
Submitted:
10 July 2025
Posted:
11 July 2025
You are already at the latest version
Abstract
Invasive candidiasis (IC) in Latin America is undergoing a significant epidemiological shift, increasingly driven by non-albicans strains such as Candida tropicalis, Candida parapsilosis, and Candidozyma auris. These pathogens often exhibit multidrug resistance, which complicates treatment and increases mortality. Diagnostic limitations, particularly in rural and public hospitals, delay detection and hinder the provision of rapid care. Environmental pressures, such as climate change and the widespread use of azoles in agriculture, appear to favor the selection of resistant and thermotolerant strains. Migratory birds may also play a role in the environmental transmission of pathogenic fungi. These factors are amplified by socioeconomic inequalities that restrict access to diagnostics and first-line antifungals. To address this growing threat, we propose a “One Health” approach that integrates environmental surveillance, antifungal management, equitable access to diagnostics, and coordinated public health strategies. Strengthening these areas is essential to reduce the burden of IC and limit the spread of antifungal resistance in the region.

Keywords:
invasive candidiasis
; antifungal resistance
; climate change
; Candidozyma auris
; Latin America
1. Introduction
Invasive candidiasis (IC) represents a growing threat in hospital settings, particularly in intensive care units (ICUs), where patient susceptibility facilitates the hematogenous spread of Candida spp. (1–3). Traditionally, Candida albicans has been the most frequently identified strains. However, in recent years, significant concern has emerged regarding non-albicans strains, such as Candida tropicalis, Candida parapsilosis, Nakaseomyces glabratus (formerly C. glabrata), and Candidozyma auris, which is a cause for great concern given their multidrug resistance to antifungal agents (1,3). These infections can manifest as candidemia or compromise deep organs such as the peritoneum, bones, or heart (4,5).
Its frequency has increased alarmingly in highly complex clinical settings, with a mortality rate that, in some series, exceeds 40%. It ranks between the fourth and fifth leading causes of healthcare-associated bloodstream infections, with the ICU being the place with the highest incidence of CI worldwide, with a rate of 5.5 to 7 cases per 1,000 admissions (2,6). In Europe, the incidence in the South of the continent was higher than in the North (5.29 vs. 3.77 per 100,000 inhabitants), which could be due to climatic variations, differences in the management of candidemia, and sociodemographic factors (7). In the United States, the rate of candidemia is 7 to 9 per 100,000 inhabitants, being higher in patients with risk factors such as age over 65, total parenteral nutrition (TPN), diabetes mellitus, diagnosis of hematological neoplastic diseases, or a history of recent hospitalization (8–10).
Various factors influence the epidemiology of this mycosis. Geographic region, environmental conditions, access to health services, and demographic characteristics of the population affect both the incidence and distribution of the strains involved, which could favor an increase in cases caused by non-albicans strains (11). In regions such as Asia and Latin America, infections by non-albicans species have a higher prevalence, with a predominance of C. tropicalis, C. auris, and C. parapsilosis, strains that are not only emerging more frequently but also have increasingly complex multi-drug resistance profiles (12,13). On the other hand, although historically most cases in high-income countries (Europe and North America) were attributed to C. albicans, recent data show an increase in infections caused by non-albicans strains, especially N. glabratus (7,13–16). This strain has been linked to elderly patients and sophisticated healthcare settings, suggesting that the transition to a more resistant candidiasis profile is a global phenomenon, not limited to resource-constrained environments (3,10,13).
2. Epidemiology of IC in Latin America
Although the epidemiology of CI in Europe and the United States is well documented, knowledge remains limited in Latin America; however, recent multicenter studies have begun to outline its regional scope. Between 2008 and 2010, a descriptive observational multicenter epidemiological surveillance study was conducted in 20 hospitals in seven Latin American countries, which reported an overall incidence of 1.18 cases per 1,000 hospital admissions (0.23 cases per 1,000 patient-days); the variation between countries was notable, with Argentina having the highest incidence (1.95 per 1,000 admissions) and Chile the lowest (0.33 per 1,000 admissions). Colombia, with data from a single center, recorded 1.96 cases per 1,000 admissions; Venezuela, 1.72 (range 1.04–2.90); Brazil, 1.38 (0.55–2.11); and both Ecuador and Honduras, 0.90 cases per 1,000 admissions (Ecuador: 0.30–1.10; Honduras: 0.88–0.98) (17,18).
Among the countries with the most robust data, Brazil stands out, where candidemia rates in ICUs have ranged from 1.2 to 2.49 cases per 1,000 admissions. In some specific series, alarming figures of up to 42.6 cases per 1,000 ICU admissions have been observed (19). Figure 1 shows the geographical distribution of the main Candida spp. isolated from patients in Latin America, highlighting the clear prevalence of C. albicans and regional variations in non-albicans strains. In terms of distribution by strain, more than 60% of cases correspond to non-albicans strains, with C. parapsilosis accounting for 20.5% and C. tropicalis for 15.3% of isolates, and some studies have reported mortality rates of up to 80% (19–21). Recently, Guinsburg et al. published a systematic review on candidemia in Brazil in 2024 that included 2,305 isolates from blood cultures, with C. albicans being the most frequent strain (37.2%), followed by C. parapsilosis (22.5%) and C. tropicalis (18,1 %) (22).
In Colombia, the incidence in ICUs was reported at 2.3 cases per 1,000 admissions (23). A retrospective descriptive observational cohort study conducted at a high-complexity hospital in Bogotá showed a significant increase in infections caused by non-albicans strains, which rose from 44% to 51% in a short period (24). The distribution of isolates in the country varies depending on the hospital. However, C. tropicalis usually ranks second in frequency, ranging from 17% to 23%, followed by C. parapsilosis, whose percentages range from 13% to 23% (23). A notable finding in Salinas' study (2022) was the increase in the isolation of N. glabratus, a strain typically associated with developed countries. This variation could be attributed to changes in comorbidities and demographic characteristics of the patients evaluated. However, the author does not propose additional hypotheses to explain this unusual behavior (24). In a multicenter observational and retrospective cohort study, C. auris was reported to be the second most isolated strain (26.1%), surpassed only by C. albicans (36.5%). This suggests a significant change in the epidemiological profile. However, the authors emphasize that, in the studied Colombian context, C. auris candidemia does not have a worse prognosis than that caused by other isolates, provided that adequate antifungal management and rigorous control of septic shock are ensured (25).
In Argentina, according to epidemiological estimation studies, the incidence varied between 1.15 and 2.25 cases per 1,000 hospital admissions, with a progressive mortality rate of between 40% and 50%; non-albicans strains predominate, accounting for 59.1% of infections, with C. parapsilosis (21.7%) and C. tropicalis (15.5%) being the most relevant (26,27). Peru reports an incidence of 2.04 cases per 1,000 hospital admissions and a mortality rate of 40%, similar to the regional average, and 70% of isolates correspond to non-albicans strains, with C. parapsilosis (25.3%) and C. tropicalis (24.7%) (17,28). In Venezuela, although published information is limited, hospital rates of 1.72 cases per 1,000 admissions have been reported, with a high proportion of infections caused by non-albicans strains (73.2%), predominantly C. tropicalis and C. parapsilosis; mortality has varied, ranging from 3% to 76% (17,20,29). Paraguay has one of the lowest incidences in the region, with 0.74 cases per 1,000 hospital admissions and an approximate mortality rate of 30%; the most common isolates are C. albicans (34.4%), C. parapsilosis (30.4%), and C. tropicalis (25.4%) (30). In Uruguay, although the available data are less complete, a study in a hospital in Montevideo found that candidemia accounted for 2.83% of all positive blood cultures, with the predominant isolates being N. glabratus (32.74%), C. albicans (27.43%), and C. parapsilosis (23,01 %), which contrasts with the patterns observed in other countries in the region (31,32). In Mexico, there is an incidence of 1.93 cases per 1,000 hospital admissions; the distribution of isolates indicates a predominance of C. albicans (60%), followed by C. tropicalis (26%) and N. glabratus (13.5%); 30-day mortality has been estimated at 40% (33–35) In Central America and the Caribbean, information is scarce; in Trinidad and Tobago, for example, approximately 70 cases of candidemia are reported each year, although detailed data on the strains involved and clinical outcomes are not available (36).
3. Risk factors for IC in Latin America
This type of mycosis includes both candidemia (infection of the bloodstream) and deep infections in organs or tissues that are normally sterile, such as peritoneal fluid, the central nervous system, or heart valves (1,4,5). The risk factors for developing IC in Latin America largely coincide with those described worldwide. In general, they consist of conditions that weaken the immune system or alter anatomical barriers, facilitating the entry and proliferation of Candida spp. (3,4,6). The main risk factors include prolonged stay in the ICU, use of TPN, exposure to broad-spectrum antibiotics, gastrointestinal surgery with intestinal opening, and prolonged immunosuppression (1,3,6,42,43).
A multicenter case-control study conducted in non-neutropenic critically ill patients from seven intensive care units (ICUs) at three university hospitals in Colombia identified the following independent risk factors associated with the development of candidemia: a hospital stay ≥ 25 days (OR 5.33; 95% CI 2.6–10.9), previous use of meropenem (OR 3.75; 95% CI 1.86–7.5), previous abdominal surgery (OR 2.9; 95% CI 1.39–6.06), and hemodialysis treatment (OR 3.35; 95% CI 1.5–7.7) (44).
Immunosuppression, whether secondary to underlying diseases (cancer, organ transplantation, or chronic renal failure) or immunosuppressive treatments (chemotherapy, corticosteroids, or biological drugs), is a key factor. In addition, the presence of multiple comorbidities in the same patient significantly increases the risk of invasive infection by Candida spp. (45,46). A systematic review with meta-analysis that evaluated the determinants for invasive Candida infection in critically ill patients showed that, apart from the classic factors, the use of broad-spectrum antibiotics (OR 5.6; 95% CI 3.6–8.8), blood transfusions (OR 4.9; 95% CI 1.5–16.3), Candida colonization (OR 4.7; 95% CI 1.6–14.3), the presence of a central venous catheter (OR 4.7; 95% CI 2.7–8.1), and TPN (OR 4.6; 95% CI 3.3–6.3) were independently associated with an elevated risk, while demographic factors lacked statistical significance, highlighting that ICU interventions and underlying comorbidities are the main drivers of this type of infection (47). Therapeutic management in Latin America faces growing challenges due to the increase in infections caused by non-albicans strains, many of which are resistant to commonly used antifungal agents. For this reason, international and regional guidelines agree in recommending the initiation of treatment with echinocandins as first-line therapy while the identification of the agent and its susceptibility profile is completed (48,49). In addition, it is essential to assess the potential involvement of target organs, given that controlling the source of infection, whether through catheter removal, abscess drainage, or surgical debridement, is key to achieving complete resolution of the clinical picture (3,6,45).
4. Diagnosis of IC in Resource-Limited Settings
The timely diagnosis of IC represents one of the main clinical challenges, especially in resource-limited settings such as those found in many Latin American countries (50). Although isolation of the fungus in blood cultures or cultures from sterile sites and histopathological identification of yeasts in tissue constitute the reference method, this method has variable sensitivity (20%–70%) and prolonged detection times, usually 3 to 5 days (51,52). These delays limit the early initiation of targeted treatment, resulting in poorer clinical outcomes. To overcome these diagnostic limitations, complementary tests have been incorporated that improve sensitivity and shorten waiting times; among them, mass spectrometry (MALDI-TOF) stands out for accurately identifying Candida spp. in a matter of minutes from cultures, in contrast to conventional methods such as VITEK®2 or API, which require an additional 24 to 48 hours after growth and can exhibit up to 72% identification errors in rare strains (51,53,54). Table 1 presents a comparison of the diagnostic methods available for IC, detailing their main advantages, limitations, and availability in Latin America.
Other useful tools include immunological tests, such as (1,3)-β-D-glucan (BDG), a pan-fungal marker that has shown 92% sensitivity, although its specificity is limited, as it can give positive results in infections caused by other fungi (46,51,55). In general, it is recommended to use it as a complementary tool to support diagnosis or to discontinue empirical antifungal treatments when clinical suspicion decreases (56). On the other hand, the use of molecular tests such as quantitative PCR in blood has shown good diagnostic performance, with sensitivity and specificity greater than 90% (57). In 2019, the MICAFEM study, conducted in 27 Spanish ICUs, was published. It compared multiplex PCR with blood cultures and abdominal fluid cultures in 176 critically ill patients at high risk of Candida infection. The PCR detected 9.1% of cases, compared to 8.0% for blood cultures and 65.3% for abdominal cultures. Only a Candida risk score ≥ 3 was significantly associated with combined positive results (OR 4.15; p = 0.03). In this group of patients, this test did not improve diagnostic performance (58).
