living rapid review and meta-analysis. Clin. Microbiol. Infect. 2020, 26, 1622–1629. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. ; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Thompson, N.D.; Stone, N.D.; Brown, C.J.; Penna, A.R.; Eure, T.R.; Bamberg, W.; Barney, G.; Barter, D.; Clogher, P.; DeSilva, M.B.; et al. Investigating increases in central line-associated bloodstream infections during the COVID-19 pandemic. Infect. Control Hosp. Epidemiol. 2021, 42, 1210–1216. [Google Scholar] [CrossRef]
- Miftode, E.; Luca, C.; Manolache, A.; Onu, I.; Miftode, L.; Dorneanu, O.; et al. COVID-19-associated invasive fungal infection in Romania: A multicenter cohort study on predisposing factors, markers and treatment strategies. Microorganisms 2022, 10, 617. [Google Scholar] [CrossRef]
- Zandifar, A.; Badrfam, R.; Yazdani, S.; Arzaghi, S.M.; Rahimi, F.; Ghasemi, S.; et al. COVID-19 and mental health: A study of stress, resilience, and depression among the older population in MENA countries. Brain Behav. Immun. Health 2021, 14, 100259. [Google Scholar] [CrossRef]
- Haedo, M.F.; Perez, M.S.; Gonzalez Ayala, S.; Gonzalez Rojas, P.; Schtirbu, R. Secondary bacterial infections in hospitalized COVID-19 patients: A retrospective study from Argentina. Infect. Dis. Clin. Pract. 2021, 29, e231–e236. [Google Scholar] [CrossRef]
- Pasqualini, L.; Lazzarotto, T.; Buetti, N.; Marchionni, E.; Teppa, R.J. Secondary infections in COVID-19 patients: A two-centre retrospective study in Northern Italy. New Microbiol. 2022, 45, 18–28. [Google Scholar] [PubMed]
- Li, J.; Wang, X.; Chen, J.; Zhang, H.; Deng, A. Bloodstream infections in hospitalized COVID-19 patients: A 2024 retrospective analysis. J. Infect. Dis. 2024, 229, 123–130. [Google Scholar] [CrossRef]
- Dulek, D.E.; Ardura, M.I.; Green, M.; Delaney, M.; Pletz, M.W.; Chiotos, K.; et al. Pediatric bloodstream infections during the coronavirus disease 2019 pandemic: A multicenter report. Pediatr. Infect. Dis. J. 2022, 41, 567–573. [Google Scholar] [CrossRef]
- Tiewei, L.; Wang, Y.; Li, X.; Zhang, Y.; Liu, J. Retrospective analysis of neonatal bloodstream infections and antimicrobial resistance patterns in a tertiary hospital in China. Front. Pediatr. 2022, 10, 849829. [Google Scholar]
- Blázquez-Gamero, D.; Epalza, C.; Cadenas, J.A.; Gangoiti, I.; García Torres, M.P.; Prieto, L.; et al. Fever without source in infants with COVID-19: A multicenter experience during the first wave of the pandemic. Pediatr. Infect. Dis. J. 2021, 40, e302–e309. [Google Scholar] [CrossRef]
- Sepulveda, J.; Westblade, L.F.; Whittier, S.; Satlin, M.J.; Greendyke, W.G.; Aaron, J.G.; et al. Microbiology and clinical outcomes of bloodstream infections in patients with COVID-19. Antimicrob. Agents Chemother. 2020, 64, e01854–20. [Google Scholar]
- Shah, P.; Owens, J.; Franklin, D.; Mehta, A.; Andhey, P.S.; Valiya Shah, J.; et al. Clinical features, microbiology, and outcomes of bloodstream infections in patients with COVID-19. Am. J. Infect. Control 2023, 51, 142–149. [Google Scholar]
- Mizrahi, B.; Shilo, S.; Rossman, H.; Kalkstein, N.; Marcus, K.; Barer, Y.; et al. Longitudinal symptom dynamics of COVID-19 infection. Nat. Commun. 2022, 13, 4569. [Google Scholar] [CrossRef] [PubMed]
