
Submitted:
05 June 2025
Posted:
05 June 2025
You are already at the latest version
Abstract
Proton pump inhibitors (PPIs) are widely prescribed medications primarily used to treat gastroesophageal reflux disease, peptic ulcer disease, and upper gastrointestinal bleeding. Despite clear therapeutic benefits in appropriate contexts, widespread overprescribing and extended use without clear indications have prompted significant concerns about associated risks. Accumulating evidence, predominantly from observational studies, suggests that long-term PPI use may lead to complications such as vitamin and mineral deficiencies, increased risks of infections, dysbiosis, renal dysfunction, bone fractures, cardiovascular disease, and certain malignancies. Recognizing these potential harms, evidence-based deprescribing strategies such as tapering, intermittent dosing, and transitions to alternative therapies, are critical to mitigate unnecessary patient exposure. Effective implementation of deprescribing requires addressing patient, provider, and institutional barriers through educational initiatives, policy support, and structured monitoring. By promoting judicious PPI prescribing and proactive stewardship practices, clinicians can significantly reduce medication-related harm and improve patient safety.
Keywords:
Proton Pump Inhibitor
; PPI
; Stewardship
; Deprescribing
; Polypharmacy
; H2RA
1. Introduction
Proton pump inhibitors (PPIs) have been one of the most commonly prescribed class of medications since their introduction in the late 1980s [1]. In 2022, omeprazole was one of the top 10 most prescribed drugs in the U.S. PPIs are indicated for treating many conditions such as gastroesophageal reflux disease (GERD), Helicobacter pylori eradication, dyspepsia, pathological hypersecretory conditions such as Zollinger-Ellison syndrome, peptic ulcer disease (PUD), and upper gastrointestinal (GI) bleeds [2]. They are also used for prevention of ulcers in high-risk patients who need chronic non-steroidal anti-inflammatory drugs (NSAIDs) or antithrombotic agents, and stress ulcer prophylaxis (SUP) in high-risk critically ill patients [2]. The use of PPIs is growing due to the increasing prevalence of hypersecretory conditions such as GERD. From 1990 to 2019, there was an increase in the total number of GERD cases globally by 77% [3]. In addition, some of these agents are available to patients over-the-counter (OTC) without a need for a prescription or proper clinical examination [4].
Generally, PPIs have been considered effective and well-tolerated; however, their use has often expanded beyond FDA-approved indications—a phenomenon known as “indication creep.” This includes prescribing PPIs for conditions lacking robust evidence of benefit, such as non-ulcer dyspepsia and stress ulcer prophylaxis in low-risk patients, as well as continuing them for durations that exceed evidence-based recommendations [5]. For example, PPIs are frequently initiated during hospitalization and inappropriately continued after discharge, often indefinitely, without a clear clinical indication [5]. Consequently, about 30-65% of hospitalized patients don’t have a documented indication for continuing PPIs, and up to 40-55% of community-dwelling patients may not have an evidence-based indication for PPI therapy [6].
Understanding the quality of evidence behind PPI prescribing practices is critical for making informed clinical decisions. The Hierarchy of Evidence Pyramid (Figure 1) provides a structured framework for evaluating the strength of research supporting clinical interventions. At the apex of the pyramid (Level 8) are Systematic Reviews and Meta-Analyses of Randomized Controlled Trials (SR-MA of RCTs), followed by Randomized Controlled Trials (RCTs) (Level 7), which are considered the gold standard for establishing causality. Levels 6 and 5 include Systematic Reviews and Meta-Analyses of mixed study designs (RCTs plus observational studies) and of observational studies alone, respectively. Observational studies (Level 4) such as cohort and case-control studies provide important real-world data but are more prone to bias. Lower down the pyramid are Descriptive studies (Level 3), Animal studies and simulations (Level 2), and expert opinions (Level 1), which offer less reliable evidence for clinical decision-making.
This hierarchy is particularly relevant when evaluating PPI therapy, as much of the evidence regarding risks—such as nutrient deficiencies, infections, and chronic diseases—derives from observational studies (Level 4) or systematic reviews of observational data (Level 5), with limited high-quality RCTs (Level 7) or SR-MAs of RCTs (Level 8) to guide practice. Therefore, while recognizing potential risks, clinicians must weigh the quality and limitations of available evidence against the established benefits of PPIs in approved indications. This understanding underscores the need for critical appraisal of the literature and careful patient selection in PPI prescribing.
Despite their widespread use and effectiveness, there are growing concerns regarding the potential short-term (2-8 weeks) and long-term (>8 weeks) risks associated with inappropriate PPI use [1]. The U.S. Food and Drug Administration (FDA) has particularly cautioned about long-term use of prescription or OTC PPIs, advising careful consideration be given to the duration and dosage of PPI use [7]. In light of these concerns, this manuscript aims to (1) assess PPI therapy effectiveness in appropriate indications, (2) examine the risks associated with their use, and (3) provide evidence-based recommendations for deprescribing strategies, thereby bridging the gap between appropriate prescribing and patient-centered care.
2. Appropriate Prescribing of PPIs
2.1. Gastroesophageal Reflux Disease
There are several appropriate indications for PPI therapy (Table 1). GERD is characterized by the troublesome symptoms and complications resulting from the reflux of stomach contents. The phenotypic manifestations of GERD encompass nonerosive reflux disease (NERD), erosive esophagitis (EE), and Barrett's esophagus (BE) [8]. PPIs function by specifically targeting the parietal cells within the stomach. Their mode of action involves inhibiting the H+/K+-adenosine triphosphatase pump, effectively suppressing the secretion of gastric acid. For the treatment of uncomplicated GERD (i.e., NERD or non-severe EE), the 2022 American College of Gastroenterology (ACG) guidelines for the diagnosis and management of GERD recommend short-term standard once-daily PPI therapy for 8 weeks [9]. Alternatively, clinicians may consider on-demand or intermittent PPI therapy instead of standard once-daily PPI treatment for these patients. Once-daily PPI treatment of NERD should be discontinued after 8 weeks if symptoms have resolved. Nevertheless, for patients who experience persistent symptoms upon discontinuing PPIs after 8 weeks, clinicians may consider on-demand therapy, where PPIs are taken solely when symptoms arise and stopped once relief is achieved instead of continuing PPIs indefinitely. PPI therapy should be reinitiated for these patients at the lowest dose that controls the symptoms. Utilizing histamine-2-receptor antagonists (H2RAs) for step-down therapy is an alternative option [9]. It is important to note, however, that a well-executed study has demonstrated the occurrence of pH control loss (known as tachyphylaxis) after one month of bedtime H2RA therapy [10].
For patients with severe EE (defined as Los Angeles Classification grade C or D on endoscopy) and BE, long-term (>8 weeks) maintenance PPI therapy (preferred over H2RA therapy) is recommended indefinitely [9]. While there are pharmacokinetic differences between various PPIs, they are considered clinically equivalent, although the dosing differs (Table 2). If patients do not respond to a once-daily PPI treatment, therapy should be optimized before doubling the dose. It is important for patients to take the PPI 30 to 60 minutes before a meal, ideally in the morning, rather than at bedtime after dinner. Splitting the standard dose, giving half before breakfast and half before dinner, may also improve effectiveness [8]. Because all PPIs are substrates of CYP2C19, genetic differences may result in various response in some patients [11]. Unlike Asian populations, genetic variations related to fast metabolism of PPIs are commonly found among North American and European populations [12]. If a clinician is considering switching PPI agents due to suboptimal response, rabeprazole or esomeprazole may be considered because they are less reliant on CYP2C19 for metabolism compared to other PPIs [9,11].
2.2. Eosinophilic Esophagitis
Eosinophilic esophagitis (EoE) is a chronic, immune-mediated disease characterized by esophageal dysfunction and significant eosinophilic infiltration of the esophageal epithelium [13]. Traditionally, PPIs have been utilized in the management of EoE, not only for their acid-suppressive properties but also due to their potential anti-inflammatory effects. PPIs may decrease the expression of eotaxin-3, a key chemokine responsible for eosinophil recruitment to the esophagus, and improve esophageal barrier function [13]. Notably, two small randomized controlled trials have administered esomeprazole 30 mg once daily for durations of 8 weeks, assessing both histologic and symptomatic responses, demonstrating a reduction in eosinophil counts and improvement in dysphagia symptoms [14,15]. The American College of Gastroenterology (ACG) suggests the use of PPIs as a treatment option for EoE, acknowledging the low quality of evidence and issuing a conditional recommendation [13]. Given the chronic nature of EoE, maintenance therapy is often necessary to prevent relapse. However, the optimal duration and dosing regimen for PPI therapy in EoE remain areas for further research. Clinicians should tailor treatment plans to individual patient responses, considering both the benefits and potential risks associated with long-term PPI use.
2.3. Peptic Ulcer Disease
PUD involves mucosal defects in the lower esophagus, gastric, or duodenal wall most commonly caused by Helicobacter pylori infection or chronic use of aspirin or NSAIDs [16,17]. The most common and severe complication of PUD is upper GI bleeding (UGIB), with other potential complications including perforation, penetration, and gastric outlet obstruction due to scarring [17]. For treatment of H. pylori infection in treatment-naïve patients, the 2024 ACG guidelines for treatment of H. pylori infection recommend optimized bismuth quadruple therapy as first-line, which includes a standard-dose PPI twice daily for 14 days [18]. Either rifabutin triple therapy, which includes a PPI for 14 days, or dual therapy with a potassium-competitive acid blocker, which acts differently than PPIs, is suggested as first-line treatment [18]. An H2RA is not recommended for patients with H. pylori infection [18]. After completion of eradication therapy, PPIs should be discontinued and patients should be reassessed at least 4 weeks after the completion of therapy. Recommendations for treatment-experienced patients with persistent H. pylori infection include regimens with either standard or double dose PPIs up to 14 days [18].
For NSAID-induced PUD, discontinuing NSAID use is a cornerstone of treatment, allowing the gastric mucosa to heal and restoring protective mechanisms. According to the 2009 ACG guidelines for prevention of NSAID-related ulcer complications, patients with a high risk of NSAID GI toxicity (e.g., history of a previously complicated ulcer or more than 2 risk factors), who require NSAID therapy, should receive alternative treatment options [19]. If anti-inflammatory treatment is deemed necessary, a COX-2 inhibitor with co-therapy using misoprostol or a PPI is recommended. However, the usefulness of misoprostol is limited by GI side effects (e.g., cramping and diarrhea) and adherence issues (e.g., four times daily dosing). Clinicians could also consider using a lower-risk NSAID such as ibuprofen [17,20]. Combining NSAIDs with a PPI significantly reduces the risk of ulcer recurrence and complications. A network meta-analysis of 82 trials including 125,053 patients reported that COX-2 inhibitors combined with PPIs were associated with the lowest risk of ulcer complications, followed by COX-2 inhibitors alone, and then by nonselective NSAIDs plus a PPI [21].
For patients at moderate risk of NSAID GI toxicity (e.g., age >65 years, high-dose NSAID therapy, previous history of uncomplicated ulcer, or concurrent use of aspirin, corticosteroids, or anticoagulants), treatment with a COX-2 inhibitor alone or in combination with a traditional nonselective NSAID plus misoprostol or a PPI can be considered. Patients at low risk of NSAID GI toxicity (e.g., no GI risk factors) can be treated with a non-selective NSAID. Duodenal ulcers tend to heal faster than gastric ulcers due to the high acidity in the stomach, which delays the healing of gastric ulcers. While most ulcers heal within 4 weeks, larger gastric ulcers (greater than 2 cm) may need up to 8 weeks of treatment [17]. Based on endoscopic findings, some patients with PUD may need to continue PPI therapy. However, most cases of PUD heal after 8 weeks of PPI therapy, making long-term PPI therapy unnecessary for most patients [22].
Patients with low or moderate GI risk who require anti-inflammatory analgesics and also need low-dose aspirin therapy for cardiovascular disease can be treated with naproxen (preferred over other NSAIDs) along with misoprostol or a PPI. Patients at high GI and high CV risk should avoid NSAIDs or COX-2 inhibitor and explore alternative therapy. Regardless of risk status, all patients initiating long-term traditional NSAID therapy should be considered for H. pylori testing. If positive, treatment should be provided. Moreover, the 2010 American College of Cardiology/American Heart Association expert consensus document on concomitant use of PPIs and thienopyridines states that PPIs are recommended to reduce GI bleeding among patients with a history of UGIB and those with multiple risk factors (e.g., advanced age; concurrent use of anticoagulants, corticosteroids, or NSAIDs; and H. pylori infection) for GI bleeding who require antiplatelet therapy [23]. Routine use of a PPI is not recommended in low-risk patients.
2.4. Uppger Gastrointestinal Bleeding
UGIB occurs when there is bleeding from the esophagus, stomach, or duodenum. For acute UGIB, the 2021 ACG guidelines for upper gastrointestinal and ulcer bleeding recommend that after achieving successful endoscopic hemostatic therapy for a bleeding ulcer, high-dose PPI therapy be administered either continuously or intermittently for a duration of three days [24]. High-dose PPI therapy is characterized by a daily dosage ≥80 mg, maintained for at least three days. A systematic review and meta-analysis (SR-MA) of 10 randomized controlled trials (RCTs) has demonstrated comparable efficacy of intermittent high-dose PPI therapy (80 mg bolus followed by 40 mg twice daily, either orally or intravenously) to continuous infusion (80 mg bolus followed by 8 mg/h infusion, intravenously) during the initial three-day period in regards to recurrent bleeding within 7 days [25]. In high-risk patients with UGIB caused by ulcers who underwent endoscopic hemostatic therapy (e.g., endoscopic features such as active bleeding, visible vessel, or adherent clot), the guidelines recommend continuing twice-daily PPI therapy from day four until 14 days following the index endoscopy. For other patients, such as those with endoscopic features like flat pigmented spots or clean bases, standard once-daily PPI therapy may be continued instead of twice-daily PPI. Depending on individual patient risk factors, such as chronic use of NSAIDs or antithrombotic agents, longer PPI therapy may be necessary beyond two weeks [16].
2.5. Stress-Related Mucosal Disease
The presence of stress-related mucosal disease (SRMD) poses a bleeding risk for critically ill patients. Individuals who develop SRMD often experience an extended ICU stay and an elevated likelihood of mortality [26]. In an attempt to prevent GI bleeding in these patients, the 2021 Surviving Sepsis Campaign (SSC) Guidelines suggest (rather than recommend) SUP for adult patients with risk factors for GI bleeding, with no preference for a specific class of acid-reducing drugs [27]. These risk factors may include: mechanical ventilation for >48 hours, traumatic brain injury, coagulopathy (platelet count <50,000/mm3 or international normalized ratio [INR] >1.5), history of GI ulceration/bleeding within the past year, and extensive burns [27]. In many cases PPIs are overlooked and continued long-term even after risk factors have resolved and patients are downgraded and/or discharged home [28]. The 2018 SUP-ICU study, which was a double-blind RCT with 3,298 patients, aimed to evaluate PPIs for SUP in critically ill patients [29]. The results showed no significant difference in 90-day mortality between the PPI and placebo groups but the incidence of clinically important GI bleeding was significantly lowered with a number needed to treat (NNT) of 59. Interestingly, subgroup analysis identified patients with more severe disease, defined as Simplified Acute Physiology Score (SAPS) II score >53, to have an increased risk of mortality in the PPI arm (RR 1.13, 95% CI 0.99-1.30; p of interaction 0.049) [30]. As a result of these findings, the SSC guidelines downgraded the “strong recommendation, low-quality of evidence” for SUP in 2016 to “weak recommendation, moderate-quality of evidence” in 2021 [27].
