Submitted:
23 June 2025
Posted:
24 June 2025
You are already at the latest version
Abstract
Background/Objectives: To present a case report of eyelid dirofilariasis and conduct a systematic review of the corresponding literature. Methods: A 79-year-old patient presented with a painless mass in the left upper eyelid of 2 months duration, which was complicated during the latter period by two episodes of recurrent periorbital edema extending to the left cheek. The ophthalmic examination did not reveal any other ocular or adnexal pathology. On MRI images, the lesion was depicted as a slightly heterogeneous solid mass with unclear borders and heterogeneous enhancement. Results: A complete surgical excision of the lesion was performed, as the possibility of malignancy could not be ruled out. The histopathological examination revealed visible cross-sections of a nematode helminth, further identified as Dirofilaria repens based on its specific microscopic morphological characteristics, which ultimately established the diagnosis of dirofilariasis. A review of the respective literature, including 117 published cases, is provided attempting to summarize the clinical and diagnostic characteristics of the ocular cases of dirofilariasis affecting in specific, the eyelids. Conclusions: Ocular dirofilariasis should be included in the differential diagnosis of every eyelid subcutaneous tumor-like nodule or cyst of unknown etiology. An in-depth familiarization with its particularities is required in any sense, especially in the forthcoming years, when the endemic regions of Dirofilaria will expand, encompassing previously unaffected geographical areas.
Keywords:
Dirofilaria repens
; parasitosis
; ocular dirofilariasis
; palpebral mass
; eyelid lesion
1. Introduction
Human dirofilariasis, albeit a rare helminthic zoonotic infection in total, represents nowadays an increasingly reported worldwide entity. This anthropozoonosis is endemic in many countries with mild, moist, semitropical or tropical climate conditions, such as the Mediterranean coast, Southern and Eastern Europe, Minor and Central Asia, North and South America, while it has also been associated with travelers’ infections [1,2]. Nevertheless, global warming (especially warm summers), linked with the continuing outspread of competent vectors in northern latitudes, along with global mobility of people, are to blame for an ongoing spread of Dirofilaria infections in previously pure zones, such as Europe [3].
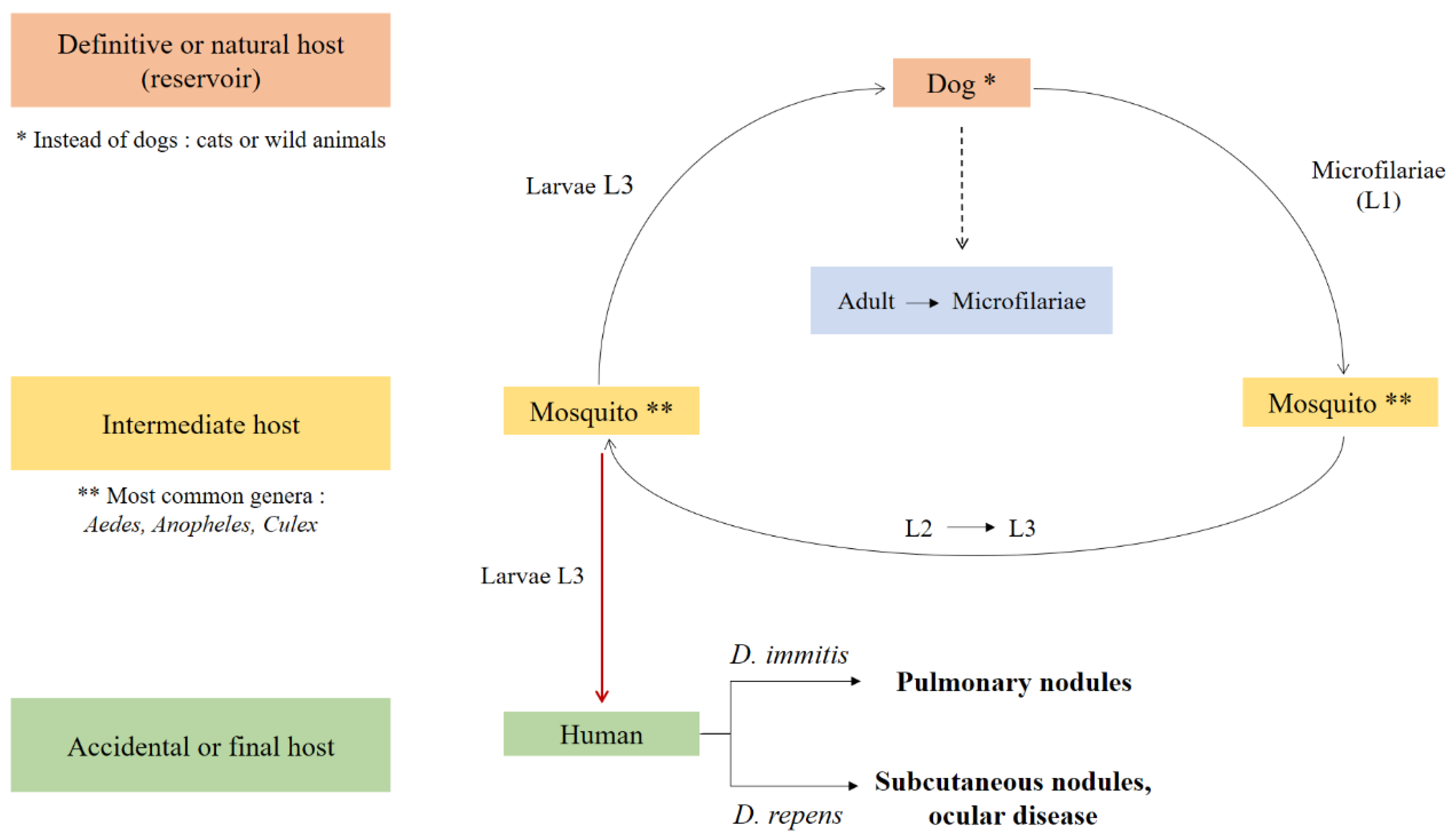
The responsible pathogen is a nematode classified in the genus Dilofilaria being transmitted to humans (the accidental or final host) via more than 70 different genera of mosquito vectors (intermediate hosts) [4] from other multiple definitive or natural hosts (reservoirs), mainly domesticated (dogs, cats) and secondly wild animals [2] (Figure 1). Out of the 40 species of Dirofilaria, only six are liable for human disease: D. repens, D. immitis, D. tenuis, D. ursi, D. striata , and D. spectans [5]. D. repens and D. immitis are the two most predominant, with D. repens being reported in the majority of cases from Europe and Greece in specific [6]. Despite that Dirofilaria species infections have been diagnosticated in various anatomical sites, ocular and periorbital localization remains one of the most frequent in general [2,6]. Due to the non-specific, polymorphic, and sometimes confusing clinical appearance, as a rule, the correct diagnosis is settled retrospectively through histopathological examination, except possibly in cases where a protruding worm is noticed during clinical evaluation [7].
