
Submitted:
14 July 2025
Posted:
15 July 2025
You are already at the latest version
Abstract
(1) Background: Femoral neck fractures (FNF) in the ageing population carry high risks of postoperative dislocation, with traditional total hip arthroplasty (THA) reporting rates up to 10%. Dual Mobility THA (DM-THA) may offer superior stability, but evidence for third-generation implants like the Zimmer Biomet G7® system re-mains limited. (2) Methods: This retrospective cohort study evaluated 120 patients (mean age 71.6 years; 74% female) with acute displaced intracapsular FNF treated with DM-THA (2017–2023) using the G7® system. Demographics, surgical details (cemented/uncemented stems), complications, and functional outcomes (Oxford Hip Score (OHS) at one year) were analysed against national benchmarks. (3) Results: Zero dislocations and two peri-prosthetic fracture (0.8%, cemented stem) occurred. Thirty-day mortality was 0.8% (below national averages). Functional recovery was excel-lent (mean OHS: 41/48; 69% scoring ≥40). Surgical complications were minimal (one deep infection 0.8%). Medical complications (anaemia 6.6%, venous thromboembolism 4.2%) aligned with expectations. Radiographs confirmed stable implants without loosening. (4) Conclusion: The G7® DM-THA system demonstrates exceptional stability and safety in FNF patients, with no dislocation risk and low peri-prosthetic fracture rates - even with cemented stems. These outcomes support its use in high-risk populations, though comparative studies with conventional THA are warranted.
Keywords:
femoral neck fractures
; dual mobility total hip arthroplasty
; prosthesis dislocation
; third-generation dual mobility cup
; periprosthetic fracture
; cemented femoral stem
; Oxford Hip Score
; elderly trauma
1. Introduction
Femoral neck fractures (FNF) represent a significant healthcare burden, particularly among elderly patients with frailty and osteoporosis, necessitating surgical interventions such as total hip arthroplasty (THA) to restore mobility and quality of life. While THA is preferred over hemiarthroplasty for displaced intracapsular FNF due to superior functional outcomes, traditional single-mobility implants carry a concerning dislocation risk of 2-10% in primary surgeries [1] and up to 9-17% in revisions [2,3], contributing to increased morbidity and mortality. Dual mobility (DM) acetabular systems, such as the G7® Biomet Zimmer with its dual articulation design and elevated rim, have emerged to address instability through enhanced biomechanical properties, including a constrained polyethene liner and larger effective femoral head diameter [4,5]. Registry studies demonstrate DM implants reduce dislocation rates to <2% in primary THA [4] and 1.6% in revisions [3], particularly in high-risk populations such as elderly patients, those with neuromuscular disorders, or individuals requiring extreme hip flexion [5,6].
However, the benefits of DM designs must be balanced against concerns regarding Peri-prosthetic Fractures (PPFs), which remain a critical complication. Systematic reviews highlight higher PPF rates in revision THA [7], with smaller studies, such as a single-centre cohort of 126 patients, reporting DM cups associated with a 76% incidence compared to 24% for conventional implants [6]. This contrast may reflect altered load transfer dynamics in DM systems, though larger studies are needed to confirm these findings. Patient-specific factors such as poor bone quality and surgical technique - including improper implant positioning or excessive bone reaming - further exacerbate fracture risks [8,9]. Despite these challenges, modular systems like the G7® offer intraoperative versatility through optimised component alignment and cemented stem utilisation [6].
Current evidence on the G7® system remains limited by a focus on elective or mixed cohorts, obscuring trauma-specific outcomes. Furthermore, no studies have systematically benchmarked G7® performance against the UK National Hip Fracture Database (NHFD) for FNF management, leaving critical gaps in understanding its risk-benefit profile in fragility fracture populations.
This study addresses these limitations by evaluating a cohort of FNF patients treated with the G7® system, with three objectives:
(1) Assess functional, safety and radiographic outcomes
(2) Quantify dislocation and PPF rates using standardised CDC and Vancouver classification criteria
(3) Contextualise results against NHFD benchmarks, including 30-day mortality.
By isolating trauma patients and stratifying complications, this investigation provides evidence to optimise implant selection and surgical protocols in high-risk populations.
2. Materials and Methods
This retrospective cohort study evaluated patients undergoing primary THA with the Zimmer Biomet G7® DM system for femoral neck fractures at Mid-Yorkshire Teaching Hospitals NHS Trust (2017–2023). Study adhered to STROBE guidelines for observational studies.
Patient Selection
Inclusion Criteria:
- Acute, displaced intracapsular femoral neck fracture (Garden III/IV)
- Primary THA using the Zimmer Biomet G7® DM acetabular system.
Exclusion Criteria:
- Pathological fractures (n=3)
- Prior ipsilateral hip arthroplasty (n=2)
To address potential selection bias, we employed a two-tiered analytical approach:
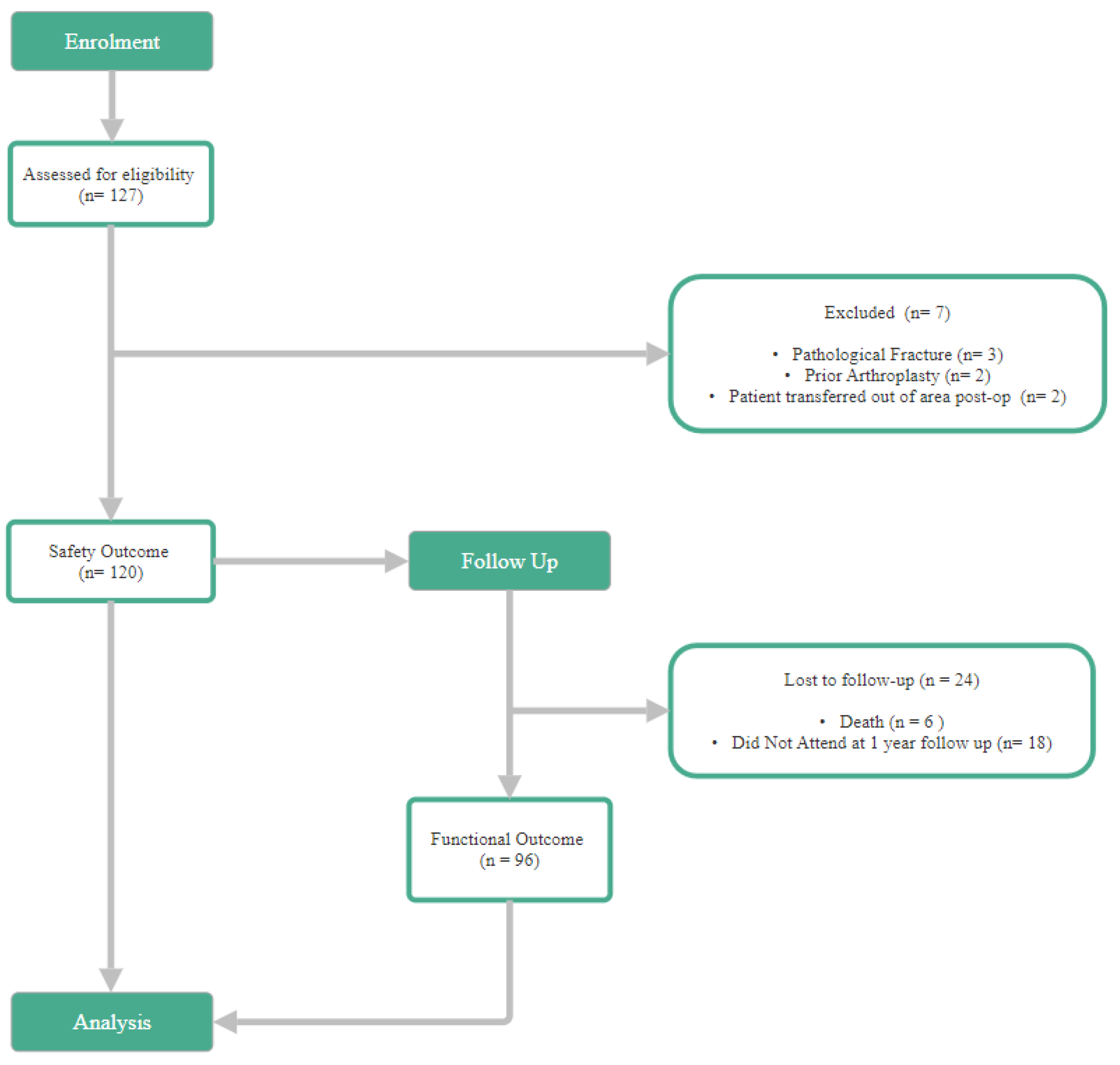
- Functional Outcomes Cohort (n=96): Patients with complete 1-year follow-up including Oxford Hip Score (OHS)
- Safety Cohort (n=120): All eligible patients, capturing early postoperative complications regardless of follow-up duration
Surgical Protocol
All procedures were performed or supervised by fellowship-trained arthroplasty surgeons
Approach:
- Posterior approach
- Anterolateral approach (Watson-Jones)
- Direct lateral approach
- Direct anterior approach (modified Smith-Petersen)
Implants:
- G7® DM shell
- Cemented (CPT/C-Stem)
- Uncemented (Corail)
Perioperative/ Postoperative Care:
- Antibiotic prophylaxis (Teicoplanin 800mg IV)
- Mechanical and chemical VTE prophylaxis
- Mobilisation within 24 hours
Outcome Measures
Functional (n=96): At 1-year follow up:
- Intra-prosthetic Dislocation Rate
- Oxford Hip Score (OHS)
Safety (n=120): Complications stratified by timing:
- Early (≤6 weeks): VTE, infection, acute kidney injury (AKI), nerve injury.
- Late (>6 weeks): Peri-prosthetic Fracture, chronic pain, limb length discrepancy.
Statistical Analysis
All analyses were performed using Python 3.12, Vision Studio Code 1.101
Descriptive Statistics:
- Continuous variables: Mean ± SD (age, OHS)
- Categorical variables: Frequencies (%)
Subgroup Analyses:
- Cemented vs. uncemented stems for complications and OHS.
- American Society of Anaesthesiologists score (ASA) stratification for complications.
Comparative Tests:
- Mann-Whitney U test: Compared mean OHS between groups (assumed non-normality, confirmed via Shapiro-Wilk test).
- Fisher’s Exact test: Compared complication rates (e.g., infection) between cemented and uncemented stems (small, expected counts).
