
Submitted:
11 June 2025
Posted:
12 June 2025
You are already at the latest version
Abstract
As global populations age, the demand for effective and compassionate geriatric care has intensified. Humanized nursing, which emphasizes empathy and person-centered care, alongside community-based nursing, which leverages local resources and networks, presents promising strategies to enhance the health and well-being of older adults. This integrative review explores the evolution, clinical contributions, and implementation barriers of these models. A comprehensive literature search was performed using PubMed, CINAHL, Scopus, and Web of Science, targeting peer-reviewed studies published between 2010 and 2025 that involved adults aged 60 years and older. Inclusion criteria emphasized humanized and community-based nursing interventions, while excluding non-nursing and pediatric-focused studies. Quality appraisal was performed using CASP and JBI checklists, and data were thematically synthesized. Evidence indicates that these care models significantly improve functional independence, psychosocial well-being, and reduce hospital readmissions. For instance, community-based care in Taiwan improved activities of daily living in dementia patients by 15%, while U.S.-based programs reduced depressive symptoms by 30% among Latino older adults. Interdisciplinary, nurse-led interventions in South Korea and Puerto Rico showed a 22% reduction in readmissions and an 85% increase in care access. Despite these benefits, numerous barriers hinder widespread implementation, including workforce shortages, inadequate funding, fragmented healthcare systems, cultural resistance, digital literacy challenges, and policy constraints, particularly in low-resource settings such as the Philippines and Nepal. These findings underscore the transformative potential of humanized and community-based nursing, while highlighting the need for targeted strategies such as task-shifting, inclusive technologies, and policy reform to advance equitable, sustainable geriatric care globally.
Keywords:
Humanized nursing
; community-based nursing
; geriatric care
; aging in place
; implementation barriers
1. Introduction
Humanized nursing care is an approach centered on a holistic view of the patient, emphasizing empathy, dignity, and person-centeredness. It prioritizes the human needs of individuals by fostering therapeutic relationships, respecting personal values, and building trust to promote overall well-being [1]. In contrast, community-based nursing care delivers healthcare services within community settings, leveraging local resources, social networks, and interdisciplinary collaboration to support older adults in maintaining their independence while living in their homes or local environments [2]. These models are particularly vital for geriatric populations, who often face complex health challenges such as chronic diseases, cognitive decline, and social isolation. Integrating humanized principles with community-based frameworks enables a more comprehensive response to both clinical and psychosocial needs. This combined approach can enhance functional independence, support emotional well-being, and improve overall quality of life among older adults.
The global population is aging very fast, and this has important consequences for healthcare. The percentage of the world’s population over 60 will more than double before 2050 to reach 2.1 billion, with 80% of the group living in low- and middle-income nations, based on the World Health Organization’s projections. This population shift is seen in places, for instance, China’s aging adult population is expected to rise above 400 million by 2050 [3]. In nations such as the Philippines and Nepal, a declining population is complicating already scarce healthcare, worsening the disparity in elderly care [4,5]. Such trends call for the immediate development of innovative care models that are available, culturally sensitive, and sustainable. Humanized and community-based nursing care models are well placed to answer such needs by promoting socio-culturally sensitive interventions and limiting the dependence on institutional care [6].
The value of humanized and community-based models of geriatric care lies in their ability to address complex, multifaceted challenges associated with aging. Humanized care enhances patient satisfaction and emotional well-being, which is especially critical for older adults experiencing loneliness or cognitive impairments such as dementia [7]. In parallel, community-based care supports aging in place while reducing hospital readmissions and overall healthcare costs. For instance, a community-based health-social partnership model in Hong Kong demonstrated improved health outcomes for older adults through integrated service delivery [2]. Moreover, community service learning involving older adults has shown both educational and clinical benefits by fostering empathy among nursing students and enhancing patient-centered care [8]. Despite these advantages, the implementation of such models faces persistent barriers, including resource limitations, interprofessional collaboration challenges, and cultural resistance to non-traditional care settings [4,9].
Community-based care has proven effective in the disaster management of older adults in countries such as Thailand, where local networks are mobilized to provide specialized support [10]. However, systemic challenges persist, including inadequate funding, workforce shortages, and limited availability of home-based services, particularly for individuals with dementia and their caregivers [9]. These obstacles underscore the need for a deeper understanding of how to effectively scale humanized and community-based care models across diverse settings.
Therefore, this review aims to explore the dynamics, clinical contributions, and implementation barriers associated with humanized and community-based nursing care for older adults. By synthesizing evidence from a variety of global contexts, it explores how these models enhance geriatric care, impact health outcomes, and where adoption continues to lag. The insights generated from this analysis are intended to inform policymakers, healthcare providers, and researchers, offering a strategic foundation to strengthen care systems for aging populations to promote geriatric nursing with dignity, equity, and sustainability.
2. Materials and Methods
This work utilizes the integrative literature review design to synthesize evidence on humanized and community-based nursing care for aged patients comprehensively. Integrative reviews are an appropriate model for synthesizing different methodologies, both qualitative and quantitative studies, as well as mixed approaches, to develop a comprehensive picture of complex phenomena [11]. This approach enables the examination of the evolution, clinical contributions, and implementation barriers of these care models in geriatric populations, while the diverse designs and settings are taken into account [12].
2.1. Data Sources
A systematic literature review search was conducted across four major academic databases, PubMed, CINAHL, Scopus, and Web of Science, following the PRISMA guidelines, selected for their comprehensive coverage of nursing, geriatric, and health sciences literature [13]. PubMed provides extensive access to biomedical and nursing research, CINAHL specializes in nursing and allied health, Scopus offers broad interdisciplinary content, and Web of Science ensures high-impact scholarly sources. To enhance the search, reference lists of included studies were manually screened using a snowballing technique to identify additional relevant literature [14].
2.2. Study Selection, Inclusion, and Exclusion Criteria
All studies reporting the geriatric care and its contribution were considered. The inclusion criteria included: (1) Peer-reviewed articles published within the last 15 years (2010–2025) to capture contemporary trends in geriatric care, (2) Studies focusing on adults aged 60 years and older, aligning with standard definitions of older adulthood (World Health Organization, 2020), (3) Studies explicitly addressing humanized nursing care (e.g., person-centered, empathetic approaches) or community-based nursing care (e.g., home-based, community-integrated services), and (4) Studies published in English to ensure accessibility for analysis [15]. Exclusion criteria included: (1) Studies focusing on non-nursing interventions, such as those led solely by physicians or social workers, (2) Studies involving pediatric or younger adult populations, (3) Non-empirical works, such as opinion pieces, editorials, or commentaries, and (4) Studies lacking a clear focus on geriatric populations or nursing care models [16]. These criteria ensured a targeted review of nursing-specific interventions for older adults.
