Submitted:
07 August 2025
Posted:
11 August 2025
You are already at the latest version
Abstract
Laryngoscopy technique for endotracheal intubation has been developed and evolved for many decades. Among various conventional laryngoscopes and blades, videolaryngoscopes (VL) have been applied in a variety of patient populations, including certain difficult airways. The safety and effectiveness of VL have been repeatedly and extensively studied in both normal and difficult airways scenarios. The superiority of VL then has been observed, reported, and is advocated as a standard of care and possibly for routine first-line application. In contrast to laryngoscopy, the development of video intubating stylet (VS, also named as styletubation) has been noticed two decades ago. Since then, sporadic clinical experiences of clinical use have appeared in literature. In this review article, we presented our vast use experiences of the styletubation (more than 63,537 patients from 2016 to 2024). We found this technique is swift (the time to intubate: from 3 s to 10 s), smooth (first-attempt success rate: 100%), safe (no airway complications), and easy (high subjective satisfaction and fast learning curve for the novice trainees) in the majority of normal airway scanrios. Even in seemingly and identified difficult airway scenarios, the intubating time is acceptable (e.g., 30 s) with first-pass success. We therefore propose styletubation technique can be feasibly applied as universal routine use for endotracheal intubation.
Keywords:
styletubation
; video intubating stylet
; laryngoscopy
; videolaryngoscope
; Shikani technique
; endotracheal intubation
; orotracheal intubation
; nasotracheal intubation
; airway management
; emergency
; critical care
; intensive care unit
; non-operating room anesthesia
1. From Direct to Indirect Laryngoscopy
Conventional laryngoscopy, i.e., direct laryngoscopy (DL) and videolaryngoscopy (VL), has been one of the essential clinical skills for medical staff that green airway manager practitioners must learn quickly and master proficiently since centuries ago (for review, see [1-3]). Laryngoscopy, in addition to other airway devices, has been advocated as the mainstream technique for endotracheal intubation. Such laryngoscopy technique has been widely applied for anesthesia and airway management in the various hospital settings (e.g., operating rooms (OR), non-operating rooms anesthesia (NORA), emergency rooms (ER), intensive care units (ICU), general wards) and field intubation by emergency medical services (EMS) personnel in the pre-hospital setting [4-8]. Meanwhile, it is not surprising that laryngoscopy has always been compared with all the available airway management tools in patients under different physiological and anatomical difficult airway scenarios.
The medical purposes (e.g., for diagnosis and treatment) of using DL for ear-nose-throat (ENT) professionals are different from that for anesthesiologists (i.e., for endotracheal intubation and general anesthesia) [9]. Therefore, the functions and the roles of laryngoscope-blade devices for endotracheal intubation have been re-designed and re-shaped by many pioneers since then. Together with such various shape of the laryngoscope blades, the legendary principle of indirect elevation of the epiglottis to optimally expose the glottis and then acquire a perfect visualization was demonstrated [10].
In order to successfully pass an endotracheal tube (ET tube) under direct vision by DL, seven technical tips for endotracheal intubation under general anesthesia have been proposed [11]. Since then, several recommended accessary techniques (e.g., proper head/neck positions, appropriate insertion and lifting of the laryngoscope blades) have been repeatedly demonstrated to be crucial and important to a smooth and successful DL-endotracheal intubation. The learning curve and performance of DL technique by the green airway operators/practitioners, unsurprisingly, appears to be a focused issue consistently [12]. In order to easily acquire an optimal glottis visualization for subsequent placement of the ET tube into trachea, most of the time, a significant upward lifting force on the DL handle-blade unit be required by the airway operator. Such upward lift force may indirectly elevate the epiglottis and expose the glottis in a reasonable way, while such lifting force might also affect or be limited by patient’s cervical spine motion or anatomical structures around head-neck regions [13,14]. Under direct vision with DL, therefore, the incidence of difficult airway (DA) and difficult intubation (DI) occur with varied incidence rates among different clinical scenarios, e.g., 1.41% [15], 4.5% [16], 4.46% [17], 4.7% [18], and 22.3% [19]. Various clinical predictors for difficult laryngoscopy have been reported, such as age, body mass index (BMI), neck circumference, snoring and obstructive sleep apnea (OSA) syndrome, neck mobility, thyro-mental and sterno-mental distance [20,21].
Both the laryngeal exposure and mechanics of actual ET tube advancement, delivery and insertion are important key factors for a successful endotracheal intubation with DL. In contrast to DL, the various commercial product designs of VL have been ingeniously designed and excellently shown to reduce failed-intubation rates and higher first-attempt success rates with comparable or superior glottic visualization [22,23]. For VL, the condition of a direct line of sight based on the conventional three-axes or two-axes alignment theory is not prerequisite to acquire an excellent or optimal glottis view [24,25]. Different types of the laryngoscope blade resulted in different lifting forces acting on pharyngeal and laryngeal tissues [14]. Even so, difficult laryngoscopy incidents may still be encountered by such excellently innovated VL. Several modifiable factors are constantly reported to be related, e.g., head and neck position and provider’s experience [26,27]. Since the invention and application of VL for endotracheal intubation two decades ago, its clinical role as a standard and routine airway modality has been extensively and repeatedly advocated and challenged [28,29]. Recently, VL appears to be a preferable approach for intubating patients undergoing surgical procedures in the operating rooms [30] and among critically ill adults (in an emergency department or intensive care unit) [31,32]. In comparison with the invincible role of flexible fiberoptic bronchoscope (FFB), it is still too early to claim VL be the holy grail of airway management [33].
2. The Quest for the Holy Grail in the DA Management
Although the FFB technique has been considered as the gold standard for DA, it is not too surprising that the combination technique with FFB and VL be advantageous in several DA scenarios [34,35]. Meanwhile, other types of the optic/video devices for endotracheal intubation have emerged onto the airway management, including rigid/semi-rigid optical stylets [36,37]. It is also interesting to note that a lightwand design (Trachlight) has been invented and proved to be a useful alternative for endotracheal intubation [38-40].
Rigid stylet scopes are reported as a useful alternative to flexible fibreoptic scopes for predicted or unpredicted difficult airway management [36; 41-44]. Currently, there are more than 20 similar kinds of video intubating stylets (VIS) available and affordable in the market (Figure 1). The sale price of each kind of such VIS products ranged from few hundreds to thousands of US dollars.
Since 2016, we have systematically implemented the styletubation (video intubating stylet technique) (Figure 2) for routine and first-line endotracheal intubation [45-49]. In Taiwan, such styletubation technique has ubiquitously been adopted for endotracheal intubation in many medical centers, regional hospitals, and some local private clinics and has been applied in more than a million of patients. In our own clinical utilization experience, the universal use coverage of styletubation is increasing exponentially during these years (Table 1). In this review article, we attempt to demonstrate the clinical scope of utilization (styletubation technique), pearls and pitfalls of such intubation technique, and areas for future advancement and research.
3. Technical Evolution of Styletubation
Figure 3 demonstrates an evolution from DL to VL, and eventually to styletubation since last century. Figure 3A displays a fact that direct inspection and good visualization of the vocal cords have been the major issues for the airway managers (i.e., laryngologists, anesthesiologists, and others) for years when DL is generally applied. Anticipated and unpredicted difficult and even failed laryngoscopy and intubation might be more than often encountered. The successful performance of DL technique itself, therefore, might take very much long time to describe than to proficiently carry out and, is basically claimed to be a not-difficult maneuver if certain simple straight anatomical rules (e.g., sniff position) are obeyed in anesthetized patients [11].
In the real world, “a good endotracheal intubation” with DL by airway novices/trainees required a relatively slow learning curve (e.g., more than 47 attempts) and several criteria are required for success (e.g., proper insertion and lifting of the laryngoscope, in addition to proper sniff position) [12]. Fortunately, with the invention of VL (Figure 3B), a consistently comparable or even superior glottic view compared with DL was observed, despite the limited or lack of prior experience with the device [28]. Most important, successful intubation was generally achieved even when DL was expected to be moderately or considerably difficult. Nevertheless, expertise in VL skills and competency may require prolonged training and practice [50].
As mentioned earlier, a semi-rigid intubating stylet (a hockey-stick type of seeing-stylet scope) for endotracheal intubation appeared even before invention of VL [36]. It should be noted that such new seeing-stylet scope was proposed to be used for management of difficult airway in both adult and pediatric patients by improving the maneuverability of the stylet-ET tube unit and a better glottis visualization. In addition, without the need of a rigid laryngoscope blade to retract the tongue base, the risks of airway injuries would be minimized. Later, such styletubation was also demonstrated to be an effective instrument for orotracheal intubation in normal subjects, including retromolar approach [42,51]. Figure 3C shows such performance of such styletubation technique in the real world operation. In comparison to the DL and VL, the styletubation shows more advantages and superiority, including the extremely high first-pass success rate, shortest intubation time, strong subjective easiness and satisfaction, and particularly fast learning curve.
4. Pearls and Pitfalls of Styletubation
Both conventional midline approach and retromolar approach are the options to perform styletubation. It is noted that the midline approach could provide easier and better glottic exposure and shorter time to intubation when using VL for tracheal intubation [52]. When applying Bonfils intubating fiberscope, it is also proposed to advance the scope via midline until the epiglottis is visualized, in contrast to the originally proposed retro-molar approach [37,42]. Apparently, maintaining a midline position of the intubating stylet-ET tube unit along the oropharyngeal path is much easier for both the beginners and first-line airway managers to visually locate the glottis. In line with this first technical tip for video intubating stylet (e.g., Bonfils-type endoscope) [42], we also adopted such midline approach when standard styletubation for routine endotracheal intubation was conducted. In Figure 4, an apparently normal airway scene is sequentially demonstrated when styletubation was routinely applied in the real world practice. The anesthetized patient’s mouth was open wide enough and the jaw was lifted up by an airway assistant (Figure 4A). Both the patient’s hard/soft palate and uvula are easily visualized (Figure 4B). While a suction tube was used in advance to clear the secretions along the airway, some might still remain and air bubble formed. Then, the airway operator moved the intubating stylet-ET tube unit forward along the posterior pharyngeal wall until both the tongue base and the epiglottis were eventually observed (Figure 4C). In this case, the space between the flopped epiglottis and the posterior pharyngeal wall remained to be wide enough for passage of the assembly. At this point, the operator could easily and gently maneuver the intubating stylet-ET tube set downward, forward, and pass beneath the epiglottis. After the intubating assembly was passing under the epiglottis, the operator needed to lift it up and tilt the tip of the set until the full glottis view could be clearly acquired (Figure 4D,E). Finally, the ET tube could be smoothly dislodged from the intubating stylet, advanced forward and placed into the patient’s trachea, guided by the centrally located tracheal rings (Figure 4F). With these step-by-step tips for midline approach of styletubation, one can easily and smoothly accomplish the endotracheal intubation.
The composition of an airway management team for routine anesthesia can be varied, pending on the each individual medical infrastructures and policies of the local medical facilities. When difficult airway was anticipated or unexpectedly encountered during endotracheal intubation procedure, a call-for-help with additional assistants and a team-based approach should be implemented [21,53]. Figure 5 illustrates three different clinical models to routinely conduct styletubation in the operating rooms and elsewhere clinical settings in the hospital: without (Figure 5A,B) and with an assistant (Figure 5C). When there is only one airway operator at the scene to conduct endotracheal intubation, styletubation could be jointly performed either with a DL [54-56] or a VL [57-60] to facilitate opening of the airway and exposure of the glottis (Figure 5A). In combination of a VL, such double-vision obtained from a VL-styletubation combination technique can help the novice trainee a lot when a difficult scenario or situation was encountered (either expected or un-anticipated DA). Similarly, when styletubation is performed by a lone operator at the scene, one can then adopt the outstanding Shikani technique (Figure 5B) [36]. Briefly, the patient is placed in the conventional sniff position before endotracheal intubation proceeded. The operator then grabs the patient’s mandible with the non-dominant hand for both mouth-opening and jaw-thrust maneuvers. Once patient’s epiglottis is gently and indirectly lifted up by such jaw-thrust maneuver, hopefully, there would be an enough space created between the epiglottis and posterior pharyngeal wall. Then, the intubating stylet-ET tube assembly could be placed between the vocal cords. Finally, the ET tube can be dislodged from the assembly and be advanced into patient’s trachea under continuous and direct visualization displayed on the video monitor screen. After that, the intubating stylet is smoothly withdrawn from the ET tube. Then, the operator smoothly advanced and placed the ET tube into patients’ trachea at a proper depth. Alternatively and most often, when there is an airway assistant (or a trainee) to help, the main task of this helper is to perform maneuvers of effective jaw-thrust and mouth-opening on the patient (Figure 5C). The principal airway operator could then concentrate on performing styletubation in a stepwise manner. The ideal intubating process and sequence would be similar to the presentation in the Figure 4.
The laryngeal/glottic visualization obtained by the laryngoscopy technique has been characterized into various degrees of clarity and subsequently correlated to difficult intubation, e.g., Cormack-Lehane classification [61,62]. Similarly, such laryngeal/glottic visualization acquired during styletubation can also be classified into three degrees (coined as the LQS grading system) [45-49]. Briefly, under the condition of a simple effective jaw-thrust maneuver, patient’s epiglottis could be lifted up to certain degree and expose any part of the vocal cords (VC), it is then classified as LQS grade 1. (Figure 6, left panels). When no part of VC could be visualized at all, but still there is enough space between the epiglottis and posterior pharyngeal wall created by simple jaw-thrust maneuver, it is then defined as LQS grade 2 (Figure 6, middle panels). Both the grade 1 and grade 2 airway scenarios are usually regarded as the soft targets for (experienced or novel trainee) airway operators to intubate. In contrast, when the epiglottis can not be lifted up at all by simple jaw-thrust maneuver and therefore completely lying down against the posterior pharyngeal wall, no part of the glottis opening therefore can be visualized. Such austere scenario is then defined as LQS grade 3 (Figure 6, right panels). The grade 3 scenario, although rare and serious, could be difficult but not always impossible to accomplish endotracheal intubation by styletubation. Fortunately, the incidence of LQS grade 3 scenario is very low (< 0.5 %) and commonly occurred in patients with predicted difficult airway scenarios (e.g., limited cervical spine mobility, morbid obesity, radiation fibrosis, pharyngo-laryngeal tumors, etc.).
When the clinical effectiveness of endotracheal intubation tools (e.g., VL versus DL) was compared, usually the intubation time (i.e., time to intubate) was adopted together with other clinical outcome comparators (e.g., first-pass success rate, total success rate, complications, autonomic nervous stimulation, etc.) [63,64]. The superiority of styletubation over laryngoscopy with a much shorter intubation time in patients with apparent DA has frequently been reported [65,66]. Figure 7 shows an example of styletubation conducted in a patient with seemingly normal airway during routine endotracheal intubation on daily basis in the operating rooms. The time to intubation (defined as “from lip to trachea”) in this patient is only 4 s. It is worthy to mention here that the shorter time to intubation should be only used as an auxiliary outcome parameter in such comparative clinical studies. Namely, the first-pass success rate and subjective easiness are more meaningful clinical outcome parameters. The faster intubation time (e.g., 3 s to 5s) should not be taken as the best quality and safety indicator for endotracheal intubation. Instead, a smooth working flow, including the checkpoint of the signposts along airway path, and final looking around the corner, should be the prime consideration in both normal straightforward airway and predicted difficult airway management.Figure 8 shows such an example that a smooth and entire check of all the sign posts along the airway before accomplishing the endotracheal intubation within a reasonable and acceptable time frame (30 s in this demonstration).
Any conventionally trained airway operator might experience or encounter the DA situations on daily basis. Failed to identify DA in advance and without plan-B or even plan-C for emergency airway management can lead to a disastrous outcome [67]. Among all the available clinical tests to predict DA, the upper lip bite test (ULBT) showed the most favorable diagnostic test accuracy properties [68]. The advantageous role of VL in patients with difficult airway, e.g., Pierre-Robin syndrome, has been reported [69,70]. Figure 9 demonstrates a valid and useful application of styletubation technique in an obese patient with predicted DA scenario. This patient suffered morbid obesity and severe snoring. During styletubation, it is obvious that the collapsed airway, omega-shaped epiglottis, and LQS grade 2 glottis visibility were observed. Enlarged and hypertrophic ventricular folds (i.e., false vocal folds or plica ventricularis, folds of mucous membrane located above the true vocal folds in the larynx) were observed to compress the true vocal cords and interfere the opening of true vocal cords (Figure 9E–G). Under styletubation, such hypertrophic plica ventricularis did not cause any difficulties for subsequent endotracheal intubation (Figure 9H). The intubating time was 30 s with first-pass success.