- Z-test for Proportions: Benchmarking against NHFD 2024 30-day mortality rate.
Significance Threshold: α = 0.05 (two-tailed).
Addressing Potential Biases
Selection Bias: Two-tiered cohort design captures all safety events.
Measurement Bias: Standardised outcome definitions and dual-data extraction. Two independent reviewers extracted complications, with discrepancies resolved by a third arbitrator.
Confounding: Acknowledged unmeasured variables (frailty, cognition) in limitations the authority that provided approval and the corresponding ethical approval code.
3. Results
Cohort Demographics
The study analysed 120 patients (Safety Cohort) who underwent G7® DM-THA for femoral neck fractures. Of these, 96 patients (90.1%) had completed 1-year follow-up (Functional cohort). Outcome of the 120 patients, the mean age was 71.6 ± 9.4 years (range 43-92), with 74.2% (n = 89) female and 25.8% (n = 31) male. Most patients were classified as ASA grade II (61.7%) or III (33.3%), reflecting a relatively high comorbidity burden typical of this trauma cohort.

Table 1.
Age Distribution.
| Mean Age | Standard Deviation | Range |
|---|---|---|
| 71.6 | 9.4 | 43-92 |
Table 2.
Gender Distribution.
| Sex | Count | % |
|---|---|---|
| Female | 89 | (74.2%) |
| Male | 31 | (25.8%) |
| Total | 120 |
Table 3.
ASA Scores.
| ASA | Count | % |
|---|---|---|
| I | 5 | (4.2%) |
| II | 74 | (61.7%) |
| III | 40 | (33.3%) |
| IV | 1 | (0.83%) |
| Total | 120 |
Implant Distribution
All patients received the 3rd-generation Zimmer Biomet G7® dual mobility acetabular cup. Femoral implant selection was based on intraoperative bone quality and patient comorbidities, with cemented stems more frequently used in older or osteoporotic patients. This section may be divided by subheadings. It should provide a concise and precise description of the experimental results, their interpretation, as well as the experimental conclusions that can be drawn.
Table 4.1.
Stem Type – Safety Cohort.
| Stem Type | Count | % | Notes |
| Cemented | 93 | 77.5 | CPT/C-Stem |
| 2 | 1.7 | C-Stem | |
| 91 | 75.8 | CPT | |
| Uncemented | 24 | 20.0 | Corail Stems |
| Unknown | 3 | 2.5 | Op note didn’t specify - excluded from stem comparisons. |
| Total | 120 |
Table 4.2.
Stem Type – Functional Cohort
| Stem Type | Count | % | Notes |
| Cemented | 73 | 76.0 | CPT/C-Stem |
| 1 | 1.0 | C-Stem | |
| 72 | 75.0 | CPT | |
| Uncemented | 20 | 20.8 | Corail Stems |
| Unknown | 3 | 3.1 | Op note didn’t specify - excluded from stem comparisons. |
| Total | 96 |
Functional Outcomes
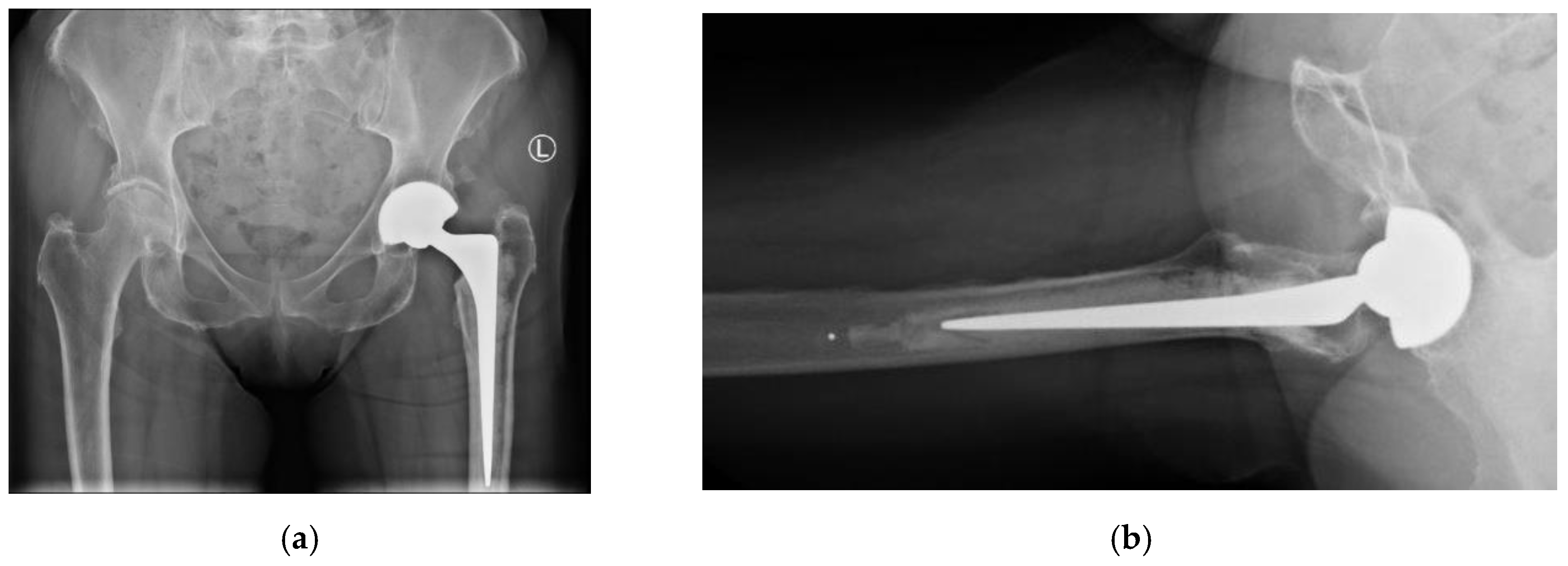
Overall, at one-year follow-up there was no case of dislocation (0.0 %), demonstrating excellent stability. All radiographs demonstrated appropriate component positioning and no radiographic loosening (AP/lateral views) of the implant.
Table 5.
Dislocation incidents upon at 1 year follow-up.
| Dislocation | Count | % | ||
|---|---|---|---|---|
| Cemented | 0 | 0 | ||
| Uncemented | 0 | 0 | ||
| Total | 0 | |||
Figure 1.
Postoperative radiographs at 1 year follow-up. 1a) AP view showing cemented CPT stem and neutral cup positioning (Left). 1b) Lateral view confirming absence of radiolucency around the acetabular component.
Figure 1.
Postoperative radiographs at 1 year follow-up. 1a) AP view showing cemented CPT stem and neutral cup positioning (Left). 1b) Lateral view confirming absence of radiolucency around the acetabular component.
At one-year follow-up, the mean OHS was 41.0 ± 8.3 (range: 5-48), with 68.8 % achieving excellent outcomes (OHS ≥40). There is no statistically significant difference in OHS was observed between cemented and uncemented stem groups (p=0.125, Mann-Whitney U test)
Table 6.
Mean Oxford Hip Score at 1-year follow up.
| Fixation Type | Mean OHS | SD | Range | 95% Confidence Interval for meanLower Bound Upper Bound | ||
|---|---|---|---|---|---|---|
| Cemented | 40.2 | 8.9 | 5-48 | 38.1 | 42.3 | |
| Uncemented | 43.9 | 4.5 | 34-38 | 41.8 | 46.0 | |
| Total | 41.0 | 8.3 | 5-48 | 38.3 | 42.7 | |
Low but non-zero risk of Peri-prosthetic Fracture (PPF) in the cemented group (1.0%) at one-year follow-up despite 75% CPT use in this study.
Table 7.
Incidents of Peri-prosthetic Fracture (PPF) at 1-year follow up.
| Peri-prosthetic Fracture | Count | % | |
|---|---|---|---|
| Cemented | 1 | 1.0 | |
| Uncemented | 0 | 0 | |
| Total | 1 |
Safety Outcomes
Complications analyses within the Safety Cohort (n=120) were stratified to separate early post-op (≤6 weeks) and long-term (>6 weeks) events, with clear definitions and clinical context. This is so we can identify different targets to assist with recovery at different phases. Overall, no dislocations were observed during follow-up, reinforcing the enhanced stability profile of the G7® dual mobility system.
Early complications (≤6 weeks) were primarily medical (6.6% Anaemia, 4.2% VTE), rather than implant related. There was one case of PPF (0.8%), which resulted in the revision of the acetabulum. There are no dislocations or early mechanical failures identified at this phase. All radiographs post-operative demonstrated appropriate component positioning and no radiographic loosening (AP/lateral views) of the implant.
Figure 2.
Bar Chart of Early Complications - Overall.
