
Submitted:
30 June 2025
Posted:
01 July 2025
You are already at the latest version
Abstract
Multi-drug resistance (MDR) remains a major health challenge in the cancer treatment, leading to treatment failure and disease recurrence. Recent advancements in nanomedicine have introduced innovative approaches to treat MDR by improving drug delivery, reducing systemic toxicity, and re-sensitizing resistant cancer cells. This review provides a comprehensive summary of various nanocarrier systems that have been developed to bypass drug efflux mechanisms, promote intracellular drug accumulation, and permit controlled release. These nanocarrier systems include liposomes, polymeric nanoparticles, metal-based nanoparticles, and supramolecular constructs. Additionally, we discuss approaches targeting the tumor microenvironment, such as reprogramming tumor-associated macrophages (TAMs), reversing immunosuppression, and manipulating cancer stem cell differentiation. Special attention is paid to co-delivery systems that combine chemotherapeutics with gene therapies, redox-active compounds, autophagy inhibitors, and nitric oxide donors to produce synergistic anticancer effects. Novel strategies such as ferroptosis-inducing nanodrugs, stimuli-responsive platforms, and ultrasonic or photothermic based improved therapies are emphasized for their ability to evade typical resistance pathways. We also go over the important examples where nanotechnology has been utilized to counter MDR specifically in colorectal, ovarian, glioblastoma, and non-small cell lung cancer, targeting mechanisms such as P-glycoprotein overexpression, MRP2 transport, MGMT-mediated repair, and EGFR-TKI resistance. While promising preclinical results highlight the translational potential of nanomedicine for overcoming MDR, clinical integration remains a challenge. Key obstacles include scalable manufacturing, regulatory alignment, and thorough safety validation. This review aims to inform the rational design and clinical translation of nanotechnology-enabled therapeutics for drug-resistant cancers by integrating mechanistic insights with nanoplatform innovation.
Keywords:
nanomedicine
; multidrug resistance
; co-delivery systems
; tumor microenvironment (TME)
; drug efflux inhibition
; stimuli-responsive nanoparticles
; cancer immunotherapy
; siRNA delivery
; ferroptosis
; targeted drug delivery
1. Introduction
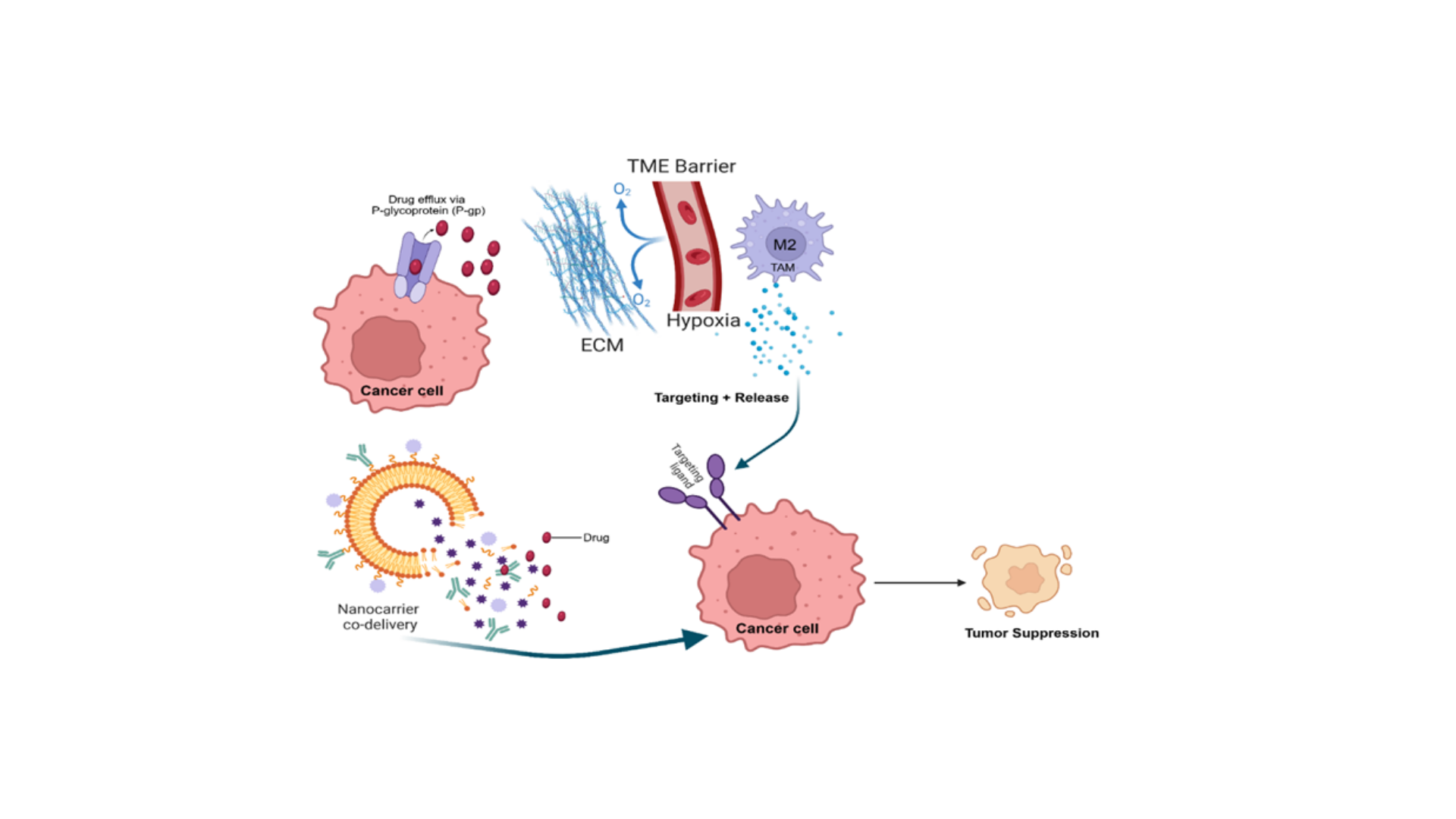
Cancer is a leading cause of global mortality, with ~20 million new cases and 9.7 million deaths in 2022 [1,2,3]. A major obstacle in effective cancer therapy is multidrug resistance (MDR), where tumors become refractory to chemotherapy, targeted agents, or radiation. In fact, up to ~90% of chemotherapy failures are attributed to acquired resistance mechanisms [4,5]. MDR arises from complex biochemical and cellular adaptations that allow cancer cells to evade drug-induced cytotoxicity. These include upregulated drug efflux pumps (e.g. P-glycoprotein), enhanced DNA repair, apoptosis suppression, and influences from the tumor microenvironment (TME) [6,7,8]. Overcoming MDR is critical to improve patient outcomes. In recent years, nanomedicine has emerged as a transformative approach to counter MDR by improving drug delivery and enabling novel combination therapies. The clinical shift toward precision, low-toxicity interventions—such as HPV-HR DNA testing for posttreatment cancer monitoring [9,10] parallels the rise of nanomedicine strategies for overcoming treatment resistance. Engineered nanoparticles (NPs) can preferentially accumulate in tumors via the enhanced permeability and retention (EPR) effect, be surface modified with targeting ligands, and co-encapsulate multiple agents (e.g. a chemotherapeutic plus an MDR modulator or gene therapy) for synergistic action [11,12]. Nanocarriers can also be designed to release cargo in response to tumor-specific stimuli (pH, enzymes, light, ultrasound), and to modulate the TME (e.g. reprogramming macrophages or degrading stroma) [11,13,14]. These properties help to evade efflux pumps, bring back drug sensitivity, and improve antitumor immunity. These capabilities uniquely position nanomedicine as a multifaceted tool to counteract resistance at the molecular, cellular, and microenvironmental levels.
This review provides a comprehensive, up-to-date analysis of the molecular mechanisms underlying MDR in cancer alongside emerging nano-strategies to address them. We begin by discussing the cellular and molecular and biochemical foundation of MDR, including drug efflux transporters, apoptotic evasion, and tumor heterogeneity. We then explore a range of advanced nanocarrier platforms, targeted delivery tactics, co-delivery systems, and stimuli-responsive therapies that jointly overcome resistance. Throughout, we emphasize molecular mechanisms and translational potential, highlighting biochemical targets (e.g. ABC transporters, apoptosis regulators) and preclinical/clinical innovations in nanomedicine for MDR [6,15,16]. Emerging modalities such as ferroptosis-inducing nanoparticles, nitric oxide (NO) releasing platforms, and photothermal/ultrasound-triggered nanotherapies are also examined. Finally, we outline the key translational challenges and propose future directions to facilitate the clinical adoption of nanomedicine in the therapy of MDR cancers.
2. Mechanisms of MDR in Cancer
Tumor cells evade therapy through multiple, often overlapping mechanisms, as detailed in recent comprehensive reviews [6]. The principal categories are:
2.1. Drug Efflux Transporters
Upregulation of ATP-binding cassette (ABC) pumps is a hallmark of MDR. P-glycoprotein (P-gp/ABCB1) is the most studied efflux pump [6]. Cryo-EM studies reveal conformational changes during substrate transport that underline its broad specificity [6,17]. Other ABC proteins such as MRP1/ABCC1 and BCRP/ABCG2 contribute to resistance against chemotherapies and targeted drugs [6,16]. For example, MRP1 can export kinase inhibitor metabolites, and BCRP confers resistance to several targeted agents [17,18]. Notably, cells can dynamically regulate transporter levels: recent data show that resistant cells reprogram ABC expression profiles under drug stress [6]. Stromal signals also impact efflux: cancer-associated fibroblasts (CAFs) can induce tumor cell ABC expression via paracrine pathways, creating a protective niche [6,19]. High efflux activity prevents intracellular drug accumulation, so inhibiting or bypassing these pumps is key to overcoming MDR. However, most platforms remain in the early translational phase, with few having progressed to clinical trials.
2.2. Apoptosis Evasion
Cancer cells often disable programmed cell death to survive therapy [6,20,21]. Overexpression of anti-apoptotic BCL-2 family proteins (BCL-2, BCL-XL, MCL-1) is commonly observed in resistant tumors [22]. Advanced proteomics show these proteins are post-translationally stabilized in MDR cells, strengthening survival [23]. Similarly, the IAP family (e.g. XIAP, cIAP1) inhibits caspases; elevated XIAP correlates with poor response to platinum chemo in ovarian cancer [24]. Tumors also inactivate p53: beyond gene mutations, recent studies identified novel posttranslational modifications of p53 that impair its apoptotic function [25]. Tumor cells can further rewire mitochondrial dynamics (increasing fusion, reducing cytochrome c release) to block intrinsic apoptosis [26,27]. They may also downregulate death receptors (FAS, TRAIL receptors) on the cell surface, evading extrinsic apoptosis [28,29]. Importantly, the TME enforces survival: CAFs and other stromal cells secrete cytokines (e.g. IL-6, IGFs) that upregulate anti-apoptotic proteins in cancer cells [30,31]. Together, these adaptations mean drugs that rely on apoptosis (most chemotherapies) become ineffective.
2.3. Enhanced DNA Repair
Many cytotoxic agents work by inducing DNA damage; resistant tumors often boost repair pathways. For instance, repeated genotoxic stress selects for cancer cells with upregulated homologous recombination and non-homologous end joining (NHEJ) repair proteins [32]. Single-cell analyses reveal plasticity: subclones with heightened DNA damage response (DDR) survive therapy, leading to radio- and chemo-resistant populations [33,34]. Cancer stem-like cells, often drug-resistant, inherently exhibit superior DNA repair and antioxidant defenses [33]. Enhanced nucleotide excision repair or base-excision repair can remove drug-induced lesions before apoptosis is triggered. Thus, inhibiting key repair enzymes (e.g. PARP, ATR) is explored to sensitize MDR tumors.
2.4. Tumor Microenvironment (TME)-Induced Resistance
The TME comprises stromal fibroblasts, immune cells (macrophages, myeloid cells), extracellular matrix (ECM), and factors like hypoxia and acidity, all of which influence drug response [35,36]. Hypoxic regions in tumors stabilize HIF-1α, which promotes cell survival pathways and selection of aggressive, stem-like cells [37]. Hypoxia also impairs drug penetration and immune function [38]. CAFs secrete ECM components (collagen, fibronectin) that increase tissue stiffness and form a physical barrier, limiting drug diffusion. They also release growth factors (TGF-β, IL-6) that activate pro-survival signaling in cancer cells [39]. Similarly, tumor-associated macrophages (TAMs) often polarize to an M2-like phenotype under TME cues, releasing IL-10, VEGF and proteases that support tumor growth, angiogenesis, and matrix remodeling [40]. MDSCs and regulatory T cells in the TME suppress anti-tumor immunity and can secrete metabolites (e.g. arginase, IDO) that reduce drug efficacy. Metabolic competition (e.g. for glucose) in the TME also stresses effector immune cells while tumor cells adapt [41]. These TME factors effectively create a fortress around tumor cells, promoting quiescence and resistance.
2.5. Epigenetic Reprogramming
Reversible changes in gene expression contribute to MDR. For example, alterations in DNA methylation or histone modification can silence tumor suppressors or activate survival genes. Recent findings show that epigenetic changes can swiftly reprogram cells to use bypass pathways under therapy [42]. Cancer cells undergoing drug tolerance states display unique chromatin landscapes that prime them for resistance. For instance, histone methylation changes may activate drug efflux or DNA repair genes. MicroRNAs and long noncoding RNAs also modulate MDR by targeting ABC transporters or apoptotic genes. Such epigenetic plasticity enables tumors to adapt transiently to drugs and later re-sensitize after drug withdrawal, complicating therapy [43,44].
In summary, MDR arises from the interplay of intrinsic tumor cell adaptations and extrinsic TME factors, enabling tumors to escape multiple therapies. Effective strategies must therefore multitask; suppress efflux, restore apoptosis, block repair, and re-engineer the TME. Nanomedicine is uniquely suited to this challenge.
3. Strategies to Overcome Multidrug Resistance
3.1. Nanocarriers Inhibiting Drug Efflux Pumps (P-gp, MRP2, etc.)
One fundamental approach to overcoming multidrug resistance (MDR) is to inhibit or evade the ATP-binding cassette (ABC) efflux transporters such as P-glycoprotein (P-gp/ABCB1), MRP1/MRP2, and BCRP. Recent nanocarrier systems have been designed to co-deliver chemotherapeutics with efflux pump inhibitors or siRNAs to suppress these transporters’ function or expression [45,46,47]. Encapsulating drugs in nanoparticles can bypass recognition by efflux pumps and even target the cell nucleus, thereby increasing intracellular drug retention. For example, polymeric micelles carrying doxorubicin (DOX) together with a P-gp siRNA showed effective P-gp gene silencing and restored drug sensitivity in resistant cancer cells [48,49]. Another strategy is using nanocarriers that disrupt cancer cell energy supply: a mitochondria-targeted hybrid nanoparticle was shown to generate ROS and consume ATP under near-infrared (NIR) light, transiently impairing P-gp function and creating a therapeutic window for chemotherapy [50,51]. Such multifaceted nano-formulations significantly increase drug accumulation in MDR tumor cells by inhibiting efflux pump activity at the protein or gene level.
3.2. Modulating the Tumor Microenvironment (TME)
The tumor microenvironment plays a critical role in MDR, contributing factors like hypoxia, dense extracellular matrix, and immunosuppressive cells (e.g. M2 tumor-associated macrophages, TAMs) [52]. Nanomedicine strategies increasingly target these components to reverse the supportive niche that fosters drug resistance. One approach is re-educating TAMs: delivering Toll-like receptor agonists or small interfering RNAs via nanoparticles can polarize macrophages from an M2 (pro-tumor, repair) phenotype to an M1 (pro-inflammatory, anti-tumor) phenotype [53]. This immunomodulation can heighten the tumor’s response to therapy and reduce MDR, as M2-like TAMs are known to promote tumor growth and drug resistance [52]. Another strategy involves extracellular matrix (ECM) remodeling to improve drug penetration. Nanocarriers functionalized with enzymes like collagenase or hyaluronidase have been used to locally degrade collagen and hyaluronic acid in tumors. For instance, collagenase-decorated nanoparticles carrying DOX showed enhanced tissue penetration and reduced tumor fibrosis, thereby overcoming the ECM barrier to drug delivery [54]. As TME-driven immune evasions such as T and NK cell suppression in non-small cell lung cancer, contributes significantly to therapeutic failure[55], nanomedicine strategies that reprogram immunosuppressive niches offer a promising route to overcome such resistance. By modulating TME factors, normalizing abnormal vasculature, reducing interstitial pressure, re-polarizing macrophages, and enzymatically softening the stroma, nanotherapies can significantly improve the efficacy of chemotherapy in otherwise resistant tumors [52,56].