The T2Candida panel is a relatively new technology that uses magnetic resonance imaging to directly detect Candida DNA in blood samples, without the need for prior culture. This test provides results in 3–5 hours, with a sensitivity of 91% and a specificity of 99%. Its main limitation is that it only detects five common strains and does not include C. auris (59–61). In research, the T2Cauris panel detects C. auris in inguinal swabs with a limit of 5 CFU/mL and provides 89% sensitivity and 98% specificity. However, data on its performance in whole blood have not yet been published (62,63). Other serological methods, such as detection of mannan antigen and anti-mannan antibodies, offer a combined sensitivity of 83% and specificity of 86% for C. albicans; however, they are less effective when evaluating other Candida strains (51,64).
Situation in Latin America: Challenges, Barriers, and Obstacles
In the Latin American context, there are significant challenges to implementing these advanced methods. The study by Falci et al. found that, by 2019, only 9% of the laboratories surveyed in the region met the minimum standards of excellence in clinical mycology (65). The availability of BDG is very limited, reaching only 17% of diagnostic centers. Molecular diagnostic techniques are accessible in 20%–26% of laboratories, and MALDI-TOF is only installed in 20%, mainly in large cities. Meanwhile, the T2Candida panel is not yet widely available in the region (50,65,66).
In most Latin American hospitals, blood cultures remain the main diagnostic tool, despite their low sensitivity and the long time required to obtain results. This limitation can delay the initiation of appropriate antifungal treatment and often lead to prolonged and inappropriate empirical use of antifungals, which promotes the development of resistance (50,65). In addition, there are institutional barriers, deficiencies in public policies, and limitations in the allocation of state budgets, as the best-equipped laboratories are concentrated in major urban centers, leaving hospitals in intermediate or rural areas without access to advanced diagnostic techniques (50,65,66). The shortage of personnel trained in clinical mycology and the lack of up-to-date epidemiological data are significant limitations, given that most of the information comes from Brazil, Colombia, Argentina, Mexico, and Chile, while in the Caribbean, Central America, and other Andean areas, no recent studies are available, underscoring the need to strengthen regional surveillance and diagnostic capabilities (17,18,27,31,35,36,67,68).
In Latin America, the identification of the emerging yeast C. auris continues to be problematic, as automated biochemical methods often confuse it with Candida haemulonii, Rhodotorula glutinis, or Saccharomyces cerevisiae. Even advanced commercial systems, such as the VITEK®2 system, show limitations in their accuracy, and although there are more affordable selective media, such as CHROMagar Candida Plus, which could facilitate its detection, their implementation is not yet widespread (69–71). It has been observed that, in the region, countries such as Colombia have established national reference centers that allow for detailed registration and confirmation of strains identification using proteomic or molecular methods (MALDI-TOF or genetic sequencing), in an effort to strengthen epidemiological surveillance and optimize the health response (70,72).
5. Regional Antifungal Resistance Patterns
Antifungal resistance in Candida strains has become a growing concern worldwide, and Latin America is no exception. Traditionally, most clinical isolates were sensitive to available antifungal agents, but in recent years, there has been a significant change in sensitivity profiles, mainly attributable to the increase in non-albicans strains and the rapid spread of C. auris (66,71,73–75). Before the emergence of C. auris in the region, antifungal resistance rates were low: C. albicans typically showed rates below 10%, while N. glabratus, C. parapsilosis, and C. tropicalis showed somewhat higher but still manageable rates. As a result, regional guidelines in effect until 2013 considered fluconazole (FCZ) as the first-line treatment in most cases, although this reality has changed dramatically (11,76,77).
The following are the main emerging non-albicans strains in Latin America, highlighting their epidemiological relevance, their capacity for hospital spread, and their antifungal resistance profiles:
- 1.
- Candida parapsilosis
Candida parapsilosis has become highly relevant in the region, not only because of its high frequency, but also because of its ability to colonize hospital environments and cause outbreaks, especially in pediatric units (78). A descriptive observational study conducted between 2009 and 2010 in 11 public and more than 85 private hospitals in South Africa assessed Candida spp. isolates in blood cultures and determined a prevalence of C. parapsilosis resistance to FCZ of 63%, with cross-resistance to voriconazole (VCZ) in 44% of cases (79). In a hospital in Mexico City (2014–2016), 38% of IC were attributed to C. parapsilosis, of which 54% were resistant to FCZ. The ERG11 analysis found the silent mutation T591C in all isolates and the substitution A395T (Y132F) in seven; four of these strains with Y132F shared an identical microsatellite profile, evidencing a clonal nosocomial outbreak (80). In a prospective descriptive observational study conducted at a tertiary care hospital in Colombia between 2018 and 2021, 123 isolates from Candida blood cultures were analyzed, of which C. parapsilosis accounted for 19.5%; of this subset, 25% showed resistance to FCZ, and among the resistant strains, 67% had mutations in the ERG11 gene (mainly Y132F and, in one case, K143R) and the remaining 33% exhibited increased efflux pump activity, thus revealing a combined resistance mechanism (81).
The increase in the percentage of C. parapsilosis isolates is alarming for two reasons: first, most patients with FCZ-resistant strains had not been previously exposed to this antifungal agent; second, a growing number of strains with reduced sensitivity to echinocandins are emerging, attributable to mutations in the FKS1 gene (82–84).
- 2.
- Candida tropicalis
In several countries in the region, C. tropicalis has established itself as the second or third most common strain associated with candidemia. In Brazil, although resistance to FCZ and VCZ remains low (<5%), a growing trend has been observed that warrants close surveillance to prevent the emergence of multidrug-resistant strains. A study that genotyped 230 clinical and environmental isolates of C. tropicalis from Latin America identified 164 genotypes and 11 possible outbreaks. This analysis detected resistance to anidulafungin (ANF), associated with the FKS1 S659P mutation in one isolate, and identified mutations in the ERG11 gene (Y132F, Y257H/N), linked to resistance or intermediate susceptibility to azoles. These findings evidence both unrecognized outbreaks and clonal spread of antifungal-resistant strains in the region. Genetic clusters have been documented in cities separated by more than 1,400 km, suggesting possible environmental spread; this strain has even been isolated in beach sand samples, reinforcing the need for a comprehensive health approach under the “One Health” perspective (85,86). Resistance to azoles stands at around 10.4%, while resistance to echinocandins remains low (0.4%) (22,85,86).
- 3.
- Nakaseomyces glabratus (formerly C. glabrata)
Nakaseomyces glabratus is currently a clinically challenging pathogen responsible for up to 30% of candidemias in some developed countries, with FCZ resistance rates of 20%–30% and up to 10% to echinocandins, associated with mutations in PDR1 and FKS2; furthermore, its virulence is based on biofilm formation, intracellular persistence, and EPA-type adhesins (15,87). In Latin America, despite the scarcity and heterogeneity of data, it has been established that resistance to N. glabratus is high and highly variable (4%–100%), while resistance to echinocandins is moderate (1%–10%), and although no resistance to polyens was detected, isolates with dose-dependent sensitivity and some cases of multidrug resistance were observed (87). In the region, resistance to FCZ varies by country: 12.8% in Argentina, 6.6% in Chile, 6.7% in Mexico, and up to 28. 6% in Brazil. Although resistance to echinocandins remains low in most countries (<2.3%), exceptions have been reported, such as in Chile, where resistance to micafungin reached 10%, reinforcing the need for constant genomic and phenotypic surveillance (15,87,88).
- 4.
- Pichia kudriavzevii (formerly C krusei)
Candidemia caused by P. kudriavzevii is less prevalent in Latin America (0.3%–1.1%) compared to the United States (2%–3%) and Europe (2%–5%), suggesting an uneven global distribution, possibly influenced by diagnostic capabilities, selective pressure from antifungal use, and regional hospital practices (89). In Latin America, P. kudriavzevii shows approximately 70% resistance to FCZ (intrinsic resistance), around 25% to VCZ, and less than 5% to echinocandins and amphotericin B (AmB). These percentages contrast with data from the United States, where resistance to VCZ is less than 5% and to echinocandins, less than 2%, which translates into a greater therapeutic challenge for this strain in the region. The highest resistance rates have been reported in Brazil (34.1% for VCZ) and Colombia (18.2% for VCZ and 7.3% for echinocandins), while in Chile, resistance to VCZ has hardly been detected (89). Due to its intrinsic resistance to FCZ, initial treatment of infections caused by this yeast should be carried out with echinocandins, considering VCZ and AmB as therapeutic alternatives. Although resistance to echinocandins is rare, it has been documented in up to 30% of cases during treatment. However, its prevalence in the region remains low; in Brazil, for example, it accounts for only 2.8% of isolates (56,61,90).
- 5.
- Other emerging yeast-like strains
- •
- Candida haemulonii complex: this yeast is emerging as an invasive pathogen, with reports in several hospitals in the region, including Mexico, Panama, and Brazil. In Brazil, it has been identified in 0.3% of cases, mainly from chronic wounds and blood cultures, and is associated with critically ill patients. It is characterized by a multidrug resistance profile, particularly to AmB and FCZ, and is often misidentified by conventional methods. Therefore, molecular diagnostics or MALDI-TOF are required for accurate identification, as well as active mycological surveillance and timely adjustment of empirical antifungal treatment (91,92).
- •
- Candida duobushaemulonii: this yeast represents an emerging threat in the context of nosocomial infections, with a marked tendency to behave as an invasive, underdiagnosed, and multidrug-resistant pathogen. It should be considered an emerging yeast of relevance in the Latin American hospital setting. The national surveillance of C. auris carried out in Panama between November 2016 and May 2017 evidenced this, and a significant number of cases of invasive infections caused by this strain were unexpectedly identified. Of the 36 suspected isolates sent to the national reference laboratory, 17 (47%) were confirmed as C. duobushaemulonii, affecting 14 patients hospitalized in six health centers in the country (37).
- •
- Meyerozyma guilliermondii complex (formerly Candida guilliermondii): considered an emerging group of opportunistic yeasts, especially in immunocompromised and hospitalized patients. Globally, it accounts for approximately 1% to 5% of candidemia cases, but its importance is increasing due to three main factors: its genetic and taxonomic diversity, an unfavorable antifungal profile, and the difficulties associated with its diagnostic identification. In Latin America, it accounts for up to 7% of candidemia cases in Peru, with the spread of M. caribbica and clade 2 of M. guilliermondii sensu stricto, both associated with azole resistance, being particularly noteworthy. In addition, multiple isolates with resistance to FCZ, AmB, and echinocandins have been documented in Brazil. Given this situation, it is crucial to incorporate molecular identification methods, establish robust antifungal surveillance systems, and adjust empirical antifungal treatment according to the local susceptibility profile. Azole resistance in this complex can vary between 40% and 70%, reinforcing the need for an individualized therapeutic approach (93).
- •
- Candida rugosa: this emerging yeast has gained relevance in the context of invasive infections, particularly in cases of candidemia, due to its worrying resistance profile to azoles. It has established itself as an opportunistic pathogen of growing importance, especially in Latin America, where it has a prevalence approximately seven times higher than in other geographical regions. In Brazil, C. rugosa accounts for up to 2.7% of isolates in ICUs, with FCZ resistance rates reaching 64.9%, and AmB-resistant isolates have also been reported. Its low sensitivity to classic azoles—FCZ (35.7%) and VCZl (55.8%)—makes these antifungals high-risk therapeutic options (94).
The increase in infections caused by non-albicans strains, together with the emergence of resistant clones in hospital settings, represents a growing challenge for public health. Given this threat, it is essential to implement epidemiological surveillance programs, strengthen the diagnostic capabilities of clinical mycology laboratories, and promote the rational use of antifungals as essential pillars for its containment (50).
Candidozyma auris (Candida auris) in Latin America
Candidozyma auris has emerged as a high-impact pathogen worldwide due to its ability to cause nosocomial outbreaks, its marked resistance to multiple classes of antifungals, and its persistence in the hospital environment. This strain represents a unique challenge, not only because of its clinical severity, but also because of the difficulties in its microbiological identification and its remarkable ability to spread. In Latin America, its presence has been documented in several countries, with Colombia, Venezuela, Brazil, and Panama having the highest number of reported cases, with mortality rates ranging from 30% to 60%. In the region, C. auris isolates predominantly belong to Clade IV, also known as the South American clade (70,71).
In terms of population burden, the infection rate for C. auris in Colombia is estimated at 2.55 cases per 100,000 inhabitants. Panama has an even higher rate, with 5.42 cases per 100,000 inhabitants, making it one of the countries with the highest incidence in the region. In contrast, Mexico has a significantly lower rate, estimated at 0.01 per 100,000 inhabitants. Other countries, such as Costa Rica, Peru, Chile, Venezuela, and Brazil, have reported fewer than 100 confirmed cases each (74).
