Submitted:
09 June 2025
Posted:
10 June 2025
You are already at the latest version
Abstract
Oral hygiene protocols and basic oral care (BOC) are paramount for patients undergoing cancer treatment; although based upon limited evidence from clinical trials. There are a range of oral care guidelines proposed in the literature mainly focusing on oral mucositis prevention. This systematic review aimed to define the best procedures and practices in the scope of oral hygiene protocols and BOC interventions for the prevention and/or treatment of oral complications in patients under cancer treatment. This systematic review was conducted according to the PRISMA guidelines, and the methods were previously established and registered in PROSPERO (CRD42022319455). Systematic search was completed in 6 databases (PubMed, Scopus, Web of Science, LILACS and Cochrane Library, and gray literature). Eleven studies were included in the qualitative analysis including non-randomized (n = 1) and randomized clinical trials (n = 6), and cohort studies (n = 4). The included studies showed the effectiveness of soft brushes for daily oral hygiene with topical fluoride, use of mouthwashes with 0.12% chlorhexidine, doxepin and benzydamine and saline solutions, as well as dental scaling/prophylaxis in decreasing the severity of oral toxicities. Although not well explored by well-designed clinical studies, BOC protocols may be effective in prevention oral toxicities from cancer therapy and are supported in multiple guidelines.
Keywords:
basic oral care
; oral mucositis
; patient education
; dental care
; guidelines
; cancer
1. Introduction
Cancer is a significant public health problem world-wide, whose incidence and mortality have been increasing, due to aging, population growth or changes in the distribution and prevalence of cancer risk factors, both of which are associated with socioeconomic development [1]. The principle contemporary treatment modalities for cancer include for solid tumors, surgical resection, radiation therapy (RT), chemotherapy (CT), targeted and immunotherapy, and for liquid tumors, chemotherapy and hematopoietic stem cell transplant [2].
RT, CT, and combined therapy for oral cancer treatment have a high potential to produce direct tissue damage of the oral cavity and some adverse effects on healthy tissues indirectly, which are often irreversible and may occur months to years after completing RT. These include xerostomia, oral mucositis (OM), dysphagia, lymphedema, radiation caries, periodontal disease, osteonecrosis of the jaw, dysgeusia and oral pain [3,4,5,6]. The management of these toxicities is essential to achieve a better quality of life.
Due to significant impact upon quality of lief, it is important to prevent both acute and late oral toxicities of cancer treatment. Pretreatment dental assessment is critical and in some cases is the only opportunity for management of preexisting dental conditions that could lead to significant and difficult to manage oral/dental toxicities and preventing complications during and following active cancer therapy [10]. Within the multidisciplinary team, the dentist is responsible for prevention and management of such oral and dental toxicities. Treatment should be directed to the needs of each patient, which could lead to large variations in the dental care given because it is up to the individual and the dental treatment planning for the care of each patient. This may lead to inequalities in the care provided [11,12].
Several review articles have been published suggesting methods to prevent and/or manage oral complications before, during, and after cancer treatment [7,8,9]. However, to the best of our knowledge, no summarized data through a systematic approach has been performed. Therefore, highlighting the important role of the dental professional in the prevention and management of the oral complications, this systematic review (SR) reviewed, analyzed and integrated published evidence assessing BOC in order to propose a standard preventive dental intervention and procedures in patients undergoing cancer treatment.
2. Material and Methods
2.1. Eligibility Criteria
The acronym PICOS was framed based on the Guidance for defining review question (CHARMS Checklist) to guide the focused review question and to determine the inclusion criteria, of which: P) Cancer patients; I) Dental procedures executed by dentists in a hospital environment, such as techniques for brushing teeth, including types of toothbrush, brushing time and frequency, mouthwashes and its best components with high levels of antimicrobial efficiency and dental prophylaxis; C) Compare the results found with previously published guides and studies; O) Evaluate the effectiveness of dental procedures in cancer patients; and S) Randomized/non-randomized clinical trials and cohorts’ studies.
In this study, articles that did not evaluate dental procedures in cancer patients performed by dentists in a hospital environment were excluded, studies in which dental procedures (described above) data were not available for data extraction due to grouping with other type of dental procedures, studies that did not clearly report or could not be calculated the odds/risk ratio, reviews case reports, short communication, personal opinions, letters, conference abstracts, and laboratory research and articles whose full texts were not available were also all excluded. Table 1 describes a checklist used to select the articles used in this study.
2.2. Information Sources and Search Strategy
Individualized search strategies were conducted on April 12nd, 2023 in these electronic databases: PubMed, Cochrane Library, Lilacs, Scopus, Web of Science and gray literature (Google Academic). (Appendix 1). The following descriptors included MeSH (Medical Subject Headings): “Mouth Neoplasms” combined with “or” and “oral cancer” an “and” “oral care”, “oral management”, “mouthrinse”, “tooth brushing”, “dental care”, “dental procedure”. The retrieved references were imported into the Endnote Web reference manager (Endnote Web, Clarivate Analytics, Philadelphia, PA), where duplicate references were removed. The search strategy is shown in Supplementary Material 1.
2.3. Selection Process
Study selection was independently and blindly performed in two phases by two authors (M.C.C and A.L.D.A), respecting the inclusion and exclusion criteria previously established. In the first phase, the titles and abstracts of the identified references were read on Rayyan® [36]. The studies which appeared to meet inclusion criteria went to the second phase of selection process, in which the full texts were read, and the eligibility criteria were confirmed. In addition, the reference lists of all included studies were read, -screened for potentially missing studies. Divergences in both phases were resolved by discussion and mutual agreement among the authors.
2.4. Data Collection Process and Data Items
The relevant data to be selected was discussed between all authors, extracted by M.C.C and cross-checked by A.L.D.A. The extracted variables were author/year, number of patients, age, oncologic treatment, complication/toxicity/treated condition, alcohol and tobacco status, follow-up time, dental intervention, moment of the dental intervention (prior to, during, and after the oncologic treatment), instructions for the dental intervention usage, main and secondary results, conclusion.
2.5. Risk of Bias Assessments
The quality of the information collected in article selected were assessed using the Joanna Briggs Institute Critical Appraisal Checklists for Randomized Clinical Trials, Non-randomized Clinical Trials and Cohort Studies [37]. One reviewer (M.C.C) independently classified each study as “high” if the percentage of “yes” scores reached up to 49% score “yes”; “moderate” if the percentage of “yes” scores was between 50% to 69%; and “low” if the percentage of “yes” scores was more than 70%.
