
Submitted:
28 July 2025
Posted:
29 July 2025
You are already at the latest version
Abstract
Background/Objectives: Individuals carrying hereditary breast and ovarian cancer (HBOC) and Lynch Syndrome (LS)-associated pathogenic variants have increased risk for cancers. The study examined the association between cancer diagnosis and health behaviors i.e., smoking, alcohol consumption, level of physical activity, and body mass index (BMI) among individuals with pathogenic variants associated with HBOC or LS.
Methods: We used baseline and 18-month follow-up data from carriers of HBOC-or LS- associated variants from the Swiss CASCADE cohort. Generalized linear models with random effects were applied.
Results: More than half (58%) of participants had at least one cancer diagnosis. Analyses of 856 observations from 518 individuals (HBOC:410, LS:108) showed that, after controlling for potential confounders, the proportion of current smokers was not significantly different between individuals diagnosed with cancer and never-diagnosed individuals (ß=4.5, p=0.18). Similarly, alcohol intake was not associated with cancer diagnosis (adjusted: ß= -0.2, p=0.51), although it was positively associated with time since genetic testing (ß=0.09, p< 0.01). Levels of physical activity were lower among individuals with cancer compared to never-diagnosed individuals (adjusted: ß= -0.5, p=0.002). There was no difference in BMI between individuals with cancer and individuals never diagnosed with cancer.
Conclusions: Findings showed a decrease in levels of physical activity among carriers of HBOC- or LS-associated variants with a cancer diagnosis compared to never-diagnosed individuals, but no differences in smoking, alcohol consumption, or BMI. It is possible that near-term health behavior adjustments among individuals with HBOC- or LS-associated variants are associated with genetic testing results.
Keywords:
cancer diagnosis
; carriers of pathogenic variants
; hereditary cancer
; lifestyle
Introduction
A cancer diagnosis can serve as a pivotal moment that can potentially trigger positive changes in health behaviors [1,2,3]. Studies show that many cancer survivors quit smoking [4,5], reduce alcohol consumption [5], increase their levels of physical activity [5], and maintain a body weight within normal range [4,6]. These changes in health behaviors are likely motivated by efforts to prevent cancer recurrence [7,8,9,10] and reduce susceptibility to other diseases [11,12]. These behavioral changes are also consistent with the 2012 American Cancer Society (ACS) Guidelines on Nutrition and Physical Activity for Cancer Survivors, which recommend exercising for at least 150 minutes per week to promote weight loss among overweight or obese survivors [13,14], and limiting alcoholic beverages to maximum 1 drink per day for females and 2 drinks per day for males [13].
However, ACS guidelines do not generally cover individuals with a genetic predisposition to cancer, such as hereditary breast and ovarian cancer (HBOC) or Lynch syndrome (LS). These syndromes account for up to 20% of common cancers, like breast, colorectal, and prostate cancer, and lethal types of cancer, like pancreatic or ovarian cancer [15,16]. HBOC is primarily associated with high penetrance genes, such as BRCA1 and BRCA2 (hereafter BRCA), while LS is associated with DNA mismatch repair genes (MLH1, MSH2, MSH6 – hereafter MMR genes) and germline EPCAM deletions [17,18]. Both syndromes share some common characteristics, including the potential for multiple cancer diagnoses. Individuals with germline pathogenic variants in BRCA or MMR genes have up to 20-fold higher risk for various types of cancer by the age of 70 years compared to the general population [19,20,21,22,23,24]. HBOC and LS individuals with a primary cancer diagnosis also have 2-fold higher risk of cancer recurrence [25,26].
A cancer diagnosis in individuals with HBOC or LS is primarily attributed to the germline predisposition. However, cancer risk is highly variable among these individuals, and little is known about why some develop cancer and others do not, and why some develop multiple cancers during their lifetime. Evidence indicates that germline pathogenic variants may interact with somatic alterations to drive carcinogenesis, and this association has been reported for breast cancer [27,28,29,30]. This could suggest a possible link between health behaviors and cancer onset or a second cancer diagnosis. Cancer risk may increase due to behaviors that contribute to DNA damage and/or higher concentration of inflammation markers, which in turn, are potentially associated with increased penetrance of the pathogenic variant [31,32,33]. Adoption of healthier behaviors may help maintain genome integrity, which helps sustain the function of the single copy of the wild-type allele, and thus, prevents or delays cancer onset [34]. Studies have shown that among carriers of pathogenic variants in BRCA or MMR genes, those who smoke or have higher BMI have significantly higher risk for breast and colorectal cancer, respectively [33,35,36,37]. Conversely, these cancer risks are negatively associated with higher levels of physical activity in these individuals [33,35,38,39,40,41]. Others reported that increased alcohol intake, more than 28 grams per day, is associated with risk of colorectal cancer among individuals diagnosed with LS [42,43]. However, no such association was found among individuals with BRCA pathogenic variants [44].
Inconsistent reports could be due to study design, involving retrospective cohorts or case-control studies assessing lifetime health behaviors based on recall from the distant past [37,38,39], which is prone to recall bias [36,40,41,45]. Little is known about near-term changes in health behaviors among individuals with HBOC- or LS- pathogenic variants in relation to a cancer diagnosis. The purpose of this study was to address limitations related to retrospective study design. We compared near-term health behaviors between individuals never diagnosed with cancer and individuals with at least one cancer diagnosis carrying HBOC- or LS- associated variants. We focused on four health behaviors, i.e., smoking, alcohol consumption, level of physical activity, and BMI as a proxy for dietary habits.
Materials and Methods
This analysis is part of the Swiss CASCADE cohort (NCT03124212) [46], a family-based, multi-center study that targets adults (>18 years old) who live in Switzerland and have been identified with HBOC- or LS-associated variants, and their biological relatives who may or may not carry the familial genetic predisposition, and they may or may not have a cancer diagnosis [46]. The study has been approved by appropriate ethics committees (BASEC 2016-02052).
Recruitment of index cases (first member in the family identified with the pathogenic variant) takes place in oncology/genetic testing centers in three linguistic regions of Switzerland. Index cases are asked to invite their biological relatives to the study. Participants complete a self-administered questionnaire at enrollment (baseline) available in local languages (German, French, Italian, or in English). Follow-up questionnaires are administered approximately every 24 months. Two reminders, each after a 6-week interval, encourage participants to complete and return their questionnaire. Participants who do not return their questionnaire after the second reminder are considered lost to follow-up. No incentives are offered for participating in the cohort; however, one participant is randomly chosen annually to receive a gift card worth CHF 300 (approximately $325).
This analysis focuses on individuals carrying HBOC- or LS-associated variants who have provided data one or two times between September 2017 and March 2025, depending on the time of enrollment in the cohort, irrespective of whether they were recruited as index cases or as relatives. Respondents were asked in each questionnaire if they ever had genetic testing and what was the test result. Relatives who did not report their genetic testing result, and if there was no available information in clinical records, were excluded from this analysis.
Primary Exposure Variables
Every questionnaire asked participants to indicate if they ever had a cancer diagnosis (“Yes”/ “No”), and if “Yes”, the specific type of cancer diagnosis, and the age of diagnosis. Time since cancer diagnosis was calculated for each participant as a continuous variable, while the value was set to 0 for never-diagnosed individuals.
Study Outcomes
Questionnaires asked participants to report their health behaviors during the past 4 weeks, in order to reduce recall bias and increase accuracy of reporting.
Smoking: Smoking status was coded as a categorial variable (“yes” coded as 1 and “no” coded as 0). Current smokers were asked to report the number of cigarettes smoked per day, which was multiplied by 7 to calculate number of cigarettes smoked per week, while never and non-current smokers were given a value of 0 for the average number of cigarettes smoked per week (continuous variable).
