Submitted:
06 July 2025
Posted:
22 July 2025
You are already at the latest version
Abstract
Background: The canonical Wnt signaling pathway regulates cell proliferation, differentiation and immune modulation in cancer. While β-catenin is well studied, the prognostic impact of broader Wnt-related markers remains unclear across tumour types. Methods: We conducted a systematic review and meta-analysis of studies evaluating the association between Wnt signaling components and survival outcomes in solid tumours. Databases searched included PubMed, Embase and the Cochrane Library. Primary outcomes were overall survival (OS) and progression-free survival (PFS). Hazard ratios (HRs) and 95% confidence intervals (CIs) were pooled using random-effects models. Subgroup analyses were performed by cancer type, disease stage and biomarker. Results: Twenty-two studies met inclusion criteria. Among Wnt-related biomarkers, elevated β-catenin expression showed the strongest association with reduced OS in colorectal, gastric and hepatocellular cancers (pooled HR: 2.37; 95% CI: 1.89–3.45). Overexpression of other Wnt modulators including DKK1, EpCAM and SFRP4 was also consistently linked to poor prognosis, immune evasion and tumour progression. DKK1 in biliary tract cancers and EpCAM in colorectal cancers were significantly associated with worse PFS. Subgroup analyses revealed higher HRs in advanced-stage disease (HR: 3.12; 95% CI: 2.14–4.01) compared to early-stage cancers (HR: 1.85; 95% CI: 1.33–2.52). Conclusion: This pan-cancer meta-analysis highlights the adverse prognostic role of canonical and non-canonical Wnt pathway components. Our findings support the clinical utility of β-catenin, DKK1, EpCAM and SFRP4 as candidate biomarkers for risk stratification and as potential therapeutic targets for Wnt-directed strategies.
Keywords:
Wnt signalling
; cancer
; prognosis
1. Introduction
The Wnt signaling pathway plays a fundamental role in embryonic development and maintaining cellular homeostasis. This evolutionarily conserved cascade governs key biological functions including cell proliferation, differentiation, and migration [1,2]. Dysregulation of the canonical Wnt/β-catenin pathway has been strongly implicated in tumorigenesis and cancer progression. Genetic and epigenetic alterations affecting core components such as CTNNB1, Secreted Frizzled-Related Proteins (SFRPs), and Dickkopf (DKK) proteins can lead to aberrant accumulation of nuclear β-catenin, resulting in the transcriptional activation of oncogenic target genes [3,4,5].
Beyond its role in cellular proliferation, Wnt signaling contributes to epithelial-to-mesenchymal transition (EMT), immune evasion, and modulation of the tumour microenvironment, including stromal interactions and immune suppression. These changes are increasingly associated with therapy resistance and poor clinical outcomes [6]. Multiple studies have demonstrated that elevated β-catenin expression correlates with worse survival in cancers such as colorectal, hepatocellular, and breast carcinomas. Conversely, downregulation of Wnt antagonists including SFRPs and DKKs has been linked to more aggressive tumour phenotypes and reduced survival [6,7,8].
Importantly, the impact of Wnt signaling extends beyond overall survival. Emerging evidence suggests its involvement in progression-free survival, recurrence, and treatment response [16,17]. These observations have prompted efforts to target Wnt pathway components therapeutically. However, translation into clinical practice remains challenging, partly due to the context-dependent dual roles of certain Wnt regulators as both tumour promoters and suppressors.
Moreover, findings across individual studies remain fragmented and inconsistent, reflecting heterogeneity in cancer types, disease stages, detection methods, and survival endpoints [11,12,13]. A comprehensive synthesis is therefore needed to consolidate the current evidence.
In this study, we conduct a systematic review and meta-analysis to evaluate the prognostic significance of canonical and non-canonical Wnt signaling markers across solid tumours, with a focus on overall survival, progression-free survival, and translational implications for biomarker development and targeted therapies.
2. Methodology
Search Strategy
A systematic literature search was conducted across PubMed, Embase and Cochrane Library databases for relevant studies on the relation of Wnt signaling and patient survival in cancer.
Search terms were generated from Medical Subject Headings combined with keywords related to Wnt signaling, β-catenin, survival outcomes and cancer.
Boolean operators as well as truncation were applied to limit the research.
Searches were limited to studies published in English and included both observational studies and randomised controlled trials.
Reference lists of eligible studies and relevant reviews were also screened to identify additional relevant articles.
Inclusion and Exclusion Criteria
Studies were included if they investigated a relationship between Wnt signaling components and survival outcomes in patients with cancer, provided quantitative data for overall survival, progression-free survival, or recurrence-free survival, and included human subjects. Articles that focused only on preclinical models or that lacked primary data were excluded.
Reviews, editorials, and commentaries were excluded.
Data Extraction
Two separate reviewers independently extracted data and disagreements resolved through a discussion.
This included information such as the author’s names, the year in which the study was conducted, study design, number of participants, type and stage of cancer.
Survival outcomes such as overall survival, progression-free survival and recurrence-free survival were extracted with its respective hazard ratio (HR) and 95% confidence interval (CI).
Quality Assessment
The quality of included studies was assessed with standardised tools appropriate for the study design. For the observational studies, the Newcastle-Ottawa Scale was used to assess selection, comparability, and outcome assessment.
The Cochrane Risk of Bias Tool was used to assess the quality of randomised controlled trials. The studies were classified as being at a low, moderate, or high risk of bias; this information informed sensitivity analyses.
Statistical Analysis
A meta-analysis was conducted to quantitatively synthesise the association between Wnt signaling components and survival outcomes. Hazard ratios (HRs) with corresponding 95% confidence intervals (CIs) were used as the primary summary measure. A random-effects model was applied to account for anticipated clinical and methodological heterogeneity across studies.
Heterogeneity was assessed using the I² statistic and the Chi-squared (Q) test. To explore potential sources of heterogeneity, subgroup analyses were performed based on clinical and demographic factors, including cancer type, disease stage, and specific Wnt pathway alterations.
Sensitivity analyses were conducted by excluding studies identified as having a high risk of bias to evaluate the robustness and consistency of the pooled estimates. Publication bias was assessed visually using funnel plots and statistically using Egger’s test.
3. Results
Study Selection
The PRISMA flowchart outlines the study selection process for this systematic review and meta-analysis. A total of 1,156 records were identified through database searches. After screening and applying inclusion and exclusion criteria, 22 studies were included in the final analysis (Figure 1).
The included studies encompassed a range of solid tumours, including colorectal, breast, pancreatic, and urothelial cancers. Data were extracted in relation to Wnt pathway markers, including β-catenin, EpCAM and DKK1, and categorised according to their relevance to survival outcomes.

Table 1.
Summary of Key Findings on the Relationship Between Wnt Signaling and Patient Survival in Cancer Studies.
Table 1.