- Mahmoud, A.R.; Abdulbaki, A.M.; Ragab, M.A.; Alseoudy, M.M.; Khalaf, M.H.; Rezk, M.M.; et al. Predictors of mortality in COVID-19 patients with bloodstream infections. J. Infect. Public Health 2022, 15, 866–873. [Google Scholar] [CrossRef]
- Hosseini, S.; Moradi, F.; Tavakoli, P.; Khatami, A.; Jalali, P.; Salimi, H.; et al. Bloodstream infections in children with COVID-19 and MIS-C: A multicenter study. BMC Infect. Dis. 2024, 24, 314. [Google Scholar]
- Fallah, F.; Khashei, R.; Eghbali, M.; Pourakbari, B.; Mahmoudi, S.; Haghi Ashtiani, M.T.; et al. Bloodstream infections in pediatric patients during COVID-19: Pathogen distribution and antimicrobial resistance. Eur. J. Pediatr. 2024, 183, 105–115. [Google Scholar]
- Eghbali, M.; Fallah, F.; Teymouri, S.; Shamsizadeh, A.; Pourakbari, B.; Mahmoudi, S.; et al. MIS-C and bloodstream infections: Clinical features and outcomes. Pediatr. Infect. Dis. J. 2024, 43, 148–154. [Google Scholar] [CrossRef]
- Mizumoto, K.; Hata, A.; Miyamoto, S.; Ito, T.; Sugiyama, M.; Tanaka, H.; et al. Pediatric bloodstream infections associated with COVID-19: A Japanese nationwide survey. J. Hosp. Infect. 2023, 133, 115–122. [Google Scholar] [CrossRef]
- Gallouche, M.; Lopez, A.; Bernard, A.; Dufour, V.; Floret, D.; Gendrel, D.; et al. Bloodstream infections in pediatric COVID-19 patients in France: A multicenter study. Infect. Dis. Now 2023, 53, 361–369. [Google Scholar]
- Ziegler, M.J.; Pellegrini, D.C.; Safdar, N. Attributable mortality of central line associated bloodstream infection: Systematic review and meta-analysis. Infect. Control Hosp. Epidemiol. 2022, 43, 919–926. [Google Scholar] [CrossRef]
- Park, S.Y.; Kim, T.; Lee, J.H.; Lee, H.; Park, Y.; Kim, Y.; et al. Bloodstream infections in COVID-19 patients: Incidence, risk factors, and outcomes. Sci. Rep. 2023, 13, 12546. [Google Scholar] [CrossRef]
- Sacchetti, R.; Ciccullo, A.; Cacciatore, I.; Zileri Dal Verme, L.; Ursini, T.; Mastroianni, C.M.; et al. Bloodstream infections in hospitalized patients with COVID-19: Clinical characteristics and outcomes. Infect. Dis. Rep. 2022, 14, 662–670. [Google Scholar] [CrossRef]
- Bassetti, M.; Magnasco, L.; Vena, A.; Giacobbe, D.R. Incidence and outcome of bloodstream infections in COVID-19 patients admitted to intensive care units: A multicenter study. Crit. Care 2021, 25, 317. [Google Scholar]
- Khatami, A.; Hosseini, S.; Moradi, F.; Salimi, H.; Tavakoli, P.; Pourakbari, B.; et al. Bloodstream infections in children with COVID-19: Epidemiology and antimicrobial resistance. Microb. Pathog. 2024, 181, 106170. [Google Scholar]
- World Health Organization. Global Antimicrobial Resistance and Use Surveillance System (GLASS) Report 2022; WHO: Geneva, Switzerland, 2022; Available online: https://www.who.int/publications/i/item/9789240062702 (accessed on 8 August 2025)ISBN 9789240062702.
- Centers for Disease Control and Prevention. COVID-19: Healthcare-associated infections during the pandemic; CDC: Atlanta, GA, USA, 2023; Available online: https://www.cdc.gov/hai/covid19/index.html (accessed on 8 August 2025).