Alcohol: Alcohol consumption was calculated both as a categorical and as a continuous variable. Participants who reported never consuming alcohol were categorized as “never” drinkers (coded as 0); those consuming alcohol 1 to 2 times per week were categorized as “light” drinkers (coded as 1); those consuming alcohol 3 to 5 times per week were categorized as “moderate” drinkers (coded as 2); and those consuming alcohol 6 or more times per week were categorized as “heavy” drinkers (coded as 3) (categorical variable). An estimation of the average number of alcoholic beverages consumed per week was calculated by multiplying the group number (“never”-0, “light”-1, “moderate”- 2, or “heavy”-3) with the average number of alcoholic beverages reported in each questionnaire (continuous variable).
Physical Activity: Participants who reported never engaging in physical activity were categorized as “no” exercisers (coded as 0); those engaging in physical activity once per week were categorized as “light” exercisers (coded as 1); those engaging in physical activity 2 to 3 times per week were categorized as “moderate” exercisers (coded as 2); and those engaging in physical activity 4 or more times per week were categorized as “heavy” exercisers (coded as 3) (categorical variable). An estimation of the total number of hours spent in physical activity per week was calculated by multiplying the group value (“never”-0, “light”-1, “moderate”- 2, or “heavy”-3) with the average number of minutes of physical activity reported in each questionnaire (continuous variable).
BMI: Participants provided their body weight in kilograms and height in centimeters in each questionnaire. BMI was calculated as a continuous variable by dividing weight in kilograms by the square of the height in meters [47]. Participants were also categorized as “underweight” (<18.5 kgm-2) (coded as 0); “normal weight” (18.5-24.9 kgm-2) (coded as 1); “overweight” (25 to 29.9 kgm-2) (coded as 2); and “obese” (≥30 kgm-2) (coded as 3) (categorical variable).
Besides age and sex, participants also reported their age at genetic testing and their age at first cancer diagnosis. Time since genetic testing and time since cancer diagnosis were computed by subtracting the date of genetic testing and the date of first cancer diagnosis from the date of questionnaire submission.
Statistical Analyses
All analyses were conducted using the R statistical software package (R version 4.4.0). Descriptive statistics include calculation of means and standard deviations, medians and range, and frequencies and proportions. Although there was less than 5% missing data, analyses were carried out only in individuals with complete data. Two proportions z-tests were applied to compare frequencies and proportions. The non-parametric Wilcoxon rank sum test was used for comparing medians of variables that did not follow a normal distribution. Statistical significance was defined as p-values <0.05.
For categorical outcomes (e.g., current smoking: yes, or no), we applied a generalized linear mixed model, while for multi-group outcomes (e.g., alcohol: never, light, moderate and heavy), we applied cumulative link mixed models. Individual IDs were incorporated as random effects (to account for multiple observations recorded for some individuals). Similarly, for each continuous variable (i.e., number of cigarettes per week; number of alcoholic drinks per week; hours spent in physical activity per week; and BMI), a linear mixed model was run with random effects of individual ID. In all random effect models, common independent variables included were age, sex, syndrome, cancer diagnosis (yes/no) and time since genetic testing. Finally, we examined the interaction effects of sex and time since cancer diagnosis, as well as sex and time since genetic testing on each of the outcome variables.
Results
By March 2025, the study included 518 individuals with HBOC- or LS-associated pathogenic variants who have provided baseline data, and 338 follow-up data records, making for a total of 856 observations included in this analysis. Among the 518 carriers, 31 did not consent to provide follow-up data. Among the remaining individuals, 35 were in the process of providing follow-up data, while 114 were lost to follow-up (Figure 1). Common reasons for lost to follow-up were becoming critically ill, having an invalid address/moved abroad, and passive refusal. The 145 participants who did not provide follow-up data were significantly younger compared to those who did (48.72±13.94 years vs. 51.32±13.09 years, p<0.01), but had similar rates of cancer diagnosis (63.4% vs. 57.3%, p=0.21) and sex distribution (female: 81.7% vs. 81.7%, p=0.26).
More than half of observations (58%) were from individuals with one or more previous cancer diagnosis, with a median of 6 years since the first diagnosis. Median time since genetic testing was 3.41 years. Most participants were female (81.7%), with the majority (79.4%) carrying HBOC-associated pathogenic variants. A larger proportion of males were never diagnosed with cancer compared to females (57.3% vs. 38.2%, p<0.01). Individuals diagnosed with cancer were older compared to those who were never-diagnosed (55.3 years vs. 45.8 years, p<0.01). Between the baseline and the follow-up questionnaire 15 participants had a new cancer diagnosis; 5 of them had no cancer diagnosis at baseline and 10 developed a second primary cancer.
There was a higher proportion of “smoking” observations among individuals never diagnosed with cancer compared to individuals with cancer, although the difference was not statistically significant (13.7% vs 11.2%, p=0.07). There was no difference in the average number of cigarettes smoked per week between the two groups (Table 1). Univariate and multivariate analyses showed no significant association between smoking status or number of cigarettes smoked per week with cancer diagnosis, age, sex, syndrome, or time since genetic testing (Table 2 and Table 3).
There was a significantly higher proportion of “never” consume alcohol observations among individuals with cancer compared to never-diagnosed individuals (Table 1). However, the proportion of “light” drinking (1-2 times/week) and “moderate” drinking observations was significantly higher among never-diagnosed individuals compared to those with cancer (Table 1). No difference was observed in proportion of “heavy” drinking observations between the two groups. Cancer diagnosis was not associated with alcohol intake in both the univariate and adjusted models (univariate: ß = -0.2, p = 0.49; adjusted: ß = -0.2, p = 0.51) (Table 2 and Table 3). Females had a lower intake of alcohol than males (ß= -1.2, p<0.01) (Table 3). There was a significant positive association between average number of alcoholic beverages consumed per week and time since genetic testing (ß=0.09, p<0.01) (Table 3). When we examined the interaction effect of sex with time since genetic testing on alcohol consumption, we found that with each time unit increase since genetic testing, males were 0.2 times more likely to report drinking alcohol (ß= 0.2, p=0.01) (Table 4).
The proportion of “moderate” exercise observations i.e., engaging in physical activity 2-3 times per week, and the median number of hours engaging in physical activity per week were significantly higher among never-diagnosed individuals compared to those with cancer (Table 1). The unadjusted and adjusted models showed that never-diagnosed individuals were significantly more likely to engage in more hours of physical activity per week compared to those with cancer (unadjusted: ß= -0.37, p=0.03; adjusted: ß= -0.5, p=0.02) (Table 2 and Table 3).
Approximately 36% of the sample were overweight or obese. The proportion of “obese” observations was significantly lower among never-diagnosed individuals compared to those with cancer (7.8% vs. 12.6%, p=0.03), although there was not a significant difference in the median BMI between the two groups (Table 1). In both the unadjusted and adjusted models, cancer diagnosis was not significantly associated with BMI (Table 2 and Table 3). Age was positively correlated with BMI (ß= 0.05, p=0.01) and females were more likely to have a lower BMI compared to males (ß= -1.8, p=0.002) (Table 3).
We found no interactions between sex and time since cancer diagnosis for any of the outcome variables (Supplementary Table S1).
Discussion
We used longitudinal data from a prospective cohort to examine near-term changes in health behaviors and their association with cancer diagnosis in a sample of individuals with HBOC- or LS-pathogenic variants. Our findings suggest that one or more cancer diagnoses is associated with minor near-term changes in health behaviors in these individuals. This finding is inconsistent with a cohort study with LS-carriers from Finland, which reported positive associations between cancer diagnosis and health behaviors [41]. The inconsistent findings may be explained either by the retrospective design in the Finnish study, and/or by the exclusive focus on near-term changes in health behaviors in our own study.
