Submitted:
01 August 2025
Posted:
01 August 2025
You are already at the latest version
Abstract
Introduction: Although Brazil has industrialized regions, such as the Southeast, it still has underdeveloped regions with poor sanitary conditions, such as the North and Northeast, similar to regions in Africa and Asia, where HEV-1 circulates. However, it is suspected that HEV occurs as a zoonosis in Brazil. Due to the wide variation in HEV prevalence across the five regions of this country, a scoping review was conducted to systematically identify any the prevalence and genotype of HEV. The following research question was formulated. Aims: to review the epidemiological peculiarities and genotype of HEV in the five regions of Brazil. Methods: This is a scoping review, conducted based on the methodological framework developed by the JBI and the Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) checklist. The searches were conducted in June and July 2025, using the following databases: MEDLINE and LILACS. A search equation was developed to map the evidence on the epidemiology of HEV infection in Brazil based on the Population, Concept, and Context (PCC) Strategy. Results: Of the 57 studies on the prevalence of hepatitis E virus infection in Brazil, 45 (78.9%) were in humans and 12 (21.1%) in swine. The overall prevalence of the IgG marker in Brazil ranged from 0.5% in the North region to 59.4% in the South region. On the other hand, the lowest prevalence of the IgM marker was recorded in the Northeast region (0.1%) and the highest in the North region (16.3%). Among the 12 studies involving pigs, the occurrence of HEV in these animals was identified in all regions of Brazil, with variations in the types of samples tested, husbandry methods, and prevalence detected. Exclusively hepatitis E viruses belonging to genotype 3 (HEV-3) were identified in all regions of Brazil where genotypic analysis was performed. Conclusion: based on the findings of this review, it can be considered that HEV infection occurs in all five regions of Brazil, with higher prevalence in the South and Southeast regions. The circulating genotype in the country is HEV-3, possibly transmitted through pig consumption and breeding interpretations.
Keywords:
hepatitis E
; serosurvey
; prevalence
; Brazil
; genotype 3
; epidemiology
; anti-HEV IgG
1. Introduction
Hepatitis E virus (HEV) is the main cause of acute enterically transmitted hepatitis worldwide [1]. Recent data from the World Health Organization (WHO) estimate that in 2021, there were approximately 20 million cases and 3,500 deaths from hepatitis E worldwide [2,3].
HEV belongs to the Hepeviridae family, Orthohepevirus genus, species A, classified into eight genotypes (HEV-1 to HEV-8) [4]. Of these, genotypes 1 to 4 have been isolated in humans, while genotypes 5 to 8 infect animals exclusively [5]. Contamination by genotypes 1 and 2 occurs via the fecal-oral route, through contaminated water, occurring in regions with poor sanitary conditions, such as Africa and Asia [6]. Sporadic cases are common, but large outbreaks also occur, affecting up to thousands of people [7]. Genotypes 3 and 4 infect humans through contaminated meat or direct contact with pigs, causing acute infections that are usually asymptomatic and self-limiting [8,9]. However, in immunocompromised patients, it can occasionally progress to chronic hepatitis and cirrhosis [10].
In recent decades, however, HEV has also been described in industrialized countries in Europe and North America through autochthonous cases. These cases are associated with genotypes 3 and 4, with epidemiological and clinical characteristics distinct from the 1 and 2 genotypes that circulate in developing countries [8,11].
In a meta-analysis conducted to assess the global prevalence of HEV, involving 287 studies and 1.099,717 patients, the percentage of anti-HEV IgG was found to be 12.47%. The data were stratified to estimate the prevalence of anti-HEV in 75 countries across six continents. The highest anti-HEV IgG positivity was found in Africa (21.76%), followed by Asia (15.80%), Europe (9.31%), North America (8.05%), South America (7.28%), and Oceania (5.99%). The data revealed that HEV-1 infection occurred mainly in India and China, and that HEV-3 was more commonly found in European countries [12].
In Latin America and the Caribbean, the overall prevalence of hepatitis E observed in a recent systematic review and meta-analysis was 9.0%, with significant heterogeneity (I² = 97.3%) and percentages ranging from 0% to 36% [13] (Magri et al 2025), respectively, in Brazil (kidney transplant [14] and hemodialysis patients [15]) and Cuba (occupational exposure in pigs [16]).
In Brazil, particularly, in a systematic review with meta-analysis conducted a few years ago, a general prevalence of anti-HEV of 6% (95% CI: 5.0–7.0) was observed, but with great heterogeneity (I² = 86.7%) between studies, ranging from 0% (95% CI: 0.0–3.0) in the state of Amazonas, in the northern region of the country [17], to 10.0% (95% CI: 7.0–15.0) in the state of Santa Catarina, in the southern region [18], confirming that HEV infection in Brazil occurs with wide variation in prevalence [19].
As a result of the short period of HEV viremia and the fact that most studies are cross-sectional, there is little data on the HEV genotype circulating in Brazil. However, the absence of descriptions of epidemic outbreaks and data evaluated in pigs suggest that HEV-3 is the circulating genotype in our environment [9]. Although Brazil has industrialized regions, such as the Southeast, it still has underdeveloped regions with poor sanitary conditions, such as the North and Northeast, similar to regions in Africa and Asia, where HEV-1 circulates [20]. However, it is suspected that HEV occurs as a zoonosis in Brazil.
Due to the wide variation in HEV prevalence across the five regions of Brazil, a scoping review was conducted to systematically map the research carried out in this area and identify any gaps in knowledge. The following research question was formulated: What are the epidemiological characteristics of HEV infection in the regions of Brazil?
2. Materials and Methods
This is a scoping review, conducted based on the methodological framework developed by the JBI [21] and the Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) checklist [22].
Eligility criteria
The eligibility criteria for this scoping review were established as follows: publications on the epidemiology of hepatitis E virus (HEV) infection in Brazil since 1995, when the first reports of the disease appeared in the country, with no language restrictions. Regarding the type of study, primary and secondary, empirical, quantitative research was selected, with preference given to cohort, case-control, and cross-sectional studies. Letters to the editor, validation studies, review articles, case reports, abstracts in event proceedings, incomplete articles, studies in the project phase, or studies without results were excluded. Articles related to HEV epidemiology in other countries and those involving the contamination of mollusks or other animals, such as horses, capybaras, and wild boars, were also excluded.
Information sources
The searches were conducted in June and July 2025, using the following databases: Medical Literature Analysis and Retrieval System Online (MEDLINE) via PubMed, MEDLINE via the Virtual Health Library (VHL), and Latin American and Caribbean Health Sciences Literature (LILACS). The gray literature was retrieved from Google Scholar, the Brazilian Digital Library of Theses and Dissertations (BDTD), and the Thesis and Dissertation Catalog (CTD) of the Coordination for the Improvement of Higher Education Personnel (CAPES).
Search
A search equation was developed to map the evidence on the epidemiology of HEV infection in Brazil. The equation is presented in Figure 1.
Selection of sources of evidence
The results obtained from the databases were exported to a Microsoft Excel® spreadsheet for independent study selection and screening by two researchers, with disagreements resolved by a third examiner. The first phase involved reading titles and abstracts. Studies that met the inclusion criteria were analyzed in the second phase by reading the full manuscripts. Finally, manual searches of the references of the included studies were performed.
Data charting process and Data itens
First, data were extracted independently by two reviewers using Microsoft Excel® spreadsheets. The information was confirmed by the third reviewer, and disagreements and doubts were resolved through discussion until consensus was reached among the authors. Data mapping was based on the JBI tool for characterizing the studies [21]. The extraction table included authorship, journal of publication, country of origin, year of publication, objectives, design, sample size, and main results regarding the identification of HEV seroprevalence in the five regions of Brazil.
3. Results
Initially, we identified 309 publications in the MEDLINE and LILACS databases. Another source was obtained through citation searching (Figure 2).
After excluding duplicates (170), we analyzed 140 references by reading the abstracts. Of these, 83 publications were subsequently excluded, leaving 57 references selected for full-text reading, which were included in the final review. Of the 57 studies on the prevalence of hepatitis E virus infection in Brazil, 45 (78.9%) were in humans and 12 (21.1%) in swine.
The distribution of the 45 studies involving HEV and humans is presented in Table 1. It was found that most studies were conducted in the Southeast region (35.5%), particularly in the state of São Paulo (87.5%), followed by the Northeast (20%) and Central West (20%). The lowest number of studies was observed in the North region (11.1%), with 3 (60%) in the state of Pará, 1 (20%) in Acre, and the other in the states of Amazonas and Rondônia (20%).
The variations in the prevalence of Hepatitis E, according to the regions of Brazil, are presented in Figure 3. The overall prevalence of the IgG marker in Brazil ranged from 0.5% in the North region to 59.4% in the South region. On the other hand, the lowest prevalence of the IgM marker was recorded in the Northeast region (0.1%) and the highest in the North region (16.3%).
Among the 12 studies involving pigs, the occurrence of hepatitis E virus (HEV) in these animals was identified in all regions of Brazil, with variations in the types of samples tested, husbandry methods, and prevalence detected. The data are presented in Table 2.
Exclusively hepatitis E viruses belonging to genotype 3 (HEV-3) were identified in all regions of Brazil where genotypic analysis was performed. Intra-genotypic diversity was evidenced by the distribution of different phylogenetic subtypes among the states and is presented in Figure 4.