2.6. Effect Measures
The objective of this SR was to examine dental management recommended for patients who will undergo cancer treatment (radiotherapy and/or chemotherapy) to achieve best dental outcomes: including caries and periodontal disease during treatment, reduced risk of fewer secondary infections in the mouth. While the measure of effect considered was the odds ratio, due to the lack of homogeneity between the articles included, it was not possible to carry out the analysis due to lack of homogeneity between the articles as the studies presented heterogeneous data, with different designs and distinct variables.
A qualitative synthesis was performed, presenting a descriptive analysis of the available evidence. The primary results of the studies were reported, presenting the procedures performed on the patients and the specifications of each, associating them with the best statistically proven results, as described in the studies.
3. Results
3.1. Study Selection
Among the total of 2.589 articles identified through search strategy, 11 articles [12,13,14,15,16,17,18,19,20,21,22] were included in the quantitative synthesis. The selection process is summarized in the PRISMA flowchart (Figure 1) and the reasons for exclusion of each of the articles that were read in full are described in Supplementary Material 2.
3.2. Study Characteristics
Data included 830 patients (607 males [73.13%]; 223 females [26.87%]; 176 not informed [37.93%]), with ages ranging from 7 to 82 years old, treated with diverse RT regimens (total dose ranging from 50 to 70 Gy), with or without concomitant CT. Mucositis was the condition more frequently treated (seven studies) [16,17,18,19,20,21,22], followed by periodontal health/biofilm control (two studies) [12,14], and osteoradionecrosis (two studies) [13,15]. Within the studies evaluating the grade of OM, two studies based their evaluation according to the RTOG (Radiation Therapy Oncology Group) grading system [13,17], while three evaluated subjectively, using an Oral Mucositis Daily Questionnaire (OMDQ) [19,21,22]. One article applied the Who score for OM and the OMDQ [16]. One study evaluated by the mean of mucositis which score was obtained by adding the single scores for each anatomic area at risk (defined as areas receiving a cumulative radiation dose of at least 4000 cGy) and dividing by the number of areas included in the RT field [20].
147 patients reported smoking and 140 alcohol use, but this information was only present in four articles [15,16,17,18]. In four studies, patients received interventions and were evaluated prior to, during, and after cancer treatment [12,13,14,15]. Oral hygiene habits before, during and after cancer treatment were reported in 3 studies [12,14,15].
The patient’s observation time ranged from 6 weeks to 10 years, with 36.3% of studies reporting a 6-month follow-up [14,16,18,19]. Table 2 presents the characteristics of the included articles.
Of the included studies, six are randomized clinical trials, where four [17,20,21,22] is reported to blind patients, the other studies of the type [18,19] do not contain such information. The four papers discuss before and during the cancer treatment the effectiveness of mouthwashes on radiotherapy toxicities, with a main focus on OM. The non-randomized clinical study evaluates the effect of an oral hygiene protocol before, during and after cancer treatment applied in the study group compared to a control group (simple oral hygiene instructions, without dental intervention) [12]. With the exception of Stockman, 2012 [16] where the effect of mouthwash during patient treatment is evaluated, the other three cohort studies [13,14,15] present the effects of oral care protocols at different stages of cancer treatment (before, during and after).
3.3. Risk of Bias in Studies
Most of the included studies were classified as having low risk of bias (n = 9; 81.0%), two (18.1%) studies as moderate risk, and one was classified as high risk (n = 0.8%). The main issues that influenced the risk of bias were identified in the methods. The detailed description of the subjects and scenario, the method used to evaluate the results were well described in most studies (n = 9; 81.0%), as well as the sample selection criteria. On the other hand, in 3 articles the information about the follow-up was not clear in details about the time (n = 27.2%). The risk of bias assessment is described in detail in Supplementary Material 3.
3.4. Results of Individual Studies
Seven studies investigated the impact of mouthwashes in the oral toxicities. Kazemian [17] demonstrated the effectiveness of benzydamine in reducing mucositis resulting from radiotherapy and its effects (such as pain), which consequently reduced the number of patients who had treatment interrupted due to complications. Samarannayake [19] also demonstrated the effectiveness of the mouthwash, however the patients in the study reported greater comfort when using 0.12% chlorhexidine, whose antimicrobial and pain effectiveness was similar. Epstein [20] demonstrates the prophylactic effect of the benzydamine mouthwash in regimens up to cumulative doses of 5000cGy of RT, where erythema and ulceration were reduced by approximately 30% compared with the placebo; 33% of benzydamine subjects remained ulcer free compared with 18% of placebo subjects and it was shown significantly delayed the use of systemic analgesics compared with placebo. Satheeshkumar [18] evaluated the effectiveness of triclosan compared to placebo (saline solution), but did not observe a statistically significant difference between them. Stockman [16] shows that concentrated solutions of calcium phosphates showed no significant difference compared to saline during cancer treatment. Leenstra [21] evaluated the effects of doxepin as a mouthwash compared to placebo, mouth and throat pain reduction was greater for doxepin, a crossover analysis of patients completing both phases confirmed that patients experienced greater mouth and throat pain reduction with doxepin, however, the mouthwash was associated with more stinging or burning, unpleasant taste, and greater drowsiness than the placebo rinse. Sio [22] studied doxepin and found similar results as well, mucositis pain during the first 4 hours was better decreased in the group, compared to diphenhydramine-lidocaine-antacid mouthwash and placebo. More drowsiness was reported with doxepin mouthwash than placebo, as well as unpleasant taste and stinging or burning.
The use of brushes with soft bristles proved to be the most suitable for oral hygiene. Regezi [15] suggested that brushing at least twice a day had significant rates of biofilm clearance, thus preventing caries, as is well known in the literature, but focusing on the importance of the softness of the bristles of the brushes so as not to traumatize the oral soft tissue during RT or CT.
Tooth surface scaling and root planning showed effectiveness in eliminating foci of bacteria, patients undergoing such procedures before cancer treatment had better periodontal results during and after treatment, with lower rates of need for invasive treatments later [14]. Periodontal treatment before oncologic treatment and after shown a decreased measurement in probing depth and gingival bleeding. Complementing these findings, Nuñez-Aguilar [12] states that polishing rough edges or surfaces resulted in fewer complaints of discomfort and mucosal injuries during cancer treatment. In addition, the study showed that restorations before cancer treatment had significant rates of prevention and maintenance of oral health for preventing bedsores in the oral mucosa. Both of these studies used fluoride gels to prevent caries at all times during cancer treatment, with effective results, as was expected.
Niewald [13] states that dental treatment procedures should be performed within at least 7 to 10 days from the last procedure until the beginning of radiotherapy, ensuring minimal tissue healing (gum, bone, and periodontal ligament). Tooth extractions should mainly be performed aiming at suturing techniques with complete tissue closure and prophylactic antibiotic therapy starting one day before the procedure, extending up to 10 days after. Tooth extractions were performed according to a written protocol under “special care” (primary tissue closure, perioperative antibiotics for 7-10 days starting one day before surgery). Patients were advised not to wear their dental prostheses up to 6–12 months after radiotherapy in order to preserve the gums. In the end, the rate of patients in the study who developed osteoradionecrosis was low, but the results show that the amount of radiation and whether hyper fractionated is a direct factor in the development of this toxicity.