Figure 1.
Graphical representation of Dirofilaria spp life cycle.
In this article, we report a case of eyelid dirofilariasis, which presented without any specific history, posing a diagnostic dilemma. The existing bibliography, relevant to this condition, is not particularly extensive and, in fact, it consists of scattered and heterogeneous data. Therefore, we herein also provide a thoroughly updated review on the subject. To the best of our knowledge, this is the first attempt in the literature to gather data from all reported clinical cases of eyelid dirofilariasis.
1.1. Case Report
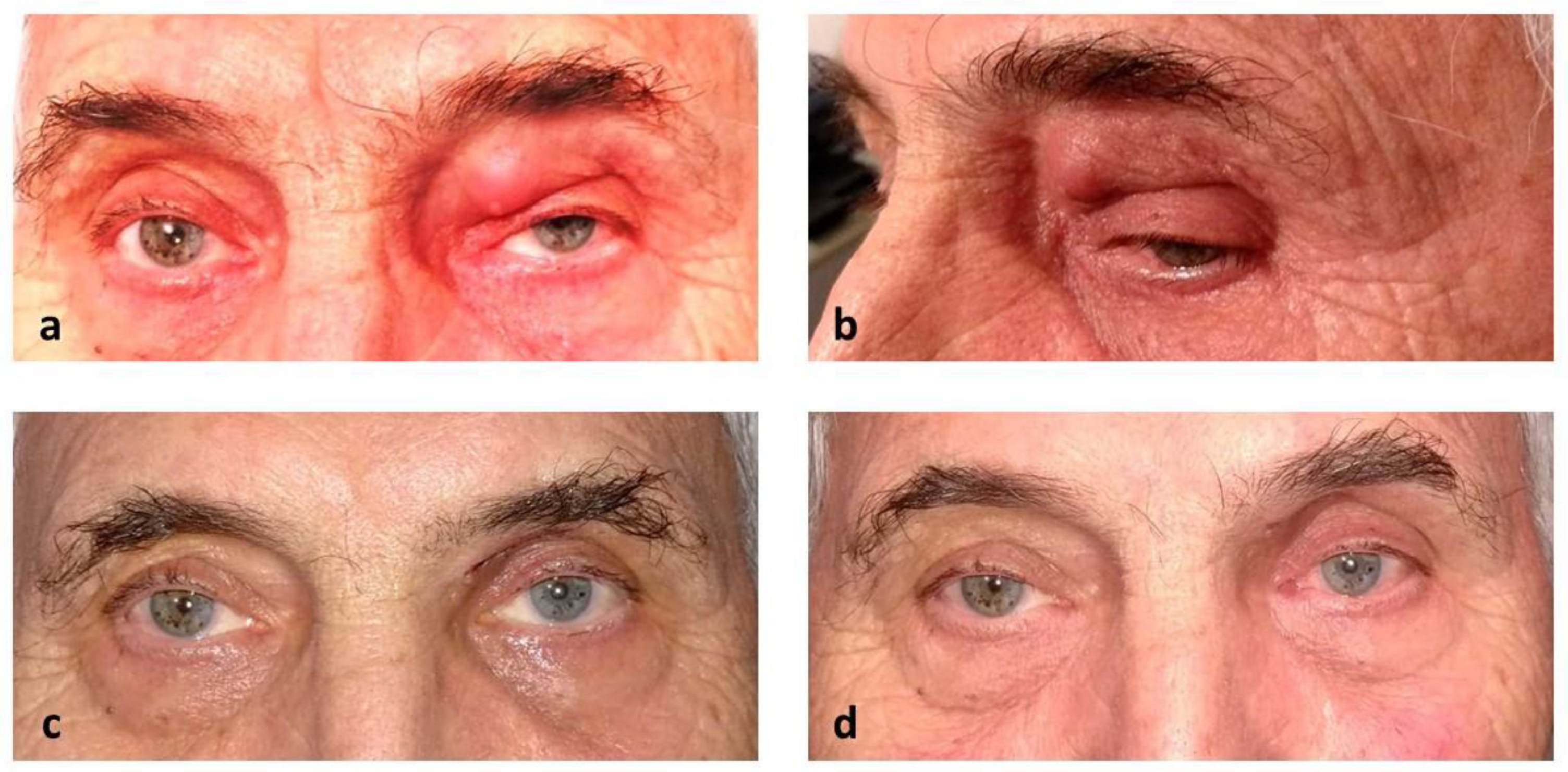
A 79-year-old male patient presented with a painless mass in his left upper eyelid of 2 months duration (Figure 2 a-b). The patient reported that during the latter period he had experienced two episodes of periorbital edema extending to the cheek. By the time of consultation, the patient was already receiving systemic antibiotic (azithromycin, 250mg/day) and corticosteroid (methylprednisolone, 16mg/day) treatment, prescribed a week earlier by another physician. The clinical examination revealed a palpable mass, firm in consistency, without any fluctuance, tenderness or signs of bite on its surface. The overlying skin had no findings, whereas no other ocular pathology was observed.
Figure 2.
Clinical photographs showing our case of dirofilariasis–related left eyelid lesion upon presentation (a & b), 1 week (c), and 1 month postoperatively (d).
Figure 2.
Clinical photographs showing our case of dirofilariasis–related left eyelid lesion upon presentation (a & b), 1 week (c), and 1 month postoperatively (d).
On further examination, MRI scan showed a slightly heterogeneous solid mass (hypo- to iso-intense in T1 and T2, respectively), with slightly irregular borders and heterogeneous enhancement with gadolinium (Figure 3 a-b). The radiologist’s report could not exclude the possibility of malignancy. Therefore, an excisional biopsy of the mass under local anesthesia was decided, which was performed 3 days later. Regarding the surgical procedure, the mass was approached through a medial sub-brow incision, and part of the overlying skin was removed. Intraoperatively, during the exploration, there were signs of adjacent tissues’ infiltration and induration. The excision of the mass was complete (excision in toto) with the excision margins reaching the periosteum. Special care was taken to preserve and avoid any damage to the levator palpebrae superioris muscle. The tissue sample was marked and sent for histopathologic evaluation.
Figure 3.
T1 (a) and T2 (b) MRI scans depicting the lesion in the left upper eyelid, and histopathological findings after H&E stain (c, d).
Figure 3.
T1 (a) and T2 (b) MRI scans depicting the lesion in the left upper eyelid, and histopathological findings after H&E stain (c, d).