In the North Region, in the state of Pará, subtypes 3c and 3f were identified. In the Northeast, in the state of Pernambuco, the isolated viruses were classified as subtype 3f. In the Central-West Region, in the state of Mato Grosso, multiple subtypes were detected: 3b and 3f in one study, and 3d, 3h, and 3i in another, demonstrating genetic diversity of HEV in the region. In the Southeast Region, in the state of Rio de Janeiro, subtype 3b was identified. In Minas Gerais, the viruses were grouped into subtypes 3c and 3i. In the state of São Paulo, subtypes 3b, 3h, and 3j were detected. In the southern region, in the state of Paraná, the isolated viruses belonged to subtype 3b. In Rio Grande do Sul, subtypes 3b, 3c, and 3h were identified.
4. Discussion
Recent estimates regarding hepatitis B and C viruses suggest a downward trend in the incidence and prevalence of these infections in Brazil, possibly as a consequence of vaccination and antiviral treatment in recent years [79,80]. However, data on the occurrence of HEV infection in this country are very scarce, which may be due to the unavailability of the anti-HEV test for patients from the Brazilian Public Unified Health System.
Brazil has a vast territorial extension and a significant population with considerable ethnic and cultural miscegenation. The Brazilian people have experienced cultural influences from indigenous peoples (the original people), which persists mainly in the North and Central West regions; from the Portuguese in the Northeast, and from Italians and Germans in the Southeast and South. Additionally, the influence of the African people is present in practically all regions of the country, brought over during the 17th and 19th centuries. Certainly, this aspect is of great importance for the wide variation in the prevalence and peculiarities of HEV in Brazil.
Due to the heterogeneity of studies conducted in Brazil, stemming from the large number of articles found—about 48 papers in the last 30 years—assessing different groups across the five different regions of the country, as well as the use of different tests, obtaining more robust data from across the territory is challenging. Nevertheless, when evaluating the data in general, there is a trend of increasing prevalence from North to South regions, with intermediate numbers in the Central West and Northeast (Table 1). Socio-demographic data also reveal a trend of higher education levels, greater purchasing power, and increased industrialization in the Southeast and South regions of Brazil.
Indeed, when observing the epidemiological data on HEV, variation among the different regions of Brazil becomes evident, particularly with a higher occurrence of this virus in the Southeast and South regions of the country. It is noteworthy, however, that some authors have suggested that differences in prevalence in the country could be attributed to the sensitivity issues of ELISA tests for detecting anti-HEV from different manufacturers [19, 81]. Nonetheless, more recent data using modern tests suggest that differences in the accuracies of anti-HEV IgG tests may not be as significant [12, 54, 82].
There is a scarcity of studies in the general population of Brazil, with the vast majority conducted on blood donors or specific groups. Initial studies particularly evaluated the occurrence of anti-HEV in patients with acute hepatitis of undetermined etiology (non-A, non-E hepatitis), in addition to blood donors. Therefore, these data were obtained using older ELISA tests. More recent studies assessed specific high-risk groups, such as drug users, hemodialysis patients, HIV soropositive individuals, transplant recipients, and patients with underlying chronic liver disease, among others (Table 1).
One of the first well-designed epidemiological studies conducted in Brazil took place in the city of São Paulo, where active searches were conducted in randomly selected households across all neighborhoods and social strata. A total of 1,059 individuals were evaluated, estimating the prevalence of anti-HEV IgG at 1.68% of the population, with a tendency to increase in older individuals and residents of the West and downtown areas of the city [46]. Shortly thereafter, similar data was observed in the city of Rio de Janeiro, also in the Southeast, in the Manguinhos Community, where an anti-HEV prevalence of 2.4% was found among 699 individuals [61]. More recently, in a small municipality in the state of São Paulo, a prevalence of 20% of anti-HEV was found among 248 individuals, with an association of the marker with the consumption of raw meat [54]. This is also indicated in Table 1.
Among blood donors, an increase in prevalence is observed in the South region of Brazil. In fact, the first article published in this country in 1997 involved 200 blood donors from Salvador, in the Northeast region, where an anti-HEV prevalence of 2% was noted [15]. Subsequently, in another two studies in this region, prevalences of 0.9% among 996 donors in Recife and 1.35% among 890 donors in Teresina were observed, both in the Brazilian Northeast [33, 36]. On the other hand, in Santa Catarina, an anti-HEV prevalence of 10% was observed among 300 blood donors [18]. Furthermore, in the neighboring state of Rio Grande do Sul, prevalences of 7.1% among 281 blood donors and 18.7% among 80 blood donors were found [65].
In general, in practically all studies, an increase in the prevalence of anti-HEV is observed with increasing age of the evaluated individuals [43, 50,53]. This aspect has already been described in a meta-analysis of European studies and is likely due to a longer duration of exposure to HEV [83]. Indeed, some studies have revealed higher anti-HEV prevalence associated with longer exposure to the virus, such as longer crack cocaine use, longer HIV infection duration, or longer residence in rural settlements [28, 32, 39].
Another interesting aspect in Brazilian studies regards the higher prevalence of HEV in patients with more advanced liver disease. In fact, some articles have documented a higher prevalence of anti-HEV in cirrhotic patients with advanced fibrosis and diabetes mellitus [57, 65]. Two articles involving patients from the Brazilian Northeast, where Schistosomiasis mansoni is endemic, revealed high prevalence of anti-HEV in patients with this parasitosis. Moreover, associations of the HEV marker with more advanced forms of schistosomiasis were also observed, raising the possibility that the virus may have worsened the evolution of the parasitosis or that more severe patients had a higher risk of contamination [31,35].
The increased risk of HEV contamination in patients with schistosomiasis may be due to a lack of sanitation and treated water in endemic regions. Indeed, some studies in Brazil reveal a higher risk of HEV contamination in areas with inadequate sewage systems, such as in rural settlements [39, 42, 45].
These findings may suggest that genotypes 1 or 2 of HEV circulate in Brazil, which present transmission via the fecal-oral route, as occurs in regions of Africa and Asia [7, 8]. However, in these regions lacking adequate sanitation infrastructure, in rural areas, domestic pig farming and consumption of game meat also occur, which is strongly related to genotypes 3 or 4 of HEV, considered zoonotic transmission [7, 8,68].
In fact, research on Brazilian studies regarding the prevalence of HEV markers in pigs reveals quite high percentages in four regions of the country, except for the North region, ranging between 60 and 80% of swine. Additionally, in virtually all studies that researched the genotype, HEV-3 was found (Table 2). Moreover, in the four studies in humans where HEV genotype research was conducted, variants of HEV-3 were found in all [28, 49, 58, 64].
Supporting these findings, in Brazil there are studies revealing a higher occurrence of anti-HEV associated with pig farming and consumption of pork and game meat [26, 34, 38, 40, 51]. It is noteworthy that in the Southeast and South regions of Brazil, where there was greater influence from Italian and German cultures, the climate is temperate and there is a habit of raising pigs for consumption of meat and its smoked derivatives during winter. Often, these farms are domestic and not very well-regulated by health surveillance agencies.
The main limitation of this review refers to the scarcity of robust studies involving significant samples of the Brazilian population across the five regions of the country, in large cities of the industrialized regions and in small municipalities in rural areas. Moreover, the heterogeneity of the studies regarding sample size, differences in ELISA kits used, and peculiarities of the various groups evaluated also pose challenges.
In conclusion, based on the findings of this review, it can be considered that HEV infection occurs in all five regions of Brazil, with higher prevalence in the South and Southeast regions. The circulating genotype in the country is HEV-3, possibly transmitted through pig consumption and breeding.
Author Contributions
“Conceptualization, C.A.M and E.P.L.; methodology, C.A.M and E.P.L.; software, C.A.M., L.R.M.G.A and E.P.L.; validation, C.A.M., L.R.M.G.A and E.P.L.; formal analysis, C.A.M., L.R.M.G.A and E.P.L.; investigation, C.A.M., L.R.M.G.A and E.P.L.; data curation, C.A.M. and L.R.M.G.A; writing—original draft preparation, C.A.M., L.R.M.G.A and E.P.L ; writing—review and editing, C.A.M., L.R.M.G.A and E.P.L; visualization, C.A.M., L.R.M.G.A and E.P.LX.X.; supervision, E.P.L; project administration, E.P.L.; All authors have read and agreed to the published version of the manuscript.”
Funding
This research received no external funding.
Data Availability Statement
No new data were created or analyzed in this study. Data sharing is not applicable to this article.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| ELISA | Enzyme-Linked Immunosorbent Assay |
| HBV | Hepatitis B virus |
| HCV | Hepatitis C virus |
| HEV | Hepatitis E virus |
| JBI | Joanna Briggs Institute |
| PCC | Population, Concept, and Context |
| PRISMA-ScR | Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews |
| WHO | World Health Organization |
References
- Debing, Y.; Moradpour, D.; Neyts, J.; Gouttenoire, J. Update on hepatitis E virology: Implications for clinical practice. J Hepatol 2016, 65, 200–212. [Google Scholar] [CrossRef]
- World Health Organization. Hepatitis E. 2025. Available online: https://www.who.int/news-room/fact-sheets/detail/hepatitis-e (accessed on 12 may 2025).
- Institute for Health Metrics and Evaluation (IHME). Acute hepatitis E—Level 4 cause. 2021. Available online: https://www.healthdata.org/research-analysis/diseases-injuries-risks/factsheets/2021-acute-hepatitis-e-level-4-disease (accessed on 12 may 2025).