We found that carriers of HBOC- or LS-associated pathogenic variants, with one or more cancer diagnosis, exercise fewer hours per week compared to their never-diagnosed counterparts. In our sample, the median time engaging in physical activity among individuals with cancer was 1 hour (60 min) per week, which is significantly less compared to 150 minutes per week, as suggested by international guidelines [13]. This is an important finding, given that physical activity may delay the onset of cancer recurrence in individuals with HBOC- or LS-pathogenic variants [40,48]. Decreased levels of physical activity in cancer survivors could be attributed to decreased functional status and/or increased levels of fatigue or other persistent symptoms, attributed to cancer treatment and its side effects [49,50]. A recent meta-analysis reported that up to 42% of cancer survivors experience significantly higher levels of fatigue compared to healthy controls [51]. In our sample, the median time since first cancer diagnosis was 6 years, which may explain the lower level of engagement in physical activity among individuals with one or more cancer diagnosis. Given the documented benefits of physical activity for cancer survivors [52,53,54], efforts should focus on establishing a systematic integration of physical activity into cancer survivorship programs. Research should also focus on uncovering the effects of physical activity on mechanisms of carcinogenesis among individuals with HBOC- or LS-pathogenic variants, which may be different from those in sporadic cancer.
There was no difference in smoking, alcohol intake, and BMI between individuals with HBOC- or LS-associated pathogenic variants with and without a cancer diagnosis. However, our sample included only 12% of current smokers, and there was not a significant difference in proportion of smoking observations between the two groups. Smoking prevalence among never-diagnosed individuals was lower compared to the general Swiss adult population (14% vs. 25%) [55,56,57], suggesting that behavioral adjustments may be triggered by genetic testing and the detection of the pathogenic variant. Studies report conflicting findings regarding the association between smoking and carcinogenesis in individuals with HBOC- or LS-pathogenic variants. Observational studies reported no association between smoking and development of ovarian or colorectal cancer in HBOC- or LS-individuals, respectively [58,59], while a machine learning modeling study reported a positive association between long-term smoking and breast carcinogenesis in carriers of pathogenic variants in BRCA genes [60]. These findings merit deeper examination, given the known carcinogenic effects of smoking in the general population, and its effects on cancer recurrence [61]. Offering smoking cessation support to individuals with a genetic predisposition to cancer can have a significant public health benefit.
Female participants reported lower levels of alcohol intake compared to males, a finding that has been reported for individuals with sporadic forms of cancer [5], but has not been confirmed for individuals with HBOC- or LS-pathogenic variants [43,44]. In our study, the proportion of participants reporting having at least one alcoholic drink per week and the average number of alcoholic drinks per week were lower compared to the general Swiss adult population (71% vs. 80% and 2.31 vs. 2.90 drinks, respectively) [56,62]. However, we found a significant positive correlation between male sex and time since genetic testing, i.e., with each increase in time unit after genetic testing, male participants were 0.2 times more likely to report drinking alcohol. Although our sample included only 18% males, this is an important finding given newer evidence suggesting that alcohol consumption may be associated with earlier onset of colorectal cancer, especially among males with LS-pathogenic variants [63,64].
Female participants had a lower BMI compared to males, a finding that has also been reported for sporadic forms of cancer [65]. Our study included a lower proportion of overall overweight or obese individuals compared to the general Swiss population of similar age range (35% vs. 42%) [56,66]. One would expect that individuals with cancer, who were on average 10 years older compared to never-diagnosed individuals in our sample, has higher BMI, since body weight typically increases over the lifetime. Consistently, the proportion of obese observations in our sample was significantly higher among individuals with cancer compared to never-diagnosed individuals. Previous studies suggested that an increased BMI infers an increased risk for colorectal cancer among males with LS-pathogenic variants but not for females [41,67,68]. Speculatively, this differential effect in females could be due to the anti-inflammatory action of endogenous estrogens, which are produced by adipose tissue [69,70,71]. More studies should further explore this association.
The main strength of the study includes the longitudinal design, where health behaviors and new cancer diagnoses were collected prospectively. Questionnaires asked participants to report their health behaviors during the past 4 weeks in order to reduce recall bias and increase accuracy. However, we cannot exclude the possibility of social desirability, self-selection, or other biases associated with self-reported health assessments. Moreover, there was a limited number of participants reporting a (new) cancer diagnosis, thus, there was limited data about near-term changes in health behavior following a cancer diagnosis. Behavioral changes may also occur at the time of genetic testing, when an individual is diagnosed with a pathogenic variant associated with cancer. Our sample was on average 3.5 years post genetic testing, and data to assess behavioral changes that occurred immediately after or close to the genetic diagnosis were not available. Gender differences should be interpreted with caution due to fewer male participants, especially among participants with HBOC-pathogenic variants. Finally, the study did not systematically assess endogenous and/or exogenous exposure to estrogens for females. Despite these limitations, the study provides a relatively large number of observations for four health behaviors, thus, provides a comprehensive description of near-term behavioral changes.
Conclusions
In conclusion, associations between health behaviors and risk for various types of cancer have been reported for the general population based on large population-based studies. This type of large data is currently not available for HBOC or LS populations due to the lower prevalence of these syndromes, lack of standardized assessments for health behaviors, and lack of infrastructure for storage and sharing of routinely collected data. Although the probability of developing cancer among HBOC or LS populations is primarily driven by the pathogenic variant [23,72,73], it is possible that the beneficial or harmful effects of modifiable risk factors are emphasized among these individuals. A healthier lifestyle could partially compensate for the strong genetic cancer predisposition by maintaining the function of the single copy of the wild allele [34]. Therefore, it is important to monitor these modifiable risk factors among individuals with HBOC- or LS-pathogenic variants, while providing support when necessary for behavioral changes. The results of our study could be used to inform cancer risk quantifications and behavioral interventions for various modifiable risk factors. Finally, there is a need for health behavior guidelines dedicated to these high-risk populations.
Authors contributions
Conceptualization: M.C.K., G.F. and M.S.; Methodology: M.C.K., G.F. and M.S.; Formal Analysis: M.S.; Investigation: M.C.K., G.F., and M.S.; Resources: M.C.K., N.B., R.G., G.F., K.H., U.Z.-H., C.M., M.R., and P.O.C.; Data curation: M.S.; Statistical Software: M.S.; Writing—original draft preparation: M.S. and M.C.K.; Writing—review and editing: M.C.K., S.A., F.B., N.B., R.G., G.F., K.H., U.Z.-H., C.M., M.R., and P.O.C.; Supervision: M.C.K., and G.F.; Project Administration: M.C.K, and M.S.; Funding Acquisition: M.C.K., N.B., R.G., K.H., C.M., M.R., U.Z.-H., and P.O.C. All authors have read and agreed with the content of the manuscript.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Table S1: Multivariate linear mixed models of the interaction effect of sex with time since cancer diagnosis.
Funding
The study was funded by the Swiss Cancer Research Foundation KFS-5293-02-2021 and KFS-6088-02-2024 (PI, Katapodi MC), the Swiss Cancer League – KLS-4294-08-2017 (PI, Katapodi MC) and the University of Basel, Office of the Vice Rector of Research (2016).
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki. The local Ethics Committees (Ethikkommission Nordwest- und Zentralschweiz; number: 2016-02052) approved the study.
Informed Consent Statement
A written informed consent was obtained from all study participants before enrolling in the study.
Data Availability Statement
Interested parties can contact the principal investigator Professor Maria C. Katapodi for data availability and accessibility through the official website of the study (https://swisscascade.ch/en/contact-2/). The Scientific Board of the Swiss CASCADE Consortium permits access to the cohort data. The data request form is available at: https://swisscascade.ch/en/research-project-data-request/.