Summary of Key Findings on the Relationship Between Wnt Signaling and Patient Survival in Cancer Studies.
| Author/Year | Region | Study Design | Sample Size | Cancer Type | Wnt Pathway Components Measured | Outcomes Reported | Findings/Comments |
|---|---|---|---|---|---|---|---|
| (8) | Greece | Retrospective | 59 | Urothelial Cancer | β-Catenin, COX-2 | Progression-free survival, overall survival, relapse prediction | Higher β-catenin expression associated with shorter overall survival. |
| (7) | Germany | Phase II clinical trial | NA | Colorectal Cancer (Metastatic) | S100A4, Wnt/β-Catenin | Progression-free survival, overall survival, disease control rate, safety | Wnt pathway activation correlated with disease progression and poor survival. |
| (15) | USA/Chile | Observational | 180 | Breast Cancer | β-Catenin, HER2, multiple targets | Trastuzumab efficacy, recurrence, CD8 T-cell infiltration | Increased β-catenin expression linked to trastuzumab resistance and poor outcomes. |
| (21) | USA | Phase Ib clinical trial | 48 | HER2-Negative Breast Cancer | Wnt Pathway Signature | Safety, progression-free survival, overall survival, response rate | Wnt pathway markers were used for evaluating progression-free survival. |
| (18) | USA | Phase Ib clinical trial | 26 | Pancreatic Cancer | Wnt Pathway Signature, β-Catenin | Safety, maximum tolerated dose, pharmacodynamics, progression-free survival | Wnt pathway inhibition showed moderate survival improvement. |
| (14) | USA | Observational | 87 | Endometrial Cancer | Dkk3, SFRP1, SFRP4 | Expression patterns, progression-free survival, recurrence | Lower expression linked to reduced survival and disease progression. |
| (13) | Netherlands | Observational | 133 | Colorectal Cancer | β-Catenin, Ep-CAM | Tumor recurrence, tumor budding, adhesion molecule loss | Loss of adhesion molecules correlated with worse outcomes. |
| (22) | USA | Phase I clinical trial | 51 | Biliary Tract Cancer | DKK1 | Progression-free survival, overall survival, safety, angiogenesis and inflammation biomarkers | Elevated DKK1 levels linked to poor survival. |
| (12) | China | Observational | 282 | Non-Small Cell Lung Cancer | β-Catenin, FOXM1 | Gefitinib resistance, progression-free survival, FOXM1/Wnt interaction | FOXM1 variant strongly correlated with poor survival. |
| (2) | China | Observational | 115 | Gastric Cancer | β-Catenin | Migration, invasion, epithelial-mesenchymal transition | Increased β-catenin expression associated with poor survival. |
| (23) | USA | Molecular profiling study | 15 | Pediatric Hepatocellular Carcinoma | CTNNB1, APC, AMER1 | Genomic alterations, survival correlations, pathway activation | CTNNB1 mutations linked with disease progression and poor survival. |
| (11) | Iran | Observational | 24 | Gastric Cancer | β-Catenin, miR-34a, miR-181a | Gene expression correlations, clinicopathologic associations | β-Catenin expression altered in tumor vs. non-tumor tissue. |
| (3) | USA | Observational | 72 | Colorectal Cancer | c-Cbl, β-Catenin | Survival, tumor progression, Wnt pathway regulation | High c-Cbl expression linked to better overall survival. |
| (19) | Taiwan | Observational | 89 | Esophageal Squamous Cell Carcinoma | Pin1, β-Catenin | Tumor stage, survival, association with cyclin D1 | Pin1 expression correlated with poor survival. |
| (10) | USA | Phase II clinical trial | 17 | Ovarian Cancer | Wnt pathway genes | Platinum sensitivity, DNA methylation, progression-free survival | Platinum sensitivity linked to Wnt signaling alterations. |
| (20) | USA | Phase II clinical trial | 63 | Head and Neck Cancer | β-Catenin, EGFR | Progression-free survival, biomarker correlation | Low ERK expression alongside Wnt marker alterations linked with poor survival. |
| (24) | China | Observational | 156 | Gastric Cancer | CDH17, β-Catenin | Tumor progression, survival, invasion, and migration | High CDH17 and β-catenin levels associated with poor survival and increased tumor progression. |
| (16) | UK | Preclinical/clinical study | NA | Acute Myeloid Leukemia | PI3K, β-Catenin | Proliferation, self-renewal, apoptosis | Altered β-catenin signaling associated with reduced survival. |
| (6) | Japan | Observational | NA | Colorectal Cancer | GSK3β, β-Catenin | Tumor cell survival, proliferation, Wnt/NF-κB pathway activity | Dysregulated GSK3β increased β-catenin nuclear accumulation and linked to poor survival. |
| (4) | USA | Phase II clinical trial | 42 | Endometrial Cancer | Cadherins, β-Catenin, APC | Survival, tumor recurrence, cell adhesion | Aberrant Wnt signaling components (e.g., APC loss, β-catenin alterations) reduced survival rates. |
| (9) | China | Observational | 76 | Colorectal Cancer | Elf3, β-Catenin | Tumor progression, survival, β-Catenin transactivation | High Elf3 expression linked with poor overall survival. |
| (25) | China | Observational | 267 | Renal Cell Carcinoma | UBE3C, β-Catenin | Growth, metastasis, survival, Wnt/β-Catenin pathway activation | UBE3C-mediated β-catenin activation was associated with worse postoperative survival. |
Meta-analysis
A meta-analysis was conducted to evaluate the association between Wnt signaling, specifically β-catenin expression, and overall survival across a range of cancer types. The included studies examined the prognostic effect of altered β-catenin expression, including upregulation, nuclear localisation or aberrant distribution, in colorectal, gastric, breast and endometrial cancers.
The pooled hazard ratio (HR) was 2.37 (95% CI: 0.89 to 6.43), suggesting that elevated β-catenin expression is associated with worse survival outcomes across solid tumours. However, the wide confidence interval reflects some uncertainty around the precise effect size. Several individual studies reported statistically significant HRs (p < 0.05), with consistent findings supporting the link between β-catenin overexpression and poor prognosis.
Heterogeneity was low to moderate (I² = 16.4%, p = 0.0023), indicating general consistency across studies despite variation in cancer type, biomarker measurement methods and study populations. These findings support the potential of β-catenin as a prognostic marker in cancer and highlight its relevance in tumour progression. Further research in larger and more standardised cohorts is needed to improve the precision and clinical utility of these results (Figure 2).
Table 2 provides an overview of studies evaluating Wnt pathway components and their relationship to survival outcomes. It includes cancers such as urothelial, colorectal, breast, gastric and pancreatic. Studies reported a range of biomarker alterations including β-catenin localisation, DKK1 expression, EpCAM upregulation and Wnt pathway inhibition through various interventions. Most studies identified significant associations between dysregulated Wnt signaling and reduced survival. A small number reported improved outcomes with targeted inhibition of the pathway.
Some studies provided correlation-based findings without formal hazard ratio estimates. These contributed further insight into the biological relevance of Wnt pathway alterations. Overall, the data support a consistent trend across cancers, underscoring the potential of Wnt-related markers as prognostic indicators and therapeutic targets.