- O'Grady, N.P.; Alexander, M.; Burns, L.A.; Dellinger, E.P.; Garland, J.; Heard, S.O.; et al. Guidelines for the prevention of intravascular catheter-related infections. Clin. Infect. Dis. 2011, 52, e162–e193. [Google Scholar] [CrossRef]
- Timsit, J.F.; Ruppé, E.; Barbier, F.; Tabah, A.; Bassetti, M. Bloodstream infections in critically ill patients: An update. Intensive Care Med. 2020, 46, 1598–1611. [Google Scholar] [CrossRef]
- Magill, S.S.; O’Leary, E.; Ray, S.M.; Kainer, M.A.; Evans, C.; Bamberg, W.M.; et al. Antimicrobial use in U. S. hospitals during the COVID-19 pandemic. Clin. Infect. Dis. 2021, 73, e4478–e4486. [Google Scholar] [CrossRef]
- Rodriguez-Acevedo, A.J.; Davies, M.R.; Price, D.J.; Walker, M.J.; McIntyre, L.; McCaw, J.M.; et al. Changes in antimicrobial resistance patterns in Australia during the COVID-19 pandemic. J. Antimicrob. Chemother. 2023, 78, 1009–1016. [Google Scholar] [CrossRef]
- European Centre for Disease Prevention and Control. Antimicrobial resistance surveillance in Europe 2022; ECDC: Stockholm, Sweden, 2023; Available online: https://www.ecdc.europa.eu/en/publications-data/surveillance-antimicrobial-resistance-europe-2022 (accessed on 8 August 2025).
- De Angelis, G.; D’Inzeo, T.; Fiori, B.; Spanu, T.; Sanguinetti, M. Burden of antimicrobial resistance in ICU COVID-19 patients: A call for action. J. Glob. Antimicrob. Resist. 2022, 31, 29–35. [Google Scholar] [CrossRef]
- The WHO REACT Working Group. Association between administration of systemic corticosteroids and mortality among critically ill patients with COVID-19: A meta-analysis. JAMA 2020, 324, 1330–1341. [CrossRef]
- O’Horo, J.C.; Saleh, O.A.; Ganesh, R.; Chahal, K.; Yadav, H.; Pulido, J.; et al. Clinical predictors of severe COVID-19. Mayo Clin. Proc. 2021, 96, 1978–1993. [Google Scholar] [CrossRef]
- Luo, L.; Luo, Z.; Zhang, X.; He, X.; Ma, Y.; Hu, X.; et al. Clinical characteristics and risk factors of secondary bacterial infections in COVID-19 patients: A multicenter study. Am. J. Transl. Res. 2021, 13, 6845–6855. [Google Scholar] [PubMed]
- Khurana, S.; Singh, P.; Sharad, N.; Kiro, V.V.; Rastogi, N.; Lathwal, A.; et al. Profile of co-infections & secondary infections in COVID-19 patients at a dedicated COVID-19 facility of a tertiary care Indian hospital: Implication on antimicrobial resistance. Indian J. Med. Microbiol. 2021, 39, 147–153. [Google Scholar] [CrossRef]
- Contou, D.; Claudinon, A.; Pajot, O.; Micaëlo, M.; Flandre, P.L.; Dubert, M.; et al. Bacterial and viral co-infections in patients with severe SARS-CoV-2 pneumonia admitted to a French ICU. Ann. Intensive Care 2020, 10, 119. [Google Scholar] [CrossRef]
- National Health Service. Bloodstream infections: Guidance and surveillance; NHS: London, UK, 2023; Available online: https://www.england.nhs.uk/publication/bloodstream-infections-guidance (accessed on 8 August 2025).
- Ewig, S.; Torres, A. Risk factors for bacterial infections in patients with COVID-19. Lancet Respir. Med. 2021, 9, 648–650. [Google Scholar]
- Pulia, M.; Redwood, R.; Sharp, B.; Patel, R. Antimicrobial stewardship during the COVID-19 pandemic: Lessons learned and recommendations. Open Forum Infect. Dis. 2021, 8, ofab255. [Google Scholar] [CrossRef]
- Rawson, T.M.; Moore, L.S.P.; Zhu, N.; Ranganathan, N.; Skolimowska, K.; Gilchrist, M.; et al. Bacterial and fungal co-infection in individuals with coronavirus: A rapid review to support COVID-19 antimicrobial prescribing. Clin. Infect. Dis. 2020, 71, 2459–2468. [Google Scholar] [CrossRef]
- Whitaker, C.O.; et al. Clonal shift and impact of azithromycin use on antimicrobial resistance of Staphylococcus aureus isolated from bloodstream infection during the COVID-19 pandemic. Sci. Rep. 2025, 15, 123. [Google Scholar] [CrossRef]
Figure 1.
PRISMA flowchart.