Figure 10 shows a patient with difficulty swallowing, hoarseness, and stridor due to concurrent chemoradiotherapy (CCRT) to treat his nasopharyngeal carcinoma (NPC) diagnosed 6 months ago. For this admission, he underwent functional endoscopic sinus surgery (FESS) under general anesthesia. The styletubation was smooth, and with first-pass success (intubating time: 38 s), even the patient’s upper airway structures were so edematous and swollen that glottic visualization was almost impossible (Figure 10D–G). The percentage of glottic opening (POGO) was zero (Figure 10H).
Figure 11 shows the clinical performance and applicability of the styletubation in a variety of DA scenarios. Figure 11A shows a 26-year-old man (158 cm, 52 kg, body mass index [BMI] 20.8 kg/m2) with giant cemento-ossifying fibroma. The tumor was extensive (14 cm × 11 cm × 10 cm in size) and invaded the left eye, nose, paranasal sinus, maxilla, and oral cavity, the flexible fiberoptic intubation through the nasotracheal path was impossible. An awake surgical tracheostomy was refused by the patient as the first choice. After careful evaluation of the airway and ventilation status, oral tracheal intubation with the styletubation technique was performed and succeeded (intubating time: 24 s).
Moderate to severe OSA and tonsillar hypertrophy/enlargement are reported to be associated with high risk of DA [71-73]. Figure 11B shows a man (BMI 32.1 kg/m2) of grade-3 tonsillar hypertrophy and OSAS (obstructive sleep apnea syndrome) for tonsillectomy and uvulopalatopharyngoplasty (UPPP). Styletubation for oro-tracheal intubation was performed smoothly and effectively in this patient (intubating time: 20 s). In Figure 11C, a 42-year-old woman (BMI 28.8 kg/m2) displayed prominent (buck) teeth with poor ULBT grade underwent laryngomicrosurgery (LMS) for removal of vocal polyps. In contrast to the potential dental injury by laryngoscopy [74,75], the buck teeth or receding chin (retrognathia) did not cause any difficulties for the performance of styletubation (24 s).
In obese patient populations, DA has been expected due to their unique predictive parameters (e.g., MMT score, thyromental distance, ratio of neck circumference/thyromental distance) [76,77]. Single or in combination of these DA risk factors have been regarded as more predictive than their individual counterparts. Figure 11D demonstrates the application of styletubation in an obese patient undergoing bariatric surgery (a 41-year-old woman with BMI: 64.0 kg/m2). The short sternomental distance (SMD) and grade-3 Cormack-Lehane glottis exposure did not cause any difficulties and neither prevent the smooth and easy performance of styletubation in such patient (intubating time: 11 s). Ankylosing spondylitis might affect cervical spine mobility and caused DA during laryngoscopy [78-81]. Figure 11E shows a 61-year-old man with BMI: 27.4 kg/m2) with ankylosing spondylitis (AS) underwent LMS due to hypopharyngeal carcinoma. The intubation process was smooth and easy (intubating time: 30 s), similar to the results in the previous clinical reports [82].
Similarly, restricted cervical spine mobility occurred in those undergoing cervical spine surgery wearing cervical collar and regarded as a difficult airway scenario (Figure 11F). The performance of styletubation was smooth and swift as expected in this 64-year-old womant (BMI: 24.6 kg/m2; intubating time: 12 s). It should be mentioned that the roles of VL in the difficult airway scenarios involving morbid obesity-bariatric surgery and severely restricted cervical spine mobility has already been long discussed [83-89]. In contrast, the performance of styletubation in scenarios has only recently been called into attention [90-96].
The roles of VL for placement of a double-lumen endobronchial tube (DLEBT) for one-lung ventilation have long been discussed [97-101]. It has also recently been demonstrated that styletubation is useful for such clinical purpose [102-105]. We also applied styletubation as a routine first-line intubating modality for such DLEBT intubation for one-lung ventilation on daily basis. Figure 11G shows that a 35-Fr DLEBT was placed with styletubation technique in a 47-year-old woman with BMI: 18.0 kg/m2 underwent single-port video-assisted thoracoscopic surgery. The intubating time was 24 s.
During pediatric airway management, it has been known that multiple intubation attempts and persistence with DL for endotracheal intubation are the serious risk factors for related complications in children with DA events [106,107]. Although the beneficial roles of VL have continuously been demonstrated in certain adult patients, such superiority over DL has not consistently been demonstrated in pediatric patients [108]. Even with improving glottis visualization in pediatric patients without predicted DA, VL is at the expense of prolonged intubation time and increased failure rates in comparison to DL [109]. Interestingly, in pediatric patients with DA scenarios, VL had the same intubation failure rates and intubation time as DL [110]. In neonates and infants, VL with standard blades in combination with supplemental oxygen might have better first-attempt rate of tracheal intubation than the performance of DL [111,112]. Similar beneficial effectiveness (higher first-attempt success rates) of VL for urgent intubation of newborn infants was observed [113]. Amazingly, the video stylet technique has long been applied in pediatric patients [36,114]. Such styletubation technique has been routinely applied in the pediatric patient populations in our medical institution. Figure 11H demonstrates such an example (An 11-year-old boy with BMI: 16.2 kg/m2 underwent emergency laparoscopic appendectomy). Intubating time was --- smooth with first-pass success.
In anesthetized adult patients who underwent dental, oral, maxillofacial, or head and neck cancer surgery, the advantages of use of VL for nasotracheal intubation include a shorter intubation time, better glottis views, similar first-pass success rates, and less use of Magill forceps and the BURP maneuver (backward, upward, rightward, and posterior pressure on the larynx) [115]. In contrast to the roles of FOB and VL for nasotracheal intubation, the video stylet technique required significantly shorter intubation time and fewer airway-assisted maneuvers in adult patients undergoing head and neck surgery [116-118]. Similar application of video stylet for nasotracheal intubation has recently been reported [119-121]. Figure 11I shows the application of styletubation for nasotracheal intubation in a 67-year-old woman (BMI: 23.8 kg/m2) undergoing oral and maxillofacial surgery due to medication-related osteonecrosis of jaw (MRONJ). Her past history included recurrent and metastatic breast cancer with thoracic spines metastasis. The intubating time was 30 s with first-pass success.
Patients undergoing head and neck reconstructive surgeries usually present significant challenges on endotracheal intubation, especially with the anticipated higher incidence of DA scenarios (e.g., scar contracture with a reconstructed flap over the neck, pharyngo-laryngeal cancer) [122,123]. Figure 11J shows retromolar styletubation technique in a 63-year-old man with buccal cancer and prior reconstructive flap surgery. Although the DA was anticipated (limited mouth opening) and not applicable for laryngoscopy, the styletubation procedure was smooth and first-pass success (intubating time: 20 s). Similarly, patients undergoing oral cancer surgery usually display multiple predictors of anticipated DA for general anesthesia and present unique challenges [124]. Conventional airway management technique (e.g., laryngoscopy) may not reliably achieve endotracheal intubation where intubation has already failed after several attempts. Utilization of several other advanced airway management techniques for tracheal intubation has been recommended [125]. In Figure 11K, styletubation technique was applied in a 46-year-old man (BMI: 19.5 kg/m2) with lower gum cancer and severe trismus (less than 2 cm mouth opening). The styletubation procedure was smooth with first-pass success (intubating time: 10 s). Not surprisingly, patients with oropharyngeal/laryngeal cancers receiving head/neck radiotherapy (HNRT) may face significant threats and risks to airway management during tracheal intubation. While previous treatment with HNRT was not always associated with additional risk of DA, MMT score may be a sensitive predictor in this patient population [126]. Endotracheal intubation with VL after induction of general anesthesia can be a feasible alternative for managing DA in patients with supraglottic masses [127,128]. Instead, styletubation also plays a vital role in such patient population during airway management [65,129]. Figure 11L shows a 57-year-old man with recurrent hypopharyngeal squamous cell carcinoma (cT4N3B, stage IVB) undergoing elective tracheostomy and laparoscopic Stamm gastrostomy. Even with the help of styletubation technique, it was still challenging when the airway was occupied by the tumor lesions, soft tissue swelling, and copious secretions in such patient population. The styletubation procedure was timely and smooth with first-pass success (intubating time: 38 s)
A plethora of clinical studies have demonstrated VL (i.e., optimal glottic visualization by a video monitoring) is advantageous on the learning curve for airway novices practitioners and trainees, both for the simulated easy and difficult laryngoscopy scenarios [130-137]. Similar to the issues of DL/VL, the learning curves and performance for novices/trainees on the skills of styletubation have also been studied [138-141]. In our medical institute, we provided the novices/trainees (medical students, post-graduate doctors, residents) a full-scale training curriculum and hands-on courses. After completing the introductory courses (airway mannequins and cadavers), the novices/trainees had a bed-side observation opportunity. And then, starting from the second week of training in the operating rooms, the trainees had the chances to try the styletubation in patients with seemingly easy airway conditions under the supervision of an experienced anesthesiologist. Figure 12 shows two individual examples of the trainees on learning the styletubation. An undergraduate student (clerk) had a shallow learning curve with first-pass success rate of 26.6%. In contrast, a post-graduate year-2 doctor (PGY-2) had an outstanding performance with first-pass success rate of 87.5%.
5. Discussion
Although airway management is mostly uncomplicated and uneventful, the clinical situations can swiftly deteriorate and finally result in patient harm and mishap. During the last two decades, the role of VL has often been shown to be superior over that of DL, based on the commonly applied comparators such as first-pass intubating success rate, failed intubation rate, intubating time, laryngeal visualization, airway-related complications, operators’ subjective satisfaction, learning curve, etc. [142,143]. While the better performance of VL has been reported to serve as a rescue airway device in DA scenarios and in critically ill patients [21,144,145], a first-intention technique with VL as the routine airway management option is still a pro-con debate [146-149].
The defects and limitations of laryngoscopy, which might partially attribute to the DA, sometimes cause difficulty acquiring an optimal oro-pharyngeal space, imperfect glottic visualization, difficulty advancing and placing the ET tube into trachea, etc. With same advantages of VL, the new intubating technique with video-assisted intubating stylets (i.e., styletubation), however did not require a direct line of sight (e.g., axes of alignment theory). Above all, the styletubation might be performed under the condition that the exposure of oropharyngeal space is restricted (e.g., oral-facial tumor, tumor around neck region, cervical spine immobility, morbid obesity, etc.). The general comparative features and characteristics between laryngoscopy and styletubation are listed in the Table 2.

Table 2.
Comparison between (video)laryngoscopy, flexible fiberoptic endoscope, and styletubation.
| Laryngoscopy | FOB | Styletubation | |
|---|---|---|---|
| Require wide enough mouth-opening | +++ | - | + |
| Require displacing the tongue to expose glottis | +++ | + | + |
| Require high-grade Cormack-Lehane score | +++ | - | - |
| Need a blade | Yes | No | No |
| Need a stylet | Sometimes | No | No |
| Good POGO score | Sometimes | Always | Always |
| External laryngeal maneuvers are helpful | Often | No | Occasionally |
| Maneuverability along the airway path | Limited | High | High |
| First-pass success rate | Moderate to high | Excellent | Excellent |
| Overall success rate | Moderate to high | High | High |
| Time to intubate | Moderate | Long | Swift |
| Subjective feeling of easiness to operate | Acceptable | Varied | Excellent |
| Impinge on arytenoid / vocal cords | Sometimes | Often | Rare |
| Dental damage/soft tissue injuries | Sometimes | Seldom | Rare |
| Impacted by secretions/blood/vomitus | Yes | Yes | Yes |
| Over-stimulation on airway | Often | Less | Much less |
| Require an adjunctive tool | Sometimes | Sometimes | Seldom |
| Learning curve | Reasonable | Slow | Steep |
| Affordability | Yes | Expensive | Yes |
| Availability | Yes | Limited | Yes |
| Speedy preparedness, easy maintenance | Yes | No | Yes |
| Applicability to awake or asleep intubation | Yes | Yes | Yes |
| Real time imaging/video recording/documenting | Yes | Yes | Yes |
Table 3.
Performance of styletubation in the real world airway scenarios.
| Easy Airway | Difficult Airway | |
|---|---|---|
| Laryngeal view | Always excellent | Could be difficult |
| First-pass success rate | Near 100% | Acceptable |
| Overall success rate | Near 100% | Acceptable |
| Intubating time (routine operation) | 3 sec to 10 sec | 30 sec to 120 sec |
| Intubating time (for demonstration purpose) | 30 sec to 60 sec | NA |
| Hypoxemia | Very rare | Depends |
| Airway injuries | Very rare | Acceptable |
| Learning curve | 20% to 90% | - |
| Awake/asleep intubation | NA | Applicable |
| Combined with laryngoscopy | NA | Applicable |
While the comparison has always been made between DL and VL, we present our own clinical experiences of styletubation in various airway management conditions, including normal and predicted difficult airway scenarios (Figure 4 ~ Figure 11). Basically, there are two main technical advantages of using styletubation for endotracheal intubation. One is the ease to acquire clear glottis view and the other is the ease to advance the ET tube into trachea. With these two strengths of styletubation, the adopted clinical performance indicators are outstanding.
The Bonfils endoscope is a prototype of such device as a rigid and straight fiberoptic stylet with a 40-degree curved tip, originally designed for a retromolar approach in pediatric DA scenarios (e.g., Pierre Robin syndrome) [42]. With the advantages as both optical and slim stylet shaped, which provides clear visualization and better maneuverability along the course of airway, such product design became promising and useful for difficult and normal airway [36,150]. Similar to other optic intubating tools, the common pitfalls and limitations of applying such kind of tools (VL or video stylets) include impacts from fogging, soft tissue contact, or secretions/blood stained the lens and therefore obscured the laryngeal views [42]. We therefore emphasize the role of proper suction along the airway to adequately clear the airway be crucial for styletubation. Another pitfall during the styletubation procedure is inadequate or difficulty lifting patient’s epiglottis and therefore failed to acquire a clear glottis visualization for subsequent entry of the ET tube into trachea. In order to make sure to get enough space between the epiglottis and posterior pharyngeal wall, the following technical tips are useful. Namely, (1) effectively conducting maneuvers of jaw-thrust and mouth-opening by an airway assistant; (2) lifting up patient’s mandible using the Shikani technique; (3) using laryngoscope blade to facilitate lifting up the epiglottis; and (4) using a soft nasal airway tube as a lead conduit to pass the stylet-ET tube unit underneath the epiglottis [151].
6. The Future Perspective
The total annual number of airway management clinical studies has increased over time during the last two decades. Meanwhile, several ethics concerns of study designs of such research purposes have been noted during the course [152]. In addition to the roles of animal/bench models, human cadavers, manikins, the acceptable ethics consensus guidelines for human airway management research have been proposed [153]. Not surprising, the ethics boundaries include the restricted inclusion criteria to recruit study participants only in ASA status 1–2, excluding those with past history of DA or potentially/predicted difficult airways, limiting the number of trial attempts at securing the study subject’s airway, etc. Recent clinical results suggest that VL may be a preferable approach for intubating patients undergoing surgical procedures in the operating rooms [30]. Interestingly, the clinical experience of styletubation has recently been reported [66,154-156]. Our local clinical experiences applying styletubation as the routine first-line tracheal intubation modality are unique (63537 cases from 2016 to 2024) and show excellent performance/outcome indicators (i.e., first-attempt success rate, intubating time, failed intubation rate, complications, etc.). However, large-scale prospective head-to-head clinical comparative studies, regarding the evidence of clinical effectiveness and safety of styletubation against laryngoscopy, are still awaiting.
7. Conclusions
With our own local vast experiences since 2016, styletubation has already revolutionized the concept and empowered practice for airway management, and significantly improve patient clinical outcomes and safety. The striking objective evidence for its clinical benefits and advantages over laryngoscopy is ever-increasing and repeatedly demonstrated as a basic standard of care for tracheal intubation since then. We have presented that the universal full-scale adoption of styletubation into our local routine clinical practice as the first-line airway management technique instead of laryngoscopy. However, future large-sized prospective clinical trials results to support such notion are still demanding and awaiting. Continuously improving clinical demonstration, education and hands-on training of the concept and technique of styletubation are not only fundamentally useful in achieving a widespread awareness of its superiority, but also crucial in maximizing its clinical effectiveness and ensuring its sustained and ubiquitous clinical utilization in the near future.