As summarized in Figure 1, multiple nanomedicine strategies have been developed to target key components of the tumor microenvironment, including TAM reprogramming, ECM remodeling, hypoxia-triggered drug release, and cytokine suppression.
3.3. Dual and Multi-Drug Co-Delivery Nanosystems
Co-delivery of multiple therapeutic agents in a single nanocarrier has emerged as a powerful method to tackle MDR. Advanced nanoparticles (liposomes, polymeric nanoparticles, dendrimers, etc.) can be engineered to carry two or more drugs simultaneously, allowing synergistic action and synchronized release. By incorporating a chemotherapeutic together with a chemosensitizer or a second drug, these nanosystems can attack cancer cells on multiple fronts. Key examples include:
3.3.1. Chemotherapy–chemosensitizer combination
Nanoparticles co-loaded with a conventional anticancer drug and an efflux pump inhibitor (e.g., DOX + tariquidar) or a reversal agent like verapamil have shown increased intracellular drug retention and cytotoxicity in resistant cell lines [57]. Similarly, the rational design of small-molecule chemotherapeutics, including benzofuran–piperazine derivatives with demonstrated cytotoxic activity, can complement nanocarrier-based delivery strategies by providing mechanistically potent payloads [58].
3.3.2. Dual chemotherapies
Co-encapsulation of two chemotherapeutics that act via different mechanisms can produce synergistic killing. For instance, a cRGD-targeted lipid nanoparticle was developed to deliver gemcitabine and paclitaxel together, achieving enhanced breast cancer cell kill rates compared to either drug alone [59]. Such co-delivery ensures both drugs are present at the tumor in the optimal ratio and timing.
3.3.3. Drug–gene combinations
Nano-carriers can concurrently deliver a drug and a genetic therapy. Quantum-dot nanoconjugates have been reported that adsorb DOX together with siRNA targeting MDR genes; this approach successfully downregulated P-gp expression and resensitized cervical cancer cells (HeLa) to chemotherapy [60,61]. Similarly, mesoporous silica nanoparticles carrying DOX plus an siRNA against MDR1 gene achieved higher tumor inhibition in an MDR breast cancer model by blocking drug efflux at the gene level. Similarly, nanocarriers co-loaded with chemotherapeutics and immunostimulatory agents, such as IL-2, represent a promising strategy to simultaneously debulk tumors and enhance immune surveillance. Previous viral vector-based studies have demonstrated the feasibility and antitumor efficacy of IL-2-mediated immunotherapy in solid tumors [62].

Table 1.
Examples of nano co-delivery systems overcoming MDR.
| Nanoformulation | Drugs/Agents | Cancer Model | Key Outcomes (synergy) |
|---|---|---|---|
| Polymeric NP (mPEG-PLGA) | Paclitaxel dimer prodrug + Tetrandrine | MDR HeLa cells (cervical) | Enhanced uptake and ROS; ≈50% higher apoptosis vs. single drug |
| Polymeric NP (PEG-coated) | SN-38 (prodrug) + Ko143 (BCRP inhibitor) | BCRP-overexpressing CRC xenograft | Reversed irinotecan resistance; ~10-fold ↓ IC₅₀ |
| Transferrin-PLGA NP | Gefitinib (EGFR-TKI) + Thymoquinone | Gefitinib-resistant NSCLC (A549/GR) | Re-sensitized to gefitinib; suppressed EMT (increased E-cadherin) |
| cRGD–Heparin NP | Cisplatin + Olaparib (PARP inhibitor) | Cisplatin-resistant ovarian | Inhibited P-gp/MRP2, ↑ DNA damage; overcame cisplatin resistance |
| Doxorubicin liposome + HCQ* | Doxorubicin + Hydroxychloroquine | DOX-resistant breast cancer | Restored apoptosis; polarized TAMs to M1 (↑TNFα, IL-12) |
By tailoring nanocarrier release profiles and surface chemistry, dual-drug nanoparticles can ensure spatial and temporal co-localization of therapeutic agents in tumor cells, effectively bypassing mechanisms of resistance and yielding greater cytotoxic effect than single-drug treatments.
3.4. Tumor-Specific Targeting and Active Delivery Systems
To maximize drug delivery to cancer cells while sparing normal tissue, researchers are functionalizing nanocarriers with tumor-targeting ligands [63]. Such active targeting helps overcome MDR by strengthening the effective drug concentration at the tumor site. Common targeting moieties include transferrin (targets transferrin receptors often overexpressed in cancers), folic acid (targets folate receptors), antibodies or fragments (against tumor antigens), and peptides like cyclic RGD (cRGD) which bind integrin α_vβ_3 on tumor endothelium and cells [64,65].
Transferrin-conjugated nanoparticles are a prominent example: in one study, Tf-decorated PLGA nanoparticles loaded with an experimental organoselenium drug were tested against drug-resistant tumor cells. The Tf-NPs showed significantly higher cytotoxicity in P-gp overexpressing cancer cell lines compared to non-targeted NPs, indicating enhanced uptake via Tf receptor-mediated endocytosis [66,67]. In 3D tumor spheroid models of an MDR ovarian cancer line (NCI/ADR-RES), the Tf-NPs likewise penetrated better and reduced spheroid growth more effectively [68,69]. Similarly, cRGD functionalization of liposomes or polymeric NPs improves their accumulation in tumors by targeting neovasculature and invasive tumor cells. cRGD-modified nanoparticles were observed to undergo receptor-mediated endocytosis into α_vβ_3-expressing cancer cells, achieving higher intracellular drug delivery than untargeted particles [70,71]. In vivo imaging confirmed that cRGD-NPs concentrate preferentially in tumors, with reduced off-target distribution to liver and lungs [70].
Other ligand-targeted nanocarriers include folate-NPs (effective in folate receptor–positive ovarian and breast cancers), EGFR-targeted immunoliposomes, HER2-targeted nanoparticles for resistant breast cancer, and aptamer-guided NPs. By actively homing to tumor cells or the tumor microenvironment, these systems increase drug efficacy against MDR tumors and mitigate systemic toxicity [70,72]. The result is a higher therapeutic index and the ability to kill resistant cancer subpopulations that might evade passive delivery. Additionally, receptor-mediated delivery strategies are increasingly leveraged in nanoparticle design to enhance tumor targeting while minimizing off-target toxicity. For instance, receptor-based frameworks have been applied to bypass efflux-mediated resistance and improve intracellular drug retention [73].
3.5. Nanotechnology in Specific Cancers: Colorectal, Breast, Ovarian, and Kidney
Multi-drug resistance manifests differently across cancer types, and nanomedicine strategies have been tailored accordingly in colorectal, breast, ovarian, and kidney cancers:
3.5.1. Colorectal Cancer (CRC)
MDR in CRC (e.g., resistance to 5-fluorouracil or oxaliplatin) is often linked to efflux pumps and cancer stem cells. Nanocarriers have been explored to deliver combination therapies and siRNAs to overcome these mechanisms [74]. For instance, lipid nanoparticles co-loading 5-FU with curcumin (a natural chemosensitizer) have shown the ability to reverse 5-FU resistance in CRC cells [74,75]. Polymeric nanosystems targeting colon cancer stem cell markers are also under investigation to prevent recurrence and MDR. Early results demonstrate that nano-delivery can enhance drug uptake in CRC and downregulate survival pathways, improving chemosensitivity [74,75]. Additionally, preclinical studies such as those using CF10 polymer formulations have shown remarkable efficacy against colorectal cancer liver metastasis model, highlighting the translational potential of optimized nanopolymers[76,77,78] .
3.5.2. Breast Cancer
Breast tumors (especially triple-negative or recurrent tumors) commonly develop MDR through P-gp overexpression. Many studies use the doxorubicin-resistant MCF-7/ADR cell model to evaluate nano-therapies. Successful approaches include PEGylated liposomes carrying DOX plus P-gp inhibitors, and pH-responsive micelles delivering dual drugs [79,80]. A notable example combining DOX with siRNA against MDR1 in a pH-sensitive chitosan-based micelle, achieving dramatically higher tumor suppression in an MCF-7/ADR mouse model (87% tumor inhibition) compared to free DOX (~50%) [81,82]. Another approach used a hyaluronic-acid modified MoS₂ nanosheet to deliver DOX and perform photothermal therapy; under NIR laser, the nano-system generated heat and downregulated P-gp expression, leading to near-complete tumor ablation in an MDR breast cancer model [83,84,85]. These examples highlight that in breast cancer, nanomedicines can restore drug potency by both chemical and physical mechanisms (gene silencing, heat, etc.).
3.5.3. Ovarian Cancer
Ovarian tumors often exhibit MDR to platinum drugs and taxanes. Nanocarriers are being designed for intraperitoneal delivery in ovarian cancer to achieve high local drug levels. As mentioned, transferrin-targeted nanoparticles have shown promise in sensitizing ovarian cancer cells (like NCI/ADR-RES) to drugs [86]. Another strategy is delivering small molecule inhibitors of anti-apoptotic pathways (e.g., BCL-2 or PI3K/Akt) alongside chemo in a single nanoplatform [87,88,89]. In preclinical studies, dual-loaded NPs (e.g., paclitaxel + Akt siRNA) demonstrated the ability to overcome paclitaxel resistance in ovarian cancer xenografts by inducing apoptosis in otherwise refractory tumors [90,91,92,93]. Ongoing translational research in ovarian cancer focuses on nano-formulations of platinum drugs, PARP inhibitors, and gene therapies to bypass resistance and reduce systemic toxicity [94,95,96].
3.5.4. Kidney (Renal Cell) Cancer
Metastatic renal cell carcinoma (RCC) can develop resistance to targeted therapies like tyrosine kinase inhibitors (TKIs) [97]. Nanomedicine efforts here aim to deliver novel therapeutics or re-sensitize tumors to TKIs. One innovative example is the use of cuprous oxide (Cu₂O) nanoparticles to overcome resistance to sunitinib (a common RCC TKI) [98]. It is reported that Cu₂O NPs induce endoplasmic reticulum stress and ROS-mediated apoptosis in renal cancer cells, thereby restoring their sensitivity to sunitinib [99]. This nanoparticle effectively modulated copper trafficking inside tumor cells, pointing to a unique ferroptosis-like mechanism to kill drug-resistant RCC cells [100]. Additionally, dual-ligand liposomes targeting both RCC cells and angiogenic endothelium have shown promise in drug-resistant kidney tumors, by concentrating drugs in the tumor microvasculature and tumor tissue simultaneously [101]. While nanotherapy in kidney cancer is still nascent, these approaches suggest that overcoming resistance to targeted agents (like TKIs) is feasible with nanoparticle delivery that triggers alternative cell-death pathways or improved drug localization.
3.6. Emerging Strategies: Ferroptosis, Autophagy Modulation, Nitric Oxide, and Gene Therapy
Beyond conventional chemo, several cutting-edge approaches leverage nanotechnology to induce non-traditional cell death pathways or to modulate cellular survival mechanisms in MDR cancers:
3.6.1. Ferroptosis Induction
Ferroptosis is an iron-dependent form of programmed cell death characterized by lipid peroxidation. Recent studies highlight that inducing ferroptosis can help kill drug-resistant cancer cells that evade apoptosis [102]. Nanomedicines are being engineered as “ferroptosis nanoinducers” for example, ultrasmall iron oxide or magnetite nanoparticles that release Fe²⁺ to catalyze lipid ROS generation, or nanocarriers delivering ferroptosis-triggering drugs (like erastin or RSL3) [103]. The versatile ferroptosis-targeted nanotherapies have shown broad potential in reversing therapy resistance by directly triggering this pathway and by feedback regulation of cellular redox state [104]. In practice, combining ferroptosis inducers with chemo or immunotherapy (via co-loaded NPs) has yielded synergistic anti-tumor effects in refractory tumors, and is a hot area of preclinical research [105,106]. Additionally, targeting DNA repair checkpoints, such as CHK1 or PARP, offers another avenue to overcome resistance. CHK1 inhibition has been shown to potentiate DNA damage and sensitize chemoresistant ovarian tumors by modulating PARPylation and metabolic stress [107,108].
3.6.2. Autophagy Inhibition
Autophagy, a cellular recycling process, is a double-edged sword in cancer; in established tumors, moderate autophagy often promotes survival under therapeutic stress, contributing to MDR [109]. Thus, blocking cytoprotective autophagy can re-sensitize cancer cells to treatment. However, systemic autophagy inhibitors (like chloroquine derivatives) have off-target effects. Nanocarriers offer a way to target autophagy inhibitors to tumors. Researchers have loaded agents such as hydroxychloroquine (HCQ) or novel autophagy blockers into tumor-targeted nanoparticles to concentrate their action in tumor cells [110,111,112]. For example, Wuliji et al. formulated amphiphilic polymer micelles co-encapsulating HCQ and DOX; these NPs preferentially accumulated in tumors and effectively overcame DOX resistance by inhibiting autophagy flux in cancer cells [112]. Such nano-formulations ensure that autophagy is sufficiently inhibited in the tumor (preventing cancer cells from “recycling” damaged organelles and drugs) while minimizing toxicity elsewhere. Notably, some teams are also exploring autophagy activation in certain contexts (since excessive autophagy can induce cell death); both inhibition and promotion of autophagy via nanomedicines are being tested as strategies to collapse the defenses of MDR tumors [112,113,114].
3.6.3. Nitric Oxide (NO) Delivery
Nitric oxide is a gaseous signaling molecule that, at high concentrations, can kill cancer cells and modulate MDR pathways. NO has been found to downregulate P-glycoprotein expression and sensitize tumors to drugs. To exploit this, researchers have developed NO-releasing nanocarriers [115,116]. One innovative system is a supramolecular peptide hydrogel loaded with a NO prodrug and DOX: when injected into a tumor, the hydrogel slowly releases NO (especially in the presence of high glutathione levels in the TME) alongside DOX [117,118]. The burst of NO not only directly damages tumor cells via oxidative stress, but also reverses P-gp–mediated MDR, making cancer cells more susceptible to DOX [119]. In vivo studies in MDR breast cancer models showed that this NO-releasing co-delivery platform significantly enhanced tumor shrinkage compared to DOX alone [120]. Another study encapsulated an NO donor and camptothecin in a PLGA nanoparticle; under the acidic conditions of the tumor, NO was generated, which destabilized the NP and triggered drug release in situ. The released NO reduced P-gp levels by ~45%, thereby permitting a much higher intracellular concentration of camptothecin [121]. These results underscore NO’s potential as a chemosensitizing agent when delivered via a controlled nanocarrier.
3.6.4. Gene Therapy and RNA Interference
Nanotechnology enables gene-based therapies to overcome MDR, such as siRNA, shRNA, mRNA or CRISPR/Cas9 systems directed against resistance-related genes [122]. Because nucleic acids alone have poor stability and delivery, nano-formulations (lipid nanoparticles, polymeric polyplexes, etc.) are essential for their clinical use [123,124]. Numerous studies have shown that siRNA against MDR1 (ABCB1) delivered by nanoparticles can knock down P-gp expression and restore drug sensitivity in vitro and in vivo [125,126,127]. For example, a hierarchical mesoporous silica nanocarrier was used to co-deliver DOX plus an anti-Pgp siRNA: the MSN protected the siRNA from degradation and released both payloads inside multidrug-resistant breast cancer cells, leading to P-gp silencing and significantly higher chemotherapy efficacy [128]. Beyond P-gp, researchers are targeting other resistance genes (BCL-2, Akt, MYC, etc.) using siRNA or even CRISPR delivered by viral-mimicking nanoparticles [129]. Similarly, modulation of oncogenic miRNAs like miR-221-5p has been implicated in chemoresistance, further justifying nanoparticle-mediated miRNA therapies in resistant ovarian cancers [130]. The upregulation of lymphoblastic leukemia-derived sequence-1 (LYL1) has been implicated in the progression and metastatic potential of ovarian cancer, highlighting it as a potential target for gene-silencing approaches. Sah et al. demonstrated the oncogenic role of LYL1 in ovarian cancer models, supporting the rationale for RNAi-loaded nanocarriers designed to reverse oncogene-driven drug resistance [131]. Early results are promising, showing that silencing or editing genes can directly reverse MDR phenotypes. However, gene therapy approaches must surmount delivery challenges and potential off-target effects and thus are often combined with nanoparticle strategies for tumor-specific, controlled delivery [132,133].