Despite being different studies in methodological design, they were the ones with the best design. Nunez-Aguilar evaluated the effects of oral hygiene guidance, restorative procedures, periodontic and surgical procedures on the patient's quality of life at each stage of treatment, by evaluating mucositis severity, gingival bleeding, pain, weight loss and trauma to the mucous. Just like Bueno, who evaluated before and after cancer treatment (180 days after) the effects of basic periodontal treatment on patients, finding decreasing the depth of periodontal probing, also resulting in an improvement in the quality of the patient's health. Samarannayake showed the effectiveness of the rinse with 0.12% chlorhexidine in improving oral mucositis, with antimicrobial activity.
4. Discussion
This SR evaluated protocols in the literature that address the issue of basic oral health care for patients undergoing cancer treatment. The importance of the toothbrush choice for daily brushing, the brushing technique, choice of alcohol-free rinses, preference for saline or chlorhexidine and the timing of these procedures are essential to guarantee success and comfort to the patient, from the dental and oncological point of view.
Mechanical cleaning of teeth is a prerequisite for good oral health, especially among cancer patients [17,23,24]. Attention to maintaining good daily oral hygiene practices, including cleaning the interdental spaces with dental floss [25]. Meurman [26] showed that tooth brushing combined with chlorhexidine rinses prevented bacteremia in immunosuppressed patients due to oncologic treatment, which supports the findings in the study of Nunez-Aguilar [12]. The administration of antibacterial agents to control oral biofilms is a recommended strategy for patients with oral cancer, considering that rinses improve the removal of oral biofilms, oral debris, promote oral hygiene and improve patient comfort during cancer therapy.
Chlorhexidine is the gold standard for chemical plaque control, but its effectiveness in preventing caries is still uncertain [27,28]. Hancock [29] recommended that patients start prophylactic chlorhexidine mouthwashes to prevent the onset of microbial infection, gingival inflammation and bleeding, and to reduce the risk of caries pre-cancer treatment. Foote [30] report that an oral rinse with chlorhexidine has potential effects on OM, such as Samarannayake [19], even though it has not shown significant effect on oral pain or in the oral carriage of the microorganisms. The benzydamine rinse showed significant action against pain with a topical analgesic effect, bringing a more comfortable experience to the patient. Epstein [20] also points out that throat pain was also reduced with benzydamine compared with placebo. Laine [31] compared the use of saline-based mouthwashes with sodium bicarbonate and show that the use of alcohol-based mouthwashes and hydrogen peroxide mouthwashes should be discontinued due to their drying and irritating effects on the oral mucosa. Stockman [16] adds to the list that calcium phosphate does not have an effective action against OM, in addition to presenting discomfort in the study group. Furthermore, the rinse with doxepin showed interesting results in controlling pain, patients showed interest in continuing the treatment even with adverse effects [32]. Doxepin has effects on both the central and peripheral nervous systems, making it an option that can be used for the treatment of radiotherapy-induced oral mucositis pain.
Fluoride prophylaxis is one of the methods of choice to combat caries, especially in patients with oral cancer due to the ease of access to the procedure [33]. Fluoride strengthens the acid resistance of dental hard tissues and can inhibit the cariogenic oral microbiota. Meyerowitz investigated different application methods used is not critical as long as the patient receives daily fluoride and understands his daily need [34].
The various problems that an oral cancer patient may face in maintaining oral health require prophylactic protocols and personalized treatment modes. Basic oral care performed by trained professionals is a necessity, in addition to the patient's daily self-care. Adherence to dental treatment recommendations can be an obstacle to prevention of complications. General principles for prevention and treatment of patients with reduced salivary flow, dental caries, and oral candidiasis are also valid for oral cancer patients. These at-risk patients need intensified prophylaxis and procedures to prevent even life-threatening systemic infections from the mouth. Good oral health care is also directly related to patients' quality of life.
The prevention of oral complications, early recognition, diagnosis and management of oral complications generally unite experience in medical and dental care within a multidisciplinary team [35]. It is important to remember that the planning of any dental treatment begins with a thorough oral examination and radiographic examinations. It is recommended that the patient continue weekly follow-up with the oral care professional during cancer therapy [9].
5. Limitations
In evaluating the studies, some limitations were found. An important point was the lack of clarity in detailing the design of the studies carried out. Some report results and conclusions that cannot be affirmed by the way the research was conducted.
During the research, we found many works with complex interventions or with a lack of details about the basic procedures. There is a need to detail the stages of adaptation of patients, which steps were taken and products used, many works only mention that this step in the treatment of the patient was done. Only with this information will it be possible to determine a basic oral care protocol supported by consistent and logical evidence.
6. Conclusion
Limited data is available on the impact of dental care prior to cancer therapy, and oral care during active cancer care. There is, however, general consensus supporting oral evaluation and treatment prior to cancer treatment and continuing oral care during and after therapy [34,35]. The findings of this review show us that preventive dental action has an impact on the quality of life of patients, in terms of controlling toxicities resulting from cancer treatment. Use of mouthwash with 0.12% chlorhexidine; soft brushes, topical fluoride applications at all stages of treatment and follow-up are essential. It is still necessary to develop a basic care protocol, basic prevention procedures in a more specific way in order to guarantee better results and more comfort to patients.
6.1. Recommendations for Future Primary Studies
After evaluating the articles in this review, we suggest the following guidelines for future studies: randomized blinded clinical trials, details of the stages of oral preparation of cancer patients, details of the cancer (type/stage), details of cancer therapy and patient demographics. Studies with good methodological design with controlled trials the goal. Publications presenting details of the of the procedures performed, including details of oral care provided, compliance with oral care recommendations, products delivery of the products used to include format of product (e.g.: rinse, cream, gel concentrations, amounts and time), directions for product use, and description of hygiene instructions for the patient , frequency and duration of products used.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Protocol and registration
The methods of this SR were established before starting the review, and the resulting protocol was based on PRISMA-P [40,41] which was registered at the International Prospective Register of SRs (PROSPERO) database under registration number CRD42022319455 [42]. Additionally, the present SR was reported according to the Preferred Reporting Items for SRs and Meta-Analyses (PRISMA) checklist [43].
Acknowledgments
The authors would like to gratefully acknowledge the Coordination for the Improvement of Higher Education Personnel (CAPES/PROEX, Brazil) process number 001, the National Council for Scientific and Technological Development (CNPq, Brazil), and the grants from São Paulo Research Foundation (FAPESP, Brazil).