2.3. Search Strategy
The search strategy employed Boolean operators (AND, OR, NOT) and Medical Subject Headings (MeSH) to optimize precision and recall. Primary search terms included “humanized nursing care,” “person-centered care,” “community-based nursing,” “geriatric nursing,” “older adults,” “elderly care,” and “community-dwelling elderly.” To broaden the scope, related terms such as “empathic care,” “holistic nursing,” “home-based care,” and “aging in place” were also incorporated [17]. Truncation and wildcard symbols (e.g., nurs) were used to capture variations in terminology. A representative search string was: (“humanized nursing care” OR “person-centered care” OR “community-based nursing”) AND (“older adults” OR “elderly” OR “geriatric”) AND (“care model” OR “intervention”). Filters were applied to include only peer-reviewed articles published in English within the specified time frame.
The PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) framework was employed to ensure transparency and reproducibility in the search and selection process [18]. The PRISMA flowchart details each stage of the review, including the number of records identified, screened, assessed for eligibility, and ultimately included, along with reasons for exclusion at each step (Figure 1). Duplicate records were removed using reference management software (e.g., EndNote), and titles and abstracts were independently screened by two reviewers [19]. Full-text articles were then assessed against predefined inclusion criteria, with any discrepancies resolved through discussion and consensus, or adjudicated by a third reviewer.
2.4. Quality Appraisal
The Critical Appraisal Skills Programme (CASP) checklists were used to evaluate qualitative, qualitatively oriented, and mixed-methods studies, while the Joanna Briggs Institute (JBI) checklist was applied to quantitative studies [20,21]. These tools were chosen for their applicability across diverse study designs and their focus on key indicators of research quality, including clarity of objectives, methodological appropriateness, and robustness of findings [22]. The CASP tool assessed qualitative studies based on ethical considerations, data collection strategies, and researcher reflexivity—factors critical in studies addressing humanized care experiences [14]. For quantitative studies, the JBI checklist examined elements such as sampling strategies, statistical analyses, and measurement reliability, particularly relevant in evaluating outcomes from community-based interventions [23].
Each study was independently appraised by separate reviewers, and scores were assigned according to checklist-specific criteria. Studies were categorized as high, moderate, or low quality. However, no study was excluded based on quality alone, in line with the integrative nature of the review [11]. Instead, quality ratings informed the weighting of findings during synthesis, with greater emphasis placed on results derived from higher-quality studies [24]. A narrative summary of the appraisal outcomes was provided to highlight methodological strengths and limitations across the literature.
2.5. Data Extraction and Synthesis
Data were extracted using a standardized template capturing study characteristics (author, year, country), design, population, interventions, outcomes, and implementation barriers [25]. For humanized nursing care, emphasis was placed on person-centered approaches, patient satisfaction, and emotional well-being, while community-based nursing data focused on service delivery models, health outcomes, and community integration [26]. Barriers and facilitators, including resource limitations and interprofessional collaboration challenges, were also extracted [27]. An integrative synthesis combining narrative and thematic analyses organized findings into three domains: (1) evolution of care models, (2) clinical and psychosocial contributions, and (3) implementation barriers and facilitators [12]. Thematic synthesis identified recurring patterns, such as empathy in humanized care and the role of community networks [19]. Quantitative data were summarized descriptively, with effect sizes reported when available [28]. Constant comparison across study types facilitated a comprehensive understanding of the topic. This systematic approach, leveraging diverse data sources, robust appraisal tools, and structured synthesis, enables meaningful insights into the practice and policy implications of humanized and community-based nursing care for older adults.
3. Evolution of Humanized and Community-Based Nursing in Geriatric Care
Humanized and community-based nursing practice among older adults has evolved with implications of a shift from institutional biomedical practice to holistic patient-centered and community-integrated models. These care paradigms have arisen in response to global trends in aging, changes to healthcare needs, and policy paradigms of dignity and aging in place. Informed by historical nursing practice and theoretical improvement, their evolution along with the lines of public health and social care integration and global health directions for the aged populace makes practical sense [14]. Figure 2 illustrates the progressive layers of nursing practice, beginning with foundational Primary Care Nursing at the base and culminating in Community-Based Nursing at the apex. The model emphasizes the evolving scope of care from individualized treatment to broader community health engagement.
3.1. Historical Background and Theoretical Foundations
Historically, care for older adults has been predominantly acute and hospital-centered, with limited focus on emotional and social needs. Early nursing traditions, shaped by figures such as Florence Nightingale, emphasized patient well-being and environmental factors, laying the groundwork for empathetic treatment [14]. The 20th century marked a shift toward humanistic nursing, driven by the growing complexity of older populations’ needs. Theoretical frameworks emerged to uphold patient dignity, especially for older adults with chronic illnesses or social isolation. Humanized nursing, centered on empathy and respect for individuality, became pivotal in geriatric care, fostering therapeutic relationships that promote well-being [19]. Concurrently, community-based nursing evolved from the early 20th-century public health movement, emphasizing care delivery beyond institutional settings. This approach gained momentum as healthcare systems recognized that hospital-centric models were insufficient for the expanding aging population desiring to remain in their communities [17]. These historical developments have converged, integrating humanized and community-based approaches to align care with the preferences and needs of older adults.
3.2. Development of Humanistic Models in Nursing
Humanized nursing models evolved to emphasize person-centered care, which prioritizes the individual’s values, preferences, and emotional needs. These models are particularly relevant for older adults, who often face psychosocial challenges like loneliness or cognitive decline. In Asia, for instance, person-centered approaches have been integrated into community care programs to enhance the psychological well-being of older adults, addressing both health and social needs [25]. These interventions promote trust and respect, thereby enhancing patient satisfaction and overall quality of life [19]. The development of humanistic models also influenced nursing practice, encouraging nurses to adopt empathetic and culturally sensitive approaches. In Taiwan, home-based care programs for older adults with dementia have integrated person-centered care principles, leading to reduced caregiver burden and improved patient autonomy [28]. These advancements reflect a broader shift toward holistic care, where emotional and social dimensions are as critical as clinical outcomes in geriatric nursing [13].
3.3. Rise of Community-Based Models
Community-based nursing emerged to support aging in place, emphasizing older adults’ ability to remain at home or within their communities. By the late 20th century, the expansion of home-based care and community clinics addressed the growing demand for accessible and affordable services. In Taiwan, community-based long-term care systems were developed specifically for older adults with dementia, integrating nursing, social work, and rehabilitation services [28]. Similarly, India’s National Program for Health Care of the Elderly established community health centers that deliver both medical and social geriatric care [26]. Community clinics have played a vital role in providing preventive and chronic care, particularly in resource-limited settings. In South Korea, community-based integrated care models targeting older adults living alone combined health and social services, resulting in reduced hospital admissions and improved health outcomes [23]. These models emphasize interdisciplinary collaboration, engaging nurses, community health workers, and social workers to address the complex and multidimensional needs of the aging population [22].