In 2016, Colombia reported the first cases confirmed using molecular techniques, which had initially been misidentified as C. haemulonii. Since then, the number of infections has shown sustained growth, consolidating the region as an area of epidemiological importance for this pathogen (74,75). A recent study documented 2,119 confirmed cases of C. auris in this country between 2016 and 2022, with candidemia being the most common clinical manifestation, accounting for 55% of cases. The rate of resistance to FCZ in these isolates was 35%, while resistance to AmB reached 33%. Fortunately, resistance to echinocandins remains uncommon (70,71,75).
Phylogenetic studies have shown that Clade IV of C. auris in Latin America did not spread as a single clonal group, but rather presents a defined geographical substructure. This pattern suggests the existence of multiple local transmission foci, rather than a common origin, and reinforces the importance of establishing continuous molecular surveillance strategies in the region (73,74). In Colombia, for example, two regional lineages have been identified: one in the center and one in the north of the country. Isolates from the north show high resistance to AmB (64%), while in the center resistance was 0% (73,95). With the aim of clarifying the origin, evolutionary history, and dispersion patterns of C. auris, a genomic sequencing study was conducted on 304 isolates collected between 2004 and 2018 from 19 countries. The results indicated that Clade IV emerged approximately 30 to 40 years ago and has a clearly defined phylogeographic structure. These findings support the hypothesis that it did not spread as a single clonal group but, after its appearance in South America, multiple local transmission foci established themselves in different countries or regions, with little genetic exchange between them (96).
Environmental contamination is recognized as a critical factor in the transmission of C. auris. In Colombia, colonization has been reported in healthcare personnel (41%) and the fungus has been detected on various hospital surfaces. In addition, this yeast has the ability to remain colonizing patients for several months, as well as persist on cleaning objects and even in freshwater bodies (97,98). A recent study succeeded in isolating C. auris in marine sediments and coastal areas where fresh and brackish waters converge, demonstrating its ability to tolerate extreme environmental conditions, such as high salinity and elevated temperatures. This remarkable adaptability has reinforced the hypothesis that climate change and environmental pressure have played a key role in its emergence as a pathogen (99). Figure 2 shows the hypothesis of the socio-environmental factors involved in the emergence of C. auris. In this molecular epidemiology study, the high resistance to amphotericin B (64%) observed in isolates from northern Colombia stands out, in contrast to the absence of resistance (0%) in isolates collected in the central part of the country (73,95). On the other hand, two main genetic clusters, named C1 and C2, have been identified in Colombia, with two subclasses within cluster C1: C1-A and C1-B. These subclasses show minor differences in the number of SNPs, suggesting sustained transmission of cluster C1 since its introduction into the country in 2016 (73,95,96). In other countries in the region, such as Brazil and Argentina, the presence of other clades, specifically Clade I and Clade III, has been documented in isolated cases. These findings suggest the possible co-circulation of different clades in these territories, which could imply multiple events of introduction or independent dispersion (74).
In terms of antifungal resistance profiles, Clade IVs show almost universal resistance to FCZ (>90%), variable resistance to AmB (between 30% and 60%, depending on the lineage), and low but documented resistance to echinocandins, reported in up to 5% of cases (72,100). Among the molecular mechanisms associated with azole resistance in C. auris are mutations in the ERG11 gene, which encodes the enzyme lanosterol 14-α-demethylase, including the variants F126L, Y132F, VF125AL, and K143R. For polyenes, the TAC1B gene has been implicated, while resistance to echinocandins has been linked to mutations in the FKS1 gene, which alter the catalytic subunit of the enzyme 1,3-β-D-glucan synthase. In addition, four non-synonymous mutations associated with resistance to amphotericin B have been identified in genes linked to transcription factors homologous to FLO8 (such as the S108N mutation) and in the PSK74852 gene, where the I139T variant was reported (73,74,95). In addition to the genetic mechanisms described above, it has the ability to form biofilms, which reduces the penetration of antifungal agents and promotes its persistence in hospital environments. Unlike other pathogenic yeasts, it does not usually colonize the gastrointestinal tract, but rather shows a marked affinity for human skin, especially in moist and folded areas such as the axillae and groin region (97,101).
Candidozyma auris can clinically present as a skin colonizer, given that, unlike other Candida strains, it does not behave as a saprophyte or commensal of the gastrointestinal tract. In addition, it is capable of causing various invasive infections, including primary fungemia, infections associated with medical devices, endocarditis, urinary and respiratory tract infections, as well as osteomyelitis (69,71,102).
In Latin America, diagnosis and identification face significant limitations, mainly due to insufficient coverage of technologies such as MALDI-TOF and identification biases present in automated systems such as VITEK®2 (bioMérieux), which can misidentify up to 22% of isolates (71). Currently, it is a notifiable disease in several countries in the region, such as Colombia and Brazil. However, control policies vary considerably between countries and institutions, and many of them still face difficulties in their implementation due to the absence of standardized protocols, limitations in infrastructure, and deficiencies in the training of health personnel (23,71,75). In response, some countries have issued national health alerts with the aim of strengthening epidemiological surveillance, improving hygiene practices in hospital settings, and promoting the rational use of antifungals (103,104). However, it is recognized that these measures must be expanded and coordinated at the regional level to effectively contain the threat posed by this multidrug-resistant yeast. The approach must evolve toward active surveillance, including environmental monitoring, phylogenetic studies, and the implementation of coordinated intersectoral actions.
6. Impact of Climate Change on Fungal Infections (Invasive Candidiasis)
Climate change is a global phenomenon that is significantly transforming public health patterns, including the emergence and spread of fungal infections such as IC. The sustained increase in atmospheric and ocean temperatures, together with changes in humidity levels and the growing frequency of extreme weather events, is altering the ecological behavior of fungi, favoring the adaptation and emergence of thermotolerant and resistant pathogenic strains (105,106). From an environmental perspective, global warming has altered the distribution and survival of fungi in habitats that were previously hostile to their development. This transformation not only affects fungal diversity and the nutrient cycle, but more worryingly, it has created conditions favorable for the natural selection of strains capable of surviving increasingly high temperatures (107).
One of the most relevant hypotheses to explain the emergence of C. auris suggests climate change as a key evolutionary driver. In 2019, Casadevall and colleagues proposed the “thermal selection hypothesis,” according to which progressive environmental warming has favored the adaptation of certain environmental fungi to higher temperatures, allowing them to overcome the thermal barrier that historically limited their ability to infect humans. This phenomenon is not exclusive to C. auris, as other emerging strains, such as Cryptococcus deuterogattii, have also shown similar patterns of adaptation (108,109).
In addition to climate change, other environmental and anthropogenic factors have been associated with the emergence of Candidozyma auris and other resistant fungi. The indiscriminate use of antifungals in agriculture, especially azoles, has exerted selective pressure on environmental microorganisms. Sharma and Kadosh (2023) found that these compounds, widely used in fruit and vegetable cultivation, may have contributed to the emergence of resistant strains in the environment, which subsequently migrate to the hospital environment (110). This hypothesis of thermal selection has been proposed in other emerging fungi (111,112).
Another emerging hypothesis suggests the possible role of wild fauna as a passive vector in the spread of resistant fungi. From a One Health perspective, García-Bustos and colleagues proposed that migratory birds could act as carriers of C. auris, facilitating its transit from natural environments to rural or urban areas, where the fungus could establish itself and eventually enter the hospital environment. This integrative approach, which links human, animal, and environmental health, is essential for understanding the complex web underlying emerging mycoses (33,113,114).
Forced migration, overcrowding, shortages of drinking water, and limited access to healthcare in refugee camps significantly increase the vulnerability of these populations to invasive fungal infections. Added to this is the threat to food security, exacerbated by climate change, which can lead to malnutrition and, with it, a marked increase in the incidence of infectious diseases, including fungal infections. In addition, extreme weather events such as floods create humid environments conducive to the germination and spread of fungal spores. These conditions favor accelerated fungal growth, facilitating the large-scale dispersion of spores and mycotoxins (102,107–109,115–117).
Overall, it is recognized that various factors contribute to the emergence of invasive mycoses such as C. auris. These include the indiscriminate use of antifungals in agriculture, water contamination, inadequate hospital practices, and forced population displacement. Added to this are the interactions between degraded ecosystems, wild fauna, and the growth of vulnerable human populations, creating a scenario favorable to the emergence and spread of resistant pathogenic fungi (97,102,110,114,118,119).
7. Access to Health Services and Inequalities in the Region
Socioeconomic inequalities and differences in access to healthcare services in Latin America have a direct and significant impact on the management of fungal infections, including IC. The gap between public and private healthcare systems, as well as between urban and rural areas, and between countries with different levels of development, leads to profoundly unequal clinical scenarios. In many cases, the patient's prognosis depends more on their geographical location or socioeconomic status than on the natural course of the disease (27,31,34,35,66). In Brazil, for example, studies have shown that the incidence of candidemia in public hospitals is more than double that in private institutions, with rates of 2.42 versus 0.91 cases per 1,000 ICU admissions, respectively. In addition, the distribution of strains differs depending on the type of institution: while C. parapsilosis predominates in public hospitals, N. glabrata is more common in private hospitals (24,66,120).
Access to antifungal treatments in Latin America also presents marked inequalities. In many countries in the region, FCZ and AmB deoxycholate are the only widely available antifungals, even though they are not always the most appropriate therapeutic option. First-line drugs, such as echinocandins or lipid formulations of AmB, have limited availability, particularly in public hospitals and rural areas. Meanwhile, 5-flucytosine—essential for the treatment of certain serious fungal infections—is available in only 20% of the hospitals evaluated (50). The prices of antifungal drugs also vary considerably between countries in the region, with costs ranging from $1 to $31 per unit of FCZ. This variation can be a significant obstacle for many patients, especially when healthcare systems do not provide comprehensive coverage for antifungal treatment (121). In Colombia, for example, the healthcare system largely covers the costs of antifungal treatments. However, the availability of medications remains uneven. While cities such as Bogotá and Medellín have a more adequate supply, many rural regions face critical shortages, limiting timely access to effective therapies (122).
In the context of an IC, a key factor is the continuing education of healthcare personnel. In centers with greater resources, access to specialized training in fungal infections is more common, which translates into more appropriate clinical management by professionals. In contrast, in settings with less access to training, significant knowledge gaps persist. In this scenario, virtual education strategies (e-learning) become highly relevant for expanding access to training. However, there are barriers that can limit its effective implementation, such as poor internet connectivity, limited proficiency in other languages, and lack of knowledge or low familiarity with technological tools by some healthcare professionals (123–126).
In response to this situation, various regional initiatives have been launched to reduce existing gaps. The Pan American Health Organization (PAHO) and the Global Action Fund for Fungal Infections (GAFFI) have established strategic alliances to improve access to essential antifungals, standardizing clinical protocols, and strengthening the diagnostic capabilities of health systems in the region (127). The use of telemedicine and virtual education is also promoted as key tools for training healthcare personnel in remote areas. However, these efforts face various challenges, including poor connectivity, language barriers, and unequal access to digital technologies, which limits their effective implementation in some regions (126,128).
Reducing mortality from IC in the region requires much more than strengthening treatment options. It involves adopting a comprehensive approach that addresses structural barriers in the health system, improves resource distribution, and ensures equitable access to diagnosis and antifungal treatment at all levels of care.
8. Impact of Housing and Environment on IC in Latin America
Although IC has been extensively studied in hospital settings, its relationship with environmental factors and living conditions in Latin America remains poorly explored. Unlike other invasive mycoses, such as histoplasmosis or cryptococcosis, in which the link with the natural environment is well documented, candidiasis has traditionally been considered a nosocomial infection. However, recent data suggest that the physical environment and living conditions may also influence the vulnerability of certain population groups to this infection (129,130). Although Candida is not a typical environmental fungus like Aspergillus or Cryptococcus, its presence has been documented in ecological niches outside the human environment. For example, strains such as C. albicans have been isolated in soil and vegetables, C. tropicalis in rivers and agricultural areas, and P. kudriavzevii in animals. In the particular case of C. auris, its detection in freshwater and marine bodies in coastal areas of Colombia reinforces the hypothesis that certain environmental settings could act as reservoirs or points of contact with humans, especially in populations with limited sanitary conditions (131,132).
