Submitted:
09 August 2025
Posted:
11 August 2025
You are already at the latest version
Abstract
Objectives: Prostate cancer (PCa) is the most common malignancy in men, with variable presentation, clinical findings and natural progres-sion. The expanding field of cancer neurobiology has highlighted peri-neural invasion, perineural tumour spread, and malignant spinal cord compression as features of interest in PCa. This study explored the in-teraction between PCa and the peripheral and central nervous systems and whether prostate cancer interacts with the central via the periph-eral nervous system. Methods: Cross-sectional study. Adult men presenting with suspected PCa to a tertiary academic hos-pital in Pretoria were recruited. Patients with PCa confirmed via his-tology were subjected to magnetic resonance imaging or neurography, which was performed between February 2022 and October 2023. His-tological and radiological data were collected for descriptive and uni-variate analyses at the 5% significance level. Magnetic resonance neu-rography (MRN) of patients with biopsy-proven PCa, which is investi-gational for the indication of assessing direct nerve infiltration by PCa. Magnetic resonance imaging (MRI) of patients with clinical suspicion of spinal cord compression (SCC) which is standard of care regardless of the possible cause. Results: Main outcome measures- Radiological evidence of perineural tumour spread. Almost half (48.3%) of the 58 men enrolled had perineural invasion on histology. Perineural tumour spread on MRI was evident in 65.8% (n = 32) of the patients. Eight pa-tients presented with spinal cord compression caused by PCa in six pa-tients and disc herniation in two patients. Soft tissue and skeletal me-tastases were present in 51.2% and 34.5% of patients, respectively. Conclusion: MRI imaging demonstrates clear interaction of PCa with the nervous system. This neurogenous route of tumour dissemination represents a novel additional mechanism by which PCa may cause neurological complications in the regions supplied by the lumbosacral plexuses and spinal cord, including neuropathic pain. Future studies incorporating MRI with positron emission tomography/computed to-mography may better illustrate nerve involvement.
Keywords:
prostate cancer
; magnetic resonance imaging
; magnetic resonance neurography
; perineural tumour spread
; perineural invasion
; spinal cord compression
1. Introduction
Prostate cancer (PCa) is the most common cancer in men [1] and the fifth leading cause of death, accounting for 7.1% of cancers in men worldwide [2]. A devastating consequence of advanced PCa is spinal cord compression (SCC), which causes paraplegia, erectile dysfunction, and urinary and faecal incontinence [3,4]. SCC occurs in 15–20% of patients with bone metastases [5] and in 7% of men who die from PCa [6].
Historically, four mechanisms of tumour metastases are recognised; contiguous, haematogenous, lymphogenous and transcoelomic spread [7]. In PCa-related SCC, the accepted mechanism is haematogenous metastasis to the lumbosacral vertebrae via Batson’s valveless venous plexus, followed by mass enlargement and extradural SCC [5,8,9]. However, the potential role of nerves in cancer dissemination is an emerging area of research. We propose that the dissemination of malignant cells via direct invasion into nerves, perineural invasion and propagation in the form of perineural tumour spread constitute neurogenous metastasis. Neurogenous, in keeping with the existing nomenclature of metastases as described above.
SCC can precede or follow PCa diagnosis. Patients typically present with gait disturbances and incontinence. Timely intervention, including corticosteroids, anti-androgens (if PCa is known), spinal imaging, and spinal radiation, may preserve function. Treatment delays often lead to irreversible damage. Magnetic resonance imaging (MRI) is the imaging modality of choice for suspected SCC [7,10]. The hypothesis that PCa may reach the spinal cord directly via an intradural route through the pelvic plexus is of growing interest.
The prostatic nerve plexus, a continuation of the inferior hypogastric plexus, contains sympathetic and parasympathetic fibres and originates from the sacral nerve roots (S2–S4), supplying both sides of the prostate. The pudendal and dorsal penile nerves, which control continence and sexual function, also arise from S2–S4. Motor and sensory control of the lower limbs is mediated by the sciatic (L4–S3) and femoral (L2–L4) nerves.
Early studies have established the prognostic importance of perineural invasion (PNI) in PCa, linking it to adverse pathology [11], biochemical recurrence [12], soft tissue progression [13], and poor outcomes [14]. The definition of PNI has evolved. Batsakis originally described PNI as tumour invasion in, around, and through the nerve [15]. Liebig et al. defined PNI more precisely as tumour cells encircling at least one-third of a nerve’s circumference or invading any nerve sheath layer [16].
MRI can also detect perineural tumour spread (PNTS) [17], a radiological entity distinct from histological PNI. PNTS features include nerve thickening, enhancement, increased T2 signal, and loss of perineural fat. Secondary signs include muscle atrophy due to denervation [18]. Clinically, PNTS may cause neuropathic pain, characterised by hypersensitivity and spontaneous pain, present in up to 40% of patients with cancer [19]. Validated tools such as the Douleur Neuropathique 4 Q and the Leeds Assessment are used to differentiate neuropathic from nociceptive pain. Neuropathic pain is typically resistant to opioids and may require adjuvants such as antidepressants, anticonvulsants, and antiarrhythmic agents [20].
Reports by Ladha and Capek document lumbosacral plexopathy due to PCa [21], including a case of bilateral involvement confirmed via MRI and magnetic resonance neurography (MRN). Katsumi reported a case of PCa-related sciatica [22]. In both cases, nerve biopsies confirmed PCa cell infiltration.