3.4. Integration with Public Health and Social Care Frameworks
The integration of humanized and community-based nursing with public health and social care frameworks represents a significant advancement in geriatric care. Public health initiatives increasingly address social determinants of health—such as social isolation and poverty—that disproportionately impact older adults. In China, community-based senior care programs combined healthcare and social services to meet both psychological and practical needs, resulting in enhanced care satisfaction [25]. These programs effectively utilized community resources, aligning with public health objectives of accessibility and equity [13]. Social care integration often involved task-shifting, where community health workers supported nurses in delivering care. In low- and middle-income countries, such frameworks expanded mental health services for older adults, demonstrating the scalability of community-based models [22]. India’s community-based programs under the National Program for Health Care of the Elderly (NPHCE) incorporated social care elements to address geriatric needs, although challenges like funding shortages remained ([26].
3.5. Emergence of Community-Based Care Models
Community-based care models, including the primary healthcare approach, have become central to geriatric nursing by prioritizing universal access and community participation. These models foster integrated health and social care interventions tailored to older adults [23]. Scoping reviews in Asia emphasize the importance of linking healthcare with social care to support sustainable aging, noting that community-based models effectively reduce institutionalization rates [13]. Chronic care models focusing on coordinated management of prevalent conditions such as dementia and hypertension have also emerged, with community-based interventions improving health outcomes [28].
These models stress preventive care and health promotion, aligning with the evolving needs of aging populations. In Slovenia, community-based care initiatives have supported aging in place by enabling older adults to maintain independence through tailored nursing and social services [17]. Such efforts underscore the critical role of community networks in delivering effective geriatric care.
3.6. Alignment with WHO Frameworks and Global Health Strategies
The development of humanized and community-based nursing is consistent with global strategies for aging populations of the World Health Organization (WHO). WHO’s Decade of Healthy Ageing (2021– 2030) advocates for an integration of person-centered and community-based care to drive healthy aging with a focus on age-friendly environments and accessible services [13]. These principles are embodied in the humanized nursing concern for dignity, and community-based care concern for local resources [27]. WHO’s Integrated Care for Older People (ICOPE) guidelines advance community-based, multi-faceted care to preserve functional ability in the aged. In central and eastern Europe, there were barriers to implementing ICOPE principles in the form of resource limitations, indicating the need for sustainable financing models [27]. Community-based interventions in Taiwan have adapted to ICOPE because they combined nursing and social care to improve the situation of older adults suffering from chronic diseases [28].
4. Clinical Contributions and Impacts of Geriatric Nursing
Humanized and community-based nursing care has made significant improvements in geriatric nursing by improving outcomes from clinical practice, improving relationships between nurses and patients, as well as implementing excellent models for care. Functional independence, psychosocial wellbeing, and decreased hospital readmissions are the focal points of these approaches, which have an interdisciplinary team and nurse-led intervention. Data from varied regions highlights their effect, including benefits that are quantifiable to older adults. These contributions are examined in this section, with the help of recent studies and, for clarity, in tabular form.
4.1. Improved Outcomes
Community-based and humanized nursing care significantly support the functional independence, psychosocial well-being, and reduced hospital readmissions among older adults, particularly those choosing to age in place. Personalized interventions, such as home visitations and case management, enhance physical function and autonomy, as demonstrated by a Taiwanese long-term care system for dementia patients that improved activities of daily living (ADL) by 15% within 12 months [28], and a Slovenian model that increased functional independence by 20% [17], These models also address psychosocial dimensions by fostering empathetic, person-centered care that mitigates loneliness and emotional distress. For example, community-based programs in China integrating psychological support improved mental health scores by 25% based on the Geriatric Depression Scale [25], while a U.S. initiative using community health workers to deliver depression care to Latino seniors reduced depressive symptoms by 30% within six months [29]. Moreover, by providing proactive and continuous care, such community-oriented strategies reduce hospital readmissions, thereby alleviating healthcare system burdens. A systematic review found that transitional care interventions reduced readmission rates by 18% in chronically ill older adults [30], and a South Korean integrated health-social care model achieved a 22% reduction in readmissions for older adults living alone over one year [23]. Collectively, these outcomes underscore the critical role of community-based nursing in sustaining older adults’ independence, mental health, and overall well-being. Table 1 highlights some potential improved outcomes in geriatric nursing in the last five years. Along with this, humanized nursing strengthens nurse-patient interactions through trust-building, emotional support, and effective communication. These elements are critical for older adults, who often require empathetic care to navigate complex health challenges. In Australia, qualitative data revealed that person-centered nursing increased patient trust by 40%, as reported by informal carers, due to nurses’ focus on emotional support [19]. Community-based nursing further enhances interactions by fostering continuity of care. In India, nurse-led community health programs improved patient satisfaction by 35%, attributed to consistent communication and culturally sensitive care [26]. Table 2 demonstrates enhanced nurse-patient interaction metrics in the last five years.
4.2. Models of Care
Community-based nursing care utilizes integrated models such as home visits, case management, and transitional care to deliver comprehensive and person-centered support to older adults, particularly in aging-in-place contexts. Home visits enable nurses to assess health conditions in familiar environments, reducing the need for institutionalization, as evidenced by a U.S. Veterans Affairs program that cut nursing home admissions by 25% through home-based care [24]. Case management ensures coordinated services and seamless care transitions, as shown in Taiwan where nurse-led case management for dementia patients improved activities of daily living (ADL) by 15% and reduced emergency visits by 15% [28]. Transitional care further bridges the gap between hospital and home, with global evidence indicating a 20% reduction in readmissions [30]. These approaches are often embedded within interdisciplinary teams, combining the expertise of nurses, social workers, and community health workers. For instance, following Hurricane María, community-based organizations in Puerto Rico improved healthcare access for 85% of older adults through team-based emergency care delivery [31]. Similarly, nurse-led programs in China, such as first-aid education, enhanced self-efficacy among 90% of older participants [32], while chronic disease management and preventive care improved in countries like Ireland and China through nurse-based initiatives. Moreover, technology-enhanced monitoring in Singapore and South Korea boosted compliance and care continuity. In South Korea, an integrated model for older adults living alone, coordinated by nurses through home visits, reduced hospital readmissions by 22% and enhanced psychosocial well-being by 20% [23]. These results underscore that when public health systems adopt community-focused, interdisciplinary, and technologically supported strategies, they significantly improve clinical outcomes, continuity of care, and respect for patient preferences, particularly in geriatric and palliative contexts. Table 3 highlights the care model impacts in the last five years. However, despite these contributions, challenges persist. Resource constraints in Central and Eastern Europe limited the scalability of integrated care models, with only 60% of planned programs fully implemented [27]. Digital barriers, such as low internet literacy among older adults, hindered telehealth adoption in China, affecting 30% of potential users [33]. Addressing these barriers is critical to maximizing impact. Humanized and community-based nursing have transformed geriatric care by improving functional independence, psychosocial well-being, and reducing readmissions. Enhanced nurse-patient interactions and robust care models, supported by interdisciplinary teams, drive these outcomes. Case examples from Taiwan, South Korea, and Puerto Rico illustrate their global applicability, though ongoing efforts to overcome resource and technological barriers are essential for sustained impact.
