Submitted:
04 July 2025
Posted:
07 July 2025
You are already at the latest version
Abstract
Background: Lower limb lymphedema (LLL) is a frequent complication after gynecological cancer treatment, with a significant impact on quality of life. Despite the common use of compression therapy in managing established lymphedema, its role in prevention remains insufficiently explored.
Methods: In this prospective randomized study, 64 women treated for gynecological malignancies were assigned to either a compression group (CG) using medium-pressure stockings (23–32 mmHg) or a no-compression group (NCG). All participants received standard education and physical activity guidance. Limb volume, symptom burden, and quality of life were assessed over 12 months.
Results: The incidence of LLL was significantly lower in the CG (3.4%) compared to the NCG (38%, p=0.003). Compression use resulted in significant reductions in limb volume and symptom severity, as well as improved physical functioning. Compliance with compression therapy was high, and patients reported good comfort and usability.
Conclusions: Medium-pressure compression stockings combined with education and physical activity are effective and well-tolerated in preventing LLL following gynecological cancer treatment.
Keywords:
lower limb lymphedema
; gynecological cancer
; compression therapy
; prevention
; quality of life
1. Background
Lower limb lymphedema (LLL) is one of the most disabling and debilitating complications following inguinofemoral lymphadenectomy and pelvic radiotherapy [1]. The reported prevalence of LLL after treatment ranges from 5% to 58% [2]. Although the majority of cases occur within the first year post-treatment, studies have demonstrated that the risk of developing lymphedema persists long-term [3]. Notably, approximately 30% of LLL cases develop ≥10 years after treatment, with the highest incidence observed following vulvar cancer therapy [4].
Gynecological cancer-related lymphedema remains significantly under-recognized and under-treated, partly due to limited awareness among healthcare professionals and patients regarding early diagnosis and management of LLL, and partly due to the lack of standardized evaluation and diagnostic protocols [5]. Limb swelling leads to pain, heaviness, erythema, and a sensation of tightness. It is estimated that 26%–67% of patients with gynecological cancer experience chronic fatigue or tiredness [6]. Fatigue is frequently reported among patients with lower limb lymphedema and interferes with physical functioning and daily activities such as housework, standing, and walking. Women affected by lymphedema are at increased risk of experiencing psychological symptoms including anxiety, depression, sleep disturbances, and fear of cancer recurrence [7], as well as recurrent infections such as dermatolymphadenitis.
Few studies have investigated physiotherapeutic interventions—such as manual lymphatic drainage, exercise programs combined with compression, or health education—for reducing the incidence of lymphedema [8,9,10]. Only a limited number of studies have evaluated the effects of low-pressure compression therapy (class I, 18–21 mmHg) in patients at risk of gynecological cancer-related lymphedema following treatment for malignant genital tumors. These studies suggest that the prophylactic use of compression stockings is both feasible and beneficial in this patient population [11,12]. However, data on the effectiveness of medium-pressure compression devices (23–32 mmHg) in reducing lymphedema incidence remain controversial. Observations from patients treated with inguinal lymphadenectomy for various malignancies have questioned the effectiveness of compression therapy in preventing LLL [13].
The optimal compression pressure for the prevention of lower limb lymphedema (LLL)—one that remains effective while maintaining long-term patient comfort and quality of life—remains a matter of ongoing debate. In particular, there is concern that prolonged use of compression may negatively affect the quality of life of women who have successfully undergone cancer treatment. Therefore, further large-scale studies are warranted to clarify the role of compression therapy in reducing the incidence of LLL.
The aim of this study was to evaluate the effectiveness of medium-pressure compression stockings (23–32 mmHg) in reducing the incidence of lower limb lymphedema and associated symptoms, as well as to assess the comfort and tolerability of compression use over a 12-month follow-up period in women undergoing treatment for gynecological malignancies.
2. Materials and Methods
2.1. Participants
Between 2017 and 2020, a total of 620 patients were evaluated for surgical treatment of gynecological malignancies. Of these, 120 women met the eligibility criteria: age ≥18 years; diagnosis of cervical, uterine, endometrial, ovarian, or vulvar cancer with planned inguinal lymphadenectomy; or a BMI >25.0 kg/m² in cases of endometrial or ovarian cancer, regardless of whether pelvic lymphadenectomy was planned.Exclusion criteria included a history of lymphedema or venous edema, Eastern Cooperative Oncology Group (ECOG) performance status >2, congestive heart failure, renal failure, hypothyroidism, leg ulcers, severe lower limb ischemia (Fontaine class ≥2), metastatic disease or recurrence, and a history of other malignancies treated within five years prior to study enrollment.Seventy-five patients who consented to participate were preoperatively randomized using a simple randomization method (random number generator) into two groups: the compression group (CG), which received compression stockings, and the no compression group (NCG), which received no prophylactic compression. Eleven patients were excluded postoperatively due to various reasons, resulting in a final sample of 64 women (n=32 in CG; n=32 in NCG).
The main reasons for withdrawal from the study included long travel distances, refusal to use compression stockings for 12 months, postoperative complications, and death.
After the 12-month intervention period, data from 60 women were analyzed (29 in CG; 31 in NCG) (Figure 1).
The two groups were comparable with respect to baseline characteristics, including body mass index (BMI), tumor localization, type of surgery, adjuvant therapy, and initial limb volume measurements. (Table 1).
2.2. Intervention
Women in the compression group (CG) were provided with individually fitted, round-knit compression stockings exerting a pressure of 23–32 mmHg (class II, according to the RAL-GZG standard classification). The recommended daily wear time was approximately nine hours. Compression garments were selected based on circumference measurements taken in the morning and were all manufactured by the same company (Medi GmbH & Co. KG, Bayreuth, Germany).
In both groups (CG and NCG), participants were encouraged to engage in regular physical activity, specifically walking for 20 minutes per day. In the CG, physical activity was performed while wearing the compression stockings.
All participants received comprehensive education regarding lymphedema prevention, including skin care, self-administered manual lymphatic drainage (simple lymphatic drainage, SLD), and general lifestyle recommendations. Proper skin hygiene included daily washing with hypoallergenic soap, careful drying—especially between the toes—and routine moisturizing.
A simplified version of manual lymph drainage aimed at stimulating lymph flow in unaffected areas of the body (neck, chest, and abdomen) was recommended for 20 minutes daily. In the CG, SLD was to be performed prior to donning the compression stockings.
2.3. Measurements
Measurements, including limb volume, weight-adjusted volume change (WAC), and disease-related symptoms, were performed preoperatively and at 3, 6, and 12 months postoperatively in both groups.
Limb volume assessment was conducted using circumference measurements taken with a standard measuring tape at 4 cm intervals, starting from the lateral malleolus and extending to the hip joint. Measurements were performed in the morning after at least 15 minutes of rest. Lower leg volume was calculated using the simplified frustum (truncated cone) volume formula [14].