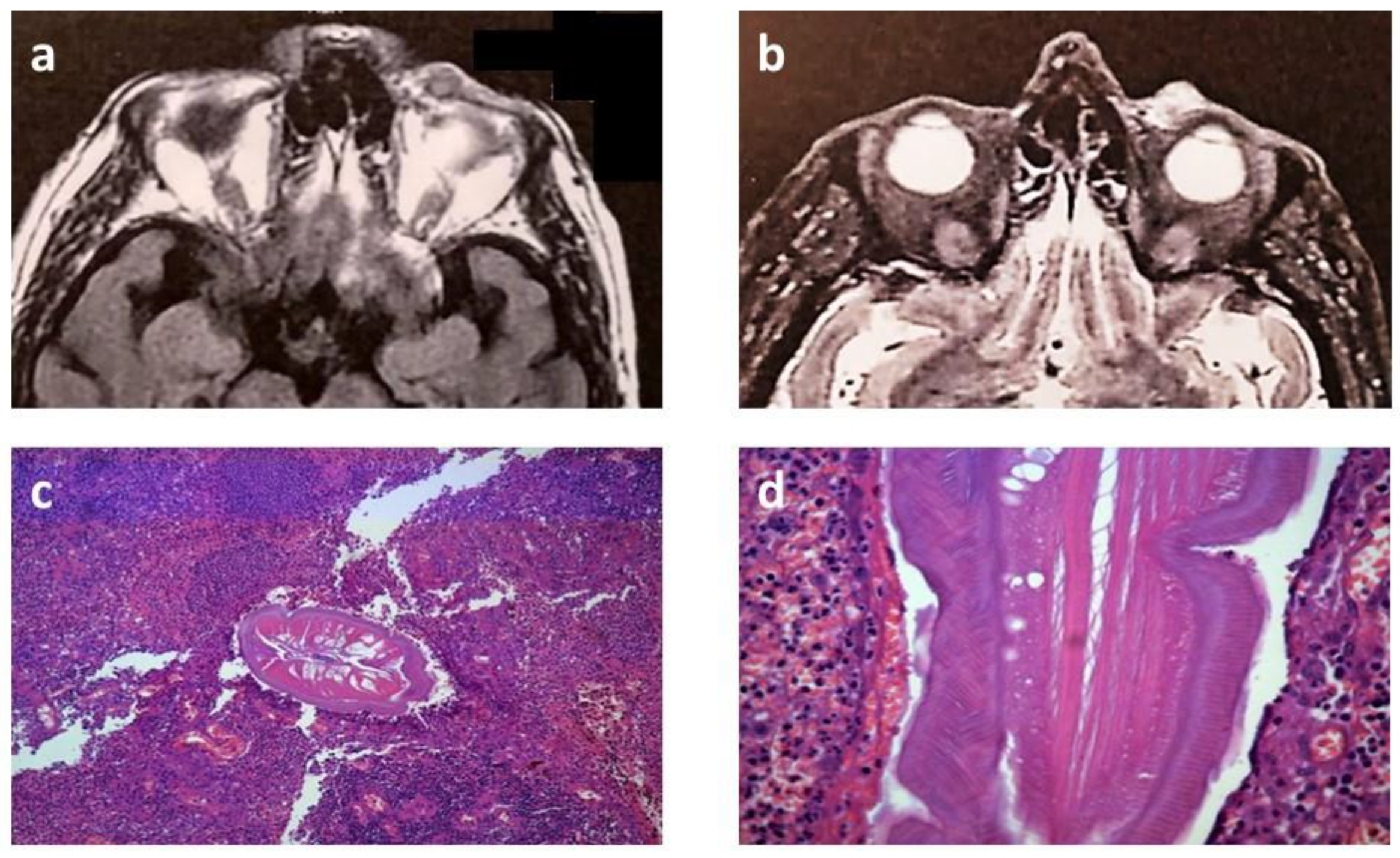
The pathology laboratory received a tissue sample of a spindle-shaped skin section measuring 1,9*1,2 cm with subcutaneous tissue thickness of 0.9 cm. For the most part, histological examination revealed growth of inflammatory granulation tissue in cutis, subcutaneous fat, and orbicularis oculi muscle with abundant inflammatory infiltrates by lymphocytes, plasma cells, and numerous neutrophils, abscessation, and bleeding sites. In one spot, there were visible cross-sections of a nematode helminth, further identified as Dilofilaria repens based on its specific microscopic morphological characteristics (Figure 3 c-d).
Postoperative edema subsided completely after 1 week. There were no visible signs of inflammation, and the wound healing of the surgical incision was uneventful (Figure 2 c-d). No recurrences or other complications were seen during a 2-year follow-up.
2. Discussion
2.1. Synopsis of Dilofiraria’s Life Cycle
As mentioned above, dirofilariasis is spread to humans through mosquito bites. Those vectors harbor larvae obtained from animal reservoirs and allow them to mature through the L2 and L3 stages. Dirofilaria nematodes are deposited in humans as third-stage filarial larvae (L3) of their life cycle, every time a female mosquito-carrier takes a blood meal (Figure 1). In human tissues, the larvae give birth to reproductively inactive adult worms, and thus no microfilaremia is detected [1,2], which signifies that the life cycle is incomplete, fully justifying the term “accidental hosts” for infected humans (biological dead end). Nonetheless, Sergiev et al. reported a case of a patient in whom microfilaremia (L1 stage) and reproductively active parasites were present, questioning our previous knowledge [8]. As a rule, worms of species D. immitis migrate to the pulmonary circulation and form pulmonary nodules, whereas D. repens worms are responsible for subcutaneous nodules, including the ocular region [9]. However, cases of subcutaneous eyelid disease linked with D. immitis have interestingly been reported as well [10].
2.2. Ocular dirofilariasis and Involved Tissues
In humans, cases of ocular dirofilariasis represent approximately one-third of the total reported incidents [11]. Regarding the involvement of ocular tissues, even though the subconjunctival area constitutes the prevailing site [12], Dirofilaria nematodes have also been isolated from lesions found in the eyelids subcutaneously, below the Tenon’s layer [13], in the orbital zones, intraocularly (in the anterior chamber or in the vitreous body) [14,15], in the retrobulbar region [16] or, lastly, in the lacrimal glands [17]. Recently, Gupta et al. reported on a case of ocular dirofilariasis leading to extensive chorioretinal damage and presented clinically as diffuse unilateral subacute neuroretinitis [18].
2.3. Eyelid Dirofilariasis
2.3.1. Literature Review - Methodology
Bibliographically, there are numerous reports of ocular dirofilariasis concerning the eyelid. We, herein, provide an up-to-date review of the literature relating to published cases. PubMed, Cochrane Library, and Web of Science databases were searched using a predefined search algorithm (Supplemental Appendix 1) for papers reporting human cases of eyelid dirofilariasis. Any relevant article written in English, German, or Greek was included, without limitations regarding study type or patient characteristics. Papers written in other languages were also included if an English abstract provided sufficient information to identify the parasite as Dirofilaria and the location of the lesion as palpebral. Records with no full-text available (e.g., conference papers) were excluded if the information provided in the abstract was not adequate. The end date of the search period was April 1st, 2024. The results were checked meticulously in order to include only cases of purely palpebral location of the lesions and exclude those that imitated such a clinical appearance. Aside from this, we also detected all the eligible cases which were mentioned as references in the results from our prior search, as well, in other reviews relevant to dirofilariasis.