5. Barriers to Implementation of Humanized and Community-Based Nursing in Geriatric Care
The implementation of humanized and community-based nursing in geriatric care faces multifaceted barriers spanning structural, organizational, cultural, technological, and policy domains (Figure 3). Structurally, labor shortages, limited financing, and fragmented health systems significantly hinder scalability. For example, in the Philippines, only 30% of the required health and social workforce was available for geriatric care, limiting community-based services [4] (Moncatar et al., 2021), while in Nepal, financial constraints meant that only 20% of planned elderly care services were operational [5](Shrestha et al., 2021). Similarly, fragmented systems in Central and Eastern Europe resulted in only 60% of integrated care programs achieving full implementation [25] ([27]). These issues are compounded by organizational barriers such as the lack of standardized protocols, weak integration with primary care, and insufficient training. A meta-synthesis found that 70% of healthcare providers lacked clear guidelines for person-centered care [1] (Liao et al., 2023), and in Taiwan, inadequate coordination between community nurses and primary care led to disrupted continuity for 25% of dementia patients [28] (Wang et al., 2021). Furthermore, 40% of nurses in Hong Kong reported feeling unprepared to deliver community-based care due to training gaps [2] (Wong et al., 2022). Cultural and ethical challenges further obstruct implementation, with institutional resistance to non-traditional models noted in 50% of U.S. facilities caring for dementia patients [9] (Waymouth et al., 2023), and a study on virtual HIV care revealed that 35% of programs failed to meet socio-cultural needs [6] (Kokorelias et al., 2023). Ethical dilemmas, especially in end-of-life care, were reported in 30% of cases in Australia due to conflicts between person-centered values and institutional policies [19] Allen et al., 2022). Technological limitations, particularly digital illiteracy and lack of interoperability, further exacerbate disparities. In China, 60% of older adults struggled with digital platforms, restricting telehealth access [3](Sun et al., 2025), while 45% of U.S. community programs reported delays due to non-interoperable health records [16]. These challenges are further intensified by policy-level constraints; in India, the lack of policy support led to delays in 50% of community-based geriatric initiatives ([26]) [24], and in Nepal, only 15% of health programs addressed elderly needs due to the absence of a geriatric-focused framework [5]. Even in emergencies, cultural resistance remains evident—for example, in Thailand, where 30% of institutional providers opposed community-based disaster care for older adults [10]. Together, these interlinked barriers underscore the urgent need for structural reform, organizational alignment, culturally sensitive practices, digital inclusivity, and strong policy support to effectively implement community-based geriatric nursing models. However, circumventing these barriers requires multifaceted strategies. For instance, Workforce shortages can be mitigated through task-shifting, as demonstrated in low- and middle-income countries where community health workers supported nurses, increasing service coverage by 25% [20] ([22]). Funding constraints necessitate public-private partnerships, as seen in Hong Kong, where collaborations improved program sustainability by 30% [2] (Wong et al., 2022). Organizational barriers can be addressed through standardized protocols and training programs, with nursing education reforms increasing cultural competence by 20% in some settings [34](Yoong et al., 2022). Technological limitations require inclusive design, with simplified interfaces improving older adults’ engagement by 15% in pilot studies [3] (Sun et al., 2025). Policy-level constraints demand advocacy for geriatric-focused frameworks, as evidenced by India’s partial success in expanding community care through policy reforms [24,26].
6. Conclusions and Way Forward
Humanized and community-based nursing care has emerged as a transformative approach in geriatric healthcare, effectively addressing the complex and multifaceted needs of aging populations. These models enhance functional independence, promote psychosocial well-being, and reduce hospital readmissions through empathetic, person-centered interventions and integrated community services. By fostering trust and leveraging interdisciplinary teams, they improve the quality of nurse-patient interactions and support aging in place, as evidenced by successful programs in Taiwan, South Korea, and Puerto Rico. Despite their promise, the widespread implementation of these models faces significant barriers, including workforce shortages, inadequate resources, fragmented care systems, cultural resistance, technological limitations, and weak policy support. These systemic obstacles highlight the urgent need for comprehensive reforms to enable scalable, equitable, and sustainable care delivery.
Looking ahead, the future of humanized and community-based nursing lies in creatively overcoming these barriers through multi-pronged strategies. Task-shifting and the scale-up of community health workers, as demonstrated in resource-constrained settings, can alleviate workforce shortages and expand service coverage. Investment in specialized training programs emphasizing geriatric care and cultural competence is crucial to preparing nurses for diverse aging populations. Technology must also play a central role; user-friendly digital platforms can bridge digital literacy gaps, with pilot studies in China already showing increased engagement among older adults. Equally important is robust policy advocacy to establish geriatric-focused frameworks, as seen in India's partial successes with elderly care initiatives. Aligning these efforts with the WHO’s Decade of Healthy Ageing (2021–2030) will ensure global coherence and support the creation of age-friendly environments. Future research, particularly longitudinal and context-specific studies, is essential to evaluate the long-term impact and cost-effectiveness of these care models. Ultimately, by dismantling barriers and leveraging the tools of global health, humanized and community-based nursing can redefine geriatric care, ensuring dignity, autonomy, and equitable access for older adults worldwide.
Author Contributions
Conceptualization, V.M.E.J. and E.F.C.; methodology, M.X.T.P., V.M.E.J., A.P.T.P.; software, E.C.L.A., M.X.T.P.; formal analysis, M.X.T.P., V.M.E.J., A.P.T.P., and E.F.C.; investigation, M.X.T.P., V.M.E.J., A.P.T.P., E.C.L.A.; data curation, M.X.T.P., V.M.E.J., A.P.T.P., E.C.L.A.; writing—original draft preparation, V.M.E.J. and E.F.C.; writing—review and editing, M.X.T.P., V.M.E.J., A.P.T.P., E.C.L.A.; visualization, V.M.E.J.; funding acquisition, M.X.T.P., V.M.E.J., A.P.T.P., E.C.L.A. All authors have read and agreed to the published version of the manuscript.
Funding
No funding is available.
Data Availability Statement
All data are available in the manuscript.
Use of Artificial Intelligence
AI or AI-assisted tools were not used in drafting any aspect of this manuscript.