To account for interlimb differences and body weight fluctuations, the weight-adjusted volume change (WAC) formula was additionally applied to quantify lymphedema independently of the contralateral limb [15].
Lymphedema-related symptoms—including pain, heaviness, skin tightness, limb numbness, genital edema, and lymphorrhea—were assessed using a 5-point Likert scale (0 = never, 4 = always).
Compression compliance in the compression group (CG) was evaluated using the International Compression Questionnaire (ICQ), which considered both the functional status prior to compression initiation and the perception of the compression garments after 12 months. Symptom severity prior to compression use was assessed using a numeric rating scale (NRS) from 0 to 10 (0 = no symptoms, 10 = worst possible severity).
Compression comfort was evaluated after 12 months and included parameters such as ease of donning/doffing, sensations immediately after donning and during daily use, ease of clothing over compression garments, and the appearance of the garment. Each domain was scored on a 0–10 NRS scale (0 = not able at all, 10 = completely able), and the scores were summed.
Compression-related side effects (e.g., skin irritation, tenderness, skin lesions, itching, warmth, throbbing, cramping, cutting-in, slippage, localized swelling, bulky sensation, or excessive tightness) were rated on a 0–10 NRS scale (0 = not present at all, 10 = very obvious), with total scores calculated.
Health-related quality of life was assessed using the European Organization for Research and Treatment of Cancer Quality of Life Questionnaire (EORTC QLQ-C30), administered at 12 months postoperatively in both groups.
Subcutaneous edema was evaluated using the pitting test, with a positive result recorded when pressure applied to the skin produced a measurable indentation:
- Grade 1 = 2 mm
- Grade 2 = 3–4 mm
- Grade 3 = 5–6 mm
- Grade 4 = ≥8 mm
Lymphedema diagnosis was confirmed if lower leg volume increased by ≥10% between two subsequent assessments, or by ≥8% in conjunction with a positive pitting sign.
2.4. Statistics
Baseline demographic data were summarized using descriptive statistics: means with standard deviations (SD) for normally distributed variables, and medians with interquartile ranges (IQR) for non-normally distributed ordinal or quantitative variables, as assessed by the Shapiro–Wilk test.
Between-group comparisons for non-normally distributed variables were performed using the Mann–Whitney U test. Within-group comparisons of non-normally distributed variables assessed at two time points were also analyzed using the Mann–Whitney U test. For variables measured more than twice within a single group, the Friedman test was applied, followed by Wilcoxon signed-rank tests with Bonferroni correction for post hoc analysis.
A p-value of <0.05 was considered statistically significant. All statistical analyses were conducted using R statistical software (version 4.2.2, Vienna, Austria).
2.5. The Sample Size
The sample size was determined based on data from a previous pilot study. It was assumed that the incidence of lower limb lymphedema in women treated for reproductive tract malignancies would be approximately 40%. The use of prophylactic compression stockings was expected to reduce the incidence to 5%. Based on these assumptions, and using a type I error (α) of 0.05 and a type II error (β) of 0.20 (power = 80%), the minimum required sample size was calculated to be 42 participants (21 per group).
This study was conducted in accordance with the principles of the Declaration of Helsinki. The research protocol was approved by the Committee of Medical Ethics at the District Medical Chamber in Kraków (Approval No. 5/KBL/OIL/2016).
3. Results
3.1. Limb Volumes and WAC
In the compression group (CG), a reduction in both right and left lower limb volumes was observed at 3, 6, and 12 months postoperatively. In contrast, the no-compression group (NCG) demonstrated an increase in limb volume over the same period. The between-group difference in volume change was statistically significant (p = 0.001).
The incidence of lymphedema was significantly lower in the CG, affecting only 3.4% of participants (1/29), compared to 38.7% (12/31) in the NCG (p = 0.003).
Weight-adjusted volume change (WAC) values were consistently lower in the CG than in the NCG at all assessed time points—3, 6, and 12 months post-surgery (p = 0.001; see Table 2 for details).
Participants diagnosed with lymphedema were excluded from further follow-up assessments in the study.
Median leg volumes (mL) at baseline and 12 months post-surgery are shown in Figure 2. A progressive reduction in LLV was observed in the compression group (CG), while an increase was noted in the non-compression group (NCG).
3.2. The Pitting Test
A positive pitting skin sign was observed in 8 women (27%) from NCG. Of these, 7 patients were classified as grade 1, and 1 patient as grade 2. The onset of this symptom occurred in 2 women at 3 months post-surgery, in 3 women at 6 months, and in 2 women at 12 months.
In 6 of these patients, the lower leg volume increased by 9% and coexisted with a positive pitting sign, suggesting early-stage lymphedema. In all cases, the swelling was localized around the ankles or the distal parts of the lower legs.
In the CG, no positive pitting skin sign was observed at 12 months postoperatively.
3.3. Compliance
Patients in the compression group wore the compression stockings for an average of 6.5 days per week, with a daily wear time of 9 hours (range: 5–12 hours).
Although most participants did not engage in structured sports activities (n = 22), the majority reported being physically active (n = 28). The most common forms of non-sport physical activity included:
- walking more than 1 km per day (n = 27),
- Nordic walking (n = 17),
- cycling (n = 11),
- and gymnastic exercises (n = 9).
Women rated the ease of using compression stockings at an average of 9.6 out of 10. Most patients (n = 27) used assistive tools for donning and doffing, such as:
- rubber gloves (n = 24),
- slippery socks or foot aids (n = 15),
- or assistance from another person (n = 15).
Ability to put on shoes over the stockings was rated at 9.9/10, and ability to dress was rated at 9.8/10.
Comfort of wearing compression stockings was rated at:
- 8.4/10 immediately after donning, and
- 8.6/10 later in the day.
The visual appearance of the stockings received an average score of 8.2/10.
3.4. Health-Related Quality of Life and Disease - Related Symptoms
An improvement in symptoms such as pain, limb heaviness, skin tension, and limb numbness was reported in the compression group (CG) beginning at 3 months postoperatively and persisting thereafter (p = 0.001). In contrast, patients in the no-compression group (NCG) experienced a worsening in the severity of these symptoms over time (Table 3).
Analysis of the EORTC QLQ-C30 questionnaire data revealed no significant differences between the compression group (CG) and the no-compression group (NCG) in global health status, symptom scales, or most functional scales at any assessment point. However, physical functioning was significantly better in the CG 12 months after surgery (p = 0.03) (Table 4).
4. Discussion
Several studies have demonstrated that compression therapy is an effective treatment modality [16,17], and a cost-effective strategy for preventing recurrent cellulitis in patients with chronic edema [18]. However, scientific evidence specifically addressing the prevention of gynecological cancer-related lymphedema remains limited.