- Purdy, M. A.; Drexler, J. F.; Meng, X. J.; Norder, H.; Okamoto, H.; Van der Poel, W. H. M.; Reuter, G.; de Souza, W. M.; Ulrich, R. G.; Smith, D. B. ICTV Virus Taxonomy Profile: Hepeviridae. The Journal of general virology 2022, 103, 10. [Google Scholar] [CrossRef]
- Wang, B.; Meng, X.J. Hepatitis E virus: host tropism and zoonotic infection. Curr Opin Microbiol 2021, 59, 8–15. [Google Scholar] [CrossRef] [PubMed]
- Kamar, N.; Bendall, R.; Legrand-Abravanel, F.; Xia, N. S.; Ijaz, S.; Izopet, J.; Dalton, H. R. Hepatitis E. Lancet 2012, 379, 2477–2488. [Google Scholar] [CrossRef] [PubMed]
- Abravanel, F.; Lhomme, S.; El Costa, H.; Schvartz, B.; Peron, J. M.; Kamar, N.; Izopet, J. Rabbit Hepatitis E Virus Infections in Humans, France. Emerging infectious diseases 2017, 23, 1191–1193. [Google Scholar] [CrossRef]
- Velavan, T. P.; Pallerla, S. R.; Johne, R.; Todt, D.; Steinmann, E.; Schemmerer, M.; Wenzel, J. J.; Hofmann, J.; Shih, J. W. K.; Wedemeyer, H.; Bock, C. T. Hepatitis E: An update on One Health and clinical medicine. Liver international 2021, 41, 1462–1473. [Google Scholar] [CrossRef]
- Moraes, D. F. D. S. D.; Mesquita, J. R.; Dutra, V.; Nascimento, M. S. J. Systematic Review of Hepatitis E Virus in Brazil: A One-Health Approach of the Human-Animal-Environment Triad. Animals (Basel) 2021, 11, 2290. [Google Scholar] [CrossRef]
- Kamar, N.; Dalton, H. R.; Abravanel, F.; Izopet, J. Hepatitis E virus infection. Clin Microbiol Rev 2014, 27, 116–38. [Google Scholar] [CrossRef]
- Spahr, C.; Knauf-Witzens, T.; Vahlenkamp, T.; Ulrich, R.G.; Johne, R. Hepatitis E virus and related viruses in wild, domestic and zoo animals: A review. Zoonoses Public Health 2018, 65, 11–29. [Google Scholar] [CrossRef]
- Li, P.; Liu, J.; Li, Y.; Su, J.; Ma, Z.; Bramer, W. M.; Cao, W.; de Man, R. A.; Peppelenbosch, M. P.; Pan, Q. The global epidemiology of hepatitis E virus infection: A systematic review and meta-analysis. Liver international 2020, 40, 1516–1528. [Google Scholar] [CrossRef] [PubMed]
- Magri, M. C.; Manchiero, C.; Dantas, B. P.; Bernardo, W. M.; Abdala, E.; Tengan, F. M. Prevalence of hepatitis E in Latin America and the Caribbean: A systematic review and meta-analysis. Public health 2025, 244, 105745. [Google Scholar] [CrossRef] [PubMed]
- Passos, A.M.; Heringer, T.P.; Medina-Pestana, J.O.; Ferraz, M.L.; Granato, C.F. First report and molecular characterization of hepatitis E virus infection in renal transplant recipients in Brazil. J Med Virol 2013, 85, 615–619. [Google Scholar] [CrossRef] [PubMed]
- Parana, R. , Cotrim, H. P.; Cortey-Boennec, M.L.; Trepo, C.; Lyra, L. Prevalence of hepatitis E virus IgG antibodies in patients from a referral unit of liver diseases in Salvador, Bahia, Brazil. Am J Trop Med Hyg 1997, 57, 60–61. [Google Scholar]
- de la Caridad Montalvo Villalba, M.; Owot, J. C.; Benedito, E. C.; Corredor, M. B.; Flaquet, P. P.; Frometa, S. S.; Wong, M. S.; Rodríguez Lay, L. deL. Hepatitis E virus genotype 3 in humans and swine, Cuba. Infection, genetics and evolution 2013, 14, 335–339. [Google Scholar]
- Kiesslich, D.; Rocha júnior, J.E.; Crispim, M.A. Prevalence of hepatitis E virus antibodies among different groups in the Amazonian basin. Trans R Soc Trop Med Hyg 2002, 96, 215. [Google Scholar] [CrossRef] [PubMed]
- Passos-Castilho, A.M.; de Sena, A.; Geraldo, A.; Spada, C.; Granato, C.F. High prevalence of hepatitis E virus antibodies among blood donors in Southern Brazil. J Med Virol 2016, 88, 361–364. [Google Scholar] [CrossRef]
- Tengan, F. M.; Figueiredo, G. M.; Nunes, A. K. S.; Manchiero, C.; Dantas, B. P.; Magri, M. C.; Prata, T. V. G.; Nascimento, M.; Mazza, C. C.; Abdala, E.; Barone, A. A.; Bernardo, W. M. Seroprevalence of hepatitis E in adults in Brazil: a systematic review and meta-analysis. Infectious diseases of poverty 2019, 8, 3. [Google Scholar] [CrossRef]
- Songtanin, B.; Molehin, A. J.; Brittan, K.; Manatsathit, W.; Nugent, K. Hepatitis E Virus Infections: Epidemiology, Genetic Diversity, and Clinical Considerations. Viruses 2023, 15, 1389. [Google Scholar] [CrossRef]
- Peters, M. D. J.; Godfrey, C.; McInerney, P.; Khalil, H.; Larsen, P.; Marnie, C.; Pollock, D.; Tricco, A. C.; Munn, Z. Best practice guidance and reporting items for the development of scoping review protocols. JBI evidence synthesis 2022, 20, 953–968. [Google Scholar] [CrossRef]
- Tricco, A. C.; Lillie, E.; Zarin, W.; O'Brien, K. K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M. D. J.; Horsley, T.; Weeks, L.; Hempel, S.; Akl, E. A.; Chang, C.; McGowan, J.; Stewart, L.; Hartling, L.; Aldcroft, A.; Wilson, M. G.; Garritty, C.; Lewin, S.; … Straus, S. E. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Annals of internal medicine 2018, 169, 467–473. [Google Scholar] [CrossRef]
- Haddaway, N. R.; Page, M. J.; Pritchard, C. C.; McGuinness, L. A. PRISMA2020: An R package and Shiny app for producing PRISMA 2020-compliant flow diagrams, with interactivity for optimised digital transparency and Open Synthesis Campbell Systematic Reviews 2022, 18, e1230.