Additionally, one small multicenter double-blind RCT found no added benefit of PPIs for SUP in critically ill mechanically ventilated patients in the ICU who were started on early enteral nutrition within 24 hours [31]. In SUP-ICU, only about half of patients had received enteral feeding [29]. This suggests that early enteral nutrition alone may be adequate for preventing stress-related GI bleeding. Moreover, a network meta-analysis found that while PPIs were more effective at preventing clinically important GI bleeding compared to H2RAs and sucralfate, they may increase the risk of pneumonia [32]. The results of the 2020 PEPTIC study, an open-label RCT with 26,828 patients, comparing the safety and efficacy of PPIs with H2RAs for SUP in critically ill patients found no significant difference in the rates of mortality or CDI but GI bleeding was lower in the PPI group with an NNT of 200 [33]. The use of enteral nutrition and incidence of pneumonia were not reported in this study. A meta-analysis of 13 RCTs, including PEPTIC trial, compared PPIs to H2RAs for SUP in 28,559 patients and found and increased risk of mortality in those who received a PPI (RR 1.05; 95% CI 1.00-1.10; I2 0%) [34]. However, a systematic review and network-meta analysis of 74 RCTs evaluating 39,569 patients found neither PPIs nor H2RAs significantly associated with either mortality or pneumonia compared to no SUP [35]. This suggests that H2RAs may be a good alternative option to PPIs in critically ill patients.
More recently, the 2024 REVISE study, a multicenter double-blind RCT evaluated pantoprazole compared to placebo for SUP in 4,821 patients on mechanical ventilation [36]. There was a significant reduction in clinically important UGIB in the ICU at 90 days (HR 0.30; 95% CI 0.19-0.47) with a NNT of 40. Additionally, 92% of patients received enteral nutrition, suggesting that there is indeed added benefit of SUP in these patients. Moreover, there were no significant difference between the groups with respect to 90-day mortality, incidence of VAP, or C. diff infection. The results were consistent in subgroup of patients with APACHE II score ≥25. An updated SR-MA of 12 RCTs evaluating PPIs to no SUP in 9,533 patients, which included REVISE, found consistent results [37]. PPIs significantly reduced clinically important UGIB with no significant effect on pneumonia, C. diff infection, or 90-day mortality, including in more severely ill patients.
The recently published 2024 SCCM-ASHP guideline for the prevention of stress-related gastrointestinal bleeding in critically ill adults provides updated evidence-based recommendations on the appropriate use of SUP in ICU patients [38]. The guideline emphasizes that SUP should be reserved for critically ill patients with established risk factors, such as coagulopathy, shock, or chronic liver disease, rather than applied broadly to all ICU patients [39]. Importantly, the panel downgraded the recommendation strength for SUP in critically ill patients compared to previous guidelines, citing concerns regarding the balance of benefits and risks. While PPIs and H2RAs remain the first-line agents for SUP, the guideline acknowledges enteral nutrition as a protective factor against UGIB, suggesting that some patients receiving adequate enteral nutrition may not require pharmacologic prophylaxis. The guideline also specifically addresses neurocritical care patients, who may be at an increased risk of UGIB due to physiological changes leading to hypersecretion of gastric acid. The use of SUP in neurocritical care adults is conditionally recommended, though the certainty of evidence remains low. A SR-MA of 11 RCTs in neurocritical care populations showed a significant reduction in UGIB with PPIs or H2RAs compared to no prophylaxis, with no significant difference between PPIs and H2RAs [40]. There was also no significant difference in rates of nosocomial pneumonia or mortality [40]. The duration of SUP should be carefully assessed, with discontinuation strongly recommended once risk factors resolve or before ICU discharge to prevent inappropriate continuation. Additionally, low-dose regimens are favored over high-dose therapy to minimize adverse effects, and a careful review of pre-existing acid-suppressive therapy is advised to avoid unnecessary continuation of PPIs in patients who were already on therapy before ICU admission. These updates reinforce the importance of deprescribing unnecessary PPIs and applying SUP judiciously, aligning with broader PPI stewardship efforts to optimize prescribing and mitigate potential harms associated with prolonged therapy.
2.6. Dyspepsia
The definition of dyspepsia encompasses the prevailing presence of epigastric pain lasting for a minimum of one month. The patient's primary concern should be the epigastric pain, although it can coincide with other upper GI symptoms like epigastric fullness, nausea, vomiting, or heartburn. The 2017 ACG guidelines for management of dyspepsia suggest that individuals under the age of 60 who are diagnosed with dyspepsia should be offered empiric PPI therapy (standard once-daily up to 8 weeks) if they test negative for H. pylori or if they remain symptomatic after undergoing H. pylori eradication therapy [41]. For patients not responding to PPIs after 8 weeks, tricyclic antidepressants and prokinetic therapy should be offered instead of continuation or escalation of PPI therapy.
3. Risks Associated with PPI Use
3.1. Malabsorption of Vitamins and Minerals
The acidic environment of the gut plays a crucial role in the absorption of essential nutrients. Long-term PPI use may result in reduced absorption and digestion of these nutrients leading to low plasma levels of vitamin B12, iron, magnesium, and calcium. Vitamin B12 deficiency is more pronounced in the elderly, with clinical manifestations include macrocytic anemia, cutaneous hyperpigmentation, irritability, loss of smell, peripheral neuropathy, and in severe cases, cognitive impairments such as dementia-like symptoms and acute psychosis [42]. While some researchers have not found an association between long-term PPI use and vitamin B12 deficiency,[43,44]. a large population-based case-control study revealed that among 25,956 patients with vitamin B12 deficiency, 12% were prescribed a ≥2-year supply of PPIs, whereas only 7% of 184,199 patients in the control group without vitamin B12 deficiency received the same treatment, establishing a significant association between the use of a ≥2-year supply of PPIs and an increased risk of developing vitamin B12 deficiency (OR 1.65, 95% CI 1.58–1.73) [45]. The strongest association was observed in users of high-dose PPIs for prolonged periods, but the risk diminished after discontinuation. A similar but weaker association was also noted with H2RAs (OR 1.25, 95% CI 1.17-1.34). A SR-MA of 25 observational studies involving 30,922 patients further examined the relationship between PPI use and vitamin B12 deficiency, revealing slightly increased risk in PPI users compared to non-users (OR 1.42, 95% CI 1.16–1.73; I2 = 54%) [46]. However, there was considerable heterogeneity among studies, and most studies found no significant difference in serum vitamin B12 levels between PPI users and non-users. The mechanism underlying the potential impact of PPIs on vitamin B12 absorption involves the suppression of gastric acid production by inhibiting gastric parietal cells, which also produce intrinsic factor—an essential component for vitamin B12 absorption [1]. Gastric acid is necessary to release vitamin B12 from protein-bound dietary sources, and hypochlorhydria induced by PPIs may contribute to bacterial overgrowth in the gut, where bacteria compete for vitamin B12, further reducing its bioavailability. A cross-sectional study of 659 adults found that prolonged PPI therapy (≥3 years) resulted in a significant decrease in vitamin B12 levels, even when accompanied by oral cyanocobalamin supplementation [47]. Supplementation of up to 50 mcg/day slowed but did not completely prevent this decline, suggesting that higher doses may be required to maintain normal levels. These findings underscore the importance of periodic monitoring of vitamin B12 levels in patients requiring long-term PPI therapy, consideration of alternative acid suppression strategies, and the potential need for higher-dose vitamin B12 supplementation in at-risk populations. Further studies are needed to determine optimal strategies to prevent PPI-associated vitamin B12 deficiency.
Similarly, treatment with PPIs may lead to a reduction in dietary iron absorption in the duodenum, potentially increasing the risk of iron deficiency anemia (IDA). Iron deficiency can cause symptoms such as fatigue, impaired physical exertion, and sleep disturbances. Gastric acid plays a crucial role in enhancing the absorption of non-heme iron by releasing it from food particles and converting it into the more absorbable ferrous form [48,49]. A SR-MA encompassing 14 observational studies found that PPI use was associated with a significantly increased risk of IDA (RR 2.56, 95% CI 1.43–4.61) [50]. These findings align with previous research. For instance, a large case-control study found that in patients without recognized risk factors for iron deficiency, prolonged PPI use (>2 years) was associated with an increased risk of iron deficiency (OR 2.49; 95% CI, 2.35-2.64), and prolonged H2RA use was also associated with an increased but smaller risk (OR 1.58; 95% CI, 1.46-1.71) [51]. The risk of iron deficiency rose with stronger acid inhibition and declined after discontinuing the medication. Another retrospective study investigating 278 cardiovascular outpatients found that PPI use was independently associated with lower hemoglobin (Hb) levels and anemia, with anemia occurring in 51% of PPI users compared to 19% in non-users (P < 0.001) [52]. However, it is worth mentioning that among a small group of patients diagnosed with Zollinger-Ellison Syndrome, a six-year duration of PPI treatment did not show any connection with a decrease in total body iron stores or the occurrence of iron deficiency [53]. These findings suggest that PPI-induced anemia may result from both iron and vitamin B12 deficiencies, particularly in long-term users. The risk appears to be dose-dependent, highlighting the importance of using the lowest effective PPI dose to mitigate potential consequences. However, the overall reduction in iron absorption is likely small in most individuals, and clinically significant effects may primarily affect vulnerable populations, such as elderly patients, women of childbearing age, and individuals with chronic gastrointestinal blood loss or inflammatory conditions. While routine iron monitoring is not universally recommended, it may be considered for vulnerable patients. Large, controlled studies are still needed to clarify the full impact of long-term PPI therapy on iron metabolism, hemoglobin levels, and overall anemia risk.
Additionally, PPI use, especially long-term, has been associated with hypomagnesemia in approximately 20% of patients, with the underlying mechanism thought to involve inhibition of transient receptor potential melastin (TRPM) 6 and 7 cation channels, which are essential for magnesium transport in the distal small intestine, large bowel, and distal convoluted tubule of nephrons [48,54]. Unlike other drug-induced hypomagnesemia, PPI-related magnesium depletion does not appear to result from tubular magnesium wasting, and PPI-induced gut microbiome dysbiosis may further impair magnesium absorption, although more research is needed [54,55]. Hypomagnesemia is associated with an increased risk of arrhythmias, cardiovascular-related death, and all-cause mortality, reinforcing the clinical importance of recognizing and managing this complication [54,56]. A SR-MA of 16 observational studies involving 131,507 patients found that PPI use was significantly associated with hypomagnesemia (adjusted OR 1.71, 95% CI 1.33-2.19, I² = 88%), though heterogeneity was high, necessitating further studies [57]. Subgroup analyses revealed a greater likelihood of hypomagnesemia with high-dose PPI use compared to low-dose therapy (OR 2.13, 95% CI 1.26-3.59, I² = 0%), emphasizing the importance of using the lowest effective dose whenever possible. Hypomagnesemia appears to be a class effect of PPIs, typically developing after a median duration of 5.5 years, although cases have been reported as early as 14 days and as late as 13 years after initiation [55]. Fortunately, magnesium levels generally recover within four days of discontinuing PPIs, while rechallenge with PPIs leads to rapid recurrence within the same timeframe. Patients at higher risk include those taking diuretics (especially loop diuretics), as these agents increase fluid and electrolyte loss, and long-term PPI use has been shown to further disrupt magnesium and calcium homeostasis in these individuals [58,59]. While most studies do not associate H2RAs with hypomagnesemia, the literature remains mixed, and some reports suggest a potential but lower risk [55,59,60]. Given these concerns, monitoring serum magnesium levels may be warranted in patients receiving concurrent diuretics, prolonged PPI therapy (especially >1 year), high-dose PPI treatment, or those at increased risk of cardiovascular complications, such as arrhythmias or prolonged QTc interval [61]. If an alternative agent, such as an H2RA, is not an option, clinicians should remain vigilant in assessing electrolyte imbalances and potential complications. For patients who develop PPI-induced hypomagnesemia, discontinuation of PPIs should be considered whenever possible, and treatment should include magnesium supplementation alongside prebiotic inulin fiber (20 to 40 g/day, as tolerated), which may enhance magnesium absorption [62]. Given the potential for serious cardiac and neuromuscular complications, careful reassessment of acid suppression therapy and patient-specific risk factors is essential to optimize treatment decisions while minimizing harm.
Moreover, PPI use has been associated with an increased risk of bone fractures, particularly hip, spine, and any-site fractures, with the risk being dose-dependent and more pronounced at higher doses [63]. While PPI-induced hypocalcemia has been proposed as a potential mechanism, available data remain inconclusive, and the exact pathophysiology is unclear [1,64,65,66]. One hypothesis suggests that PPIs may hinder paracellular calcium transport by increasing luminal pH, similar to how they impair magnesium absorption in the intestines [1]. However, short-term acid suppression does not appear to significantly impact calcium absorption, as demonstrated in randomized studies [64,65]. A post-hoc analysis of the LOTUS and SOPRAN trials, which evaluated patients undergoing anti-reflux surgery or long-term PPI therapy (5 and 12 years, respectively), found no significant differences in calcium and vitamin D serum levels between PPI users and non-users [44]. While profound acid suppression may reduce calcium absorption over time, this effect appears minimal for water-soluble calcium salts or calcium from dairy products, and consuming calcium with a mildly acidic meal can fully counteract the malabsorption of water-insoluble calcium in achlorhydria, further questioning the role of PPI-induced calcium deficiency in fracture risk [67]. Despite this, a meta-analysis of 24 observational studies involving over 2 million patients found that short-term (defined as < 1 year) and long-term PPI use was associated with a 20% increased risk of hip fracture (RR 1.20, 95% CI 1.14–1.28, I2 = 77%), with the risk being higher in patients using higher doses, though significant heterogeneity across studies limits the strength of this conclusion [68]. Importantly, this increased fracture risk was not observed in patients using H2RAs (RR 1.03, 95% CI 0.85-1.26, I2 =84%) [68]. Similar findings have been reported for spine and any-site fractures, again with no observed risk among H2RA users, though study heterogeneity remains a limitation [69]. Additionally, patients on chronic PPI therapy have a higher prevalence of osteoporosis compared to non-users, with the risk potentially more pronounced in postmenopausal women [70,71]. Given these concerns, chronic PPI therapy should be used cautiously, particularly in elderly and postmenopausal women, to minimize the risk of bone fractures. In high-risk patients, including those with osteoporosis or a history of fractures, the use of risedronate has demonstrated promising results in maintaining bone mineral density and reducing fracture risk [72].