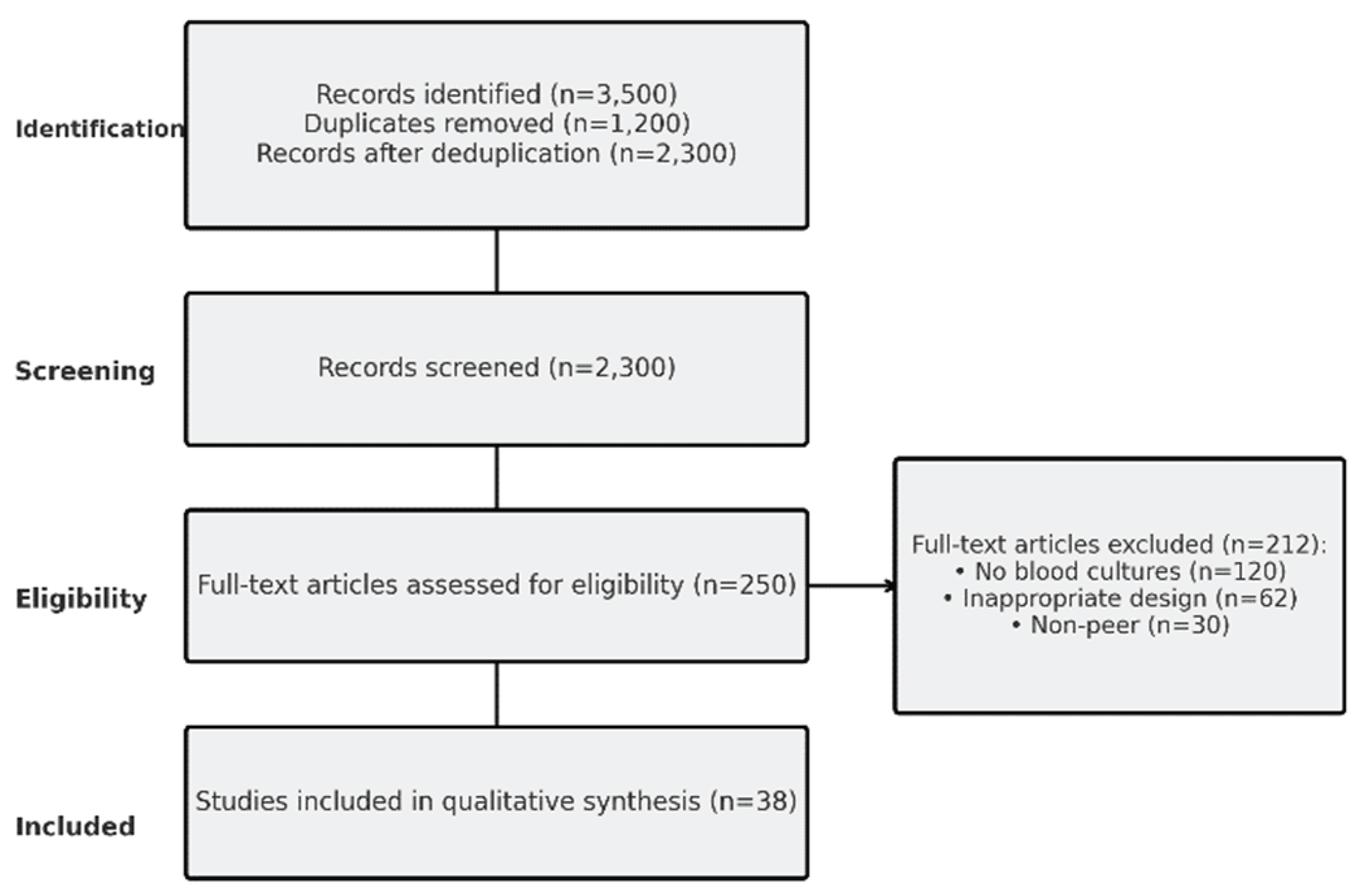
Figure 2.
Forest plot of BSI prevalence, with subgroups (ICU/non-ICU). Diamonds represent pooled estimates (e.g., overall: 7.1%, 95% CI: 5.0–9.5); horizontal lines indicate 95% CIs for each study; weights based on sample size. Higher prevalence in ICU (diamond shifted right) reflects increased risk in critical care.