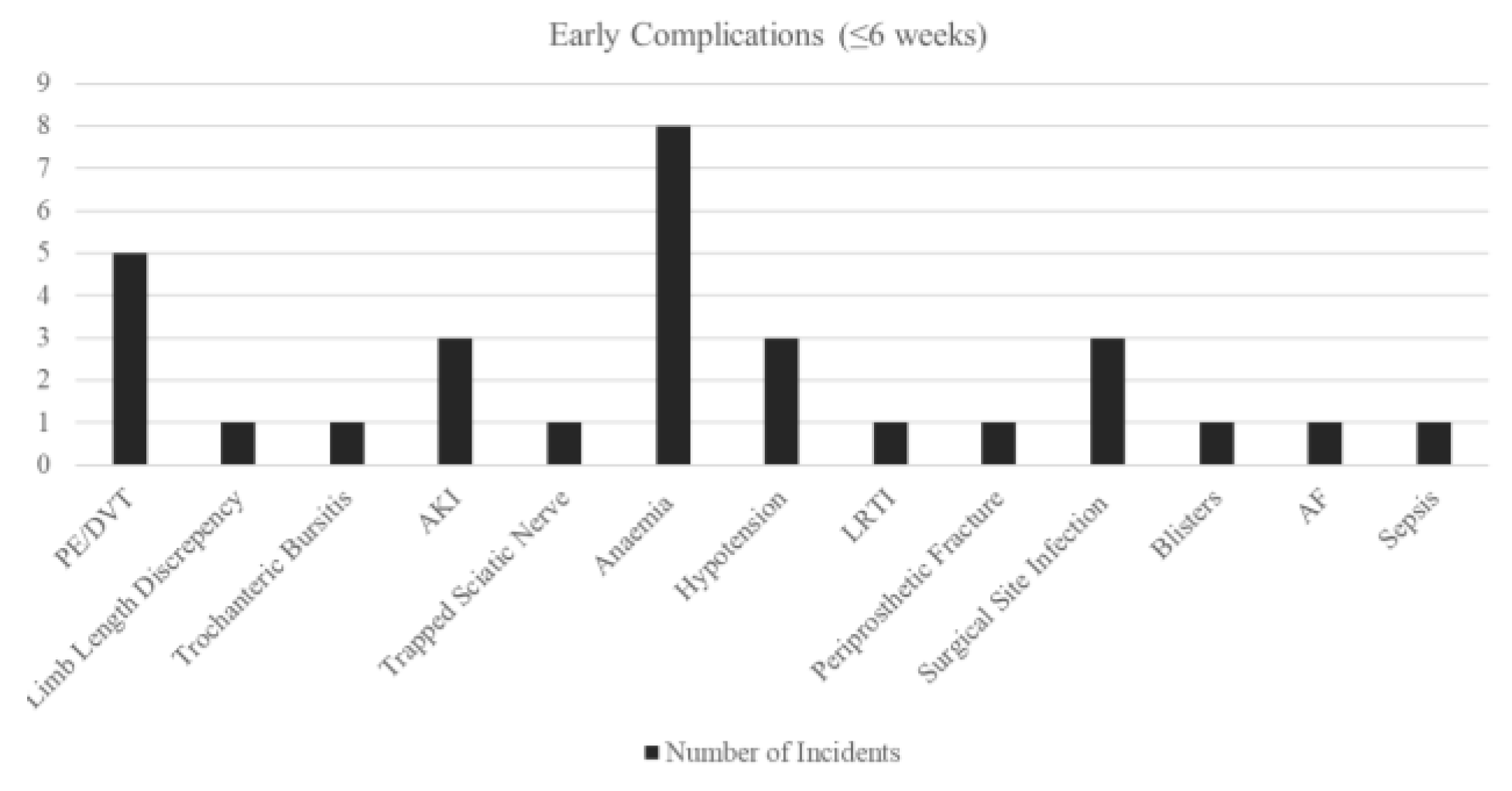
Figure 3.
Bar Chart of Early Complications - by Cement Types.
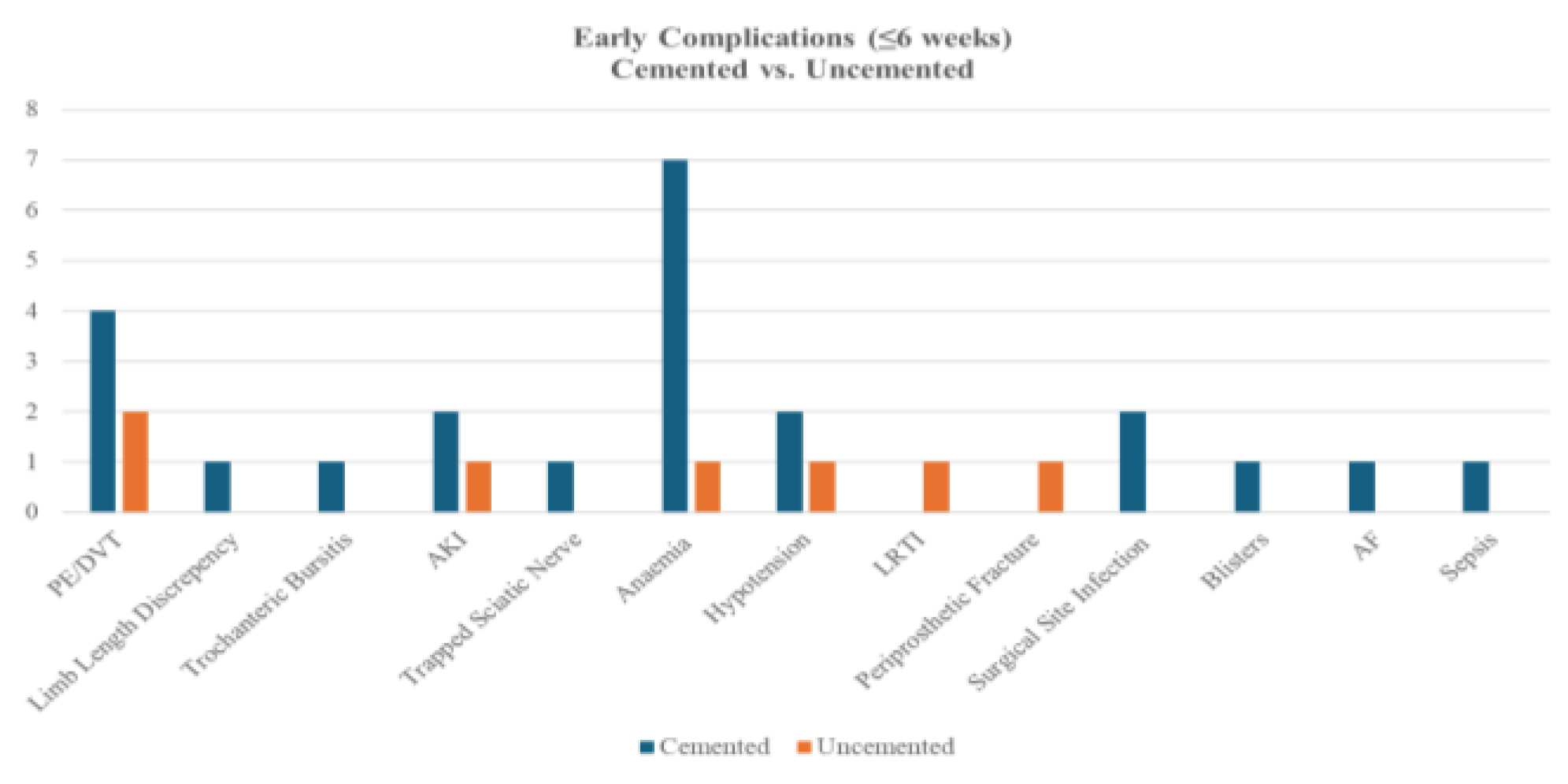
A comparison of early complications between cemented (n=93) and uncemented (n=24) procedures revealed no statistically significant differences in overall or individual complication rates (all p>0.05, Fisher’s Exact test). Cemented fixation showed non-significantly higher rates of anaemia (7.5% vs. 4.2%), PE/DVT (4.3% vs. 8.3%), and surgical site infection (2.2% vs. 0%), while uncemented fixation had a numerically higher incidence of PPF (4.2% vs. 0%).
Figure 4.
Bar Chart of Early Complications - by ASA groups.
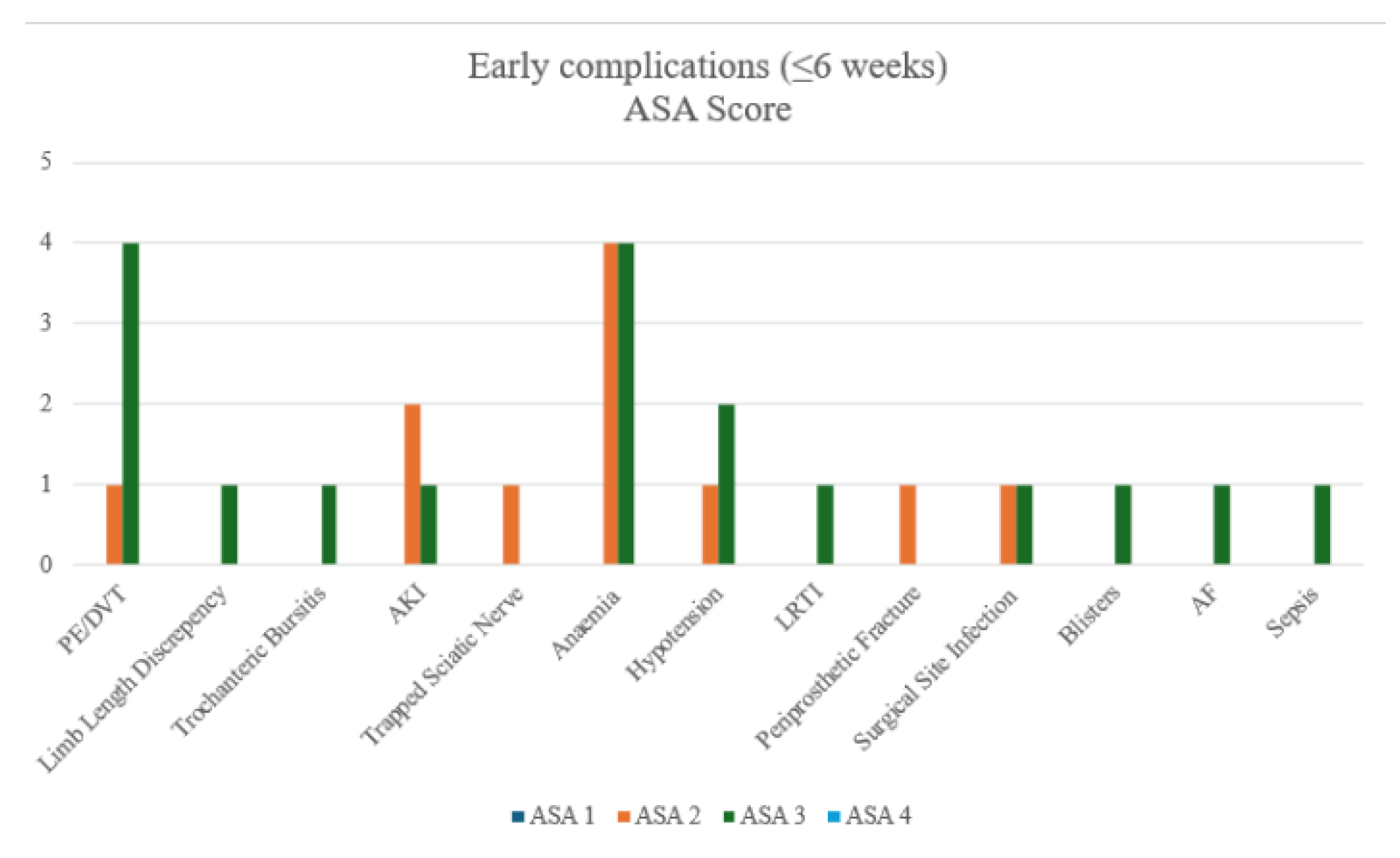
After merging ASA groups for analysis, High-risk group (ASA 3+4) patients had significantly higher PE/DVT rates than Low-risk groups (ASA 1+2) (9.8% vs. 1.3%, p=0.0459). No other complications differed significantly, though anaemia occurred most frequently in both high-risk and low-risk ASA groups.