3.2. Cardiovascular Disease and Death
The association between PPI use and cardiovascular (CV) disease remains controversial, with conflicting evidence across observational studies and randomized trials. Several mechanisms have been proposed, including endothelial dysfunction and aging, impaired nitric oxide–mediated vasodilation, negative inotropic effects, and hypomagnesemia [73,74]. PPIs may also interfere with the antiplatelet activity of clopidogrel via competition for CYP2C19 metabolism, although this interaction has not been definitively confirmed in RCTs. While observational studies have raised concerns about potential cardiovascular harm, causality has not been established, and further research is needed.
A SR-MA of 16 RCTs involving 7,540 patients with GERD found that PPI use was associated with an increased risk of CV events (RR 1.70, 95% CI 1.13–2.56, I² = 0%), with the highest risk observed in those receiving long-term treatment (>8 weeks) (RR 2.33, 95% CI 1.33–4.08) [75]. In a longitudinal cohort study, PPI use was linked to a small but statistically significant increase in CV mortality—17 deaths per 1,000 patients more than H2RA users—with risk increasing with longer durations of PPI exposure [76]. In 2009, the FDA issued a safety warning regarding the concomitant use of PPIs and clopidogrel, advising clinicians to avoid this combination when possible, particularly with omeprazole, which inhibits CYP2C19 and may reduce the activation and effectiveness of clopidogrel.
A SR-MA of 15 RCTs evaluating clopidogrel alone versus clopidogrel plus a PPI in 50,366 patients with coronary heart disease found that patients not receiving a PPI had a significantly lower risk of several outcomes, including major adverse cardiovascular events (MACE) (RR 0.82, 95% CI 0.77–0.88), myocardial infarction recurrence (RR 0.72, 95% CI 0.57–0.90), stent thrombosis (RR 0.71, 95% CI 0.56–0.92), target vessel revascularization (RR 0.77, 95% CI 0.63–0.93), and stroke (RR 0.72, 95% CI 0.67–0.76), while rates of all-cause death, CV death, and bleeding were similar between groups [77]. However, results from the COGENT trial, an RCT evaluating patients with coronary artery disease receiving dual antiplatelet therapy (aspirin and clopidogrel) with or without prophylactic omeprazole, found no significant increase in cardiovascular events with PPI use, while demonstrating a significant reduction in upper GI bleeding. Notably, the study was terminated early due to loss of funding [78].
Other observational studies have reported increased risks of new or recurrent stroke, myocardial infarction, CV death, and MACE in PPI users, including those not on clopidogrel [79,80,81,82,83,84]. In contrast, a meta-analysis of RCTs (eight RCTs evaluating MACE in 4,124 patients and four RCTs evaluating MI in 2,356 patients) found no increased risk of MACE (RR 0.89, 95% CI 0.34–2.33, I² = 0%) or MI (RR 1.19, 95% CI 0.25–5.73, I² = 0%), consistent with the COGENT findings [84]. Furthermore, a SR-MA of 19 RCTs including 43,943 patients with coronary artery disease on antithrombotic agents found no significant difference in MACE, MI, CV death, or all-cause mortality among patients receiving PPIs [85].
A separate SR-MA similarly found that while observational studies suggested an increased risk of all-cause mortality and MI—particularly when PPIs were combined with clopidogrel—RCTs did not support this association, highlighting inconsistencies in the evidence and the need for further prospective research [86]. Some observational studies have also suggested that H2RAs may not be associated with increased risk of MI or mortality [76,87]. While some experts propose substituting H2RAs for PPIs in patients at elevated cardiovascular risk, current evidence does not clearly support avoiding PPI monotherapy solely on the basis of cardiovascular concerns. Therefore, PPIs should not be withheld from appropriate candidates due to unproven cardiovascular risk, though prescribers should remain vigilant, particularly in patients with existing CV disease or those receiving clopidogrel.
3.3. Altered Immune Function, Dysbiosis, and Antimicrobial Resistance
PPIs exert significant effects on host immune defenses, the gut microbiota, and the risk of colonization with antimicrobial-resistant organisms. At the level of the innate immune system, PPIs impair the function of macrophages and neutrophils—critical first responders to microbial invasion. A systematic review revealed that PPI exposure disrupts essential immune mechanisms, including phagocytosis, chemotaxis, cytokine production, and reactive oxygen/nitrogen species generation [88]. PPIs have cytotoxic effects on polymorphonuclear neutrophils, inducing apoptosis via caspase-dependent pathways, and impair their ability to generate bactericidal reactive oxygen species (ROS) and reactive nitrogen species (RNS) [88]. They also interfere with phagolysosomal acidification and protease activity necessary for bacterial degradation [88]. Additionally, PPIs reduce neutrophil and macrophage migration by inhibiting chemotactic signaling, such as p38 MAPK phosphorylation and intracellular calcium mobilization [88]. Beyond impairing innate immune clearance, PPIs alter Toll-like receptor (TLR) signaling and suppress transcriptional responses needed for cytokine production, including IL-1β, TNF-α, and IL-12. These effects are largely mediated through inhibition of V-ATPases, which disrupt lysosomal acidification, SNARE protein interactions, and downstream inflammatory signaling [88]. These immunosuppressive effects compromise host defense and may partially explain the increased risk of infections such as pneumonia and Clostridioides difficile in chronic PPI users, especially those who are immunocompromised or critically ill.
Beyond immune modulation, PPIs promote microbial dysbiosis along the entire gastrointestinal (GI) tract [89]. Although alpha diversity (species richness) is often preserved, chronic PPI use consistently alters beta diversity, reflecting significant shifts in microbial community composition [90]. At the phylum level, PPIs increase Firmicutes and Proteobacteria, while decreasing Bacteroidetes. At the family and genus level, beneficial commensals such as Bifidobacteriaceae, Ruminococcaceae, and Lachnospiraceae decline, whereas potentially pathogenic taxa such as Streptococcaceae, Enterococcaceae, Veillonella, and Enterobacteriaceae become more prevalent. In the oral cavity, four weeks of PPI use is associated with increased Fusobacterium and Leptotrichia in the periodontal pocket and decreased Neisseria and Veillonella in saliva, which may facilitate translocation of these taxa to the lower GI tract [91]. In the esophagus, PPI-induced dysbiosis manifests as an increased abundance of Firmicutes and decreased Bacteroidetes and Proteobacteria, possibly reversing the microbial shift seen in reflux and Barrett’s esophagus, where gram-negative genera such as Veillonella, Prevotella, Haemophilus, and Campylobacter predominate [89]. Some of these species are implicated in inflammation and carcinogenesis, such as Fusobacterium nucleatum, which has been linked to poor prognosis in esophageal cancer [92]. In the stomach, chronic acid suppression favors overgrowth of Streptococcaceae, followed by Prevotellaceae, Campylobacteraceae, and Leptotrichiaceae, contributing to increased bacterial load, reduced diversity, and a shift toward genotoxic species such as Peptostreptococcus stomatis and Parvimonas micra. These organisms may promote gastric carcinogenesis, especially in the presence of Helicobacter pylori [89]. In the small intestine, PPIs predispose patients to small intestinal bacterial overgrowth (SIBO), with increased Streptococcus, Staphylococcus, Escherichia, Klebsiella, Veillonella, and Clostridium, and possibly reduced Actinobacteria and Bifidobacteria [89]. These changes promote inflammation, bile acid deconjugation, fat malabsorption, and complications such as spontaneous bacterial peritonitis or hepatic encephalopathy in cirrhotic patients. In the colon, long-term PPI use leads to a reduction in commensal diversity, decreased Ruminococcaceae, and increased Enterobacteriaceae, Enterococcaceae, and Lactobacillaceae, alongside the emergence of oral-origin species like Fusobacterium nucleatum [89]. This colonic dysbiosis contributes to heightened risks of Clostridioides difficile infection, inflammatory bowel disease flares, and possibly colorectal cancer [89].
Importantly, emerging data highlight the association between PPI use and increased acquisition of antimicrobial-resistant organisms. A nested case-control study involving 2,239 hospitalized adults demonstrated that PPI use within 30 days was associated with a significantly increased risk of acquiring extended-spectrum β-lactamase (ESBL)- or carbapenemase-producing Enterobacterales (adjusted incidence rate ratio [aIRR] 1.48, 95% CI 1.15–1.91), with a dose-dependent trend observed in those receiving twice-daily dosing [93]. Sensitivity analyses and a prospectively matched validation cohort confirmed the findings, reinforcing the plausibility of a causal association. In addition, a SR-MA of 26 observational studies (n = 29,382) found that gastric acid suppression was associated with a 74% increased odds of intestinal colonization with multidrug-resistant organisms (MDROs), including ESBL-producing Enterobacterales and vancomycin-resistant enterococci (VRE) (OR 1.74, 95% CI 1.40–2.16, I2 = 68%), though there was significant heterogeneity [94]. These findings suggest that acid suppression impairs colonization resistance and facilitates the persistence of drug-resistant strains, possibly due to the combined effects of dysbiosis, reduced gastric acidity, and impaired host immunity. As such, PPIs may represent a modifiable risk factor in the broader context of antimicrobial resistance, especially among hospitalized or immunocompromised patients Notably, H2RAs have not been associated with this increased risk [93]. Taken together, these data underscore the multifaceted consequences of chronic PPI use on host immunity, gut microbiota, and pathogen resistance, reinforcing the importance of careful patient selection, appropriate indication, and routine reassessment of PPI therapy. Where feasible, use of the lowest effective dose or switching to H2RAs may mitigate these risks.
3.4. Enteric Infections
Several studies have demonstrated an association between PPI use and an increased risk of enteric infections, such as Clostridioides difficile infections (CDI). These infections may result from gastric acid resistance (i.e., decreased gastric acid allowing bacterial organisms to reach the intestine more easily) [95]. Although C. difficile spores are generally resistant to acidic environments, they may germinate in the presence of bile salts; however, vegetative forms are typically destroyed by low pH. PPIs may allow these forms to survive in less acidic environments, allowing colonization of the intestinal lumen [95]. Another proposed mechanism is that PPIs impair the gastric barrier, altering the gut microbiome, leading to CDI [95]. A 15-month prospective observational study evaluated 4143 hospitalized patients in six Canadian hospitals [96]. In multivariate analysis, PPI use was identified as an independent predictor of health care-associated CDI (OR 2.16, 95% CI 1.03-4.56) but not H2RAs (OR 0.55, 95% CI 0.21-1.49) [96]. The risk of CDI with PPI use appears to remain elevated up to 1 year after discontinuation of PPI [97]. Multiple SR-MAs of observational studies have found a significant association between CDI and PPI use [98,99,100,101,102,103,104,105,106]. For example, a SR-MA of 42 observational studies evaluating 313,000 patients found significant association between PPI use, compared to non-use, and increased risk of both incident (OR 1.74, 95% CI 1.47-2.85, I2 = 85%) and recurrent CDI (OR 2.51, 95% CI 1.16-5.44, I2 = 78%) [101]. Compared to PPIs, switching to H2RAs was associated with significantly lower risk of incident CDI (OR 0.71, 95% CI 0.53-0.97). Another SR-MA of 16 observational studies evaluating 7,703 patients found significant increased risk of recurrent CDI with PPI use (OR 1.66, 95% CI 1.18-2.34) but not with H2RAs (OR 1.37, 95% CI 0.95-1.99) [103]. The increased risk of recurrent CDI with PPI use was shown again in a larger SR-MA of 16 observational studies that evaluated 57,477 patients (OR 1.69, 95% CI 1.46-1.96, I2 = 56%) [106]. Lastly, a SR-MA of 50 observational studies evaluating 342,532 patients found that PPI use is associated with increased risk of hospital-acquired CDI (OR 1.29, 95% CI 1.14-1.44, I2 = 81%) but not community-associated CDI (OR 1.17, 95% CI 0.74-1.59, I2 = 75%) [105]. In regards to H2RAs, a SR-MA of 33 observational studies evaluating 201,834 patients found a significant increase in risk of CDI with H2RA use (OR 1.44, 95% CI 1.22-1.70, I2 = 71%) [107]. Unfortunately, all of these SR-MAs had significant heterogeneity, requiring further studies for definitive conclusions [98,99,100,101,102,103,104,105,106]. Importantly, a large, prospective, placebo-controlled randomized trial conducted over a three-year period found that standard-dose pantoprazole (40 mg daily) was not significantly associated with adverse events, except for a modest increase in the risk of enteric infections (OR 1.33; 95% CI, 1.01–1.75) [108]. Notable, a study evaluating 306 patients found that daily PPI use was an independent, dose-dependent risk factor for increased mortality in patients with CDI [109]. Prolonged PPI use was associated with gut dysbiosis—specifically, reduced levels of beneficial bacteria such as Ruminococcus gnavus and Prevotella copri, and increased levels of Parabacteroides merdae and C. difficile—which in turn was linked to higher mortality rates [109]. These findings suggest the need for caution when prescribing PPIs to chronically ill patients with CDI. The use of H2RAs, on the other hand, seems to have a relatively low risk of CDI when considering the totality of currently available evidence [101,110,111].
Beyond CDI, PPI use has also been linked to increased susceptibility to other enteric infections. Suppressed gastric acid impairs host defenses against organisms such as Salmonella, Campylobacter, Escherichia coli, and Shigella, facilitating their survival and growth [112]. A SR-MA of six observational studies involving 11,280 patients reported a higher risk of community-acquired enteric infections with PPI use (OR 3.33, 95% CI 1.84–6.02), as well as a smaller but significant risk with H2RAs (OR 2.03, 95% CI 1.05–3.92) [113]. A subsequent updated SR-MA of nine observational studies found similar increased risk with PPIs (OR 4.28, 95% CI 3.01-6.08, I2 = 85%), with higher strength of association for Salmonella and Campylobacter [114]. However, there was significant heterogeneity between the studies [113,114]. A more recent population-based cohort study evaluating 154,590 adult inpatients also found increased risk with both agents, but again higher with PPIs (OR 5.53, 95% CI 1.26-1.42) than with H2RAs (OR 1.34, 95% CI 1.26-1.42) [115]. Additionally, a large case-control study using a national dataset of 860,483 patients found that continuous PPI use was significantly associated with increased risk of viral gastroenteritis during peak seasonal outbreaks (adjusted OR 1.81, 95% CI 1.41–2.31), reinforcing concerns that PPIs impair mucosal immunity across a spectrum of pathogens [116]. These infections may be more severe in immunocompromised individuals or those with comorbidities. Furthermore, PPI use is a proposed risk factor for traveler’s diarrhea, possibly due to survival of enteropathogens such as toxigenic E. coli or Shigella spp [112].