One of the most important aspects from a social and environmental point of view is the quality of housing. In many urban areas of Latin America, informal settlements and marginalized neighborhoods lack basic services such as drinking water, adequate ventilation, and sanitation. These conditions favor the proliferation of opportunistic microorganisms and can facilitate colonization by yeasts, especially in humid or contaminated environments. Although the direct relationship between these conditions and IC has not yet been fully demonstrated, overcrowding and poor housing conditions have been associated with an increased risk of superficial infections, such as oral and vulvovaginal candidiasis. In addition, the high prevalence of chronic noncommunicable diseases in contexts of poverty—such as diabetes mellitus and chronic kidney disease—significantly increases the risk of invasive Candida infections (131,132).
Other Invasive Mycoses
The influence of the environment on invasive aspergillosis is closely related to exposure to spores present in the air, especially in contexts where construction work is being carried out or where ventilation systems are inadequate. These factors have been implicated in hospital outbreaks, as they facilitate the spread of Aspergillus conidia in clinical areas (18,35). In addition, there are isolated studies on other mycoses that support this perspective. In Brazil, for example, Cryptococcus gattii has been isolated from household dust in wooden houses located in the Amazon region, demonstrating that indoor spaces can also act as reservoirs for pathogenic fungi. Although such a direct link has not been established in the case of Candida, moisture accumulation and environmental contamination could play a role in its spread or in increasing the host's vulnerability (133).
Gaps in the literature and emerging hypotheses: in general, there are few studies exploring the link between housing conditions and IC, as most publications focus exclusively on hospital settings. However, in Argentina, there has been evidence of variation in the distribution of Candida strains causing invasive infections, associated with socioeconomic factors such as income level in dollars and type of healthcare institution (public or private) (66).
9. Conclusions
IC has become a significant threat to public health in Latin America. Its increasing incidence, especially in ICUs, and the high mortality rate associated with it highlight a clinical urgency that cannot be ignored. Although historically attributed to C. albicans, there is currently an epidemiological shift toward non-albicans strains, many of which are resistant to the most commonly used antifungal agents.
The emergence of C. auris, characterized by its remarkable ability to spread, resistance to multiple antifungals, and persistence in the environment, has highlighted the structural weaknesses of health systems in the region. Gaps in diagnosis, limited availability of effective therapies, and unequal access to medical care have left many populations in a vulnerable situation, especially in public health systems, rural areas, or impoverished communities.
In addition to these clinical and technical issues, social and environmental factors amplify the impact of fungal infections. Climate change, the indiscriminate use of antifungals in agriculture, poor housing conditions, and structural inequalities in healthcare systems create an environment favorable for the emergence of resistant pathogens and the spread of serious fungal infections.
To address this challenge, it is essential to adopt a comprehensive and coordinated approach that transcends the strictly hospital setting. It is necessary to strengthen mycological surveillance systems, ensure equitable access to advanced diagnostic tests and state-of-the-art antifungals, and train health personnel at all levels of care.
Regional research must be intensified, especially in countries where information on IC is limited, to obtain a more accurate picture of its actual burden and local characteristics. Only on this basis will it be possible to design effective, contextualized, and evidence-based public policies. It is time to look beyond the microscope and move toward solutions that integrate science, public health, and social justice.
Author Contributions
Conceptualization, J.C.M., P.R.-P., J.M.O.; Methodology, J.C.M., P.R.-P.; Software, J.C.M.; Validation, J.C.M. and P.R.-P.; Formal analysis, J.M.O. and J.C.M.; Investigation, J.C.M. and P.R.-P.; Resources, J.C.M.; Data curation, J.C.M.; Drafting—preparation of the original draft, J.C.M., P.R.-P., J.M.O.; Drafting—review and editing, J.C.M., P.R.-P.; Visualization, J.C.M., P.R.-P.; Supervision, J.C.M. and P.R.-P.; Project management, J.C.M., P.R.-P. All authors have read and approved the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The authors have reviewed and edited the result and assume full responsibility for the content of this publication.
Conflicts of interest
The authors declare no conflicts of interest.
References
- Campion EW, Kullberg BJ, Arendrup MC. Invasive Candidiasis. Campion EW, editor. N Engl J Med [Internet]. 2015 [cited 2025 Apr 29];373(15):1445–56. Available from: https://pubmed.ncbi.nlm.nih.gov/26444731/. [CrossRef]
- Pappas PG, Lionakis MS, Arendrup MC, Ostrosky-Zeichner L, Kullberg BJ. Invasive candidiasis. Nat Rev Dis Primers. 2018 May 11;4. [CrossRef]
- Lass-Flörl C, Kanj SS, Govender NP, Thompson GR, Ostrosky- Zeichner L, Govrins MA. Invasive candidiasis. Nat Rev Dis Primers [Internet]. 2024 Dec 1 [cited 2025 Apr 29];10(1). Available from: https://pubmed.ncbi.nlm.nih.gov/38514673/. [CrossRef]
- Soriano A, Honore PM, Puerta-Alcalde P, Garcia-Vidal C, Pagotto A, Gonçalves-Bradley DC, et al. Invasive candidiasis: current clinical challenges and unmet needs in adult populations. Journal of Antimicrobial Chemotherapy [Internet]. 2023 [cited 2025 Apr 29];78:1569–85. [CrossRef]
- Pappas PG, Lionakis MS, Arendrup MC, Ostrosky-Zeichner L, Kullberg BJ. Invasive candidiasis. Nat Rev Dis Primers [Internet]. 2018 May 11 [cited 2025 Apr 29];4. Available from: https://pubmed.ncbi.nlm.nih.gov/29749387/. [CrossRef]
- Noppè E, Robert J, Eloff P, Keane S, Martin-Loeches I. A Narrative Review of Invasive Candidiasis in the Intensive Care Unit. Therapeutic Advances in Pulmonary and Critical Care Medicine [Internet]. 2024 Jan 12 [cited 2025 Apr 29];19:29768675241304684. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC11693998/. [CrossRef]
- Koehler P, Stecher M, Cornely OA, Koehler D, Vehreschild MJGT, Bohlius J, et al. Morbidity and mortality of candidaemia in Europe: an epidemiologic meta-analysis. Clinical Microbiology and Infection. 2019 Oct 1;25(10):1200–12. [CrossRef]
- Seagle EE, Jackson BR, Lockhart SR, Jenkins EN, Revis A, Farley MM, et al. Recurrent Candidemia: Trends and Risk Factors Among Persons Residing in 4 US States, 2011–2018. Open Forum Infect Dis [Internet]. 2022 Oct 1 [cited 2025 Apr 29];9(10):ofac545. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC9620433/. [CrossRef]
- Toda M, Williams SR, Berkow EL, Farley MM, Harrison LH, Bonner L, et al. Population-Based Active Surveillance for Culture-Confirmed Candidemia — Four Sites, United States, 2012–2016. MMWR Surveillance Summaries [Internet]. 2019 [cited 2025 Apr 29];68(8):1–17. Available from: https://pubmed.ncbi.nlm.nih.gov/31557145/. [CrossRef]
- Ricotta EE, Lai YL, Babiker A, Strich JR, Kadri SS, Lionakis MS, et al. Invasive Candidiasis Species Distribution and Trends, United States, 2009–2017. J Infect Dis [Internet]. 2020 Apr 1 [cited 2025 Apr 29];223(7):1295. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC8030726/. [CrossRef]
- Quindós G. Epidemiology of candidaemia and invasive candidiasis. A changing face. Rev Iberoam Micol. 2014 Jan;31(1):42–8. [CrossRef]
- Wang H, Xu YC, Hsueh PR. Epidemiology of candidemia and antifungal susceptibility in invasive Candida species in the Asia-Pacific region. Future Microbiol. 2016 Nov 1;11(11):1461–77. [CrossRef]
- Giacobbe DR, Maraolo AE, Simeon V, Magnè F, Pace MC, Gentile I, et al. Changes in the relative prevalence of candidaemia due to non-albicans Candida species in adult in-patients: A systematic review, meta-analysis and meta-regression. Mycoses [Internet]. 2020 Apr 1 [cited 2025 Apr 29];63(4):334–42. Available from: https://pubmed.ncbi.nlm.nih.gov/31997414/. [CrossRef]
- Murray CJ, Ikuta KS, Sharara F, Swetschinski L, Robles Aguilar G, Gray A, et al. Global burden of bacterial antimicrobial resistance in 2019: a systematic analysis. The Lancet [Internet]. 2022 Feb 12 [cited 2025 Apr 5];399(10325):629–55. Available from: https://www.thelancet.com/action/showFullText?pii=S0140673621027240. [CrossRef]
- Frías-De-león MG, Hernández-Castro R, Conde-Cuevas E, García-Coronel IH, Vázquez-Aceituno VA, Soriano-Ursúa MA, et al. Candida glabrata Antifungal Resistance and Virulence Factors, a Perfect Pathogenic Combination. Pharmaceutics [Internet]. 2021 Oct 1 [cited 2025 May 12];13(10):1529. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC8538829/. [CrossRef]
- Giacobbe DR, Maraolo AE, Simeon V, Magnè F, Pace MC, Gentile I, et al. Changes in the relative prevalence of candidaemia due to non-albicans Candida species in adult in-patients: A systematic review, meta-analysis and meta-regression. Mycoses [Internet]. 2020 Apr 1 [cited 2025 Apr 29];63(4):334–42. Available from: https://pubmed.ncbi.nlm.nih.gov/31997414/. [CrossRef]
- Nucci M, Queiroz-Telles F, Alvarado-Matute T, Tiraboschi IN, Cortes J, Zurita J, et al. Epidemiology of Candidemia in Latin America: A Laboratory-Based Survey. PLoS One [Internet]. 2013 Mar 19 [cited 2025 Apr 29];8(3):e59373. Available from: https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0059373. [CrossRef]
- Nucci M, Queiroz-Telles F, Tobón AM, Restrepo A, Colombo AL. Epidemiology of opportunistic fungal infections in latin America. Clinical Infectious Diseases [Internet]. 2010 Sep 1 [cited 2025 Apr 29];51(5):561–70. Available from: https://dx.doi.org/10.1086/655683. [CrossRef]
- da Silva RB, Neves RP, Hinrichsen SL, de Lima-Neto RG. Candidemia in a public hospital in Northeastern Brazil: Epidemiological features and risk factors in critically ill patients. Rev Iberoam Micol [Internet]. 2019 Oct 1 [cited 2025 Apr 29];36(4):181–5. Available from: https://www.elsevier.es/es-revista-revista-iberoamericana-micologia-290-articulo-candidemia-in-public-hospital-in-S1130140619300567. [CrossRef]
- da Matta DA, Souza ACR, Colombo AL. Revisiting Species Distribution and Antifungal Susceptibility of Candida Bloodstream Isolates from Latin American Medical Centers. Journal of Fungi 2017, Vol 3, Page 24 [Internet]. 2017 May 17 [cited 2025 May 1];3(2):24. Available from: https://www.mdpi.com/2309-608X/3/2/24/htm. [CrossRef]
- Wille MP, Guimarães T, Campos Furtado GH, Colombo AL. Historical trends in the epidemiology of candidaemia: analysis of an 11-year period in a tertiary care hospital in Brazil. Mem Inst Oswaldo Cruz [Internet]. 2013 [cited 2025 Apr 29];108(3):288. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC4005563/. [CrossRef]
- Hamburger FG, Gales AC, Colombo AL. Systematic Review of Candidemia in Brazil: Unlocking Historical Trends and Challenges in Conducting Surveys in Middle-Income Countries. Mycopathologia [Internet]. 2024 Aug 1 [cited 2025 May 12];189(4). Available from: https://pubmed.ncbi.nlm.nih.gov/38940953/. [CrossRef]
- Cortés JA, Ruiz JF, Melgarejo-Moreno LN, Lemos E V. Candidemia en Colombia. Biomédica [Internet]. 2020 [cited 2025 May 1];40(1):195. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC7357379/. [CrossRef]
- Alexander Salinas Cesar. CARACTERÍSTICAS CLÍNICAS, MICROBIOLÓGICAS Y DESENLACES DE LA CANDIDIASIS INVASORA EN ADULTOS EN UN HOSPITAL DE ALTA COMPLEJIDAD [Internet]. [Bogota]: Universidad del Rosario; 2020 [cited 2025 May 1]. Available from: https://repository.urosario.edu.co/server/api/core/bitstreams/f33a1a7a-13f7-48ac-b4f8-6c2025c7bdc9/content.