Magnetic resonance neurography (MRN), first described by Filler et al. [23] in 1993, uses modified MRI sequences to visualise peripheral nerves. MRN exploits prolonged T2 relaxation times and combines contrast-enhanced T1-weighting, fat suppression and blood-signal suppression techniques to create a ‘neurogram’. MRN has shown the most promise in imaging brachial and lumbosacral plexopathies [24], but its application in cancer neurobiology is expanding.
This study aimed to determine whether patients with PCa show radiological evidence of tumour interaction with the 1) peripheral nervous system (PNS), 2) central nervous system (CNS), and 3) whether the PNS serves as a conduit for CNS involvement. The histological finding of PNI in PCa, anatomy of the pelvic nerve plexus, proximity of the prostate to the lumbosacral spine and presentation of patients with SCC present a unique opportunity for further interrogation of tumour-nerve interactions through the spatial imaging. MRI and MRN were used to trace peripheral nerves from the prostate to the lumbosacral spine. We sought radiological evidence of cancer tracking along the nerves toward the spinal cord.
2. Materials and Methods
This cross-sectional study was conducted as follows. Following informed consent, adult male patients with suspected PCa presenting to Steve Biko Academic Hospital in Pretoria, South Africa, were screened. Patients with histologically confirmed PCa were enrolled between February 2022 and October 2023. MRI and MRN were performed at state and private facilities, using protocols summarised in Table 1. The study was approved by the University of Pretoria Health Research Ethics Committee (Ref: 276/2021) and conducted according to the university’s code of research ethics and the Declaration of Helsinki. Patient and public participation in research design and conduct was not a requirement at the time of protocol submission.
Variables
Data were collected from clinical history including the presence of neurological fallout, blood tests, histology, and MRI. Back pain, back trauma, and HIV were assessed as confounders of abnormal nerve findings. Elevated prostate-specific antigen (PSA), routinely measured in suspected PCa, was an inclusion criterion.
Histological variables included Gleason score, International Society of Uropathologists (ISUP) grade group, and presence of PNI. MRI/MRN assessments included evidence of PNTS in pelvic nerves, nerve roots, compression of the spinal cord, and midsagittal distances from the prostate base to the sacral promontory and the sacrococcygeal junction.
Sample size
This study forms part of a larger project studying the interaction of PCa with the nervous system. The calculated sample size was 158. The patient enrolment is summarised in Figure 1. The inclusion criteria for the overall project was all adult males presenting with suspected PCa who consented to prostate biopsy, 171 patients were enrolled. The patients who had biopsy-proven PCa were to proceed to MRI/N, 104 met this criterion. Resource constraints in the state hospital, where the MRI machine was out of service for a prolonged period led to most of the scans being performed in private. The costs of private services set a limit on the total number of patients who could be scanned. Fifty-eight patients were enrolled into this leg of the project.
Statistical analysis
Data were analysed using Stata Standard Edition 18.0. The data were descriptively analysed. Normality of the continuous variables was assessed using the Shapiro‒Wilk test. Normally distributed variables are reported as the mean and standard deviation (; [SD]). Nonnormally distributed continuous variables are presented as medians and interquartile ranges (25th–75th percentiles). Categorical variables are reported as frequencies and percentages (n [%]). Student’s t test was used to assess continuous data distribution, variance homogeneity, and data independence. The study used a 5% significance level.
3. Results
Fifty-eight patients were enrolled in the study, 19 were imaged in a state facility and 39 at a private facility.
The average age was 66.6 years (+/- 8.1 SD), the average PSA was 35.3 μg/L (IQR 14–157). HIV was negative in 49 patients (92.5%) and positive in four patients (7.5%). Histologically, 28 patients (48.3%) were classified as high-risk based on Gleason score. ISUP grade grouping showed a near-equal distribution between intermediate-risk (n = 23, 39.7%) and high/very high-risk (n = 22, 37.9%) categories. PNI was present in 28 patients (48.3%). The histology, MRI and MRN findings are summarised in Table 2.
The median prostate volume was 32.5 cc (IQR 25–56), ranging from 8 to 261 cc. More than half of the patients had a prostate volume of ≤40 cc. Soft tissue metastases were present in 30 patients (51.2%) in the following structures in order of frequency: extracapsular extension, seminal vesicles, lymph nodes, bladder wall, pelvic diaphragm and rectum. No pelvic sidewall metastases were observed.
PNTS was identified in 32 patients (65.3%). The individual features of PTNS are shown in Table 2. Seven patients had only enhancement, 11 had only reduced perineural fat, and the remainder showed multiple features.
Among the 32 patients with radiological PNTS, 15 had histological PNI, while 16 did not. Of the 18 patients without radiological PNTS data, seven had histological PNI, and 11 did not. A correlation matrix (Table 3) showed associations between PSA and Gleason score, PSA and ISUP grade, and Gleason score and ISUP grade. No significant correlations were found between PNTS and any other variables.
Eight patients with suspected SCC underwent MRI, not the extended MRN sequence. The findings are shown in Table 4 and Figure 2. In four patients, the presentation of SCC preceded the diagnosis of PCa. The other four patients were diagnosed with PCa before presenting with inability to walk. The cause of SCC was unrelated to PCa in two patients and was attributed to disc prolapse. Four patients had PNTS and nerve root compression, with no evidence of skeletal involvement or neurological fallout. Five patients had dural and epidural thickening and enhancement.