In summary, these emerging nano-strategies aim to attack MDR cancer cells via novel mechanisms inducing ferroptotic cell death, shutting down autophagy survival pathways, using bioactive gases like NO, or reprogramming gene expression – thereby supplementing conventional cytotoxic drugs and overcoming resistance that arises from classic mechanisms.
3.7. Stimuli-Responsive Nanotherapies: Ultrasound, Photothermal, and Sonodynamic Approaches
Stimuli-responsive nanomedicine adds another layer of innovation to combat MDR by using external triggers (such as light or sound) to activate drug delivery or kill tumor cells by non-chemical means [134,135]. These approaches can bypass drug efflux and damage resistant cells through physical mechanisms:
3.7.1. Photothermal Therapy (PTT)
This involves nanoparticles that absorb NIR laser light and convert it to heat, selectively killing cancer cells or disrupting their membranes. Photothermal agents (gold nanoshells, nanorods, carbon nanomaterials, graphene oxide, etc.) can be loaded with chemotherapeutics for a combined effect. Under NIR irradiation, the localized heating can enhance drug release from the nanocarrier and also sensitize tumor cells (e.g., by causing protein denaturation or ATP depletion) [136,137,138]. PTT has been shown to downregulate efflux pumps: for example, mild hyperthermia (≈52°C) generated by MoS₂ nanosheets caused a significant reduction in P-gp levels in MDR breast cancer cells [139,140]. In one study, PLGA nanoparticles co-loaded with DOX and indocyanine green (ICG, an FDA-approved NIR dye) were used to treat MCF-7/ADR tumors. NIR laser exposure of these NP in tumors led to heat generation (from ICG) and triggered DOX release; the combination of chemotherapy + PTT effectively destroyed drug-resistant breast cancer cells in vitro and in vivo [141]. Photothermal nano-therapy thus provides a way to physically eradicate cancer cells that might survive chemical therapy, and when integrated with drug delivery, it produces a synergistic anti-MDR effect.
3.7.2. Ultrasound and Sonodynamic Therapy (SDT)
Ultrasound can penetrate deep into tissues and be focused on tumor sites, making it a valuable trigger for drug release or activation of sonosensitizers [142,143]. In SDT, a sonosensitizer compound (often a porphyrin, IR780, or other ROS-generating molecule) is delivered by a nanoparticle and produces cytotoxic reactive oxygen species when exposed to low-intensity ultrasound. This strategy is particularly useful against hypoxic or deep-seated MDR tumors [144,145]. A recent breakthrough involved cRGD-targeted gold nanoparticles loaded with the EGFR inhibitor gefitinib and the sonosensitizer IR780 [146]. The gold shell provided a photothermal effect (for on-demand drug release) and IR780 generated ROS under ultrasound; together, this low-temperature PTT + SDT combination was able to overcome acquired TKI resistance in an EGFR-mutant NSCLC model [146]. The ultrasound-triggered ROS helped kill cancer cells independent of drug action, while also impairing cellular defense mechanisms, and the mild heating facilitated drug uptake [147,148]. Beyond this, ultrasound is also used to trigger drug release from acoustically responsive nanocarriers (like liposomes or microbubbles) at the tumor site, ensuring a high local drug concentration that can overwhelm efflux pumps [149,150]. Sonodynamic and ultrasound-triggered therapies are still in translational stages, but they exhibit tremendous potential to non-invasively eliminate MDR cancer cells and can be repeated or spatially controlled with imaging guidance (many ultrasound-sensitive NPs also serve as contrast agents) [151].
3.7.3. Other External Triggers
Magnetic field–responsive nanoparticles (e.g., iron oxide NP for magnetic hyperthermia or drug targeting), photodynamic therapy (light-activated generation of singlet oxygen using NP-delivered photosensitizers), and radiation-triggered nanoparticle release are additional modalities under exploration [152,153]. For instance, magnetically heated nanoparticles or X-ray-activated liposomes could help in circumventing resistance by causing direct tumor cell damage or by releasing drugs in a burst when the tumor vasculature is most permeable. These methods, often termed “externally responsive nanotherapies,” can be combined with chemotherapy to potentiate treatment effects [154]. By carefully tuning the stimulus (laser wavelength, ultrasound frequency, magnetic field strength), clinicians can activate the nanoparticle only at the tumor site, thereby achieving high precision [154,155].
In summary, stimuli-responsive nanotherapies offer a way to attack MDR tumors using physical forces (heat, sound, light) that cancer cells are less equipped to resist. When coupled with smart nanocarriers, these approaches release drugs at the optimal time or bypass biochemical resistance entirely, and they have demonstrated impressive results in preclinical MDR cancer models [156]. To illustrate the diversity and mechanisms of nanocarrier-based co-delivery systems that successfully circumvent MDR in different cancers, a schematic representation of selected strategies is shown in Figure 2, corresponding to the formulations detailed in Table 2.
3.8. Innovative and Underexplored Nanomedicine Strategies for MDR Cancers
While significant attention has been given to co-delivery systems, tumor microenvironment modulation, and stimuli-responsive release strategies, recent studies have spotlighted a new wave of highly promising nanomedicine innovations. These approaches, while underrepresented in earlier clinical trials, are gaining traction for their ability to circumvent traditional resistance mechanisms through novel physicochemical properties and delivery modalities.
3.8.1. Magnetic Nanoparticles for Theranostics and Targeted Therapy
Magnetic nanoparticles (MNPs), particularly superparamagnetic iron oxide nanoparticles (SPIONs), offer dual functionality as both therapeutic and diagnostic agents [157]. When guided by an external magnetic field, MNPs can accumulate at the tumor site with high specificity, allowing for concentrated drug delivery [158]. Moreover, magnetic hyperthermia where MNPs generate localized heat in response to an alternating magnetic field has demonstrated synergy with chemotherapeutics and the capacity to downregulate drug efflux pumps like P-gp [159]. This form of image-guided, magnetically targeted therapy is especially promising for difficult-to-treat or deep-seated tumors.
3.8.2. Intratumoral Administration of Nano Drug Delivery Systems
Intratumoral injection of nano-formulations bypasses systemic pharmacokinetic barriers and delivers high drug concentrations directly into tumor tissue [160]. This strategy enhances local therapeutic efficacy while reducing off-target toxicity. Various delivery systems such as hydrogels, polymeric micelles, and dendritic nanogels have been engineered for sustained and localized drug release following intratumoral injections. This modality is particularly effective in poorly vascularized or desmoplastic tumors, where systemic delivery fails to achieve adequate penetration [161,162].
3.8.3. Polydopamine (PDA) Nanoparticles in Drug Delivery and Immune Modulation
Polydopamine-based nanoparticles exhibit excellent biocompatibility, surface adhesion, and responsiveness to oxidative environments [163]. PDA nanocarriers have been to provide immune modulation, photothermal effect and chemotherapeutic effect simultaneously. [164]. These nanoparticles generate heat when exposed to near-infrared light which can damage cancer cell membranes or sensitize resistant cells to chemotherapy [165]. Additionally, PDA systems have shown promise in modulating immune responses by carrying Toll-like receptor agonists or checkpoint inhibitors, thus bridging drug delivery with tumor immunotherapy [166].
3.8.4. Inorganic Nanoparticles in Overcoming Resistance
Inorganic nanomaterials, including gold nanoparticles, mesoporous silica, and quantum dots offer unique optical, electrical, and structural features [167]. These carriers are not only effective in delivering therapeutics but also enhance imaging and diagnosis. Several studies have demonstrated that inorganic NPs can induce ROS generation, promote apoptosis, and even directly interfere with intracellular resistance pathways [168,169,170]. Quantum-dot conjugates, for instance, allow real-time tracking while co-delivering siRNA and chemotherapeutic agents to downregulate MDR-associated genes [171,172].
3.8.5. Oral Nanoformulations for Colorectal Cancer
Oral administration of nanomedicine is particularly valuable in colorectal cancer therapy [173]. Engineered nanoparticles with pH-sensitive or mucoadhesive properties can bypass gastric degradation and release drugs specifically in the colon [174,175]. Co-formulations combining 5-FU with natural chemosensitizers like curcumin have shown enhanced drug retention and MDR reversal [176]. These systems offer improved patient compliance and the potential to deliver both cytotoxic and immunomodulatory agents directly to the tumor site, which is crucial in colorectal tumors with localized resistance profiles [177].
Together, these underexplored strategies highlight the evolving landscape of nanomedicine for drug-resistant cancers. Their distinct mechanisms ranging from magnetic targeting and localized hyperthermia to oxidative disruption and site-specific oral delivery complement established approaches and provide new opportunities to overcome therapeutic resistance in challenging cancer subtypes.
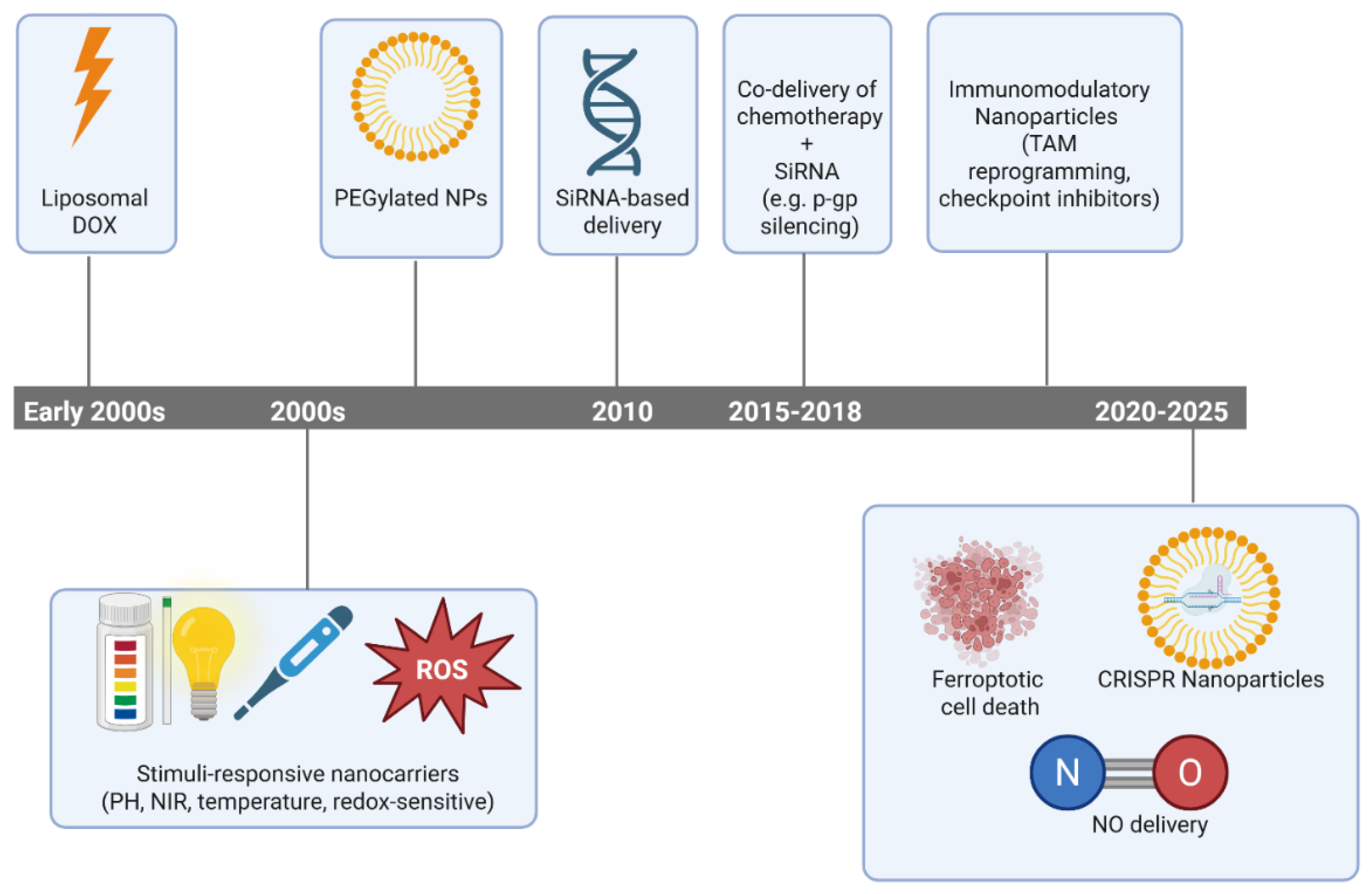
Figure 3.
The Historical development of nanomedicine platforms aimed at reversing MDR, highlighting the evolution from conventional liposomal drugs to gene-editing and ferroptosis-inducing nanocarriers.
Figure 3.
The Historical development of nanomedicine platforms aimed at reversing MDR, highlighting the evolution from conventional liposomal drugs to gene-editing and ferroptosis-inducing nanocarriers.
4. Clinical Translation: Limitations and Challenges
Despite the plethora of promising nanomedicine strategies in preclinical studies, translating these innovations into clinical use faces significant challenges. The first consideration is the complexity of regulatory approval for nanodrugs. Nanomedicines often don’t fit neatly into existing regulatory categories, they may be classified as drugs, biologics, devices, or combination products, which complicates the approval pathway [178]. Regulatory agencies like the FDA and EMA have been cautious, requiring extensive characterization of nanoparticle physicochemical properties, manufacturing consistency, and toxicity profiles. Key hurdles include:
4.1. Sandardization and Characterization:
There is a lack of standardized guidelines specific to nanomedicines [178]. Small variations in formulation (particle size, surface charge, etc.) can dramatically alter a nanoparticle’s behavior in vivo [179]. Thus, companies must implement advanced analytical techniques and strict quality controls to ensure batch-to-batch consistency and well-characterized products [178,180]. Demonstrating reproducibility and stability of complex nanoparticle formulations (which may comprise multiple components like polymers, lipids, targeting ligands, and drugs) is much more involved than for small-molecule drugs. This also affects the development of “nanosimilars” (generic versions of nanodrugs), where establishing equivalence is non-trivial [180,181].
4.2. Safety and Toxicity Concerns
While nanocarriers can reduce the systemic toxicity of potent drugs, the long-term fate of nanoparticles in the body is not fully understood. Issues such as accumulation in the reticuloendothelial system (liver, spleen), unforeseen immunogenic reactions, or off-target effects of the nanoparticle components must be addressed [182]. Extensive preclinical studies are needed to evaluate biocompatibility, for example, whether the NP triggers complement activation or how it is excreted or metabolized [183]. Some high-profile nanodrugs have failed in trials due to toxicity or immune-related adverse events not predicted by animal models [184,185]. Rare but severe immune-mediated reactions to pharmacological agents, such as sulfasalazine-induced DRESS syndrome, underscore the importance of vigilant safety profiling and post-marketing surveillance in both traditional and nanomedicine therapies [186]. In addition to manufacturing and scalability, successful integration of nanomedicine into real-world clinical settings requires alignment with hospital practices, prescriber behaviors, and resource availability. System-level challenges, such as noncompliance with prescription-writing standards, delayed IV-to-oral transitions, and inconsistent infection management protocols highlight the barriers to adopting complex therapeutic innovations like nanomedicine in routine care [187,188,189]. Moreover, including pharmacists in clinical audit workflows has shown to improve adherence to treatment protocols and could support future implementation of nanomedicine [190]. Overcoming MDR in a tumor is controversial if nanotherapy cannot be used safely in patients, so ensuring safety profiles and conducting rigorous toxicity studies (including looking at chronic exposure) is essential [191,192].
4.3. Manufacturing and Scalability
Producing nanomedicines at a commercial scale with uniform quality is challenging [193]. Techniques used in the lab (like microfluidic mixing or small-batch emulsification) may not easily translate to industrial scale. Additionally, sterile filtering or validating complex nanoconjugates can be difficult [194]. Scaling up often requires significant engineering and process development, and any process changes might alter the NP properties, sending developers back to perform comparability studies [195]. For example, standardized methods for the growth, purification, and titration of virus-based therapies, such as oncolytic herpes simplex viruses, have been developed to improve process reproducibility and safety, offering insights applicable to viral and gene-based nanocarriers [196]. Scaling up contributes to the high cost of bringing nanodrugs to the market [197]. Manufacturing complexities also tie into regulatory hurdles, as changes in a nanomedicine’s production may trigger the need for new safety evaluations [198,199].