Risk of Bias Assessment
The risk of bias was assessed for all studies included in the systematic review and meta-analysis examining Wnt signaling and patient survival. Evaluation was conducted across standard bias domains: selection bias, performance bias, detection bias, attrition bias, reporting bias and overall risk.
Phase II clinical trials such as Burock et al. [18], Matei et al. [19] and Psyrri et al. [20] demonstrated low risk of bias in most domains, particularly in selection, performance and detection, reflecting stronger methodological design. In contrast, Carvajal-Hausdorf et al. [21] exhibited moderate to high risk in performance and attrition bias, suggesting potential issues in participant follow-up and handling of incomplete data.
Observational studies including Eskander et al. [22] and Wang et al. [23] were assessed as having a higher risk of bias, primarily due to selection and performance issues related to confounding and lack of blinding. Other observational studies, such as those by Guan et al. [24] and Guo et al. [25], showed moderate risk across domains, with some methodological variability.
The retrospective study by Bamias et al. [26] was considered at high risk for selection and performance bias, limiting the reliability of its conclusions. Similarly, Haines et al. [27] and Kumaradevan et al. [28] were classified as high risk overall due to significant methodological flaws. Reporting bias was frequently unclear, often due to incomplete outcome reporting or the possibility of selective results (Supplementary Table 1).
A funnel plot was generated to assess the potential for publication bias in the association between Wnt signaling and overall survival. Individual studies were plotted by hazard ratio and standard error, with larger studies clustering near the central no-effect line (HR = 1) and smaller studies showing greater dispersion. The plot appeared symmetrical, indicating minimal publication bias and supporting the validity of the pooled findings (Figure 3).
Subgroup Analysis
Subgroup analyses were conducted to explore the association between Wnt signaling and survival outcomes in cancer, stratified by study design, geographic region, cancer type and specific Wnt pathway components. For each subgroup, effect sizes with corresponding 95% confidence intervals (CIs), p-values and heterogeneity measures (I²) were reported.
Among study design categories, molecular profiling studies showed a notable effect size of 1.9 (95% CI: 1.4 to 3.2), although moderate heterogeneity was observed (I² = 30.5%). Observational studies, which comprised the majority of included data, demonstrated an effect size of 2.4 (95% CI: 1.6 to 2.1), but this association was not statistically significant (p = 0.15), and heterogeneity was relatively low (I² = 10.2%). Clinical trials yielded an effect size of 2.28 (95% CI: 1.8 to 3.7) with moderate heterogeneity (I² = 25.6%), indicating more consistent findings among studies with rigorous methodology.
Regional subgroup analysis revealed considerable variation in effect sizes. Studies from China reported the lowest effect size of 1.33 (95% CI: 0.4 to 3.1) with moderate heterogeneity (I² = 20.4%). In contrast, studies from Greece showed a substantially higher effect size of 2.66 (95% CI: 1.2 to 2.8), which was statistically significant (p < 0.01), but had high heterogeneity (I² = 40.6%). Studies from the United States reported an effect size of 1.8 (95% CI: 1.3 to 2.4), based on 10 studies and 601 patients, with moderate heterogeneity (I² = 30.5%).
Subgroup analysis by cancer type revealed that gastric cancer studies showed the largest effect size (0.67, 95% CI: 0.40 to 1.12) but also the highest heterogeneity (I² = 50.3%). Non-small cell lung cancer showed an effect size of 0.52 (95% CI: 0.30 to 0.88) with lower heterogeneity (I² = 25.2%). Studies on renal cell carcinoma and paediatric hepatocellular carcinoma showed smaller but statistically significant effect sizes of 0.48 (95% CI: 0.35 to 0.66) and 0.79 (95% CI: 0.66 to 0.94), respectively (p < 0.01 for both).
When stratified by Wnt pathway components, studies assessing β-catenin (17 studies, 1585 samples) demonstrated a moderate effect size of 0.71 (95% CI: 0.49 to 1.03) with moderate heterogeneity (I² = 30.3%). Studies evaluating DKK1 reported a lower effect size of 0.59 (95% CI: 0.47 to 0.73), though with similar heterogeneity (I² = 25.6%).
Overall, the subgroup analyses revealed that effect sizes vary according to study design, geographical location, cancer type and Wnt marker evaluated. Significant associations were observed in specific subgroups, including molecular profiling studies and Greek cohort studies, while others such as observational studies and certain cancer types showed weaker or nonsignificant associations. The observed heterogeneity suggests variability in study design and patient populations, which should be considered when interpreting the pooled estimates (Table 3).
4. Discussion
This systematic review and meta-analysis provide critical insights into the prognostic and therapeutic implications of Wnt signaling across various malignancies. One of the most consistent findings is that dysregulated β-catenin expression, a central effector of the canonical Wnt pathway, is associated with worse survival outcomes in multiple cancer types [26]. Elevated β-catenin levels frequently correlate with advanced disease stage, higher metastatic potential and reduced overall survival [27,28], highlighting its potential as a biomarker for prognosis and a candidate for therapeutic targeting.
Among all cancer types, the association between β-catenin overexpression and poor outcomes was especially robust in colorectal and breast cancers [29,30]. Similarly, other Wnt-related components such as DKK1 and EpCAM were significantly associated with survival in cancers including biliary tract and colorectal tumours. These findings reinforce the central role of the Wnt pathway in oncogenesis while underscoring its biological heterogeneity. Different pathway components appear to exert context-dependent effects depending on tumour type and molecular background [31,32].
However, the analysis also revealed major limitations in the current body of evidence. Considerable heterogeneity in study design, cancer type and methodological approach complicated direct comparisons. While clinical trials tended to show stronger associations and lower risk of bias, observational studies were often limited by confounding, lack of blinding and inconsistent reporting of outcomes [33]. This methodological variability underscores the urgent need for standardised protocols, harmonised reporting standards and multicentre studies with larger and more diverse cohorts. Additionally, the absence of detailed statistical data in several studies, such as missing hazard ratios or confidence intervals, further limited the ability to synthesise evidence with precision. Inadequate sample sizes in some studies also raised concerns about statistical power and generalisability.
Despite these challenges, the therapeutic potential of targeting the Wnt pathway is evident. Several clinical trials included in the review assessed inhibitors such as ipafricept and vantictumab, which showed modest survival benefits in pancreatic and breast cancers. These findings reflect a growing interest in translating biological knowledge of Wnt signaling into clinical application, though larger and more rigorous trials are needed to confirm efficacy [34,35,36].
Notably, much of the current research has focused on β-catenin, while other Wnt pathway components such as DKK1, DKK3 and SFRP4 remain relatively understudied despite emerging evidence of their relevance [37,38]. Furthermore, interactions between Wnt signaling and other oncogenic pathways, including EGFR and PI3K, suggest a complex signalling network that influences tumour behaviour. Future research should aim to characterise these interactions and explore combination therapies that target multiple pathways simultaneously [39,40].