For each of the registered reports, we extracted information on: first author’s name, year of publication; number of total reported cases and those of eyelid disease; region and country of origin; relevant travel history; demographic characteristics of patients (sex, age); lesion localization; nematode species and sex; molecular confirmation of the diagnosis; presenting symptoms and signs; selected treatment; final outcome and/or recurrences.
2.3.2. Literature review - Results
The literature search revealed 117 published cases of eyelid dirofilariasis [10,11,14,15,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83,84,85,86,87,88,89,90,91,92,93,94,95,96,97,98,99]. A flow chart of the article selection process is presented in Supplemental Figure 1. Case characteristics are summarized in Table 1, while all cases are presented in full detail in Supplemental Table 1.

Table 1.
Summary of case characteristics.
| Total cases, N | 117 | |
|
Patient age Median Mean (±standard deviation) Range |
39 years 40.1 (±18) years 11 months - 77 years |
|
|
Patient sex, n (%) Female Male Not reported |
69 41 7 |
(59) (35) (6) |
|
Lesion localization, n (%)
Upper eyelid Lower eyelid Lateral canthus Medial canthus Not reported |
64 35 1 1 16 |
(54.7) (29.9) (0.85) (0.85) (13.7) |
|
Geographic region†, n (%) Eastern Europe Southern Europe Western Europe Central Asia Eastern Asia Western Asia South-eastern Asia Southern Asia Northern America Northern Africa Not reported |
34 19 11 2 2 5 4 31 6 2 1 |
(29.1) (16.2) (9.4) (1.7) (1.7) (4.3) (3.4) (26.5) (5.1) (1.7) (0.9) |
| Reported travel history to an endemic region, n (%) | 10 | (8.5) |
|
Nematode sex, n (%) Female Male Not reported |
31 7 79 |
(26.5) (6) (67.5) |
|
Nematode species, n (%) D. repens D. immitis D. tenuis D. hongkongensis Not reported |
103 2 4 1 7 |
(88) (1.7) (3.4) (0.9) (6) |
| Molecular confirmation of the diagnosis, n (%) | 20 | (17.1) |
†Subdivision according to the United Nations geoscheme. Available from: https://unstats.un.org/unsd/methodology/m49/.
The mean age of the patients was 40.1 years, ranging between 11 months and 77 years, with a slight gender predilection toward females (69/117 cases, 59%). More than half of the reported cases originated from Eastern Europe (29.1%) and Southern Asia (26.5%), with Southern Europe following in the third place (16.2%). In ten cases, a relevant travel history was reported. The upper eyelid was predominantly affected (54.7% of all cases), followed by the lower eyelid (29.9%) and median and lateral canthus (0.85% each), while the localization of the lesion was not specified in 13.7% of the cases. As far as the responsible nematode is concerned, D. repens was identified in the vast majority of cases with eyelid dirofilariasis (103/117, 88%), while four cases of D. tenuis, two cases of D. immitis, and one case of D. hongkongensis were also reported. A positive PCR confirmed the diagnosis in 20 patients (17.1%). When nematode sex was specified (38 cases), female parasites were found in a greater proportion (81.6%).
2.3.3. Clinical Appearance
In the vast majority of cases, a solid palpable mass or a subcutaneous nodule of the eyelid is noticed during clinical evaluation. Typically, eyelid dirofilariasis masses are single; multiple simultaneous locations imply multiple separate inoculations [76]. These lesions can be firm in consistency or swollen, with well-defined borders, movable or static, painful or painless, and progressively growing, whereas they are typically accompanied by local signs of inflammation (such as tenderness, redness, hyperemia), itchiness, or sometimes overlying brownish skin discoloration. These signs can yet be completely absent, and then the lesions masquerade clinically as non-inflammatory swelling [69]. In several cases, patients presented with a lesion of threadlike appearance [63,69,70,86,88], indicating with a quick inspection towards the probable subcutaneous presence of a worm, and some of them complained of a sensation of movement under their skin, owing to the motility of the living parasite [43,56,63,86,92].
Before the perception of eyelid symptomatology, patients can refer to having experienced flulike symptoms [65], recurrent episodes of edema [69,85,88], or diffuse migratory erythematous rash [66]. Extreme incidents have also been reported, regarding the emergence of a live motile nematode following the eruption of the eyelid lesion [76,88] or even the far migration of a nematode through the subcutis from the lower left eyelid to the neck, the axilla, the abdominal wall and finally the lower right eyelid [52]. A peculiarity of the case reported herein is the fact that our patient described two past episodes of recurrent periorbital edema extending to the cheek, before consulting our department eventually.
2.3.4. Laboratory Investigation
In human dirofilariasis in general, serological detection of specific antibodies or PCR of blood samples are not incorporated in the diagnostic process, as the microfilariae, which act as primordial triggers of the immune response, cannot typically develop in human hosts in cases of filarial infections [4]. For the same reason, the blood smear is negative for microfilaremia, whereas an increase of serum IgE levels might be rarely present [72]. Eosinophilia bibliographically, is more common in cases owed to D. immitis instead of D. repens, but regardless of that, it does not represent a consistent finding [100]. The most valuable examination remains until today the histopathological analysis of the biopsy material, which certifies the diagnosis of dirofilariasis and allows additionally the identification of the culpable species based on the morphometric microscopic characteristics of the eradicated nematode. In recent decades, the PCR method has been utilized by pathologists in order to facilitate diagnosis in samples where the helminths are destroyed beyond identification or in samples containing only a small part of the helminth [61,101]. The need for further taxonomic distinguishing of subtypes of the filariae can be met, except for PCR, by DNA and mitochondrial 12S ribosomal RNA (12S rRNA) gene sequencing [81]. Interestingly, in a case histopathologically consistent with D. repens, 12S rRNA analysis identified the parasite as D. hongkongensis, suggesting that several cases could be reclassified upon molecular confirmation of the diagnosis [94].