4.4. Efficacy in Human Tumors
A well-known challenge in cancer nanomedicine is the gap between preclinical efficacy (often in mouse xenograft models) and clinical efficacy in human patients [200]. The enhanced permeability and retention (EPR) effect, which allows nanoparticles to accumulate in tumors due to leaky vasculature, is variable in humans – many human tumors have irregular blood supply or higher interstitial pressure that limits nanoparticle penetration [201,202]. Consequently, some nanoparticles that work in mice don’t achieve sufficient tumor delivery in patients [203]. Heterogeneity among patients and tumor types means that nanomedicines might benefit some patients more than others [204]. For clinical translation, better methods to image and verify NP delivery in human tumors are needed (e.g., PET or MRI-labeled nanoparticles) to select patients most likely to benefit [204].
4.5. Economic and Practical Considerations
The cost of developing and producing nanomedicines can be substantially higher than for traditional drugs [205]. This includes the cost of specialized facilities and analytical assays. These costs can make nanodrugs expensive, potentially limiting patient access or insurance acceptance [206]. Additionally, regulatory approval times can be longer due to the need for expert consultations on nanotech aspects [207]. From a practical standpoint, the shelf-life and storage conditions of nanomedicines (some may require cold storage or have shorter stability) can be a logistical challenge for distribution [208,209]. Real-world implementation of nanomedicine must also account for disparities in patient comprehension, as limited health literacy has been shown to hinder cancer care engagement and decision-making in vulnerable populations [210].
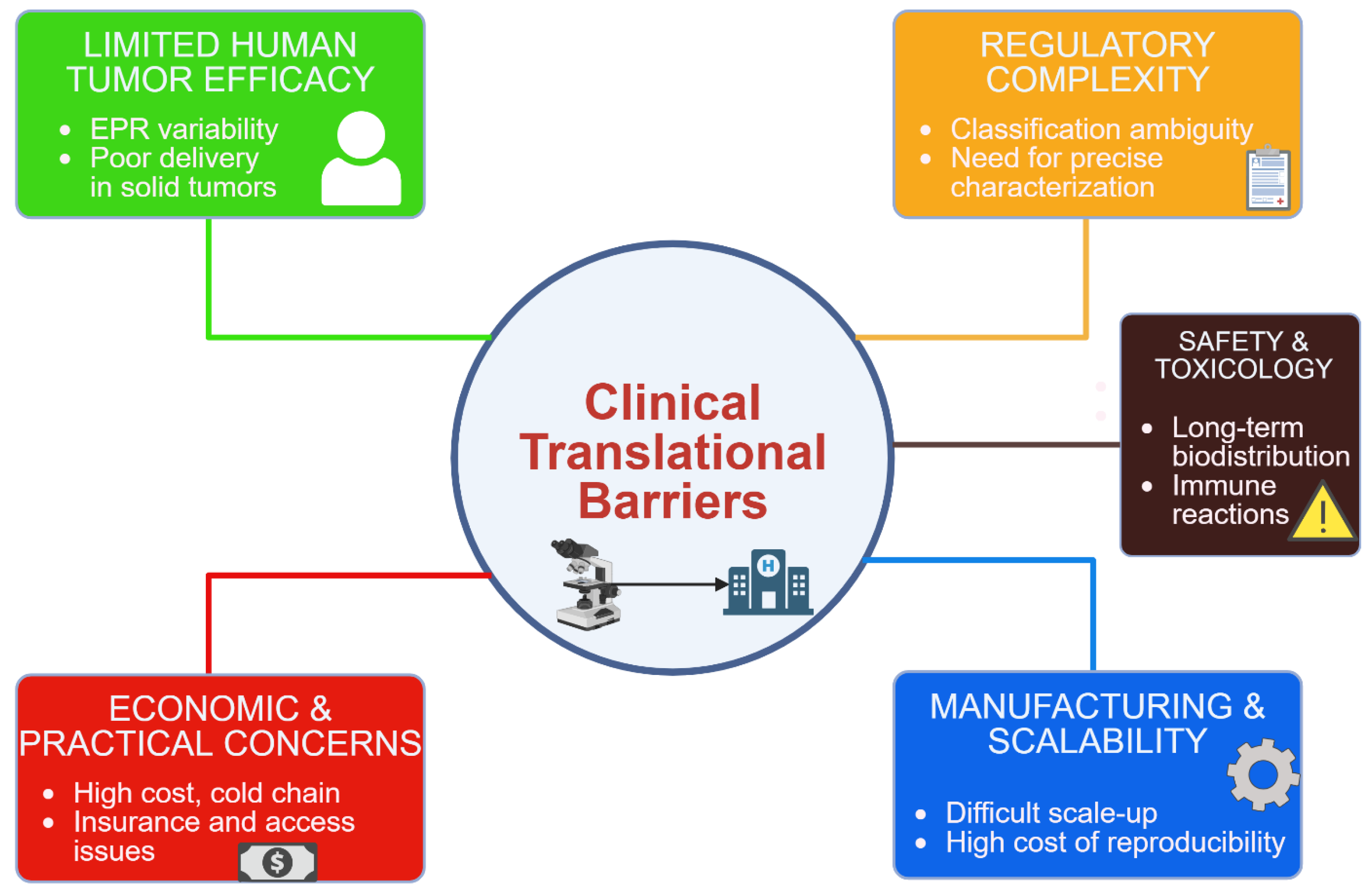
Figure 4.
Key challenges in the clinical translation of nanomedicine for multidrug-resistant (MDR) cancers. The schematic summarizes five major hurdles: (1) regulatory complexity due to overlapping classification and lack of standardization; (2) safety and toxicity concerns including unpredictable biodistribution and immune responses; (3) manufacturing and scalability issues affecting reproducibility and cost; (4) limited clinical efficacy stemming from tumor heterogeneity and variable nanoparticle delivery; and (5) economic and logistical barriers related to high production costs, cold chain requirements, and limited accessibility. Addressing these interconnected limitations is essential for successful bench-to-bedside translation.
Figure 4.
Key challenges in the clinical translation of nanomedicine for multidrug-resistant (MDR) cancers. The schematic summarizes five major hurdles: (1) regulatory complexity due to overlapping classification and lack of standardization; (2) safety and toxicity concerns including unpredictable biodistribution and immune responses; (3) manufacturing and scalability issues affecting reproducibility and cost; (4) limited clinical efficacy stemming from tumor heterogeneity and variable nanoparticle delivery; and (5) economic and logistical barriers related to high production costs, cold chain requirements, and limited accessibility. Addressing these interconnected limitations is essential for successful bench-to-bedside translation.
Despite these challenges, progress is being made. A growing number of nanomedicines have achieved clinical approval (including many liposomal drugs, polymer–drug conjugates, and nanoparticle-albumin-bound drugs), proving that regulatory and manufacturing hurdles are surmountable [211]. As of mid-2025, over 100 nanotechnology-based therapeutics or diagnostics have been approved for clinical use [212], though most are reformulations of existing drugs rather than novel MDR-targeting systems [213]. Importantly, lessons from these successes are informing next-generation designs: for instance, using biodegradable materials to improve safety, simplifying nanoparticle compositions to ease manufacturing, and developing clear regulatory standards [214]. Collaborations between academia, industry, and regulatory bodies are ongoing to refine guidelines specific to nanomedicine [215]. In parallel, clinical trial designs are adapting, sometimes incorporating patient stratification (e.g., selecting patients with leaky tumors or certain biomarkers for nanoparticle uptake) to demonstrate benefit [216,217].
5. Conclusions
In conclusion, while nanomedicine offers innovative solutions to overcome cancer MDR – through targeted delivery, co-therapy, microenvironment modulation, and externally-triggered release – the journey from bench to bedside requires careful navigation of regulatory, safety, and production challenges. Ongoing innovations and a better understanding of how nanoparticles behave in patients will help ensure that the most promising laboratory breakthroughs can be translated into real-world cancer therapies [218]. The continued success of nanomedicine in the clinic will pave the way for these multi-modal MDR-reversing strategies to become part of standard cancer care in the future.
Author Contributions
For research articles with several authors, a short paragraph specifying their individual contributions must be provided. The following statements should be used “Conceptualization, S.K.Y., V.B.C., K.B.R.; methodology, S.K.Y., V.B.C., K.B.R.; software, N.U.P., M.S.D.; validation, N.U.P., M.S.D., K.B.R.; formal analysis, M.S.D., K.B.R.; investigation, N.U.P., M.S.D., K.B.R.; resources, N.U.P., M.S.D., K.B.R.; data curation, S.K.Y., V.B.C.; writing—original draft preparation, S.K.Y., V.B.C.; writing—review and editing, N.U.P., M.S.D., K.B.R.; visualization, N.U.P., M.S.D.; supervision, N.U.P., M.S.D., K.B.R.; project administration, N.U.P., M.S.D., K.B.R.; funding acquisition, S.K.Y., K.B.R.
Funding
NIL.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
Not applicable.
Conflicts of Interest
NIL.
References
- Bray, F.; Laversanne, M.; Sung, H.; Ferlay, J.; Siegel, R.L.; Soerjomataram, I.; Jemal, A. Global Cancer Statistics 2022: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin 2024, 74, 229–263. [CrossRef]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin 2021, 71, 209–249. [CrossRef]
- Ferlay, J.; Colombet, M.; Soerjomataram, I.; Parkin, D.M.; Piñeros, M.; Znaor, A.; Bray, F. Cancer Statistics for the Year 2020: An Overview. Int J Cancer 2021. [CrossRef]
- Emran, T.B.; Shahriar, A.; Mahmud, A.R.; Rahman, T.; Abir, M.H.; Siddiquee, M.F.-R.; Ahmed, H.; Rahman, N.; Nainu, F.; Wahyudin, E.; et al. Multidrug Resistance in Cancer: Understanding Molecular Mechanisms, Immunoprevention and Therapeutic Approaches. Front. Oncol. 2022, 12. [CrossRef]
- Ward, R.A.; Fawell, S.; Floc’h, N.; Flemington, V.; McKerrecher, D.; Smith, P.D. Challenges and Opportunities in Cancer Drug Resistance. Chem Rev 2021, 121, 3297–3351. [CrossRef]
- Roszkowska, M. Multilevel Mechanisms of Cancer Drug Resistance. International Journal of Molecular Sciences 2024, 25, 12402. [CrossRef]
- Wang, X.; Zhang, H.; Chen, X. Drug Resistance and Combating Drug Resistance in Cancer. Cancer Drug Resist 2019, 2, 141–160. [CrossRef]
- Vasan, N.; Baselga, J.; Hyman, D.M. A View on Drug Resistance in Cancer. Nature 2019, 575, 299–309. [CrossRef]
- Huddleston, C.; Mani, C.; Sah, N.; Courtney, E.; Reese, K.; Stroever, S.; Palle, K.; Reedy, M.B. Evaluating Efficacy of Cervical HPV-HR DNA Testing as Alternative to PET/CT Imaging for Posttreatment Cancer Surveillance: Retrospective Proof-of-Concept Study. Cancer Epidemiology, Biomarkers & Prevention 2025, OF1–OF5. [CrossRef]
- Huddleston, C.; Fakhreddine, A.B.; Stroever, S.; Young, R.; Sah, N.; Palle, K.; Reedy, M. Abstract 1305: Comparison of HPV-DNA Testing to PET-CT Imaging as Prognostic Test Following Definitive Treatment for Cervical Cancer: A Retrospective Proof-of-Concept Study. Cancer Research 2024, 84, 1305. [CrossRef]
- Sabir, S.; Thani, A.S.B.; Abbas, Q. Nanotechnology in Cancer Treatment: Revolutionizing Strategies against Drug Resistance. Front Bioeng Biotechnol 2025, 13, 1548588. [CrossRef]
- Souri, M.; Soltani, M.; Moradi Kashkooli, F.; Kiani Shahvandi, M. Engineered Strategies to Enhance Tumor Penetration of Drug-Loaded Nanoparticles. J Control Release 2022, 341, 227–246. [CrossRef]
- Chen, D.; Liu, X.; Lu, X.; Tian, J. Nanoparticle Drug Delivery Systems for Synergistic Delivery of Tumor Therapy. Front. Pharmacol. 2023, 14. [CrossRef]
- Rehman, M.U.; Khan, A.; Imtiyaz, Z.; Ali, S.; Makeen, H.A.; Rashid, S.; Arafah, A. Current Nano-Therapeutic Approaches Ameliorating Inflammation in Cancer Progression. Semin Cancer Biol 2022, 86, 886–908. [CrossRef]
- Rehman, M.U.; Khan, A.; Imtiyaz, Z.; Ali, S.; Makeen, H.A.; Rashid, S.; Arafah, A. Current Nano-Therapeutic Approaches Ameliorating Inflammation in Cancer Progression. Semin Cancer Biol 2022, 86, 886–908. [CrossRef]
- Wilkens, S. Structure and Mechanism of ABC Transporters. F1000Prime Rep 2015, 7, 14. [CrossRef]
- Alfarouk, K.O.; Stock, C.-M.; Taylor, S.; Walsh, M.; Muddathir, A.K.; Verduzco, D.; Bashir, A.H.H.; Mohammed, O.Y.; Elhassan, G.O.; Harguindey, S.; et al. Resistance to Cancer Chemotherapy: Failure in Drug Response from ADME to P-Gp. Cancer Cell Int 2015, 15, 71. [CrossRef]
- Wang, J.; Seebacher, N.; Shi, H.; Kan, Q.; Duan, Z. Novel Strategies to Prevent the Development of Multidrug Resistance (MDR) in Cancer. Oncotarget 2017, 8, 84559–84571. [CrossRef]
- Targeting Interleukin-6 as a Strategy to Overcome Stroma-Induced Resistance to Chemotherapy in Gastric Cancer - PubMed Available online: https://pubmed.ncbi.nlm.nih.gov/30927911/ (accessed on 28 May 2025).
- Chen, S.-Q.; Li, J.-Q.; Wang, X.-Q.; Lei, W.-J.; Li, H.; Wan, J.; Hu, Z.; Zou, Y.-W.; Wu, X.-Y.; Niu, H.-X. EZH2-Inhibitor DZNep Enhances Apoptosis of Renal Tubular Epithelial Cells in Presence and Absence of Cisplatin. Cell Div 2020, 15, 8. [CrossRef]
- Deng, Y.W.; Hao, W.J.; Li, Y.W.; Li, Y.X.; Zhao, B.C.; Lu, D. Hsa-miRNA-143-3p Reverses Multidrug Resistance of Triple-Negative Breast Cancer by Inhibiting the Expression of Its Target Protein Cytokine-Induced Apoptosis Inhibitor 1 In Vivo. J Breast Cancer 2018, 21, 251–258. [CrossRef]
- Venkatadri, R.; Muni, T.; Iyer, A.K.V.; Yakisich, J.S.; Azad, N. Role of Apoptosis-Related miRNAs in Resveratrol-Induced Breast Cancer Cell Death. Cell Death Dis 2016, 7, e2104. [CrossRef]
- Archer, T.C.; Ehrenberger, T.; Mundt, F.; Gold, M.P.; Krug, K.; Mah, C.K.; Mahoney, E.L.; Daniel, C.J.; LeNail, A.; Ramamoorthy, D.; et al. Proteomics, Post-Translational Modifications, and Integrative Analyses Reveal Molecular Heterogeneity within Medulloblastoma Subgroups. Cancer Cell 2018, 34, 396-410.e8. [CrossRef]
- Devi, G.R.; Finetti, P.; Morse, M.A.; Lee, S.; de Nonneville, A.; Van Laere, S.; Troy, J.; Geradts, J.; McCall, S.; Bertucci, F. Expression of X-Linked Inhibitor of Apoptosis Protein (XIAP) in Breast Cancer Is Associated with Shorter Survival and Resistance to Chemotherapy. Cancers 2021, 13, 2807. [CrossRef]
- Targeting P53 Pathways: Mechanisms, Structures and Advances in Therapy | Signal Transduction and Targeted Therapy Available online: https://www.nature.com/articles/s41392-023-01347-1 (accessed on 29 May 2025).