- Ortiz-Roa C, Valderrama-Rios MC, Sierra-Umaña SF, Rodríguez JY, Muñetón-López GA, Solórzano-Ramos CA, et al. Mortality Caused by Candida auris Bloodstream Infections in Comparison with Other Candida Species, a Multicentre Retrospective Cohort. Journal of Fungi [Internet]. 2023 Jul 1 [cited 2025 May 12];9(7). Available from: https://pubmed.ncbi.nlm.nih.gov/37504704/. [CrossRef]
- Tiraboschi IN, Pozzi NC, Farías L, García S, Fernández NB. Epidemiología, especies, resistencia antifúngica y evolución de las candidemias en un hospital universitario de Buenos Aires, Argentina, durante 16 años. Revista Chilena de Infectologia [Internet]. 2017 Oct 1 [cited 2025 May 1];34(5):431–40. Available from: https://pubmed.ncbi.nlm.nih.gov/29488584/. [CrossRef]
- Riera FO, Caeiro JP, Denning DW. Burden of serious fungal infections in Argentina. Journal of Fungi [Internet]. 2018 Jun 1 [cited 2025 May 1];4(2). Available from: https://pubmed.ncbi.nlm.nih.gov/29695056/. [CrossRef]
- Rodriguez L, Bustamante B, Huaroto L, Agurto C, Illescas R, Ramirez R, et al. A multi-centric Study of Candida bloodstream infection in Lima-Callao, Peru: Species distribution, antifungal resistance and clinical outcomes. PLoS One [Internet]. 2017 Apr 1 [cited 2025 May 1];12(4):e0175172. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC5395148/. [CrossRef]
- Mesa1 LM, Arcaya2 NM, Pineda S3 MR, Luengo3 HB, Calvo4 BM. Candidemia en el Hospital Universitario de Maracaibo, Estado Zulia, Venezuela 2000-2002. Revista de la Sociedad Venezolana de Microbiología [Internet]. 2005 [cited 2025 May 1];25(2):109–13. Available from: http://ve.scielo.org/scielo.php?script=sci_arttext&pid=S1315-25562005000200010&lng=es&nrm=iso&tlng=es.
- Aguilar G, Araujo P, Lird G, Insaurralde S, Kawabata A, Ayala E, et al. Identificación y perfil de sensibilidad de Candida spp. aisladas de hemocultivos en hospitales de Paraguay. Revista Panamericana de Salud Pública [Internet]. 2020 Sep 1 [cited 2025 May 1];44(1):e34. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC7498287/. [CrossRef]
- Macedo-Viñas M, Denning DW. Estimating the Burden of Serious Fungal Infections in Uruguay. Journal of Fungi [Internet]. 2018 Mar 1 [cited 2025 May 1];4(1):37. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC5872340/. [CrossRef]
- Carbia M, Medina V, Bustillo C, Martínez C, González MP, Ballesté R. Study of Candidemia and its Antifungal Susceptibility Profile at the University Hospital of Montevideo, Uruguay. Mycopathologia [Internet]. 2023 Dec 1 [cited 2025 May 1];188(6):919–28. Available from: https://pubmed.ncbi.nlm.nih.gov/37314581/. [CrossRef]
- Reyes-Montes M del R, Duarte-Escalante E, Martínez-Herrera E, Acosta-Altamirano G, Frías-De León MG. Current status of the etiology of candidiasis in Mexico. Rev Iberoam Micol [Internet]. 2017 Oct 1 [cited 2025 May 2];34(4):203–10. Available from: https://www.elsevier.es/es-revista-revista-iberoamericana-micologia-290-articulo-current-status-etiology-candidiasis-in-S1130140617300864. [CrossRef]
- Corzo-León DE, Perales-Martínez D, Martin-Onraet A, Rivera-Martínez N, Camacho-Ortiz A, Villanueva-Lozano H. Monetary costs and hospital burden associated with the management of invasive fungal infections in Mexico: a multicenter study. The Brazilian Journal of Infectious Diseases [Internet]. 2018 Sep 1 [cited 2025 May 2];22(5):360. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC9428020/. [CrossRef]
- Corzo-León DE, Armstrong-James D, Denning DW. Burden of serious fungal infections in Mexico. Mycoses [Internet]. 2015 Oct 1 [cited 2025 May 2];58:34–44. Available from: https://pubmed.ncbi.nlm.nih.gov/26449505/. [CrossRef]
- Gousy N, Adithya Sateesh B, Denning DW, Latchman K, Mansoor E, Joseph J, et al. Fungal Infections in the Caribbean: A Review of the Literature to Date. Journal of Fungi [Internet]. 2023 Dec 1 [cited 2025 May 2];9(12). Available from: https://pubmed.ncbi.nlm.nih.gov/38132779/. [CrossRef]
- Ramos R, Caceres DH, Perez M, Garcia N, Castillo W, Santiago E, et al. Emerging Multidrug-Resistant Candida duobushaemulonii Infections in Panama Hospitals: Importance of Laboratory Surveillance and Accurate Identification. J Clin Microbiol [Internet]. 2018 Jul 1 [cited 2025 May 12];56(7):e00371-18. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC6018349/. [CrossRef]
- la Garza PR de, Cruz-de la Cruz C de la, Bejarano JIC, Romo AEL, Delgado JV, Ramos BA, et al. A multicentric outbreak of Candida auris in Mexico: 2020 to 2023. Am J Infect Control [Internet]. 2024 Dec 1 [cited 2025 May 4];52(12). Available from: https://pubmed.ncbi.nlm.nih.gov/39059713/. [CrossRef]
- Gousy N, Adithya Sateesh B, Denning DW, Latchman K, Mansoor E, Joseph J, et al. Fungal Infections in the Caribbean: A Review of the Literature to Date. Journal of Fungi [Internet]. 2023 Dec 1 [cited 2025 Jun 7];9(12). Available from: https://pubmed.ncbi.nlm.nih.gov/38132779/. [CrossRef]
- Márquez F, Iturrieta I, Calvo M, Urrutia M, Godoy-Martínez P, Márquez F, et al. Epidemiología y susceptibilidad antifúngica de especies causantes de candidemia en la ciudad de Valdivia, Chile. Revista chilena de infectología [Internet]. 2017 Oct 1 [cited 2025 Jun 11];34(5):441–6. Available from: http://www.scielo.cl/scielo.php?script=sci_arttext&pid=S0716-10182017000500441&lng=es&nrm=iso&tlng=es. [CrossRef]
- de Oliveira CS, Colombo AL, Francisco EC, de Lima B, Gandra RF, de Carvalho MCP, et al. Clinical and epidemiological aspects of Candidemia in eight medical centers in the state of Parana, Brazil: Parana Candidemia Network. The Brazilian Journal of Infectious Diseases [Internet]. 2021 Jan 1 [cited 2025 May 8];25(1):101041. Available from: https://www-sciencedirect-com.ez.urosario.edu.co/science/article/pii/S1413867020301689?utm_source=chatgpt.com. [CrossRef]
- de Almeida BL, Agnelli C, Guimarães T, Sukiennik T, Lima PRP, Salles MJC, et al. Candidemia in ICU Patients: What Are the Real Game-Changers for Survival? Journal of Fungi [Internet]. 2025 Feb 1 [cited 2025 Apr 29];11(2). Available from: https://pubmed.ncbi.nlm.nih.gov/39997446/. [CrossRef]
- Motoa G, Muñoz JS, Oñate J, Pallares CJ, Hernández C, Villegas MV. Epidemiology of Candida isolates from Intensive Care Units in Colombia from 2010 to 2013. Rev Iberoam Micol [Internet]. 2016 Jan 1 [cited 2025 Apr 29];34(1):17–22. Available from: https://www.elsevier.es/es-revista-revista-iberoamericana-micologia-290-articulo-epidemiology-candida-isolates-from-intensive-S1130140616300286. [CrossRef]
- Ortíz Ruiz G, Osorio J, Valderrama S, Álvarez D, Elías Díaz R, Calderón J, et al. Factores de riesgo asociados a candidemia en pacientes críticos no neutropénicos en Colombia. Med Intensiva [Internet]. 2016 Apr 1 [cited 2025 May 8];40(3):139–44. Available from: https://pubmed.ncbi.nlm.nih.gov/26725105/. [CrossRef]
- Riera FO, Caeiro JP, Angiolini SC, Vigezzi C, Rodriguez E, Icely PA, et al. Invasive Candidiasis: Update and Current Challenges in the Management of This Mycosis in South America. Antibiotics [Internet]. 2022 Jul 1 [cited 2025 May 9];11(7). Available from: https://pubmed.ncbi.nlm.nih.gov/35884131/. [CrossRef]
- Vazquez JA, Whitaker L, Zubovskaia A. Invasive Candidiasis in the Intensive Care Unit: Where Are We Now? J Fungi (Basel) [Internet]. 2025 Mar 27 [cited 2025 May 9];11(4). Available from: http://www.ncbi.nlm.nih.gov/pubmed/40278079. [CrossRef]
- Thomas-Rüddel DO, Schlattmann P, Pletz M, Kurzai O, Bloos F. Risk Factors for Invasive Candida Infection in Critically Ill Patients: A Systematic Review and Meta-analysis. Chest [Internet]. 2022 Feb 1 [cited 2025 May 9];161(2):345–55. Available from: https://pubmed.ncbi.nlm.nih.gov/34673022/. [CrossRef]
- Oñate JM, Rivas P, Pallares C, Saavedra CH, Martínez E, Coronell W, et al. Colombian consensus on the diagnosis, treatment, and prevention of Candida Spp. disease in children and adults,. Infectio [Internet]. 2019 [cited 2025 May 8];23(3):271–304. Available from: http://www.scielo.org.co/scielo.php?script=sci_arttext&pid=S0123-93922019000300271&lng=en&nrm=iso&tlng=en. [CrossRef]
- Cornely OA, Sprute R, Bassetti M, Chen SCA, Groll AH, Kurzai O, et al. Global guideline for the diagnosis and management of candidiasis: an initiative of the ECMM in cooperation with ISHAM and ASM. Lancet Infect Dis [Internet]. 2025 May [cited 2025 May 8];25(5):e280–93. Available from: https://pubmed.ncbi.nlm.nih.gov/39956121/. [CrossRef]
- Riera F, Cortes Luna J, Rabagliatti R, Scapellato P, Caeiro JP, Chaves Magri MM, et al. Antifungal stewardship: the Latin American experience. Antimicrobial Stewardship & Healthcare Epidemiology [Internet]. 2023 Dec 5 [cited 2025 May 8];3(1):e217. Available from: https://www.cambridge.org/core/journals/antimicrobial-stewardship-and-healthcare-epidemiology/article/antifungal-stewardship-the-latin-american-experience/E5CB1CC83BF1CC032E1A774F52BEB4FE. [CrossRef]
- Barantsevich N, Barantsevich E. Diagnosis and Treatment of Invasive Candidiasis. Antibiotics [Internet]. 2022 Jun 1 [cited 2025 May 11];11(6):718. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC9219674/. [CrossRef]
- Bassetti M, Giacobbe DR, Vena A, Wolff M. Diagnosis and Treatment of Candidemia in the Intensive Care Unit. Semin Respir Crit Care Med. 2019;40(4):524–39. [CrossRef]
- Kassim A, Pflüger V, Premji Z, Daubenberger C, Revathi G. Comparison of biomarker based Matrix Assisted Laser Desorption Ionization-Time of Flight Mass Spectrometry (MALDI-TOF MS) and conventional methods in the identification of clinically relevant bacteria and yeast. BMC Microbiol. 2017 May 25;17(1). [CrossRef]
- Van Veen SQ, Claas ECJ, Kuijper EJ. High-throughput identification of bacteria and yeast by matrix-assisted laser desorption ionization-time of flight mass spectrometry in conventional medical microbiology laboratories. J Clin Microbiol [Internet]. 2010 Mar [cited 2025 May 11];48(3):900–7. Available from: https://pubmed.ncbi.nlm.nih.gov/20053859/. [CrossRef]
- Nguyen MH, Wissel MC, Shields RK, Salomoni MA, Hao B, Press EG, et al. Performance of candida real-time polymerase chain reaction, β-D-glucan assay, and blood cultures in the diagnosis of invasive candidiasis. Clinical Infectious Diseases. 2012 May 1;54(9):1240–8. [CrossRef]
- Cortés JA, Valderrama-Rios MC, Peçanha-Pietrobom PM, Júnior MS, Diaz-Brochero C, Robles-Torres RR, et al. Evidence-based clinical standard for the diagnosis and treatment of candidemia in critically ill patients in the intensive care unit. The Brazilian Journal of Infectious Diseases [Internet]. 2024 [cited 2025 May 11];29(1):104495. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC11846572/. [CrossRef]
- Avni T, Leibovici L, Paul M. PCR diagnosis of invasive candidiasis: Systematic review and meta-analysis. J Clin Microbiol [Internet]. 2011 Feb [cited 2025 May 11];49(2):665–70. Available from: https://pubmed.ncbi.nlm.nih.gov/21106797/. [CrossRef]