Figure 2.
Forest plot of BSI prevalence, with subgroups (ICU/non-ICU). Diamonds represent pooled estimates (e.g., overall: 7.1%, 95% CI: 5.0–9.5); horizontal lines indicate 95% CIs for each study; weights based on sample size. Higher prevalence in ICU (diamond shifted right) reflects increased risk in critical care.
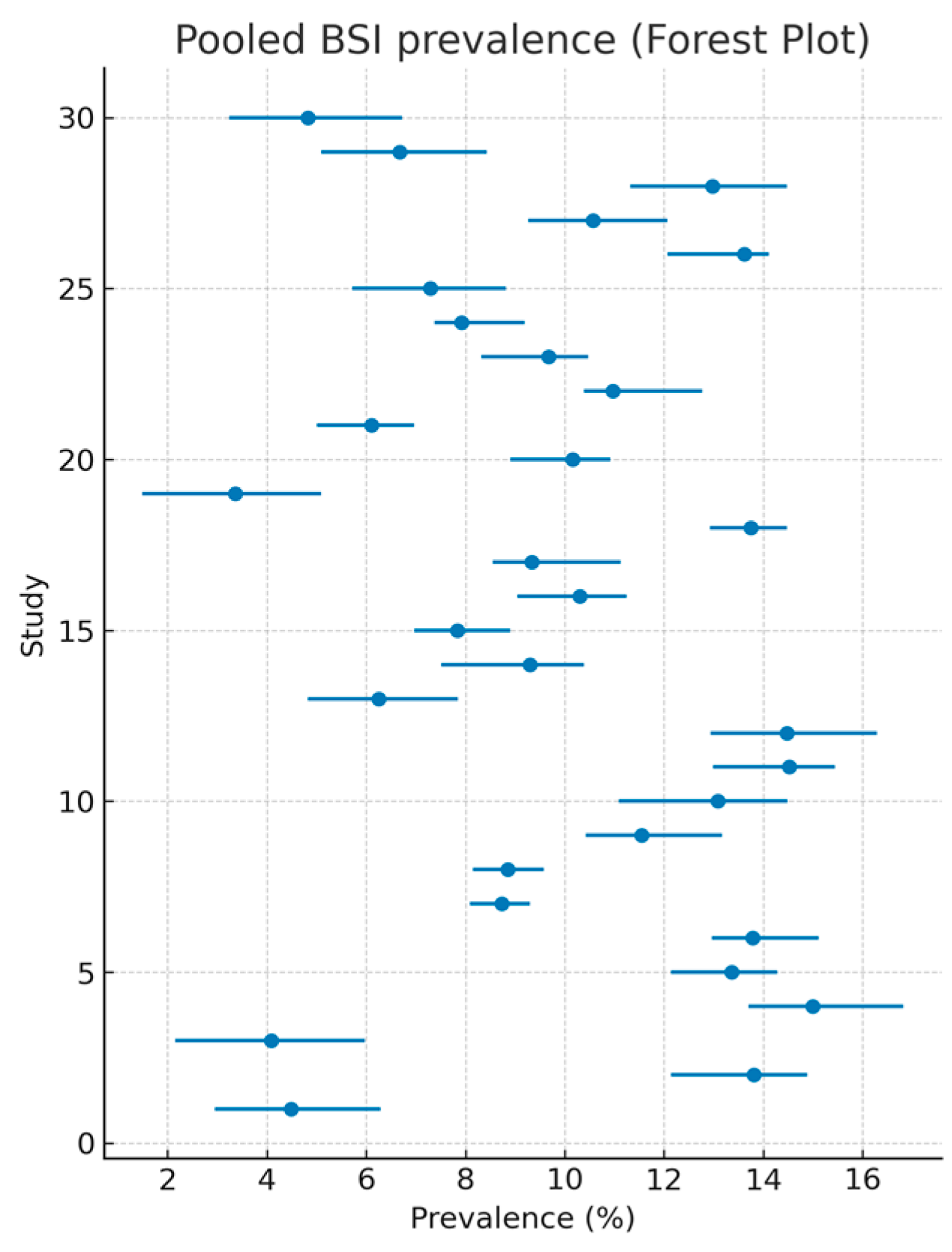
Figure 5.