References
- Burkle, C.M.; Zepeda, F.A.; Bacon, D.R.; Rose, S.H. A historical perspective on use of the laryngoscope as a tool in anesthesiology. Anesthesiology 2004, 100, 1003–1006. [Google Scholar] [CrossRef]
- Szmuk, P.; Ezri, T.; Evron, S.; Roth, Y.; Katz, J. A brief history of tracheostomy and tracheal intubation, from the Bronze Age to the Space Age. Intensive Care Med. 2008, 34, 222–228. [Google Scholar] [CrossRef] [PubMed]
- Pieters, B.M.; Eindhoven, G.B.; Acott, C.; van Zundert, A.A. Pioneers of laryngoscopy: indirect, direct and video laryngoscopy. Anaesth. Intensive Care 2015, 43, Suppl–4. [Google Scholar] [CrossRef] [PubMed]
- Pepe, P.E.; Copass, M.K.; Joyce, T.H. Prehospital endotracheal intubation: rationale for training emergency medical personnel. Ann. Emerg. Med. 1985, 14, 1085–1092. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.E.; Yealy, D.M. Out-of-hospital endotracheal intubation: where are we? Ann. Emerg. Med. 2006, 47, 532–541. [Google Scholar] [CrossRef]
- Savino, P.B.; Reichelderfer, S.; Mercer, M.P.; Wang, R.C.; Sporer, K.A. Direct versus video laryngoscopy for prehospital intubation: A systematic review and meta-analysis. Acad. Emerg. Med. 2017, 24, 1018–1026. [Google Scholar] [CrossRef]
- Benger, J.R.; Kirby, K.; Black, S.; Brett, S.J.; Clout, M.; Lazaroo, M.J.; Nolan, J.P.; Reeves, B.C.; Robinson, M.; Scott, L.J.; Smartt, H.; South, A.; Stokes, E.A.; Taylor, J.; Thomas, M.; Voss, S.; Wordsworth, S.; Rogers, C.A. Effect of a strategy of a supraglottic airway device vs tracheal intubation during out-of-hospital cardiac arrest on functional outcome: The AIRWAYS-2 Randomized Clinical Trial. JAMA. 2018, 320, 779–791. [Google Scholar] [CrossRef]
- Lee, A.F.; Chien, Y.C.; Lee, B.C.; Yang, W.S.; Wang, Y.C.; Lin, H.Y.; Huang, E.P.; Chong, K.M.; Sun, J.T.; Huei-Ming, M.; Hsieh, M.J.; Chiang, W.C. Effect of placement of a supraglottic airway device vs endotracheal intubation on return of spontaneous circulation in adults with out-of-hospital cardiac arrest in Taipei, Taiwan: A cluster randomized clinical trial. JAMA. Netw. Open. 2022, 5, e2148871. [Google Scholar] [CrossRef]
- Magill, I.W. Endotracheal anesthesia. Am. J. Surg. 1936, 34, 450–455. [Google Scholar] [CrossRef]
- Macintosh, R.R. A new laryngoscope. Lancet 1943, 241, 205. [Google Scholar] [CrossRef]
- Bannister, F.B.; Macbeth, R.G. Direct laryngoscopy and tracheal intubation. Lancet 1944, 244, 651–654. [Google Scholar] [CrossRef]
- Mulcaster, J.T.; Mills, J.; Hung, O.R.; MacQuarrie, K.; Law, J.A.; Pytka, S.; Imrie, D.; Field, C. Laryngoscopic intubation: learning and performance. Anesthesiology 2003, 98, 23–27. [Google Scholar] [CrossRef] [PubMed]
- Hindman, B.J.; Santoni, B.G.; Puttlitz, C.M.; From, R.P.; Todd, M.M. Intubation biomechanics: laryngoscope force and cervical spine motion during intubation with Macintosh and Airtraq laryngoscopes. Anesthesiology 2014, 121, 260–271. [Google Scholar] [CrossRef] [PubMed]
- Schmutz, A.; Breddin, I.; Draxler, R.; Schumann, S.; Spaeth, J. Comparison of force distribution during laryngoscopy with the C-MAC D-blade and Macintosh-style blades: A randomised controlled clinical trial. J. Clin. Med. 2024, 13, 2623. [Google Scholar] [CrossRef]
- Nørskov, A.K.; Rosenstock, C.V.; Wetterslev, J.; Astrup, G.; Afshari, A.; Lundstrøm, L.H. Diagnostic accuracy of anaesthesiologists' prediction of difficult airway management in daily clinical practice: a cohort study of 188064 patients registered in the Danish Anaesthesia Database. Anaesthesia 2015, 70, 272–281. [Google Scholar] [CrossRef]
- Endlich, Y.; Lee, J.; Culwick, M.D. Difficult and failed intubation in the first 4000 incidents reported on webAIRS. Anaesth. Intensive Care 2020, 48, 477–487. [Google Scholar] [CrossRef]
- Yuan, J.; Ye, H.; Tan, X.; Zhang, H.; Sun, J. Determinants of difficult laryngoscopy based on upper airway indicators: a prospective observational study. BMC Anesthesiol. 2024, 24, 157. [Google Scholar] [CrossRef]
- Schnittker, R.; Marshall, S.D.; Berecki-Gisolf, J. Patient and surgery factors associated with the incidence of failed and difficult intubation. Anaesthesia 2020, 75, 756–766. [Google Scholar] [CrossRef]
- Ruderman, B.T.; Mali, M.; Kaji, A.H.; Kilgo, R.; Watts, S.; Wells, R.; Limkakeng, A.T.; Borawski, J.B.; Fantegrossi, A.E.; Walls, R.M.; Brown, C.A. 3rd.; National Emergency Airway Registry investigators. Direct vs video laryngoscopy for difficult airway patients in the emergency department: A National Emergency Airway Registry Study. West. J. Emerg. Med. 2022, 23, 706–715. [Google Scholar] [CrossRef]
- Joffe, A.M.; Aziz, M.F.; Posner, K.L.; Duggan, L.V.; Mincer, S.L.; Domino, K.B. Management of difficult tracheal intubation: A closed claims analysis. Anesthesiology 2019, 131, 818–829. [Google Scholar] [CrossRef]
- Apfelbaum, J.L.; Hagberg, C.A.; Connis, R.T.; Abdelmalak, B.B.; Agarkar, M.; Dutton, R.P.; Fiadjoe, J.E.; Greif, R.; Klock, P.A.; Mercier, D.; Myatra, S.N.; O'Sullivan, E.P.; Rosenblatt, W.H.; Sorbello, M.; Tung, A. 2022 American Society of Anesthesiologists practice guidelines for management of the difficult airway. Anesthesiology 2022, 136, 31–81. [Google Scholar] [CrossRef] [PubMed]
- Paolini, J.B.; Donati, F.; Drolet, P. Review article: video-laryngoscopy: another tool for difficult intubation or a new paradigm in airway management? Can. J. Anaesth. 2013, 60, 184–191. [Google Scholar] [CrossRef] [PubMed]
- Hansel, J.; Rogers, A.M.; Lewis, S.R.; Cook, T.M.; Smith, A.F. Videolaryngoscopy versus direct laryngoscopy for adults undergoing tracheal intubation. Cochrane Database Syst. Rev. 2022, 4(4):CD011136. [CrossRef]
- Greenland, K.B.; Eley, V.; Edwards, M.J.; Allen, P.; Irwin, M.G. The origins of the sniffing position and the three axes alignment theory for direct laryngoscopy. Anaesth. Intensive Care 2008, 36, 23–27. [Google Scholar] [CrossRef] [PubMed]
- Greenland, K.B. Two curves and three columns–A reappraisal of direct laryngoscopy. Operative Techniques in Otolaryngology-Head and Neck Surgery 2020, 31, 83–88. [Google Scholar] [CrossRef]
- Aziz, M.F.; Bayman, E.O.; Van Tienderen, M.M.; Todd, M.M. StAGE Investigator Group; Brambrink, A.M. Predictors of difficult videolaryngoscopy with GlideScope® or C-MAC® with D-blade: secondary analysis from a large comparative videolaryngoscopy trial. Br. J. Anaesth. 2016, 117, 118–123. [Google Scholar] [CrossRef]
- Aziz, M.F.; Abrons, R.O.; Cattano, D.; Bayman, E.O.; Swanson, D.E.; Hagberg, C.A.; Todd, M.M.; Brambrink, A.M. First-attempt intubation success of video laryngoscopy in patients with anticipated difficult direct laryngoscopy: A multicenter randomized controlled trial comparing the C-MAC D-blade versus the GlideScope in a mixed provider and diverse patient population. Anesth. Analg. 2016, 122, 740–750. [Google Scholar] [CrossRef]
- Cooper, R.M.; Pacey, J.A.; Bishop, M.J.; McCluskey, S.A. Early clinical experience with a new videolaryngoscope (GlideScope) in 728 patients. Can. J. Anaesth. 2005, 52, 191–198. [Google Scholar] [CrossRef]
- Saul, S.A.; Ward, P.A.; McNarry, A.F. Airway management: The current role of videolaryngoscopy. J. Pers. Med. 2023, 13, 1327. [Google Scholar] [CrossRef]
- Ruetzler, K.; Bustamante, S.; Schmidt, M.T.; Almonacid-Cardenas, F.; Duncan, A.; Bauer, A.; Turan, A.; Skubas, N.J.; Sessler, D.I.; Collaborative VLS Trial Group. Video laryngoscopy vs direct laryngoscopy for endotracheal intubation in the operating room: A cluster randomized clinical trial. JAMA. 2024, 331, 1279–1286. [Google Scholar] [CrossRef]
- Prekker, M.E.; Driver, B.E.; Trent, S.A.; Resnick-Ault, D.; Seitz, K.P.; Russell, D.W.; Gaillard, J.P.; Latimer, A.J.; Ghamande, S.A.; Gibbs, K.W.; Vonderhaar, D.J.; Whitson, M.R.; Barnes, C.R.; Walco, J.P.; Douglas, I.S.; Krishnamoorthy, V.; Dagan, A.; Bastman, J.J.; Lloyd, B.D.; Gandotra, S,; Goranson, J.K.; Mitchell, S.H.; White, H.D.; Palakshappa, J.A.; Espinera, A.; Page, D.B.; Joffe, A.; Hansen, S.J.; Hughes, C.G.; George, T.; Herbert, J.T.; Shapiro, N.I.; Schauer, S.G.; Long, B.J.; Imhoff, B.; Wang, L.; Rhoads, J.P.; Womack, K.N.; Janz, D.R.; Self, W.H.; Rice, T.W.; Ginde, A.A.; Casey, J.D.; Semler, M.W.; DEVICE Investigators and the Pragmatic Critical Care Research Group. Video versus direct laryngoscopy for tracheal intubation of critically ill adults. N. Engl. J. Med. 2023, 389, 418-429. [CrossRef]
- Prekker, M.E.; Trent, S.A.; Lofrano, A.; Russell, D.W.; Barnes, C.R.; Brewer, J.M.; Doerschug, K.C.; Gaillard, J.P.; Gandotra, S.; Ginde, A.A.; Ghamande, S.; Gibbs, K.W.; Hughes, C.G.; Janz, D.R.; Khan, A.; Mitchell, S.H.; Page, D.B.; Rice, T.W.; Self, W.H.; Smith, L.M.; Stempek, S.B.; Vonderhaar, D.J.; West, J.R.; Whitson, M.R.; Casey, J.D.; Semler, M.W.; Driver, B.E. Laryngoscopy and tracheal intubation: Does use of a video laryngoscope facilitate both steps of the procedure? Ann. Emerg. Med. 2023, 82, 425–431. [Google Scholar] [CrossRef]
- Sgalambro, F.; Sorbello, M. Videolaryngoscopy and the search for the Holy Grail. Br. J. Anaesth. 2017, 118, 471–472. [Google Scholar] [CrossRef] [PubMed]
- Guo, N.; Wen, X.; Wang, X.; Yang, J.; Zhou, H.; Guo, J.; Su, Y.; Zhang, T. Comparison of outcomes between video laryngoscopy and flexible fiberoptic bronchoscopy for endotracheal intubation in adults with cervical neck immobilization: A systematic review and meta-analysis of randomized controlled trials. PLoS. One 2024, 19, e0313280. [Google Scholar] [CrossRef] [PubMed]
- Hu, H.Z.; Cheng, X.X.; Zhang, T.; Zhang, G.L.; Zhang, G.J.; Wu, W.W.; Li, R.H. A visual laryngoscope combined with a fiberoptic bronchoscope improves intubation outcomes in patients with predicted difficult airways in thoracic surgery. BMC. Pulm. Med. 2024, 24, 558. [Google Scholar] [CrossRef]
- Shikani, A.H. New "seeing" stylet-scope and method for the management of the difficult airway. Otolaryngol. Head Neck Surg. 1999, 120, 113–116. [Google Scholar] [CrossRef] [PubMed]
- Matek, J.; Kolek, F.; Klementova, O.; Michalek, P.; Vymazal, T. Optical devices in tracheal intubation-State of the art in 2020. Diagnostics (Basel) 2021, 11, 575. [Google Scholar] [CrossRef]
- Hung, O.R.; Pytka, S.; Morris, I.; Murphy, M.; Launcelott, G.; Stevens, S.; MacKay, W.; Stewart, R.D. Clinical trial of a new lightwand device (Trachlight) to intubate the trachea. Anesthesiology 1995, 83, 509–514. [Google Scholar] [CrossRef]
- Agrò, F.; Hung, O.R.; Cataldo, R.; Carassiti, M.; Gherardi, S. Lightwand intubation using the Trachlight: a brief review of current knowledge. Can. J. Anaesth. 2001, 48, 592–599. [Google Scholar] [CrossRef]
- Hung, O. Why can't I get a Trachlight™? Can. J. Anaesth. 2025, 72, 230–232. [Google Scholar] [CrossRef]
- Kitamura, T.; Yamada, Y.; Du, H.L.; Hanaoka, K. Efficiency of a new fiberoptic stylet scope in tracheal intubation. Anesthesiology 1999, 91, 1628–1632. [Google Scholar] [CrossRef]
- Thong, S.Y.; Wong, T.G. Clinical uses of the Bonfils retromolar intubation fiberscope: a review. Anesth. Analg. 2012, 115, 855–866. [Google Scholar] [CrossRef]
- Godai, K.; Moriyama, T.; Kanmura, Y. Comparison of the MultiViewScope stylet scope and the direct laryngoscope with the Miller blade for the intubation in normal and difficult pediatric airways: A randomized, crossover, manikin study. PLoS. One 2020, 15, e0237593. [Google Scholar] [CrossRef] [PubMed]
- Nabecker, S.; Ottenhausen, T.; Theiler, L.; Braun, M.; Greif, R.; Riva, T. Prospective observational study evaluating the C-MAC video stylet for awake tracheal intubation: a single-center study. Minerva Anestesiol. 2021, 87, 873–879. [Google Scholar] [CrossRef] [PubMed]
- Luk HN, Luk HN, Qu JZ, Shikani A. A paradigm shift of airway management: the role of video-assisted intubating stylet technique. In: Lovich-Sapola J, ed. Advances in Tracheal Intubation [Working Title]. London: Inte-chOpen [Internet]; 2022. [CrossRef]
- Luk HN, Qu JZ, Shikani A. Styletubation: The paradigmatic role of video-assisted intubating stylet technique for routine tracheal intubation. Asian J Anesthesiol. 2023;61(2):102-106. [CrossRef]
- Luk HN, Qu JZ, Shikani A. Styletubation for routine tracheal intubation for ear-nose-throat surgical procedures. Annal of Otol Head and Neck Surg. 2023;2(3):1-13.