- Nieto M, Robles JC, Causse M, Gutiérrez L, Cruz Perez M, Ferrer R, et al. Polymerase Chain Reaction Versus Blood Culture to Detect Candida Species in High-Risk Patients with Suspected Invasive Candidiasis: The MICAFEM Study. Infect Dis Ther [Internet]. 2019 Sep 1 [cited 2025 May 11];8(3):429–44. Available from: https://link-springer-com.ez.urosario.edu.co/article/10.1007/s40121-019-0248-z. [CrossRef]
- Tang DL, Chen X, Zhu CG, Li ZW, Xia Y, Guo XG. Pooled analysis of T2 Candida for rapid diagnosis of candidiasis. BMC Infect Dis [Internet]. 2019 Sep 11 [cited 2025 May 11];19(1):1–8. Available from: https://bmcinfectdis.biomedcentral.com/articles/10.1186/s12879-019-4419-z. [CrossRef]
- Monday LM, Acosta TP, Alangaden G. T2Candida for the Diagnosis and Management of Invasive Candida Infections. Journal of Fungi 2021, Vol 7, Page 178 [Internet]. 2021 Mar 3 [cited 2025 May 11];7(3):178. Available from: https://www.mdpi.com/2309-608X/7/3/178/htm. [CrossRef]
- Mallick DC, Kaushik N, Goyal L, Mallick L, Singh P. A Comprehensive Review of Candidemia and Invasive Candidiasis in Adults: Focus on the Emerging Multidrug-Resistant Fungus Candida auris. Diseases [Internet]. 2025 Mar 24 [cited 2025 May 9];13(4). Available from: http://www.ncbi.nlm.nih.gov/pubmed/40277804. [CrossRef]
- Sexton DJ, Bentz ML, Welsh RM, Litvintseva AP. Evaluation of a new T2 Magnetic Resonance assay for rapid detection of emergent fungal pathogen Candida auris on clinical skin swab samples. Mycoses [Internet]. 2018 Oct 1 [cited 2025 May 11];61(10):786–90. Available from: https://pubmed.ncbi.nlm.nih.gov/29938838/. [CrossRef]
- Sexton DJ, Bentz ML, Welsh RM, Litvintseva AP. Evaluation of a new T2 Magnetic Resonance assay for rapid detection of emergent fungal pathogen Candida auris on clinical skin swab samples. Mycoses [Internet]. 2018 Oct 1 [cited 2025 May 11];61(10):786–90. Available from: /doi/pdf/10.1111/myc.12817. [CrossRef]
- Mikulska M, Calandra T, Sanguinetti M, Poulain D, Viscoli C. The use of mannan antigen and anti-mannan antibodies in the diagnosis of invasive candidiasis: recommendations from the Third European Conference on Infections in Leukemia. Crit Care [Internet]. 2010 Dec 8 [cited 2025 May 11];14(6):R222. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC3219989/. [CrossRef]
- Falci DR, Pasqualotto AC. Clinical mycology in Latin America and the Caribbean: A snapshot of diagnostic and therapeutic capabilities. Mycoses [Internet]. 2019 Apr 1 [cited 2025 May 11];62(4):368–73. Available from: /doi/pdf/10.1111/myc.12890. [CrossRef]
- Riera F, Caeiro JP, Cornely OA, Salmanton-García J, Reyes NDA, Morales A, et al. The Argentinian landscape of mycological diagnostic capacity and treatment accessibility. Med Mycol [Internet]. 2023 Jun 5 [cited 2025 May 11];61(6):58. Available from: https://dx-doi-org.ez.urosario.edu.co/10.1093/mmy/myad058. [CrossRef]
- Cortés JA, Reyes P, Gómez CH, Cuervo SI, Rivas P, Casas CA, et al. Clinical and epidemiological characteristics and risk factors for mortality in patients with candidemia in hospitals from Bogotá, Colombia. Brazilian Journal of Infectious Diseases [Internet]. 2014 [cited 2025 May 1];18(6):631–7. Available from: https://pubmed.ncbi.nlm.nih.gov/25181401/. [CrossRef]
- Alvarez-Moreno CA, Cortes JA, Denning DW. Burden of fungal infections in Colombia. Journal of Fungi [Internet]. 2018 Jun 1 [cited 2025 Jun 11];4(2). Available from: https://pubmed.ncbi.nlm.nih.gov/29561795/. [CrossRef]
- Garcia-Bustos V, Cabanero-Navalon MD, Ruiz-Saurí A, Ruiz-Gaitán AC, Salavert M, Tormo M, et al. What do we know about candida auris? State of the art, knowledge gaps, and future directions. Microorganisms [Internet]. 2021 Oct 1 [cited 2025 May 8];9(10). Available from: https://pubmed.ncbi.nlm.nih.gov/34683498/. [CrossRef]
- Escandón P, Cáceres DH, Lizarazo D, Lockhart SR, Lyman M, Duarte C. Laboratory-based surveillance of Candida auris in Colombia, 2016–2020. Mycoses. 2022 Feb 1;65(2):222–5. [CrossRef]
- Escandón P, Lockhart SR, Chow NA, Chiller TM. Candida auris: a global pathogen that has taken root in Colombia. Biomédica [Internet]. 2023 [cited 2025 May 4];43(Suppl 1):278. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC10599714/. [CrossRef]
- Escandón P, Lockhart SR, Chow NA, Chiller TM. Candida auris: a global pathogen that has taken root in Colombia. Biomédica [Internet]. 2023 [cited 2025 Apr 29];43(Suppl 1):278. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC10599714/. [CrossRef]
- Escandón P, Chow NA, Caceres DH, Gade L, Berkow EL, Armstrong P, et al. Molecular Epidemiology of Candida auris in Colombia Reveals a Highly Related, Countrywide Colonization With Regional Patterns in Amphotericin B Resistance. Clinical Infectious Diseases [Internet]. 2019 Jan 1 [cited 2025 May 5];68(1):15–21. Available from: https://dx.doi.org/10.1093/cid/ciy411. [CrossRef]
- Lanna M, Lovatto J, de Almeida JN, Medeiros EA, Colombo AL, García-Effron G. Epidemiological and Microbiological aspects of Candidozyma auris (Candida auris) in Latin America: A literature review. Journal of Medical Mycology [Internet]. 2025 Jun 1 [cited 2025 May 4];35(2). Available from: https://pubmed.ncbi.nlm.nih.gov/40215876/. [CrossRef]
- Martinez-Parada I, Agudelo-Quintero E, Prado-Molina DG, Serna-Trejos JS. Current situation of Candida auris in Colombia, 2021. Anales de la Facultad de Medicina. 2021;82(3):242–3. [CrossRef]
- Zuluaga Rodríguez A, de Bedout Gómez C, Agudelo Restrepo CA, Hurtado Parra H, Arango Arteaga M, Restrepo Moreno Á, et al. Sensibilidad a fluconazol y voriconazol de especies de Candida aisladas de pacientes provenientes de unidades de cuidados intensivos en Medellín, Colombia (2001–2007). Rev Iberoam Micol [Internet]. 2010 Jul 1 [cited 2025 May 1];27(3):125–9. Available from: https://www.elsevier.es/es-revista-revista-iberoamericana-micologia-290-articulo-sensibilidad-fluconazol-voriconazol-especies-candida-S1130140610000616. [CrossRef]
- Colombo AL, Cortes JA, Zurita J, Guzman-Blanco M, Alvarado Matute T, de Queiroz Telles F, et al. Recommendations for the diagnosis of candidemia in Latin America. Rev Iberoam Micol [Internet]. 2013 Jul 1 [cited 2025 May 11];30(3):150–7. Available from: https://www.elsevier.es/es-revista-revista-iberoamericana-micologia-290-articulo-recommendations-for-diagnosis-candidemia-in-S1130140613000533. [CrossRef]
- Govrins M, Lass-Flörl C. Candida parapsilosis complex in the clinical setting. Nature Reviews Microbiology 2023 22:1 [Internet]. 2023 Sep 6 [cited 2025 May 12];22(1):46–59. Available from: https://www.nature.com/articles/s41579-023-00961-8. [CrossRef]
- Govender NP, Patel J, Magobo RE, Naicker S, Wadula J, Whitelaw A, et al. Emergence of azole-resistant Candida parapsilosis causing bloodstream infection: Results from laboratory-based sentinel surveillance in South Africa. Journal of Antimicrobial Chemotherapy [Internet]. 2016 Jul 1 [cited 2025 May 12];71(7):1994–2004. Available from: https://pubmed.ncbi.nlm.nih.gov/27125552/. [CrossRef]
- Corzo-Leon DE, Peacock M, Rodriguez-Zulueta P, Salazar-Tamayo GJ, MacCallum DM. General hospital outbreak of invasive candidiasis due to azole-resistant Candida parapsilosis associated with an Erg11 Y132F mutation. Med Mycol [Internet]. 2021 Jul 1 [cited 2025 May 12];59(7):664–71. Available from: https://pubmed.ncbi.nlm.nih.gov/33305313/. [CrossRef]
- Ceballos-Garzon A, Peñuela A, Valderrama-Beltrán S, Vargas-Casanova Y, Ariza B, Parra-Giraldo CM. Emergence and circulation of azole-resistant C. albicans, C. auris and C. parapsilosis bloodstream isolates carrying Y132F, K143R or T220L Erg11p substitutions in Colombia. Front Cell Infect Microbiol [Internet]. 2023 [cited 2025 May 12];13. Available from: https://pubmed.ncbi.nlm.nih.gov/37026059/. [CrossRef]
- Franconi I, Rizzato C, Poma N, Tavanti A, Lupetti A. Candida parapsilosis sensu stricto Antifungal Resistance Mechanisms and Associated Epidemiology. Journal of Fungi [Internet]. 2023 Aug 1 [cited 2025 May 12];9(8):798. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC10456088/. [CrossRef]
- Ning Y, Xiao M, Perlin DS, Zhao Y, Lu M, Li Y, et al. Decreased echinocandin susceptibility in Candida parapsilosis causing candidemia and emergence of a pan-echinocandin resistant case in China. Emerg Microbes Infect [Internet]. 2023 [cited 2025 May 12];12(1). Available from: https://www.tandfonline.com/doi/pdf/10.1080/22221751.2022.2153086. [CrossRef]
- Daneshnia F, de Almeida Júnior JN, Ilkit M, Lombardi L, Perry AM, Gao M, et al. Worldwide emergence of fluconazole-resistant Candida parapsilosis: current framework and future research roadmap. Lancet Microbe [Internet]. 2023 Jun 1 [cited 2025 May 12];4(6):e470–80. Available from: https://pubmed.ncbi.nlm.nih.gov/37121240/. [CrossRef]
- Favarello LM, Nucci M, Queiroz-Telles F, Guimarães T, Salles MJ, Sukiennik TCT, et al. Trends towards lower azole susceptibility among 200 Candida tropicalis bloodstream isolates from Brazilian medical centres. J Glob Antimicrob Resist [Internet]. 2021 Jun 1 [cited 2025 May 12];25:199–201. Available from: https://pubmed.ncbi.nlm.nih.gov/33812048/. [CrossRef]
- Spruijtenburg B, Baqueiro CCSZ, Colombo AL, Meijer EFJ, de Almeida JN, Berrio I, et al. Short Tandem Repeat Genotyping and Antifungal Susceptibility Testing of Latin American Candida tropicalis Isolates. Journal of Fungi [Internet]. 2023 Feb 1 [cited 2025 May 12];9(2):207. Available from: https://www.mdpi.com/2309-608X/9/2/207/htm. [CrossRef]
- Martínez-Herrera E, Frías-De-león MG, Hernández-Castro R, García-Salazar E, Arenas R, Ocharan-Hernández E, et al. Antifungal Resistance in Clinical Isolates of Candida glabrata in Ibero-America. Journal of Fungi 2022, Vol 8, Page 14 [Internet]. 2021 Dec 26 [cited 2025 May 12];8(1):14. Available from: https://www.mdpi.com/2309-608X/8/1/14/htm. [CrossRef]
- Colombo AL, Garnica M, Aranha Camargo LF, Da Cunha CA, Bandeira AC, Borghi D, et al. Candida glabrata: An emerging pathogen in Brazilian tertiary care hospitals. Med Mycol [Internet]. 2013 [cited 2025 Jun 17];51(1):38–44. Available from: https://pubmed.ncbi.nlm.nih.gov/22762208/. [CrossRef]
- Nguyen TA, Kim HY, Stocker S, Kidd S, Alastruey-Izquierdo A, Dao A, et al. Pichia kudriavzevii (Candida krusei): A systematic review to inform the World Health Organisation priority list of fungal pathogens. Med Mycol [Internet]. 2024 Jun 1 [cited 2025 Jun 17];62(6). Available from: https://pubmed.ncbi.nlm.nih.gov/38935911/. [CrossRef]
- Nguyen TA, Kim HY, Stocker S, Kidd S, Alastruey-Izquierdo A, Dao A, et al. Pichia kudriavzevii (Candida krusei): A systematic review to inform the World Health Organisation priority list of fungal pathogens. Med Mycol [Internet]. 2024 Jun 1 [cited 2025 May 12];62(6):myad132. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC11210618/. [CrossRef]