Although the beneficial physiological effects of compression therapy on lymphatic function—such as reducing pressure in initial lymphatic vessels, limiting interstitial fluid filtration, enhancing lymphatic reabsorption, stimulating lymphangion contractions, and exerting anti-inflammatory effects via activation of the parasympathetic (vagal) system—have been well documented [19,20,21,22], prophylactic compression-based physiotherapy has not yet been adopted as a standard of care for gynecological cancer survivors.
Most of the current literature on secondary lymphedema prevention has focused on the upper limbs in the context of breast cancer surgery [23,24,25]. In contrast, considerably less is known about the prevention of lower limb lymphedema (LLL) following treatment for gynecologic malignancies. Notably, prospective randomized controlled trials evaluating the long-term effects of postoperative compression therapy—especially when initiated preoperatively and combined with structured exercise—are still lacking in this patient population.
To the best of our knowledge, this is the first prospective randomized study to demonstrate the effectiveness of medium-pressure compression stockings (23–32 mmHg), combined with physical exercise and patient education, administered over a one-year period, in the prevention of early lower limb lymphedema (LLL) in women undergoing gynecological cancer surgery.
Patients in the compression group experienced significant reductions in limb volume and symptom severity compared to the control group, indicating the potential of this multifaceted approach as an effective preventive strategy.
Our findings highlight the importance of early implementation of compression therapy as part of preventive care and stand in contrast to prior studies in this field.
For example, a small pilot study by Sawan et al. involving seven patients with vulvar cancer reported a greater mean increase in leg volume among patients who did not wear compression stockings compared to those who used them for six months; however, the difference was not statistically significant [11].
Similarly, Shallwani et al. found no significant difference in the incidence of clinically diagnosed lymphedema between groups. Nevertheless, the mean leg volume increased more in the control group, and exploratory data suggested a potential delay in lymphedema onset in the intervention group using compression therapy [12].
In contrast, our study demonstrated a significantly lower incidence of lower limb lymphedema: 3.4% (1/29) in the compression group versus 38.7% (12/31) in the control group (p = 0.003). These results suggest that an early, structured intervention combining medium-pressure compression stockings, education, and physical activity may offer substantial preventive benefits for gynecological cancer survivors.
No significant benefit from medium-pressure compression stockings (23–32 mmHg, class II) in the prevention of lower limb lymphedema (LLL) was observed in the study by Stuiver et al. [13]. A major limitation of that study was the heterogeneity of the patient population, which included individuals with melanoma and various urogenital cancers at different stages of clinical progression.
Unexpected findings were also reported by Zhang et al., who found that progressive resistance exercise training (PRET) was more effective than graduated compression stockings (GCS; 15–20 mmHg) in preventing LLL after pelvic lymphadenectomy for cervical cancer [26]. The PRET group had a significantly lower risk of developing lymphedema (p < 0.001), whereas the GCS and control groups showed only a non-significant protective trend. In that study, patients were instructed to wear GCS for at least 23 hours per day, which led to frequent dissatisfaction, especially during summer months, due to symptoms such as pruritus, heat, or blistering. These issues suggest that poor adherence—likely related to discomfort or inappropriate use—may have affected outcomes. Furthermore, the data raise questions about the necessity of continuous 23-hour compression, particularly given that compression is most effective during daytime activity, when lymphatic flow is enhanced by movement.
Similarly, Woods et al. concluded that prophylactic compression stockings did not significantly reduce the development of lymphedema [27]. However, the study lacked reliable data on patient compliance, making it unclear whether compression was used consistently or as prescribed.
Several factors have been identified as contributing to non-adherence with compression therapy, including discomfort, pain, poor fit or aesthetics, difficulty with donning and doffing, and seasonal discomfort related to heat. Environmental factors such as high temperature may also negatively impact patient compliance.
The results of our study contrast with previous research not only in terms of the lower incidence of lymphedema in the compression group, but also with respect to the duration of compression use and high patient compliance. Participants in our study wore compression stockings for an average of 6.5 days per week, 9 hours per day, over a 12-month period, and reported high levels of satisfaction. The extended duration of compression use appears justified, as lymphedema most commonly develops within the first year after oncologic treatment—or even later.
Beyond reducing objective limb volume, compression therapy also alleviated subjective symptoms of lower limb discomfort, contributing to improved perceived quality of life. Importantly, compression use did not exacerbate any symptoms; on the contrary, it significantly reduced the severity of multiple complaints. These findings suggest that compression stockings not only fail to reduce well-being, as sometimes feared, but may in fact enhance certain dimensions of patient comfort and daily functioning.
Health-related quality of life (HRQoL) assessed at 12 months was comparable between the two groups, with the exception of physical functioning, which was significantly better in the compression group. This difference may be explained by greater confidence in engaging in physical activity among compression wearers, who were likely less concerned about triggering lymphedema and more able to maintain regular domestic and daily living tasks.
At present, there is no consensus regarding the optimal method for detecting subclinical or early-stage lymphedema, and diagnostic criteria remain non-standardized. The variability in assessment tools and thresholds used across studies may contribute to delayed intervention and limit the comparability of findings across research settings [5].
Our prospective surveillance model—incorporating circumferential measurements, symptom monitoring, and skin assessments—proved to be both reliable and practical for the early detection of lower limb lymphedema. Circumferential tape measurement was selected as an inexpensive, reproducible, and widely accessible method suitable for routine clinical use [28].
In addition, we utilized the weight-adjusted volume change (WAC) formula, originally developed to quantify arm volume changes in patients following bilateral mastectomy and to identify risk factors for breast cancer-related lymphedema (BCRL) [15]. This method takes into account individual limb volume fluctuations as well as overall body weight changes, offering a more personalized assessment.
In our study, WAC values significantly decreased in the compression group at 12 months post-surgery, further supporting the beneficial effect of medium-pressure compression therapy as part of a preventive strategy.
The use of the weight-adjusted volume change (WAC) formula may be particularly valuable for quantifying gynecological cancer-related lymphedema, especially in patients undergoing bilateral inguinofemoral lymphadenectomy and pelvic radiotherapy. This method offers a sensitive and individualized approach to early detection by accounting for both limb-specific changes and overall body weight fluctuations.
However, the limited number of studies utilizing the WAC formula in this specific patient population makes direct comparison with existing literature challenging. Further research is warranted to validate its clinical utility and to establish standardized thresholds for the early detection and monitoring of lower limb lymphedema in women treated for gynecologic malignancies.
Another important aspect concerns the pressure exerted by compression garments in patients at risk of developing lymphedema. The optimal pressure range for compression stockings in the prevention of lower limb lymphedema (LLL) remains an open question. According to the RAL-GZG standard classification, a pressure range of 23–32 mmHg (medium compression, class II) is considered therapeutic, particularly in the treatment of lymphedema and chronic venous disease [22].