- Peiris-Pagès, M.; Bonuccelli, G.; Sotgia, F.; Lisanti, M.P. Mitochondrial Fission as a Driver of Stemness in Tumor Cells: mDIVI1 Inhibits Mitochondrial Function, Cell Migration and Cancer Stem Cell (CSC) Signalling. Oncotarget 2018, 9, 13254–13275. [CrossRef]
- Kashatus, D.F. The Regulation of Tumor Cell Physiology by Mitochondrial Dynamics. Biochem Biophys Res Commun 2018, 500, 9–16. [CrossRef]
- Fas Receptor - an Overview | ScienceDirect Topics Available online: https://www.sciencedirect.com/topics/biochemistry-genetics-and-molecular-biology/fas-receptor (accessed on 29 May 2025).
- Leonard, B.C.; Johnson, D.E. Signaling by Cell Surface Death Receptors: Alterations in Head and Neck Cancer. Adv Biol Regul 2018, 67, 170–178. [CrossRef]
- Henke, E.; Nandigama, R.; Ergün, S. Extracellular Matrix in the Tumor Microenvironment and Its Impact on Cancer Therapy. Front Mol Biosci 2020, 6, 160. [CrossRef]
- Tao, L.; Huang, G.; Song, H.; Chen, Y.; Chen, L. Cancer Associated Fibroblasts: An Essential Role in the Tumor Microenvironment. Oncol Lett 2017, 14, 2611–2620. [CrossRef]
- Sobanski, T.; Rose, M.; Suraweera, A.; O’Byrne, K.; Richard, D.J.; Bolderson, E. Cell Metabolism and DNA Repair Pathways: Implications for Cancer Therapy. Front Cell Dev Biol 2021, 9, 633305. [CrossRef]
- Bhat, G.R.; Sethi, I.; Sadida, H.Q.; Rah, B.; Mir, R.; Algehainy, N.; Albalawi, I.A.; Masoodi, T.; Subbaraj, G.K.; Jamal, F.; et al. Cancer Cell Plasticity: From Cellular, Molecular, and Genetic Mechanisms to Tumor Heterogeneity and Drug Resistance. Cancer Metastasis Rev 2024, 43, 197–228. [CrossRef]
- Torborg, S.R.; Li, Z.; Chan, J.E.; Tammela, T. Cellular and Molecular Mechanisms of Plasticity in Cancer. Trends Cancer 2022, 8, 735–746. [CrossRef]
- Wang, Q.; Shao, X.; Zhang, Y.; Zhu, M.; Wang, F.X.C.; Mu, J.; Li, J.; Yao, H.; Chen, K. Role of Tumor Microenvironment in Cancer Progression and Therapeutic Strategy. Cancer Med 2023, 12, 11149–11165. [CrossRef]
- Anderson, N.M.; Simon, M.C. Tumor Microenvironment. Curr Biol 2020, 30, R921–R925. [CrossRef]
- Hassan Venkatesh, G.; Abou Khouzam, R.; Shaaban Moustafa Elsayed, W.; Ahmed Zeinelabdin, N.; Terry, S.; Chouaib, S. Tumor Hypoxia: An Important Regulator of Tumor Progression or a Potential Modulator of Tumor Immunogenicity? Oncoimmunology 10, 1974233. [CrossRef]
- Zheng, Z.; Bian, C.; Wang, H.; Su, J.; Meng, L.; Xin, Y.; Jiang, X. Prediction of Immunotherapy Efficacy and Immunomodulatory Role of Hypoxia in Colorectal Cancer. Ther Adv Med Oncol 2022, 14, 17588359221138383. [CrossRef]
- Kazakova, A.N.; Lukina, M.M.; Anufrieva, K.S.; Bekbaeva, I.V.; Ivanova, O.M.; Shnaider, P.V.; Slonov, A.; Arapidi, G.P.; Shender, V.O. Exploring the Diversity of Cancer-Associated Fibroblasts: Insights into Mechanisms of Drug Resistance. Front Cell Dev Biol 2024, 12, 1403122. [CrossRef]
- Pan, Y.; Yu, Y.; Wang, X.; Zhang, T. Tumor-Associated Macrophages in Tumor Immunity. Front Immunol 2020, 11, 583084. [CrossRef]
- Sui, H.; Dongye, S.; Liu, X.; Xu, X.; Wang, L.; Jin, C.Q.; Yao, M.; Gong, Z.; Jiang, D.; Zhang, K.; et al. Immunotherapy of Targeting MDSCs in Tumor Microenvironment. Front Immunol 2022, 13, 990463. [CrossRef]
- Gregg, C. Starvation and Climate Change—How to Constrain Cancer Cell Epigenetic Diversity and Adaptability to Enhance Treatment Efficacy. Front. Ecol. Evol. 2021, 9. [CrossRef]
- Hajji, N.; García-Domínguez ,Daniel J; Hontecillas-Prieto ,Lourdes; O’Neill ,Kevin; de Álava ,Enrique; and Syed, N. The Bitter Side of Epigenetics: Variability and Resistance to Chemotherapy. Epigenomics 2021, 13, 397–403. [CrossRef]
- Lai, T.-Y.; Ko, Y.-C.; Chen, Y.-L.; Lin, S.-F. The Way to Malignant Transformation: Can Epigenetic Alterations Be Used to Diagnose Early-Stage Head and Neck Cancer? Biomedicines 2023, 11, 1717. [CrossRef]
- Zhang, Q.; Li, F. Combating P-Glycoprotein-Mediated Multidrug Resistance Using Therapeutic Nanoparticles. Current Pharmaceutical Design 2013, 19, 6655–6666.
- Wu, Z.; Zhang, J.; Hao, J.; Liu, P.; Liu, X. Understanding Efflux-Mediated Multidrug Resistance in Botrytis Cinerea for Improved Management of Fungicide Resistance. Microbial Biotechnology 2025, 18, e70074. [CrossRef]
- Qiao, D.; Tang, S.; Aslam, S.; Ahmad, M.; To, K.K.W.; Wang, F.; Huang, Z.; Cai, J.; Fu, L. UMMS-4 Enhanced Sensitivity of Chemotherapeutic Agents to ABCB1-Overexpressing Cells via Inhibiting Function of ABCB1 Transporter.
- Nie, Y.; Fu, G.; Leng, Y. Nuclear Delivery of Nanoparticle-Based Drug Delivery Systems by Nuclear Localization Signals. Cells 2023, 12, 1637. [CrossRef]
- Kievit, F.M.; Wang, F.Y.; Fang, C.; Mok, H.; Wang, K.; Silber, J.R.; Ellenbogen, R.G.; Zhang, M. Doxorubicin Loaded Iron Oxide Nanoparticles Overcome Multidrug Resistance in Cancer in Vitro. Journal of Controlled Release 2011, 152, 76–83. [CrossRef]
- Jin, L.; Xu, Y.; Chen, F.; Yu, D.; Liang, H.; Liang, Z.; Liu, Z.; Li, H.; Liu, J.; Tan, H.; et al. Mitochondria-Targeted and pH-Triggered Charge-Convertible Polymeric Micelles for Anticancer Therapy. Materials & Design 2022, 224, 111290. [CrossRef]
- He, W.; Dong, S.; Zeng, Q. Functional Nucleic Acid Nanostructures for Mitochondrial Targeting: The Basis of Customized Treatment Strategies. Molecules 2025, 30, 1025. [CrossRef]
- Wang, S.; Wang, J.; Chen, Z.; Luo, J.; Guo, W.; Sun, L.; Lin, L. Targeting M2-like Tumor-Associated Macrophages Is a Potential Therapeutic Approach to Overcome Antitumor Drug Resistance. npj Precis. Onc. 2024, 8, 1–19. [CrossRef]
- Mendes, B.B.; Sousa, D.P.; Conniot, J.; Conde, J. Nanomedicine-Based Strategies to Target and Modulate the Tumor Microenvironment. Trends in Cancer 2021, 7, 847–862. [CrossRef]
- Extracellular Matrix Remodeling in Tumor Progression and Immune Escape: From Mechanisms to Treatments | Molecular Cancer | Full Text Available online: https://molecular-cancer.biomedcentral.com/articles/10.1186/s12943-023-01744-8 (accessed on 29 May 2025).
- Mestiri, S.; Sami, A.; Sah, N.; El-Ella, D.M.A.; Khatoon, S.; Shafique, K.; Raza, A.; Mathkor, D.M.; Haque, S. Cellular Plasticity and Non-Small Cell Lung Cancer: Role of T and NK Cell Immune Evasion and Acquisition of Resistance to Immunotherapies. Cancer Metastasis Rev 2025, 44, 27. [CrossRef]
- Wang, Y.; Zhou, Q.; Luo, W.; Yang, X.; Zhang, J.; Lou, Y.; Mao, J.; Chen, J.; Wu, F.; Hou, J.; et al. A Collagenase-Decorated Cu-Based Nanotheranostics: Remodeling Extracellular Matrix for Optimizing Cuproptosis and MRI in Pancreatic Ductal Adenocarcinoma. J Nanobiotechnology 2024, 22, 689. [CrossRef]
- Iqubal, M.K.; Kaur, H.; Md, S.; Alhakamy, N.A.; Iqubal, A.; Ali, J.; Baboota, S. A Technical Note on Emerging Combination Approach Involved in the Onconanotherapeutics. Drug Deliv 29, 3197–3212. [CrossRef]
- Schumacher, T.J.; Sah, N.; Palle, K.; Rumbley, J.; Mereddy, V.R. Synthesis and Biological Evaluation of Benzofuran Piperazine Derivatives as Potential Anticancer Agents. Bioorganic & Medicinal Chemistry Letters 2023, 93, 129425. [CrossRef]
- Gabizon, A.; Ohana, P.; Amitay, Y.; Gorin, J.; Tzemach, D.; Mak, L.; Shmeeda, H. Liposome Co-Encapsulation of Anti-Cancer Agents for Pharmacological Optimization of Nanomedicine-Based Combination Chemotherapy. Cancer Drug Resist 2021, 4, 463–484. [CrossRef]
- Fang, G.; Zhang, A.; Zhu, L.; Wang, Q.; Sun, F.; Tang, B. Nanocarriers Containing Platinum Compounds for Combination Chemotherapy. Front Pharmacol 2022, 13, 1050928. [CrossRef]
- Xu, M.; Han, X.; Xiong, H.; Gao, Y.; Xu, B.; Zhu, G.; Li, J. Cancer Nanomedicine: Emerging Strategies and Therapeutic Potentials. Molecules 2023, 28, 5145. [CrossRef]
- Wang, H.; Borlongan, M.; Hemminki, A.; Basnet, S.; Sah, N.; Kaufman, H.L.; Rabkin, S.D.; Saha, D. Viral Vectors Expressing Interleukin 2 for Cancer Immunotherapy. Human Gene Therapy 2023, 34, 878–895. [CrossRef]
- Chehelgerdi, M.; Chehelgerdi, M.; Allela, O.Q.B.; Pecho, R.D.C.; Jayasankar, N.; Rao, D.P.; Thamaraikani, T.; Vasanthan, M.; Viktor, P.; Lakshmaiya, N.; et al. Progressing Nanotechnology to Improve Targeted Cancer Treatment: Overcoming Hurdles in Its Clinical Implementation. Mol Cancer 2023, 22, 169. [CrossRef]
- YU, B.; TAI, H.C.; XUE, W.; LEE, L.J.; LEE, R.J. Receptor-Targeted Nanocarriers for Therapeutic Delivery to Cancer. Mol Membr Biol 2010, 27, 286–298. [CrossRef]
- Nethi, S.K.; Bhatnagar, S.; Prabha, S. Synthetic Receptor-Based Targeting Strategies to Improve Tumor Drug Delivery. AAPS PharmSciTech 2021, 22, 93. [CrossRef]
- Altuwaijri, N.; Atef, E. Transferrin-Conjugated Nanostructured Lipid Carriers for Targeting Artemisone to Melanoma Cells. Int J Mol Sci 2024, 25, 9119. [CrossRef]
- Scheeren, L.E.; Nogueira-Librelotto, D.R.; Macedo, L.B.; de Vargas, J.M.; Mitjans, M.; Vinardell, M.P.; Rolim, C.M.B. Transferrin-Conjugated Doxorubicin-Loaded PLGA Nanoparticles with pH-Responsive Behavior: A Synergistic Approach for Cancer Therapy. J Nanopart Res 2020, 22, 72. [CrossRef]
- Tosca, E.M.; Ronchi, D.; Facciolo, D.; Magni, P. Replacement, Reduction, and Refinement of Animal Experiments in Anticancer Drug Development: The Contribution of 3D In Vitro Cancer Models in the Drug Efficacy Assessment. Biomedicines 2023, 11, 1058. [CrossRef]
- Nunes, A.S.; Barros, A.S.; Costa, E.C.; Moreira, A.F.; Correia, I.J. 3D Tumor Spheroids as in Vitro Models to Mimic in Vivo Human Solid Tumors Resistance to Therapeutic Drugs. Biotechnol Bioeng 2019, 116, 206–226. [CrossRef]
- Zhang, J.; Zhang, P.; Zou, Q.; Li, X.; Fu, J.; Luo, Y.; Liang, X.; Jin, Y. Co-Delivery of Gemcitabine and Paclitaxel in cRGD-Modified Long Circulating Nanoparticles with Asymmetric Lipid Layers for Breast Cancer Treatment. Molecules 2018, 23, 2906. [CrossRef]
- Xing, H.; Hwang, K.; Lu, Y. Recent Developments of Liposomes as Nanocarriers for Theranostic Applications. Theranostics 2016, 6, 1336–1352. [CrossRef]
- Macedo, L.B.; Nogueira-Librelotto, D.R.; Mathes, D.; Pieta, T.B.; Mainardi Pillat, M.; Rosa, R.M. da; Rodrigues, O.E.D.; Vinardell, M.P.; Rolim, C.M.B. Transferrin-Decorated PLGA Nanoparticles Loaded with an Organoselenium Compound as an Innovative Approach to Sensitize MDR Tumor Cells: An In Vitro Study Using 2D and 3D Cell Models. Nanomaterials 2023, 13, 2306. [CrossRef]
- Sah, N.; Shaik, A.A.; Acharya, G.; Dunna, M.; Silwal, A.; Sharma, S.; Khan, S.; Bagchi, S. Receptor-Based Strategies for Overcoming Resistance in Cancer Therapy. Receptors 2024, 3, 425–443. [CrossRef]
- Ashique, S.; Bhowmick, M.; Pal, R.; Khatoon, H.; Kumar, P.; Sharma, H.; Garg, A.; Kumar, S.; Das, U. Multi Drug Resistance in Colorectal Cancer- Approaches to Overcome, Advancements and Future Success. Advances in Cancer Biology - Metastasis 2024, 10, 100114. [CrossRef]
- Yang, R.; Liu, Y.; Yang, N.; Zhang, T.; Hou, J.; He, Z.; Wang, Y.; Sun, X.; Shen, J.; Jiang, H.; et al. Combination of miR159 Mimics and Irinotecan Utilizing Lipid Nanoparticles for Enhanced Treatment of Colorectal Cancer. Pharmaceutics 2024, 16, 570. [CrossRef]
- Sah, N.; Luna, P.; Mani, C.; Gmeiner, W.; Palle, K. Abstract 6178: A Novel Second-Generation Nano-Fluoropyrimidine to Treat Metastatic Colorectal Cancer and Overcome 5-Fluorouracil Resistance. Cancer Research 2023, 83, 6178. [CrossRef]
- Sah, N.; Luna, P.; Mani, C.; Gmeiner, W.; Palle, K. A Novel Fluoropyrimidine Drug to Treat Recalcitrant Colorectal Cancer. The Journal of Pharmacology and Experimental Therapeutics 2023, 385, 441. [CrossRef]
- Okechukwu, C.C.; Ma, X.; Sah, N.; Mani, C.; Palle, K.; Gmeiner, W.H. Enhanced Therapeutic Efficacy of the Nanoscale Fluoropyrimidine Polymer CF10 in a Rat Colorectal Cancer Liver Metastasis Model. Cancers 2024, 16, 1360. [CrossRef]
- Lainetti, P. de F.; Leis-Filho, A.F.; Laufer-Amorim, R.; Battazza, A.; Fonseca-Alves, C.E. Mechanisms of Resistance to Chemotherapy in Breast Cancer and Possible Targets in Drug Delivery Systems. Pharmaceutics 2020, 12, 1193. [CrossRef]
- Murren, J.R.; Durivage, H.J.; Buzaid, A.C.; Reiss, M.; Flynn, S.D.; Carter, D.; Hait, W.N. Trifluoperazine as a Modulator of Multidrug Resistance in Refractory Breast Cancer. Cancer Chemother Pharmacol 1996, 38, 65–70. [CrossRef]
- Zlotnikov, I.D.; Streltsov, D.A.; Ezhov, A.A.; Kudryashova, E.V. Smart pH- and Temperature-Sensitive Micelles Based on Chitosan Grafted with Fatty Acids to Increase the Efficiency and Selectivity of Doxorubicin and Its Adjuvant Regarding the Tumor Cells. Pharmaceutics 2023, 15, 1135. [CrossRef]
- Butt, A.M.; Amin, M.C.I.M.; Katas, H.; Abdul Murad, N.A.; Jamal, R.; Kesharwani, P. Doxorubicin and siRNA Codelivery via Chitosan-Coated pH-Responsive Mixed Micellar Polyplexes for Enhanced Cancer Therapy in Multidrug-Resistant Tumors. Mol Pharm 2016, 13, 4179–4190. [CrossRef]
- Hu, L.; Song, Z.; Wu, B.; Yang, X.; Chen, F.; Wang, X. Hyaluronic Acid-Modified and Doxorubicin-Loaded Au Nanorings for Dual-Responsive and Dual-Imaging Guided Targeted Synergistic Photothermal Chemotherapy Against Pancreatic Carcinoma. Int J Nanomedicine 2024, 19, 13429–13442. [CrossRef]
- Intelligent MoS2 Nanotheranostic for Targeted and Enzyme-/pH-/NIR-Responsive Drug Delivery To Overcome Cancer Chemotherapy Resistance Guided by PET Imaging | ACS Applied Materials & Interfaces Available online: https://pubs.acs.org/doi/10.1021/acsami.7b17506.