- Françoiseid U, Desnos-Ollivier M, Govic Y Le, Sitbon K, Valentino R, Peugny S, et al. Candida haemulonii complex, an emerging threat from tropical regions? PLoS Negl Trop Dis [Internet]. 2023 Jul 1 [cited 2025 May 12];17(7):e0011453. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC10437918/. [CrossRef]
- de Almeida JN, Assy JGPL, Levin AS, del Negro GMB, Giudice MC, Tringoni MP, et al. Candida haemulonii Complex Species, Brazil, January 2010–March 2015 - Volume 22, Number 3—March 2016 - Emerging Infectious Diseases journal - CDC. Emerg Infect Dis [Internet]. 2016 Mar 1 [cited 2025 May 12];22(3):561–3. Available from: https://wwwnc.cdc.gov/eid/article/22/3/15-1610_article. [CrossRef]
- Ghasemi R, Lotfali E, Rezaei K, Madinehzad SA, Tafti MF, Aliabadi N, et al. Meyerozyma guilliermondii species complex: review of current epidemiology, antifungal resistance, and mechanisms. Brazilian Journal of Microbiology [Internet]. 2022 Dec 1 [cited 2025 May 12];53(4):1761. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC9679122/. [CrossRef]
- Pfaller MA, Diekema DJ, Colombo AL, Kibbler C, Ng KP, Gibbs DL, et al. Candida rugosa, an Emerging Fungal Pathogen with Resistance to Azoles: Geographic and Temporal Trends from the ARTEMIS DISK Antifungal Surveillance Program. J Clin Microbiol [Internet]. 2006 Oct 1 [cited 2025 May 12];44(10):3578. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC1594768/. [CrossRef]
- Misas E, Escandón PL, Gade L, Caceres DH, Hurst S, Le N, et al. Genomic epidemiology and antifungal-resistant characterization of Candida auris , Colombia, 2016–2021 . mSphere [Internet]. 2024 Feb 28 [cited 2025 May 5];9(2). Available from: https://pubmed.ncbi.nlm.nih.gov/38299868/. [CrossRef]
- Chow NA, Muñoz JF, Gade L, Berkow EL, Li X, Welsh RM, et al. Tracing the evolutionary history and global expansion of candida auris using population genomic analyses. mBio [Internet]. 2020 Mar 1 [cited 2025 May 5];11(2). Available from: https://pubmed.ncbi.nlm.nih.gov/32345637/. [CrossRef]
- Sabino R, Veríssimo C, Pereira ÁA, Antunes F. Candida auris, an agent of hospital-associated outbreaks: Which challenging issues do we need to have in mind? Microorganisms [Internet]. 2020 Feb 1 [cited 2025 May 8];8(2). Available from: https://pubmed.ncbi.nlm.nih.gov/32012865/. [CrossRef]
- Casadevall A, Kontoyiannis DP, Robert V. On the emergence of candida auris: climate change, azoles, swamps, and birds. mBio. 2019;10(4). [CrossRef]
- Escandón P. Novel Environmental Niches for Candida auris: Isolation from a Coastal Habitat in Colombia. Journal of Fungi 2022, Vol 8, Page 748 [Internet]. 2022 Jul 19 [cited 2025 May 4];8(7):748. Available from: https://www.mdpi.com/2309-608X/8/7/748/htm. [CrossRef]
- Lanna M, Lovatto J, de Almeida JN, Medeiros EA, Colombo AL, García-Effron G. Epidemiological and Microbiological aspects of Candidozyma auris (Candida auris) in Latin America: A literature review. Journal of Medical Mycology [Internet]. 2025 Jun 1 [cited 2025 May 1];35(2):101546. Available from: https://www-sciencedirect-com.ez.urosario.edu.co/science/article/pii/S1156523325000150?utm_source=chatgpt.com. [CrossRef]
- Du H, Bing J, Hu T, Ennis CL, Nobile CJ, Huang G. Candida auris: Epidemiology, biology, antifungal resistance, and virulence. PLoS Pathog. 2020 Oct 22;16(10). [CrossRef]
- Frías-De-León MG, García-Salazar E, Reyes-Montes M del R, Duarte-Escalante E, Acosta-Altamirano G. Opportunistic Yeast Infections and Climate Change: The Emergence of Candida auris. 2022 [cited 2025 May 8];161–79. Available from: https://link.springer.com/chapter/10.1007/978-3-030-89664-5_10. [CrossRef]
- Patricia Escandón, Carolina Duarte, Sandra Rivera. Alerta por emergencia global de infecciones invasivas causadas por la levadura multirresistente, Candida auris [Internet]. Bogota; [cited 2025 Jun 15]. Available from: https://www.ins.gov.co/buscador-eventos/Informacin%20de%20laboratorio/Alerta-por%20emergencia-Candida%20auris-Colombia.pdf.
- Clara-Noguera M, Orozco S, Lizarazo D, Escandón P, Clara-Noguera M, Orozco S, et al. Prevalencia de Candida auris en departamentos de Colombia durante la vigilancia por el laboratorio (2018-2021). Infectio [Internet]. 2024 [cited 2025 Jun 15];28(4):241–5. Available from: http://www.scielo.org.co/scielo.php?script=sci_arttext&pid=S0123-93922024000400241&lng=en&nrm=iso&tlng=es. [CrossRef]
- Naz S, Fatima Z, Iqbal P, Khan A, Zakir I, Ullah H, et al. An introduction to climate change phenomenon. Building Climate Resilience in Agriculture: Theory, Practice and Future Perspective. 2021 Oct 21;3–16.
- Jaramillo A, Mendoza-Ponce A. Climate Change Overview. 2022 [cited 2025 May 8];1–18. Available from: https://link-springer-com.ez.urosario.edu.co/chapter/10.1007/978-3-030-89664-5_1.
- Sedik S, Egger M, Hoenigl M. Climate Change and Medical Mycology. Infect Dis Clin North Am [Internet]. 2024 Mar 1 [cited 2025 May 8];39(1). Available from: https://pubmed.ncbi.nlm.nih.gov/39701899/. [CrossRef]
- Van Rhijn N, Bromley M. The consequences of our changing environment on life threatening and debilitating fungal diseases in humans. Journal of Fungi [Internet]. 2021 [cited 2025 May 8];7(5). Available from: https://pubmed.ncbi.nlm.nih.gov/34067211/. [CrossRef]
- Seidel D, Wurster S, Jenks JD, Sati H, Gangneux JP, Egger M, et al. Impact of climate change and natural disasters on fungal infections. Lancet Microbe [Internet]. 2024 Jun 1 [cited 2025 May 8];5(6):e594–605. Available from: https://www.thelancet.com/action/showFullText?pii=S2666524724000399. [CrossRef]
- Sharma C, Kadosh D. Perspective on the origin, resistance, and spread of the emerging human fungal pathogen Candida auris. PLoS Pathog [Internet]. 2023 Mar 1 [cited 2025 May 8];19(3 March). Available from: https://pubmed.ncbi.nlm.nih.gov/36952448/. [CrossRef]
- Misseri G, Ippolito M, Cortegiani A. Global warming “heating up” the ICU through Candida auris infections: The climate changes theory. Crit Care. 2019 Dec 19;23(1). [CrossRef]
- Van Rhijn N, Bromley M. The consequences of our changing environment on life threatening and debilitating fungal diseases in humans. Journal of Fungi. 2021;7(5). [CrossRef]
- Garcia-Bustos V, Cabanero-Navalon MD, Ruiz-Saurí A, Ruiz-Gaitán AC, Salavert M, Tormo M, et al. What do we know about candida auris? State of the art, knowledge gaps, and future directions. Microorganisms [Internet]. 2021 Oct 1 [cited 2025 May 5];9(10). Available from: https://pubmed.ncbi.nlm.nih.gov/34683498/. [CrossRef]
- Garcia-Bustos V, Cabañero-Navalon MD, Ruiz-Gaitán A, Salavert M, Tormo-Mas MÁ, Pemán J. Climate change, animals, and Candida auris: insights into the ecological niche of a new species from a One Health approach. Clinical Microbiology and Infection [Internet]. 2023 Jul 1 [cited 2025 May 8];29(7):858–62. Available from: https://pubmed.ncbi.nlm.nih.gov/36934871/. [CrossRef]
- Salazar-Hamm P, Torres-Cruz TJ. The Impact of Climate Change on Human Fungal Pathogen Distribution and Disease Incidence. Curr Clin Microbiol Rep [Internet]. 2024 Sep 1 [cited 2025 May 8];11(3):140–52. Available from: https://link-springer-com.ez.urosario.edu.co/article/10.1007/s40588-024-00224-x. [CrossRef]
- George ME, Gaitor TT, Cluck DB, Henao-Martínez AF, Sells NR, Chastain DB. The impact of climate change on the epidemiology of fungal infections: implications for diagnosis, treatment, and public health strategies. Ther Adv Infect Dis [Internet]. 2025 [cited 2025 May 8];12:20499361251313840. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC11815821/. [CrossRef]
- Seidel D, Wurster S, Jenks JD, Sati H, Gangneux JP, Egger M, et al. Impact of climate change and natural disasters on fungal infections. Lancet Microbe [Internet]. 2024 Jun 1 [cited 2025 May 8];5(6):e594–605. Available from: https://pubmed.ncbi.nlm.nih.gov/38518791/. [CrossRef]
- Chakrabarti A, Sood P. On the emergence, spread and resistance of Candida auris: Host, pathogen and environmental tipping points. J Med Microbiol [Internet]. 2021 Feb 18 [cited 2025 May 8];70(3). Available from: https://pubmed.ncbi.nlm.nih.gov/33599604/. [CrossRef]
- Casadevall A, Kontoyiannis DP, Robert V. On the emergence of candida auris: climate change, azoles, swamps, and birds. mBio [Internet]. 2019 [cited 2025 May 8];10(4). Available from: https://pubmed.ncbi.nlm.nih.gov/31337723/. [CrossRef]
- Colombo AL, Garnica M, Aranha Camargo LF, Da Cunha CA, Bandeira AC, Borghi D, et al. Candida glabrata: An emerging pathogen in Brazilian tertiary care hospitals. Med Mycol [Internet]. 2013 [cited 2025 May 8];51(1):38–44. Available from: https://pubmed.ncbi.nlm.nih.gov/22762208/. [CrossRef]
- Kneale M, Bartholomew JS, Davies E, Denning DW. Global access to antifungal therapy and its variable cost. Journal of Antimicrobial Chemotherapy [Internet]. 2016 Dec 1 [cited 2025 May 8];71(12):3599–606. Available from: https://pubmed.ncbi.nlm.nih.gov/27516477/. [CrossRef]
- Valladales-Restrepo LF, Ospina-Cano JA, Aristizábal-Carmona BS, López-Caicedo DF, Toro-Londoño M, Gaviria-Mendoza A, et al. Study of Prescription-Indication of Outpatient Systemic Anti-Fungals in a Colombian Population. A Cross-Sectional Study. Antibiotics [Internet]. 2022 Dec 1 [cited 2025 May 8];11(12):1805. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC9774786/. [CrossRef]
- Van Zyl C, Badenhorst M, Hanekom S, Heine M. Unravelling ‘low-resource settings’: a systematic scoping review with qualitative content analysis. BMJ Glob Health [Internet]. 2021 Jun 3 [cited 2025 May 8];6(6):5190. Available from: https://gh.bmj.com/content/6/6/e005190. [CrossRef]
- Laks M, Guerra CM, Miraglia JL, Medeiros EA. Distance learning in antimicrobial stewardship: innovation in medical education. BMC Med Educ [Internet]. 2019 Jun 7 [cited 2025 May 8];19(1):191. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC6555969/. [CrossRef]
- Barteit S, Guzek D, Jahn A, Bärnighausen T, Jorge MM, Neuhann F. Evaluation of e-learning for medical education in low- and middle-income countries: A systematic review. Comput Educ [Internet]. 2020 Feb 1 [cited 2025 May 8];145:103726. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC7291921/. [CrossRef]
- Otero P, Hersh W, Luna D, González Bernaldo De Quirós F. A medical informatics distance-learning course for Latin America: Translation, implementation and evaluation. Methods Inf Med. 2010;49(3):310–5. [CrossRef]
- GAFFI y OPS unen fuerzas para combatir las infecciones causadas por hongos en América Latina y el Caribe - OPS/OMS | Organización Panamericana de la Salud [Internet]. [cited 2025 May 8]. Available from: https://www.paho.org/es/noticias/14-5-2024-gaffi-ops-unen-fuerzas-para-combatir-infecciones-causadas-por-hongos-america.