Previous studies have shown that even low-pressure compression (18–21 mmHg) may be effective in preventing upper limb lymphedema in breast cancer survivors [25]; however, this pressure level appears to be insufficient for gynecological cancer survivors, as indicated in the studies by Sawan and Shallwani [11,12]. In healthy women, compression stockings exerting 18–29 mmHg at the ankle and 15–23 mmHg at the calf have been shown to reduce leg edema [29]. Based on these observations, the pressure range of 23–32 mmHg used in our study was considered optimal.
On the one hand, this medium pressure was effective in preventing postoperative swelling and lymphedema. On the other hand, it was also well tolerated and did not negatively impact comfort or quality of life in our patients. Compression may improve fluid balance by reducing capillary filtration and enhancing fluid reabsorption into both the venous and lymphatic systems, yet its role as a risk-reduction strategy for lymphedema remains incompletely understood [30].
Physical exercise may further promote lymphatic drainage and has been shown to be safe for individuals with or at risk of lymphedema. However, current evidence does not confirm a direct effect of exercise alone on reducing limb volume in at-risk patients [31]. Nevertheless, there is broad agreement that physical activity plays a critical role in the health of gynecological cancer survivors. The American College of Sports Medicine recommends exercise as a safe and beneficial intervention during and after cancer treatment. Regular physical activity may improve overall survival, reduce the risk of recurrence, and lower cancer-related mortality [32].
The benefits of exercise in gynecologic cancer survivors have been well documented and include reduced fatigue, improved physical function, better weight management, and enhanced quality of life (QoL) [31,33].
A systematic review and meta-analysis have demonstrated that various forms of exercise—including active, aerobic, and aquatic training—do not exacerbate gynecological cancer-related lymphedema and can therefore be safely recommended for women following treatment for gynecological malignancies [31]. The duration of exercise sessions may vary from 15 to 50 minutes, depending on individual health status and tolerance.
However, there is currently no consensus on whether physical activity should be performed with or without compression garments in patients at risk of developing LLL. Some studies suggest that wearing compression stockings or bandages during exercise may maximize the reduction of lower limb swelling. In fact, this combined approach has been shown to be more effective than compression therapy alone in gynecological cancer survivors with established LLL [34,35].
A synergistic mechanism has been proposed to explain this enhanced effect. When used during exercise, compression garments may improve lymphatic valve function, support lymphatic vessel contractility, promote fluid reabsorption, and limit excess interstitial fluid accumulation [20].
It has been suggested that active limb exercise performed under appropriate compression (20–60 mmHg) may serve as an effective conservative treatment for lymphedema and can be safely implemented as a daily routine [16]. In our study, 20 minutes of daily walking while wearing medium-pressure compression stockings (23–32 mmHg) was shown to be highly beneficial in improving physical function.
This simple, low-cost intervention may represent a practical and effective preventive strategy for gynecological cancer survivors at risk of developing lower limb lymphedema.
Limited evidence also supports the role of health education [36] and the early application of Complex Decongestive Therapy (CDT) [1,9,10] in reducing the incidence of lower limb lymphedema (LLL) in patients following gynecological cancer surgery. According to the consensus of the International Society of Lymphology, CDT is primarily recommended for patients with established lymphedema.
One of the core components of CDT—compression bandaging—has been shown to be highly effective in reducing limb volume, as reported in the study by Wu et al. [1]. However, this method may be less suitable for long-term prophylactic use in at-risk populations, due to its complexity and limited practicality in routine self-management.
Importantly, patient adherence is a key determinant of success in preventive physiotherapy programs. In our study, participants successfully learned proper donning and doffing techniques for compression stockings and were able to perform simplified manual lymphatic drainage (SLD) with relative ease.
The combined strategy of structured health education, regular monitoring, and early compression-based physiotherapy yielded promising outcomes. This integrative approach appears to be both feasible and effective for gynecological cancer survivors at risk of developing lower limb lymphedema.
Limitations and Strengths
One major limitation of our study is the relatively small sample size, which limited the ability to perform subgroup analyses related to specific risk factors for lymphedema development. Additionally, nine patients were excluded after surgical verification—three due to postoperative complications and six due to cancer recurrence or metastasis. Furthermore, two participants withdrew from the study, citing general discomfort, lack of consent for 12-month compression use, or unwillingness to continue participation.
Another limitation is the relatively short follow-up period. Previous research has shown that a substantial proportion of patients develop lower limb lymphedema more than one year postoperatively. Therefore, future studies with longer follow-up durations are needed to evaluate the long-term efficacy of compression therapy combined with health education in gynecological cancer survivors.
Despite these limitations, the study has several important strengths. The use of a homogeneous patient population, along with high adherence to compression therapy—both in terms of correct application and consistent daily use—contributed to the reliability of the findings. Participants also demonstrated regular follow-up attendance, enhancing data completeness.
Moreover, the study offers direct clinical relevance. Its findings suggest a practical, low-cost, and easily implementable strategy for preventing lower limb lymphedema in gynecological cancer survivors—one that may be readily integrated into routine oncologic care.
5. Conclusions
Compression stockings exerting a pressure range of 23–32 mmHg, when combined with regular physical activity and structured health education, represent a safe, well-tolerated, and effective strategy for preventing postsurgical swelling and the development of lower limb lymphedema (LLL) between 3 and 12 months after inguinofemoral lymphadenectomy and pelvic radiotherapy.
Future clinical trials are warranted to further optimize compression protocols and to establish standardized, evidence-based recommendations for the prevention of LLL in at-risk gynecological cancer survivors.
Funding
This research received no external funding. Medi provided class II compression stockings free of charge for the participants in this study.Medi had no role in the study design, data collection, analysis, interpretation, or in the decision to submit the manuscript for publication.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Committee of Medical Ethics at the District Medical Chamber in Kraków (protocol code 5/KBL/OIL/2016).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Acknowledgments
The authors would like to thank all the patients who participated in the study.
Conflicts of Interest
The authors declare no conflict of interest.
Registered ClinicalTrials.gov Identifier: NCT06873984
Andrzej Frycz Modrzewski Krakow University Protocol Record Csplwgm-AFMKU,
Compression Stockings for Lymphedema Prevention in Gynecologic Cancer
Patients,is registered and will be posted on the ClinicalTrials.gov public website.