- Vitral, C.L.; da Silva-Nunes, M.; Pinto, M.A.; et al. Hepatitis A and E seroprevalence and associated risk factors: a community-based cross-sectional survey in rural Amazonia. BMC Infect. Dis. 2014, 14, 458. [Google Scholar] [CrossRef]
- Vasconcelos, M.P.A.; de Oliveira, J.M.; Sánchez-Arcila, J.C.; et al. Seroprevalence of the Hepatitis E Virus in Indigenous and Non-Indigenous Communities from the Brazilian Amazon Basin. Microorganisms 2024, 12, 365. [Google Scholar] [CrossRef]
- Souza, A.J.S.; Oliveira, C.M.A.; Sarmento, V.P.; et al. Hepatitis E virus infection among rural Afro-descendant communities from the eastern Brazilian Amazon. Rev. Soc. Bras. Med. Trop. 2018, 51, 803–807. [Google Scholar] [CrossRef] [PubMed]
- Souza, A.J.S.; Malheiros, A.P.; Sarmento, V.P.; et al. Serological and molecular retrospective analysis of hepatitis E suspected cases from the Eastern Brazilian Amazon 1993–2014. Rev. Soc. Bras. Med. Trop. 2019, 52, e20180465. [Google Scholar] [CrossRef] [PubMed]
- Nascimento, R.S.; Baia, K.L.N.; de Souza, S.B.; et al. Hepatitis E Virus in People Who Use Crack-Cocaine: A Cross-Sectional Study in a Remote Region of Northern Brazil. Viruses 2021, 13, 926. [Google Scholar] [CrossRef]
- Paraná, R.; Vitvitski, L.; Andrade, Z.; et al. Acute sporadic non-A, non-B hepatitis in Northeastern Brazil: etiology and natural history. Hepatology 1999, 30, 289–293. [Google Scholar] [CrossRef] [PubMed]
- Lyra, A.C.; Pinho, J.R.; Silva, L.K.; et al. HEV, TTV and GBV-C/HGV markers in patients with acute viral hepatitis. Braz. J. Med. Biol. Res. 2005, 38, 767–775. [Google Scholar] [CrossRef]
- Passos-Castilho, A.M.; de Sena, A.; Domingues, A.L.; et al. Hepatitis E virus seroprevalence among schistosomiasis patients in Northeastern Brazil. Braz. J. Infect. Dis. 2016, 20, 262–266. [Google Scholar] [CrossRef]
- Bezerra, L.A.; de Oliveira-Filho, E.F.; Silva, J.V.J. Júnior; et al. Risk analysis and seroprevalence of HEV in people living with HIV/AIDS in Brazil. Acta Trop. 2019, 189, 65–68. [Google Scholar]
- Cunha, G.G.; Bezerra, L.A.; Silva Júnior, J.V.J.; Gonçales, J.P.; Montreuil, A.C.B.; Côelho, M.R.C.D. Analysis of seroprevalence and risk factors for hepatitis E virus (HEV) in donation candidates and blood donors in Northeast Brazil. Braz. J. Microbiol. 2022, 53, 1995–2001. [Google Scholar] [CrossRef]
- Araújo, L.R.M.G.; Batista, A.D.; Côelho, M.R.C.D.; et al. Seroprevalence of hepatitis E virus in patients with chronic liver disease. Braz. J. Microbiol. 2024, 55, 357–364. [Google Scholar] [CrossRef]
- Gomes, C.T.O.; Mariz, C.A.; Batista, A.D.; et al. Seroprevalence of Hepatitis E Virus Among Schistosomiasis mansoni Patients Residing in Endemic Zone in Brazil. Trop. Med. Infect. Dis. 2024, 9, 310. [Google Scholar] [CrossRef]
- Silva-Sampaio, J.P.; Sinimbu, R.B.; Marques, J.T.; Neto, A.F.O.; Villar, L.M. Seroprevalence of hepatitis E virus infection in blood donors from Piauí State, Northeast Brazil. Braz. J. Infect. Dis. 2025, 29, 104466. [Google Scholar] [CrossRef]
- Martins, R.M.; Freitas, N.R.; Kozlowski, A.; et al. Seroprevalence of hepatitis E antibodies in a population of recyclable waste pickers in Brazil. J. Clin. Virol. 2014, 59, 188–191. [Google Scholar] [CrossRef]
- Freitas, N.R.; Santana, E.B.; Silva, Á.M.; et al. Hepatitis E virus infection in patients with acute non-A, non-B, non-C hepatitis in Central Brazil. Mem. Inst. Oswaldo Cruz 2016, 111, 692–696. [Google Scholar] [CrossRef]
- Freitas, N.R.; Teles, S.A.; Caetano, K.A.A.; et al. Hepatitis E seroprevalence and associated factors in rural settlers in Central Brazil. Rev. Soc. Bras. Med. Trop. 2017, 50, 675–679. [Google Scholar] [CrossRef]
- Oliveira, J.M.N.S.; Freitas, N.R.; Teles, S.A.; et al. Prevalence of hepatitis E virus RNA and antibodies in a cohort of kidney transplant recipients in Central Brazil. Int. J. Infect. Dis. 2018, 69, 41–43. [Google Scholar] [CrossRef]
- Teles, S. A.; Caetano, K. A. A.; Carneiro, M. A. D. S.; Villar, L. M.; Stacciarini, J. M.; Martins, R. M. B. Hepatitis E Prevalence in Vulnerable Populations in Goiânia, Central Brazil. Viruses 2023, 15, 2070. [Google Scholar] [CrossRef] [PubMed]
- Assis, S.B.; Souto, F.J.; Fontes, C.J.; Gaspar, A.M. Prevalence of hepatitis A and E virus infection in school children of an Amazonian municipality in Mato Grosso State. Rev. Soc. Bras. Med. Trop. 2002, 35, 155–158. [Google Scholar] [CrossRef] [PubMed]
- Silva, S.M.; Oliveira, J.M.; Vitral, C.L.; Vieira, K.A.; Pinto, M.A.; Souto, F.J. Prevalence of hepatitis E virus antibodies in individuals exposed to swine in Mato Grosso, Brazil. Mem. Inst. Oswaldo Cruz 2012, 107, 338–341. [Google Scholar] [CrossRef] [PubMed]
- Castro, V.O.L.; Tejada-Strop, A.; Weis, S.M.S.; et al. Evidence of hepatitis E virus infections among persons who use crack cocaine from the Midwest region of Brazil. J. Med. Virol. 2019, 91, 151–154. [Google Scholar] [CrossRef]
- Weis-Torres, S.M.D.S.; França, A.O.; Granato, C.; Passarini, A.; Motta-Castro, A.R.C. Seroprevalence of hepatitis E virus infection among volunteer blood donors in Central Brazil. Braz. J. Infect. Dis. 2022, 26, 102350. [Google Scholar] [CrossRef]
- Focaccia, R.; da Conceição, O.J.; Sette, H. Jr.; Sabino, E.; Bassit, L.; Nitrini, D.R.; et al. Estimated Prevalence of Viral Hepatitis in the General Population of the Municipality of São Paulo, Measured by a Serologic Survey of a Stratified, Randomized and Residence-Based Population. Braz J Infect Dis 1998, 2, 269–284. [Google Scholar]
- Gonçales, N.S.; Pinho, J.R.; Moreira, R.C.; et al. Hepatitis E virus immunoglobulin G antibodies in different populations in Campinas, Brazil. Clin. Diagn. Lab. Immunol. 2000, 7, 813–816. [Google Scholar] [CrossRef]
- Hering, T.; Passos, A.M.; Perez, R.M.; et al. Past and current hepatitis E virus infection in renal transplant patients. J. Med. Virol. 2014, 86, 948–953. [Google Scholar] [CrossRef] [PubMed]
- Passos-Castilho, A.M.; de Sena, A.; Reinaldo, M.R.; Granato, C.F. Hepatitis E virus infection in Brazil: results of laboratory-based surveillance from 1998 to 2013. Rev. Soc. Bras. Med. Trop. 2015, 48, 468–470. [Google Scholar] [CrossRef]
- Passos-Castilho, A.M.; Reinaldo, M.R.; Sena, A.; Granato, C.F.H. High prevalence of hepatitis E virus antibodies in Sao Paulo, Southeastern Brazil: analysis of a group of blood donors representative of the general population. Braz. J. Infect. Dis. 2017, 21, 535–539. [Google Scholar] [CrossRef] [PubMed]
- Bricks, G.; Senise, J.F.; Pott Junior, H.; et al. Seroprevalence of hepatitis E virus in chronic hepatitis C in Brazil. Braz. J. Infect. Dis. 2018, 22, 85–91. [Google Scholar] [CrossRef]
- Ferreira, A.C.; Gomes-Gouvêa, M.S.; Lisboa-Neto, G.; et al. Serological and molecular markers of hepatitis E virus infection in HIV-infected patients in Brazil. Arch. Virol. 2018, 163, 43–49. [Google Scholar] [CrossRef]
- Bricks, G.; Senise, J.F.; Pott-Jr, H.; et al. Previous hepatitis E virus infection, cirrhosis and insulin resistance in patients with chronic hepatitis C. Braz. J. Infect. Dis. 2019, 23, 45–52. [Google Scholar] [CrossRef] [PubMed]
- Araújo, D.C.A.; de Oliveira, J.M.; Haddad, S.K.; et al. Declining prevalence of hepatitis A and silent circulation of hepatitis E virus infection in southeastern Brazil. Int. J. Infect. Dis. 2020, 101, 17–23. [Google Scholar] [CrossRef]