2.3.5. Imaging Findings
Regarding imaging findings, the literature in question is relatively limited. High-resolution ultrasonography (USG), CT, and MRI scans have been used as part of the diagnostic investigation. In USG, the lesions were hypoechoic (compatible with their cystic nature) [37,68,75,76,85] and, within them, motile, tube-like enfolded structures with parallel echogenic walls (possibly the live worms) were distinguished [68,75]. In other cases [15,66,68,70], a CT scan showed heterogeneous [68] or homogenous [66] well-defined masses or swelling [70] of soft tissue density, with enhanced periphery in one particular occasion [68]. Concerning the MRI findings, the lesions may manifest with cystic characteristics, in shape of an enclosed sac [91], with a center of high signal on T2w images, an encircling capsule of low signal on T1w and T2w images [102] and plausible intermediate signal intensities of tubular shape within the lesion in STIR images, indicating towards the worm [75]. Apart from this data, a rim enhancement of the capsule and parts of the lesion’s content may also be revealed on post-contrast fat saturation T1w images due to circumambient inflammation [75,102]. At this point, due to restricted data, knowledge can be drawn from our case report as well, where the MRI revealed a mass of heterogeneous signal intensity and enhancement, with ill-defined edges, displaying an alternative MRI pattern.
2.3.6. Management
Despite that surgical removal of the nematode or excision of the whole lesion is the treatment of choice, it should be performed always after considering the sensitivity of the affected eye’s region, the plausible risks or the final cosmetic outcome, choosing a conservative approach if the danger outweighs the profit of the patients [86]. In cases of eyelid localization, surgical excision is usually preferable because it is a definitive cure, and a diagnosis of malignancy cannot be easily ruled out [2]. Irrespective of each case’s particularities, efforts must be made to extract intact nematodes or intact nodules encompassing the nematodes, so that an inflammatory or anaphylactic response will not be triggered [1].
Pharmacological therapy with anthelmintic agents is not recommended in instances of human ocular dirofilariasis, as no efficacy has been proven [1,2]; besides microfilaraemia, a prerequisite that could justify such a therapeutic approach, is rarely developed in patients’ blood. Notwithstanding the foregoing, some clinicians report having treated their patients either with diethylcarbamazine or ivermectin, supplementary after the surgical removal of the nematode or, instead of that, as sole treatment due to cosmetic reasons [70,76,89], with a good post-surgical response, demonstrating reduced edema.
3. Conclusions
In a nutshell, ocular eyelid dirofilariasis should always be included in the differential diagnosis of a subcutaneous cyst, granuloma, or tumor-like nodule, accompanied or not by episodes of periorbital swelling, especially in countries where Dirofilaria cases have been reported. In the years to come, as the endemicity of such cases is about to change radically and embody immune geographical areas, a high index of suspicion and familiarity with the clinical and laboratory manifestations of ocular dirofilariasis is required hereafter in many fields of clinical medicine.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Author Contributions
Conceptualization, N.Z. A.D. and A.T.; methodology, A.D., A.K. S.A., G.L. and A.T.; software, G.L., A.K. and A.T.; validation, A.T. and G.L.; formal analysis, A.K., A.T., A.D., S.A. and D.M.; investigation, A.D., A.K., G.L., A.T. and D.M.; resources, N.Z.D.M. and S.A.; data curation, A.K., G.L. and A.D.; writing—original draft preparation, A.T., G.L., A.K. and A.D.; writing—review and editing, N.Z., S.A, D.M. and A.T.; visualization, D.M., A.K. and G.L.; supervision, N.Z., S.A. and A.T. All authors have read and agreed to the published version of the manuscript.
Institutional Review Board Statement
This study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board and Ethics Committee of the 2nd Ophthalmology Department, Aristotle University of Thessaloniki, Papageorgiou General Hospital.
Data Availability Statement
The raw data supporting this study’s findings are available from the corresponding author upon request.
Funding Statement: This research received no external funding.
Declaration of patient consent: The authors certify that they have received all necessary patient consent forms. The patient has provided their written consent through a suitable form for their clinical data and images to be included in the journal.
Conflicts of Interest
The authors declare no conflict of interest. No proprietary interest in any of the products mentioned in the study. No conflict of interest. No financial grants or funds were received in support of the study. The contents of this manuscript have not been copyrighted or published previously and will not be submitted elsewhere while the publication process is active. There are no directly related manuscripts or abstracts, published or unpublished, by any authors of this paper.
References
- Diaz, JH. Increasing risks of human dirofilariasis in travelers. J Travel Med. 2015;22(2):116–23.
- Simón F, Siles-Lucas M, Morchón R, González-Miguel J, Mellado I, Carretón E, et al. Human and animal dirofilariasis: the emergence of a zoonotic mosaic. Clin Microbiol Rev. 2012 Jul;25(3):507–44.
- Genchi C, Rinaldi L, Mortarino M, Genchi M, Cringoli G. Climate and Dirofilaria infection in Europe. Vet Parasitol. 2009 Aug 26;163(4):286–92.
- Capelli G, Genchi C, Baneth G, Bourdeau P, Brianti E, Cardoso L, et al. Recent advances on Dirofilaria repens in dogs and humans in Europe. Parasit Vectors. 2018 Dec 19;11(1):663.
- Aspock H. Dirofilaria and dirofilarioses; Introductory remarks. In: Proceedings of Helminthological Colloquium, Vienna. 2003. p. 5.
- Genchi C, Kramer LH, Rivasi F. Dirofilarial infections in Europe. Vector Borne Zoonotic Dis. 2011 Oct;11(10):1307–17.
- Pampiglione S, Canestri Trotti G, Rivasi F. Human dirofilariasis due to Dirofilaria (Nochtiella) repens: a review of world literature. Parassitologia. 1995 Dec;37(2–3):149–93.
- Sergiev VP, Supriaga VG, Morozov EN, Zhukova LA. [Human dirofilariasis: diagnosis and the pattern of pathogen-host relations]. Med Parazitol (Mosk). 2009;(3):3–6.
- McCall JW, Genchi C, Kramer LH, Guerrero J, Venco L. Heartworm disease in animals and humans. Adv Parasitol. 2008;66:193–285.
- Kagei N, Tanaka K, Okamura R, Korenaga M, Tada I. A report of the first case of Dirofilaria infection in the eyelid region in Japan. Jpn J Med Sci Biol. 1985;38(5–6):223–7.
- Pampiglione S, Rivasi F. Human dirofilariasis due to Dirofilaria (Nochtiella) repens: an update of world literature from 1995 to 2000. Parassitologia. 2000 Dec;42(3–4):231–54.
- Harizanov RN, Jordanova DP, Bikov IS. Some aspects of the epidemiology, clinical manifestations, and diagnosis of human dirofilariasis caused by Dirofilaria repens. Parasitol Res. 2014 Apr;113(4):1571–9.
- Sathyan P, Manikandan P, Bhaskar M, Padma S, Singh G, Appalaraju B. Subtenons infection by Dirofilaria repens. Indian J Med Microbiol. 2006 Jan;24(1):61–2.
- Kalogeropoulos CD, Stefaniotou MI, Gorgoli KE, Papadopoulou CV, Pappa CN, Paschidis CA. Ocular Dirofilariasis: A Case Series of 8 Patients. Middle East Afr J Ophthalmol. 2014;21(4):312–6.