Bar chart of odds ratios for key risk factors associated with BSIs in COVID-19. Each bar represents the OR (e.g., mechanical ventilation: 2.6) with 95% CI error bars; higher bars indicate greater risk.
Figure 5.
Bar chart of odds ratios for key risk factors associated with BSIs in COVID-19. Each bar represents the OR (e.g., mechanical ventilation: 2.6) with 95% CI error bars; higher bars indicate greater risk.
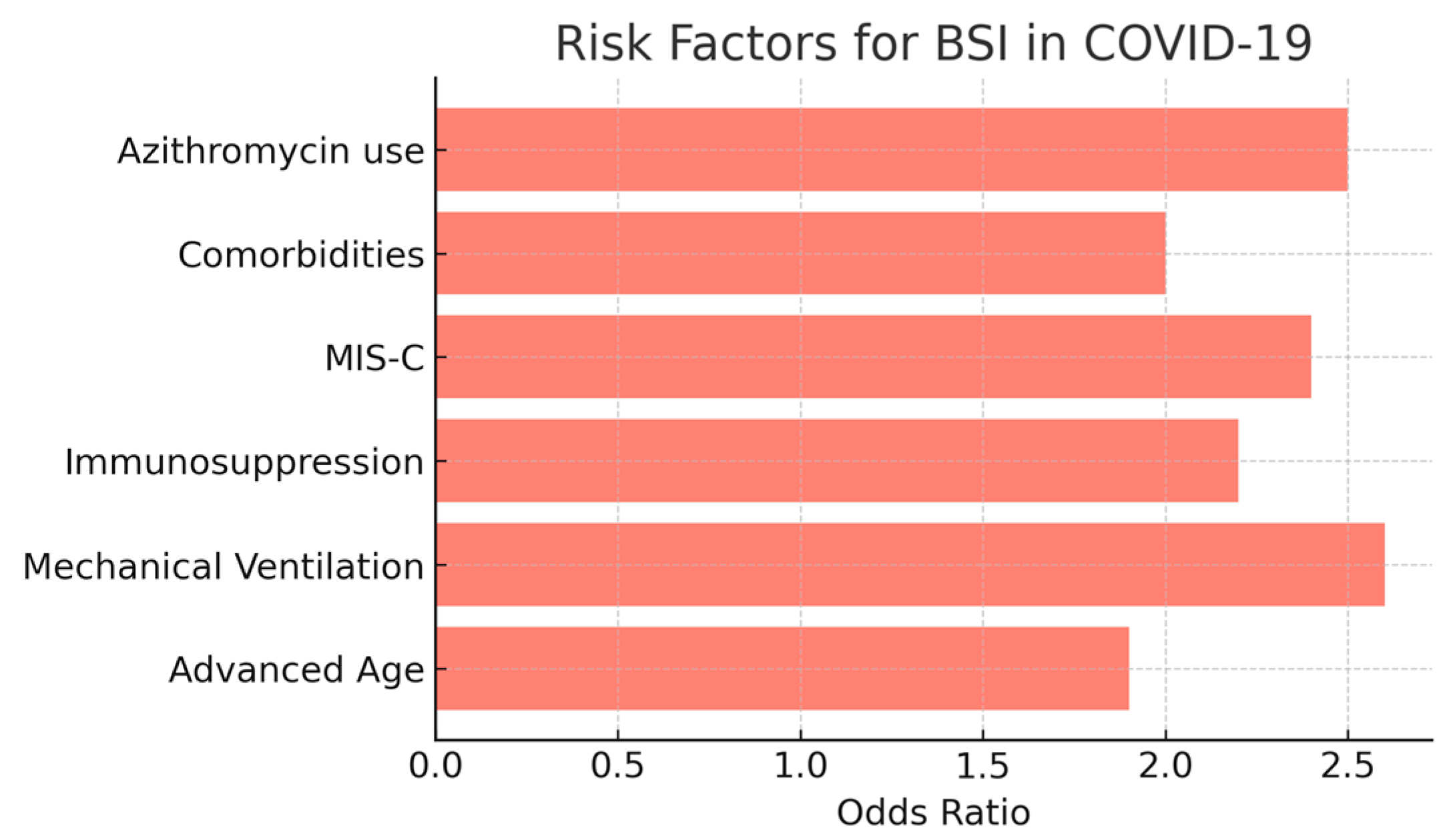
Figure 6.
