Submitted:
26 May 2025
Posted:
26 May 2025
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Introduction
World Health Organization (WHO) has recommended widespread vaccination to prevent the coronavirus disease 2019 (COVID-19) pandemic. At the moment, vaccines from different manufacturers, with different composition and mechanism of action are available on the world market. Due to the urgency and necessity for the production of large quantities of vaccines, they have undergone short clinical trials, but it is still necessary to monitor the occurrence of side effects for at least five years (post-marketing surveillance).
Case report
Patient No. 1, a 47-year-old female, was vaccinated twice against COVID -19 with the AstraZeneca vaccine and her Anti-TPO antibodies increased 10-fold three months after receiving the second dose. Concentration of T4 was at the lower limit and TSH titer was elevated. One month after receiving the third dose, Pfizer -BioNtech vaccine, based on the clinical picture and laboratory tests, she was diagnosed with Hashimoto’s disease.
Patient No. 2, a 47-year-old male, has received two doses of Sinopharm vaccine against COVID-19. On regular physical examination, ultrasound revealed micro-nodules in the thyroid gland. Laboratory tests showed an increased titer of Anti- TPO antibodies with a preserved hormonal status of the thyroid gland. After receiving the third dose of the same vaccine, the Anti -TPO titer remained at the previous level.
Conclusion
In some patients, vaccines against COVID-19 may increase the titer of Thyroid autoimmune antibodies leading to subclinical or clinical manifestations of Hashimoto's disease. The reasons are specific action of different types of vaccines, the overdose of vaccines in relation to body mass index as well as the place of vaccine application. It is recommended to monitor for a while the titer of anti-thyroid antibodies in persons vaccinated against COVID-19.
Keywords:
Hashimoto's disease
; COVID-19
; AstraZeneka
; Pfizer-BioNTech
; Sinopharm
1. Introduction
The thyroid produces hormones that help regulate the metabolism of carbohydrates, lipids and proteins. There are two forms of acute and chronic thyroiditis, namely hyperthyroidism (Morbus Graves-Basedowii) and hypothyroidism (Hashimoto’s disease). At the root of these diseases is autoantibody-mediated lymphocyte cytotoxicity.
Mankind has encountered a major COVID-19 pandemic. In addition to the use of appropriate drugs in the therapy, vaccines from various manufacturers are widely used in the prevention of the disease. The primary role of vaccines would be alleviation of severe symptoms and to stop the spreading of infection, thus reducing the percentage of the sick persons. However, in addition to the mentioned benefits, vaccines can also cause certain harmful effects on the recipient’s health. Just as other vaccines against certain viruses (human papillomavirus, influenza and hepatitis B) can cause autoimmune diseases such as Graves’ disease and Hashimoto’s thyroiditis, vaccines against COVID-19 can lead to autoimmunity that is primarily directed against thyroid gland [1].
Some authors explain the development of autoimmunity by the harmful effects of adjuvants, commonly used in vaccines to potentiate the immune response. If the animal is injected with its own thyroglobulin mixed with Freund’s adjuvant (emulsion of mineral oil, acid-resistant microorganisms and emulsifiers), lymphocytic infiltration of the thyroid gland occurs [2]. Cases where patients developed autoimmunity to the thyroid gland (elevated anti-thyroid antibodies, disorder of thyroid hormone secretion) a few days after vaccination have been reported. A case of subacute thyroiditis after receiving Pfizer-BioNTech mRNA vaccine for COVID-19 has also been reported [3]. As a consequence of subacute thyroiditis, fever occurs in 28-83% of cases [4]. Anaphylactic shock have been reported following the administration of the Pfizer-BioNTech vaccine [5], which is a common occurrence and a reaction of some patients to the presence of polyethylene glycol ( PEG), adjuvant in the vaccine. Other adjuvants such as silicones and mineral oils can also cause severe clinical manifestations that can endanger the patient’s life [6].