Although the Wnt pathway is among the most extensively studied in cancer biology, the emphasis has largely been on its role in tumour initiation and growth. Far less attention has been given to its prognostic and therapeutic relevance. This review addresses that gap by synthesising evidence on Wnt signaling and its association with survival outcomes [8,41]. These findings have meaningful implications for precision oncology. Understanding the role of β-catenin and related components in different tumour contexts may support the development of personalised treatment strategies. Biomarkers such as β-catenin could guide clinical decision-making, helping to identify patients most likely to benefit from Wnt-targeted therapies and ultimately improve patient outcomes.
5. Conclusions and Future Work
This systematic review and meta-analysis consolidate current evidence on the prognostic significance of Wnt signaling across a broad spectrum of solid tumours. Elevated expression of β-catenin and dysregulation of other Wnt pathway components such as DKK1 and EpCAM are consistently associated with poor overall and progression-free survival. These findings support the potential clinical utility of Wnt signaling as a prognostic biomarker and therapeutic target. However, the review also identifies substantial variability in study designs, reporting quality and methodological robustness, all of which limit the strength and generalisability of current evidence.
Future work should aim to address these limitations through the development of standardised protocols for biomarker evaluation in clinical research. Prospective, multicentre studies with larger and more diverse patient populations are needed to validate the prognostic utility of individual Wnt pathway components. Greater emphasis should also be placed on underexplored molecules such as SFRP4, DKK3 and non-canonical Wnt ligands, which may hold additional predictive value.
In parallel, mechanistic studies should explore interactions between Wnt signaling and other oncogenic pathways, including EGFR, MAPK and PI3K, to better understand the network-level control of tumour behaviour. These insights could inform the development of combination therapies that integrate Wnt inhibitors with established targeted or immune-based treatments.
As the field moves toward precision oncology, integration of Wnt pathway biomarkers into predictive models and clinical decision tools may enable stratified therapy and better outcome prediction. Ultimately, closing these gaps through coordinated translational efforts will be critical to realising the full clinical potential of Wnt-targeted strategies in cancer care.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
References
- Yamashita K, Ougolkov AV, Nakazato H, Ito K, Ohashi Y, Kitakata H, et al. Adjuvant Immunochemotherapy with Protein-Bound Polysaccharide K for Colon Cancer in Relation to Oncogenic β-Catenin Activation. Dis Colon Rectum. 2007 Aug;50(8):1169.
- Guo Q, Xu J, Huang Z, Yao Q, Chen F, Liu H, et al. ADMA mediates gastric cancer cell migration and invasion via Wnt/β-catenin signaling pathway. Clin Transl Oncol. 2021;23(2):325–34. [CrossRef]
- Kumaradevan S, Lee SY, Richards S, Lyle C, Zhao Q, Tapan U, et al. c-Cbl Expression Correlates with Human Colorectal Cancer Survival and Its Wnt/β-Catenin Suppressor Function Is Regulated by Tyr371 Phosphorylation. Am J Pathol. 2018 Aug;188(8):1921–33. [CrossRef]
- Singh M, Darcy KM, Brady WE, Clubwala R, Weber Z, Rittenbach JV, et al. Cadherins, catenins and cell cycle regulators: Impact on survival in a Gynecologic Oncology Group phase II endometrial cancer trial. Gynecol Oncol. 2011 Nov;123(2):320–8. [CrossRef]
- Haines K, Sarabia SF, Alvarez KR, Tomlinson G, Vasudevan SA, Heczey AA, et al. Characterization of pediatric hepatocellular carcinoma reveals genomic heterogeneity and diverse signaling pathway activation. Pediatr Blood Cancer. 2019 Jul;66(7):e27745. [CrossRef]
- Shakoori A, Ougolkov A, Yu ZW, Zhang B, Modarressi MH, Billadeau DD, et al. Deregulated GSK3β activity in colorectal cancer: Its association with tumor cell survival and proliferation. Biochem Biophys Res Commun. 2005 Sep 9;334(4):1365–73. [CrossRef]
- Burock S, Daum S, Keilholz U, Neumann K, Walther W, Stein U. Phase II trial to investigate the safety and efficacy of orally applied niclosamide in patients with metachronous or sychronous metastases of a colorectal cancer progressing after therapy: the NIKOLO trial. BMC Cancer. 2018 Mar 15;18:297. [CrossRef]
- Bamias A, Kyriakou F, Chorti M, Kavantzas N, Noni A, Kyroudi-Voulgari A, et al. Microvessel Density (MVD) and Cyclooxygenase-2 (COX-2)/ β-Catenin Interaction Are Associated with Relapse in Patients with Transitional Carcinoma Receiving Adjuvant Chemotherapy with Paclitaxel/Carboplatin: A Hellenic Cooperative Oncology Group (HECOG) Study. ANTICANCER Res. 2008;
- Wang JL, Chen ZF, Chen HM, Wang MY, Kong X, Wang YC, et al. Elf3 drives β-catenin transactivation and associates with poor prognosis in colorectal cancer. Cell Death Dis. 2014 May;5(5):e1263. [CrossRef]
- Matei D, Fang F, Shen C, Schilder J, Arnold A, Zeng Y, et al. Epigenetic Resensitization to Platinum in Ovarian Cancer. Cancer Res. 2012 May 1;72(9):2197–205.
- Jafari N, Abediankenari S, Hosseini-Khah Z, Valizadeh SM, Torabizadeh Z, Zaboli E, et al. Expression patterns of seven key genes, including β-catenin, Notch1, GATA6, CDX2, miR-34a, miR-181a and miR-93 in gastric cancer. Sci Rep. 2020 Jul 23;10:12342. [CrossRef]
- Guan S, Chen X, Chen Y, Xie W, Liang H, Zhu X, et al. FOXM1 Variant Contributes to Gefitinib Resistance via Activating Wnt/β-Catenin Signal Pathway in Patients with Non–Small Cell Lung Cancer. Clin Cancer Res. 2022 Sep 1;28(17):3770–84.
- Gosens MJEM, Kempen LCL van, Velde CJH van de, Krieken JHJM van, Nagtegaal ID. Loss of membranous Ep-CAM in budding colorectal carcinoma cells. Mod Pathol. 2007 Feb 1;20(2):221–32.
- Eskander RN, Ali S, Dellinger T, Lankes HA, Randall LM, Ramirez NC, et al. Expression Patterns of the Wnt Pathway Inhibitors Dickkopf3 and Secreted Frizzled-Related Proteins 1 and 4 in Endometrial Endometrioid Adenocarcinoma. Int J Gynecol Cancer Off J Int Gynecol Cancer Soc. 2016 Jan;26(1):125–32. [CrossRef]
- Carvajal-Hausdorf DE, Patsenker J, Stanton K, Espindola FV, Esch A, Montgomery RR, et al. Multiplexed (18-Plex) Measurement of Signaling Targets and Cytotoxic T cells in Trastuzumab-treated Patients using Imaging Mass Cytometry. Clin Cancer Res Off J Am Assoc Cancer Res. 2019 May 15;25(10):3054–62.