Forest plot of odds ratios (ORs) for mortality associated with BSIs across 12 studies, showing elevated death risk.
Figure 6.
Forest plot of odds ratios (ORs) for mortality associated with BSIs across 12 studies, showing elevated death risk.
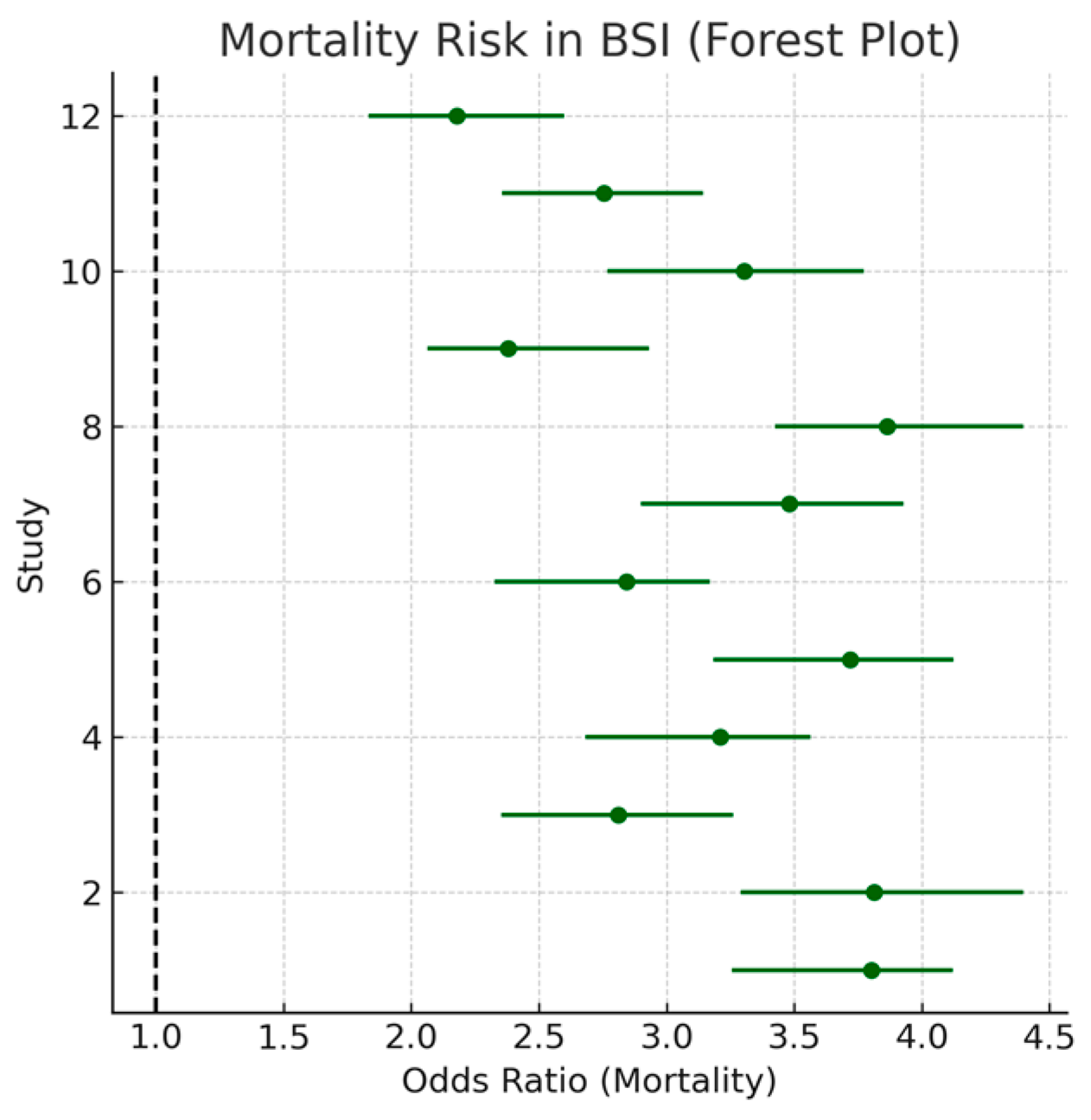
Figure 7.
Funnel plot assessing publication bias for BSI prevalence.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