4. Discussion
This study addressed three objectives: (1) to determine whether PCa interacts with the PNS, (2) whether it interacts with the CNS, and (3) whether CNS involvement occurs via the PNS. Fifty-eight patients were enrolled in the study.
The average patient age and PSA levels were consistent with previously reported data. Nearly half (48.3%, n = 28) of the cohort fell into the intermediate- or high-risk categories by ISUP grade. High-grade disease typically indicates advanced cancer, reflecting greater architectural disorganisation as reflected by higher Gleason or ISUP scores. In low- and middle-income countries, including South Africa, patients with PCa often present late due to delays in healthcare access, low health literacy, unemployment, and low income [25]. Studies from South Africa confirm this trend, with patients frequently presenting with high PSA levels, high-grade tumours, or metastatic disease [26,27,28,29].
Contiguous soft tissue spread was observed in 51.2% of patients. Lymph node metastasis (38%) and skeletal and vertebral metastases (34.5%) reflected lymphatic and hematogenous spread, respectively (Table 2). Of the four currently recognised mechanisms of metastasis, we did not explore transcoelomic spread, but it may be relevant in future studies given the location of the CNS within the discrete, fluid-lined meningeal cavity. A novel additional mechanism of tumour spread, neurogenous metastasis, is the focus of this study.
Interaction between PCa and the PNS
Radiological evidence of PTNS was found in 69.1% of patients, and histological evidence of PNI was found in 48.3%. PNI is a well-established prognostic factor and is routinely reported per international guidelines [30]. PNI is associated with adverse pathology [11], biochemical recurrence [12], soft tissue progression [13], and poor prognosis [14].
MRN is a noninvasive modality that enables visualisation of nerve structures along their course, distinguishing them from the surrounding vasculature and tissue [23,24,31]. In this study, MRN visualised nerves directly invaded by cancer. PNTS was visualised in the inferior hypogastric plexus, femoral nerve, sciatic nerve, and lumbar and sacral nerve roots. Prior case reports confirmed PNTS through nerve biopsies, typically years after initial PCa diagnosis. PNTS has been observed in the lumbosacral nerve roots and plexus [32], the lumbosacral plexus only [33], the lumbosacral plexus and sciatic nerve [34], bilateral lumbosacral plexuses [21], and the sciatic nerve [22]. Invasive nerve procedures carry a high risk of permanent motor or sensory deficits [35]. In two case reports, neurological symptoms preceded PCa diagnosis; in others, symptoms arose years later. Confirmation of PNTS via MRN may eliminate the need for surgical biopsy and allow earlier treatment initiation. Neuropathic symptoms, including pain, gait disturbance, and sensory or motor deficits, should prompt MRN assessment for PNTS.
The average distances from the prostate base to the sacrococcygeal junction (74.1 mm) and the sacral promontory (79.3 mm) represent the shortest linear path to the spinal cord, although actual nerve length is longer due to anatomical complexity. These distances may help estimate the time to potential spinal cord involvement if the rate of propagation of tumour cells in PNTS is determined, particularly in patients with PNI at diagnosis. Future studies to determine the rate of propagation could be modelled on what is known about the rate of nerve regeneration following injury which is 1 mm per day [36,37].
Interaction between PCa and the CNS
Eight patients presented with SCC, indicating possible interaction of PCa with the CNS; four patients did not have a prior diagnosis of PCa. In six patients, PCa was the underlying cause; in two, disc herniation was responsible (Table 3). Malignant SCC is a well-known complication of advanced cancers, including prostate, breast, and lung cancers [7]. Early detection is critical for neurological recovery [38].
Currently, cancer cells are believed to reach the spinal cord via haematogenous spread into Batson’s valveless venous plexus and the vertebral bodies, with subsequent expansion of the malignant mass causing SCC [8], which occurred in four patients in our study. One patient (SCC 7) had compression from vertebral collapse, and another exhibited concentric dural and epidural thickening without compression from vertebral collapse or an expanding metastatic vertebral deposit (SCC 5). These findings underscore the need for comprehensive imaging to differentiate PCa-related causes from other causes and guide appropriate management.
CNS involvement via the PNS
One patient had dural and epidural thickening with enhancement and no compression from vertebral related metastases. This finding suggests a neurogenous route of CNS invasion. Hebert-Blouin et al. proposed direct perineural spread from the pelvic plexus to the lumbosacral plexus as a potential mechanism for dural metastases [33]. Our findings support this hypothesis. The meninges may prevent intradural metastases, dural and epidural involvement can cause SCC via an extradural route, as in patient SCC5.
Additionally, four patients with radiological PNTS but no neurological symptoms were present, including one with dorsal root ganglion enhancement and no skeletal metastases. These findings suggest subclinical PNTS with potential for progression. Serial imaging may provide further insights.
The limitations of the study include the single-centre design, small sample size, and lack of serial imaging. Multi-centre studies involving larger sample sizes will be important in determining the generalisability of the findings. The high cost of MRN may limit its widespread use in resource-constrained settings. We propose three future directions:
- (1)
- Combine MRN with positron emission tomography/computed tomography to improve specificity for PNTS and exclude other causes of nerve inflammation
- (2)
- Correlate PNTS with the radiological TNM stage, PIRADS score, grade of disease per Gleason score or ISUP grade grouping or PNI to refine prognostic implications.