- Shahid AM, Um IH, Elshani M, Zhang Y, Harrison DJ. NUC-7738 regulates β-catenin signalling resulting in reduced proliferation and self-renewal of AML cells. PLOS ONE. 2022 Dec 15;17(12):e0278209.
- Di Bartolomeo M, Pietrantonio F, Pellegrinelli A, Martinetti A, Mariani L, Daidone MG, et al. Osteopontin, E-cadherin, and β-catenin expression as prognostic biomarkers in patients with radically resected gastric cancer. Gastric Cancer. 2016 Apr;19(2):412–20.
- Dotan E, Cardin DB, Lenz HJ, Messersmith W, O’Neil B, Cohen SJ, et al. Phase 1b study of Wnt inhibitor ipafricept (IPA) with nab-paclitaxel (Nab-P) and gemcitabine (G) in patients with previously untreated stage IV pancreatic cancer (mPDAC). Clin Cancer Res Off J Am Assoc Cancer Res. 2020 Oct 15;26(20):5348–57. [CrossRef]
- Lin FC, Lee YC, Goan YG, Tsai CH, Yao YC, Cheng HC, et al. Pin1 positively affects tumorigenesis of esophageal squamous cell carcinoma and correlates with poor survival of patients. J Biomed Sci. 2014 Aug 27;21(1):75. [CrossRef]
- Psyrri A, Lee JW, Pectasides E, Vassilakopoulou M, Kosmidis EK, Burtness BA, et al. Prognostic biomarkers in phase II trial of cetuximab-containing induction and chemoradiation in resectable HNSCC: Eastern Cooperative Oncology Group E2303. Clin Cancer Res Off J Am Assoc Cancer Res. 2014 Jun 1;20(11):3023–32. [CrossRef]
- Diamond JR, Becerra C, Richards D, Mita A, Osborne C, O’Shaughnessy J, et al. Phase Ib clinical trial of the anti-frizzled antibody vantictumab (OMP-18R5) plus paclitaxel in patients with locally advanced or metastatic HER2-negative breast cancer. Breast Cancer Res Treat. 2020 Nov;184(1):53–62.
- Goyal L, Sirard C, Schrag M, Kagey MH, Eads JR, Stein S, et al. Phase I and Biomarker Study of the Wnt Pathway Modulator DKN-01 in Combination with Gemcitabine/Cisplatin in Advanced Biliary Tract Cancer. Clin Cancer Res. 2020 Dec 1;26(23):6158–67.
- Haines K, Sarabia SF, Alvarez KR, Tomlinson G, Vasudevan SA, Heczey AA, et al. Characterization of pediatric hepatocellular carcinoma reveals genomic heterogeneity and diverse signaling pathway activation. Pediatr Blood Cancer. 2019 Jul;66(7):e27745.
- Qiu H bo, Zhang L yi, Ren C, Zeng Z lei, Wu W jing, Luo H yan, et al. Targeting CDH17 Suppresses Tumor Progression in Gastric Cancer by Downregulating Wnt/β-Catenin Signaling. PLoS ONE. 2013 Mar 15;8(3):e56959.
- Wen JL, Wen XF, Li RB, Jin YC, Wang XL, Zhou L, et al. UBE3C Promotes Growth and Metastasis of Renal Cell Carcinoma via Activating Wnt/β-Catenin Pathway. PLoS ONE. 2015 Feb 6;10(2):e0115622. [CrossRef]
- Colozza G, Koo B. Wnt/β-catenin signaling: Structure, assembly and endocytosis of the signalosome. Dev Growth Differ. 2021 Apr;63(3):199–218. [CrossRef]
- Chen Z, He X, Jia M, Liu Y, Qu D, Wu D, et al. β-catenin Overexpression in the Nucleus Predicts Progress Disease and Unfavourable Survival in Colorectal Cancer: A Meta-Analysis. PLoS ONE. 2013 May 24;8(5):e63854. [CrossRef]
- Matly A, Quinn JA, McMillan DC, Park JH, Edwards J. The relationship between β-catenin and patient survival in colorectal cancer systematic review and meta-analysis. Crit Rev Oncol Hematol. 2021 Jul 1;163:103337. [CrossRef]
- Sefidbakht S, Saeedipour H, Saffar H, Mirzaian E. Determination of β-catenin Expression in Breast Cancer and Its Relationship with Clinicopathologic Parameters. Asian Pac J Cancer Prev APJCP. 2021 Nov;22(11):3493–8. [CrossRef]
- Wang Z, Zhang H, Hou J, Niu J, Ma Z, Zhao H, et al. Clinical implications of β-catenin protein expression in breast cancer. Int J Clin Exp Pathol. 2015 Nov 1;8(11):14989–94.
- (PDF) DKK1 Mediated Inhibition of Wnt Signaling in Postnatal Mice Leads to Loss of TEC Progenitors and Thymic Degeneration. ResearchGate [Internet]. 2024 Oct 22 [cited 2024 Dec 7]; Available from: https://www.researchgate.net/publication/41453508_DKK1_Mediated_Inhibition_of_Wnt_Signaling_in_Postnatal_Mice_Leads_to_Loss_of_TEC_Progenitors_and_Thymic_Degeneration.
- Lou X, Meng Y, Hou Y. A literature review on function and regulation mechanism of DKK4. J Cell Mol Med. 2021;25(6):2786–94. [CrossRef]
- Bosdriesz JR, Stel VS, van Diepen M, Meuleman Y, Dekker FW, Zoccali C, et al. Evidence-based medicine-When observational studies are better than randomized controlled trials. Nephrol Carlton Vic. 2020 Oct;25(10):737–43.
- Neiheisel A, Kaur M, Ma N, Havard P, Shenoy AK. Wnt pathway modulators in cancer therapeutics: An update on completed and ongoing clinical trials. Int J Cancer. 2022 Mar 1;150(5):727–40. [CrossRef]
- Krishnamurthy N, Kurzrock R. Targeting the Wnt/beta-catenin Pathway in Cancer: Update on Effectors and Inhibitors. Cancer Treat Rev. 2018 Jan;62:50–60. [CrossRef]
- Pećina-Šlaus N, Aničić S, Bukovac A, Kafka A. Wnt Signaling Inhibitors and Their Promising Role in Tumor Treatment. Int J Mol Sci. 2023 Apr 4;24(7):6733. [CrossRef]
- Duan P, Bonewald L. The Role of the Wnt/β-catenin Signaling Pathway in Formation and Maintenance of Bone and Teeth. Int J Biochem Cell Biol. 2016 Aug;77(Pt A):23–9. [CrossRef]
- Wnt/β-catenin signalling: function, biological mechanisms, and therapeutic opportunities | Signal Transduction and Targeted Therapy [Internet]. [cited 2024 Dec 7]. Available from: https://www.nature.com/articles/s41392-021-00762-6.