- Conte, D.D.; Luna, L.K.S.; Passarini, A.; et al. Hepatitis E virus infection among patients with altered levels of alanine aminotransferase. Braz. J. Infect. Dis. 2021, 25, 101655. [Google Scholar] [CrossRef] [PubMed]
- Moraes, A.C.P.; Gouvea, M.G.; Ferreira, A.C.; et al. The impact of hepatitis E infection on hepatic fibrosis in liver transplanted patients for hepatitis C infection. Braz. J. Infect. Dis. 2021, 25, 101587. [Google Scholar] [CrossRef]
- Zitelli, P.M.Y.; Gomes-Gouvêa, M.; Mazo, D.F.; et al. Hepatitis E virus infection increases the risk of diabetes and severity of liver disease in patients with chronic hepatitis C virus infection. Clinics (Sao Paulo) 2021, 76, e3270. [Google Scholar]
- Ribeiro, L.B.; Reche, L.A.; Nastri, A.C.S.S.; et al. Acute Hepatitis Related to Hepatitis E Virus Genotype 3f Infection in Brazil. J. Med. Virol. 2024, 96, e70024. [Google Scholar] [CrossRef]
- Zicker, M.; Pinho, J.R.R.; Welter, E.A.R.; et al. The Risk of Reinfection or Primary Hepatitis E Virus Infection at a Liver Transplant Center in Brazil: An Observational Cohort Study. Viruses 2024, 16, 301. [Google Scholar] [CrossRef]
- Trinta, K.S.; Liberto, M.I.; de Paula, V.S.; Yoshida, C.F.; Gaspar, A.M. Hepatitis E virus infection in selected Brazilian populations. Mem. Inst. Oswaldo Cruz 2001, 96, 25–29. [Google Scholar] [CrossRef]
- Santos, D.C.; Souto, F.J.; Santos, D.R.; Vitral, C.L.; Gaspar, A.M. Seroepidemiological markers of enterically transmitted viral hepatitis A and E in individuals living in a community located in the North Area of Rio de Janeiro, RJ, Brazil. Mem. Inst. Oswaldo Cruz 2002, 97, 637–640. [Google Scholar] [CrossRef]
- Bortoliero, A.L.; Bonametti, A.M.; Morimoto, H.K.; Matsuo, T.; Reiche, E.M. Seroprevalence for hepatitis E virus (HEV) infection among volunteer blood donors of the Regional Blood Bank of Londrina, State of Paraná, Brazil. Rev. Inst. Med. Trop. Sao Paulo 2006, 48, 87–92. [Google Scholar] [CrossRef] [PubMed]
- Hardtke, S.; Rocco, R.; Ogata, J.; et al. Risk factors and seroprevalence of hepatitis E evaluated in frozen-serum samples (2002–2003) of pregnant women compared with female blood donors in a Southern region of Brazil. J. Med. Virol. 2018, 90, 1856–1862. [Google Scholar] [CrossRef] [PubMed]
- Moss da Silva, C.; Oliveira, J.M.; Mendoza-Sassi, R.A.; et al. Detection and characterization of hepatitis E virus genotype 3 in HIV-infected patients and blood donors from southern Brazil. Int. J. Infect. Dis. 2019, 86, 114–121. [Google Scholar] [CrossRef] [PubMed]
- Costa, M.B.; Gouvêa, M.S.G.; Chuffi, S.; et al. Seroprevalence of hepatitis E virus in risk populations and blood donors in a referral hospital in the south of Brazil. Sci. Rep. 2021, 11, 6011. [Google Scholar] [CrossRef]
- Zorzetto, R.; Klein, R.L.; Erpen, L.M.S.; et al. Unusual high prevalence of antibodies to hepatitis E virus in South Brazil. FEMS Microbiol. Lett. 2021, 368, fnab076. [Google Scholar] [CrossRef] [PubMed]
- Souza, A.J.; Gomes-Gouvêa, M.S.; Soares, M.d.C.; et al. HEV infection in swine from Eastern Brazilian Amazon: evidence of co-infection by different subtypes. Comp. Immunol. Microbiol. Infect. Dis. 2012, 35, 477–485. [Google Scholar] [CrossRef] [PubMed]
- Oliveira-Filho, E.F.; Lopes, K.G.S.; Cunha, D.S.; et al. Risk Analysis and Occurrence of Hepatitis E Virus (HEV) in Domestic Swine in Northeast Brazil. Food Environ. Virol. 2017, 9, 256–259. [Google Scholar] [CrossRef]
- Oliveira-Filho, E.F.; Dos Santos, D.R.; Durães-Carvalho, R.; et al. Evolutionary study of potentially zoonotic hepatitis E virus genotype 3 from swine in Northeast Brazil. Mem. Inst. Oswaldo Cruz 2019, 114, e180585. [Google Scholar] [CrossRef]
- Costa Lana, M.V.; Gardinali, N.R.; da Cruz, R.A.; et al. Evaluation of hepatitis E virus infection between different production systems of pigs in Brazil. Trop. Anim. Health Prod. 2014, 46, 399–404. [Google Scholar] [CrossRef]
- Campos, C.G.; Silveira, S.; Schenkel, D.M.; et al. Detection of hepatitis E virus genotype 3 in pigs from subsistence farms in the state of Mato Grosso, Brazil. Comp. Immunol. Microbiol. Infect. Dis. 2018, 58, 11–16. [Google Scholar] [CrossRef]
- Vitral, C.L.; Pinto, M.A.; Lewis-Ximenez, L.L.; Khudyakov, Y.E.; dos Santos, D.R.; Gaspar, A.M. Serological evidence of hepatitis E virus infection in different animal species from the Southeast of Brazil. Mem. Inst. Oswaldo Cruz 2005, 100, 117–122. [Google Scholar] [CrossRef]
- Santos, D.R.; de Paula, V.S.; de Oliveira, J.M.; Marchevsky, R.S.; Pinto, M.A. Hepatitis E virus in swine and effluent samples from slaughterhouses in Brazil. Vet. Microbiol. 2011, 149, 236–241. [Google Scholar] [CrossRef]
- Amorim, A.R.; Mendes, G.S.; Pena, G.P.A.; Santos, N. Hepatitis E virus infection of slaughtered healthy pigs in Brazil. Zoonoses Public Health 2018, 65, 501–504. [Google Scholar] [CrossRef]
- Cortez, A.; Metorima, C.S.; Miyagi, S.A.T.; Sousa, A.O.; Peyser, A.V.; Castro, A.M.M.G.; et al. High genetic diversity of hepatitis E virus in swine in São Paulo State, Brazil. Arq. Bras. Med. Vet. Zootec. 2021, 73, 1237–1242. [Google Scholar] [CrossRef]
- Gardinali, N.R.; Barry, A.F.; da Silva, P.F.; de Souza, C.; Alfieri, A.F.; Alfieri, A.A. Molecular detection and characterization of hepatitis E virus in naturally infected pigs from Brazilian herds. Res. Vet. Sci. 2012, 93, 1515–1519. [Google Scholar] [CrossRef] [PubMed]
- Passos-Castilho, A.M.; Granato, C.F.H. High frequency of hepatitis E virus infection in swine from South Brazil and close similarity to human HEV isolates. Braz. J. Microbiol. 2017, 48, 373–379. [Google Scholar] [CrossRef]
- Silva, M.S.; Silveira, S.; Caron, V.S.; et al. Backyard pigs are a reservoir of zoonotic hepatitis E virus in southern Brazil. Trans. R. Soc. Trop. Med. Hyg. 2018, 112, 14–21. [Google Scholar] [CrossRef] [PubMed]
- Mariz, C. A.; Braga, C.; Albuquerque, M.F. P. M.; Luna, C. F.; Salustiano, D. M.; Freire, N. M.; Morais, C. N. L.; Lopes, E. P. Occurrence of hepatitis B and C virus infection in socioeconomic population strata from Recife, Pernambuco, Northeast Brazil. Revista Brasileira De Epidemiologia 2024, 27, e240033. [Google Scholar] [CrossRef]
- Polaris Observatory HCV Collaborators. Global change in hepatitis C virus prevalence and cascade of care between 2015 and 2020: a modelling study. Lancet Gastroenterol Hepatol 2022, 7, 396–415.
- Villalobos, N.V.F.; Kessel, B.; Rodiah, I.; Ott, J.J.; Lange, B.; Krause, G. Seroprevalence of hepatitis E virus infection in the Americas: Estimates from a systematic review and meta-analysis. PLOS ONE 2022, 17, e0269253. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, J. M.; Dos Santos, D. R. L.; Pinto, M. A. Hepatitis E Virus Research in Brazil: Looking Back and Forwards. Viruses 2023, 15, 548. [Google Scholar] [CrossRef] [PubMed]
- Hartl, J.; Otto, B.; Madden, R.G.; Webb, G.; Woolson, K.L.; Kriston, L.; et al. Hepatitis E seroprevalence in Europe: a meta-analysis. Viruses 2016, 8, 211. [Google Scholar] [CrossRef]
Figure 1.
Population, Concept, and Context (PCC) Strategy. Pernambuco, Brazil, 2025.
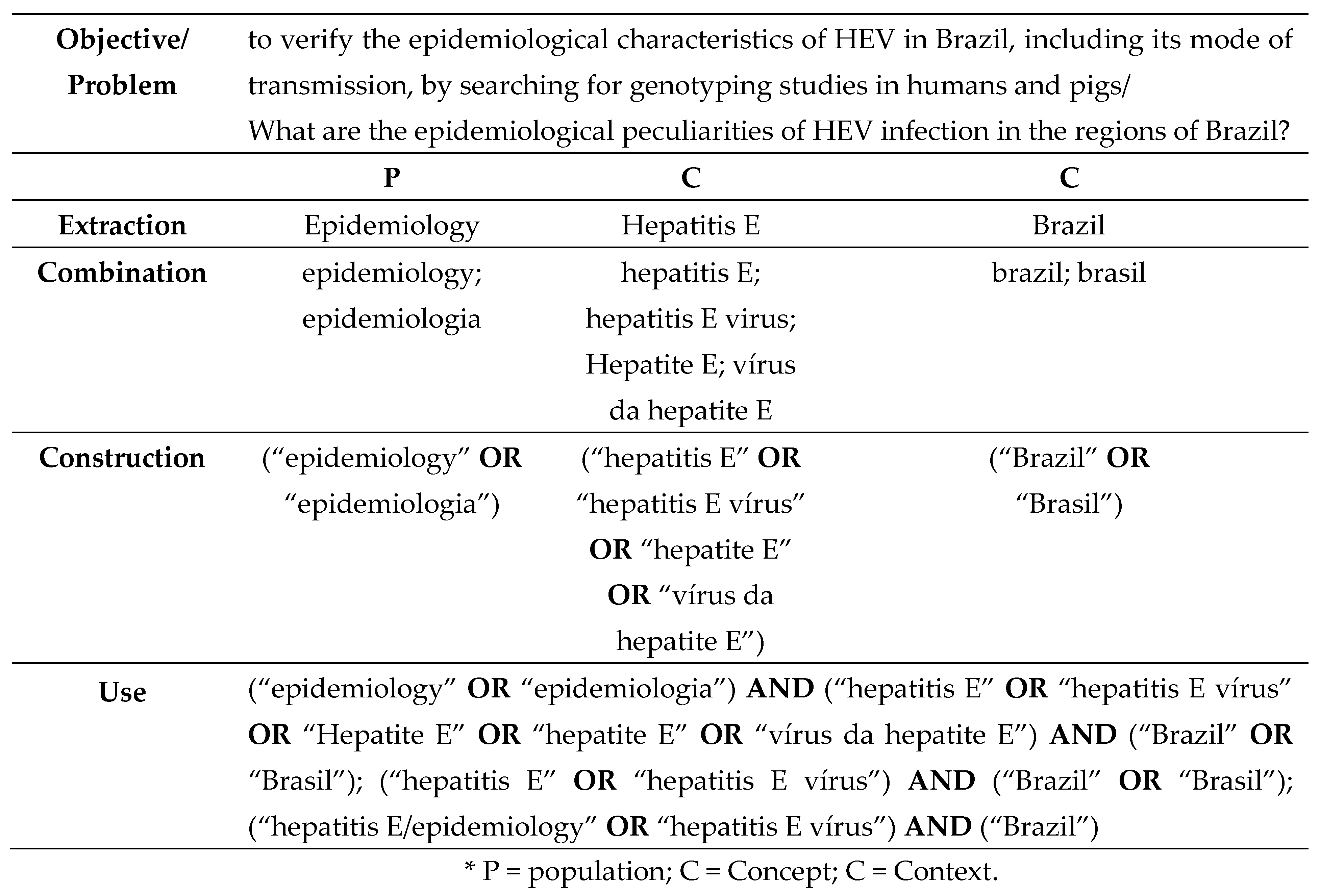
Figure 2.