- (3)
- Incorporate MRN data into mathematical models to predict the spread of cancer cells along nerve fibres.
5. Conclusions
This study demonstrates that PCa interacts with the PNS and CNS. PTNS was frequently identified via MRN, supporting a neurogenous route of dissemination of PCa.
Author Contributions
Conceptualization, K. Mathabe and M. Sathekge.; methodology, K. Mathabe., N Matjomane and M Sathekge.; formal analysis, K. Mathabe and M Mkhabela.; investigation, K Mathabe., Z Lockhat., I de Beil., K Kollapen and N Singh.; resources, K Mathabe, Z Lockhat and M Sathekge.; data curation, K. Mathabe.; writing—original draft preparation, K. Mathabe.; writing—review and editing, K Mathabe., N Matjomane., Z Lockhat., I de Beil., K Kollapen., N Singh., M Mkhabele and M Sathekge; visualization, K. Mathabe.; supervision, M. Sathekge.; project administration, K. Mathabe and N. Matjomane.; funding acquisition, K. Mathabe and M Sathekge. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the National Research Foundation, grant number BAAP 210315589925-PR-2024 and the Discovery Foundation, South Africa, grant number 049479.
Institutional Review Board Statement
The study was approved by the University of Pretoria Health Sciences Research Ethics Committee (reference number 276/2021).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data is available from the author on request.
Acknowledgments
The authors would like to thank the doctors and nurses in the department of Urology at Steve Biko Academic Hospital, the brave patients who agreed to participate in the study, the radiography and administrative staff at Maine Radiology, Dr F Joseph, Mr F Meintjes, Dr L Cassim, Dr C Tosh, Prof Z Dlamini and PACRI for their invaluable contributions. During the preparation of this manuscript/study, the author(s) used Napkin AI v3, version for the purposes of creating the image in Figure 1. The authors have reviewed and edited the output and take full responsibility for the content of this publication.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| CNS | central nervous system |
| DWI | diffusion-weighted image |
| ISUP | International Society of Uropathologists |
| MRI | magnetic resonance imaging |
| MRN | magnetic resonance neurography |
| PCa | prostate cancer |
| PNI | perineural invasion as observed via histology |
| PNS | peripheral nervous system |
| PNTS | perineural tumour spread as observed via radiological imaging |
| PSA | prostate-specific antigen |
| SCC | spinal cord compression |
| SPIR | spectral presaturation with inversion recovery |
| STIR | short T1 inversion recovery |
| T1W | T1-weighted |
| T2W | T2-weighted |
References
- ASCO. Prostate cancer statistics. Available online: https://www.cancer.net/cancer-types/prostate-cancer/statistics (accessed on 22 May 2022).
- Rawla, P. Epidemiology of Prostate Cancer. World journal of oncology 2019, 10, 63–89. [Google Scholar] [CrossRef]
- Osborn, J.L.; Getzenberg, R.H.; Trump, D.L. Spinal cord compression in prostate cancer. J Neurooncol 1995, 23, 135–147. [Google Scholar] [CrossRef]
- Tazi, H.; Manunta, A.; Rodriguez, A.; Patard, J.J.; Lobel, B.; Guillé, F. Spinal cord compression in metastatic prostate cancer. Eur Urol 2003, 44, 527–532. [Google Scholar] [CrossRef]
- Tsuzuki, S.; Park, S.H.; Eber, M.R.; Peters, C.M.; Shiozawa, Y. Skeletal complications in cancer patients with bone metastases. Int J Urol 2016, 23, 825–832. [Google Scholar] [CrossRef]
- Loblaw, A.; Mitera, G. Malignant extradural spinal cord compression in men with prostate cancer. Curr Opin Support Palliat Care 2011, 5, 206–210. [Google Scholar] [CrossRef]