Long-term issues (>6 weeks) were dominated by chronic hip pain (5.0%). The table also includes ones from the early stage developed into chronic. There was one PPF (0.8%) at 8 months, post-fall. All radiographs at follow up demonstrated appropriate component positioning. There were no cases of cup migration, subsidence, or aseptic loosening during the follow-up period. The dual mobility articulation showed no signs of polyethene wear, dissociation, or intra-prosthetic dislocation.
Long-term complications occurred in both cemented (n=93) and uncemented (n=24) cohorts, with no statistically significant differences detected (all p>0.05, Fisher’s exact test). Cemented procedures demonstrated numerically higher rates of chronic hip pain (5.4% vs. 4.2%), trochanteric bursitis (2.2% vs. 0%), and leg length discrepancy (2.2% vs. 0%). Uncemented procedures reported no cases of sciatic nerve injury, deep infection, heterotopic ossification, or PPF, though event rates were low overall.
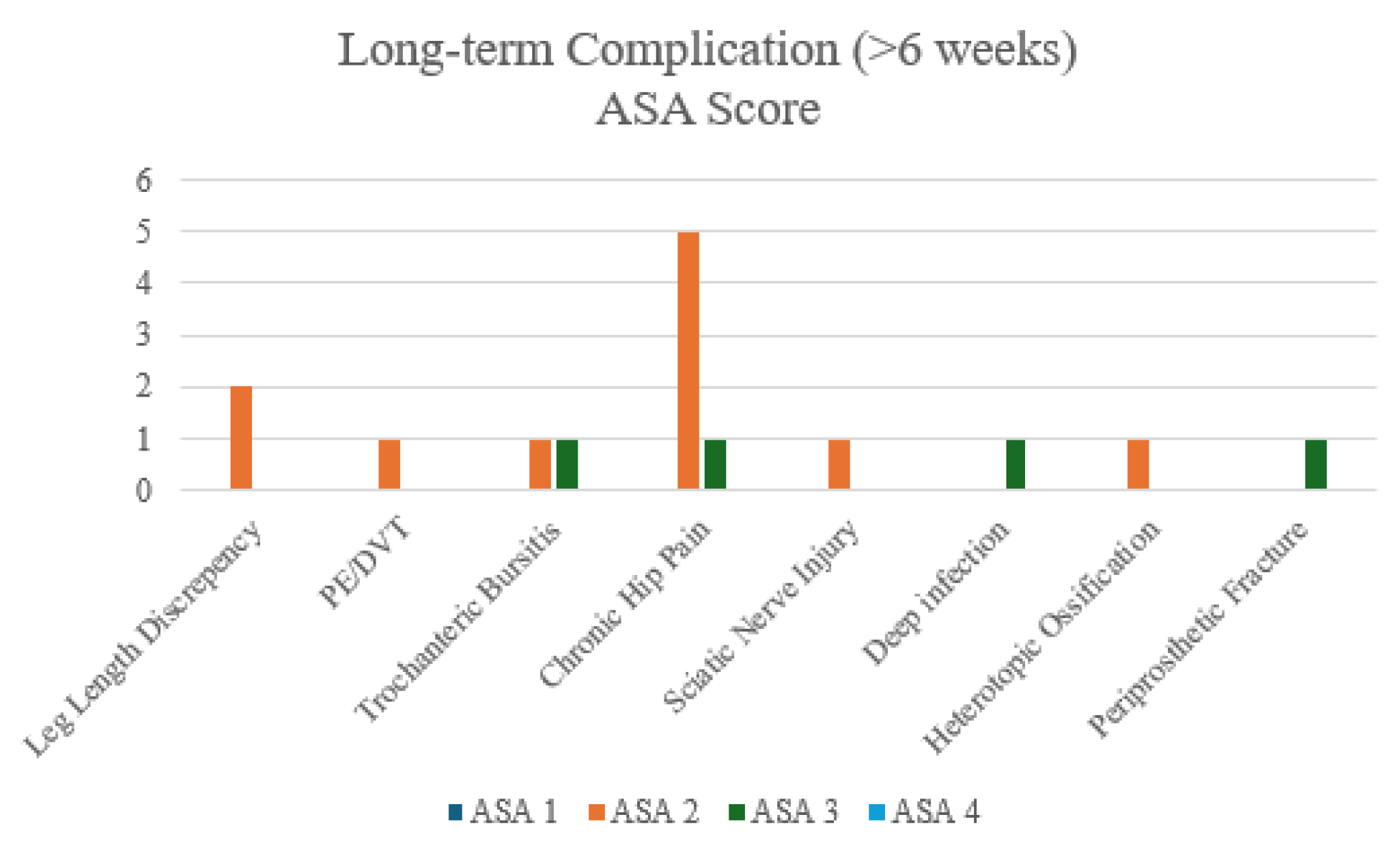
After merging ASA groups, no complications differed significantly. Though chronic hip pain shown to be the most prominent long-term complications after DM-THA
Figure 5.
Bar Chart of Long-term Complications - Overall.
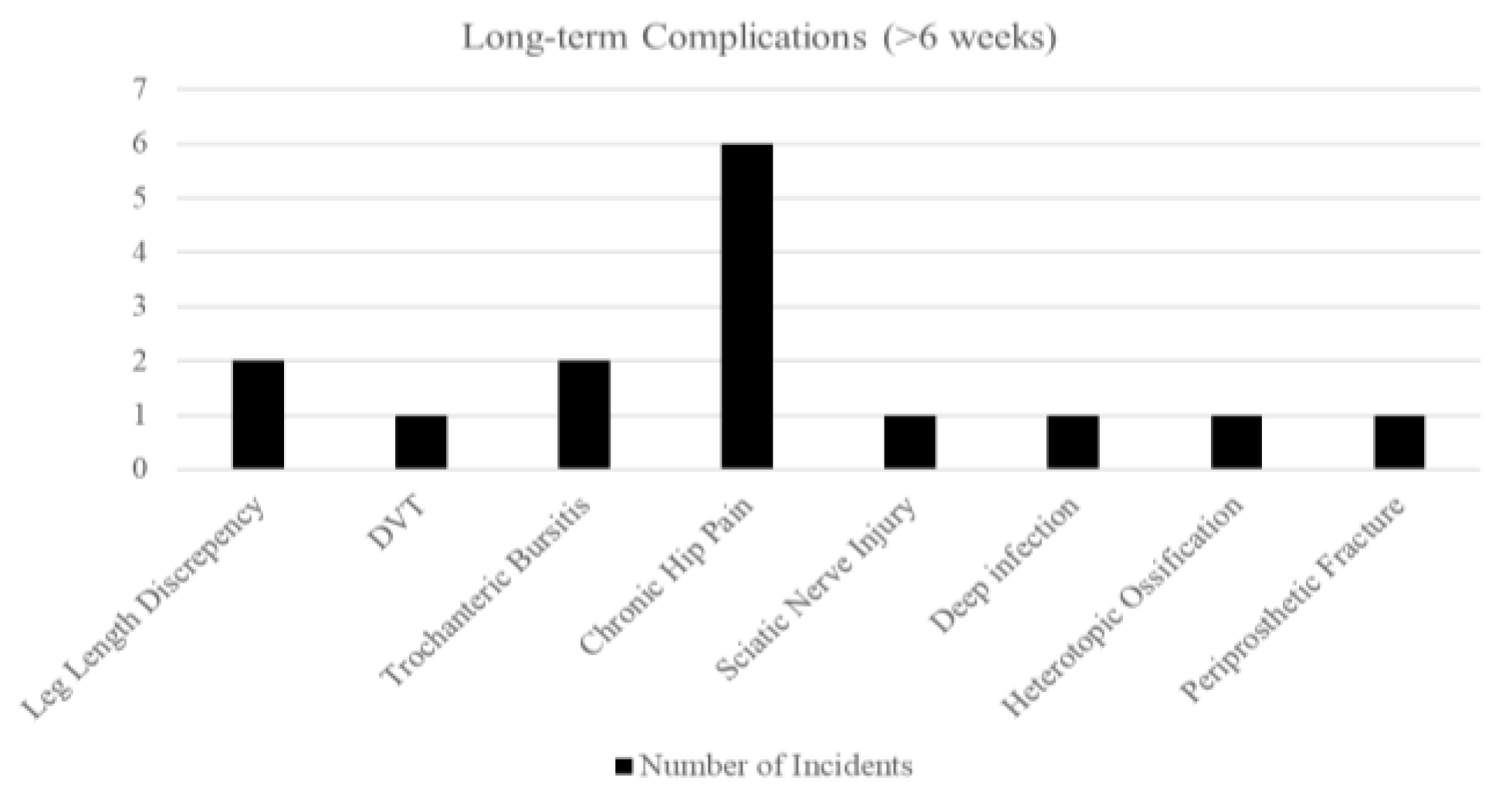
Figure 6.
Bar Chart of Long-term Complications - by Cement Types.