PRISMA Flow Diagram, generated with the PRISMA Flow Diagram tool [23], schematically visualizing the article selection process.
Figure 2.
PRISMA Flow Diagram, generated with the PRISMA Flow Diagram tool [23], schematically visualizing the article selection process.
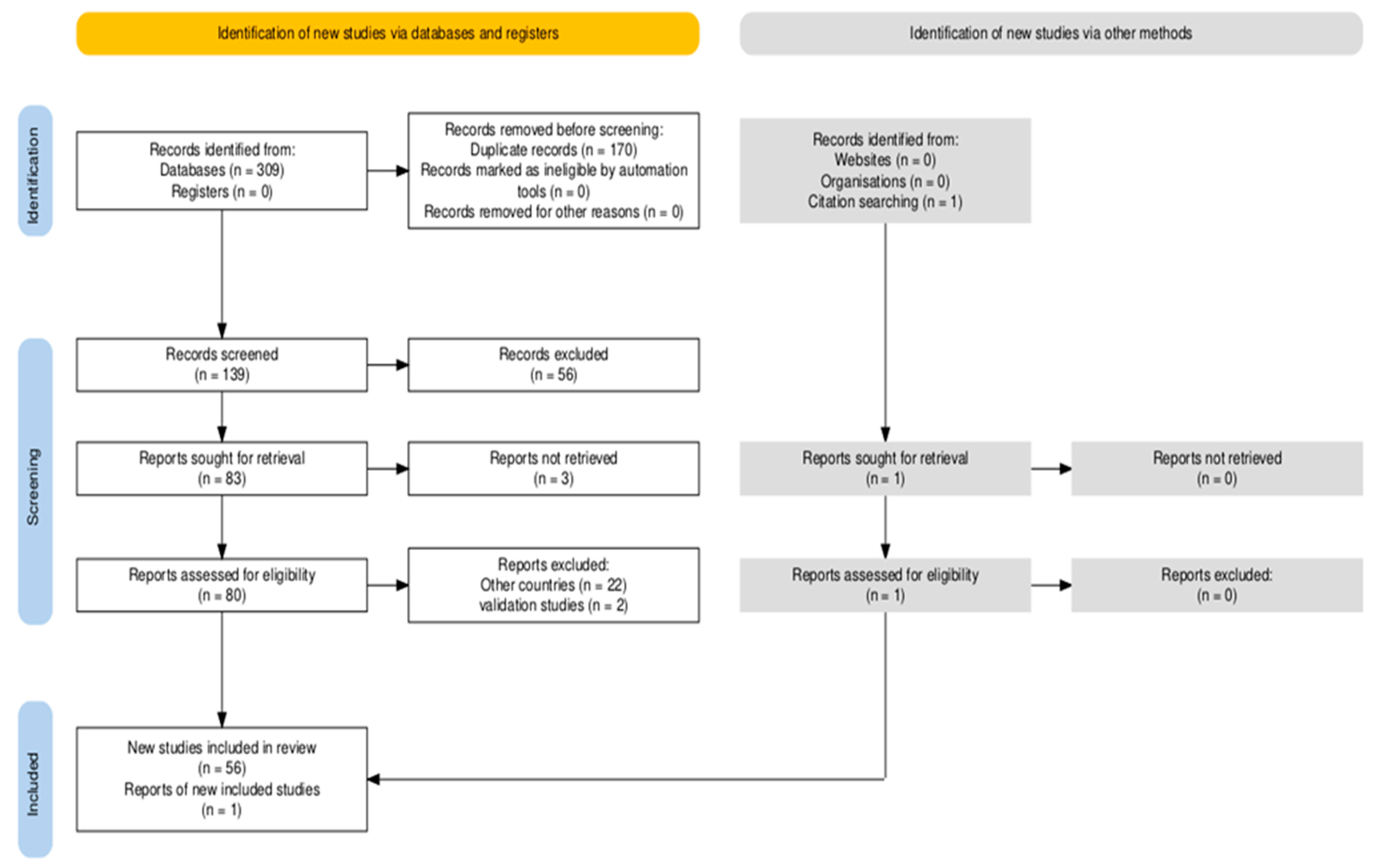
Figure 3.
Prevalence of HEV infection markers (IgG and IgM) in the Brazilian population, according to the five major regions of the country, 1995–2025.
Figure 3.
Prevalence of HEV infection markers (IgG and IgM) in the Brazilian population, according to the five major regions of the country, 1995–2025.
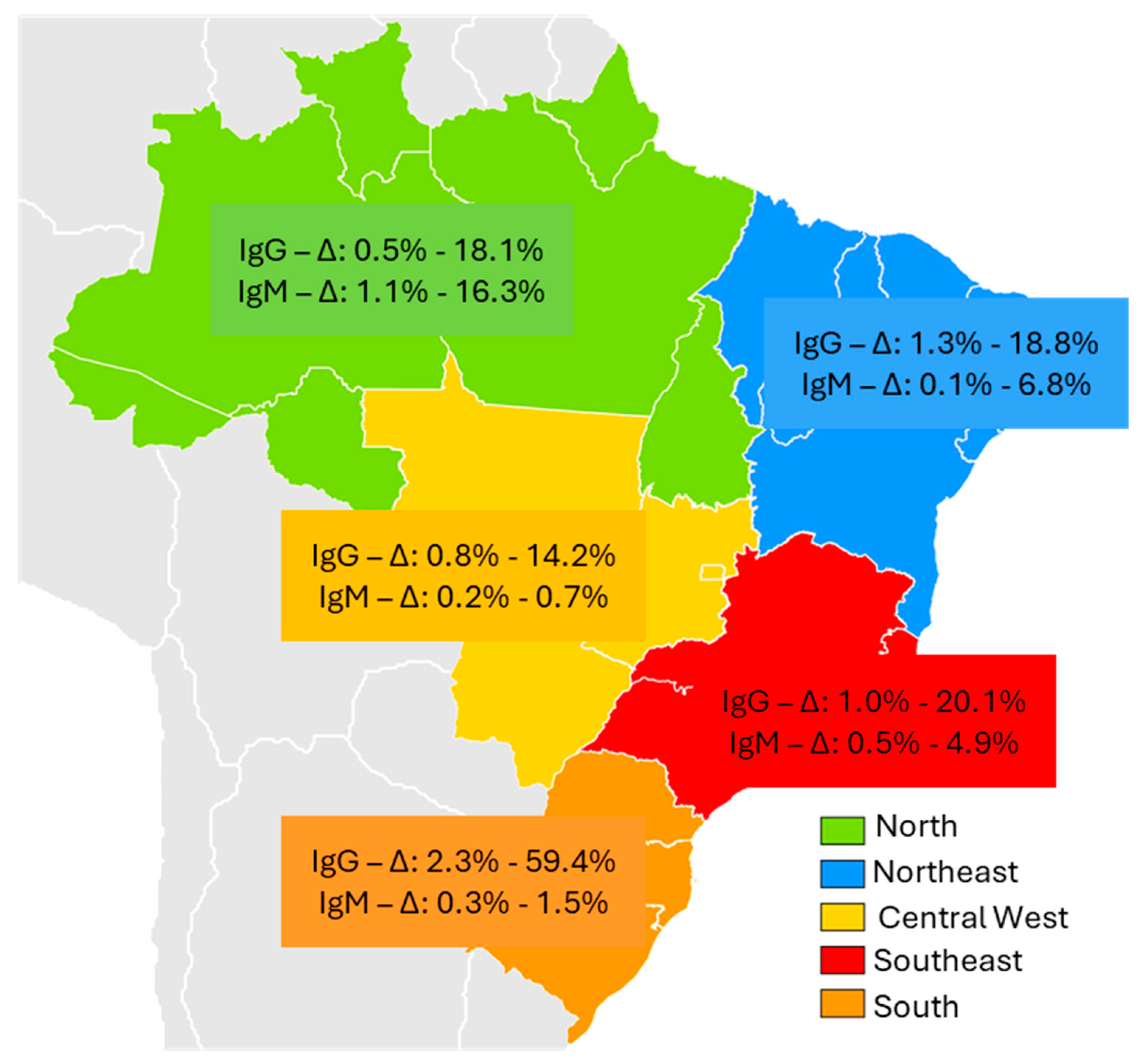
Figure 4.