- Bhat S, Saldanha M, Mendonca N. Periocular dirofilariasis: A case series. Orbit. 2016;35(2):100–2.
- Eligi C, Scasso CA, Eligi B, Busoni F. [Retrobulbar orbital dirofilariasis. A case report]. Radiol Med. 1995 Sep;90(3):334–5.
- Sethi A, Puri V, Dogra N. An unusual presentation of lacrimal gland dirofilariasis. Indian J Ophthalmol. 2017 Jul;65(7):615–7.
- Gupta P, Pradeep S, Biswas J, Rishi P, Muthusamy R. Extensive Chorio-retinal Damage Due to Dirofilaria Repens- Report of a Case. Ocul Immunol Inflamm. 2021 Aug 18;29(6):1142–4.
- Font RL, Neafie RC, Perry HD. Subcutaneous dirofilariasis of the eyelid and ocular adnexa. Report of six cases. Arch Ophthalmol. 1980 Jun;98(6):1079–82.
- Delage A, Lauraire MC, Eglin G. [Is human Dirofilaria (Nochtiella) repens parasitosis mor frequent than it appears on the Mediterranean coast?]. Bull Soc Pathol Exot. 1995;88(3):90–4.
- Spina F, Saraniti G, Randazzo S, Dal Bello A, Vallone G, Gorgone G. [2 cases of ocular filariasis]. Bull Mem Soc Fr Ophtalmol. 1986;97:57–61.
- Pampiglione S, Brollo A, Ciancia EM, De Benedittis A, Feyles E, Mastinu A, et al. [Human subcutaneous dirofilariasis: 8 more cases in Italy]. Pathologica. 1996 Apr;88(2):91–6.
- Cancrini G, Favia G, Giannetto S, Merulla R, Russo R, Ubaldino V, et al. Nine more cases of human infections by Dirofilaria repens diagnosed in Italy by morphology and recombinant DNA technology. Parassitologia. 1998 Dec;40(4):461–6.
- Kondrazkyi V, Parkhomienco L. Palpebral dirofilariasis. Vestn Ophthalmol. 1977;93(3):78–9.
- Avdiukhina TI, Supriaga VG, Postnova VF, Kuimova RT, Mironova NI, Murashov NE, et al. [Dirofilariasis in the countries of the CIS: an analysis of the cases over the years 1915-1996]. Med Parazitol (Mosk). 1997;(4):3–7.
- Koroev, AI. [Filaria under the skin of the eyelid]. Vestn Oftalmol. 1954;33(1):43.
- Merkusceva I, Cemerizkaia M, Iliuscenko A, Elin I, Malash S. Merkusceva IV, Cemerizkaia MV, Iliuscenko AA, Elin IS, Malash SL, 1981. Dirofilaria repens, nematode, in human eye. Sdravookhran Bjelorussyi 1: 67-68 (in Russian). Sdravookhran Bjelorussyi. 1981;1:67–8.
- Avdiukhina TI, Lysenko AI, Supriaga VG, Postnova VF. [Dirofilariasis of the vision organ: registry and analysis of 50 cases in the Russian Federation and in countries of the United Independent States]. Vestn Oftalmol. 1996;112(3):35–9.
- Postnova VF, Kovtunov A, Abrosimova L, Avdiukhina T, Mishina L, Posorelciuk TIa OV, et al. Dirofilariasis in man new cases. Medsk Parazitol. 1997;1:6–9.
- Dissanaike AS, Abeyewickreme W, Wijesundera MD, Weerasooriya MV, Ismail MM. Human dirofilariasis caused by Dirofilaria (Nochtiella) repens in Sri Lanka. Parassitologia. 1997 Dec;39(4):375–82.
- Pampiglione S, Rivasi F, Angeli G, Boldorini R, Incensati RM, Pastormerlo M, et al. Dirofilariasis due to Dirofilaria repens in Italy, an emergent zoonosis: report of 60 new cases. Histopathology. 2001 Apr;38(4):344–54.
- Raju K, Anju A, Vijayalakshmi M. Subcutaneous Dirofilaria Repens Infection of the Eyelid - A Report of Two Cases. Kerala Journal of Ophthalmology. 2008;XX(3):294–6.
- Szénási Z, Kovács AH, Pampiglione S, Fioravanti ML, Kucsera I, Tánczos B, et al. Human dirofilariosis in Hungary: an emerging zoonosis in central Europe. Wien Klin Wochenschr. 2008;120(3–4):96–102.
- Salomváry B, Korányi K, Kucsera I, Szénási Z, Czirják S. A new case of ocular dirofilariosis in Hungary. Szemészet. 2005;142:231–5.
- Parlagi G, Sumi Á, Elek G, Varga I. Orbital dirofilariosis.(Szemüregi dirofilariosis). Szemészet. 2000;137:105–7.
- Elek G, Minik K, Pajor L, Parlagi G, Varga I, Vetési F, et al. New human Dirofilarioses in Hungary. Pathol Oncol Res. 2000;6(2):141–5.
- Fodor E, Fok E, Maka E, Lukáts O, Tóth J. Recently recognized cases of ophthalmofilariasis in Hungary. Eur J Ophthalmol. 2009;19(4):675–8.
- Nath R, Gogoi R, Bordoloi N, Gogoi T. Ocular dirofilariasis. Indian J Pathol Microbiol. 2010;53(1):157–9.
- Iddawela D, Ehambaram K, Wickramasinghe S. Human ocular dirofilariasis due to Dirofilaria repens in Sri Lanka. Asian Pac J Trop Med. 2015 Dec;8(12):1022–6.
- Miterpáková M, Antolová D, Ondriska F, Gál V. Human Dirofilaria repens infections diagnosed in Slovakia in the last 10 years (2007-2017). Wien Klin Wochenschr. 2017 Sep;129(17–18):634–41.
- Hrčkova G, Kuchtová H, Miterpáková M, Ondriska F, Cibíček J, Kovacs S. Histological and molecular confirmation of the fourth human case caused by Dirofilaria repens in a new endemic region of Slovakia. J Helminthol. 2013 Mar;87(1):85–90.
- Velev V, Vutova K, Pelov T, Tsachev I. Human Dirofilariasis in Bulgaria Between 2009 and 2018. Helminthologia. 2019 Sep;56(3):247–51.
- Velev, V. Several Cases of Ocular Dirofilariasis in Bulgaria. Med Princ Pract. 2020 Dec;29(6):588–90.
- Riebenbauer K, Weber PB, Walochnik J, Karlhofer F, Winkler S, Dorfer S, et al. Human dirofilariosis in Austria: the past, the present, the future. Parasit Vectors. 2021 Apr 29;14(1):227.