Acknowledgments
The study was funded by the Swiss Cancer Research Foundation KFS-5293-02-2021 and KFS-6088-02-2024 (PI, Katapodi MC), the Swiss Cancer League – KLS-4294-08-2017 (PI, Katapodi MC) and the University of Basel, Office of the Vice Rector of Research (2016). We acknowledge the contributions of the Swiss CASCADE Consortium members and individuals in helping running the Swiss CASCADE cohort: Mekdes Alemu, Murat Aykut, Vasiliki Baroutsou, Ariana Bonfanti, Rachel Bunger, Pascal Dueblin, Muriel Fluri, Viola Heinzelmann-Schwarz, Camille Kumps, Christian Kurzeder, Ashley Machen, Corinna Elena Luca, Carla Pedrazzani, Marielle Rutquist, Lisa Schiess, Sandra Schmidt, Eveline Schönau, and Catrina Uhlmann Nussbaum.
Conflicts of Interest
All authors declare no conflict of interest.
References
- Choy, K.T.; Lam, K.; Kong, J.C. Exercise and colorectal cancer survival: an updated systematic review and meta-analysis. Int. J. Color. Dis. 2022, 37, 1751–1758. [Google Scholar] [CrossRef] [PubMed]
- Drageset, S.; Lindstrøm, T.C.; Underlid, K. “I just have to move on”: Women’s coping experiences and reflections following their first year after primary breast cancer surgery. Eur. J. Oncol. Nurs. 2016, 21, 205–211. [Google Scholar] [CrossRef]
- Hansen, J.M.; Nagle, C.M.; Ibiebele, T.I.; Grant, P.T.; Obermair, A.; Friedlander, M.L.; DeFazio, A.; Webb, P.M. ; Ovarian Cancer Prognosis Lifestyle Study Group Ahealthy lifestyle survival among women with ovarian cancer Int, J. Cancer 2020, 147, 3361–3369. [Google Scholar] [CrossRef]
- Hawkins, M.L.; Buys, S.S.; Gren, L.H.; Simonsen, S.E.; Kirchhoff, A.C.; Hashibe, M. Do cancer survivors develop healthier lifestyle behaviors than the cancer-free population in the PLCO study? J. Cancer Surviv. 2017, 11, 233–245. [Google Scholar] [CrossRef]
- Kanera, I.M.; Bolman, C.A.W.; Mesters, I.; Willems, R.A.; Beaulen, A.A.J.M.; Lechner, L. Prevalence and correlates of healthy lifestyle behaviors among early cancer survivors. BMC Cancer 2016, 16, 1–18. [Google Scholar] [CrossRef]
- Tollosa, D.N.; Holliday, E.; Hure, A.; Tavener, M.; James, E.L. Multiple health behaviors before and after a cancer diagnosis among women: A repeated cross-sectional analysis over 15 years. Cancer Med. 2020, 9, 3224–3233. [Google Scholar] [CrossRef]
- Tsay, S.-L.; Ko, W.-S.; Lin, K.-P. The Lifestyle Change Experiences of Cancer Survivors. J. Nurs. Res. 2017, 25, 328–335. [Google Scholar] [CrossRef] [PubMed]
- Demark-Wahnefried, W.; Aziz, N.M.; Rowland, J.H.; Pinto, B.M. Riding the Crest of the Teachable Moment: Promoting Long-Term Health After the Diagnosis of Cancer. J. Clin. Oncol. 2005, 23, 5814–5830. [Google Scholar] [CrossRef] [PubMed]
- Paek, J.; Son, S.; Choi, Y.J. E-cigarette and cigarette use among cancer survivors versus general population: a case-control study in Korea. J. Cancer Surviv. 2021, 16, 741–750. [Google Scholar] [CrossRef] [PubMed]
- Sung, H.; Hyun, N.; Leach, C.R.; Yabroff, K.R.; Jemal, A. Association of First Primary Cancer With Risk of Subsequent Primary Cancer Among Survivors of Adult-Onset Cancers in the United States. JAMA 2020, 324, 2521–2535. [Google Scholar] [CrossRef]
- Hawkins, M.L.; EBlackburn, B.; Rowe, K.; Snyder, J.; Deshmukh, V.G.; Newman, M.; Fraser, A.; Smith, K.; Herget, K.; AGanz, P.; et al. Endocrine and Metabolic Diseases Among Colorectal Cancer Survivors in a Population-Based Cohort. JNCI J. Natl. Cancer Inst. 2019, 112, 78–86. [Google Scholar] [CrossRef]
- Yang, K.; Liu, Z.; Thong, M.S.Y.; Doege, D.; Arndt, V. Higher Incidence of Diabetes in Cancer Patients Compared to Cancer-Free Population Controls: A Systematic Review and Meta-Analysis. Cancers 2022, 14, 1808. [Google Scholar] [CrossRef]
- WHOO WHO guidelines on physical activity and sedentary behaviour; World Health Organization: Geneva, 2020; pp. 1–582.
- Demark-Wahnefried, W.; Rogers, L.Q.; Alfano, C.M.; Thomson, C.A.; Courneya, K.S.; Meyerhardt, J.A.; Stout, N.L.; Kvale, E.; Ganzer, H.; Ligibel, J.A. Practical clinical interventions for diet, physical activity, and weight control in cancer survivors. CA: A Cancer J. Clin. 2015, 65, 167–189. [Google Scholar] [CrossRef]
- Lux, M.P.; Fasching, P.A.; Beckmann, M.W. Hereditary breast and ovarian cancer: review and future perspectives. J. Mol. Med. 2005, 84, 16–28. [Google Scholar] [CrossRef]
- Sehgal, R.; Sheahan, K.; O’Connell, P.R.; Hanly, A.M.; Martin, S.T.; Winter, D.C. Lynch Syndrome: An Updated Review. Genes 2014, 5, 497–507. [Google Scholar] [CrossRef] [PubMed]
- On behalf of the SEOMHereditary Cancer Working, G.r.o.u.p.; Llort, G.; Chirivella, I.; Morales, R.; Serrano, R.; Sanchez, A.B.; Teulé, A.; Lastra, E.; Brunet, J.; Balmaña, J.; et al. SEOM clinical guidelines in Hereditary Breast and ovarian cancer. Clin. Transl. Oncol. 2015, 17, 956–961. [Google Scholar] [CrossRef]
- da Silva, F.C.C.; Valentin, M.D.; Ferreira, F.d.O.; Carraro, D.M.; Rossi, B.M. Mismatch repair genes in Lynch syndrome: a review. Sao Paulo Med J. 2009, 127, 46–51. [Google Scholar] [CrossRef]
- Møller, P.; Seppälä, T.; Bernstein, I.; Holinski-Feder, E.; Sala, P.; Evans, D.G.; Lindblom, A.; Macrae, F.; Blanco, I.; Sijmons, R.; et al. Cancer incidence and survival in Lynch syndrome patients receiving colonoscopic and gynaecological surveillance: first report from the prospective Lynch syndrome database. Gut 2015, 66, 464–472. [Google Scholar] [CrossRef]
- Samadder, N.J.; Giridhar, K.V.; Baffy, N.; Riegert-Johnson, D.; Couch, F.J. Hereditary cancer syndromes—A primer on diagnosis and management: Part 1: Breast-ovarian cancer syndromes. Mayo Clinic Proceedings; 2019: Elsevier.
- Howlader, N.; Noone, A.; Krapcho, M.; Miller, D.; Brest, A.; Yu, M.; et al. Cancer Statistics Review, 1975–2016. National Cancer Institute. 2019.