Funding
This work was supported by Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES, Brazil) processes number 8887.640785/2021-00. None of the authors received research support from companies or similar organizations that may gain or lose financially through publication of this manuscript. A.L.D.A. is a Post-Doctoral researcher who holds a fellowship funded by The São Paulo Research Foundation (FAPESP: 2021/14585-7).
Competing Interests
The authors have no relevant financial or non-financial interests to disclose.
Author Contributions
All authors made substantial contributions to the conception (M.C.C.; A.R.S.S.; A.C.P.R.), draft and material preparation, data collection and analysis (M.C.C.; M.I.A.W; M.E.P.O.; A.G.C.N.; A.L.D.A.;), and review (M.E.P.O.; A.G.C.N.; A.L.D.A.; A.R.S.S.; A.C.P.R.) of the data for the work.
Ethical approval
Does not apply.
Consent to participate
Does not apply.
Consent for publication
Does not apply.
References
- Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018 Nov;68(6):394-424. Epub 2018 Sep 12. Erratum in: CA Cancer J Clin. 2020 Jul;70(4):313. [CrossRef]
- Caribé-Gomes F, Chimenos-Küstner E, López-López J, Finestres-Zubeldia F, Guix-Melcior B. Dental management of the complications of radio and chemotherapy in oral cancer. Med Oral. 2003 May-Jul;8(3):178-87. English, Spanish.
- Mosel DD, Bauer RL, Lynch DP, Hwang ST. Oral complications in the treatment of cancer patients. Oral Dis. 2011;17:550-9.
- Epstein, JB., Hong, C., Logan, RM., Barasch, A., Gordon, SM., Oberlee-Edwards, L. A systematic review of orofacial pain in patients receiving cancer therapy. Support Care Cancer, 2012; 18:1023–1031.
- Burlage, FR., Coppes, RP., Meertens, H., Stokman, MA., & Vissink, A. Parotid and submandibular/sublingual salivary flow during high dose radiotherapy. Radiation Oncology, 2001; 61:271–274.
- Almståhl, A., Finizia, C., Carlén, A., Fagerberg-Mohlin, B., & Alstad, T. Explorative study on mucosal and major salivary secretion rates, caries and plaque microflora in head and neck cancer patients. International Journal of Dental Hygiene, 2018; 16:450–458.
- Moon, DH., Moon, SH., Wang, K., Weissler, MC., Hackman, TG., Zanation, A. M. Incidence of, and risk factors for, mandibular osteoradionecrosis in patients with oral cavity and oropharynx cancers. Oral Oncology, 2017; 72:98–103.
- Pauli, N., Johnson, J., Finizia, C., Andréll, P. The incidence of trismus and long-term impact on health-related quality of life in patients with head and neck cancer. Acta Oncologica, 2013; 52:1137–1145.
- De Sanctis, V., Bossi, P., Sanguineti, G., Trippa, F., Ferrari, D., Bacigalupo, A. Mucositis in head and neck cancer patients treated with radiotherapy and systemic therapies: Literature review and consensus statements. Critical Reviews in Oncology/Hematology, 2016; 100:147–166.
- Jensen, S. B., Jarvis, V., Zadik, Y., Barasch, A., Ariyawardana, A., Hovan, A. Systematic review of miscellaneous agents for the management of oral mucositis in cancer patients. Support Care Cancer, 2013; 21:3223–3232.
- Lanzós, I., Herrera, D., Lanzós, E., Sanz, M. A critical assessment of oral care protocols for patients under radiation therapy in the regional University Hospital Network of Madrid. Journal of Clinical and Experimental Dentistry, Spain, 2015; 27: 613–621.
- Nuñez-Aguilar J, Fernández-Olavarría A, Oliveros-López LG, Torres-Lagares D, Serrera-Figallo MA, Gutiérrez-Corrales A, Gutiérrez-Pérez JL. Evolution of oral health in oral cancer patients with and without dental treatment in place: Before, during and after cancer treatment. J Clin Exp Dent. 2018; 1,10(2):158-165. [CrossRef]
- Niewald M, Fleckenstein J, Mang K, Holtmann H, Spitzer WJ, Rübe C. Dental status, dental rehabilitation procedures, demographic and oncological data as potential risk factors for infected osteoradionecrosis of the lower jaw after radiotherapy for oral neoplasms: a retrospective evaluation. Radiat Oncol. 2013 Oct 2;8:227. [CrossRef]
- Bueno AC, Ferreira RC, Barbosa FI, Jham BC, Magalhães CS, Moreira AN. Periodontal care in patients undergoing radiotherapy for head and neck cancer. Support Care Cancer. 2013 Apr; 21(4):969-75.
- Regezi JA, Courtney RM, Kerr DA. Dental management of patients irradiated for oral cancer. Cancer 1976; 38: 994- 1000.
- Stokman MA, Burlage FR, Spijkervet FK. The effect of a calcium phosphate mouth rinse on (chemo) radiation induced oral mucositis in head and neck cancer patients: a prospective study. Int J Dent Hyg. 2012 Aug;10(3):175-80. [CrossRef]
- Kazemian A, Kamian S, Aghili M, Hashemi FA, Haddad P. Benzydamine for prophylaxis of radiation-induced oral mucositis in head and neck cancers: a double-blind placebo-controlled randomized clinical trial. Eur J Cancer Care (Engl). 2009 Mar;18(2):174-8. [CrossRef]
- Satheeshkumar PS, Chamba MS, Balan A, Sreelatha KT, Bhatathiri VN, Bose T. Effectiveness of triclosan in the management of radiation-induced oral mucositis: a randomized clinical trial. J Cancer Res Ther. 2010 Oct-Dec;6(4):466-72.
- Samaranayake LP, Robertson AG, MacFarlane TW, Hunter IP, MacFarlane G, Soutar DS, Ferguson MM. The effect of chlorhexidine and benzydamine mouthwashes on mucositis induced by therapeutic irradiation. Clin Radiol. 1988 May;39(3):291-4. [CrossRef]
- Epstein JB, Silverman S Jr, Paggiarino DA, Crockett S, Schubert MM, Senzer NN, Lockhart PB, Gallagher MJ, Peterson DE, Leveque FG. Benzydamine HCl for prophylaxis of radiation-induced oral mucositis: results from a multicenter, randomized, double-blind, placebo-controlled clinical trial. Cancer. 2001 Aug 15;92(4):875-85.