References
- Wu, X. , Liu Y., Zhu D., Wang F., Ji J., Yan H. Early prevention of complex decongestive therapy and rehabilitation exercise for prevention of lower extremity lymphedema after operation of gynecologic cancer. Asian J. Surg. 2021, 44, 111–115. [Google Scholar] [CrossRef] [PubMed]
- Hayes, S.C. , Janda M., Ward L.C., et al. Lymphedema following gynecological cancer: Results from a prospective, longitudinal cohort study on prevalence, incidence and risk factors. Gynecol. Oncol. 2017, 146, 623–629. [Google Scholar] [CrossRef] [PubMed]
- Yoshihara, M. , Shimono R., Tsuru S., et al. Risk factors for late-onset lower limb lymphedema after gynecological cancer treatment: A multi-institutional retrospective study. Eur. J. Surg. Oncol. 2020, 46, 1334–1338. [Google Scholar] [CrossRef] [PubMed]
- Huang, J. , Yu N., Wang X., Long X. Incidence of lower limb lymphedema after vulvar cancer: A systematic review and meta-analysis. Medicine 2017, 96, e8722. [Google Scholar] [CrossRef]
- Ward, L.C. , Covens A., Thomas E.J., Armer J.M. Lymphedema measurements and associated patient outcomes: Toward standardization. Gynecol. Oncol. 2022, 160, 625–632. [Google Scholar] [CrossRef]
- Hsu, Y.Y. , Liu C.Y., Ho C.L., Hsu K.F. Determinants of quality of life related to lower limb lymphedema in women with gynecological cancer surgery. Asia-Pac. J. Oncol. Nurs. 2023, 10, 100153. [Google Scholar] [CrossRef]
- Bowman, C. , Piedalue K.A., Baydoun M., Carlson L.E. The quality of life and psychosocial implications of cancer-related lower-extremity lymphedema: A systematic review of the literature. J. Clin. Med. 2020, 9, 3200. [Google Scholar] [CrossRef]
- Tümkaya M.N., Seven M. Interventions for prevention and management of gynecological cancer-related lower limb lymphedema: A systematic scoping review. Semin. Oncol. Nurs. 2024, in press. [CrossRef]
- Wang, X. , Ding Y., Cai H.Y., et al. Effectiveness of modified complex decongestive physiotherapy for preventing lower extremity lymphedema after radical surgery for cervical cancer: A randomized controlled trial. Int. J. Gynecol. Cancer 2020, 30, 757–763. [Google Scholar] [CrossRef]
- Daggez, M. , Koyuncu E.G., Kocabaş R., Yener C. Prophylactic complex physiotherapy in gynecologic cancer survivors: Patient-reported outcomes based on a lymphedema questionnaire. Int. J. Gynecol. Cancer 2023, 33, 1928–1933. [Google Scholar] [CrossRef]
- Sawan, S. , Mugnai R., de Barros Lopes A., Hughes A., Edmondson R.J. Lower-limb lymphedema and vulval cancer: Feasibility of prophylactic compression garments and validation of leg volume measurement. Int. J. Gynecol. Cancer 2009, 19, 1649–1654. [Google Scholar] [CrossRef]
- Shallwani, S.M. , Towers A., Newman A., et al. Feasibility of a pilot randomized controlled trial examining a multidimensional intervention in women with gynecological cancer at risk of lymphedema. Curr. Oncol. 2021, 28, 455–470. [Google Scholar] [CrossRef] [PubMed]
- Stuiver, M.M. , de Rooij J.D., Lucas C., et al. No evidence of benefit from class-II compression stockings in the prevention of lower-limb lymphedema after inguinal lymph node dissection: Results of a randomized controlled trial. Lymphology 2013, 46, 120–131. [Google Scholar] [PubMed]
- Sitzia, J. Volume measurement in lymphoedema treatment: Examination of formulae. Eur. J. Cancer Care (Engl.) 1995, 4, 11–16. [Google Scholar] [CrossRef] [PubMed]
- Miller, C.L. , Specht M.C., Horick N., et al. A novel, validated method to quantify breast cancer-related lymphedema (BCRL) following bilateral breast surgery. Lymphology 2013, 46, 64–74. [Google Scholar]
- International Society of Lymphology. The diagnosis and treatment of peripheral lymphedema: 2023 Consensus document of the International Society of Lymphology. Lymphology 2023, 56, 1–25.
- Liu, F. , Liu N.F., Wang L., et al. Treatment of secondary lower limb lymphedema after gynecologic cancer with complex decongestive therapy. Lymphology 2021, 54, 122–132. [Google Scholar]
- Webb, E. , Bissett B., Neeman T., et al. Compression therapy is cost-saving in the prevention of lower limb recurrent cellulitis in patients with chronic edema. Lymphat. Res. Biol. 2023, 21, 160–168. [Google Scholar] [CrossRef]