- Kuchenbaecker, K.B.; Hopper, J.L.; Barnes, D.R.; Phillips, K.A.; Mooij, T.M.; Roos-Blom, M.J.; Jervis, S.; van Leeuwen, F.E.; Milne, R.L.; Andrieu, N.; Goldgar, D.E.; et al. Risks of breast, ovarian, and contralateral breast cancer for BRCA1 and BRCA2 mutation carriers. JAMA. 2017, 317, 2402–2416. [Google Scholar] [CrossRef] [PubMed]
- Antoniou, A.; Pharoah, P.D.; Narod, S.; Risch, H.A.; Eyfjord, J.E.; Hopper, J.L.; Loman, N.; Olsson, H.; Johannsson, O.; Borg, A.; et al. Average Risks of Breast and Ovarian Cancer Associated with BRCA1 or BRCA2 Mutations Detected in Case Series Unselected for Family History: A Combined Analysis of 22 Studies. Am. J. Hum. Genet. 2003, 72, 1117–1130. [Google Scholar] [CrossRef]
- Barrow, E.; Hill, J.; Evans, D.G. Cancer risk in Lynch Syndrome. Fam. Cancer 2013, 12, 229–240. [Google Scholar] [CrossRef] [PubMed]
- Song, Y.; Barry, W.T.; Seah, D.S.; Tung, N.M.; Garber, J.E.; Lin, N.U. Patterns of recurrence and metastasis in BRCA1/BRCA2-associated breast cancers. Cancer. 2020, 126, 271–280. [Google Scholar] [CrossRef]
- Haraldsdottir, S.; Hampel, H.; Wu, C.; Weng, D.Y.; Shields, P.G.; Frankel, W.L.; Pan, X.; de la Chapelle, A.; Goldberg, R.M.; Bekaii-Saab, T. Patients with colorectal cancer associated with Lynch syndrome and MLH1 promoter hypermethylation have similar prognoses. Anesthesia Analg. 2016, 18, 863–868. [Google Scholar] [CrossRef]
- Carter, H.; Marty, R.; Hofree, M.; Gross, A.M.; Jensen, J.; Fisch, K.M.; Wu, X.; DeBoever, C.; Van Nostrand, E.L.; Song, Y.; et al. Interaction landscape of inherited polymorphisms with somatic events in cancer. Cancer discovery. 2017, 7, 410–423. [Google Scholar] [CrossRef]
- Zhu, B.; Mukherjee, A.; Machiela, M.J.; Song, L.; Hua, X.; Shi, J.; Garcia-Closas, M.; Chanock, S.J.; Chatterjee, N. An investigation of the association of genetic susceptibility risk with somatic mutation burden in breast cancer. Br. J. Cancer 2016, 115, 752–760. [Google Scholar] [CrossRef]
- Bodily, W.R.; Shirts, B.H.; Walsh, T.; Gulsuner, S.; King, M.-C.; Parker, A.; Roosan, M.; Piccolo, S.R.; Galli, A. Effects of germline and somatic events in candidate BRCA-like genes on breast-tumor signatures. PLOS ONE 2020, 15, e0239197. [Google Scholar] [CrossRef] [PubMed]
- Cheng, H.H.; Sokolova, A.O.; Schaeffer, E.M.; Small, E.J.; Higano, C.S. Germline and Somatic Mutations in Prostate Cancer for the Clinician. J. Natl. Compr. Cancer Netw. 2019, 17, 515–521. [Google Scholar] [CrossRef] [PubMed]
- Pasanisi, P.; Bruno, E.; Venturelli, E.; Morelli, D.; Oliverio, A.; Baldassari, I.; Rovera, F.; Iula, G.; Taborelli, M.; Peissel, B.; et al. A Dietary Intervention to Lower Serum Levels of IGF-I in BRCA Mutation Carriers. Cancers 2018, 10, 309. [Google Scholar] [CrossRef]
- Bhardwaj, P.; Iyengar, N.M.; Zahid, H.; Carter, K.M.; Byun, D.J.; Choi, M.H.; Sun, Q.; Savenkov, O.; Louka, C.; Liu, C.; et al. Obesity promotes breast epithelium DNA damage in women carrying a germline mutation in BRCA1 or BRCA2. Sci. Transl. Med. 2023, 15, eade1857. [Google Scholar] [CrossRef]
- Daniele, A.; Divella, R.; Pilato, B.; Tommasi, S.; Pasanisi, P.; Patruno, M.; Digennaro, M.; Minoia, C.; Dellino, M.; Pisconti, S.; et al. Can harmful lifestyle, obesity and weight changes increase the risk of breast cancer in BRCA 1 and BRCA 2 mutation carriers? A Mini review. Hered. Cancer Clin. Pr. 2021, 19, 1–8. [Google Scholar] [CrossRef]
- Berndt, S.I.; Platz, E.A.; Fallin, M.D.; Thuita, L.W.; Hoffman, S.C.; Helzlsouer, K.J. Mismatch repair polymorphisms and the risk of colorectal cancer. Int. J. Cancer 2007, 120, 1548–1554. [Google Scholar] [CrossRef]
- Friebel, T.M.; Domchek, S.M.; Rebbeck, T.R. Modifiers of Cancer Risk in BRCA1 and BRCA2 Mutation Carriers: Systematic Review and Meta-Analysis. J. Natl. Cancer Inst. 2014, 106, dju091. [Google Scholar] [CrossRef]
- Pande, M.; Lynch, P.M.; Hopper, J.L.; Jenkins, M.A.; Gallinger, S.; Haile, R.W.; LeMarchand, L.; Lindor, N.M.; Campbell, P.T.; Newcomb, P.A.; et al. Smoking and Colorectal Cancer in Lynch Syndrome: Results from the Colon Cancer Family Registry and The University of Texas M.D. Anderson Cancer Center. Clin. Cancer Res. 2010, 16, 1331–1339. [Google Scholar] [CrossRef] [PubMed]
- van Duijnhoven, F.J.B.; Botma, A.; Winkels, R.; Nagengast, F.M.; Vasen, H.F.A.; Kampman, E. Do lifestyle factors influence colorectal cancer risk in Lynch syndrome? Fam. Cancer 2013, 12, 285–293. [Google Scholar] [CrossRef]
- Coletta, A.M.; Peterson, S.K.; Gatus, L.A.; Krause, K.J.; Schembre, S.M.; Gilchrist, S.C.; Arun, B.; You, Y.N.; Rodriguez-Bigas, M.A.; Strong, L.L.; et al. Diet, weight management, physical activity and Ovarian & Breast Cancer Risk in women with BRCA1/2 pathogenic Germline gene variants: systematic review. Hered. Cancer Clin. Pract. 2020, 18, 1–24. [Google Scholar]
- Coletta, A.M.; Peterson, S.K.; Gatus, L.A.; Krause, K.J.; Schembre, S.M.; Gilchrist, S.C.; Pande, M.; Vilar, E.; You, Y.N.; Rodriguez-Bigas, M.A.; et al. Energy balance related lifestyle factors and risk of endometrial and colorectal cancer among individuals with lynch syndrome: a systematic review. Fam. Cancer 2019, 18, 399–420. [Google Scholar] [CrossRef]
- Kehm, R.D.; Genkinger, J.M.; MacInnis, R.J.; John, E.M.; Phillips, K.A.; Dite, G.S.; Milne, R.L.; Zeinomar, N.; Liao, Y.; Knight, J.A.; et al. Recreational physical activity is associated with reduced breast cancer risk in adult women at high risk for breast cancer: a cohort study of women selected for familial and genetic risk. Cancer Research. 2020, 80, 116–125. [Google Scholar] [CrossRef] [PubMed]
- Sievänen, T.; Törmäkangas, T.; Laakkonen, E.K.; Mecklin, J.P.; Pylvänäinen, K.; Seppälä, T.T.; Peltomäki, P.; Sipilä, S.; Sillanpää, E. Body weight, physical activity, and risk of cancer in Lynch syndrome. Cancers 2021, 13, 1849. [Google Scholar] [CrossRef] [PubMed]
- Miguchi, M.; Hinoi, T.; Tanakaya, K.; Yamaguchi, T.; Furukawa, Y.; Yoshida, T.; Tamura, K.; Sugano, K.; Ishioka, C.; Matsubara, N.; et al. Alcohol consumption and early-onset risk of colorectal cancer in Japanese patients with Lynch syndrome: a cross-sectional study conducted by the Japanese Society for Cancer of the Colon and Rectum. Surg. Today 2018, 48, 810–814. [Google Scholar] [CrossRef]
- Dashti, S.G.; Buchanan, D.D.; Jayasekara, H.; Ait Ouakrim, D.; Clendenning, M.; Rosty, C.; Winship, I.M.; Macrae, F.A.; Giles, G.G.; Parry, S.; et al. Alcohol Consumption and the Risk of Colorectal Cancer for Mismatch Repair Gene Mutation CarriersAlcohol Intake and Colorectal Cancer Risk in Lynch Syndrome. Cancer Epidemiology, Biomarkers & Prevention 2017, 26, 366–375. [Google Scholar]
- Li, H. ; Terry MB, Antoniou AC, Phillips KA, Kast K, Mooij TM, Engel C, Noguès C, Stoppa-Lyonnet D, Lasset C, et, a. l. Alcohol consumption, cigarette smoking, and risk of breast cancer for BRCA1 and BRCA2 mutation carriers: results from The BRCA1 and BRCA2 Cohort Consortium. Cancer Epidemiology, Biomarkers & Prevention 2020, 29, 368–378. [Google Scholar]
- Botma, A.; Nagengast, F.M.; Braem, M.G.; Hendriks, J.C.; Kleibeuker, J.H.; Vasen, H.F.; Kampman, E. Body Mass Index Increases Risk of Colorectal Adenomas in Men With Lynch Syndrome: The GEOLynch Cohort Study. J. Clin. Oncol. 2010, 28, 4346–4353. [Google Scholar] [CrossRef]
- Katapodi, M.C.; Viassolo, V.; Caiata-Zufferey, M.; Nikolaidis, C.; Bührer-Landolt, R.; Buerki, N.; Graffeo, R.; Horváth, H.C.; Kurzeder, C.; Rabaglio, M.; et al. Cancer Predisposition Cascade Screening for Hereditary Breast/Ovarian Cancer and Lynch Syndromes in Switzerland: Study Protocol. JMIR Res. Protoc. 2017, 6, e184. [Google Scholar] [CrossRef]
- Prevention CfDCa. Healthy Weight, Nutrition, and Physical Activity: About Adult BMI 2023 [Available from: https://www.cdc.gov/healthyweight/assessing/bmi/adult_bmi/index.html#:~:text=Body%20mass%20index%20(BMI)%20is,weight%2C%20overweight%2C%20and%20obesity.