- Leenstra JL, Miller RC, Qin R, Martenson JA, Dornfeld KJ, Bearden JD, Puri DR, Stella PJ, Mazurczak MA, Klish MD, Novotny PJ, Foote RL, Loprinzi CL. Doxepin rinse versus placebo in the treatment of acute oral mucositis pain in patients receiving head and neck radiotherapy with or without chemotherapy: a phase III, randomized, double-blind trial (NCCTG-N09C6 [Alliance]). J Clin Oncol. 2014 May 20;32(15):1571-7. Epub 2014 Apr 14. [CrossRef]
- Sio TT, Le-Rademacher JG, Leenstra JL, Loprinzi CL, Rine G, Curtis A, Singh AK, Martenson JA Jr, Novotny PJ, Tan AD, Qin R, Ko SJ, Reiter PL, Miller RC. Effect of Doxepin Mouthwash or Diphenhydramine-Lidocaine-Antacid Mouthwash vs. Placebo on Radiotherapy-Related Oral Mucositis Pain: The Alliance A221304 Randomized Clinical Trial. JAMA. 2019 Apr 16;321(15):1481-1490. [CrossRef]
- Epstein JB, Güneri P, Barasch A. Appropriate and necessary oral care for people with cancer: guidance to obtain the right oral and dental care at the right time. Support Care Cancer. 2014 Jul;22(7):1981-8. Epub 2014 Mar 28. [CrossRef]
- Huang BS, Wu SC, Lin CY, Fan KH, Chang JT, Chen SC. The effectiveness of a saline mouth rinse regimen and education programme on radiation-induced oral mucositis and quality of life in oral cavity cancer patients: A randomised controlled trial. Eur J Cancer Care (Engl). 2018 Mar;27(2).
- Bonnaure-Mallet M, Bunetel L, Tricot-Doleux S, Guérin J, Bergeron C, LeGall E. Oral complications during treatment of malignant diseases in childhood: effects of tooth brushing. Eur J Cancer 1998; 34:1588–91.
- Meurman JH, Grönroos L. Oral and dental health care of oral cancer patients: hyposalivation, caries and infections. Oral Oncol. 2010 Jun; 46(6):464-7. Epub 2010 Mar 21. [CrossRef]
- Antunes H, Ferreira E, Faria L, Schirmer M, Rodrigues PC, Small I, et al. Streptococcal bacteraemia in patients submitted to hematopoietic stem cell transplantation: the role of tooth brushing and use of chlorhexidine. Med Oral Patol Oral Cir Bucal 2010; 15:303–9.
- Autio-Gold J. The role of chlorhexidine in caries prevention. Oper Dent 2008; 33:710–6.
- Hancock PJ, Epstein JB, Sadler GR. Oral and dental management related to radiation therapy for head and neck cancer. J Can Dent Assoc. 2003 Oct;69(9):585-90.
- Foote RL, Loprinizi CL, Frank AR, O’Fallon JR, Gulavita S, Twefik HH, and others. Randomized trial of a chlorhexidine mouthwash for alleviation of radiation-induced mucositis. J Clin Oncol 1994; 12(12):2630–3.
- Laine P, Meurman JH, Murtomaa H, Lindqvist C, Torkko H, Pyrhönen S, et al. One-year trial of the effect of rinsing with an amine fluoride–stannous– fluoride-containing mouthwash on gingival index scores and salivary microbial counts in lymphoma patients receiving cytostatic drugs. J Clin Periodontol 1993; 20:628–34.
- Sudoh Y, Cahoon EE, Gerner P, Wang GK. Tricyclic antidepressants as long-acting local anesthetics. Pain. 2003;103(1-2):49-55. [CrossRef]
- Epstein JB, Chin EA, Jacobson JJ, Rishiraj B, Le N. The relationships among fluoride, cariogenic oral flora, and salivary flow rate during radiation therapy. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1998; 86:286–92.
- Meyerowitz C, Watson 2nd GE. The efficacy of an intraoral fluoride-releasing system in irradiated head and neck cancer patients: a preliminary study. J Am Dent Assoc 1998; 129:1252–9.
- Epstein JB, van der Meij EH, Lunn R, Stevenson-Moore P. Effects of compliance with fluoride gel application on caries and caries risk in patients after radiation therapy for head and neck cancer. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1996; 82:268–75.
- Mourad Ouzzani, Hossam Hammady, Zbys Fedorowicz, and Ahmed Elmagarmid. Rayyan — a web and mobile app for systematic reviews. Systematic Reviews (2016) 5:210. [CrossRef]
- Moola S, Munn Z, Tufanaru C, Aromataris E, Sears K, Sfetcu R, Currie M, Lisy K, Qureshi R, Mattis P, Mu P (2020) Chapter 7: Systematic reviews of etiology and risk. In: Aromataris E, Munn Z (eds) JBI manual for evidence synthesis. JBI. Available from https://synthesismanual.jbi.global. [CrossRef]
- Lalla RV, Bowen J, Barasch A, Elting L, Epstein J, Keefe DM, McGuire DB, Migliorati C, Nicolatou-Galitis O, Peterson DE, Raber-Durlacher JE, Sonis ST, Elad S; Mucositis Guidelines Leadership Group of the Multinational Association of Supportive Care in Cancer and International Society of Oral Oncology (MASCC/ISOO). MASCC/ISOO clinical practice guidelines for the management of mucositis secondary to cancer therapy. Cancer. 2014 May 15;120(10):1453-61. [CrossRef]
- Elad S, Cheng KKF, Lalla RV, Yarom N, Hong C, Logan RM, Bowen J, Gibson R, Saunders DP, Zadik Y, Ariyawardana A, Correa ME, Ranna V, Bossi P; Mucositis Guidelines Leadership Group of the Multinational Association of Supportive Care in Cancer and International Society of Oral Oncology (MASCC/ISOO). MASCC/ISOO clinical practice guidelines for the management of mucositis secondary to cancer therapy. Cancer. 2020 Oct 1;126(19):4423-4431. [CrossRef]
- National Comprehensive Cancer Network (2021) Head and neck cancers (Version3.2021). https://www.nccn.org/professionals/physician_gls/pdf/head-and-neck.pdf.
- Shamseer L, Moher D, Clarke M et al (2015) Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: elaboration and explanation OPEN ACCESS. BMJ. [CrossRef]
- Cuzzullin MC, Pérez-de-Oliveira, Normando AGC, Santos-Silva AR, Prado-Ribeiro, AC (2021) Basic oral care in cancer patients: a systematic review. In: PROSPERO CRD42022319455 Available from: https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42022319455.
- Page MJ, Moher D, Bossuyt PM et al (2021) PRISMA 2020 explanation and elaboration: updated guidance and exemplars for reporting systematic reviews. BMJ (Clinical research ed) 372:n160–n160. [CrossRef]
Figure 1.
PRISMA 2020 flow diagram for new systematic reviews which included searches of databases, registers and other sources. From: Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 2021;372:n71. doi: 10.1136/bmj.n71. For more information, visit: http://www.prisma-statement.org/.