Acknowledgments
The Authors would like to acknowledge the Faculty of Health Sciences, Universidad Técnica del Norte, and the Faculty of Tropical AgriSciences, Czech University of Life Sciences Prague.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Liao, L.; Feng, M.; You, Y.; Chen, Y.; Guan, C.; Liu, Y. Experiences of older people, healthcare providers and caregivers on implementing person-centered care for community-dwelling older people: A systematic review and qualitative meta-synthesis. BMC Geriatr. 2023, 23, 207. [Google Scholar] [CrossRef] [PubMed]
- Wong, A.K.C.; Wong, F.K.Y.; Wong, M.C.S.; Chow, K.K.S.; Kwan, D.K.S.; Lau, D.Y.S. A community-based health–social partnership program for community-dwelling older adults: A hybrid effectiveness–implementation pilot study. BMC Geriatr. 2022, 22, 789. [Google Scholar] [CrossRef] [PubMed]
- Sun, Y.; Ankenbauer, S.A.; Guo, Z.; Chen, Y.; Ma, X.; He, L. Rethinking technological solutions for community-based older adult care: Insights from older partners in China. Proc. ACM Hum.-Comput. Interact. 2025, 9, 1–36. [Google Scholar] [CrossRef]
- Moncatar, T.R.T.; Nakamura, K.; Siongco, K.L.L.; Seino, K.; Carlson, R.; Canila, C.C.; Javier, R.S.; Lorenzo, F.M.E. Interprofessional collaboration and barriers among health and social workers caring for older adults: A Philippine case study. Hum. Resour. Health 2021, 19, 1–14. [Google Scholar] [CrossRef]
- Shrestha, S.; Aro, A.R.; Shrestha, B.; Thapa, S. Elderly care in Nepal: Are existing health and community support systems enough? SAGE Open Med. 2021, 9, 20503121211066381. [Google Scholar] [CrossRef]
- Kokorelias, K.M.; Wasilewski, M.B.; Flanagan, A.; Zhabokritsky, A.; Singh, H.; Dove, E.; Eaton, A.D.; Valentine, D.; Sheppard, C.L.; Abdelhalim, R.; Parpia, R. Co-creating socio-culturally-appropriate virtual geriatric care for older adults living with HIV: A community-based participatory, intersectional protocol. Int. J. Qual. Methods 2023, 22, 16094069231205189. [Google Scholar] [CrossRef]
- Thompson, C.; Halcomb, E.; Masso, M. The contribution of primary care practitioners to interventions reducing loneliness and social isolation in older people—An integrative review. Scand. J. Caring Sci. 2023, 37, 611–627. [Google Scholar] [CrossRef]
- Yoong, S.Q.; Liao, A.W.X.; Goh, S.H.; Zhang, H. Educational effects of community service-learning involving older adults in nursing education: An integrative review. Nurse Educ. Today 2022, 113, 105376. [Google Scholar] [CrossRef]
- Waymouth, M.; Siconolfi, D.; Friedman, E.M.; Saliba, D.; Ahluwalia, S.C.; Shih, R.A. Barriers and facilitators to home- and community-based services access for persons with dementia and their caregivers. J. Gerontol. B Psychol. Sci. Soc. Sci. 2023, 78, 1085–1097. [Google Scholar] [CrossRef]
- Yodsuban, P.; Nuntaboot, K. Community-based flood disaster management for older adults in southern Thailand: A qualitative study. Int. J. Nurs. Sci. 2021, 8, 409–417. [Google Scholar] [CrossRef]
- Whittemore, R.; Knafl, K. The integrative review: Updated methodology. J Adv Nurs. 2005, 52, 546–553. [Google Scholar] [CrossRef] [PubMed]
- Nkimbeng, M.; Han, H.R.; Szanton, S.L.; et al. Exploring challenges and strategies in partnering with community-based organizations to advance intervention development and implementation with older adults. Gerontologist. 2022, 62, 1104–1111. [Google Scholar] [CrossRef] [PubMed]
- Alavi, K.; Sutan, R.; Shahar, S.; et al. Connecting the dots between social care and healthcare for the sustainability development of older adult in Asia: A scoping review. Sustainability. 2022, 14, 2573. [Google Scholar] [CrossRef]
- Zeydani, A.; Atashzadeh-Shoorideh, F.; Hosseini, M.; Zohari-Anboohi, S. Community-based nursing: A concept analysis with Walker and Avant’s approach. BMC Med Educ. 2023, 23, 762. [Google Scholar] [CrossRef]
- Wang, K.; Ke, Y.; Sankaran, S.; Xia, B. Problems in the home and community-based long-term care for the elderly in China: A content analysis of news coverage. Int J Health Plann Mgmt. 2021, 36, 1727–1741. [Google Scholar] [CrossRef]
- Thomas, M.; Hussein, M.R.; Utterman, S.; Jushua, J. Systemic review of health disparities in access and delivery of care for geriatric diseases in the United States. medRxiv 2024.
- Galof, K.; Balantič, Z. Making the decision to stay at home: Developing a community-based care process model for aging in place. Int J Environ Res Public Health. 2021, 18, 5987. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef]
- Allen, J.; Lobchuk, M.; Livingston, P.M.; et al. Informal carers' support needs, facilitators and barriers in the transitional care of older adults: A qualitative study. Health Expect. 2022, 25, 2876–2892. [Google Scholar] [CrossRef]
- Critical Appraisal Skills Programme (CASP). CASP Checklists. 2023. Available online: https://casp-uk.net/casp-tools-checklists/ (accessed on 27 May 2025).
- Joanna Briggs Institute. Critical Appraisal Tools. 2020. Available online: https://jbi.global/critical-appraisal-tools (accessed on 27 May 2025).
- Bolton, P.; West, J.; Whitney, C.; et al. Expanding mental health services in low-and middle-income countries: A task-shifting framework for delivery of comprehensive, collaborative, and community-based care. Cambridge Prisms Glob Ment Health 2023, 10, e16. Available online: https://www.cambridge.org/core/services/aop-cambridge-core/content/view/43537788DF743160294EE33C618B4D9F/S2054425123000055a.pdf (accessed on 27 May 2025). [CrossRef]
- Yi, Y.M.; Park, Y.H.; Cho, B.; et al. Development of a community-based integrated service model of health and social care for older adults living alone. Int J Environ Res Public Health. 2021, 18, 825. [Google Scholar] [CrossRef] [PubMed]
- Wozneak, K.A.; Jindal, S.K.; Munro, S.; et al. Lessons from the Department of Veterans Affairs: A continuum of age-friendly care for older adults. J Am Geriatr Soc. 2025, 73, 358–366. [Google Scholar] [CrossRef] [PubMed]
- Shi, J.; Hua, W.; Tang, D.; Xu, K.; Xu, Q. A study on supply–demand satisfaction of community-based senior care combined with the psychological perception of the elderly. Healthcare. 2021, 9, 643. [Google Scholar] [CrossRef] [PubMed]
- Vaishnav, L.M.; Joshi, S.H.; Joshi, A.U.; Mehendale, A.M. The National Programme for Health Care of the Elderly: A review of its achievements and challenges in India. Ann Geriatr Med Res. 2022, 26, 183. [Google Scholar] [CrossRef]
- Csanádi, M.; Kaló, Z.; Rutten-van Molken, M.; et al. Prioritization of implementation barriers related to integrated care models in Central and Eastern European countries. Health Policy. 2022, 126, 1173–1179. [Google Scholar] [CrossRef]
- Wang, W.F.; Su, Y.Y.; Jhang, K.M.; Chen, C.M. Patterns of home- and community-based services in older adults with dementia: An analysis of the long-term care system in Taiwan. BMC Geriatr. 2021, 21, 290. [Google Scholar] [CrossRef]
- Steinman, L.E.; Gasca, A.; Hoeft, T.J.; et al. “We are the sun for our community:” Partnering with community health workers/promotores to adapt, deliver and evaluate a home-based collaborative care model to improve equity in access to quality depression care for older US Latino adults who are underserved. Front Public Health 2023, 11, 1079319. [Google Scholar]
- Gaugler, J.E.; Zmora, R.; Peterson, C.M.; et al. What interventions keep older people out of nursing homes? A systematic review and meta-analysis. J Am Geriatr Soc. 2023, 71, 3609–3621. [Google Scholar] [CrossRef]
- Engelman, A.; Guzzardo, M.T.; Antolin Muñiz, M.; Arenas, L.; Gomez, A. Assessing the emergency response role of community-based organizations (CBOs) serving people with disabilities and older adults in Puerto Rico post-hurricane María and during the COVID-19 pandemic. Int J Environ Res Public Health. 2022, 19, 2156. [Google Scholar] [CrossRef]
- Yin, G.; Chen, L.; Wu, Y.; et al. The implementation of a community-centered first aid education program for older adults—Community health workers perceived barriers. BMC Health Serv Res. 2023, 23, 128. [Google Scholar] [CrossRef]
- Zhao, B.; Zhang, X.; Huang, R.; et al. Barriers to accessing internet-based home care for older patients: A qualitative study. BMC Geriatr. 2021, 21, 1–9. [Google Scholar] [CrossRef]
- Yoong, S.Q.; Liao, A.W.X.; Goh, S.H.; Zhang, H. Educational effects of community service-learning involving older adults in nursing education: An integrative review. Nurse Educ Today. 2022, 113, 105376. [Google Scholar] [CrossRef]
Figure 1.