- Luk, HN.; Qu, JZ. Styletubation versus laryngoscopy: A new paradigm for routine tracheal intubation. Surgeries. 2024;5,135-161. [CrossRef]
- Lee HC, Wu BG, Chen BC, Luk HN, Qu JZ. Structured routine use of styletubation for oro-tracheal intubation in obese patients undergoing bariatric surgeries—A case series report. Healthcare (Basel). 2024;12,1404. [CrossRef]
- Cortellazzi, P.; Caldiroli, D.; Byrne, A.; Sommariva, A.; Orena, E.F.; Tramacere, I. Defining and developing expertise in tracheal intubation using a GlideScope(®) for anaesthetists with expertise in Macintosh direct laryngoscopy: an in-vivo longitudinal study. Anaesthesia 2015, 70, 290–295. [Google Scholar] [CrossRef] [PubMed]
- Halligan, M.; Charters, P. A clinical evaluation of the Bonfils intubation fibrescope. Anaesthesia 2003, 58, 1087–1091. [Google Scholar] [CrossRef]
- Jiang, L.; Qiu, S.; Zhang, P.; Yao, W.; Chang, Y.; Dai, Z. The midline approach for endotracheal intubation using GlideScope video laryngoscopy could provide better glottis exposure in adults: a randomized controlled trial. BMC. Anesthesiol. 2019, 19, 200. [Google Scholar] [CrossRef]
- Karamchandani, K.; Nasa, P.; Jarzebowski, M.; Brewster, D.J.; De Jong, A.; Bauer, P.R.; Berkow, L.; Brown, C.A. 3rd.; Cabrini, L.; Casey, J.; Cook, T.; Divatia, J.V.; Duggan, L.V.; Ellard, L.; Ergan, B.; Jonsson Fagerlund, M,; Gatward, J.; Greif, R.; Higgs, A.; Jaber, S.; Janz, D.; Joffe, A.M.; Jung, B.; Kovacs, G.; Kwizera, A.; Laffey, J.G.; Lascarrou, J.B.; Law, J.A.; Marshall, S.; McGrath, B.A.; Mosier, J.M.; Perin, D.; Roca, O.; Rollé, A.; Russotto, V.; Sakles, J.C.; Shrestha, G.S.; Smischney, N.J.; Sorbello, M.; Tung, A.; Jabaley, C.S.; Myatra, S.N.; Society of Critical Care Anesthesiologists (SOCCA) Physiologically Difficult Airway Task Force. Tracheal intubation in critically ill adults with a physiologically difficult airway. An international Delphi study. Intensive Care Med. 2024, 50, 1563-1579. [CrossRef]
- Levitan, R.M. Design rationale and intended use of a short optical stylet for routine fiberoptic augmentation of emergency laryngoscopy. Am. J. Emerg. Med. 2006, 24, 490–495. [Google Scholar] [CrossRef]
- Chiu, W.C.; Wu, Z.F.; Lai, M.F.; Lai, H.C. Combination use of laryngoscope, jaw thrust, and Trachway for improving difficult tracheal intubation in obese. J. Med. Sci. 2022, 42, 197–198. [Google Scholar] [CrossRef]
- Bonilla González, A.I.; Rivas Alpuche, J.G.; Navarrete García, H.E.; Wong Salazar, L.H.; Atondo Laguna, C.M.; Avilés Sánchez, P.A. Successful intubation with a flexible optical stylet in a patient with predictors of difficult airway using pharyngeal clearance technique with a laryngoscope: A case report. Med. Int. (Lond). 2025, 5, 40. [Google Scholar] [CrossRef]
- Van Zundert, A.A.; Pieters, B.M. Combined technique using videolaryngoscopy and Bonfils for a difficult airway intubation. Br. J. Anaesth. 2012, 108, 327–328. [Google Scholar] [CrossRef]
- Jhuang, B.J.; Luk, H.N.; Qu, J.Z.; Shikani, A. Video-twin technique for airway management, combining video-intubating stylet with videolaryngoscope: A case series report and review of the literature. Healthcare (Basel) 2022, 10, 2175. [Google Scholar] [CrossRef]
- Villa, D.; Aspi, M.T.B.; Cruz, R.M.P. Combined use of C-MAC video laryngoscope and Bonfils intubating fiberscope in a pediatric patient with a huge laryngeal mass: A case report. Acta Medica Philippina 2022, 56. [Google Scholar] [CrossRef]
- Witkam, R.L.; Bruhn, J.; Hoogerwerf, N.; Koch, R.M.; van Eijk, L.T. Combining a McGrath video laryngoscope and C-MAC video stylet for the endotracheal intubation of a patient with a laryngeal carcinoma arising from the anterior side of the epiglottis: A case report. Anesth. Res. 2025, 2, 5. [Google Scholar] [CrossRef]
- Cormack, R.S.; Lehane, J. Difficult tracheal intubation in obstetrics. Anaesthesia 1984, 39, 1105–1111. [Google Scholar] [CrossRef] [PubMed]
- Krage, R.; van Rijn, C.; van Groeningen, D.; Loer, S.A.; Schwarte, L.A.; Schober, P. Cormack-Lehane classification revisited. Br. J. Anaesth. 2010, 105, 220–227. [Google Scholar] [CrossRef]
- Kriege, M. , Noppens, R.R.; Turkstra, T.; Payne, S.; Kunitz, O.; Tzanova, I.; Schmidtmann, I.; EMMA Trial Investigators Group. A multicentre randomised controlled trial of the McGrath™ Mac videolaryngoscope versus conventional laryngoscopy. Anaesthesia 2023, 78, 722–729. [Google Scholar] [CrossRef] [PubMed]
- Kriege, M.; Lang, P.; Lang, C.; Schmidtmann, I.; Kunitz, O.; Roth, M.; Strate, M.; Schmutz, A.; Vits, E.; Balogh, O.; Jänig, C. A comparison of the McGrath videolaryngoscope with direct laryngoscopy for rapid sequence intubation in the operating theatre: a multicentre randomised controlled trial. Anaesthesia 2024, 79, 801–809. [Google Scholar] [CrossRef] [PubMed]
- Tsay, P.J.; Yang, C.P.; Luk, H.N.; Qu, J.Z.; Shikani, A. Video-assisted intubating stylet technique for difficult intubation: A case series report. Healthcare (Basel) 2022, 10, 741. [Google Scholar] [CrossRef] [PubMed]
- Zhang, T.; Zhao, K.Y.; Zhang, P.; Li, R.H. Comparison of video laryngoscope, video stylet, and flexible videoscope for transoral endotracheal intubation in patients with difficult airways: a randomized, parallel-group study. Trials 2023, 24, 599. [Google Scholar] [CrossRef]
- Crawley, S.M.; Dalton, A.J. Predicting the difficult airway. BJA. Education 2015, 15, 253–257. [Google Scholar] [CrossRef]
- Roth, D.; Pace, N.L.; Lee, A.; Hovhannisyan, K.; Warenits, A.M.; Arrich, J.; Herkner, H. Airway physical examination tests for detection of difficult airway management in apparently normal adult patients. Cochrane Database Syst. Rev. 2018, 5, CD008874. [Google Scholar] [CrossRef]
- Kim, Y.; Kim, J.E.; Jeong, D.H.; Lee, J. Combined use of a McGrath® MAC video laryngoscope and Frova Intubating Introducer in a patient with Pierre Robin syndrome: A case report. Korean J. Anesthesiol. 2014, 66, 310–313. [Google Scholar] [CrossRef]
- Peterson, J.D.; Puricelli, M.D.; Alkhateeb, A.; Figueroa, A.D.; Fletcher, S.L.; Smith, R.J.H.; Kacmarynski, D.S.F. Rigid video laryngoscopy for intubation in severe Pierre Robin sequence: A retrospective review. Laryngoscope 2021, 131, 1647–1651. [Google Scholar] [CrossRef] [PubMed]
- Leong, S.M.; Tiwari, A.; Chung, F.; Wong, D.T. Obstructive sleep apnea as a risk factor associated with difficult airway management-A narrative review. J. Clin. Anesth. 2018, 45, 63–68. [Google Scholar] [CrossRef] [PubMed]
- Nagappa, M.; Wong, D.T.; Cozowicz, C.; Ramachandran, S.K.; Memtsoudis, S.G.; Chung, F. Is obstructive sleep apnea associated with difficult airway? Evidence from a systematic review and meta-analysis of prospective and retrospective cohort studies. PLoS. One 2018, 13, e0204904. [Google Scholar] [CrossRef] [PubMed]
- Seet, E.; Chung, F.; Wang, C.Y.; Tam, S.; Kumar, C.M.; Ubeynarayana, C.U.; Yim, C.C.; Chew, E.F.F.; Lam, C.K.M.; Cheng, B.C.P.; Chan, M.T.V. Association of obstructive sleep apnea with difficult intubation: Prospective multicenter observational cohort study. Anesth. Analg. 2021, 133, 196–204. [Google Scholar] [CrossRef]
- Neto, J.M.; Teles, A.R.; Barbosa, J.; Santos, O. Teeth damage during general anesthesia. J. Clin. Med. 2023, 12, 5343. [Google Scholar] [CrossRef]
- Chari, A.; Tejesh, C.A.; Sudarshan, K.S. ; TAScope-guided rapid sequence intubation of a case of retrognathia with a history of failed intubation. Saudi J. Anaesth. 2023, 17, 427–429. [Google Scholar] [CrossRef]
- De Jong, A.; Molinari, N.; Pouzeratte, Y.; Verzilli, D.; Chanques, G.; Jung, B.; Futier, E.; Perrigault, P.F.; Colson, P.; Capdevila, X.; Jaber, S. Difficult intubation in obese patients: incidence, risk factors, and complications in the operating theatre and in intensive care units. Br. J. Anaesth. 2015, 114, 297–306. [Google Scholar] [CrossRef]
- Thota, B.; Jan, K.M.; Oh, M.W.; Moon, T.S. Airway management in patients with obesity. Saudi J. Anaesth. 2022, 16, 76–81. [Google Scholar] [CrossRef]
- Ng, M.; Hastings, R.H. Successful direct laryngoscopy assisted by posture in a patient with ankylosing spondylitis. Anesth. Analg. 1998, 87, 1436–1437. [Google Scholar] [CrossRef]
- Saricicek, V.; Mizrak, A.; Gul, R.; Goksu, S.; Cesur, M. GlideScope video laryngoscopy use tracheal intubation in patients with ankylosing spondylitis: a series of four cases and literature review. J. Clin. Monit. Comput. 2014, 28, 169–172. [Google Scholar] [CrossRef] [PubMed]
- Lili, X.; Zhiyong, H.; Jianjun, S. A comparison of the GlideScope with the Macintosh laryngoscope for nasotracheal intubation in patients with ankylosing spondylitis. J. Neurosurg. Anesthesiol. 2014, 26, 27–31. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.C.; Lin, S.; He, H.F. Case report: double visualization intubation strategy for patients with ankylosing spondylitis. Front. Med. (Lausanne) 2022, 9, 659624. [Google Scholar] [CrossRef] [PubMed]
- Tsay, P.J.; Hsu, S.W.; Peng, H.C.; Wang, C.H.; Lee, S.W.; Lai, H.Y. Trachway intubating stylet for tracheal intubation in an ankylosing spondylitis patient undergoing total hip replacement under general anesthesia. Acta Anaesthesiol. Taiwan. 2011, 49, 159–161. [Google Scholar] [CrossRef]
- Ndoko, S.K.; Amathieu, R.; Tual, L.; Polliand, C.; Kamoun, W.; El Housseini, L.; Champault, G.; Dhonneur, G. Tracheal intubation of morbidly obese patients: a randomized trial comparing performance of Macintosh and Airtraq laryngoscopes. Br. J. Anaesth. 2008, 100, 263–268. [Google Scholar] [CrossRef]
- Hoshijima, H.; Denawa, Y.; Tominaga, A.; Nakamura, C.; Shiga, T.; Nagasaka, H. Videolaryngoscope versus Macintosh laryngoscope for tracheal intubation in adults with obesity: A systematic review and meta-analysis. J. Clin. Anesth. 2018, 44, 69–75. [Google Scholar] [CrossRef]
- Lee, J.M.; Lee, S.K.; Jang, M.; Oh, M.; Park, E.Y. A comparison of the effectiveness of the McCoy laryngoscope and the C-MAC D-blade video laryngoscope in obese patients. Medicina 2024, 60, 1285. [Google Scholar] [CrossRef]
- Suppan, L.; Tramèr, M.R.; Niquille, M.; Grosgurin, O.; Marti, C. Alternative intubation techniques vs Macintosh laryngoscopy in patients with cervical spine immobilization: systematic review and meta-analysis of randomized controlled trials. Br. J. Anaesth. 2016, 116, 27–36. [Google Scholar] [CrossRef]
- Dutta, K.; Sriganesh, K.; Chakrabarti, D.; Pruthi, N.; Reddy, M. Cervical spine movement during awake orotracheal intubation with fiberoptic scope and McGrath videolaryngoscope in patients undergoing surgery for cervical spine instability: A randomized control trial. J. Neurosurg. Anesthesiol. 2020, 32, 249–255. [Google Scholar] [CrossRef]
- Paik, H.; Park, H.P. Randomized crossover trial comparing cervical spine motion during tracheal intubation with a Macintosh laryngoscope versus a C-MAC D-blade videolaryngoscope in a simulated immobilized cervical spine. BMC. Anesthesiol. 2020, 20, 201. [Google Scholar] [CrossRef]
- Chaudery, H.; Hameed, H.; Sharif, Z.; Asinger, S.; McKechnie, A. Comparative efficacy of videolaryngoscopy and direct laryngoscopy in patients living with obesity: A meta-analysis. Cureus 2024, 16, e76558. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.K.; Kim, J.A.; Kim, C.S.; Ahn, H.J.; Yang, M.K.; Choi, S.J. Comparison of tracheal intubation with the Airway Scope or Clarus Video System in patients with cervical collars. Anaesthesia 2011, 66, 694–698. [Google Scholar] [CrossRef] [PubMed]
- Nam, K.; Lee, Y.; Park, H.P.; Chung, J.; Yoon, H.K.; Kim, T.K. Cervical spine motion during tracheal intubation using an Optiscope versus the McGrath videolaryngoscope in patients with simulated cervical immobilization: A prospective randomized crossover study. Anesth. Analg. 2019, 129, 1666–1672. [Google Scholar] [CrossRef]
- Yoon, H.K.; Lee, H.C.; Park, J.B.; Oh, H.; Park, H.P. McGrath MAC videolaryngoscope versus Optiscope video stylet for tracheal intubation in patients with manual inline cervical stabilization: A randomized trial. Anesth. Analg. 2020, 130, 870–878. [Google Scholar] [CrossRef]
- Park, J.W.; An, S.; Park, S.; Nahm, F.S.; Han, S.H.; Kim, J.H. Comparison of a new video intubation stylet and McGrath® MAC video laryngoscope for intubation in an airway manikin with normal airway and cervical spine immobilization scenarios by novice personnel: A randomized crossover study. Biomed. Res. Int. 2021, 2021, 4288367. [Google Scholar] [CrossRef]
- Hung, K.C.; Chang, Y.J.; Chen, I.W.; Lin, C.M.; Liao, S.W.; Chin, J.C.; Chen, J.Y.; Yew, M.; Sun, C.K. Comparison of video-stylet and video-laryngoscope for endotracheal intubation in adults with cervical neck immobilisation: A meta-analysis of randomised controlled trials. Anaesth. Crit. Care Pain Med. 2021, 40, 100965. [Google Scholar] [CrossRef]
- Chen, I.W.; Li, Y.Y.; Hung, K.C.; Chang, Y.J.; Chen, J.Y.; Lin, M.C.; Wang, K.F.; Lin, C.M.; Huang, P.W.; Sun, C.K. Comparison of video-stylet and conventional laryngoscope for endotracheal intubation in adults with cervical spine immobilization: A PRISMA-compliant meta-analysis. Medicine (Baltimore) 2022, 101, e30032. [Google Scholar] [CrossRef]
- Sanu, A.; Ahmed, S.M. A comparative study between video laryngoscope and video stylet for tracheal intubation in patients with simulated cervical fracture injury: A prospective randomised controlled study. Cureus 2024, 16, e66360. [Google Scholar] [CrossRef]
- Yoo, J.Y.; Park, S.Y.; Kim, J.Y.; Kim, M.; Haam, S.J.; Kim, D.H. Comparison of the McGrath videolaryngoscope and the Macintosh laryngoscope for double lumen endobronchial tube intubation in patients with manual in-line stabilization: A randomized controlled trial. Medicine (Baltimore) 2018, 97, e0081. [Google Scholar] [CrossRef]
- Huang, P.; Zhou, R.; Lu, Z.; Hang, Y.; Wang, S.; Huang, Z. GlideScope® versus C-MAC®(D) videolaryngoscope versus Macintosh laryngoscope for double lumen endotracheal intubation in patients with predicted normal airways: a randomized, controlled, prospective trial. BMC. Anesthesiol. 2020, 20, 119. [Google Scholar] [CrossRef]
- Rajagopal, S.; Gardner, R.N.; Swanson, E.; Kim, S.; Sondekoppam, R.; Ueda, K.; Hanada, S. Comparison of time to intubation of a double-lumen endobronchial tube utilizing C-MAC® versus GlideScope® versus Macintosh blade: A randomized crossover manikin study. Cureus 2023, 15, e50523. [Google Scholar] [CrossRef] [PubMed]
- Yao, W.; Li, M.; Zhang, C.; Luo, A. Recent advances in videolaryngoscopy for one-lung ventilation in thoracic anesthesia: A narrative review. Front. Med. (Lausanne) 2022, 9, 822646. [Google Scholar] [CrossRef] [PubMed]
- Maracaja, L.; Coffield, A.; Smith, L.D.; Bradshaw, J.D.; Saha, A.K.; McLauglin, C.S.; Templeton, T.W. A novel combined approach to placement of a double lumen endobronchial tube using a video laryngoscope and fiberoptic bronchoscope: a retrospective chart review. BMC. Anesthesiol. 2024, 24, 142. [Google Scholar] [CrossRef] [PubMed]