Figure 1.
PRISMA 2020 flow diagram for new systematic reviews which included searches of databases, registers and other sources. From: Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 2021;372:n71. doi: 10.1136/bmj.n71. For more information, visit: http://www.prisma-statement.org/.
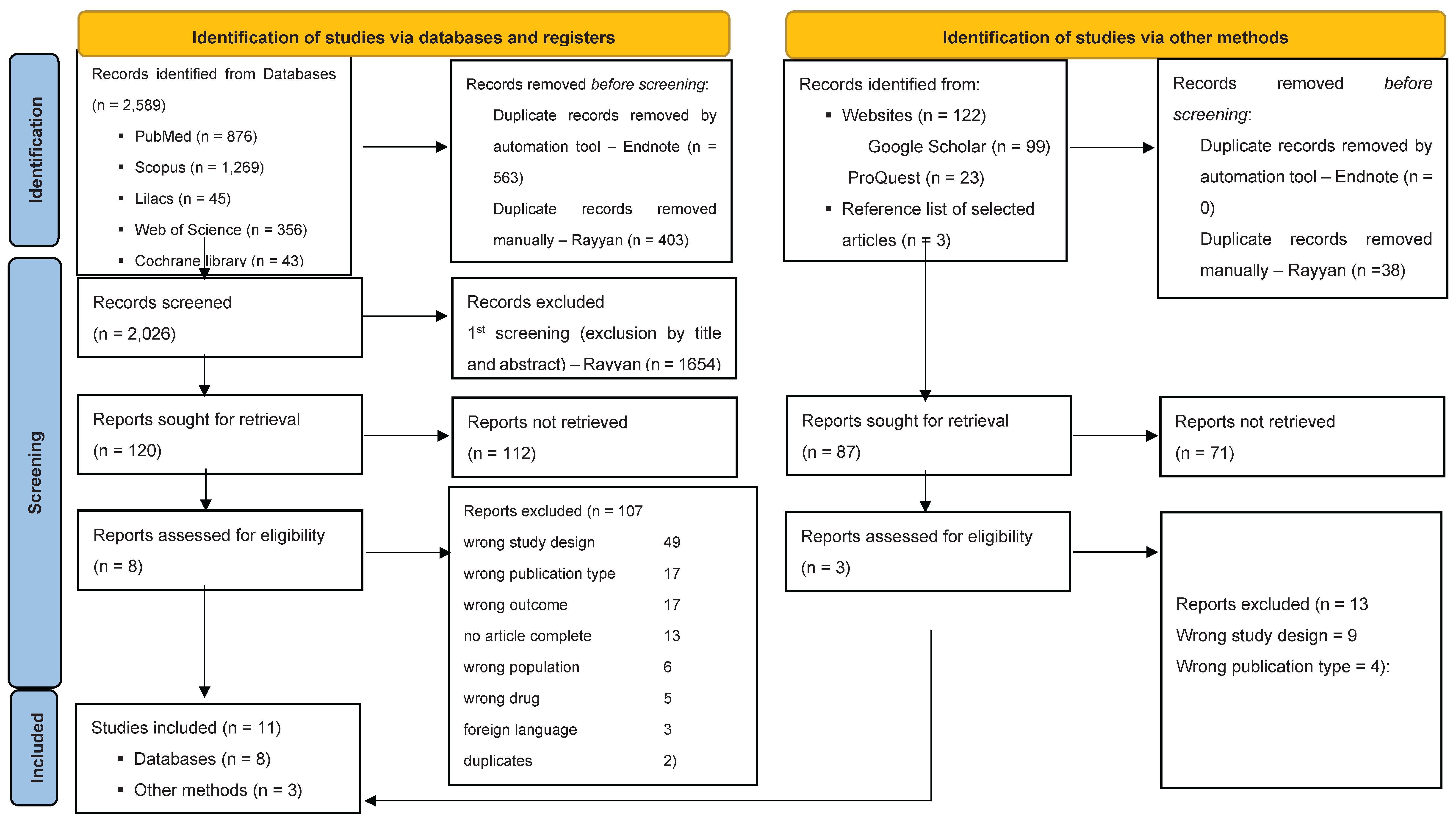

Table 1.
Standard checklist to report clinical trials and studies reporting basic oral procedures for oncological patients.
Table 1.
Standard checklist to report clinical trials and studies reporting basic oral procedures for oncological patients.
|
Trial design and identification |
- Identification as randomized clinical trial and description of the trial design. - Provide the medical center where the patients were treated. |
|---|---|
|
Ethics and registration |
- Provide Center or city ethics committee - Ensure that the trial is registered in a publicly-accessible trials register database |
|
Population |
- Describe oncological treatment patients are being submitted (such as radiotherapy, chemotherapy, stem cell transplant). - Detail the eligibility criteria and sample size. - Define the control group: placebo, different protocols or another reference treatment. - Include procedures for randomization, patients’ allocation and patient-blinding. |
|
Oral care intervention |
- Specific description of the oral care procedure, such as toothbrush used, mouth rising used and concentration, prophylaxis, dental floss type, fluor application - The moment performed said procedures, before, during or after the oncological treatment - Duration taken and technique to perform the procedures |
Table 2.
Included studies.