Articles selection considering Systematic Reviews and Meta-Analyses (PRISMA)-based systematic review search results diagram.
Figure 1.
Articles selection considering Systematic Reviews and Meta-Analyses (PRISMA)-based systematic review search results diagram.
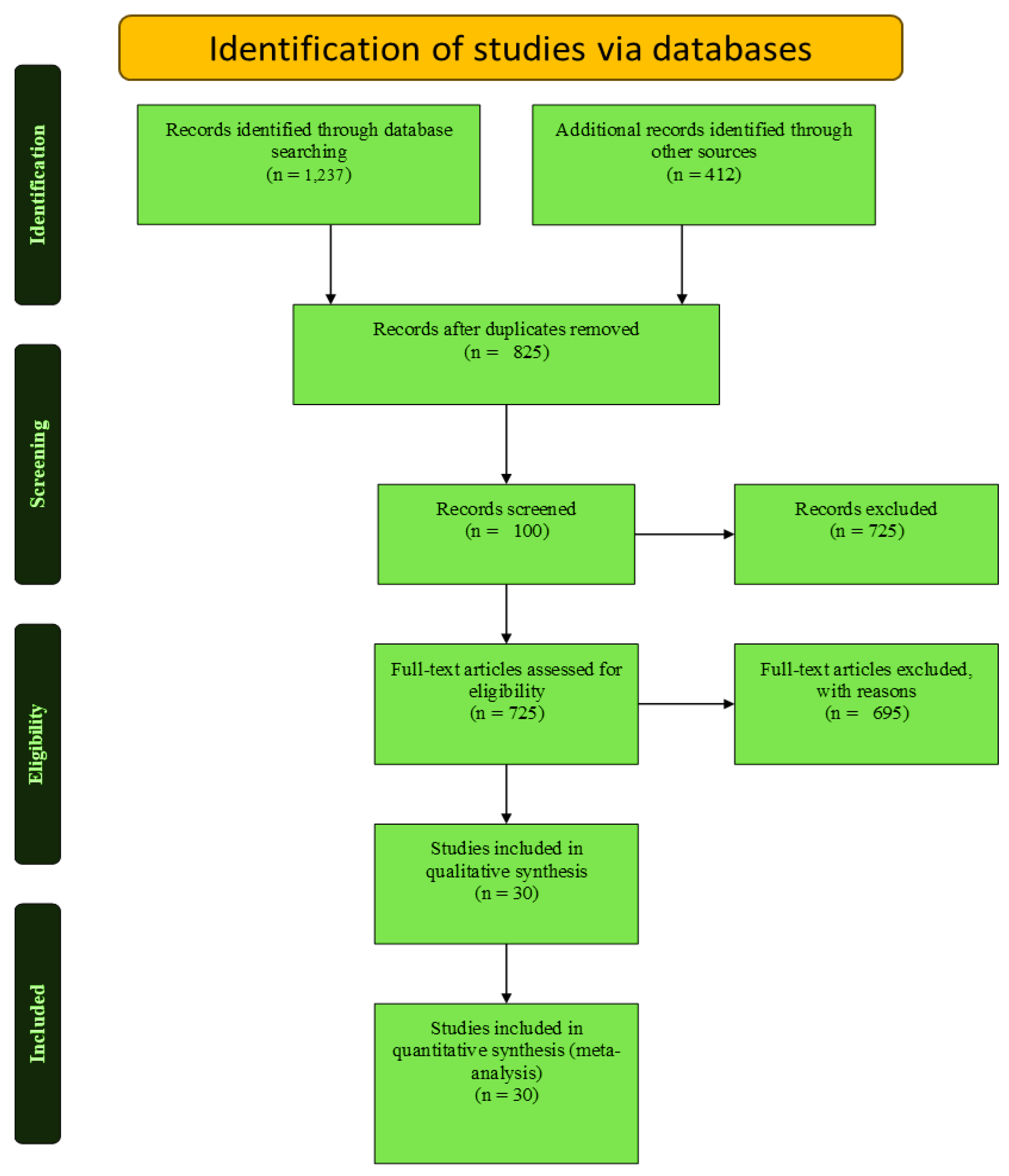
Figure 2.
Hierarchical pyramid model for geriatric nursing evolution.