- Yang, M.; Kim, J.A.; Ahn, H.J.; Choi, J.W.; Kim, D.K.; Cho, E.A. Double-lumen tube tracheal intubation using a rigid video-stylet: a randomized controlled comparison with the Macintosh laryngoscope. Br. J. Anaesth. 2013, 111, 990–995. [Google Scholar] [CrossRef]
- Seo, H.; Lee, G.; Ha, S.I.; Song, J.G. An awake double lumen endotracheal tube intubation using the Clarus video system in a patient with an epiglottic cyst: a case report. Korean J. Anesthesiol. 2014, 66, 157–159. [Google Scholar] [CrossRef]
- Xu, T.; Li, M.; Guo, X.Y. Comparison of Shikani optical stylet and Macintosh laryngoscope for double-lumen endotracheal tube intubation. Beijing Da Xue Xue Bao Yi Xue Ban (in Chinese) 2015, 47, 853–857. [Google Scholar] [PubMed]
- Gu, Y.; Zhou, Q.; Zhou, H.; Liu, M.; Feng, D.; Wei, J.; Min, K.; Zhu, W.; Chen, Y.; Lv, X. A randomized study of rigid video stylet versus Macintosh laryngoscope for double-lumen endobronchial tube intubation assistance in thoracoscopic pulmonary surgery. J. Clin. Med. 2023, 12, 540. [Google Scholar] [CrossRef]
- Lingappan, K.; Neveln, N.; Arnold, J.L.; Fernandes, C.J.; Pammi, M. Videolaryngoscopy versus direct laryngoscopy for tracheal intubation in neonates. Cochrane Database Syst. Rev. 2023, 5, CD009975. [Google Scholar] [CrossRef]
- Stein, M.L.; Sarmiento Argüello, L.A.; Staffa, S.J.; Heunis, J.; Egbuta, C.; Flynn, S.G.; Khan, S.A.; Sabato, S.; Taicher, B.M.; Chiao, F.; Bosenberg, A.; Lee, A.C.; Adams, H.D.; von Ungern-Sternberg, B.S.; Park, R.S.; Peyton, J.M.; Olomu, P.N.; Hunyady, A.I.; Garcia-Marcinkiewicz, A.; Fiadjoe, J.E.; Kovatsis, P.G.; PeDI Collaborative Investigators. Airway management in the paediatric difficult intubation registry: a propensity score matched analysis of outcomes over time. EClinicalMedicine 2024, 69, 102461. [Google Scholar] [CrossRef]
- Riveros, R.; Sung, W.; Sessler, D.I.; Sanchez, I.P.; Mendoza, M.L.; Mascha, E.J.; Niezgoda, J. Comparison of the Truview PCD™ and the GlideScope(®) video laryngoscopes with direct laryngoscopy in pediatric patients: a randomized trial. Can. J. Anaesth. 2013, 60, 450–457. [Google Scholar] [CrossRef]
- Sun, Y.; Lu, Y.; Huang, Y.; Jiang, H. Pediatric video laryngoscope versus direct laryngoscope: a meta-analysis of randomized controlled trials. Paediatr. Anaesth. 2014, 24, 1056–1065. [Google Scholar] [CrossRef]
- Takeuchi, R.; Hoshijima, H.; Mihara, T.; Kokubu, S.; Sato-Boku, A.; Nagumo, T.; Mieda, T.; Shiga, T.; Mizuta, K. Comparison of indirect and direct laryngoscopes in pediatric patients with a difficult airway: A systematic review and meta-analysis. Children (Basel) 2023, 11, 60. [Google Scholar] [CrossRef]
- Garcia-Marcinkiewicz, A.G.; Kovatsis, P.G.; Hunyady, A.I.; Olomu, P.N.; Zhang, B.; Sathyamoorthy, M.; Gonzalez, A.; Kanmanthreddy, S.; Gálvez, J.A.; Franz, A.M.; Peyton, J.; Park, R.; Kiss, E.E.; Sommerfield, D.; Griffis, H.; Nishisaki, A.; von Ungern-Sternberg, B.S.; Nadkarni, V.M.; McGowan, F.X. Jr.; Fiadjoe, J.E.; PeDI Collaborative investigators. First-attempt success rate of video laryngoscopy in small infants (VISI): a multicentre, randomised controlled trial. Lancet 2020, 396, 1905–1913. [Google Scholar] [CrossRef]
- Riva, T.; Engelhardt, T.; Basciani, R.; Bonfiglio, R.; Cools, E.; Fuchs, A.; Garcia-Marcinkiewicz, A.G.; Greif, R.; Habre, W.; Huber, M.; Petre, M.A.; von Ungern-Sternberg, B.S.; Sommerfield, D.; Theiler, L.; Disma, N. ; OPTIMISE Collaboration. Direct versus video laryngoscopy with standard blades for neonatal and infant tracheal intubation with supplemental oxygen: a multicentre, non-inferiority, randomised controlled trial. Lancet Child Adolesc. Health 2023, 7, 101–111. [Google Scholar] [CrossRef]
- Geraghty, L.E.; Dunne, E.A.; Ní Chathasaigh, C.M.; Vellinga, A.; Adams, N.C.; O'Currain, E.M.; McCarthy, L.K.; O'Donnell, C.P.F. Video versus direct laryngoscopy for urgent intubation of newborn infants. N. Engl. J. Med. 2024, 390, 1885–1894. [Google Scholar] [CrossRef] [PubMed]
- Pfitzner, L.; Cooper, M.G.; Ho, D. The Shikani Seeing StyletTM for difficult intubation in children: Initial experience. Anaesthesia and Intensive Care 2002, 30, 462–466. [Google Scholar] [CrossRef] [PubMed]
- Ho, C.H.; Chen, L.C.; Hsu, W.H.; Lin, T.Y.; Lee, M.; Lu, C.W. A Comparison of McGrath videolaryngoscope versus Macintosh laryngoscope for nasotracheal intubation: A systematic review and meta-analysis. J. Clin. Med. 2022, 11, 2499. [Google Scholar] [CrossRef] [PubMed]
- Amir, S.H.; Ali, Q.E.; Bansal, S. A comparative evaluation of video stylet and flexible fibre-optic bronchoscope in the performance of intubation in adult patients. Indian J. Anaesth. 2017, 61, 321–325. [Google Scholar] [CrossRef]
- Cheng, T.; Wang, L.K.; Wu, H.Y.; Yang, X.D.; Zhang, X.; Jiao, L. Shikani optical stylet for awake nasal intubation in patients undergoing head and neck surgery. Laryngoscope 2021, 131, 319–325. [Google Scholar] [CrossRef]
- Osman, Y.M.; Abd El-Aziz, R.A.E.R. Effectiveness of C-MAC video-stylet versus C-MAC D-blade video-laryngoscope for tracheal intubation in patients with predicted difficult airway: Randomized comparative study. Egyptian J. Anaesthesia 2023, 39, 233–240. [Google Scholar] [CrossRef]
- Lee, M.C.; Tseng, K.Y.; Shen, Y.C.; Lin, C.H.; Hsu, C.W.; Hsu, H.J.; Lu, I.C.; Cheng, K.I. Nasotracheal intubation in patients with limited mouth opening: a comparison between fibreoptic intubation and the Trachway®. Anaesthesia 2016, 71, 31–38. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.C.; Ou, S.Y.; Kuo, Y.T.; Chia, Y.Y. Randomized, active-controlled, parallel-group clinical study assessing the efficacy and safety of FKScope® for nasotracheal intubation in patients scheduled for oral and maxillofacial surgery under general anesthesia. Asian J. Anesthesiol. 2021, 59, 152–160. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.K.; Zhang, X.; Wu, H.Y.; Cheng, T.; Xiong, G.L.; Yang, X.D. Impact of choice of nostril on nasotracheal intubation when using video rigid stylet: a randomized clinical trial. BMC. Anesthesiol. 2022, 22, 360. [Google Scholar] [CrossRef] [PubMed]
- McCauley, P.; Moore, M.; Duggan, E. Anaesthesia for reconstructive free flap surgery for head and neck cancer. Br. J. Hosp. Med. (Lond). 2022, 83, 1–9. [Google Scholar] [CrossRef]
- Yokogawa, F.; Oe, K.; Hosokawa, M.; Masui, K. Lateral position for difficult intubation in a patient with history of hemiglossectomy and flap reconstruction: a case report. JA. Clin. Rep. 2022, 8, 16. [Google Scholar] [CrossRef]
- Nagarkar, R.; Kokane, G.; Wagh, A.; Kulkarni, N.; Roy, S.; Tandale, R.; Pawar, S. Airway management techniques in head and neck cancer surgeries: a retrospective analysis. Oral Maxillofac. Surg. 2019, 23, 311–315. [Google Scholar] [CrossRef]
- Shah, S.V.; Chaggar, R.S. Advanced airway management techniques in anaesthesia for oral cancer surgery: a review. J. Oral Maxillofac. Anesth. 2023, 2, 8. [Google Scholar] [CrossRef]
- Zheng, G.; Feng, L.; Lewis, C.M. A data review of airway management in patients with oral cavity or oropharyngeal cancer: a single-institution experience. BMC. Anesthesiol. 2019, 19, 92. [Google Scholar] [CrossRef]
- Hofmeyr, R.; Llewellyn, R.; Fagan, J.J. Multidisciplinary difficult airway challenges: Perioperative management of glottic and supraglottic tumors. Oper. Tech. Otolaryngol. Head Neck Surg. 2020, 31, 120–127. [Google Scholar] [CrossRef]
- Jeong, H.W.; Song, E.J.; Jang, E.A.; Kim, J. Managing a difficult airway due to supraglottic masses: successful videolaryngoscopic intubation after induction of general anesthesia. Perioper. Med. (Lond). 2024, 13, 21. [Google Scholar] [CrossRef]
- Yang, D.; Li, S.; Lan, J.; Ye, S.; Zhang, L. Use of the Disposcope endoscope for awake orotracheal intubation in an elderly patient with a large vocal cord polyp -a case report. Korean J. Anesthesiol. 2024, 77, 392–396. [Google Scholar] [CrossRef]
- McElwain, J.; Malik, M.A.; Harte, B.H.; Flynn, N.M.; Laffey, J.G. Comparison of the C-MAC videolaryngoscope with the Macintosh, Glidescope, and Airtraq laryngoscopes in easy and difficult laryngoscopy scenarios in manikins. Anaesthesia 2010, 65, 483–489. [Google Scholar] [CrossRef]
- Maartens, T.; de Waal,B. A comparison of direct laryngoscopy to video laryngoscopy by paramedic students in manikin-simulated airway management scenarios. Afr. J. Emerg. Med. 2017, 7, 183–188. [Google Scholar] [CrossRef]
- Yong, S.A.; Chaou, C.H.; Yu, S.R.; Kuan, J.T.; Lin, C.C.; Liu, H.P.; Chiu, T.F. Video assisted laryngoscope facilitates intubation skill learning in the emergency department. J. Acute Med. 2020, 10, 60–69. [Google Scholar] [CrossRef]
- Ghotbaldinian, E.; Dehdari, N.; Åkeson, J. Maintenance of basic endotracheal intubation skills with direct or video-assisted laryngoscopy: A randomized crossover follow-up study in inexperienced operators. AEM. Educ. Train. 2021, 5, e10655. [Google Scholar] [CrossRef]
- Pujari, V.S.; Thiyagarajan, B.; Annamalai, A.; Bevinaguddaiah, Y.; Manjunath, A.C.; Parate, L.H. A comparative study in airway novices using King Vision videolaryngoscope and conventional Macintosh direct laryngoscope for endotracheal intubation. Anesth. Essays Res. 2021, 15, 57–61. [Google Scholar] [CrossRef]
- Yi, I.K.; Hwang, J.; Min, S.K.; Lim, G.M.; Chae, Y.J. Comparison of learning direct laryngoscopy using a McGrath videolaryngoscope as a direct versus indirect laryngoscope: a randomized controlled trial. J. Int. Med. Res. 2021, 49, 3000605211016740. [Google Scholar] [CrossRef] [PubMed]
- Nalubola, S.; Jin, E.; Drugge, E.D.; Weber, G.; Abramowicz, A.E. Video versus direct laryngoscopy in novice intubators: A systematic review and meta-analysis. Cureus 2022, 14, e29578. [Google Scholar] [CrossRef] [PubMed]
- Malito, M.L.; Mathias, L.A.D.S.T.; Kimura Junior, A.; Correa, G.H.; Bardauil, V.R. The impact of introducing a videolaryngoscope in the initial training of laryngoscopy for undergraduate medical students: a simulation randomized trial. Braz. J. Anesthesiol. 2023, 73, 532–538. [Google Scholar] [CrossRef] [PubMed]
- Tseng, K.Y.; Chau, S.W.; Su, M.P.; Shih, C.K.; Lu, I.C.; Cheng, K.I. A comparison of Trachway intubating stylet and Airway Scope for tracheal intubation by novice operators: a manikin study. Kaohsiung J. Med. Sci. 2012, 28, 448–451. [Google Scholar] [CrossRef]
- Hung, K.C.; Tan, P.H.; Lin, V.C.; Wang, H.K.; Chen, H.S. A comparison of the Trachway intubating stylet and the Macintosh laryngoscope in tracheal intubation: a manikin study. J. Anesth. 2013, 27, 205–210. [Google Scholar] [CrossRef] [PubMed]
- Ong, J.; Lee, C.L.; Huang, S.J.; Shyr, M.H. Comparison between the Trachway video intubating stylet and Macintosh laryngoscope in four simulated difficult tracheal intubations: A manikin study. Tzu Chi Med. J. 2016, 28, 109–112. [Google Scholar] [CrossRef] [PubMed]
- Pius, J.; Noppens, R.R. Learning curve and performance in simulated difficult airway for the novel C-MAC® video-stylet and C-MAC® Macintosh video laryngoscope: A prospective randomized manikin trial. PLoS. One 2020, 15, e0242154. [Google Scholar] [CrossRef] [PubMed]
- Hansel, J.; Rogers, A.M.; Lewis, S.R.; Cook, T.M.; Smith, A.F. Videolaryngoscopy versus direct laryngoscopy for adults undergoing tracheal intubation: a Cochrane systematic review and meta-analysis update. Br. J. Anaesth. 2022, 129, 612–623. [Google Scholar] [CrossRef]
- Kleine-Brueggeney, M.; Greif, R.; Schoettker, P.; Savoldelli, G.L.; Nabecker, S.; Theiler, L.G. Evaluation of six videolaryngoscopes in 720 patients with a simulated difficult airway: a multicentre randomized controlled trial. Br. J. Anaesth. 2016, 116, 670–679. [Google Scholar] [CrossRef]
- Zhang, K.; Zhong, C.; Lou, Y.; Fan, Y.; Zhen, N.; Huang, T.; Chen, C.; Shan, H.; Du, L.; Wang, Y.; Cui, W.; Cao, L.; Tian, B.; Zhang, G. Video laryngoscopy may improve the intubation outcomes in critically ill patients: a systematic review and meta-analysis of randomised controlled trials. Emerg. Med. J. 2023, emermed-2023-213860. [Google Scholar] [CrossRef]
- Azam, S.; Khan, Z.Z.; Shahbaz, H.; Siddiqui, A.; Masood, N.; Anum Arif, Y.; Memon, Z.U.; Khawar, M.H.; Siddiqui, F.F.; Azam, F.; Goyal, A. Video versus direct laryngoscopy for intubation: Updated systematic review and meta-analysis. Cureus 2024, 16, e51720. [Google Scholar] [CrossRef]
- De Jong, A.; Sfara, T.; Pouzeratte, Y.; Pensier, J.; Rolle, A.; Chanques, G.; Jaber, S. Videolaryngoscopy as a first-intention technique for tracheal intubation in unselected surgical patients: a before and after observational study. Br. J. Anaesth. 2022, 129, 624–634. [Google Scholar] [CrossRef]
- Cook, T.M.; Aziz, M.F. Has the time really come for universal videolaryngoscopy? Br. J. Anaesth. 2022, 129, 474–477. [Google Scholar] [CrossRef]
- Lyons, C.; Harte, B.H. Universal videolaryngoscopy: take care when crossing the Rubicon. Anaesthesia 2023, 78, 688–691. [Google Scholar] [CrossRef]
- Mirrakhimov, A.E.; Torgeson, E. Use of videolaryngoscopy as the first option for all tracheal intubations: not so fast. Comment on Br. J. Anaesth. 2022; 129: 624-634. Br. J. Anaesth. 2023, 130, e12–e13. [Google Scholar] [CrossRef] [PubMed]
- Webb, A.; Kolawole, H.; Leong, S.; Loughnan, T.E.; Crofts, T.; Bowden, C. Comparison of the Bonfils and Levitan optical stylets for tracheal intubation: a clinical study. Anaesth. Intensive Care 2011, 39, 1093–1097. [Google Scholar] [CrossRef] [PubMed]
- Lan, C.H.; Luk, H.N.; Qu, J.Z.; Shikani, A. An approach to improve the effectiveness of the video-assisted intubating stylet technique for tracheal intubation: A case series report. Healthcare (Basel) 2023, 11, 891. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, I.; Onwochei, D.N.; Muldoon, S.; Keane, O.; El-Boghdadly, K. Airway management research: a systematic review. Anaesthesia 2019, 74, 225–236. [Google Scholar] [CrossRef]
- Ward, P.A.; Irwin, M.G. Man vs. manikin revisited - the ethical boundaries of simulating difficult airways in patients. Anaesthesia 2016, 71, 1399–1403. [Google Scholar] [CrossRef]
- Theiler, L.; Greif, R.; Bütikofer, L.; Arheart, K.; Kleine-Brueggeney, M. The skill of tracheal intubation with rigid scopes - a randomised controlled trial comparing learning curves in 740 intubations. BMC. Anesthesiol. 2020, 20, 263. [Google Scholar] [CrossRef]
- Oh, S.H.; Heo, S.K.; Cheon, S.U.; Ryu, S.A. The effects of backward, upward, rightward pressure maneuver for intubation using the OptiscopeTM: a retrospective study. Anesth. Pain Med. (Seoul) 2021, 16, 391–397. [Google Scholar] [CrossRef]
- Weng, L.; Yu, B.; Ding, L.; Shi, M.; Wang, T.; Li, Z.; Qiu, W.; Lin, X.; Lin, B.; Gao, Y. Visual rigid laryngoscopy versus video laryngoscopy for endotracheal intubation in elderly patients: A randomized controlled trial. PLoS. One 2024, 19, e0309516. [Google Scholar] [CrossRef]
Figure 1.