Distribution of the different phylogenetic subtypes of HEV genotype 3, according to the five major regions of Brazil, 1995–2025.
Figure 4.
Distribution of the different phylogenetic subtypes of HEV genotype 3, according to the five major regions of Brazil, 1995–2025.
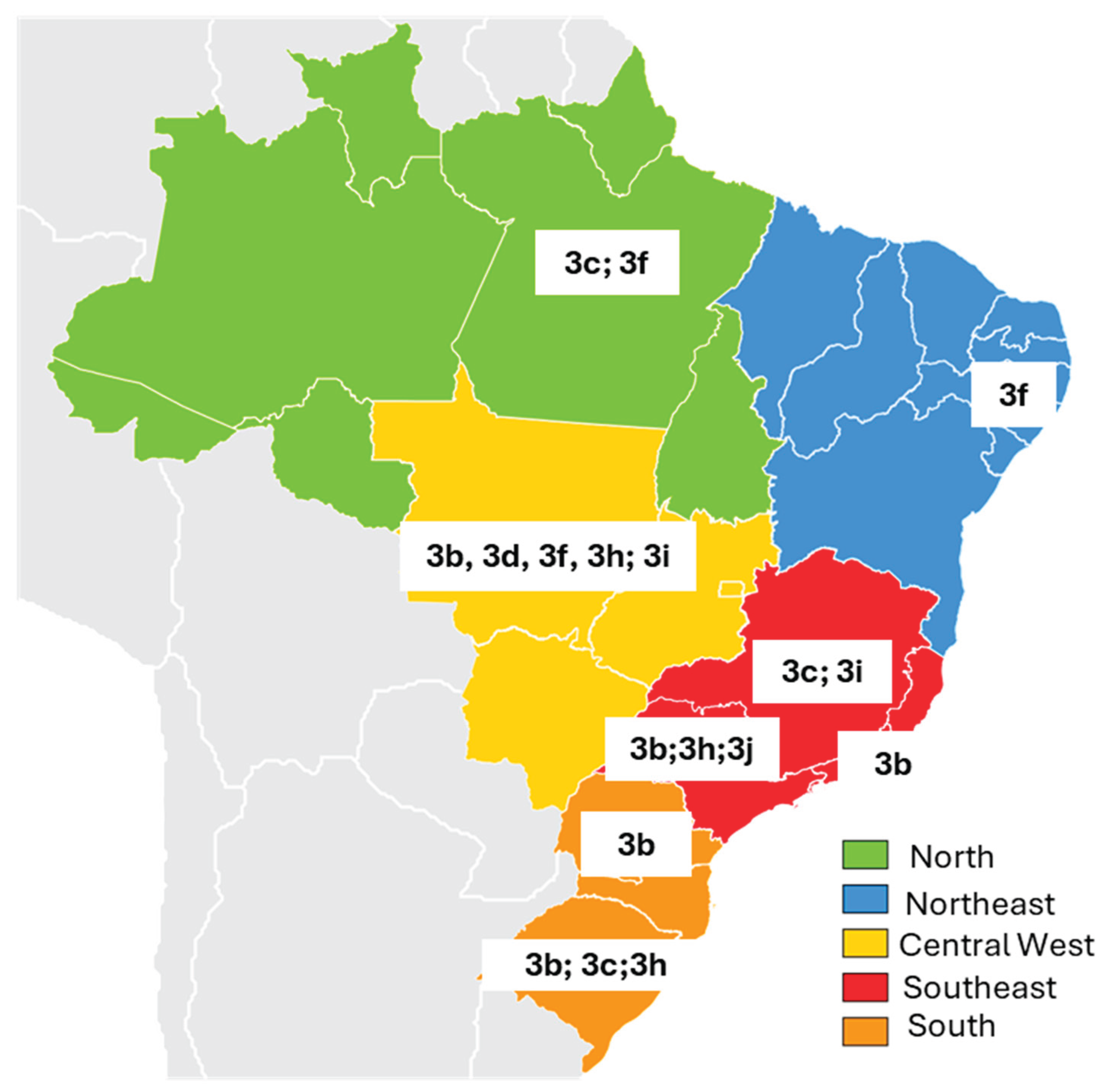

Table 1.
Articles published between 1995 and 2025 describing the prevalence and epidemiological peculiarities of HEV markers in Brazil, according to the five major regions of the country.
Table 1.
Articles published between 1995 and 2025 describing the prevalence and epidemiological peculiarities of HEV markers in Brazil, according to the five major regions of the country.
| Brazil Region | Author/Year | Type of study | Selected population | Epidemiological Peculiarities | Sample size |
Anti-HEV prevalence |
RNA | Genotype | |
| IgG n (%) | IgM n (%) | ||||||||
| North | |||||||||
| Acre | Vitral CL et al., 2014 [24] |
Retrospective cross-sectional | Residents of an agricultural settlement in 2004 | Age > 21 years | 388 | 50 12,8% |
7 16,3% |
n/a | n/a |
| Amazônia/ Rondônia | Vasconcelos MP et al., 2024 [25] | Cross-sectional | Yanomani Indians Urban and rural areas |
HEV in urban areas (2.97%), rural areas (14.2%) and village areas (2.8%) | 811 |
556,8% |
n/a | n/a | n/a |
| Pará | Souza AJS et al., 2018 [26] | Cross-sectional | Afro-descendant community | Young men reported eating bushmeat | 535 | 3 0,5% |
6 1,1% |
negative | n/a |
| Souza AJS et al., 2019 [27] | Cross-sectional | Suspected cases of acute hepatitis | Male gender (55.2%) | 318 | 29 9,1% |
16 5,0% |
Negative | n/a | |
| Nascimento RS et al., 2021 [28] | Cross-sectional | Crack cocaine users | Poorer and homeless; longer use of crack cocaine | 437 | 79 18,1% |
6 1,4% |
Positive | 3c | |
| Northeast | |||||||||
| Bahia | Paraná R et al., 1997 [15] | Retrospective cross-sectional | 200 Blood donors 392 hemodialyzed |
Blood donors | 200 | 4 2% |
n/a | n/a | n/a |
| Paraná R et al. 1999 [29] | Cross-sectional | Acute sporadic non-A, non-B (NANB) | Aminotransferses elevation. | 43 |
512% |
negative | n/a | n/a | |
| Lyra AC et al., 2005 [30] | Cross-sectional | Patients with acute viral hepatitis | Higher prevalence of HEV in patients with acute hepatitis | 73 | 21 28,8% |
56.8% |
n/a | n/a | |
| Pernambuco | Passos-Castilho AM et al., 2016 [31] | Retrospective cross-sectional | Patients with schistosomiasis mansoni | Patients treated at a referral hospital with advanced forms of the disease | 80 | 15 18,8% |
negative | negative | n/a |
| Bezerra LA et al., 2019 [32] | Cross-sectional | People living with HIV/AIDS | Higher HIV infection time | 366 | 15 4,1% |
n/a | Negative | n/a | |
| Cunha GG et al., 2022 [33] | Cross-sectional | Blood candidates and donors | All male gender, consumption of pork and chicken | 996 | 9 0,9% |
n/a | n/a | n/a | |
| Araújo LRMG et al., 2024 [34] | Cross-sectional | Patients with chronic liver disease | Contact with pigs and more advanced liver disease | 227 | 7 3,08% |
n/a | negative | n/a | |
| Gomes CTO et al., 2024 [35] | Retrospective cross-sectional | Patients with schistosomiasis mansoni | More advanced periportal fibrosis (Niamey D/E/F) | 286 | 15 5.24% |
Negative | Negative | n/a | |
| Piaui | Silva-Sampaio JP et al., 2025 [36] | Cross-sectional | Blood donors | 66.7% male gender, 75% age ≥ 30 years |
890 | 12 1,35% |
1 0,1% |
negative | n/a |
| Central West | |||||||||
| Goiás | Martins RM et al., 2014 [37] | Prevalence survey | Recyclable material collectors | Contact with human feces (87.5%) and animal feces (75%) | 431 | 22 5,1% |
3 0,7% |
negative | n/a |
| Freitas NR et al., 2016 [38] | Cross-sectional | Patients with acute viral hepatitis | Consumo carne de porco (95%) e animais selvagens (75%) | 379 | 20 5,3% |
1 0,3% |
negative | n/a | |
| Freitas NR et al., 2017 [39] | Cross-sectional | Rural settlement | 75% male gender, Time in rural settlement > 5 years | 464 | 16 3,4% |
n/a | negative | n/a | |
| Oliveira JMNS et al., 2018 [40] | Cohort | kidney transplant recipients | 100% Previous hemodialysis, Consumption of wild animal meat (87.5%) | 316 | 8 2,5% |
1 0,3% |
negative | n/a | |
| Teles AS et al. 2023 [41] | Cross-sectional | Recyclers, immigrants, refugees, and homeless people | Homeless; Recyclers | 459 | 4 0,87% |
1 0,2% |
negative | ||
| Mato Grosso | Assis SB et al., 2002 [42] | Prevalence survey | School children | Absence of sanitary sewage. | 487 | 22 4,5% |
n/a | n/a | n/a |
| Silva SM et al., 2022 [43] | Cross-sectional | Pig handlers | age ≥ 50 years, Longer exposure to pigs | 310 | 26 8,4% |
n/a | n/a | n/a | |
| Mato Grosso do Sul | Castro VOL et al., 2018 [44] | Cross-sectional | Crack users | Low education level (73.7%), unprotected sexual intercourse | 698 | 99 14,2% |
2 0,28% |
negative | n/a |
| Weis-Torres SMDS et al., 2022 [45] | Retrospective cross-sectional | Blood donors | 75% male, 70% age ≥ 30 years; Lack of sewage system | 250 | 16 6.4% |
Negative | n/a | n/a | |
| Southeast | |||||||||
| São Paulo | Focaccia R et al.,1998 [46] | Prevalence survey | General population | 1,059 | 1.68% | n/a | n/a | n/a | |
| Gonçales NS et al., 2000 [47] | Cross-sectional | Blood donors and staff at a university hospital, | blood donors with elevated ALT, and cleaning staff | 375 | 18 4,8% |
n/a | n/a | n/a | |
| Hering T et al., 2014 [48] | Cross-sectional | Kidney transplant | Transplant patients with elevated aminotransferases | 192 | 28 15% |
n/a | 20 10% |
n/a | |
| Passos-Castilho AM et al., 2015 [49] | Retrospective cross-sectional | Patients with clinical suspicion of HEV | age ≥ 40 years | 2,271 | 47 2,1% |
27 4,9% |
1 | 3b | |
| Passos-Castilho AM et al., 2017 [50] | Cross-sectional | Blood donors | age ≥45 years | 500 | 49 9,8% |
1 | negative | n/a | |
| Bricks G et al., 2018 [51] | Cross-sectional | Chronic HCV patients | contact with pigs and consumption of pork | 618 | 63 10,2% |
negative | n/a | n/a | |
| Ferreira AC et al., 2018 [52] | Cross-sectional | People living with HIV | age ≥40 years | 354 | 38 10,7% |
51,4% |
negative | n/a | |
| Bricks G et al., 2019 [53] | Cross-sectional | Chronic HCV patients | age ≥60 years; contact with pigs | 618 | 63 10,2% |
negative | n/a | n/a | |