- Cavezzi, A. , Cornu-Thenard A., Bergan J.J., et al. Compression therapy, autonomic nervous system, and heart rate variability: A narrative review and our preliminary personal experience. Phlebology 2022, 37, 739–753. [Google Scholar] [CrossRef]
- Partsch, H. Compression therapy: Clinical and experimental evidence. Ann. Vasc. Dis. 2012, 5, 416–422. [Google Scholar] [CrossRef]
- King, M. , Deveaux A., White H., Rayson D. Compression garments versus compression bandaging in decongestive lymphatic therapy for breast cancer-related lymphedema: A randomized controlled trial. Support Care Cancer 2012, 20, 1031–1036. [Google Scholar] [CrossRef]
- Rabe, E. , Partsch H., Hafner J., et al. Indications for medical compression stockings in venous and lymphatic disorders: An evidence-based consensus statement. Phlebology 2018, 33, 163–184. [Google Scholar] [CrossRef]
- Keeley, V. The early detection of breast cancer treatment-related lymphedema of the arm. Lymphat. Res. Biol. 2020, 19, 51–55. [Google Scholar] [CrossRef] [PubMed]
- Davies, C. , Levenhagen K., Ryans K., Perdomo M., Gilchrist L. Interventions for breast cancer-related lymphedema: Clinical practice guideline from the academy of oncologic physical therapy of APTA. Phys. Ther. 2020, 100, 1163–1179. [Google Scholar] [CrossRef] [PubMed]
- Ochalek, K. , Gradalski T., Partsch H. Preventing early postoperative arm swelling and lymphedema manifestation by compression sleeves after axillary lymph node interventions in breast cancer patients: A randomized controlled trial. J. Pain Symptom Manage. 2017, 54, 346–354. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J. , Zhou C., Ma Q., Zhang Y., Zhang X. Preventing lower limb lymphedema after pelvic lymphadenectomy with progressive resistance exercise training: A randomized controlled trial. Asia-Pac. J. Oncol. Nurs. 2024, 11, 100333. [Google Scholar] [CrossRef]
- Woods, M. , Ruddell S., Sandsund C., Thomas K., Shaw C. A service development evaluation of retrospective data exploring prophylactic risk-reducing advice for patients with gynecological cancers. J. Gynecol. Surg. 2020, 36, 198–204. [Google Scholar] [CrossRef]
- Sayegh, H.E. , Asdourian M.S., Swaroop M.N., et al. Diagnostic methods, risk factors, prevention, and management of breast cancer-related lymphedema: Past, present, and future directions. Curr. Breast Cancer Rep. 2017, 9, 111–121. [Google Scholar] [CrossRef]
- Sugisawa, R. , Unno N., Saito T., et al. Effects of compression stockings on elevation of leg lymph pumping pressure and improvement of quality of life in healthy female volunteers: A randomized controlled trial. Lymphat. Res. Biol. 2016, 14, 95–103. [Google Scholar] [CrossRef]
- Stout, N. , Partsch H., Szolnoky G., et al. Chronic edema of the lower extremities: International consensus recommendations for compression therapy clinical research trials. Int. Angiol. 2012, 31, 316–329. [Google Scholar]
- Hsu, Y.Y. , Nguyen T.T., Chou Y.J., Ho C.L. Effects of exercise on lower limb lymphedema in gynecologic cancer: A systematic review and meta-analysis. Eur. J. Oncol. Nurs. 2024, 70, 102550. [Google Scholar] [CrossRef]
- Schmitz, K.H. , Courneya K.S., Matthews C., et al. American college of sports medicine roundtable on exercise guidelines for cancer survivors. Med. Sci. Sports Exerc. 2010, 42, 1409–1426. [Google Scholar] [CrossRef]
- Hayes, S.C. , Singh B., Reul-Hirche H., et al. The effect of exercise for the prevention and treatment of cancer-related lymphedema: A systematic review with meta-analysis. Med. Sci. Sports Exerc. 2022, 54, 2136–2147. [Google Scholar] [CrossRef]
- Fukushima, T. , Tsuji T., Sano Y., et al. Immediate effects of active exercise with compression therapy on lower-limb lymphedema. Support Care Cancer 2017, 25, 2603–2610. [Google Scholar] [CrossRef] [PubMed]
- Abe, K. , Tsuji T., Oka A., et al. Postural differences in the immediate effects of active exercise with compression therapy on lower limb lymphedema. Support Care Cancer 2021, 29, 6535–6543. [Google Scholar] [CrossRef] [PubMed]
- Liao, X. , Cao G., Yang L., Wang C., Tian C. Postoperative effectiveness of comprehensive nursing intervention for lymphedema in gynecological cancer: A controlled study. Altern. Ther. Health Med. 2023, 29, 242–247. [Google Scholar]
Figure 1.
Study participants flow chart.
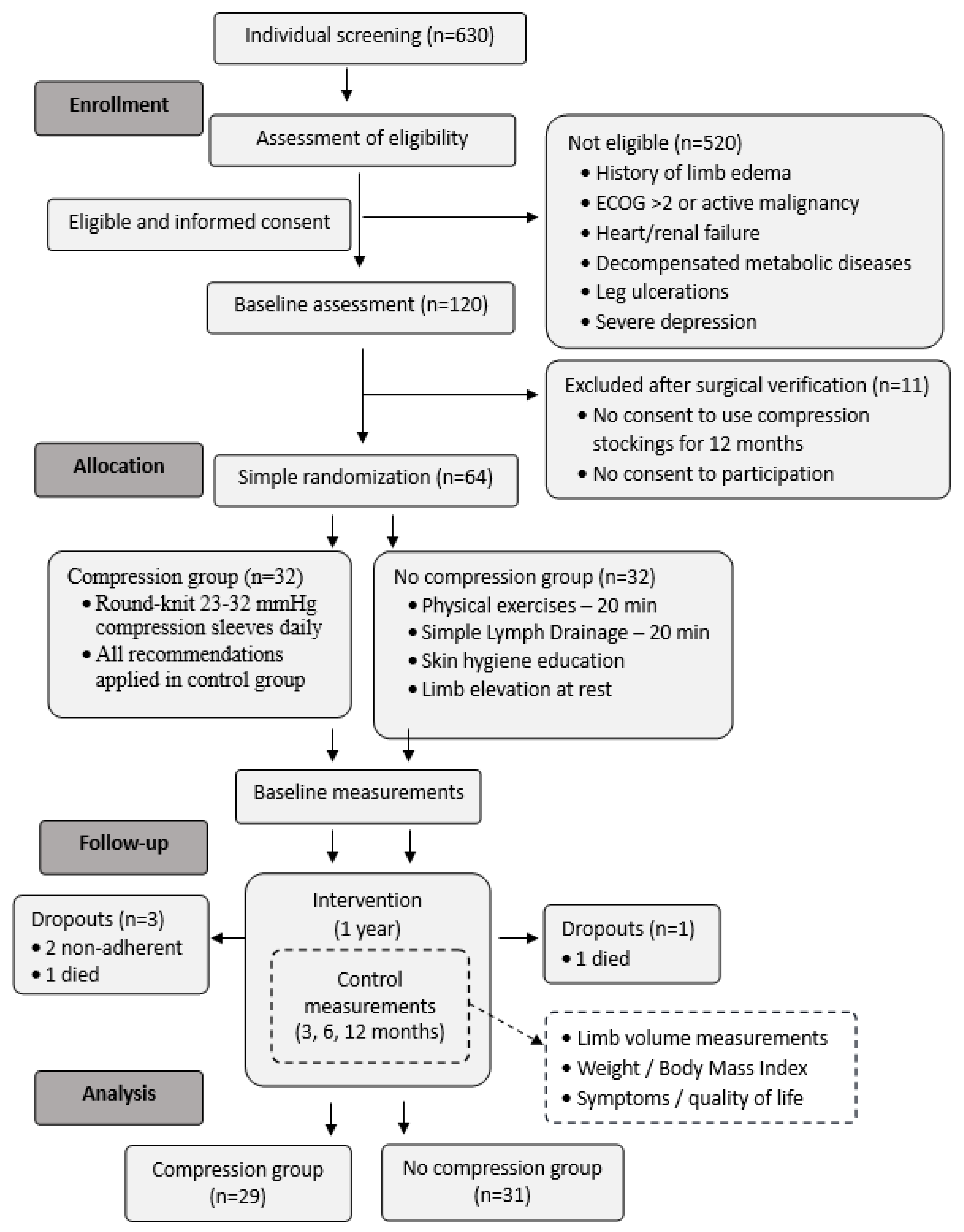
Figure 2.
Median change in lower limb volume (LLV) over time within the analyzed groups.