- Cao, Y.; Ren, Q.; Hao, R.; Sun, Z. Innovative Strategies to Boost Photothermal Therapy at Mild Temperature Mediated by Functional Nanomaterials. Materials & Design 2022, 214, 110391. [CrossRef]
- Macedo, L.B.; Nogueira-Librelotto, D.R.; Mathes, D.; Pieta, T.B.; Mainardi Pillat, M.; Rosa, R.M. da; Rodrigues, O.E.D.; Vinardell, M.P.; Rolim, C.M.B. Transferrin-Decorated PLGA Nanoparticles Loaded with an Organoselenium Compound as an Innovative Approach to Sensitize MDR Tumor Cells: An In Vitro Study Using 2D and 3D Cell Models. Nanomaterials 2023, 13, 2306. [CrossRef]
- Gong, J.; Shi, T.; Liu, J.; Pei, Z.; Liu, J.; Ren, X.; Li, F.; Qiu, F. Dual-Drug Codelivery Nanosystems: An Emerging Approach for Overcoming Cancer Multidrug Resistance. Biomedicine & Pharmacotherapy 2023, 161, 114505. [CrossRef]
- Yoo, H.; Kim, Y.; Kim, J.; Cho, H.; Kim, K. Overcoming Cancer Drug Resistance with Nanoparticle Strategies for Key Protein Inhibition. Molecules 2024, 29, 3994. [CrossRef]
- Luobin, L.; Wanxin, H.; Yingxin, G.; Qinzhou, Z.; Zefeng, L.; Danyang, W.; Huaqin, L. Nanomedicine-Induced Programmed Cell Death in Cancer Therapy: Mechanisms and Perspectives. Cell Death Discov. 2024, 10, 1–13. [CrossRef]
- Yang, H.; Mao, W.; Rodriguez-Aguayo, C.; Mangala, L.S.; Bartholomeusz, G.; Iles, L.R.; Jennings, N.B.; Ahmed, A.A.; Sood, A.K.; Lopez-Berestein, G.; et al. Paclitaxel Sensitivity of Ovarian Cancer Can Be Enhanced by Knocking down Pairs of Kinases That Regulate MAP4 Phosphorylation and Microtubule Stability. Clin Cancer Res 2018, 24, 5072–5084. [CrossRef]
- Demuytere, J.; Carlier, C.; Van de Sande, L.; Hoorens, A.; De Clercq, K.; Giordano, S.; Morosi, L.; Matteo, C.; Zucchetti, M.; Davoli, E.; et al. Preclinical Activity of Two Paclitaxel Nanoparticle Formulations After Intraperitoneal Administration in Ovarian Cancer Murine Xenografts. Int J Nanomedicine 2024, 19, 429–440. [CrossRef]
- Nagumo, Y.; Villareal, M.O.; Isoda, H.; Usui, T. RSK4 Confers Paclitaxel Resistance to Ovarian Cancer Cells, Which Is Resensitized by Its Inhibitor BI-D1870. Biochemical and Biophysical Research Communications 2023, 679, 23–30. [CrossRef]
- Nunes, M.; Silva, P.M.A.; Coelho, R.; Pinto, C.; Resende, A.; Bousbaa, H.; Almeida, G.M.; Ricardo, S. Generation of Two Paclitaxel-Resistant High-Grade Serous Carcinoma Cell Lines With Increased Expression of P-Glycoprotein. Front Oncol 2021, 11, 752127. [CrossRef]
- Summey, R.; Uyar, D. Ovarian Cancer Resistance to PARPi and Platinum-Containing Chemotherapy. Cancer Drug Resist 2022, 5, 637–646. [CrossRef]
- The Future of Ovarian Cancer: Innovation, Treatment and Hope Available online: https://www.icr.ac.uk/about-us/icr-news/detail/the-future-of-ovarian-cancer--innovation--treatment-and-hope (accessed on 29 May 2025).
- Kaur, P.; Singh, S.K.; Mishra, M.K.; Singh, S.; Singh, R. Nanotechnology for Boosting Ovarian Cancer Immunotherapy. Journal of Ovarian Research 2024, 17, 202. [CrossRef]
- Kamli, H.; Li, L.; Gobe, G.C. Limitations to the Therapeutic Potential of Tyrosine Kinase Inhibitors and Alternative Therapies for Kidney Cancer. Ochsner J 2019, 19, 138–151. [CrossRef]
- Yang, Q.; Wang, Y.; Yang, Q.; Gao, Y.; Duan, X.; Fu, Q.; Chu, C.; Pan, X.; Cui, X.; Sun, Y. Cuprous Oxide Nanoparticles Trigger ER Stress-Induced Apoptosis by Regulating Copper Trafficking and Overcoming Resistance to Sunitinib Therapy in Renal Cancer. Biomaterials 2017, 146, 72–85. [CrossRef]
- Lai, Y.; Zeng, T.; Liang, X.; Wu, W.; Zhong, F.; Wu, W. Cell Death-Related Molecules and Biomarkers for Renal Cell Carcinoma Targeted Therapy. Cancer Cell International 2019, 19, 221. [CrossRef]
- Lei, G.; Tang, L.; Yu, Y.; Bian, W.; Yu, L.; Zhou, J.; Li, Y.; Wang, Y.; Du, J. The Potential of Targeting Cuproptosis in the Treatment of Kidney Renal Clear Cell Carcinoma. Biomedicine & Pharmacotherapy 2023, 167, 115522. [CrossRef]
- Li, J.; Wu, K.; Zhang, J.; Gao, H.; Xu, X. Progress in the Treatment of Drug-Loaded Nanomaterials in Renal Cell Carcinoma. Biomedicine & Pharmacotherapy 2023, 167, 115444. [CrossRef]
- Zhou, Q.; Meng, Y.; Li, D.; Yao, L.; Le, J.; Liu, Y.; Sun, Y.; Zeng, F.; Chen, X.; Deng, G. Ferroptosis in Cancer: From Molecular Mechanisms to Therapeutic Strategies. Sig Transduct Target Ther 2024, 9, 1–30. [CrossRef]
- Jing, L.; Xiao, W.; Hu, Z.; Liu, X.; Yuan, M. A Systematic Review of Nanoparticle-Mediated Ferroptosis in Glioma Therapy. Int J Nanomedicine 2025, 20, 5779–5797. [CrossRef]
- Carlos, A.; Mendes, M.; Cruz, M.T.; Pais, A.; Vitorino, C. Ferroptosis Driven by Nanoparticles for Tackling Glioblastoma. Cancer Letters 2025, 611, 217392. [CrossRef]
- Wu, B.; Zhang, B.; Li, B.; Wu, H.; Jiang, M. Cold and Hot Tumors: From Molecular Mechanisms to Targeted Therapy. Sig Transduct Target Ther 2024, 9, 1–65. [CrossRef]
- Mohapatra, A.; Mohanty, A.; Park, I.-K. Inorganic Nanomedicine—Mediated Ferroptosis: A Synergistic Approach to Combined Cancer Therapies and Immunotherapy. Cancers 2024, 16, 3210. [CrossRef]
- Acharya, G.; Mani, C.; Sah, N.; Saamarthy, K.; Young, R.; Reedy, M.B.; Sobol, R.W.; Palle, K. CHK1 Inhibitor Induced PARylation by Targeting PARG Causes Excessive Replication and Metabolic Stress and Overcomes Chemoresistance in Ovarian Cancer. Cell Death Discov. 2024, 10, 1–15. [CrossRef]
- Targeting Metabolic and DNA Damage Checkpoint Indu...: Full Text Finder Results Available online: https://resolver-ebscohost-com.ezproxy.ttuhsc.edu/openurl?sid=google&auinit=G&aulast=Acharya&atitle=Targeting+Metabolic+and+DNA+Damage+Checkpoint+Induces+Excessive+DNA+Damage+and+Causes+Synergistic+Lethality+in+GLShigh+Chemoresistant+Ovarian+Cancer+Cells&title=Environmental+and+Molecular+Mutagenesis&volume=65&date=2024&spage=18&issn=0893-6692 (accessed on 10 June 2025).
- Long, X.; Yan, J.; Zhang, Z.; Chang, J.; He, B.; Sun, Y.; Liang, Y. Autophagy-Targeted Nanoparticles for Effective Cancer Treatment: Advances and Outlook. NPG Asia Mater 2022, 14, 1–16. [CrossRef]
- Wei, W.; Rosenkrans, Z.T.; Luo, Q.-Y.; Lan, X.; Cai, W. Exploiting Nanomaterial-Mediated Autophagy for Cancer Therapy. Small Methods 2019, 3, 1800365. [CrossRef]
- Yuan, Z.; He, J.; Li, Z.; Fan, B.; Zhang, L.; Man, X. Targeting Autophagy in Urological System Cancers: From Underlying Mechanisms to Therapeutic Implications. Biochimica et Biophysica Acta (BBA) - Reviews on Cancer 2024, 1879, 189196. [CrossRef]
- Long, X.; Yan, J.; Zhang, Z.; Chang, J.; He, B.; Sun, Y.; Liang, Y. Autophagy-Targeted Nanoparticles for Effective Cancer Treatment: Advances and Outlook. NPG Asia Mater 2022, 14, 1–16. [CrossRef]
- He, K.; Chen, M.; Liu, J.; Du, S.; Ren, C.; Zhang, J. Nanomedicine for Cancer Targeted Therapy with Autophagy Regulation. Front Immunol 2024, 14, 1238827. [CrossRef]
- Dowaidar, M. Guidelines for the Role of Autophagy in Drug Delivery Vectors Uptake Pathways. Heliyon 2024, 10, e30238. [CrossRef]
- Wang, L.; Chang, Y.; Feng, Y.; Li, X.; Cheng, Y.; Jian, H.; Ma, X.; Zheng, R.; Wu, X.; Xu, K.; et al. Nitric Oxide Stimulated Programmable Drug Release of Nanosystem for Multidrug Resistance Cancer Therapy. Nano Lett 2019, 19, 6800–6811. [CrossRef]
- de la Cruz-Ojeda, P.; Flores-Campos, R.; Dios-Barbeito, S.; Navarro-Villarán, E.; Muntané, J. Role of Nitric Oxide in Gene Expression Regulation during Cancer: Epigenetic Modifications and Non-Coding RNAs. Int J Mol Sci 2021, 22, 6264. [CrossRef]
- Cauwenbergh, T.; Ballet, S.; Martin, C. Peptide Hydrogel-Drug Conjugates for Tailored Disease Treatment. Materials Today Bio 2025, 31, 101423. [CrossRef]
- Falcone, N.; Ermis, M.; Tamay, D.G.; Mecwan, M.; Monirizad, M.; Mathes, T.G.; Jucaud, V.; Choroomi, A.; Barros, N.; Zhu, Y.; et al. Peptide Hydrogels as Immunomaterials and Their Use in Cancer Immunotherapy Delivery. Adv Healthc Mater 2023, 12, e2301096. [CrossRef]
- Yadav, P.; Ambudkar, S.V.; Rajendra Prasad, N. Emerging Nanotechnology-Based Therapeutics to Combat Multidrug-Resistant Cancer. J Nanobiotechnology 2022, 20, 423. [CrossRef]
- Ashique, S.; Garg, A.; Hussain, A.; Farid, A.; Kumar, P.; Taghizadeh-Hesary, F. Nanodelivery Systems: An Efficient and Target-specific Approach for Drug-resistant Cancers. Cancer Med 2023, 12, 18797–18825. [CrossRef]
- Wang, L.; Chang, Y.; Feng, Y.; Li, X.; Cheng, Y.; Jian, H.; Ma, X.; Zheng, R.; Wu, X.; Xu, K.; et al. Nitric Oxide Stimulated Programmable Drug Release of Nanosystem for Multidrug Resistance Cancer Therapy. Nano Lett 2019, 19, 6800–6811. [CrossRef]
- Esmaeilpour, D.; Ghomi, M.; Zare, E.N.; Sillanpää, M. Recent Advances in DNA Nanotechnology for Cancer Detection and Therapy: A Review. International Journal of Biological Macromolecules 2025, 307, 142136. [CrossRef]
- Sousa, C.; Videira, M. Dual Approaches in Oncology: The Promise of siRNA and Chemotherapy Combinations in Cancer Therapies. Onco 2025, 5, 2. [CrossRef]
- Tong, L.; Liu, D.; Cao, Z.; Zheng, N.; Mao, C.; Liu, S.; He, L.; Liu, S. Research Status and Prospect of Non-Viral Vectors Based on siRNA: A Review. Int J Mol Sci 2023, 24, 3375. [CrossRef]
- Yhee, J.Y.; Song, S.; Lee, S.J.; Park, S.-G.; Kim, K.-S.; Kim, M.G.; Son, S.; Koo, H.; Kwon, I.C.; Jeong, J.H.; et al. Cancer-Targeted MDR-1 siRNA Delivery Using Self-Cross-Linked Glycol Chitosan Nanoparticles to Overcome Drug Resistance. Journal of Controlled Release 2015, 198, 1–9. [CrossRef]
- Mir, S.A.; Hamid, L.; Bader, G.N.; Shoaib, A.; Rahamathulla, M.; Alshahrani, M.Y.; Alam, P.; Shakeel, F. Role of Nanotechnology in Overcoming the Multidrug Resistance in Cancer Therapy: A Review. Molecules 2022, 27, 6608. [CrossRef]
- Maimaitijiang, A.; He, D.; Li, D.; Li, W.; Su, Z.; Fan, Z.; Li, J. Progress in Research of Nanotherapeutics for Overcoming Multidrug Resistance in Cancer. International Journal of Molecular Sciences 2024, 25, 9973. [CrossRef]
- Meng, H.; Mai, W.X.; Zhang, H.; Xue, M.; Xia, T.; Lin, S.; Wang, X.; Zhao, Y.; Ji, Z.; Zink, J.I.; et al. Co-Delivery of an Optimal Drug/siRNA Combination Using Mesoporous Silica Nanoparticle to Overcome Drug Resistance in Breast Cancer In Vitro and In Vivo. ACS Nano 2013, 7, 994–1005. [CrossRef]
- Kim, H.-K.; Cheong, H.; Kim, M.-Y.; Jin, H.-E. Therapeutic Targeting in Ovarian Cancer: Nano-Enhanced CRISPR/Cas9 Gene Editing and Drug Combination Therapy. Int J Nanomedicine 2025, 20, 3907–3931. [CrossRef]
- Omy, T.R.; Sah, N.; Reedy, M.; Acharya, G.; Palle, K. Abstract 3090: miRNA-221-5p-Mediated Epigenetic Regulation Promotes Chemoresistance and Offers Therapeutic Potential in Ovarian Cancer. Cancer Research 2025, 85, 3090. [CrossRef]
- Sah, N.; Peddibhotla, S.; Richardson, B.; Luna, P.; Bansal, N.A.; Mani, C.; Reedy, M.; Palle, K. Abstract A084: Oncogenic Role for Upregulated Lymphoblastic Leukemia Derived Sequence-1 in the Progression of Ovarian Cancer and Its Metastasis. Cancer Epidemiology, Biomarkers & Prevention 2023, 32, A084. [CrossRef]
- Tong, L.; Liu, D.; Cao, Z.; Zheng, N.; Mao, C.; Liu, S.; He, L.; Liu, S. Research Status and Prospect of Non-Viral Vectors Based on siRNA: A Review. Int J Mol Sci 2023, 24, 3375. [CrossRef]
- Maimaitijiang, A.; He, D.; Li, D.; Li, W.; Su, Z.; Fan, Z.; Li, J. Progress in Research of Nanotherapeutics for Overcoming Multidrug Resistance in Cancer. International Journal of Molecular Sciences 2024, 25, 9973. [CrossRef]
- Agiba, A.M.; Arreola-Ramírez, J.L.; Carbajal, V.; Segura-Medina, P. Light-Responsive and Dual-Targeting Liposomes: From Mechanisms to Targeting Strategies. Molecules 2024, 29, 636. [CrossRef]
- Rout, B.; Maharana, S.K.; Jain, A. Stimuli-Responsive Nanoparticles: A Novel Approach for Melanoma Treatment. J Nanopart Res 2025, 27, 34. [CrossRef]
- Szwed, M.; Jost, T.; Majka, E.; Gharibkandi, N.A.; Majkowska-Pilip, A.; Frey, B.; Bilewicz, A.; Fietkau, R.; Gaipl, U.; Marczak, A.; et al. Pt-Au Nanoparticles in Combination with Near-Infrared-Based Hyperthermia Increase the Temperature and Impact on the Viability and Immune Phenotype of Human Hepatocellular Carcinoma Cells. Int J Mol Sci 2025, 26, 1574. [CrossRef]
- He, X.; Zhang, S.; Tian, Y.; Cheng, W.; Jing, H. Research Progress of Nanomedicine-Based Mild Photothermal Therapy in Tumor. Int J Nanomedicine 2023, 18, 1433–1468. [CrossRef]
- Gold Nanoparticles in Photothermal Therapy - CD Bioparticles Available online: https://www.cd-bioparticles.com/support/gold-nanoparticles-in-photothermal-therapy.html (accessed on 29 May 2025).