The emergence of video intubating stylets onto the airway management tools market. The basic structures of such optic intubating devices include a video monitor, handle, and a J-shaped (or hockey stick-shaped) semi-rigid/rigid stylet.
Figure 1.
The emergence of video intubating stylets onto the airway management tools market. The basic structures of such optic intubating devices include a video monitor, handle, and a J-shaped (or hockey stick-shaped) semi-rigid/rigid stylet.

Figure 2.
The styletubation (video intubating stylet technique for endotracheal intubation). Left panels: (upper) Video intubating stylet with a endotracheal tube (ET tube); (middle) The ET tube is mounted onto the intubating stylet with/without a stopper; (lower) The tip of the intubating stylet contained a high-resolution CMOS camera lens and LEDs light source at the tip of the malleable intubating stylet and connected to a detachable video monitor. The resolution of the acquired image is perfect. It should be emphasized that the video intubating stylet is situated inside the ET tube. Right panel: Six different commercial products of video intubating stylets are ubiquitously available in each operating room in our department.
Figure 2.
The styletubation (video intubating stylet technique for endotracheal intubation). Left panels: (upper) Video intubating stylet with a endotracheal tube (ET tube); (middle) The ET tube is mounted onto the intubating stylet with/without a stopper; (lower) The tip of the intubating stylet contained a high-resolution CMOS camera lens and LEDs light source at the tip of the malleable intubating stylet and connected to a detachable video monitor. The resolution of the acquired image is perfect. It should be emphasized that the video intubating stylet is situated inside the ET tube. Right panel: Six different commercial products of video intubating stylets are ubiquitously available in each operating room in our department.

Figure 3.
Evolution of endotracheal intubation techniques from (A) conventional direct laryngoscopy (DL), to (B) videolaryngoscopy (VL), and to (C) styletubation. In addition to better acquired glottis visualization on the monitor, the styletubation technique can allow the airway operator to keep a safer distance away from the patient.
Figure 3.
Evolution of endotracheal intubation techniques from (A) conventional direct laryngoscopy (DL), to (B) videolaryngoscopy (VL), and to (C) styletubation. In addition to better acquired glottis visualization on the monitor, the styletubation technique can allow the airway operator to keep a safer distance away from the patient.

Figure 4.
Midline approach of styletubation in a normal airway scenario. A 31-year-old man (body mass index-BMI: 28.0 kg/m2) underwent reduction of nasal bone fracture and deep complicated facial wound debridement. (A) Wide mouth opening. (B) Uvula. (C) Epiglottis. (D andE) Glottic visualization. (F) Tracheal rings.
Figure 4.
Midline approach of styletubation in a normal airway scenario. A 31-year-old man (body mass index-BMI: 28.0 kg/m2) underwent reduction of nasal bone fracture and deep complicated facial wound debridement. (A) Wide mouth opening. (B) Uvula. (C) Epiglottis. (D andE) Glottic visualization. (F) Tracheal rings.
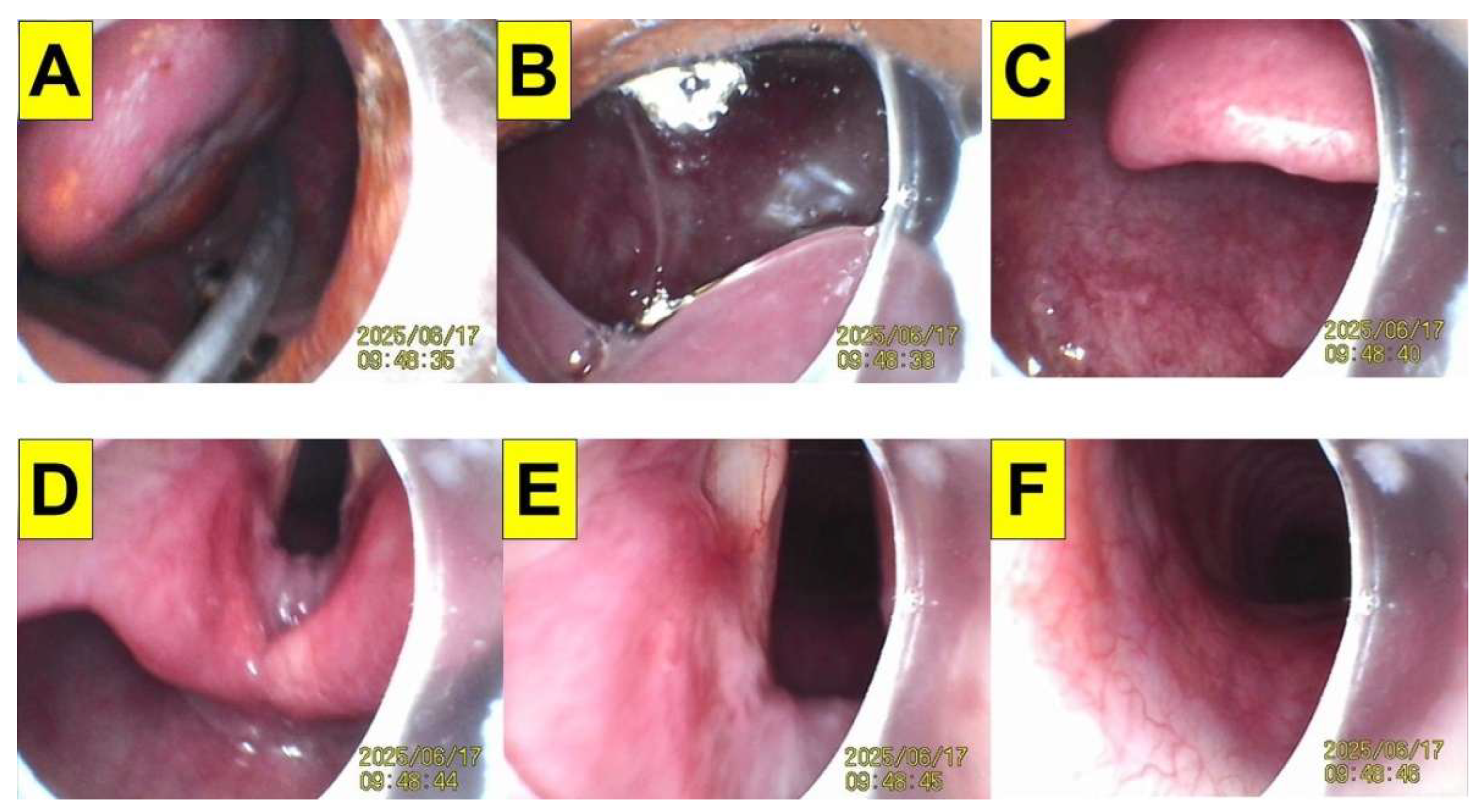
Figure 5.
Three common techniques to perform styletubation. Upper panels: Airway operator’s gesture & team-based approach for styletubation for trans-oral endotracheal intubation. Middle and lower panels: Video images of epiglottis, glottis and vocal cords. (A) One-person model with a styletubation-VL combined technique in a 16-year-old man (BMI: 30.7 kg/m2). Intubating time: 6 s. (B) One-person model with the Shikani technique in a 75-year-old woman (BMI: 26.7 kg/m2). Intubating time: 11 s. (C) Two-operator model in a 76-year–old man (BMI: 23.4 kg/m2). Intubating time: 18 s. (Both airway operators are PGY doctors).
Figure 5.
Three common techniques to perform styletubation. Upper panels: Airway operator’s gesture & team-based approach for styletubation for trans-oral endotracheal intubation. Middle and lower panels: Video images of epiglottis, glottis and vocal cords. (A) One-person model with a styletubation-VL combined technique in a 16-year-old man (BMI: 30.7 kg/m2). Intubating time: 6 s. (B) One-person model with the Shikani technique in a 75-year-old woman (BMI: 26.7 kg/m2). Intubating time: 11 s. (C) Two-operator model in a 76-year–old man (BMI: 23.4 kg/m2). Intubating time: 18 s. (Both airway operators are PGY doctors).
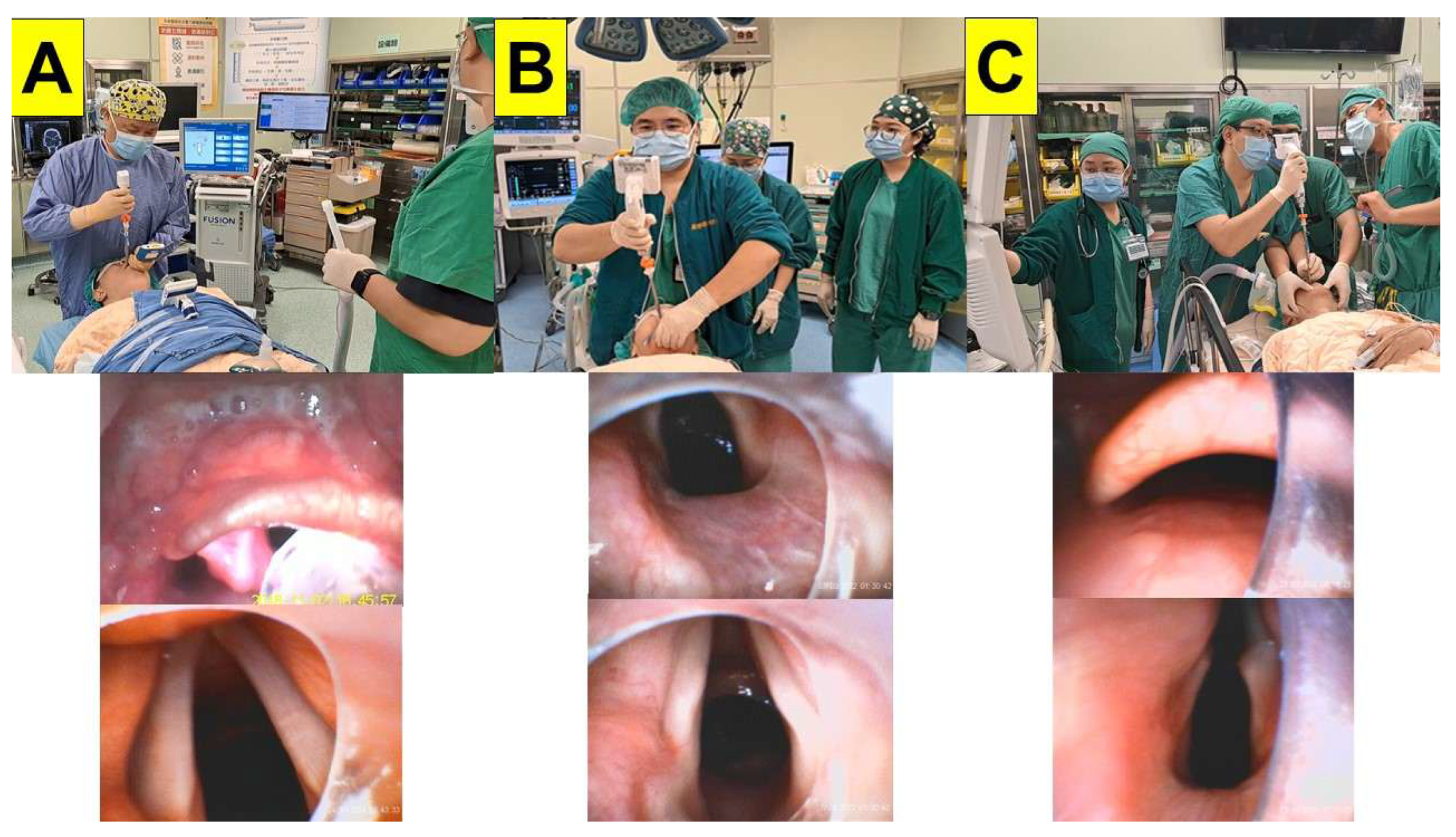
Figure 6.
The LQS grading score on glottis visualization by styletubation technique. (Upper panels) Grade 1: Able to see any part of the vocal cords through the lower edge of the epiglottis (denoted by the white star) in a 64-year-old woman (BMI: 22.2 kg/m2). Intubating time: 30 s (for demonstration). (Middle panels) Grade 2: None of glottis, except the epiglottis, can be observed in a 17-year-old man (BMI: 23.6 kg/m2). Still, there is enough space left between the epiglottis and posterior pharyngeal wall to allow the ET tube-stylet set to pass through. Intubating time: 30 s (for demonstration). (Lower panels) Grade 3: A 48-year-old man (BMI: 20.5 kg/m2); upper lip bite test (ULBT): class 2; modified Mallampati scoring (MMT): class IV; neck circumference 35 cm; sterno-mental distance (SMD) 16 cm). The space under the epiglottis is so narrow and restricted that the passage of ET tube-stylet unit appears to be challenging and difficult. Intubating time: 17 s.
Figure 6.
The LQS grading score on glottis visualization by styletubation technique. (Upper panels) Grade 1: Able to see any part of the vocal cords through the lower edge of the epiglottis (denoted by the white star) in a 64-year-old woman (BMI: 22.2 kg/m2). Intubating time: 30 s (for demonstration). (Middle panels) Grade 2: None of glottis, except the epiglottis, can be observed in a 17-year-old man (BMI: 23.6 kg/m2). Still, there is enough space left between the epiglottis and posterior pharyngeal wall to allow the ET tube-stylet set to pass through. Intubating time: 30 s (for demonstration). (Lower panels) Grade 3: A 48-year-old man (BMI: 20.5 kg/m2); upper lip bite test (ULBT): class 2; modified Mallampati scoring (MMT): class IV; neck circumference 35 cm; sterno-mental distance (SMD) 16 cm). The space under the epiglottis is so narrow and restricted that the passage of ET tube-stylet unit appears to be challenging and difficult. Intubating time: 17 s.