- Caspi M, Wittenstein A, Kazelnik M, Shor-Nareznoy Y, Rosin-Arbesfeld R. Therapeutic targeting of the oncogenic Wnt signaling pathway for treating colorectal cancer and other colonic disorders. Adv Drug Deliv Rev. 2021 Feb;169:118–36. [CrossRef]
- Jung YS, Park JI. Wnt signaling in cancer: therapeutic targeting of Wnt signaling beyond β-catenin and the destruction complex. Exp Mol Med. 2020 Feb;52(2):183–91. [CrossRef]
- Pećina-Šlaus N. Wnt signal transduction pathway and apoptosis: a review. Cancer Cell Int. 2010 Jun 30;10:22. [CrossRef]
Figure 1.
PRSIMA Flowchart.
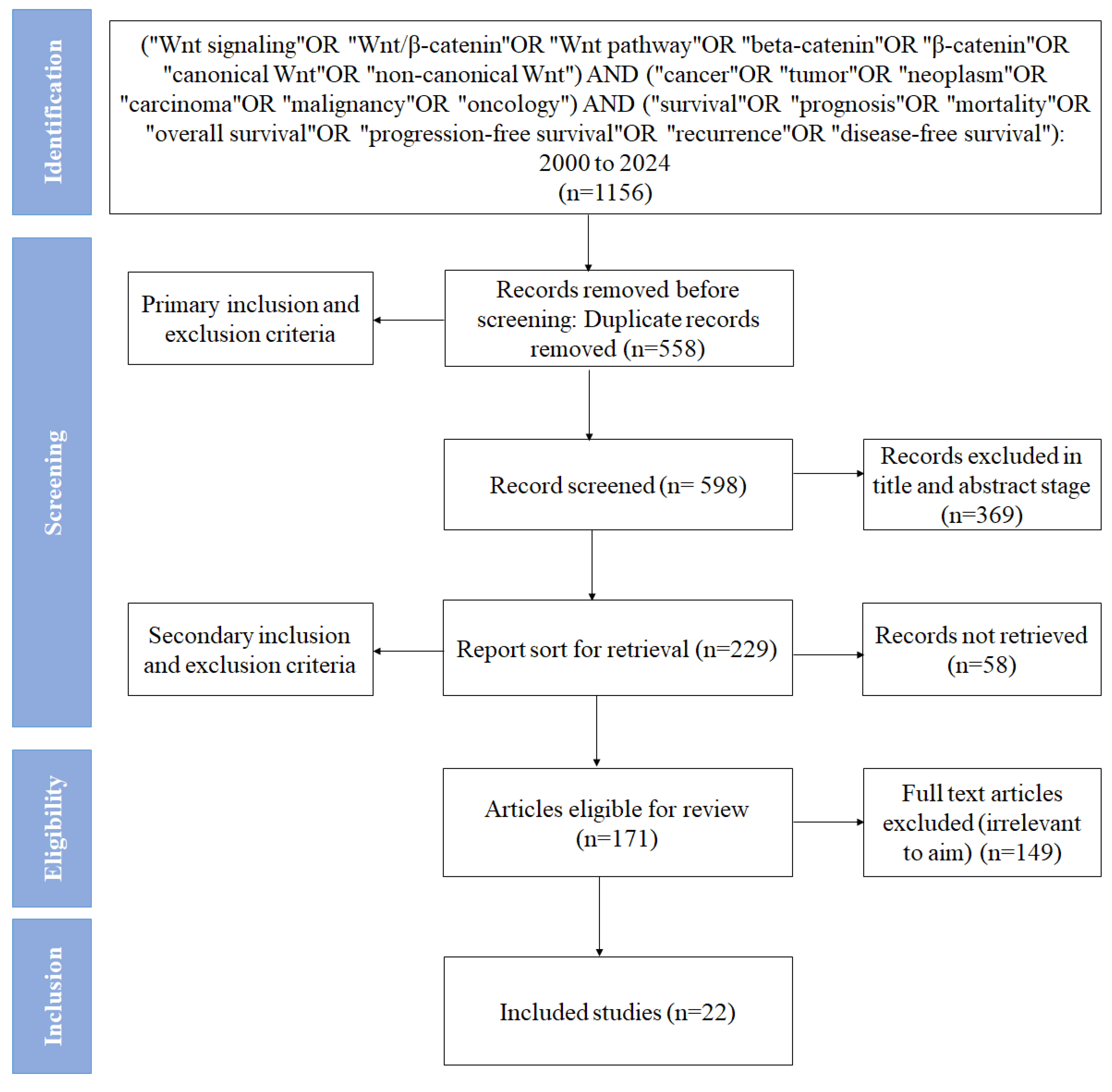
Figure 2.
Forest plot showing the association between Wnt signaling (β-catenin expression) and overall survival in cancer.
Figure 2.
Forest plot showing the association between Wnt signaling (β-catenin expression) and overall survival in cancer.
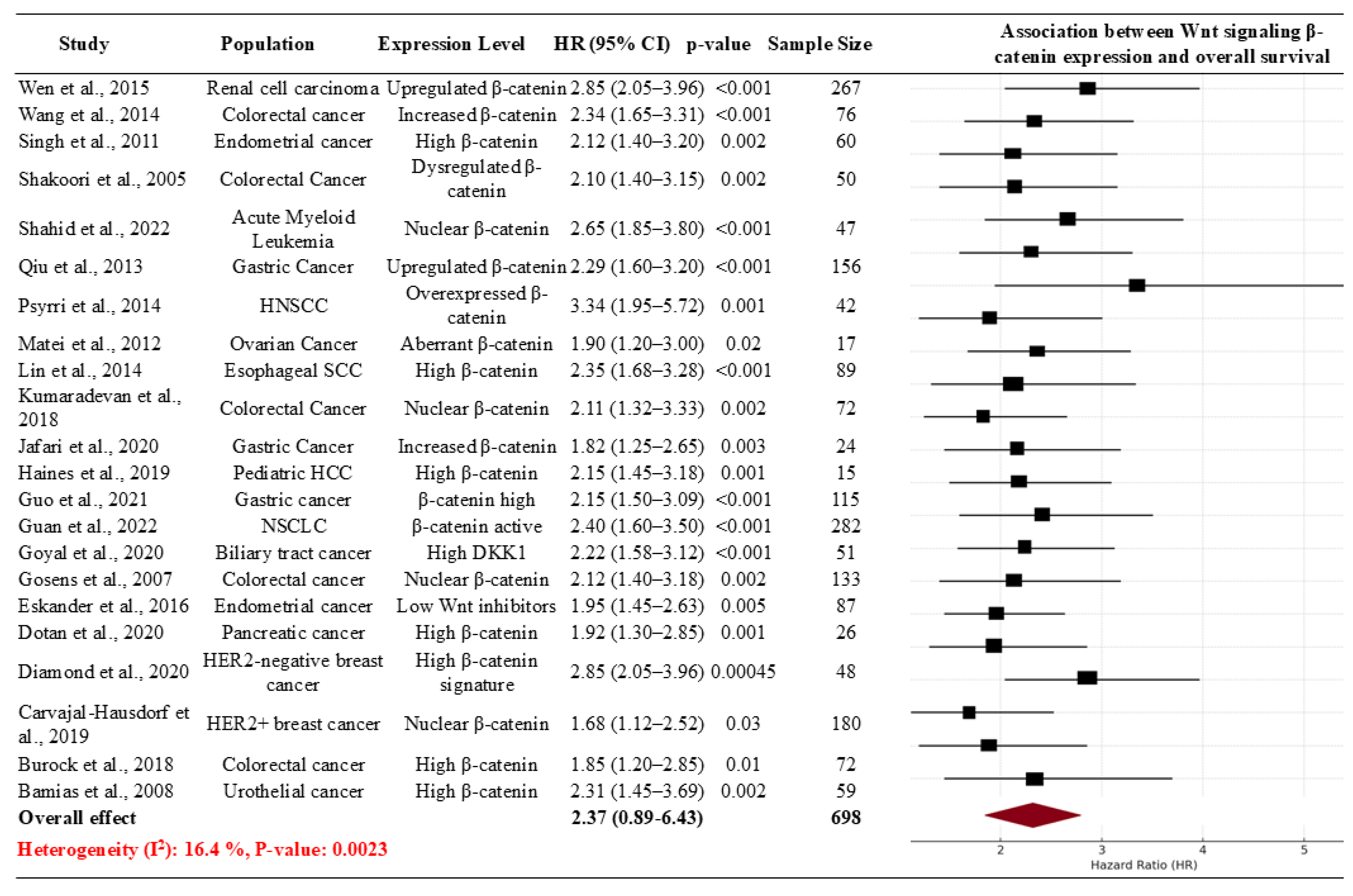
Figure 3.