- Ayana, G.; Ryu, J.; Choe, S. Ultrasound-Responsive Nanocarriers for Breast Cancer Chemotherapy. Micromachines (Basel) 2022, 13, 1508. [CrossRef]
- Pourmadadi, M.; Tajiki, A.; Hosseini, S.M.; Samadi, A.; Abdouss, M.; Daneshnia, S.; Yazdian, F. A Comprehensive Review of Synthesis, Structure, Properties, and Functionalization of MoS2; Emphasis on Drug Delivery, Photothermal Therapy, and Tissue Engineering Applications. Journal of Drug Delivery Science and Technology 2022, 76, 103767. [CrossRef]
- Chen, H.-H.; Lu, I.-L.; Liu, T.-I.; Tsai, Y.-C.; Chiang, W.-H.; Lin, S.-C.; Chiu, H.-C. Indocyanine Green/Doxorubicin-Encapsulated Functionalized Nanoparticles for Effective Combination Therapy against Human MDR Breast Cancer. Colloids Surf B Biointerfaces 2019, 177, 294–305. [CrossRef]
- Awad, N.S.; Paul, V.; AlSawaftah, N.M.; ter Haar, G.; Allen, T.M.; Pitt, W.G.; Husseini, G.A. Ultrasound-Responsive Nanocarriers in Cancer Treatment: A Review. ACS Pharmacol Transl Sci 2021, 4, 589–612. [CrossRef]
- Al Refaai, K.A.; AlSawaftah, N.A.; Abuwatfa, W.; Husseini, G.A. Drug Release via Ultrasound-Activated Nanocarriers for Cancer Treatment: A Review. Pharmaceutics 2024, 16, 1383. [CrossRef]
- Pan, M.; Hu, D.; Yuan, L.; Yu, Y.; Li, Y.; Qian, Z. Newly Developed Gas-Assisted Sonodynamic Therapy in Cancer Treatment. Acta Pharm Sin B 2023, 13, 2926–2954. [CrossRef]
- Yu, J.; Hu, J.-R.; Tian, Y.; Lei, Y.-M.; Hu, H.-M.; Lei, B.-S.; Zhang, G.; Sun, Y.; Ye, H.-R. Nanosensitizer-Assisted Sonodynamic Therapy for Breast Cancer. J Nanobiotechnology 2025, 23, 281. [CrossRef]
- Lv, W.; Wu, H.; Zhang, Y.; Li, H.; Shu, H.; Su, C.; Zhu, Y.; Wang, T.; Nie, F. cRGD-Targeted Gold-Based Nanoparticles Overcome EGFR-TKI Resistance of NSCLC via Low-Temperature Photothermal Therapy Combined with Sonodynamic Therapy. Biomater. Sci. 2023, 11, 1677–1691. [CrossRef]
- Collins, V.G.; Hutton, D.; Hossain-Ibrahim, K.; Joseph, J.; Banerjee, S. The Abscopal Effects of Sonodynamic Therapy in Cancer. Br J Cancer 2025, 132, 409–420. [CrossRef]
- Zhang, Y.; Zhao, Y.; Zhang, Y.; Liu, Q.; Zhang, M.; Tu, K. The Crosstalk between Sonodynamic Therapy and Autophagy in Cancer. Front. Pharmacol. 2022, 13. [CrossRef]
- Jeong, Y.-G.; Park, J.-H.; Khang, D. Sonodynamic and Acoustically Responsive Nanodrug Delivery System: Cancer Application. Int J Nanomedicine 2024, 19, 11767–11788. [CrossRef]
- Foglietta, F.; Giacone, M.; Durando, G.; Canaparo, R.; Serpe, L. Sonodynamic Treatment Triggers Cancer Cell Killing by Doxorubicin in P-Glycoprotein-Mediated Multidrug Resistant Cancer Models. Advanced Therapeutics 2024, 7, 2400070. [CrossRef]
- Tharkar, P.; Varanasi, R.; Wong, W.S.F.; Jin, C.T.; Chrzanowski, W. Nano-Enhanced Drug Delivery and Therapeutic Ultrasound for Cancer Treatment and Beyond. Front Bioeng Biotechnol 2019, 7, 324. [CrossRef]
- Bañobre-López, M.; Teijeiro, A.; Rivas, J. Magnetic Nanoparticle-Based Hyperthermia for Cancer Treatment. Rep Pract Oncol Radiother 2013, 18, 397–400. [CrossRef]
- Li, G.; Wang, C.; Jin, B.; Sun, T.; Sun, K.; Wang, S.; Fan, Z. Advances in Smart Nanotechnology-Supported Photodynamic Therapy for Cancer. Cell Death Discov. 2024, 10, 1–18. [CrossRef]
- Deng, W.; Chen, W.; Clement, S.; Guller, A.; Zhao, Z.; Engel, A.; Goldys, E.M. Controlled Gene and Drug Release from a Liposomal Delivery Platform Triggered by X-Ray Radiation. Nat Commun 2018, 9, 2713. [CrossRef]
- Gibney, M. X-Ray-Triggered Liposomes Deliver Precisely Controlled Cancer Treatment | Fierce Pharma Available online: https://www.fiercepharma.com/r-d/x-ray-triggered-liposomes-deliver-precisely-controlled-cancer-treatment (accessed on 4 June 2025).
- Lv, W.; Wu, H.; Zhang, Y.; Li, H.; Shu, H.; Su, C.; Zhu, Y.; Wang, T.; Nie, F. cRGD-Targeted Gold-Based Nanoparticles Overcome EGFR-TKI Resistance of NSCLC via Low-Temperature Photothermal Therapy Combined with Sonodynamic Therapy. Biomater. Sci. 2023, 11, 1677–1691. [CrossRef]
- Spoială, A.; Ilie, C.-I.; Motelica, L.; Ficai, D.; Semenescu, A.; Oprea, O.-C.; Ficai, A. Smart Magnetic Drug Delivery Systems for the Treatment of Cancer. Nanomaterials 2023, 13, 876. [CrossRef]
- BSN, A.B.B.L. Magnetic Nanoparticles for Drug Delivery Available online: https://www.news-medical.net/health/Magnetic-Nanoparticles-for-Drug-Delivery.aspx (accessed on 5 June 2025).
- Ren, Y.; Zhang, H.; Chen, B.; Cheng, J.; Cai, X.; Liu, R.; Xia, G.; Wu, W.; Wang, S.; Ding, J.; et al. Multifunctional Magnetic Fe3O4 Nanoparticles Combined with Chemotherapy and Hyperthermia to Overcome Multidrug Resistance. Int J Nanomedicine 2012, 7, 2261–2269. [CrossRef]
- Yun, W.S.; Kim, J.; Lim, D.-K.; Kim, D.-H.; Jeon, S.I.; Kim, K. Recent Studies and Progress in the Intratumoral Administration of Nano-Sized Drug Delivery Systems. Nanomaterials 2023, 13, 2225. [CrossRef]
- Katopodi, T.; Petanidis, S.; Floros, G.; Porpodis, K.; Kosmidis, C. Hybrid Nanogel Drug Delivery Systems: Transforming the Tumor Microenvironment through Tumor Tissue Editing. Cells 2024, 13, 908. [CrossRef]
- Koirala, M.; DiPaola, M. Overcoming Cancer Resistance: Strategies and Modalities for Effective Treatment. Biomedicines 2024, 12, 1801. [CrossRef]
- Acter, S.; Moreau, M.; Ivkov, R.; Viswanathan, A.; Ngwa, W. Polydopamine Nanomaterials for Overcoming Current Challenges in Cancer Treatment. Nanomaterials 2023, 13, 1656. [CrossRef]
- Dong, Z.; Gong, H.; Gao, M.; Zhu, W.; Sun, X.; Feng, L.; Fu, T.; Li, Y.; Liu, Z. Polydopamine Nanoparticles as a Versatile Molecular Loading Platform to Enable Imaging-Guided Cancer Combination Therapy. Theranostics 2016, 6, 1031–1042. [CrossRef]
- Li, Z.; Wang, B.; Zhang, Z.; Wang, B.; Xu, Q.; Mao, W.; Tian, J.; Yang, K.; Wang, F. Radionuclide Imaging-Guided Chemo-Radioisotope Synergistic Therapy Using a 131I-Labeled Polydopamine Multifunctional Nanocarrier. Mol Ther 2018, 26, 1385–1393. [CrossRef]
- Zhou, X.; Wang, L.; Wu, Y.; Lin, X.; Liu, F.; Sun, X.; Song, K.; Jiang, C.; Zhao, F.; Li, X. Bioactive Polydopamine Nanomedicines-Assisted Cancer Immunotherapy. Materials Today Bio 2025, 32, 101864. [CrossRef]
- Długosz, O.; Matyjasik, W.; Hodacka, G.; Szostak, K.; Matysik, J.; Krawczyk, P.; Piasek, A.; Pulit-Prociak, J.; Banach, M. Inorganic Nanomaterials Used in Anti-Cancer Therapies:Further Developments. Nanomaterials 2023, 13, 1130. [CrossRef]
- Newton Amaldoss, M.J.; Sorrell, C.C. ROS Modulating Inorganic Nanoparticles: A Novel Cancer Therapeutic Tool. Recent Adv Drug Deliv Formul 2022, 16, 84–89. [CrossRef]
- Mohapatra, A.; Mohanty, A.; Park, I.-K. Inorganic Nanomedicine—Mediated Ferroptosis: A Synergistic Approach to Combined Cancer Therapies and Immunotherapy. Cancers 2024, 16, 3210. [CrossRef]
- Bharde, A. Targeting Redox Homeostasis in Tumor Cells Using Nanoparticles. In Handbook of Oxidative Stress in Cancer: Therapeutic Aspects; Springer, Singapore, 2022; pp. 1–17 ISBN 9789811612473.
- Pareek, A.; Kumar, D.; Pareek, A.; Gupta, M.M. Advancing Cancer Therapy with Quantum Dots and Other Nanostructures: A Review of Drug Delivery Innovations, Applications, and Challenges. Cancers (Basel) 2025, 17, 878. [CrossRef]
- He, Z.-Y.; Jin, Z.-H.; Zhan, M.; Qin, Z.; Li, Z.; Xu, T. Advances in Quantum Dot-Mediated siRNA Delivery. Chinese Chemical Letters 2017, 28, 1851–1856. [CrossRef]
- Wang, N.; Chen, L.; Huang, W.; Gao, Z.; Jin, M. Current Advances of Nanomaterial-Based Oral Drug Delivery for Colorectal Cancer Treatment. Nanomaterials 2024, 14, 557. [CrossRef]
- Kanojia, N.; Thapa, K.; Verma, N.; Rani, L.; Sood, P.; Kaur, G.; Dua, K.; Kumar, J. Update on Mucoadhesive Approaches to Target Drug Delivery in Colorectal Cancer. Journal of Drug Delivery Science and Technology 2023, 87, 104831. [CrossRef]
- Gvozdeva, Y.; Staynova, R. pH-Dependent Drug Delivery Systems for Ulcerative Colitis Treatment. Pharmaceutics 2025, 17, 226. [CrossRef]
- Jakobušić Brala, C.; Karković Marković, A.; Kugić, A.; Torić, J.; Barbarić, M. Combination Chemotherapy with Selected Polyphenols in Preclinical and Clinical Studies—An Update Overview. Molecules 2023, 28, 3746. [CrossRef]
- C. de S. L. Oliveira, A.L.; Schomann, T.; de Geus-Oei, L.-F.; Kapiteijn, E.; Cruz, L.J.; de Araújo Junior, R.F. Nanocarriers as a Tool for the Treatment of Colorectal Cancer. Pharmaceutics 2021, 13, 1321. [CrossRef]
- 4dm1n_diversatechnologies Overcoming Regulatory Hurdles in Clinical Translation of Nanomedicine. DIVERSA 2025.
- Foulkes, R.; Man, E.; Thind, J.; Yeung, S.; Joy, A.; Hoskins, C. The Regulation of Nanomaterials and Nanomedicines for Clinical Application: Current and Future Perspectives. Biomater Sci 2020, 8, 4653–4664. [CrossRef]
- Agrahari, V.; and Hiremath, P. Challenges Associated and Approaches for Successful Translation of Nanomedicines Into Commercial Products. Nanomedicine 2017, 12, 819–823. [CrossRef]
- Desai, N. Challenges in Development of Nanoparticle-Based Therapeutics. AAPS J 2012, 14, 282–295. [CrossRef]
- Safety Concerns with Nanotechnology in Medicine - Society for Brain Mapping and Therapeutics 2024.
- Dobrovolskaia, M.A.; Aggarwal, P.; Hall, J.B.; McNeil, S.E. Preclinical Studies To Understand Nanoparticle Interaction with the Immune System and Its Potential Effects on Nanoparticle Biodistribution. Mol Pharm 2008, 5, 487–495. [CrossRef]
- Desai, N. Challenges in Development of Nanoparticle-Based Therapeutics. AAPS J 2012, 14, 282–295. [CrossRef]
- Bedőcs, P.; Szebeni, J. The Critical Choice of Animal Models in Nanomedicine Safety Assessment: A Lesson Learned From Hemoglobin-Based Oxygen Carriers. Front Immunol 2020, 11, 584966. [CrossRef]
- Sah, N.; Ramaiah, B.; Koneri, R. Sulfasalazine-Induced Drug Rash with Eosinophilia and Systemic Symptoms Syndrome in a Seronegative Spondyloarthritis Patient: A Case Report. Indian Journal of Pharmacology 2021, 53, 391. [CrossRef]
- Varghese, J.; Sah, N.; Ramaiah, B. PDG50 Obstacles in the IV to ORAL Antibiotic Shift for Eligible Patients at a Tertiary Care Hospital. Value in Health 2020, 23, S527. [CrossRef]
- Sah, N.; Ramaiah, B.; Abdulla; Gupta, A.K.; Thomas, S.M. Noncompliance with Prescription-Writing Guidelines in an OutpatientDepartment of a Tertiary Care Hospital: A Prospective, Observational Study. rjps 2020, 10. [CrossRef]
- Varghese, J.; Sah, N.; Thomas, S.M.; Jose, J.C.; Ramaiah, B.; Koneri, R. PDG6 Clinical Evaluation of Skin and Soft Tissue Infections in Inpatient Versus Outpatient Setting at a Tertiary Care Hospital - a Prospective Study. Value in Health 2020, 23, S521–S522. [CrossRef]
- Sah, N.; Ramaiah, B.; Koneri, R. The Pharmacist Role in Clinical Audit at an Indian Accredited Hospital: An Interventional Study. IJOPP 2019, 12, 117–125. [CrossRef]
- 4dm1n_diversatechnologies Overcoming Regulatory Hurdles in Clinical Translation of Nanomedicine. DIVERSA 2025.