- Dashti, S.G.; Win, A.K.; Hardikar, S.S.; Glombicki, S.E.; Mallenahalli, S.; Thirumurthi, S.; Peterson, S.K.; You, Y.N.; Buchanan, D.D.; Figueiredo, J.C.; et al. Physical activity and the risk of colorectal cancer in Lynch syndrome. Int. J. Cancer 2018, 143, 2250–2260. [Google Scholar] [CrossRef]
- Gultekin, S.C.; Cakir, A.B.; Guc, Z.G.; Ozalp, F.R.; Keskinkilic, M.; Yavuzsen, T.; Yavuzsen, H.T.; Karadibak, D. The comparison of functional status and health-related parameters in ovarian cancer survivors with healthy controls. Support. Care Cancer 2024, 32, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Luctkar-Flude, M.F.; Groll, D.L.; Tranmer, J.E.; Woodend, K. Fatigue and physical activity in older adults with cancer: a systematic review of the literature. Cancer Nursing. 2007, 30, E35–E45. [Google Scholar] [CrossRef] [PubMed]
- Matsunaga, M.; He, Y.; Khine, M.T.; Shi, X.; Okegawa, R.; Li, Y.; Yatsuya, H.; Ota, A. Prevalence, severity, and risk factors of cancer-related fatigue among working cancer survivors: a systematic review and meta-analysis. J. J. Cancer Surviv. 2024, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Koper, M.; Bochenek, O.; Nowak, A.; Kałuża, J.; Konaszczuk, A.; Ratyna, K.; Kozyra, O.; Szypuła, Z.; Paluch, K.; Skarbek, M. From Diagnosis to Recovery: The Life-Changing Benefits of Exercise for Cancer Patients. Qual. Sport 2024, 20, 54212–54212. [Google Scholar] [CrossRef]
- Yeganeh, L.; Willey, S.; Wan, C.S.; Khomami, M.B.; Chehrazi, M.; Cook, O.; Webber, K. The effects of lifestyle and behavioural interventions on cancer recurrence, overall survival and quality of life in breast cancer survivors: A systematic review and network meta-analysis. Maturitas 2024, 185, 107977. [Google Scholar] [CrossRef]
- An, K.-Y.; Min, J.; Lee, D.H.; Kang, D.-W.; Courneya, K.S.; Jeon, J.Y. Exercise Across the Phases of Cancer Survivorship: A Narrative Review. Yonsei Med J. 2024, 65, 315–323. [Google Scholar] [CrossRef] [PubMed]
- Jakob, J.; Cornuz, J.; Diethelm, P. Prevalence of tobacco smoking in Switzerland: do reported numbers underestimate reality? Swiss Medical Weekly. 2017, 147, w14437. [Google Scholar]
- Suter, F.; Pestoni, G.; Sych, J.; Rohrmann, S.; Braun, J. Alcohol consumption: context and association with mortality in Switzerland. Eur. J. Nutr. 2022, 62, 1331–1344. [Google Scholar] [CrossRef] [PubMed]
- Karavasiloglou, N.; Pestoni, G.; Pannen, S.T.; Schönenberger, K.A.; Kuhn, T.; Rohrmann, S. How prevalent is a cancer-protective lifestyle? Adherence to the 2018 World Cancer Research Fund/American Institute for Cancer Research cancer prevention recommendations in Switzerland. Br. J. Nutr. 2022, 130, 904–910. [Google Scholar] [CrossRef]
- Power, R.F.; Doherty, D.E.; Horgan, R.; Fahey, P.; Gallagher, D.J.; Lowery, M.A.; Cadoo, K.A. Modifiable risk factors and risk of colorectal and endometrial cancers in Lynch Syndrome: a systematic review and Meta-analysis. JCO Precis. Oncol. 2024, 8, e2300196. [Google Scholar] [CrossRef] [PubMed]
- Gersekowski, K.; Na, R.; Alsop, K.; Delahunty, R. ; Goode EL, Cunningham JM, Winham SJ, Pharoah PDP, Song H,Webb, P. M. Risk factors for ovarian cancer by BRCA status: a collaborative case-only analysis. Cancer Epidemiology, Biomarkers & Prevention. 2024, 33, 586–592. [Google Scholar]
- Conte, L.; Rizzo, E.; Civino, E.; Tarantino, P.; De Nunzio, G.; De Matteis, E. Enhancing Breast Cancer Risk Prediction with Machine Learning: Integrating BMI, Smoking Habits, Hormonal Dynamics, and BRCA Gene Mutations—A Game-Changer Compared to Traditional Statistical Models? Appl. Sci. 2024, 14, 8474. [Google Scholar] [CrossRef]
- Jones, M.E.; Schoemaker, M.J.; Wright, L.B.; Ashworth, A.; Swerdlow, A.J. Smoking and risk of breast cancer in the Generations Study cohort. Breast Cancer Res. 2017, 19, 1–14. [Google Scholar] [CrossRef]
- Office, F.S. Swiss Health Survey 2017: alcohol consumption. 2019 10th August 2024.
- Church, D.N. More than just a hangover – alcohol and carcinogenesis in Lynch syndrome. Dis. Model. Mech. 2023, 16. [Google Scholar] [CrossRef]
- Fujiyoshi, K.; Sudo, T.; Fujita, F.; Chino, A.; Akagi, K.; Takao, A.; Yamada, M.; Tanakaya, K.; Ishida, H.; Komori, K. Risk of first onset of colorectal cancer associated with alcohol consumption in Lynch syndrome: a multicenter cohort study. Int. J. Clin. Oncol. 2022, 27, 1051–1059. [Google Scholar] [CrossRef] [PubMed]
- Zutshi, M.; Hull, T.; Shedda, S.; Lavery, I.; Hammel, J. Gender differences in mortality, quality of life and function after restorative procedures for rectal cancer. Color. Dis. 2012, 15, 66–73. [Google Scholar] [CrossRef] [PubMed]
- Office, F.S. Swiss Health Survey 2017: overweight and obesity. 2020.