- Sutcliffe, P.; Connock, M.; Shyangdan, D.; Court, R.; Kandala, N.B.; Clarke, A. A systematic review of evidence on malignant spinal metastases: natural history and technologies for identifying patients at high risk of vertebral fracture and spinal cord compression. Health Technol Assess 2013, 17, 1–274. [Google Scholar] [CrossRef] [PubMed]
- Bubendorf, L.; Schopfer, A.; Wagner, U.; Sauter, G.; Moch, H.; Willi, N.; Gasser, T.C.; Mihatsch, M.J. Metastatic patterns of prostate cancer: an autopsy study of 1,589 patients. Hum Pathol 2000, 31, 578–583. [Google Scholar] [CrossRef] [PubMed]
- Chen, T.C. Prostate cancer and spinal cord compression. Oncology (Williston Park) 2001, 15, 841–855. [Google Scholar]
- Laur, O.; Nandu, H.; Titelbaum, D.S.; Nunez, D.B.; Khurana, B. Nontraumatic Spinal Cord Compression: MRI Primer for Emergency Department Radiologists. Radiographics 2019, 39, 1862–1880. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.; Lin, X.; Lin, S.X.; Lu, M.; Deng, T.; Wang, Z.; Olumi, A.F.; Dahl, D.M.; Wang, D.; Blute, M.L.; et al. Impact of biopsy perineural invasion on the outcomes of patients who underwent radical prostatectomy: a systematic review and meta-analysis. Scand J Urol 2019, 53, 287–294. [Google Scholar] [CrossRef]
- Zhang, L.-j.; Wu, B.; Zha, Z.-l.; Qu, W.; Zhao, H.; Yuan, J.; Feng, Y.-j. Perineural invasion as an independent predictor of biochemical recurrence in prostate cancer following radical prostatectomy or radiotherapy: a systematic review and meta-analysis. BMC Urology 2018, 18, 5. [Google Scholar] [CrossRef]
- Yang, T.; Wang, C.; Liu, Y.; Zhu, X.; Wang, W.; Xu, C.; Wang, X.; Chi, Y.; Huang, S.; Wu, D. Perineural Invasion as a Risk Factor For Soft Tissue Progression in Patients With Metastatic Castration-Resistant Prostate Cancer After Abiraterone Resistance. Clin Genitourin Cancer 2024, 22, 102125. [Google Scholar] [CrossRef] [PubMed]
- Zhao, J.; Chen, J.; Zhang, M.; Tang, X.; Sun, G.; Zhu, S.; Liu, J.; Zhang, H.; Zhang, X.; Yin, X.; et al. The clinical significance of perineural invasion in patients with de novo metastatic prostate cancer. Andrology 2019, 7, 184–192. [Google Scholar] [CrossRef]
- Batsakis, J.G. Nerves and Neurotropic Carcinomas. Annals of Otology, Rhinology & Laryngology 1985, 94, 426–427. [Google Scholar] [CrossRef]
- Liebig, C.; Ayala, G.; Wilks, J.A.; Berger, D.H.; Albo, D. Perineural invasion in cancer: a review of the literature. Cancer 2009, 115, 3379–3391. [Google Scholar] [CrossRef]
- Bakst, R.L.; Glastonbury, C.M.; Parvathaneni, U.; Katabi, N.; Hu, K.S.; Yom, S.S. Perineural Invasion and Perineural Tumor Spread in Head and Neck Cancer. International Journal of Radiation Oncology, Biology, Physics 2019, 103, 1109–1124. [Google Scholar] [CrossRef] [PubMed]
- Ong, C.K.; Chong, V.F. Imaging of perineural spread in head and neck tumours. Cancer Imaging 2010, 10 Spec no A, S92–98. [Google Scholar] [CrossRef]
- Yoon, S.Y.; Oh, J. Neuropathic cancer pain: prevalence, pathophysiology, and management. Korean J Intern Med 2018, 33, 1058–1069. [Google Scholar] [CrossRef]
- Blanchard, C. Guide to the Treatment of Cancer Pain in South Africa; South Africa, 2015; p. 93.
- Capek, S.; Howe, B.M.; Tracy, J.A.; García, J.J.; Amrami, K.K.; Spinner, R.J. Prostate cancer with perineural spread and dural extension causing bilateral lumbosacral plexopathy: case report. J Neurosurg 2015, 122, 778–783. [Google Scholar] [CrossRef]
- Katsumi, S.; Soshi, S.; Kajiwara, T.; Saito, M. Sciatica Caused by Perineural Spread of Prostate Cancer. Cureus 2023, 15, e38057. [Google Scholar] [CrossRef]
- Filler, A.G.; Howe, F.A.; Hayes, C.E.; Kliot, M.; Winn, H.R.; Bell, B.A.; Griffiths, J.R.; Tsuruda, J.S. Magnetic resonance neurography. Lancet (London, England) 1993, 341, 659–661. [Google Scholar] [CrossRef]