- Agrahari, V.; and Hiremath, P. Challenges Associated and Approaches for Successful Translation of Nanomedicines Into Commercial Products. Nanomedicine 2017, 12, 819–823. [CrossRef]
- Agrahari, V.; and Hiremath, P. Challenges Associated and Approaches for Successful Translation of Nanomedicines Into Commercial Products. Nanomedicine 2017, 12, 819–823. [CrossRef]
- Clark, B. Lab to Industry: Scaling Up Nanotechnology for Practical Applications. Journal of Nanomaterials & Molecular Nanotechnology 2024, 2024.
- Policy Statements & Letters | Advocacy | ASGCT - American Society of Gene & Cell Therapy | ASGCT - American Society of Gene & Cell Therapy Available online: https://www.asgct.org/advocacy/policy-statement-landing/2023/manufacturing-changes-and-comparability-for-human (accessed on 5 June 2025).
- Nguyen, H.-M.; Sah, N.; Humphrey, M.R.M.; Rabkin, S.D.; Saha, D. Growth, Purification, and Titration of Oncolytic Herpes Simplex Virus. J Vis Exp 2021, 10.3791/62677. [CrossRef]
- Nanomedicine Market Share, Size & Growth Report | 2032 Available online: https://www.skyquestt.com/report/nanomedicine-market (accessed on 5 June 2025).
- Đorđević, S.; Gonzalez, M.M.; Conejos-Sánchez, I.; Carreira, B.; Pozzi, S.; Acúrcio, R.C.; Satchi-Fainaro, R.; Florindo, H.F.; Vicent, M.J. Current Hurdles to the Translation of Nanomedicines from Bench to the Clinic. Drug Deliv Transl Res 2022, 12, 500–525. [CrossRef]
- Navigating Nanomedicine Regulatory Requirements in 2024 Available online: https://www.izon.com/news/navigating-nanomedicine-regulatory-requirements-in-2023 (accessed on 5 June 2025).
- Richmond, A.; Su, Y. Mouse Xenograft Models vs GEM Models for Human Cancer Therapeutics. Dis Model Mech 2008, 1, 78–82. [CrossRef]
- Shen, X.; Pan, D.; Gong, Q.; Gu, Z.; Luo, K. Enhancing Drug Penetration in Solid Tumors via Nanomedicine: Evaluation Models, Strategies and Perspectives. Bioactive Materials 2024, 32, 445–472. [CrossRef]
- Yuan, Z.; Li, Y.; Zhang, S.; Wang, X.; Dou, H.; Yu, X.; Zhang, Z.; Yang, S.; Xiao, M. Extracellular Matrix Remodeling in Tumor Progression and Immune Escape: From Mechanisms to Treatments. Molecular Cancer 2023, 22, 48. [CrossRef]
- Kim, J.; Cho, H.; Lim, D.-K.; Joo, M.K.; Kim, K. Perspectives for Improving the Tumor Targeting of Nanomedicine via the EPR Effect in Clinical Tumors. Int J Mol Sci 2023, 24, 10082. [CrossRef]
- Swetha, K.L.; Roy, A. Tumor Heterogeneity and Nanoparticle-Mediated Tumor Targeting: The Importance of Delivery System Personalization. Drug Deliv Transl Res 2018, 8, 1508–1526. [CrossRef]
- Ph.D, D.P.B. Nanomedicine: Advantages and Disadvantages Available online: https://www.azonano.com/article.aspx?ArticleID=6707 (accessed on 5 June 2025).
- Bosetti, R.; and Jones, S.L. Cost–Effectiveness of Nanomedicine: Estimating the Real Size of Nano-Costs. Nanomedicine 2019, 14, 1367–1370. [CrossRef]
- Hejmady, S.; Singhvi ,Gautam; Saha ,Ranendra Narayan; and Dubey, S.K. Regulatory Aspects in Process Development and Scale-up of Nanopharmaceuticals. Therapeutic Delivery 2020, 11, 341–343. [CrossRef]
- Das, A.; Adhikari, S.; Deka, D.; Baildya, N.; Sahare, P.; Banerjee, A.; Paul, S.; Bisgin, A.; Pathak, S. An Updated Review on the Role of Nanoformulated Phytochemicals in Colorectal Cancer. Medicina (Kaunas) 2023, 59, 685. [CrossRef]
- Degobert, G.; Aydin, D. Lyophilization of Nanocapsules: Instability Sources, Formulation and Process Parameters. Pharmaceutics 2021, 13, 1112. [CrossRef]
- Richardson, B.; Anderson, A.; Lakey, K.; Hickham, L.; Sah, N.; Mani, C.; Palle, K.; Reedy, M. Assessing the Need and Implementation of Health Literacy Testing for New Gynecologic Oncology Patients in West Texas: A Prospective Pilot Study. Texas Public Health Journal 2025, 77, 18–24.
- Wei, A.; Mehtala, J.G.; Patri, A.K. Challenges and Opportunities in the Advancement of Nanomedicines. J Control Release 2012, 164, 236–246. [CrossRef]
- Deb, T. Nanomedicine Statistics and Facts (2025). Market.us Media 2025.
- Rodríguez-Gómez, F.D.; Monferrer, D.; Penon, O.; Rivera-Gil, P. Regulatory Pathways and Guidelines for Nanotechnology-Enabled Health Products: A Comparative Review of EU and US Frameworks. Front Med (Lausanne) 2025, 12, 1544393. [CrossRef]
- Tracey, S.R.; Smyth, P.; Barelle, C.J.; Scott, C.J. Development of next Generation Nanomedicine-Based Approaches for the Treatment of Cancer: We’ve Barely Scratched the Surface. Biochem Soc Trans 2021, 49, 2253–2269. [CrossRef]
- 4dm1n_diversatechnologies Overcoming Regulatory Hurdles in Clinical Translation of Nanomedicine. DIVERSA 2025.
- Clinical Trial Designs Incorporating Predictive Biomarkers. Available online: https://www.broadinstitute.org/publications/broad7862 (accessed on 5 June 2025).
- Wang, Y.; Ma, Z.; Wong, K.-C.; Li, X. Nature-Inspired Multiobjective Patient Stratification from Cancer Gene Expression Data. Information Sciences 2020, 526, 245–262. [CrossRef]
- Mao, Y.; Xie, J.; Yang, F.; Luo, Y.; Du, J.; Xiang, H. Advances and Prospects of Precision Nanomedicine in Personalized Tumor Theranostics. Front Cell Dev Biol 2024, 12, 1514399. [CrossRef]
Figure 1.
TME modulation via Nanoparticles.
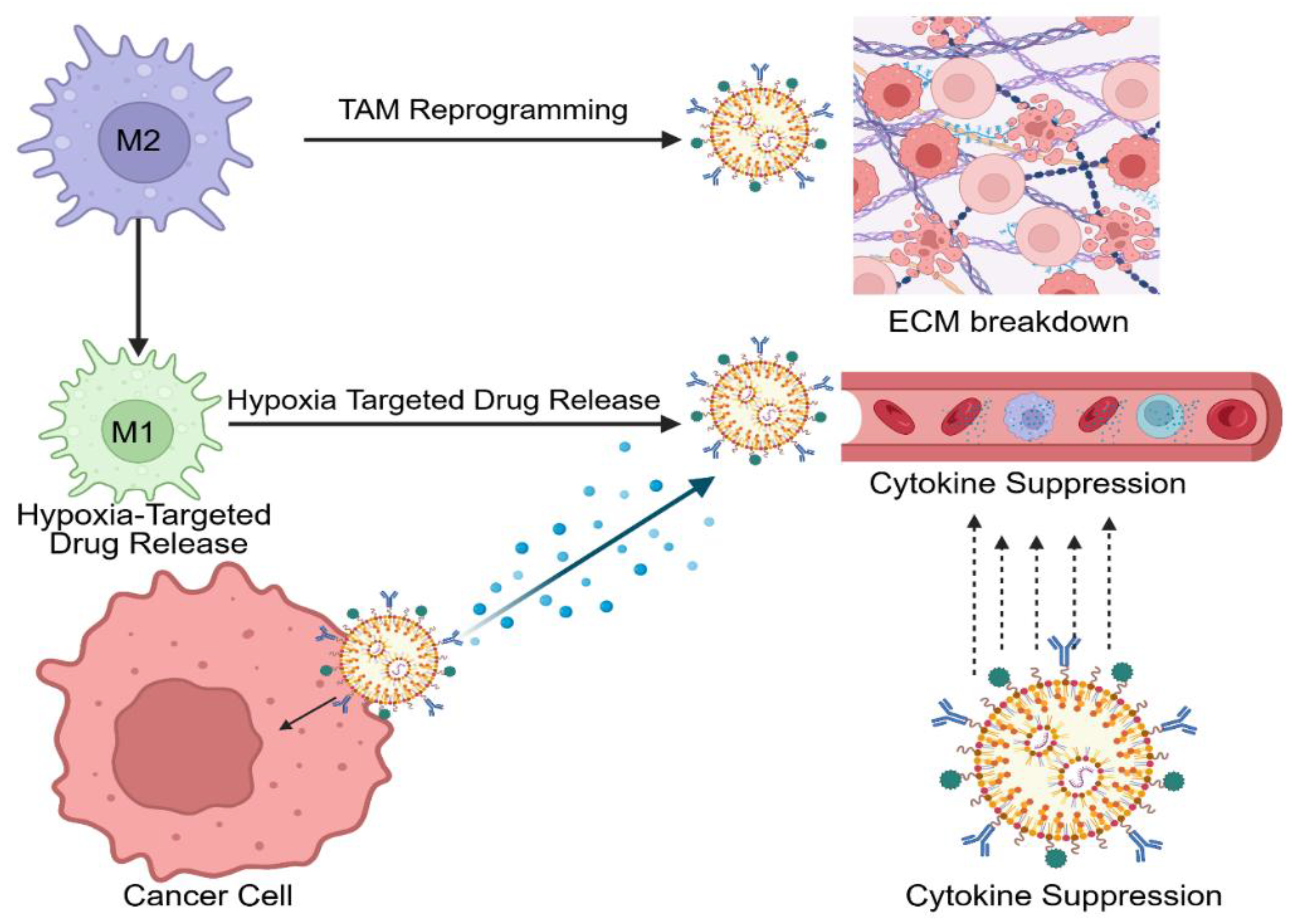
Figure 2.
Mechanistic Pathways of Nanomedicine Co-Delivery Platforms Targeting Multidrug Resistance Across Diverse Cancer Types.
Figure 2.
Mechanistic Pathways of Nanomedicine Co-Delivery Platforms Targeting Multidrug Resistance Across Diverse Cancer Types.
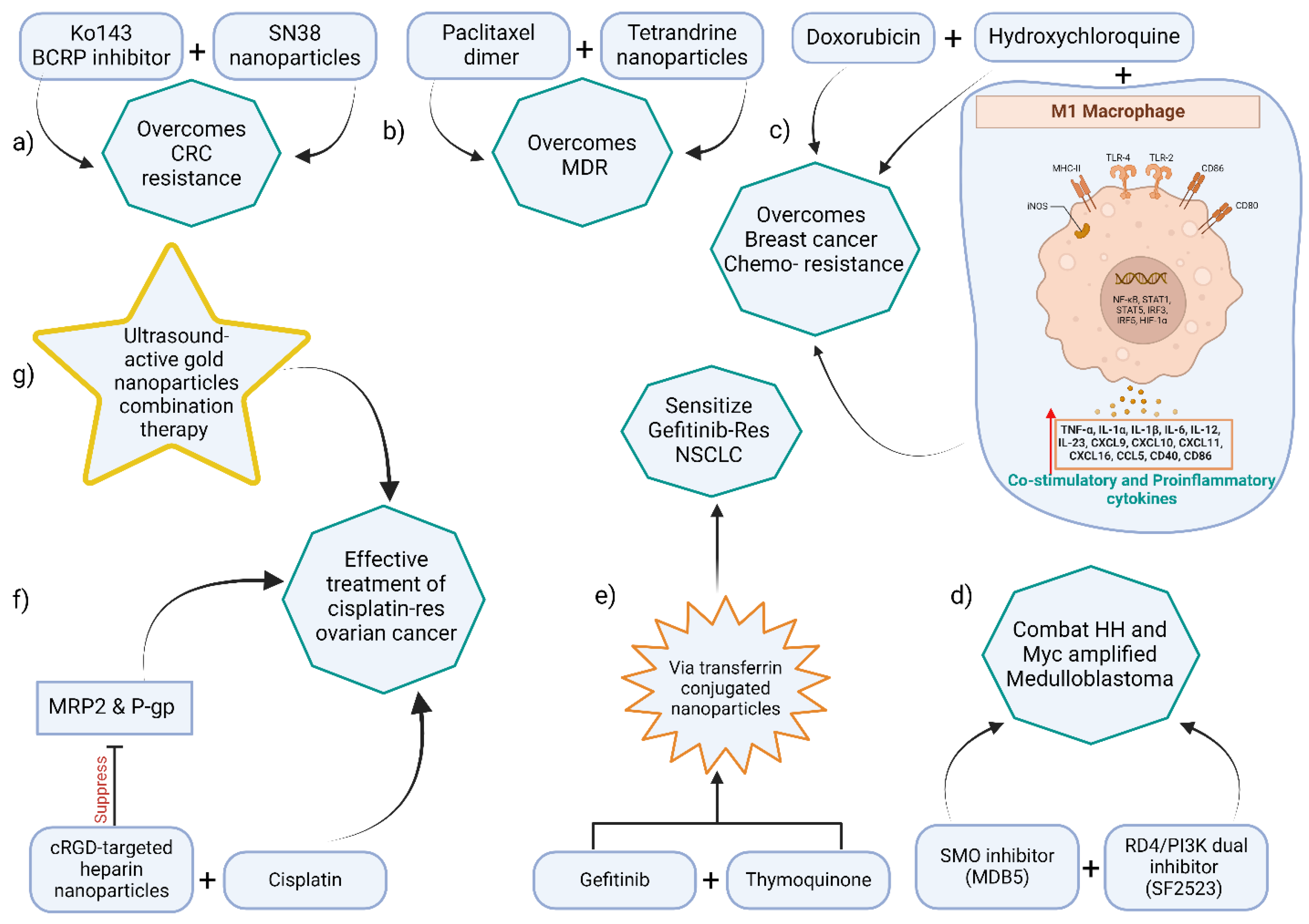
Table 2.
Stimuli-responsive nanotherapy modalities for MDR cancer.
| Stimulus | Mechanism (effects) | Representative Cancer Model/Type |
|---|---|---|
| Ultrasound (US)/SDT | Cavitation increases drug uptake; triggers ROS from sonosensitizers (deep penetration) | Pancreatic cancer, breast cancer, brain (glioblastoma) |
| Photothermal (PTT) | NIR light → nanoparticle heats tumor (45–60°C), causing protein denaturation and cell death (efflux-independent) | Skin, head/neck, breast tumors (where NIR penetrates) |
| Chemophotodynamic (PDT) | Light activates photosensitizer → ROS (singlet O₂); synergizes with chemo | Superficial tumors, MDR melanoma models |
| Sonodynamic (US + sensitizer) | Ultrasound activates sensitizer → ROS; deep-tissue effect | Deep tumors (brain, pancreas) |
| Hyperthermia | Elevated temperature triggers drug release (thermosensitive liposomes) and tumor cell death | Liver (HCC), prostate |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