Finally, PPIs may predispose patients to small intestinal bacterial overgrowth (SIBO), a condition characterized by excessive bacterial colonization in the small intestine. Hypochlorhydria induced by PPI use disrupts the normal intraluminal environment, allowing for abnormal proliferation of bacteria. A SR-MA of 11 observational studies (n=3,134) found a significant association between PPI use and SIBO when diagnosis was made using duodenal/jejunal aspirates—the gold standard (OR 7.59, 95% CI 1.81–31.89)—but not when using glucose hydrogen breath testing [117]. Similarly, a SR-MA of 19 observational studies (n=7,055) reported a pooled OR of 1.71 (95% CI 1.20–2.43, I2 = 84%) for SIBO with PPI use, with risk persisting across subgroups and testing modalities [118]. Subgroup analysis of high-quality studies also showed a significant, though more modest, association (OR 1.31, 95% CI 1.01–1.69, I2 = 28%). Symptoms of SIBO include bloating, diarrhea, and nutrient malabsorption, and its occurrence in PPI users has raised concern, especially in patients with irritable bowel syndrome (IBS) or cirrhosis. Clinicians should remain vigilant when evaluating patients with unexplained gastrointestinal symptoms or malabsorption, especially if they have a history of long-term or high-dose PPI use. Together, these findings suggest that PPI therapy—while often necessary—should be judiciously prescribed and periodically reassessed, particularly in patients with risk factors for infections or existing gut dysbiosis. H2RAs, where appropriate, may offer a safer alternative.
3.5. Peritonitis and Hepatic Encephalopathy
The association between PPI use and infectious complications extends beyond traditional enteric infections, raising particular concern in patients with cirrhosis. Individuals with cirrhosis are especially vulnerable to spontaneous bacterial peritonitis (SBP) due to a constellation of factors, including impaired gastrointestinal motility, increased intestinal permeability, immune dysfunction, and frequent use of acid-suppressive therapy. Gastric acid suppression, particularly from PPIs, may exacerbate the risk by promoting SIBO, facilitating bacterial translocation across the intestinal wall, and compromising mucosal defenses [119]. A SR-MA of eight observational studies involving 3,815 patients with cirrhosis found that PPI use was associated with a significantly increased risk of SBP (OR 3.15, 95% CI 2.09–4.74, I² = 57%), while H2RA use was not (OR 1.71, 95% CI 0.97–3.01, I² = 0%) [119]. However, this analysis was limited by its heavy reliance on data from conference abstracts and a small sample size in the H2RA group. More robust evidence comes from a SR-MA of 17 observational studies including 8,204 cirrhotic patients, which demonstrated a significant association between PPI use and SBP (OR 2.17, 95% CI 1.46–3.23, I² = 86%) [120]. Another SR-MA of 16 studies (n = 8,145) confirmed this association (OR 2.11, 95% CI 1.46–3.06, I² = 85%) but found no significant relationship between PPI use and post-SBP mortality (OR 1.54, 95% CI 0.92–2.59, I² = 49%) [121]. Interestingly, in patients undergoing peritoneal dialysis, the risk profile appears reversed. A SR-MA of six observational studies involving 829 patients found that H2RA use was associated with a significantly increased risk of peritonitis (OR 1.40, 95% CI 1.01–1.93, I² = 8%), whereas PPI use was not (OR 1.13, 95% CI 0.72–1.77, I² = 34%) [122]. One proposed explanation involves differences in drug metabolism: cytochrome P450 enzyme activity, which governs PPI metabolism, is markedly reduced in cirrhosis, potentially resulting in higher systemic PPI exposure and increased risk of adverse outcomes [122]. In contrast, H2RAs may accumulate to higher levels in patients with kidney disease, such as those on dialysis, potentially accounting for their increased infection risk in this population.
In addition to SBP, PPI use in cirrhosis has been linked to hepatic encephalopathy (HE), a serious neuropsychiatric complication. Several observational studies have reported a dose-dependent increase in the risk of HE and all-cause mortality among cirrhotic patients taking PPIs [123,124,125,126]. A SR-MA of seven observational studies evaluating 4,574 patients demonstrated a significant association between PPI use and HE (OR 1.50, 95% CI 1.25–1.75, I² = 14%) [127]. These findings may be explained by increased ammonia production and absorption secondary to SIBO and mucosal inflammation induced by dysbiosis. Although the evidence is largely observational and subject to confounding, the consistency of the signal across multiple studies and the biological plausibility of the proposed mechanisms suggest that PPIs should be used with caution in patients with advanced liver disease. Given these risks, acid-suppressive therapy in cirrhotic patients should be carefully justified, and the lowest effective dose should be used for the shortest duration necessary. H2RAs may be considered as an alternative in selected patients, particularly those without renal impairment. Further prospective studies are needed to clarify the comparative safety of PPIs versus H2RAs in patients with cirrhosis and to better delineate dose-response relationships.
3.6. Respiratory Infections
Acid-suppressive therapy, particularly with PPIs, has been associated with an increased risk of respiratory infections, including community-acquired pneumonia (CAP), hospital-acquired pneumonia (HAP), ventilator-associated pneumonia (VAP), and viral infections such as COVID-19. Several mechanisms have been proposed to explain this association, including gastric acid suppression leading to microaspiration of colonized gastric contents, alteration of the upper aerodigestive microbiome, and impairment of neutrophil function. A SR-MA of 13 observational studies including over 2 million patients revealed that PPI use significantly increased the risk of CAP compared to non-use (OR 1.37, 95% CI 1.22–1.53, I² = 88%), with the highest risk occurring within the first 30 days of use (OR 1.49, 95% CI 1.34–1.66, I² = 93%) [128]. Interestingly, the increased risk has not been observed with long-term PPI use [129]. This risk appears especially pronounced among patients with acute stroke, where PPI use was associated with higher rates of aspiration pneumonia (adjusted RR 2.37, 95% CI 1.36–4.17, I² = 0%) in a SR-MA of 5 cohort studies, whereas the association with H2RAs did not reach statistical significance (adjusted RR 1.73, 95% CI 0.74–4.25, I² = 68%) [130]. Regarding nosocomial pneumonia, a large prospective cohort study (n = 63,878) found that acid-suppressive medication use was significantly associated increased risk of HAP (adjusted OR 1.3, 95% CI 1.1-1.4), with PPIs posing the greatest risk [131]. Notably, the number needed to harm was estimated to be 111, implying potentially over 180,000 excess cases annually in the U.S. attributed to inappropriate acid suppression. Similarly, a SR-MA of 23 RCTs (n=4,168) found a significant increase in risk of HAP with H2RA use (RR 1.22, 95% CI 1.01-1.48, I² = 31%) [132]. Among mechanically ventilated patients, a randomized double-blind trial comparing pantoprazole to ranitidine found a significantly higher incidence of VAP in the pantoprazole group (30%) compared to the ranitidine group (10%) (P = 0.006) [133]. However, there was no significant difference in hospital mortality (10% vs. 5%, P = 0.245), although methodological limitations and small sample size limit the interpretation [133].
Concerns have also emerged about the impact of PPIs on COVID-19 outcomes. A SR-MA of 12 observational studies including 290,455 patients found that PPI use was not associated with increased susceptibility to COVID-19 infection (OR 1.56, 95% CI 0.48–5.05, I² = 99.7%), but it was significantly associated with worse outcomes (composite of mortality and severe COVID-19) (OR 1.85, 95% CI 1.13–3.03, I² = 90%) [134]. A separate SR-MA of 15 retrospective cohort studies involving 18,109 patients confirmed this association, reporting that PPI use significantly increased the risk of severe COVID-19 (HR 1.53, 95% CI 1.20–1.95, I² = 75%) but not incidence of COVID-19 (HR 1.26, 95% CI 0.89–1.79, I² = 85%), whereas H2RA use was not significantly associated with severe COVID-19 (HR 0.90, 95% CI 0.56–1.44, I² = 75%) but significantly decreased incidence of COVID-19 (HR 0.86, 95% CI 0.76–0.97, I² = 0%) [135]. The proposed mechanisms include impaired viral clearance, dysbiosis, and reduced neutrophil function secondary to acid suppression. Collectively, these findings support the notion that PPI use increases the risk of various respiratory infections. While the absolute risks may vary depending on patient populations, clinical context, and duration of use, clinicians should apply heightened vigilance when prescribing PPIs in patients at elevated risk for respiratory complications, such as those with recent stroke, advanced age, or active COVID-19. Alternative strategies, such as deprescribing unnecessary PPIs or switching to H2RAs when appropriate, may mitigate these risks.
3.7. Malignancy
Emerging evidence suggests that chronic PPI use may increase the risk of several malignancies, particularly those of the gastrointestinal and hepatobiliary systems. Multiple mechanisms have been proposed to explain this association, including chronic hypergastrinemia, dysbiosis, impaired nutrient absorption, N-nitrosamine formation, and pro-inflammatory signaling pathways. A large umbrella review found that PPI use was associated with an increased risk of gastric, pancreatic, colorectal, and liver cancer, a decreased risk of breast cancer, and no association with esophageal cancer [136]. Gastrin, whose levels increase with chronic acid suppression, has been shown to stimulate the proliferation of enterochromaffin-like cells and may promote tumor growth via activation of cholecystokinin-B/gastrin receptors and the MAPK/ERK1/2 pathway. Additionally, bacterial overgrowth and reduced gastric acidity promote the formation of N-nitroso compounds—known carcinogens—which may contribute to carcinogenesis in the upper GI tract.
A SR-MA of 24 observational studies involving over 8 million participants found that PPI use was significantly associated with an increased risk of gastric cancer (RR 1.82, 95% CI 1.46–2.29, I² = 95%) but not colorectal cancer (RR 1.22, 95% CI 0.95–1.55, I² = 97%) [137]. Notably, a duration-dependent trend was identified for gastric cancer risk (<1 year: RR 1.56; 1–3 years: RR 1.75; >3 years: RR 2.32), but no such trend was found for colorectal cancer [137]. The gastric cancer risk was especially elevated for non-cardiac cancers, which may be related to sustained gastric mucosal injury and chronic inflammation. Furthermore, post-Helicobacter pylori eradication, prolonged PPI use may create a gastric environment conducive to carcinogenesis through enhanced N-nitrosamine formation.
Similarly, in a SR-MA of 24 observational studies with over 2.7 million individuals, long-term PPI use has been associated with hepatocellular carcinoma (OR 1.69, 95% CI 1.30–2.20, I² = 94%), biliary tract cancers (OR 1.79, 95% CI 1.63–1.97, I² = 42%), and pancreatic cancers (OR 1.61, 95% CI 1.23–2.11, I² = 99%), with risks observed across both Asian and Western populations [138]. Mechanistically, PPI-induced changes in bile acids, dysbiosis, hypergastrinemia, and impaired vitamin B12 absorption may contribute to oncogenesis in these regions. A SR-MA of 7 observational studies (n=546,199) found that PPI use was associated with an increased risk of pancreatic cancer (RR 1.73, 95% CI 1.16–2.57, I² = 99%), though sensitivity analyses yielded mixed results and highlighted the need for better data on dose and duration [139]. While the same study suggested a possible increased risk with H2RAs (RR 1.26, 95% CI 1.02–1.57, I² = 86%), the association was weaker and not consistently significant [139].
Conversely, PPIs may exhibit antitumor effects in certain settings. For instance, intermittent high-dose PPI therapy combined with chemotherapy has shown promise in breast cancer by modifying the acidic tumor microenvironment and improving drug efficacy [136]. Preclinical studies indicate that esomeprazole can inhibit triple-negative breast cancer cell proliferation in a dose-dependent manner. However, these findings remain preliminary and warrant further investigation. Taken together, the available evidence indicates a possible association between long-term PPI use and site-specific malignancies, especially in the gastric and hepatobiliary systems. The risk appears to be influenced by the duration and intensity of acid suppression. Clinicians should exercise caution when prescribing prolonged PPI therapy, particularly in patients with additional cancer risk factors. Further well-designed prospective studies are needed to clarify causality and better delineate the risk across cancer types.
3.8. Impaired Kidney Function
The long-term use of PPIs has been increasingly associated with a spectrum of adverse renal outcomes, including acute interstitial nephritis (AIN), acute kidney injury (AKI), chronic kidney disease (CKD), and end-stage kidney disease (ESKD). PPI-induced AIN is thought to arise from an idiosyncratic, cell-mediated hypersensitivity reaction that is independent of dose or duration. The resulting interstitial inflammation may cause irreversible damage if unrecognized, and in 30–70% of biopsy-confirmed AIN cases, kidney function does not fully recover even after drug discontinuation [140]. This incomplete recovery can establish a trajectory from AIN to CKD and ESKD, even in the absence of overt AKI. In a population-based study of over 500,000 new PPI users, the incidence of AIN was 11.98 per 100,000 person-years [141]. A SR-MA of 7 observational studies involving over 2.4 million participants found that PPI use was associated with a significant increased risk of AKI (RR 1.61, 95% CI 1.16–2.22, I² = 98%) [142]. The mechanism is thought to involve inflammatory injury, possibly aggravated by PPI-induced hypomagnesemia or oxidative stress. Another SR-MA of 9 observational studies confirmed this association, with PPI use linked to an increased risk of AKI compared to both non-users (RR 1.44, 95% CI 1.08–1.91, I² = 98%) and H2RA users (RR 1.32, 95% CI 1.17–1.51, I² = 0%), suggesting that the observed association may be specific to the pharmacologic effects of PPIs rather than general to all acid-suppressing agents, though significant heterogeneity was observed among the included studies [140].
Regarding CKD, multiple meta-analyses have established a significant association with PPI therapy. A SR-MA of 12 observational studies and one RCT, incorporating over 1 million patients, showed that PPI use was linked to a significant increased risk of incident CKD compared to non-users (HR 1.26, 95% CI 1.16–1.38, I² = 87%) and compared to H2RA users (HR 1.34, 95% CI 1.13–1.59, I² = 87%) [143]. This association remained consistent across sensitivity analyses and regardless of study design or follow-up duration. The findings were further supported by an earlier SR-MA linking PPI use to a significant increased risk of CKD compared to both non-users (RR 1.36, 95% CI 1.07–1.72, I² = 99%) and H2RA users (RR 1.28, 95% CI 1.24–1.33, I² = 0%) [140]. Progression to ESRD was also reported in PPI users compared to non-users (RR 1.42, 95% CI 1.28–1.58, I² = 28%) and H2RA users (RR 1.32, 95% CI 1.28–1.37, I² not reported) [140].
Particularly vulnerable to these adverse effects are patients already living with kidney impairment, such as those on hemodialysis. A SR-MA of 12 observational studies specifically investigated the impact of PPI use in hemodialysis [144]. PPI use was linked to a higher risk of hypomagnesemia, which is already common in end-stage renal disease and is associated with cardiovascular morbidity. In addition, PPI use in this population was associated with an increased risk of bone fractures, including hip fractures. The risk of abdominal aortic calcification was also elevated, suggesting vascular toxicity as another potential consequence of long-term PPI exposure. Notably, PPI use was associated with increased all-cause mortality among hemodialysis patients, raising serious concerns about the safety of continued therapy in this high-risk population. Although H2RAs are not completely without risk, multiple studies suggest they are associated with significantly lower incidence rates of AKI, CKD, and ESKD compared to PPIs [143]. These findings highlight the need for careful consideration when initiating or continuing PPI therapy, particularly in patients with existing renal dysfunction or other risk factors for kidney disease. Where possible, prescribers should consider deprescribing unnecessary PPIs, using the lowest effective dose, or switching to H2RAs as a potentially safer alternative. Further prospective studies are needed to clarify causality and explore individualized risk mitigation strategies.