- Ku, V.; Cox, C.; Mikeska, A.; MacKay, B. Magnetic Resonance Neurography for Evaluation of Peripheral Nerves. J Brachial Plex Peripher Nerve Inj 2021, 16, e17–e23. [Google Scholar] [CrossRef] [PubMed]
- Brand, N.R.; Qu, L.G.; Chao, A.; Ilbawi, A.M. Delays and Barriers to Cancer Care in Low- and Middle-Income Countries: A Systematic Review. Oncologist 2019, 24, e1371–e1380. [Google Scholar] [CrossRef]
- Babb, C.; Urban, M.; Kielkowski, D.; Kellett, P. Prostate cancer in South Africa: pathology based national cancer registry data (1986-2006) and mortality rates (1997-2009). Prostate Cancer 2014, 2014, 419801. [Google Scholar] [CrossRef]
- Benedict, M.O.A.; Steinberg, W.; Claassen, F.; Mofolo, N. The profile of Black South African men diagnosed with prostate cancer in the Free State, South Africa. South African Family Practice 2022, 64. [Google Scholar] [CrossRef]
- Le Roux, H.A.; Urry, R.J.; Sartorius, B.; Aldous, C. Prostate Cancer at a regional hospital in South Africa: we are only seeing the tip of the iceberg. S Afr J Surg 2015, 53, 57–62. [Google Scholar]
- Marais, B.; Klopper, G.; John, J. Prostate cancer perspective: Africa versus the world. South African Medical Journal 2024, 114, 21–25. [Google Scholar] [CrossRef] [PubMed]
- Egevad, L.; Judge, M.; Delahunt, B.; Humphrey, P.A.; Kristiansen, G.; Oxley, J.; Rasiah, K.; Takahashi, H.; Trpkov, K.; Varma, M.; et al. Dataset for the reporting of prostate carcinoma in core needle biopsy and transurethral resection and enucleation specimens: recommendations from the International Collaboration on Cancer Reporting (ICCR). Pathology 2019, 51, 11–20. [Google Scholar] [CrossRef]
- Soldatos, T.; Andreisek, G.; Thawait, G.K.; Guggenberger, R.; Williams, E.H.; Carrino, J.A.; Chhabra, A. High-resolution 3-T MR neurography of the lumbosacral plexus. Radiographics 2013, 33, 967–987. [Google Scholar] [CrossRef]
- Ladha, S.S.; Spinner, R.J.; Suarez, G.A.; Amrami, K.K.; Dyck, P.J. Neoplastic lumbosacral radiculoplexopathy in prostate cancer by direct perineural spread: an unusual entity. Muscle Nerve 2006, 34, 659–665. [Google Scholar] [CrossRef]
- Hébert-Blouin, M.N.; Amrami, K.K.; Myers, R.P.; Hanna, A.S.; Spinner, R.J. Adenocarcinoma of the prostate involving the lumbosacral plexus: MRI evidence to support direct perineural spread. Acta Neurochir (Wien) 2010, 152, 1567–1576. [Google Scholar] [CrossRef] [PubMed]
- Babu, M.A.; Spinner, R.J.; Dyck, P.J.; Amrami, K.K.; Nathan, M.A.; Kawashima, A.; Howe, B.M. Recurrent prostatic adenocarcinoma with perineural spread to the lumbosacral plexus and sciatic nerve: comparing high resolution MRI with torso and endorectal coils and F-18 FDG and C-11 choline PET/CT. Abdom Imaging 2013, 38, 1155–1160. [Google Scholar] [CrossRef] [PubMed]
- Westlake, B.; Pipitone, O.; Tedesco, N.S. Time to Functional Outcome Optimization After Musculoskeletal Tumor Resection. Cureus 2022, 14, e27317. [Google Scholar] [CrossRef]
- Yang, L.J.S.; Chung, K.C. CHAPTER 2 - Physiology of nerve injury and regeneration. In Practical Management of Pediatric and Adult Brachial Plexus Palsies, Chung, K.C., Yang, L.J.S., McGillicuddy, J.E., Eds.; W.B. Saunders: Philadelphia, 2012; pp. 13–20. [Google Scholar]
- Gordon, T. Peripheral Nerve Regeneration and Muscle Reinnervation. Int J Mol Sci 2020, 21. [Google Scholar] [CrossRef]
- Crnalic, S.; Hildingsson, C.; Bergh, A.; Widmark, A.; Svensson, O.; Lofvenberg, R. Early diagnosis and treatment is crucial for neurological recovery after surgery for metastatic spinal cord compression in prostate cancer. Acta oncologica (Stockholm, Sweden) 2013, 52, 809–815. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Patient enrolment.
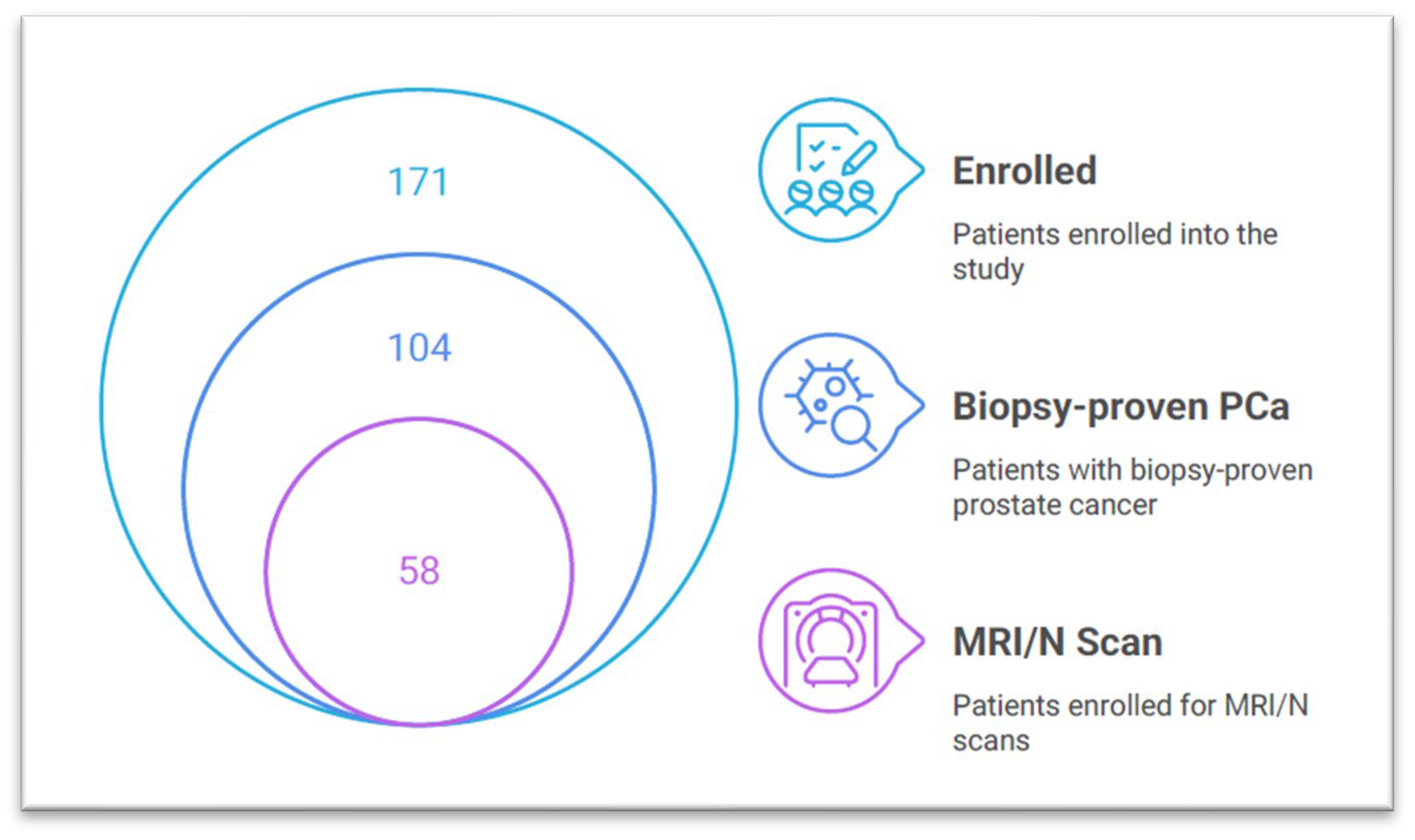
Figure 2.