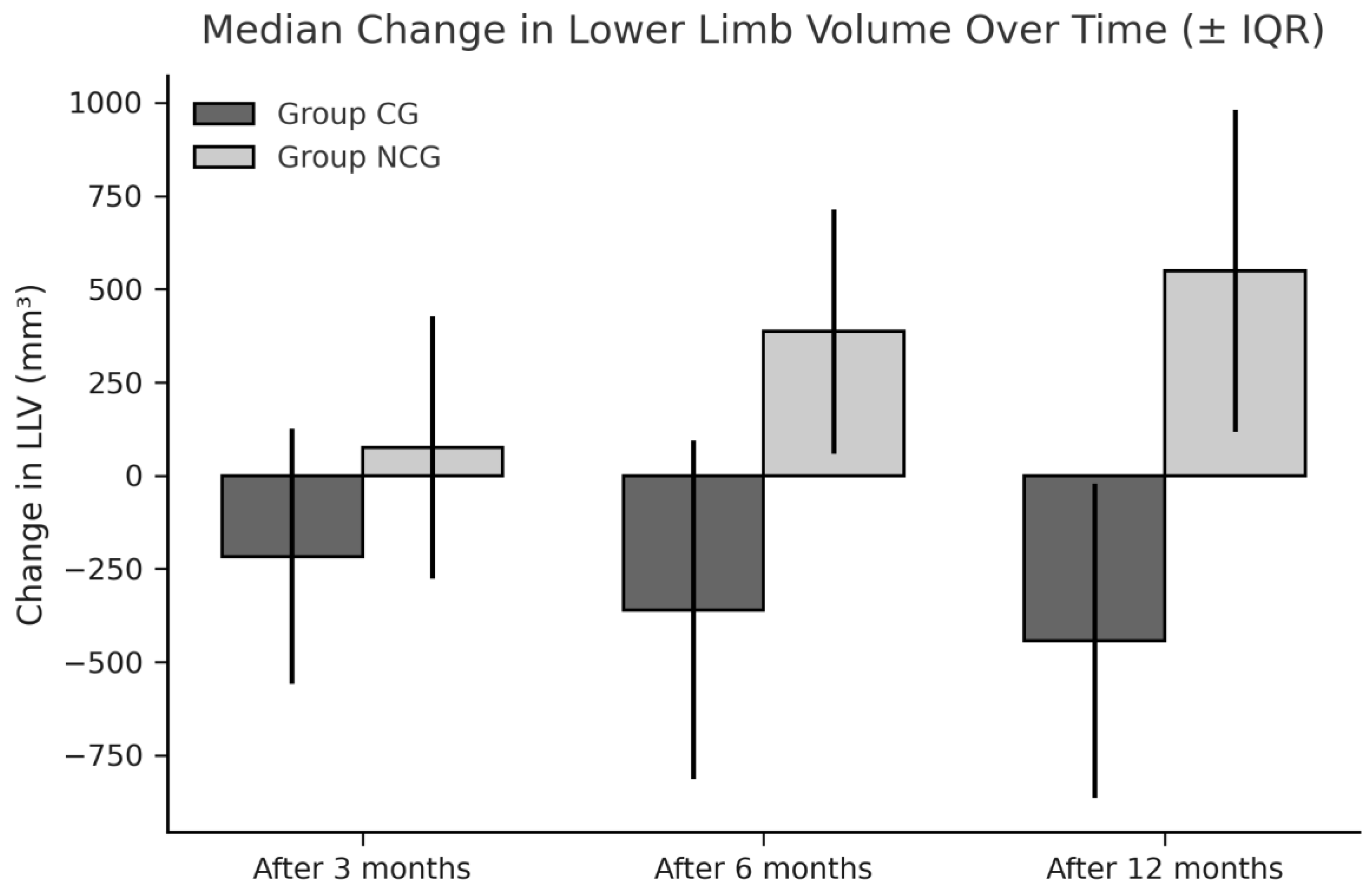

Table 1.
Baseline characteristics of enrolled patients.
| Parameter (n or median, IQR) | CG (n=29) | NCG group (n=31) | P-value |
|---|---|---|---|
| Age (years) | 53.5 (15.25) | 58 (14.0) | 0.06* |
| Height (m) | 1.61 (0.11) | 1.58 (0.09) | 0.3* |
| Weight (kg) | 70.0 (16.5) | 75.0 (19.0) | 0.9* |
| Body mass index (kg/m2) | 26.9 (4.6) | 28.0 (8.6) | 0.5* |
| Professionally active | 19 | 16 | |
| Tumor localization (n) | |||
| Ovaries | 7 | 7 | 0.6** |
| Cervix uteri | 8 | 8 | |
| Corpus uteri | 12 | 15 | |
| Vulva | 2 | 1 | |
| Complementary therapy (n) | |||
| Lymphadenectomy | 29 | 31 | |
| Radiotherapy | 26 | 26 | 0.7** |
| Limb volumes (L) | |||
| ...Right | 8.13 (1.36) | 7.82 (2.28) | 0.8* |
| Left | 8.30 (1.93) | 7.90 (2.17) | 0.9* |
| ...Right and left | 16.60 (3.58) | 15.95 (4.38) | 0.9* |
* Mann-Whitney test; ** Fisher’s exact test; IQR: interquartile range, CG, Compression Group, NCG, No Compression Group.
Table 2.
Edema occurrence and volume changes (mL) within the analyzed groups.
| Parameter (n or median, IQR) | CG (n=29) | NCG (n=31) | P-value |
|---|---|---|---|
| Edema occurrence (n) | 1 | 12 | 0.003* |
| Limb volume changes | |||
| Right limb | |||
| Within 3 months | -86.13 (349.40) | 97.05 (315.27) | 0.049** |
| Within 6 months | -157.33 (480.43) | 193 (836.04) | 0.022** |
| Within 12 months | -259.33 (540.99) | 250.05 (546.81) | 0.001** |
| P-value | 0.01*** | 0.07*** | |
| Left limb | |||
| Within 3 months | -155.66 (285.45) | 36.80 (388.09) | 0.051** |
| Within 6 months | -198.42 (94.43) | 151.37 (384.09) | 0.019** |
| Within 12 months | -137.10 (497.68) | 250.51 (366.36) | 0.002** |
| P-value | 0.011*** | 0.06*** | |
| Right and left limb | |||
| Within 3 months | -216.88 (684.90) | 75.34 (162.36) | 0.032** |
| Within 6 months | -359.81 (375.47) | 386.96 (655.08) | 0.004** |
| Within 12 months | -443.01 (841.88) | 549.07 (861.70) | 0.001** |
| P-value | 0.011*** | 0.011*** | |
| WAC | |||
| Right limb | |||
| Within 3 months | -0.01 (0.04) | 0.02 (0.06) | 0.004** |
| Within 6 months | -0.03 (0.06) | 0.03 (0.02) | 0.003** |
| Within 12 months | -0.06 (0.08) | 0.02 (0.05) | 0.001** |
| P-value | 0.001*** | 0.9*** | |
| Left limb | |||
| Within 3 months | -0.02 (0.05) | 0.01 (0.05) | 0.002** |
| Within 6 months | -0.03 (0.07) | 0.02 (0.05) | 0.003** |
| Within 12 months | -0.05 (0.07) | 0.02 (0.05) | 0.001** |
| P-value | 0.001*** | 0.3*** | |
| Right and left limb | |||
| Within 3 months | -0.02 (0.03) | 0.02 (0.03) | 0.001** |
| Within 6 months | -0.03 (0.05) | 0.02 (0.03) | <0.001** |
| Within 12 months | -0.05 (0.06) | 0.02 (0.04) | <0.001** |
| P-value | 0.001*** | 0.4*** |
* Chi square test; ** Mann-Whitney test; *** Friedman test with post hoc analysis; WAC, weight-adjusted volume change; IQR, interquartile range, CG, Compression Group, NCG, No Compression Group.