3.9. Cognitive Impairments
Long-term PPI use may contribute to cognitive impairment through several indirect mechanisms, including nutrient deficiencies such as vitamin B12, which is essential for neurological function. Vitamin B12 plays a critical role in the methionine cycle and DNA methylation, and deficiency may impair gene regulation related to neuronal survival and increase susceptibility to neurodegenerative conditions such as Alzheimer’s disease. A SR-MA of 116 studies found that vitamin B12 levels were significantly lower in patients with Alzheimer’s disease, supporting the biological plausibility of this association [145]. It is hypothesized that reduced methionine levels from B-vitamin deficiencies could result in hypomethylation and overexpression of genes involved in Alzheimer’s pathology. [145]. However, despite these mechanistic theories, the clinical association between PPI use and cognitive impairment remains unclear.
Early observational studies raised concern over a potential link between PPI use and dementia. A population-based study of 15,726 adults aged 40 years and older found a significant increased risk of dementia among PPI users (adjusted HR 1.22, 95% CI 1.05–1.42), while a prospective cohort of 73,679 individuals aged 75 years and older reported an even higher risk (HR 1.44, 95% CI 1.36–1.52) [146,147]. These findings contributed to widespread concern and further investigation. However, subsequent meta-analyses have not found this risk [148,149,150,151]. Notably, a recent SR-MA synthesized data from 16 observational studies and one RCT involving over 1.25 million participants and found no significant association between PPI use and dementia (HR 0.98, 95% CI 0.85–1.13, I² = 99%) [152]. Although significant heterogeneity existed across studies, the findings remained consistent regardless of study design or geographic location. The same meta-analysis also evaluated the association between H2RA use and dementia [152]. Although the pooled hazard ratio for H2RA users showed a non-significant trend toward increased dementia risk (HR 1.20, 95% CI 0.98–1.47, I² = 86%), the high degree of heterogeneity and lack of statistical significance precluded definitive conclusions. Prior studies had similarly shown inconsistent results for H2RAs, and recent evidence does not suggest a strong association.
In summary, while long-term PPI use may contribute to cognitive decline through intermediary mechanisms such as B12 deficiency, the current body of evidence does not support a direct association between PPI or H2RA use and increased risk of dementia or Alzheimer’s disease. In clinical practice, concerns about dementia should not preclude necessary PPI use, but should reinforce the importance of periodic medication review and avoidance of unnecessary long-term therapy.
3.10. Myopathy
Although rare, PPI-associated myopathy has been documented in the literature, ranging in severity from mild muscle aches to severe rhabdomyolysis [153]. The mechanism remains unclear but may involve direct myocyte toxicity, mitochondrial dysfunction, or altered calcium handling. A review of the literature evaluated 11 published case reports and an analysis of 292 cases from the WHO adverse event database (VigiBase) to characterize this potential association [154]. The median patient age was 56 years (range: 12 to 78), with no clear trend in dosage, time to onset, or duration of therapy. Notably, symptoms typically resolved upon discontinuation of the PPI, and in some cases, re-exposure resulted in recurrence of myopathy symptoms, strengthening the case for causality.
Although myopathy is not widely recognized as a class effect of PPIs, this small body of evidence suggests it may occur idiosyncratically in susceptible individuals. Given the lack of a consistent dose-response relationship, routine monitoring is not currently recommended. However, clinicians should be vigilant when patients on PPIs present with unexplained muscle symptoms, particularly if no alternative explanation is apparent. In such cases, discontinuing the PPI and switching to an alternative acid-suppressing therapy may be prudent. As with other rare adverse events, further pharmacovigilance and mechanistic studies are warranted to clarify the relationship between PPI use and myopathy.
3.11. Microscopic Colitis
Microscopic colitis (MC), characterized by chronic watery diarrhea with normal endoscopic findings, encompasses two main histologic subtypes: collagenous colitis and lymphocytic colitis. PPIs have been implicated in the development of MC, potentially through increased colonic permeability, disruption of epithelial barrier integrity, and alteration of the gut microbiome [155]. Several population-based case-control studies and systematic reviews have demonstrated a significant association between PPI use and MC [155,156,157,158,159]. In a Danish nationwide study of 10,652 patients with histologically confirmed MC, current PPI use was associated with a markedly increased risk of collagenous colitis (adjusted OR [aOR] 6.98, 95% CI 6.45–7.55) and lymphocytic colitis (aOR 3.95, 95% CI 3.60–4.33), with lansoprazole showing the strongest association (aOR 15.74 for collagenous colitis and aOR 6.87 for lymphocytic colitis) [157]. Risk was highest with current PPI use and declined with past use, suggesting a temporal relationship. Another nested case–control study using Dutch primary care data (n = 1.5 million) similarly found that current PPI use within the past 3 months significantly increased the risk of MC (OR 7.3, 95% CI 4.5–12.1 compared with never users) [155]. After accounting for diagnostic delay and confounding-by-indication, the risk remained significant (OR 10.6, 95% CI 1.8–64.2 compared with colonoscopy-negative controls).
A recent SR-MA of 13 observational studies involving 304,482 patients confirmed this association, showing an overall increased risk of MC with PPI use (OR 2.65, 95% CI 1.81–3.50, I² = 98%), with consistent findings across both histologic subtypes and a stronger signal in female patients [159]. In contrast, H2RAs were not consistently associated with MC (OR 2.70, 95% CI 0.32–5.08, I² = 99%), suggesting a class-specific effect [159]. These findings underscore the importance of reviewing acid-suppressive therapy in patients presenting with unexplained chronic diarrhea, particularly in older adults or those with autoimmune conditions. Discontinuation of PPIs often leads to resolution of symptoms and histologic improvement, supporting a causal relationship. A comprehensive summary of SR-MA on PPI-associated risks is presented in Table 3, highlighting key findings across various clinical outcomes.
4. Recommendations for Deprescribing PPIs
4.1. Deprescribing Strategies
Deprescribing involves the gradual withdrawal and cessation of medications to address polypharmacy and inappropriate medication use. Approaches to deprescribing PPIs encompass: 1) intermittent PPI use for a defined period to alleviate reflux-related symptoms or facilitate esophageal healing upon relapse; 2) on-demand PPI use until symptom resolution and restarting only after symptoms resurface; 3) abrupt or tapered therapy discontinuation (e.g., tapering the PPI dose by 50% every week or two, or increasing the interval between doses to every other day before discontinuation); 4) switching to an alternative therapy (e.g., transitioning from PPIs to H2RAs); 5) lowering the daily dose [2,8]. These approaches can effectively manage symptoms while minimizing overall PPI exposure. It is important to note that when PPIs are prescribed appropriately, the potential benefits typically outweigh the risks. Conversely, when PPIs are prescribed inappropriately, even minor risks become significant as there is no potential benefit. In addition, lifestyle modifications play a supportive role in the deprescribing process. Recommendations include weight loss for overweight patients, elevating the head of the bed, avoiding late meals, smoking cessation, and reducing alcohol and caffeine intake. These non-pharmacologic interventions can help maintain symptom control during and after the deprescribing process [160].
4.2. Criteria for Deprescribing
Identifying appropriate candidates for PPI deprescribing is a critical step in optimizing therapy. Evidence-based recommendations suggest deprescribing in adults who have completed at least four to eight weeks of PPI therapy for conditions such as uncomplicated GERD or non-ulcer dyspepsia, provided symptoms have resolved. [6,8,9,41]. For patients with non-erosive reflux disease (NERD) or mild erosive esophagitis (Los Angeles grades A or B), standard once-daily PPI for up to eight weeks is appropriate; after symptom resolution, options include discontinuation, transitioning to on-demand or intermittent PPI use, or using H₂RAs or antacids for symptom control.8,9 Conversely, long-term PPI therapy is generally indicated for high-risk conditions, including complicated GERD with severe erosive esophagitis (Los Angeles grades C or D) or Barrett’s esophagus, where indefinite PPI therapy is recommended [9]. Patients with a history of UGIB, active peptic ulcers, or hypersecretory conditions such as Zollinger–Ellison syndrome also typically require continued PPI therapy [16]. In contrast, long-term PPI therapy is often unnecessary for other indications such as SUP in critically ill patients, which should be limited to the duration of risk factors and discontinued when risk resolves [38]. Regular medication reviews are critical, as studies indicate that on average one in two patients on chronic PPI therapy lack a valid ongoing indication [6]. Special consideration should be given to older adults, as chronic PPI use beyond eight weeks is generally considered inappropriate in individuals aged 65 and older, unless they have a high-risk indication.
4.3. Long-Term Monitoring
After initiating PPI deprescribing, careful monitoring is essential to manage potential rebound acid hypersecretion and ensure sustained symptom control. Rebound symptoms typically emerge within two to four weeks after discontinuation and can mimic the original condition, leading patients to resume PPI therapy unnecessarily. To mitigate rebound symptoms, patients should be educated about this possibility and provided with strategies to manage them, such as the use of antacids or H₂RAs during the tapering process. Follow-up appointments should be scheduled to assess symptom recurrence and adjust the management plan as needed. Studies have shown that a significant proportion of patients remain symptom-free after PPI discontinuation when appropriate monitoring and support are in place [160].
In patients continuing PPIs long-term, it may be beneficial to monitor patients based on individual risks. For example, it may be beneficial to monitor serum vitamin B12 levels in elderly patients receiving chronic PPI therapy due to the possible risk of cognitive impairment. Otherwise, for patients who have no other risk factors for vitamin B12 deficiency, routine monitoring of serum vitamin B12 is not recommended [9]. Routine monitoring of bone mineral density, serum creatinine, or magnesium is also not recommended [67]. However, chronic PPI therapy should be prescribed with caution especially in patients already prone to osteoporosis and fractures. For patients aged 65 years and older, the American Geriatrics Society’s 2023 Beers Criteria strongly recommend avoiding PPIs for >8 weeks unless for high-risk patients (e.g., oral corticosteroids or chronic NSAID use), erosive esophagitis, Barrett’s esophagitis, pathologic hypersecretory condition, or demonstrated need for maintenance treatment (e.g., because of failure of a drug discontinuation trial or H2RA therapy) [161]. It may be prudent to monitor serum magnesium levels in patients at risk of arrhythmias [61]. Close monitoring of renal function or consultation with a nephrologist is advised when using PPIs in patients with kidney dysfunction [9]. Prescribers should be aware of the risks when prescribing PPIs, especially in patients with predisposing risk factors such as the elderly, post-menopausal women, hospitalized and immunocompromised patients, and those on concurrent antibiotic therapy.
4.4. Challenges and Barriers
Deprescribing PPIs presents several challenges at the patient, provider, and system levels. Patients may resist discontinuation due to fear of symptom recurrence or a belief that the medication is essential for their well-being. Educating patients about the potential risks of long-term PPI use and the benefits of deprescribing, along with providing a clear tapering plan, can help address these concerns [162]. Providers may face barriers such as uncertainty about the safety of deprescribing, lack of awareness of current guidelines, and time constraints during clinical encounters. Additionally, the absence of clear documentation regarding the original indication for PPI therapy can hinder decision-making. System-level challenges include fragmented care, where multiple providers may be involved in a patient's treatment, leading to a lack of coordination in deprescribing efforts. Institutional policies that do not support or prioritize medication reviews can also impede deprescribing initiatives.
4.5. Policy and Stewardship Considerations
Implementing institutional strategies can enhance the success of PPI deprescribing efforts. Clinical decision support tools integrated into electronic health records can prompt clinicians to reassess the necessity of ongoing PPI therapy, particularly in patients who have been on treatment for extended periods. Pharmacist-led interventions, including medication therapy management and comprehensive medication reviews, have been effective in identifying inappropriate PPI use and facilitating deprescribing [6]. Educational initiatives targeting healthcare providers can increase awareness of the risks associated with long-term PPI use and promote adherence to deprescribing guidelines. Policy measures, such as requiring justification for PPI prescriptions beyond a certain duration or implementing automatic stop orders for inpatient PPI therapy without a clear indication, can also support deprescribing efforts. Establishing a culture of regular medication review and deprescribing within healthcare institutions is crucial for optimizing PPI use and minimizing potential harms.
5. Conclusions
Introduced in the 1980s, PPIs are highly effective medications when prescribed appropriately for evidence-based indications such as GERD, peptic ulcer disease, and upper GI bleeding. However, widespread inappropriate use and prolonged therapy without clear clinical justification have become common, contributing to preventable patient harms. Long-term use of PPIs can impact the absorption of essential nutrients such as vitamin B12, iron, magnesium, and calcium, potentially leading to deficiencies, neurological issues, and bone fractures. PPI use has also been linked to potential cardiovascular risks, possibly due to interactions with other medications or effects like endothelial dysfunction, but findings remain inconsistent across various studies, with some showing increased cardiovascular events and others not showing significant adverse effects. PPI use is linked to a range of infections, including Clostridioides difficile and Salmonella, promotes conditions like SIBO, increases pneumonia risks, and is associated with drug-resistant bacterial colonization, while H2RAs generally present fewer infection concerns. PPI use is linked to kidney diseases such as AKI and CKD, possibly due to immune responses and long-term effects, while H2RA use appears safer. The association between PPI use and cognitive issues, including dementia and Alzheimer's, remains inconsistent and debated, with H2RA's connection also being unclear. Long-term PPI use might increase the risk of gastric and pancreatic cancers, whereas H2RA use doesn't show the same risk for gastric cancer. There's also a potential, yet rare, link between PPIs and myopathy symptoms, urging caution among clinicians.
Clinicians should regularly reassess the need for ongoing PPI therapy, considering both the individual patient's risk profile and current evidence-based guidelines. Implementing targeted deprescribing strategies—including dose tapering, intermittent or on-demand dosing, switching to safer alternatives like H₂-receptor antagonists, and emphasizing lifestyle modifications—can significantly mitigate these risks. Effective deprescribing requires overcoming patient and provider barriers through education, clear communication, and structured institutional support, including pharmacist-led initiatives and integrated clinical decision support systems. Ultimately, responsible stewardship of PPIs, supported by regular medication reviews and an evidence-informed deprescribing culture, is essential to optimizing patient outcomes and reducing the burden of medication-related harms.
Author Contributions
A.P., M.H.C.N., and A.F. contributed equally to conceptualization, methodology, investigation, resources, data curation, writing—original draft preparation, and writing—review and editing; supervision, A.F. All authors have read and agreed to the published version of the manuscript.