Magnetic resonance (MR) and magnetic resonance neurography (MRN) images.
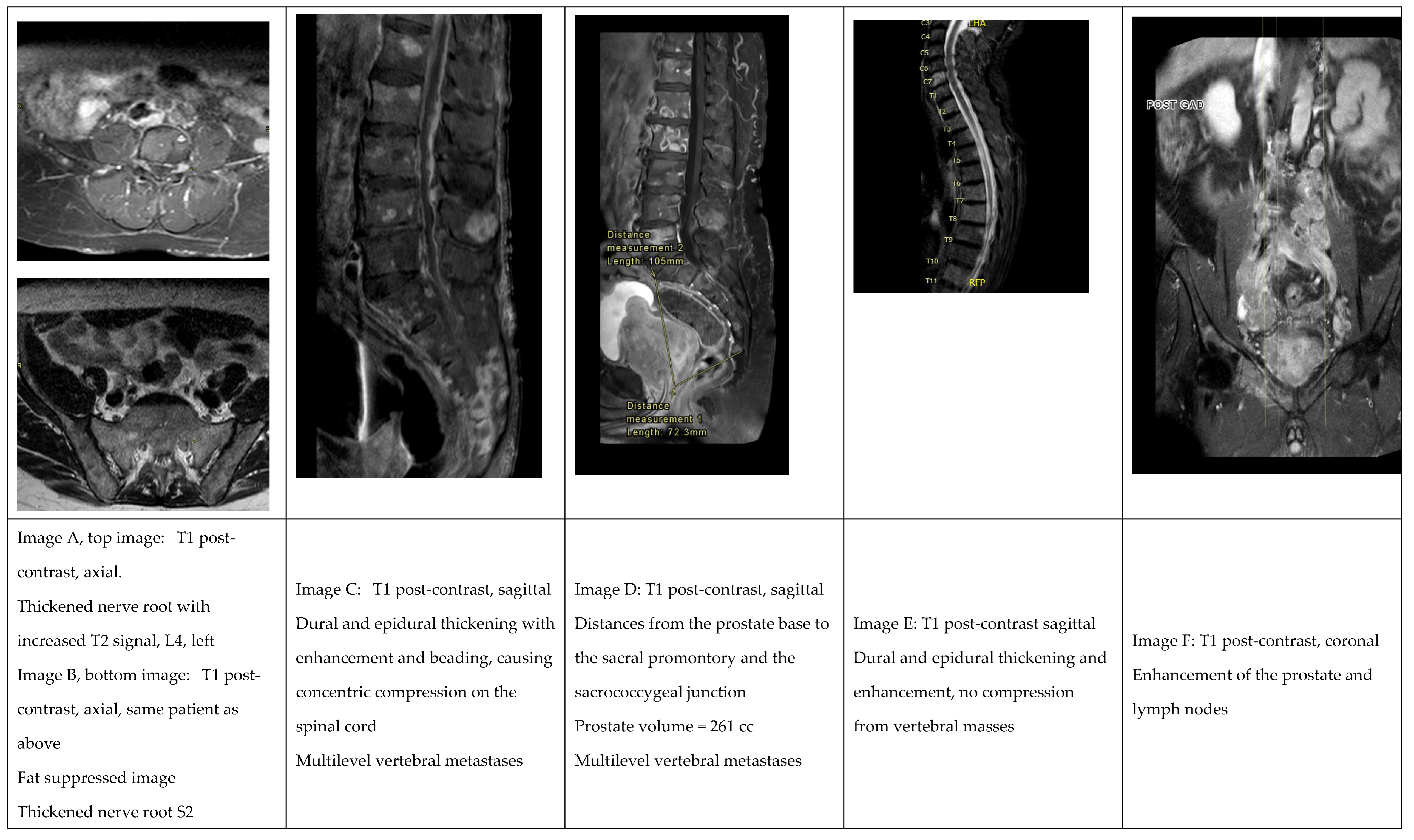

Table 1.
The magnetic resonance imaging (MRI) and magnetic resonance neurography (MRN) protocols used and patient profile in the state and private facility.
Table 1.