Table 3.
Symptom burden within the analyzed groups.
| Problem mean±SD and median(IQR) |
CG (n=29) |
P-value within group** |
NCG (n=31) |
P-value within group** |
P-value between groups* |
|---|---|---|---|---|---|
| Pain within the limbs | |||||
| At baseline | 1.39±0.57 1.0(1.0) | 1.33±0.61 1.0(0.75) | 0.049 | ||
| After 3 months | 1.41±0.57 1.0(1.0) | 1.0 | 1.50±0.63 1.0(1.0) | 0.07 | 0.6 |
| After 6 months | 1.29±0.53 1.0(0.25) | 0.2 | 1.57±0.63 1.5(1.0) | 0.04 | 0.6 |
| After 12 months | 1.32±0.55 1.0(1.0) | 0.5 | 1.59±0.68 1.0 (1.0) | 0.05 | 0.1 |
| Limb heaviness | |||||
| At baseline | 1.26±0.39 1.0(0.5) | 1.23±0.43 1.0 (0.0) | 0.8 | ||
| After 3 months | 1.33±0.48 1.0(1.0) | 0.5 | 1.27±0.52 1.0(0.0) | 0.8 | 0.5 |
| After 6 months | 1.33±0.48 1.0(1.0) | 0.5 | 1.73±0.74 2.0 (1.0) | 0.004 | 0.036 |
| After 12 months | 1.54±0.58 1.5(1.0) | 0.06 | 1.62±0.68 2.0(1.0) | 0.003 | 0.7 |
| Skin tension | |||||
| At baseline | 1.18±0.41 1.0(0.0) | 1.23±0.43 1.0(0.0) | 0.7 | ||
| After 3 months | 1.28±0.46 1.0(1.0) | 0.5 | 1.43±0.50 1.0 (1.0) | 0.04 | 0.3 |
| After 6 months | 1.43±0.57 1.0(1.0) | 0.2 | 1.60±0.67 1.0(1.0) | 0.003 | 0.1 |
| After 12 months | 1.43±0.57 1.0(1.0) | 0.008 | 1.48±0.63 1.0(1.0) | 0.04 | 0.8 |
| Limb numbness | |||||
| At baseline | 1.64±0.68 1.0(1.0) | 1.47±0.5 1.0(1.0) | 0.3 | ||
| After 3 months | 1.46±0.58 1.0(1.0) | 0.09 | 1.70±0.65 2.0(1.0) | 0.02 | 0.2 |
| After 6 months | 1.43±0.50 1.0(1.0) | 0.01 | 1.73±0.64 2.0(1.0) | 0.04 | 0.04 |
| After 12 months | 1.43±0.50 1.0(1.0) | 0.09 | 1.69±0,60 2.0(1.0) | 0.08 | |
| Genital edema | |||||
| At baseline | 1.0±0 1.0(0.0) | 1.0±0.0 1.0(0.0) | 1.0 | ||
| After 3 months | 1.08±0.27 1.0(0.0) | 0.3 | 1.07±0.25 1.0(0.0) | 0.3 | 0.9 |
| After 6 months | 1.0±0 1.0(0.0) | 1.0 | 1.17±-.46 1.0(1.0) | 0.09 | 0.049 |
| After 12 months | 1.0±0 1.0(0.0) | 1.0 | 1.07±0.26 1.0(0.0) | 0.4 | 0.1 |
| Lymphorrhea | |||||
| At baseline | 1.0±0 1.0(0.0) | 1.0±0 1.0(0.0) | 1.0 | ||
| After 3 months | 1.0±0 1.0(0.0) | 1.0 | 1.03±0.18 1.0(0.0) | 1.0 | 0.4 |
| After 6 months | 1.0±0 1.0(0.0) | 1.0 | 1.13±0.43 1.0(0.0) | 0.2 | 0.09 |
| After 12 months | 1.0±0 1.0(0.0) | 1.0 | 1.00±0.00 1.0 (0.0) | 1.0 | 1.0 |
* Mann-Whitney Utest; ** P-value according to the baseline, Wilcoxon paired test; IQR, interquartile range.
Table 4.
Quality of life according to EORTC QLQ-C30 Questionnaire after 12 months.
| Parameter median (IQR) |
CG (n=29) |
NCG (n=31) |
P-value |
|---|---|---|---|
| Global health status | 75 (25.0) | 66.67 (16.67) | 0.3 |
| Physical functioning | 93.33 (13.33) | 86.67 (20.0) | 0.03 |
| Role functioning | 100 (20.83) | 83.33 (16.67) | 0.8 |
| Emotional functioning | 83.33 (25.0) | 75.0 (25.0) | 0.9 |
| Cognitive functioning | 91.67 (33.33) | 83.33 (16.67) | 0.5 |
| Social functioning | 100 (16.67) | 100 (16.67) | 0.9 |
| Fatigue | 22.22 (33.33) | 22.22 (22.22) | 0.5 |
| Nausea and vomiting | 0.0 (0.0) | 0.0 (12.5) | 0.8 |
| Pain | 16.67 (33.3) | 25.0 (33.33) | 0.3 |
| Dyspnea | 0.0 (0.0) | 0.0 (33.33) | 0.2 |
| Insomnia | 33.33 (33.33) | 33.33 (33.33) | 0.9 |
| Appetite loss | 0.0 (0.0) | 0.0 (33.33) | 0.4 |
| Constipation | 16.67 (33.33) | 0.0 (33.33) | 0.4 |
| Diarrhea | 0.0 (0.0) | 0.0 (0.0) | 0.4 |
| Financial difficulties | 0.0 (33.3) | 0.0 (33.3) | 0.6 |
Comparison between the groups (Mann–Whitney U test). IQR, interquartile range; EORTC, European Organization for Research and Treatment of Cancer, CG, Compression Group, NCG, No Compression Group.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