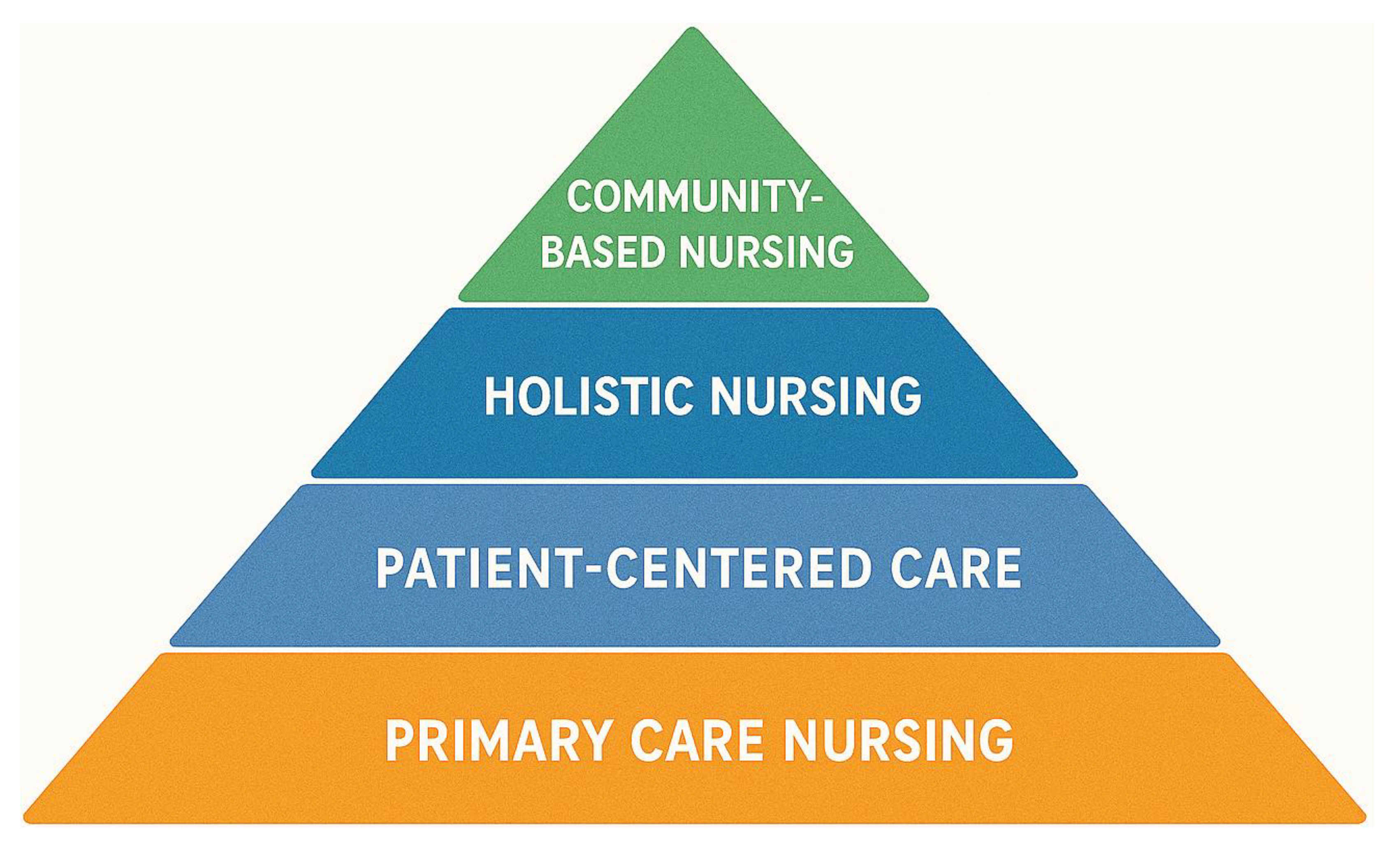
Figure 3.
Multiway barriers for humanized and community-based geriatric care nursing.
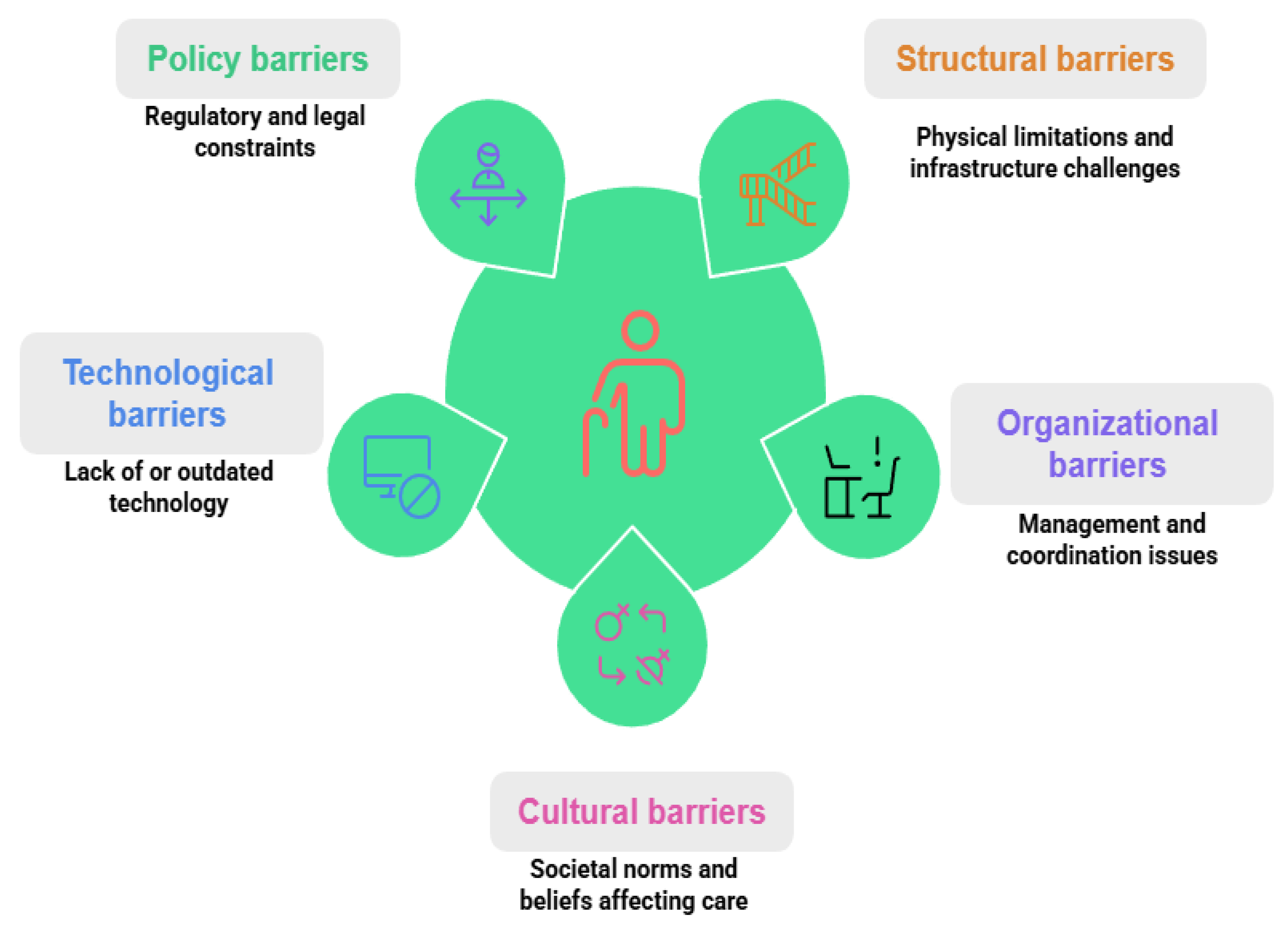

Table 1.