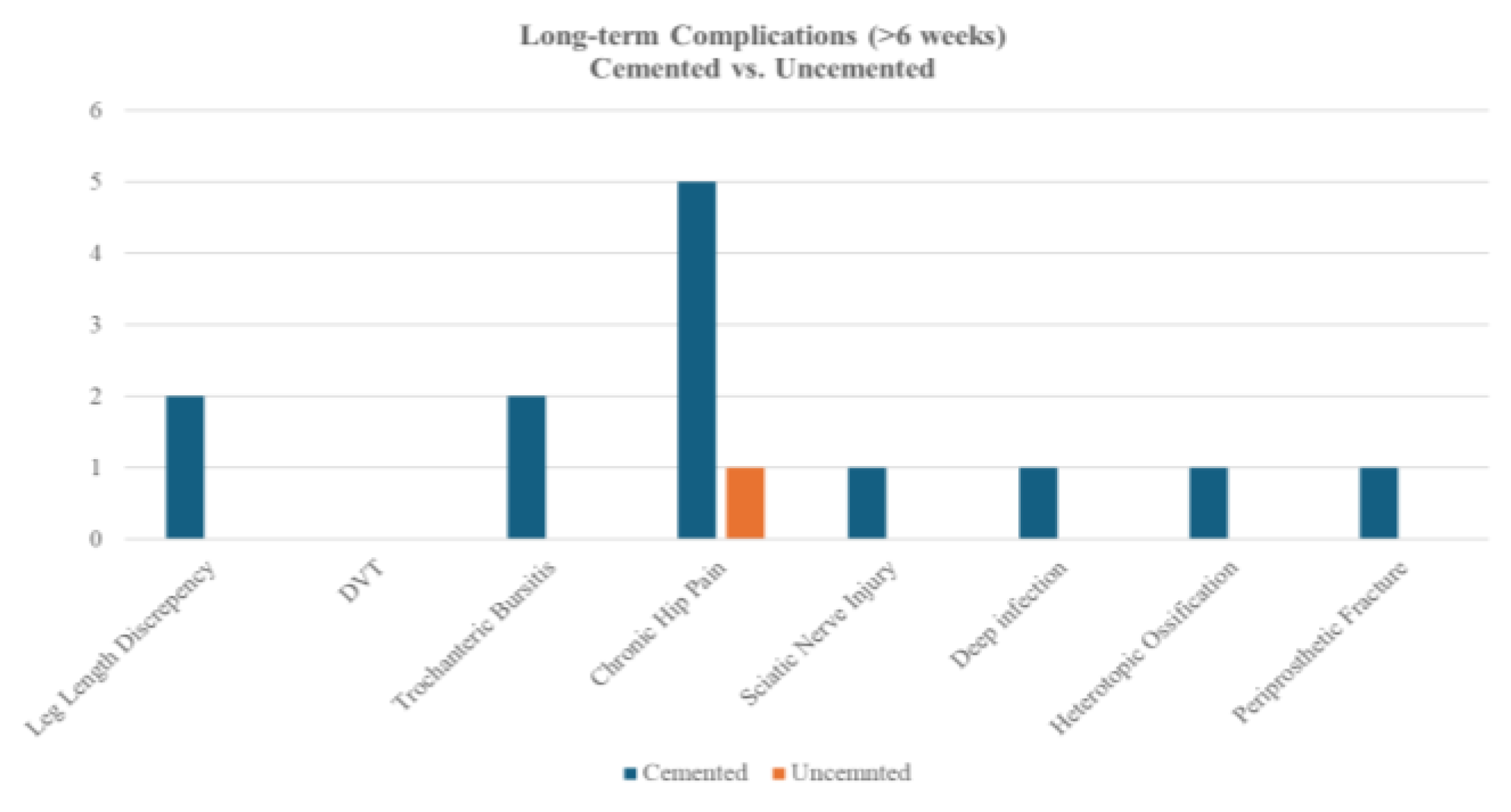
Figure 7.
Bar Chart of Long-term Complications - by ASA groups.
Benchmarking against national outcomes
Thirty-day mortality in the study cohort was 0.8% (1/120), compared to 6.0% (4,314/71,901) in the UK National Hip Fracture Database (NHFD 2024. A two-sample Z-test for proportions demonstrated a statistically significant difference between the two groups (p=0.017).
Table 8.
Comparison if adjusted thirty-days mortality rate.
| Adjusted 30-day Mortality Rate | This study | NHFD 2024 |
|---|---|---|
| Count | 1 | 4314 |
| % | 0.8 | 6.0 |
4. Discussion
Principle Findings
This study demonstrates that the third-generation Zimmer Biomet G7® dual mobility (DM) system provides excellent early outcomes in patients undergoing total hip arthroplasty (THA) for femoral neck fractures (FNF).
Intra-prosthetic Dislocation
The most prominent finding with the dual mobility THA in FNF patients was the 0% dislocation rate, an outcome that emphasises the enhanced stability offered by the dual mobility design. Radiographic evaluations confirmed satisfactory implant positioning with no evidence of loosening, migration, or intra-prosthetic dislocation, further supporting the mechanical reliability of the G7® DM system in this high-risk trauma population. In a high-risk population, traditionally prone to instability (dislocation rates of 4-10% are commonly cited for standard THA after FNF, with some series reporting rates as high as 22% [10,11]), achieving zero dislocations is noteworthy. Even the large HEALTH trial (NEJM 2019) found a 4.7% dislocation rate in the THA group (versus 2.4% for hemiarthroplasty) despite the strict inclusion of healthier patients [12].
This finding aligns with a growing body of evidence that dual mobility implants dramatically reduce dislocation risk compared to conventional designs [11,13,14]. The dual articulation and enlarged effective head size (“head-neck ratio”) of the DM design increase the jump distance required for the head to dislocate [11], thereby resisting prosthetic dislocation even under extremes of motion and/or less-than-ideal positioning. A comparative series by Zagorov et al. found no dislocations with primary dual mobility THA in femoral neck fracture patients, versus an 11.1% dislocation rate in those with a standard cup [15]. Large registry data support this stability benefit, reporting a 60% reduction in dislocation risk with dual mobility relative to fixed-bearing implants [16]. Similarly, a 2021 meta-analysis by Mufarrih et al [17] noted an average dislocation rate of only 1.87% with DM-THA for fractures, significantly lower than previously reported rates with single-bearing cups.
The surgical approach may have contributed: a posterior approach if used, demands meticulous soft tissue repair to mitigate its higher baseline instability risk (3-8% dislocation with the posterior approach [11] vs 0.5-0.6% with lateral approach [18]). A recent UK multicentre study of THA for fractures (n=295) reported a 0% dislocation rate with DM components vs 5.7% with conventional cups when using a posterior approach [10]. That study found DM cups lowered dislocation risk by more than 4-fold without increasing other complications. In our institution, posterior approach is primarily employed which is known to cut dislocation rates to ~1% [11]. Notably, no trade-off in function was evident - as discussed below - suggesting that any approach-related limp was minimal.
Moreover, DM may enable a more liberal rehabilitation (with immediate full weight-bearing and fewer motion restrictions), converting into better early stability through restored muscle tone and patient confidence in the new hip. Even typically high-risk patients (e.g. those with cognitive impairment or poor compliance) seem to benefit from the forgiving nature of dual mobility bearings - prior studies have reported zero dislocations in dementia patients managed with DM-THA for hip fractures [19].
Our findings reinforce that the DM designs, combined with an optimised surgical approach and technique, can eliminate early dislocations in the frail population, a major improvement in safety and a reduction in one of the most feared complications of hip arthroplasty.
Oxford Hip Score (OHS)
Beyond stability, functional recovery in this cohort has been excellent, as evidenced by a mean Oxford Hip OHS of 41.0 ± 8.3 and 68.8% of patients achieving excellent outcomes (OHS ≥ 40) at 1-year follow-up. This corresponds to patients experiencing only mild residual symptoms in daily life - an outcome on a par with, if not exceeding, typical post-THA recovery for osteoarthritis patients [20]. For context, registry data indicate that the average OHS about 3 months after elective primary THA is ~34 points, improving to ~40 by one year [20]. Verhaegen et al. found that hip fracture patients treated with THA by arthroplasty specialists achieved a mean OHS of ~43 at final follow-up, statistically equivalent to the outcomes of matched THA patients treated for elective osteoarthritis [21]. In their study the dislocation rate was 1.7% (with no dual mobility used), suggesting that when arthroplasty is performed under optimal conditions, fracture patients can attain functional scores on par with elective cases. Our OHS results, while slightly lower, remain within the “excellent” range and underscore the benefits of total hip arthroplasty in restoring function for displaced neck fractures.
Achieving an OHS in the 40s so early after surgery suggests that these hip fracture patients rapidly regained mobility and quality of life comparable to elective-surgery patients. Such robust patient-reported outcomes likely stem from multiple factors.
First, DM implants do not appear to compromise the range of motion or hip function; by design, they allow a large jump distance and arc of motion before impingement [22]. The greater range of safe motion and intrinsic stability may allow patients to move without fear, facilitating more aggressive rehabilitation and return to activities. In our study, patients were mobilised as early as the first postoperative day under the supervision of physiotherapists, utilising the DM cup’s freedom of movement to encourage early functional use of the limb. This is consistent with reports that DM-THA can confer superior range-of-motion and functional scores versus conventional THA in elderly fracture patients [11]. Agarwala et al., for example, demonstrated significantly higher Harris hip scores and the ability to perform high-flexion activities (such as squatting or sitting cross-legged) in a dual mobility group compared to a standard THR group [11]. Mechanistically, the large effective head of a dual mobility implant delays impingement and permits a wider arc of motion before instability, which not only prevents dislocation but also enables patients to resume routine movements (like bending to dress or cutting toenails) with greater ease.
Secondly, the surgical approach and soft tissue handling influence functional recovery. If a lateral approach was utilised, one might expect some abductor insufficiency. In our study, a posterior approach was primarily used, which generally has less impact on the hip abductors. This is confirmed by our high OHS, which suggests that any limp or muscle weakness was minimal and transient. Indeed, dual mobility technology has been cited as an enabler for surgeons to use familiar approaches (like posterior) in fracture patients without incurring the usual penalty of higher dislocation rates [23].
In summary, the combination of implant stability and tailored surgical technique in our study allowed patients to achieve rapid and meaningful functional restoration after what is often a life-altering injury. Our findings suggest that leveraging a dual mobility construct to minimise instability, we achieved both the low re-operation benefits of THA and excellent patient-reported function (mean OHS ~41) in an elderly fracture cohort.
Peri-prosthetic Fractures (PPF)
The rate of Peri-prosthetic Fracture (PPF) in total was 1.7% and early postoperative (first 90 days) PPF was 0.8%, which is in line with or lower than rates reported elsewhere. Large registry-based studies on primary THA note that early postoperative PPF occurs in 1-2% of cases [24].
Intraoperative or early postoperative femoral fractures are a known hazard in osteoporotic bone, particularly if uncemented stems or forceful impaction techniques are used [24]. For example, a recent single-centre report (6,788 THAs) documented a 1.9% incidence of PPF within 90 days, with significantly more fractures occurring when using a cementless “compaction” technique as opposed to broaching (2.3% vs 1.3%) [24]. Our low fracture rate possibly reflects careful surgical technique and appropriate implant choice for this vulnerable population; most patients in our study received cemented femoral implants. In the context of hip fracture, adherence to cemented fixation has been emphasised to reduce PPF risk in osteoporotic bone [25]. Cementing the stem improves implant fit in poor-quality bone and has been shown to reduce PPF risks relative to press-fit designs, though with an acceptable trade-off of a small risk of cementation syndrome. However, the absence of stem-type association in our study (both PPFs occurred in cemented stems) challenges fracture theories, instead, implicating bone quality and fall dynamics as primary determinants.