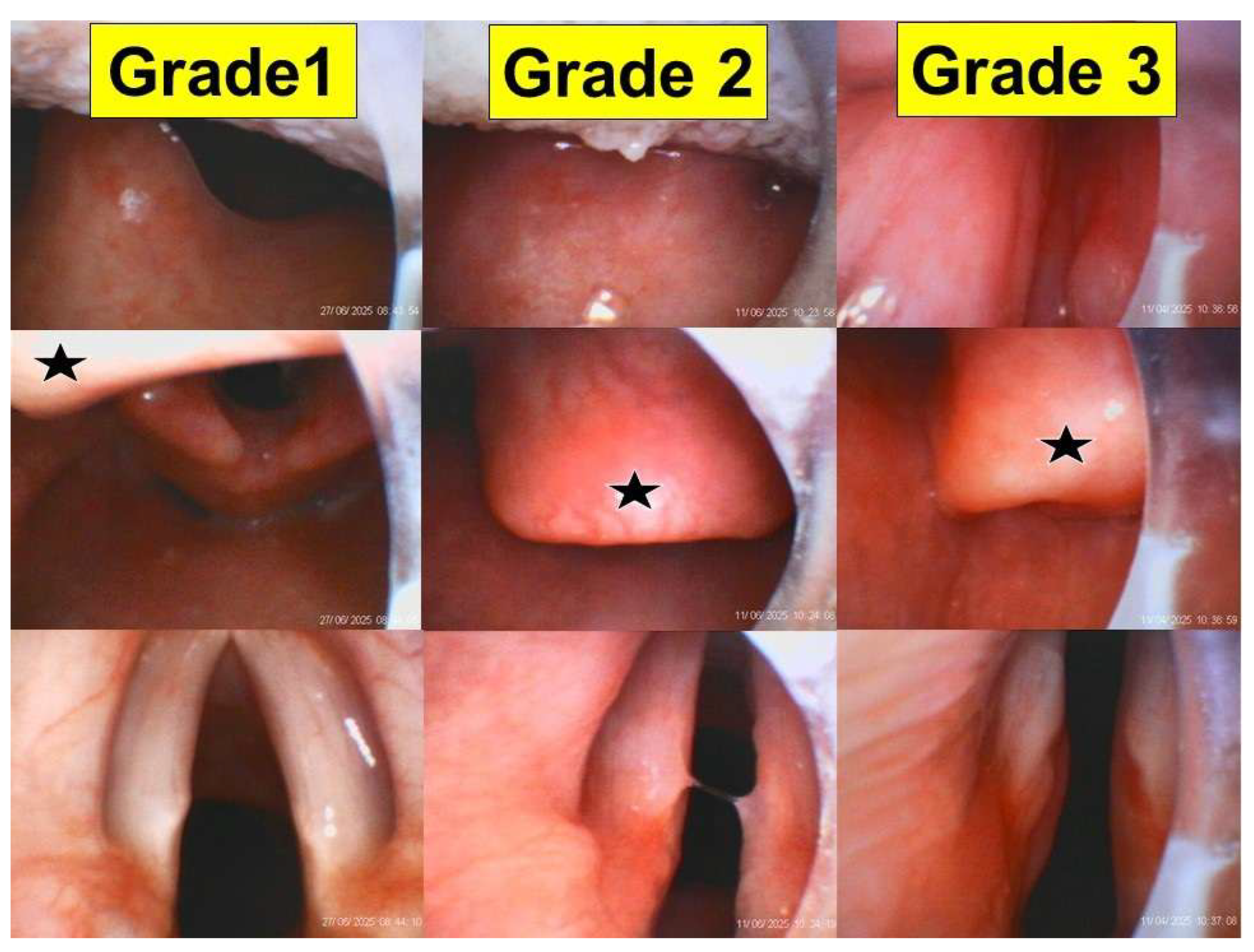
Figure 7.
Examples of swift and easy endotracheal intubation by styletubation in normal airway scenarios. (A) Intubation time: 4 s. A 48-year-old woman with BMI: 20.5 kg/m2 and MMC: class II.
Figure 7.
Examples of swift and easy endotracheal intubation by styletubation in normal airway scenarios. (A) Intubation time: 4 s. A 48-year-old woman with BMI: 20.5 kg/m2 and MMC: class II.
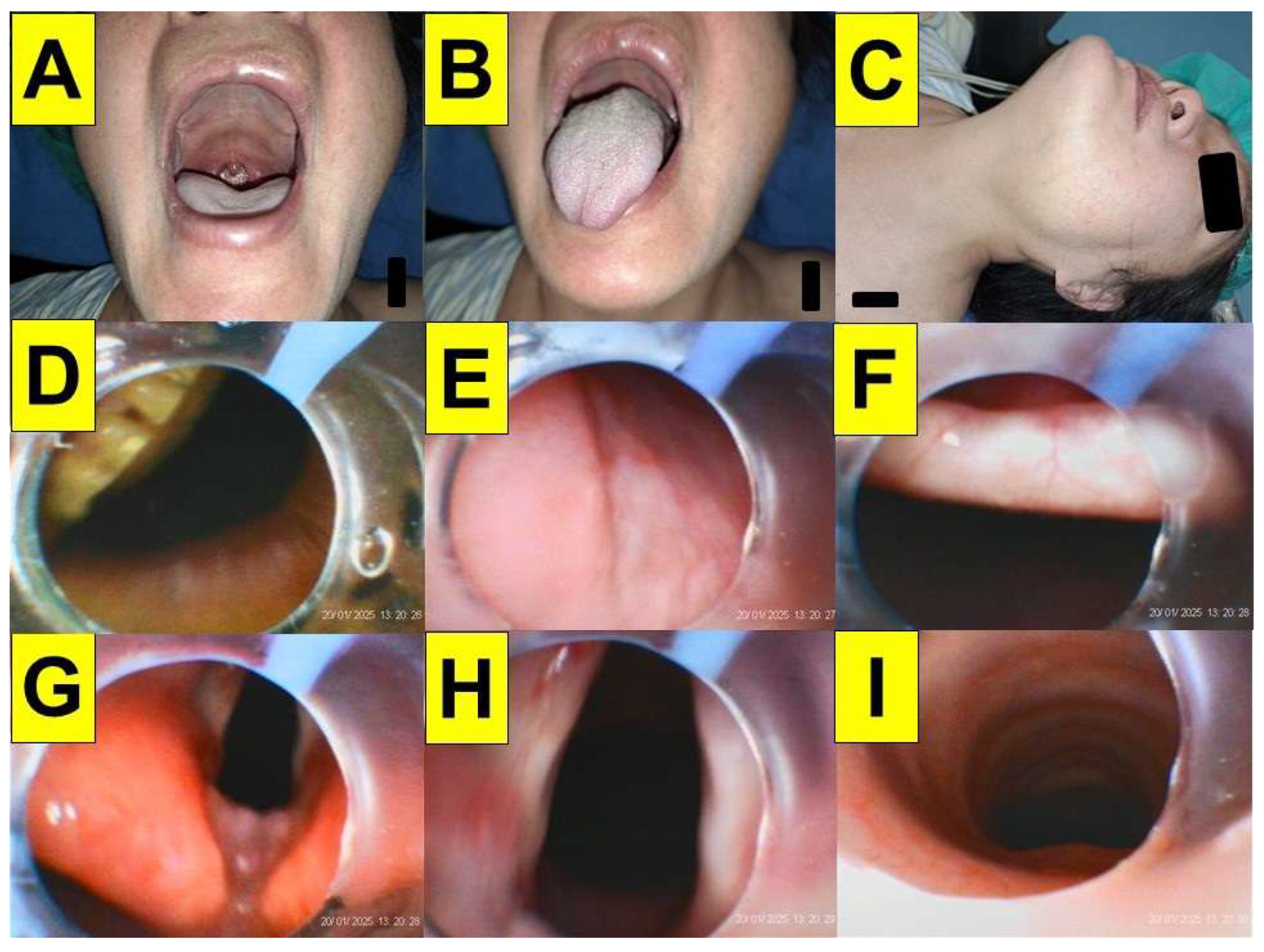
Figure 8.
An example easy, smooth and look-around-the-corner process of styletubation. A 64-year-old woman (BMI: 22.2 kg/m2). LQS grade 1. Time from lip to trachea is 30 s with first-pass success.
Figure 8.
An example easy, smooth and look-around-the-corner process of styletubation. A 64-year-old woman (BMI: 22.2 kg/m2). LQS grade 1. Time from lip to trachea is 30 s with first-pass success.
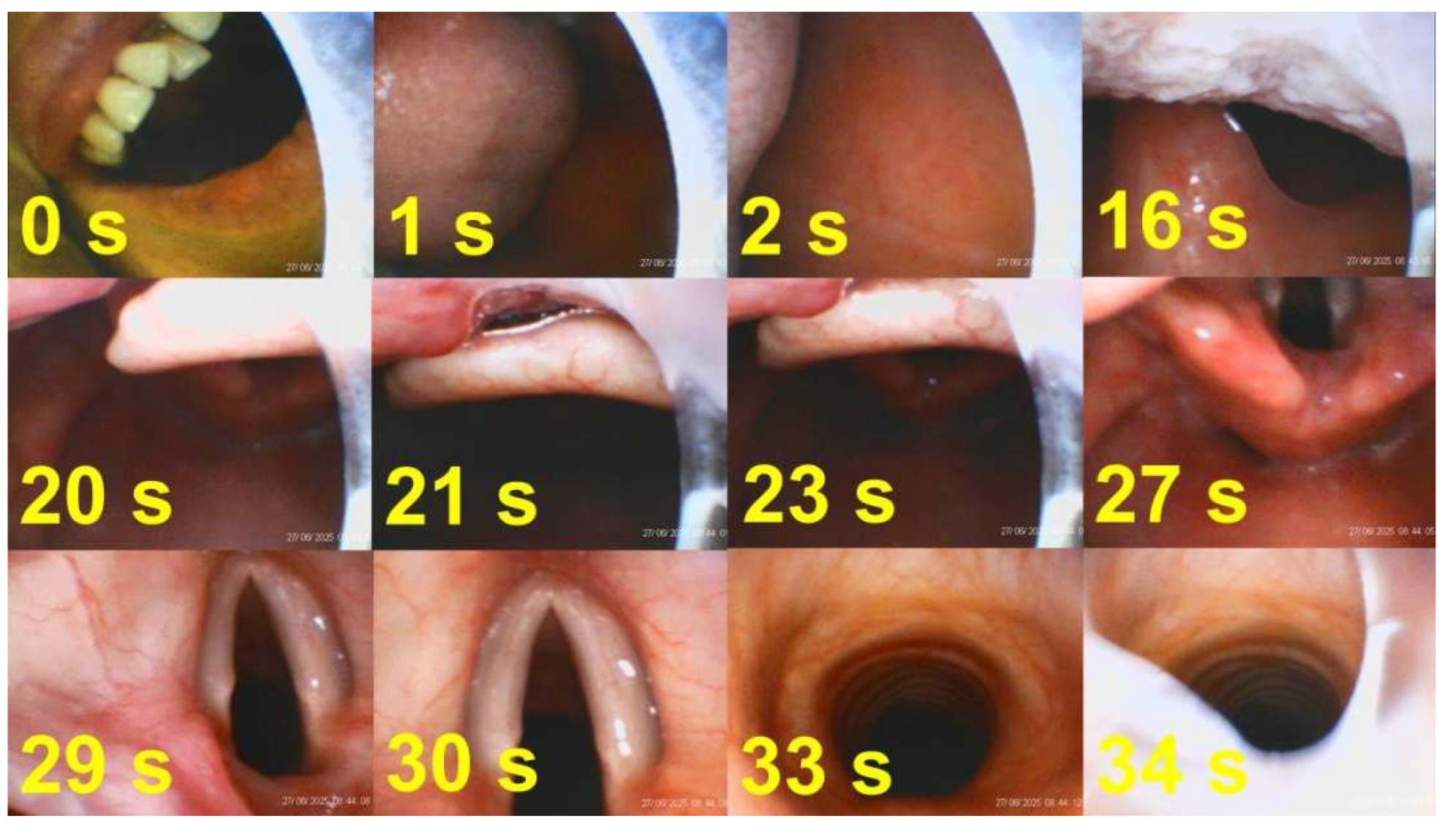
Figure 9.
Application of styletubation in a morbid obesity patient. This is a 46-year-old man with a BMI 55.4 kg/m2; MMC: class II. ; inter-incisor distance 4.5 cm; neck circumference 53 cm; sterno-mental distance (SMD) 15 cm; with OSAS history. (A~C) Narrow oro-pharyngeal space; (D) An omega-shaped epiglottis; (E~G) glottis visualization with plica ventricularis; (H) Tracheal rings. The nasal airway-suction tube assembly (in green color) was applied to clear the secretions and as a guide for subsequent styletubation. The intubating time was 30 s with first-pass success. .
Figure 9.
Application of styletubation in a morbid obesity patient. This is a 46-year-old man with a BMI 55.4 kg/m2; MMC: class II. ; inter-incisor distance 4.5 cm; neck circumference 53 cm; sterno-mental distance (SMD) 15 cm; with OSAS history. (A~C) Narrow oro-pharyngeal space; (D) An omega-shaped epiglottis; (E~G) glottis visualization with plica ventricularis; (H) Tracheal rings. The nasal airway-suction tube assembly (in green color) was applied to clear the secretions and as a guide for subsequent styletubation. The intubating time was 30 s with first-pass success. .
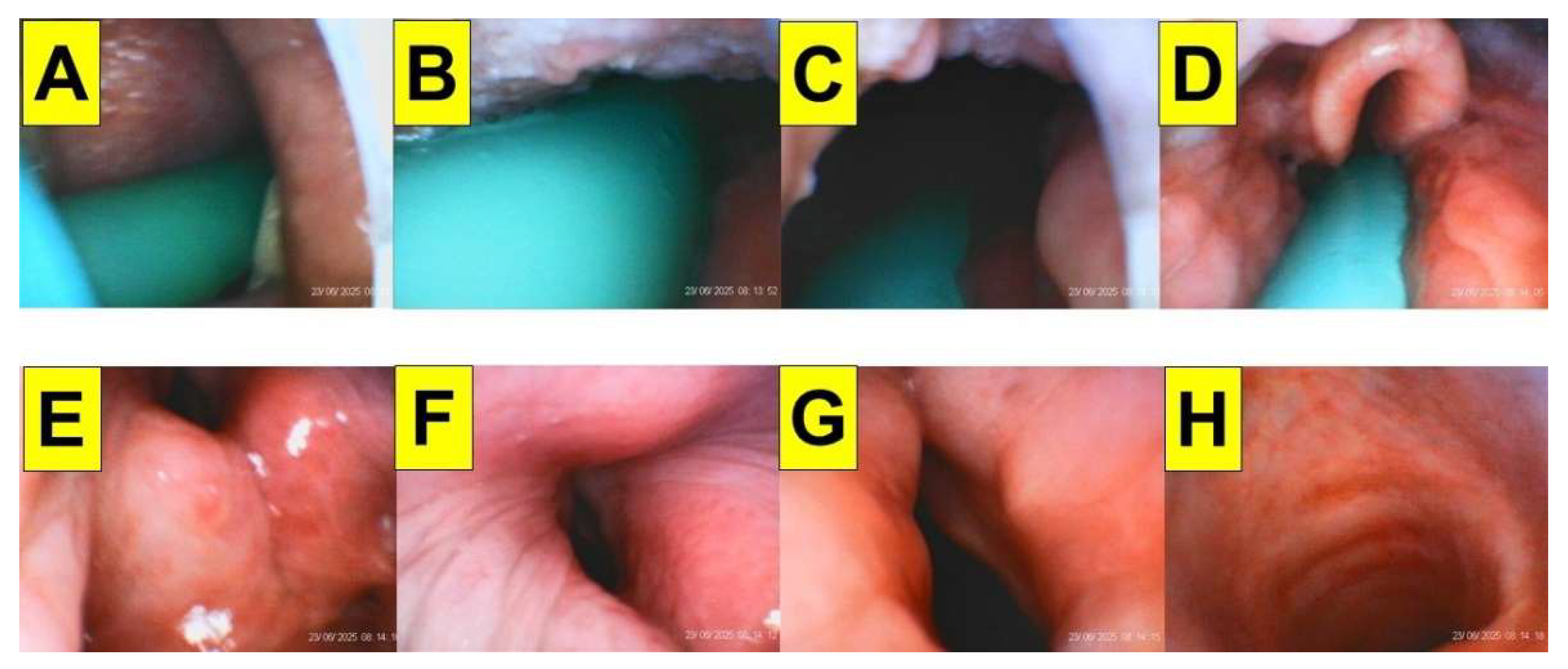
Figure 10.
Usefulness of styletubation technique applied in a DA scenario. A 61-year-old man underwent bilateral functional endoscopic sinus surgery (FESS) under the impression of sinusitis and nasal polyps. He was diagnosed of nasopharyngeal carcinoma (NPC) with cT3N1M0 and completed concurrent chemoradiotherapy (CCRT) 6 months ago. Hoarseness, difficulty swallowing, severe neck stiffness and moderate stridor were noted after this admission. (A & B) Limited mouth-opening and tongue size. (C) Swollen uvula. (D) Narrow pharyngeal space. (E) Swollen folded and omega-shaped epiglottis. (F & G) Jaw-thrust maneuver could only lift up the epiglottis to a mild degree and only a culvert-shaped space was created. (H) Swollen glottis, a tiny glottic aperture, and no clear true vocal cords were observed. (I) Tracheal rings. Intubation was swift and smooth (38 s) with first-pass success.
Figure 10.
Usefulness of styletubation technique applied in a DA scenario. A 61-year-old man underwent bilateral functional endoscopic sinus surgery (FESS) under the impression of sinusitis and nasal polyps. He was diagnosed of nasopharyngeal carcinoma (NPC) with cT3N1M0 and completed concurrent chemoradiotherapy (CCRT) 6 months ago. Hoarseness, difficulty swallowing, severe neck stiffness and moderate stridor were noted after this admission. (A & B) Limited mouth-opening and tongue size. (C) Swollen uvula. (D) Narrow pharyngeal space. (E) Swollen folded and omega-shaped epiglottis. (F & G) Jaw-thrust maneuver could only lift up the epiglottis to a mild degree and only a culvert-shaped space was created. (H) Swollen glottis, a tiny glottic aperture, and no clear true vocal cords were observed. (I) Tracheal rings. Intubation was swift and smooth (38 s) with first-pass success.