| Araújo DCA et al., 2020 [54] | Cross-sectional | Residents of a small municipality in São Paulo | consumption of raw meat | 248 | 50 20,7% |
negative | n/a | n/a | |
| Conte DD et al., 2021 [55] | Cross-sectional | Patients in the Emergency Room with altered levels of Alanine aminotransferases | Altered levels of Alanine aminotransferases | 401 | n/a | 2 of 90 2.2% |
16of 311 5.1% |
n/a | |
| Moraes ACP et al., 2021 [56] | Cohort | Liver transplants | HBV/HCV coinfected | 294 | 24 8.2% |
6 2% |
17 5,8% |
n/a | |
| Zitelli PMY et al., 2021 [57] | Cross-sectional | Chronic HCV patients | More advanced liver disease; more Type-2DM, | 181 | 22 12% |
3 1,6% |
9 4,9% |
n/a | |
| Ribeiro LB et al., 2024 [58] | Cross-sectional | Patients with acute viral hepatitis | Elevated aminotransferases | 91 | 12 13.2% |
4 4.4% |
1 | 3f | |
| Zicker M et al., 2024 [59] | Prospective | Liver transplanted and donors | n/a | 190 | 19 10% |
1 0.53% |
negative | n/a | |
| Rio de Janeiro | Trinta KS et al., 2001 [60] | Retrospective cross-sectional | acute viral hepatitis; hemodialysis; intravenous drug users; blood donors; | n/a | 1,115 | 2.1% acute viral hepatitis 6.2% hemodialysis; 11.8% UDIVs; 4,.3% blood donors |
n/a | n/a | n/a |
| Santos DC et al., 2002 [61] | Cross-sectional | Manguinhos Community | age ≥40 years | 699 | 17 2.4% |
n/a | n/a | n/a | |
| South | |||||||||
| Paraná | Bortoliero AL et al., 2006 [62] | Cross-sectional | Blood donors | There was no association with sociodemographic variables | 996 | 23 2.3% |
n/a | n/a | n/a |
| Hardtke S et al., 2018 [63] | Cross-sectional | 209 pregnant women; 199 female blood donor | age ≥40 years; >3 number of pregnancies | 408 | 91 22,5% |
n/a | negative | n/a | |
| Santa Catarina | Passos-Castilho AM et al., 2016 [18] | Cross-sectional | Blood donors | 300 | 30 10% |
1 0,3% |
negative | n/a | |
| Rio Grande do Sul | Moss da Silva SC et al., 2019 [64] | Cross-sectional | PVHIV; Blood donors | age ≥40 years; poor sanitation; alcohol use |
601 | 42 6,98% |
n/a | 8 1,33% |
3 |
| Costa et al., 2021 [65] | Cross-sectional | cirrhosis; crack users; liver transplanted; blood donors | higher in cirrhosis; crack users; liver transplanted patients and blood donors | 400 | 78 19,5% |
6 1,5% |
negative | n/a | |
| Zorzeto R et al., 2021 [66] | Cross-sectional | Blood samples were from laboratories | age ≥40 years | 3,000 | 1,783 59,4% |
n/a | negative | n/a | |
Table 2.
Prevalence and genotypic characteristics of HEV infection in pigs, according to the five major regions of the country, 1995–2025.
Table 2.
Prevalence and genotypic characteristics of HEV infection in pigs, according to the five major regions of the country, 1995–2025.
| Brazil Region | State | Author/Year | Herd Characteristics | Biological sample tested |
Total (n=) |
Prevalence HEV | RNA | Genotype | |
|
IgG n(%) |
IgM n(%) |
||||||||
| North | Pará | Souza AJ et al, 2012 [67] | Six-month-old pigs from a licensed slaughterhouse (60%) and a slaughterhouse not registered with health regulatory agencies (40%). Samples collected during slaughter. | Serum, feces and liver | 151 | 13 8.6% |
0 | 15* 9.9% |
3c; 3f |
| Northeast | Pernambuco | Oliveira-Filho EF et al., 2017 [68] | Coming from a slaughterhouse located in the metropolitan region of Recife (30%) and farms in the rural region of the state (70%) | Serum | 325 | 266 82% |
- | n/a | n/a |
| Pernambuco | Oliveira-Filho EF et al., 2019 [69] | Animals aged two to six months, from farms that use intensive and extensive production systems. | Feces | 119 | - | - | 2 (1.68%) |
3f |
|
| Central West | Mato Grosso | Costa Lana et al., 2014 [70] | Four-month-old animals from large-scale farms (50%) and family farms (50%). Overall, 18 (72%) of the 25 pigs presented microscopic liver lesions, characterized by fibrosis and portal inflammation. | Bile, liver and feces | 25 | - | - | 15** 83,3% |
3b;3f |
| Mato Grosso | Campos CG et al., 2018 [71] | Growing piglets of both sexes, between three and four months of age, and breeding females, between eight and twenty-four months of age, from subsistence farms. | Serum and feces | 150 | - | - | 12 8% |
3d; 3h;3i |
|
| Southeast | Rio de Janeiro | Vitral CL et al., 2005 [72] | Pigs ranging in age from 1 to > 25 weeks in four commercial herds | Serum | 357 | 227 63.6% |
- | n/a | n/a |
| Rio de janeiro | dos Santos DR et al., 2011 [73] | Healthy animals aged > five months, from three legal slaughterhouses. | Bile | 115 | - | - | 11*** 9.6% |
3b |
|
| Minas Gerais | Amorim AR et al., 2018 [74] | Healthy animals for slaughter at a state slaughterhouse. No macroscopic lesions were observed in the livers of slaughtered pigs during bile collection. | Bile | 335 | - | - | 51 15.2% |
3c;3i |
|
| São Paulo | Cortez A et al., 2021 [75] | Samples from a state swine biobank. | Feces | 89 | - | - | 7 7.86% |
3b; 3h; 3j |
|
| South | Paraná | Gardinali NR et al., 2012 [76] | Samples came from maturation cycle farms (58.3%) and grow-to-slaughter farms (41.7%). All pigs were asymptomatic. | Feces | 170 | - | - | 26 15.3% |
3b |
| Paraná | Passos-Castilho AM et al., 2017 [77] | Animals aged between four and 16 weeks old from a small rural property in the region. | Feces | 170 | - | - | 34 20% |
3b |
|
| Rio Grande do Sul | da Silva MS et al., 2018 [78] | Animals from farms located near peri-urban areas or landfills, indigenous reservations, and farms that feed pigs with food scraps. Samples from two different periods were analyzed: 2012 (50.6%) and 2014 (49.4%) | Serum | 1444 | 1034 71.6% |
- | 6**** 0.8% |
3b; 3c; 3h |
|
* Authors report that, interestingly, in the present study, HEV RNA was detected more frequently among pigs without serological evidence of HEV infection: among fifteen pigs with positive PCR, only one had detectable anti-HEV IgG. The samples analyzed in the present study were obtained from pigs at slaughter age (approximately six months), which may have led to the failure to detect IgM antibodies. ** Among the 18 animals with microscopic liver lesions, HEV RNA was detected in eight (32%) of the pigs by nested PCR and in seven (28%) of the pigs by IHC in at least one of the samples analyzed from each animal. *** Viral loads observed for bile samples ranged from 101 to 105 genome copies/mL. **** 6/713 samples analyzed for the year 2014.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