- De Fátima Dos Santos A, Alves HJ, Nogueira JT, Torres RM, Do Carmo Barros Melo M. Telehealth distance education course in latin America: Analysis of an experience involving 15 countries. Telemedicine and e-Health [Internet]. 2014 Aug 1 [cited 2025 May 8];20(8):736–41. Available from: https://pubmed.ncbi.nlm.nih.gov/24901742/. [CrossRef]
- Jenks JD, Aneke CI, Al-Obaidi MM, Egger M, Garcia L, Gaines T, et al. Race and ethnicity: Risk factors for fungal infections? PLoS Pathog. 2023 Jan 1;19(1). [CrossRef]
- Jenks JD, Prattes J, Wurster S, Sprute R, Seidel D, Oliverio M, et al. Social determinants of health as drivers of fungal disease. EClinicalMedicine [Internet]. 2023 Dec 1 [cited 2025 May 12];66:102325. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC10694587/. [CrossRef]
- Karen del Carmen Morales-Ramírez RASSCPFAFEDERMP. Environmental and Social Determinants Related to Candidiasi. In: Payam Behzadi, editor. Candida albicans - Epidemiology and Treatment [Internet]. Iran: IntechOpen; 2024 [cited 2025 May 12]. p. 1–122. Available from: https://www.intechopen.com/chapters/1180029. [CrossRef]
- Graham H, White PCL. Social determinants and lifestyles: integrating environmental and public health perspectives. Public Health [Internet]. 2016 Dec 1 [cited 2025 May 12];141:270–8. Available from: https://www-sciencedirect-com.ez.urosario.edu.co/science/article/pii/S0033350616302505. [CrossRef]
- Brito-Santos F, Barbosa GG, Trilles L, Nishikawa MM, Wanke B, Meyer W, et al. Environmental Isolation of Cryptococcus gattii VGII from Indoor Dust from Typical Wooden Houses in the Deep Amazonas of the Rio Negro Basin. PLoS One [Internet]. 2015 Feb 17 [cited 2025 May 12];10(2):e0115866. Available from: https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0115866. [CrossRef]
Figure 1.
Distribution of Candida spp. in Latin America. Data are drawn from published studies originating from each country. (17,22,25,26,28–30,32,33,37–41).
Figure 1.
Distribution of Candida spp. in Latin America. Data are drawn from published studies originating from each country. (17,22,25,26,28–30,32,33,37–41).
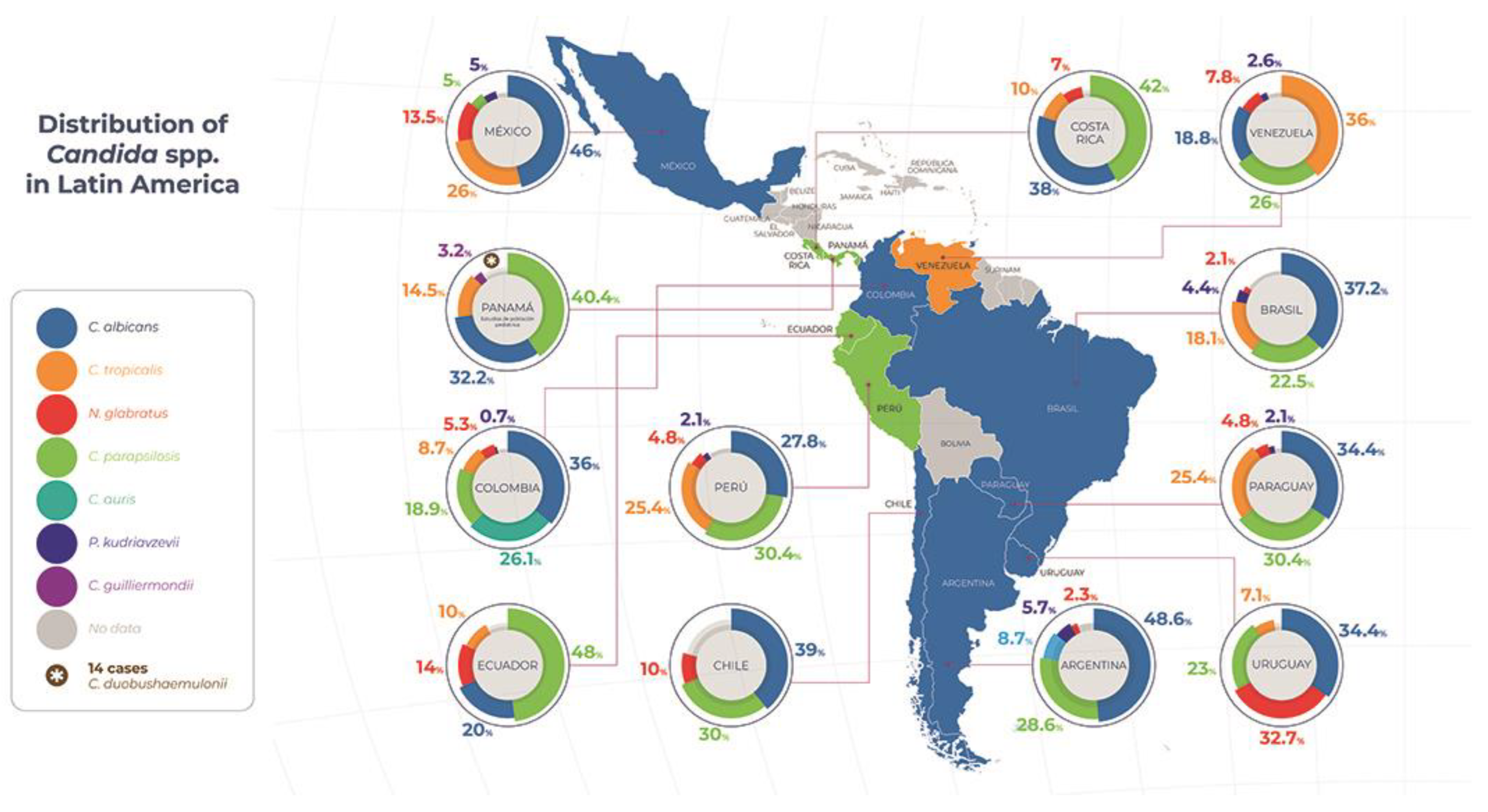
Figure 2.
Environmental and anthropogenic drivers of Candida auris emergence. Climate change promotes thermal adaptation of environmental fungi, while widespread agricultural azole use applies selective pressure that breeds resistant strains capable of invading clinical settings. Wildlife, especially migratory birds, can then passively transport these fungi from natural habitats into rural, urban, and healthcare environments, exemplifying a One Health interplay of human, animal, and environmental factors in the rise of invasive fungal diseases.
Figure 2.
Environmental and anthropogenic drivers of Candida auris emergence. Climate change promotes thermal adaptation of environmental fungi, while widespread agricultural azole use applies selective pressure that breeds resistant strains capable of invading clinical settings. Wildlife, especially migratory birds, can then passively transport these fungi from natural habitats into rural, urban, and healthcare environments, exemplifying a One Health interplay of human, animal, and environmental factors in the rise of invasive fungal diseases.
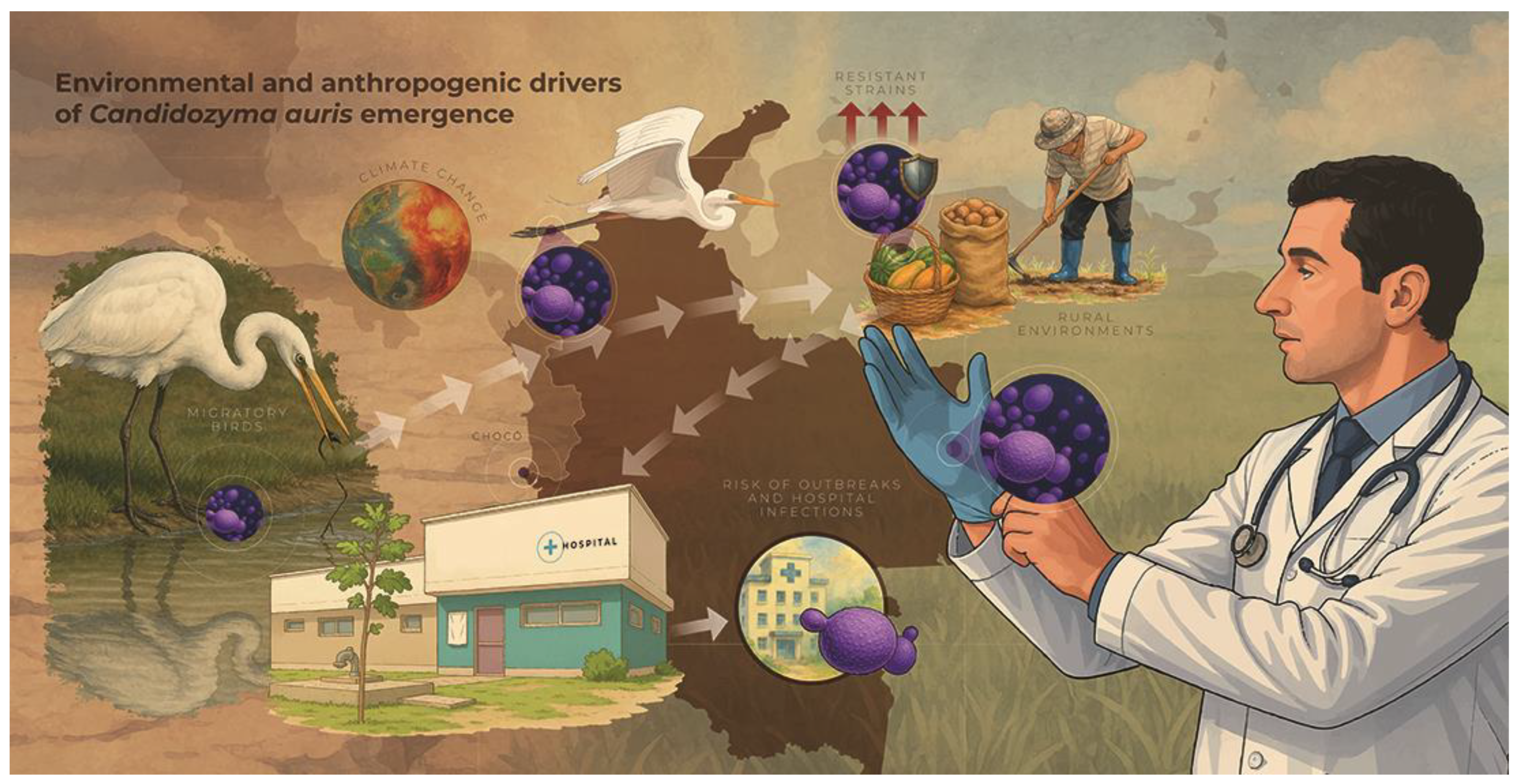

Table 1.
Comparison of diagnostic tests for IC in Latin America.
| Diagnostic method | Main advantages | Main limitations | Availability in Latin America |
|---|---|---|---|
| Blood culture | - Reference standard: isolation, identification, and susceptibility testing | - Prolonged duration (3–4 days) - Moderate sensitivity (21%–71%) |
Widely available in most hospitals |
| 1,3-β-D-glucan (serum) | - High sensitivity for invasive candidiasis (92%) - Useful for ruling out systemic infection |
- Low specificity (positive in other mycoses) - High cost |
Absent in most centers |
| Mannan/Antimannan (serum) | - Allows detection of circulating Candida antigens | - Reduced sensitivity (55%–60%) - Interlaboratory variability |
Very scarce: infrequent clinical use |
| Quantitative PCR (in blood) | - Results in a few hours - Sensitivity 92%; specificity 95% | - Requires reference laboratory and highly trained personnel | Only 20% of centers in Argentina |
| T2Candida (magnetic resonance imaging) | - Direct and rapid detection (3–5 hours) - Sensitivity 91%; specificity 99% |
- Very high cost - Only five specific strains |
Almost unavailable; very limited data |
| MALDI-TOF MS | - Identification of strains in minutes from the culture | - Expensive equipment - Requires previous cultivation |
Available in 20–50% of high-volume laboratories |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