Thyroid hormones are necessary for a normal, active life. The thyroid gland is highly susceptible to autoimmunity and it is influenced by various environmental factors (iodine, selenium, tobacco smoke), contagious diseases and certain drugs [7]. It has been hypothesized that different genes are responsible for the increased prevalence of thyroid disease [8].
Autoimmune thyroid diseases, such as Hashimoto’s thyroiditis, which causes hypothyroidism, and Graves’ disease, which causes hyperthyroidism, affect about 5% of the human population. Both diseases are characterized by infiltration of the thyroid by T and B lymphocytes and the production of thyroid autoantibodies directed against thyroid peroxidase (anti-TPO), thyroglobulin (anti-TG) and TSH receptors (TRABs) [9,10].
COVID-19 in the acute and convalescent phase, beside damage of other organs, can disrupt the normal function of the thyroid gland [11,12,13]. About 20% of patients after COVID-19 in the recovery phase had an increased concentration of autoantibodies to thyroid peroxidase (Anti-TPO), which suggests the onset of autoimmune thyroid disease [14]. After acute COVID-19 illness, most patients recover from thyroid dysfunction; however, anti TPO antibodies remain present. Some authors have tried to attribute the presence of anti-TPOAb in patients with long COVID (LC) to a protective role in the acute phase of COVID-19 [15].
In long-term clinical practice, it is known that as a consequence of autoimmune thyroiditis or Hashimoto’s disease, hypothyroidism or normal levels of thyroid hormones in the blood and increased TSH concentration occur. T cytotoxic lymphocytes destroy the thyroid gland with activated T helper lymphocytes. The main diagnostic character of this disease is the chronic existence of Anti TPO and anti TG antibodies produced by B lymphocytes [16,17].