Funding
There is no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Malfertheiner P, Kandulski A, Venerito M. Proton-pump inhibitors: understanding the complications and risks. Nat Rev Gastroenterol Hepatol. [CrossRef]
- Boghossian TA, Rashid FJ, Thompson W, et al. Deprescribing versus continuation of chronic proton pump inhibitor use in adults. Cochrane Database Syst Rev, 2017. [CrossRef]
- Zhang D, Liu S, Li Z, Wang R. Global, regional and national burden of gastroesophageal reflux disease, 1990-2019: update from the GBD 2019 study. Ann Med. [CrossRef]
- Johnson DA, Katz PO, Armstrong D, et al. The Safety of Appropriate Use of Over-the-Counter Proton Pump Inhibitors: An Evidence-Based Review and Delphi Consensus. Drugs. [CrossRef]
- Clarke K, Adler N, Agrawal D, et al. Indications for the Use of Proton Pump Inhibitors for Stress Ulcer Prophylaxis and Peptic Ulcer Bleeding in Hospitalized Patients. Am J Med. [CrossRef]
- Farrell B, Pottie K, Thompson W, et al. Deprescribing proton pump inhibitors: Evidence-based clinical practice guideline. Can Fam Physician 2017, 63, 354–364.
- PRILOSEC (Omeprazole) [package insert]. AstraZeneca Pharmaceuticals LP, Wilmington, DE; 2012.
- Fass, R. Gastroesophageal Reflux Disease. N Engl J Med. Sep 29 2022;387(13):1207-1216. [CrossRef]
- Katz PO, Dunbar KB, Schnoll-Sussman FH, Greer KB, Yadlapati R, Spechler SJ. ACG Clinical Guideline for the Diagnosis and Management of Gastroesophageal Reflux Disease. Am J Gastroenterol, 2022. [CrossRef]
- Fackler WK, Ours TM, Vaezi MF, Richter JE. Long-term effect of H2RA therapy on nocturnal gastric acid breakthrough. Gastroenterology. [CrossRef]
- Lima JJ, Thomas CD, Barbarino J, et al. Clinical Pharmacogenetics Implementation Consortium (CPIC) Guideline for CYP2C19 and Proton Pump Inhibitor Dosing. Clin Pharmacol Ther. [CrossRef]
- Hunfeld NG, Touw DJ, Mathot RA, et al. A comparison of the acid-inhibitory effects of esomeprazole and pantoprazole in relation to pharmacokinetics and CYP2C19 polymorphism. Aliment Pharmacol Ther. [CrossRef]
- Dellon ES, Muir AB, Katzka DA, et al. ACG Clinical Guideline: Diagnosis and Management of Eosinophilic Esophagitis. Am J Gastroenterol, 2025. [CrossRef]
- Peterson KA, Thomas KL, Hilden K, Emerson LL, Wills JC, Fang JC. Comparison of esomeprazole to aerosolized, swallowed fluticasone for eosinophilic esophagitis. Dig Dis Sci. [CrossRef]
- Moawad FJ, Veerappan GR, Dias JA, Baker TP, Maydonovitch CL, Wong RK. Randomized controlled trial comparing aerosolized swallowed fluticasone to esomeprazole for esophageal eosinophilia. Am J Gastroenterol. [CrossRef]
- Laine, L. CLINICAL PRACTICE. Upper Gastrointestinal Bleeding Due to a Peptic Ulcer. N Engl J Med, 2016. [Google Scholar] [CrossRef]
- Vakil, N. Peptic Ulcer Disease: A Review. JAMA, 2024. [Google Scholar] [CrossRef]
- Chey WD, Howden CW, Moss SF, et al. ACG Clinical Guideline: Treatment of Helicobacter pylori Infection. Am J Gastroenterol, 2024. [CrossRef]
- Lanza FL, Chan FK, Quigley EM, Practice Parameters Committee of the American College of G. Guidelines for prevention of NSAID-related ulcer complications. Am J Gastroenterol. [CrossRef]
- Castellsague J, Riera-Guardia N, Calingaert B, et al. Individual NSAIDs and upper gastrointestinal complications: a systematic review and meta-analysis of observational studies (the SOS project). Drug Saf, 2012. [CrossRef]
- Yuan JQ, Tsoi KK, Yang M, et al. Systematic review with network meta-analysis: comparative effectiveness and safety of strategies for preventing NSAID-associated gastrointestinal toxicity. Aliment Pharmacol Ther. [CrossRef]
- Lanas A, Chan FKL. Peptic ulcer disease. Lancet, 2017. [CrossRef]
- Abraham NS, Hlatky MA, Antman EM, et al. ACCF/ACG/AHA 2010 expert consensus document on the concomitant use of proton pump inhibitors and thienopyridines: a focused update of the ACCF/ACG/AHA 2008 expert consensus document on reducing the gastrointestinal risks of antiplatelet therapy and NSAID use. A Report of the American College of Cardiology Foundation Task Force on Expert Consensus Documents. J Am Coll Cardiol, 2010. [CrossRef]
- Laine L, Barkun AN, Saltzman JR, Martel M, Leontiadis GI. ACG Clinical Guideline: Upper Gastrointestinal and Ulcer Bleeding. Am J Gastroenterol. [CrossRef]
- Sachar H, Vaidya K, Laine L. Intermittent vs continuous proton pump inhibitor therapy for high-risk bleeding ulcers: a systematic review and meta-analysis. JAMA internal medicine. [CrossRef]
- Bardou M, Quenot JP, Barkun A. Stress-related mucosal disease in the critically ill patient. Nat Rev Gastroenterol Hepatol. [CrossRef]
- Evans L, Rhodes A, Alhazzani W, et al. Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock 2021. Crit Care Med, 2021. [CrossRef]
- Blackett JW, Faye AS, Phipps M, Li J, Lebwohl B, Freedberg DE. Prevalence and Risk Factors for Inappropriate Continuation of Proton Pump Inhibitors After Discharge From the Intensive Care Unit. Mayo Clin Proc. [CrossRef]
- Krag M, Marker S, Perner A, et al. Pantoprazole in Patients at Risk for Gastrointestinal Bleeding in the ICU. N Engl J Med, 2018. [CrossRef]
- Marker S, Perner A, Wetterslev J, et al. Pantoprazole prophylaxis in ICU patients with high severity of disease: a post hoc analysis of the placebo-controlled SUP-ICU trial. Intensive Care Med. [CrossRef]
- El-Kersh K, Jalil B, McClave SA, et al. Enteral nutrition as stress ulcer prophylaxis in critically ill patients: A randomized controlled exploratory study. J Crit Care. [CrossRef]
- Alhazzani W, Alshamsi F, Belley-Cote E, et al. Efficacy and safety of stress ulcer prophylaxis in critically ill patients: a network meta-analysis of randomized trials. Intensive Care Med. [CrossRef]
- Australian PIft, New Zealand Intensive Care Society Clinical Trials Group AHSCCSCN, the Irish Critical Care Trials G, et al. Effect of Stress Ulcer Prophylaxis With Proton Pump Inhibitors vs Histamine-2 Receptor Blockers on In-Hospital Mortality Among ICU Patients Receiving Invasive Mechanical Ventilation: The PEPTIC Randomized Clinical Trial. JAMA, 2020. [CrossRef]
- Lee TC, Goodwin Wilson M, Lawandi A, McDonald EG. Proton Pump Inhibitors Versus Histamine-2 Receptor Antagonists Likely Increase Mortality in Critical Care: An Updated Meta-Analysis. Am J Med. [CrossRef]
- Wang Y, Ge L, Ye Z, et al. Efficacy and safety of gastrointestinal bleeding prophylaxis in critically ill patients: an updated systematic review and network meta-analysis of randomized trials. Intensive Care Med, 1987. [CrossRef]
- Cook D, Deane A, Lauzier F, et al. Stress Ulcer Prophylaxis during Invasive Mechanical Ventilation. N Engl J Med, 2024. [CrossRef]
- Wang Y, Parpia S, Ge L, et al. Proton-Pump Inhibitors to Prevent Gastrointestinal Bleeding - An Updated Meta-Analysis. NEJM Evid. [CrossRef]
- MacLaren R, Dionne JC, Granholm A, et al. Society of Critical Care Medicine and American Society of Health-System Pharmacists Guideline for the Prevention of Stress-Related Gastrointestinal Bleeding in Critically Ill Adults. Crit Care Med, 2024. [CrossRef]
- Granholm A, Zeng L, Dionne JC, et al. Predictors of gastrointestinal bleeding in adult ICU patients: a systematic review and meta-analysis. Intensive Care Med. [CrossRef]
- Daou M, Dionne JC, Teng JFT, et al. Prophylactic acid suppressants in patients with primary neurologic injury: A systematic review and meta-analysis of randomized controlled trials. J Crit Care. [CrossRef]
- Moayyedi P, Lacy BE, Andrews CN, Enns RA, Howden CW, Vakil N. ACG and CAG Clinical Guideline: Management of Dyspepsia. Am J Gastroenterol. [CrossRef]
- Langan RC, Goodbred AJ. Vitamin B12 Deficiency: Recognition and Management. Am Fam Physician 2017, 96, 384–389.
- den Elzen WP, Groeneveld Y, de Ruijter W, et al. Long-term use of proton pump inhibitors and vitamin B12 status in elderly individuals. Aliment Pharmacol Ther, 2008. [CrossRef]
- Attwood SE, Ell C, Galmiche JP, et al. Long-term safety of proton pump inhibitor therapy assessed under controlled, randomised clinical trial conditions: data from the SOPRAN and LOTUS studies. Aliment Pharmacol Ther. [CrossRef]
- Lam JR, Schneider JL, Zhao W, Corley DA. Proton pump inhibitor and histamine 2 receptor antagonist use and vitamin B12 deficiency. JAMA, 2013. [CrossRef]
- Choudhury A, Jena A, Jearth V, et al. Vitamin B12 deficiency and use of proton pump inhibitors: a systematic review and meta-analysis. Expert Rev Gastroenterol Hepatol. [CrossRef]
- Dharmarajan TS, Kanagala MR, Murakonda P, Lebelt AS, Norkus EP. Do acid-lowering agents affect vitamin B12 status in older adults? J Am Med Dir Assoc. [CrossRef]
- Elias E, Targownik LE. The Clinician's Guide to Proton Pump Inhibitor Related Adverse Events. Drugs. [CrossRef]
- Schade SG, Cohen RJ, Conrad ME. Effect of hydrochloric acid on iron absorption. N Engl J Med, 1968. [CrossRef]
- Ali, MD. Proton Pump Inhibitors' Use and Risk of Iron Deficiency Anaemia: A Systematic Review and Meta-analysis. Curr Rev Clin Exp Pharmacol. [CrossRef]
- Lam JR, Schneider JL, Quesenberry CP, Corley DA. Proton Pump Inhibitor and Histamine-2 Receptor Antagonist Use and Iron Deficiency. Gastroenterology. [CrossRef]
- Shikata T, Sasaki N, Ueda M, et al. Use of proton pump inhibitors is associated with anemia in cardiovascular outpatients. Circ J. [CrossRef]
- Stewart CA, Termanini B, Sutliff VE, et al. Iron absorption in patients with Zollinger-Ellison syndrome treated with long-term gastric acid antisecretory therapy. Aliment Pharmacol Ther. [CrossRef]
- Touyz RM, de Baaij JHF, Hoenderop JGJ. Magnesium Disorders. N Engl J Med, 2024. [CrossRef]
- Hess MW, Hoenderop JG, Bindels RJ, Drenth JP. Systematic review: hypomagnesaemia induced by proton pump inhibition. Aliment Pharmacol Ther. [CrossRef]
- El-Charabaty E, Saifan C, Abdallah M, et al. Effects of proton pump inhibitors and electrolyte disturbances on arrhythmias. Int J Gen Med. [CrossRef]
- Srinutta T, Chewcharat A, Takkavatakarn K, et al. Proton pump inhibitors and hypomagnesemia: A meta-analysis of observational studies. Medicine (Baltimore). [CrossRef]
- Danziger J, William JH, Scott DJ, et al. Proton-pump inhibitor use is associated with low serum magnesium concentrations. Kidney Int. [CrossRef]
- Zipursky J, Macdonald EM, Hollands S, et al. Proton pump inhibitors and hospitalization with hypomagnesemia: a population-based case-control study. PLoS Med. [CrossRef]
- Kieboom BC, Kiefte-de Jong JC, Eijgelsheim M, et al. Proton pump inhibitors and hypomagnesemia in the general population: a population-based cohort study. Am J Kidney Dis. [CrossRef]
- Lazzerini PE, Bertolozzi I, Finizola F, et al. Proton Pump Inhibitors and Serum Magnesium Levels in Patients With Torsades de Pointes. Front Pharmacol. [CrossRef]
- Hess MW, de Baaij JH, Broekman M, et al. Inulin significantly improves serum magnesium levels in proton pump inhibitor-induced hypomagnesaemia. Aliment Pharmacol Ther. [CrossRef]
- Yang YX, Lewis JD, Epstein S, Metz DC. Long-term proton pump inhibitor therapy and risk of hip fracture. JAMA, 2006. [CrossRef]
- Hansen KE, Jones AN, Lindstrom MJ, et al. Do proton pump inhibitors decrease calcium absorption? J Bone Miner Res. [CrossRef]
- Wright MJ, Sullivan RR, Gaffney-Stomberg E, et al. Inhibiting gastric acid production does not affect intestinal calcium absorption in young, healthy individuals: a randomized, crossover, controlled clinical trial. J Bone Miner Res. [CrossRef]
- O'Connell MB, Madden DM, Murray AM, Heaney RP, Kerzner LJ. Effects of proton pump inhibitors on calcium carbonate absorption in women: a randomized crossover trial. Am J Med. [CrossRef]
- Freedberg DE, Kim LS, Yang YX. The Risks and Benefits of Long-term Use of Proton Pump Inhibitors: Expert Review and Best Practice Advice From the American Gastroenterological Association. Gastroenterology. [CrossRef]
- Poly TN, Islam MM, Yang HC, Wu CC, Li YJ. Proton pump inhibitors and risk of hip fracture: a meta-analysis of observational studies. Osteoporos Int. [CrossRef]
- Yu EW, Bauer SR, Bain PA, Bauer DC. Proton pump inhibitors and risk of fractures: a meta-analysis of 11 international studies. Am J Med. [CrossRef]
- Liu J, Li X, Fan L, et al. Proton pump inhibitors therapy and risk of bone diseases: An update meta-analysis. Life Sci, 2019. [CrossRef]