- Botma, A.; Nagengast, F.M.; Braem, M.G.; Hendriks, J.C.; Kleibeuker, J.H.; Vasen, H.F.; Kampman, E. Body Mass Index Increases Risk of Colorectal Adenomas in Men With Lynch Syndrome: The GEOLynch Cohort Study. J. Clin. Oncol. 2010, 28, 4346–4353. [Google Scholar] [CrossRef]
- Campbell, P.T.; Cotterchio, M.; Dicks, E.; Parfrey, P.; Gallinger, S.; McLaughlin, J.R. Excess Body Weight and Colorectal Cancer Risk in Canada: Associations in Subgroups of Clinically Defined Familial Risk of Cancer. Cancer Epidemiology Biomarkers Prev. 2007, 16, 1735–1744. [Google Scholar] [CrossRef]
- Straub, R.H. The Complex Role of Estrogens in Inflammation. Endocr. Rev. 2007, 28, 521–574. [Google Scholar] [CrossRef]
- Nelson, L.R.; Bulun, S.E. Estrogen production and action. Journal of the American Academy of Dermatology. 2001, 45, S116–S24. [Google Scholar] [CrossRef]
- Leeners, B.; Geary, N.; Tobler, P.N.; Asarian, L. Ovarian hormones and obesity. Hum. Reprod. Updat. 2017, 23, 300–321. [Google Scholar] [CrossRef]
- Chen, S.; Parmigiani, G. Meta-analysis of BRCA1 and BRCA2 penetrance. Journal of Clinical Oncology. 2007, 25, 1329. [Google Scholar] [CrossRef] [PubMed]
- Nassour, A.-J.; Jain, A.; Hui, N.; Siopis, G.; Symons, J.; Woo, H. Relative Risk of Bladder and Kidney Cancer in Lynch Syndrome: Systematic Review and Meta-Analysis. Cancers 2023, 15, 506. [Google Scholar] [CrossRef]
Figure 1.
Study participants who completed baseline and/or follow-up questionnaires.
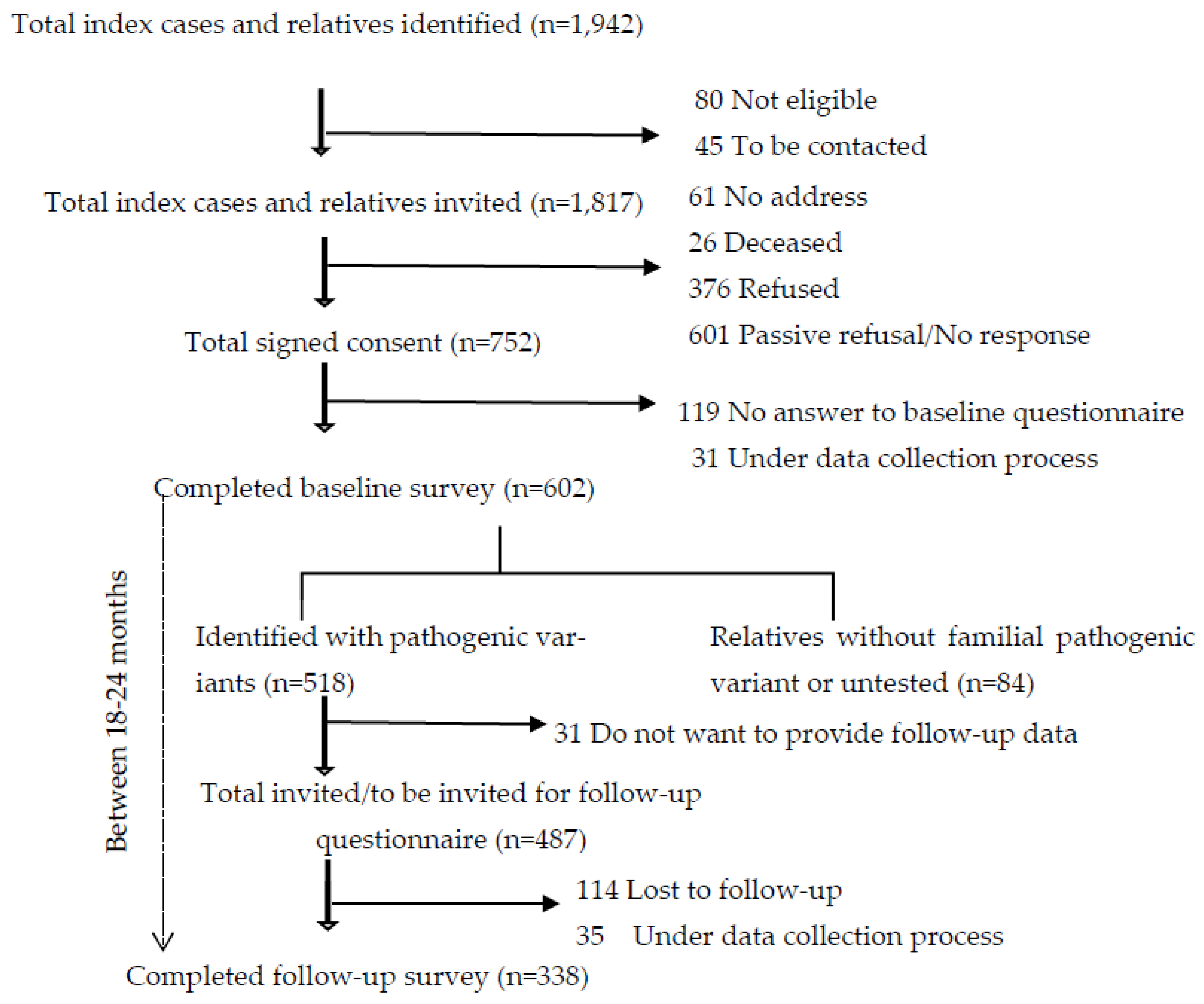

Table 1.
Observations from carriers of germline HBOC- and LS-associated pathogenic variants with or without cancer diagnosis.
Table 1.
Observations from carriers of germline HBOC- and LS-associated pathogenic variants with or without cancer diagnosis.