In this paper, two cases of autoimmune thyroid disease (Hashimoto’s thyroiditis,) that are thought to be a consequence of vaccination against COVID-19 are presented. Also, the paper contains hypotheses explaining the reasons and possible mechanisms leading to autoimmune thyroid attack in vaccinated persons.
2. Case Description
2.1. Case 1
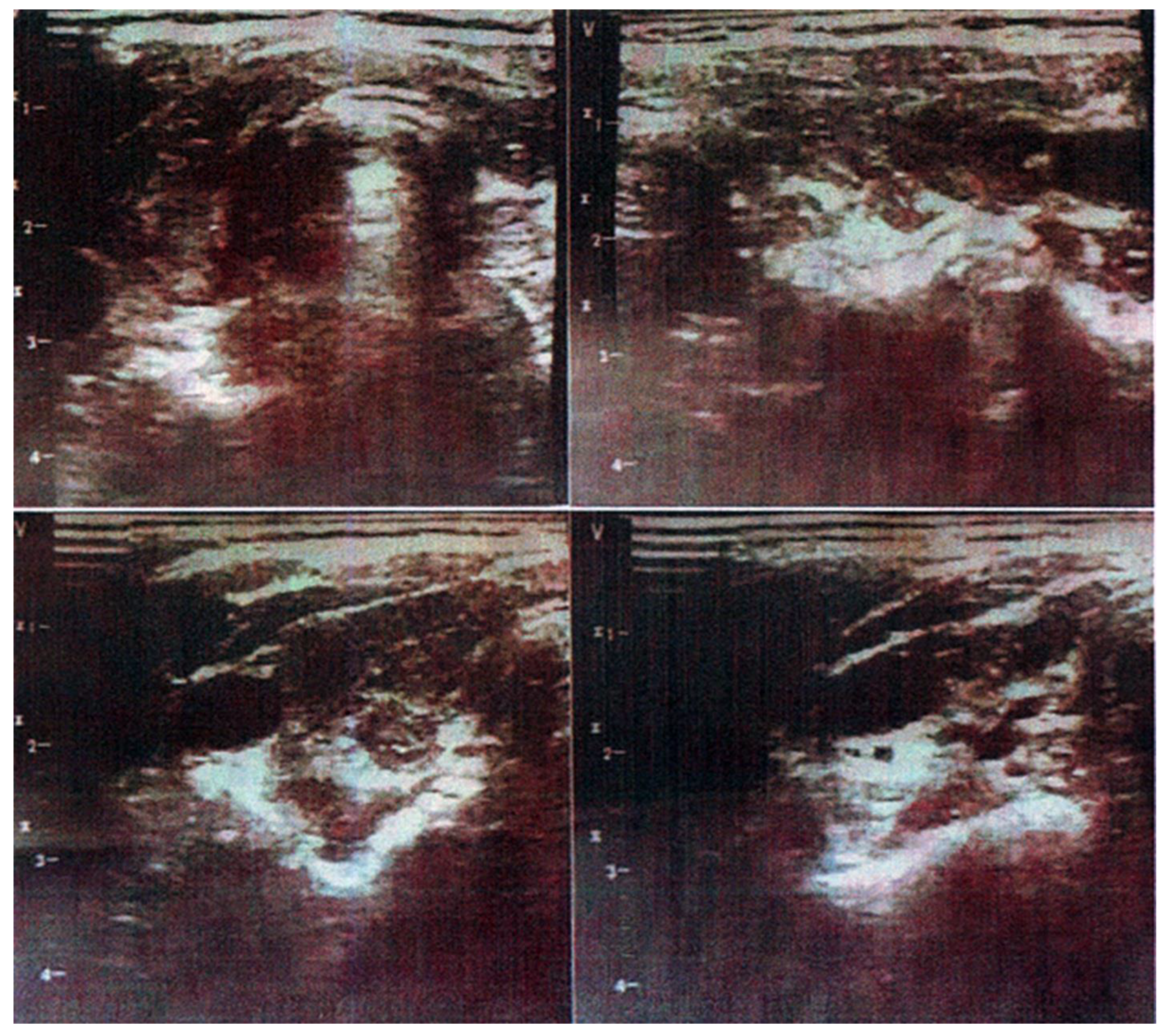
A 47-year-old woman, BMI = 19.15 (normal body weight) received AstraZeneka / Covishield (Manufactured and batch number: Serum Ins. Of India PVT, LTD, 4120Z001) vaccine against COVID-19 on 27.02.2021. and the second dose on 21.05.2021. (AstraZeneca B.V., the Netherlands, ABX3115). She received the third dose on November 19, 2021, Pfizer-BioNTech manufactured by BioNtech-Manufacturing GMBH, FF2832; (Table 1). At the end of September, the patient felt drowsy, intolerance to cold, neck stiffness and on her own initiative she did thyroid ultrasound and analysis of thyroid hormones. Level of T4 was at the lower reference limit (57.9 nmol / L) and TSH concentration was elevated (16.7) (Graph 1). Immunohistochemical method showed that level of Anti-TPO antibodies was increased 10-fold (309.5 IU / ml), while the level of Anti TG antibodies was within reference limits. At the beginning of 2022, there was a sharp increase in Anti-TPO antibodies and the concentration was 1326.00 (Table 1). At the Clinic for Endocrinology, Diabetes and Metabolic Diseases, Haschimoto’s disease (chronic thyroiditis) was diagnosed and she was introduced to hormone replacement therapy. Family history showed two cases of thyroid disease (mother and sister).
Figure 1.
Thyroid Ultrasound of Patient No 1.Presentation of an ultrasound image of the thyroid gland With an observed chronic inflammatory process.
Figure 1.
Thyroid Ultrasound of Patient No 1.Presentation of an ultrasound image of the thyroid gland With an observed chronic inflammatory process.