It is also noteworthy that dual mobility cups themselves have not been associated with any increase in PPF risk. In a UK multicentre study, the PPF rate was ~2% overall and did not differ between the dual mobility and conventional bearing cohorts [10]. Likewise, our 0.8% PPF in the functional cohort, incidence suggests that adopting the dual mobility system combined with CPT the stem did not introduce new fracture complications compared to historical controls. However, it also underscores that while rare, vigilance is required to prevent and address this complication.
The incidences of other surgical complications were low (2.5% superficial infection and 0.83% deep infection). There was also no deep infection in the 30-day postoperative window - an indication of stringent antiseptic protocols and appropriate antibiotic prophylaxis. Other complication rates in our series were low, and importantly we recorded no intra-prosthetic dissociations of the dual mobility liner - a rare complication unique to these implants (typically <1% in literatures [25]). All radiographs (postoperative and at 1-year follow-up) demonstrated appropriate component positioning and no radiographic loosening (AP/lateral views) of the implant. These findings further indicate the robustness of the surgical and institutional protocols.
In summary, the low surgical complication profile observed suggests that a DM-THA can be introduced into the hip fracture pathway without incurring excessive early risks if surgeons adhere to geriatric-specific surgical principles and the hospital system supports the patient’s perioperative needs.
Early Complications
The early medical complications were a noteworthy concern. Postoperative anaemia occurred in 6.6% of cases, reflecting perioperative blood loss and the limited physiological reserve in this frail, elderly fracture population. Although this rate is comparatively modest, given that transfusion rates up to 22.2% have been reported after hip arthroplasty in some centres [26], precautions are needed for the optimisation of management. Interestingly, there was no significant difference between low-risk and high-risk ASA groups, contradicting the mainstream findings of high ASA class (III/IV) being identified as an independent predictor of postoperative transfusion and medical complications in arthroplasty cohorts [27]. However, the relatively high incidence rate still underscores the importance of vigilant perioperative blood conservation, consideration of preoperative optimisation (e.g. treating pre-existing anaemia) and timely transfusion for high-risk patients whenever feasible.
Venous thromboembolism (VTE) was another significant early complication, with an incidence of 4.2% in our cohort. Encouragingly, no fatal pulmonary embolism (PE) occurred. Cases of deep vein thrombosis (DVT) and PE were concentrated in the ASA III/IV cohort. This observation aligns with reports in the arthroplasty literature that patients with higher ASA scores - indicative of greater comorbidity burden - have elevated risks of VTE after total hip or knee replacement [28]. In the context of femoral neck fractures, several factors compound the thromboembolic risk: advanced age, acute trauma, immobilisation before surgery, and medical comorbidities (e.g. cardiac failure, malignancy, or coagulation disorders common in ASA III/IV). Our VTE rate is slightly higher than those reported in elective primary THA series with rigorous prophylaxis, which is understandable given the acute fracture setting. It highlights the need for aggressive thromboprophylaxis (such as early chemical prophylaxis and mechanical compression) and early postoperative mobilisation in this vulnerable group. Therefore, identifying ASA III/IV patients as elevated risk allows clinicians to tailor prophylactic strategies and monitoring (including extended prophylaxis post-discharge) to mitigate VTE incidence.
Long-term Complication
At one-year follow-up, 5.0% of the cohort reported chronic hip pain, which dominated the long-term issues. This aligns with and is much lower than some reports from large cohorts (e.g. a Danish registry study noted at least 12.1% of patients with significant chronic hip pain [29]). Although not significant, ASA I/II patients reported more persistent hip pain, compared to ASA III/IV patients following G7® dual mobility THA for femoral neck fracture. This contradicts the theory of greater comorbidity burdens has worse pain outcomes [30]. These findings have important implications for rehabilitation strategies: patients may benefit from tailored postoperative care, with enhanced multimodal analgesia, vigilant monitoring, and specialised physiotherapy input to mitigate chronic pain and optimise functional recovery [31].
Mortality Rate and Benchmarking
Our study’s 30-day mortality of 0.8% is significantly low when benchmarked against The UK National Hip Fracture Database (NHFD). The UK NHFD reports a risk-adjusted 30-day mortality of approximately 6% for hip fracture patients [32]. Historically, hip fracture carries high early mortality; other cohorts have documented roughly 5-13% mortality by 30 days in this population [33,34]. This is especially encouraging given that THA in fractures is a more extensive procedure than hemiarthroplasty; our results indicate that with proper patient selection and optimised care, the broader surgery (THA with a DM cup) can be safely tolerated even by elderly, frail patients. We also acknowledge that patient selection might play a role - candidates for THA (as opposed to hemiarthroplasty) are often the fitter hip fracture patients (good cognition, ambulatory baseline), which could inherently confer a survival advantage.
Against this background, the 0.8% thirty-day mortality in our series potentially implies that our protocol successfully mitigated the usual drivers of hip fracture mortality - namely perioperative medical complications like cardiac events, venous thromboembolism, and infections [34]. Several institutional practices likely contributed to improved survival. We employ a coordinated multidisciplinary perioperative pathway, consisting of orthopaedic surgeons, geriatricians, anaesthetists, physiotherapists, and nursing staff who collaborate from admission through discharge. This orthogeriatric co-management model has demonstrated improvements in survival and early outcomes in many studies [35]. In our study, nearly all patients received their THA within a day of presentation, often after preoperative optimisation by the geriatric team (addressing anaemia, hydration, heart failure, etc.). Additionally, modern anaesthesia and enhanced recovery protocols (including regional nerve blocks, judicious fluid management, and early mobilisation on Day 1 post-op) have likely contributed to the survival benefit.
Reassuringly, the use of a DM implant itself does not appear to adversely affect mortality; prior studies have found no significant difference in early or medium-term mortality between DM versus standard implants in fracture patients [10]. Thus, our outcomes suggest that a DM-THA can be safely adopted in this high-risk group without incurring the higher early mortality commonly associated with hip fractures when system-level best practices are in place, including multidisciplinary care and fast-track management.
Health Economics
Finally, it is worth considering the broader implications and cost of using DM-THA for hip fractures. Dual mobility implants are more expensive upfront than standard THA bearings or hemiarthroplasty; however, our results indicate a potential cost offset through complication avoidance. A single dislocation event in an elderly patient can incur significant costs - hospital readmission, revision surgery, rehabilitation, and the morbidity of prolonged immobility. By achieving a zero-dislocation rate, our series likely avoided several such costly events. Health-economic analyses from other centres support this trade-off: for example, a Markov modelling based on a large registry found that routine use of dual mobility in primary THA would save roughly €28 million per 100,000 cases by preventing dislocations and their downstream costs [16]. Barlow et al. similarly reported that a dual mobility implant could remain cost-effective even if its price were up to $1000 more than a conventional implant, given the expense of treating dislocation and revision is so high [36]. Additionally, implant longevity must be considered when interpreting early success: dual mobility cups have evolved to address earlier problems (like polyethene wear or intra-prosthetic dislocation seen in first-generation designs). Modern highly cross-linked polyethene, improved locking mechanisms, and refined implant geometry have greatly lowered the risk of intra-prosthetic dislocation and wear-related failures in contemporary DM systems [11]. This bodes well for the cost-effectiveness of DM-THA in the long run, as implant survivorship appears excellent -for instance, Neri et al. reported 25-year survivorship with no dislocations using a dual mobility construct [37]. Thus, when considering system-level outcomes, the dual mobility THA strategy in FNF patients seems to offer a superior early outcome (stability and function) which likely reduces downstream healthcare utilisation, and any initial cost premium of the implant is justified by the reduction in complication-related expenditures. Our early results suggest that, in the setting of a comprehensive care model, dual mobility THA not only yields outstanding clinical outcomes for femoral neck fracture patients but also may be a prudent choice from a health economics perspective, benefiting both patients and the healthcare system.
Strength of the Study
Standardised Implant Selection: A key strength is the uniform use of the Zimmer Biomet G7® dual mobility acetabular system for all patients. This standardisation eliminates inter-prosthetic variability and ensures that outcome differences are not confounded by differing implant designs. By focusing on a single, modern dual mobility (DM) implant throughout the cohort, our study avoids the heterogeneity seen in prior series that combined various implant types, thereby improving the internal validity of the comparisons. Unlike some previous reports limited by mixed implant methodologies or small sample sizes (e.g., Alberio et al [38]) our consistent implant strategy strengthens the interpretability of our results in attributing outcomes directly to the G7® system.
Consistent Surgical Technique and Expertise: All procedures were performed by experienced arthroplasty surgeons following a uniform surgical approach and standardised technique. This high level of surgical consistency minimises technical variability across cases, thereby enhancing the reliability of outcome assessment. Notably, high surgeon volume and experience are known to correlate with lower complication rates -for example, surgeons performing fewer than ~35 hip arthroplasties per year face higher dislocation and revision risks [39]. In our study, operations were conducted at a high-volume arthroplasty centre by surgeons likely above this volume threshold, which is conducive to optimising patient outcomes. The consistent use of the same approach, fixation method, and post-operative protocols across all patients further reduces confounders that could bias the early outcome evaluation.
Multidisciplinary Perioperative Care Protocols: We implemented a comprehensive multidisciplinary care pathway for femoral neck fracture patients undergoing THA, involving close collaboration between orthopaedic surgeons, geriatric medicine, anaesthesiology, nursing, and rehabilitation services. This standardised “shared care” protocol ensured timely surgery, optimised medical management, and coordinated rehabilitation for all patients. Such an approach is supported by literature showing that coordinated co-management programs (e.g. “Code Hip”) significantly improve perioperative metrics and patient outcomes in hip fracture care [40]. Indeed, multidisciplinary protocols have been associated with faster time-to-surgery, improved early mobilisation, reduced complication rates, and even lower mortality in geriatric hip fracture populations [41]. The use of these protocols in our study likely contributed to more uniform and improved early recovery, thereby enhancing the generalisability of our findings to real-world clinical practice where similar protocols are increasingly advocated.