- Lammerhuber C, Auer H, Bartl G, Dressler H. Subkutane Dirofilaria (Nochtiella) repens-Infektion im Oberlidbereich. Spektrum der Augenheilkunde. 1990;4(4):162–4.
- Faust EC, Agosín M, Garcia-laverde A, Sayad WY, Johnson VM, Murray NA. Unusual Findings of Filarial Infections in Man. American Journal of Tropical Medicine and Hygiene. 1952;1(2):239–49.
- Zhaboedov GD, Shupik AL. [Case of dirofilariasis of the eye in the Poltava district]. Oftalmol Zh. 1976;31(6):467–8.
- Blodi FC, Saparoff GR. [A dirofilaria granulom of the lid and the orbid (author’s transl)]. Klin Monbl Augenheilkd. 1977 Aug;171(2):222–4.
- Jariya P, Sucharit S. Dirofilaria repens from the eyelid of a woman in Thailand. Am J Trop Med Hyg. 1983 Nov;32(6):1456–7.
- Mak JW, Thanalingam V. Human infection with Dirofilaria (Nochtiella) sp.(Nematoda: Filarioidea), probably D. repens, in Malaysia. Tropical Biomedicine. 1984;1(2):109–13.
- Baumann, J. [Worm infection (Dirofilaria conjunctivae) in the ENT area]. Laryngol Rhinol Otol (Stuttg). 1987 Sep;66(9):480–3.
- Pampiglione S, Canestri-Trotti G, Piro S, Maxia C. [Palpebral dirofilariasis in man: a case in Sardinia]. Pathologica. 1989;81(1071):57–62.
- Pampiglione S, Manilla G, Canestri-Trotti G. [Human dirofilariasis in Italy: a new palpebral case with spontaneous healing in Abruzzo]. Parassitologia. 1990 Dec;32(3):381–4.
- Georgouli M, Loukaki M, Lentari A, Hinou F, Karaiskos H, Golemati P. An unusual case of human dirofilariasis located in the subcutaneous tissue of the lower eyelid. Acta Microbiologica Hellenica. 1991;36:213–20.
- Soylu M, Ozcan K, Yalaz M, Varinli S, Slem G. Dirofilariasis: an uncommon parasitosis of the eye. Br J Ophthalmol. 1993 Sep;77(9):602–3.
- Fuentes I, Cascales A, Ros JM, Sansano C, Gonzalez-Arribas JL, Alvar J. Human subcutaneous dirofilariasis caused by Dirofilaria repens in Ibiza, Spain. Am J Trop Med Hyg. 1994 Oct;51(4):401–4.
- van den Ende J, Kumar V, van Gompel A, van Den Enden E, Puttemans A, Geerts M, et al. Subcutaneous dirofilariasis caused by Dirofilaria (nochtiella) repens in a Belgian patient. International journal of dermatology. 1995;34(4):274–7.
- Awadalla HN, Bayoumi DM, Ibrahim IR. The first case report of suspected human dirofilariasis in the eyelid of a patient from Alexandria. J Egypt Soc Parasitol. 1998 Dec;28(3):941–3.
- Sekhar HS, Srinivasa H, Batru RR, Mathai E, Shariff S, Macaden RS. Human ocular dirofilariasis in Kerala Southern India. Indian J Pathol Microbiol. 2000 Jan;43(1):77–9.
- Striukova IL, Goncharova OV, Gul’iants VA. [Dirofilariasis in the practice of an ophthalmologist]. Vestn Oftalmol. 2001;117(3):43–4.
- Vakalis N, Vougioukas N, Patsoula E, Spanakos G, Sioutopoulou DO, Vamvakopoulos NC. Genotypic assignment of infection by Dirofilaria repens. Parasitol Int. 2002 Jun;51(2):163–9.
- Dzamić AM, Arsić-Arsenijević V, Radonjić I, Mitrović S, Marty P, Kranjcić-Zec IF. Subcutaneous Dirofilaria repens infection of the eyelid in Serbia and Montenegro. Parasite. 2004 Jun;11(2):239–40.
- Ittyerah TP, Mallik D. A case of subcutaneous dirofilariasis of the eyelid in the South Indian state of Kerala. Indian Journal of Ophthalmology. 2004 Sep;52(3):235.
- Aiello A, Aiello P, Aiello F. A case of palpebral dirofilariasis. Eur J Ophthalmol. 2005;15(3):407–8.
- Siepmann K, Wannke B, Neumann D, Rohrbach JM. Subcutaneous tumor of the lower eyelid: a potential manifestation of a Dirofilaria repens infection. Eur J Ophthalmol. 2005;15(1):129–31.
- Beden U, Hokelek M, Acici M, Umur S, Gungor I, Sullu Y. A case of orbital dirofilariasis in Northern Turkey. Ophthalmic Plast Reconstr Surg. 2007;23(4):329–31.
- Abdel-Rahman SM, Mahmoud AE, Galal L a. A, Gustinelli A, Pampiglione S. Three new cases of human infection with Dirofilaria repens, one pulmonary and two subcutaneous, in the Egyptian governorate of Assiut. Ann Trop Med Parasitol. 2008 Sep;102(6):499–507.
- Smitha M, Rajendran V, Devarajan E, Anitha P. Case report: Orbital dirofilariasis. Indian J Radiol Imaging. 2008 Feb;18(1):60–2.
- Mannino G, Contestabile MT, Medori EM, Mannino C, Enrici MM, Marangi M, et al. Dirofilaria Repens in the Eyelid: Case Report of Subcutaneous Manifestation. European Journal of Ophthalmology. 2009 May;19(3):475–7.
- Shenoi SD, Kumar P, Johnston SP, Khadilkar UN. Cutaneous dirofilariasis presenting as an eyelid swelling. Trop Doct. 2009 Jul;39(3):189–90.
- Dang TCT, Nguyen TH, Do TD, Uga S, Morishima Y, Sugiyama H, et al. A human case of subcutaneous dirofilariasis caused by Dirofilaria repens in Vietnam: histologic and molecular confirmation. Parasitol Res. 2010 Sep;107(4):1003–7.
- Khurana S, Singh G, Bhatti HS, Malla N. Human subcutaneous dirofilariasis in India: a report of three cases with brief review of literature. Indian J Med Microbiol. 2010;28(4):394–6.
- Kotigadde S, Ramesh SA, Medappa KT. Human dirofilariasis due to Dirofilaria repens in southern India. Trop Parasitol. 2012 Jan;2(1):67–8.
- Sahdev SI, Sureka SP, Sathe PA, Agashe R. Ocular dirofilariasis: still in the dark in western India? J Postgrad Med. 2012;58(3):227–8.
- Gopinath TN, Lakshmi KP, Shaji PC, Rajalakshmi PC. Periorbital dirofilariasis—Clinical and imaging findings: Live worm on ultrasound. Indian J Ophthalmol. 2013 Jun;61(6):298–300.