2.2. Case 2
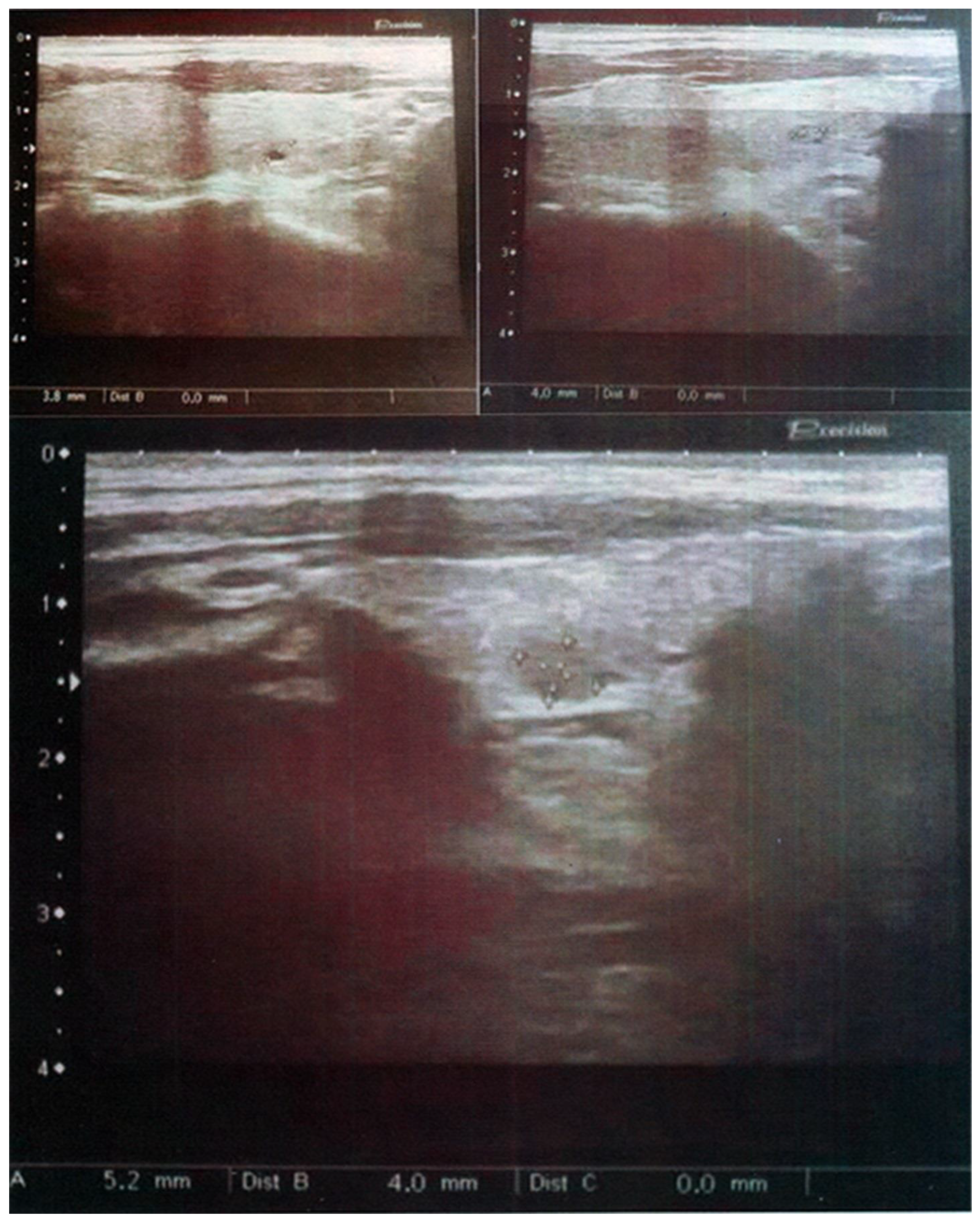
A 47-year-old man, BMI=23.7 (normal body weight) received three vaccines against COVID-19 on 24.01; 14.02; 19.11. 2011 (Table 1). All three doses were Sinopharm type, manufactured by Beijing Institute of B.P., LTD, 202012191; 202012194; 2021082808. On regular annual physical examination (September 2021), thyroid ultrasound showed several 4-5 mm micro-nodules in both, left and right thyroid lobes and the patient was advised for further hormonal analysis and analysis of Anti -TPO and Anti-TG antibodies (Graph 2). The patient did not have any complications and clinical manifestations of thyrotoxicosis. A routine blood test revealed slight increased cholesterol and HDL cholesterol. After laboratory analysis of blood, normal hormonal status of the thyroid gland was established with an increased titer of antibodies to thyroid peroxidase (Anti-TPO = 187IU / ml). After two months, anti -TPO values were similar (Anti TPO = 180.4) (Table 1). The patient was admitted At the Clinic for Endocrinology, Diabetes and Metabolic Diseases in February 2022, where he was diagnosed with an initial stage of Hashimoto’s disease was not given therapy and was advised to have a thyroid examination once a year. The patient denied the existence of a family history of thyroid disease.