- da Maia TF, de Camargo BG, Pereira ME, de Oliveira CS, Guiloski IC. Increased Risk of Fractures and Use of Proton Pump Inhibitors in Menopausal Women: A Systematic Review and Meta-Analysis. Int J Environ Res Public Health, 2022. [CrossRef]
- Roux C, Goldstein JL, Zhou X, Klemes A, Lindsay R. Vertebral fracture efficacy during risedronate therapy in patients using proton pump inhibitors. Osteoporos Int. [CrossRef]
- Castellana C, Pecere S, Furnari M, et al. Side effects of long-term use of proton pump inhibitors: practical considerations. Pol Arch Intern Med, 2021. [CrossRef]
- Manolis AA, Manolis TA, Melita H, Katsiki N, Manolis AS. Proton pump inhibitors and cardiovascular adverse effects: Real or surreal worries? Eur J Intern Med. [CrossRef]
- Sun S, Cui Z, Zhou M, et al. Proton pump inhibitor monotherapy and the risk of cardiovascular events in patients with gastro-esophageal reflux disease: a meta-analysis. Neurogastroenterol Motil. [CrossRef]
- Xie Y, Bowe B, Yan Y, Xian H, Li T, Al-Aly Z. Estimates of all cause mortality and cause specific mortality associated with proton pump inhibitors among US veterans: cohort study. BMJ. [CrossRef]
- Pang J, Wu Q, Zhang Z, et al. Efficacy and safety of clopidogrel only vs. clopidogrel added proton pump inhibitors in the treatment of patients with coronary heart disease after percutaneous coronary intervention: A systematic review and meta-analysis. Int J Cardiol Heart Vasc. [CrossRef]
- Bhatt DL, Cryer BL, Contant CF, et al. Clopidogrel with or without omeprazole in coronary artery disease. N Engl J Med, 2010. [CrossRef]
- Charlot M, Ahlehoff O, Norgaard ML, et al. Proton-pump inhibitors are associated with increased cardiovascular risk independent of clopidogrel use: a nationwide cohort study. Ann Intern Med, 2010. [CrossRef]
- Li S, Liu F, Chen C, et al. Real-World Relationship Between Proton Pump Inhibitors and Cerebro-Cardiovascular Outcomes Independent of Clopidogrel. Int Heart J, 2019. [CrossRef]
- Goodman SG, Clare R, Pieper KS, et al. Association of proton pump inhibitor use on cardiovascular outcomes with clopidogrel and ticagrelor: insights from the platelet inhibition and patient outcomes trial. Circulation, 2012. [CrossRef]
- Wang YF, Chen YT, Luo JC, Chen TJ, Wu JC, Wang SJ. Proton-Pump Inhibitor Use and the Risk of First-Time Ischemic Stroke in the General Population: A Nationwide Population-Based Study. Am J Gastroenterol. [CrossRef]
- Shah NH, LePendu P, Bauer-Mehren A, et al. Proton Pump Inhibitor Usage and the Risk of Myocardial Infarction in the General Population. PLoS One. [CrossRef]
- Batchelor R, Kumar R, Gilmartin-Thomas JFM, Hopper I, Kemp W, Liew D. Systematic review with meta-analysis: risk of adverse cardiovascular events with proton pump inhibitors independent of clopidogrel. Aliment Pharmacol Ther. [CrossRef]
- Shang YS, Zhong PY, Ma Y, Bai N, Niu Y, Wang ZL. Efficacy and Safety of Proton Pump Inhibitors in Patients With Coronary Artery Diseases Receiving Oral Antiplatelet Agents and/or Anticoagulants: A Systematic Review and Meta-Analysis. J Cardiovasc Pharmacol, 2022. [CrossRef]
- Farhat N, Fortin Y, Haddad N, et al. Systematic review and meta-analysis of adverse cardiovascular events associated with proton pump inhibitors used alone or in combination with antiplatelet agents. Crit Rev Toxicol. [CrossRef]
- Shih CJ, Chen YT, Ou SM, Li SY, Chen TJ, Wang SJ. Proton pump inhibitor use represents an independent risk factor for myocardial infarction. Int J Cardiol, 2014. [CrossRef]
- Fowler JF, Eubank TA, Garey KW. Proton pump inhibitor effect on macrophage and neutrophil function: a systematic review. Front Immunol. [CrossRef]
- Bruno G, Zaccari P, Rocco G, et al. Proton pump inhibitors and dysbiosis: Current knowledge and aspects to be clarified. World J Gastroenterol, 2019. [CrossRef]
- Clooney AG, Bernstein CN, Leslie WD, et al. A comparison of the gut microbiome between long-term users and non-users of proton pump inhibitors. Aliment Pharmacol Ther. [CrossRef]
- Mishiro T, Oka K, Kuroki Y, et al. Oral microbiome alterations of healthy volunteers with proton pump inhibitor. J Gastroenterol Hepatol. [CrossRef]
- Yamamura K, Baba Y, Nakagawa S, et al. Human Microbiome Fusobacterium Nucleatum in Esophageal Cancer Tissue Is Associated with Prognosis. Clin Cancer Res, 2016. [CrossRef]
- Willems RPJ, Schut MC, Kaiser AM, et al. Association of Proton Pump Inhibitor Use With Risk of Acquiring Drug-Resistant Enterobacterales. JAMA Netw Open, 2023. [CrossRef]
- Willems RPJ, van Dijk K, Ket JCF, Vandenbroucke-Grauls C. Evaluation of the Association Between Gastric Acid Suppression and Risk of Intestinal Colonization With Multidrug-Resistant Microorganisms: A Systematic Review and Meta-analysis. JAMA internal medicine, 2020. [CrossRef]
- Jump RL, Pultz MJ, Donskey CJ. Vegetative Clostridium difficile survives in room air on moist surfaces and in gastric contents with reduced acidity: a potential mechanism to explain the association between proton pump inhibitors and C. difficile-associated diarrhea? Antimicrob Agents Chemother. [CrossRef]
- Loo VG, Bourgault AM, Poirier L, et al. Host and pathogen factors for Clostridium difficile infection and colonization. N Engl J Med, 2011. [CrossRef]
- Inghammar M, Svanstrom H, Voldstedlund M, et al. Proton-Pump Inhibitor Use and the Risk of Community-Associated Clostridium difficile Infection. Clin Infect Dis, 2021. [CrossRef]
- Tleyjeh IM, Bin Abdulhak AA, Riaz M, et al. Association between proton pump inhibitor therapy and clostridium difficile infection: a contemporary systematic review and meta-analysis. PLoS One. [CrossRef]
- Janarthanan S, Ditah I, Adler DG, Ehrinpreis MN. Clostridium difficile-associated diarrhea and proton pump inhibitor therapy: a meta-analysis. Am J Gastroenterol. [CrossRef]
- Deshpande A, Pant C, Pasupuleti V, et al. Association between proton pump inhibitor therapy and Clostridium difficile infection in a meta-analysis. Clin Gastroenterol Hepatol. [CrossRef]
- Kwok CS, Arthur AK, Anibueze CI, Singh S, Cavallazzi R, Loke YK. Risk of Clostridium difficile infection with acid suppressing drugs and antibiotics: meta-analysis. Am J Gastroenterol. [CrossRef]
- Arriola V, Tischendorf J, Musuuza J, Barker A, Rozelle JW, Safdar N. Assessing the Risk of Hospital-Acquired Clostridium Difficile Infection With Proton Pump Inhibitor Use: A Meta-Analysis. Infect Control Hosp Epidemiol. [CrossRef]
- Tariq R, Singh S, Gupta A, Pardi DS, Khanna S. Association of Gastric Acid Suppression With Recurrent Clostridium difficile Infection: A Systematic Review and Meta-analysis. JAMA internal medicine, 2017. [CrossRef]
- Trifan A, Stanciu C, Girleanu I, et al. Proton pump inhibitors therapy and risk of Clostridium difficile infection: Systematic review and meta-analysis. World J Gastroenterol, 2017. [CrossRef]
- Cao F, Chen CX, Wang M, et al. Updated meta-analysis of controlled observational studies: proton-pump inhibitors and risk of Clostridium difficile infection. J Hosp Infect. [CrossRef]
- D'Silva KM, Mehta R, Mitchell M, et al. Proton pump inhibitor use and risk for recurrent Clostridioides difficile infection: a systematic review and meta-analysis. Clin Microbiol Infect, 2021. [CrossRef]
- Tleyjeh IM, Abdulhak AB, Riaz M, et al. The association between histamine 2 receptor antagonist use and Clostridium difficile infection: a systematic review and meta-analysis. PLoS One. [CrossRef]
- Moayyedi P, Eikelboom JW, Bosch J, et al. Safety of Proton Pump Inhibitors Based on a Large, Multi-Year, Randomized Trial of Patients Receiving Rivaroxaban or Aspirin. Gastroenterology. [CrossRef]
- Lin CY, Cheng HT, Kuo CJ, et al. Proton Pump Inhibitor-Induced Gut Dysbiosis Increases Mortality Rates for Patients with Clostridioides difficile Infection. Microbiol Spectr, 2022. [CrossRef]
- Barletta JF, Sclar DA. Proton pump inhibitors increase the risk for hospital-acquired Clostridium difficile infection in critically ill patients. Crit Care, 2014. [CrossRef]
- Seo SI, You SC, Park CH, et al. Comparative risk of Clostridium difficile infection between proton pump inhibitors and histamine-2 receptor antagonists: A 15-year hospital cohort study using a common data model. J Gastroenterol Hepatol. [CrossRef]
- Bavishi C, Dupont HL. Systematic review: the use of proton pump inhibitors and increased susceptibility to enteric infection. Aliment Pharmacol Ther. [CrossRef]
- Leonard J, Marshall JK, Moayyedi P. Systematic review of the risk of enteric infection in patients taking acid suppression. Am J Gastroenterol. [CrossRef]
- Hafiz RA, Wong C, Paynter S, David M, Peeters G. The Risk of Community-Acquired Enteric Infection in Proton Pump Inhibitor Therapy: Systematic Review and Meta-analysis. Ann Pharmacother. [CrossRef]
- Kuo CJ, Lin CY, Chen CW, et al. Risk of Enteric Infection in Patients with Gastric Acid Supressive Drugs: A Population-Based Case-Control Study. J Pers Med, 2021. [CrossRef]
- Vilcu AM, Sabatte L, Blanchon T, et al. Association Between Acute Gastroenteritis and Continuous Use of Proton Pump Inhibitors During Winter Periods of Highest Circulation of Enteric Viruses. JAMA Netw Open, 2019. [CrossRef]
- Lo WK, Chan WW. Proton pump inhibitor use and the risk of small intestinal bacterial overgrowth: a meta-analysis. Clin Gastroenterol Hepatol. [CrossRef]
- Su T, Lai S, Lee A, He X, Chen S. Meta-analysis: proton pump inhibitors moderately increase the risk of small intestinal bacterial overgrowth. J Gastroenterol. [CrossRef]
- Deshpande A, Pasupuleti V, Thota P, et al. Acid-suppressive therapy is associated with spontaneous bacterial peritonitis in cirrhotic patients: a meta-analysis. J Gastroenterol Hepatol. [CrossRef]
- Xu HB, Wang HD, Li CH, et al. Proton pump inhibitor use and risk of spontaneous bacterial peritonitis in cirrhotic patients: a systematic review and meta-analysis. Genet Mol Res, 2015. [CrossRef]
- Yu T, Tang Y, Jiang L, Zheng Y, Xiong W, Lin L. Proton pump inhibitor therapy and its association with spontaneous bacterial peritonitis incidence and mortality: A meta-analysis. Dig Liver Dis. [CrossRef]
- Zhong HJ, Lin D, Lu ZY, Yang WY, Chen Y. Use of gastric-acid suppressants may be a risk factor for enteric peritonitis in patients undergoing peritoneal dialysis: A meta-analysis. J Clin Pharm Ther. [CrossRef]
- Dam G, Vilstrup H, Watson H, Jepsen P. Proton pump inhibitors as a risk factor for hepatic encephalopathy and spontaneous bacterial peritonitis in patients with cirrhosis with ascites. Hepatology. [CrossRef]
- Nardelli S, Gioia S, Ridola L, Farcomeni A, Merli M, Riggio O. Proton Pump Inhibitors Are Associated With Minimal and Overt Hepatic Encephalopathy and Increased Mortality in Patients With Cirrhosis. Hepatology. [CrossRef]
- De Roza MA, Kai L, Kam JW, et al. Proton pump inhibitor use increases mortality and hepatic decompensation in liver cirrhosis. World J Gastroenterol, 2019. [CrossRef]
- Tsai CF, Chen MH, Wang YP, et al. Proton Pump Inhibitors Increase Risk for Hepatic Encephalopathy in Patients With Cirrhosis in A Population Study. Gastroenterology. [CrossRef]
- Ma YJ, Cao ZX, Li Y, Feng SY. Proton pump inhibitor use increases hepatic encephalopathy risk: A systematic review and meta-analysis. World J Gastroenterol, 2019. [CrossRef]
- Xun X, Yin Q, Fu Y, He X, Dong Z. Proton Pump Inhibitors and the Risk of Community-Acquired Pneumonia: An Updated Meta-analysis. Ann Pharmacother. [CrossRef]
- Lambert AA, Lam JO, Paik JJ, Ugarte-Gil C, Drummond MB, Crowell TA. Risk of community-acquired pneumonia with outpatient proton-pump inhibitor therapy: a systematic review and meta-analysis. PLoS One. [CrossRef]
- Marchina S, Doros G, Modak J, Helenius J, Aycock DM, Kumar S. Acid-suppressive medications and risk of pneumonia in acute stroke patients: A systematic review and meta-analysis. J Neurol Sci. [CrossRef]
- Herzig SJ, Howell MD, Ngo LH, Marcantonio ER. Acid-suppressive medication use and the risk for hospital-acquired pneumonia. JAMA. [CrossRef]
- Eom CS, Jeon CY, Lim JW, Cho EG, Park SM, Lee KS. Use of acid-suppressive drugs and risk of pneumonia: a systematic review and meta-analysis. CMAJ, 2011. [CrossRef]
- Bashar FR, Manuchehrian N, Mahmoudabadi M, Hajiesmaeili MR, Torabian S. Effects of ranitidine and pantoprazole on ventilator-associated pneumonia: a randomized double-blind clinical trial. Tanaffos 2013, 12, 16–21.