Comprehensive Outcome Assessment: The study’s evaluation framework was broad in scope, capturing clinical, radiographic, and functional outcomes for a holistic assessment of the dual mobility THA’s performance. Clinically, we monitored not only dislocation and revision rates but also other complications (e.g. Peri-prosthetic Fractures, infections) and patient survival, providing a thorough safety profile. Radiographically, all patients underwent scheduled postoperative imaging to assess component positioning, osseointegration signs, and the presence of radiolucent lines or heterotopic ossification, based on standardised criteria. This allowed us to confirm robust implant fixation and identify any early hardware issues (none of which were significant in our series, as no cases of component loosening were detected and osseointegration signs were high at 1 year). The inclusion of validated functional indices -alongside objective measures -is a considerable strength, as it gauges the quality of recovery from the patient’s perspective. Many large-scale investigations into DM-THA focus predominantly on hard endpoints like dislocation or revision [42], often lacking granular data on postoperative function or radiographic healing. Furthermore, even when functional outcomes are assessed in the literature, the evidence has often been of at longer follow-ups (e.g., Santiago et al [43]). By capturing high-quality functional outcome data out to the early follow-up interval and combining it with clinical and radiographic analyses, our study offers a richly detailed picture of how the G7® dual mobility system performs in practice. This comprehensive approach provides confidence that improvements (or issues) were not missed and that our conclusions about the efficacy of the implant are well-rounded and patient centred.
Collectively, these strengths underscore the methodological robustness of our study and distinguish it from earlier investigations that often-had narrower scopes or less controlled designs. Our use of a homogenous implant and surgical approach, within a multidisciplinary care framework, and diligent follow-up with multi-faceted outcome collection, enhances the internal validity and reliability of the findings. In addition, by aligning our outcome measures with common clinical benchmarks (NHFD), we ensure that our results are directly comparable to real-world data and existing literature. This alignment with real-world benchmarks means that the early outcomes reported here for the G7® dual mobility THA can serve as a meaningful point of reference for both clinicians and researchers. In summary, the study’s rigorous design and execution strengthen the credibility of the conclusions and provide a high-quality evidence base regarding the use of dual mobility THA in femoral neck fracture patients. The comprehensive and standardised approach we adopted can inform future research and support the generalisability of our findings to broader clinical practice.
Limitation of the Study
Single-centre design: This study was conducted at a single institution, which inherently limits the external validity of the findings. Results from one centre may not fully generalize to other hospitals or populations, as differences in patient demographics, surgical techniques, and perioperative protocols across institutions could lead to different outcomes. Therefore, caution is needed when extrapolating our results to broader settings.
Short-to-mid-term follow-up: Our follow-up was restricted to the short-to-mid-term, so long-term outcomes remain unknown. This limited follow-up means we could not assess the durability of the G7® dual mobility implant or detect complications that might manifest only in the longer term. The lack of long-term data introduces uncertainty about the sustained benefits of the implant and the possibility of delayed adverse events or failures that could emerge over time. Consequently, any conclusions about implant longevity or late complication rates should be viewed as preliminary.
Limited sample size in subgroups: While the overall sample size provides insight into early outcomes, the number of patients in certain subgroups was small. Only a few patients in our cohort received uncemented femoral stems, which limits the power to analyse outcomes for that subgroup. Such small subgroup numbers can undermine statistical power, increase the risk of type II error (missing a true effect) and warrant caution in interpreting any apparent lack of differences. As a result, findings related to these sub-cohorts (e.g. the performance of uncemented stems) should be considered exploratory rather than definitive.
Lack of blinding: The study did not employ blinding of patients, surgeons, or outcome assessors, which introduces potential bias. Knowledge of the implant type by the care team and patients could have influenced postoperative management or subjective outcome reporting (performance and response bias). Similarly, outcome assessors aware of the treatment may have unconscious expectations that skew the evaluation of results. Because no blinding was in place, there is an inherent risk that positive outcomes may have been overestimated or certain negative outcomes under-recognised, so the results must be interpreted with appropriate caution.
Potential confounding from patient selection: Finally, as an observational (non-randomised) study, our findings are subject to possible selection and confounding bias. Patients were not randomly assigned to treatment; instead, the inclusion relied on clinical decisions and eligibility criteria, which may have favoured enrolling relatively healthier or more active patients for THA. If those selected patients had inherently better prognoses, it could confound the association between the dual mobility implant and the outcomes observed. In other words, differences in baseline characteristics or unmeasured variables might partly explain the favourable early outcomes. We attempted to control for known factors, but residual confounding may remain due to the study design. This limitation means that one should be cautious in ascribing all observed benefits solely to the implant, as some effects could stem from the patient population selected.
Future Directions
Long-Term Outcomes: Extended follow-up studies are needed to determine the durability of the G7® dual mobility construct. The current evidence is limited to short-term results, so the sustained benefits of dual mobility (e.g. continued low dislocation rates) and any late complications (such as polyethene wear or PPF) remain uncertain. Long-term surveillance (5-10 years and beyond) will clarify implant survivorship and safety, ensuring that early advantages persist over timepubmed.ncbi.nlm.nih.gov. Such data are especially critical given the high life expectancy variance in this patient population and the need to anticipate revision rates in older adults.
Randomised Trials and Comparative Studies: High-quality comparative research is crucial to validate the benefits of dual mobility THA in hip fractures. A sufficiently powered RCT with dislocation as the primary endpoint would definitively quantify the reduction in instability afforded by dual mobility components versus standard THA or hemiarthroplasty. Additionally, comparative trials should evaluate functional recovery, complication rates, and mortality, to ensure that the stability gains do not come at the expense of other outcomes (noting that some meta-analyses have found worse short-term outcomes [43]). Rigorous head-to-head evidence will guide surgeons in choosing the optimal arthroplasty approach for displaced femoral neck fractures.
Optimal Implant Fixation Strategies: Investigations are needed to identify the best fixation and surgical techniques for dual mobility THA in fracture patients. Elderly fracture populations often have poor bone quality, raising questions about cemented versus uncemented fixation for both acetabular cups and femoral stems. Our data contradicted early data and suggested no significant differences in outcomes (such as dislocations, early complications and PPF) between cemented and uncemented stem fixation. Future research should explore how these findings translate to dual mobility systems.
Health Economic Evaluation: The cost-effectiveness of adopting dual mobility THA for hip fractures must be rigorously assessed. Dual mobility implants are typically more expensive upfront, but they may avert downstream costs by preventing dislocations and reoperations. A recent modelling study suggests that using dual mobility in displaced neck fractures can be cost-effective in patients under 80, provided the dislocation risk is substantially reduced [44]. However, these analyses rely on assumptions that need validation in real-world settings. Future research should incorporate health economic evaluations alongside clinical trials - measuring quality-adjusted life years (QALYs), implant costs, complication costs, and overall healthcare utilisation. Particularly, if dual mobility THA indeed lowers revision or institutional care needs (due to fewer complications), it could offer long-term cost savings despite higher implant costs. Confirming this through prospective economic studies or registry data will be important for policymakers and hospital systems. Ultimately, demonstrating value for money will facilitate wider adoption if the clinical benefits are borne out.
5. Conclusions
The early experience with the G7® Zimmer Biomet Dual Mobility Total Hip Arthroplasty (DM-THA) for Femoral Neck Fractures (FNFs) at our centre has been extremely positive. Zero dislocations, 30-day mortality far below national averages (0.8%), excellent patient-reported function comparable to elective THA results (mean Oxford Hip Score of 41), and a low complication rate; these findings reinforce the growing consensus that DM-THA is an optimal strategy for displaced FNF in elderly or high-risk patients, offering the advantages of a total hip replacement (improved mobility) while minimising the historically high risk of instability. The results likely reflect a collaboration between advanced implant technology (dual mobility’s intrinsic stability), surgical technique (appropriate approach and meticulous tissue handling), patient physiology (relatively fit patients optimized for surgery), and system-level supports (geriatric co-management).