Both patients used Thyroxyl supplementation, one capsule daily, from the time they were diagnosed with thyroid problems until they arrived at the Clinic for Endocrinology, Diabetes and Metabolic Diseases (two months).
Figure 2.
Thyroid Ultrasound of Patient No 2.In the left and right lobes of the thyroid gland, micronodules up to 5 mm in size were observed.
Figure 2.
Thyroid Ultrasound of Patient No 2.In the left and right lobes of the thyroid gland, micronodules up to 5 mm in size were observed.
3. Discussion
In both presented cases, patients have normal weight (BMI). Giving the same dose of vaccine to patients with different body weights is a major problem in the vaccination process. It was observed that patients with lower body weight had strong responses to the second dose of vaccine, while larger and heavier people with higher BMI tolerated it more easily. The answer lies in the different amount of blood in lighter and heavier recipients, where heavier patients have more blood (7% of total body weight) and since the same dose of vaccine is given, patients with lower body weight are expected to have higher concentrations of antigen per liter of blood. Higher antigen concentration also causes a more intense immune response of the recipient.
Due to cases of certain unwanted and adverse reactions to vaccines against COVID-19 [5], the use of the vaccine in people with a family history of type 1 diabetes, Hashimoto’s disease, lupus and rheumatoid arthritis should be excluded.
The vaccine is used to introduce virus in the body so it can react more easily to potential contact. Therefore, it is my opinion that it is not necessary to give a second dose at all, especially not a booster dose, because these are futile attempts to create a longer and lasting immunity to the SARS-CoV-2 virus and the damage can be long-lasting and immeasurable. It is especially absurd in the world of medicine to give vaccines every few months in order to maintain active humoral immunity. By reacting to the virus infection, the organism proves that cellular immunity exists, that there are memory B lymphocytes that are the key to a quick response to viral infection.
Theoretically, the question of the origin of the virus itself arises, because the reactions are very strange. If the virus exists since 1960s and circulates in the human population, then contact with the virus would cause a mild reaction. If the virus is created in the laboratory and represents something new, unknown to the immune system, then a more violent immune reaction should be expected with a possible fatal outcome [18]. In this case, the first dose of vaccine may be justified for recognition and adaptation of organism to the new virus (something similar are allergic reactions, some people have antibodies to allergens and some do not). However, we must be aware that our body will react to any substance of biological or chemical origin that we encounter for the first time. Immunity is learned and acquired over the years, especially in childhood, in children ages 1-5 years [18].
Vaccines give active immunity (circulating antibodies in the blood) up to three months. Revaccination is just a test of a stronger immune response to the virus. Vaccine administration causes an increased synthesis of the antibodies specific to the introduced antigen; the second dose 4 weeks after the first and the third dose after 6 weeks, drastically increases the circulating antibodies of the IgG class (Table). However, the question is what harmful consequences can result from such a quantity of circulating antibodies in the recipient’s blood. Adjuvants in vaccines can cause anaphylactic shock [5,6], increased antigen concentration and repeated irritation of the immune system, leading to disorders and overexertion of the Homeostatic Immune System [18] and excess production of antibodies. This can lead to errors in Ab synthesis, creating Abs that attack its own antigens on the cell surface, thus causing the occurrence of autoimmunity.