| Author, year | Condition | Moment of the dental intervention | Dental intervention | Main Results | Conclusion | ||
|---|---|---|---|---|---|---|---|
| Epstein, 2001 Kazemian, 2009 |
Mucositis Mucositis |
Before, during and after the oncologic treatment Before and during the oncologic treatment |
Benzydamine (to rinse 1.5 mg/mL benzydamine [15mL] for 2 minutes, 4 – 8 times daily before and during RT, and for 2 weeks after completion of RT and a Control group - placebo (excipients included approximately 10% alcohol by volume, menthol, peppermint oil, clove oil, and other flavoring agents). Benzydamine (to rinse with 15 ml of 0.15% for 2 min, 4 times a day from the first day of RT to the end of the treatment.) |
Benzydamine produced a 26.3% reduction in mean mucositis compared with placebo for the overall 0 –5000-cGy interval (P 5=0.009). Subjects receiving conventional RT with or without chemotherapy, the mean of mucositis scores showed a 30% reduction in erythema and ulceration with benzydamine over the cumulative RT interval of 0 –5000 cGy compared with placebo (P 5=0.006). Also, benzydamine produced statistically significant reductions in mucositis in the highest two RT intervals compared with placebo: 36% in the 2500 –3750-cGy interval (P=. 0.001) and 25.3% in the 3750 –5000-cGy interval (P 5 0.006). In addition, a prophylactic effect of benzydamine on oral mucositis was significant, mucositis scores in oropharyngeal areas at risk for ulceration in both treatment groups remained in the 0 –1 range (no ulceration) at cumulative RT exposures of 3750 and 5000 cGy. Smoking before and during RT (P= 0.008), chemoradiation (P = 0.002), and receiving benzydamine (P = 0.001) significantly affected the grade of mucositis at the end of the treatment. Benzydamine produced a statistically significant reduction in mucositis during RT. There was a statistically significant difference in the grade 3 mucositis in the two groups, which was 43.6% (n = 17) in the benzydamine group and 78.6% (n = 33) in the placebo group (P = 0.001). Grade 3 mucositis was 2.6 times more frequent in the placebo group (relative risk = 2.6, 95% CI = 1.38–5). Smoking cigarettes significantly reduced the incidence of mucositis grade 3 (P = 0.01; relative risk = 0.48, 95% CI = 0.29–0.81). Also, chemoradiation significantly increased the incidence of this parameter. |
The use of benzydamine 0.15% oral rinse is significant as a routine prophylactic in patients with head and neck carcinoma receiving a variety of RT regimens. Benzydamine 0.15% oral rinse was safe and well tolerated. It significantly reduced RT-induced mucositis, which also decreased the interruption of the treatment by the patients. The prophylactic usage of this local medication may decrease the mucosal complications of RT and therefore increase local tumor control. |
||
| Control group - Placebo | |||||||
|
Leenstra, 2014 Samarannayake, 1988 |
Mucositis Mucositis |
During the oncologic treatment During the oncologic treatment |
Doxepin (to rinse with a solution of doxepin 25mg, diluted to 5mL with 2.5 mL of sterile or distilled water. Control group - placebo rinse prepared in a similar manner) Both groups, the patients swished the solution in their mouth for 1minute, gargled, and expectorated. Chlorhexidine [to rinse with 15ml of 0.2% w/v aqueous chlorhexidine gluconate (Hibitane-ICI Pharmaceuticals) for 30 s twice daily] |
The mean mouth and throat pain reduction was greater for doxepin (-9.1) compared with placebo (-4.7; difference, -4.4; 95% CI, -6.7 to -2.1; P <.001). Crossover analysis of the two phases showed intrapatient changes of 4.1 for the doxepin-placebo arm and -2.8 for the placebo-doxepin arm; the treatment difference of doxepin versus placebo was -3.5. Which means an average mouth and throat pain score reduction of -2.0 (36.3%) from baseline for doxepin compared with -1.0 (18.9%) for placebo at 30 minutes after rinse (P =.0032). However, the crossover data in the second phase also confirmed that doxepin had more stinging and burning and worse taste and also caused more drowsiness (P =.0297). The yeast carriage rate was significantly higher than the coliform carriage rate in both groups (p < 0.05). The most common coliform found was Klebsiella pneumoniae. Patients using chlorhexidine presented less discomfort. The loss of weight in the control group was four times higher than the study group. The difference noted was highly significant (t=3.73; df = 22; P<0.01). |
Doxepin rinse is statistically significantly superior to a placebo in treating oral mucositis pain from head and neck radiotherapy with or without chemotherapy. However, further study is warranted to fully elucidate the use of this doxepin rinse in this setting. Patients’ acceptance of chlorhexidine Is better than benzydamine but there is a little difference between the two mouthwashes both in controlling pain and mucositis or in the oral carriage of the microorganisms studied. |
||
| Benzydamine [to rinse with 15 ml of 0.15% w/v benzydamine hydrochloride ('Difflam', Carnegie Medical] |
|||||||
|
Satheeshkumar, 2010 |
Mucositis |
During the oncologic treatment |
Triclosan mouth rinse [to rinse with M/S Colgate Palmolive India Ltd (Colgate Plax) containing triclosan 0.03% W/V] |
From grade 2-3, there was no statistical difference between the study and control groups (P>0.05). One patient (8%) in the study group and 10 patients (83%) in the control group progressed on to grade 4 mucositis. The effect of treatment in control of severity of mucositis was tested statistically by Chi square test and was found significant at a very higher level (P<0.001). With regard to reversal of mucositis from grade 3 to grade 0, the study group had taken only a mean of 23.6 days in place of 36.5 days in the control group. The Students′ test was significant at 5% level (P<0.05). When considering the time taken for shifting from liquid to semisolid, it was 14.18 days in the study group and 27.17 days in the control group (P<0.05). The time taken to resume solid food from liquid was 25.1 days in the study group and 44.67 days in the control group respectively (P<0.01). |
The calcium phosphate mouth rinse seems to have no influence on the frequency, duration and severity of oral mucositis during CRT in patients with head and neck cancer. |
||
| Control group - Sodium bicarbonate (2 g of sodium bicarbonate powder) | |||||||
|
Sio, 2019 Stockman, 2012 |
Mucositis Mucositis |
During the oncologic treatment During the oncologic treatment |
Doxepin (92 patients to rinse with randomized to doxepin mouthwash [25 mg/5 mL water]; 91 patients to diphenhydramine-lidocaine-antacid; and 92 patients to placebo). Calcium phosphate (to rinse twice with 15 ml solution for 1 min, four times a day) |
Mucositis pain during the first 4 hours decreased by 11.6 points in the doxepin mouthwash group, by 11.7 points in the diphenhydramine-lidocaine-antacid mouthwash group, and by 8.7 points in the placebo group. The between-group difference was 2.9 points (95% CI, 0.2-6.0; P = .02) for doxepin mouthwash vs. placebo and 3.0 points (95% CI, 0.1-5.9; P = .004) for diphenhydramine-lidocaine-antacid mouthwash vs. placebo. More drowsiness was reported with doxepin mouthwash vs. placebo (by 1.5 points [95% CI, 0-4.0]; P = .03), unpleasant taste (by 1.5 points [95% CI, 0-3.0]; P = .002), and stinging or burning (by 4.0 points [95% CI, 2.5-5.0]; P < .001). The mean weight loss after 6 weeks of radiation was 4.0 kg (SD 3.7) in the CP mouth rinse group and in the control group 3.5 kg (SD 3.1) (P = 0.7). Use of gastric tubes was necessary in 12 of the 25 patients in the CP mouth rinse group (55%) and in six of the 11 patients in the control group (48%) (P = 0.8). No significant difference was found for oral pain between both groups. |