- Senanayake MP, Infaq MLM, Adikaram SGS, Udagama PV. Ocular and subcutaneous dirofilariasis in a Sri Lankan infant: an environmental hazard caused by dogs and mosquitoes. Paediatr Int Child Health. 2013 Dec;33(2):111–2.
- Shankar MK, Shet S, Gupta P, Nadgir SD. Sac over the sac - a rare case of subcutaneous dirofilariasis over the lacrimal sac area. Nepal J Ophthalmol. 2014;6(2):224–6.
- Werner JU, Wacker T, Lang GK. [Subcutaneous dirofilariasis of the eyelid]. Klin Monbl Augenheilkd. 2014 Sep;231(9):924–5.
- Choi SH, Kim N, Paik JH, Cho J, Chai JY. Orbital dirofilariasis. Korean J Ophthalmol. 2014 Dec;28(6):495–6.
- Dóczi I, Bereczki L, Gyetvai T, Fejes I, Skribek Á, Szabó Á, et al. Description of five dirofilariasis cases in South Hungary and review epidemiology of this disease for the country. Wien Klin Wochenschr. 2015 Sep;127(17–18):696–702.
- Kutlutürk I, Tamer GZS, Karabaş L, Erbesler AN, Yazar S. A rapidly emerging ocular zoonosis; Dirofilaria repens. Eye (Lond). 2016 Apr;30(4):639–41.
- Smets M, De Potter P. First cases of ocular dirofilariasis caused by drofilaria repens in Belgium. Acta Ophthalmologica [Internet]. 2016 [cited 2024 Apr 29];94(S256). Available from: https://onlinelibrary.wiley.com/doi/abs/10.1111/j.1755-3768.2016.0572.
- Jessani LG, Patil S, Annapurneshwari D, Durairajan S, Gopalakrishnan R. Human ocular dirofilariasis due to Dirofilaria repens: an underdiagnosed entity or emerging filarial disease? International Journal of Infectious Diseases. 2016;45:177.
- Nagpal S, Kulkarni V. Periorbital Dirofilariasis: A Rare Case from Western India. J Clin Diagn Res. 2016 Mar;10(3):OD12-14.
- Gushсhina MB, Egorova EV, Yuzhakova NS, Mal’kov SA. [Orbital case of ocular dirofilariasis]. Vestn Oftalmol. 2017;133(2):82–5.
- Rodríguez-Calzadilla M, Ruíz-Benítez MW, de-Francisco-Ramírez JL, Redondo-Campos AR, Fernández-Repeto-Nuche E, Gárate T, et al. Human dirofilariasis in the eyelid caused by Dirofilaria repens: An imported case. Arch Soc Esp Oftalmol. 2017 Sep;92(9):439–41.
- Blaizot R, Receveur MC, Millet P, Otranto D, Malvy DJM. Systemic Infection With Dirofilaria repens in Southwestern France. Ann Intern Med. 2018 Feb 6;168(3):228–9.
- Lindner AK, Tappe D, Gertler M, Equihua Martinez G, Richter J. A live worm emerging from the eyelid. J Travel Med. 2018 Jan 1;25(1).
- Mani A, Khan MA, Kumar VP. Subcutaneous dirofilariasis of the eyelid. Med J Armed Forces India. 2019 Jan;75(1):112–4.
- Pupić-Bakrač A, Pupić-Bakrač J, Jurković D, Capar M, Lazarić Stefanović L, Antunović Ćelović I, et al. The trends of human dirofilariasis in Croatia: Yesterday - Today - Tomorrow. One Health. 2020 Dec;10:100153.
- Mihaljevic B, Ivekovic R, Zrinscak O, Vatavuk Z. [Subcutaneous Tumor of the Upper Eyelid: Infestation by Dirofilaria repens]. Klin Monbl Augenheilkd. 2020 Jan;237(1):32–4.
- Gebauer J, Ondruš J, Kulich P, Novotný L, Sałamatin R, Husa P, et al. The first case of periorbital human dirofilariasis in the Czech Republic. Parasitol Res. 2021 Feb;120(2):739–42.
- Agrawal S, Modaboyina S, Raj N, Das D, Bajaj MS. Eyelid Dirofilaria During COVID-19 Pandemic: A Telemedicine Diagnosis. Cureus. 2021 Jun;13(6):e15525.
- Tirakunwichcha S, Sansopha L, Putaporntip C, Jongwutiwes S. Case Report: An Eyelid Nodule Caused by Candidatus Dirofilaria hongkongensis Diagnosed by Mitochondrial 12S rRNA Sequence. Am J Trop Med Hyg. 2022 Jan 5;106(1):199–203.
- Szostakowska B, Ćwikłowska A, Marek-Józefowicz L, Czaplewski A, Grzanka D, Kulawiak-Wasielak N, et al. Concurrent subcutaneous and ocular infections with Dirofilaria repens in a Polish patient: a case report in the light of epidemiological data. Parasitol Int. 2022 Feb;86:102481.
- Rymgayłło-Jankowska B, Ziaja-Sołtys M, Flis B, Bogucka-Kocka A, Żarnowski T. Subcutaneous Dirofilariosis of the Eyelid Brought to Poland from the Endemic Territory of Ukraine. Pathogens. 2023 Jan 28;12(2):196.
- Shaikh Z, Kar P, Mohanty S, Dey M, Samal DK. Ocular dirofilariasis: A report from Odisha. Indian J Med Microbiol. 2023;45:100388.
- Camacho M, Antonietti M, Sayegh Y, Colson JD, Kunkler AL, Clauss KD, et al. Ocular Dirofilariasis: A Clinicopathologic Case Series and Literature Review. Ocular Oncology and Pathology. 2023 Dec 9;10(1):43–52.
- Gitanjali MM, Konapur PG, Kolakkadan H, Azeez KN. Human dirofilariasis - Unforeseen lesion in subcutaneous nodules: Case series from a tertiary care hospital, Wayanad. Indian J Pathol Microbiol. 2024;67(1):204–6.
- Zvornicanin J, Zvornicanin E, Numanovic F, Delibegovic Z, Husic D, Gegic M. Ocular Dirofilariasis in Bosnia and Herzegovina: A Case Report and Review of the Literature. J Curr Ophthalmol. 2020 Jul 4;32(3):293–6.
- Trenkić BM, Otašević S, Stanković BG, Tasić A, Trenkić M. Human ocular dirofilariosis: Clinical and epidemiological features. Acta medica medianae. 2014;53(1):80–4.
- Groell R, Ranner G, Uggowitzer MM, Braun H. Orbital dirofilariasis: MR findings. AJNR Am J Neuroradiol. 1999 Feb;20(2):285–6.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