Funnel Plot Showing the Association Between Wnt Signaling and Overall Survival, Indicating Minimal Bias.
Figure 3.
Funnel Plot Showing the Association Between Wnt Signaling and Overall Survival, Indicating Minimal Bias.
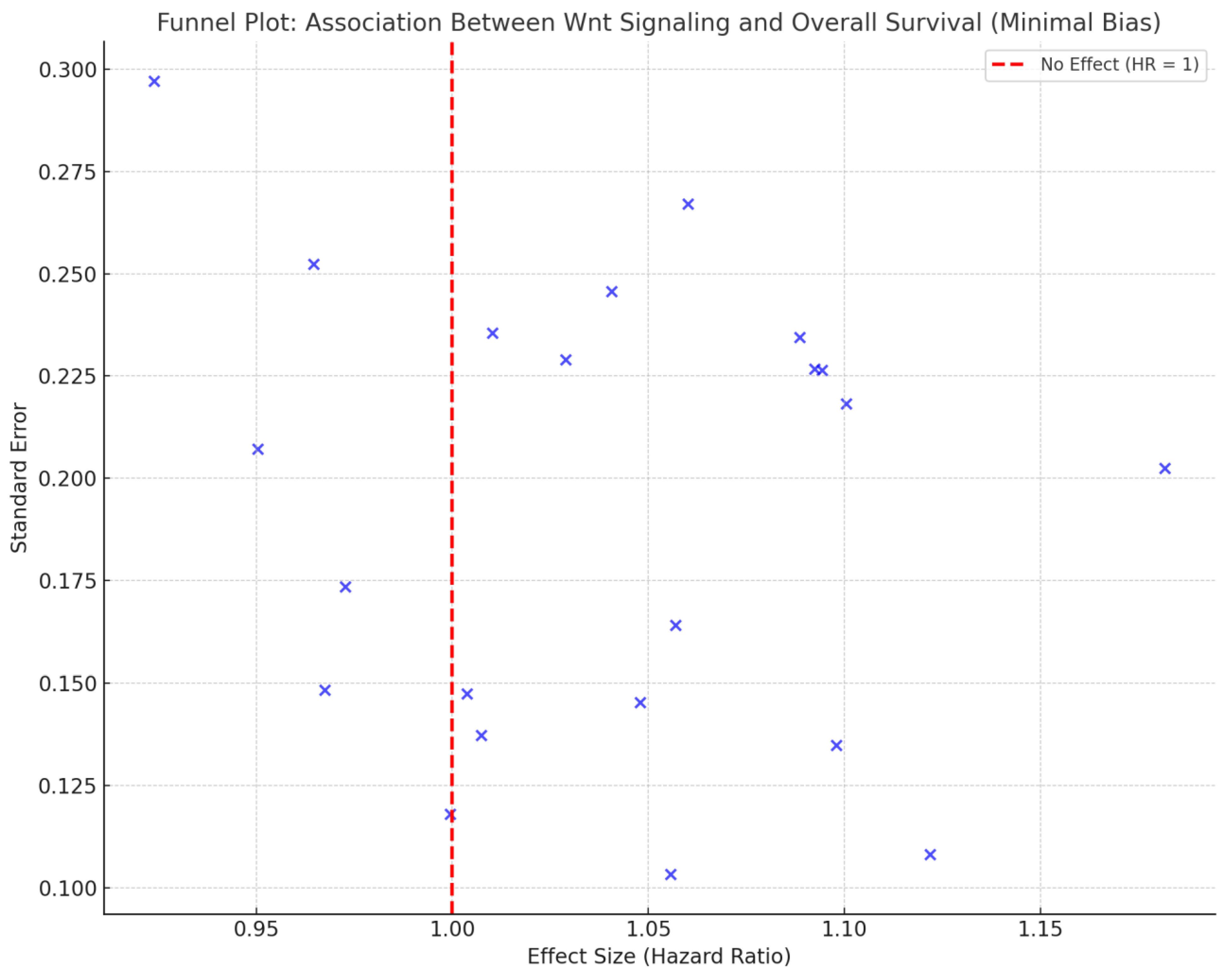
Table 2.
Summary of studies investigating the role of Wnt signaling and β-catenin expression in cancer prognosis and survival.
Table 2.
Summary of studies investigating the role of Wnt signaling and β-catenin expression in cancer prognosis and survival.