Our results, together with evidence from high-quality studies suggest that G7®’s dual mobility addresses the chief vulnerabilities of FNF patients - instability and immobility - without exaggerating the operative risk. Future follow-up will determine if these early gains are sustained long-term, but our early data strongly support the adoption of DM designs in the FNF population to optimise stability, function, and overall recovery. The present interpretation emphasises that clinical and system innovations -from implant design to care pathways - together contribute to superior outcomes, offering a blueprint for improving the care of vulnerable hip fracture patients in a high-impact, real-world setting.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Funding
This research received no external funding.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Acknowledgments
We thank Mr. James Zhangly (University of Leeds) for their expert assistance with Python statistical analysis.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| FNF | Femoral Neck Fracture |
| THA | Total Hip Arthroplasty |
| DM | Dual Mobility |
| PPF | Peri-prosthetic Fracture |
| DM-THA | Dual Mobility Total Hip Arthroplasty |
| OHS | Oxford Hip Score |
| NHFD | National Hip Fracture Database |
| AP | Anterior-Posterior |
| DVT | Deep Vein Thrombosis |
| VTE | Venous Thromboembolism |
| PE | Pulmonary Embolism |
| QALY | Quality-Adjusted Life Years |
| AKI | Acute Kidney Injury |
| LRTI | Lower Respiratory Tract Infection |
| AF | Atrial Fibrillation |
Appendix A
Appendix A - CONSORT-style flow diagram
References
- Kunutsor, S. K.; et al. Risk factors for dislocation after primary total hip replacement: a systematic review and meta-analysis of 125 studies involving approximately five million hip replacements. The Lancet Rheumatology 2019, 1, e111–e121. [Google Scholar] [CrossRef] [PubMed]
- Guo, L.; et al. Risk factors for dislocation after revision total hip arthroplasty: A systematic review and meta-analysis. International Journal of Surgery 2017, 38, 123–129. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, A.; Batailler, C.; Fary, C.; Servien, E.; Lustig, S. Dual Mobility Cups in Revision Total Hip Arthroplasty: Efficient Strategy to Decrease Dislocation Risk. The Journal of Arthroplasty 2020, 35, 500–507. [Google Scholar] [CrossRef] [PubMed]
- Pai, F.-Y.; et al. Risk factors and modes of failure in the modern dual mobility implant. A systematic review and meta-analysis. BMC Musculoskelet Disord 2021, 22, 541. [Google Scholar] [CrossRef] [PubMed]
- Diallo, M.; et al. Dual mobility total hip replacement: a 15-year experience in Burkina Faso. Pan Afr Med J 2022, 41. [Google Scholar] [CrossRef] [PubMed]
- Sappey-Marinier, E.; Viste, A.; Blangero, Y.; Desmarchelier, R.; Fessy, M.-H. A comparative study about the incidence of dislocation and peri-prosthetic fracture between dual mobility versus standard cups after primary total hip arthroplasty. International Orthopaedics (SICOT) 2019, 43, 2691–2695. [Google Scholar] [CrossRef] [PubMed]
- Deng, Y.; et al. Risk factors for periprosthetic femoral fractures around total hip arthroplasty: a systematic review and meta-analysis. ANZ Journal of Surgery 2020, 90, 441–447. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.-W.; Kim, W.-Y.; Song, J.-H.; Kim, J.-H.; Lee, H.-H. Factors Affecting Periprosthetic Bone Loss after Hip Arthroplasty. Hip & Pelvis 2021, 33, 53–61. [Google Scholar] [CrossRef] [PubMed]
- Lygrisse, K. A.; et al. Femoral Neck Notching in Dual Mobility Implants: Is This a Reason for Concern? The Journal of Arthroplasty 2021, 36, 2843–2849. [Google Scholar] [CrossRef] [PubMed]
- Hoggett, L.; et al. Post-operative complications following total hip arthroplasty for trauma: A multicentre cohort study comparing dual mobility with conventional acetabular bearings. Journal of Orthopaedics 2023, 40, 34–37. [Google Scholar] [CrossRef] [PubMed]
- Agarwala, S.; Katariya, A.; Vijayvargiya, M.; Shetty, V.; Swami, P. M. Superior functional outcome with dual mobility THR as compared to conventional THR in fracture neck femur: a prospective cohort study. SICOT-J 2021, 7, 42. [Google Scholar] [CrossRef] [PubMed]
- The HEALTH Investigators. Total Hip Arthroplasty or Hemiarthroplasty for Hip Fracture. N Engl J Med 2019, 381, 2199–2208. [Google Scholar] [CrossRef] [PubMed]
- Assi, C.; et al. Outcomes of total hip arthroplasty using dual mobility cups following failed internal fixation of proximal femoral fractures at a mean follow-up of 6 years. SICOT-J 2024, 10, 3. [Google Scholar] [CrossRef] [PubMed]
- You, D.; et al. Outcomes of total hip arthroplasty using dual mobility components in patients with a femoral neck fracture: a systematic review and meta-analysis. The Bone & Joint Journal 2020, 102-B, 811–821. [Google Scholar]
- Department of Orthopaedics and Traumatology, University Hospital St. Marina, Varna, Bulgaria. et al. DUAL MOBILITY CUPS REDUCE DISLOCATION RATE IN TOTAL HIP ARTHROPLASTY FOR DISPLACED FEMORAL NECK FRACTURES. JofIMAB 2018, 24, 2077–2081. [CrossRef]
- Epinette, J.-A.; Lafuma, A.; Robert, J.; Doz, M. Cost-effectiveness model comparing dual-mobility to fixed-bearing designs for total hip replacement in France. Orthopaedics & Traumatology: Surgery & Research 2016, 102, 143–148. [Google Scholar]
- Mufarrih, S. H.; Qureshi, N. Q.; Masri, B.; Noordin, S. Outcomes of total hip arthroplasty using dual-mobility cups for femoral neck fractures: a systematic review and meta-analysis. HIP International 2021, 31, 12–23. [Google Scholar] [CrossRef] [PubMed]
- Zijlstra, W. P.; De Hartog, B.; Van Steenbergen, L. N.; Scheurs, B. W.; Nelissen, R. G. H. H. Effect of femoral head size and surgical approach on risk of revision for dislocation after total hip arthroplasty: An analysis of 166,231 procedures in the Dutch Arthroplasty Register (LROI). Acta Orthopaedica 2017, 88, 395–401. [Google Scholar] [CrossRef] [PubMed]
- Graversen, A. E.; Jakobsen, S. S.; Kristensen, P. K.; Thillemann, T. M. No dislocations after primary hip arthroplasty with the dual mobility cup in displaced femoral neck fracture in patients with dementia. A one-year follow-up in 20 patients. SICOT-J 2017, 3, 9. [Google Scholar] [CrossRef] [PubMed]
- Galea, V. P.; et al. Patient-acceptable symptom state for the Oxford Hip Score and Forgotten Joint Score at 3 months, 1 year, and 2 years following total hip arthroplasty: a registry-based study of 597 cases. Acta Orthopaedica 2020, 91, 372–377. [Google Scholar] [CrossRef] [PubMed]
- Verhaegen, J.C. F.; et al. Is Outcome of Total Hip Arthroplasty for Hip Fracture Inferior to That of Arthritis in a Contemporary Arthroplasty Practice? The Journal of Arthroplasty 2023, 38, S276–S283. [Google Scholar] [CrossRef] [PubMed]
- Zimmer Biomet. Dual Mobility Total Hip Arthroplasty in Displaced Femoral Neck Fracture. (2022).
- Hailer, N. P.; Weiss, R. J.; Stark, A.; Kärrholm, J. The risk of revision due to dislocation after total hip arthroplasty depends on surgical approach, femoral head size, sex, and primary diagnosis: An analysis of 78,098 operations in the Swedish Hip Arthroplasty Register. Acta Orthopaedica 2012, 83, 442–448. [Google Scholar] [CrossRef] [PubMed]
- Høvik, Ø.; Aamodt, A.; Amlie, E.; Sivertsen, E. A. Increased risk of intraoperative and early postoperative periprosthetic femoral fracture with compaction compared with broaching in cementless THA: a single-center study of 6,788 hips. ActaO 2024, 95. [Google Scholar] [CrossRef] [PubMed]
- Jensen, S. Evaluation of dual-mobility total hip arthroplasty in elderly patients with femoral neck fracture or hip osteoarthritis. (Faculty of Health Sciences Aarhus University, 2019).
- Hart, A.; et al. Blood Transfusion in Primary Total Hip and Knee Arthroplasty. Incidence, Risk Factors, and Thirty-Day Complication Rates. The Journal of Bone and Joint Surgery 2014, 96, 1945–1951. [Google Scholar] [CrossRef] [PubMed]
- Hong, D.-L.; et al. Factors contributing to perioperative blood transfusion during total hip arthroplasty in patients continuing preoperative aspirin treatment: a nomogram prediction model. BMC Musculoskelet Disord 2025, 26, 138. [Google Scholar] [CrossRef] [PubMed]
- McHugh, M.; et al. Aspirin is Not for Everyone: Discharge to Non-home Facilities After Total Hip and Knee Arthroplasty Increases Risk of Venous Thromboembolism. Arthroplasty Today 2024, 27, 101368. [Google Scholar] [CrossRef] [PubMed]
- Nikolajsen, L.; Brandsborg, B.; Lucht, U.; Jensen, T.S.; Kehlet, H. Chronic pain following total hip arthroplasty: a nationwide questionnaire study. Acta Anaesthesiol Scand 2006, 50, 495–500. [Google Scholar] [CrossRef] [PubMed]
- Zhang, B.; et al. Risk factors for pain after total hip arthroplasty: a systematic review. Arthroplasty 2023, 5, 19. [Google Scholar] [CrossRef] [PubMed]
- Van Zundert, T.C.R. V.; Gatt, S. P.; van Zundert, A. A. J. Anesthesia and perioperative pain relief in the frail elderly patient. Saudi J Anaesth 2023, 17, 566–574. [Google Scholar] [CrossRef] [PubMed]
- NHFD Outcomes benchmark summary 2024. (2025).
- NHFD_2023_Annual_Report.
- University of Maryland Medical Center. Mortality in Hip Fracture Patients: Identifying the Prognostic Value of Troponin.
- Gao, F.; et al. Orthogeriatric co-managements lower early mortality in long-lived elderly hip fracture: a post-hoc analysis of a prospective study. BMC Geriatr 2023, 23, 571. [Google Scholar] [CrossRef] [PubMed]
- Barlow, B. T.; McLawhorn, A. S.; Westrich, G. H. The Cost-Effectiveness of Dual Mobility Implants for Primary Total Hip Arthroplasty: A Computer-Based Cost-Utility Model. The Journal of Bone and Joint Surgery 2017, 99, 768–777. [Google Scholar] [CrossRef] [PubMed]
- Neri, T.; Philippot, R.; Farizon, F.; Boyer, B. Results of primary total hip replacement with first generation Bousquet dual mobility socket with more than twenty five years follow up. About a series of two hundred and twelve hips. International Orthopaedics (SICOT) 2017, 41, 557–561. [Google Scholar] [CrossRef] [PubMed]
- Alberio, R. L.; Rusconi, M.; Martinetti, L.; Monzeglio, D.; Grassi, F. A. Total Hip Arthroplasty (THA) for Femoral Neck Fractures: Comparison between Standard and Dual Mobility Implants. Geriatrics 2021, 6, 70. [Google Scholar] [CrossRef] [PubMed]
- Ravi, B.; et al. Relation between surgeon volume and risk of complications after total hip arthroplasty: propensity score matched cohort study. BMJ 2014, 348, g3284. [Google Scholar] [CrossRef] [PubMed]
- VanTienderen, R. J.; et al. Implementation of a Multidisciplinary ‘Code Hip’ Protocol is Associated with Decreased Time to Surgery and Improved Patient Outcomes. Geriatr Orthop Surg Rehabil 2021, 12, 21514593211004904. [Google Scholar] [CrossRef] [PubMed]
- Salvador-Marín, J.; et al. Efficacy of a multidisciplinary care protocol for the treatment of operated hip fracture patients. Sci Rep 2021, 11, 24082. [Google Scholar] [CrossRef] [PubMed]
- Bloemheuvel, E. M.; Van Steenbergen, L. N.; Swierstra, B. A. Low revision rate of dual mobility cups after arthroplasty for acute hip fractures: report of 11,857 hip fractures in the Dutch Arthroplasty Register (2007-2019). Acta Orthop 2021, 92, 36–39. [Google Scholar] [CrossRef] [PubMed]
- Santiago, M. S.; et al. Outcomes of dual mobility versus conventional total hip arthroplasty for patients with femoral neck fractures: a systematic review and meta-analysis including registry data. J Orthop Surg Res 2025, 20, 405. [Google Scholar] [CrossRef] [PubMed]
- Montgomery, S.; et al. Cost-effectiveness of dual-mobility components in patients with displaced femoral neck fractures. The Bone & Joint Journal 2021, 103-B, 1783–1790. [Google Scholar]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