In the patient No. 1 thyroid cell damage and increased synthesis of Anti -TPO Ab was noticed after the third dose of mRNA vaccine. A similar finding has been confirmed by other authors [3]. This type of vaccine is in the form of lipid granules that can via blood infiltrate nonspecific into any somatic cell of the recipient (muscle, nerve and in this case, thyroid cells). The immune system destroys cells expressing viral proteins on their surface causes the destruction of cells itself, so that unwanted damage to different types of cells can occur. Therefore, the use of RNA vaccines and possible adverse effects should be reconsidered. In the case of the vaccines against COVID-19, it is justified that the intake of the vaccine follows the natural intake of the virus in this case, nasal mucosa. It is desirable that an immunological reaction takes place on the mucosa of the upper respiratory organs, which will undoubtedly damage the infected cells, but the mucosal cells have a great power of regeneration unlike other somatic cells./*greater regeneration power than other somatic cells.
Although only two cases are presented in this paper, the author is familiar with many cases of Hasimoto’s disease after receiving vaccines for COVID-19 from the immediate environment. Therefore, it is necessary to inform health public about possible side effects such as Hashimoto’s thyroiditis. The onset of the disease is quiet and unnoticeable for years until there is an imbalance of thyroid hormones and hypothyroidism.
Author Contributions
Conceptualization, D.N.; methodology, D.G. and J.J.; software, D.M.; validation, D.N., I.S., D.M, D.G and J.J.; formal Analysis, D.N.; investigation, D.N., D.G. and J.J..; data curation, D.N..; writing—original draft preparation, D.N.; writing—review and editing, D.N.; visualization, D.N.; supervision, D.N. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
To exclude this statement.
Conflicts of Interest
The authors declare no conflicts of interest.
Acknowledgments
This work was supported by the Ministry of Education, Science and Technological Development of the Republic of Serbia (grant No. 200110).
References
- Giusti M, Maio A. Acute thyroid swelling with severe hypothyroid myxoedema after COVID-19 vaccination. Clinical Case Reports. (2021) 9(12). [CrossRef]
- Vera-Lastra O, Ordinola Navarro A, Cruz Domiguez MP, Medina G, Sánchez Valadez TI, Jara LJ. Two Cases of Graves’ Disease Following SARS-CoV-2 Vaccination: An Autoimmune/Inflammatory Syndrome Induced by Adjuvants. Thyroid. (2021) 31(9):1436–9. [CrossRef]
- Franquemont S, Galvez J. Subacute Thyroiditis After mRNA Vaccine for Covid-19. Journal of the Endocrine Society. (2021) 5(Supplement_1):A956–7. [CrossRef]
- Bahl S, Babu PM, Capatana F, Khan I, Adlan M, Premawardhana LDKE. Sub-Acute Thyroiditis Presenting as Pyrexia of Uknown Origin. Journal of the Endocrine Society. (2021) 5(Supplement_1):A956–6. [CrossRef]
- Castells MC, Phillips EJ. Maintaining Safety with SARS-CoV-2 Vaccines. Longo DL, editor. New England Journal of Medicine. (2021) 384(7):643–9. [CrossRef]
- Bragazzi NL, Hejly A, Watad A, Adawi M, Amital H, Shoenfeld Y. ASIA syndrome and endocrine autoimmune disorders. Best Practice & Research Clinical Endocrinology & Metabolism. (2020) 34(1):101412. [CrossRef]