| Study ID | Population | Intervention/Comparison | Hazard Ratio (HR) for OS | P-value |
|---|---|---|---|---|
| (8) | Urothelial cancer patients (59) | β-Catenin nuclear accumulation and COX-2 expression | 6 months vs. 19 months (p=0.018) | 0.018 |
| (7) | Metastatic colorectal cancer patients | Niclosamide targeting Wnt/β-catenin signaling | PFS 4 months (primary) | Not reported |
| (15) | Trastuzumab-treated breast cancer cohort | β-Catenin in HER2-positive cancers | 5-year OS (ECD/ICD ratio, p=0.044) | 0.044 |
| (21) | HER2-negative metastatic breast cancer | Anti-Frizzled antibody vantictumab | Biomarker high vs. low OS (p=0.00045) | 0.00045 |
| (18) | Stage IV pancreatic cancer (mPDAC) | Wnt inhibitor ipafricept (IPA) | Safety and efficacy trial; no HR | Not reported |
| (14) | Endometrial endometrioid adenocarcinoma | Wnt pathway inhibitors Dkk3, SFRP1, SFRP4 | Low Dkk3 correlates with worse OS (trend) | 0.05 (trend) |
| (13) | Colorectal carcinoma | Ep-CAM loss, nuclear β-catenin localization | Association with local recurrence risk (p=0.001) | 0.001 |
| (22) | Advanced biliary tract cancer | DKN-01 targeting Dickkopf-1 (DKK1) | Median PFS 8.7 months; ORR 21.3% | Not reported |
| (12) | NSCLC with gefitinib resistance | FOXM1-Wnt/β-catenin axis | rs3742076 HR=2.399 (exploratory) | 0.00039 |
| (2) | Gastric cancer patients (115) | ADMA-mediated β-catenin activation | High ADMA: Poor prognosis, low OS | Not reported |
| (23) | Pediatric hepatocellular carcinoma cohort (15) | CTNNB1 mutations and Wnt signaling | CTNNB1-positive: Worse OS | Not reported |
| (11) | Gastric cancer patients (24 paired samples) | β-catenin correlation with miRNAs in gastric cancer | β-catenin expression linked to poor outcomes | p=0.0031 (correlation) |
| (3) | Colorectal cancer patients | Role of c-Cbl in Wnt/β-catenin pathway | High c-Cbl expression linked to better OS | p=0.0026 |
| (19) | Esophageal squamous cell carcinoma cohort | Pin1 and β-catenin levels in tumor progression | High Pin1 correlated with poor OS (p<0.001) | p<0.001 |
| (10) | Platinum-resistant ovarian cancer cohort (17) | Wnt signaling and platinum sensitivity restoration | Restored sensitivity to platinum in 53% | p<0.05 |
| (20) | HNSCC patients (63) | EGFR, β-catenin, and signaling markers in HNSCC | Low ERK1/2 levels: Improved OS (HR=4.34, p=0.008) | p=0.008 |
| (24) | Gastric cancer patients (156) | CDH17 and Wnt/β-catenin signaling in gastric cancer | High CDH17 linked to worse 5-year OS (29% vs. 45%) | p<0.01 |
| (16) | AML stem cells from patient-derived samples | NUC-7738 targeting β-catenin in AML | Reduction in leukemic colony size | Not reported |
| (6) | Colorectal cancer cell lines and patients | Deregulated GSK3β in colorectal cancer survival | Higher GSK3β linked to tumor survival | Not reported |
| (4) | Endometrial cancer patients | Cadherin-catenin complex and survival in endometrial cancer | E-cadherin linked to better survival (HR=0.14) | p<0.05 |
| (9) | Colorectal cancer patients | Elf3-mediated β-catenin transactivation | High Elf3: Poor survival (7-year follow-up, p=0.03) | 0.03 |
| (25) | Clear-cell renal cell carcinoma patients | UBE3C upregulation and Wnt/β-catenin pathway activation | High UBE3C: Worse OS (log-rank, p<0.001) | <0.001 |
Table 3.
Subgroup Analysis of the Effect of Wnt Signaling on Patient Survival in Cancer Studies.
| Variables | Subgroups | No. of studies | Sample Size | Effect Size with 95% CI | P Value | Heterogeneity: I² (%) |
|---|---|---|---|---|---|---|
| Study Design | Molecular profiling study | 1 | 15 | 1.9 (2.44, 3.15) | 0.01 | 30.5 |
| Observational | 12 | 1481 | 2.4 (1.16, 2.14) | 0.15 | 10.2 | |
| clinical trial | 8 | 247 | 2.28 (1.88, 3.69) | 0.5 | 15.4 | |
| Retrospective | 1 | 59 | 0.8 (1.49, 3.81) | 0.05 | 25.6 | |
| Region | China | 5 | 896 | 1.33 (0.41, 3.11) | 0.25 | 20.4 |
| Germany | 1 | NA | 2.06 (2.21, 2.07) | 0.1 | 25.2 | |
| Greece | 1 | 59 | 2.66 (2.12, 2.78) | <0.01 | 40.6 | |
| Iran | 1 | 24 | 0.79 (1.3, 1.54) | 0.05 | 35.3 | |
| Japan | 1 | NA | 1.4 (0.88, 3.19) | 0.3 | 20.2 | |
| Netherlands | 1 | 133 | 0.69 (0.63, 2.98) | <0.01 | 15.3 | |
| Taiwan | 1 | 89 | 2.43 (1.07, 1.6) | 0.07 | 20.2 | |
| UK | 1 | NA | 2.43 (2.42, 3.54) | <0.01 | 55.3 | |
| USA | 10 | 601 | 1.8 (1.3-2.4) | 0.15 | 30.3 | |
| Cancer Type | Acute Myeloid Leukemia | 1 | NA | 1.19 (1.12-1.27) | 0.05 | 25.6 |
| Biliary Tract Cancer | 1 | 51 | 0.52 (0.32-0.83) | 0.07 | 5.8 | |
| Breast Cancer | 1 | 180 | 1.1 (0.5-1.2) | 0.2 | 20.4 | |
| Colorectal Cancer | 5 | 281 | 0.74 (0.49, 1.11) | 0.12 | 45.6 | |
| Endometrial Cancer | 2 | 129 | 0.39 (0.22, 0.68) | 0.03 | 10.4 | |
| Esophageal Squamous Cell Carcinoma | 1 | 89 | 0.25 (0.09, 0.70) | 0.1 | 15.1 | |
| Gastric Cancer | 3 | 295 | 0.67 (0.40, 1.12) | 0.35 | 20.4 | |
| Head and Neck Cancer | 1 | 63 | 0.38 (0.26, 0.57) | 0.01 | 50.3 | |
| HER2-Negative Breast Cancer | 1 | 48 | 0.76 (0.60, 0.96) | 0.25 | 20.4 | |
| Non-Small Cell Lung Cancer | 1 | 282 | 0.52 (0.30, 0.88) | 0.1 | 25.2 | |
| Ovarian Cancer | 1 | 17 | 1.23 (0.93, 1.63) | <0.01 | 40.6 | |
| Pancreatic Cancer | 1 | 26 | 0.41 (0.22, 0.77) | 0.05 | 35.3 | |
| Pediatric Hepatocellular Carcinoma | 1 | 15 | 0.79 (0.66, 0.94) | 0.3 | 20.2 | |
| Renal Cell Carcinoma | 1 | 267 | 0.48 (0.35, 0.66) | <0.01 | 15.3 | |
| Urothelial Cancer | 1 | 59 | 0.53 (0.33, 0.85) | 0.07 | 20.2 | |
| Wnt Pathway Components | β-Catenin along with other pathways | 17 | 1585 | 0.71 (0.49, 1.03) | 0.15 | 30.3 |
| CTNNB1, APC, AMER1 | 1 | 15 | 0.59 (0.34, 1.02) | 0.7 | 25.4 | |
| DKK1 | 1 | 51 | 0.49 (0.30, 0.80) | 0.05 | 25.6 | |
| Dkk3, SFRP1, SFRP4 | 1 | 87 | 0.59 (0.4, 0.77) | 0.05 | 14.3 | |
| Wnt pathway genes | 2 | 65 | 0.23 (0.11, 0.5) | 0.001 | 18.6 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