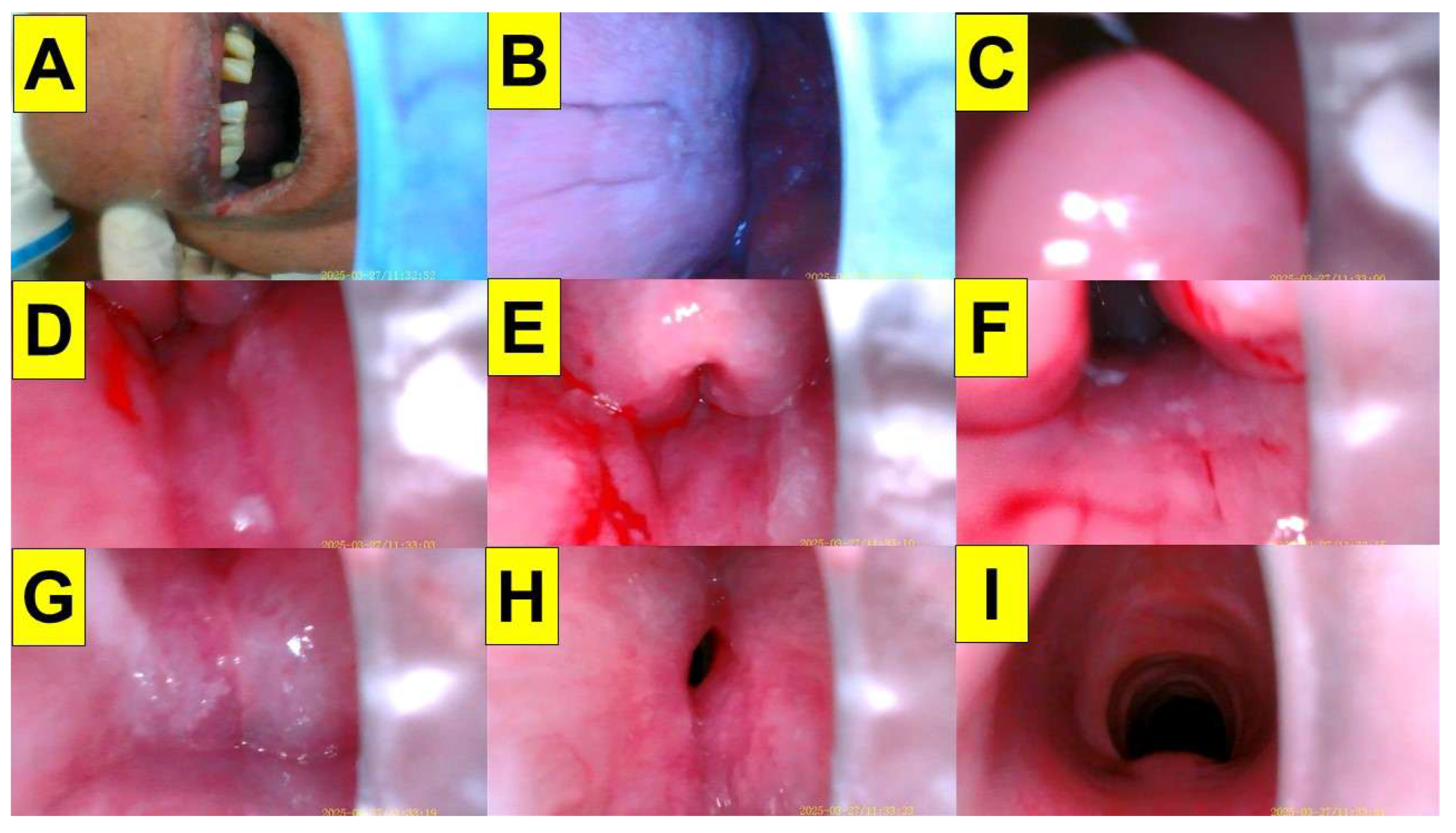
Figure 11.
Application of styletubation in various DA scenarios. (A) Giant cemento-ossifying fibroma. Intubating time: 24 s. (B) Bilateral tonsillar hypertrophy, grade 3 and OSAS. Intubating time: 20 s. (C) Buck teeth. Intubating time: 24 s. (D) Obesity with OSA undergoing bariatric surgery. Intubating time: 11 s. (E) Ankylosing spondylitis undergoing LMS. Intubating time: 30 s. (F) Restricted cervical spine mobility with cervical collar. Intubating time: 12 s. (G) Double-lumen endobronchial tube intubation. Intubating time: 24 s. (H) Pediatric endotracheal intubation. (I) Naso-tracheal intubation in a patient with jaw necrosis. Intubating time: 30 s. (J) Retromolar approach of styletubation in a patient with prior buccal carcinoma and reconstruction flap. Intubating time: 20 s. (K) Trismus in a patient with lower gum cancer. Intubating time: 10 s. (L) Hypopharyngeal cancer. Intubating time: 38 s.
Figure 11.
Application of styletubation in various DA scenarios. (A) Giant cemento-ossifying fibroma. Intubating time: 24 s. (B) Bilateral tonsillar hypertrophy, grade 3 and OSAS. Intubating time: 20 s. (C) Buck teeth. Intubating time: 24 s. (D) Obesity with OSA undergoing bariatric surgery. Intubating time: 11 s. (E) Ankylosing spondylitis undergoing LMS. Intubating time: 30 s. (F) Restricted cervical spine mobility with cervical collar. Intubating time: 12 s. (G) Double-lumen endobronchial tube intubation. Intubating time: 24 s. (H) Pediatric endotracheal intubation. (I) Naso-tracheal intubation in a patient with jaw necrosis. Intubating time: 30 s. (J) Retromolar approach of styletubation in a patient with prior buccal carcinoma and reconstruction flap. Intubating time: 20 s. (K) Trismus in a patient with lower gum cancer. Intubating time: 10 s. (L) Hypopharyngeal cancer. Intubating time: 38 s.
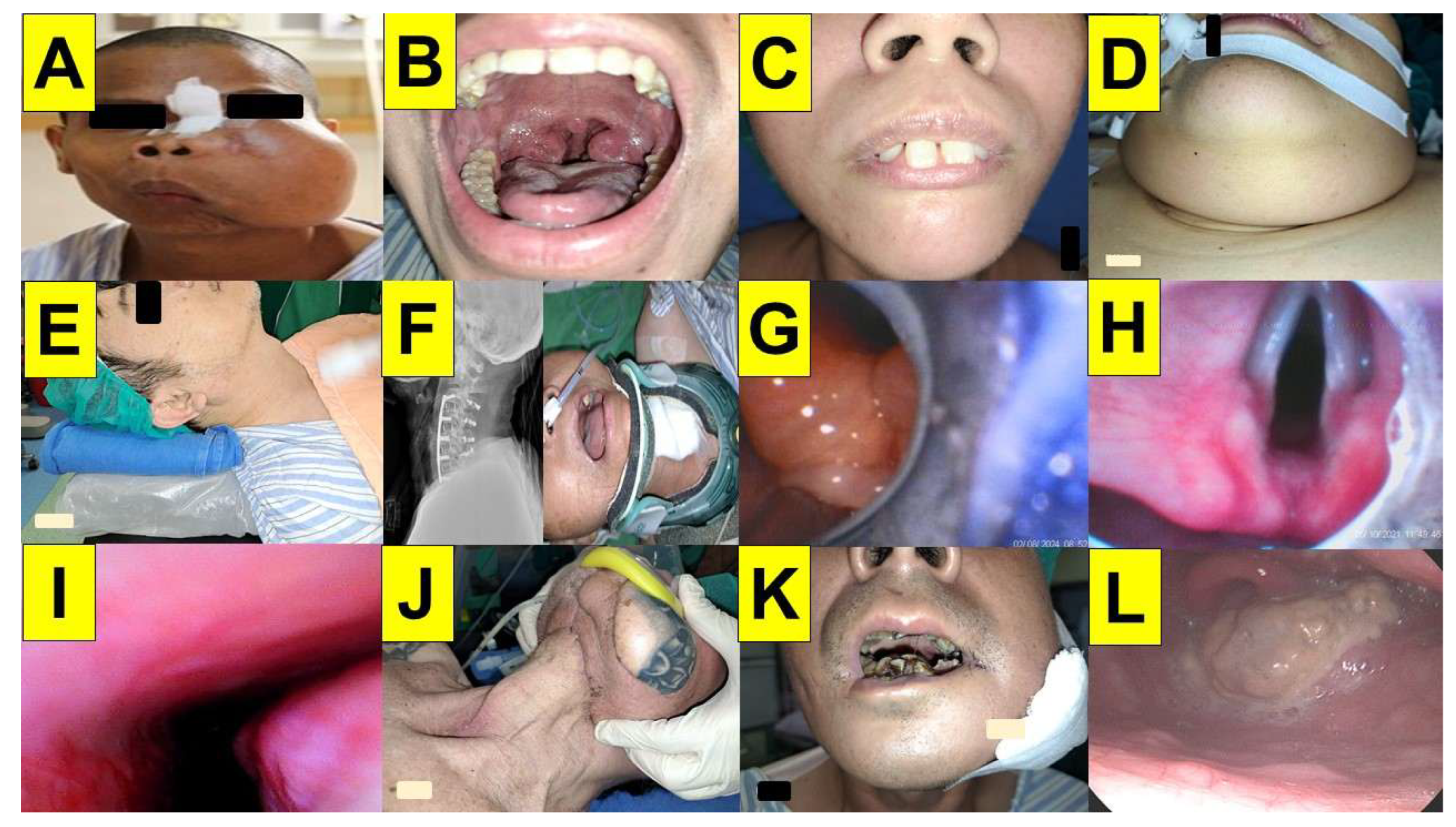
Figure 12.
The learning curve for the “green” airway management trainees in the real world. The patient is a 36-year-old woman (BMI 20.4 kg/m2) undergoing dilation of the Eustachian tube (balloon tuboplasty). (A) A clerk medical student, who has gone through the regular airway training program, failed to intubate this patient with styletubation (the trial duration was 60 s). The first-pass success rate for her all experience in styletubation is 26.6% (failure in 11 cases out of 15 intubated patients) during her two-week training course) (B) A post-graduate year 2 (PGY-2) doctor had previous experiences of using laryngoscopy. The time to intubation was 10 s with first-pass success in the same patient as that in (A). The first-pass success rate for her experience in styletubation is 87.5% (failure in 8 cases out of 64 intubated patients during her 4-week training course).
Figure 12.
The learning curve for the “green” airway management trainees in the real world. The patient is a 36-year-old woman (BMI 20.4 kg/m2) undergoing dilation of the Eustachian tube (balloon tuboplasty). (A) A clerk medical student, who has gone through the regular airway training program, failed to intubate this patient with styletubation (the trial duration was 60 s). The first-pass success rate for her all experience in styletubation is 26.6% (failure in 11 cases out of 15 intubated patients) during her two-week training course) (B) A post-graduate year 2 (PGY-2) doctor had previous experiences of using laryngoscopy. The time to intubation was 10 s with first-pass success in the same patient as that in (A). The first-pass success rate for her experience in styletubation is 87.5% (failure in 8 cases out of 64 intubated patients during her 4-week training course).
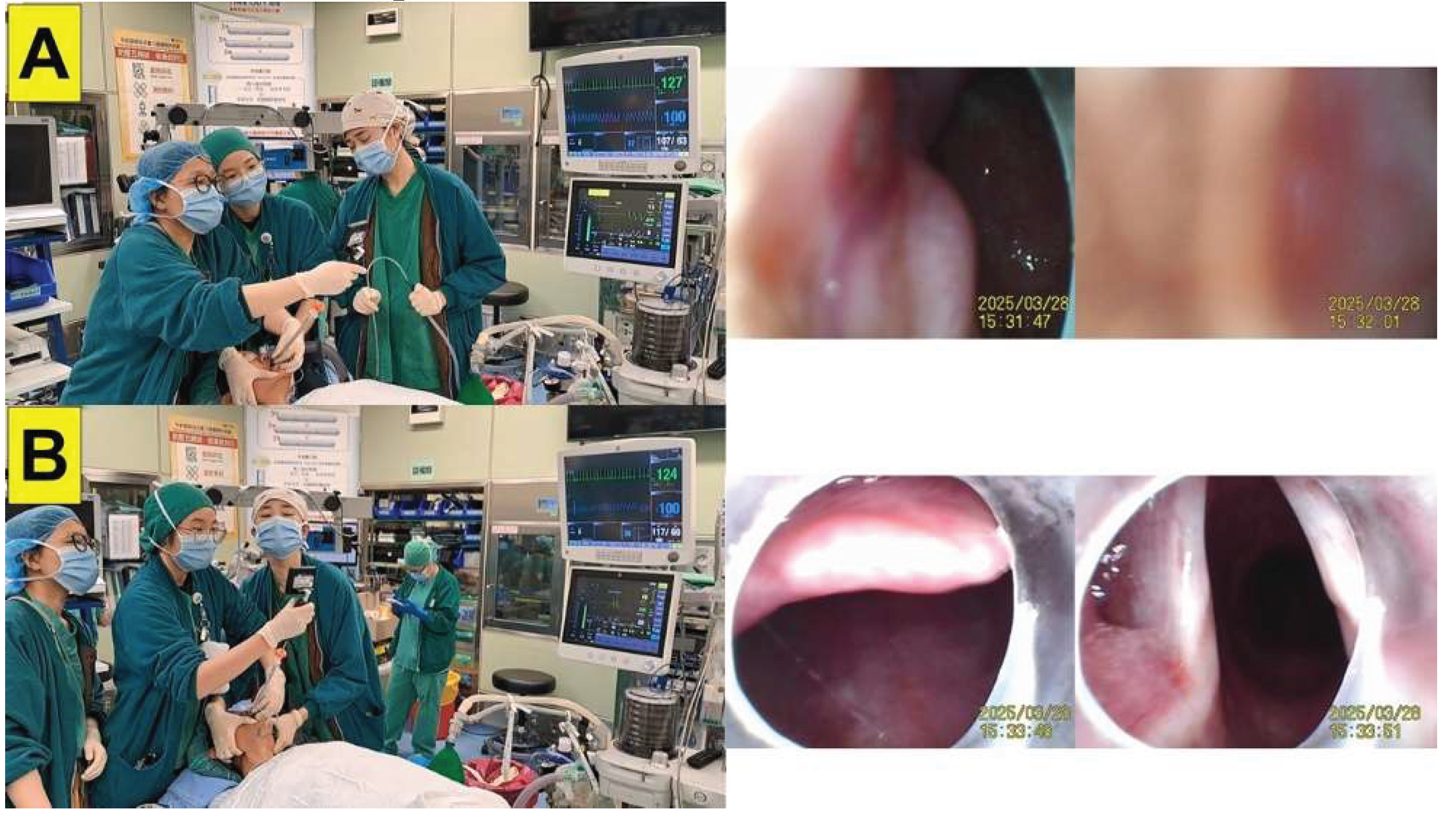
Table 1.
Universal use coverage of styletubation technique for routine first-line tracheal intubation in the Department of Anesthesia, Hualien Tzuchi Medical Center, Hualien, Taiwan between 2016 and 2024.
Table 1.
Universal use coverage of styletubation technique for routine first-line tracheal intubation in the Department of Anesthesia, Hualien Tzuchi Medical Center, Hualien, Taiwan between 2016 and 2024.
| 2016 | 2017 | 2018 | 2019 | 2020 | 2021 | 2022 | 2023 | 2024 | ||
|---|---|---|---|---|---|---|---|---|---|---|
| Total anesthesia number | 16077 | 17831 | 17998 | 19307 | 19721 | 19244 | 19765 | 22438 | 25046 | |
| GA number | 15339 | 16893 | 17497 | 18481 | 19009 | 18574 | 19061 | 22099 | 24368 | |
| LMA-GA number | 5544 | 5134 | 5816 | 5902 | 5863 | 5714 | 4932 | 5763 | 6585 | |
| ET-GA number | 5953 | 6504 | 6920 | 6966 | 7418 | 6982 | 7602 | 8329 | 8889 | |
| VL | 0 | 0 | 20 | 100 | 635 | 336 | 305 | 280 | 350 | |
| Styletubation | 5953 | 6504 | 6900 | 6866 | 6783 | 6646 | 7297 | 8049 | 8539 | |
GA: general anesthesia. LMA: laryngeal mask airway. ET: endotracheal tube. VL: videolaryngoscope. There are 19 operating rooms in the surgical theatre. The anesthesia team is composed of 16 anesthesiologists and 65 certified registered nurse anesthetists.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