- Pranata R, Huang I, Lawrensia S, et al. Proton pump inhibitor on susceptibility to COVID-19 and its severity: a systematic review and meta-analysis. Pharmacol Rep. [CrossRef]
- Kim HB, Kim JH, Wolf BJ. Acid suppressant use in association with incidence and severe outcomes of COVID-19: a systematic review and meta-analysis. Eur J Clin Pharmacol. [CrossRef]
- Zhang ML, Fan YX, Meng R, et al. Proton Pump Inhibitors and Cancer Risk: An Umbrella Review and Meta-analysis of Observational Studies. Am J Clin Oncol, 2022. [CrossRef]
- Guo H, Zhang R, Zhang P, et al. Association of proton pump inhibitors with gastric and colorectal cancer risk: A systematic review and meta-analysis. Front Pharmacol. [CrossRef]
- Zhou W, Chen X, Fan Q, Yu H, Jiang W. Using proton pump inhibitors increases the risk of hepato-biliary-pancreatic cancer. A systematic review and meta-analysis. Front Pharmacol. [CrossRef]
- Laoveeravat P, Thavaraputta S, Vutthikraivit W, et al. Proton pump inhibitors and histamine-2 receptor antagonists on the risk of pancreatic cancer: a systematic review and meta-analysis. QJM, 2020. [CrossRef]
- Nochaiwong S, Ruengorn C, Awiphan R, et al. The association between proton pump inhibitor use and the risk of adverse kidney outcomes: a systematic review and meta-analysis. Nephrol Dial Transplant, 2018. [CrossRef]
- Blank ML, Parkin L, Paul C, Herbison P. A nationwide nested case-control study indicates an increased risk of acute interstitial nephritis with proton pump inhibitor use. Kidney Int. [CrossRef]
- Yang Y, George KC, Shang WF, Zeng R, Ge SW, Xu G. Proton-pump inhibitors use, and risk of acute kidney injury: a meta-analysis of observational studies. Drug Des Devel Ther. [CrossRef]
- Ang SP, Chia JE, Valladares C, Patel S, Gewirtz D, Iglesias J. Association between Proton Pump Inhibitor Use and Risk of Incident Chronic Kidney Disease: Systematic Review and Meta-Analysis. Biomedicines, 2024. [CrossRef]
- Zhang Y, Deng D, Zhang R, Yi J, Dong J, Sha L. Relationship between Proton Pump Inhibitors and Adverse Effects in Hemodialysis Patients: A Systematic Review and Meta-Analysis. Kidney Blood Press Res. [CrossRef]
- de Wilde MC, Vellas B, Girault E, Yavuz AC, Sijben JW. Lower brain and blood nutrient status in Alzheimer's disease: Results from meta-analyses. Alzheimers Dement (N Y). [CrossRef]
- Tai SY, Chien CY, Wu DC, et al. Risk of dementia from proton pump inhibitor use in Asian population: A nationwide cohort study in Taiwan. PLoS One. [CrossRef]
- Gomm W, von Holt K, Thome F, et al. Association of Proton Pump Inhibitors With Risk of Dementia: A Pharmacoepidemiological Claims Data Analysis. JAMA Neurol. [CrossRef]
- Song YQ, Li Y, Zhang SL, Gao J, Feng SY. Proton pump inhibitor use does not increase dementia and Alzheimer's disease risk: An updated meta-analysis of published studies involving 642305 patients. PLoS One. [CrossRef]
- Li M, Luo Z, Yu S, Tang Z. Proton pump inhibitor use and risk of dementia: Systematic review and meta-analysis. Medicine (Baltimore). [CrossRef]
- Desai M, Nutalapati V, Srinivasan S, et al. Proton pump inhibitors do not increase the risk of dementia: a systematic review and meta-analysis of prospective studies. Dis Esophagus, 2020. [CrossRef]
- Khan MA, Yuan Y, Iqbal U, et al. No Association Linking Short-Term Proton Pump Inhibitor Use to Dementia: Systematic Review and Meta-analysis of Observational Studies. Am J Gastroenterol. [CrossRef]
- Wang H, Tian L, Yan X. No association between acid suppressant use and risk of dementia: an updated meta-analysis. Eur J Clin Pharmacol. [CrossRef]
- Clark DW, Strandell J. Myopathy including polymyositis: a likely class adverse effect of proton pump inhibitors? Eur J Clin Pharmacol. [CrossRef]
- Colmenares EW, Pappas AL. Proton Pump Inhibitors: Risk for Myopathy? Ann Pharmacother. [CrossRef]
- Masclee GM, Coloma PM, Kuipers EJ, Sturkenboom MC. Increased risk of microscopic colitis with use of proton pump inhibitors and non-steroidal anti-inflammatory drugs. Am J Gastroenterol. [CrossRef]
- Capurso G, Marignani M, Attilia F, et al. Lansoprazole-induced microscopic colitis: an increasing problem? Results of a prospecive case-series and systematic review of the literature. Dig Liver Dis. [CrossRef]
- Bonderup OK, Nielsen GL, Dall M, Pottegard A, Hallas J. Significant association between the use of different proton pump inhibitors and microscopic colitis: a nationwide Danish case-control study. Aliment Pharmacol Ther. [CrossRef]
- Zhang SW, Xu RH, Chen D. Drug Exposure and Risk of Microscopic Colitis: A Systematic Review and Meta-Analysis. Dig Dis. [CrossRef]
- Tarar ZI, Farooq U, Gandhi M, et al. Are Drugs Associated with Microscopic Colitis? A Systematic Review and Meta-Analysis. Diseases, 2022. [CrossRef]
- Lee TC, McDonald EG. Deprescribing Proton Pump Inhibitors: Overcoming Resistance. JAMA internal medicine, 2020. [CrossRef]
- By the American Geriatrics Society Beers Criteria Update Expert P. American Geriatrics Society 2023 updated AGS Beers Criteria(R) for potentially inappropriate medication use in older adults. J Am Geriatr Soc. [CrossRef]
- Jones KF, Stolzmann K, Wormwood J, et al. Patient-Directed Education to Promote Deprescribing: A Nonrandomized Clinical Trial. JAMA internal medicine, 2024. [CrossRef]
Figure 1.
Hierarchy of Evidence Pyramid.
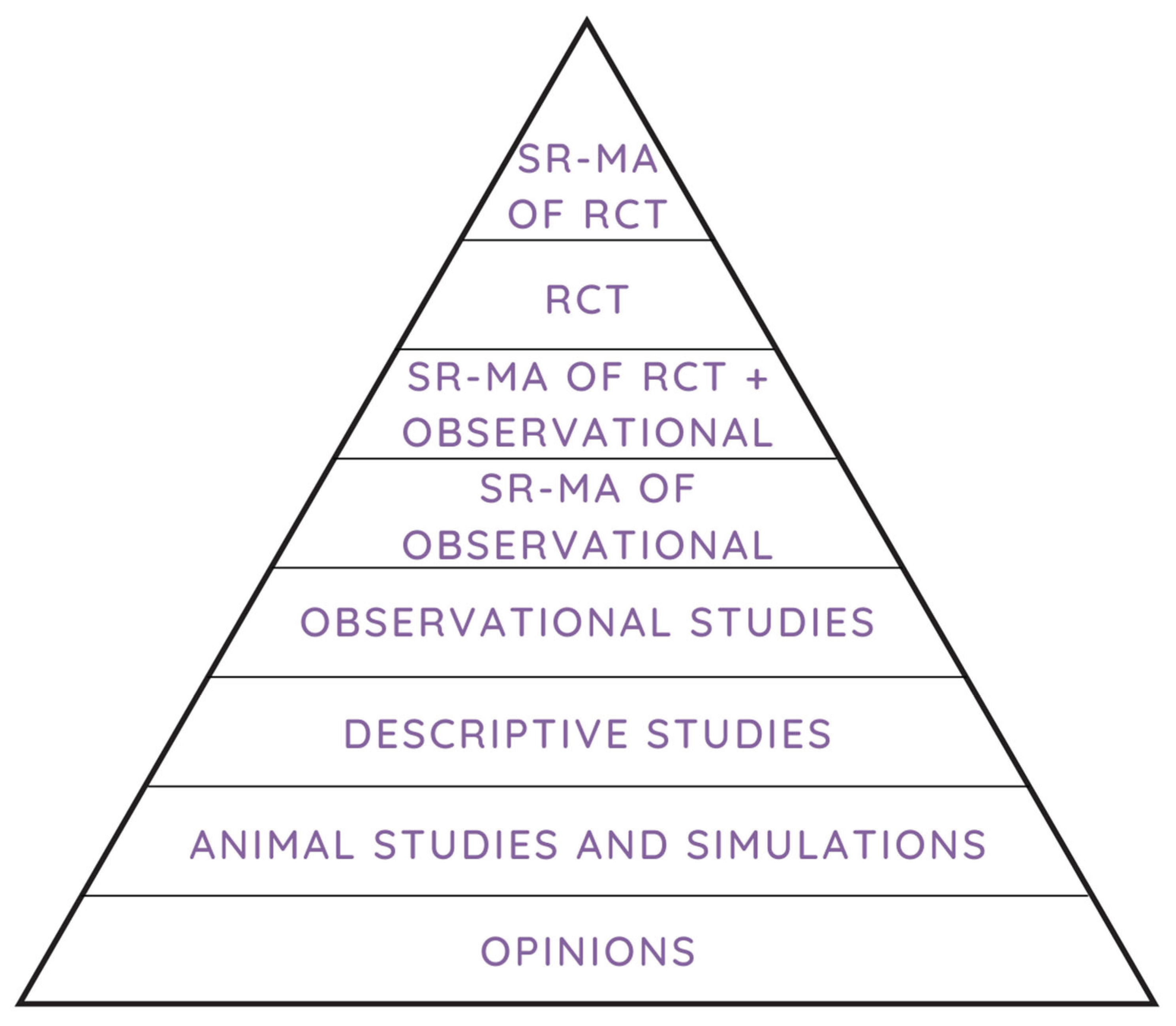

Table 1.
Summary of Recommendations for Appropriate PPI Use.
| Common Indications for PPI use | Recommendations |
|---|---|
| Uncomplicated GERD (NERD or non-severe EE) |
|
| Complicated GERD (Severe EE or BE) |
|
| Eosinophilic Esophagitis |
|
| PUD |
|
| Chronic NSAID or antithrombotic use (primary prevention) |
|
| Upper GI Bleed |
|
| SUP in critically ill patients |
|
| Dyspepsia |
|
1 Caution: tachyphylaxis with long term use. 2 Risk factors: coagulopathy, mechanical ventilation > 48 hours, TBI, history of GI ulceration or bleeding within the past year, extensive burns. 3 high dose NSAID use, age >65 years, history of previously complicated or uncomplicated ulcer, dual-antiplatelet therapy on concurrent anticoagulant therapy, corticosteroid use, H. pylori. LIS, lung injury score; MODS, multiple organ dysfunction syndrome.
Table 2.
Characteristics of Proton Pump Inhibitors.
| PPI | Standard Dose | Low Dose | High Dose | Metabolism |
|---|---|---|---|---|
| Dexlansoprazole (Dexilant), Capsule | 30-60 mg once daily | 30 mg once daily | 60 mg twice daily | CYP2C19, CYP3A4 |
| Esomeprazole (Nexium), IV, Capsule, EC Tablet, Available OTC | 20-40 mg once daily | 20 mg once daily | 40 mg twice daily | CYP2C19, CYP3A4 |
| Lansoprazole (Prevacid), Capsule, Tablet,Available OTC | 30 mg once daily | 15 mg once daily | 30 mg twice daily | CYP2C19, CYP3A4 |
| Omeprazole (Prilosec), Capsule, Tablet,Available OTC | 20 mg once daily | 10 mg once daily | 20 mg twice daily | CYP2C19, CYP3A4 |
| Pantoprazole (Protonix), IV, Tablet, Suspension | 40 mg once daily | 20 mg once daily | 40 mg twice daily | CYP2C19, CYP3A4 |
| Rabeprazole (Aciphex), Tablet, Sprinkle Capsule | 20 mg once daily | 10 mg once daily | 20 mg twice daily | CYP3A4, CYP2C19 |
Table 3.
Summary of Systematic Reviews and Meta-Analyses on PPI-Associated Risks.
| Condition | SR-MA Details | Effect Estimate (Ratio [95% CI]) |
Heterogeneity (I2) | Ref |
|---|---|---|---|---|
| Vitamin B12 Deficiency | 25 observational studies, n=30,922 | ↑OR 1.42 (1.16-1.73) | 54% | [46]. |
| Iron Deficiency Anemia | 14 observational studies, n=? | ↑RR 2.56 (1.43-4.61) | ? | [50]. |
| Hypomagnesemia | 16 observational studies, n=131,507 | ↑OR 1.71 (1.33-2.19) | 88% | [57]. |
| Fracture Risk | 24 observational studies, n=2,103,800 | ↑RR 1.20 (1.14-1.28) | 77% | [68]. |
| Cardiovascular Events in General (GERD Patients) | 16 RCTs, n=7,540 | ↑RR 1.70 (1.13-2.56) | 0% | [75]. |
| Cardiovascular Evens in Clopidogrel Users | 15 RCTs, n=50,366 | ↑RR 1.22 (1.14-1.30) | Not Reported | [77]. |
| Stroke in Clopidogrel Users | 15 RCTs, n=50,366 | ↑RR 1.39 (1.32-1.49) | Not Reported | [77]. |
| Cardiovascular Events in Patients with CAD | 19 RCTs, n=43,943 | ↔RR 1.05 (0.96-1.15) | 0% | [85]. |
| All-cause Mortality in Patients with CAD | 19 RCTs, n=43,943 | ↔RR 0.84 (0.69-1.01) | 0% | [85]. |
| MDRO Colonization | 26 observational studies, n=29,382 | ↑OR 1.74 (95% CI 1.40-2.16) | 68% | [94]. |
| CDI, Incident | 42 observational studies, n=313,000 | ↑OR 1.74 (1.47-2.85) | 85% | [101]. |
| CDI, Recurrent | 42 observational studies, n=313,000 | ↑OR 2.51 (1.16-5.44) | 78% | [101]. |
| CDI, Recurrent | 16 observational studies, n=57,477 | ↑OR 1.69 (1.46-1.96) | 56% | [106]. |
| SIBO | 19 observational studies, n=7,055 | ↑OR 1.71 (1.20-2.43) | 84% | [118]. |
| SBP in Cirrhosis | 17 observational studies, n=8,204 | ↑OR 2.17 (1.46-3.23) | 86% | [120]. |
| HE in Cirrhosis | 7 observational studies, n=4,574 | ↑OR 1.50 (1.25-1.75) | 14% | [127]. |
| CAP | 13 observational studies, n=2,098,804 | ↑OR 1.37 (1.22-1.53) | 88% | [128]. |
| Severe COVID-19 | 12 observational studies, n=290,455 | ↑OR 1.85 (1.13-3.03) | 90% | [134]. |
| Gastric Cancer | 24 observational studies, n=8,066,349 | ↑RR 1.82 (1.46-2.29) | 95% | [137]. |
| Colorectal Cancer | 24 observational studies, n=8,066,349 | ↔RR 1.22 (0.95-1.55) | 97% | [137]. |
| Hepatocellular Carcinoma | 24 observational studies, n=2,741,853 | ↑OR 1.69 (1.30-2.20) | 94% | [138]. |
| Biliary Tract Cancers | 24 observational studies, n=2,741,853 | ↑OR 1.79 (1.63-1.97) | 42% | [138]. |
| Pancreatic Cancers | 24 observational studies, n=2,741,853 | ↑OR 1.61 (1.23-2.11) | 99% | [138]. |
| AKI | 7 observational studies, n=2,404,236 | ↑RR 1.61 (1.16-2.22) | 98% | [142]. |
| CKD | 12 observational studies and 1 RCT, n=1,144,056 | ↑HR 1.26 (1.16-1.38) | 87% | [143]. |
| Dementia | 16 observational studies and 1 RCT, n=1,251,562 | ↔HR 0.98 (CI 0.85-1.13) | 99% | [152]. |
| Microscopic Colitis | 13 observational studies, n=304,482 | ↑OR 2.65 (1.81-3.50) | 98% | [159]. |
For effect size, ↑ indicates significantly increased risk with PPI use, and ↔ indicates no statistically significant difference. For I², red shading indicates high heterogeneity (I² ≥50%), yellow indicates moderate heterogeneity (I² 25-49%), and green indicates no significant heterogeneity (I² <25%).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