| Overall number of observations N=856 (%) |
Observations from individuals never diagnosed with cancer N=357 (%) |
Observations from individuals with at least one cancer diagnosis a N=499 (%) |
p-value | |
|---|---|---|---|---|
| Demographic and clinical characteristics | ||||
| Sex | ||||
| Male | 157 (18.3) | 90 (25.2%) | 67 (13.4%) | <0.01b |
| Female | 699 (81.7) | 267 (74.8%) | 432 (86.6%) | <0.01 b |
| Age [mean, (SD)], years | 51.4 (13.1) | 45.8 (13.1) | 55.3 (11.4) | <0.01c |
| Syndrome | ||||
| HBOC | 680 (79.4) | 305 (85.4%) | 375 (75.2%) | <0.01 b |
| LS | 176 (20.6) | 52 (14.6%) | 124 (24.8%) | <0.01 b |
| Median time since genetic testing (Q1-Q3), years | 3.41 (2.00-6.30) | 3.00 (1.93-5.65) | 3.73 (2.01-6.71) | 0.0042c |
| Median number of cancer diagnosis (Q1-Q3), (range) | - | - | 1 (1 – 1) | |
| Median time since first cancer diagnosis (Q1-Q3), years | - | - | 6.00 (3.0 -12.28) | |
| Health Behaviors | ||||
| Current smoking (missing=3) | ||||
| Yes | 105 (12.3) | 49 (13.7%) | 56 (11.2%) | 0.07b |
| No | 748 (87.4) | 308 (86.3%) | 440 (88.2% | 0.47 b |
| Average number of cigarettes [mean, (SD)] smoked per week | 72.24 (64.17) | 51.90 (40.45) | 90.7 (75.59) | 0.31 d |
| Alcohol (missing=12) | ||||
| Never (0) | 258 (30.1) | 81 (22.7%) | 177 (35.5%) | <0.01 b |
| Light (1-2/week) | 379 (44.3) | 173 (48.5%) | 206 (41.3%) | 0.04 b |
| Moderate (3-5/week) | 130 (15.2) | 65 (18.2%) | 65 (13.0%) | 0.05b |
| Heavy (≥6/week) | 77 (9.0) | 28 (7.8%) | 49 (9.8%) | 0.38 b |
| Average number of alcoholic beverages [mean, (SD)] per week (missing=12) | 2.31 (3.77) | 2.42 (3.59) | 2.23 (3.89) | 0.47 d |
| Physical activity (missing=12) | ||||
| No exercise (0) | 97 (11.3) | 31 (8.7%) | 66 (13.2%) | 0.05b |
| Light exercise (1/week) | 240 (28.0) | 97 (27.2%) | 143 (28.7%) | 0.69 b |
| Moderate exercise (2-3/week) | 358 (41.8) | 171 (47.9%) | 187 (37.5%) | 0.002 b |
| Heavy exercise (≥4/week) | 149 (17.4) | 56 (15.7%) | 93 (18.6%) | 0.30 b |
| Median hours of physical activity (IQRe) per week (missing=55) | 1.00 (0.3-2.0) | 1.0 (0.5 – 2.0) | 1.0 (0.25 – 2.0) | 0.05c |
| Body Mass Index (BMI) | ||||
| Underweight (<18.5 kgm-2), | 30 (3.5) | 10 (2.8%) | 20 (4.0%) | 0.44 b |
| Normal weight (18.5-24.9 kgm-2) | 498 (58.2) | 211 (59.1%) | 287 (57.5%) | 0.69 b |
| Overweight (25.0-29.9 kgm-2) | 215 (25.1) | 97 (27.2%) | 118 (23.6%) | 0.27 b |
| Obese (≥30 kgm-2) | 91 (10.6) | 28 (7.8%) | 63 (12.6%) | 0.03 b |
| Median BMI (Q1-Q3) (missing=22), kgm-2 | 23.6 (21.3-27.1) | 23.4 (21.3 -26.5) | 23.9 (21.2 – 27.4) | 0.43c |
a: any cancer diagnosis (brain, lung, liver, small intestine, colon, rectal, kidney, urinary tract, prostate, breast invasive, ductal carcinoma in situ, ovarian, uterus, cervix, fallopian tubes, thyroid, non-Hodgkin lymphoma, and multiple myeloma); b: two proportion Z-test; c: Wilcoxon rank sum test; d: t-test; e IQR= Interquartile Range (Q1-Q3).
Table 2.
Univariate models with random effects of ID variable.
| Smoking | Alcohol | Physical activity | Body Mass Index (BMI) | |||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Current smoking status (yes or no) a |
Average number of cigarettes smoked per week c | Alcohol intake group (never, light, moderate, heavy) b |
Average number of alcoholic beverages per week c |
Physical activity group (no exercise, light, moderate, heavy) b |
Average hours of physical activity per week c |
BMI (underweight, normal weight, overweight, obese) b | BMI c | |||||||||||||
| OR | 95% CI | Est. | Std.er. | p | OR | 95% CI | Est. | Std.er. | p | OR | 95% CI | Est. | Std.er. | p | OR | 95% CI | Est. | Std.er. | p | |
| Cancer diagnosis | 0.8 | 0.10-6.0 | 2.4 | 2.8 | 0.38 | 0.5 | 0.2-1.3 | -0.2 | 0.3 | 0.49 | 0.81 | 0.6-1.1 | -0.37 | 0.17 | 0.03 | 0.8 | 0.2-3.3 | 0.4 | 0.3 | 0.3 |
a: Generalized mixed model; b: Cumulative link mixed model, c: Linear mixed model.
Table 3.
Multivariate models with random effects of ID variable.
| Smoking | Alcohol | Physical activity | Body Mass Index (BMI) | |||||||||||||||||
| Current smoking status (yes or no) a |
Average number of cigarettes smoked per week c | Alcohol intake group (never, light, moderate, heavy) b |
Average number of alcoholic beverages per week c |
Physical activity group (no exercise, light, moderate, heavy) b |
Average hours of physical activity per week c |
BMI group (underweight, normal weight, overweight, obese) b | BMI c | |||||||||||||
| OR | 95% CI | Est. | Std.er. | p | OR | 95% CI | Est. | Std.er. | p | OR | 95% CI | Est. | Std.er. | p | OR | 95% CI | Est. | Std.er. | p | |
| Cancer diagnosis | 1.05 | 0.01-11.1 | 4.5 | 3.3 | 0.18 | 0.36 | 0.11-1.20 | -0.2 | 0.3 | 0.51 | 0.7 | 0.5-1.1 | -0.5 | 0.2 | 0.02 | 0.83 | 0.32-2.13 | 0.3 | 0.4 | 0.43 |
| Age in years | 0.97 | 0.9-1.1 | -0.2 | 0.1 | 0.24 | 1.03 | 0.99-1.08 | 0.02 | 0.01 | 0.06 | 1.01 | 1.0-1.03 | 0.01 | 0.01 | 0.13 | 0.93 | 0.92-0.93 | 0.05 | 0.02 | 0.01 |
| Female (ref: male) |
0.59 | 0.03-10.6 | -3.3 | 4.4 | 0.46 | 0.49 | 0.11-2.24 | -1.2 | 0.4 | <0.01 | 1.0 | 0.6-1.7 | -0.05 | 0.3 | 0.85 | - | - | -1.8 | 0.6 | 0.002 |
| HBOC (ref: LS) |
1.09 | 0.08-15.7 | 2.9 | 4.0 | 0.47 | 0.55 | 0.12-2.51 | -0.70 | 0.4 | 0.10 | 0.8 | 0.5-1.2 | 0.20 | 0.2 | 0.38 | - | - | -0.2 | 0.5 | 0.64 |
| Time since genetic testing | 1.00 | 0.8-1.3 | -0.1 | 0.3 | 0.67 | 1.13 | 0.99-1.29 | 0.09 | 0.03 | <0.01 | 1.01 | 1.0-1.05 | -0.01 | 0.02 | 0.87 | - | - | -0.04 | 0.04 | 0.60 |
a: Generalized mixed model; b: Cumulative link mixed model, c: Linear mixed model.
Table 4.
Multivariate linear mixed models of the interaction effect of sex with time since genetic testing.
Table 4.
Multivariate linear mixed models of the interaction effect of sex with time since genetic testing.
| Average number of cigarettes smoked per week | Average number of alcoholic beverages per week | Average hours of physical activity per week | Body Mass Index | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Est. | Std.er. | p | Est. | Std.er. | p | Est. | Std.er. | p | Est. | Std.er. | p | |
| Female (ref: male) | -7.8 | 5.5 | 0.16 | -0.7 | 0.6 | 0.24 | -0.3 | 0.3 | 0.32 | -2.3 | 0.7 | 0.01 |
| Time since genetic testing | -1.1 | 0.6 | 0.08 | 0.2 | 0.07 | <0.01 | -0.02 | 0.04 | 0.66 | -0.01 | 0.07 | 0.21 |
| Female * time since genetic testing | 1.04 | 0.7 | 0.14 | -0.1 | 0.08 | 0.08 | 0.02 | 0.04 | 0.62 | 0.07 | 0.08 | 0.36 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