The magnetic resonance imaging (MRI) and magnetic resonance neurography (MRN) protocols used and patient profile in the state and private facility.
| Category | State | Private sector |
| Patient profile | Ambulant and wheelchair-bound patients | Only ambulant patients |
| Scanner used | Philips Achieva 1.5T scanner with dedicated spine coil | GE 3 Tesla Signa Pioneer 2.0 and GE 1.5 Tesla Signa Voyager |
| Imaging scope | The standard metastatic spine MRI protocol was modified to include the pelvis to assess the spread of perineural tumours. | The lumbosacral spine and pelvis were scanned separately with high-resolution protocols. |
| Spine protocol | Short T1 inversion recovery (STIR) sagittal and coronal T1-weighted (T1W) spectral presaturation with inversion recovery (SPIR) post-Gadolinium (sagittal, coronal, selected axial) |
STIR coronal and sagittal T2 sagittal and axial T1 pre- and post-contrast in all three planes |
| Pelvis protocol | T2-weighted spectral adiabatic inversion recovery coronal T1W axial using the Principle of Selective Excitation Technique T1W SPIR post-Gadolinium (axial and coronal) Diffusion-weighted imaging (DWI) |
T2 high resolution in three planes T1 axial and coronal (pre- and postcontrast) DWI with b values of 1400 STIR coronal |
| Contrast agent | Gadolinium | Gadovist |
Table 2.
Histological, MRI and MRN findings.
| Variable (n) | Number (%) |
| Histological findings (58) | |
| Gleason score | |
| Low grade | 13 (22.4%) |
| Intermediate grade 7 = 4+3 | 17 (29.3%) |
| High grade | 28 (48.3%) |
| ISUP | |
| 1 | 13 (22.4%) |
| 2 | 17 (29.3%) |
| 3 | 6 (10.3%) |
| 4 | 16 (27.6%) |
| 5 | 6 (10.3%) |
| PNI present | 28 (48.3%) |
| MRI spine, pelvis (58) | |
| Institution | |
| State | 19 (32.8) |
| Private | 39 (67.2) |
| Soft tissue metastases | |
| Extracapsular | 29 (64.4%) |
| Seminal vesicle | 26 (55.3%) |
| Lymph nodes | 19 (38%) |
| Bladder wall | 10 (20.8%) |
| Pelvic diaphragm | 3 (6.5%) |
| Rectum | 2 (4.1%) |
| Pelvic wall | 0 (0%) |
| Bony metastases | |
| Pelvis | 15 (30.8%) |
| Vertebrae | 16 (30.6%) |
| Femur | 4 (8.5%) |
| Midsagittal distance | |
| Sacral promontory | 79.3 (13.2) |
| Sacrococcygeal junction | 74.1 (10.2) |
| Perineural tumour spread | |
| Reduced perineural fat | 24 (49%) |
| Thickening | 20 (40.8%) |
| Increased T2 signal | 17 (34.7%) |
| Enhancement | 7 (14.3%) |
| Secondary changes: Denervation | 1 (2.0%) |
| No nerve changes | 17 (34.7%) |
Table 3.
Correlation matrix to investigate the associations between PNTS and PSA, ISUP grade, Gleason score and age.
Table 3.
Correlation matrix to investigate the associations between PNTS and PSA, ISUP grade, Gleason score and age.
| PNTS | PSA | ISUP | Gleason Score | Age | |
| PNTS | 1.00 | ||||
| PSA ρ p value |
0.299 0.05 |
1.00 |
|||
| ISUP ρ p value |
0.023 0.87 |
0.437 <0.001 |
1.00 |
||
| Gleason Score ρ p value |
0.003 0.98 |
0.418 <0.001 |
0.964 <0.001 |
1.00 |
|
| Age ρ p value |
0.252 0.08 |
0.008 0.93 |
0.031 0.76 |
0.031 0.76 |
1.00 |
Table 4.
Characteristics of patients who presented with spinal cord compression (SCC).
| Patient ID | Known PCa | PNI | Disc bulge | Osseous vertebral metastases | Soft tissue mass | Cause of compression |
|---|---|---|---|---|---|---|
| SCC1 | Yes | No | Yes, not compressive | Yes, widespread, fracture T12 | Yes (thoracic and sacral) | Soft tissue impingement on the spinal cord, T12, and sacral nerve roots |
| SCC 2 | Yes | Yes | Yes, multiple levels, compressive at C5/6, C6/7, L4/5 | No | No | Disc herniation, bilateral L4/5 nerve root |
| SCC 3 | Yes | Yes | Yes, diffuse, not compressive | Yes, widespread | Yes, enhancing, thickened epidural and dura, not compressive | Osseous compression bilateral S1 nerve root impingement |
| SCC 4 | Yes | Yes | Yes, C3/4, C4/5 | Yes | Yes | Soft tissue, T10/11 nerve root, right side |
| SCC 5 | No | Yes | Yes, diffuse, not compressive | Yes, sacrum, pelvis | Yes, enhancing, thickened epidural and dura involving the entire spine, compressive | Spinal canal narrowing plus lobulated impressions on the cord due to soft tissue, buckling of the cauda equina |
| SCC 6 | No | Yes | Yes | No | Osseous compression, L2 | |
| SCC 7 | No | Yes | Yes | No | Vertebral collapse with compression, T3 | |
| SCC 8 | No | Yes | Yes, not compressive | Yes, widespread | No | Disc herniation, L5/S1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