- Saranac L, Zivanovic S, Bjelakovic B, Stamenkovic H, Novak M, Kamenov B. Why Is the Thyroid So Prone to Autoimmune Disease. Hormone Research in Paediatrics. (2011) 75(3):157–65. [CrossRef]
- Casto C, Pepe G, Li Pomi A, Corica D, Aversa T, Wasniewska M. Hashimoto’s Thyroiditis and Graves’ Disease in Genetic Syndromes in Pediatric Age. Genes. (2021) 12(2):222. [CrossRef]
- Jacobson DL, Gange SJ, Rose NR, Graham NMH. Epidemiology and Estimated Population Burden of Selected Autoimmune Diseases in the United States. Clinical Immunology and Immunopathology. (1997) 84(3):223–43. [CrossRef]
- Cappa M, Bizzarri C, Crea F. Autoimmune Thyroid Diseases in Children. Journal of Thyroid Research. (2011) 2011:1–13. [CrossRef]
- Hussain M, Jabeen N, Raza F, Shabbir S, Baig AA, Amanullah A, et al. Structural Variations in Human ACE2 may Influence its Binding with SARS-CoV-2 Spike Protein. Journal of Medical Virology. (2020) 92(9). [CrossRef]
- Nalbandian A, Sehgal K, Gupta A, Madhavan MV, McGroder C, Stevens JS, et al. Post-acute COVID-19 syndrome. Nature Medicine. (2021) 27(4):1–15. [CrossRef]
- Boaventura P, Macedo S, Ribeiro F, Jaconiano S, Soares P. Post-COVID-19 Condition: Where Are We Now? Life. (2022) 12(4):517. [CrossRef]
- Murugan AK, Alzahrani AS. SARS-CoV-2: Emerging Role in the Pathogenesis of Various Thyroid Diseases. Journal of Inflammation Research. (2021) Volume 14:6191–221. [CrossRef]
- Lui DTW, Lee CH, Chow WS, Lee ACH, Tam AR, Pang P, et al. Long COVID in Patients With Mild to Moderate Disease: Do Thyroid Function and Autoimmunity Play a Role? Endocrine Practice. (2021) 27(9):894–902. [CrossRef]
- Caturegli P, De Remigis A, Rose NR. Hashimoto thyroiditis: Clinical and diagnostic criteria. Autoimmunity Reviews. (2014) 13(4-5):391–7. [CrossRef]
- Groenewegen KL, Mooij CF, van Trotsenburg ASP. Persisting symptoms in patients with Hashimoto’s disease despite normal thyroid hormone levels: Does thyroid autoimmunity play a role? A systematic review. Journal of Translational Autoimmunity. (2021) 4:100101. [CrossRef]
- Nikolic DM. Covid-19: A Hypothetical View on Infection. Virology & Immunology Journal. (2020) 4(2):1–3. [CrossRef]

Table 1.
Presentation of laboratory hormonal and immunological parameters.
| Patient No 1 | Patient No 2 | |||||
| Type and date of vaccination | 1. AstraZeneca (27.02.2021.) 2. AstraZeneka (21.05.2021.) 3. Pfizer BioNTech (19.11.2021.) |
1.Sinopharm (24.01.2021.) 2. Sinopharm (14.02.2021.) 3. Sinopharm (19.11.2021.) |
||||
| Date of analysis | 28.09.2021. | 4.01.2022. | 21.09.2021. | 10.12.2021. | ||
| Parameters | Value | Value | Reference value | Value | Value | Reference value |
| T3 | 1.21 | 1.09 | 1.10-3.10 | 4.56 | 3.1-6.8 | |
| T4 | 57.9 | 69.88 | 58.0-161.0 | 17.08 | 12-22 | |
| TSH | 16.700 | 25.49 | 0.400-4.00 | 0.400-4.00 | ||
| Anti TPO | 309.5 | 1326.00 | ≤34 | 187.00 | 180.4 | ≤34 |
| Anti Tg | 79.61 | ≤115 | 33.82 | ≤115 | ||
| BMI | 19.15 (normal body weight) | 23.7 (normal body weight) | ||||
The table shows the type of Covid vaccine, the time of immunization, the levels of hormones T3, T4, TSH and antibody concentrations.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