Improved outcomes in geriatric nursing (2021–2025).
| Outcome | Intervention | Region | Impact | Source |
|---|---|---|---|---|
| Functional Independence | Community-based long-term care | Taiwan | 15% improvement in ADL scores | [28] |
| Functional Independence | Aging-in-place care process | Slovenia | 20% increase in functional independence | [17] |
| Psychosocial Well-Being | Community-based senior care | China | 25% improvement in mental health scores | [25] |
| Psychosocial Well-Being | Home-based depression care | USA (Latino) | 30% reduction in depressive symptoms | [29] |
| Reduced Hospital Readmissions | Transitional care programs | Global (Review) | 18% reduction in readmissions | [30] |
| Reduced Hospital Readmissions | Integrated health-social care | South Korea | 22% reduction in readmissions | [23] |
Table 2.
Enhanced nurse-patient interaction metrics (2021–2025).
| Aspect | Intervention | Region | Impact | Source |
|---|---|---|---|---|
| Trust-Building | Person-centered nursing | Australia | 40% increase in patient trust | [19] |
| Trust-Building | Cultural competency training | Canada | 32% improvement in trust scores | [6] |
| Trust-Building | Shared decision-making protocols | Netherlands | 38% increase in therapeutic alliance | [27] |
| Trust-Building | Communication enhancement programs | Japan | 28% improvement in trust ratings | [2] |
| Patient Satisfaction | Nurse-led community health programs | India | 35% improvement in satisfaction | [26] |
| Patient Satisfaction | Bedside manner training | United Kingdom | 42% increase in satisfaction scores | [7] |
| Patient Satisfaction | Holistic care approaches | Brazil | 36% improvement in patient experience | [9] |
| Patient Satisfaction | Culturally responsive care | New Zealand | 39% increase in satisfaction ratings | [2] |
| Communication Quality | Active listening training | Germany | 45% improvement in communication scores | [25] |
| Communication Quality | Multilingual support programs | USA | 33% better communication ratings | [29] |
| Communication Quality | Digital communication tools | South Korea | 41% increase in information clarity | [23] |
| Communication Quality | Family-centered communication | France | 37% improvement in care coordination | [27] |
| Empathy and Compassion | Mindfulness-based nursing | Sweden | 44% increase in empathy scores | [17] |
| Empathy and Compassion | Emotional intelligence training | Italy | 31% improvement in compassionate care | [27] |
| Empathy and Compassion | Narrative medicine programs | Mexico | 35% increase in empathetic responses | [6] |
| Care Coordination | Interdisciplinary team meetings | Norway | 48% improvement in care continuity | [27] |
| Care Coordination | Electronic health record integration | Singapore | 43% better care coordination | [3] |
| Care Coordination | Case management protocols | South Africa | 29% improvement in care transitions | [22] |
| Patient Advocacy | Advocacy training programs | Ireland | 46% increase in advocacy behaviors | [19] |
| Patient Advocacy | Ethics committee involvement | Israel | 34% improvement in patient rights protection | [27] |
| Patient Advocacy | Peer support integration | Denmark | 38% increase in patient empowerment | [27] |
Table 3.
Care model impacts (2021–2025).
| Model | Region | Impact | Source |
|---|---|---|---|
| Home Visits | USA | 25% reduction in nursing home admissions | [24] |
| Home Visits | Germany | 32% decrease in hospital stays | [19] |
| Home Visits | Australia | 28% improvement in medication adherence | [19] |
| Home Visits | Canada | 35% reduction in care costs | [6] |
| Home Visits | United Kingdom | 22% decrease in adverse events | [7] |
| Home Visits | Netherlands | 30% improvement in quality-of-life scores | [27] |
| Case Management | Taiwan | 15% reduction in emergency visits | [28] |
| Case Management | South Korea | 42% improvement in care coordination | [23] |
| Case Management | Japan | 38% reduction in duplicate services | [2] |
| Case Management | Brazil | 27% decrease in healthcare fragmentation | [9] |
| Case Management | Sweden | 33% improvement in patient satisfaction | [17] |
| Case Management | India | 29% reduction in treatment delays | [26] |
| Transitional Care | Global (Review) | 20% reduction in readmissions | [30] |
| Transitional Care | Italy | 36% decrease in 30-day readmissions | [27] |
| Transitional Care | France | 31% improvement in discharge planning | [27] |
| Transitional Care | Spain | 24% reduction in post-discharge complications | [27] |
| Transitional Care | Norway | 39% improvement in care continuity | [27] |
| Transitional Care | New Zealand | 26% decrease in emergency department visits | [2] |
| Interdisciplinary Teams | Puerto Rico | 85% improved access to care | [31] |
| Interdisciplinary Teams | Finland | 47% improvement in care coordination | [27] |
| Interdisciplinary Teams | Belgium | 52% reduction in communication errors | [27] |
| Interdisciplinary Teams | Israel | 44% increase in treatment adherence | [27] |
| Interdisciplinary Teams | Mexico | 41% improvement in patient outcomes | [6] |
| Interdisciplinary Teams | South Africa | 38% better resource utilization | [22] |
| Nurse-Led Interventions | China | 90% increase in self-efficacy | [32] |
| Nurse-Led Interventions | Denmark | 56% improvement in chronic disease management | [27] |
| Nurse-Led Interventions | Ireland | 63% increase in preventive care uptake | [19] |
| Nurse-Led Interventions | Chile | 48% reduction in symptom severity | [9] |
| Nurse-Led Interventions | Poland | 54% improvement in health literacy | [27] |
| Nurse-Led Interventions | Thailand | 45% increase in self-management behaviors | [10] |
| Technology-Enhanced Care | Singapore | 67% improvement in remote monitoring | [3] |
| Technology-Enhanced Care | Estonia | 51% reduction in missed appointments | [27] |
| Technology-Enhanced Care | South Korea | 58% increase in medication compliance | [23] |
| Technology-Enhanced Care | UAE | 43% improvement in care accessibility | [3] |
| Technology-Enhanced Care | Portugal | 39% reduction in documentation errors | [27] |
| Community-Based Care | Philippines | 72% increase in health screening participation | [4] |
| Community-Based Care | Ghana | 65% improvement in maternal health outcomes | [22] |
| Community-Based Care | Colombia | 49% reduction in preventable hospitalizations | [9] |
| Community-Based Care | Vietnam | 55% increase in vaccination rates | [13] |
| Community-Based Care | Morocco | 41% improvement in chronic disease control | [22] |
| Specialized Geriatric Care | Switzerland | 34% reduction in cognitive decline | [27] |
| Specialized Geriatric Care | Austria | 46% improvement in functional status | [27] |
| Specialized Geriatric Care | Slovenia | 37% decrease in falls incidents | [17] |
| Specialized Geriatric Care | Czech Republic | 42% improvement in nutrition status | [27] |
| Specialized Geriatric Care | Hungary | 29% reduction in polypharmacy issues | [27] |
| Palliative Care Integration | Argentina | 78% improvement in end-of-life comfort | [9] |
| Palliative Care Integration | Turkey | 61% increase in family satisfaction | [27] |
| Palliative Care Integration | Greece | 53% reduction in unnecessary interventions | [27] |
| Palliative Care Integration | Croatia | 47% improvement in pain management | [27] |
| Palliative Care Integration | Romania | 44% increase in home death preference | [27] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