The use of doxepin mouthwash or diphenhydramine-lidocaine-antacid mouthwash vs. placebo significantly reduced oral mucositis pain during the first 4 hours after administration. | ||
| Control group - salt/baking soda solution (1 tsp. of salt and 1 tsp. of baking soda in a liter of tap water) at least eight times a day to remove sticky saliva and debris. | The CP mouth rinse seems to have no influence on the frequency, duration and severity of oral mucositis during (chemo) radiation in patients with head and neck cancer. | ||||||
|
Bueno, 2013 |
Biofilm |
Prior to the oncologic treatment |
1. Oral hygiene instructions included instruction on brushing and interdental cleaning, 2. coronal scaling (using an ultrasonic instrument), and polishing, 3. a kit containing a toothbrush and toothpaste. 4. The patients were prescribed 1 % neutral fluoride solution to be used once daily; designed to prevent caries and postoperative sensitivity. The use of other mouthwashes was not allowed. |
1. Reduction in PD (probing depth) between the T0/T1 (p00.02) and T0/T2 (p00.00), 2. reduction in the frequency of PI (plaque index) and BOP (bleeding on probing) observed between the baseline assessment and 180 days after RT |
Patients undergoing RT to the head and neck region with or without CT do not show aggravations of their clinical periodontal status for up to 6 months after cancer treatment if they also receive periodontal therapy and maintenance. |
||
| During the oncologic treatment | 1. Coronal polishing, 2. Topical application of 1 % neutral fluoride gel, 3. Reinforcement of oral hygiene | ||||||
| After the oncologic treatment | 1. Coronal polishing, 2. Topical application of 1 % neutral fluoride gel, 3. Reinforcement of oral hygiene | ||||||
|
Nunez-Aguilar, 2018 |
Biofilm |
Prior to, during, and after the oncologic treatment |
1. Teaching of oral hygiene, treatment of fluoride and chlorhexidine, scaling and polishing, scaling and root planning, selective carvings, to prevent bedsores in the oral mucosa teeth with sharp edges billed, prosthetic review, fillings, dental extractions. 2. Teachings of oral hygiene, use of chlorhexidine and fluoride 3. Survey before the oncological treatment, after starting the treatment, and with 60% of the treatment complete |
20 patients (47.78%) indicated that they had not had sore gums during CRT in the experimental group against 35 (87.5%) in the control group; In the experimental group, 7 patients (17.07%) had not had bleeding gums during CRT, in the control group 35 patients had had bleeding gums; in the experimental group, 4 patients (9.75%) had ulcers during CRT, in the control group, 35 patients (87.5%). 7 patients (17.07%) in the experimental group stated that they had a toothache after CRT. In the control group, 23 patients (57.5%); 8 patients (19.51%) in the experimental group affirmed they had sore gums after CRT, in the control group 23 patients (57.5%); in the experimental group, 7 patients (17.07%), had bleeding gums after CRT, in the control group of 36 patients (87.80%). |
Implementation of prevention protocols and the improvement in oral health among these patients is necessary. |
||
|
Niewald, 2013 |
Osteoradionecrosis |
Prior to the oncologic treatment |
1. Tooth extraction (followed up by an interval of at least 7– 10 days using soft diet, valid antibiosis and prosthodontic abstention) with primary tissue closure, 2. Endodontic treatment, 3. Removal of root remainders with primary tissue closure, 4. Conserving treatment |
11 patients (12%) were found to have developed infected osteoradionecrosis during follow-up. The one-year prevalence was 5%, the two- and three-year prevalence 15% - treated by conventionally fractionated RT applying doses of 50Gy (1 pat.), 60Gy (4 pats.), 64Gy (3 pats.), and 70Gy (3 pats.), respectively. 9/64 patients (14%) having been operated on had IORN compared to only 8% in the non-surgical patients. Oral mucositis grade II WHO was found in 47 patients (54%), grades III and IV in further 5 patients (6%, n = 87). Sialadenosis (dryness of mouth) was found in 72 patients (82%; grade: 22 patients (25%), grade 2: 38 patients (43%), grade 3: 12 patients (14%); n = 88). |
This meticulous dental care resulted in an incidence of IORN of 12%, all of them had undergone conventionally fractionated radiotherapy. It was very interesting to see that in the hyperfractionated group no IORN occurred at all. |
||
| During the oncologic treatment | Fluoridation was performed according to dental advice | We only conclude that a poor dental status, conventional fractionation and local tumor progression may enhance the risk of IORN. Meticulous dental care resulted in an incidence of IORN of 12%, all of them had undergone conventionally fractionated radiotherapy. In the hyperfractionated group no IORN occurred at all. Significant prognostic factors could not be found. | |||||
| After the oncologic treatment | 1. Patients were advised not to wear their dental prostheses up to 6–12 months after RT, 2. Tooth extraction with primary tissue closure, 3. Tooth extraction with primary tissue closure and conservative treatment, 4. Conservative treatment | ||||||
|
Regezi, 1976 |
Osteonecrosis, mucositis, dysgeusia, dysphagia |
Prior to the oncologic treatment |
1. Extraction of no salvageable teeth (teeth with gross dental caries, periapical pathology, advanced periodontal disease, and teeth supported by neoplasm). 2. Dental prophylaxis 3. Restorative dental procedures as needed 4. Initiation of oral hygiene regimen a. Tooth brush instruction with soft brushes, (patients were instructed to brush q.i.d. and to follow each brushing with oral lavage and fluoride rinse) b. Oral lavage instruction (1 liter warm water with 1 teaspoon each of NaCI and NaHC03) c. Sodium fluoride rinse instruction (1 teaspoon 3yo NaF held in mouth 1 minute, then expectorated). This rinse was discontinued during acute mucositis because of mucosal irritation. |
Oral hygiene status went from fair/poor at initial examination to good/fair after radiation therapy; Patients had normal healthy periodontium (25%), gingivitis (25%), and mild to moderate periodontitis (50%). Periodontal disease did not progress at a rate greater than would expect in a non-irradiated population. Teeth decay increased 20% following irradiation. All patients had mucositis, which became evident after 2 to 4 weeks of therapy (dysgeusia, dysphagia, dysorhexia, and pain). Overgrowth of Candida albicans was demonstrated in these patients. These symptoms subsided in 3 to 4 weeks after therapy. According to initiating factors, osteoradionecrosis was more frequent in posterior mandible due periapical/periodontal factor, and in mylohyoid ridge due trauma; according to the site, 50% occurred in the floor of mouth. After radiation therapy, it was necessary to extract teeth from 10 patients. |
It can be concluded from the data presented that the complications osteoradionecrosis, dental caries, and periodontal disease associated with radiation therapy for oral cancer can be reasonably well controlled using the regimen employed in this study. |
||
| During the oncologic treatment | 1. Weekly prophylaxis with fluoridated polishing paste 2. Prescriptions for pain relievers, dietary supplements, and antifungal or antibiotic agents when needed |
||||||
| After the oncologic treatment | 1. Oral and neck examination for detection of recurrent or new neoplastic diseases 2. Dental prophylaxis 3. Restoration dental procedures as needed 4. Reinforcement of the previously instituted oral hygiene regimen |
CRT: chemoradiation therapy; RT: radiotherapy.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



